 Mitja Krajnc1,2*
Mitja Krajnc1,2* Andrijana Koceva
Andrijana Koceva- 1Department of Endocrinology and Diabetology, Clinic of Internal Medicine, University Medical Centre Maribor, Maribor, Slovenia
- 2Faculty of Medicine, University of Maribor, Maribor, Slovenia
Background: Clinical obesity is a prevalent chronic disease, significantly increasing morbidity and mortality while impairing quality of life. As diet and physical activity interventions often prove ineffective in the long term, with increasing use of pharmacotherapy, drug shortages and injection aversion present a challenge. The role of oral semaglutide at a dose of 14 mg (registered for type 2 diabetes) as a treatment for obesity in patients without diabetes remains undefined.
Methods: In the retrospective real-world study, which included 93 adults without diabetes (57% women, average age 52 years), we assessed whether treatment with 14 mg oral semaglutide over one year is associated with lower body weight, body mass index (BMI), waist circumference, blood pressure, heart rate, and obesity staging according to EOSS.
Results: Of the 93 subjects recruited, 82 (88%) were receiving oral semaglutide at a dose of 14 mg after one year. After one year of treatment body weight was significantly lower by 5.7% (5.9 kg) in completers, and BMI decreased significantly by an average of 2 kg/m². There was also a significant reduction in waist circumference by 5.5 cm and a decrease in EOSS score by 0.1. Clinically significant weight loss was achieved in 46% of all participants, with rare individuals experiencing a decrease of ≥ 15%. Adverse effects were mostly mild, with nausea reported by 23% and vomiting and diarrhoea by 12% of participants.
Conclusions: Obesity treatment with oral semaglutide at a dose of 14 mg showed marked interindividual variability, with approximately half achieving clinically significant reductions – mostly under 10%. Although less effective than injectable therapy, oral semaglutide at a dose of 14 mg had a favorable safety profile and may be suitable in selected clinical scenarios.
1 Introduction
Globally, 13% of adults are obese, while in Slovenia, based on data from 2020, approximately 20% of adults aged 25 to 74 are obese, and 39% are overweight (1, 2). Obesity is significantly associated with adverse health outcomes, quality of life and increased mortality. Clinically, its definition is based on the body mass index (BMI), which is calculated as the ratio of body weight to the square of height. In Caucasian individuals, a BMI of 30 kg/m² or higher is considered obese, although the known limitations of BMI must be acknowledged (1, 3). Abdominal fat distribution, e.g. measured by waist circumference, is independently associated with cardiovascular disease and mortality, regardless of BMI (4).
In obesity management, apart from assessing nutritional status and physical capacity, it is crucial to identify individual causes and contributing factors and evaluate medical, functional, and psychological complications (5, 6). The Edmonton Obesity Staging System (EOSS) is commonly used to assess obesity severity. Higher EOSS categories are independently associated with greater overall and specific mortality in individuals with obesity (7). The primary goal of obesity treatment is to improve health, with weight monitoring serving as a proxy indicator of treatment efficacy. A weight loss of at least 5% is considered clinically significant, while a 15% reduction effectively improves most obesity-related complications and conditions. The target weight loss varies depending on the specific complications associated with obesity (1, 6, 8).
The foundation of obesity treatment is lifestyle modification, the long-term effectivness of which is often limited and insufficient, even in intensive lifestyle programs. Pharmacological intervention is indicated for individuals with obesity (BMI > 30) or overweight (BMI > 27) if comorbidities are present (9–11). Semaglutide is a synthetic GLP-1 receptor agonist (GLP-1 RA). It mimics the action of the natural hormone but has improved stability and a longer half-life, allowing for less frequent dosing (12). Semaglutide is the active ingredient in Ozempic® and Rybelsus®, which are registered for type 2 diabetes treatment and Wegovy®, which is indicated for obesity treatment. Wegovy pens contain higher doses of semaglutide (up to 2.4 mg weekly), whereas the maximum Ozempic dose is 1 mg weekly (13, 14). Beyond their beneficial effects on blood glucose and weight, GLP-1 RAs are associated with a reduced risk of numerous conditions, including cardiovascular events and a reduction in mortality (16). Oral semaglutide (Rybelsus®) is currently approved for the treatment of adults with type 2 diabetes who have not achieved adequate glycemic control with non-pharmacological measures. It is available in three daily doses (3 mg, 7 mg, and 14 mg), with dose escalation every four or more weeks (15). The efficacy and safety of oral semaglutide (Rybelsus) for type 2 diabetes have been extensively studied in the PIONEER trials (17) and a 14 mg daily dose of Rybelsus is considered equivalent to 0.5 mg Ozempic weekly, although oral absorption variability is significantly higher (18). Favorable results on weight have been reported for higher doses of oral semaglutide (25 and 50 mg daily), which are not yet in clinical use (19). And injectable semaglutide has demonstrated significant weight loss efficacy with mild to moderate gastrointestinal-related side effects and treatment discontinuation in only 7% of participants (20).
In Slovenia, access to effective obesity medications remains limited and pharmacological obesity treatment is not reimbursed. Wegovy® is unavailable, Ozempic® is difficult to obtain due to global shortages (21), and tirzepatide is newly available but at a higher price. Many patients proactively request semaglutide tablets for weight loss. A review of existing literature using keywords such as oral semaglutide, obesity and weight loss revealed a lack of reliable data on the use and efficacy of oral semaglutide, at doses approved for type 2 diabetes, in individuals with obesity but without diabetes. In response, we retrospectively evaluated the efficacy and safety of oral semaglutide at a dose of 14 mg for obesity treatment in this population.
2 Materials and methods
2.1 Study design and population
Our study was retrospective and observational, based on real-world data from clinical practice. We reviewed and analyzed available medical records (both electronic and paper-based reports) of adults (aged ≥ 18 years) who, by current professional guidelines for obesity treatment (8, 9, 11), were prescribed oral semaglutide (Rybelsus) between 2021 and 2023 for obesity treatment (defined as a BMI ≥30 kg/m²). The prescribed treatment followed the dosing regimen for type 2 diabetes: 3 mg on an empty stomach for the first 30 days, 7 mg on an empty stomach for the next 30 days (second month), and 14 mg on an empty stomach daily from the third month onward. Participants were managed in one of two specialized endocrinology outpatient clinics (either in a hospital or a private center) where obesity management is routinely conducted.
We excluded individuals with concomitant diabetes of any type, those who were overweight or had normal body weight, and individuals with confirmed or suspected syndromic or monogenic obesity. We also excluded individuals whose BMI was likely attributable to increased muscle mass rather than excess body fat, as BMI may overestimate obesity in such cases. The contraindications and precautions stated in the approved Summary of Product Characteristics were considered during prescription (18). Women of childbearing potential were advised to use a reliable method of contraception during the treatment period.
After reviewing the medical records of all patients prescribed oral semaglutide for obesity in both outpatient clinics, we included those who provided informed consent for data collection and analysis in the study. Participants were eligible if we had the following data available at the start of treatment (day 0) and at the follow-up after one year (365 ± 14 days):
● Before treatment initiation: sex, age (years), body weight (kg), waist circumference (cm), height (cm), body mass index (BMI), systolic and diastolic blood pressure, heart rate, and Edmonton Obesity Staging System (EOSS) score.
● After one year for those taking Rybelsus 14 mg daily: age (years), body weight (kg), waist circumference (cm), height (cm), BMI, systolic and diastolic blood pressure, heart rate, adverse effects related to the medication (type, severity), and EOSS score.
● After one year for those who discontinued or did not reach the 14 mg dose: adverse effects related to the medication (type, severity) and reason for treatment discontinuation.
The study included 93 individuals. During the first outpatient visit, participants received a brief (approximately 30-minute) focused counselling on non-pharmacological treatment of obesity, based on national guidelines (11). This included dietary advice and recommendations regarding physical activity. All patients were also encouraged to enroll in a free structured, multidisciplinary lifestyle modification weight loss program at a local health center. The program, consisting of 30 sessions over 4 months, focuses on acquiring practical knowledge and skills to change dietary and physical activity habits and provides cognitive-behavioural psychological support.
Body weight measurements were performed using a calibrated personal scale, verified by an accredited laboratory. Participants were advised to fast before weighing. Body weight results were rounded to the nearest kilogram. Height was measured in a standing position from the crown of the head to the soles of the feet and rounded to the nearest centimeter. BMI was calculated using the standard formula. Waist circumference was measured following WHO recommendations, at the midpoint between the lowest palpable rib and the highest point of the iliac crest, rounded to the nearest centimeter. Systolic and diastolic blood pressure and heart rate were measured using a calibrated automatic upper-arm blood pressure monitor employing the oscillometric method, following the guidelines of the European Society of Cardiology (22). The EOSS obesity staging score was assessed by an endocrinologist based on published criteria (23).
Due to the retrospective nature of the study, no medical interventions were performed on participants as part of the research, all data used in the study had been collected during routine outpatient care. The medication had been prescribed by endocrinologist involved in obesity treatment, with the participants’ consent and agreement. Although semaglutide has well-documented clinical benefits, participants were informed that oral semaglutide, unlike the injectable form, is not officially approved for obesity treatment. All participants provided informed consent for data collection and analysis in an anonymized format, obtained by their treating specialist. Our institution’s Medical Ethics Committee ethically reviewed and approved the study.
2.2 Statistical analysis
We conducted a power analysis for the study, considering a minimally relevant effect size (δ) of a 5 kg weight change, a two-tailed test, a minimum desired power of 0.9, and α = 0.05. Using a paired t-test, we determined that the sample size in our study was statistically sufficient.
The Shapiro-Wilk test was used to assess the normality of variable distributions and the distribution of differences in values before and after treatment. Normally distributed variables were described using the mean and standard deviation, while non-normally distributed variables were reported using the median and interquartile range.
Relative changes in body weight were calculated using the formula:
We categorized participants based on their weight loss percentages (≥5%, 10%, and 15%) and reported the proportions of individuals experiencing specific adverse effects at mild, moderate, or severe levels. To compare pre- and post-treatment data, we used the paired Student’s t-test when the assumption of normality was met. Otherwise, we applied the Wilcoxon signed-rank test. We also calculated 95% confidence intervals. To compare the subgroups of completers and non-completers, we used the unpaired sample Student’s t-test or the Mann-Whitney U test, respectively.
Statistical analysis was conducted using the latest open-source software, Jamovi (2.6.2), available online at https://www.jamovi.org. A p-value < 0.05 was considered statistically significant.
3 Results
After one year, 82 subjects (88%) were receiving oral semaglutide at a dose of 14 mg (completers), while 11 subjects or 12% (non-completers) had either discontinued treatment earlier due to adverse effects or lack of efficacy, or were taking a lower dose (7 mg daily). Most completers (49%) were initially classified as EOSS stage 2, 28% as stage 1, 17% as stage 3, and one participant as stage 4, the rest as stage 0. Only three participants joined a structured, multidisciplinary lifestyle intervention program, all of which within the first two months of the initial visit.
We compared the baseline characteristics of the subgroups of completers and non-completers. No statistically significant differences were found between the subgroups for any of the characteristics (p>0.05 for all comparisons). Table 1 presents the baseline demographic and clinical characteristics of all participants, while Table 2 presents the differences in assessed parameters and their significance between the baseline and the one-year follow-up in 82 completers.
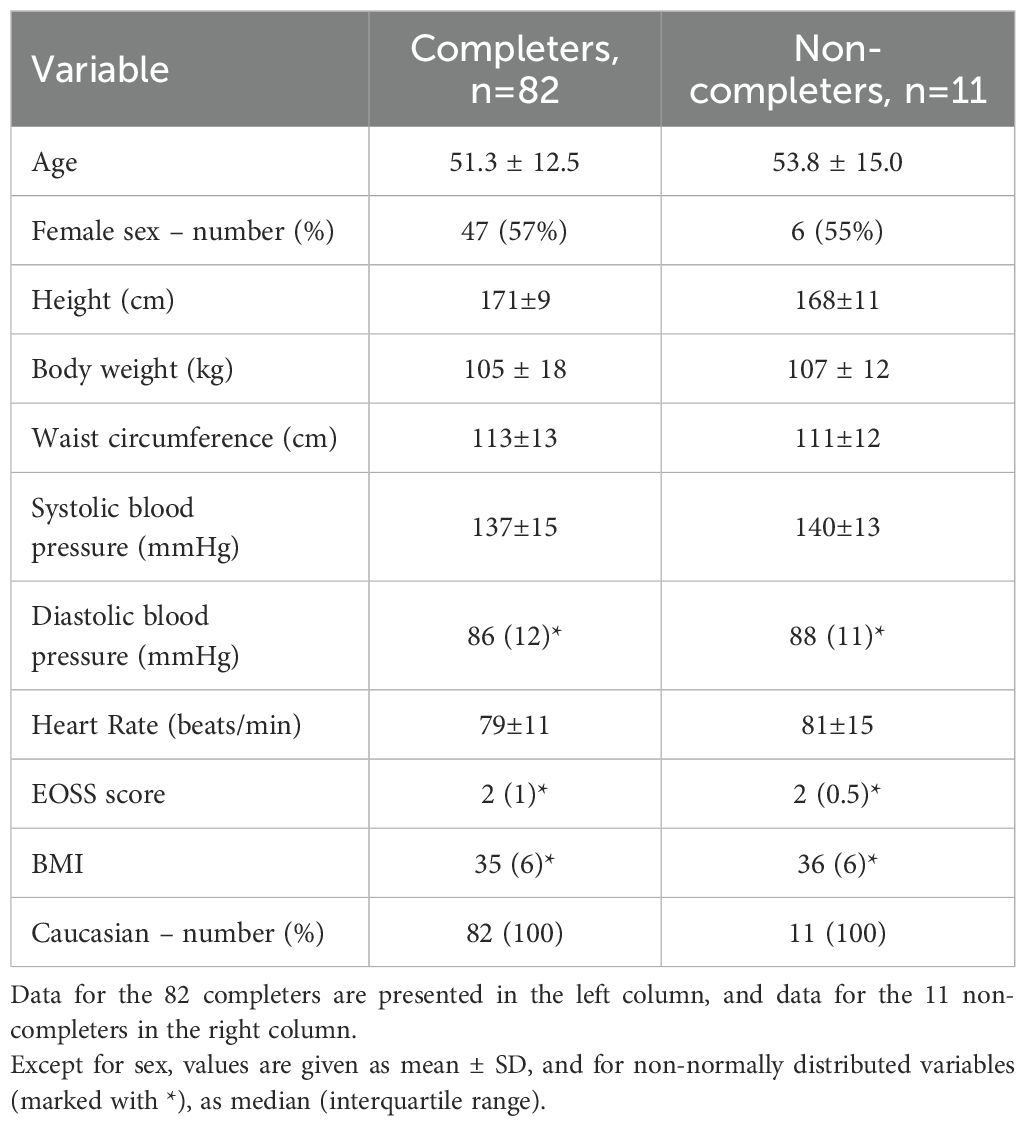
Table 1. Demographic and clinical characteristics of study participants before initiating treatment.
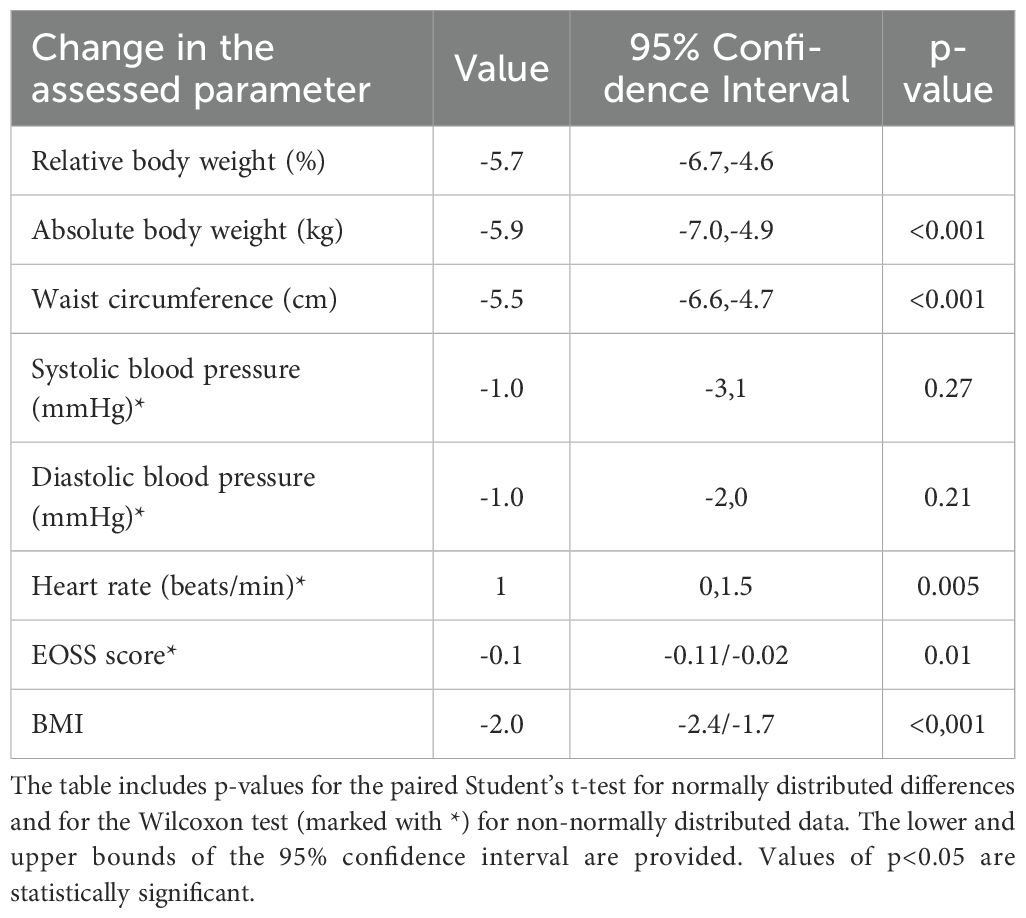
Table 2. Changes in assessed parameters between the one-year follow-up and baseline and their statistical significance in completers (n=82).
The maximal relative weight change in completers was -17%, and the minimal was +3%. After one year, 48% had lost less than 5% of their body weight, while 4% had lost more than 15% of their body weight. Data on distribution of completers by their weight loss categories are presented in Figure 1, while Figure 2 presents the proportion of completers by BMI categories at the baseline and after one year of treatment.

Figure 1. Distribution of completers by weight loss categories (n=82).
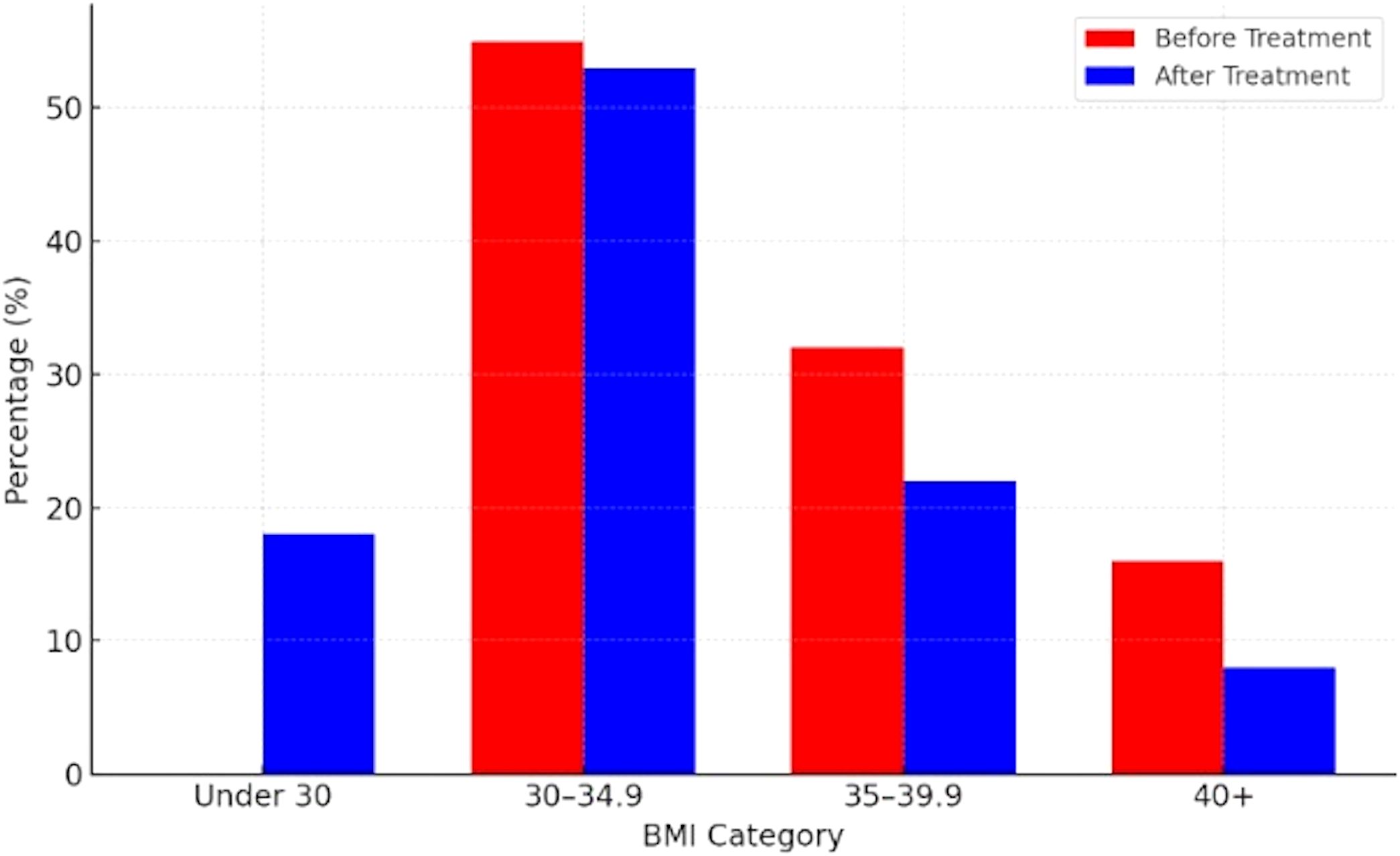
Figure 2. Proportion of completers by BMI category before and after treatment (n=82).
We also observed a significant decrease in waist circumference that was less than with tirzepatide at all maintenance doses, subcutaneous semaglutide 2.4 mg weekly, and oral semaglutide at a dose of 50 mg daily (19, 20, 27). There was also a mild decrease in systolic and diastolic blood pressure, but these changes were not statistically significant. A small but significant increase in the heart rate (by 1 bpm) was noted, which, according to the literature, has no meaningful health implications.
Of the 93 participants in our study, 11 patients (12%) discontinued treatment. Five non-completers discontinued treatment due to self-perceived insufficient weight loss, while six could not take the recommended dose due to adverse effects. Among these six, two experienced severe vomiting at the dose of 14 mg, three had moderate to severe nausea, and one had severe diarrhoea. Of these six, two were taking a lower dose (7 mg) and tolerated it well. The most frequently reported side effect among the completers in our study was nausea, affecting 23% of participants. Vomiting and diarrhoea were the next most common, each affecting 12%. Constipation and nonspecific abdominal pain followed, each reported by 6% of participants. None of the participants experienced hypoglycemia, newly developed or worsened depressive disorders, or newly diagnosed gallbladder diseases. None of the participants experienced a serious adverse event as defined by the European Medicines Agency (EMA) (24), and no confirmed case of acute pancreatitis was found. Table 3 presents reported adverse events that completers attributed to the medication after one year of treatment with oral semaglutide 14 mg daily.
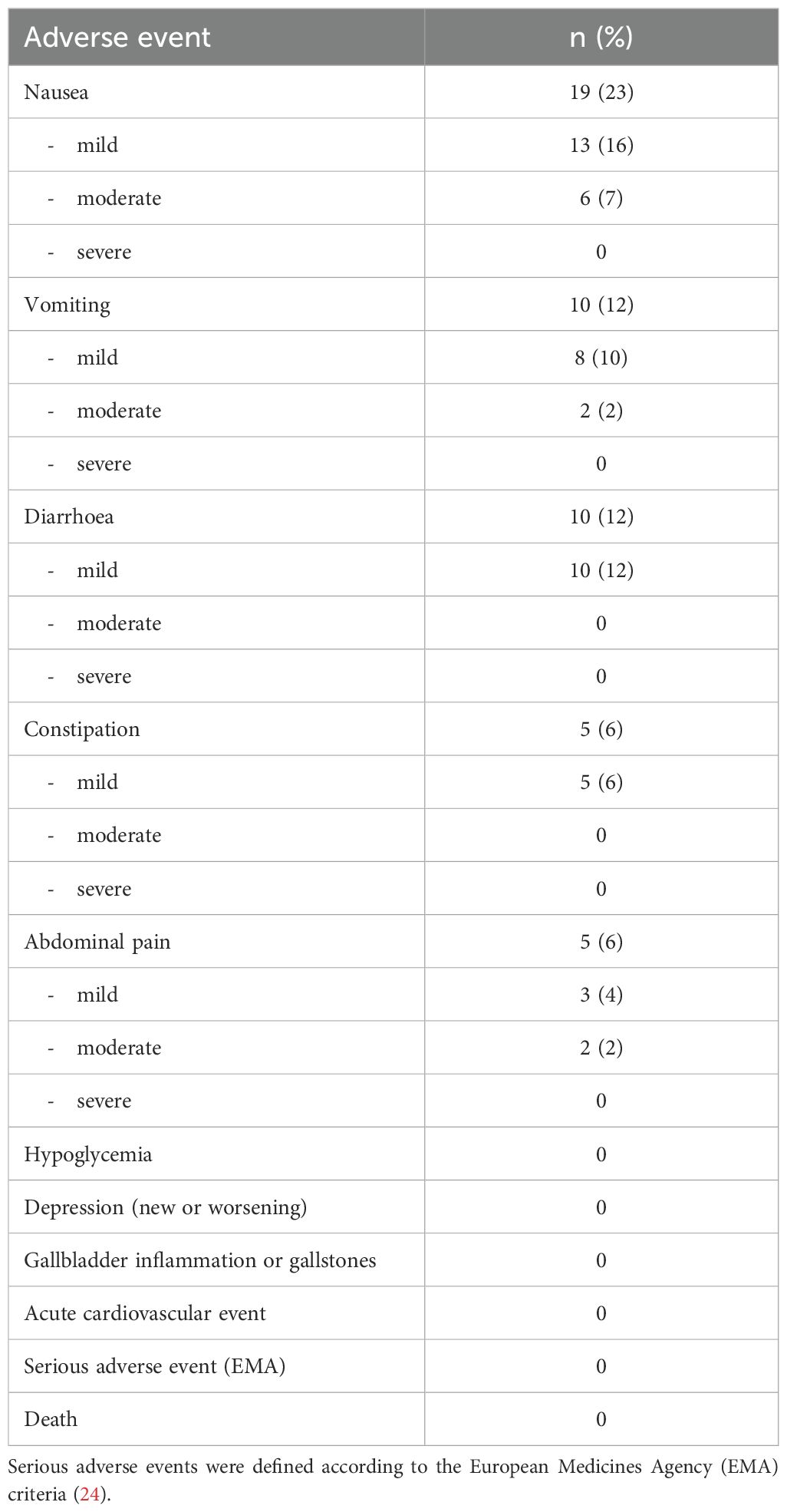
Table 3. Adverse events reported by completers after one year of treatment.
3 Discussion
Eighty-two participants, who continued with 14 mg oral semaglutide (the highest dose registered for managing type 2 diabetes) for one year experienced a significant average weight loss of 5.7% (5.9 kg), along with a reduction in BMI by an average of 2 kg/m². While the average weight loss reached the clinically significant threshold of ≥ 5%, a notable 48% of completers did not meet this criterion. Overall, 54% of all 93 enrolled individuals failed to achieve the 5% weight loss target. Only 4% of completers experienced a weight reduction of 15% or more, which is associated with substantial improvements in various obesity-related negative outcomes (8). Our findings indicate a considerable interindividual variability and relatively modest effect of oral semaglutide ar the studied dose on body weight, which is predominantly mild to moderate.
There are some head-to-head comparative studies between anti-obesity drugs, e.g. for subcutaneous semaglutide and tirzepatide in a large cohort study or subcutaneous semaglutide and liraglutide in a randomized trial (25, 26). For oral semaglutide in adults without diabetes, the following comparisons are based on studies investigating individual drugs, and differences in participant characteristics, study designs, and treatment durations should be noted.
According to our findings and published data, oral semaglutide at a dose of 14 mg is significantly less effective for weight loss in individuals with obesity than tirzepatide (a dual GLP-1 and GIP agonist). In a randomized controlled trial, tirzepatide at doses of 10 mg and 15 mg resulted in an average weight reduction of 20% and 21%, respectively, while the 5 mg dose led to a 15% weight loss, compared to 3% with placebo. Clinically significant weight loss of at least 5% was achieved by 89% and 91% of participants, while 67–71% lost at least 15% of their body weight. Among our participants, nausea incidence was comparable to the lowest maintenance dose of tirzepatide, while fewer reported constipation or diarrhoea (27). Real-world data also indicate that most users of tirzepatide without diabetes lost more than 10% of body weight with an average loss of 12.7% (28).
In a randomized controlled trial invastigating the efficacy of subcutaneous semaglutide injections at a dose of 2.4 mg weekly for obesity treatment, participants experienced an average weight loss of 15% and a BMI reduction by an average of 5.5 kg/m² after 68 weeks (20). More than 86% of participants achieved clinically significant weight loss of at least 5%, and 51% of participants lost over 15% of their body weight (20). Compared to our study, a slightly lower percentage of participants reported nausea (17%), diarrhoea (16%), and vomiting (7%), which is unexpected given that their dose and exposure to semaglutide were significantly higher. However, 6% of participants reported serious adverse events, and 3% discontinued treatment due to side effects. Unlike our study, some cases of hypoglycemia and gallbladder disease were reported (20). In a large real-world study, only 10% of users followed recommended dose increases for subcutaneous semaglutide but they generally resembled trial participants (29). Weight loss in a regular clinical setting was similar to weight loss in randomized clinical trials (30).
In the PIONEER 1 study (31), which investigated monotherapy with oral semaglutide in type 2 diabetes, participants on 14 mg semaglutide experienced an average weight loss of 4 kg after 26 weeks (31). At least 5% weight loss was achieved by 41% of participants (compared to 15% with placebo), which is similar to our results. However, BMI in PIONEER 1 was 32 on average (31), lower than in our study, and semaglutide is known to be less effective for weight loss in individuals with type 2 diabetes. In our study, nausea, vomiting, or constipation were reported at slightly higher rates. Given that participants in real-world conditions were aware of their treatment and could be well-informed about potential side effects, a nocebo effect might have contributed to these results.
Additionally, in the OASIS 1 trial (19), oral semaglutide at a dose of 50 mg, which is not yet available for clinical use in obesity or type 2 diabetes, induced an average of 15% weight loss, with 85% of participants achieving at least 5% weight loss (compared to 26% with placebo) and 54% achieving at least 15% weight loss. Participants BMI also decreased by an average of 5.6 kg/m² (19).
According to our data and published data on other medications, we can indirectly infer that oral semaglutide at a dose of 14 mg is associated with less weight loss and a smaller reduction in BMI compared to tirzepatide at all maintenance doses, subcutaneous semaglutide at 2.4 mg weekly, and oral semaglutide at 50 mg daily. The weight loss effect of 14 mg oral semaglutide appears numerically comparable to older obesity treatments: orlistat (360 mg daily) with 8% weight loss and 51% achieving at least 5% weight loss, naltrexone-bupropion (32/360 mg) with 6% weight loss and with 48% achieving at least 5% weight loss and liraglutide (3 mg daily) with 8 kg weight loss and 63% achieving at least 5% weight loss (1, 9). The most common adverse effects of oral semaglutide are gastrointestinal, including nausea, diarrhea, vomiting, constipation, dyspepsia and upper abdominal pain. Most adverse effects are mild to moderate, transient, and not associated with treatment discontinuation. During treatment, monitoring is required regarding the potential occurrence of acute pancreatitis, gallbladder disease, suicidal ideation, medullary thyroid carcinoma, acute kidney injury, and worsening of diabetic retinopathy (15, 17, 18). In our study the most frequently reported side effect was nausea, affecting 23% of participants, followed by vomiting and diarrhoea, each affecting 12%, and constipation and nonspecific abdominal pain reported by 6% of participants. The majority of adverse events were mild, and although among our participants 6% discontinued treatment due to side effects, none experienced a serious adverse event.
The retrospective and observational design of our study facilitated faster execution, however, several limitations must be acknowledged. The risk of selection bias is inherent to retrospective observational studies. In our study, pharmacological treatment with oral semaglutide was prescribed only to patients who were both able to self-fund their treatment and motivated to seek obesity care. Due to the non-randomized and observational design of the study, causality cannot be established. Nonetheless, the magnitude of weight loss observed exceeded what would be anticipated from placebo or lifestyle modifications alone, particularly in the absence of a structured diet and physical activity program, which only three participants attended. This likely minimized the potential confounding influence of intesive lifestyle modification. Additionally, the low number of lifestyle program participants precluded any meaningful comparison between participants and non-participants, and the overall limited sample size restricted the ability to conduct subgroup analyses in general. Furthermore, the absence of a comparator group also weakens the robustness of the conclusions. Finally, the study was conducted in Caucasian adults, limiting the findings’ generalizability to more diverse populations.
From a clinical perspective, oral semaglutide may be particularly useful in patients who decline injectable therapy, when injectable medications are unavailable, or as an initial therapy before transitioning to more potent treatment options. Considering the ongoing shortage of injectable incretin-based therapies, future research should aim to prioritize randomized controlled trials evaluating the efficacy of oral semaglutide in patients without diabetes, as well as include a broader demographic spectrum, integrate pharmacological treatment with structured non-pharmacological interventions and improve control over potential confounders, especially those related to lifestyle.
5 Conclusions
In conclusion, the present study, which evaluated oral semaglutide at a daily dose of 14 mg for the treatment of obesity in adults without diabetes, demonstrated substantial interindividual variability in weight loss response in a real-world setting. Approximately half of the participants experienced a clinically significant reduction in body weight, although this reduction was mostly less than 10%. The treatment demonstrated a favorable safety profile, with no major safety concerns observed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The Maribor University Medical Centre medical ethics committee(document number UKC-MB-KME-50/24). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MK: Methodology, Writing – original draft, Formal Analysis, Supervision, Writing – review & editing, Data curation, Conceptualization, Investigation. NK: Writing – original draft, Data curation, Formal Analysis, Visualization, Writing – review & editing. AK: Conceptualization, Writing – review & editing, Supervision, Writing – original draft, Methodology.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
In the past, MK and AK have received lecture honoraria from Novo Nordisk and Eli Lilly. NK has no conflicts of interest to declare.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lingvay I, Cohen RV, le Roux CW, and Sumithran P. Obesity in adults. Lancet. (2024) 404:972–87. doi: 10.1016/S0140-6736(24)01210-8
2. Determinante zdravja – dejavniki tveganja: čezmerna hranjenost in debelost. Ljubljana: NIJZ, Zdravstveni statistični letopis Slovenije (2022). Available online at: https://nijz.si/wp-content/uploads/2024/03/3.2_Cezmerna_hranjenost_in_debelost_2022-Z.pdf.
3. Obesity classification. In: World obesity federation. London, UK: World Obesity Federation. Available online at: https://www.worldobesity.org/about/about-obesity/obesity-classification (Accessed January 10, 2025).
4. Medina-Inojosa JR, Batsis JA, Supervia M, Somers VK, Thomas RJ, Jenkins S, et al. Relation of waist-hip ratio to long-term cardiovascular events in patients with coronary artery disease. Am J Cardiol. (2018) 121:903. doi: 10.1016/j.amjcard.2017.12.038
5. van der Valk ES, van der Akker ELT, Savas M, Kleinendorst L, Visser JA, Van Haelst MM, et al. A comprehensive diagnostic approach to detect underlying causes of obesity in adults. Obes Rev. (2019) 20:795–804. doi: 10.1111/obr.12836
6. NICE guideline. In: Overweight and obesity management. London, UK: National Institute for Health and Care Excellence. Available online at: https://www.nice.org.uk/guidance/ng246 (Accessed January 10, 2025).
7. Bioletto F, Ponzo V, Goitre I, Stella B, Rahimi F, Parasiliti-Caprino M, et al. Complementary role of BMI and EOSS in predicting all-cause and cause-specific mortality in people with overweight and obesity. Nutrients. (2024) 16:3433–40. doi: 10.3390/nu16203433
8. Durrer Schutz D, Busetto L, Dicker D, Forpour-Lambert N, Pryke R, Toplak H, et al. European practical and patient-centred guidelines for adult obesity management in primary care. Obes Facts. (2019) 12:40–66. doi: 10.1159/000496183
9. Garvey WT, Mechanick JI, Brett EM, Garber AJ, Hurley DL, Jastreboff AM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. (2016) 22:S3:1–203.
10. Yumuk V, Tsigos C, Fried M, Schindler K, Busetto L, Micic D, et al. European Guidelines for obesity management in adults. Obes Facts. (2015) 8:402–34. doi: 10.1159/000442721
11. Janež A, Epšek M, Klen J, Kunst G, Marušič D, Rotar Pavlič D, et al. Strokovna priporočila za zdravljenje debelosti z zdravili (Professional Guidelines for the Pharmacological Treatment of Obesity). Ljubljana: Slovensko osteološko društvo (2022).
12. Nauck MA and Meier JJ. The incretin effect in healthy individuals and those with type 2 diabetes: physiology, pathophysiology, and response to therapeutic interventions. Lancet Diabetes Endocrinol. (2016) 4:525–36. doi: 10.1016/S2213-8587(15)00482-9
13. Wegovy summary of product characteristics. Available online at: https://www.ema.europa.eu/en/documents/product-information/wegovy-epar-product-information_en.pdf (Accessed February 10, 2025).
14. Ozempic Summary of Product characteristics. Available online at: https://www.ema.europa.eu/en/documents/product-information/ozempic-epar-product-information_en.pdf (Accessed February 10, 2025).
15. Rybelsus Summary of Product characteristics. Available online at: https://ec.europa.eu/health/documents/community-register/2021/20210818152819/anx_152819_sl.pdf (Accessed February 10, 2025).
16. Xie Y, Choi T, and Al-Aly Z. Mapping the effectiveness and risks of GLP-1 receptor agonists. Nat Med. (2025) 31(3):951–62. doi: 10.1038/s41591-024-03412-w.
17. Thethi TK, Pratley R, and Meier JJ. Efficacy, safety and cardiovascular outcomes of once-daily oral semaglutide in patients with type 2 diabetes: The PIONEER programme. Diabetes Obesity Metab. (2020) 22:1263–77. doi: 10.1111/dom.14054
18. Rybelsus highlights of prescribing information . Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/213051s018lbl.pdf (Accessed January 25, 2025).
19. Knop FK, Aroda VR, do Vale RD, Holst-Hansen T, Laursen PN, Rosenstock J, et al. Oral semaglutide 50 mg taken once per day in adults with overweight or obesity (OASIS 1): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. (2023) 402:705–19. doi: 10.1016/S0140-6736(23)01185-6
20. Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, et al. Once-weekly semaglutide in adults with overweight or obesity. NEJM. (2021) 384:989–1002. doi: 10.1056/NEJMoa2032183
21. Novo Nordisk’s Ozempic shortage expected to continue into Q4. New York, US: Reuters (2024). Available online at: https://www.reuters.com/business/healthcare-pharmaceuticals/novo-nordisks-ozempic-shortage-expected-continue-into-q4-2024-09-02.
22. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. (2018) 39:3021–104. doi: 10.1093/eurheartj/ehy339
23. Sharma AM and Kushner RF. A proposed clinical staging system for obesity. Int J Obes (Lond). (2009) 33:289–95. doi: 10.1038/ijo.2009.2
24. Serious adverse reaction. Available online at: https://www.ema.europa.eu/en/glossary-terms/serious-adverse-reaction (Accessed January 10, 2025).
25. Rodriguez PJ, Goodwin Cartwright BM, Gratzl S, Brar R, Baker C, Gluckman TJ, et al. Semaglutide vs tirzepatide for weight loss in adults with overweight or obesity. JAMA Intern Med. (2024) 184:1056–64. doi: 10.1001/jamainternmed.2024.2525
26. Rubino DM, Greenway FL, Khalid U, O'Neil PM, Rodenstock J, Sorrig R, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight or obesity with-out diabetes. The STEP 8 randomized clinical trial. JAMA. (2022) 327:138–50. doi: 10.1001/jama.2021.23619
27. Jastreboff AM, Arone LJ, Ahmad NN, Wharton S, Connert L, Alves B, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. (2022) 387:205–16. doi: 10.1056/NEJMoa2206038
28. Hankosky ER, Desai K, Chinthammit C, Grabner M, Stockbower G, He X, et al. 2084-LB: Real-World Effectiveness of Tirzepatide among People with Obesity or Overweight without Type 2 Diabetes (T2D). Diabetes. (2024) 73:2084–LB. doi: 10.2337/db24-2084-LB
29. Ladebo L, Ernst MT, Mailhac A, Dirksen C, Bojsen-Moller KN, and Pottegard A. Real-world use of semaglutide for weight management: patient characteristics and dose titration—A danish cohort study. Diabetes Care. (2024) 47:1834–7. doi: 10.2337/dc24-1082
30. Ghusn W, de la Rosa A, Sacoto D, Cifuentes L, Campos A, Feris F, et al. Weight loss outcomes associated with semaglutide treatment for patients with overweight or obesity. JAMA Netw Open. (2022) 5:e2231982. doi: 10.1001/jamanetworkopen.2022.31982
31. Aroda VR, Rosenstock J, Terauchi Y, Altuntas Y, Lalic NM, Morales Villegas EC, et al. PIONEER 1: randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care. (2019) 42:1724–32. doi: 10.2337/dc19-0749
Keywords: obesity, oral semaglutide, GLP-1 receptor agonist, efficacy, safety, real-world evidence, weight loss
Citation: Krajnc M, Kuhar N and Koceva A (2025) Oral semaglutide for the treatment of obesity: a retrospective real-world study. Front. Endocrinol. 16:1593334. doi: 10.3389/fendo.2025.1593334
Received: 13 March 2025; Accepted: 13 May 2025;
Published: 29 May 2025.
Edited by:
Claire Joanne Stocker, Aston University, United KingdomReviewed by:
Edward Wargent, University of Buckingham, United KingdomWinnie Mathur, Mohak Hitech Speciality Hospital, India
Grażyna Nowicka, Medical University of Warsaw, Poland
Copyright © 2025 Krajnc, Kuhar and Koceva. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mitja Krajnc, bWl0amEua3Jham5jQHVrYy1tYi5zaQ==