 David Aristizábal-Colorado1,2
David Aristizábal-Colorado1,2 David Corredor-Rengifo1,2Santiago Sierra-Castillo3Carolina López-Corredor4David-Alexander Vernaza-Trujillo2,5,6Danilo Weir-Restrepo7
David Corredor-Rengifo1,2Santiago Sierra-Castillo3Carolina López-Corredor4David-Alexander Vernaza-Trujillo2,5,6Danilo Weir-Restrepo7 Juan S. Izquierdo-Condoy8*
Juan S. Izquierdo-Condoy8* Esteban Ortiz-Prado8
Esteban Ortiz-Prado8 Jorge Rico-Fontalvo9,10Juan-Esteban Gómez-Mesa11,12Alin Abreu-Lomba13
Jorge Rico-Fontalvo9,10Juan-Esteban Gómez-Mesa11,12Alin Abreu-Lomba13 Wilfredo-Antonio Rivera-Martínez2,14
Wilfredo-Antonio Rivera-Martínez2,14- 1Internal Medicine Department, Universidad Libre, Cali, Colombia
- 2Grupo Interinstitucional de Medicina Interna (GIMI1), Universidad Libre, Cali, Colombia
- 3Epidemiology Department, Universidad Centros de Estudios en Salud (CES), Medellín, Colombia
- 4Medicine Program, Universidad Santiago de Cali, Cali, Colombia
- 5Department of Public Health, Pontificia Universidad Javeriana, Cali, Colombia
- 6Clinical Research Center, Clínica Imbanaco, Cali, Colombia
- 7Internal Medicine Department, Universidad Centros de Estudios en Salud (CES), Medellin, Colombia
- 8One Health Research Group, Universidad de las Américas, Quito, Ecuador
- 9Department of Nephrology, Faculty of Medicine, Universidad Simón Bolívar, Barranquilla, Colombia
- 10Latin American Society of Nephrology and Arterial Hypertension (SLANH), Ciudad de Panama, Panama
- 11Cardiology Department, Fundación Valle del Lili, Cali, Colombia
- 12Department of Health Sciences, Universidad Icesi, Cali, Colombia
- 13Endocrinology Department, Clínica Imbanaco, Cali, Colombia
- 14Endocrinology Department, Universidad de Antioquia, Medellín, Colombia
Cardiovascular and renal complications remain leading causes of morbidity and mortality among individuals with type 2 diabetes mellitus (T2DM). Since 2015, large-scale cardiovascular outcome trials (CVOTs) have demonstrated that sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) significantly reduce the risk of major adverse cardiovascular events, cardiovascular mortality, and heart failure hospitalization in patients with T2DM and established cardiovascular disease or high-risk profiles. These findings—originating from landmark trials such as EMPA-REG OUTCOME, LEADER, and SUSTAIN-6—have led to substantial revisions in international guidelines from the European Society of Cardiology, American College of Cardiology, and American Heart Association, which now recommend the use of SGLT2i or GLP-1 RAs, often in conjunction with metformin. SGLT2i have shown robust effects in reducing heart failure hospitalization and slowing the progression of chronic kidney disease, while GLP-1 RAs have demonstrated superior efficacy in reducing atherothrombotic events, particularly non-fatal stroke. Additionally, emerging data supports the complementary use of both drug classes, revealing additive benefits on cardiovascular and renal outcomes without increased toxicity. This narrative review summarizes the mechanisms of action, clinical efficacy, safety profiles, and sex-specific outcomes associated with SGLT2i and GLP-1 RAs. It also highlights key evidence supporting their combined use and underscores their critical role in optimizing long-term outcomes in patients with T2DM and cardiovascular disease.
1 Introduction
Cardiovascular disease (CVD) continues to be a significant global health concern, with ischemic stroke and acute myocardial infarction ranking as the second and third leading causes of death worldwide in 2019 (1). In 2020, an estimated 523 million people were affected by CVD, resulting in approximately 19 million deaths—an 18.7% increase compared to 2010 (2). In parallel, type 2 diabetes mellitus (T2DM) continues to rise, with 536.6 million individuals affected globally in 2021. This figure is projected to increase to 783.2 million by 2045 (3). The CALIBER UK study highlights that peripheral arterial disease (16.2%), heart failure, stable angina, non-fatal myocardial infarction, and cerebrovascular accidents are common cardiovascular complications in T2DM patients after 5.5 years of follow-up (4).
The complex interaction between diabetes mellitus (DM) and cardiovascular events complicates patient management. Individuals with T2DM frequently have multiple cardiovascular risk factors, including obesity (32.9%), hypertension (32-80%), and dyslipidemia (39%) (5–8). Moreover, factors such as oxidative stress, hypercoagulability, endothelial dysfunction, and autonomic neuropathy contribute significantly to CVD risk in T2DM patients (5).
The association between glycemic control and cardiovascular outcomes in DM patients has been long studied (9–11). However, recent evidence shows conflicting results regarding the benefits of strict glycemic control on reducing cardiovascular events. Although stringent glycemic targets (HbA1c ≤ 6.5%) may yield benefits on microvascular complications, their impact on cardiovascular mortality remains uncertain (12, 13). Moreover, pursuing overly strict control may increase the risk of hypoglycemia, weight gain, and all-cause mortality (14, 15).
To address these challenges, novel pharmacological therapies such as sodium-glucose cotransporter-2 inhibitors (SGLT-2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have emerged, offering cardioprotective benefits (16, 17). These agents have been shown to reduce cardiovascular mortality, slow chronic kidney disease (CKD) progression, and decrease heart failure (HF) hospitalizations (17–19). Leading clinical guidelines now recommend the combined or monotherapy use of SGLT-2i and GLP-1 RAs in patients with T2DM and CVD or those at high cardiovascular risk (20, 21).
The aim of this review is to enhance our understanding of the role of SGLT-2i and GLP-1 RAs in managing patients with T2DM and CVD. By highlighting key findings and clinical implications, this review aims to provide valuable information for healthcare professionals involved in the care of these patients.
2 Material and methods
This narrative literature review examines the use of SGLT-2 inhibitors and GLP-1 RAs in patients with T2DM and CVD. The review included a comprehensive search of peer-reviewed articles published between January 2010 and November 2024 conducted using the PubMed and Medline databases, supplemented by the inclusion of relevant studies from earlier periods when clinically justified. Articles were primarily selected based on clinical relevance and their inclusion in current international guidelines for the management of patients with CVD and T2DM. The search strategy incorporated the following Boolean logic; (SGLT-2 inhibitors) AND (GLP-1 receptor agonists) AND (type 2 diabetes mellitus) AND (cardiovascular diseases).
The review process comprised three distinct stages:
1. An exhaustive search of documentary material using PubMed and Medline databases.
2. Classification and selection of the most relevant articles based on predefined evaluation criteria.
3. Detailed analysis and synthesis of the extracted data.
The initial search yielded 564 articles. Inclusion criteria were studies involving adult patients (≥18 years) with T2DM and CVD; evaluation of SGLT-2 inhibitors or GLP-1 receptor agonists; and reporting of cardiovascular or renal outcomes. Eligible study designs included randomized controlled trials, observational studies (cohort or case-control), systematic reviews, and meta-analyses. Only peer-reviewed, indexed publications were considered. Data extraction and review were independently conducted by three authors (DAC, DCR, and SSC) using a standardized data collection form. A total of 407 records were excluded based on title and abstract screening, and 113 full-text articles were assessed for eligibility. The final manuscript was reviewed by experts in endocrinology, nephrology, and cardiology, who provided critical feedback and ensured comprehensive bibliographic coverage.
3 Results
3.1 Mechanism of action and clinical impact
3.1.1 Mechanism of action of SGLT2 inhibitors
Phlorizin, a botanical extract, is a non-specific inhibitor of sodium-glucose transporter proteins. Its discovery traces back over 150 years to research on glucosuria (22). Since then, various types of SGLT proteins have been identified. SGLT2i, in particular, target the sodium-glucose cotransporter 2, which is primarily located in the proximal tubular epithelium. This protein is responsible for roughly 90% of renal glucose reabsorption, and by inhibiting it, SGLT2i effectively disrupt this reabsorption process (23).
By blocking sodium-glucose cotransporter 2 in the S1 and S2 segments of the proximal tubule, SGLT2i significantly reduce glucose reabsorption, promoting urinary glucose excretion. This creates a state of “relative hypoglycemia,” which has several beneficial effects, including reductions in both systolic and diastolic blood pressure through decreased circulating volume and improved glomerular hyperfiltration control. Additionally, SGLT2i can lower HbA1c levels by 0.5-1.0% and support weight loss (24, 25). Increased natriuresis and sodium delivery to the distal nephron, induced by SGLT2 inhibition, are key in renal protection, normalizing the tubuloglomerular feedback mechanism, a principal driver of hyperfiltration (17, 19, 25).
Studies have indicated that increased expression of the sodium-hydrogen exchanger isoform 1 (NHE-1) is linked to heart failure and may contribute to the development of hypertrophy and cardiac injury during ischemia and reperfusion (26, 27). SGLT2i have been shown to reduce myocardial fibrosis, a critical factor in heart failure progression. Additionally, they may promote the use of ketone bodies as an alternative energy source for the myocardium, potentially reducing the production of reactive oxygen species (ROS) (24, 26).
Of note, long-term use of SGLT2i may lead to a reduction in glycosuric efficacy, without a corresponding decline in cardiovascular benefits. This phenomenon is thought to result from compensatory mechanisms, such as increased SGLT1 activity and upregulation of SGLT2 expression. These findings support the rationale for dual SGLT1/SGLT2 inhibition as a potential therapeutic strategy (28–30).
3.2 Complications and side effects of SGLT2 inhibitors
The most common side effect of SGLT-2 inhibitors is polyuria, resulting from osmotic diuresis. Genital tract infections, affecting approximately 10-15% of women and less frequently in men, are another potential adverse effect (31, 32). Euglycemic diabetic ketoacidosis (euDKA), a rare but serious complication, has been primarily reported in patients with type 1 diabetes and may be precipitated by acute illnesses, inappropriate insulin dose reductions, or omissions (31).
Skin infections, such as Fournier’s gangrene, have been reported; their association with SGLT-2 inhibitors requires further confirmation through large, randomized trials (31). Genital fungal infections are up to four times more common in patients using SGLT-2 inhibitors (31, 32). The results of the CANVAS study showed a possible increased risk of amputations; however, neither this result nor the increased risk of fractures has been documented in other clinical trials of canagliflozin or other SGLT2 inhibitors, so further studies are required to establish a definitive link (32–35).
SGLT2 inhibitors should be discontinued in specific clinical scenarios to mitigate potential adverse events. Severe or recurrent genital mycotic infections and urinary tract infections warrant treatment suspension if they become problematic (36, 37). Patients presenting with euglycemic diabetic ketoacidosis require immediate cessation of SGLT2i therapy (36). Furthermore, it is recommended that SGLT2 inhibitors be discontinued during the perioperative period due to the risk of euDKA. This risk increases during the physiological stress associated with surgery and preoperative fasting, which can precipitate euDKA even in the absence of significant hyperglycemia. Additionally, treatment should be halted in elderly or frail individuals experiencing severe dehydration or orthostatic hypotension (36, 38).
Canagliflozin specifically should be discontinued in patients with a heightened risk of amputations, including those with a history of amputations, severe peripheral neuropathy, severe peripheral arterial disease, or active lower-limb ulcers or infections, as well as in individuals with an increased fracture risk, particularly those with previous osteoporotic fractures (34, 36, 37, 39). Although SGLT2 inhibitors do not typically increase the risk of AKI, their use should be halted during episodes of acute renal impairment (39). Although rare, cases of Fournier’s gangrene also necessitate immediate discontinuation of SGLT2 inhibitors to prevent further complications.
3.3 Mechanism of action of GLP1 receptor agonists
GLP-1 is a hormone belonging to the incretins that is produced in the gastrointestinal tract, by L cells, in response to the intake of nutrients, especially fat and glucose (40). Its release stimulates an increase in insulin secretion when stimulated by glucose at sufficient plasma levels (40). The effects of GLP-1 are not limited to the endocrinological component; there are receptors for these at the brain, liver, and gastrointestinal tract (41). It can influence renal function by increasing diuresis and natriuresis, and it can impact cardiac function by enhancing contractility and promoting cardiomyocyte survival. Additionally, GLP-1 can improve muscle insulin sensitivity and glucose uptake (42). These effects, including hemodynamic, metabolic, and anti-inflammatory actions, contribute to the cardio and renoprotective properties of GLP-1 RAs. By reducing intraglomerular pressure, decreasing inflammation, and mitigating oxidative stress, GLP-1 RAs can help preserve renal function, independent of glycemic control (43).
GLP-1 RAs like liraglutide and semaglutide, offer a therapeutic advantage over native GLP-1 by being resistant to degradation by dipeptidyl peptidase-4 (DPP-4). This resistance allows for prolonged exposure to GLP-1, resulting in sustained physiological effects. By activating GLP-1 receptors in the hypothalamus and brainstem, these analogs promote satiety, leading to reduced food intake and weight loss (40, 44).
Studies as Network Meta-analysis and clinical trials have shown that GLP1-RA can achieve a statistically significant decrease in HbA1C compared to placebo, as well as a weight reduction ranging between 1.3 and 8.65 kg (40, 45, 46). Furthermore, these analogues have the ability to stimulate natriuresis by inhibiting sodium reabsorption by decreasing the activity of sodium-hydrogen exchanger 3 (NHE3), resulting in a reduction in blood pressure in patients with diabetes (40, 46). In animal models, a modulatory effect has also been observed at the level of the carotid sinus, suggesting that this pharmacological class may influence sympathetic tone regulation during hyperglycemic states (47).
With regard to cardioprotection, several mechanisms have been proposed. GLP-1 RAs reduce macrophage adhesion to the endothelium, thereby inhibiting the formation of atherosclerotic plaques; they also suppress platelet activity, which may further contribute to cardiovascular protection (40). Moreover, these agents enhance cardiac glucose uptake and ATP production by increasing GLUT-1 translocation (40), and they modulate antioxidant, anti-inflammatory, and anti-apoptotic pathways (48).
3.4 Complications and side effects of GLP-1 RAs
Common side effects associated with GLP-1 receptor agonists (GLP-1 RAs) include gastrointestinal symptoms such as nausea (25–60%), diarrhea, and vomiting (5–15%) (16, 46). Although these adverse effects can be bothersome, they rarely lead to treatment discontinuation. Importantly, clinical trials have not demonstrated an increased risk of hypoglycemia with GLP-1 RAs compared to placebo (16). Less frequent side effects include injection site reactions, headaches, and nasopharyngitis (16).
While some studies have suggested a possible association between GLP-1 RAs and acute kidney injury (AKI), this has not been confirmed and appears to occur primarily in patients with underlying risk factors such as dehydration or severe gastrointestinal symptoms (49). Reports of preneoplastic pancreatic ductal disease exist, but experimental findings in mice have not been consistently replicated in human clinical trials. Although a potential association between GLP-1 RAs and gastrointestinal tumors has been proposed, current evidence does not support an increased risk of colorectal neoplasia (50).
GLP-1 RA therapy should be discontinued under specific clinical conditions to minimize risk. While a definitive causal relationship has not been established, the occurrence of acute pancreatitis necessitates immediate drug withdrawal, as recommended by the American Diabetes Association and the American College of Cardiology (37, 51). These agents are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2, based on findings from preclinical studies (21).
Treatment cessation should also be considered in patients who develop gallbladder complications, such as acute cholecystitis. Caution and close monitoring are warranted in individuals with preexisting diabetic retinopathy, due to a higher incidence of retinopathy-related complications observed in clinical trials, particularly with semaglutide (21, 37). In rare instances, severe hypersensitivity reactions, including anaphylaxis, require immediate discontinuation of GLP-1 RA therapy (52). Additionally, although uncommon, reported cases of diabetic ketoacidosis (DKA) associated with GLP-1 RAs also warrant prompt treatment cessation (53).
4 Cardiovascular results
4.1 Evidence of SGLT2 inhibitors in patients with DM2
The management of DM requires a long-term perspective, emphasizing the importance of medication safety over time. The Food and Drug Administration (FDA) mandates that clinical trials demonstrate the cardiovascular safety of anti-diabetic medications. To assess this, randomized trials typically evaluate the primary outcome of “major adverse cardiovascular events” (MACE), which includes cardiovascular death, non-fatal stroke, and non-fatal myocardial infarction (MI). This rigorous evaluation has led to the accelerated recognition of the cardioprotective, renoprotective, and vasoprotective effects of SGLT2i (54, 55) (Figure 1).
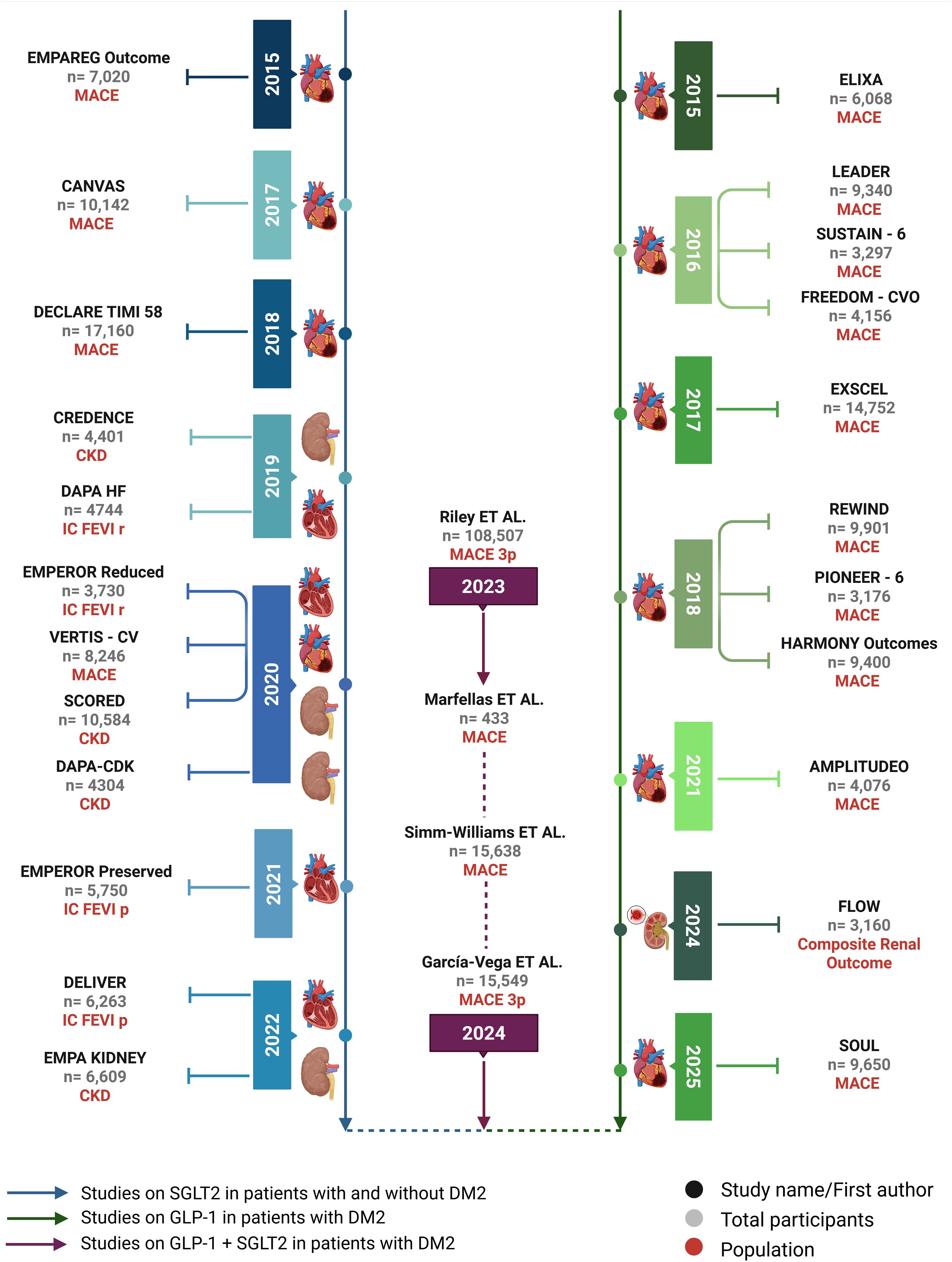
Figure 1. Timeline of major studies on SGLT-2i and GLP-1. The left axis displays key cardiovascular and renal outcome trials involving SGLT2 inhibitors, including studies in patients with and without T2DM. The right axis presents pivotal trials assessing GLP-1 receptor agonists in T2DM populations. The central column highlights observational studies and meta-analyses investigating the combined use of both drug classes. Study populations, primary outcomes (e.g., MACE, CKD, HF), and sample sizes are indicated for each trial.
4.1.1 Cardiovascular outcomes in SGLT2 inhibitors: safety studies
The EMPA-REG OUTCOME trial, which included 7020 patients with T2DM, was the first to demonstrate the cardiovascular protective effects of empagliflozin (54, 56). Patients were randomized to receive empagliflozin 10 mg, 25 mg, or placebo. After 3.1 years of follow-up, the trial showed a significant 14% reduction in the relative risk (RR) of MACE. Secondary outcomes included a 38% reduction in hospitalizations for HF and a 32% reduction in all-cause mortality (56).
Subsequent trials, such as CANVAS and DECLARE-TIMI 58, have further confirmed the cardiovascular benefits of SGLT-2 inhibitors. CANVAS demonstrated a 14% reduction in MACE in patients with T2DM and a high cardiovascular risk (34). CANVAS demonstrated a 14% reduction in MACE in patients with T2DM and a high cardiovascular risk. DECLARE-TIMI 58, which included a larger population with a lower baseline risk of CVD, did not show a significant reduction in MACE overall but did demonstrate a 27% reduction in hospitalizations for HF in a subgroup of patients with a history of myocardial infarction (54, 57). The explanation for the discrepancy in the reduction of MACE in patients treated with SGLT2i in DECLARE-TIMI 58 suggests that the benefits of SGLT2i may be more pronounced in patients with a higher risk of cardiovascular disease.
4.1.2 Cardiovascular results in studies aimed at CVD
The CREDENCE clinical trial evaluated the effects of canagliflozin (100 mg daily) versus placebo in 4,401 patients with T2DM and CKD. While primarily designed to assess renal outcomes, the trial also demonstrated significant cardiovascular benefits. A 20% relative risk reduction in MACE, including myocardial infarction, stroke, and cardiovascular death and a 30% relative risk reduction in hospitalizations for HF (58).
The VERTIS trial, involving 8246 patients with T2DM, compared ertugliflozin 5 mg or 15 mg daily to placebo for 3.5 years. While ertugliflozin did not outperform placebo for MACE, it significantly reduced hospitalizations for HF by 30% (59).
The SCORED clinical study, which included 10,584 patients with T2DM and an estimated glomerular filtration rate (eGFR) of 25–60 ml/m²/1.73 m², evaluated the effects of sotagliflozin on cardiovascular death and hospitalization for HF. After 16 months, sotagliflozin demonstrated a significant reduction in the primary endpoint (HR: 0.74; 95% CI: 0.63 - 0.88; P<0.001) (60).
A meta-analysis of five double-blind placebo-controlled trials involving 46,969 patients showed that SGLT-2 inhibitors were associated with a 14% reduction in all-cause mortality and a 9% reduction in MACE. Hospitalizations for HF were also reduced by 31% compared to placebo. However, SGLT-2 inhibitors were associated with an increased risk of diabetic ketoacidosis (RR 2.59 CI95% 1.57, 4.27) and genital infections (RR 3.50 CI95% 3.09, 3.95) (17).
4.2 SGLT2i outcomes in patients with HF
The cardiovascular benefits of SGLT-2i are particularly evident in reducing the risk of hospitalization for HF, both in patients with and without T2DM. The DAPA-HF trial, which included 4744 patients with LVEF ≤40%, demonstrated a 26% reduction in the RR of hospitalization or emergency room visits for HF within 28 days of randomization (54, 61). The cardiovascular benefits of SGLT-2i are particularly evident in reducing the risk of hospitalization for HF, both in patients with and without T2DM. The DAPA-HF trial, which included 4744 patients with LVEF ≤40%, demonstrated a 26% reduction in the RR of hospitalization or emergency room visits for HF within 28 days of randomization. Furthermore, patients treated with dapagliflozin experienced a lower rate of cardiovascular death (9.6% vs. 11.5%), reflecting an 18% reduction in RR. In addition to these objective outcomes, the DAPA-HF study assessed quality of life using the Kansas City Cardiomyopathy Questionnaire (KCCQ) and found a significant improvement in the dapagliflozin-treated group compared to placebo, indicating a positive impact on patient-reported symptoms (62).
The EMPEROR-REDUCED trial, which included 3730 patients with HF and a left ventricular ejection fraction (LVEF) ≤40%, demonstrated a 25% reduction in the RR of cardiovascular death and HF hospitalization with empagliflozin 10 mg daily compared to placebo; hospitalization from IC was reduced approximately 30% (RR 0,70; IC del 95%, 0,58 a 0,85; P <0,001). While empagliflozin did not significantly reduce all-cause mortality, it improved renal outcomes, with a slower decline in GFR compared to placebo (63). Regarding renal outcomes, the decline in GFR was slower in the empagliflozin group, with an estimated –0.55 ml per minute per 1.73 m², compared with placebo, which was –2.28 ml per minute per year. This led to a reduction in the incidence of the composite renal outcome, defined as chronic dialysis, kidney transplantation, and a sustained decline in GFR (63).
Another trial that evaluated the efficacy and safety of empagliflozin was EMPEROR-Preserved; it included 5,988 patients with heart failure with preserved left ventricular ejection fraction, regardless of whether the patients had T2DM. Participants were randomly assigned to receive empagliflozin 10 mg or placebo once daily. There was a reduction in the RR in the primary outcome (cardiovascular death and hospitalization for heart failure) (RR 0.79, 95% CI 0.69-0.90). Highlighting the decrease in hospitalization for HF (0.71; 95% CI 0.60-0.83). In this study, it was unclear whether these benefits were preserved in subgroups of patients with higher left ventricular ejection fraction (>60%), as the result was not statistically significant (RR 0.87; 95% CI; 0.69-1.10) (64). It is also unclear whether this benefit was retained in patients who started treatment during the subacute phase, or in patients with an improved LVEF (54, 64).
In the DELIVER trial, in which participants were randomly assigned to receive dapagliflozin 10 mg or placebo once daily, 6263 patients with HF with LVEF >40% were enrolled. A significant reduction in RR was observed in the primary outcomes, such as cardiovascular death or worsening of HF, compared with placebo in the overall population (RR 0.82, 95% CI 0.73 to 0.92). Worsening of HF in the group of patients receiving dapagliflozin was 23% lower. These results were consistent both in patients with LVEF of 60% or more and in those <60%. In addition, the results were similar in prespecified subgroups, including patients with or without diabetes (65).
The SOLOIST-WHF trial evaluated the efficacy and safety of sotagliflozin in 1,222 patients with HF who were recently hospitalized for worsening of their baseline condition. This study demonstrated a significant risk reduction in a composite of cardiovascular death and worsening of HF (RR 0.67; 95% CI 0.52 to 0.85). Regarding hospitalizations and emergency department visits, the decrease in RR was 36%. These results were independent of LVEF (>50% or ≤50%) (66).
The DAPA-HF, EMPEROR-REDUCED, EMPEROR-Preserved, DELIVER and other trials mentioned above consistently demonstrate the efficacy of SGLT-2i in patients with HF, regardless of LVEF or the presence of diabetes. These studies establish SGLT-2i as a cornerstone therapy for HF across the disease spectrum (54, 61). Multiple meta-analyses performed on the most important studies have confirmed a significant risk reduction for a composite of cardiovascular death and hospitalization for heart failure, with the risk reduction for hospitalization being greater (67–69). In addition to the positive cardiovascular outcomes demonstrated in the studies discussed, early initiation of SGLT-2i is increasingly emphasized to reduce associated complications. This approach is supported by evidence on the results of studies such as the EMPULSE trial and the DICTATE-AHF trial (70–75).
SGLT2i have consistently demonstrated cardiovascular benefits in meta-analyses and recent studies, confirming their robust efficacy regardless of ejection fraction or the presence of diabetes. These findings support their role as a cornerstone therapy in the management of heart failure across the entire clinical spectrum (Table 1).
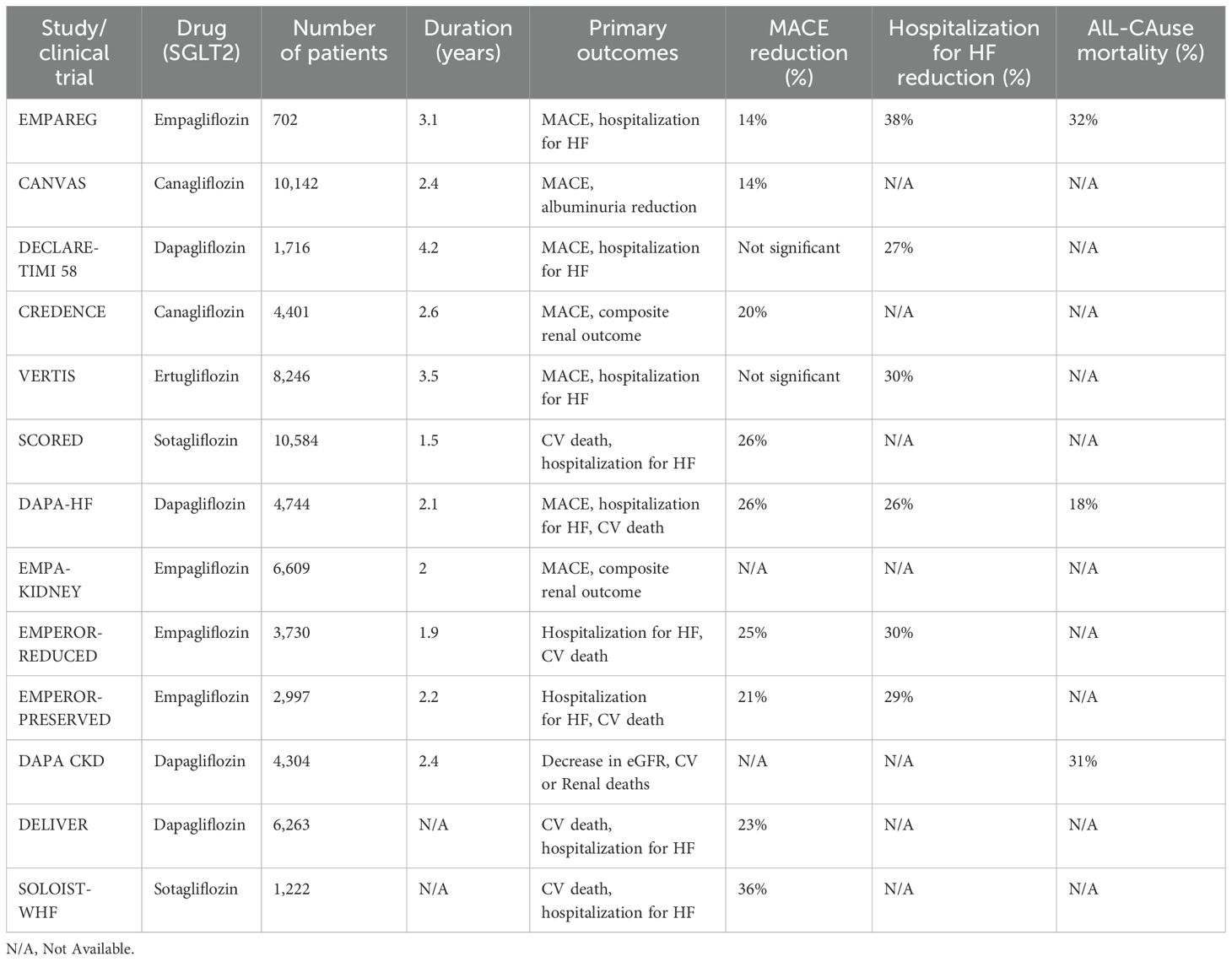
Table 1. Summary of the main studies with SGLT-2i.
4.3 GLP-1 RAs in patients with DM2
Several randomized clinical trials have demonstrated the cardiovascular benefits of GLP-1 RAs in patients with T2DM. Five of these trials have shown superiority in reducing MACE compared to placebo, while all have confirmed the cardiovascular safety of GLP-1 RAs (76).
4.3.1 Cardiovascular outcomes in GLP-1 RAs studies
The ELIXA trial, which included 6068 patients, was the first to investigate the cardiovascular effects of GLP-1 RAs. While lixisenatide 20 μg once daily did not demonstrate a significant reduction in the primary outcome of four-point MACE (RR1.02; 95% CI, 0.89–1.17), it was shown to be non-inferior to placebo in terms of cardiovascular safety (77).
The first study to demonstrate superiority over placebo was the LEADER study, in which 9,340 patients were assigned to either liraglutide or placebo. There was a significant reduction in the risk of MACE of 3 points (RR 0.87; 95% CI, 0.78-0.97). Regarding the cardiovascular mortality rate in patients with liraglutide, it was lower compared to placebo (RR 0.78; 95% CI, 0.66-0.93), and when analyzed in mortality due to any cause, it was also lower in the liraglutide group with a reduction of the RR by 15%. The rate of non-fatal stroke, non-fatal MI, and hospitalization for HF did not show significant differences (78). Semaglutide injection and CV impact was evaluated using the SUSTAIN-6 trial (designed as a non-inferiority trials), which primarily showed a reduction in the rate of non-fatal stroke events (RR 0.61; 95% CI, 0.38–0.99), as well as a decrease in the rate of MACE by 26% (79).
Other contemporary studies, such as the EXSCEL and FREEDOM trials evaluated the cardiovascular effects of exenatide, a GLP-1 RA (80, 81). EXSCEL found a 9% reduction in the relative risk (RR) of three-point MACE. While there were reductions in cardiovascular death (12%) and all-cause mortality (14%), the rates of fatal myocardial infarction (MI) and hospitalization for MI were not significantly different (80). The FREEDOM trial, with a median follow-up of 1.33 years, did not demonstrate a statistically significant difference in four-point MACE (RR 1.21; 95% CI, 0.90–1.63) (81).
The REWIND trial investigated the cardiovascular benefits of dulaglutide, a GLP-1 receptor agonist, in a population of 9,901 patients with T2DM aged 50+ and either established CVD or risk factors. The primary outcome was the first occurrence of a composite endpoint of non-fatal myocardial infarction, non-fatal stroke, or cardiovascular death. Dulaglutide significantly reduced the risk of this primary composite outcome by 12% compared to placebo (p=0.026). Gastrointestinal adverse events during follow-up were statistically significant (82).
Oral semaglutide has been studied in PIONEER 6 (designed as a non-inferiority trials), with a mean follow-up of 1.3 years and positive results for the primary endpoint: the MACE rate was reduced by 21% but did not achieve statistically significant differences. Furthermore, an important reduction in the number of deaths due to stroke was observed in the semaglutide treatment group (RR 0.49; 95% CI, 0.27-0.92). Regarding non-fatal myocardial infarction, there was no statistically significant difference (RR 1.18; 95% CI, 0.73-1.90) (83). For this drug, the ongoing SOUL trial has shown promising preliminary results, indicating a 14% reduction in the risk of MACE (84). The results of this study are expected in 2025.
The AMPLITUDE-O trial, which studied Efpeglenatide versus placebo with a mean follow-up of 1.81 years, demonstrated a significant 27% reduction in MACE. It also showed a reduction in heart failure (RR 0.61; 95% CI, 0.38–0.98) and cardiovascular mortality (RR 0.72; 95% CI, 0.50–1.03) (85).
Another study evaluating cardiovascular outcomes of GLP-1RAs was the HARMONY study. Albiglutide 30 mg was administered once weekly and enrolled a total of 9463 subjects aged ≥40 years with T2DM and established CVD. The albiglutide-treated group had a 3-point lower risk of MACE (0.78; 95% CI, 0.68–0.90). There was also a positive result for the rate of nonfatal myocardial infarction events, which was lower for the albiglutide group (RR 0.75; 0.61–0.90). However, the results were not positive for cardiovascular death (RR 0.93; 95% CI, 0.73–1.19) or stroke (RR 0.86; 95% CI, 0.66–1.14). It should be noted that this study did not evaluate hospitalization for HF (86).
A comprehensive meta-analysis by Giugliano et al. (2021) evaluated the cardiovascular benefits of GLP-1 RAs in patients with T2DM. The analysis, which included several of the above-mentioned, demonstrated a 14% reduction in the relative risk (RR) of MACE with GLP-1 RAs compared to placebo (87). Another meta-analysis also demonstrated that GLP-1s have a robust effect in reducing MACE (RR 0.87; 95% CI, 0.81-0.94) and death from any cause (RR 0.89; 95% CI, 0.83-0.95) (88). Positive results have also been found on HF, where GLP-1RAs could significantly reduce the incidence of hospital admission for heart failure by 11% (89).
Recent evidence has further substantiated the cardiovascular benefits of GLP-1 RAs. The SOUL trial (2025), a large-scale, double-blind, placebo-controlled study, evaluated once-daily oral semaglutide in 9,650 patients with T2DM and established atherosclerotic cardiovascular disease, chronic kidney disease, or both. Over a median follow-up of 49.5 months, oral semaglutide reduced the risk of MACE by 14% compared to placebo (HR 0.86; 95% CI, 0.77–0.96; p = 0.006), primarily driven by reductions in non-fatal MI and major adverse limb events. Approximately 27% of participants were on background SGLT2 inhibitor therapy at baseline; however, no significant interaction was observed, suggesting complementary cardiovascular protection mechanisms (90).
GLP-1 RAs significantly reduce the risk of MACE. Systematic reviews and meta-analyses confirm their overall cardiovascular benefits, demonstrating reductions in the relative risk of MACE, all-cause mortality, and hospitalizations for heart failure.
4.4 Role of GLP-1 RAs in arrhythmias and stroke
A meta-analysis by Liu et al. (2022) suggests that GLP-1 RAs may be associated with a reduced risk of atrial arrhythmias. This analysis included five trials with a total of 31,314 patients. While the study found that semaglutide specifically reduced the risk of atrial arrhythmias and atrial fibrillation (AF), other studies have reported conflicting results regarding the arrhythmia risk associated with GLP-1 RAs (91).
GLP-1RAs have been shown to significantly reduce postprandial levels of triglycerides, apolipoprotein (Apo) B48 and ApoC-III, independently of gastric emptying. In addition, liraglutide has been shown to significantly modify lipoprotein metabolism by reducing chylomicron production. Additionally, they exert a neuroprotective effect independently of blood glucose levels (92). Some of the antiatherosclerotic effects that contribute to stroke prevention are increased plaque stability, reduced vascular smooth muscle proliferation, and increased nitric oxide, all of which translate into improved endothelial function (92). This effect has been observed in several cardiovascular outcome clinical trials. GLP-1RAs have been shown to exert a protective factor by reducing stroke (RR 0.84; 95% CI, 0.77-0.93) (93) (Table 2).
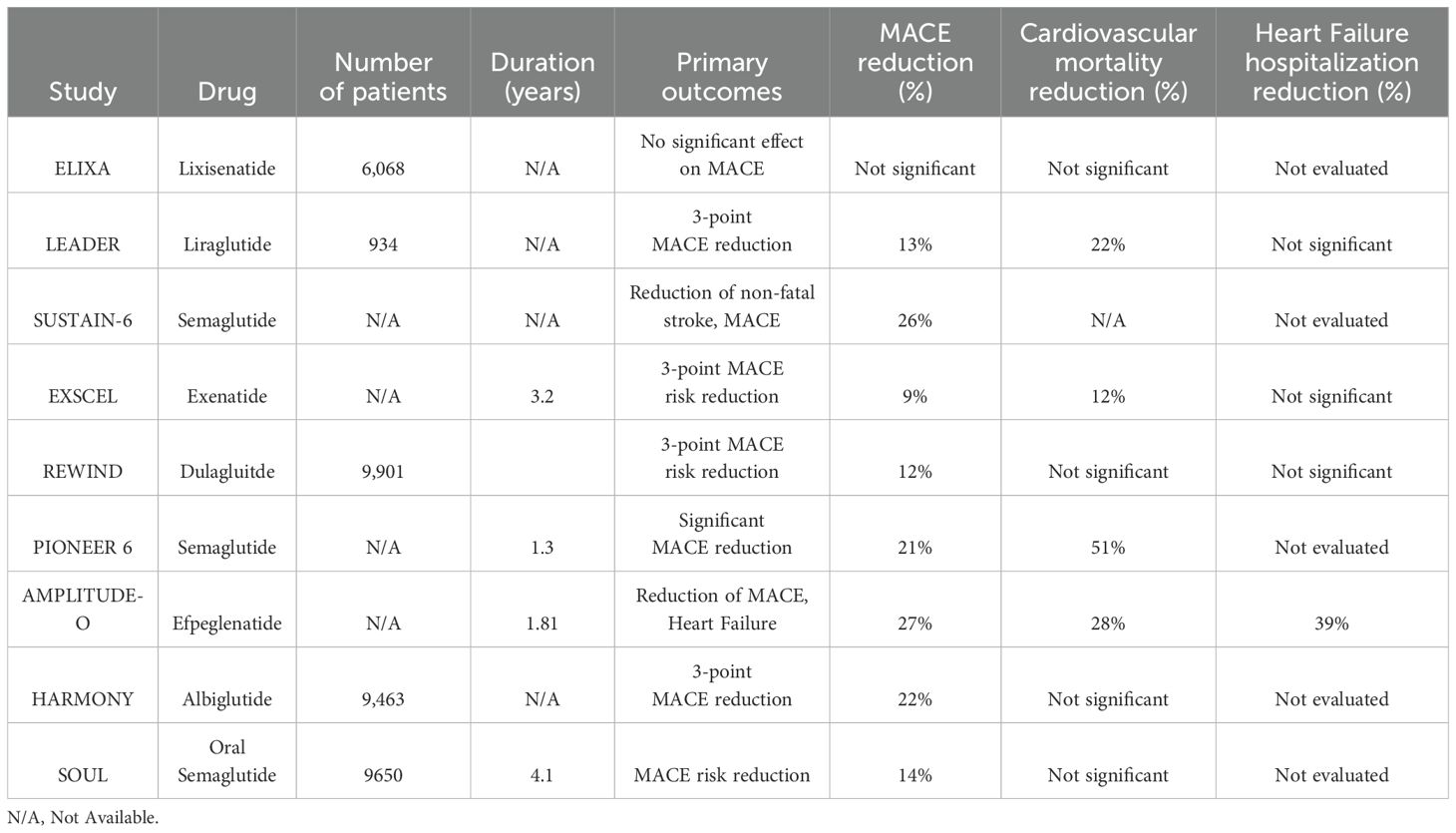
Table 2. Summary of the main studies with GLP1-AR.
4.5 Impact of SGLT-2 inhibitors and GLP-1 receptor agonists on kidney function
Multiple clinical trials have demonstrated the renoprotective effects of SGLT-2i and GLP-1 RAs in patients with T2DM and CKD. Studies such as EMPA-REG, CANVAS and DECLARE-TIMI 58, while not primarily focused on renal outcomes, have consistently shown that these medications can help preserve renal function (89, 94). In the EMPA-REG study, empagliflozin significantly reduced the risk for the composite renal outcome, which included doubling of serum creatinine, progression of macroalbuminuria, initiation of renal replacement therapy, or renal death (56). The CANVAS trial was a cardiovascular safety study; however, it suggested the presence of the renoprotective effects of canagliflozin in patients with T2DM and CKD. Canagliflozin-treated patients experienced a slower decline in GFR and an 18% reduction in the urea-albumin-creatinine ratio. Additionally, the risk of sustained doubling of serum creatinine, end-stage renal disease, and renal death was lower in the canagliflozin group (34).
Subsequent studies, such as CREDENCE, DAPA-CKD, and EMPA-KIDNEY, were specifically designed to investigate the renoprotective effects of SGLT-2i. The CREDENCE clinical trial evaluated the effects of canagliflozin 100 mg daily versus placebo in 4401 patients with T2DM and chronic kidney disease (CKD). With a mean follow-up of 2.6 years, the study demonstrated a 34% reduction in the relative risk (RR) of a composite renal outcome, including dialysis requirement, a decline in glomerular filtration rate (GFR) <15 ml/m²/1.73 m², kidney transplant requirement, doubling of creatinine, and cardiovascular or renal death (58).
The DAPA-CKD trial, which specifically evaluated the efficacy of dapagliflozin in patients with CKD, regardless of T2DM status, found a 39% reduction in the relative risk of a composite renal outcome, including a decline in GFR by at least 50%, end-stage renal disease, or renal or cardiovascular death. Dapagliflozin-treated patients had a lower incidence of these events 6.6% vs. 11.3% in the placebo group (0.61; 95% CI, 0.51 to 0.72) (95).
The results of the EMPA-KIDNEY study showed that its primary endpoint was the first occurrence of the composite outcome of kidney disease progression, defined as end-stage kidney disease, a sustained decline in eGFR to <10 mL per minute per 1.73 m², a sustained decline in eGFR of ≥40% from baseline, renal death, or cardiovascular death. The study included 6,609 patients, who were followed for 2.0 years. Emplagliflozin demonstrated a 28% reduction in the risk of the primary endpoint. In addition, it also showed a reduction in the risk of kidney disease progression by 29% (0.71; 95% CI; 0.62–0.81) (96).
Regarding GLP-1 RAs, the LEADER, SUSTAIN-6, REWIND, PIONEER 6 and AMPLITUDE-O studies have shown nephroprotective effect, especially in preventing the occurrence of macroalbuminuria. In the LEADER study, the group treated with liraglutide had a lower risk of nephropathy, with a reduction of 26% (78). In the SUSTAIN-6 trial, it was observed that semaglutide reduced the risk of nephropathy in patients treated with the drug compared to those treated with placebo (79). On the other hand, in the AMPLITUDE-O study, which included 4,076 patients, was shown that efpeglenatide significantly reduced the composite renal outcomes by 32% (a decrease in renal function or the occurrence of macroalbuminuria according to criteria defined in the study) (0.68; 95% CI, 0.57-0.79). This significant difference between the GLP-1 and placebo groups was mainly driven by a marked reduction in the incidence of macroalbuminuria (59). The REWIND trial also provided results consistent with previous studies. This study showed that the dulaglutide treated group had a lower risk of a composite renal outcome, (which includes the occurrence of macroalbuminuria, a 30% decrease in estimated glomerular filtration rate (eGFR) or the need for renal replacement therapy, (0.85, 95% CI 0 77–0.93), and the strongest statistically significant outcome was the reduction in the occurrence of macroalbuminuria (97).
The FLOW trial enrolled 3533 patients with T2DM and chronic kidney disease at high risk for kidney failure, cardiovascular events, and death. Participants were randomly assigned to receive subcutaneous semaglutide 1.0 mg weekly or placebo. The primary outcome was major kidney disease events. The semaglutide group experienced a 24% lower risk of the primary outcome compared to the placebo group (p<0.001). Additionally, the semaglutide group had an 18% lower risk of MACE (98). However, the SOUL trial, evaluating oral semaglutide, did not demonstrate a statistically significant reduction in major kidney disease events (90).
SGLT2 inhibitors have demonstrated significant renoprotective effects in patients with type 2 diabetes and CKD, reducing the risk of renal disease progression, the need for dialysis or kidney transplantation, and renal or cardiovascular mortality. GLP-1 RAs also confer renal benefits, particularly by reducing macroalbuminuria and slowing the progression of nephropathy. Together, these findings underscore the important role both drug classes play in renal protection for patients with type 2 diabetes.
4.6 Sex differences in cardiovascular outcomes
Subgroup analyses from the DAPA-HF trial revealed that women with heart failure experienced a reduction in the primary composite outcome with dapagliflozin (RR 0.79; 95% CI, 0.59–1.06), comparable to men (RR 0.73; 95% CI, 0.63–0.85), with no significant interaction by sex (62). Similar findings were reported in the CANVAS and EMPA-REG OUTCOME trials, where no significant sex-based differences were observed (34, 56). In contrast, a meta-analysis by Rivera et al. (2023) demonstrated a significant reduction in the primary composite outcome for both men (RR 0.77; 95% CI, 0.72–0.84; p < 0.00001) and women (RR 0.75; 95% CI, 0.67–0.84; p < 0.00001) receiving SGLT-2 inhibitors compared to placebo (99). Another meta-analysis evaluating three CVOTs with SGLT-2 inhibitors (N = 34,322) showed a reduction in MACE in men (RR 0.90; 95% CI, 0.83–0.97; p = 0.006), whereas in women, the risk reduction did not reach statistical significance (RR 0.88; 95% CI, 0.77–1.00; p = 0.06) (100).
Regarding safety, women experienced a higher incidence of genital infections while on SGLT-2 inhibitors, likely due to anatomical predisposition, which may impact treatment adherence (31).
For GLP-1 receptor agonists, the REWIND trial demonstrated a reduction in cardiovascular events with dulaglutide, with a trend toward greater benefit in women, although statistical significance was not achieved (RR 0.85; 95% CI, 0.71–1.02) vs. men (RR 0.90; 95% CI, 0.79–1.04; p = 0.60) (82). In the SUSTAIN-6 trial, no sex-based differences in cardiovascular outcomes were observed, indicating similar efficacy across genders (79). A meta-analysis including seven GLP-1 RA trials demonstrated significant MACE reduction in both men (RR 0.88; 95% CI, 0.82–0.93; p < 0.0001) and women (RR 0.88; 95% CI, 0.79–0.99; p = 0.03) (100).
In terms of safety, gastrointestinal adverse effects—particularly nausea—were common across both sexes, but women reported higher rates of intolerance, which may lead to treatment discontinuation (46). These observations underscore the importance of incorporating sex-specific factors when selecting GLP-1 RAs, favoring their use in women at elevated stroke risk, with potential dose adjustments to optimize adherence (8, 91).
The reduction in MACE with SGLT-2 inhibitors appears to be less consistent in women with type 2 diabetes than in men, while GLP-1 receptor agonists provide similar cardiovascular benefits across sexes.
4.7 Combined use of SGLT2i and GLP-1 RAs
Several studies have explored the combination of GLP-1 RAs and SGLT-2 inhibitors in patients with T2DM. Randomized clinical trials, such as DURATION-8, SUSTAIN-9, and AWARD-10, have documented the use of GLP-1 RAs in patients already receiving SGLT-2 inhibitors, demonstrating efficacy without adverse effects on the studied population (96, 97). Similarly, sub analyses of studies like EXSCEL, AMPLITUDE-O, HARMONY, CANVAS, DECLARE-TIMI 58, and VERTIS-CV have shown a positive impact with the concomitant use of GLP-1 RAs and SGLT-2 inhibitors, irrespective of whether the initial intervention involved GLP-1 RAs or SGLT-2 inhibitors (34, 57, 59, 80, 85, 101–105).
Among the studies evaluating GLP-1 RAs and SGLT-2 inhibitors, the study conducted by Riley et al. through the TriNetX network stands out. This study included approximately 2.2 million participants and compared cardiovascular outcomes among patients treated without GLP-1 RAs or SGLT-2 inhibitors, with one of these drug classes, or with a combination of both. After five years of follow-up in patients with T2DM, the GLP-1 RAs and SGLT-2 inhibitors groups demonstrated significant reductions in mortality, CHD, HF, AF, stroke, peripheral vascular disease, and CKD, regardless which one of the drugs or its combination were used. Notably, the simultaneous use of both pharmacological classes provided a significantly greater benefit in outcomes such as mortality, hospitalizations, heart failure, and CKD (106).
Building on the findings of the aforementioned trials, several meta-analyses have been conducted since 2019 to evaluate the safety and efficacy of combining GLP-1 RAs and SGLT-2 inhibitors. In 2019, Castellana et al. performed a meta-analysis focusing on patients with T2DM who required rescue medication for hyperglycemia and had a follow-up period of at least 24 weeks. This study demonstrated significant improvements in parameters such as HbA1c, body weight, and lipid profiles, along with a reduced need for rescue medications to control hyperglycemia (107), an effect that has been demonstrated again in other meta-analyses carried out subsequently (108). Additionally, to date it has been demonstrated to have an adequate safety profile by not increasing adverse effects with the combination of these pharmacological groups (108–111).
Among the prospective studies on this pharmacological combination, real-world evidence also plays a significant role. For instance, García-Vega et al. conducted a prospective study involving patients treated in Galicia between 2018 and 2022. The study included 15,549 patients who received either the combination therapy of GLP-1 RAs and SGLT-2 inhibitors or monotherapy with one of these drug classes. After an average follow-up of 19 months, the combination therapy did not demonstrate a reduction in coronary heart disease or ischemic stroke events compared to monotherapy. However, notable benefits were observed in other outcomes, including a 31% reduction in hospital admissions for heart failure and a 32% decrease in all-cause mortality (112).
Other high-profile studies on the use of GLP-1 RAs and SGLT-2 inhibitors combination therapy were conducted by Marfellas et al. (84, 96),. Marfellas et al. recruited patients with T2DM who had experienced acute myocardial infarction (AMI) and had been treated with one of these drug groups within the three months preceding the acute event. Patients with HbA1c >7% were initiated on the complementary drug to complete the GLP-1 RA + SGLT-2i combination therapy. The primary endpoint was a composite of cardiovascular death, recurrent acute coronary syndrome, and heart failure related to AMI after two years of follow-up. Among the 443 patients who completed the study, the combination therapy group demonstrated an ≈84% reduction in the primary endpoint (113).
Simms-Williams et al. conducted a population-based cohort study involving 15,638 patients receiving the combination therapy. Their findings revealed a ≈30% reduction in MACE compared to monotherapy. Regarding renal outcomes, the combination therapy showed a reduction in events that did not reach statistical significance when compared to SGLT-2i monotherapy. In contrast, when analyzing stroke outcomes, the effect was more pronounced with GLP-1 RAs, which provided the greatest contribution to the reduction of stroke events. However, a 57% reduction in renal events was observed compared to those receiving only GLP-1 RAs (114).
In 2024, Ahmad and Sabbour conducted a meta-analysis encompassing data from over 110,000 patients, encompassing 13 investigations that evaluated the combined use of GLP-1 RAs and SGLT-2 inhibitors. The findings demonstrated a significant reduction in all-cause mortality, with an odds ratio of 0.49 (95% CI [0.41–0.60]; p < 0.00001). Additional benefits included reductions in body mass index (BMI), blood pressure levels, HbA1c, and fasting blood glucose, observed after a minimum of six months of clinical follow-up (111).
Notably, the study by Marfellas et al. focused on a cohort of patients following a coronary event, providing insights into the cardiovascular benefits of the therapeutic combination in this high-risk population. In contrast, Simms-Williams et al. analyzed patients initially treated with GLP-1 RAs or SGLT2i, subsequently adding the second agent to evaluate the effects of combination therapy compared to monotherapy and differencing across groups (113, 114). The study by Riley et al., despite its retrospective design, represents the largest dataset to date, offering robust evidence on cardiovascular and renal outcomes associated with this therapeutic strategy (106). Lastly, the analysis by García-Vega et al. incorporated stroke outcomes, broadening the scope of evidence for this combination therapy in real-world settings (112). The meta-analyses reviewed highlight the favorable safety profile of the pharmacological therapy, alongside its efficacy in optimizing clinical parameters, particularly glycemic control and lipid profiles (Table 3).
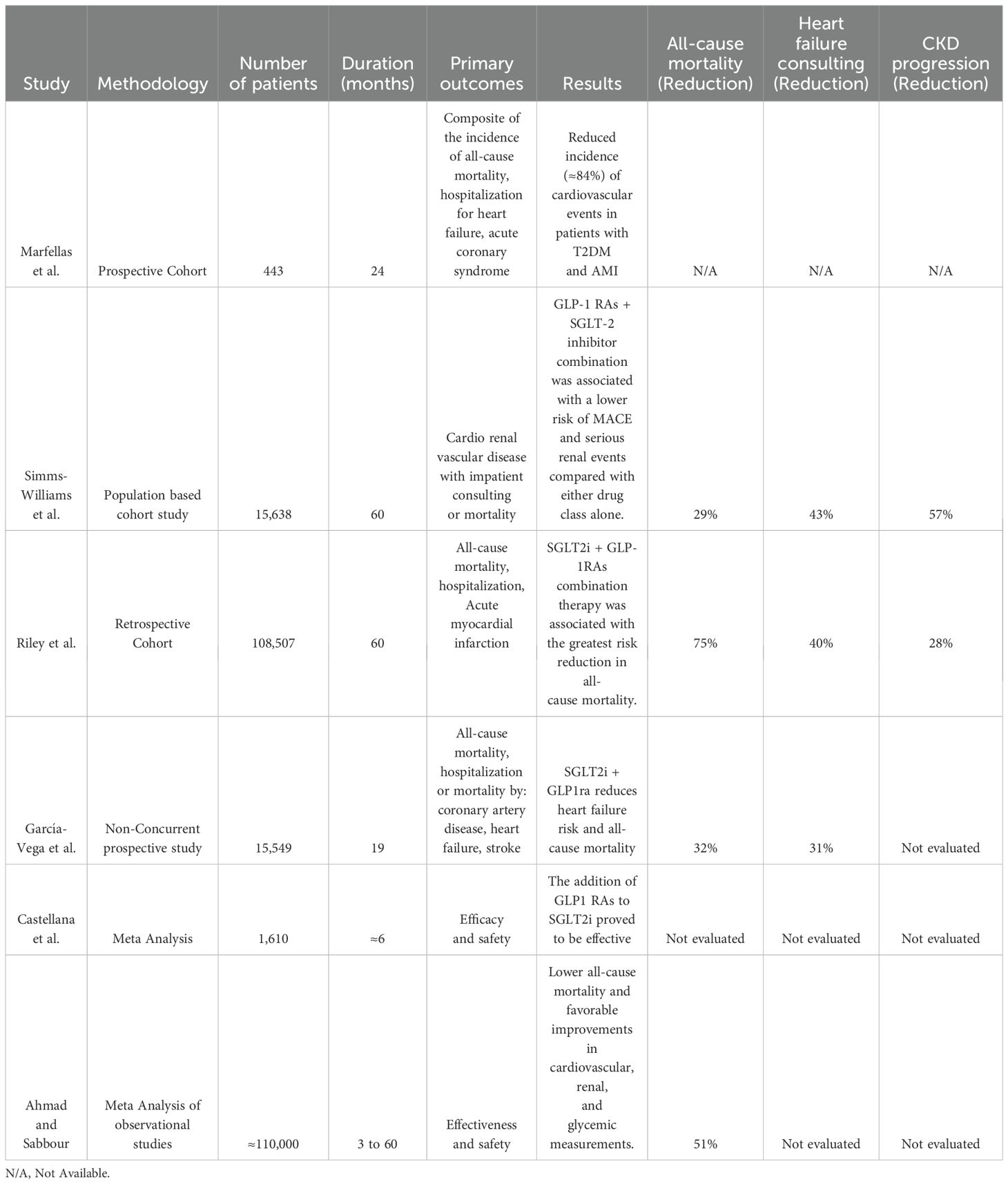
Table 3. Summary of the main studies with combined use of GLP1-AR and SGLT2 inhibitors.
With respect to the SOUL trial, oral semaglutide demonstrated a 14% reduction in MACE outcomes, independent of concurrent SGLT2 inhibitor use. The combination therapy also exhibited a favorable safety profile in this trial (115).
To date, current evidence suggests that the combination of SGLT2 inhibitors and GLP-1 receptor agonists is generally well-tolerated. The adverse events observed align with the known safety profiles of each class used individually, with no indication of synergistic toxicity. This combination represents a promising therapeutic strategy for improving cardiovascular, renal, and metabolic outcomes in patients with T2DM.
5 Conclusions
The use of SGLT-2 inhibitors and GLP-1 RAs in patients with cardiovascular risk has been well-established over the past decade. When considering the initiation of these therapies, it is important to consider patient-specific factors. Patients with existing heart or kidney disease may benefit from starting SGLT-2 inhibitors therapy, while those with a higher risk of developing these conditions, such as obese patients and those with no cardiogenic stroke, may benefit more from GLP-1 RAs. However, it is essential to note that when additional pharmacological intervention is required to control diabetes mellitus, the choice between SGLT-2 inhibitors and GLP-1 RAs should be based on the patient’s individual needs and the specific medications already being used. The combination of SGLT-2 inhibitors and GLP-1 RAs offer additive benefits in reducing cardiovascular and renal risk in patients with diabetes and should be considered.
Author contributions
DA: Resources, Funding acquisition, Formal analysis, Software, Conceptualization, Methodology, Writing – original draft, Investigation, Data curation. DC: Conceptualization, Data curation, Methodology, Writing – original draft, Investigation, Software, Resources, Formal analysis. SS: Investigation, Methodology, Writing – original draft, Software, Formal analysis, Data curation, Resources. CL: Formal analysis, Investigation, Resources, Writing – original draft, Data curation, Methodology, Software. DV: Validation, Resources, Data curation, Methodology, Software, Writing – original draft, Investigation. DW: Investigation, Writing – original draft, Supervision, Methodology, Software, Resources, Formal analysis. JI: Methodology, Visualization, Validation, Investigation, Supervision, Resources, Writing – review & editing, Funding acquisition, Software, Project administration. EO: Validation, Investigation, Writing – review & editing, Supervision, Methodology, Software, Funding acquisition, Resources, Project administration. JR: Methodology, Visualization, Investigation, Validation, Funding acquisition, Supervision, Writing – review & editing. JG: Software, Investigation, Supervision, Visualization, Writing – review & editing, Validation. AA: Visualization, Methodology, Investigation, Software, Writing – review & editing, Validation. WR: Project administration, Visualization, Validation, Writing – review & editing, Supervision, Software, Investigation.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fendo.2025.1663787.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
JR-F declares that he has received honoraria for lectures for AstraZeneca, Boehringer Ingelheim, Novo Nordisk, Lilly, Sanofi, Novartis, Abbvie, Merck, and Bayer. He has participated in Advisory Board with AstraZeneca, Boehringer Ingelheim, Bayer, and Novo Nordisk. J-EG-M declares that he has received honoraria for lectures for AstraZeneca, Bayer, Boheringer Ingelheim, Merck, and Xinetixs Pharma. He has participated in Advisory Board with AstraZeneca, and Boheringer Ingelheim.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fendo.2025.1663787.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Coronado F, Melvin SC, Bell RA, and Zhao G. Global responses to prevent, manage, and control cardiovascular diseases. Prev Chronic Dis. (2022) 19:E84. doi: 10.5888/pcd19.220347
3. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183. doi: 10.1016/j.diabres.2021.109119
4. Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet Diabetes Endocrinol. (2015) 3:105–13. doi: 10.1016/S2213-8587(14)70219-0
5. Dal Canto E, Ceriello A, Rydén L, Ferrini M, Hansen TB, Schnell O, et al. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol. (2019) 26:25–32. doi: 10.1177/2047487319878371
6. Kaze AD, Santhanam P, Musani SK, Ahima R, and Echouffo-Tcheugui JB. Metabolic dyslipidemia and cardiovascular outcomes in type 2 diabetes mellitus: findings from the look AHEAD study. J Am Heart Assoc. (2021) 10:e016947. doi: 10.1161/JAHA.120.016947
7. Azam M, Sakinah LF, Kartasurya MI, Fibriana AI, Minuljo TT, and Aljunid SM. Prevalence and determinants of obesity among individuals with diabetes in Indonesia. F1000Research. (2022) 11:1063. doi: 10.12688/f1000research.125549.3
8. Haile TG, Mariye T, Tadesse DB, Gebremeskel GG, Asefa GG, and Getachew T. Prevalence of hypertension among type 2 diabetes mellitus patients in Ethiopia: a systematic review and meta-analysis. Int Health. (2023) 15:235–41. doi: 10.1093/inthealth/ihac060
9. Rodríguez-Gutiérrez R and Montori VM. Glycemic control for patients with type 2 diabetes mellitus: our evolving faith in the face of evidence. Circ Cardiovasc Qual Outcomes. (2016) 9:504–12. doi: 10.1161/CIRCOUTCOMES.116.002901
10. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. (1998) 352:837–53. doi: 10.1016/S0140-6736(98)07019-6
11. The DCCT Research Group. Diabetes Control and Complications Trial (DCCT): results of feasibility study. The DCCT Research Group. Diabetes Care. (1987) 10:1–19. doi: 10.2337/diacare.10.1.1
12. Hemmingsen B, Lund SS, Gluud C, Vaag A, Almdal T, Hemmingsen C, et al. Intensive glycaemic control for patients with type 2 diabetes: systematic review with meta-analysis and trial sequential analysis of randomised clinical trials. BMJ. (2011) 343:d6898. doi: 10.1136/bmj.d6898
13. Monami M, Candido R, Pintaudi B, Targher G, Mannucci E, and of the SID-AMD joint panel for Italian Guidelines on Treatment of Type 2 Diabetes. Improvement of glycemic control in type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis NMCD. (2021) 31:2539–46. doi: 10.1016/j.numecd.2021.05.010
14. Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, Byington RP, Goff DC, Bigger JT, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. (2008) 358:2545–59. doi: 10.1056/NEJMoa0802743
15. Crabtree T, Ogendo J-J, Vinogradova Y, Gordon J, and Idris I. Intensive glycemic control and macrovascular, microvascular, hypoglycemia complications and mortality in older (age ≥60years) or frail adults with type 2 diabetes: a systematic review and meta-analysis from randomized controlled trial and observation studies. Expert Rev Endocrinol Metab. (2022) 17:255–67. doi: 10.1080/17446651.2022.2079495
16. Kilickap M, Kozluca V, Tan TS, and Akbulut Koyuncu IM. GLP-1 receptor agonists and SGLT-2 inhibitors in patients with versus without cardiovascular disease: A systematic review, meta-analysis, and trial sequential analysis. Angiology. (2024) 75:820–30. doi: 10.1177/00033197231183229
17. Marilly E, Cottin J, Cabrera N, Cornu C, Boussageon R, Moulin P, et al. SGLT2 inhibitors in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials balancing their risks and benefits. Diabetologia. (2022) 65:2000–10. doi: 10.1007/s00125-022-05773-8
18. Peronard R and Mayntz S. Comment on “SGLT2 inhibitors, and how they work beyond the glucosuric effect”. Am J Cardiovasc Drugs. (2024) 25:129–30. doi: 10.1007/s40256-024-00706-9
19. Kosiborod MN, Abildstrøm SZ, Borlaug BA, Butler J, Rasmussen S, Davies M, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med. (2023) 389:1069–84. doi: 10.1056/NEJMoa2306963
20. Marx N, Federici M, Schütt K, Müller-Wieland D, Ajjan RA, Antunes MJ, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes: Developed by the task force on the management of cardiovascular disease in patients with diabetes of the European Society of Cardiology (ESC). Eur Heart J. (2023) 44:ehad192. doi: 10.1093/eurheartj/ehad192
21. Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. (2022) 45:2753–86. doi: 10.2337/dci22-0034
22. Rieg T and Vallon V. Development of SGLT1 and SGLT2 inhibitors. Diabetologia. (2018) 61:2079–86. doi: 10.1007/s00125-018-4654-7
23. Hsia DS, Grove O, and Cefalu WT. An update on SGLT2 inhibitors for the treatment of diabetes mellitus. Curr Opin Endocrinol Diabetes Obes. (2017) 24:73–9. doi: 10.1097/MED.0000000000000311
24. Aristizábal-Colorado D, Ocampo-Posada M, Rivera-Martínez WA, Corredor-Rengifo D, Rico-Fontalvo J, Gómez-Mesa JE, et al. SGLT2 inhibitors and how they work beyond the glucosuric effect. State of the art. Am J Cardiovasc Drugs. (2024) 24:707–18. doi: 10.1007/s40256-024-00673-1
25. Fonseca-Correa JI and Correa-Rotter R. Sodium-glucose cotransporter 2 inhibitors mechanisms of action: A review. Front Med. (2021) 8:777861. doi: 10.3389/fmed.2021.777861
26. Pabel S, Hamdani N, Luedde M, and Sossalla S. SGLT2 inhibitors and their mode of action in heart failure-has the mystery been unravelled? Curr Heart Fail Rep. (2021) 18:315–28. doi: 10.1007/s11897-021-00529-8
27. Hiraizumi M, Akashi T, Murasaki K, Kishida H, Kumanomidou T, Torimoto N, et al. Transport and inhibition mechanism of the human SGLT2-MAP17 glucose transporter. Nat Struct Mol Biol. (2024) 31:159–69. doi: 10.1038/s41594-023-01134-0
28. Heerspink HJL, Perkins BA, Fitchett DH, Husain M, and Cherney DZI. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation. (2016) 134:752–72. doi: 10.1161/CIRCULATIONAHA.116.021887
29. Abdul-Ghani MA, DeFronzo RA, and Norton L. Novel hypothesis to explain why SGLT2 inhibitors inhibit only 30-50% of filtered glucose load in humans. Diabetes. (2013) 62:3324–8. doi: 10.2337/db13-0604
30. Lam-Chung CE. Comprehensive review of SGLT2 inhibitors’ efficacy through their diuretic mode of action in diabetic patients. Front Endocrinol. (2023) 14:1174692. doi: 10.3389/fendo.2023.1174692
31. Li D, Wang T, Shen S, Fang Z, Dong Y, and Tang H. Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: A meta-analysis of randomized controlled trials. Diabetes Obes Metab. (2017) 19:348–55. doi: 10.1111/dom.12825
32. Pittampalli S, Upadyayula S, Mekala HM, and Lippmann S. Risks vs benefits for SGLT2 inhibitor medications. Fed Pract. (2018) 35:45–8.
33. Watts NB, Bilezikian JP, Usiskin K, Edwards R, Desai M, Law G, et al. Effects of canagliflozin on fracture risk in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab. (2016) 101:157–66. doi: 10.1210/jc.2015-3167
34. Neal B, Perkovic V, and Matthews DR. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. (2017) 377:2099. doi: 10.1056/NEJMc1712572
35. Aristizábal-Colorado D, Ocampo-Posada M, Rivera-Martínez WA, Corredor-Rengifo D, Rico-Fontalvo J, Gómez-Mesa JE, et al. Author’s reply to Peronard and Mayntz: “SGLT2 inhibitors, and how they work beyond the glucosuric effect. ” Am J Cardiovasc Drugs. (2025) 25:131–3. doi: 10.1007/s40256-024-00707-8
36. American Diabetes Association Professional Practice Committee. 13. Older adults: standards of care in diabetes-2025. Diabetes Care. (2025) 48:S266–82. doi: 10.2337/dc25-S013
37. Das SR, Everett BM, Birtcher KK, Brown JM, Januzzi JL, Kalyani RR, et al. 2020 Expert consensus decision pathway on novel therapies for cardiovascular risk reduction in patients with type 2 diabetes: A report of the American College of Cardiology Solution set oversight committee. J Am Coll Cardiol. (2020) 76:1117–45. doi: 10.1016/j.jacc.2020.05.037
38. Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. (2018) 41:2669–701. doi: 10.2337/dci18-0033
39. McGill JB and Subramanian S. Safety of sodium-glucose co-transporter 2 inhibitors. Am J Cardiol. (2019) 124 Suppl 1:S45–52. doi: 10.1016/j.amjcard.2019.10.029
40. Pandey S, Mangmool S, and Parichatikanond W. Multifaceted roles of GLP-1 and its analogs: A review on molecular mechanisms with a cardiotherapeutic perspective. Pharm Basel Switz. (2023) 16:836. doi: 10.3390/ph16060836
41. Müller TD, Finan B, Bloom SR, D’Alessio D, Drucker DJ, Flatt PR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. (2019) 30:72–130. doi: 10.1016/j.molmet.2019.09.010
42. Andrikou E, Tsioufis C, Andrikou I, Leontsinis I, Tousoulis D, and Papanas N. GLP-1 receptor agonists and cardiovascular outcome trials: An update. Hell J Cardiol HJC Hell Kardiologike Epitheorese. (2019) 60:347–51. doi: 10.1016/j.hjc.2018.11.008
43. Rico-Fontalvo J, Reina M, Soler MJ, Unigarro-Palacios M, Castañeda-González JP, Quintero JJ, et al. Kidney effects of Glucagon-Like Peptide 1 (GLP1): from molecular foundations to a pharmacophysiological perspective. J Bras Nefrol. (2024) 46:e20240101. doi: 10.1590/2175-8239-JBN-2024-0101en
44. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. (2018) 27:740–56. doi: 10.1016/j.cmet.2018.03.001
45. Kayaniyil S, Lozano-Ortega G, Bennett HA, Johnsson K, Shaunik A, Grandy S, et al. A network meta-analysis comparing exenatide once weekly with other GLP-1 receptor agonists for the treatment of type 2 diabetes mellitus. Diabetes Ther Res Treat Educ Diabetes Relat Disord. (2016) 7:27–43. doi: 10.1007/s13300-016-0155-1
46. Hinnen D. Glucagon-like peptide 1 receptor agonists for type 2 diabetes. Diabetes Spectr Publ Am Diabetes Assoc. (2017) 30:202–10. doi: 10.2337/ds16-0026
47. Pauza AG, Thakkar P, Tasic T, Felippe I, Bishop P, Greenwood MP, et al. GLP1R attenuates sympathetic response to high glucose via carotid body inhibition. Circ Res. (2022) 130:694–707. doi: 10.1161/CIRCRESAHA.121.319874
48. Maack C, Kartes T, Kilter H, Schäfers H-J, Nickenig G, Böhm M, et al. Oxygen free radical release in human failing myocardium is associated with increased activity of rac1-GTPase and represents a target for statin treatment. Circulation. (2003) 108:1567–74. doi: 10.1161/01.CIR.0000091084.46500.BB
49. Filippatos TD, Panagiotopoulou TV, and Elisaf MS. Adverse effects of GLP-1 receptor agonists. Rev Diabetes Stud RDS. (2014) 11:202–30. doi: 10.1900/RDS.2014.11.202
50. Nuffield Department of Population Health Renal Studies Group, SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists’ Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet Lond Engl. (2022) 400:1788–801. doi: 10.1016/S0140-6736(22)02074-8
51. American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2025. Diabetes Care. (2025) 48:S181–206. doi: 10.2337/dc25-S009
52. Long B, Pelletier J, Koyfman A, and Bridwell RE. GLP-1 agonists: A review for emergency clinicians. Am J Emerg Med. (2024) 78:89–94. doi: 10.1016/j.ajem.2024.01.010
53. Zhang J, Ma Y, Zu Q, Wang X, and Zhang Y. GLP-1 receptor agonist–induced diabetic ketoacidosis: A case report. Med (Baltimore). (2024) 103:e39799. doi: 10.1097/MD.0000000000039799
54. Akiyama H, Nishimura A, Morita N, and Yajima T. Evolution of sodium-glucose co-transporter 2 inhibitors from a glucose-lowering drug to a pivotal therapeutic agent for cardio-renal-metabolic syndrome. Front Endocrinol. (2023) 14:1111984. doi: 10.3389/fendo.2023.1111984
55. Seidu S, Alabraba V, Davies S, Newland-Jones P, Fernando K, Bain SC, et al. SGLT2 inhibitors - the new standard of care for cardiovascular, renal and metabolic protection in type 2 diabetes: A narrative review. Diabetes Ther Res Treat Educ Diabetes Relat Disord. (2024) 15:1099–124. doi: 10.1007/s13300-024-01550-5
56. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. (2015) 373:2117–28. doi: 10.1056/NEJMoa1504720
57. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. (2019) 380:347–57. doi: 10.1056/NEJMoa1812389
58. Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. (2019) 380:2295–306. doi: 10.1056/NEJMoa1811744
59. Cannon CP, Pratley R, Dagogo-Jack S, Mancuso J, Huyck S, Masiukiewicz U, et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N Engl J Med. (2020) 383:1425–35. doi: 10.1056/NEJMoa2004967
60. Sridhar VS, Bhatt DL, Odutayo A, Szarek M, Davies MJ, Banks P, et al. Sotagliflozin and kidney outcomes, kidney function, and albuminuria in type 2 diabetes and CKD: A secondary analysis of the SCORED trial. Clin J Am Soc Nephrol CJASN. (2024) 19:557–64. doi: 10.2215/CJN.0000000000000414
61. Rolek B, Haber M, Gajewska M, Rogula S, Pietrasik A, and Gąsecka A. SGLT2 inhibitors vs. GLP-1 agonists to treat the heart, the kidneys and the brain. J Cardiovasc Dev Dis. (2023) 10:322. doi: 10.3390/jcdd10080322
62. McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. (2019) 381:1995–2008. doi: 10.1056/NEJMoa1911303
63. Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. (2020) 383:1413–24. doi: 10.1056/NEJMoa2022190
64. Anker SD, Butler J, Filippatos GS, Jamal W, Salsali A, Schnee J, et al. Evaluation of the effects of sodium-glucose co-transporter 2 inhibition with empagliflozin on morbidity and mortality in patients with chronic heart failure and a preserved ejection fraction: rationale for and design of the EMPEROR-Preserved Trial. Eur J Heart Fail. (2019) 21:1279–87. doi: 10.1002/ejhf.1596
65. Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. (2022) 387:1089–98. doi: 10.1056/NEJMoa2206286
66. Bhatt DL, Szarek M, Steg PG, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in patients with diabetes and recent worsening heart failure. N Engl J Med. (2021) 384:117–28. doi: 10.1056/NEJMoa2030183
67. McGuire DK, Shih WJ, Cosentino F, Charbonnel B, Cherney DZI, Dagogo-Jack S, et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: A meta-analysis. JAMA Cardiol. (2021) 6:148–58. doi: 10.1001/jamacardio.2020.4511
68. Vaduganathan M, Docherty KF, Claggett BL, Jhund PS, de Boer RA, Hernandez AF, et al. SGLT-2 inhibitors in patients with heart failure: a comprehensive meta-analysis of five randomised controlled trials. Lancet Lond Engl. (2022) 400:757–67. doi: 10.1016/S0140-6736(22)01429-5
69. Vernaza-Trujillo DA, Bautista LYR, Espinosa CMR, Castillo S, Corredor-Rengifo D, Aristizabal-Colorado D, et al. Impact of SGLT2 inhibitors on preventing heart failure hospitalizations in Colombian patients with uncontrolled type 2 diabetes mellitus. Cureus. (2025) 17:1–13. doi: 10.7759/cureus.77725
70. Voors AA, Angermann CE, Teerlink JR, Collins SP, Kosiborod M, Biegus J, et al. The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: a multinational randomized trial. Nat Med. (2022) 28:568–74. doi: 10.1038/s41591-021-01659-1
71. Biegus J, Voors AA, Collins SP, Kosiborod MN, Teerlink JR, Angermann CE, et al. Impact of empagliflozin on decongestion in acute heart failure: the EMPULSE trial. Eur Heart J. (2023) 44:41–50. doi: 10.1093/eurheartj/ehac530
72. Mebazaa A, Davison B, Chioncel O, Cohen-Solal A, Diaz R, Filippatos G, et al. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF): a multinational, open-label, randomised, trial. Lancet Lond Engl. (2022) 400:1938–52. doi: 10.1016/S0140-6736(22)02076-1
73. Rivera-Martínez W, Mejía-Cardona A, Salazar-Solarte A, Aristizabal-Colorado D, Garces-Villabon L, Pinillos-Senior O, et al. Impacto en desenlaces intrahospitalarios con el inició de un iSGLT2 en insuficiencia cardíaca aguda descompensada. Rev Colomb Cardiol. (2025) 32:78–89. doi: 10.24875/RCCAR.24000056
74. Cox ZL, Collins SP, Hernandez GA, McRae AT, Davidson BT, Adams K, et al. Efficacy and safety of dapagliflozin in patients with acute heart failure. J Am Coll Cardiol. (2024) 83:1295–306. doi: 10.1016/j.jacc.2024.02.009
75. Echeverría LE, Rojas LZ, Serrano-García AY, Botero DR, Cantillo-Reines M, Jurado AM, et al. Impact of early SGLT2 inhibitors prescription on acute decompensated heart failure outcomes: insights from a real-world setting. Rev Esp Cardiol Engl Ed. (2023) 93(2):160–72. doi: 10.1016/j.rec.2025.02.006
76. Rangaswami J, Bhalla V, de Boer IH, Staruschenko A, Sharp JA, Singh RR, et al. Cardiorenal protection with the newer antidiabetic agents in patients with diabetes and chronic kidney disease: A scientific statement from the American Heart Association. Circulation. (2020) 142:e265–86. doi: 10.1161/CIR.0000000000000920
77. Pfeffer MA, Claggett B, Diaz R, Dickstein K, Gerstein HC, Køber LV, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. (2015) 373:2247–57. doi: 10.1056/NEJMoa1509225
78. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JFE, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. (2016) 375:311–22. doi: 10.1056/NEJMoa1603827
79. Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. (2016) 375:1834–44. doi: 10.1056/NEJMoa1607141
80. Holman RR, Bethel MA, Mentz RJ, Thompson VP, Lokhnygina Y, Buse JB, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. (2017) 377:1228–39. doi: 10.1056/NEJMoa1612917
81. Ruff CT, Baron M, Im K, O’Donoghue ML, Fiedorek FT, and Sabatine MS. Subcutaneous infusion of exenatide and cardiovascular outcomes in type 2 diabetes: a non-inferiority randomized controlled trial. Nat Med. (2022) 28:89–95. doi: 10.1038/s41591-021-01584-3
82. Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet Lond Engl. (2019) 394:121–30. doi: 10.1016/S0140-6736(19)31149-3
83. Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. (2019) 381:841–51. doi: 10.1056/NEJMoa1901118
84. McGuire DK, Busui RP, Deanfield J, Inzucchi SE, Mann JFE, Marx N, et al. Effects of oral semaglutide on cardiovascular outcomes in individuals with type 2 diabetes and established atherosclerotic cardiovascular disease and/or chronic kidney disease: Design and baseline characteristics of SOUL, a randomized trial. Diabetes Obes Metab. (2023) 25:1932–41. doi: 10.1111/dom.15058
85. Gerstein HC, Sattar N, Rosenstock J, Ramasundarahettige C, Pratley R, Lopes RD, et al. Cardiovascular and renal outcomes with efpeglenatide in type 2 diabetes. N Engl J Med. (2021) 385:896–907. doi: 10.1056/NEJMoa2108269
86. Hernandez AF, Green JB, Janmohamed S, D’Agostino RB, Granger CB, Jones NP, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-controlled trial. Lancet Lond Engl. (2018) 392:1519–29. doi: 10.1016/S0140-6736(18)32261-X
87. Giugliano D, Scappaticcio L, Longo M, Caruso P, Maiorino MI, Bellastella G, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. (2021) 20:189. doi: 10.1186/s12933-021-01366-8
88. Lee MMY, Kristensen SL, Gerstein HC, McMurray JJV, and Sattar N. Cardiovascular and mortality outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A meta-analysis with the FREEDOM cardiovascular outcomes trial. Diabetes Metab Syndr. (2022) 16:102382. doi: 10.1016/j.dsx.2021.102382
89. Kristensen SL, Rørth R, Jhund PS, Docherty KF, Sattar N, Preiss D, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. (2019) 7:776–85. doi: 10.1016/S2213-8587(19)30249-9
90. McGuire DK, Marx N, Mulvagh SL, Deanfield JE, Inzucchi SE, Pop-Busui R, et al. Oral semaglutide and cardiovascular outcomes in high-risk type 2 diabetes. N Engl J Med. (2025) 392:2001–12. doi: 10.1056/NEJMoa2501006
91. Parab P, Chaudhary P, Mukhtar S, Moradi A, Kodali A, Okoye C, et al. Role of glucagon-like peptide-1 (GLP-1) receptor agonists in cardiovascular risk management in patients with type 2 diabetes mellitus: A systematic review. Cureus. (2023) 15:e45487. doi: 10.7759/cureus.45487
92. Vergès B, Aboyans V, Angoulvant D, Boutouyrie P, Cariou B, Hyafil F, et al. Protection against stroke with glucagon-like peptide-1 receptor agonists: a comprehensive review of potential mechanisms. Cardiovasc Diabetol. (2022) 21:242. doi: 10.1186/s12933-022-01686-3
93. Li J, Ji C, Zhang W, Lan L, and Ge W. Effect of new glucose-lowering drugs on stroke in patients with type 2 diabetes: A systematic review and Meta-analysis. J Diabetes Complications. (2023) 37:108362. doi: 10.1016/j.jdiacomp.2022.108362
94. Nagahisa T and Saisho Y. Cardiorenal protection: potential of SGLT2 inhibitors and GLP-1 receptor agonists in the treatment of type 2 diabetes. Diabetes Ther Res Treat Educ Diabetes Relat Disord. (2019) 10:1733–52. doi: 10.1007/s13300-019-00680-5
95. Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou F-F, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. (2020) 383:1436–46. doi: 10.1056/NEJMoa2024816
96. The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med. (2023) 388:117–27. doi: 10.1056/NEJMoa2204233
97. Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and renal outcomes in type 2 diabetes: an exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet Lond Engl. (2019) 394:131–8. doi: 10.1016/S0140-6736(19)31150-X
98. Pratley RE, Tuttle KR, Rossing P, Rasmussen S, Perkovic V, Nielsen OW, et al. Effects of semaglutide on heart failure outcomes in diabetes and chronic kidney disease in the FLOW trial. J Am Coll Cardiol. (2024) 84:1615–28. doi: 10.1016/j.jacc.2024.08.004
99. Rivera FB, Tang VAS, De Luna DV, Lerma EV, Vijayaraghavan K, Kazory A, et al. Sex differences in cardiovascular outcomes of SGLT-2 inhibitors in heart failure randomized controlled trials: A systematic review and meta-analysis. Am Heart Hournal Plus Cardiol Res Pract. (2023) 26:100261. doi: 10.1016/j.ahjo.2023.100261
100. Singh AK and Singh R. Gender difference in cardiovascular outcomes with SGLT-2 inhibitors and GLP-1 receptor agonist in type 2 diabetes: A systematic review and meta-analysis of cardio-vascular outcome trials. Diabetes Metab Syndr. (2020) 14:181–7. doi: 10.1016/j.dsx.2020.02.012
101. Clegg LE, Penland RC, BaChina S, Boulton DW, Thuresson M, Heerspink HJL, et al. Effects of exenatide and open-label SGLT2 inhibitor treatment, given in parallel or sequentially, on mortality and cardiovascular and renal outcomes in type 2 diabetes: insights from the EXSCEL trial. Cardiovasc Diabetol. (2019) 18:138. doi: 10.1186/s12933-019-0942-x
102. Lam CSP, Ramasundarahettige C, Branch KRH, Sattar N, Rosenstock J, Pratley R, et al. Efpeglenatide and clinical outcomes with and without concomitant sodium-glucose cotransporter-2 inhibition use in type 2 diabetes: exploratory analysis of the AMPLITUDE-O trial. Circulation. (2022) 145:565–74. doi: 10.1161/CIRCULATIONAHA.121.057934
103. Neves JS, Borges-Canha M, Vasques-Nóvoa F, Green JB, Leiter LA, Granger CB, et al. GLP-1 receptor agonist therapy with and without SGLT2 inhibitors in patients with type 2 diabetes. J Am Coll Cardiol. (2023) 82:517–25. doi: 10.1016/j.jacc.2023.05.048
104. Arnott C, Neuen BL, Heerspink HJL, Figtree GA, Kosiborod M, Lam CS, et al. The effects of combination canagliflozin and glucagon-like peptide-1 receptor agonist therapy on intermediate markers of cardiovascular risk in the CANVAS program. Int J Cardiol. (2020) 318:126–9. doi: 10.1016/j.ijcard.2020.06.011
105. Cahn A, Wiviott SD, Mosenzon O, Murphy SA, Goodrich EL, Yanuv I, et al. Cardiorenal outcomes with dapagliflozin by baseline glucose-lowering agents: Post hoc analyses from DECLARE-TIMI 58. Diabetes Obes Metab. (2021) 23:29–38. doi: 10.1111/dom.14179
106. Riley DR, Essa H, Austin P, Preston F, Kargbo I, Ibarburu GH, et al. All-cause mortality and cardiovascular outcomes with sodium-glucose Co-transporter 2 inhibitors, glucagon-like peptide-1 receptor agonists and with combination therapy in people with type 2 diabetes. Diabetes Obes Metab. (2023) 25:2897–909. doi: 10.1111/dom.15185
107. Ma H, Lin Y-H, Dai L-Z, Lin C-S, Huang Y, and Liu S-Y. Efficacy and safety of GLP-1 receptor agonists versus SGLT-2 inhibitors in overweight/obese patients with or without diabetes mellitus: a systematic review and network meta-analysis. BMJ Open. (2023) 13:e061807. doi: 10.1136/bmjopen-2022-061807
108. Li C, Luo J, Jiang M, and Wang K. The efficacy and safety of the combination therapy with GLP-1 receptor agonists and SGLT-2 inhibitors in type 2 diabetes mellitus: A systematic review and meta-analysis. Front Pharmacol. (2022) 13. doi: 10.3389/fphar.2022.838277
109. Guo M, Gu J, Teng F, Chen J, Ma X, Chen Q, et al. The efficacy and safety of combinations of SGLT2 inhibitors and GLP-1 receptor agonists in the treatment of type 2 diabetes or obese adults: a systematic review and meta-analysis. Endocrine. (2020) 67:294–304. doi: 10.1007/s12020-019-02175-6
110. Patoulias D, Stavropoulos K, Imprialos K, Katsimardou A, Kalogirou M-S, Koutsampasopoulos K, et al. Glycemic efficacy and safety of glucagon-like peptide-1 receptor agonist on top of sodium-glucose co-transporter-2 inhibitor treatment compared to sodium-glucose co-transporter-2 inhibitor alone: A systematic review and meta-analysis of randomized controlled trials. Diabetes Res Clin Pract. (2019) 158:107927. doi: 10.1016/j.diabres.2019.107927
111. Ahmad A and Sabbour H. Effectiveness and safety of the combination of sodium-glucose transport protein 2 inhibitors and glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of observational studies. Cardiovasc Diabetol. (2024) 23:99. doi: 10.1186/s12933-024-02192-4
112. García-Vega D, Cinza-Sanjurjo S, Eiras S, and González-Juanatey JR. Combined sodium-glucose-transporters inhibitors and glucagon-like-peptide receptor agonist compared with monotherapy improves long-term survival: A real-world registry. Am J Med. (2024) 137:761–769.e1. doi: 10.1016/j.amjmed.2024.04.032
113. Marfella R, Prattichizzo F, Sardu C, Rambaldi PF, Fumagalli C, Marfella LV, et al. GLP-1 receptor agonists-SGLT-2 inhibitors combination therapy and cardiovascular events after acute myocardial infarction: an observational study in patients with type 2 diabetes. Cardiovasc Diabetol. (2024) 23:10. doi: 10.1186/s12933-023-02118-6
114. Simms-Williams N, Treves N, Yin H, Lu S, Yu O, Pradhan R, et al. Effect of combination treatment with glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter-2 inhibitors on incidence of cardiovascular and serious renal events: population based cohort study. BMJ. (2024) 385:e078242. doi: 10.1136/bmj-2023-078242
115. Marx N, Deanfield JE, Mann JFE, Arechavaleta R, Bain SC, Bajaj HS, et al. Oral semaglutide and cardiovascular outcomes in people with type 2 diabetes, according to SGLT2i use: prespecified analyses of the SOUL randomized trial. Circulation. (2025) 151:1639–50. doi: 10.1161/CIRCULATIONAHA.125.074545
Keywords: cardiovascular outcomes, SGLT2 inhibitors, GLP-1 agonists, combination therapy, heart failure, renal outcomes
Citation: Aristizábal-Colorado D, Corredor-Rengifo D, Sierra-Castillo S, López-Corredor C, Vernaza-Trujillo D-A, Weir-Restrepo D, Izquierdo-Condoy JS, Ortiz-Prado E, Rico-Fontalvo J, Gómez-Mesa J-E, Abreu-Lomba A and Rivera-Martínez W-A (2025) A decade of progress in type 2 diabetes and cardiovascular disease: advances in SGLT2 inhibitors and GLP-1 receptor agonists – a comprehensive review. Front. Endocrinol. 16:1605746. doi: 10.3389/fendo.2025.1605746
Received: 03 April 2025; Accepted: 20 June 2025;
Published: 07 July 2025; Corrected: 15 August 2025.
Edited by:
Tatsuya Sato, Sapporo Medical University, JapanReviewed by:
Nina Japundzic-Zigon, University of Belgrade, SerbiaJennifer E. Richard, University of Gothenburg, Sweden
Copyright © 2025 Aristizábal-Colorado, Corredor-Rengifo, Sierra-Castillo, López-Corredor, Vernaza-Trujillo, Weir-Restrepo, Izquierdo-Condoy, Ortiz-Prado, Rico-Fontalvo, Gómez-Mesa, Abreu-Lomba and Rivera-Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan S. Izquierdo-Condoy, anVhbjFpenF1aWVyZG8xMUBnbWFpbC5jb20=