 Iwona Rotter
Iwona Rotter Żaneta Ciosek
Żaneta Ciosek Anna Syroka
Anna Syroka Aleksandra Ryl
Aleksandra Ryl- Department of Medical Rehabilitation and Clinical Physiotherapy, Pomeranian Medical University, Szczecin, Poland
Background: This cross-sectional study aimed to examine the relationship between total testosterone (TT) levels, the diagnosis of testosterone deficiency syndrome (TDS), and high-sensitivity C-reactive protein (hsCRP) concentrations in aging men. The analysis also included selected hormonal and anthropometric parameters.
Methods: Serum hsCRP levels were measured. Additionally, serum levels of TT, estradiol (E2), dehydroepiandrosterone sulfate (DHEA-S), insulin (I), and sex hormone-binding protein (SHBG) were assessed using ELISA. Patients were divided based on the presence or absence of a TDS diagnosis.
Results: In patients without TDS, no significant correlation was observed between hsCRP levels and other measured variables. However, higher hsCRP levels were associated with an increased BMI, larger waist and hip circumferences, and elevated triglyceride (TAG) levels compared to patients with lower hsCRP concentrations.
Conclusions: The co-occurrence of testosterone deficiency and elevated inflammatory markers such as hsCRP was associated with less favorable metabolic and anthropometric profiles. While causality cannot be inferred from this observational study, the findings suggest a possible link between systemic inflammation and testosterone deficiency in aging men. These associations merit further investigation in longitudinal and mechanistic studies to clarify directionality and underlying biological pathways.
1 Introduction
Testosterone is the primary male sex hormone and androgen in males. Testosterone is synthesized in 95% in the testes and to a much lesser extent in the adrenal cortex. Besides its action on the male reproductive system, testosterone nonspecifically intensifies overall metabolism and affects muscle mass and strength, fat distribution, bone mass, and erythropoiesis (1). However, there is no doubt that age-related changes in the function of internal secretion organs play a significant role in the aging process, especially in men, where age-related reduction in gonadal androgen production leads to testosterone deficiency and the so-called testosterone deficiency syndrome (TDS). It can significantly deteriorate the quality of life and negatively affect the function of many organs and systems (1).
C-reactive protein (CRP) levels, a marker of inflammation, may be inversely correlated with testosterone levels in men (2). This relationship could have significant clinical implications, as both low testosterone levels and chronic inflammation are associated with numerous health issues in men, including an increased risk of cardiovascular disease, erectile dysfunction, decreased libido, osteoporosis, and depression. Gaining insight into the pathways connecting CRP and testosterone could support the creation of new treatments for individuals with testosterone deficiency and chronic inflammatory conditions. The complex interplay between testosterone, inflammation, and disease is strongly modulated by adipose tissue, which enhances aromatase activity – an enzyme responsible for the conversion of testosterone into estradiol. This enzymatic transformation inhibits the hypothalamic–pituitary axis, thereby diminishing testosterone synthesis (3). Visceral adipose tissue acts as a metabolically active organ that secretes inflammatory mediators such as cytokines, adipokines, and various pro-inflammatory agents, including IL-6, IL-1β, TNF-α, and plasminogen activator inhibitor-1, all of which contribute to both systemic and localized vascular inflammation and impairment. Moreover, adipose tissue releases leptin, which suppresses the hypothalamic–pituitary–gonadal axis by interfering with gonadotropin signaling in Leydig cells, resulting in reduced androgen production (4). While these mechanistic pathways are supported by the secretion profile of visceral adipose tissue, it should be noted that the present analysis primarily relied on hsCRP as the inflammatory marker. Although hsCRP is a widely used surrogate of systemic inflammation, it may not fully capture the complexity of the inflammatory milieu associated with obesity-related hypogonadism. In particular, cytokines such as IL-6, TNF-α, and adipokines like leptin could provide additional mechanistic insights and better reflect tissue-specific inflammatory processes. Therefore, future studies should incorporate a broader panel of inflammatory markers to more accurately characterize the immunometabolic alterations underlying the pathophysiology of obesity-induced testosterone deficiency.
Testosterone plays a sig ificant ole in inhibiting adipose tissue formation and the expression of various adipocytokines, such as leptin, TNF-α, IL-6, and IL-1, and it is positively associated with adiponectin levels (5). A decline in testosterone secretion significantly contributes to changes in the body composition of aging males (6), marked by a decrease in fat-free mass and an increase in fat mass. Moreover, adipose tissue begins to release proinflammatory cytokines, leading to elevated serum leptin and CRP levels, coupled with decreased adiponectin levels (7, 8).
Low levels of testosterone, as well as high levels of C-reactive protein (CRP), have been linked to increased all-cause mortality risk in men (6, 9). Testosterone regulates cytokine expression through androgen receptors, modulating the inflammatory response (10). Studies suggest a bidirectional relationship between obesity-stimulated cytokine levels and TT (11). Obesity, comorbidities, and aging may play a key role in this relationship, contributing to androgen deficiency through the secretion of adipocytokines and CRP (10).
While the precise mechanism through which testosterone influences these responses remains uncertain, laboratory evidence suggests that testosterone has the ability to suppress proinflammatory cytokines while potentially up-regulating anti-inflammatory cytokines. Recognizing the association between androgens and inflammation is critical, given the pivotal role inflammation plays in the pathogenesis of numerous diseases. If a significant association is established, it could provide justification for considering androgen replacement therapy to enhance outcomes for patients with inflammatory disorders.
The literature on this topic exhibits a diversity of perspectives regarding the relationship between CRP and androgens in men and androgen levels. Numerous studies indicate the existence of a relationship between these two parameters; however, the results of these studies are often contradictory and dependent on various factors. Some studies suggest an inverse correlation between CRP and testosterone (4, 12). Conversely, other studies fail to corroborate such a distinct relationship (13, 14). The diversity of results from previous studies highlights the need for further research that considers both hormonal and anthropomorphic factors influencing this relationship. The aim of the study was to analyze the relationship between TT concentration and diagnosing TDS and hsCRP in aging men in relation to selected hormonal and anthropometric parameters.
2 Materials and methods
The study involved 313 male volunteers aged 50 to 75 years (mean age: 61.31 ± 6.33), recruited through primary care physicians in Szczecin, Poland, who provided comprehensive information about the study’s aims and procedures. Participation was contingent upon written, informed consent, which was obtained from all individuals prior to enrollment. Men were excluded if they had diabetes, were undergoing cancer treatment, used neuroleptics, antidepressants, or steroids, were receiving testosterone therapy, or had liver or thyroid disorders, ascites, or hernias located along the linea alba or in postoperative scars. The study protocol was approved by the Bioethics Committee of the Pomeranian Medical University in Szczecin (KB-0012/155/16) and followed the ethical principles of the Declaration of Helsinki for research involving human subjects.
Anthropometric measurements were conducted, including body mass, height, and abdominal circumference, with the calculation of body mass index (BMI) (15).
2.1 Collecting research material
Blood samples were drawn from the ulnar vein in fasted subjects between 7:30 am and 9:00 am. The blood was collected into tubes containing a clotting activator and gel separator, followed by centrifugation. Subsequently, the serum was stored at -70°C.
2.2 Determination of hormo al a d biochemical param ters
High sensitivity C-reactive protein levels in the serum were measured using a spectrophotometric method with ready-made reage t kits (Biolabo, Aqua-Med, Łódź, Poland). Additionally, serum concentrations of hormones such as total testostero e (TT), estradiol (E2), dehydroepiandrosterone sulfate (DHEA-S), insulin (I), and sex hormone binding protein (SHBG) were assessed via ELISA using commercially available reagent kits (DRG-MedTek, Warsaw, Poland). The tests were performed in a certified research laboratory that participates in the quality control program conducted by the Central Center for Quality Research in Laboratory Diagnostics (COJBwDL). The laboratory has a quality management system certificate IS0 9001:2008 and PN-EN 152224:2013.
2.3 Criteria for group division
The diagnosis of TDS syndrome adhered to the consensus recommendations established by the International Society of Andrology (ISA), International Society for the Study of the Aging Male (ISSAM), European Association of Urology (EAU), European Academy of Andrology (EAA), and American Society of Andrology (ASA) (16). Patients exhibiting total testosterone (TT) levels below 2.5 ng/ml or within the range of 2.5 ng/ml to 3.5 ng/ml, alongside clinical symptoms assessed using the Morley questionnaire (17), were categorized into the TT-deficient group. The study showed that 127 men with TDS showed concerns on the Morley adropause scale, whereas in the group of men without TDS, 3 men showed these symptoms. In the study, the cut -off value of hs CRP was considered to be 3 mg/l (18). The study design is presented in Figure 1.
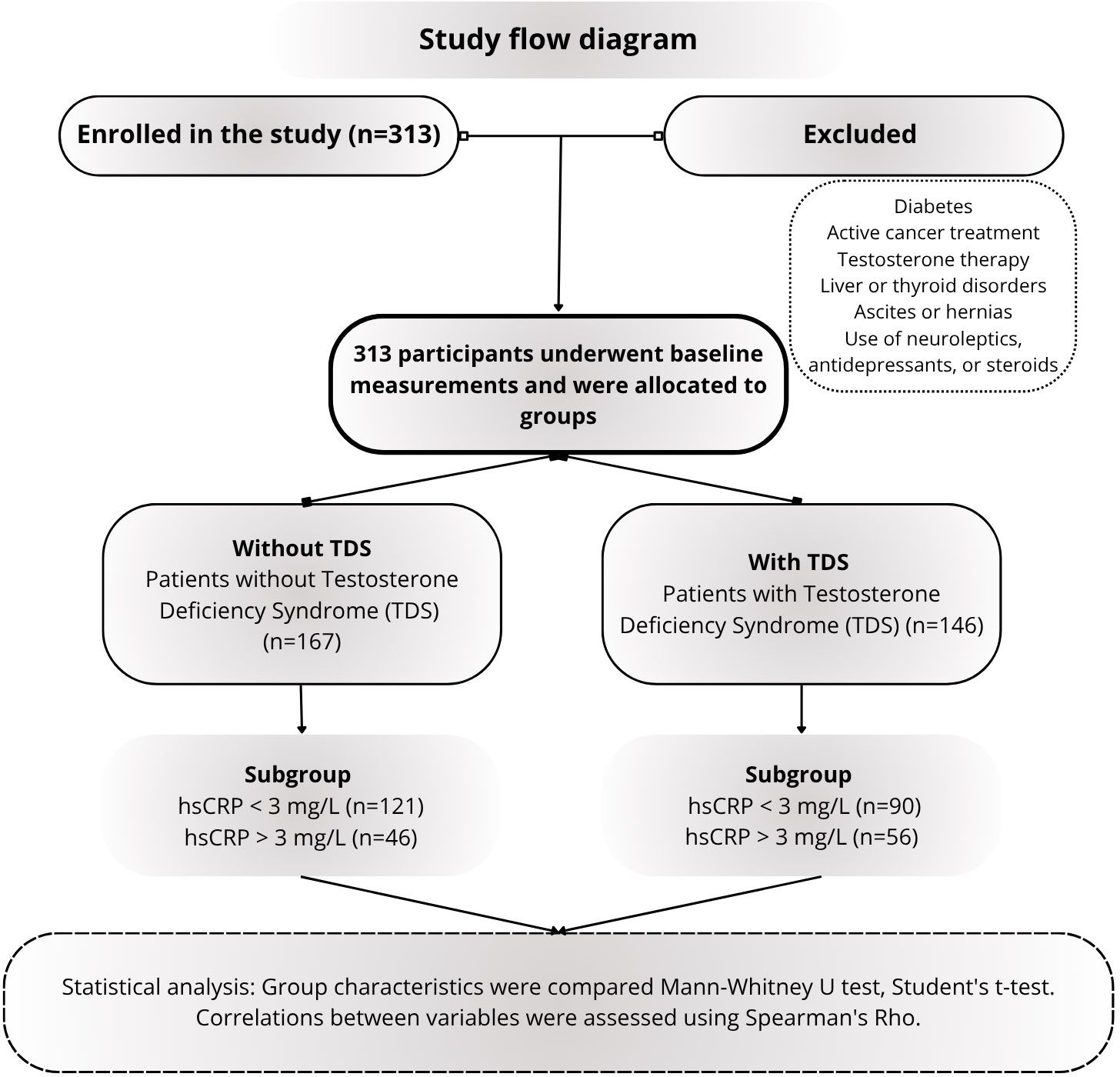
Figure 1. Design of the research conducted, taking into account the study groups; testosterone deficiency syndrome (TDS), TT, total testosterone; LH, luteinizing hormone; SHBG, sex hormone binding globulin; DHEA-S, dehydroepiandrosterone sulfate; E2, estradiol; I, Insulin; hsCRP, high sensitivity C-reactive protein.
2.4 Statistical analysis
The statistical analysis was car ied out utilizing the Statist ca 13.1 software. Within this analysis, the group’s characteristics were deli eated, showcasing m dian alues, means, and standard deviations, as well as minimum and maximum values. Normality assessm nts of distributions were conducted employing the Shapiro-Wilk test. Group compariso s were executed utilizing either the Mann-Whitney U test or the Student’s t-test. Additionally, Spearman’s Rho correlation analysis was conducted. Results with a p value less than or equal to 0.05 were considered statistically significant.
3 Results
The study investigated the correlation between anthropometric factors, hormone levels, and hsCRP concentrations in patients with and without testosterone deficiency (Table 1). The analysis highlighted statistically significant differences between the two groups concerning body mass, BMI, waist circumference, and hip circumference. Furthermore, variations were observed in testosterone (TT), sex hormone-binding globulin (SHBG), estradiol (E2), insulin (I), and hsCRP levels among these patients. In Table 2, the relationship between anthropometric factors, and hormone levels in the group of patients without testosterone deficiency was analyzed based on hsCRP concentration. The analysis did not show any correlation in the group of patients without TDS based on the level of hsCRP concentration. In Table 3, the relationship between anthropometric factors, and hormone levels in the group of patients with testosterone deficiency (TDS) was analyzed based on hsCRP concentration. It was indicated that patients with higher hsCRP levels exhibit a higher BMI, larger waist and hip circumferences, and higher triglyceride (TAG) levels compared to patients with lower hsCRP concentrations. The study also conducted an analysis examining the correlation between anthropometric and hormonal indicators and the hsCRP value (Table 4). Results revealed that among patients without TDS, a positive correlation exists between hsCRP value and waist circumference (R=0.155, p=0.045), alongside a negative correlation with total testosterone (R=-0.182, p=0.018). Conversely, within the TDS patient cohort, a positive association was observed between hsCRP value and body mass (R=0.213, p=0.010), BMI (R=0.300, p=0.001), hip circumference (R=0.275, p=0.001), and waist circumference (R=0.305, p=0.0001).
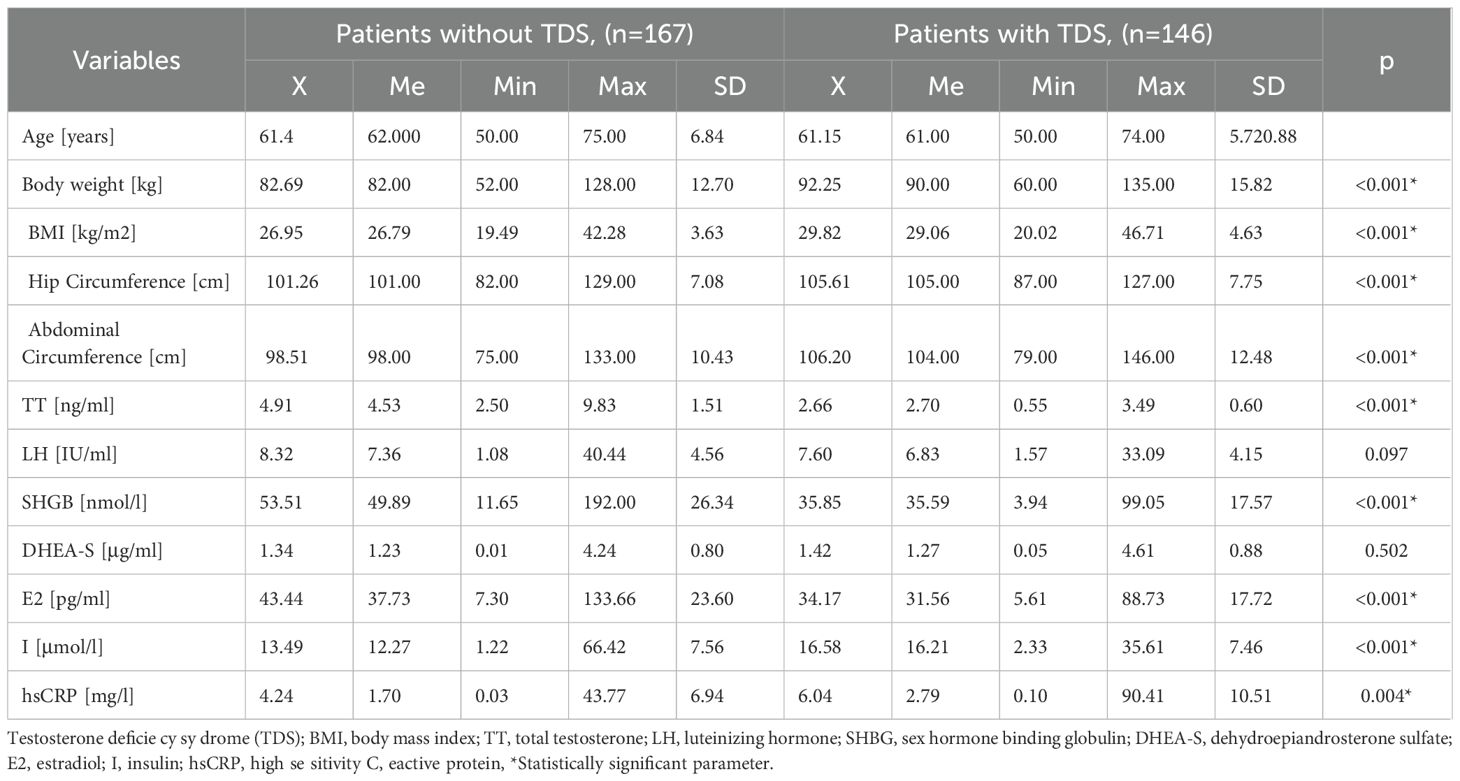
Table 1. Relationship between anthropometric factors, hormone levels, and hsCRP in patients with and without testosterone deficiency.
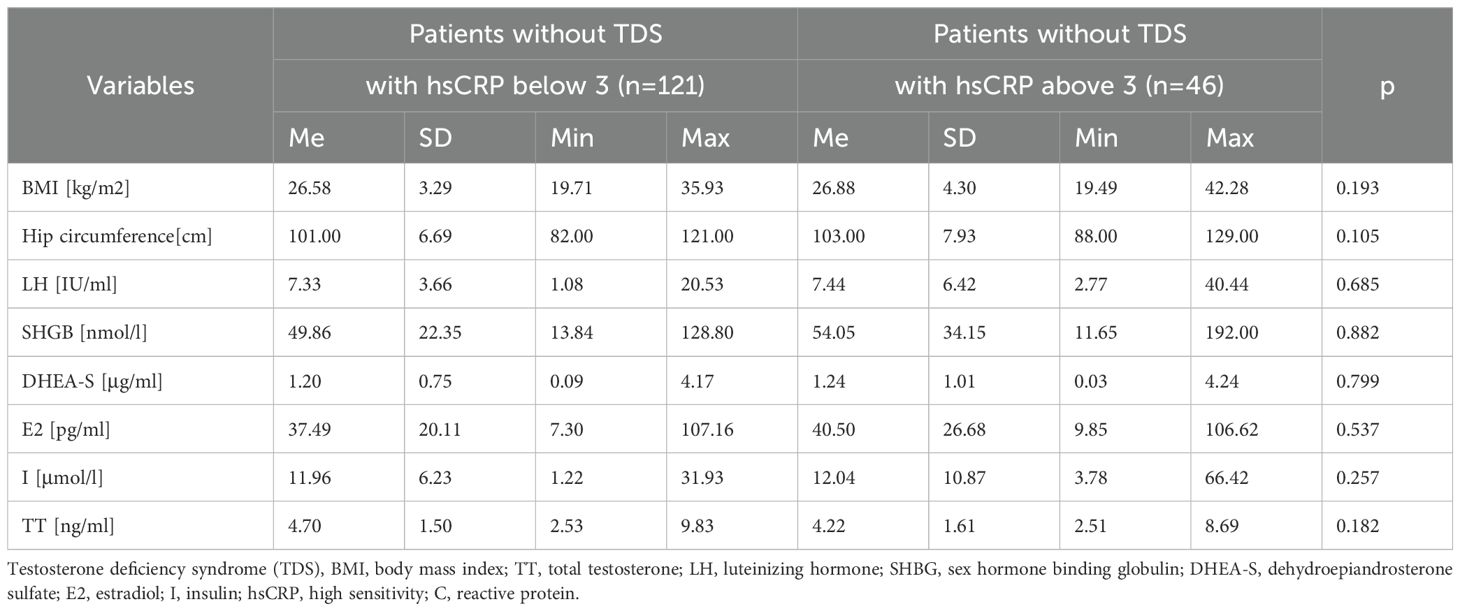
Table 2. Relationship between anthropometric factors, and hormone levels in the group of patients without testosterone deficiency according to hsCRP concentration.
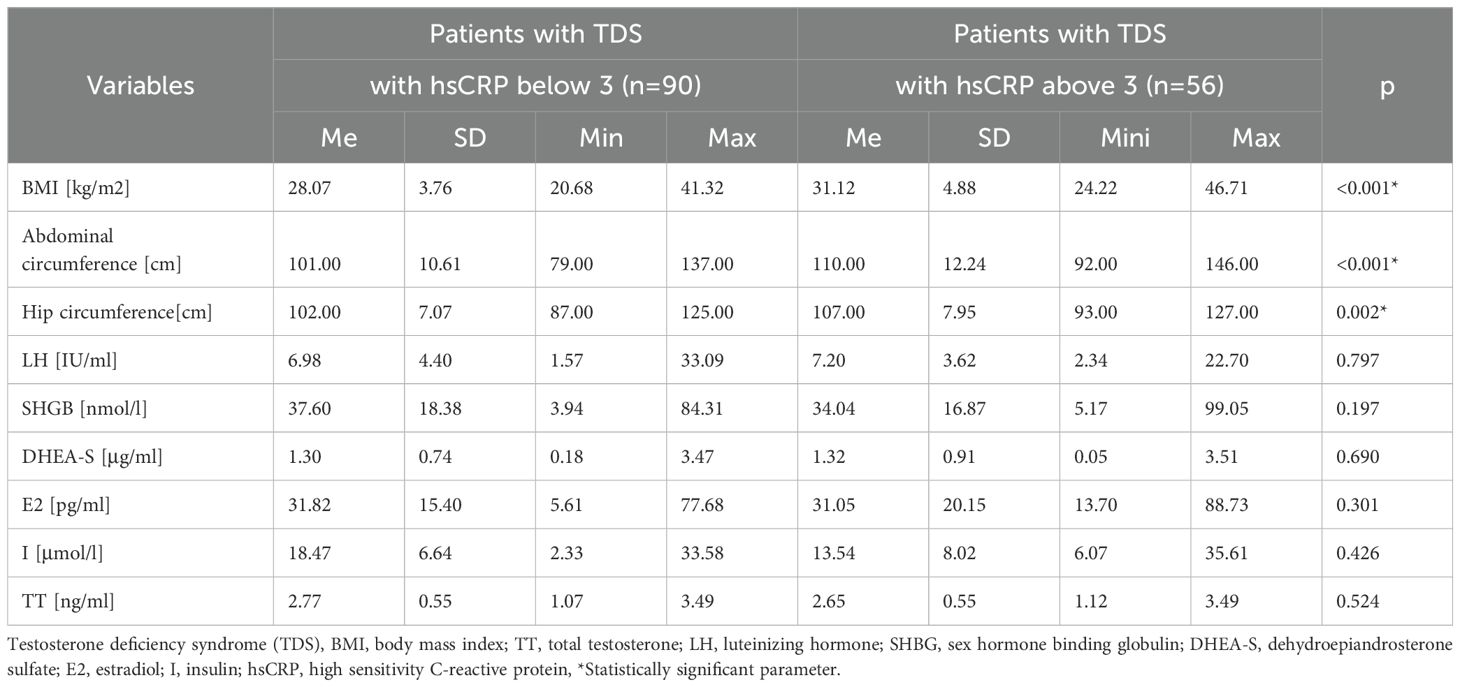
Table 3. The relationship between anthropometric factors, and hormone levels in the group of patients with testosterone deficiency syndrome (TDS) according to hsCRP concentration.
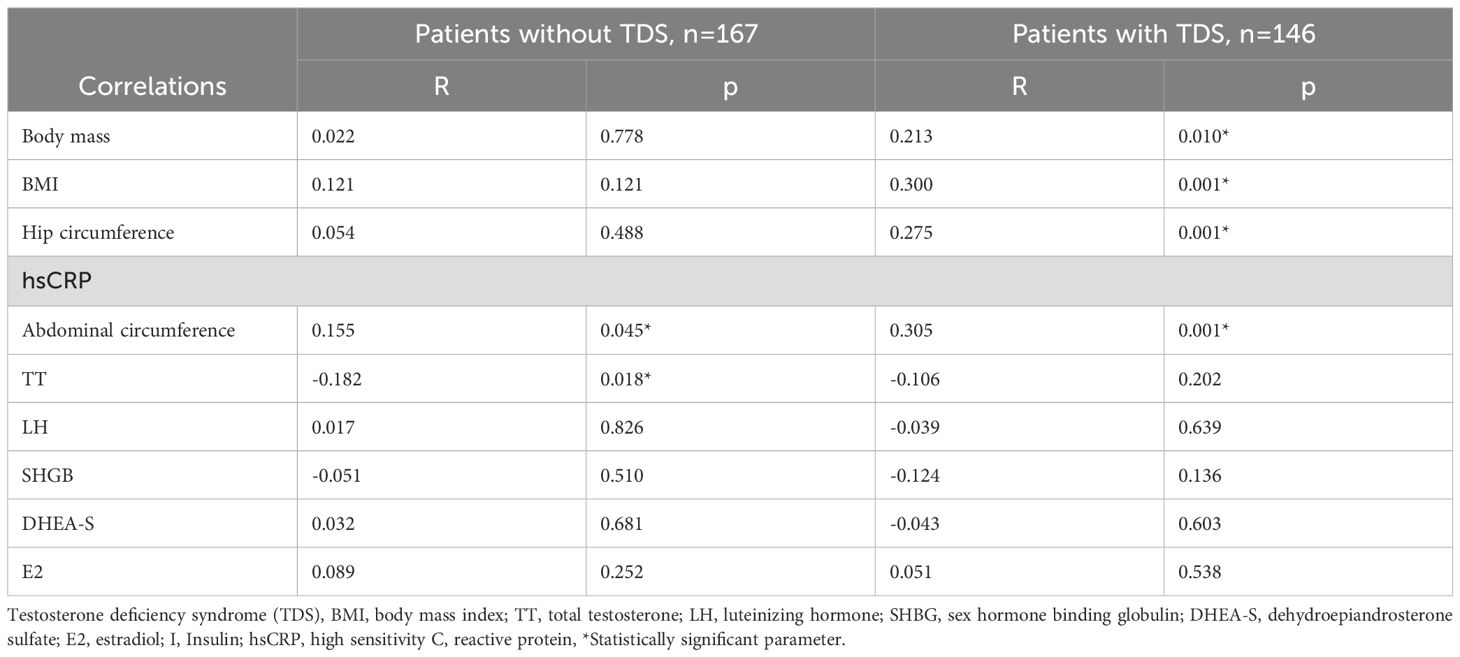
Table 4. Analysis of correlation between anthropometric and hormonal indicators and hsCRp value.
4 Discussion
In recent years, extensive research has delved into the connections between testosterone and the inflammatory process (19). However, the recognition of bidirectional mechanisms linking the immune and endocrine systems dates back at least two decades (20). Testosterone has been associated with the suppression of pro-inflammatory substances and promotion of anti-inflammatory cytokines, potentially contributing to reduced inflammation. Furthermore, assertions regarding the anti-inflammatory properties of testosterone stem from observations of heightened inflammatory cytokine levels in hypogonadal men and reductions in inflammatory markers observed in testosterone supplementation studies (20). Conversely, an inflammatory process, indicative of heightened oxidative stress, has been associated with negative influences on androgen levels (21). This relationship has been noted both through direct disruption of reproductive tissue and by impairing the regulatory mechanisms of the hypothalamic–pituitary–gonadal (HPG) axis.Testosterone deficiency syndrome is diagnosed when low serum testosterone levels coincide with clinical symptoms of hypogonadism. Research involving over 2,000 men in the United States indicated that nearly 39% of men aged over 45 exhibit biochemical indicators of testosterone deficiency (22). In contrast, a study involving 890 men showed that testosterone deficiency was present in 20% of individuals aged 60–89 years, 30% in those aged 70–79, and 50% in participants over 80 years old (23). These results underscore the widespread prevalence of testosterone deficiency in older men when considering biochemical markers.
In our research, higher hsCRP concentrations were associated with elevated BMI values, larger waist and hip circumferences, and higher TAG levels compared to patients with lower concentrations of this parameter. This relationship between hsCRP levels and anthropometric parameters such as body weight and abdominal circumference has been widely documented. For instance, Fernandes et al. (24) reported that individuals who maintained regular physical activity were less likely to exhibit elevated hsCRP levels. Specifically, high physical activity levels were associated with lower hsCRP in both men (OR=0.44 [0.30 to 0.65]) and women (OR=0.35 [0.16 to 0.76]). Among overweight or obese individuals and smokers, those who were constantly active also had a lower likelihood of elevated hsCRP levels compared to their physically inactive peers. Further evidence comes from studies involving individuals with schizophrenia, where BMI and hsCRP have been linked to abnormal lipid profiles (25). A direct association between BMI and hsCRP was observed across demographic variables such as age, sex, ethnicity, and education. Additionally, hsCRP showed an inverse relationship with HDL cholesterol in the overall sample and among those with overweight or obesity, but not in individuals of normal weight. These findings suggest that inflammation and dyslipidemia are more commonly associated with overweight and obesity in individuals with schizophrenia.
Similar conclusions were reached by Buljubasic et al. (26), who found that hsCRP levels may mediate the relationship between primary hypertension and overweight. However, it is important to recognize the limitations of BMI as a measure. While widely used, BMI does not distinguish between lean and fat mass, meaning that individuals with identical BMI values may have significantly different body compositions. For this reason, bioelectrical impedance analysis (BIA) is increasingly recommended as a more precise method for assessing body composition, including the proportions of fat and lean tissue. Moreover, our research findings suggest a positive correlation between hsCRP levels and waist circumference (R=0.155, p=0.045), and a negative correlation with TT (R=-0.182, p=0.018) in patients without TDS. In contrast, among patients with TDS, hsCRP levels were positively associated with body mass (R=0.213, p=0.010), BMI (R=0.300, p=0.001), hip circumference (R=0.275, p=0.001), and waist circumference (R=0.305, p=0.0001).
Tremellen et al. reported that reduced testosterone levels in men were significantly associated with elevated inflammatory markers, particularly in individuals with obesity (27). However, findings by Grandys et al. (2021) indicated that the relationship between testosterone and inflammation markers such as CRP and ferritin (FER) was influenced by body mass index and not independent of it (20). In a cross-sectional study by Maggio et al., involving 473 men over the age of 65 from the InCHIANTI cohort (a population-based study of older adults in the Chianti region of Tuscany, Italy), an inverse correlation was observed between testosterone levels and the concentration of soluble IL-6 receptor (sIL-6r) – a receptor fragment that may enhance IL-6 activity. No similar associations were found for other inflammatory markers. These findings suggest a close interplay between reduced testosterone levels and intensified pro-inflammatory activity in older males (28). Supporting this, Kaplan et al. also reported an inverse association between serum testosterone and high-sensitivity C-reactive protein (hsCRP) in elderly men (29). Other studies have similarly reported associations between low testosterone (hypogonadism) and elevated hsCRP and additional inflammatory markers in aging males (20, 30, 31).
A further prospective study identified a connection between elevated hsCRP levels and reduced concentrations of bioavailable testosterone in both cross-sectional and longitudinal analyses. Notably, this association remained significant after adjusting for potential confounders, and men with higher hsCRP levels were more likely to develop hypogonadism over a ten-year period. It is worth noting that some long-term registry studies have shown that testosterone therapy is associated with progressive reductions in hsCRP levels, for example the study by Yassin et al. (32). However, as these are observational studies, they should be interpreted cautiously due to the possibility of residual confounding and the absence of randomized allocation, which limits the ability to draw causal conclusions.
In contrast, Zhao et al. (2015) conducted a study of 289 younger and 4212 older Chinese participants using a separate-sample Mendelian randomization approach to mitigate reverse causation. Their results did not reveal any significant association between endogenous testosterone and systemic inflammation markers, including hsCRP. Based on these findings, the authors concluded that testosterone may not exert anti-inflammatory effects in the context of chronic diseases linked to low-grade systemic inflammation (33). These discrepancies between observational and genetic studies highlight the complexity of the relationship between testosterone and inflammation and suggest that, although testosterone’s anti-inflammatory properties may be supported by mechanistic and some clinical data, they are not yet definitively established.
In animal models, Crisostomo et al. demonstrated that testosterone administration prior to ischemic events was associated with intensified inflammatory responses in both male and female castrated rats, as evidenced by increased activation of signaling proteins p38 and SPAK/JNK, which are involved in myocardial inflammation (34).
Overall, existing studies suggest a negative correlation between testosterone and inflammatory status. Testosterone therapy has been associated with beneficial modulation of inflammatory pathways and may correspond to clinical improvement. In hypogonadal men, testosterone replacement has been linked to a 39% reduction in mortality risk, with a hazard ratio of 0.61 (95% CI: 0.42–0.88) compared to those not receiving treatment (35). Moreover, testosterone supplementation has been associated with reductions in visceral fat, fasting plasma glucose (FPG), and triglyceride levels in older men, potentially contributing to lower hsCRP levels and a reduced likelihood of cardiovascular events. Traish et al. reported a significantly lower rate of cardiovascular mortality in patients treated with testosterone undecanoate compared to those in the untreated control group (36). Finally, recent evidence indicates that long-term testosterone therapy (lasting at least six months) is consistently associated with decreased hsCRP concentrations in aging men with testosterone deficiency (37, 38).
This study has several limitations. The most significant is the potential for selection bias due to the recruitment method. Participants were volunteers referred by primary care physicians rather than selected from a random population sample. This approach may have attracted individuals who are more health-conscious or have specific pre-existing health concerns, thereby limiting the generalizability of our findings to the broader population of older men. Furthermore, the study did not collect detailed, controlled data on socio-economic status, diet, or lifestyle factors, which prevented adjustment for potential confounders. As a result, the declarative sociodemographic data that was collected may be of limited reliability. Additionally, no information was gathered regarding the specific motivation behind participants’ decisions to take part in the study. Future research should incorporate multi-marker inflammatory profiling, including cytokines such as interleukin-6 (IL-6) and tumor necrosis factor alpha (TNF-α), to provide a more comprehensive understanding of the inflammatory milieu potentially associated with testosterone deficiency syndrome in aging men.
In the conducted study, the presence of TDS was associated with elevated hsCRP levels compared to patients without testosterone deficiency. The concurrent presence of testosterone deficiency and elevated inflammatory markers may correlate with alterations in both biochemical and anthropometric parameters. It is also important to consider that hormonal changes in aging men may be influenced by lifestyle-related factors.
5 Conclusions
In the conducted study, the presence of TDS was associated with elevated hsCRP levels compared to patients without testosterone deficiency. The concurrent presence of testosterone deficiency and elevated inflammatory markers may correlate with changes in both biochemical and anthropometric parameters. It is important to note that age-related hormonal changes in men may also be influenced by modifiable lifestyle factors. Therefore, promoting a healthy lifestyle, regular physical activity, and a balanced diet appears essential for reducing systemic inflammation. Additionally, attention should be given to the potential compounding effects of altered testosterone levels and increased levels of pro-inflammatory cytokines associated with excessive body mass.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The Bioethics Committee of the Pomeranian Medical University in Szczecin (KB-0012/155/16). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
IR: Formal Analysis, Software, Visualization, Writing – review & editing. ŻC: Formal Analysis, Investigation, Methodology, Writing – original draft. AS: Resources, Validation, Writing – review & editing. AR: Conceptualization, Formal Analysis, Methodology, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research received no external funding Institutional Review Board Statement: This research adhered to the guidelines set forth by the Bioethics Committee of the Pomeranian Medical University in Szczecin (KB-0012/159/12), in accordance with the principles outlined in the Helsinki.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of int r st
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Barone B, Napolitano L, Abate M, Cirillo L, Reccia P, Passaro F, et al. The role of testosterone in the elderly: What do we know? Int J Mol Sci. (2022) 23:3535.
2. Kupelian V, Chiu GR, Araujo AB, Williams RE, Clark RV, and McKinlay JB. Association of sex hormones and C-reactive protein levels in men. Clin Endocrinol (Oxf). (2010) 72:527–33.
3. Ebrahimi F, Urwyler SA, Straumann S, Doerpfeld S, Bernasconi L, Neyer P, et al. IL-1 antagonism in men with metabolic syndrome and low testosterone: A randomized clinical trial. J Clin Endocrinol Metab. (2018) 1:3466–76. doi: 10.1210/jc.2018-00739
4. Stefanakis K, Upadhyay J, Ramirez-Cisneros A, Patel N, Sahai A, and Mantzoros CS. Leptin physiology and pathophysiology in energy homeostasis, immune function, neuroendocrine regulation and bone health. Metabolism. (2024) 161:156056.
5. Payne GA, Tune JD, and Knudson JD. Leptin-induced endothelial dysfunction: a target for therapeutic interventions. Curr Pharm Des. (2014) 20:603–8.
7. Finkelstein JS, Lee H, Burnett-Bowie SAM, Pallais JC, Yu EW, Borges LF, et al. Gonadal st roids and body composition, strength, and sexual function in men. N Engl J Med. (2013) 369(11):1011–22. doi: 10.1056/NEJMoa1206168
8. Mohamad NV, Wong SK, Wan Hasan WN, Jolly JJ, Nur-Farhana MF, Ima-Nirwana S, et al. The relationship between ci culating t stost rone and nflammatory cytokines in men. Aging Male. (2019) 22:129–40.
9. Araujo AB, Dixo JM, Sua z EA, Murad MH, Guey LT, and Wittert GA. Clinical review: Endogenous testostero e a d mo tality in m n: a systematic review and meta-analysis. J Clin Endocrinol Metab. (2011) 96:3007–19.
10. Traish A, Bola os J, Nair S, Saad F, and Morgentaler A. Do androgens modulate the pathophysiological pathways of inflammation? Appraising the contemporary evidence. J Clin Med. (2018) 7:549.
11. Fernandez CJ, Chacko EC, and Pappachan JM. Male obesity-related secondary hypogonadism - pathophysiology, clinical implications and management. Eur Endocrinol. (2019) 15:83–90.
12. Osmancevic A, Ottarsdottir K, Hellgren M, Lindblad U, and Daka B. High C-reactive protein is associated with increased risk of biochemical hypogonadism: A population-based cohort study. Endocr. Connect. (2022) 11:e220141.
13. Malkin CJ, Pugh PJ, Jones RD, Kapoor D, Channer KS, and Jones TH. The effect of testosterone replacement on endogenous inflammatory cytokines and lipid profiles in hypogonadal men. J Clin Endocrinol Metab. (2004) 89:3313–8.
14. Nakhai-Pour HR, Grobbee DE, Emmelot-Vonk MH, Bots ML, Verhaar HJ, and van der Schouw YT. Oral testosterone supplementation and chronic low-grade inflammation in elderly men: A 26-week randomized, placebo-controlled trial. Am Heart J. (2007) 154:1228.e1–1228.e7.
15. Flegal KM, Kit BK, Orpana H, and Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. (2013) 309:71–82.
16. Kula K and Słowikowska-Hilczer J. Late-onset hypogonadism in men. Endokrynol. Pol. (2012) 63:15–9.
18. Roberts WL, CDC, and AHA. CDC/AHA Workshop on Markers of Inflammation and Cardiovascular Disease: Application to Clinical and Public Health Practice: laboratory tests available to assess inflammation – performance and standardization: a background paper. Circulation. (2004) 110:e572–6.
19. Gencer B, Bonomi M, Adorni MP, Sirtori CR, Mach F, and Ruscica M. Cardiovascular risk and testosterone - from subclinical atherosclerosis to lipoprotein function to heart failure. Rev Endocr. Metab Disord. (2021) 22:257–74.
20. Grandys M, Majerczak J, Zapart-Bukowska J, Duda K, Kulpa JK, and Zoladz JA. Lowered serum testosterone concentration is associated with enhanced inflammation and worsened lipid profile in men. Front Endocrinol (Lausanne). (2021) 12:735638.
21. Darbandi M, Darbandi S, Agarwal A, Sengupta P, Durairajanayagam D, Henkel R, et al. Reactive oxygen species and male reproductive hormones. Reprod Biol Endocrinol. (2018) 16:87.
22. Mulligan T, Frick MF, Zuraw QC, Stemhagen A, and McWhirter C. Prevalence of hypogonadism in males aged at 45 years: the HIM Study. Int J Clin Pract. (2006) 60(7):762–9. doi: 10.1111/j.1742-1241.2006.00992.x
23. Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR, and Baltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free testosterone levels in healthy men: Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. (2001) 86(2):724–31. doi: 10.1210/jcem.86.2.7219
24. Fernandes RA, Ritti-Dias RM, Balagopal PB, Conceição RDO, Santos RD, Cucato GG, et al. Self-initiated physical activity is associated with high sensitivity C-reactive protein: A longitudinal study in 5,030 adults. Atherosclerosis. (2018) 273:131–5. doi: 10.1016/j.atherosclerosis.2018.02.011
25. Boozalis T, Devaraj S, and Okusaga OO. Correlations between body mass index, plasma high-sensitivity C-reactive protein and lipids in patients with schizophrenia. Psychiatr Q. (2019) 90:101–10.
26. Buljubasic D, Drenjancevic I, Kibel A, Zibar L, Vizjak V, Mandic S, et al. Myeloperoxidase (MPO) and high sensitivity C-reactive protein (hsCRP) as inflammatory biomarkers of endothelial and leukocyte activation in overweight hypertensive patients. Arterial Hypertension. (2021) 25:15–21.
27. Tremellen K, McPhee N, and Pearce K. Metabolic endotoxaemia related inflammation is associated with hypogonadism in overweight men. Basic Clin Androl. (2017) 27:5.
28. Maggio M, Basaria S, Ceda GP, Ble A, Ling SM, Bandinelli S, et al. The relationship between testosterone and molecular markers of inflammation in older men. J Endocrinol Invest. (2005) 28:116–9.
29. Kaplan SA, Johnson-Levonas AO, Lin J, Shah AK, and Meehan AG. Elevated high sensitivity C-reactive protein levels in aging men with low testosterone. Aging Male. (2010) 13:108–12.
30. Bhatia V, Chaudhuri A, Tomar R, Dhindsa S, Ghan m H, and Dandona P. Low testosterone and high C-reactive protein concentrations p edict low h matocrit in type 2 d ab t s. Diabetes Care. (2006) 29:2289–94.
31. Nakhai Pour HR, Grobbee DE, and Mull r M. an der Schouw, Y.T. Association of endogenous sex hormone with C-reactive protein levels in middle-aged and elderly men. Clin Endocrinol. (2007) 66:394–8.
32. Yassin AA, Nettleship J, Almehmadi Y, Salman M, and Saad F. Effects of continuous long-term testosterone therapy (TTh) on anthropometric, endocrine and metabolic parameters for up to 10 years in 115 hypogonadal elderly men: real-life experience from an observational registry study. Andrologia. (2016) 48:793–9. doi: 10.1111/and.12514
33. Zhao J, Jia g C, Lam TH, Liu B, Ch ng KK, Xu L, et al. Ge etically predicted testosterone and systemic inflammation in men: a separate -sample Mendelian randomization a alysis in older Chinese men. PloS One. (2015) 10:e0126442.
34. Crisostomo PR, Wang M, Wairiuko GM, et al. Brief exposure to exogenous testosterone increases death signaling and adversely affects myocardial function after ischemia. Am J Physiol Regul Integr Comp Physiol. (2006) 290:R1168–74.
35. Shores MM, Smith NL, Forsberg CW, Anawalt BD, and Matsumoto AM. Testosterone treatment and mortality in men with low testosterone levels. J Clin Endocrinol Metab. (2012) 97:2050–8.
36. Traish AM, Haider A, Haider KS, Doros G, and Saad F. Long-term testosterone therapy improves cardiometabolic function and reduces risk of cardiovascular disease in men with hypogonadism: A real-life observational registry study setting comparing treated and untreated (Control) groups. J Cardiovasc Pharmacol Ther. (2017) 22:414–33. doi: 10.1177/1074248417691136
37. Vertkin AL, Naumov AV, Morgunov LY, Kalinchenko SY, Krivtsova EV, Arinina EN, et al. Testosterone effects on cardiovascular risk factors in men with metabolic syndrome. Cardiovasc Ther Prev. (2008) 7:68–75.
Keywords: testosterone, aging men, Hs-CRP, hormonal, deficiency
Citation: Rotter I, Ciosek Ż, Syroka A and Ryl A (2025) A cross-sectional study of testosterone deficiency and inflammatory markers in older men. Front. Endocrinol. 16:1606949. doi: 10.3389/fendo.2025.1606949
Received: 14 May 2025; Accepted: 17 July 2025;
Published: 31 July 2025.
Edited by:
Phiwayinkosi V. Dludla, University of Zululand, South AfricaReviewed by:
Genaro Christian Barrientos, University of Chile, ChileFarid Saad, Gulf Medical University, United Arab Emirates
Copyright © 2025 Rotter, Ciosek, Syroka and Ryl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aleksandra Ryl, YWxla3NhbmRyYS5yeWxAcHVtLmVkdS5wbA==