 Stephen Ludgate1,2*†
Stephen Ludgate1,2*† Anne McGowan1,2†Carla Moran3,4,5†Roberto Attanasio6†
Anne McGowan1,2†Carla Moran3,4,5†Roberto Attanasio6† Miloš Žarković7†
Miloš Žarković7† Endre Vezekenyi Nagy8†
Endre Vezekenyi Nagy8† Roberto Negro9†
Roberto Negro9† Enrico Papini10†Chagit Adler Cohen11
Enrico Papini10†Chagit Adler Cohen11 Ersin Akarsu12†
Ersin Akarsu12† Maria Alevizaki13†Göksun Ayvaz14†Tomasz Bednarczuk15†Biljana Nedeljković Beleslin7†Eszter Berta8†
Maria Alevizaki13†Göksun Ayvaz14†Tomasz Bednarczuk15†Biljana Nedeljković Beleslin7†Eszter Berta8† Miklos Bodor8†
Miklos Bodor8† Anna Maria Borissova16†
Anna Maria Borissova16† Mihail Boyanov17,18†Camille Buffet19†
Mihail Boyanov17,18†Camille Buffet19† Maria-Cristina Burlacu20†Jamina Ćirić7†
Maria-Cristina Burlacu20†Jamina Ćirić7† Juan J. Díez21,22,23†Harald Dobnig24,25†Valentin Fadeyev26†Benjamin C. T. Field27†
Juan J. Díez21,22,23†Harald Dobnig24,25†Valentin Fadeyev26†Benjamin C. T. Field27† Eric Fliers28†Dagmar Führer-Sakel29†
Eric Fliers28†Dagmar Führer-Sakel29† Juan Carlos Galofré30,31†
Juan Carlos Galofré30,31† Tommi Hakala32†Jan Jiskra33†
Tommi Hakala32†Jan Jiskra33† Peter A. Kopp34†
Peter A. Kopp34† Michael Krebs35†
Michael Krebs35† Michal Kršek33†Martin Kužma36†
Michal Kršek33†Martin Kužma36† Ivica Lazúrová37†Laurence Leenhardt19†Vitaliy Luchytskiy38†Miguel Melo39†
Ivica Lazúrová37†Laurence Leenhardt19†Vitaliy Luchytskiy38†Miguel Melo39† Saara Metso40†
Saara Metso40† Tatyana Morgunova26†
Tatyana Morgunova26† Dan Alexandru Niculescu41†
Dan Alexandru Niculescu41† Božidar Perić42†
Božidar Perić42† Tereza Planck43†
Tereza Planck43† Catalina Poiana41†
Catalina Poiana41† Francisca Marques Puga44†
Francisca Marques Puga44† Eyal Robenshtok45†Patrick Rosselet46†
Eyal Robenshtok45†Patrick Rosselet46† Marek Ruchala47†Kamilla Ryom Riis48†
Marek Ruchala47†Kamilla Ryom Riis48† Alla Shepelkevich49†Mykola D. Tronko50†Jacob Stampe Frølich48
Alla Shepelkevich49†Mykola D. Tronko50†Jacob Stampe Frølich48 David Unuane51†Irfan Vardarli52,53†
David Unuane51†Irfan Vardarli52,53† W. Edward Visser54†Andromachi Vryonidou55†
W. Edward Visser54†Andromachi Vryonidou55† Younes Ramazan Younes56†Elena Yurenya57Petros Perros58†
Younes Ramazan Younes56†Elena Yurenya57Petros Perros58† Laszlo Hegedüs48†
Laszlo Hegedüs48†- 1The School of Medicine, Trinity College Dublin, The University of Dublin, Dublin, Ireland
- 2Robert Graves Institute, Tallaght University Hospital, Dublin, Ireland
- 3Diabetes and Endocrinology Section, Beacon Hospital, Dublin, Ireland
- 4School of Medicine, University College Dublin, Dublin, Ireland
- 5Endocrine Department, St Vincent’s University Hospital, Dublin, Ireland
- 6Scientific Committee Associazione Medici Endocrinologi, Udine, Italy
- 7Faculty of Medicine, University of Belgrade, Belgrade, Serbia
- 8Division of Endocrinology, Department of Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 9Division of Endocrinology V.Fazzi Hospital, Department of Experimental Medicine, University of Salento, Lecce, Italy
- 10Department of Endocrinology and Metabolism, Regina Apostolorum Hospital, Lifenet Health Group, Rome, Italy
- 11Rabin Medical Center, Tel-Aviv University, Tel-Aviv, Israel
- 12Department of Internal Medicine, Division of Endocrinology, Faculty of Medicine, Gaziantep University, Gaziantep, Türkiye
- 13Endocrine Unit and Diabetes Centre, Department of Clinical Therapeutics, Alexandra Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
- 14Koru Ankara Hospital, Department of Endocrinology and Metabolism, Ankara, Türkiye
- 15Department of Internal Medicine and Endocrinology, Medical University of Warsaw, Warsaw, Poland
- 16Clinic of Endocrinology and Metabolism, University Hospital “Sofiamed”, Medical Faculty, Sofia University “Saint Kliment Ohridski”, Sofia, Bulgaria
- 17Clinic of Endocrinology and Metabolism, University Hospital “Alexandrovska”, Sofia, Bulgaria
- 18Department of Internal Medicine, Medical University, Sofia, Bulgaria
- 19Sorbonne Universitè, GRC n16, GRC Thyroid Tumors, Thyroid Pathology and Endocrine Tumor Department, AP-HP, Hôpital Pitié-Salpêtriére, Paris, France
- 20Department of Endocrinology and Nutrition, Cliniques Universitaires St-Luc, Université Catholique de Louvain, Brussels, Belgium
- 21Department of Endocrinology, Hospital Universitario Puerta de Hierro Majadahonda, Madrid, Spain
- 22Instituto de Investigación Sanitaria Puerta de Hierro Segovia de Arana, Madrid, Spain
- 23Department of Medicine, Universidad Autónoma de Madrid, Madrid, Spain
- 24Thyroid Endocrinology Osteoporosis Institute Dobnig, Graz, Austria
- 25Thyroid Practice for Radiofrequency Ablation, Vienna, Austria
- 26Department of Endocrinology No. 1, N.V. Sklifosovsky Institute of Clinical Medicine, I.M. Sechenov First Moscow State Medical University, Moscow, Russia
- 27Section of Clinical Medicine, Faculty of Health and Medical Sciences, University of Surrey, Guildford, United Kingdom
- 28Department of Endocrinology & Metabolism, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
- 29Department of Endocrinology, Diabetes and Metabolism, University Hospital Essen, University-Duisburg-Essen, Essen, Germany
- 30Department of Endocrinology, Clínica Universidad de Navarra, Pamplona, Spain
- 31Instituto de Investigación Sanitaria de Navarra, Pamplona, Spain
- 32Department of Surgery, Tampere University Hospital, Tampere, Finland
- 333rd Department of Medicine, 1st Faculty of Medicine, Charles University, General University Hospital, Prague, Czechia
- 34Division of Endocrinology, Diabetology and Metabolism, University of Lausanne, Lausanne, Switzerland
- 35Internal Medicine III, Division of Endocrinology, Medical University of Vienna, Vienna, Austria
- 365th Department of Internal Medicine, Medical Faculty of Comenius University and University Hospital, Bratislava, Slovakia
- 37P.J. Šafárik University Košice, 1st Department of Internal Medicine of the Medical Faculty, Košice, Slovakia
- 38Department of Reproductive Endocrinology, Institute of Endocrinology and Metabolism Named After V.P. Komissarenko, National Academy of Medical Science of Ukraine, Kyiv, Ukraine
- 39Department of Endocrinology, Diabetes and Metabolism Coimbra Local Health Unit, Medical Faculty, University of Coimbra, Coimbra, Portugal
- 40Department of Endocrinology, Tampere University Hospital, Tampere, Finland
- 41Department of Endocrinology, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania
- 42Department of Endocrinology, Diabetes and Metabolic Diseases “Mladen Sekso”, University Hospital Center “Sisters of Mercy”, Zagreb, Croatia
- 43Department of Endocrinology, Skåne University Hospital, Malmö, Sweden
- 44Serviço de Endocrinologia, Diabetes e Metabolismo, ULS São João, Porto, Portugal
- 45Endocrinology Institute, Rabin Medical Center, Gray Faculty of Medicine, Tel Aviv University, Tel-Aviv, Israel
- 46Cabinet Médical 2, Rue Bellefontaine, Lausanne, Switzerland
- 47Department of Endocrinology, Metabolism and Internal Medicine, Poznan University of Medical Sciences, Poznan, Poland
- 48Department of Endocrinology, Odense University Hospital, Odense, Denmark
- 49Department of Endocrinology, Belarusian State Medical University, Minsk, Belarus
- 50V.P. Komissarenko Institute of Endocrinology and Metabolism, National Academy of Medical Science of Ukraine, Kyiv, Ukraine
- 51Department of Internal Medicine, Endocrine Unit, UZ Brussel, Vrije Universiteit Brussel, Brussels, Belgium
- 52Department of Medicine I, Klinikum Vest GmbH Knappschaftskrankenhaus Recklinghausen, Academic Hospital, Ruhr-University Bochum, Recklinghausen, Germany
- 535th Medical Department, Division of Endocrinology and Diabetes, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany
- 54Rotterdam Thyroid Center, Department of Internal Medicine, Erasmus MC, Rotterdam, Netherlands
- 55Department of Endocrinology and Diabetes Centre, Hellenic Red Cross Hospital, Athens, Greece
- 56East Surrey Hospital, Surrey and Sussex Healthcare NHS Trust, Redhill, United Kingdom
- 57Minsk Endocrinology Medical Center, Minsk, Belarus
- 58Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom
Purpose: Treatment-resistant depression (TRD) is most commonly defined as depression that has not responded to two different pharmacological agents used for an adequate period of time. We explored the views of European specialists via survey, regarding the use of thyroid hormone (TH) in euthyroid patients with TRD as part of ‘Treatment of Hypothyroidism in Europe by Specialists: An International Survey’ (THESIS).
Methods: The question “Thyroid hormones may be indicated in biochemically euthyroid patients with treatment resistant depression” was posed to specialists from 28 countries.
Results: 5695 valid responses were received following 17,232 invitations (33.0% response rate; 65% female, 90% endocrinologists). 348 (6.1%) stated that TH may be indicated in biochemically euthyroid patients with TRD. This view was more common in males (p<0.01), respondents who saw ≥100 patients with hypothyroidism per year (p<0.01), respondents who worked in private practice (p=0.05) and respondents who were not members of international specialist associations (p=0.05). Geographical variation existed with respondents in Eastern Europe significantly more likely to use TH in TRD (p<0.01). Linear regression showed a statistically significant reduction in the use of TH for TRD with increasing gross national income (F-statistic=7.35, CI -0.15 - -0.02, p=0.01). TH in TRD was recommended in psychiatry guidelines but not endocrinology guidelines.
Conclusion: While there is limited evidence for their use, over 6% of respondents stated that TH may be indicated in TRD. Due to the risk of iatrogenic thyrotoxicosis and increased morbidity the use of TH should be addressed in relevant endocrinology guidelines and consensus should be reached between specialties.
Introduction
Treatment of Hypothyroidism in Europe by Specialists: An International Survey (THESIS) is a large European survey examining the views of the use of thyroid hormones (TH) among thyroid specialists in Europe. The survey was undertaken between 2019–2021 and most countries have previously published their national data (1–21).
The purpose of the THESIS survey was to evaluate the clinical practices of thyroid specialists across Europe for both evidence-based purposes as well as non-typical uses for TH (22, 23). Here, we report data with respect to thyroid specialists’ views on the use of TH in biochemically euthyroid patients with treatment-resistant depression (TRD).
Inconsistency in the literature exists regarding the definition of TRD and a unified international guideline definition is lacking. The most frequently used definition is a diagnosis of depression that previously failed two treatments with antidepressant medications, following adequate dose and duration (24).
The association between the thyroid gland and psychiatric disorders was first described by Parry in his posthumous paper in 1825 where he described an increased incidence of “nervous affectations” in patients with thyroid disorders (25). Over the last 50 years, data examining the relationship between the thyroid gland and psychiatric disorders, specifically depression has emerged, and there is a bi-directional association between hypo- as well as hyperthyroidism and psychiatric disorders, including depression (26, 27). Changes in the hypothalamic-pituitary-thyroid (HPT) axis in patients experiencing depression have been investigated and subsequently the role of TH in treating depression on the HPT axis has been explored (28). The hypothesis for many of these studies is that changes observed in the HPT-axis may be explained by cerebral serotonin deficiency and treatment with liothyronine (T3) may reverse this change (28, 29).
Studies exist examining the connection between hypothyroidism and depression and a number of trials have been performed examining the role of TH in the treatment of depression (26, 27). Initial trials examining T3 as an augmentation agent for individuals who did not respond to antidepressants took place in the 1960s and 1970s (30–32). Those trials reported a benefit in supplementing standard treatment with T3 in patients with depression. A meta-analysis published in 2001 supported the use of T3 in the augmentation of tricyclic antidepressants (33). Since then, a number of placebo-controlled trials examining the role of T3 in the treatment of depression and TRD were performed. A large systematic review and network meta-analysis in 2022 examining augmentation agents in TRD suggested that T3 was an effective augmentation agent in the disease (34). However, a Danish systematic review and meta-analysis in 2020 did not support the use of TH in TRD and a 2015 review of augmentation agents also suggested that additional data were required to advise the use of TH in TRD, so its use remains controversial (35, 36). Despite this, TH is currently recommended as an augmentation agent in TRD in a number of national and international psychiatric guidelines (37, 38). Its use, however, is not currently recommended in any national or international guidelines on hypothyroidism (39). There is little evidence to support the use of levothyroxine (T4) in the management of TRD and it is not currently recommended in any national or international guideline on depression or hypothyroidism (37, 39).
The aim of this manuscript was to document the characteristics and views of thyroid specialists from the 28 countries who participated in the THESIS survey with respect to the use of TH in biochemically euthyroid patients with TRD.
Material and methods
Ethical approval for this study was obtained from the relevant institutional review board, and the research was conducted in accordance with the principles outlined in the Declaration of Helsinki. This study is a sub-analysis of the THESIS survey, which has previously been described in detail (22, 23). It is an anonymous online survey which was conducted between 2019 and 2021. The online questionnaire (see Supplementary Data) consisted of eight questions about physician characteristics and twenty-three questions concerning the use of TH in various clinical settings. The questionnaire was initially developed in English and then tested in a pilot study which was distributed to Italian endocrinologists (1).
Guidelines for internet-based electronic surveys (CHERRIES) were followed in this study (40). European countries with a population of over 4 million people were selected for the survey and thyroid specialists who were members of national endocrine and/or thyroid scientific professional organizations were targeted. The project was overseen by a Steering Committee (LH, EVN, EP, PP, RA, and RN). Two national leads from each participating country, along with the Steering Committee, ensured the authenticity of the data collected.
The key question for this analysis was whether “Thyroid hormones may be indicated in biochemically euthyroid patients with depression resistant to antidepressant medications.” Previous sub analyses examined responses for the use of TH in antibody positive women with unexplained infertility, euthyroid patients with enlarging goiter and euthyroid patients with obesity (41–43).
Geographic regions were defined in accordance with the United Nations Statistics Division (UNSD) definition: Northern Europe (Denmark, Finland, Ireland, Sweden, UK); Western Europe (Austria, Belgium, France, Germany, the Netherlands, Switzerland); Southern Europe (Croatia, Greece, Italy, Portugal, Serbia, Slovenia, Spain); Eastern Europe (Belarus, Bulgaria, Czech Republic, Hungary, Poland, Romania, Russian Federation, Slovakia, Ukraine); and Western Asia (Israel, Turkey) (44). Data on gross national income (GNI) per capita in USD via the Atlas methodology was taken from the World Bank Data Catalogue from 2024 (45). Rates of antidepressant prescribing in Europe were taken from the Organisation of Economic Co-operation and Development (OECD) pharmaceutical consumption data on antidepressants for the year 2020, where data was available for countries that participated in the THESIS survey (46). These data is given in defined daily doses per 1000 inhabitants per day.
On completion of the survey, authors established if each country had (A) national guidelines for the treatment of thyroid diseases, including hypothyroidism, (B) national guidelines for the treatment of depression or specific guidelines for TRD and (C) whether these guidelines addressed the use of TH in depression or TRD. In cases where national guidelines were absent, project leaders investigated whether any specific international guidelines were officially recommended by each country’s national society, and whether these guidelines supported or discouraged the use of TH in depression or TRD. Where it was unclear whether national guidelines existed, national leads were contacted.
Statistical analyses
Only responses containing complete demographic information were included in the analysis. Statistical analyses were conducted using ‘R’ software (47). Survey data were not weighted, reflecting the characteristics of the information collected. Qualitative variables were presented as frequencies or proportions, while quantitative variables were presented as means with standard deviations.
To evaluate associations between qualitative variables, chi-square and Cramer’s V tests were employed. When applicable, linear regression analyses were performed using the statistical and ordinal R packages (48). A significance level of 5% was applied to all analyses. Effect size, reported alongside p-values, was used to determine the practical relevance of results, following guidelines to avoid emphasizing statistically significant but practically irrelevant findings (49, 50). Cramer’s V was interpreted using Rea and Parker’s scale, where values below 0.1 indicated insignificant associations, values between 0.1 and 0.2 indicated weak associations, values between 0.2 and 0.4 were moderate, values between 0.4 and 0.6 were relatively strong, and values above 0.6 indicated strong associations (49).
Results
Baseline characteristics of all respondents
We received 5695 valid responses following 17,232 invitations (33.0% valid response rate). The characteristics of these respondents have previously been described in detail (22, 23). The characteristics are summarized in Table 1 and the response rates of each group as to whether they prescribe TH in biochemically euthyroid patients with TRD. Of note, 65.0% were female (3700/5695), 90.1% were endocrinologists (5132/5695) and the mean age was 49 ± 12 years. 78.8% of respondents had more than 10 years in clinical practice (4487/5693) and 83.4% treated over 50 patients with hypothyroidism each year (4732/5677).
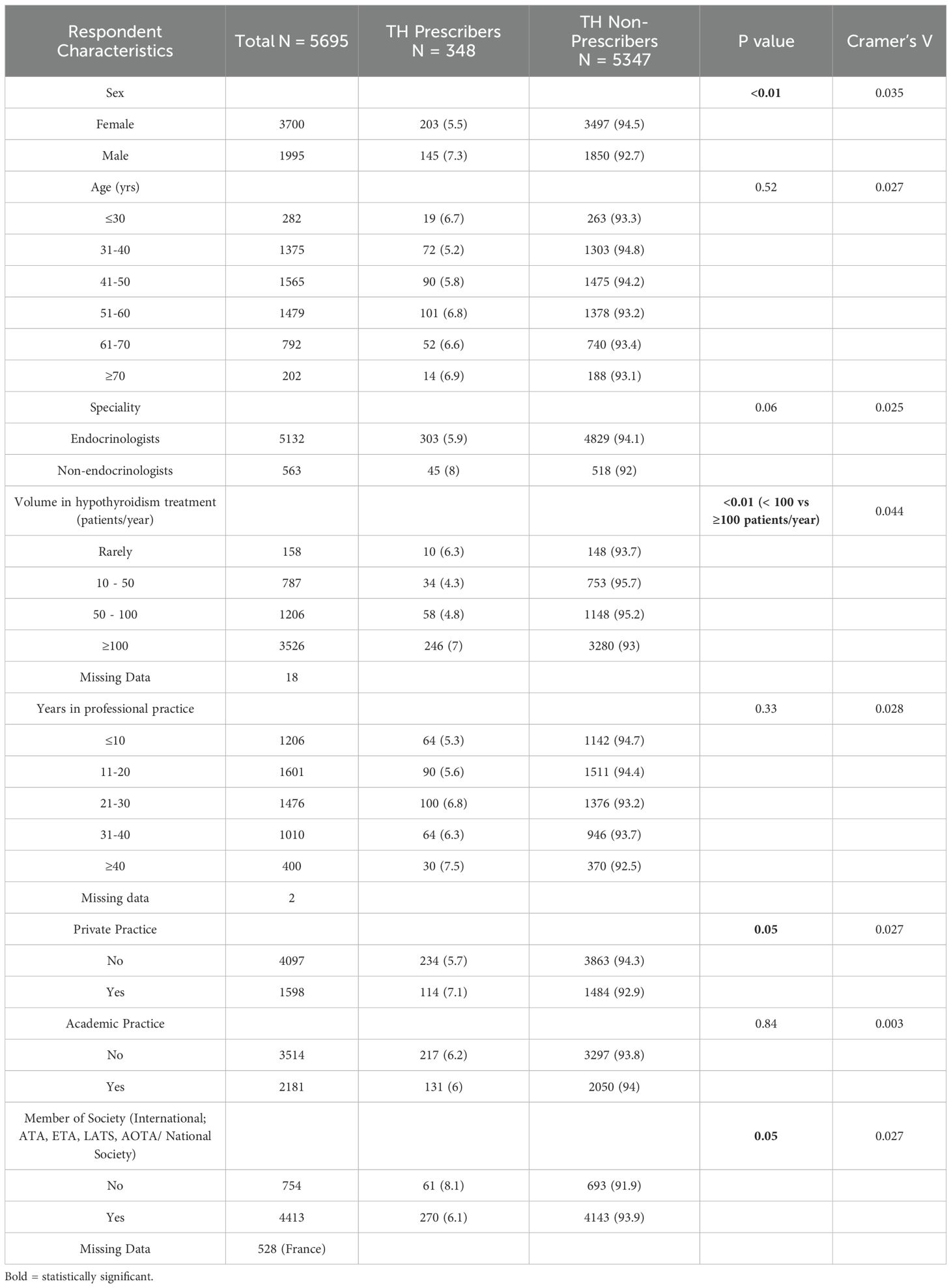
Table 1. Table showing number of respondents in each category, response of each group, p value and Cramers’ V for each characteristic.
Baseline characteristics and demographics of respondents who consider TH for biochemically euthyroid patients with TRD
Of the valid responses received, 348 (6.1%) of the 5695 respondents stated that TH might be indicated in the treatment of biochemically euthyroid patients with TRD (Table 1). Male respondents more commonly thought that TH was indicated compared to female respondents (7.3% vs. 5.5% p<0.01, Cramer’s V 0.035). Physicians who were not members of international endocrinology organizations or societies were more likely to prescribe TH in TRD (8.1% vs. 6.1%, p = 0.05, Cramer’s V = 0.027).
Of those respondents who considered TH in biochemically euthyroid patients with TRD, 70.7% (246/348) treated ≥100 patients with hypothyroidism per year (7% vs 4.7%, p < 0.01, Cramer’s V = 0.044). Of these 246 respondents, 94.7% were endocrinologists (233/246) with 36.2% (89/246) practicing in an academic center. In the THESIS survey, non-endocrinologists more commonly considered prescribing TH in biochemically euthyroid patients with TRD than endocrinologists, however this was not statistically significant (8% vs. 5.9%, p = 0.06, Cramer’s V = 0.025).
Age of respondents or years in clinical practice were not associated with differences in the rates of prescribing TH in biochemically euthyroid patients with TRD.
Academic practice was also not associated with differences in TH prescribing in TRD, however physicians engaging in private practice were more likely to use TH for this indication (7.1% vs. 5.7%, p = 0.05, Cramer’s V = 0.027).
National and regional variations associated with prescribing of TH in biochemically euthyroid patients with TRD
The responses from national regional groups showed a wide variation on the attitude towards the use of TH in biochemically euthyroid patients with TRD. These findings have been summarized in Table 2. The highest proposed rates of prescription of TH for TRD were seen in Serbia (22.2%), Bulgaria (15.8%) and Slovakia (12.2%) with the lowest prescription rates seen in Ireland, Sweden (both 2.6%) and Italy (1.7%) (Figure 1). There was a statistically significant difference between Eastern and Northern, Southern and Western European respondents combined with regards to the use of TH in TRD (8.6% vs. 5%, p < 0.01, Cramer’s V = 0.067) (Figure 2).
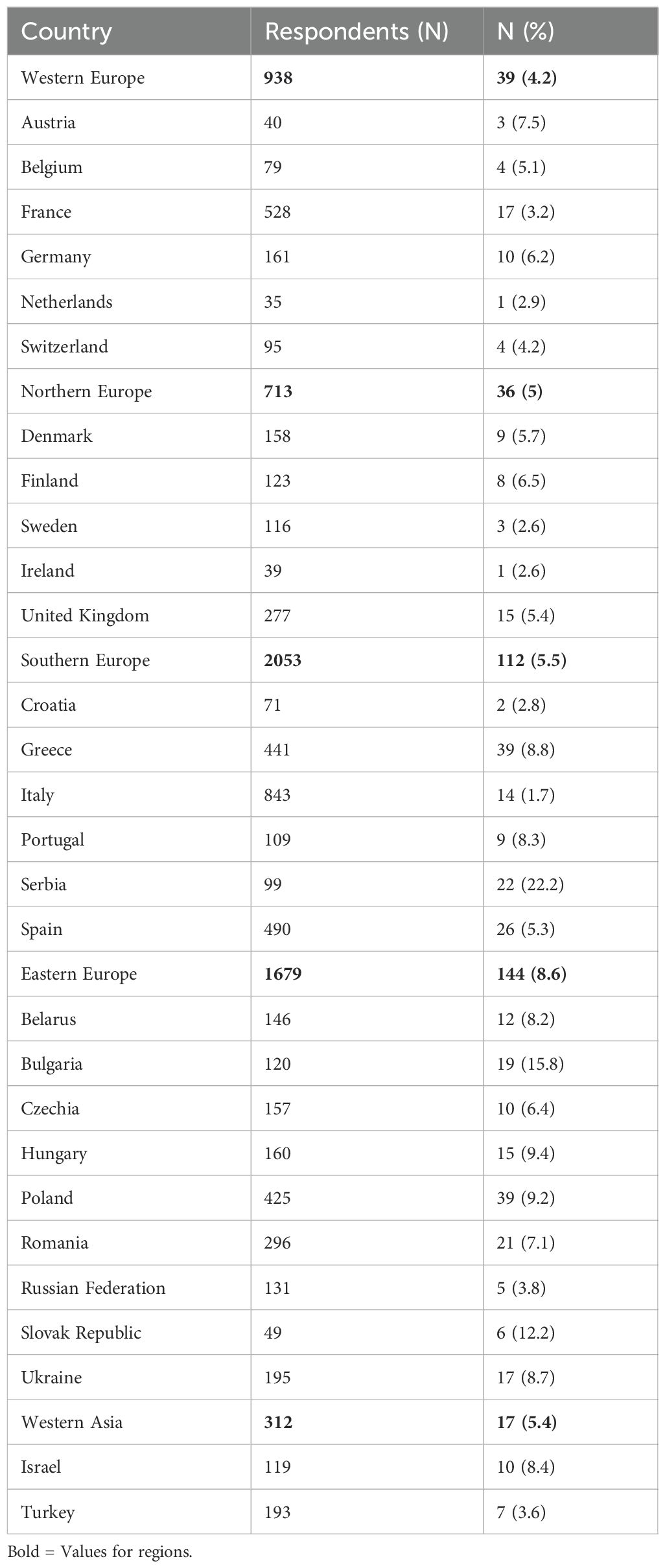
Table 2. Table showing the number of respondents with positive response rate (and %) for each country in the THESIS survey.
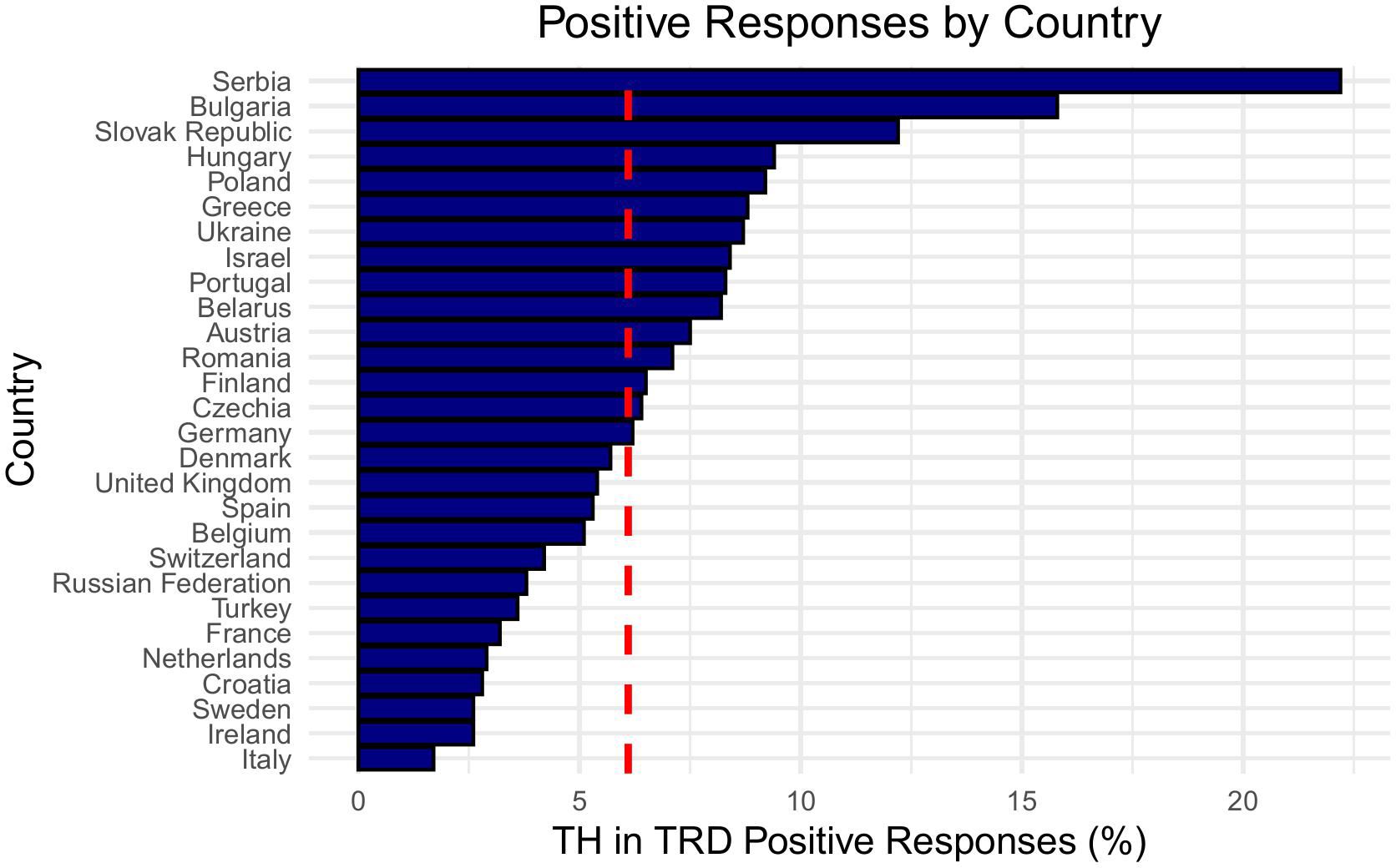
Figure 1. Bar chart showing positive responses by country, ranked from highest to lowest. Serbia leads with the highest percentage, followed by Bulgaria and the Slovak Republic. Italy has the lowest percentage. The x-axis represents percentage of positive responses, with a red dashed line showing the mean positive response rate of 6.1%.
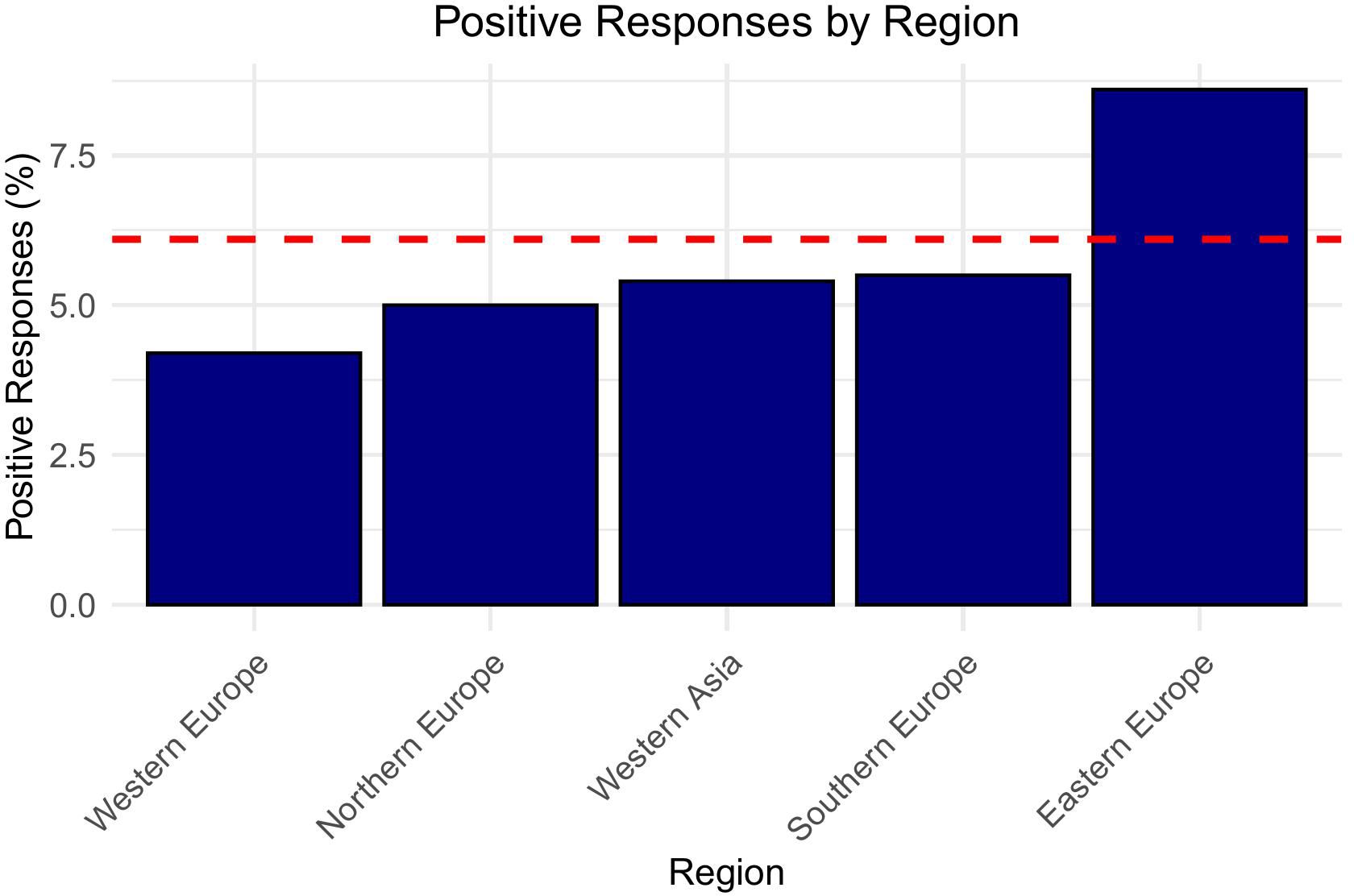
Figure 2. Bar graph titled “Positive Responses by Region” shows positive response percentages for five regions: Western Europe, Northern Europe, Western Asia, Southern Europe, and Eastern Europe. Eastern Europe has the highest percentage, above a red dashed line representing the mean positive response rate of 6.1%.
Prevalence of prescription of anti-depressant medications
Countries included in the THESIS study, which were also included in the OECD antidepressant consumption data in 2020, demonstrate heterogeneity in prescribing anti-depressant medication across the participating nations. Anti-depressant medications were most commonly prescribed in the UK, Portugal and Sweden and least commonly in Croatia, Hungary and Poland. We found that TH use in TRD was not statistically associated with the rates of antidepressant prescribing in countries with available data (F- statistic: 0.1661, CI: −0.055 to 0.037, p-value: 0.6884) (Figure 3).
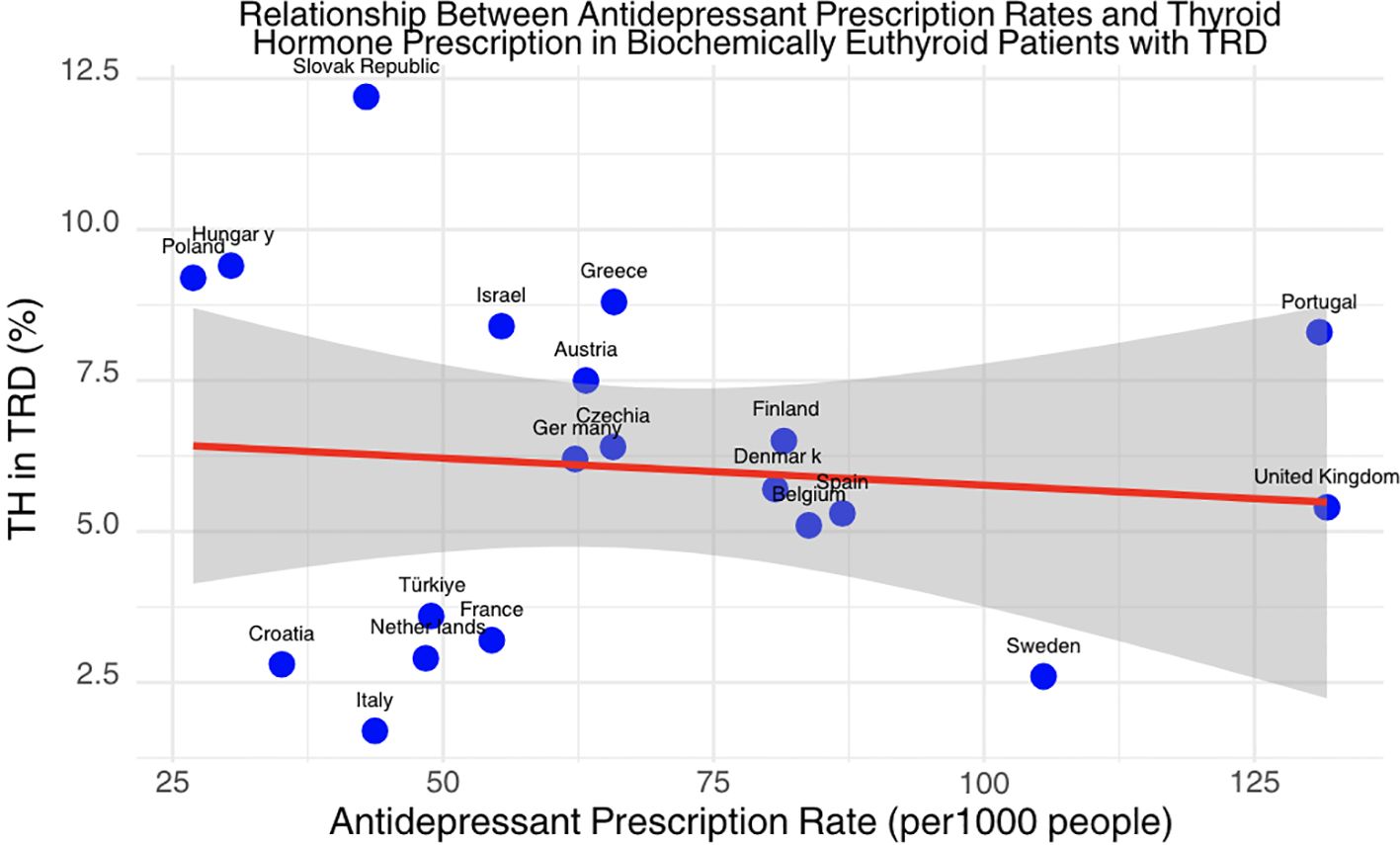
Figure 3. Scatter plot showing the relationship between antidepressant prescription rates and thyroid hormone prescription rates in biochemically euthyroid patients with TRD. The x-axis represents antidepressant prescription rates per 1,000 people, and the y-axis represents the percentage of thyroid hormone use in TRD.
Gross national income and use of TH in TRD
We calculated linear regression of rates of TH use in TRD in countries vs GNI. This showed a statistically significant reduction in the use of TH for TRD with increasing GNI (F statistic = 7.35, CI -0.15 - -0.02, p = 0.01) (Figure 4).
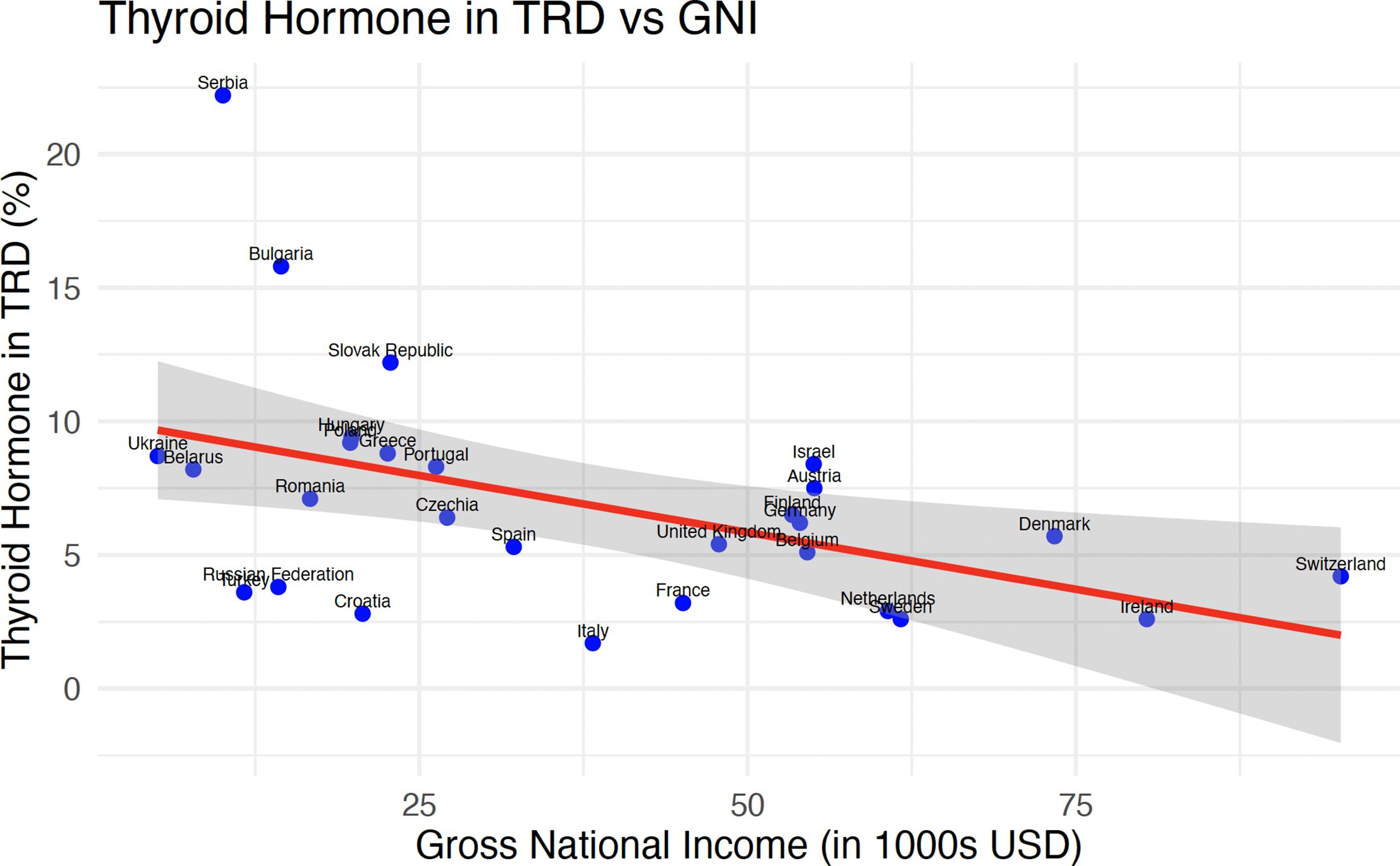
Figure 4. Scatter plot showing the relationship between thyroid hormone levels in TRD and GNI in thousands of USD.
Guidelines and use of TH in TRD
Of the 28 countries that participated in the THESIS survey, 13 had national guidelines for hypothyroidism. Of these 13 countries, no guidelines address TRD and only one guideline addresses the use of TH in euthyroid patients with depression, which does not recommend the use of TH in euthyroid patients with depression (51).
Six of the 28 countries who participated in the THESIS survey have specific guidelines for TRD, four of which (66%) recommend T3 in euthyroid patients with TRD, as an augmentation agent with antidepressant medications. A further 10 countries in the survey have national guidelines for depression. Two of these (20%) guidelines on depression recommend T3 in euthyroid patients with depression, again as an augmentation agent. A summary of all national guidelines is included in Table 3.
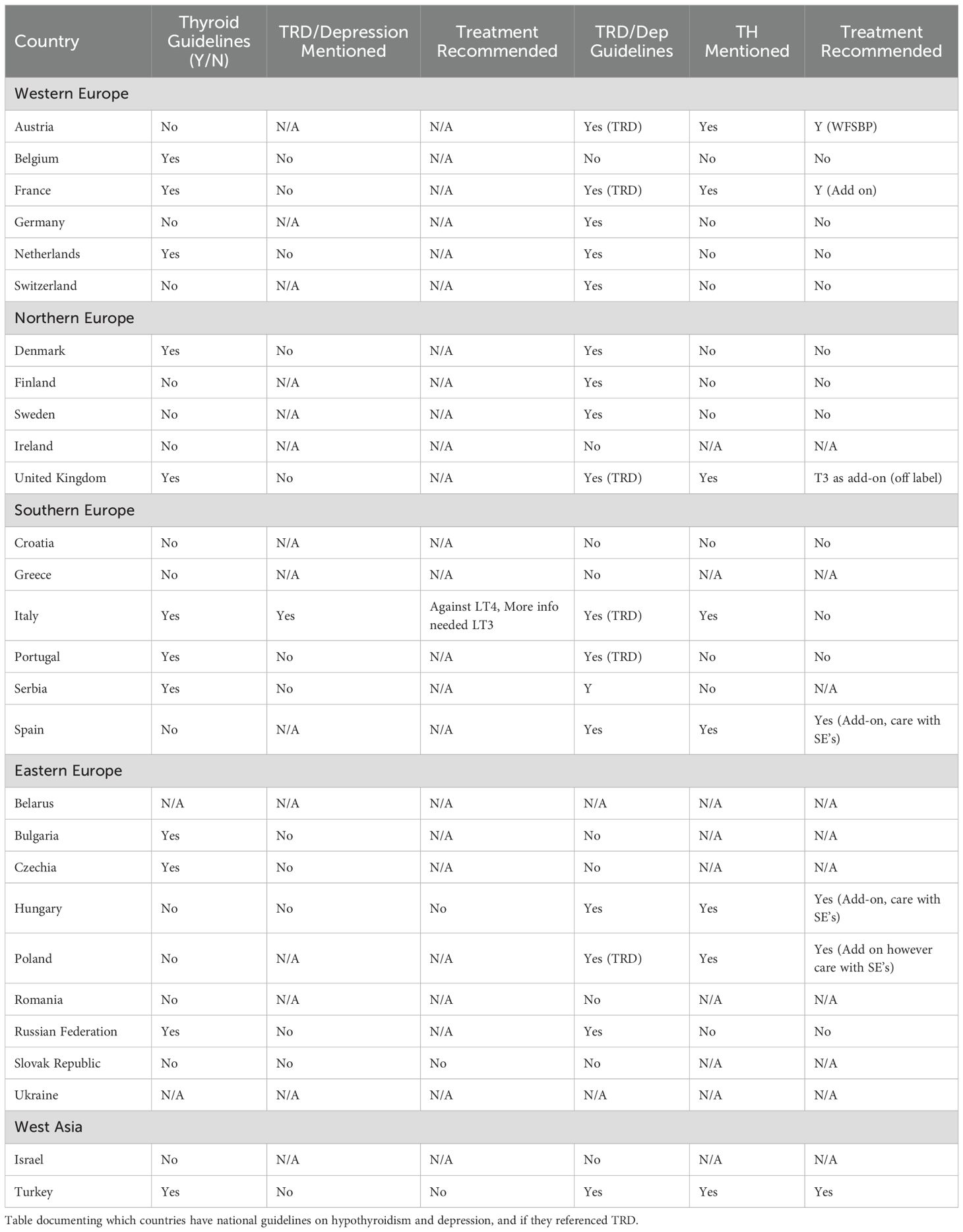
Table 3. Table documenting which countries have national guidelines on hypothyroidism and depression, and if they referenced TRD or levothyroxine use in depression/TRD.
A number of international guidelines are used by nations in the THESIS survey. The ATA guidelines discuss the use of both T4 and T3 in euthyroid patients with depression recommend neither (39). The European Thyroid Association (ETA) did not have a general guideline on hypothyroidism at the time of the THESIS survey and so did not address the use of TH in depression or TRD.
We reviewed six prominent international psychiatry guidelines which have previously been described as the ‘major American and European guidelines.’ (52) The World Federation of Societies of Biological Psychiatry (WFSBP), the American Psychiatric Association (APA), the British Association for Psychopharmacology (BAP), The Canadian Network for Mood and Anxiety Treatments (CANMAT), The Texas Medication Algorithm Project (TMAP) and the National Institute for Health and Care Excellence (NICE) guidelines on major depressive disorders and TRD, all recommend T3 as an adjunct treatment in euthyroid patients with TRD (37, 53–57).
Discussion
The THESIS survey demonstrated that just over 6% of physicians treating hypothyroidism across Europe consider TRD as a potential indication for TH in biochemically euthyroid patients. While this figure is small, it still represents a significant number (348) of specialists surveyed. We noted that male specialists were more likely to prescribe TH in TRD than their female counterparts. It has previously been shown that female physicians are more likely to practice conservative prescribing and are also more likely to follow best practice guidelines (58–60). It is also documented that risk taking of all types is more common in males compared to females and a number of guidelines warn of potential side effects using TH in patients with TRD (53, 61). While the overall rate of use of TH in biochemically euthyroid patients with TRD in male specialists remains low (7.3%), these factors may account for differences observed.
Specialists who thought TH was indicated in biochemically euthyroid patients with TRD were more likely to see a higher number of patients with hypothyroidism (Table 1). It is possible that patients seeing these physicians had previously seen a number of other specialists and had exhausted alternative treatment options. In these instances, these physicians may be aware of the limited evidence for TH as an adjunct therapy in TRD (34). Some of the key trials showing evidence for TH in the treatment of TRD include a trial from 1993 which compared T3 as an adjuvant to standard treatment compared to placebo and lithium, with improvement observed in patients treated with T3 (62). A trial conducted in 1990 by the same group demonstrated that T3 was superior to T4 in the treatment of TRD (63). T3 has also been shown to accelerate the response to tricyclic antidepressants (33). The largest randomized controlled trial to date, carried out in 2011 by Fang et al, demonstrated a benefit to augmenting paroxetine with T3 with increasing remission rates in patients with TRD seen, as defined by the 17-item Hamilton Rating Scale for Depression, however this trial was limited by a small sample size (64). All of these trials are included in the 2022 systematic review and network meta-analysis that showed a statistically significant benefit to T3 as an augmentation agent in TRD (34). That publication included five studies that looked at T3 as an augmentation agent. This included head to head, placebo-controlled and mixed arm trials. Network meta-analyses compare direct, indirect and mixed evidence and it has previously been described how some conclusions from these analyses may not be clearly justified (65).
The use of TH for euthyroid patients with TRD remains controversial, however, and a number of studies have found no benefit in the treatment of TRD. A meta-analysis published in 2020 which examined papers investigating the use of TH in the treatment of TRD included 10 studies, with 663 patients, and concluded that there was not sufficient evidence for the use of TH in the treatment of unipolar TRD (35). One study included in this meta-analysis examined T3 and lithium as adjuvant therapies in the treatment of TRD and found that neither agent improved outcomes significantly (66). A placebo-controlled trial, carried out in 1987, did not show a benefit with the use of T3 in patients with depression who had failed imipramine treatment (67). A 2006 study by Joffe et al. also found no benefit in the use of T3 as an adjuvant treatment in a double blind, placebo controlled trial (68). A systematic review and meta-analysis published in 2023 on early augmentation agents in TRD noted large inter study differences between different agents as well as differing definitions of TRD which made interpretation difficult and warned against a one size fits all approach in patients with this condition (69). A systematic review and meta-analysis published in 2019 aimed to classify the effectiveness of augmentation therapies in TRD by examining randomized controlled trials with at least ten patients, however, only one study involving TH (Fang et al.) met the criteria for the analysis (70).
Specialists who recommended TH for euthyroid patients with TRD were less likely to be a member of an international society. This correlates with the absence of endocrinology guideline recommendation for the use of TH in TRD. Of the national guidelines on hypothyroidism, Italy’s guidelines were the only ones which addressed the use of TH in euthyroid patients with depression (51). They do not recommend the use of TH in euthyroid patients with depression. Austrian national guidelines on the treatment of TRD recommend T3 as an augmentation agent when monotherapy has failed and this guideline is adapted from the WFSBP guidelines (71). French guidelines on TRD recommend T3 as an augmentation agent to be used with a variety of antidepressants and the NICE guidelines in the UK advise T3 be used as an adjunct off-label with specialist input (38, 53). Polish guidelines reference four trials which showed a benefit of TH in TRD in their recommendation (72).
The WFSBP guidelines are internationally recognized for the treatment of major depressive disorders, including TRD (37). These guidelines recommend antidepressant augmentation with T3 where monotherapy has failed. The APA guidelines on major depressive disorders were last released in 2010 and recommended the use of TH as an augmentation agent with ‘moderate clinical confidence.’ (55) The BAP guidelines from 2015 recommend the use of T3 as an augmentation agent and The CANMAT 2023 update on Clinical Guidelines for Management of Major Depressive Disorder in Adults also recommend T3 as an augmentation agent where monotherapy has failed (56, 57). The TMAP guidelines recommend T3 as a stage 1 adjunct (54).
The THESIS survey also showed large inter-regional differences in the views on prescribing TH in euthyroid patients with TRD, as high as 8.6% in Eastern Europe and as low as 4.2% and 5% in Western Europe and Northern Europe respectively (Table 2). The overall rate in Southern Europe was 5.5% however rates in Italy (1.7%) and Spain (5.3%) were more in keeping with Western and Northern European rates while rates in Greece (8.8%) and Serbia (22.2%) were consistent with prescribing patterns observed in Eastern Europe. We did not have antidepressant prescribing data available for all countries who participated in the THESIS survey, however a statistically significant relationship between these rates and the views of respondents in our survey was not observed. A potential cause for this may have been the increased medication adherence in countries with higher GNI, despite the rate of prescribing having no correlation to countries’ GNI (73). A previous study published in 2010 reported the highest percentage of patients taking prescribed anti-depressants regularly was Sweden. The lowest rates of adherence were reported in Italy, Slovak Republic and Czech Republic (73). Medication cost may have been an issue in some of the countries surveyed. The linear regression (Figure 2) showed a statistically significant relationship with decreasing rates of TH prescribing in biochemically euthyroid patients with TRD with increasing GNI. This large variation of GNI in countries in Southern Europe may explain the differing views of respondents in this region. It is possible that specialists in low GNI countries may have a need to use alternative agents for the treatment of TRD more than their Western or Northern European peers due to medication costs. OECD data show that each of Spain, Germany and Italy spent over 19 times more than each of Romania, Hungary or the Slovak Republic in 2022 (74).
Relevance, strength and limitations of the THESIS study
The THESIS survey is the largest survey conducted on the use of TH with respect to the number of participating countries and also number of valid responses. Given the volume, aggregate responses are likely to represent practices throughout Europe (22, 23). The response rate is similar to previous comparable surveys (75, 76). Therefore, the data collected by the THESIS survey is most likely representative of the views of European specialists on TH use. Data have previously been published on the use of TH in Australia and Latin America and are now being expanded to other continents (77, 78).
Limitations in this study include definitions in the question posed in the survey. The question posed to respondents was whether TH was indicated in euthyroid patients with TRD. It is possible that this may have been interpreted differently by respondents, and some may not have included T3 when considering the question, given the lower evidence for T4 as an adjunct for TRD. Potentially different responses would have been received, had T3 been specified. Another limitation of this study is the varying definition of TRD. While it is commonly described as previously in this paper, there are varying definitions which may have impacted the responses in our survey. It is also possible that this definition may change in different regions surveyed. We did not seek the volume of patients with depression or TRD, which individual respondents encounter in clinical practice that may have given better insight into prescribing practices. Primary care physicians were also not surveyed, who are typically the first to treat both patients with depression and hypothyroidism (79). Limitations also include selection bias inherent in volunteering to participate in surveys.
Conclusions
The majority of respondents to the THESIS survey (93.9%) do not believe that TH is indicated in biochemically euthyroid patients with TRD. Of the 348 respondents (6.1%) who do believe that it is indicated, this view was associated with (i) respondent characteristics: male, higher volume of hypothyroid patients, private practice and not a member of an international professional organization and (ii) national characteristics: Eastern European, low GNI. Prescribers should be aware that the prescription of TH in biochemically euthyroid patients with TRD may lead to iatrogenic and the misuse of T3 should be addressed, not only in hypothyroidism but also in all non-hypothyroid conditions (80, 81). The literature does not support the use of T4 in the treatment of TRD and it is not currently recommended in any guidelines. Due to limited evidence, the use of T3 in TRD is not currently supported by professional endocrinology associations however more research is needed in this area. Our findings raise questions regarding the use of TH in TRD across Europe and highlight the need for further studies investigating TH as an augmentation agent in TRD, as well as a consensus position from both endocrinology and psychiatry bodies regarding the use of TH in TRD.
Data availability statement
The datasets presented in this article are not readily available because Data is the property of the THESIS sub-committee. Requests to access the datasets should be directed to bHVkZ2F0ZXNAdGNkLmll.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
SL: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. AM: Writing – original draft, Writing – review & editing, Formal Analysis, Supervision, Validation. CM: Supervision, Validation, Writing – original draft, Writing – review & editing. RA: Conceptualization, Supervision, Writing – review & editing. MŽ: Conceptualization, Data curation, Validation, Writing – review & editing. EN: Data curation, Formal Analysis, Supervision, Validation, Writing – review & editing. RN: Supervision, Validation, Writing – review & editing. EP: Supervision, Validation, Writing – review & editing. CA: Validation, Writing – review & editing. EA: Validation, Writing – review & editing. MA: Validation, Writing – review & editing. GA: Writing – review & editing. TB: Writing – review & editing. BB: Writing – review & editing. EB: Writing – review & editing. MkB: Writing – review & editing. AB: Writing – review & editing. MhB: Writing – review & editing. CB: Writing – review & editing. MaB: Writing – review & editing. JĆ: Writing – review & editing. JD: Writing – review & editing. HD: Writing – review & editing. VF: Writing – review & editing. BF: Writing – review & editing. EF: Writing – review & editing. DF-S: Writing – review & editing. JG: Writing – review & editing. TH: Writing – review & editing. JJ: Writing – review & editing. PK: Writing – review & editing. MKe: Writing – review & editing. MKs: Writing – review & editing. MKu: Writing – review & editing. IL: Writing – review & editing. LL: Writing – review & editing. VL: Writing – review & editing. MM: Writing – review & editing. SM: Writing – review & editing. TM: Writing – review & editing. DN: Writing – review & editing. BP: Writing – review & editing. TP: Writing – review & editing. CP: Writing – review & editing. FM: Writing – review & editing. ER: Writing – review & editing. PR: Writing – review & editing. MR: Writing – review & editing. KR: Writing – review & editing. AS: Writing – review & editing. MT: Writing – review & editing. JF: Writing – review & editing. DU: Writing – review & editing. IV: Writing – review & editing. WV: Writing – review & editing. AV: Writing – review & editing. YY: Writing – review & editing. EY: Writing – review & editing. PP: Writing – review & editing. LH: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors express their gratitude to all national endocrine and thyroid professional societies, along with their members, who provided responses to the THESIS survey.
Conflict of interest
LH, PP, EP, EN and JG received consultancy fees from Institut Biochimique SA. Author IV was employed by the company Klinikum Vest GmbH Knappschaftskrankenhaus Recklinghausen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
APA, American Psychiatric Association; ATA, American Thyroid Association; BAP, British Association for Psychopharmacology; CANMAT, The Canadian Network for Mood and Anxiety Treatments; ETA, European Thyroid Association; GNI, Gross national income; HPT, Hypothalamic-pituitary-thyroid; NICE, National Institute for Health and Care Excellence; OECD, Organization of Economic Co-operation and Development; T3, Liothyronine; T4, Thyroxine; TH, Thyroid hormone; THESIS, Treatment of Hypothyroidism in Europe by Specialists: An International Survey; TMAP, Texas Medication Algorithm Project; TRD, Treatment resistant depression; UK, United Kingdom of Great Britain and Northern Ireland; UNSD, United Nations Statistics Division; USD, United States of America Dollar; WFSBP, World Federation of Societies of Biological Psychiatry.
References
1. Negro R, Attanasio R, Nagy EV, Papini E, Perros P, and Hegedüs L. Use of thyroid hormones in hypothyroid and euthyroid patients; the 2019 Italian survey. Eur Thyroid J. (2020) 9:25–31. doi: 10.1159/000502057
2. Borissova A-MI, Boyanov M, Attanasio R, Hegedüs L, Nagy E, Negro R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* questionnaire survey of Bulgarian physicians. Endocrinologia. (2020) 25:299–309.
3. Niculescu DA, Attanasio R, Hegedüs L, Nagy EV, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A thesis* Questionnaire survey of Romanian physicians* Thesis: treatment of hypothyroidism in Europe by specialists: an international survey. Acta Endocrinol (Bucharest). (2020) 16:462. doi: 10.4183/aeb.2020.462
4. Bednarczuk T, Attanasio R, Hegedüs L, Nagy EV, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* questionnaire survey of Polish physicians.* THESIS: Treatment of hypothyroidism in Europe by specialists: an international survey. Endokrynol Polska. (2021) 72:357–65. doi: 10.5603/EP.a2021.0048
5. Riis KR, Frølich JS, Hegedüs L, Negro R, Attanasio R, Nagy EV, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A 2020 THESIS questionnaire survey of members of the Danish Endocrine Society. J Endocrinol Invest. (2021) 44:2435–44. doi: 10.1007/s40618-021-01555-y
6. Planck T, Lantz M, Perros P, Papini E, Attanasio R, Nagy EV, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2020 THESIS questionnaire survey of members of the Swedish endocrine society. Front Endocrinol. (2021) 12:795111. doi: 10.3389/fendo.2021.795111
7. Shepelkevich AP, Dydyshka YV, Yurenya EV, Lobashova VL, Attanasio R, Hegedüs L, et al. Features of the use of synthetic analogues of thyroid hormones: а 2020 THESIS* questionnaire survey of members of the Belarusian Public Medical Association of Endocrinology and Metabolism. Problems Endocrinol. (2021) 68:18–26. doi: 10.14341/probl12828
8. Metso S, Hakala T, Attanasio R, Nagy E, Negro R, Papini E, et al. Kilpirauhashormonien käyttö kilpirauhasen vajaatoiminnan hoidossa: thesis-kyselytutkimus. Suomen Lääkärilehti. (2021) 76:2885–9.
9. Buffet C, Belin L, Attanasio R, Negro R, Hegedüs L, Nagy EV, et al. Real-life practice of thyroid hormone use in hypothyroid and euthyroid patients: A detailed view from the THESIS questionnaire survey in France. Annales d’Endocrinol. (2022) 83:27–34. doi: 10.1016/j.ando.2021.11.002
10. Paschou SA, Alevizaki M, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2020 THESIS questionnaire survey of members of the Hellenic Endocrine Society. Hormones. (2022) 2022:1–9. doi: 10.1007/s42000-021-00335-w
11. Burlacu MC, Attanasio R, Hegedüs L, Nagy EV, Papini E, Perros P, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* survey of Belgian specialists* THESIS: treatment of hypothyroidism in Europe by specialists: an international survey. Thyroid Res. (2022) 15:3. doi: 10.1186/s13044-022-00121-9
12. Berta E, Lengyel IM, Hegedűs L, Papini E, Perros P, Negro R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of Hungarian physicians. Orvosi Hetilap. (2022) 163:463–72. doi: 10.1556/650.2022.32412
13. Jiskra J, Paleček J, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2020 THESIS questionnaire survey of members of the Czech Society of Endocrinology. BMC Endocrine Disord. (2022) 22:117. doi: 10.1186/s12902-022-01027-1
14. Galofré JC, Attanasio R, Hegedüs L, Nagy E, Negro R, Papini E, et al. Use of thyroid hormone in hypothyroid patients and euthyroid subjects in Spain: A THESIS* questionnaire survey. Endocrinol Diabetes Y Nutricion. (2022) 69:520–9. doi: 10.1016/j.endinu.2021.07.003
15. Puga FM, Simões H, Melo M, Attanasio R, Hegedüs L, Nagy E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of Portuguese endocrinologists. Rev Portuguesa Endocrinol Diabetes E Metabol. (2022) 17:9–18. doi: 10.26497/AO210050
16. Vardarli I, Brandenburg T, Hegedüs L, Attanasio R, Nagy EV, Papini E, et al. A questionnaire survey of German thyroidologists on the use of thyroid hormones in hypothyroid and euthyroid patients: the THESIS (treatment of hypothyroidism in Europe by specialists: an international survey) collaborative. Exp Clin Endocrinol Diab. (2022) 130:577–86. doi: 10.1055/a-1832-0644
17. Ayvaz G, Akarsu E, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. The use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS* questionnaire survey of Turkish physicians. Turkish J Endocrinol Metab. (2022) 26:85–91. doi: 10.5152/tjem.2022.22024
18. Nedeljković-Beleslin B, Attanasio R, Hegedüs L, Nagy EV, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients–a THESIS questionnaire survey of Serbian physicians. Srpski Arhiv Za Celokupno Lekarstvo. (2022) 150:667–74.
19. Mustafa M, Ali E, McGowan A, McCabe L, Hegedüs L, Attanasio R, et al. Use of Thyroid Hormones in Hypothyroid and Euthyroid Patients: A THESIS questionnaire survey of members of the Irish Endocrine Society. Irish J Med Sci (1971-). (2023) 192:2179–87. doi: 10.1007/s11845-022-03235-z
20. Younes YR, Perros P, Hegedüs L, Papini E, Nagy EV, Attanasio R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of UK endocrinologists. Clin Endocrinol. (2023) 98:238–48. doi: 10.1111/cen.14812
21. Sasson L, Kaminer K, Cohen CA, Hegedüs L, Negro R, Nagy EV, et al. Thyroid hormone use in clinical practice by Israeli endocrinologists: a THESIS* questionnaire survey: * Treatment of hypothyroidism in Europe by specialists: an international survey. Thyroid Res. (2025) 18:12. doi: 10.1186/s13044-024-00219-2
22. Žarković M, Attanasio R, Nagy EV, Negro R, Papini E, and Perros P. Characteristics of specialists treating hypothyroid patients: the “THESIS” collaborative. Front Endocrinol. (2023) 14:1225202. doi: 10.3389/fendo.2023.1225202
23. Attanasio R, Žarković M, Papini E, Nagy EV, Negro R, Perros P, et al. Patients’ Persistent symptoms, clinician demographics, and geo-economic factors are associated with choice of therapy for hypothyroidism by european thyroid specialists: the “THESIS” Collaboration. Thyroid. (2024) 34:429–41. doi: 10.1089/thy.2023.0580
24. Gaynes BN, Lux L, Gartlehner G, Asher G, Forman-Hoffman V, Green J, et al. Defining treatment-resistant depression. Depression Anxiety. (2020) 37:134–45. doi: 10.1002/da.22968
25. D’haenen HA, den Boer JA, Willner P, and D’haenen H. Biological psychiatry Vol. 1. New Jersey: Wiley Hoboken (2002).
26. Brandt F, Thvilum M, Almind D, Christensen K, Green A, and Hegedüs L. Hyperthyroidism and psychiatric morbidity: evidence from a Danish nationwide register study. Eur J Endocrinol. (2014) 170:341–8. doi: 10.1530/EJE-13-0708
27. Thvilum M, Brandt F, Almind D, Christensen K, Brix TH, and Hegedüs L. Increased psychiatric morbidity before and after the diagnosis of hypothyroidism: a nationwide register study. Thyroid. (2014) 24:802–8. doi: 10.1089/thy.2013.0555
28. Kirkegaard C and Faber J. The role of thyroid hormones in depression. Eur J Endocrinol. (1998) 138:1–9. doi: 10.1530/eje.0.1380001
29. Joffe RT and Marriott M. Thyroid hormone levels and recurrence of major depression. Am J Psychiatry. (2000) 157:1689–91. doi: 10.1176/appi.ajp.157.10.1689
30. Prange AJ Jr., Wilson IC, Rabon AM, and Lipton MA. Enhancement of imipramine antidepressant activity by thyroid hormone. Am J Psychiatry. (1969) 126:457–69. doi: 10.1176/ajp.126.4.457
31. Wilson I, Prange A Jr, McClane T, Rabon A, and Lipton M. Thyroid-hormone enhancement of imipramine in nonretarded depressions. New Engl J Med. (1970) 282:1063–7. doi: 10.1056/NEJM197005072821903
32. Wheatley D. Potentiation of amitriptyline by thyroid hormone. Arch Gen Psychiatry. (1972) 26:229–33. doi: 10.1001/archpsyc.1972.01750210037008
33. Altshuler LL, Bauer M, Frye MA, Gitlin MJ, Mintz J, Szuba MP, et al. Does thyroid supplementation accelerate tricyclic antidepressant response? A review and meta-analysis of the literature. Am J Psychiatry. (2001) 158:1617–22. doi: 10.1176/appi.ajp.158.10.1617
34. Nuñez NA, Joseph B, Pahwa M, Kumar R, Resendez MG, Prokop LJ, et al. Augmentation strategies for treatment resistant major depression: a systematic review and network meta-analysis. J Affect Disord. (2022) 302:385–400. doi: 10.1016/j.jad.2021.12.134
35. Lorentzen R, Kjaer JN, Østergaard SD, and Madsen MM. Thyroid hormone treatment in the management of treatment-resistant unipolar depression: a systematic review and meta-analysis. Acta Psychiatr Scandinavica. (2020) 141:316–26. doi: 10.1111/acps.13154
36. Bauer M, Ravindran AV, Zhou X, Qin B, Del Giovane C, Li Q, et al. Comparative efficacy, acceptability, and tolerability of augmentation agents in treatment-resistant depression: systematic review and network meta-analysis. J Clin Psychiatry. (2015) 76:3423. doi: 10.4088/JCP.14r09204
37. Bauer M, Severus E, Möller H-J, Young AH, and Disorders WTFoUD. Pharmacological treatment of unipolar depressive disorders: summary of WFSBP guidelines. Int J Psychiatry Clin Practice. (2017) 21:166–76. doi: 10.1080/13651501.2017.1306082
38. Bennabi D, Charpeaud T, Yrondi A, Genty JB, Destouches S, Lancrenon S, et al. Clinical guidelines for the management of treatment-resistant depression: French recommendations from experts, the French Association for Biological Psychiatry and Neuropsychopharmacology and the fondation FondaMental. BMC Psychiatry. (2019) 19:1–12. doi: 10.1186/s12888-019-2237-x
39. Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, et al. Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid. (2014) 24:1670–751. doi: 10.1089/thy.2014.0028
40. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. (2004) 6:e.34.
41. Galofré JJ, Díez JJ, Attanasio R, Nagy EV, Negro R, Papini E, et al. Treatment of obesity with thyroid hormones in Europe. Data from the THESIS* Collaboration. J Endocrinol Invest. (2024) 2024:1–12. doi: 10.1007/s40618-024-02409-z
42. Negro R, Žarković M, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of levothyroxine for euthyroid, thyroid antibody positive women with infertility: Analyses of aggregate data from a survey of European thyroid specialists (Treatment of Hypothyroidism in Europe by Specialists: An International Survey). Clin Endocrinol. (2024) 101:180–90. doi: 10.1111/cen.15099
43. Papini E, Attanasio R, Žarković M, Nagy EV, Negro R, Perros P, et al. Thyroid hormones for euthyroid patients with simple goiter growing over time: a survey of European thyroid specialists. Endocrine. (2025) 87:262–72. doi: 10.1007/s12020-024-04002-z
45. The World Bank Group. GNI per capita ranking, atlas method and PPP based data catalog. Washington DC: The World Bank Group (2024).
46. OECD. Antidepressant pharmaceutical consumption. Paris, France: The Organisation for Economic Co-operation and Development (2020).
47. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2024).
48. Liang J, Bi G, and Zhan C. Multinomial and ordinal Logistic regression analyses with multi-categorical variables using R. Ann Transl Med. (2020) 8:982.
49. Rea LM and Parker RA. Designing and conducting survey research: A comprehensive guide. Hoboken, New Jersey: John Wiley & Sons (2014).
50. Sullivan GM and Feinn R. Using effect size—or why the P value is not enough. J Graduate Med Educ. (2012) 4:279–82. doi: 10.4300/JGME-D-12-00156.1
51. Biondi B, Bartalena L, Chiovato L, Lenzi A, Mariotti S, Pacini F, et al. Recommendations for treatment of hypothyroidism with levothyroxine and levotriiodothyronine: a 2016 position statement of the Italian Society of Endocrinology and the Italian Thyroid Association. J Endocrinol Invest. (2016) 39:1465–74. doi: 10.1007/s40618-016-0511-z
52. Davidson JR. Major depressive disorder treatment guidelines in America and Europe. J Clin Psychiatry. (2010) 71:27767. doi: 10.4088/JCP.9058se1c.04gry
53. Health NIf and Excellence C. Depression in adults: treatment and management. London, United Kingdom: National Institute for Health and Care Excellence (NICE (2022).
54. Suehs B, Argo TR, Bendele SD, Crismon ML, Trivedi MH, and Kurian B. Texas medication algorithm project procedural manual. Major depressive disorder algorithms. Texas: Texas Department of State Health Services (2008).
55. Gelenberg AJ, Freeman MP, Markowitz JC, Rosenbaum JF, Thase ME, Trivedi MH, et al. American Psychiatric Association practice guidelines for the treatment of patients with major depressive disorder. Am J Psychiatry. (2010) 167:9–118.
56. Cleare A, Pariante CM, Young AH, Anderson IM, Christmas D, Cowen PJ, et al. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2008 British Association for Psychopharmacology guidelines. J Psychopharmacol. (2015) 29:459–525. doi: 10.1177/0269881115581093
57. Lam RW, Kennedy SH, Adams C, Bahji A, Beaulieu S, and Bhat V, Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l’humeur et de l’anxiété (CANMAT) 2023: Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. Can J Psychiatry. (2024) 69(9):641–87. doi: 10.1177/07067437241245384
58. Mishra A, Read SH, and Rochon PA. Influence of physician sex and gender on prescribing practices among older adults. J Am Geriatr Society. (2020) 68:2764–7. doi: 10.1111/jgs.16851
59. Rochon PA, Gruneir A, Bell CM, Savage R, Gill SS, Wu W, et al. Comparison of prescribing practices for older adults treated by female versus male physicians: a retrospective cohort study. PloS One. (2018) 13:e0205524. doi: 10.1371/journal.pone.0205524
60. Baumhäkel M, Müller U, and Böhm M. Influence of gender of physicians and patients on guideline-recommended treatment of chronic heart failure in a cross-sectional study. Eur J Heart Failure. (2009) 11:299–303. doi: 10.1093/eurjhf/hfn041
61. Byrnes JP, Miller DC, and Schafer WD. Gender differences in risk taking: A meta-analysis. psychol Bull. (1999) 125:367. doi: 10.1037/0033-2909.125.3.367
62. Joffe RT, Singer W, Levitt AJ, and MacDonald C. A placebo-controlled comparison of lithium and triiodothyronine augmentation of tricyclic antidepressants in unipolar refractory depression. Arch Gen Psychiatry. (1993) 50:387–93. doi: 10.1001/archpsyc.1993.01820170065008
63. Joffe RT and Singer W. A comparison of triiodothyronine and thyroxine in the potentiation of tricyclic antidepressants. Psychiatry Res. (1990) 32:241–51. doi: 10.1016/0165-1781(90)90029-5
64. Fang Y, Yuan C, Xu Y, Chen J, Wu Z, Cao L, et al. A pilot study of the efficacy and safety of paroxetine augmented with risperidone, valproate, buspirone, trazodone, or thyroid hormone in adult Chinese patients with treatment-resistant major depression. J Clin Psychopharmacol. (2011) 31:638–42. doi: 10.1097/JCP.0b013e31822bb1d9
65. Cipriani A, Higgins JP, Geddes JR, and Salanti G. Conceptual and technical challenges in network meta-analysis. Ann Internal Med. (2013) 159:130–7. doi: 10.7326/0003-4819-159-2-201307160-00008
66. Nierenberg AA, Fava M, Trivedi MH, Wisniewski SR, Thase ME, McGrath PJ, et al. A comparison of lithium and T 3 augmentation following two failed medication treatments for depression: a STAR* D report. Am J Psychiatry. (2006) 163:1519–30. doi: 10.1176/ajp.2006.163.9.1519
67. Gitlin MJ, Weiner H, Fairbanks L, Hershman JM, and Friedfeld N. Failure of T3 to potentiate tricyclic antidepressant response. J Affect Disord. (1987) 13:267–72. doi: 10.1016/0165-0327(87)90046-2
68. Joffe RT, Sokolov ST, and Levitt AJ. Lithium and triiodothyronine augmentation of antidepressants. Can J Psychiatry. (2006) 51:791–3. doi: 10.1177/070674370605101209
69. Scott F, Hampsey E, Gnanapragasam S, Carter B, Marwood L, Taylor RW, et al. Systematic review and meta-analysis of augmentation and combination treatments for early-stage treatment-resistant depression. J Psychopharmacol. (2023) 37:268–78. doi: 10.1177/02698811221104058
70. Strawbridge R, Carter B, Marwood L, Bandelow B, Tsapekos D, Nikolova VL, et al. Augmentation therapies for treatment-resistant depression: systematic review and meta-analysis. Br J Psychiatry. (2019) 214:42–51. doi: 10.1192/bjp.2018.233
71. Kasper S EA, Sachs G, Aichhorn W, Bartova L, Bengesser S, Buchmayer F, et al. Treatment-resistant depression: diagnosis and treatment, consensus-statement. Special Jatros Neurol Psychiatry. (2022).
72. Gałecki P and Bliźniewska-Kowalska K. Treatment-resistant depression—Recommendations of the National Consultant in the field of psychiatry. Psychiatr Pol. (2021) 55:1–15. doi: 10.12740/PP/OnlineFirst/115208
73. Lewer D, O’Reilly C, Mojtabai R, and Evans-Lacko S. Antidepressant use in 27 European countries: associations with sociodemographic, cultural and economic factors. Br J Psychiatry. (2015) 207:221–6. doi: 10.1192/bjp.bp.114.156786
74. OECD. Pharmaceutical Sales. Paris, France: The Organisation for Economic Co-operation and Development (2022).
75. Winther KH, Papini E, Attanasio R, Negro R, and Hegedüs L. A 2018 European Thyroid Association survey on the use of selenium supplementation in Hashimoto’s thyroiditis. Eur Thyroid J. (2020) 9:99–105. doi: 10.1159/000504781
76. Brito JP, Nagy EV, Singh Ospina N, Žarković M, Dosiou C, Fichter N, et al. A survey on the management of thyroid eye disease among American and European Thyroid Association members. Thyroid. (2022) 32:1535–46. doi: 10.1089/thy.2022.0172
77. Lafontaine N, Brown SJ, Perros P, Papini E, Nagy EV, Attanasio R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A survey of members of the Endocrine Society of Australia. Clin Endocrinol. (2024) 100:477–85. doi: 10.1111/cen.15049
78. Cassemiro JF, Ilera V, Batalles S, Reyes A, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2022 THESIS questionnaire survey of members of the Latin American Thyroid Society (LATS). Thyroid Res. (2023) 16:40. doi: 10.1186/s13044-023-00182-4
79. Díez JJ and Iglesias P. Control of thyroid dysfunction in Spanish population registered in the primary care clinical database: An analysis of the proportion of patients with thyrotropin values outside the reference range. Hormone Metab Res. (2023) 55:184–90. doi: 10.1055/a-2014-4589
80. Hegedüs L, Nagy EV, Papini E, and Perros P. Limiting the use and misuse of liothyronine in hypothyroidism. Nat Rev Endocrinol. (2025) 21:3–4. doi: 10.1038/s41574-024-01055-y
Keywords: TRD (treatment-resistant depression), thyroid, thyroid hormone, liothyroinine, levothyroxine
Citation: Ludgate S, McGowan A, Moran C, Attanasio R, Žarković M, Nagy EV, Negro R, Papini E, Adler Cohen C, Akarsu E, Alevizaki M, Ayvaz G, Bednarczuk T, Beleslin BN, Berta E, Bodor M, Borissova AM, Boyanov M, Buffet C, Burlacu M-C, Ćirić J, Díez JJ, Dobnig H, Fadeyev V, Field BCT, Fliers E, Führer-Sakel D, Galofré JC, Hakala T, Jiskra J, Kopp PA, Krebs M, Kršek M, Kužma M, Lazúrová I, Leenhardt L, Luchytskiy V, Melo M, Metso S, Morgunova T, Niculescu DA, Perić B, Planck T, Poiana C, Marques Puga F, Robenshtok E, Rosselet P, Ruchala M, Riis KR, Shepelkevich A, Tronko MD, Frølich JS, Unuane D, Vardarli I, Visser WE, Vryonidou A, Younes YR, Yurenya E, Perros P and Hegedüs L (2025) The use of thyroid hormones in the treatment of euthyroid patients with treatment-resistant depression. Data from a survey of 5695 European national endocrine professional organization members. Front. Endocrinol. 16:1665720. doi: 10.3389/fendo.2025.1665720
Received: 14 July 2025; Accepted: 29 August 2025;
Published: 23 September 2025.
Edited by:
Silvia Martina Ferrari, Medical and Molecular Pathology and Critical Area University of Pisa, ItalyReviewed by:
Valerio Caruso, University of Pisa, ItalySaai Ram Thejas, RVM Institute of Medical Sciences and Research Center, India
Copyright © 2025 Ludgate, McGowan, Moran, Attanasio, Žarković, Nagy, Negro, Papini, Adler Cohen, Akarsu, Alevizaki, Ayvaz, Bednarczuk, Beleslin, Berta, Bodor, Borissova, Boyanov, Buffet, Burlacu, Ćirić, Díez, Dobnig, Fadeyev, Field, Fliers, Führer-Sakel, Galofré, Hakala, Jiskra, Kopp, Krebs, Kršek, Kužma, Lazúrová, Leenhardt, Luchytskiy, Melo, Metso, Morgunova, Niculescu, Perić, Planck, Poiana, Marques Puga, Robenshtok, Rosselet, Ruchala, Riis, Shepelkevich, Tronko, Frølich, Unuane, Vardarli, Visser, Vryonidou, Younes, Yurenya, Perros and Hegedüs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stephen Ludgate, bHVkZ2F0ZXNAdGNkLmll
†ORCID: Stephen Ludgate, orcid.org/0000-0002-9597-9471
Anne McGowan, orcid.org/0000-0003-4222-622X
Carla Moran, orcid.org/0000-0002-7318-7166
Roberto Attanasio, orcid.org/0000-0002-1417-287X
Miloš Žarković, orcid.org/0000-0001-9977-5970
Endre Vezekenyi Nagy, orcid.org/0000-0002-9286-6471
Roberto Negro, orcid.org/0000-0001-9282-4530
Enrico Papini, orcid.org/0000-0003-4790-2733
Ersin Akarsu, orcid.org/0000-0003-2786-6616
Maria Alevizaki, orcid.org/0000-0003-3726-5793
Göksun Ayvaz, orcid.org/0000-0002-1213-6832
Tomasz Bednarczuk, orcid.org/0000-0002-5752-8709
Biljana Nedeljković Beleslin, orcid.org/0000-0002-1687-9297
Eszter Berta, orcid.org/0000-0003-0439-9867
Miklos Bodor, orcid.org/0000-0002-0789-5156
Anna Maria Borissova, orcid.org/0000-0003-0553-408X
Mihail Boyanov, orcid.org/0000-0002-5695-2831
Camille Buffet, orcid.org/0000-0003-1389-4157
Maria-Cristina Burlacu, orcid.org/0000-0002-8437-3933
Jamina Ćirić, orcid.org/0000-0001-6960-9699
Juan J. Díez, orcid.org/0000-0002-2017-0694
Harald Dobnig, orcid.org/0000-0001-7574-9292
Valentin Fadeyev, orcid.org/0000-0002-3026-6315
Benjamin C. T. Field, orcid.org/0000-0002-1883-1588
Eric Fliers, orcid.org/0000-0001-8048-9050
Dagmar Führer-Sakel, orcid.org/0000-0003-0357-4192
Juan Carlos Galofré, orcid.org/0000-0003-0227-3566
Tommi Hakala, orcid.org/0000-0002-9373-4462
Jan Jiskra, orcid.org/0000-0003-0920-4854
Peter A. Kopp, orcid.org/0000-0001-5980-0529
Michael Krebs, orcid.org/0000-0002-9265-7274
Michal Kršek, orcid.org/0000-0002-5941-3489
Martin Kužma, orcid.org/0000-0002-1294-1217
Ivica Lazúrová, orcid.org/0000-0002-3163-1097
Laurence Leenhardt, orcid.org/0000-0003-4131-6813
Vitaliy Luchytskiy, orcid.org/0000-0002-3515-3264
Miguel Melo, orcid.org/0000-0002-8365-1380
Saara Metso, orcid.org/0000-0001-8197-7603
Tatyana Morgunova, orcid.org/0000-0003-1500-1586
Dan Alexandru Niculescu, orcid.org/0000-0002-6439-3523
Božidar Perić, orcid.org/0000-0001-9998-4895
Tereza Planck, orcid.org/0000-0003-1398-5067
Catalina Poiana, orcid.org/0000-0002-5795-3318
Francisca Marques Puga, orcid.org/0000-0002-9510-419X
Eyal Robenshtok, orcid.org/0000-0002-6268-4212
Patrick Rosselet, orcid.org/0009-0004-3793-8163
Marek Ruchala, orcid.org/0000-0002-6296-7220
Kamilla Ryom Riis, orcid.org/0000-0003-2679-7153
Alla Shepelkevich, orcid.org/0000-0002-8213-2968
Mykola D. Tronko, orcid.org/0000-0001-7421-0981
David Unuane, orcid.org/0000-0002-8488-1735
Irfan Vardarli, orcid.org/0009-0009-2554-0971
W. Edward Visser, orcid.org/0000-0002-5248-863X
Andromachi Vryonidou, orcid.org/0000-0002-0544-5952
Younes Ramazan Younes, orcid.org/0000-0003-0929-1003
Petros Perros, orcid.org/0000-0001-7320-5574
Laszlo Hegedüs, orcid.org/0000-0002-9691-7619