 Josep León-Mengíbar1
Josep León-Mengíbar1 Marcelino Bermúdez-López2,3
Marcelino Bermúdez-López2,3 José Manuel Valdivielso2
José Manuel Valdivielso2 Reinald Pamplona4
Reinald Pamplona4 Gerard Torres5Dídac Mauricio6Eva Castro-Boqué2Elvira Fernández2
Gerard Torres5Dídac Mauricio6Eva Castro-Boqué2Elvira Fernández2 Assumpta Caixàs7Marta Bueno1
Assumpta Caixàs7Marta Bueno1 Andreea Ciudin8Marta Hernández1
Andreea Ciudin8Marta Hernández1 Rafael Simó8Cristina Hernández8*
Rafael Simó8Cristina Hernández8* Albert Lecube8* on behalf of the ILERVAS project collaborators
Albert Lecube8* on behalf of the ILERVAS project collaborators- 1Department of Endocrinology and Nutrition, University Hospital Arnau de Vilanova de Lleida, Obesity, Diabetes and Metabolism (ODIM) Research Group, Institut de Recerca Biomèdica de Lleida (IRBLleida), University of Lleida, Lleida, Spain
- 2Vascular and Renal Translational Research Group, Institut de Recerca Biomèdica de Lleida (RBLleida), Renal Research Network (RICORS2040, ISCIII), Lleida, Spain
- 3Department of Experimental Medicine, University of Lleida, Lleida, Spain
- 4Department of Experimental Medicine, University of Lleida, Institut de Recerca Biomèdica de Lleida (IRBLleida), Lleida, Spain
- 5Translational Research in Respiratory Medicine, University Hospital Arnau de Vilanova and Santa Maria, Institut de Recerca Biomèdica de Lleida (IRBLleida), CIBER of Respiratory Diseases (CIBERES), Institute of Health Carlos III, Lleida, Spain
- 6Department of Endocrinology and Nutrition, Hospital de la Santa Creu i Sant Pau, CIBERDEM (Institute of Health Carlos III), Autonomous University of Barcelona, Barcelona, Spain
- 7Department of Endocrinology and Nutrition, Parc Taulí Hospital Universitari, Institut d’Investigació i Innovació Parc Taulí (IPT-CERCA), Medicine Department, Universitat Autònoma de Barcelona, Sabadell, Spain
- 8Department Endocrinology and Nutrition, University Hospital Vall d’Hebron, Diabetes and Metabolism Research Group, Institut de Recerca Vall d’Hebron (VHIR), CIBERDEM (Institute of Health Carlos III), Barcelona, Spain
Background: Traditional body mass index (BMI) does not adequately reflect adipose tissue distribution and associated cardiovascular (CV) risk. To improve risk stratification, the European Association for the Study of Obesity (EASO) proposes to extend the diagnosis of obesity to include individuals with a BMI of 25–30 kg/m², a waist-to-height ratio (WtHR) ≥0.5, and any obesity-related complication.
Objective: To examine whether this new definition of obesity can better identify the presence of subclinical atheromatosis disease (SAD) in terms of arterial plaque burden compared to the classical BMI-based definition.
Methods: A cross-sectional including 8,330 participants from the ILERVAS project (ClinicalTrials.gov Identifier: NCT03228459), aged 45–70 years with low-to-moderate CV risk and no previous CV disease, was included. Obesity was classified using traditional (BMI ≥ 30 kg/m²) and new definitions. Atherosclerosis was assessed through Doppler ultrasound of carotid and femoral arteries. Logistic regression models adjusted for cardiovascular risk factors were used to evaluate associations between obesity definitions and SAD.
Results: The new definition increased obesity prevalence from 37.2% to 71.7%. It also revealed higher detection of atheromatous plaques (72.9% vs. 68.6%, p < 0.001) and affected more vascular territories. Multivariable analysis showed the new definition independently predicted overall plaque presence (OR 1.54, 95% CI 1.22–1.94, p < 0.001) and femoral atherosclerosis (OR 1.36, 95% CI 1.10–1.68, p = 0.004). Similar results were obtained when only WtHR was considered, excluding obesity-related complications.
Conclusion: The new obesity definition identifies more efficiently individuals at risk for atherosclerosis, especially in the femoral region, compared to the classic BMI definition. Further studies to assess the cost-effectiveness of this approach seem warranted.
Introduction
Obesity is increasingly recognized as a complex, multifactorial, chronic, non-communicable, and relapsing disease with profound implications for both individual health and public healthcare systems worldwide (1). Despite its well-established role in the development of numerous non-communicable diseases, the clinical approach to diagnosing and managing obesity has not yet been fully aligned with the standardized processes applied to other chronic conditions (2–4). Recent evidence supports the conceptual shift from “obesity” to “obesities,” underlining that not only the amount of adipose tissue but also its distribution and functional characteristics are critical determinants in the pathophysiology of the disease and in guiding personalized therapeutic approaches (2, 4).
Body mass index (BMI) has been the cornerstone of obesity assessment in the last decades (5, 6). However, growing evidence suggests that BMI alone is insufficient to accurately reflect adipose tissue distribution or its metabolic health consequences (4, 7). While BMI-based thresholds guide diagnosis and treatment, they fail to account for individual differences in fat distribution and metabolic function (5–7). Consequently, individuals with the same BMI may exhibit markedly different metabolic profiles and health risks, with some classified as having obesity showing minimal cardiometabolic impairment, and others, despite a BMI < 30 kg/m2, experiencing severe obesity-related complications due to excess visceral adipose tissue (VAT). These discrepancies underscore the need to move beyond BMI-centric diagnostic models (2, 8). Accordingly, experts now advocate for the inclusion of complementary anthropometric measures, such as waist circumference, waist-to-height ratio (WtHR), and body composition metrics to improve risk stratification and clinical decision making (8, 9).
Visceral adiposity has emerged as a key contributor to cardiometabolic risk, independently of total body weight (9). VAT is metabolically active and by secreting free fatty acids and adipokines such as leptin, TNF-α, and IL-6 contributes to fostering systemic inflammation, endothelial dysfunction, and insulin resistance (10–13). These pathophysiological changes provide a mechanistic link between visceral adiposity and cardiovascular disease (CVD). In this context, atherosclerotic plaque formation represents a key clinical manifestation of VAT-driven vascular damage. Although plaque development is central to the progression of CVD, its pathogenesis is complex and appears to vary across vascular territories depending on the dominant underlying risk factors (14, 15).
In line with this updated understanding, the European Association for the Study of Obesity (EASO) has proposed a revised framework for the diagnosis, staging, and management of obesity, aligning with the current understanding of obesity as an adiposity-based chronic disease (ABCD) (4). This framework expands the diagnostic threshold beyond the traditional BMI ≥30 kg/m² to include individuals with BMI between 25 and 30 kg/m², a WtHR ≥ 0.5 and the presence of any obesity-related complication. This could allow for a more accurate identification of individuals at risk for obesity-related complications due to central adiposity accumulation (2).
In this context, our study aims to compare the predictive value of this revised definition of obesity with the traditional BMI-based criterion in identifying the presence of atheromatous plaque across different vascular territories in a large cohort of individuals at low to moderate cardiovascular (CV) risk from the province of Lleida, Spain. By integrating a more refined assessment of central adiposity, this approach may improve CV risk stratification, thus leading to more effective preventive strategies.
Methods
Study population, metabolic status, and patient selection
The ongoing prospective ILERVAS study (ClinicalTrials.gov Identifier: NCT03228459) investigates the progression of subclinical atherosclerotic disease (SAD) in individuals with low to moderate cardiovascular risk (16, 17). However, for the present manuscript, only baseline data were analyzed, and therefore the study design corresponds to a cross-sectional analysis. A total of 8,330 participants were initially recruited between January 2015 and December 2017 from 30 primary healthcare centers in Lleida, Spain. The inclusion criteria were as follows: participants were aged between 45 and 70 years and had no prior history of CVD, including angina, myocardial infarction, stroke, peripheral artery disease, heart failure, or any vascular surgery/procedure. Additionally, they had to present at least one cardiovascular risk factor, such as dyslipidemia, arterial hypertension, a BMI ≥ 30 kg/m², smoking, or a first-degree relative with premature CVD (myocardial infarction, stroke, or peripheral arterial disease) before the age of 55 years in men or 65 years in women. Individuals with any form of diabetes mellitus, chronic kidney disease, active neoplasia, a life expectancy of less than 18 months, or pregnancy were excluded.
Height and body weight were measured with participants wearing light clothing and without shoes. Waist circumference was measured in a standing position with a flexible tape positioned midway between the hip bone and the lower rib, and recorded to the nearest 0.1 cm. The classical definition of obesity was defined as a BMI ≥ 30 kg/m². Conversely, the new definition of obesity also included those participants with a BMI between 25 and 30 kg/m² who exhibited a WtHR ≥ 0.5 and at least one obesity-related health condition such as dyslipidemia, arterial hypertension, prediabetes, or sleep apnea (2).
Total cholesterol levels (mg/dl) were assessed in all participants using a non-fasting dried capillary blood sample (obtained via fingertip puncture) analyzed with the REFLOTRON® Plus system (Roche Diagnostics, GmbH, Germany) (16, 17). A complete lipid profile, including HDL cholesterol, LDL cholesterol, and triglycerides, was measured only in participants whose total cholesterol levels ≥ 200 mg/dl after fasting for at least 6 hours, or ≥ 250 mg/dl regardless of fasting duration. Blood pressure was measured three times using an automated device [Omron M6 Comfort HEM-7221-E (Omron Healthcare, Kyoto, Japan)] after participants rested for 5 minutes. The measurements, spaced two minutes apart, were averaged from the last two readings to calculate the mean. Pulse pressure was determined as the difference between systolic and diastolic blood pressures. Prediabetes status was defined following current American Diabetes Association guidelines (18). The prevalence of dyslipidemia and hypertension were determined based on patients who were assigned a diagnostic code according to the International Classification of Diseases (ICD) Code. Smoking status was documented as non-smoker, current smoker, or former smoker, the latter defined as participants who had quit smoking for at least one year.
Prescribed treatments for hypertension and lipid management were extracted from prescription records and pharmacy invoicing data provided by the Catalan Health Service. This information is annually consolidated into the Information System for Research in Primary Care (SIDIAP) database. Antihypertensive therapies included ACE inhibitors, diuretics, angiotensin receptor blockers, beta-blockers, calcium channel blockers, and other antihypertensive agents. Lipid-lowering medications encompassed statins, fibrates, ezetimibe, and omega-3 fatty acids.
Assessment of atheromatous plaque burden by ultrasound study
After having patients classified based on BMI or the new criteria proposed by EASO an ultrasound study was performed. The bilateral carotid arteries (common, bifurcation, internal, and external) and femoral arteries (common and superficial) were examined. Images were acquired using a Vivid-I Doppler Ultrasound system (General Electric Healthcare, Waukesha, WI, USA) equipped with a 12L-RS broadband linear probe operating at frequencies between 5 and 13 MHz. Standardized and validated protocols for image acquisition and interpretation, based on the guidelines from the International Society of Ultrasound in Medicine and Biology, were employed to minimize inter-operator variability and reduce type II errors (19). Sonographers, specifically trained in vascular ultrasound techniques with at least five years of experience in similar studies, were selected to ensure consistency in image quality. These professionals remained blinded to the participants’ clinical histories to avoid potential biases during the evaluation.
Subclinical atheromatosis was defined as the presence of any plaque in the twelve evaluated vascular regions (20). A plaque was well-defined when the focal intima-media thickness was ≥1.5 mm, projecting into the arterial lumen (21). All detected plaques were measured, and the total plaque area (cm²) was calculated using a standardized quantitative method (22).
Statistical analysis
The normality of continuous variables was assessed using the Shapiro-Wilk test and visual inspection of quantile–quantile plots. Owing to the non-normal distribution of the data detected, quantitative dates were expressed as the medians with interquartile ranges. Categorical variables were reported as absolute frequencies. Group comparisons were conducted using Pearson’s chi-squared test for categorical variables and the Mann-Whitney U test for quantitative variables.
Univariable logistic regression was used to assess the presence of obesity in relation to SAD. Additionally, we employed a multivariable bidirectional stepwise logistic and lineal regression model to assess the presence of SAD and the number of plaques, adjusting for confounding factors such as sex, age, prediabetes status, total cholesterol, triglycerides, hypertension (yes/no), obesity (yes/no), pulse pressure, and smoking. The probability thresholds for entering and removing variables from the model were set at ≤0.05 and ≥0.10, respectively. Further, a multivariable stepwise linear regression model was applied to evaluate the total plaque area, incorporating the same set of confounders. Both logistic and linear regression models were performed separately for the classical and new definitions of obesity. Since several obesity-related complications included in the new obesity classification are actually risk factors for atherosclerosis development, a third analysis was also conducted only considering WtHR ≥ 0.5. This approach permitted us to better explore the genuine relationship between central adiposity and the presence of SAD.
The outcomes of the regression analyses were presented as odds ratios (OR) and beta coefficients with 95% confidence intervals (CIs) for logistic and linear models, respectively. Model calibration and discrimination were assessed using the Hosmer-Lemeshow goodness-of-fit test and the area under the receiver operating characteristic curve, respectively. The goodness-of-fit for the linear regression models was evaluated using adjusted R². All statistical analyses were conducted using STATA software version 16 and R Statistical Software version 4.1.2, with a significance threshold set at 0.05 (23).
Ethical considerations
The ILERVAS study protocol received approval from the Ethics Committee of the University Hospital Arnau de Vilanova (initial approval: CEIC-1410, 19/12/2014). All participants provided written informed consent prior to inclusion in the study. The research was conducted in accordance with the ethical principles established in the Declaration of Helsinki and adhered to Spain’s data protection regulations.
Results
The main clinical and metabolic characteristics of the study participants classified according to both the classical and the new definition of obesity are detailed in Tables 1, 2. Based on the classical definition, 37.2% of participants were classified as having obesity. This prevalence increased significantly to 71.7% under the new definition. Individuals classified as having obesity by either definition exhibited a higher percentage of prediabetes and higher baseline blood glucose levels, presented higher rates of hypertension and pulse pressure, and were more frequently non-smokers. Notably, participants identified as having obesity under the new definition also showed a more atherogenic lipid profile and a higher prescription rate of lipid-lowering therapies compared to those not classified as obese. When participants with overweight (BMI 25–30 kg/m²) and abdominal obesity (WtHR ≥ 0.5) were included, regardless of the presence of adiposity-related comorbidities, the prevalence of obesity increased to 78.8% in our cohort, while maintaining the main clinical and metabolic characteristic described above (Table 3).
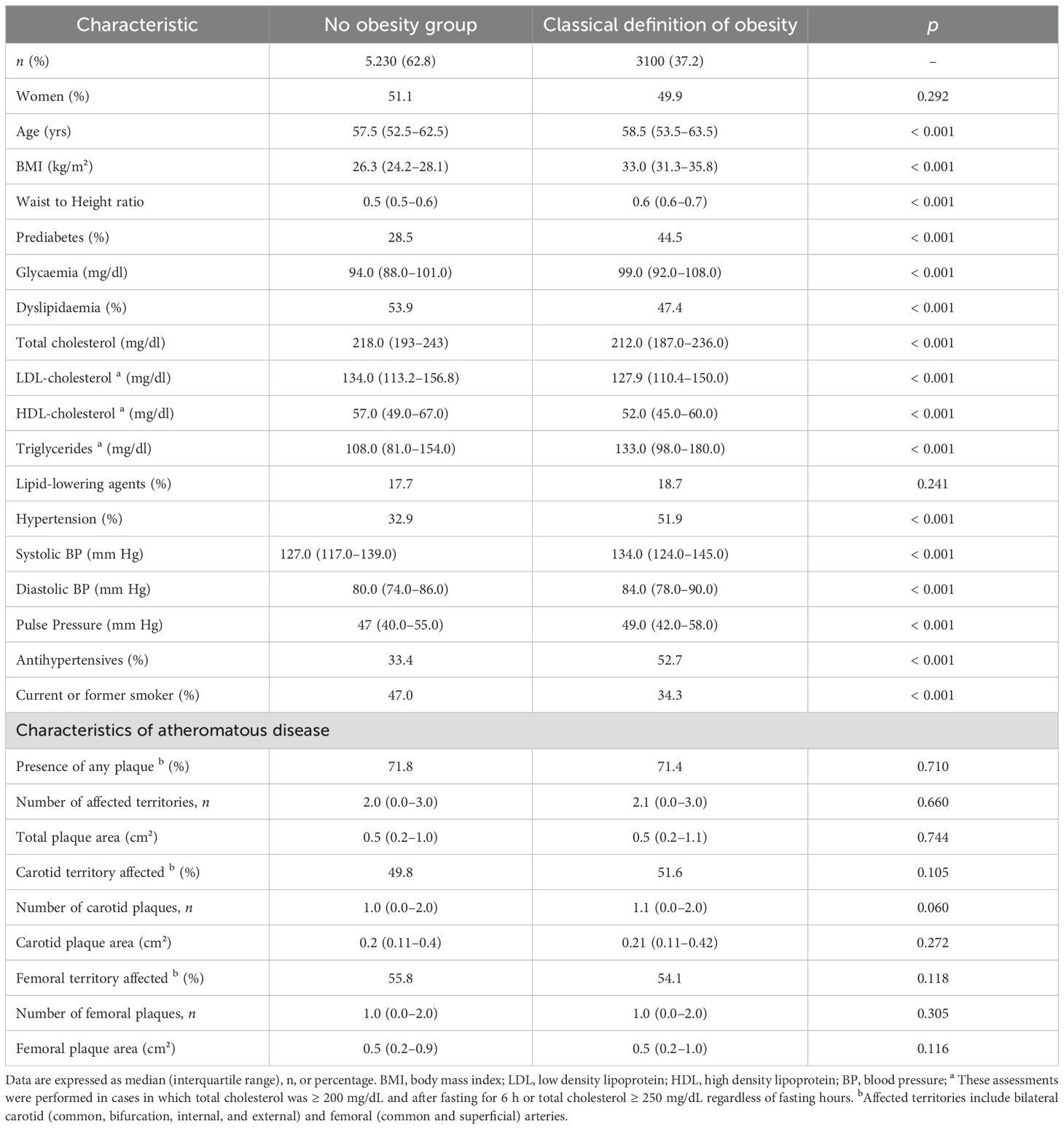
Table 1. Baseline clinical and metabolic characteristics, and atheromatous status of participants based on the classical definition of obesity (BMI ≥ 30 kg/m²).
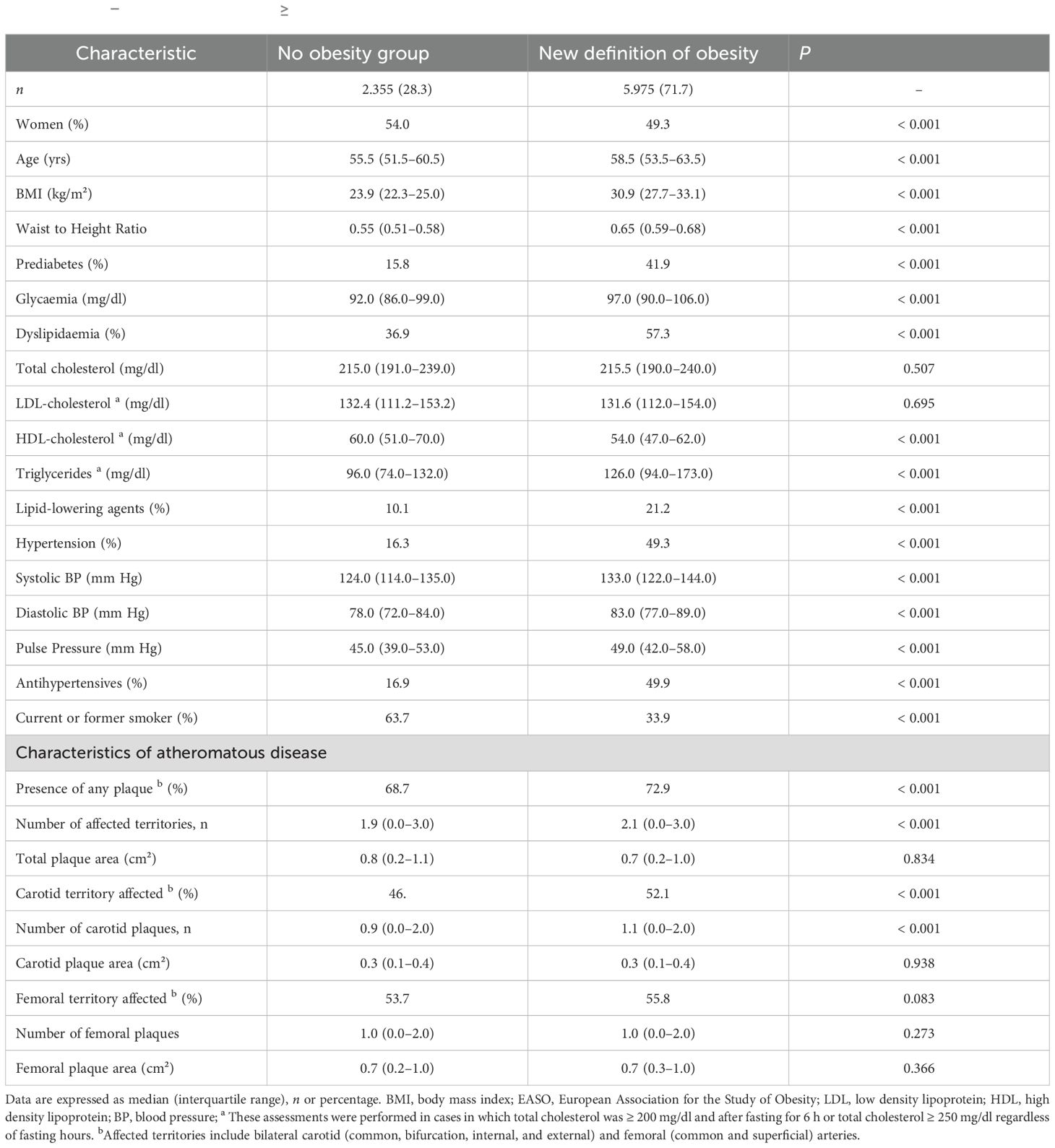
Table 2. Baseline clinical and metabolic characteristics, and atheromatous status of participants based on the new definition of obesity (BMI ≥30 kg/m² plus BMI 25–30 kg/m² with a WtHR ≥ 0.5 and at least one obesity-related health condition) proposed by EASO.
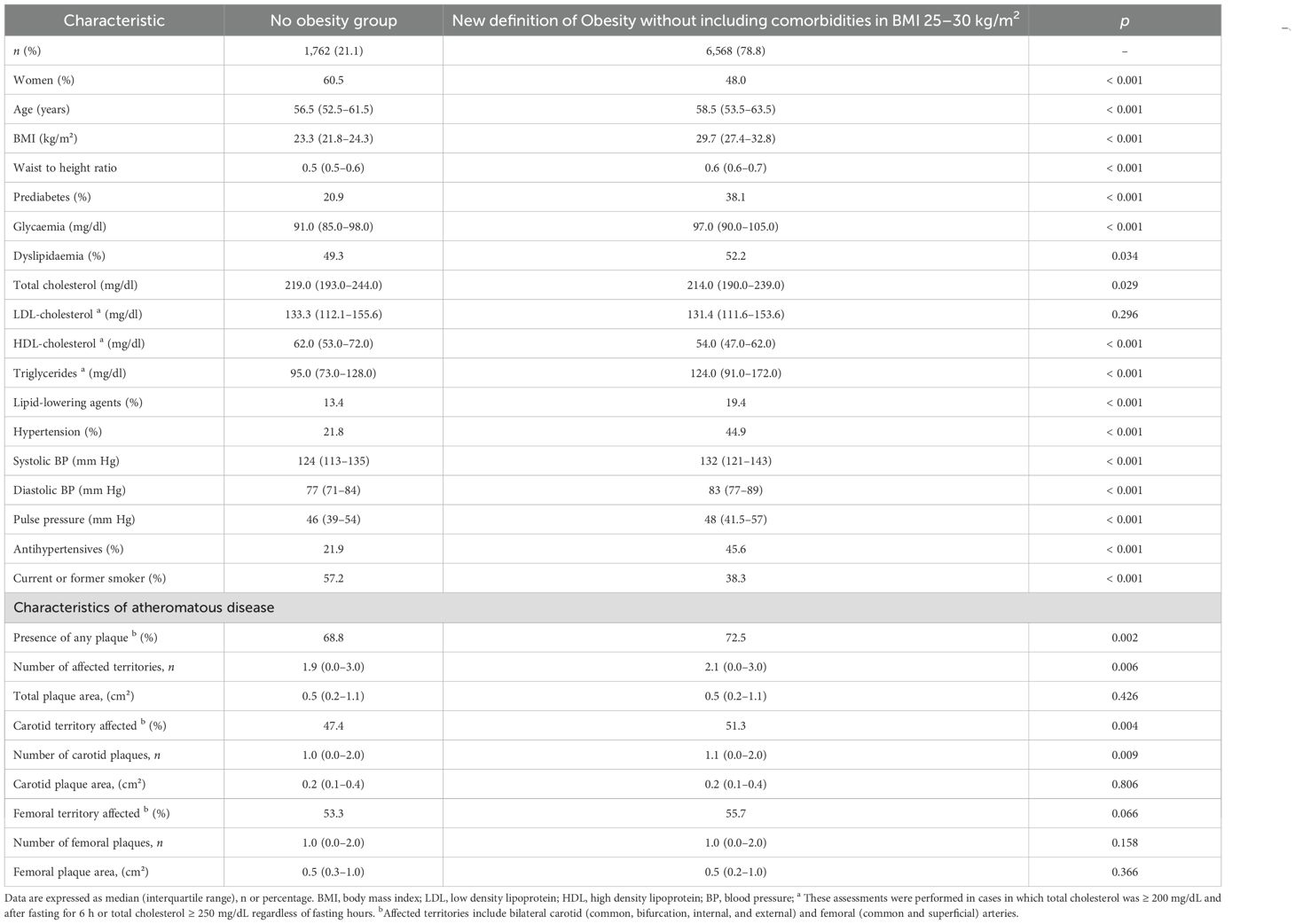
Table 3. Baseline clinical and metabolic characteristics, and atheromatous status of participants adding to the classical definition of obesity (BMI ≥ 30 kg/m²) those participants with overweight (BMI 25–30 kg/m²) and abdominal obesity (WtHR ≥ 0.5).
Regarding atherosclerotic disease, the classical definition of obesity showed no statistically significant differences in the prevalence of atheromatous disease across territories compared with participants without obesity. In contrast, the new definition identified a higher prevalence of plaques in the obesity group (72.9% vs. 68.6%; p < 0.001), with more affected territories (2.1 vs. 1.9; p < 0.001), with the carotid being more frequent (52.1% vs. 46.3%; p < 0.001) (Tables 1, 2). When only subjects with abdominal obesity (WtHR ≥ 0.5) but no comorbidities were included, similar patterns of increased atherosclerotic burden were observed (Table 3).
When multivariable logistic regression was performed to examine the factors independently associated with SAD, the new EASO obesity criteria emerged as an independent predictor of overall plaque presence (OR 1.54, 95% CI 1.22–1.94, p < 0.001) and of femoral plaque (OR 1.36, 95% CI 1.10–1.68, p = 0.004), but not of carotid plaque (p = 0.290) (Table 4). Similar results were observed when this definition was replaced by only abdominal obesity (WtHR ≥ 0.5) (Table 5). In contrast, a BMI ≥ 30 kg/m2 alone was not an independent predictor of SAD, neither overall nor in any vascular territory (Table 6).
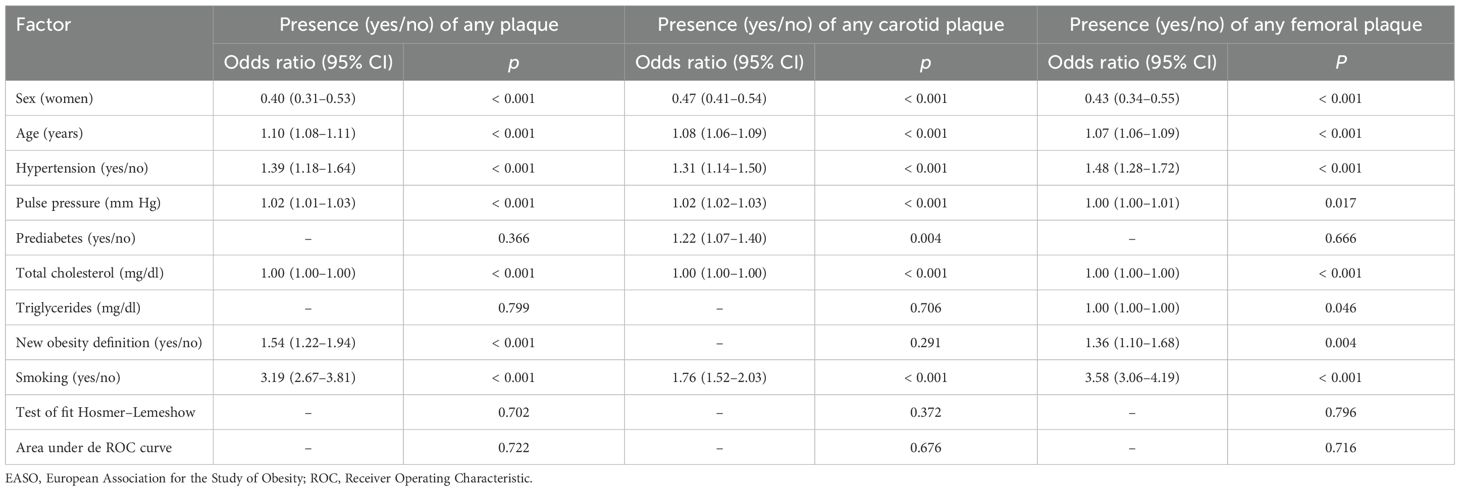
Table 4. Stepwise logistic regression model to assess factors independently associated with the presence of any plaque, plaque in carotid territories, or plaque in femoral territories according to the new definition of obesity proposed by EASO.
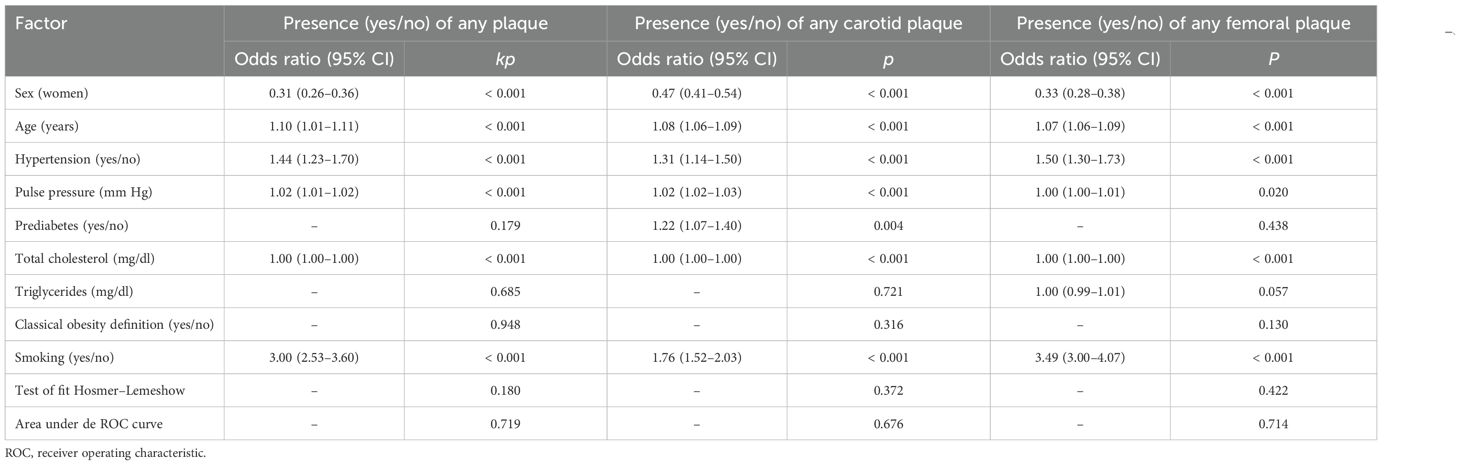
Table 5. Stepwise logistic regression model to detect factors independently associated with the presence of any plaque, plaque in carotid territories, or plaque in femoral territories according to the classical definition of obesity.
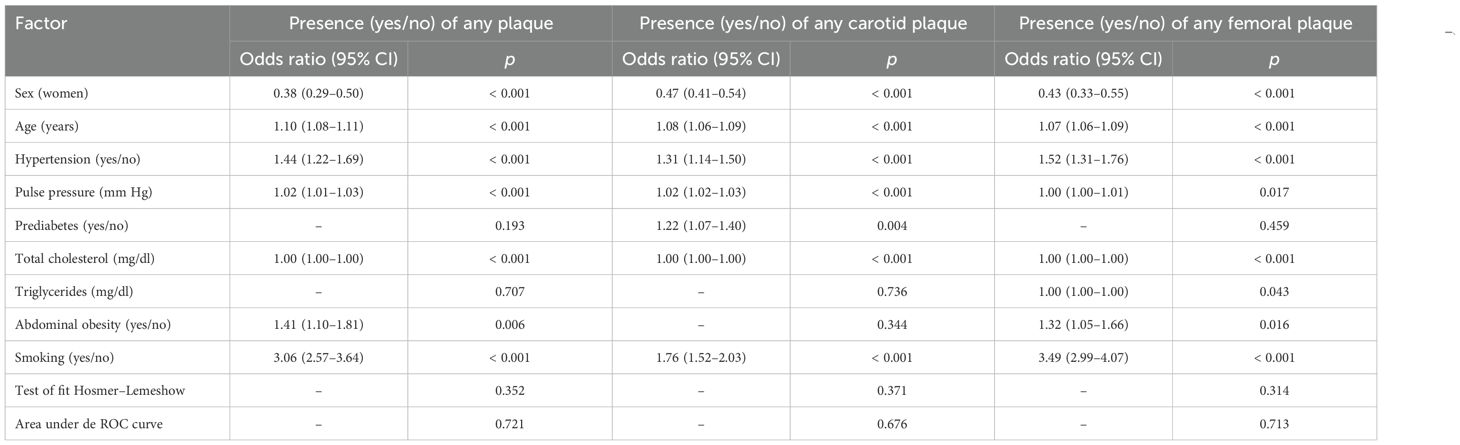
Table 6. Stepwise logistic regression model to assess factors independently associated with the presence of any plaque, plaque in carotid territories, or plaque in femoral territories when individuals with overweight and abdominal obesity (WtHR ≥ 0.5) were included in the model.
Discussion
To our knowledge, this is the first study to evaluate the new criteria for the diagnosis of obesity and its association with the presence of SAD in a large cohort of participants with low to moderate cardiovascular risk. Our findings demonstrate that these updated criteria offer greater predictive capacity for atherosclerotic burden by emphasizing central adiposity over BMI alone. These results align with previous studies that have highlighted the significance of central adiposity, particularly VAT, in the development of cardiovascular and atheromatous diseases, rather than overall body mass (2, 8, 9). Therefore, our analysis suggests that adiposity may play a different role in the development of SAD across different vascular territories, with a higher impact on femoral atherosclerosis.
VAT is a known metabolically active tissue that contributes to cardiovascular risk through multiple mechanisms. First, VAT is highly proinflammatory, producing adipokines such as leptin, TNF-α, and IL-6, which promote endothelial dysfunction, inflammation, and insulin resistance. These factors collectively lead to atherosclerosis and CVD (10, 11). Secondly, the “portal hypothesis” suggests that visceral fat releases free fatty acids directly into the portal circulation, leading to an enhancement of hepatic insulin resistance, hepatic glucose production, and dyslipidemia, also key risk factors for CVD (12). In this context, the American Heart Association (AHA) also emphasizes that visceral adiposity is strongly linked to metabolic complications such as hypertriglyceridemia, hyperinsulinemia, and glucose intolerance, making it a more accurate predictor of cardiovascular risk than overall body mass (12). Moreover, prospective studies have demonstrated that visceral fat is independently associated with incident CVD and all-cause mortality, whereas subcutaneous fat does not exhibit the same correlation (13). For instance, the Multi-Ethnic Study of Atherosclerosis found that higher levels of visceral fat were significantly associated with an increased risk of coronary heart disease (13).
In this context, the WtHR has been used as a criterion for better characterizing central adiposity and has proven to be a strong predictor of CVD. Supporting this, our data shows that individuals with overweight and abdominal adiposity, regardless of associated comorbidities, present a higher risk of presenting SAD, with a stronger association observed in the femoral territories. Similarly, a prospective cohort study from the UK Biobank demonstrated that WtHR was associated with ischemic CVD, heart attacks, and ischemic strokes, independently of overall body weight (24). Moreover, the AHA considers WtHR a superior predictor of CVD compared to BMI (12). In line with these findings, a meta-analysis of 31 prospective studies further reinforces the association between higher WtHR and a significantly increased risk of CVD (25). Reinforcing this evidence and moving toward a paradigm shift in obesity management, the EASO has recently introduced a new framework that aligns obesity diagnosis with chronic disease standards (2). This change is based on the recognition that the diagnostic criteria for obesity should extend beyond BMI, acknowledging that body fat distribution significantly impacts health (2). More specifically, this new framework includes individuals with a lower BMI (≥25–30 kg/m2) but increased abdominal fat accumulation and the presence of any medical, functional, or psychological impairments or complications in the definition of obesity, hence reducing the risk of undertreatment in this particular group of patients compared to the current BMI-based definition (2). Our findings support this new position statement, as only patients meeting the new obesity criteria exhibited a worse glycemic and hypertensive profile, required more prescriptions for antihypertensive and lipid-lowering therapies, and showed an increased prevalence of SAD.
Our study provides the first evidence regarding the significant association between the new obesity definition and the presence of atheroma plaques in femoral artery territory. This finding is particularly relevant as atherosclerosis is a multifaceted disease influenced by factors such as hemodynamic forces, genetic predisposition, sex, immune status, oxidative stress, and chronic low-grade inflammation (26). While the specific pathogenic mechanisms underlying plaque formation and their variable impact across vascular territories are not yet fully understood, evidence suggests that the localization of atherosclerotic plaques plays a pivotal role in disease progression (14, 15).
Taking into consideration studies on femoral plaque burden, such as that by Vaudo et al., evidence suggests that patients with metabolic syndrome exhibit increased intima-media thickness (IMT) at the femoral site compared to healthy controls. Their findings indicate that femoral IMT is directly associated with LDL cholesterol, triglycerides, and glycemia (27). Similarly, the Progression of Early Subclinical Atherosclerosis (PESA) study demonstrated a significant association between femoral plaque burden and factors such as age, sex, smoking, and dyslipidemia, with comparable results observed in the Aragón Worker’s Heath Study (AWHS) (28, 29). Conversely, our results also suggest that the impact of obesity on the development of atheromatous disease in carotid territories may be more associated with other CV risk factors, such as hypertension, prediabetes, or smoking, which would potentially play a more significant role in its development. The proximity of femoral arteries to abdominal visceral adipose tissue (VAT) may further contribute to this process through paracrine signaling mechanisms that favor the formation of dense, calcified plaques (30–33). Imaging studies using magnetic resonance have also shown that femoral plaques typically contain smaller necrotic cores and fewer intraplaque hemorrhages compared to carotid plaques, further highlighting their distinct pathophysiological profile (34).
The high prevalence of obesity found in our study merits further comments. Our data show that 37.2% of individuals with low-to-moderate CV risk recruited in the ILERVAS cohort had a BMI ≥30 kg/m², nearly double the prevalence reported in Spain (overall prevalences of obesity and overweight of 18.7% and 55.8%, respectively) (35). These elevated rates can likely be attributed to the inclusion criteria, which required participants to be over 45 years of age and present at least one CV risk factor—obesity, as defined by BMI, being one of them. The prevalence rose above 70% when we included individuals with overweight and abdominal adiposity, regardless of the presence of obesity-related comorbidities. Apart from the characteristics of our study, the further increase of obesity following the new EASO criteria, together with the elevated prevalence of SAD revealed in this population, opens up a new scenario not only in epidemiological terms but also in the sustainability of healthcare systems due to the huge economic burden of the associated treatments.
Our study has several limitations that warrant discussion. First, its cross-sectional design prevents us from establishing causal relationships. Second, the assessment of atherosclerosis was confined to the carotid and femoral territories, excluding other vascular regions such as the aorta or coronary arteries, which are also relevant to measuring cardiovascular risk. Additionally, our study exclusively included individuals with at least one cardiovascular risk factor, which may partly explain the high prevalence of SAD observed. However, when including participants with overweight and abdominal obesity without associated obesity-related comorbidities, the results remained consistent, further highlighting the role of VAT in the development of CVD. Finally, a complete lipid profile was only performed in patients with total cholesterol ≥ 200 mg/dl, which may have led to missing atherogenic dyslipidemia in individuals with normal LDL or total cholesterol. Despite these limitations, an important strength of our study is the inclusion of a large, well-characterized cohort of individuals at low-to-moderate cardiovascular risk without established cardiovascular disease.
In summary, this study underscores the critical role of VAT in influencing atheromatosis, particularly in femoral territories, which may have significant implications for CV risk assessment and clinical management. Our results also suggest that the shifting from BMI toward the new obesity definition that includes WtHR, which represents a move from a weight-centered approach to one based on visceral adiposity, leads to earlier identification of SAD, and, therefore, more targeted interventions for individuals at risk of developing serious cardiovascular conditions can be implemented.
ILERVAS Project collaborators
Carolina López-Cano, Eva Miquel, Marta Ortega, Ferran Barbé, Jordi de Batlle, Silvia Barril, Manuel Portero-Otín, Mariona Jové, Josep Franch-Nadal, Esmeralda Castelblanco, Pere Godoy, Montse Martinez- Alonso, and Cristina Farràs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the University Hospital Arnau de Vilanova (Approval number: CEIC-1410). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JL-M: Conceptualization, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. MB-L: Data curation, Investigation, Writing – review & editing. JV: Data curation, Investigation, Writing – review & editing. RP: Investigation, Methodology, Writing – review & editing. GT: Investigation, Methodology, Writing – review & editing. DM: Investigation, Methodology, Writing – review & editing. EC-B: Data curation, Writing – review & editing. EF: Data curation, Investigation, Writing – review & editing. ACa: Investigation, Writing – review & editing. MB: Investigation, Writing – review & editing. ACi: Investigation, Writing – review & editing. MH: Investigation, Writing – review & editing. RS: Conceptualization, Writing – review & editing. CH: Conceptualization, Methodology, Writing – review & editing. AL: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study has been funded by the Instituto de Salud Carlos III (ISCIII) throught the project PI21/00462 and co-funded by the European Union. Authors in the study also participate in this other grants: PI21/01099, PMP21/00109, PMP22/00073, PI23/00237 and RD24/0004/0015 (Institute of Health Carlos III, European Regional Development Fund, “A way to build Europe), PID2022-141964OB-I00 (Ministerio de Ciencia, Innovación y Universidades, co-funded by the European Regional Development Fund, “A way to build Europe”), the Spanish Ministry of Science, Innovation, and Universities (PID2023-152233OB-100, co-funded by the European Regional Development Fund, “A way to build Europe”), and the Generalitat of Catalonia: Agency for Management of University and Research Grants (2021SGR00990) and Department of Health (SLT002/16/00250).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor LB declared a past co-authorship with the author Andreea Ciudin.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bray GA, Kim KK, Wilding JPH, and World Obesity Federation. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev. (2017) 18:715–23. doi: 10.1111/obr.12551
2. Busetto L, Dicker D, Frühbeck G, Halford JCG, Sbraccia P, Yumuk V, et al. A new framework for the diagnosis, staging and management of obesity in adults. Nat Med. (2024) 30:2395–99. doi: 10.1038/s41591-024-03095-3
3. Burki T. European Commission classifies obesity as a chronic disease. Lancet Diabetes Endocrinol. (2021) 9:418. doi: 10.1016/S2213-8587(21)00145-5
4. Frühbeck G, Busetto L, Dicker D, Yumuk V, Goossens GH, Hebebrand J, et al. The ABCD of obesity: an EASO position statement on a diagnostic term with clinical and scientific implications. Obes Facts. (2019) 12:131–36. doi: 10.1159/000497124
5. Yumuk V, Tsigos C, Fried M, Schindler K, Busetto L, Micic D, et al. European guidelines for obesity management in adults. Obes Facts. (2015) 8:402–24. doi: 10.1159/000442721
6. Garvey WT, Mechanick JI, Brett EM, Garber AJ, Hurley DL, Jastreboff AM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. (2016) 22:1–203. doi: 10.4158/EP161365.GL
7. Wharton S, Lau DCW, Vallis M, Sharma AM, Biertho L, Campbell-Scherer D, et al. Obesity in adults: a clinical practice guideline. CMAJ. (2020) 192:E875–91. doi: 10.1503/cmaj.191707
8. Goossens GH. The metabolic phenotype in obesity: fat mass, body fat distribution, and adipose tissue function. Obes Facts. (2017) 10:207–15. doi: 10.1159/000471488
9. Ashwell M, Gunn P, and Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. (2012) 13:275–86. doi: 10.1111/j.1467-789X.2011.00952.x
10. Koenen M, Hill MA, Cohen P, and Sowers JR. Obesity, adipose tissue and vascular dysfunction. Circ Res. (2021) 128:951–68. doi: 10.1161/CIRCRESAHA.121.318093
11. Alexopoulos N, Katritsis D, and Raggi P. Visceral adipose tissue as a source of inflammation and promoter of atherosclerosis. Atherosclerosis. (2014) 233:104–12. doi: 10.1016/j.atherosclerosis.2013.12.023
12. Cornier MA, Després JP, Davis N, Grossniklaus DA, Klein S, Lamarche B, et al. Assessing adiposity: a scientific statement from the American Heart Association. Circulation. (2011) 124:1996–2019. doi: 10.1161/CIR.0b013e318233bc6a
13. Mongraw-Chaffin M, Allison MA, Burke GL, Criqui MH, Matsushita K, Ouyang P, et al. CT-derived body fat distribution and incident cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis. J Clin Endocrinol Metab. (2017) 102:4173–83. doi: 10.1210/jc.2017-01113
14. Polak JF, Person SD, Wei GS, Godreau A, Jacobs DR, Harrington A, et al. Segment-specific associations of carotid intima-media thickness with cardiovascular risk factors: the coronary artery risk development in young adults (CARDIA) study. Stroke. (2010) 41:9–15. doi: 10.1161/STROKEAHA.109.566596
15. Zarins CK, Giddens DP, Bharadvaj BK, Sottiurai VS, Mabon RF, Glagov S, et al. Carotid bifurcation atherosclerosis. Quantitative correlation of plaque localization with flow velocity profiles and wall shear stress. Circ Res. (1983) 53:502–14. doi: 10.1161/01.RES.53.4.502
16. Betriu À, Farràs C, Abajo M, Martinez-Alonso M, Arroyo D, Barbé F, et al. Randomised intervention study to assess the prevalence of subclinical vascular disease and hidden kidney disease and its impact on morbidity and mortality: the ILERVAS project. Nefrologia. (2016) 36:389–96. doi: 10.1016/j.nefro.2016.02.008
17. Bermúdez-López M, Martínez-Alonso M, Castro-Boqué E, Betriu À, Cambray S, Farràs C, et al. Subclinical atheromatosis localization and burden in a low-to-moderate cardiovascular risk population: the ILERVAS study. Rev Esp Cardiol (Engl Ed). (2021) 74:1042–53. doi: 10.1016/j.rec.2020.09.015
18. American Diabetes Association. Diagnosis and classification of diabetes. In: Standards of care in diabetes-2024. Diabetes Care. (2024) 47:S20–42. doi: 10.2337/dc24-S002
19. Sabetai MM, Tegos TJ, Nicolaides AN, Dhanjil S, Pare GJ, Stevens JM, et al. Reproducibility of computer-quantified carotid plaque echogenicity: can we overcome the subjectivity? Stroke. (2000) 31:2189–96. doi: 10.1161/01.STR.31.9.2189
20. Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Desvarieux M, et al. Advisory board of the 3rd Watching the Risk Symposium 2004, 13th European Stroke Conference. Mannheim intima-media thickness consensus. Cerebrovasc Dis. (2004) 18:346–9. doi: 10.1159/000081812
21. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. (2008) 21:93–111. doi: 10.1016/j.echo.2007.11.011
22. Tiozzo E, Gardener H, Hudson BI, Dong C, Della-Morte D, Crisby M, et al. High-density lipoprotein subfractions and carotid plaque: the Northern Manhattan Study. Atherosclerosis. (2014) 237:163–8. doi: 10.1016/j.atherosclerosis.2014.09.002
23. R Core Team. R: A Language and Environment for Statistical Computing. 1999–2025 R Foundation for Statistical Computing. (2025). Available online at: https://cran.r-project.org/doc/manuals/r-release/fullrefman.pdf (Accessed October 1, 2025).
24. Feng Q, Bešević J, Conroy M, Omiyale W, Woodward M, Lacey B, et al. Waist-to-height ratio and body fat percentage as risk factors for ischemic cardiovascular disease: a prospective cohort study from UK Biobank. Am J Clin Nutr. (2024) 119:1386–96. doi: 10.1016/j.ajcnut.2024.03.018
25. Xue R, Li Q, Geng Y, Wang H, Wang F, Zhang S, et al. Abdominal obesity and risk of CVD: a dose-response meta-analysis of thirty-one prospective studies. Br J Nutr. (2021) 126:1420–30. doi: 10.1017/S0007114521000064
26. VanderLaan PA, Reardon CA, and Getz GS. Site specificity of atherosclerosis: site-selective responses to atherosclerotic modulators. Arterioscler Thromb Vasc Biol. (2004) 24:12–22. doi: 10.1161/01.ATV.0000105054.43931.f0
27. Vaudo G, Marchesi S, Siepi D, Brozzetti M, Mannarino MR, Pirro M, et al. Metabolic syndrome and preclinical atherosclerosis: focus on femoral arteries. Metabolism. (2007) 56:541–6. doi: 10.1016/j.metabol.2006.11.016
28. López-Melgar B, Fernández-Friera L, Oliva B, García-Ruiz JM, Peñalvo JL, Gómez-Talavera S, et al. Subclinical atherosclerosis burden by 3D ultrasound in mid-life: the PESA study. J Am Coll Cardiol. (2017) 70:301–13. doi: 10.1016/j.jacc.2017.05.033
29. Laclaustra M, Casasnovas JA, Fernández-Ortiz A, Fuster V, León-Latre M, Jiménez-Borreguero LJ, et al. Femoral and carotid subclinical atherosclerosis association with risk factors and coronary calcium: the AWHS study. J Am Coll Cardiol. (2016) 67:1263–74. doi: 10.1016/j.jacc.2015.12.056
30. Vasamsetti SB, Natarajan N, Sadaf S, Florentin J, and Dutta P. Regulation of cardiovascular health and disease by visceral adipose tissue-derived metabolic hormones. J Physiol. (2023) 601:2099–120. doi: 10.1113/JP282728
31. Li N, Cheng W, Huang T, Yuan J, Wang X, Song M, et al. Vascular adventitia calcification and its underlying mechanism. PloS One. (2015) 10:e0132506. doi: 10.1371/journal.pone.0132506
32. Kim S, Lee ES, Lee SW, Kim YH, Lee CH, Jo DG, et al. Site-specific impairment of perivascular adipose tissue on advanced atherosclerotic plaques using multimodal nonlinear optical imaging. Proc Natl Acad Sci United States America. (2019) 116:17765–74. doi: 10.1073/pnas.1902007116
33. Krohn JB, Hutcheson JD, Martínez-Martínez E, Irvin WS, Bouten CV, Bertazzo S, et al. Discoidin domain receptor-1 regulates calcific extracellular vesicle release in vascular smooth muscle cell fibrocalcific response via transforming growth factor-β signaling. Arteriosclerosis Thrombosis Vasc Biol. (2016) 36:525–33. doi: 10.1161/ATVBAHA.115.307009
34. Helck A, Bianda N, Canton G, Yuan C, Hippe DS, Reiser MF, et al. Intra-individual comparison of carotid and femoral atherosclerotic plaque features with in vivo MR plaque imaging. Int J Cardiovasc Imaging. (2015) 31:1611–8. doi: 10.1007/s10554-015-0737-4
35. Gutiérrez-González E, García-Solano M, Pastor-Barriuso R, Fernández de Larrea-Baz N, Rollán-Gordo A, Peñalver-Argüeso B, et al. Socio-geographical disparities of obesity and excess weight in adults in Spain: insights from the ENE-COVID study. Front Public Health. (2023) 11:1195249. doi: 10.3389/fpubh.2023.1195249
Keywords: obesity, central adiposity, subclinical atheromatous disease, cardiovascular risk factors, waist-to-height ratio
Citation: León-Mengíbar J, Bermúdez-López M, Valdivielso JM, Pamplona R, Torres G, Mauricio D, Castro-Boqué E, Fernández E, Caixàs A, Bueno M, Ciudin A, Hernández M, Simó R, Hernández C and Lecube A (2025) Impact of the new EASO obesity definition on the detection of atheromatosis in subjects with low-to-moderate cardiovascular risk. Front. Endocrinol. 16:1689960. doi: 10.3389/fendo.2025.1689960
Received: 21 August 2025; Accepted: 22 September 2025;
Published: 10 October 2025.
Edited by:
Luca Busetto, University of Padua, ItalyReviewed by:
Dror Dicker, Hasharon Hospital Rabin Medical Center, IsraelPaolo Sbraccia, University of Rome Tor Vergata, Italy
Copyright © 2025 León-Mengíbar, Bermúdez-López, Valdivielso, Pamplona, Torres, Mauricio, Castro-Boqué, Fernández, Caixàs, Bueno, Ciudin, Hernández, Simó, Hernández and Lecube. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Hernández, Y3Jpc3RpbmEuaGVybmFuZGV6QHZoaXIub3Jn; Albert Lecube, YWxiZXJ0LmxlY3ViZUB2YWxsaGVicm9uLmNhdA==