 Lidia Castro-Feijóo1*†
Lidia Castro-Feijóo1*† José-Ignacio Labarta-Aizpún2*†
José-Ignacio Labarta-Aizpún2*† Marta Ramon-Krauel3*†Diana Primiano4Diego Yeste Fernández5Isabel González Casado6 on behalf of the ConverGHe Working Group
Marta Ramon-Krauel3*†Diana Primiano4Diego Yeste Fernández5Isabel González Casado6 on behalf of the ConverGHe Working Group- 1Unidad de Endocrinología Pediátrica, Hospital Clínico Universitario de Santiago de Compostela, Instituto de Investigación Sanitaria de Santiago de Compostela, IDIS, Santiago de Compostela, Spain
- 2Unidad de Endocrinología, Servicio de Pediatría, Hospital Universitario Miguel Servet, Instituto Investigación Sanitaria Aragón, Zaragoza, Spain
- 3Servicio de Endocrinología Pediátrica, Hospital Sant Joan de Déu, Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, Barcelona, Spain
- 4Medical Affairs, Pfizer S.L.U., Madrid, Spain
- 5Servicio de Endocrinología Pediátrica, Hospital Universitari Vall d’Hebron, Universitat Autònoma de Barcelona, Barcelona, Spain
- 6Servicio de Endocrinología Pediátrica, Hospital Universitario La Paz, Madrid, Spain
Background: Long-acting growth hormone (LAGH) formulations have emerged as an alternative to daily recombinant human growth hormone (rhGH) in pediatric growth hormone deficiency (GHD). Although evidence from meta-analyses and randomized trials supports their efficacy and safety, real-life data are still lacking, and therefore clinical guidance on their implementation remains limited.
Objective: To develop expert-based recommendations for the clinical use of LAGH in pediatric GHD within Spain.
Methods: A two-round Delphi approach was used. Based on a literature review, a scientific committee comprised of pediatric endocrinologists developed a questionnaire structured into three domains: (1) Main benefits of LAGH vs. daily rhGH; (2) Candidate profiles for LAGH therapy; and (3) Considerations for initiating LAGH and treatment monitoring. Panelists rated their level of agreement with each questionnaire statement on a 9-point Likert scale. Consensus was defined as ≥66.67% of responses on the same tertile as the median, labelled as disagreement on scores of 1–3, intermediate on scores of 4–6, and agreement on scores 7–9. Statements that did not reach consensus were reformulated and re-evaluated in round 2.
Results: After two rounds, all statements achieved consensus on agreement. Specifically, consensus was reached on 92% of the statements in round 1 and three revised items related to insulin-like growth factor-1 (IGF-1), pharmacokinetics and dose adjustment criteria, as well as the use of LAGH in patients at risk of hypoglycemia, achieved consensus in round 2. The recommendations emphasize the similar efficacy and safety of LAGH compared to rhGH, raising its special interest in cases of poor adherence to daily formulations (e.g. adolescents, injection-related anxiety, multiple comorbid treatments or complex family circumstances), although LAGH should also be considered in other settings in a patient-centered approach. In addition, they provide guidance on key issues related to adequate dose initiation and titration, as well as therapeutic monitoring.
Conclusion: This is the first Delphi consensus to provide national-level guidance on integrating LAGH into pediatric GHD care, offering practical recommendations based on current evidence and national expert opinion. Future long-term real-world experience will contribute to address questions regarding long-term efficacy and safety, and practice-related points such as indication and monitoring.
1 Introduction
Growth hormone deficiency (GHD) is a rare condition with an estimated incidence ranging from 1 in 3,000 to 1 in 10,000 live births (1–3). It occurs due to an inadequate secretion of growth hormone (GH), leading to growth-retardation, biochemical, metabolic, and psychological defects if untreated. GHD is typically diagnosed based on growth patterns and confirmed through biochemical testing, including GH stimulation tests, insulin-like growth factor-1 (IGF-1) and insulin-like growth factor-binding protein 3 (IGFBP-3) levels and, when necessary, neuroimaging of the pituitary region and genetic studies. It may be idiopathic, congenital or acquired, and present either as an isolated or as part of combined pituitary hormone deficiencies (4).
The standard of care for pediatric GHD for over three decades has been daily subcutaneous injections of recombinant human GH (rhGH), which have proven to be safe and effective in increasing growth velocity and achieving expected adult height (4, 5). Despite the effectiveness of daily rhGH, the burden of daily injections can negatively impact adherence, particularly in children and adolescents. Studies have shown that up to two-thirds of pediatric patients miss more than one injection per week, a factor strongly associated with suboptimal growth outcomes (6–8). Furthermore, adherence has been shown to decrease from 85% to 74% from the first to the third year of GH replacement, with the greatest decrease in males, adolescents and patients with childhood-onset GHD (9). Challenges to adherence may include needle aversion, inconsistent home routines, or lack of caregiver support.
To address these limitations, long-acting GH (LAGH) formulations have been developed to reduce injection frequency to weekly dosing while maintaining therapeutic efficacy, with non-inferiority demonstrated in pivotal phase III trials when compared to daily rhGH (10–12). Several formulations of LAGH with different pharmacokinetic and pharmacodynamic profile were developed and are currently being studied in children. Those include unmodified rhGH in a depot formulation (Eutropin Plus®, LG Life Sciences, approved in South Korea), pegylated rhGH (Jintrolong®, GenSci, approved in China), modified rhGH with increased albumin binding (somapacitan, Sogroya®, Novo Nordisk), prodrug formulation (lonapegsomatropin, Skytrofa®, Ascendis Pharma) and rhGH fusion proteins (somatrogon, NGENLA®, Pfizer/OPKO) (13). Of these, only somatrogon and somapacitan included Spanish patients in their respective clinical development programs and have been provided with a national code by the Spanish Agency of Medicines and Medical Devices (AEMPS), with somatrogon being the unique LAGH formulation currently marketed in Spain for the treatment of children and adolescents from 3 years of age with growth disturbance due to insufficient secretion of GH (4). In this regard, it should be emphasized that, while the indications currently approved by regulatory agencies for rhGH treatment also include growth disorders associated with other non-GHD conditions, for the time being the indications for LAGH are limited to GHD (14).
Although treatment with daily rhGH has been shown to be safe and effective in the long-term (5), similar studies to evaluate LAGH are not yet available. Additionally, the unique pharmacokinetic and pharmacodynamic profile of each LAGH requires different dosing and monitoring compared to daily rhGH injections, which may pose an added challenge for the management of these formulations (15, 16). International consensus statements have begun to address some of these gaps (17), but national guidance is needed to align with local regulations, practices, and patient needs. This consensus aims to provide clear guidance on how to integrate LAGH into the routine clinical care of pediatric patients with GHD, based on expert recommendations and supported by current evidence. This will facilitate suitable patient selection, proper treatment initiation and long-term monitoring, while also highlighting current gaps to guide future efforts.
2 Methods
2.1 Study design and participants
This study comprised a systematic literature review, followed by the development of evidence-based statements, which were then evaluated using a two-round Delphi consensus methodology.
The process involved a scientific committee comprising three advisors and 27 panelists, all pediatric endocrinologists practicing in Spain. Advisors were designated based on their expertise in treating children with daily rhGH and LAGH, as well as their involvement in LAGH publications and clinical trials. As the Delphi methodology is qualitative by nature, the expert committee selected panelists to vote on the statements based on several criteria, including membership of leading scientific societies such as the Spanish Society of Pediatric Endocrinology (SEEP), and having more than 10 years’ experience in managing pediatric GHD.
2.2 Systematic literature review
A targeted literature review was conducted using PubMed and Embase, applying both free-text and MeSH terms, aimed at identifying key evidence regarding LAGH and potential controversies. Search terms included growth-hormone deficiency (GHD) therapy, recombinant human growth hormone (rhGH), long-acting growth hormone (LAGH), treatment efficacy and safety, adherence and convenience, quality of life, treatment monitoring, and candidate patient profiles. The search focused on phase II and III clinical trials, regulatory documents, relevant consensus statements, and real-world studies when available, prioritizing those of more recent publication. Additionally, abstracts from international congresses were reviewed to capture emerging data not yet published in journals.
2.3 Development of Delphi questionnaire
The advisors reviewed the selected reports from the systematic literature review and drafted a proposal for statements, emphasizing on those topics considered most controversial or relevant. The statements were refined during two in-person meetings held in November 2024 to agree on the final approach. An expert methodologist was present during the meetings to ensure quality and rigor in the elaboration of the statements.
2.4 Two-round Delphi process
The Delphi process consisted of two rounds of voting by the expert panel. In round 1, the panel was asked to rate their level of agreement with each statement in the questionnaire on a 9-point Likert scale, from 1 (strongly disagree) to 9 (strongly agree) (18). For this purpose, an in-person meeting was held in January 2025 where voting was conducted anonymously via an interactive platform and comments from the panelists were collected.
The first-round results were discussed by the scientific committee in an online meeting in February 2025. Those statements that did not reach the consensus threshold were modified based on feedback from the expert panel and were either rephrased or split into separate sentences to improve their comprehensibility. In round 2, the updated questionnaire was redistributed, removing all statements that met the consensus threshold in round 1 and including only those that did not, resulting in a splitting of one of these statements into two separate recommendations. Panelists were again asked to rate statements that had not reached consensus using the same criteria described for round 1 via an anonymous online survey to streamline the process.
2.5 Statistical analysis
Descriptive statistics were used to summarize the demographic characteristics and the scores obtained for each statement. Consensus was defined as ≥66.67% of responses on the same tertile as the median, labelled as disagreement on scores of 1–3, intermediate on scores of 4–6, and agreement on scores 7–9. The Kolmogorov–Smirnov test was used to evaluate goodness-of-fit of the data to a normal distribution. Internal consistency of the Delphi questionnaire was evaluated with Cronbach’s α (excellent reliability: α≥0.90; good reliability: α = 0.80-0.90; moderate-good reliability: α = 0.70-0.80; moderate-acceptable reliability: α = 0.60-0.70; poor reliability: α = 0.50-0.60; unacceptable reliability: α<0.50) (19). Spearman’s correlation coefficient was used to evaluate the correlation between rounds, by statement and for the entire questionnaire (0-0.25 = slight or no correlation; 0.26-0.50 = weak correlation; 0.51-0.75 = moderate to strong correlation) (20). The increase in the coefficient of variation between the two rounds was analyzed to determine whether a third round was necessary. All the statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 28.0.
3 Results
3.1 Literature review and Delphi questionnaire
A total of 56 reports were selected for inclusion in the literature review after an assessment of their clinical relevance to the proposed scope. Based on this evidence, the scientific committee finally yielded 37 statements categorized into three major domains: (1) Main benefits of LAGH vs. daily rhGH (11 statements); (2) Candidate profiles for LAGH therapy (14 statements); and (3) Considerations for initiating LAGH and treatment monitoring (12 statements). In turn, each domain was divided into several subtopics to facilitate the structuring of the information.
3.2 Delphi study
All 27 of the selected panelists completed both rounds of the Delphi questionnaire. A total of 37 statements were initially evaluated across the three domains using a 9-point Likert scale. In round 1, consensus was reached on 34/37 (92%) statements. The remaining items were reconsidered in round 2, after one of the statements was split in two for better understanding, all of which ultimately reached consensus. The median agreement across statements was 88.9% (IQR 7-9). Supplementary Figure 1 and Supplementary Figure 2 (Supplementary Material) show the results of Likert-scale voting distribution by statement for round 1 and 2, respectively.
The questionnaire had excellent internal consistency (Cronbach α=0.957 [p<0.001] (Table 1). The Spearman correlation coefficient for the questionnaire was strong (0.922 [p<0.001]), indicating a high quantitative correlation between the two rounds. The increase in the coefficient of variation between rounds did not exceed 10%, and in absolute terms was less than 1% (0.1870 ± 0.1127 and 0.1781 ± 0.1113 for round 1 and 2, respectively), which justified the decision to forgo a third round.
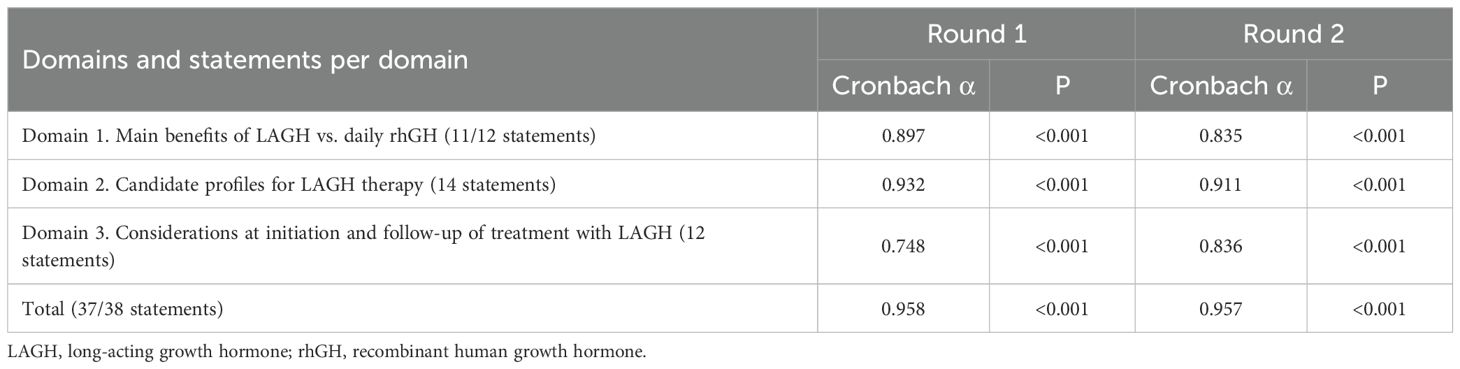
Table 1. Delphi questionnaire reliability.
3.3 Consensus statements
3.3.1 Domain 1: main benefits of LAGH vs. daily rhGH
This domain included 11 statements that focused on the clinical and perceived advantages of LAGH compared to daily rhGH. Ten of these statements achieved consensus in round 1, while one statement (S11, concerning the interpretation of IGF-1 levels) was revised for round 2. The panel considered the statement too broad, as it combined the pharmacokinetic timing of IGF-1 peaks with whether IGF-1 levels remain within normal ranges. As a result, the item was split into two independent statements, reaching a high degree of agreement for both in round 2 (92.6% and 85.2%, respectively). Regarding the other topics discussed, there was a high degree of agreement that the efficacy of LAGH is similar to that of daily rhGH (88.9%), with no differences observed in the monitoring of laboratory parameters such as metabolic, biochemical, and thyroid function (88.9%), or in bone progression (92.6%), although all panelists unanimously agreed that long-term safety is still unknown. LAGH formulations were also perceived to have a higher incidence of mild injection-site reactions (92.6%) and a higher degree of immunogenicity compared to daily rhGH. However, the latter has no implications on clinical response (96.3%). The panel also reached a high degree of consensus about the lower interference of LAGH in the daily lives of patients and caregivers (96.3%). Although it was also agreed that satisfaction with LAGH is greater and adherence is expected to be higher than with daily rhGH, the percentage of agreement was lower (77.8% and 74.1%, respectively). However, it was emphasized that long-term studies are needed to quantify the impact of LAGH on health-related quality of life (96.3%) (Table 2).
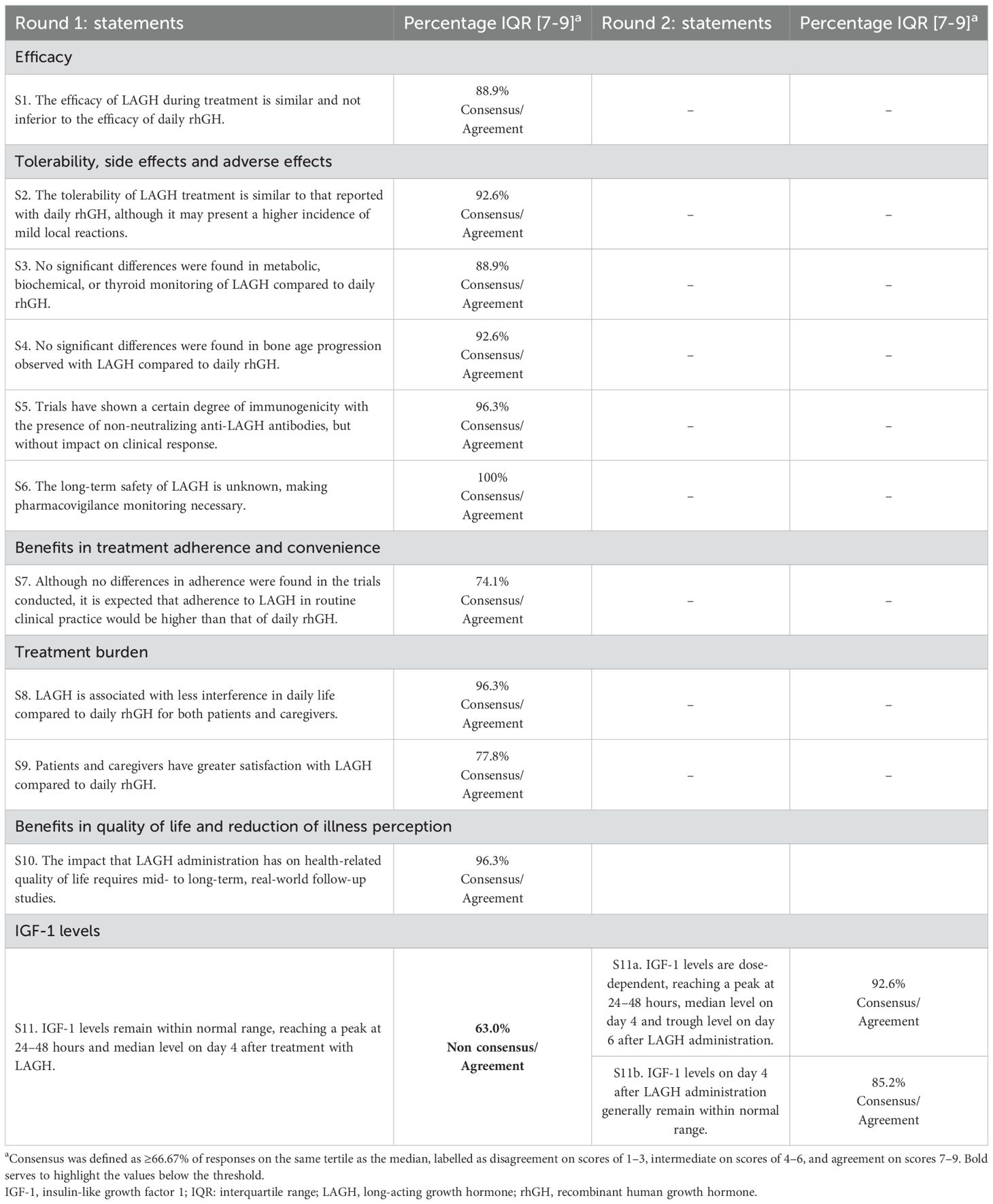
Table 2. Results of the two-step Delphi process for the statements on domain 1.
3.3.2 Domain 2: candidate profiles for LAGH therapy
Thirteen of the 14 statements in this domain reached consensus in round 1. One statement (S14), related to the non-recommendation of LAGH use in patients with severe GH deficiency and risk of hypoglycemia, did not initially reach consensus and was modified to indicate that caution should be exercised in this case, being accepted in round 2 with a high percentage of agreement (88.9%). There was also a high degree of consensus to not recommend the use of LAGH in specific profiles such as cancer survivors with acquired GHD (88.9%) or patients with GHD associated to other conditions (e.g. mitochondrial disorders, Fanconi anemia, Prader-Willi syndrome, genetic syndromes) until more long-term evidence of its safety profile is generated (92.6%). However, the panel endorsed the use of LAGH in scenarios such as adolescent patients (85.2%), needle phobia or anxiety related to treatment administration (96.3%), poor adherence to daily injections (81.5%), patients with behavioral disorders or neurodiversity (92.6%), and concurrent therapies requiring multiple injections (96.3%). Regarding switching to LAGH, there was consensus that it should be considered whenever requested by the patient or caregiver taking into account the patient’s characteristics (81.5%). Although the agreement was at the threshold limit, the transition to self-administration was perceived as an appropriate moment to inform about the availability of LAGH formulations. Additionally, it was also agreed that proposing the switch to LAGH is not recommended for patients with a good response, tolerance, and satisfaction with daily rhGH (74.1%) (Table 3).
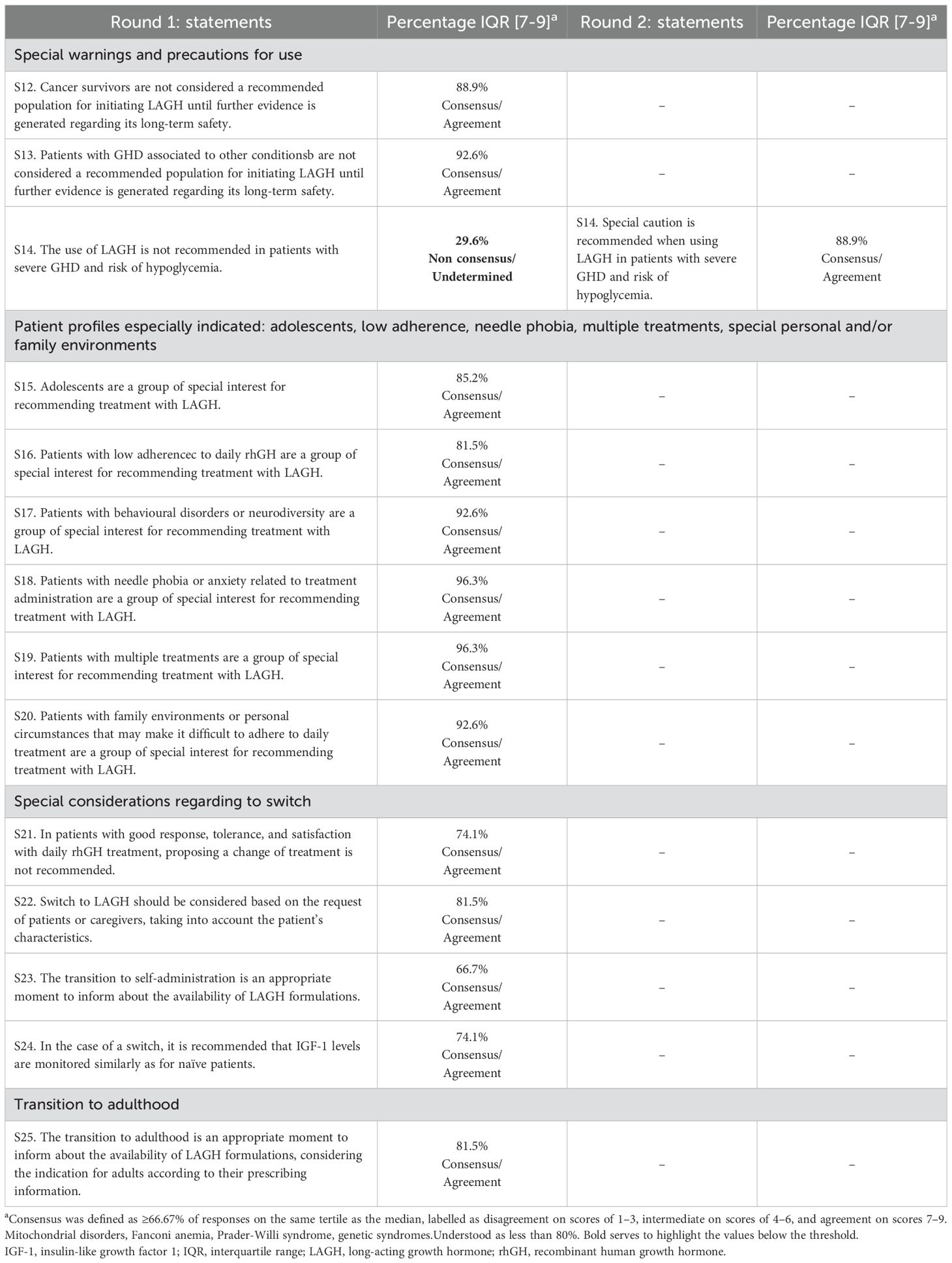
Table 3. Results of the two-step Delphi process for the statements on domain 2.
3.3.3 Domain 3: considerations for initiating LAGH and treatment monitoring
This domain included 12 statements that focused on various considerations for the initiation of treatment with LAGH and proper monitoring of its efficacy and safety. Eleven of these statements achieved consensus in round 1, while one statement (S31, confirmation of IGF-1 level deviation for dose reduction) was revised and accepted in round 2 with a moderate level of agreement (74.1%). Regarding the other topics discussed, there was a high degree of agreement that the decision to initiate treatment with LAGH should be shared between the physician, family and patient (88.9%). All panelists unanimously highlighted the importance of providing therapeutic education on LAGH administration and adequately informing the family about the current state of knowledge about LAGH before initiating treatment. The panel also reached a high degree of consensus that LAGH dose adjustment during follow-up should be individualized based on growth rate, adverse reactions, and serum IGF-1 concentration (96.3%), with dose reassessment initially at 3 months after initiation of treatment and then every 6 months (74.1%). Furthermore, it was also agreed that monitoring of LAGH treatment should include biochemical and hormonal safety profile follow-up 3 months after initiation and every 6–12 months thereafter (81.5%), biannual auxological follow-up (88.9%), and annual bone age monitoring (85.2%). Finally, there was a strong consensus that IGF-1 determination should be performed on day 4 after the last LAGH administration or alternatively by normalization formulas (92.6%), using assays with reliable reference data based on age, sex, and pubertal status (96.3%) (Table 4).
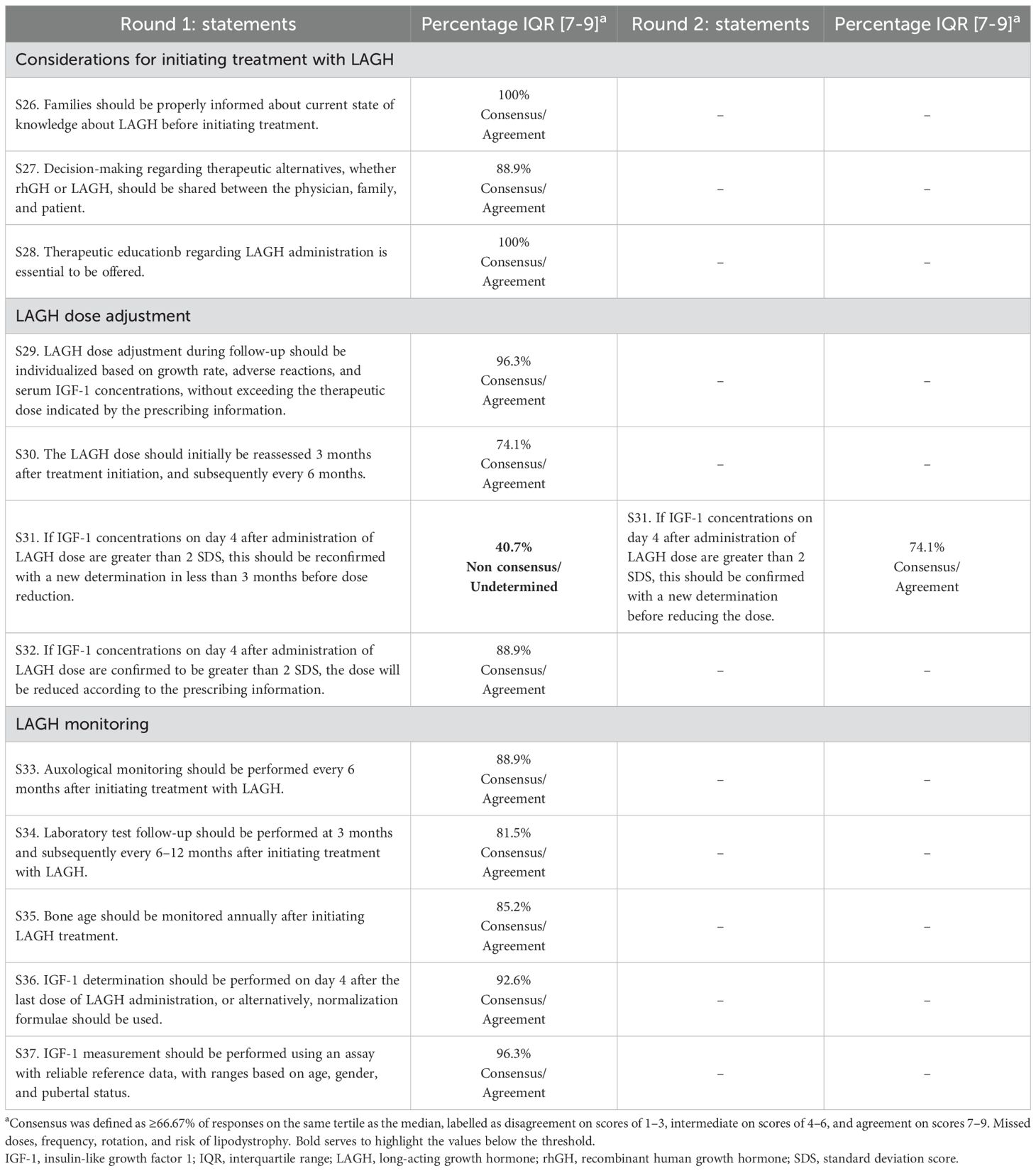
Table 4. Results of the two-step Delphi process for the statements on domain 3.
4 Discussion
This is the first Delphi study regarding the use of LAGH in Spain with the aim of providing guidance on its integration into clinical practice. This issue has been addressed in several recent studies, such as the international consensus published by Maniatis et al., 2025 (17), and the recommendations made by Linglart et al., 2024 (21) which are applicable to the current management of LAGH formulations in France. Our consensus is closely aligned with the conclusions drawn in these studies, further strengthened using a more rigorous, systematized working method, such as the Delphi approach. The study panel was able to reach a high degree of consensus among leading pediatric endocrinologists in Spain on relevant aspects of the clinical use of LAGH formulations in children with GHD, with a particular focus on its potential benefits compared with daily rhGH, main considerations for initiating therapy and treatment monitoring, and patient profiles that may benefit most from a weekly dosing regimen. Nevertheless, this Delphi process also revealed uncertain issues, particularly regarding the lack of long-term data to enhance current knowledge of LAGH, and the need to improve clinicians’ understanding of its unique pharmacokinetic characteristics to enable appropriate dose adjustment and IGF-1 monitoring in both naïve patients and those switching from daily rhGH.
4.1 Domain 1: main benefits of LAGH vs. daily rhGH
The high degree of consensus reached by the panel reveals that LAGH formulations are perceived as a novel therapeutic option with similar efficacy to daily rhGH in terms of growth velocity, height standard deviation score (SDS), and bone age progression, which is widely described in several published systematic reviews, meta-analyses, and phase II and III pivotal trials (10–12, 22–30). However, it is emphasized that, while the evidence is clear in the short term, data on final adult height outcomes remain limited, making longer-term follow-up necessary. Similarly, the panel’s perception of the safety profile of LAGH is consistent with currently available data, which have shown a similar incidence of treatment-emergent adverse events compared with daily rhGH, in most cases mild or moderate in severity (10, 12, 22–28). Nevertheless, the available clinical trials to date have revealed some differences in tolerability and safety profiles between different LAGH formulations, which explains some of the clarifications included in the consensus statements. On the one hand, while the levels of non-neutralizing anti-drug antibodies observed for somapacitan and lonapegsomatropin were similar to those reported for rhGH (11, 12), an increase was observed with somatrogon (10). However, as confirmed by the published evidence, it should be emphasized that this has no implications on clinical outcomes (10, 12, 29). On the other hand, injection site pain was reported infrequently in trials of somapacitan, variably in lonapegsomatropin trials and at a high frequency in somatrogon trials, however mostly mild to moderate (10), which can probably be explained by factors such as the volume of each injection, preservatives in buffer solution, needle size, or other needle features (23). Regarding local reactions, it is also hypothesized that the higher incidence reported with somatrogon compared to other LAGH formulations may be due to more thorough recording than in other trials (10). Overall, long-term safety remains an important unknown due to the limited duration of follow-up with LAGH compared to daily rhGH (26), emphasizing the importance for future studies and pharmacovigilance monitoring. GH registries are valuable data sources to evaluate efficacy and safety of GH treatment. Long-term phase IV LAGH studies, including real-world practice, will improve understanding and are needed to demonstrate these benefits and the cost-effectiveness of LAGH. GloBE-Reg (Global Registry For Novel Therapies In Rare Bone & Endocrine Conditions) is an international registry project that focuses on effectiveness and safety of any GH treatment, including LAGH. Pfizer is participating in this international registry through Pfizer Registry of Outcomes in Growth hormone RESearch (PROGRES) as a phase IV substudy of daily rhGH and LAGH. Similarly, other industries are also participating such as the REAL10 study of somapacitan in children with GH deficiency. Sharing data in a unique international registry will increase the power of the information obtained and will allow the development of evidence-based information (31, 32).
Regarding adherence to LAGH, current evidence shows no difference compared to daily rhGH, most likely because the studies were not designed to assess this endpoint (10, 28, 29). Nonetheless, although the level of consensus was moderate for this statement, it is hypothesized that reducing the frequency of injections may improve adherence to treatment. In this regard, it is also emphasized that devices which allow for certification and monitoring of adherence are desirable, as they are likely to have a positive impact on therapeutic compliance (33, 34). The available data on the impact of LAGH on health-related quality of life is also at present limited (35), which aligns with the panel’s stance. In this regard, doubts have been expressed as to whether future evidence will be able to provide any conclusive information, primarily because of the way in which it is currently defined in questionnaires and the difficulty of objectively assessing this issue in real-life clinical practice. However, the available evidence does support that LAGH reduces the treatment burden on patients’ and caregivers’ lives (12, 36–39), as reflected by the high level of agreement on these items.
Besides, the unique pharmacokinetic profile of LAGH seems to explain the initial lack of consensus and debate regarding IGF-1 levels. Again, the published evidence shows differences between formulations, documenting an increase in IGF-1 levels with LAGH compared with daily rhGH (10–12, 24–26). However, it is emphasized that the percentage of patients who may present a transient elevation during the initial 24–48 hours after administration above the normal range of 2 SDS is small (40).
4.2 Domain 2: candidate profiles for LAGH therapy
Concerning candidate profiles for LAGH therapy, there is no literature directly supporting the use of LAGH in specific circumstances; rather, consensus recommendations are based primarily on indirect evidence (17).
The high degree of consensus reached by the panel reveals that LAGH formulations are perceived as a new therapeutic option especially recommended for patients with poor adherence to daily rhGH, such as adolescent patients in particular, or those with specific situations that may complicate compliance with the therapeutic regimen (e.g. patients with needle phobia or injection-related anxiety, patients with behavioral disorders or neurodiversity, patients on multiple treatments, or patients with special family environments and/or personal circumstances). As described in the literature, adolescents represent a group with particularly low adherence to daily rhGH (41–43). Besides, considering that treatment non-adherence is a complex and multifactorial problem influenced by socio-family factors, injection problems, or treatment fatigue, among others (44–48), it is expected that, due to its dosage characteristics, real-life adherence to LAGH will improve when compared with daily administration formulations. In this regard, several published studies support a lower treatment burden, a better patient and caregiver experience, less interference with daily life, and higher scores regarding therapeutic adherence with LAGH (37, 39). Therefore, its indication for GHD should be always considered on an individual basis, if no contraindications are present. Nevertheless, when it comes to patients receiving multiple treatments, it is also important to carefully assess LAGH treatment, taking patient safety into account based on their underlying pathology.
There was also a high level of agreement to not recommend LAGH treatment for certain special populations, such as cancer survivors or patients with GHD associated with other conditions (e.g., mitochondrial diseases, Fanconi anemia, Prader-Willi syndrome, and other genetic syndromes). Current evidence does not support an association between daily rhGH replacement therapy and primary tumor or cancer recurrence in GHD children (5, 49–51). This information is still unknown for LAGH formulations, emphasizing the need for long-term surveillance into safety in this regard. Nonetheless, the use of LAGH in toddler patients with severe GHD has been subject of discussion due to the high risk of hypoglycemia, particularly given the lower GH levels in the days prior to the next dose. The agreement ultimately reached by the panel concerning this item suggests special caution when considering the use of LAGH in this profile without age specification, assuming that the treatment will be prescribed according to the indications approved by the medical agencies. However, the need to perform blood glucose monitoring is emphasized in severe GHD with risk of hypoglycemia, especially in the 1–2 days prior to each injection (21).
Regarding switching from daily rhGH to LAGH, the panel favored a patient-centered approach. While switching is not recommended in patients with good response, tolerance and satisfaction with daily rhGH treatment, there is a high degree of agreement that LAGH should be considered under an individualized approach if requested by the patient or caregiver, acknowledging the importance of patient preference in decision-making. However, it is striking that the agreement reached regarding the appropriateness of the transition to self-administration to inform about the availability of LAGH formulations is moderate, whereas the transition to adulthood is widely considered to be appropriate. In this regard, it should be noted that somapacitan is already indicated for the treatment of GHD in adults, while somatrogon and lonapegsomatropin are currently restricted to pediatric use. Whenever it occurs, it is recommended that IGF-1 levels are monitored similarly as for naïve patients, bearing in mind that deviations greater than 2 SDS may be more frequent after the switch (52).
4.3 Domain 3: considerations for initiating LAGH and treatment monitoring
Regarding considerations prior to initiating treatment, the available evidence supports the fact that, given the different pharmacological characteristics and the lack of long-term experience with these new formulations, LAGH should only be prescribed after the patient and/or their caregivers have been fully informed (53). This is consistent with the panel’s perception, which unanimously agreed on the need to adequately inform the family about the current state of knowledge about LAGH. Similarly, therapeutic education is widely perceived as essential for maximizing the benefits of LAGH therapy. In this regard, the importance of avoiding the erroneous assumption that LAGH does not require injection site rotation due to its lower dosing frequency is emphasized. As stated in the prescribing information for the available formulations, the injection site should be rotated with each administration to avoid the risk of lipodystrophy (54–56). The importance of therapeutic education on other critical aspects, such as the time window for administering a missed dose, is also underscored. This is particularly relevant given that the pharmacokinetics of different LAGH formulations lead to varying timeframes (3 days for somatrogon and somapacitan, and -2/+2 days for lonapegsomatropin) (17). In line with the available evidence, which recognizes the growing interest in involving patients in therapeutic decision-making (39), the panel also acknowledges a high level of consensus on the importance of shared decision-making between physicians, caregivers and patients. However, it should be noted that access to available options may differ between hospitals or regions.
On the other hand, although the starting dose is established by the prescribing information for each product—0.66 mg/kg/week for somatrogon, 0.24 mg/kg/week for lonapegsomatropin and 0.16 mg/kg/week for somapacitan—issues such as dose adjustment during treatment or the management of a suboptimal response remain topics of debate (57). It should be taken into consideration that direct dose comparisons between different formulations, whether between rhGH and LAGH or between available LAGH formulations, are not adequate. In this regard, the panel highly agreed that LAGH dosing during treatment should be individualized based on growth velocity, adverse effects, and serum IGF-1 levels, without exceeding the therapeutic dose approved by the medical agencies. While weight is undoubtedly a factor to consider when determining the initial dose, it does not appear to be as relevant in titration. This suggests that future knowledge may reveal that the dose does not necessarily need to be increased if the patient adequately meets the other criteria at the follow-up visit. However, it is strongly emphasized that its use will always be carried out under the conditions approved by the medical agencies.
Regarding response monitoring, the clinical trials for LAGH included dose adjustments beginning at 3 months and then every 6 months based on efficacy and safety (10–12, 26). However, this statement had a slightly lower consensus, likely reflecting clinical uncertainty about optimal dosing intervals. Furthermore, the frequency of confirming possible deviations in IGF-1 levels above 2 SDS was a topic of discussion, but a moderate consensus was ultimately reached on the proposed statement. It is emphasized that, beyond confirming possible deviations through laboratory results, active investigation should be conducted into whether there is a plausible factor that could explain them. Finally, while the prescribing information for LAGH establish an evaluation of efficacy and safety at 6- to 12-month intervals (54–56), this consensus provides more detailed and agreed-upon follow-up guidelines with a high degree of agreement. Additionally, considering the unique pharmacokinetics of LAGH and the importance of IGF-1 measurement in response monitoring, it is finally agreed that this determination must be performed on day 4 (96 hours) after administration, representing the mean IGF-1 value, ideally through reliable assays, adjusted by pubertal status, sex, race. This differs slightly for lonapegsomatropin, as its monitoring must be performed 108 hours after administration (56, 58). Alternatively, normalization formulae, which can be used to allow adjustments to predict mean IGF-1 and IGF-1 SDS values depending on time after dose, has been created to enable physicians to monitor the treatment (59–61). However, the need to generate more long-term evidence to understand the relationship between estimated peak and estimated average IGF-1 levels at steady state, and its influence on the short- and long-term safety and efficacy of LAGH therapy, is also emphasized.
4.4 Limitations and future work
Although the scope of the panel was limited to Spain, this consensus was strengthened by full panel retention across rounds and representation from experienced pediatric endocrinologists from across the country. By combining expert clinical assessment and a targeted literature review, the process yielded practical recommendations to guide national implementation, while remaining adaptable to the evolving international landscape. Although the panel did not include patients or caregivers, literature on patient preferences and treatment burden informed related recommendations, and future updates should incorporate direct patient input where feasible.
Future work should focus on validating these recommendations in real-world settings, particularly regarding adherence, patient-reported outcomes, pharmacoeconomics and cost-effectiveness, the effect on other parameters such as body composition, and safety in underrepresented groups. Continued efforts to harmonize IGF-1 monitoring protocols, refine dose optimization strategies, and generate clinical experience will be essential for the consistent use of LAGH across diverse clinical settings.
5 Conclusion
This is the first Delphi consensus that provides expert-based recommendations for the use of long-acting growth hormone (LAGH) in pediatric growth hormone deficiency, based on current evidence and clinical use in Spain. Most statements reached a strong agreement, while areas of uncertainty, mainly related to IGF-1 monitoring and dose adjustment, suggest an evolving clinical practice. The recommendations offer practical guidance for identifying patients who are most likely to benefit from LAGH, particularly those with adherence challenges. Future long-term real-world experience will help to address questions regarding long-term efficacy and safety and practice-related points such as indication and monitoring. Recommendations are intended to be used to support national implementation while remaining adaptable to future international guidelines.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Author contributions
LC-F: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. J-IL-A: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. MR-K: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. DP: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. DY: Methodology, Supervision, Validation, Writing – review & editing. IG: Methodology, Supervision, Validation, Writing – review & editing.
The ConverGHe Working Group
Consorcio Hospital General Universitario de Valencia (Alcón Saez JJ), Clínica Universidad de Navarra (Alija Merillas MJ), Hospital Materno Infantil de Badajoz (Arroyo Díez FJ), Hospital Clínico Universitario de Valladolid (Bahíllo Curieses MP), Hospital Universitario Marqués de Valdecilla (Bertholt Zuber ML), Hospital Clínico Universitario Lozano Blesa (Bueno Lozano G), Hospital Clínico Universitario de Santiago de Compostela (Cabanas Rodríguez P, Castro-Feijóo L), Hospital Universitario Sant Joan de Déu (Casano Sancho P, Ramon-Krauel M), Hospital Universitario de Navarra (Chueca Guindulain MJ), Hospital Universitario Parc Taulí (Corripio Collado R), Hospital Universitario Materno Infantil Miguel Servet (de Arriba Muñoz A, Labarta-Aizpún JI), Hospital Universitario Son Espases (de Sotto-Esteban D), Osi ARABA- Hospital Universitario de ARABA, Universidad del País Vasco UPV-EHU (Díez López I), Hospital Clínico Universitario Virgen de la Arrixaca (Escribano Muñoz MA, Martos Tellos JM), Hospital Universitario de Basurto (Fernández Ramos MC), Hospital Universitario Virgen del Rocío (Gómez Gila AL), Hospital Universitario La Paz (González Casado I), Instituto de Investigación e Innovación Biomédica de Cádiz (INiBICA), Facultad de Medicina, Universidad de Cádiz, Hospital Universitario Puerta del Mar (Lechuga Sancho AM), Hospital Universitari Doctor Josep Trueta (López Bermejo A), Hospital Universitari Politècnic la Fe de Valencia (Moreno Macián MF), Pfizer S.L.U. Spain (Primiano D), Hospital Universitario Materno Infantil de Gran Canaria (Quinteiro González S), Hospital Álvaro Cunqueiro (Rey Cordo L), Hospital Universitario Central de Asturias (Riaño Galán I), Hospital Universitario Cruces (Rica Echevarría I), Hospital Universitario Gregorio Marañón (Rodríguez Sánchez A), Hospital Universitari Vall d'Hebron (Yeste Fernández D).
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was sponsored by Pfizer S.L.U. Spain.
Acknowledgments
The authors gratefully acknowledge Pfizer S.L.U. Spain for their logistical and financial support during the preparation of this document, the medical writing services provided by María Guerra (VML Health Spain) and the statistical support provided by Juan José de la Cruz (Universidad Autónoma de Madrid).
Conflict of interest
LC-F received advisory board fees from Pfizer and Novo Nordisk and speaker fees from Pfizer, Novo Nordisk, Merck and Sandoz. J-IL-A received advisory board fees from Pfizer and Novo Nordisk and speaker fees from Pfizer, Novo Nordisk, Merck and Sandoz. MR-K received advisory board fees from Merck, Novo Nordisk, Palobiofarma, Pfizer, Sandoz, Sanofi and speaker fees from Novo Nordisk, Pfizer, Rhythm and Sandoz. DP is a full-time employee of Pfizer S.L.U. and holds stock and stock options in Pfizer Inc. DY received advisory board fees from Pfizer and Merck and speaker fees from Pfizer and Merck.
The remaining author declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1718161/full#supplementary-material
References
1. Hage C, Gan HW, Ibba A, Patti G, Dattani M, Loche S, et al. Advances in differential diagnosis and management of growth hormone deficiency in children. Nat Rev Endocrinol. (2021) 17:608–24. doi: 10.1038/s41574-021-00539-5, PMID: 34417587
2. Alatzoglou KS, Webb EA, Le Tissier P, and Dattani MT. Isolated growth hormone deficiency (GHD) in childhood and adolescence: recent advances. Endocr Rev. (2014) 35:376–432. doi: 10.1210/er.2013-1067, PMID: 24450934
3. Ranke MB. Short and long-term effects of growth hormone in children and adolescents with GH deficiency. Front Endocrinol (Lausanne). (2021) 12:720419. doi: 10.3389/fendo.2021.720419, PMID: 34539573
4. Castro-Feijóo L, Cabanas P, Tejera R, Iglesias JM, and del acción GH. Long-acting growth hormone. Rev Española Endocrinología Pediátrica. (2024) 15:47–56. doi: 10.3266/RevEspEndocrinolPediatr.pre2024.Apr.896
5. Maghnie M, Ranke MB, Geffner ME, Vlachopapadopoulou E, Ibáñez L, Carlsson M, et al. Safety and efficacy of pediatric growth hormone therapy: results from the full KIGS cohort. J Clin Endocrinol Metab. (2022) 107:3287–301. doi: 10.1210/clinem/dgac517, PMID: 36102184
6. Cutfield WS, Derraik JG, Gunn AJ, Reid K, Delany T, Robinson E, et al. Non-compliance with growth hormone treatment in children is common and impairs linear growth. PloS One. (2011) 6:e16223. doi: 10.1371/journal.pone.0016223, PMID: 21305004
7. Graham S, Weinman J, and Auyeung V. Identifying potentially modifiable factors associated with treatment non-adherence in paediatric growth hormone deficiency: A systematic review. Horm Res Paediatr. (2018) 90:221–7. doi: 10.1159/000493211, PMID: 30522126
8. Koledova E, Stoyanov G, Ovbude L, and Davies PSW. Adherence and long-term growth outcomes: results from the easypod(™) connect observational study (ECOS) in paediatric patients with growth disorders. Endocr Connect. (2018) 7:914–23. doi: 10.1530/ec-18-0172, PMID: 29976785
9. Auer MK, Stieg MR, Hoffmann J, and Stalla GK. Is insulin-like growth factor-I a good marker for treatment adherence in growth hormone deficiency in adulthood? Clin Endocrinol (Oxf). (2016) 84:862–9. doi: 10.1111/cen.13030, PMID: 26824335
10. Deal CL, Steelman J, Vlachopapadopoulou E, Stawerska R, Silverman LA, Phillip M, et al. Efficacy and safety of weekly somatrogon vs daily somatropin in children with growth hormone deficiency: A phase 3 study. J Clin Endocrinol Metab. (2022) 107:e2717–e28. doi: 10.1210/clinem/dgac220, PMID: 35405011
11. Thornton PS, Maniatis AK, Aghajanova E, Chertok E, Vlachopapadopoulou E, Lin Z, et al. Weekly lonapegsomatropin in treatment-naïve children with growth hormone deficiency: the phase 3 heiGHt trial. J Clin Endocrinol Metab. (2021) 106:3184–95. doi: 10.1210/clinem/dgab529, PMID: 34272849
12. Miller BS, Blair JC, Rasmussen MH, Maniatis A, Kildemoes RJ, Mori J, et al. Weekly somapacitan is effective and well tolerated in children with GH deficiency: the randomized phase 3 REAL4 trial. J Clin Endocrinol Metab. (2022) 107:3378–88. doi: 10.1210/clinem/dgac513, PMID: 36062966
13. Miller BS, Velazquez E, and Yuen KCJ. Long-acting growth hormone preparations - current status and future considerations. J Clin Endocrinol Metab. (2020) 105:e2121–33. doi: 10.1210/clinem/dgz149, PMID: 31676901
14. Rojo Portolés MP, Carvaquilla Urquí A, Patón García-Donas MC, and Aragonés Gallego A. Hormona de crecimiento: indicaciones y utilidad clínica. Form Act Pediatr Aten Prim. (2015) 8:127–34. Available online at: https://fapap.es/files/639-1273-RUTA/04_FAPAP_3_2015_Hormona_crecimiento.pdf (Accessed September 30, 2025)
15. Grillo MS, Frank J, and Saenger P. Long acting growth hormone (LAGH), an update. Front Pediatr. (2023) 11:1254231. doi: 10.3389/fped.2023.1254231, PMID: 37842029
16. Pampanini V, Deodati A, Inzaghi E, and Cianfarani S. Long-acting growth hormone preparations and their use in children with growth hormone deficiency. Horm Res Paediatr. (2023) 96:553–9. doi: 10.1159/000523791, PMID: 35220308
17. Maniatis A, Cutfield W, Dattani M, Deal C, Collett-Solberg PF, Horikawa R, et al. Long-acting growth hormone therapy in pediatric growth hormone deficiency: A consensus statement. J Clin Endocrinol Metab. (2025) 110:e1232–e40. doi: 10.1210/clinem/dgae834, PMID: 39672599
18. McMillan SS, King M, and Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharm. (2016) 38:655–62. doi: 10.1007/s11096-016-0257-x, PMID: 26846316
19. George DM and Mallery P. SPSS for Windows step by step: A simple guide and reference. 4th edition. Boston, MA: Allyn & Bacon (2003).
20. Martínez Ortega RM, Tuya Pendás LC, Martínez Ortega M, Pérez Abreu A, and Cánovas AM. El coeficiente de correlación de los rangos de Spearman caracterización. Rev Haban Cienc Med. (2009) 8. Available online at: http://scielo.sld.cu/scielo.php?script=sci_isoref&pid=S1729-519X2009000200017&lng=es&tlng=es (Accessed September 30, 2025)
21. Linglart A, Coutant R, Polak M, and Nicolino M. Long-acting growth hormone in the management of GHD in France. Arch Pediatr. (2024) 31:357–64. doi: 10.1016/j.arcped.2024.03.009, PMID: 39030125
22. Mameli C, Orso M, Calcaterra V, Wasniewska MG, Aversa T, Granato S, et al. Efficacy, safety, quality of life, adherence and cost-effectiveness of long-acting growth hormone replacement therapy compared to daily growth hormone in children with growth hormone deficiency: A systematic review and meta-analysis. Pharmacol Res. (2023) 193:106805. doi: 10.1016/j.phrs.2023.106805, PMID: 37236413
23. de Fries Jensen L, Antavalis V, Odgaard-Jensen J, Rossi A, Pietropoli A, and Højby M. Efficacy and safety of somapacitan relative to somatrogon and lonapegsomatropin in pediatric growth hormone deficiency: systematic literature review and network meta-analysis. Adv Ther. (2024) 41:4098–124. doi: 10.1007/s12325-024-02966-y, PMID: 39261416
24. Yang Y, Bai X, Yuan X, Zhang Y, Chen S, Yang H, et al. Efficacy and safety of long-acting growth hormone in children with short stature: a systematic review and meta-analysis. Endocrine. (2019) 65:25–34. doi: 10.1007/s12020-019-01950-9, PMID: 31119649
25. Tsurayya G, Nazhifah CA, Pirwanja MR, Zulfa PO, Tatroman MRR, Fakri F, et al. Once-weekly somapacitan as an alternative management of growth hormone deficiency in prepubertal children: A systematic review and meta-analysis of randomized controlled trial. Children (Basel). (2024) 11(2):227. doi: 10.3390/children11020227, PMID: 38397339
26. Zadik Z, Zelinska N, Iotova V, Skorodok Y, Malievsky O, Mauras N, et al. An open-label extension of a phase 2 dose-finding study of once-weekly somatrogon vs. once-daily Genotropin in children with short stature due to growth hormone deficiency: results following 5 years of treatment. J Pediatr Endocrinol Metab. (2023) 36:261–9. doi: 10.1515/jpem-2022-0359, PMID: 36732285
27. Horikawa R, Tanaka T, Hasegawa Y, Yorifuji T, Ng D, Rosenfeld RG, et al. Efficacy and safety of once-weekly somatrogon compared with once-daily somatropin (Genotropin®) in Japanese children with pediatric growth hormone deficiency: results from a randomized phase 3 study. Horm Res Paediatr. (2022) 95:275–85. doi: 10.1159/000524600, PMID: 35417909
28. Sävendahl L, Battelino T, Brod M, Højby Rasmussen M, Horikawa R, Juul RV, et al. Once-weekly somapacitan vs daily GH in children with GH deficiency: results from a randomized phase 2 trial. J Clin Endocrinol Metab. (2020) 105:e1847–61. doi: 10.1210/clinem/dgz310, PMID: 31917835
29. Sävendahl L, Battelino T, Højby Rasmussen M, Brod M, Saenger P, and Horikawa R. Effective GH replacement with once-weekly somapacitan vs daily GH in children with GHD: 3-year results from REAL 3. J Clin Endocrinol Metab. (2022) 107:1357–67. doi: 10.1210/clinem/dgab928, PMID: 34964458
30. Zadik Z, Zelinska N, Iotova V, Skorodok Y, Malievskiy OA, Mauras N, et al. OR21–04 long-term efficacy and safety of once-weekly somatrogon in pediatric. J Endocr Soc. (2023) 7:bvad114.1522. doi: 10.1210/jendso/bvad114.1522
31. Çetinkaya S, Eren E, Erdoğan F, and Darendeliler F. Rationale for long-acting growth hormone therapy and future aspects. J Clin Res Pediatr Endocrinol. (2025) 17:1–8. doi: 10.4274/jcrpe.galenos.2024.2023-11-8, PMID: 38488050
32. Chen SC, Bryce J, Chen M, Charmandari E, Choi JH, Dou X, et al. Development of a minimum dataset for the monitoring of recombinant human growth hormone therapy in children with growth hormone deficiency: A gloBE-reg initiative. Horm Res Paediatr. (2024) 97:365–73. doi: 10.1159/000533763, PMID: 37703843
33. Zdravkovic V, Vorgucin I, Stankovic S, Milenkovic T, Cvetkovic Z, Koledova E, et al. Real-world data on growth hormone therapy adherence using a connected injection device and catch-up growth in children with growth disorders in Serbia. Horm Res Paediatr. (2024) 97(suppl 3):1–737. P2–150. doi: 10.1159/000541189
34. Kotnik P, Murn Berkopec B, Morrow LM, and Battelino T. Healthcare professional (HCP) perceptions towards Mallya® Connectivity Cap & App for long-acting growth hormone: results from a Slovenia Participatory Study. Horm Res Paediatr (2024) 97(suppl 3):1–737. P2–158. doi: 10.1159/000541189
35. Loftus J, Quitmann J, and Valluri SR. Health-related quality of life in pre-pubertal children with pediatric growth hormone deficiency: 12-month results from a phase 3 clinical trial of once-weekly somatrogon versus once-daily somatropin. Curr Med Res Opin. (2024) 40:175–84. doi: 10.1080/03007995.2023.2290623, PMID: 38053515
36. Mori J, Ohata Y, Fujisawa Y, Sato Y, Röhrich S, Rasmussen MH, et al. Effective growth hormone replacement with once-weekly somapacitan in Japanese children with growth hormone deficiency: Results from REAL4, a phase 3 clinical trial. Clin Endocrinol (Oxf). (2024) 100:389–98. doi: 10.1111/cen.15025, PMID: 38368603
37. Maniatis AK, Carakushansky M, Galcheva S, Prakasam G, Fox LA, Dankovcikova A, et al. Treatment burden of weekly somatrogon vs daily somatropin in children with growth hormone deficiency: A randomized study. J Endocr Soc. (2022) 6:bvac117. doi: 10.1210/jendso/bvac117, PMID: 36101713
38. Miller BS, Blair JC, Rasmussen MH, Maniatis A, Mori J, Böttcher V, et al. Effective GH replacement with somapacitan in children with GHD: REAL4 2-year results and after switch from daily GH. J Clin Endocrinol Metab. (2023) 108:3090–9. doi: 10.1210/clinem/dgad394, PMID: 37406251
39. McNamara M, Turner-Bowker DM, Westhead H, Yaworsky A, Palladino A, Gross H, et al. Factors driving patient preferences for growth hormone deficiency (GHD) injection regimen and injection device features: A discrete choice experiment. Patient Prefer Adherence. (2020) 14:781–93. doi: 10.2147/ppa.S239196, PMID: 32431492
40. Fisher DM, Rosenfeld RG, Jaron-Mendelson M, Amitzi L, Koren R, and Hart G. Pharmacokinetic and pharmacodynamic modeling of MOD-4023, a long-acting human growth hormone, in growth hormone deficiency children. Horm Res Paediatr. (2017) 87:324–32. doi: 10.1159/000470842, PMID: 28399519
41. Rosenfeld RG and Bakker B. Compliance and persistence in pediatric and adult patients receiving growth hormone therapy. Endocr Pract. (2008) 14:143–54. doi: 10.4158/ep.14.2.143, PMID: 18308651
42. Hartmann K, Ittner J, Müller-Rossberg E, Schönau E, Stephan R, Ullrich KP, et al. Growth hormone treatment adherence in prepubertal and pubertal children with different growth disorders. Horm Res Paediatr. (2013) 80:1–5. doi: 10.1159/000351800, PMID: 23860437
43. Lass N and Reinehr T. Low treatment adherence in pubertal children treated with thyroxin or growth hormone. Horm Res Paediatr. (2015) 84:240–7. doi: 10.1159/000437305, PMID: 26279278
44. Gomez R, Ahmed SF, Maghnie M, Li D, Tanaka T, and Miller BS. Treatment Adherence to Injecta ble Treatments in Pediatric Growth Hormone Deficiency Compared With Injecta ble Treatments in Other Chronic Pediatric Conditions: A Systematic Literature Review. Front Endocrinol (Lausanne). (2022) 13:795224. doi: 10.3389/fendo.2022.795224, PMID: 35299969
45. Mohseni S, Heydari Z, Qorbani M, and Radfar M. Adherence to growth hormone therapy in children and its potential barriers. J Pediatr Endocrinol Metab. (2018) 31:13–20. doi: 10.1515/jpem-2017-0157, PMID: 29216008
46. Fisher BG and Acerini CL. Understanding the growth hormone therapy adherence paradigm: a systematic review. Horm Res Paediatr. (2013) 79:189–96. doi: 10.1159/000350251, PMID: 23635797
47. Aydın BK, Aycan Z, Sıklar Z, Berberoğlu M, Ocal G, Cetinkaya S, et al. Adherence to growth hormone therapy: results of a multicenter study. Endocr Pract. (2014) 20:46–51. doi: 10.4158/ep13194.or, PMID: 24013997
48. Acerini CL, Segal D, Criseno S, Takasawa K, Nedjatian N, Röhrich S, et al. Shared decision-making in growth hormone therapy-implications for patient care. Front Endocrinol (Lausanne). (2018) 9:688. doi: 10.3389/fendo.2018.00688, PMID: 30524377
49. Allen DB, Backeljauw P, Bidlingmaier M, Biller BM, Boguszewski M, Burman P, et al. GH safety workshop position paper: a critical appraisal of recombinant human GH therapy in children and adults. Eur J Endocrinol. (2016) 174:P1–9. doi: 10.1530/eje-15-0873, PMID: 26563978
50. Boguszewski MCS, Boguszewski CL, Chemaitilly W, Cohen LE, Gebauer J, Higham C, et al. Safety of growth hormone replacement in survivors of cancer and intracranial and pituitary tumours: a consensus statement. Eur J Endocrinol. (2022) 186:P35–p52. doi: 10.1530/eje-21-1186, PMID: 35319491
51. Tidblad A, Bottai M, Smedby KE, Albertsson-Wikland K, and Sävendahl L. Long-term risk of neoplastic events after childhood growth hormone treatment: a population-based cohort study in Sweden. Front Endocrinol (Lausanne). (2024) 15:1360139. doi: 10.3389/fendo.2024.1360139, PMID: 38505755
52. Coyne E, Muthuvel G, and Gutmark-Little I. Clinical outcomes of switching to lonapegsomatropin from somatropin for treatment of pediatric growth hormone deficiency. J Pediatr Endocrinol Metab. (2025) 38:248–53. doi: 10.1515/jpem-2024-0496, PMID: 39843388
53. Woelfle J, Schnabel D, and Binder G. The treatment of growth disorders in childhood and adolescence. Dtsch Arztebl Int. (2024) 121:96–106. doi: 10.3238/arztebl.m2023.0247, PMID: 38051162
54. European Medicines Agency (EMA). Summary of product characteristics for NGENLA® (Pfizer/OPKO) (2022). Available online at: https://www.ema.europa.eu/en/documents/product-information/ngenla-epar-product-information_en.pdf (Accessed September 30, 2025).
55. European Medicines Agency (EMA). Summary of product characteristics for Sogroya® (Novo Nordisk) (2021). Available online at: https://www.ema.europa.eu/en/documents/product-information/sogroya-epar-product-information_en.pdf (Accessed September 30, 2025).
56. European Medicines Agency (EMA). Summary of product characteristics for Skytrofa® (Ascendis Pharma) (2022). Available online at: https://www.ema.europa.eu/en/documents/product-information/skytrofa-epar-product-information_en.pdf (Accessed September 30, 2025).
57. Collett-Solberg PF, Ambler G, Backeljauw PF, Bidlingmaier M, Biller BMK, Boguszewski MCS, et al. Diagnosis, genetics, and therapy of short stature in children: A growth hormone research society international perspective. Horm Res Paediatr. (2019) 92:1–14. doi: 10.1159/000502231, PMID: 31514194
58. Clemmons DR. Consensus statement on the standardization and evaluation of growth hormone and insulin-like growth factor assays. Clin Chem. (2011) 57:555–9. doi: 10.1373/clinchem.2010.150631, PMID: 21285256
59. Kildemoes RJ, Backeljauw PF, Højby M, Blair JC, Miller BS, Mori J, et al. Model-based analysis of IGF-I response, dosing, and monitoring for once-weekly somapacitan in children with GH deficiency. J Endocr Soc. (2023) 7:bvad115. doi: 10.1210/jendso/bvad115, PMID: 37818403
60. Miller BS and Yuen KCJ. Spotlight on lonapegsomatropin once-weekly injection and its potential in the treatment of growth hormone deficiency in pediatric patients. Drug Des Devel Ther. (2022) 16:2055–66. doi: 10.2147/dddt.s336285, PMID: 35791404
Keywords: long-acting growth hormone, pediatric growth hormone deficiency, recombinant human growth hormone, Delphi consensus, children
Citation: Castro-Feijóo L, Labarta-Aizpún J-I, Ramon-Krauel M, Primiano D, Yeste Fernández D and González Casado I (2025) Delphi-based Spanish consensus on the use of long-acting growth hormone in pediatric growth hormone deficiency: recommendations from the ConverGHe Working Group. Front. Endocrinol. 16:1718161. doi: 10.3389/fendo.2025.1718161
Received: 03 October 2025; Accepted: 11 November 2025; Revised: 07 November 2025;
Published: 04 December 2025.
Edited by:
Sandro Loche, Bambino Gesù Children’s Hospital (IRCCS), ItalyReviewed by:
Stefano Zucchini, IRCCS University Hospital of Bologna Sant Orsola Polyclinic, ItalyAbdullah Alherbish, Alhabib Medical Group, Saudi Arabia
Copyright © 2025 Castro-Feijóo, Labarta-Aizpún, Ramon-Krauel, Primiano, Yeste Fernández and González Casado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lidia Castro-Feijóo, bGlkaWEuY2FzdHJvLmZlaWpvb0BzZXJnYXMuZXM=; José-Ignacio Labarta-Aizpún, amlsYWJhcnRhQHNhbHVkLmFyYWdvbi5lcw==; Marta Ramon-Krauel, bWFydGEucmFtb25Ac2pkLmVz
†These authors have contributed equally to this work and share first authorship