 Musawa Mukupa1*
Musawa Mukupa1* Cosmas Zyambo2
Cosmas Zyambo2 Masauso Moses Phiri1,3
Masauso Moses Phiri1,3 Richard Zulu1Tulani Francis L. Matenga4Kumbulani Mabanti2Anna Hainze5Ahmed Ogwell6
Richard Zulu1Tulani Francis L. Matenga4Kumbulani Mabanti2Anna Hainze5Ahmed Ogwell6 William DeJong7
William DeJong7 Dhally M. Menda8
Dhally M. Menda8 Angela Rizzo9Fastone Goma1
Angela Rizzo9Fastone Goma1 Tom Achoki9,10
Tom Achoki9,10
- 1Centre for Primary Care Research, Lusaka, Zambia
- 2Department of Community and Family Medicine, School of Public Health, University of Zambia, Lusaka, Zambia
- 3Department of Pathology and Microbiology, School of Medicine, University of Zambia, Lusaka, Zambia
- 4Department of Health Promotion and Education, School of Public Health, University of Zambia, Lusaka, Zambia
- 5Brands on a Mission, Nairobi, Kenya
- 6United Nations Foundation, Washington, DC, United States
- 7Department of Public Health and Community Medicine, Tufts University, Medical School, Boston, MA, United States
- 8Churches Health Association of Zambia, Lusaka, Zambia
- 9AB InBev Foundation, New York, NY, United States
- 10African Institute for Health Policy, Nairobi, Kenya
Introduction: Illicit alcohol, existing outside legal frameworks, lacks safety standards and may contain harmful substances. In Africa, the illicit alcohol market is pervasive, contributing to significant public health challenges. The state in Zambia may not be so different where abuse of alcohol was associated to unintended injuries, suicidal ideation and physical fights that in some cases lead to death. This mirrors these challenges; according to the Zambia Stepwise Survey for Non-Communicable Diseases (NCDs) Risk Factors (2017), 21.7% of adults consume alcohol, with urban areas experiencing higher rates of illicit production.
Aim: The study aimed to assess the public health risk implications associated with the production and retail of illicit alcohol based on the hygiene and sanitation of these premises. A quantitative approach was employed in Livingstone, Lusaka, and Ndola.
Methods: We employed a quantitative approach was conducted in Livingstone, Lusaka, and Ndola. A hygiene and sanitation observation tool obtained from the Lusaka City Council was adapted and utilized to evaluate the conditions of these premises.
Results: The study found that Livingstone exhibited the highest rate of unavailability of water supply at illicit alcohol production sites, with 18% lacking access to water, while Lusaka had 13% without water supply of the zones selected, all sites in Ndola had water supply.
Conclusion: Given the growing trend of consuming illicit alcohol in such unsanitary environments, urgent interventions are warranted. The study recommends the implementation of enforcement of regulations, including regular inspections and enhanced enforcement mechanisms, to ensure hygienic and sanitary production practices.
1 Introduction
Alcohol consumption is a prevalent cultural practice, but its excessive use poses significant public health concerns globally with heavy episodic alcohol use affecting most adults and is the third leading cause of death (1–3). According to the WHO, in 2022, harmful use of alcohol accounted for more than 3 million deaths, making up 5.3% of all deaths globally (4). In Africa, the illicit alcohol market is pervasive, contributing to significant public health challenges. A study conducted in Nigeria revealed a significant disparity between producers' knowledge and their actual hygiene practices, with a majority displaying poor practice levels (5). The state in Zambia may not be so different where abuse of alcohol was associated to unintended injuries, suicidal ideation and physical fights that in some cases lead to death (6). This mirrors these challenges; according to the Zambia Stepwise Survey for Non-Communicable Diseases (NCDs) Risk Factors (2017), 21.7% of adults consume alcohol (7, 8), with urban areas experiencing higher rates of illicit production. The burden of age-standardized alcohol-attributable disease and injury was highest in the WHO African region, of which Zambia is a part (9).
The Zambia Stepwise Survey for Non-Communicable Diseases (NCDs) Risk Factors (2017) found that 21.7% of respondents were current alcohol drinkers, with significant gender differences (32.0% for men compared to 11.8% for women) (7). These may be prone to suicidal ideation, involved in fights and also be involved in road accidents (6, 10). The prevalence of current drinkers was highest among men aged 30–44 years (37.8%) and women aged 60–69 years (15.3%) (7). Urban women reported a significantly higher percentage of current drinkers (15.7%) than rural women (7.8%) (7). Additionally, the Zambia Global School Health Survey 2004 revealed that 42.6% of students in grades 7–10 across 47 schools in 9 provinces had consumed alcohol on one or more occasions in the last 30 days (11). This statistic poses a significant risk to children, as early exposure to alcohol can lead to a range of adverse health outcomes and behavioral issues. The consumption of alcohol at such a young age is associated with an increased likelihood of developing alcohol use disorders later in life, as well as heightened vulnerability to engaging in risky behaviors, including unprotected sex and substance abuse (12–14).
Safety and hygiene are crucial in alcohol production. The alcohol industry ideally adheres to Good Manufacturing Practice (GMP) standards. However, observations at illicit production sites reveal non-compliance with GMP guidelines (15). Illicit alcohol production typically occurs in informal settings characterized by low-income families, where hygiene and sanitation standards are often substandard or nonexistent (16–18). Common practices include the use of contaminated water sources, inadequate cleaning of equipment, and improper storage of raw materials. These practices create an environment conducive to microbial contamination, including bacteria, fungi, and molds, which can proliferate throughout the production process and contaminate the final product (18, 19).
The Zambia cholera outbreak of the 2023/24 rainy season showed Lusaka to be a major cholera hotspot and prompted recommendations to strengthen interventions such as area-targeted interventions (CATI). A report authored by the Africa Centres for Disease Control and Prevention (Africa CDC) further suggested improving water, sanitation, and hygiene interventions, recommending quality monitoring, disinfection, and inspections. The Africa CDC press release also confirmed that the Zambian cholera outbreak in October 2023 was first detected in Matero and Kanyama, areas known for illicit alcohol production and retail, although no studies have directly linked the outbreak with these activities (20).
The existing body of research on sanitation and hygiene often overlooks the critical intersection between public health and illicit alcohol production and retail. This knowledge gap represents a significant deficiency in understanding the public health risks associated with this industry. By bridging this divide, our study aims to illuminate the relationship between sanitation, hygiene, and public health risks in illicit alcohol production and retail. Through comprehensive investigation and analysis, this paper seeks to provide crucial insights to inform targeted interventions, policies, and public health strategies to mitigate adverse effects on individuals and communities. Addressing this research gap is imperative to safeguard public health and promote sustainable development in the context of illicit alcohol production and retail.
This study aims to bridge the gap between global knowledge and the realities in Zambia by examining hygiene and sanitation practices in illicit alcohol production in Zambia. The results from this study will inform targeted interventions that can mitigate public health risks associated with this pervasive issue.
2 Methodology
2.1 Study design and sites
The study employed a quantitative approach and was conducted in three urban and peri-urban areas in Zambia: Livingstone, Lusaka, and Ndola. The study was conducted between June and December, 2023. The selection of these study sites was purposeful. Lusaka, the capital city of Zambia, and Ndola located in the Copper Belt region, were chosen due to their reported high consumption of illicit alcohol, attributed to undeclared (tax leakage) production of alcohol and smuggling. Livingstone was also purposefully sampled as a border city that shares a border with Namibia, Botswana, and Zimbabwe. Despite the choice of sites being justified based on the known high-risk areas for illicit alcohol production and consumption in Zambia, the potential limitation is the focus on urban and peri-urban areas. This may lead to the findings not being generalized to rural settings where alcohol production and consumption dynamics might differ.
2.2 Study setting
In Lusaka, we selected the following Zones or areas: COMESA market, Matero, Kanyama, and Mtendere. Kamanga, Bauleni, and Chibolya were purposefully chosen due to their reputation as hotspots for home-produced alcohols used for commercial purposes. In Ndola, we selected the main market areas: Main Masala, Chifubu, and Kaloko. Lastly, in Livingstone, we selected Town Centre (Zimbabwe market), Maramba, Linda, Libuyu, and Dambwa. We included all retailers within a 1 km radius who willingly consented to participate in the study. The data collection phase was time-bound and limited to one month.
2.3 Data collection
This study aimed to assess public health risk implications based on factors such as hygiene and sanitation in the production and retail of illicit alcohol. This was done by observation of the environment or surroundings of the place where the illicit alcohol is being distilled or sold. A hygiene and sanitation tool were adapted from the local city council to measure and ascertain levels of hygiene. The variables included presence of iron drums, solid waste management, water availability, toilets, and infestations. These variables were adapted from the local council tool because they are defined as key indicators of environmental health and sanitation by the local council, which directly impact the safety and quality of alcohol production. For example, the use of iron drums, especially if rusted or previously used for hazardous materials, poses a significant risk of chemical contamination i.e iron poisoning. Similarly, the availability of clean water and proper waste management reduces the likelihood of biological contamination, while the presence of toilets and pest infestations reflects the overall hygiene standards of the production environment, all of which are critical to public health risk.
The target study sites were places where illicit alcohol was produced and sold and where bulk opaque beers were served in barrels in the selected areas of Livingstone, Lusaka, and Ndola. The type of drums, the presence of water supply, and toilets were assessed using the checklist. Within the time-bound one-month limit of data collection fieldwork, 207 producers were recruited for the study.
We used experienced research assistants whom we trained for a period of four days, with the data collection tools pre-tested and refined on Day 5. Before fieldwork, a pre-study exercise of mapping the health zones in each city was undertaken to determine the number of alcohol producers and retailers to be reached in the main study. Data were primarily collected utilizing phone tablets with Open Data Collect (ODK). The socio-demographic collected included age, gender, education and marital status.
2.4 Statistical analysis
Statistical analyses were performed using STATA version 17. Descriptive statistics were calculated for all variables, including means, standard deviations, and frequencies. To evaluate hygiene standards among producers and retailers, we employed the chi-squared test to determine statistically significant differences in hygiene scores across different cities. A significance level of p < 0.05 was established, indicating that results with p-values below this threshold were considered statistically significant.
2.5 Data management
Data on hygiene and sanitation conditions were collected through structured questionnaires administered to the owners or managers of illicit alcohol premises. The questionnaire captured information on the cleanliness of production areas, availability of sanitation facilities, and safety measures to prevent contamination. Data were collected in Livingstone, Lusaka, and Ndola, and entered into statistical software following rigorous quality control procedures to ensure accuracy.
2.6 Ethical consideration
All potential participants were informed about the study and provided written consent before data collection. Data collection procedures were designed to avoid disrupting the normal flow of business. Interviewers were instructed to proceed with the observations only when the retailer/producer was not actively dealing with customers or in their immediate vicinity. Ethical approval for the study was obtained from the University of Zambia Biomedical Research Ethics Committee (UNZABREC REF. No. 4272-2023). Permission to conduct the study was sought from the National Health Research Authority (NHRA).
3 Results
3.1 Sociodemographic characteristics of participants
Based on Table 1, the participants were predominantly female across all three geographical areas (Livingstone, Lusaka, and Ndola). The female representation ranged from 84% to 93%, while males comprised 6% to 16%. The producers and retailers spanned various age groups. The largest group, at 20% to 38%, fell within the 36–45-year-old range, followed by 46–59-year-olds at 30% to 41%. 18–25year-olds constituted the smallest age group, ranging from 7% to 14%. In terms of education, a significant portion (40% to 56%) of the participants had primary school education (G1-G7). Those with no formal schooling ranged from 6% to 17%. Higher education levels were less common, with college/university degrees ranging from 3% to 4% and high school education (G10-12) at 7% to 23%. Regarding marital status, most producers and retailers (45%) were married, with city-specific variations ranging from 39% to 48%. The second largest group consisted of widowed individuals, representing 24% in Ndola, 26% in Lusaka, and 33% in Livingstone. As expected, most participants (ranging from 90% to 100%, with an average of 95%) were self-employed.
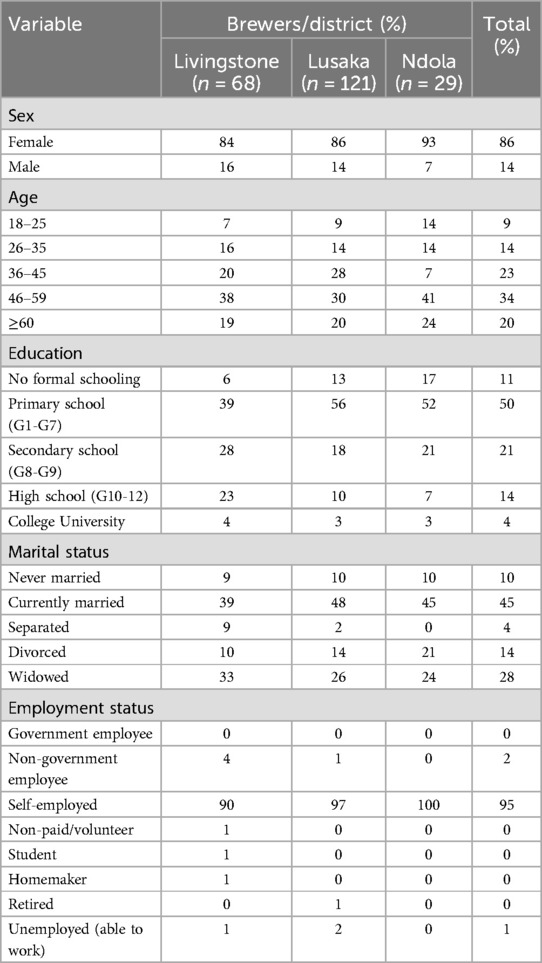
Table 1. Sociodemographic characteristics of retailers and producers.
3.2 Hygiene and sanitation of the premises
The data from 207 producers across Livingstone, Lusaka, and Ndola indicates significant public health risks associated with the production of illicit alcohol (Figure 1). Some key findings focus on improper storage containers: a high proportion (88%) of producers rely on plastic drums for storage, which can be susceptible to leaching chemicals or harboring bacteria if not properly cleaned and maintained. There was also the presence of dirty equipment, with more than half (60%) of producers found using dirty drums, further increasing the risk of contamination in the end product. We also found limited sanitation facilities, where a significant number of producers (68% in Luska, 10% in Livingstone) lack toilets, raising concerns about overall hygiene practices and potential fecal contamination. Solid waste mismanagement is evident, as only 26% of the production sites have proper management of solid waste, suggesting potential breeding grounds for pests and pathogens. While not the most prevalent concern, 13% of producers reported inadequate water supply, which could hinder proper cleaning and sanitation during production. A concerningly high proportion (58%) of producers reported infestations, which could contaminate ingredients or equipment and pose health risks to consumers.
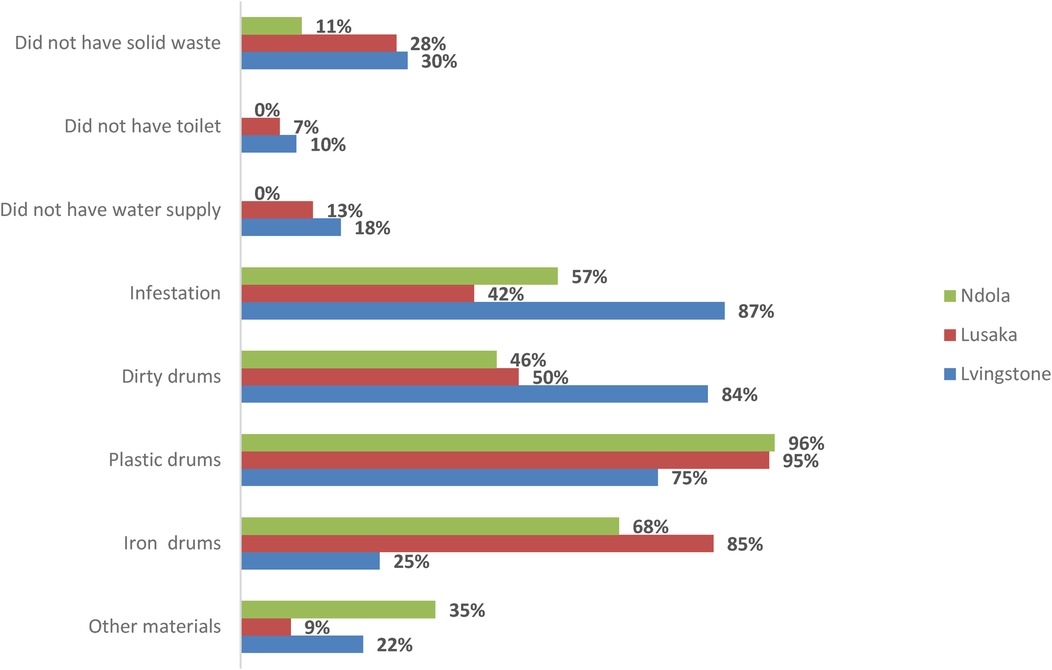
Figure 1. Hygiene and sanitation of the producers in production of illicit alcohol.
These findings highlight the potential public health hazards associated with consuming illicit alcohol in Zambia. The use of improper containers, dirty equipment, and a lack of sanitation facilities significantly increases the risk of contamination by bacteria, parasites, or other harmful pathogens. Additionally, inadequate water supply and infestations further exacerbate these risks.
3.3 Comparison between districts
Illicit alcohol producers in Livingstone reported the highest percentages for deficiencies in solid waste management (30%), inadequate toilet facilities (10%) and water supply challenges (18%). Notably, the use of iron and dirty drums, were most prevalent among producers in Lusaka. Ndola and Livingstone, however, exhibited a higher proportion using storage materials other than plastic or iron drums. These findings highlight the critical public health risks associated with hygiene and sanitation in the illicit production of spirits and opaque alcohol across all three sites.
3.4 Comparative analysis across hygiene indicators
A comparative analysis of Livingstone, Lusaka, and Ndola across various hygiene indicators reveals distinct disparities (Table 2). Sites in Lusaka consistently displayed higher proportions across several indicators: solid waste management (57.4%), toilet facilities (53.3%), water supply (53.8%), iron storage (72.7%), presence of plastic drums (58.2%), and presence of other materials (76.8%). Livingstone generally had production sites and retailers with moderate proportions across indicators, such as solid waste management (37.0%), toilet facilities (46.6%), and water supply (46.1%). Ndola consistently reported lower proportions across several key indicators, including toilet facilities (0%), water supply (0%), and infestation (13.2%).
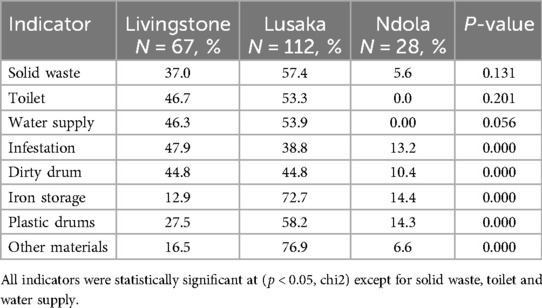
Table 2. Proportion of illicit alcohol production sites and retailers by district and hygiene and sanitation indicators.
4 Discussion
The widespread proliferation of illicit alcohol production and retail sites across the country is a matter of great concern. Our investigation into the hygiene and sanitation of illicit production sites uncovers a complex landscape of unhealthy practices. The study showed a higher dominance of women in illicit alcohol production (Livingstone: F: 84%, M: 16%, Lusaka: F: 86%, M: 14%, Ndola: 93%, M: 7%). Ndola showed the highest percentage of women involved in the illicit trade. This may be associated with the presence of mines on the Copperbelt, which traditionally employ more men than women (21, 22). Currently, training institutions for mine workers, such as universities, colleges and technical institutes, are still dominated by male students, leading women to take up illicit alcohol production or trade as an alternative income-generation strategy (21, 23). The Zambian labor market shows similar trends, where women are more likely to be employed in the informal sector, such as retail, and where the median age of the population is relatively young (24, 25). The predominance of women in this sector reflects broader socio-economic trends where women often resort to informal sectors for income generation (21, 23).
The study showed that the age group most involved in the production and trade of illicit alcohol is between 46 and 59 years and most producers have formal education corresponding to primary school (G1-G7), are married (45%), and self-employed (81%). This could suggest that illicit alcohol serves as a source of income for some Zambian families. The younger group of producers and retailers, between the ages of 18 and 25 years, shows that Livingstone had 7%, Lusaka 9%, and Ndola had the highest with 14%. This young population is also at risk of drinking the illicit alcohol they produce or retail. This is because the illicit alcohol is cheaper and more accessible than licit or legally produced alcohol beverages sold at liquor stores (26, 27).
The study observed the sanitation and levels of hygiene in the production and retail sites. The variables observed included solid waste, toilets, water supply, infestations, dirty drums, iron storage, and plastic drums used for storage. The P- Value for infestations, dirty drums, iron storage, and plastic storages was significant. Ndola showed the lowest rate in the absence of water at the production sites.
The study revealed that Livingstone exhibited the highest unavailability of water supply at illicit alcohol production sites, with 18% lacking access to water of the 3 zones selected, while Lusaka had 13% without water supply of the 7 zones selected, and all sites in Ndola had adequate water supply from the 3 zones selected. These low rates of water availability could contribute to the spread of infectious diseases, such as recent outbreaks of cholera, as water and sanitation play a crucial role in cholera transmission. The unavailability of water supply at these sites could be as a result of high cost of either drilling boreholes or connecting to the public water supply system (28). The high incidence of cholera cases in Lusaka district, identifying it as a hotspot, can be attributed to localized outbreaks affecting specific wards or compounds, such as Mandevu, Matero, and Kabanana, which are often sites of illicit alcohol production (29). Zambia has recently experienced various cholera outbreaks, with the most recent occurring around October 2023 and continuing into 2024. This outbreak was highly fatal, with a case fatality rate of 4%, which is four times the World Health Organization threshold. Most of the cases occurred in December 2023 and January 2024, with Lusaka having more than 7,783 cases as reported by the Zambia National Public Health Institute (30, 31).
The widespread utilization of plastic drums, dirty containers, and inadequate toilet facilities poses significant public health and environmental risks. Moreover, solid waste mismanagement, insufficient water supply, and infestations exacerbate these concerns. The use of plastic materials is linked to various severe adverse effects such as cancers, birth defects, and impaired immunity (32). Regional disparities in hygiene and sanitation practices were also evident, with respondents in Lusaka reporting the highest percentages of deficiencies in solid waste management, inadequate toilet facilities, water supply challenges, and reliance on plastic drums. This could potentially lead to infestations with rodents and cockroaches, while respondents in Livingstone reported a higher prevalence of using iron and dirty drums. In contrast, Ndola exhibited a high proportion of using storage materials other than plastic or iron drums.
These findings underscore the critical need for stricter regulations and enforcement to ensure that all alcohol producers, including those currently producing and selling illicit alcohol, follow best practice regarding hygiene and sanitation. Public health education campaigns are essential to raise awareness of the risks associated with consuming illicit alcohol.
5 Conclusion and recommendation
Our investigation into hygiene and sanitation public health risks associated with illicit alcohol production and retail in Zambia highlights pressing concerns that demand immediate attention. To address these challenges effectively, we propose a multifaceted approach encompassing regulatory, educational, and supportive measures.
Comprehensive public awareness campaigns are vital to inform consumers about the health risks associated with consuming illicit alcohol. By enhancing public understanding, individuals can make informed decisions regarding their alcohol consumption habits, thereby reducing the incidence of related health issues. Moreover, stakeholders must collaborate to develop and promote alternative livelihoods for those engaged in illicit alcohol production, addressing the underlying socioeconomic factors driving participation in this illicit trade. Additionally, targeted training programs are essential for educating illicit alcohol producers on proper hygiene practices and the role they play in preventing disease outbreaks, such as cholera.
In conclusion, it is imperative that stakeholders including policymakers, community leaders, and health organizations—collaborate to establish comprehensive strategies aimed at mitigating these public health risks. By prioritizing interventions that address hygiene and sanitation in illicit alcohol production, we can protect vulnerable populations and promote healthier communities.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
All potential participants were informed about the study and provided written consent before data collection. Data collection procedures were designed to avoid disrupting the normal flow of business. Interviewers were instructed to proceed with the observations only when the retailer/producer was not actively dealing with customers or in their immediate vicinity. Ethical approval for the study was obtained from the University of Zambia Biomedical Research Ethics Committee (UNZABREC REF. No. 4272-2023). Permission to conduct the study was sought from the National Health Research Authority (NHRA). Additionally, courtesy calls and introductory letters were requested from Zambia Revenue Authority (ZRA) officials, District Commissioners of each district, Local Councils, and the Police Headquarters.
Author contributions
MM: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Project administration. CZ: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Data curation, Supervision. MP: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Project administration, Data curation, Supervision, Validation. RZ: Conceptualization, Methodology, Writing – review & editing. TM: Writing – review & editing, Conceptualization, Methodology, Project administration. KM: Conceptualization, Data curation, Writing – review & editing. AH: Resources, Writing – review & editing, Funding acquisition, Methodology. AO: Methodology, Writing – review & editing. WD: Conceptualization, Methodology, Writing – review & editing. DM: Methodology, Writing – review & editing, Conceptualization. AR: Funding acquisition, Methodology, Resources, Writing – review & editing. FG: Conceptualization, Methodology, Writing – review & editing, Supervision, Project administration. TA: Conceptualization, Funding acquisition, Methodology, Resources, Writing – review & editing, Visualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The research and preparation of this manuscript were supported by funding from the AB InBev Foundation. The content is solely the responsibility of the authors and does not necessarily represent the views of AB InBev or the AB InBev Foundation. By contract, CPCR and the authors had final, independent decision authority on all content.
Acknowledgments
We wish to thank Brands on a Mission, AB InBev, the sponsors of the study, University of Zambia Biomedical Research Ethics Committee (UNZABREC), and National Health Research Authority (NHRA) for granting us permission to undertake this study. We also would like to thank all the participants for providing all essential information.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sudhinaraset M, Wigglesworth C, Takeuchi DT. Social and cultural contexts of alcohol use: influences in a social–ecolokgical framework. Alcohol Res. (2016) 38(1):35. doi: 10.15288/arcr.2016.38.1.35
2. Herdiana Y. Alcohol in daily products: health risks, cultural considerations, and economic impacts. Risk Manag Healthc Policy. (2025) 18:217–37. doi: 10.2147/rmhp.s495493
3. Goma M, Ng’ambi WF, Zyambo C. Predicting harmful alcohol use prevalence in sub-Saharan Africa between 2015 and 2019: evidence from population-based HIV impact assessment. PLoS One. (2024) 19(10):e0301735. doi: 10.1371/journal.pone.0301735
4. World Health Organization. Alcohol. World Health Organization (2022). Available at: https://www.afro.who.int/health-topics/alcohol (Accessed September 22, 2024)
5. Etim OO, Okon AJ, Olanrewaju OE, Inah SA. Public health risk knowledge, awareness and hygiene practices of producers of artisanal drinks using previously disposed plastic bottles in Calabar municipality, Cross River state, Nigeria. Glob J Pure Appl Sci. (2022) 28(2):201–11. doi: 10.4314/gjpas.v28i2.10
6. Pengpid S, Peltzer K. Prevalence and correlates of suicidal behaviour among a national population-based sample of adults in Zambia. S Afr J Psychiatr. (2021) 27:1566. doi: 10.4102/sajpsychiatry.v27i0.1566
7. World Health Organization. Zambia steps survey for non-communicable diseases. Zambia Report for 2017. World Health Organisation (2017). Available at: https://www.afro.who.int/publications/zambia-steps-survey-non-communicable-diseases-zambia-report-2017 (accessed April 2, 2024)
8. Zyaambo C, Babaniyi O, Songolo P, Muula AS, Rudatsikira E, Siziya S. Alcohol consumption and its correlates among residents of mining town, Kitwe, Zambia: 2011 population based survey. Am Med J. (2013) 4(1):6–11. doi: 10.3844/amjsp.2013.6.11
9. Shield KD, Manthey J, Rylett M, Margaret R, Charlotte P, Ashley W, et al. National, regional, and global burdens of disease from 2000 to 2016 attributable to alcohol use: a comparative risk assessment study. Lancet Public Health. (2020) 5(1):e51–61. doi: 10.1016/S2468-2667(19)30231-2
10. Ministry of Health. National Alcohol Policy. Zambia: Ministry of Health (2018). Available at: https://www.policyvault.africa/wp-content/uploads/policy/ZMB455.pdf (Accessed September 22, 2024).
11. Swahn MH, Ali B, Palmier JB, Sikazwe G, Mayeya J. Alcohol marketing, drunkenness, and problem drinking among Zambian youth: findings from the 2004 global school-based student health survey. J Environ Public Health. (2011) 2011(1):497827. doi: 10.1155/2011/497827
12. Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Arch Pediatr Adolesc Med. (2006) 160(7):739–46. doi: 10.1001/archpedi.160.7.739
13. Hingson R, Heeren T, Winter MR, Wechsler H. Early age of first drunkenness as a factor in college students’ unplanned and unprotected sex attributable to drinking. Pediatrics. (2003) 111(1):34–41. doi: 10.1542/peds.111.1.34
14. Stueve A, O’Donnell LN. Early alcohol initiation and subsequent sexual and alcohol risk behaviors among urban youths. Am J Public Health. (2005) 95(5):887–93. doi: 10.2105/AJPH.2003.026567
15. Lorca TA. Why should the malting and brewing industry be concerned about food safety? Part 1. Tech. Q. Master Brew. Assoc. Am. (2016) 53:34–8. doi: 10.1094/TQ-53-1-0112-01
16. Walls H, Cook S, Matzopoulos R, London L. Advancing alcohol research in low-income and middle-income countries: a global alcohol environment framework. BMJ Glob Health. (2020) 5(4):e001958. doi: 10.1136/bmjgh-2019-001958
17. Ferreira-Borges C, Parry CD, Babor TF. Harmful use of alcohol: a shadow over sub-saharan Africa in need of workable solutions. Int J Environ Res Public Health. (2017) 14(4):346. doi: 10.3390/ijerph14040346
18. Hlangwani E, Adebiyi JA, Doorsamy W, Adebo OA. Processing, characteristics and composition of umqombothi (a South African traditional beer). Processes. (2020) 8(11):1451. doi: 10.3390/pr8111451
19. Jackson T. Dying for a drink: how the consumption of home brews affects health within the Kibera Slum of Nairobi, Kenya. Independent Study Project (ISP) Collection (2015). Available at: https://digitalcollections.sit.edu/cgi/viewcontent.cgi?article=3049&context=isp_collection (Accessed April, 15, 2025).
20. CDC. Africa CDC support on cholera outbreak in Zambia. Africa CDC (2024). Available at: https://africacdc.org/news-item/africa-cdc-support-on-cholera-outbreak-in-zambia/ (Accessed April 04, 2024).
21. Kalinda R, Thankian K. Women and mining in Zambia: opportunities and challenges. J Sci Res Rep. (2023) 29(4):34–43. doi: 10.9734/jsrr/2023/v29i41742
22. Phiri B, Chileshe PR. Gender in Zambian mining: women in nonmetalliferous smallscale surface mining sector. International Journal of Engineering Research & Technology. (2015) 4(7):1226–33. doi: 10.17577/IJERTV4IS070600
23. Haworth A. Local alcohol issues in Zambia. In: Haworth A, Simpson, R, editors. Moonshine Markets: Issues in Unrecorded Alcohol Beverage Production and Consumption. New York: Psychology Press (2004). p. 39–66. doi: 10.4324/9780203503560
24. Vanek J, Chen M, Carré F, Heintz J, Hussmanns R. Statistics on the informal economy: definitions, regional estimates and challenges. Women in Informal Employment: Globalizing and Organizing (WIEGO) Working Paper (2014). p. 47–59. Available at: https://www.wiego.org/wp-content/uploads/2019/09/Vanek-Statistics-WIEGO-WP2.pdf (Accessed April 04, 2024).
25. Bonnet F, Vanek J, Chen M. Women and Men in the Informal Economy: A Statistical Brief. Geneva: International Labour Office (2019). Available at: https://www.ilo.org/sites/default/files/wcmsp5/groups/public/@ed_protect/@protrav/@travail/documents/publication/wcms_711798.pdf (Accessed April 15, 2025).
26. Romelsjö A, Branting M. Consumption of illegal alcohol among adolescents in Stockholm county. Contemp Drug Probl. (2000) 27(2):315–33. doi: 10.1177/009145090002700207
27. Mungandi K, Likwa RN, Hamoonga TE, Banda J, Zyambo C. Predictors of alcohol consumption among adolescents and young adults in Lusaka, Zambia. Afr Health Sci. (2022) 22(4):704–15. doi: 10.4314/ahs.v23i1.12
28. Gething PW, Ayling S, Mugabi J, Muximpua OD, Kagulura SS, Joseph G. Cholera risk in Lusaka: a geospatial analysis to inform improved water and sanitation provision. PLoS Water. (2023) 2(8):e0000163. doi: 10.1371/journal.pwat.0000163
29. Mwaba J, Debes AK, Shea P, Mukonka V, Chewe O, Chisenga C, et al. Identification of cholera hotspots in Zambia: a spatiotemporal analysis of cholera data from 2008 to 2017. PLoS Negl Trop Dis. (2020) 14(4):e0008227. doi: 10.1371/journal.pntd.0008227
30. ZNPHI. Zambia cholera situation report. ZNPHI (2024). Available at: file:///C:/Users/DELL/Downloads/8-212-PB%20(1).pdf (Accessed March 29, 2024).
31. U.S. Embassy, Zambia. Health Alert—U.S. Embassy. Lusaka, Zambia: Cholera Outbreak (2024). Available at: https://zm.usembassy.gov/health-alert-cholera-outbreak/ (Accessed April 02, 2024).
Keywords: illicit alcohol, hygiene, sanitation, alcohol production, alcohol retailers
Citation: Mukupa M, Zyambo C, Phiri MM, Zulu R, Matenga TFL, Mabanti K, Hainze A, Ogwell A, DeJong W, Menda DM, Rizzo A, Goma F and Achoki T (2025) Hygiene and sanitation public health risks in illicit alcohol production and retail in Zambia. Front. Epidemiol. 5:1461874. doi: 10.3389/fepid.2025.1461874
Received: 30 July 2024; Accepted: 24 January 2025;
Published: 28 April 2025.
Edited by:
Pengpeng Ye, Chinese Center For Disease Control and Prevention, ChinaReviewed by:
Queran Lin, Imperial College London, United KingdomWei Wang, Capital Medical University, China
Copyright: © 2025 Mukupa, Zyambo, Phiri, Zulu, Matenga, Mabanti, Hainze, Ogwell, DeJong, Menda, Rizzo, Goma and Achoki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Musawa Mukupa, bXVzYXdhbXVrdXBhQGdtYWlsLmNvbQ==