 Kunyi Li
Kunyi Li Maolin Li2
Maolin Li2- 1Department of Neurology, the Second People’s Hospital of Chengdu, Chengdu, China
- 2Department of Neurology, People’s Hospital of Deyang City, Deyang, China
- 3Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu, China
- 4Department of Neurology, Chongqing North-Kuanren General Hospital, ChongQing, China
Background: Acute disseminated encephalomyelitis (ADEM) is a rare demyelinating disorder that is often misdiagnosed. To improve early diagnosis, we performed a systematic review and meta-analysis of clinical features, outcomes for ADEM in adults.
Methods: The PubMed, Embase, Web of Science and Cochrane Library databases were searched for studies reporting the clinical features of adults with ADEM between January 1990 and May 2021. A random-effects meta-analysis model was used to pool data on clinical features and functional outcomes.
Results: Twelve studies examining 437 adults with ADEM met the inclusion criteria. Overall, the clinical features and diagnostic findings observed in more than two-thirds of the patients were white matter lesions [87.1%, 95% confidence interval (CI)=75-95.6], polyfocal onset (80.5%, 95% CI=50.5-98.9) and pyramidal signs (68.7%, 95% CI =40.0-91.9). The mortality rate was 7.8% (95% CI = 3.3–13.5), and the risk of residual deficits was 47.5% (95% CI = 31.8–63.4).
Conclusions: Adults with ADEM had worse outcomes than children. Clinicians should maintain high clinical suspicion for patients presenting with certain clinical features and diagnostic findings.
Introduction
Acute disseminated encephalomyelitis (ADEM) is a rare immune-mediated inflammatory demyelinating disorder of the central nervous system (CNS) (1, 2) that was first described in a patient after smallpox infection 250 years ago (3). Although it occurs at all ages, because it is commonly preceded by viral infections or vaccinations, ADEM is more common in children than in adults (2). With the ongoing COVID-19 pandemic and subsequent vaccination use, the incidence of ADEM may increase (4).
Early and accurate diagnosis is important to start prompt treatment and improve outcomes. Due to the lack of specific biomarkers, clinical features play a vital role in the diagnosis of ADEM (5). Other demyelinating disorders, such as multiple sclerosis (MS), may be indistinguishable from ADEM at initial presentation (6). Recently, the International Pediatric Multiple Sclerosis Study Group (IPMSSG) proposed a consensus definition of ADEM for children (7). Due to discrepancies in clinical features between children and adults, this consensus definition may not be suitable for diagnosis in adults. To date, no specific diagnostic criteria have been established for adults.
Recently, several studies have focused on the clinical features of ADEM in adults and found that adult patients had worse outcomes than children (8, 9). However, most of these studies were single-centre studies with small sample sizes. Worldwide data on the clinical features of ADEM in adults are still inconclusive. A systematic evaluation using an evidence-based approach is urgent. To better characterize this rare clinical entity, we conducted a systematic meta-analysis to investigate the clinical features and outcomes of ADEM in adults.
Methods
Literature Search
Two review authors (L.W, Q.C. W) independently searched the PubMed, Embase, Web of Science and Cochrane Library databases. The study search was limited to articles published in English between January 1990 and May 2021. The search terms used in each database included acute disseminated encephalomyelitis and adults (Supplementary Material I).
Eligibility Criteria and Data Extraction
All eligible studies were cohort studies with ADEM patients older than 14 years reporting clinical features and outcomes. Each study reported at least 5 patients. We excluded patients with central nervous system infection, vasculitis, or other autoimmune diseases. Data extracted from eligible studies included the first author, publication year, country, study design, population demographics, clinical features, imaging findings, CSF results, treatment and outcomes including the death and residual deficits. Two study investigators (K.Y.L and M.L.L) independently extracted data from selected articles. Disagreement or uncertainties were resolved by consensus with a third investigator (L.W). To deal with missing data, the study authors were contacted, when necessary.
Quality Assessment
Quality rating of the included studies was performed through the National Institutes of Health Quality Assessment Tool for Case Series Studies (10, 11). Articles were rated as good, fair, or poor independently by two investigators (K.Y.L and M.L.L). If ratings were different, two investigators discussed the articles to reach an agreement.
Certainty of Evidence
Certainty of evidence was evaluated by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. The quality of evidence was rated as high, moderate, low, or very low (12).
Statistical Analysis
The crude frequencies of clinical presentations, and outcomes were first computed for each study and then double-arcsine transformed using the Freeman-Tukey method (13). Meta-analyses with the command metaprop and metan were used to calculate pooled estimates of proportions (95% CI) and pooled estimates of means (95%CI) of clinical presentations, and outcomes. Heterogeneity was tested using Cochran’s Q statistic, and a p value below 0.1 indicated significant heterogeneity. The extent of heterogeneity was quantified using the I2 statistic (14). Because of substantial heterogeneity among the included studies, a random-effects model was used to adjust for this prior to pooling the study-specific frequencies of clinical presentations, diagnostic findings, and functional outcomes. To determine whether a single study had a disproportional influence on the pooled results, a “leave-one-out” sensitivity analysis was performed to calculate the robustness of the pooled results (15). To investigate the potential sources of heterogeneity, we performed subgroup analyses according to location (Europe/Asia/South America) and follow-up time (≤6 months/>6 months). Publication bias was assessed by visual inspection of funnel plots, and tested for significance by using Begg’s rank correlation test and Egger’s regression test (16, 17). All p values were two-sided, and a p value below 0.05 was considered statistically significant. All statistical analyses were performed using STATA version 14.0 (STATA, College Station, TX).
Results
Study Selection and Characteristics
This systematic review and meta-analysis was conducted following the PRISMA guidelines (Supplementary Material II). Figure 1 shows the study selection process and the results of the meta-analysis. The initial search strategy identified 2066 articles. After removing 491 duplicates, a total of 1575 articles were reviewed for relevance by titles and abstracts, and 45 articles remained for further investigation. After detailed assessments, 12 articles (8, 9, 18–27) met the inclusion criteria and were included in this meta-analysis. Forest plots of all the meta-analyses were available in Supplementary Material III.
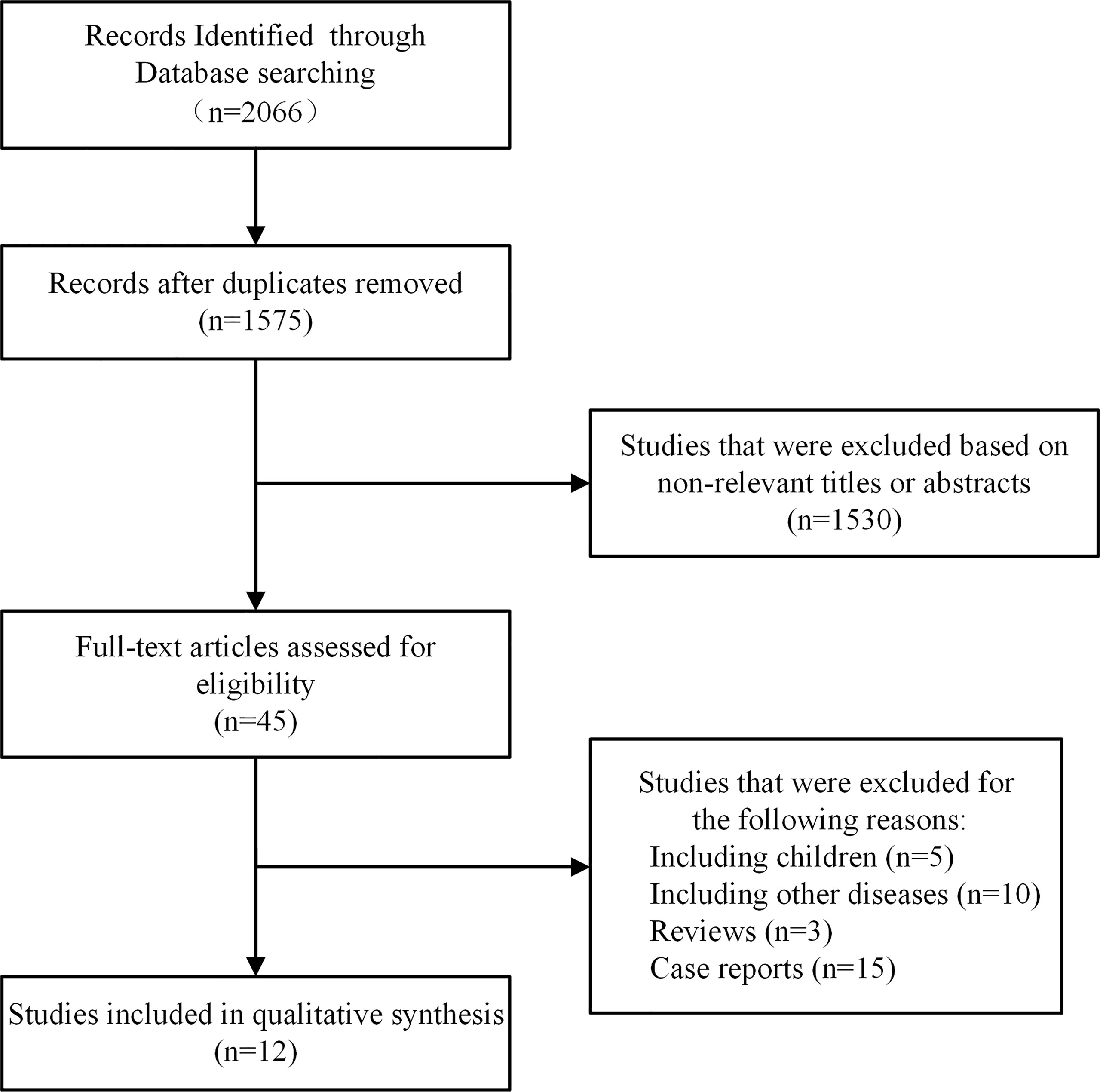
Figure 1 Flowchart of the included studies.
Quality Assessment
The included studies were rated as good [8(66.6%)] or fair [4 (33.3%)] quality, which were assessed by the National Institutes of Health Quality Assessment Tool for Case Series Studies.
Certainty of Evidence
The qualities of the evidence were assessed by GRADE guidelines. Observational studies started with a “low quality” rating, and the quality of evidence was downgraded for the “imprecision”. Thus, the overall qualities of the evidence were rated as “very low” (Supplementary Material IV).
Table 1 summarizes the baseline characteristics of all included studies. In total, 12 included studies were published between 2000 and 2020 and involved a total of 437 cases, with 11 retrospective studies and 1 prospective study. Nine were single-centre studies, and 3 were multicentre studies. Of these studies, 4 were from Europe, 4 were from Asia, 1 was from Oceania, 1 was from North America, 1 was from South America and 1 was from both Asia and North America. A total of 41.7% of patients were male, and the mean age was 37.1 ± 23.1 years. A total of 45.7% of patients met the IPMSSG criteria for ADEM at presentation (7).
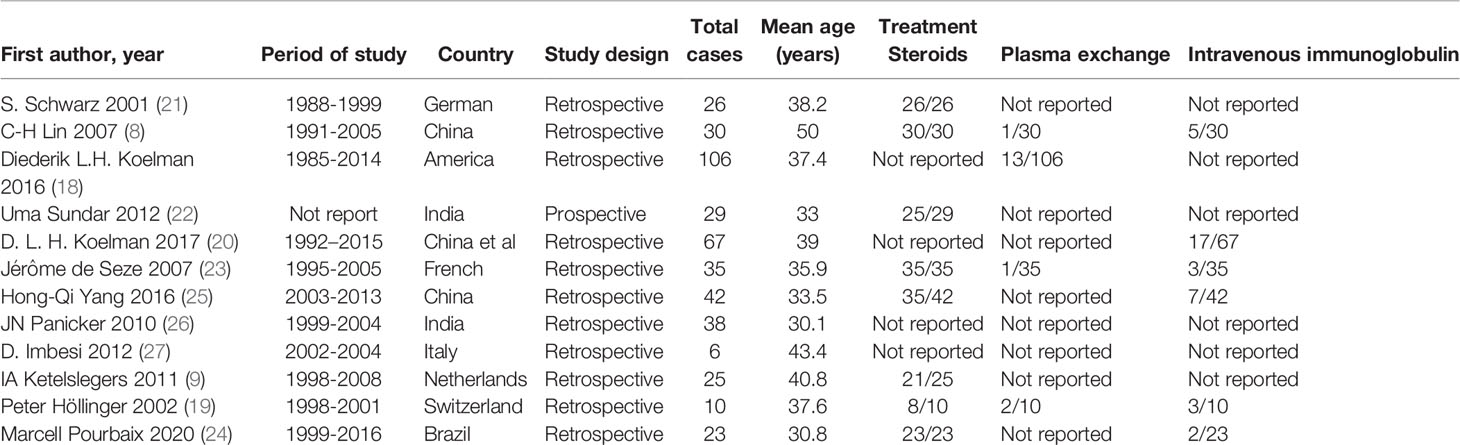
Table 1 Characteristics of included studies in the meta-analysis.
Characteristics at Initial Presentation
Table 2 summarizes the clinical features provided by the 12 studies.
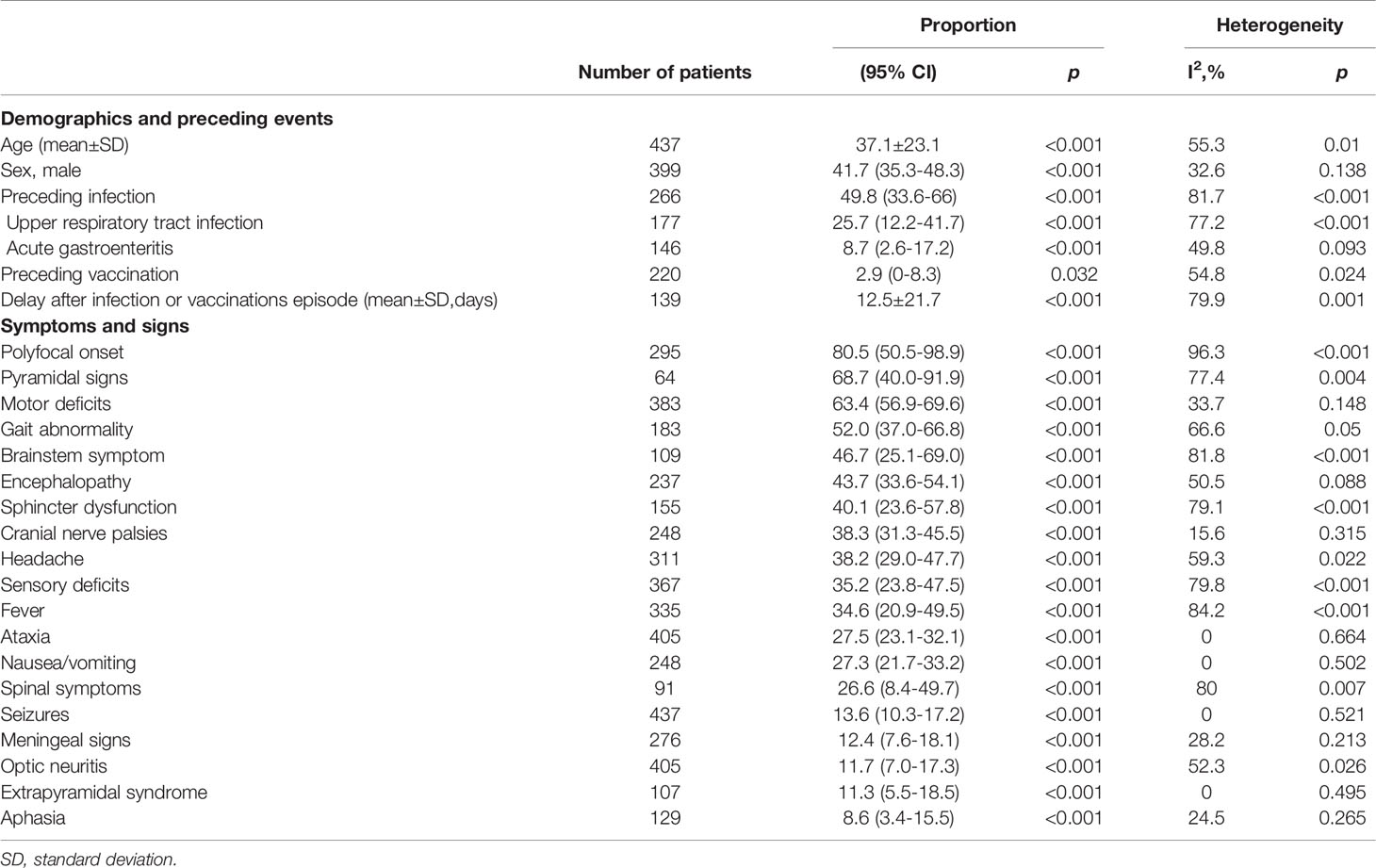
Table 2 Clinical features in patients with ADEM.
Clear antecedent events (infectious event or vaccination) preceded the illness in half of the patients [51.7%, 95% confidence interval (CI) 38.2–65.0]. The interval between the preceding event and illness onset varied, ranging from 0 to 60 days (mean 12.5 ± 21.7 days). Preceding infections mostly involved the upper respiratory tract (25.7%, 95% CI 12.2-41.7) and less often involved the gastrointestinal tract (8.7%, 95% CI 2.6-17.2). Immunizations accounted for only 2.9% (95% CI 0.0-8.3) of cases.
Figure 2 shows the frequencies of symptoms and signs at presentation. Most patients (80.5%, 95% CI 50.5–98.9) had a polyfocal clinical presentation. The most common clinical features included pyramidal signs (68.7%, 95% CI 40.0-91.9), motor deficits (63.4%, 95% CI 56.9–69.6), gait abnormalities (52.0%, 95% CI 37.0-66.8), brainstem symptoms (46.7%, 95% CI 25.1-69.0) and encephalopathy (43.7%, 95% CI 33.6-54.1).
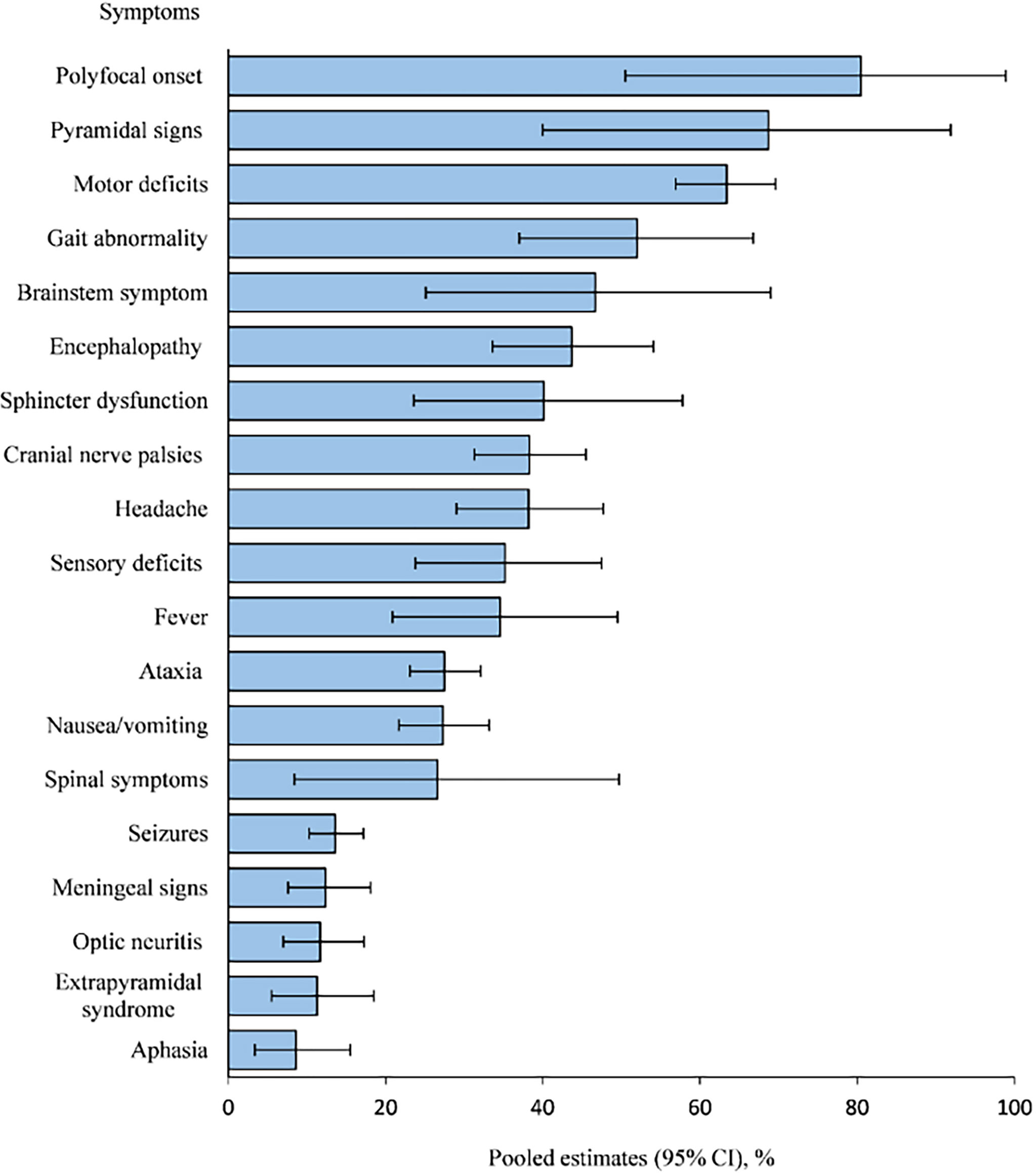
Figure 2 Symptoms and signs of patients with ADEM.
MRI Features
A summary of the imaging findings of patients with ADEM is provided in Table 3. Among the patients who underwent MRI examinations, more than 90% of patients (91.6%, CI 75.0-95.6) presented with abnormal brain MRI findings. Gadolinium-enhancing lesions occurred in nearly 3/5 patients (58.0%, CI 33.6-80.7). The most frequent location of involvement was white matter (87.1%, CI 81.5-98.4), including periventricular white matter (43.2%, 95% CI 26.8-60.3) and subcortical areas (41.9%, 95% CI 31.8-52.2). In addition, an abnormal spinal cord was evident in nearly 41.6% (CI 14.4-51.2) of patients, including spinal cord lesions in > 2 segments in 1/3 of ADEM patients (31.6% CI 14.4-51.2).
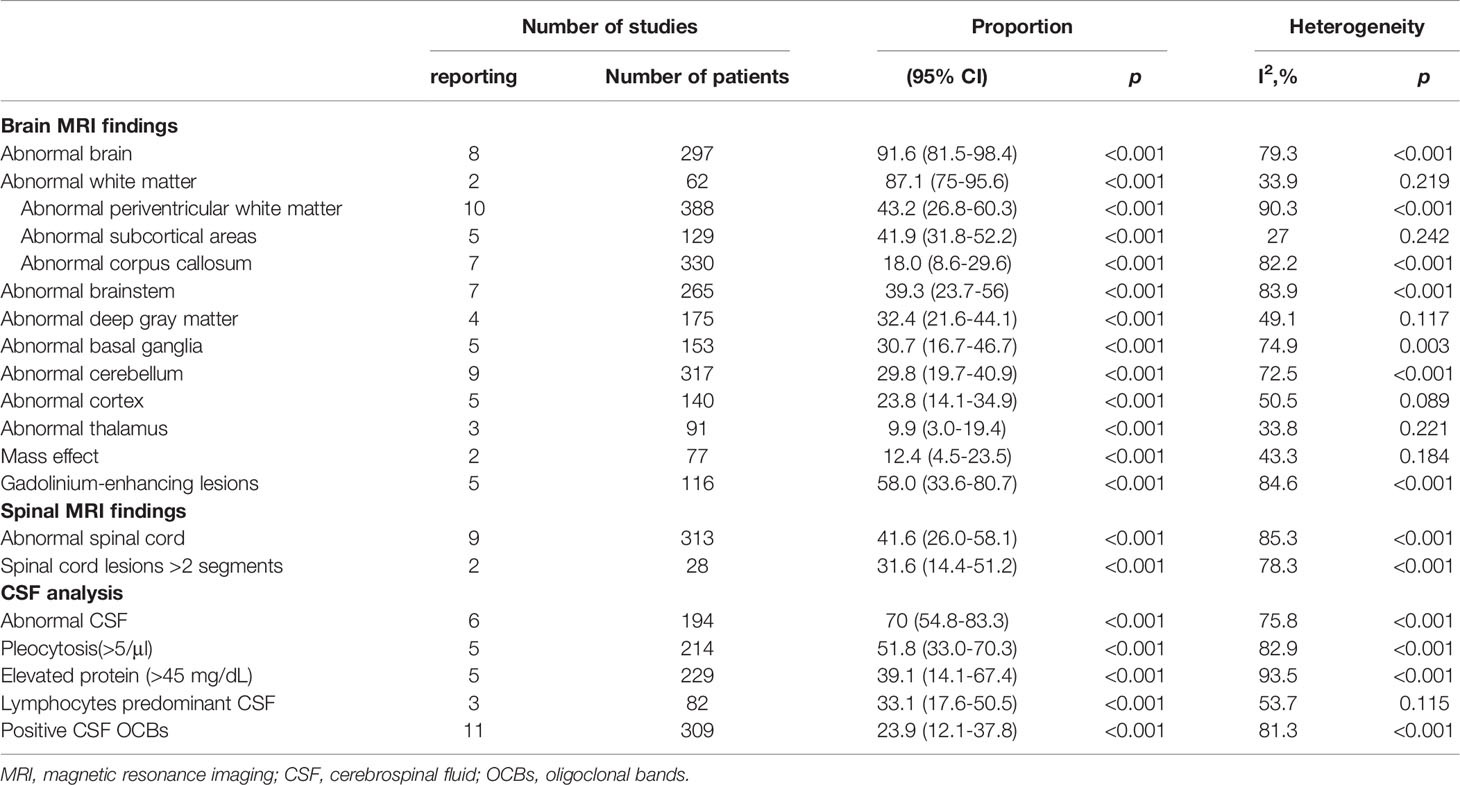
Table 3 Diagnostic findings of patients at admission.
Laboratory Findings
CSF results were abnormal in 70.0% (95% CI 54.8–83.8) of adult patients with ADEM. Pleocytosis occurred in 51.8% (95% CI 33.0–70.3) of patients. CSF protein was increased (> 45 mg/dL) in 39.1% (95% CI 14.1-67.4) of patients. 23.9% (CI 12.1-37.8) of patients showed positive OCB results in CSF. Among the three included studies, 60 patients were tested for aquaporin-4 (AQP4) antibody in serum and all were negative (9, 18, 20).
Treatment and Functional Outcomes
Treatments and patient outcomes are shown in Table 1 and 4. The mean duration of hospitalization was 23.1 days, ranging from 1 to 167 days, and 39.7% (95% CI 23.5-57.1) of patients required admission to the ICU. A total of 95.2% (95% CI 87.4-99.7) of patients were treated with corticosteroids, 16.4% (95% CI 9.2-24.9) were treated with intravenous immunoglobulin G (IVIg), and 7.3% (95% CI 2.0-14.7) were treated with plasma exchange (PLEX).
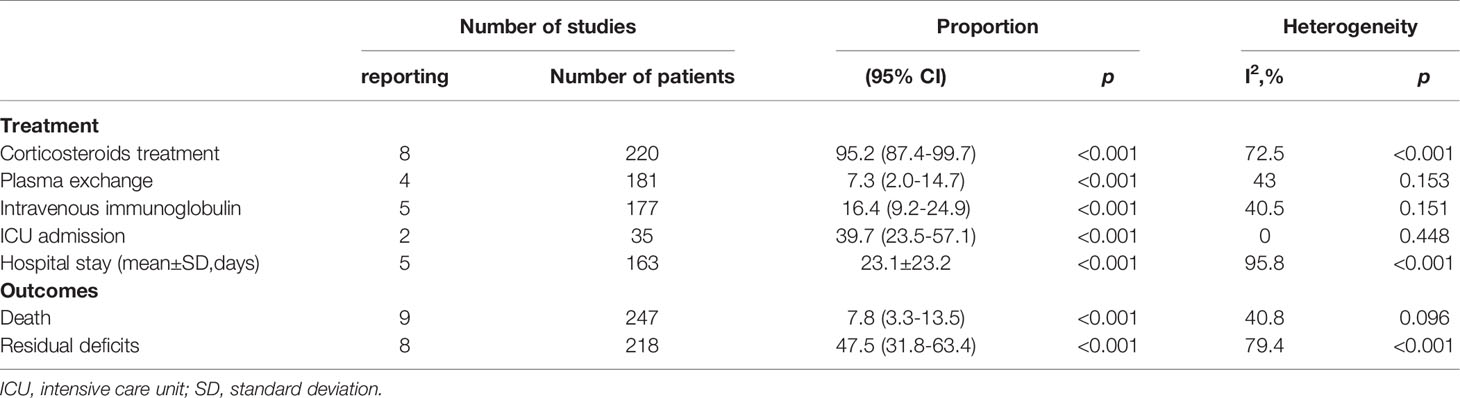
Table 4 Treatment and outcomes of patients with ADEM.
A total of 7.8% (95% CI 3.3-13.5) of patients died and nearly half of the patients (47.5%, 95% CI 36.8-63.4) suffered from residual deficits during the follow-up (2.8 ± 3.6 years). In addition, the recurrence of ADEM occurred in 7.2% (95% CI 2.0-20.8) of patients.
Sensitivity Analysis of Mortality
The “leave-one-out” sensitivity analysis (Supplementary Material V) indicated that the mortality ranged from 6.3% (95% CI 2.8-10.7) to 9.8% (95% CI 5.5-11.5). Thus, no single study had a disproportional effect on the pooled results. Publication bias was not significant, based on visual inspection of funnel plots and the results of Begg’s test and Egger’s test (Supplementary Material VI).
Table 5 summarizes the results of the subgroup meta-analysis of mortality. We determined region-specifc mortality in ADEM adults in Europe, Asia, and Americas. Patients living in Asia (14.5%) had higher mortality than those in other areas (0.4-5.0%). The follow-up time-specifc mortality in ADEM adults was 4.3% for the first 3 months, and 11.0% for more than 3 months.

Table 5 Subgroup analyses for mortality in ADEM adults.
Discussion
The lack of available discrete biomarkers remains a challenge in the diagnosis of ADEM. Currently, the diagnostic criteria of the International Paediatric Multiple Sclerosis Society Group (IPMSSG), which are evaluated by clinical and neuroimaging features, have been partly successful in diagnosing paediatric ADEM. Without alternative criteria for the adult population, the IPMSSG criteria have also been applied in adults in recent studies (28). However, the clinical and imaging profile of ADEM differs substantially according to age (29). Applying the IPMSSG criteria to all adults diagnosed with ADEM leaves more than half of cases without a diagnosis (18, 20). To guide clinical diagnosis and interventions for ADEM adults, we tried to combine our main findings of clinical features and the IPMSSG criteria to propose a summary of the key observations in ADEM adults (Table 6).
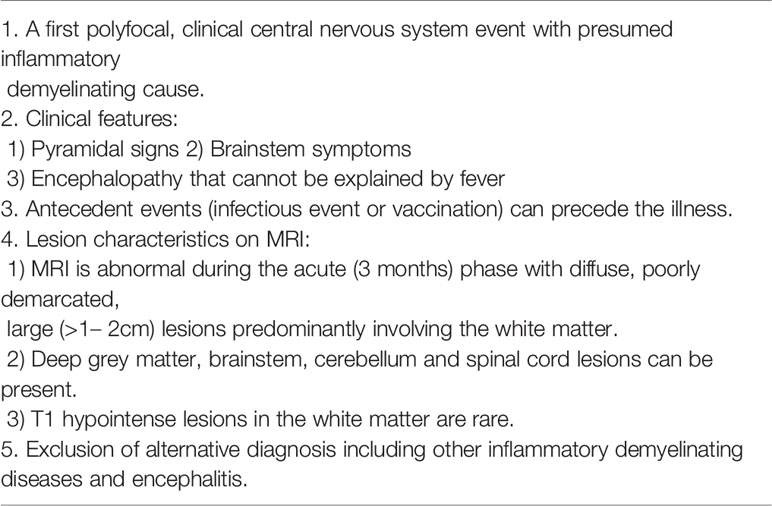
Table 6 A summary of the key observations in ADEM adults.
Among 437 ADEM adults included in 12 studies, ADEM could occur in any age group, with a mean age at onset of 37.1 years. The ratio of males to females with ADEM changes with advancing age. A male predominance has been shown in most studies of paediatric cohorts (30, 31). For adults, we found that the ratio of females was higher than that of males, which is consistent with other inflammatory demyelinating diseases, such as multiple sclerosis (MS) (32).
ADEM symptoms may initially present after a prodromal period of several days or weeks (mean 12.5 days), which may not occur in MS (21, 33). A history of a precipitating event (previous infection or vaccinations) was not a prerequisite for the diagnosis of ADEM, which occurred in half of adult patients. The relationship between precipitating events and the occurrence of ADEM remains controversial, and possible mechanisms may include either molecular mimicry or direct inflammatory damage to myelinated neurons (34).Seasonal variation in the ADEM frequency (with peaks in spring and winter) supports its infectious aetiology (9). Patients with prior infection commonly had respiratory or gastrointestinal viral infections, such as rubella, mumps, measles, varicella, smallpox, and Epstein-Barr virus and infrequently had post bacterial infections, such as Mycoplasma pneumonia (35, 36). The severity of ADEM may be closely associated with different types of prior infection (37). A recent study included 30 ADEM cases after COVID-19 with a predominance of adult cases, possibly because adults are more likely to be infected by COVID-19 (38). For these adult cases, the average age was 50 years, which is older than those in previous reports of ADEM adults (39). More severe cases occur in older adults who often have multiple complications (40). Notably, ADEM can also occur in patients with asymptomatic COVID-19 infection (41). Postvaccination ADEM has occurred with various vaccines, including hepatitis B, hepatitis A, influenza, yellow fever, rubella, and poliomyelitis tetanus vaccines (22–24). In addition, a few recent studies reported that patients developed ADEM after being vaccinated for COVID-19 (42, 43). As postvaccination ADEM is rare, no definitive conclusions can be drawn about the association between a specific vaccine and the real risk of ADEM (44).
The clinical presentation is heterogeneous depending on the area involved in the demyelinating process. Four-fifths of the patients had a polyfocal clinical presentation associated with multifocal neurological deficits. Patients could show prodromal symptoms such as fever, headache, nausea, and vomiting. Fever was less common in adults than in paediatric patients, implying that age-related changes in the immune response, especially inflammatory cytokine reactions, might partially explain this difference (8). As fever is an unusual symptom in other demyelinating diseases, such as MS, this symptom may support the diagnosis of ADEM (21). The acute phase occurs with encephalopathy, which may be subtle, especially in the early course, and is often noted as “irritability” or “sleepiness” rather than confusion or obtundation (45). Studies in paediatric cohorts have shown encephalopathy, with rates ranging from 58.3% to 74% (8, 9, 18). In adults, the occurrence of encephalopathy is clinically important, as its absence may help identify other diseases, such as MS, which is less likely to present with encephalopathy (21). However, the frequency of encephalopathy in adults is relatively low (43.7%), suggesting that the absence of encephalopathy should not discourage neurologists from diagnosing this disease in adults. Encephalopathy is essential for the diagnosis of ADEM according to the IPMSSG criteria. These criteria may be overly restrictive for adults. We found that motor deficits, including hemiplegia, paraplegia and quadriplegia, were the most common clinical features, which occurred in more than three-fifths of patients, implying that pyramidal tract lesions are involved in most cases. Another common clinical feature is ataxia, which is rare in MS (46). Atypical symptoms, including meningeal signs, seizures and neuropsychiatric symptoms, may resemble CNS infectious diseases, highlighting a certain variability in the clinical presentation of ADEM. Thus, further auxiliary examinations including MRI imaging and CSF examinations are needed (5).
A previous study suggested that the clinical diagnosis of ADEM is mainly based on neuroimaging findings in clinical practice (47). MRI is a highly sensitive technique for detecting white matter abnormalities and is the preferred examination method for the diagnosis of ADEM (48). FLAIR and T2-weighted MR imaging is suitable for lesions detection. Lesions in most of ADEM patients show vasogenic cerebral edema on diffusion weighted imaging (DWI), which is beneficial to establish a differential diagnosis with other diseases (cytotoxic edema), such as acute cerebral infarction (49). ADEM is characterized by multifocal inflammatory demyelinating lesions in white matter (87.1%). Lesions are typically large and localized asymmetrically and have poorly defined margins. The deep grey matter is frequently involved (32.4%), often symmetrically, while cortical areas (23.8%) are involved to a lesser extent (29). The frequency of gadolinium-enhancing lesions is highly variable among studies, ranging from 30.0% to 95.2%, which may depend on the time of MRI evaluation. Notably, nearly one-tenth of ADEM adults present with a normal MRI or a delay of a few days to a few weeks between symptom onset and the appearance of MRI abnormalities (29). Thus, a normal MRI in the first days after symptom onset does not rule out a diagnosis of ADEM, and a follow-up MRI is needed for these patients. Compared with children, adults present with more frequent involvement of the periventricular areas and less often with involvement of the basal ganglia (8, 9). In addition, neuroimaging is useful to distinguish CNS demyelination diseases from other causes, such as MS and neuromyelitis optica spectrum disorder (NMOSD). Lesions in the thalamus and basal ganglia are more typical of ADEM than MS (50). Callosal lesions have been reported to occur in more than half of patients with MS (51, 52) but only in nearly one-fifth of adults with ADEM. Furthermore, a recent study compared callosal lesions on MRI among adults with CNS demyelinating diseases and found that radial lesions, defined as strip-shaped lesions spreading vertically from the lower surface to the upper surface of the corpus callosum, may be characteristic of MS and NMOSD but are rarely observed in ADEM (53). Moreover, a paediatric cohort study found that T1 hypointense lesions and more than two periventricular lesions may be MRI characteristics for distinguishing MS from ADEM, which requires further confirmation in an adult population (54). The spinal cord is also commonly involved in ADEM; however, an isolated spinal cord lesion without supratentorial involvement is unusual, which is different from NMOSD (55, 56).
CSF examinations in suspected ADEM should be performed rapidly after hospital admission to differentiate ADEM from other disorders, such as infection, MS and NMOSD. ADEM often presents as nonspecific inflammatory changes in most ADEM patients, including pleocytosis (51.8%) and elevated protein levels (39.1%) (29). Compared with the high incidence of CSF oligoclonal bands (OCBs) (>80%) in MS, positive CSF OCBs occurred in only one-fifth of ADEM adults (57). Among ADEM patients with positive OCBs, identical serum and CSF OCBs (‘mirror pattern’) were the most common pattern, suggesting predominant systemic immune activation, which is likely a consequence of infection or vaccination. However, most patients had CSF-restricted OCBs in MS. These results indicate that the detection of OCBs in both CSF and serum could help discriminate ADEM from MS (58). Autoantibodies targeting myelin oligodendrocyte glycoprotein (anti-MOG-IgG) are a marker of several central nervous system inflammatory demyelinating disorders, including ADEM, bilateral optic neuritis, transverse myelitis, and brainstem encephalitis. MOG-IgG positive children presented as ADEM in approximately 50% of cases, whereas adults in less than 10% (59). In children, high MOG-IgG at onset with declining antibody levels may be associated with a monophasic disease course and more likely to have a favorable long-term prognosis (60). While, persistent MOG-IgG may imply a recurrent disease course (61). Due to the limited ADEM cases in adults, further larger-scale longitudinal studies are needed to evaluate the value of MOG antibody in ADEM adults.
EEG is useful for the evaluation of brain function, especially if neuroimaging and CSF findings are negative (19). Diffuse background slowing is the most common finding, which may provide an alternative explanation for the encephalopathy observed in these patients (3, 26). In addition, the presence of focal slowing or epileptiform discharges may support seizures in ADEM patients.
Functional outcomes of ADEM in paediatric patients are generally favourable. Adults had a more unfavourable functional outcome and slower recovery: nearly one-tenth of adult patients died, and residual deficits occurred in nearly half of the patients during the follow-up. In addition, two-fifths of adult patients required admission to the intensive care unit (ICU). Moreover, the duration of hospitalization was longer for adults than for children (2, 9). The discrepancy in functional outcomes may be related to the reduced plasticity of the ageing brain and differences in immune responses, which has been hypothesized previously in a mouse model (62). Our analysis of the follow-up time-specifc mortality indicated that half of deaths occurred after the first 3 months. This finding stresses the importance of follow-up.
Previous studies suggested that impaired consciousness and seizures were associated with poor outcomes, while patients with fever, nonreactive CSF and a low lesion load on MRI were more likely to have a good outcome (8, 22, 26). However, due to the different risk factors and endpoints among these studies, it is difficult to merge and analyze the common risk factors among these studies. Moreover, recurrence may occur in adults, affecting 0% to 22.6% of patients according to different studies, and follow-up visits may be necessary (8, 18, 23, 25) As the prognosis of ADEM in adults is worse, more rapid and aggressive treatment may contribute to a better outcome in these patients (9). No randomized trials have identified the best treatment for ADEM, and small observational studies and expert opinions are the main basis for therapy. The most effective therapy for ADEM remains unclear. Based on the hypothesis of immune-mediated damage, the standard treatment is unspecific immunosuppressive therapy. High doses of corticosteroids are the first-line treatment and are used in most patients. Intravenous immunoglobulins (IVIGs) and plasma exchange (PLEX) are considered second-line treatment in patients with resistance or contraindications to steroids (3, 63, 64). Notably, PLEX could also be effective as rescue therapy in paediatric ADEM (65). Moreover, patients with contrast-enhancing lesions or mass effect may have the greatest benefit from PLEX (66). In addition, for a few patients with intracranial mass effects, decompressive craniectomy may be a lifesaving intervention for such cases (67, 68).
Limitation
This study has several limitations. First, most of the included studies were retrospective with small sample sizes and some auxiliary examinations could not be available for all patients. Second, there were possible causes of heterogeneity among the included studies based on the inclusion of different races, studies conducted in different countries. The lack of continuity in the diagnostic criteria used throughout the past decades could also cause heterogeneity, an uniform diagnostic criteria is urgent, thus we proposed a summary of the key observations in ADEM adults. Fourth, only a few included studies evaluated prognostic factors, which should be investigated in further studies. Fifth, the examination of MOG antibody is absent in the original articles, which should be conducted in further studies. Finally, no randomized trials for the treatment of ADEM were found, and which treatment may be the best is unclear. Due to the limitations mentioned above, these data should be interpreted with caution, and further large and well-designed studies are needed to confirm the conclusions of this study.
Conclusion
The outcomes of ADEM in adults are worse than those in children. Considering the differences in the clinical characteristics of ADEM between adults and children, to distinguish ADEM from other CNS demyelination diseases, diagnostic criteria specialized for adults are needed. In addition, controlled trials are needed to evaluate the effectiveness and safety of different immunotherapies for this disease.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
JW, XD and KL had the idea for the study. KL, ML, LW and QW collected the data. All authors drafted and revised the paper, and approved the final version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.870867/full#supplementary-material
References
1. Noorbakhsh F, Johnson RT, Emery D, Power C. Acute Disseminated Encephalomyelitis: Clinical and Pathogenesis Features. Neurol Clin (2008) 26:759–780, ix. doi: 10.1016/j.ncl.2008.03.009
2. Pohl D, Alper G, Van Haren K, Kornberg AJ, Lucchinetti CF, Tenembaum S, et al. Acute Disseminated Encephalomyelitis: Updates on an Inflammatory CNS Syndrome. Neurology (2016) 87:S38–45. doi: 10.1212/WNL.0000000000002825
3. Otallah S. Acute Disseminated Encephalomyelitis in Children and Adults: A Focused Review Emphasizing New Developments. Mult Scler (2021) 27:1153–60. doi: 10.1177/1352458520929627
4. Manzano G, McEntire C, Martinez-Lage M, Mateen F, Hutto S. Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalitis Following COVID-19: Systematic Review and Meta-Synthesis. Neurology(R) Neuroimmunol Neuroinflamm (2021) 8:e1080. doi: 10.1212/NXI.0000000000001080
5. Paolilo RB, Deiva K, Neuteboom R, Rostásy K. Acute Disseminated Encephalomyelitis: Current Perspectives. Children (Basel) (2020) 7:210. doi: 10.3390/children7110210
6. Koelman D, Mateen F. Acute Disseminated Encephalomyelitis: Current Controversies in Diagnosis and Outcome. J Neurol (2015) 262:2013–24. doi: 10.1007/s00415-015-7694-7
7. Krupp LB, Tardieu M, Amato MP, Banwell B, Chitnis T, Dale RC, et al. International Pediatric Multiple Sclerosis Study Group Criteria for Pediatric Multiple Sclerosis and Immune-Mediated Central Nervous System Demyelinating Disorders: Revisions to the 2007 Definitions. Mult Scler (2013) 19:1261–7. doi: 10.1177/1352458513484547
8. Lin CH, Jeng JS, Hsieh ST, Yip PK, Wu RM. Acute Disseminated Encephalomyelitis: A Follow-Up Study in Taiwan. J Neurol Neurosurg Psychiatry (2007) 78:162–7. doi: 10.1136/jnnp.2005.084194
9. Ketelslegers IA, Visser IE, Neuteboom RF, Boon M, Catsman-Berrevoets CE, Hintzen RQ, et al. Disease Course and Outcome of Acute Disseminated Encephalomyelitis Is More Severe in Adults than in Children. Mult Scler (2011) 17:441–8. doi: 10.1177/1352458510390068
10. D'Antona L, Jaime Merchan MA, Vassiliou A, Watkins LD, Davagnanam I, Toma AK, et al. Clinical Presentation, Investigation Findings, and Treatment Outcomes of Spontaneous Intracranial Hypotension Syndrome: A Systematic Review and Meta-Analysis. JAMA Neurol (2021) 78:329–37. doi: 10.1001/jamaneurol.2020.4799
11. National Heart, Lung, and Blood Institute. Study Quality Assessment Tools, in: Quality Assessment Tool for Case Series Studies (Accessed March 20,2022).
12. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. Bmj (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
13. Miller JJ. The Inverse of the Freeman – Tukey Double Arcsine Transformation. Am Statistician (1978) 32:138–8. doi: 10.1080/00031305.1978.10479283
14. Higgins JP, Thompson SG. Quantifying Heterogeneity in a Meta-Analysis. Stat Med (2002) 21:1539–58. doi: 10.1002/sim.1186
15. Wallace BC, Schmid CH, Lau J, Trikalinos TA. Meta-Analyst: Software for Meta-Analysis of Binary, Continuous and Diagnostic Data. BMC Med Res Methodol (2009) 9:80. doi: 10.1186/1471-2288-9-80
16. Egger M, Davey Smith G, Schneider M, Minder C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. Bmj (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
17. Begg CB, Mazumdar M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics (1994) 50:1088–101. doi: 10.2307/2533446
18. Koelman DL, Chahin S, Mar SS, Venkatesan A, Hoganson GM, Yeshokumar AK, et al. Acute Disseminated Encephalomyelitis in 228 Patients: A Retrospective, Multicenter US Study. Neurology (2016) 86:2085–93. doi: 10.1212/WNL.0000000000002723
19. Höllinger P, Sturzenegger M, Mathis J, Schroth G, Hess C. Acute Disseminated Encephalomyelitis in Adults: A Reappraisal of Clinical, CSF, EEG, and MRI Findings. J Neurol (2002) 249:320–9. doi: 10.1007/s004150200012
20. Koelman DL, Benkeser DC, Xu Y, Neo SX, Tan K, Katsuno M, et al. Acute Disseminated Encephalomyelitis in China, Singapore and Japan: A Comparison With the USA. Eur J Neurol (2017) 24:391–6. doi: 10.1111/ene.13220
21. Schwarz S, Mohr A, Knauth M, Wildemann B, Storch-Hagenlocher B. Acute Disseminated Encephalomyelitis: A Follow-Up Study of 40 Adult Patients. Neurology (2001) 56:1313–8. doi: 10.1212/WNL.56.10.1313
22. Sundar U, Shrivastava MS. Acute Disseminated Encephalomyelitis–A Prospective Study of Clinical Profile and in-Hospital Outcome Predictors. J Assoc Physicians India (2012) 60:21–6.
23. de Seze J, Debouverie M, Zephir H, Lebrun C, Blanc F, Bourg V, et al. Acute Fulminant Demyelinating Disease: A Descriptive Study of 60 Patients. Arch Neurology (2007) 64:1426–32. doi: 10.1001/archneur.64.10.1426
24. Guimaraes MPM, Nascimento ACB, Alvarenga RMP. CLINICAL Course of Acute Disseminated Encephalomyelitis in Adults From Rio De Janeiro: Retrospective Study of 23 Cases and Literature Review. Multiple Sclerosis Related Disord (2020) 46:102424. doi: 10.1016/j.msard.2020.102424
25. Yang H, Zhao W, Yang W, Li Y, Sun Z, Chen S, et al. Clinical Profiles and Short-Term Outcomes of Acute Disseminated Encephalomyelitis in Adult Chinese Patients. J Clin Neurol (Seoul Korea) (2016) 12:282–8. doi: 10.3988/jcn.2016.12.3.282
26. Panicker JN, Nagaraja D, Kovoor JM, Subbakrishna DK. Descriptive Study of Acute Disseminated Encephalomyelitis and Evaluation of Functional Outcome Predictors. J Postgrad Med (2010) 56:12–6. doi: 10.4103/0022-3859.62425
27. Imbesi D, Calabrò R, Gervasi G, Casella C, Vita G, Musolino R, et al. Does HLA Class II Haplotype Play a Role in Adult Acute Disseminated Encephalomyelitis? Preliminary Findings From a Southern Italy Hospital-Based Study. Arch Italiennes Biologie (2012) 150:1–4. doi: 10.4449/aib.v150i1.1384
28. Chen Y, Ma F, Xu Y, Chu X, Zhang J. Incidence of Acute Disseminated Encephalomyelitis in the Jiangsu Province of China, 2008-2011. Mult Scler J Exp Transl Clin (2015) 1:2055217315594831. doi: 10.1177/2055217315594831
29. Berzero G, Cortese A, Ravaglia S, Marchioni E. Diagnosis and Therapy of Acute Disseminated Encephalomyelitis and Its Variants. Expert Rev Neurother (2016) 16:83–101. doi: 10.1586/14737175.2015.1126510
30. Murthy SN, Faden HS, Cohen ME, Bakshi R. Acute Disseminated Encephalomyelitis in Children. Pediatrics (2002) 110:e21. doi: 10.1542/peds.110.2.e21
31. Tenembaum S, Chamoles N, Fejerman N. Acute Disseminated Encephalomyelitis: A Long-Term Follow-Up Study of 84 Pediatric Patients. Neurology (2002) 59:1224–31. doi: 10.1212/WNL.59.8.1224
32. Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple Sclerosis. Lancet (2018) 391:1622–36. doi: 10.1016/S0140-6736(18)30481-1
33. Charles M. McAlpine's Multiple Sclerosis, 2nd Ed. Neurology (1991) 41:959–9. doi: 10.1212/WNL.41.6.959
34. Esposito S, Di Pietro GM, Madini B, Mastrolia MV, Rigante D. A Spectrum of Inflammation and Demyelination in Acute Disseminated Encephalomyelitis (ADEM) of Children. Autoimmun Rev (2015) 14:923–9. doi: 10.1016/j.autrev.2015.06.002
35. Fallis AG. Harrison's Principles of Internal Medicine, 19th edition. New York:McGraw Hill (2013).
36. Marchioni E, Ravaglia S, Piccolo G, Furione M, Zardini E, Franciotta D, et al. Postinfectious Inflammatory Disorders: Subgroups Based on Prospective Follow-Up. Neurology (2005) 65:1057–65. doi: 10.1212/01.wnl.0000179302.93960.ad
37. Bennetto L, Scolding N. Inflammatory/post-Infectious Encephalomyelitis. J Neurol Neurosurg Psychiatry (2004) 75 Suppl 1:i22–28. doi: 10.1136/jnnp.2003.034256
38. Mehta NS, Mytton OT, Mullins E, Fowler TA, Falconer CL, Murphy OB, et al. SARS-CoV-2 (COVID-19): What Do We Know About Children? A Systematic Review. Clin Infect Dis (2020) 71:2469–79. doi: 10.2139/ssrn.3558015
39. Zelada-Ríos L, Pacheco-Barrios K, Galecio-Castillo M, Yamunaqué-Chunga C, Álvarez-Toledo K, Otiniano-Sifuentes R, et al. Acute Disseminated Encephalomyelitis and COVID-19: A Systematic Synthesis of Worldwide Cases. J neuroimmunology (2021) 359:577674. doi: 10.1016/j.jneuroim.2021.577674
40. Helms J, Meziani F. Neurologic Features in Severe SARS-CoV-2 Infection. N Engl J Med (2020) 382:2268–70. doi: 10.1056/NEJMc2008597
41. Abdi S, Ghorbani A, Fatehi F. The Association of SARS-CoV-2 Infection and Acute Disseminated Encephalomyelitis Without Prominent Clinical Pulmonary Symptoms. J Neurological Sci (2020) 416:117001. doi: 10.1016/j.jns.2020.117001
42. Vogrig A, Janes F, Gigli G, Curcio F, Negro I, D'Agostini S, et al. Acute Disseminated Encephalomyelitis After SARS-CoV-2 Vaccination. Clin Neurol Neurosurgery (2021) 208:106839. doi: 10.1016/j.clineuro.2021.106839
43. Ozgen Kenangil G, Ari B, Guler C, Demir M. Acute Disseminated Encephalomyelitis-Like Presentation After an Inactivated Coronavirus Vaccine. Acta Neurologica Belgica (2021) 121:1089-91. doi: 10.1007/s13760-021-01855-3
44. Torisu H, Okada K. Vaccination-Associated Acute Disseminated Encephalomyelitis. Vaccine (2019) 37:1126–9. doi: 10.1016/j.vaccine.2019.01.021
45. Fridinger SE, Alper G. Defining Encephalopathy in Acute Disseminated Encephalomyelitis. J Child Neurol (2014) 29:751–5. doi: 10.1177/0883073813489732
46. Santoro J, Chitnis T. Diagnostic Considerations in Acute Disseminated Encephalomyelitis and the Interface With MOG Antibody. Neuropediatrics (2019) 50:273–9. doi: 10.1055/s-0039-1693152
47. Boesen MS, Blinkenberg M, Koch-Henriksen N, Thygesen LC, Uldall PV, Magyari M, et al. Implications of the International Paediatric Multiple Sclerosis Study Group Consensus Criteria for Paediatric Acute Disseminated Encephalomyelitis: A Nationwide Validation Study. Dev Med Child Neurol (2018) 60:1123–31. doi: 10.1111/dmcn.13798
48. Singh S, Prabhakar S, Korah IP, Warade SS, Alexander M. Acute Disseminated Encephalomyelitis and Multiple Sclerosis: Magnetic Resonance Imaging Differentiation. Australas Radiol (2000) 44:404–11. doi: 10.1046/j.1440-1673.2000.00845.x
49. Zuccoli G, Panigrahy A, Sreedher G, Bailey A, Laney Ejt, La Colla L. Vasogenic Edema Characterizes Pediatric Acute Disseminated Encephalomyelitis. Neuroradiology (2014) 56:679–84. doi: 10.1007/s00234-014-1379-2
50. Verhey LH, Branson HM, Shroff MM, Callen DJ, Sled JG, Narayanan S, et al. MRI Parameters for Prediction of Multiple Sclerosis Diagnosis in Children With Acute CNS Demyelination: A Prospective National Cohort Study. Lancet Neurol (2011) 10:1065–73. doi: 10.1016/S1474-4422(11)70250-2
51. Ito S, Mori M, Makino T, Hayakawa S, Kuwabara S. “Cloud-Like Enhancement” Is a Magnetic Resonance Imaging Abnormality Specific to Neuromyelitis Optica. Ann Neurol (2009) 66:425–8. doi: 10.1002/ana.21753
52. Garg N, Reddel SW, Miller DH, Chataway J, Riminton DS, Barnett Y, et al. The Corpus Callosum in the Diagnosis of Multiple Sclerosis and Other CNS Demyelinating and Inflammatory Diseases. J Neurol Neurosurg Psychiatry (2015) 86:1374–82. doi: 10.1136/jnnp-2014-309649
53. Cai MT, Zhang YX, Zheng Y, Fang W, Ding MP. Callosal Lesions on Magnetic Resonance Imaging With Multiple Sclerosis, Neuromyelitis Optica Spectrum Disorder and Acute Disseminated Encephalomyelitis. Mult Scler Relat Disord (2019) 32:41–5. doi: 10.1016/j.msard.2019.04.019
54. Callen DJ, Shroff MM, Branson HM, Li DK, Lotze T, Stephens D, et al. Role of MRI in the Differentiation of ADEM From MS in Children. Neurology (2009) 72:968–73. doi: 10.1212/01.wnl.0000338630.20412.45
55. Singh S, Alexander M, Korah IP. Acute Disseminated Encephalomyelitis: MR Imaging Features. Am J Roentgenology (1999) 173:1101–7. doi: 10.2214/ajr.173.4.10511187
56. Sechi E, Krecke K, Messina S, Buciuc M, Pittock S, Chen J, et al. Comparison of MRI Lesion Evolution in Different Central Nervous System Demyelinating Disorders. Neurology (2021) 97:e1097–109. doi: 10.1212/WNL.0000000000012467
57. Dobson R, Ramagopalan S, Davis A, Giovannoni G. Cerebrospinal Fluid Oligoclonal Bands in Multiple Sclerosis and Clinically Isolated Syndromes: A Meta-Analysis of Prevalence, Prognosis and Effect of Latitude. J Neurol Neurosurg Psychiatry (2013) 84:909–14. doi: 10.1136/jnnp-2012-304695
58. Franciotta D, Columba-Cabezas S, Andreoni L, Ravaglia S, Jarius S, Romagnolo S, et al. Oligoclonal IgG Band Patterns in Inflammatory Demyelinating Human and Mouse Diseases. J Neuroimmunol (2008) 200:125–8. doi: 10.1016/j.jneuroim.2008.06.004
59. Hegen H, Reindl M. Recent Developments in MOG-IgG Associated Neurological Disorders. Ther Adv Neurol Disord (2020) 13:1756286420945135. doi: 10.1177/1756286420945135
60. aumann M, Hennes EM, Schanda K, Karenfort M, Kornek B, Seidl R, et al. Children With Multiphasic Disseminated Encephalomyelitis and Antibodies to the Myelin Oligodendrocyte Glycoprotein (MOG): Extending the Spectrum of MOG Antibody Positive Diseases. Mult Scler (2016) 22:1821–9. doi: 10.1177/1352458516631038
61. Hacohen Y, Wong YY, Lechner C, Jurynczyk M, Wright S, Konuskan B, et al. Disease Course and Treatment Responses in Children With Relapsing Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease. JAMA Neurol (2018) 75:478–87. doi: 10.1001/jamaneurol.2017.4601
62. Matejuk A, Hopke C, Vandenbark AA, Hurn PD. Middle-Age Male Mice Have Increased Severity of Experimental Autoimmune Encephalomyelitis and Are Unresponsive to Testosterone Therapy. J Immunol (2005) 174:2387–95. doi: 10.4049/jimmunol.174.4.2387
63. Steiner I, Kennedy PG. Acute Disseminated Encephalomyelitis: Current Knowledge and Open Questions. J Neurovirol (2015) 21:473–9. doi: 10.1007/s13365-015-0353-z
64. Massa S, Fracchiolla A, Neglia C, Argentiero A, Esposito S. Update on Acute Disseminated Encephalomyelitis in Children and Adolescents. Children (Basel) (2021) 8:280. doi: 10.3390/children8040280
65. Eyre M, Hacohen Y, Lamb K, Absoud M, Agrawal S, Gadian J, et al. Utility and Safety of Plasma Exchange in Paediatric Neuroimmune Disorders. Dev Med Child Neurol (2019) 61:540–6. doi: 10.1111/dmcn.14150
66. Magaña S, Keegan B, Weinshenker B, Erickson B, Pittock S, Lennon V, et al. Beneficial Plasma Exchange Response in CNS Inflammatory Demyelination. Arch Neurol (2011) 68:870. doi: 10.1001/archneurol.2011.34
67. Algahtani H, Shirah B, Alassiri A, Algahtani S. Decompressive Craniectomy as a Lifesaving Intervention for Acute Disseminated Encephalomyelitis (ADEM). Multiple sclerosis related Disord (2021) 47:102612. doi: 10.1016/j.msard.2020.102612
Keywords: ADEM, clinical feature, outcome, meta, adult
Citation: Li K, Li M, Wen L, Wang Q, Ding X and Wang J (2022) Clinical Presentation and Outcomes of Acute Disseminated Encephalomyelitis in Adults Worldwide: Systematic Review and Meta-Analysis. Front. Immunol. 13:870867. doi: 10.3389/fimmu.2022.870867
Received: 09 February 2022; Accepted: 03 May 2022;
Published: 09 June 2022.
Edited by:
Todd Hardy, Concord Repatriation General Hospital, AustraliaReviewed by:
Michael Eyre, King’s College London, United KingdomSuvasini Sharma, University of Delhi, India
Copyright © 2022 Li, Li, Wen, Wang, Ding and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xin Ding, ZGluZ3hpbjEwNUAxNjMuY29t; Jian Wang, NDI1MjM3NDhAcXEuY29t