 Matilde Bandeira1,2*†‡
Matilde Bandeira1,2*†‡ Eduardo Dourado1,2†‡
Eduardo Dourado1,2†‡ Ana Teresa Melo1,2
Ana Teresa Melo1,2 Patrícia Martins1,2Vanessa Fraga3José Luís Ferraro4André Saraiva5Marlene Sousa5Hugo Parente6Catarina Soares6Ana Margarida Correia7Diogo Esperança Almeida7Sara Paiva Dinis8
Patrícia Martins1,2Vanessa Fraga3José Luís Ferraro4André Saraiva5Marlene Sousa5Hugo Parente6Catarina Soares6Ana Margarida Correia7Diogo Esperança Almeida7Sara Paiva Dinis8 Ana Sofia Pinto8Filipe Oliveira Pinheiro9
Ana Sofia Pinto8Filipe Oliveira Pinheiro9 Maria Seabra Rato9Tiago Beirão10Beatriz Samões10Bernardo Santos11Carolina Mazeda11Ana Teodósio Chícharo12
Maria Seabra Rato9Tiago Beirão10Beatriz Samões10Bernardo Santos11Carolina Mazeda11Ana Teodósio Chícharo12 Margarida Faria13Agna Neto13Maria Helena Lourenço14Luísa Brites15Marília Rodrigues15
Margarida Faria13Agna Neto13Maria Helena Lourenço14Luísa Brites15Marília Rodrigues15 Joana Silva-Dinis16
Joana Silva-Dinis16 João Madruga Dias17Filipe C. Araújo18Nádia Martins19Maura Couto19Ana Valido20
João Madruga Dias17Filipe C. Araújo18Nádia Martins19Maura Couto19Ana Valido20 Maria José Santos2,3
Maria José Santos2,3 Sofia Carvalho Barreira1,2
Sofia Carvalho Barreira1,2 João Eurico Fonseca1,2
João Eurico Fonseca1,2 Raquel Campanilho-Marques1,2
Raquel Campanilho-Marques1,2- 1Serviço de Reumatologia, Centro Hospitalar Universitário Lisboa Norte, Centro Académico de Medicina de Lisboa (CAML), Lisboa, Portugal
- 2Unidade de Investigação em Reumatologia, Instituto de Medicina Molecular, Faculdade de Medicina, Universidade de Lisboa, CAML, Lisboa, Portugal
- 3Serviço de Reumatologia, Hospital Garcia de Orta, Almada, Portugal
- 4Serviço de Reumatologia, Hospital Beatriz Ângelo, Loures, Portugal
- 5Serviço de Reumatologia, Centro Hospitalar Universitário de Coimbra, Coimbra, Portugal
- 6Serviço de Reumatologia, Unidade Local de Saúde do Alto Minho, Ponte de Lima, Portugal
- 7Serviço de Reumatologia, Hospital de Braga, Braga, Portugal
- 8Serviço de Reumatologia, Unidade Local de Saúde da Guarda, Guarda, Portugal
- 9Serviço de Reumatologia, Centro Hospitalar Universitário de São João, Porto, Portugal
- 10Serviço de Reumatologia, Centro Hospitalar de Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal
- 11Serviço de Reumatologia, Centro Hospitalar do Baixo Vouga, Aveiro, Portugal
- 12Serviço de Reumatologia, Centro Hospitalar Universitário do Algarve, Faro, Portugal
- 13Serviço de Reumatologia, Hospital Nélio Mendonça, Serviços de Saúde da Região Autónoma da Madeira, Funchal, Portugal
- 14Serviço de Reumatologia, Centro Hospitalar de Lisboa Ocidental, Lisboa, Portugal
- 15Serviço de Reumatologia, Centro Hospitalar de Leiria, Leiria, Portugal
- 16Serviço de Reumatologia, Centro Hospitalar Universitário de Lisboa Central, Lisboa, Portugal
- 17Serviço de Reumatologia, Centro Hospitalar de Médio Tejo, Tomar, Portugal
- 18Serviço de Reumatologia, Hospital CUF Cascais, Cascais, Portugal
- 19Serviço de Reumatologia, Centro Hospitalar Tondela-Viseu, Viseu, Portugal
- 20Serviço de Reumatologia, Unidade Local de Saúde do Litoral Alentejano, Santiago do Cacém, Portugal
Objectives: Idiopathic inflammatory myopathies (IIM) are a group of rare disorders that can affect the heart. This work aimed to find predictors of cardiac involvement in IIM.
Methods: Multicenter, open cohort study, including patients registered in the IIM module of the Rheumatic Diseases Portuguese Register (Reuma.pt/Myositis) until January 2022. Patients without cardiac involvement information were excluded. Myo(peri)carditis, dilated cardiomyopathy, conduction abnormalities, and/or premature coronary artery disease were considered.
Results: 230 patients were included, 163 (70.9%) of whom were females. Thirteen patients (5.7%) had cardiac involvement. Compared with IIM patients without cardiac involvement, these patients had a lower bilateral manual muscle testing score (MMT) at the peak of muscle weakness [108.0 ± 55.0 vs 147.5 ± 22.0, p=0.008] and more frequently had oesophageal [6/12 (50.0%) vs 33/207 (15.9%), p=0.009] and lung [10/13 (76.9%) vs 68/216 (31.5%), p=0.001] involvements. Anti-SRP antibodies were more commonly identified in patients with cardiac involvement [3/11 (27.3%) vs 9/174 (5.2%), p=0.026]. In the multivariate analysis, positivity for anti-SRP antibodies (OR 104.3, 95% CI: 2.5-4277.8, p=0.014) was a predictor of cardiac involvement, regardless of sex, ethnicity, age at diagnosis, and lung involvement. Sensitivity analysis confirmed these results.
Conclusion: Anti-SRP antibodies were predictors of cardiac involvement in our cohort of IIM patients, irrespective of demographical characteristics and lung involvement. We suggest considering frequent screening for heart involvement in anti-SRP-positive IIM patients.
Introduction
Idiopathic inflammatory myopathies (IIM) are rare systemic rheumatic disorders that primarily affect the muscle, joints, skin, and lungs in varying degrees. Although less often recognised, cardiovascular complications represent a major cause of death (1).
Myocarditis is a classic and severe but uncommon manifestation of IIM (2), while conduction abnormalities and diastolic dysfunction are more common (3, 4). Usually asymptomatic and not life-threatening, pericarditis is reported in 4-25% of IIM patients (5). Pulmonary hypertension appears to be mostly secondary to interstitial lung disease (ILD) and unlikely in the absence of antisynthetase antibodies (5). An increased incidence of accelerated atherosclerosis is also recognised in most rheumatic inflammatory diseases, including IIM (5).
Inflammation similar to that found in skeletal muscle is seen in both the heart muscle (3, 6) and the conduction system (6) in autopsies of IIM patients. Additionally, magnetic resonance imaging (MRI) studies showed an association between myocardial enhancement on MRI and diastolic dysfunction (7). These studies suggest that myocardial inflammation is a primary driver of heart dysfunction and conduction abnormalities in IIM.
Despite the recognition of several forms of cardiac involvement in IIM, specific guidelines for the screening, diagnosis, treatment, and follow-up are still lacking (8). An important first step towards the definition of optimal screening strategies is the identification of clinically useful predictors.
A large multicenter study reported that smoking was more prevalent in patients with cardiac involvement (9). However, smoking was also more frequent in patients with ILD, and no multivariate analysis was performed to evaluate whether it was an independent predictor of cardiac involvement, adjusted for the presence of ILD (9). It has also been reported that patients with anti-Mi2 antibodies more frequently have chest pain than IIM patients without any myositis-specific antibody (MSA), despite having no known cardiovascular disease (10). Finally, there have been reports, although sometimes contradictory (10, 11), of an association between cardiac involvement and the presence of anti-signal recognition particle (SRP) antibodies (12, 13). However, the only study with a large cohort that confirmed this association did not exclude the possible influence of other confounders (13).
Given the currently identified clinical unmet need, this work aimed to identify predictors of cardiac involvement in IIM patients.
Methods
This study is a multicenter cohort study, including patients registered in the IIM module of the Rheumatic Diseases Portuguese Register (14) (Reuma.pt/Myositis) from April 2019 until January 2022. The study is based on a retrospective analysis of prospectively collected data. Patients without information regarding the presence or absence of cardiac involvement were excluded. After data extraction, key missing data were identified and retrieved from the patients’ local clinical files.
Cardiac involvement was defined as myocarditis, pericarditis, dilated cardiomyopathy, conduction abnormalities, and/or premature coronary artery disease occurring due to IIM, according to the physician’s clinical judgement. Of note, cancer-associated myositis was defined as the onset of IIM within three years of a cancer diagnosis (15).
All patients were followed within the context of a Rheumatology department in a tertiary centre, and all cases of cardiac involvement were reviewed by the authors. The patients were screened for anti-nuclear antibodies (ANA) with indirect immunofluorescence assay (IIFA) on HEp-2 cells, MSA and myositis-associated autoantibodies (MAA) status by EUROLINE Autoimmune Inflammatory Myopathies 16 Ag (IgG) immunoblot.
Descriptive statistics were presented as median ± interquartile range for continuous variables and absolute and relative frequencies for categorical variables. Univariate analysis was performed using chi-square, Fisher’s exact, Mann-Whitney or t-test, as appropriate. Patients without cardiac involvement were used as a control group for this analysis. Predictors of cardiac involvement, adjusted for sex and age at diagnosis, were identified through binomial logistic regression modelling. The linearity of the continuous variables with respect to the logit of the dependent variable was assessed via the Box-Tidwell test. Correlated variables and cases with missing information were excluded from the multivariate analysis in order to fulfil all assumptions necessary to ensure the validity of the regression. Sensitivity analysis was performed by developing additional binomial logistic models. The statistical analysis was performed with SPSS/IBM version 23. The Bonferroni correction for multiple comparisons was applied to get α<0.05. Accordingly, in the univariate analysis, definite associations were defined by p<0.004 (marked with **) and likely associations by p<0.05 (marked with *).
The study was conducted according to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Centro Académico de Medicina de Lisboa (195/21). Included patients signed the Reuma.pt informed consent and data were fully anonymised throughout the entire research process. Reuma.pt is approved by the national data protection board (Comissão Nacional de Proteção de Dados) and by the Ethics Committee of all participating centres.
Results
In this study, 230 patients were included. Over two-thirds of the patients (N=163/230, 70.9%) were females. Most patients were Caucasians (N=105/117, 89.7%), but African (N=11/117, 9.4%) and Asian (N=1/117, 0.9%) ancestries were also represented. The median age at disease onset was 49.0 ± 25.0 years, and the median age at diagnosis was 50.1 ± 25.0 years. The median disease duration at the last follow-up was 4.8 ± 6.5 years.
Thirteen patients (5.7%) had cardiac involvement, some with more than one feature. Six patients (2.6%) had clinically evident myocarditis, five (2.2%) had conduction abnormalities, three (1.3%) had dilated cardiomyopathy, two (0.9%) had pericarditis, and two (0.9%) had premature coronary artery disease.
In our cohort, Caucasians were less likely to have cardiac involvement than other ethnicities (p<0.001**). Among patients with cardiac involvement, four (57.1%) were Caucasian, two (28.6%) had African ancestry, and one (14.3%) had Asian ancestry. On the other hand, patients without heart involvement were predominantly Caucasian (91.8%), and 8.2% had African ancestry. Regarding sex, age at diagnosis, and other demographic variables, as well as smoking and alcohol intake habits, there were no statistically significant differences between the groups (Table 1). Mortality was also not significantly different between both groups [1/13 (7.7%) vs 9/217 (4.1%), p=0.448]. Of note, patients with cardiac involvement had a significantly shorter disease duration than controls [1.4 ± 0.9 vs 6.1 ± 5.7 years, p=0.003**].
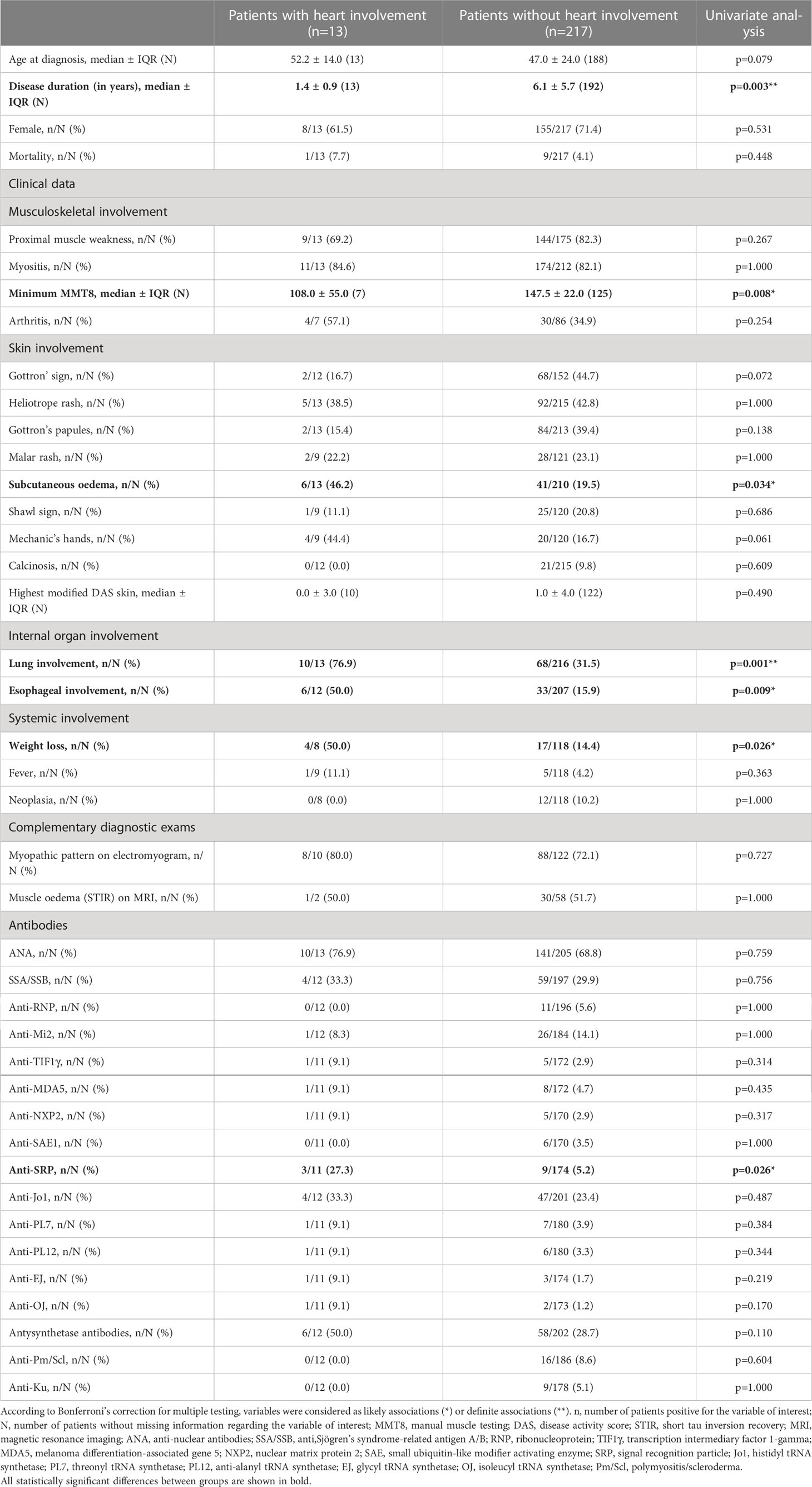
Table 1 Clinical and serological features of patients with and without cardiac involvement.
Patients with cardiac involvement had a lower bilateral manual muscle testing score (MMT) than controls at the peak of muscle weakness [108.0 ± 55.0 vs 147.5 ± 22.0, p=0.008*]. In addition, patients with cardiac involvement more frequently had elevated creatine kinase (CK) throughout follow-up than controls [12/12 (100.0%) vs 131/177 (74.0%), p=0.041*]. On the other hand, there were no significant differences concerning the highest serum CK level throughout follow-up [1522.5 ± 6053.0 vs 1300.0 ± 2555.0, p=0.866]. In addition, there were no statistically significant differences between groups for serum aldolase, myoglobin, or lactate dehydrogenase levels.
Patients with cardiac involvement more frequently had oesophageal [6/12 (50.0%) vs 33/207 (15.9%), p=0.009*] and lung [10/13 (76.9%) vs 68/216 (31.5%), p=0.001**] involvements compared to the control group. Skin involvement was globally similar between groups. However, subcutaneous oedema was more frequent in patients with cardiac involvement [6/13 (46.2%) vs 41/210 (19.5%), p=0.034*]. Additionally, weight loss was more frequent in patients with cardiac involvement [6/12 (50.0%) vs 33/207 (15.9%), p=0.009*]. Joint, gastrointestinal and vascular involvements and the prevalence of cancer-associated myositis, dysphonia, and fever were not statistically different between groups.
Anti-SRP [3/11 (27.3%) vs 9/174 (5.2%), p=0.026*] antibodies were more commonly identified in patients with cardiac involvement. There were no statistically significant differences between groups regarding antisynthetase antibodies (individually or as a group) or any other MSA or MAA.
In the multivariate analysis, anti-SRP antibodies positivity (OR 104.3, 95%CI: 2.5-4277.8, p=0.014) was identified as a predictor of cardiac involvement in IIM patients, regardless of sex, ethnicity, age at diagnosis, and lung involvement. The remaining variables were not statistically significant predictors of cardiac involvement. However, only 81 patients were included in this model due to the high level of missing data on the ethnicity variable. In order to overcome this issue, a sensitivity analysis was performed, excluding this variable from the model. A model without ethnicity included 159 patients and also endorsed anti-SRP antibodies as independent predictors of cardiac involvement in IIM patients (OR 6.0, 95%CI: 1.1-31.8, p=0.035). In the latter model, lung involvement was also a predictor of cardiac involvement (OR 5.0, 95%CI: 1.2-21.7, p=0.031). Additionally, we also confirmed anti-SRP association with cardiac involvement (OR 19.4, 95%CI: 1.8-206.0, p=0.014) in a multivariate model with sex, age at diagnosis, lung involvement and minimum MMT8 as covariates. In this latter model, the remaining variables were not statistically significant predictors of cardiac involvement. A model including both ethnicity and minimum MMT8 was not used because the high number of patients missing data on these two variables leads to a statistical model with an overwhelmingly small number of included patients.
Discussion
According to the literature, cardiovascular involvement in IIM patients ranges from 6-75%, depending on selection criteria, the definition of cardiovascular involvement, and the methods used to detect it (4, 16). The prevalence of cardiac involvement in our cohort was on the lower end of this spectrum. However, we should emphasise that we only considered cardiac involvement, excluding other types of vascular involvement (Table 2). This was a critical methodological decision that was pre-defined in the project protocol because vascular involvement is very loosely defined and could include manifestations such as Raynaud’s phenomenon, which is very prevalent in IIM and was not the focus of our work. Additionally, our study used real-world data from a national registry, so we cannot ensure that all patients were systematically screened for extramuscular involvement, which might have allowed for the underdiagnosing of subclinical cardiac involvement. Of note, all patients were followed in Rheumatology departments in tertiary centres. The aforementioned factors may have contributed to the arguably low prevalence of cardiac involvement in the Reuma.pt/Myositis cohort. Another factor that may have contributed is the recently improved IIM diagnostic capacity, for which we have a set of autoantibodies that help diagnose patients early in their disease course. Considering these biomarkers are recent, they were probably not available at the time of the previous studies regarding the prevalence of cardiac involvement in IIM. Therefore, our cohort may include more patients diagnosed and treated early who did not develop clinically apparent heart disease.

Table 2 Characteristics of the patients with cardiac involvement.
MSA and MAA have a prognostic influence on IIM, and different autoantibodies have been associated with different clinical characteristics (17–19). Although these associations have been well-established for lung, skin, or muscular manifestations, the same does not apply to cardiovascular manifestations.
There is some evidence in the previously published literature that there may be an association between anti-SRP and cardiac involvement in IIM, particularly cardiac disease-related symptoms and electrocardiographic and echocardiogram changes (12, 13). However, this association has been inconsistently reported (10, 11), with some studies suggesting a link between the positivity for this antibody and ILD but not cardiac manifestations (20). Recent evidence suggests that anti-SRP antibodies may have a pathogenic role targeting skeletal muscle (21, 22), with muscle fibre necrosis being confirmed in mice with transferred anti-SRP (23). Whether this contributes to cardiac involvement remains unclear. This background information helped recognise the likely association between anti-SRP antibodies and cardiac involvement in the univariate analysis as meaningful. Furthermore, the possibility of ILD being a confounder for this association (20) highlighted the need for including lung involvement in any multivariate analyses built to test anti-SRP association with cardiac involvement. In our cohort, anti-SRP antibodies were independently associated with cardiac involvement, regardless of sex, ethnicity, age at diagnosis, and lung involvement. This association was challenged by different multivariate models but was highly consistent in all of them.
This work supports previous reports of the association between the positivity of anti-SRP antibodies and cardiac involvement in IIM patients. Moreover, we attested to this association independently of lung involvement and further confirmed it through sensitivity analysis. These results were obtained in a South European cohort with a large representation of Caucasian patients, and additional validation in multiethnic cohorts is needed. Further research using large international cohorts, such as MyoNet, may potentially identify other clinical biomarkers that can help stratify the risk of cardiac involvement in IIM patients. In the meantime, considering our findings, we suggest a closer screening for heart disease in anti-SRP-positive patients.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of Centro Académico de Medicina de Lisboa (195/21). The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors contributed to the follow-up and recruitment of patients as well as data insertion. All authors re-evaluated their own cases of cardiac involvement. ED, MB and RC-M developed the project. MB and ED did the statistical analysis and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dankó K, Ponyi A, Constantin T, Borgulya G, Szegedi G. Long-term survival of patients with idiopathic inflammatory myopathies according to clinical features: a longitudinal study of 162 cases. Med (Baltimore). (2004) 83(1):35–42. doi: 10.1097/01.md.0000109755.65914.5e
2. Lundberg IE. Cardiac involvement in autoimmune myositis and mixed connective tissue disease. Lupus. (2005) 14(9):708–12. doi: 10.1191/0961203305lu2205oa
3. Denbow CE, Lie JT, Tancredi RG, Bunch TW. Cardiac involvement in polymyositis: a clinicopathologic study of 20 autopsied patients. Arthritis Rheumatol (1979) 22(10):1088–92. doi: 10.1002/art.1780221007
4. Gottdiener JS, Sherber HS, Hawley RJ, Engel WK. Cardiac manifestations in polymyositis. Am J Cardiol (1978) 41(7):1141–9. doi: 10.1016/0002-9149(78)90871-8
5. Schwartz T, Diederichsen LP, Lundberg IE, Sjaastad I, Sanner H. Cardiac involvement in adult and juvenile idiopathic inflammatory myopathies. RMD Open (2016) 2(2):e000291. doi: 10.1136/rmdopen-2016-000291
6. Haupt HM, Hutchins GM. The heart and cardiac conduction system in polymyositis-dermatomyositis: a clinicopathologic study of 16 autopsied patients. Am J Cardiol (1982) 50(5):998–1006. doi: 10.1016/0002-9149(82)90408-8
7. Diederichsen LP, Simonsen JA, Diederichsen AC, Hvidsten S, Hougaard M, Junker P, et al. Cardiac abnormalities in adult patients with polymyositis or dermatomyositis as assessed by noninvasive modalities. Arthritis Care Res (Hoboken). (2016) 68(7):1012–20. doi: 10.1002/acr.22772
8. Fasano S, Iacono D, Riccardi A, Ciccia F, Valentini G. The role of aspirin in the primary prevention of accelerated atherosclerosis in systemic autoimmune rheumatic diseases. Rheumatol (Oxford). (2020) 59(12):3593–602. doi: 10.1093/rheumatology/keaa335
9. Lilleker JB, Vencovsky J, Wang G, Wedderburn LR, Diederichsen LP, Schmidt J, et al. The EuroMyositis registry: an international collaborative tool to facilitate myositis research. Ann Rheum Dis (2018) 77(1):30–9. doi: 10.1136/annrheumdis-2017-211868
10. Hengstman GJD, Brouwer R, Egberts WTMV, Seelig HP, Jongen PJ, van Venrooij WJ, et al. Clinical and serological characteristics of 125 Dutch myositis patients. myositis specific autoantibodies aid in the differential diagnosis of the idiopathic inflammatory myopathies. J Neurol (2002) 249(1):69–75. doi: 10.1007/pl00007850
11. Kao AH, Lacomis D, Lucas M, Fertig N, Oddis CV. Anti-signal recognition particle autoantibody in patients with and patients without idiopathic inflammatory myopathy. Arthritis Rheumatol (2004) 50(1):209–15. doi: 10.1002/art.11484
12. Love LA, Leff RL, Fraser DD, Targoff IN, Dalakas M, Plotz PH, et al. A new approach to the classification of idiopathic inflammatory myopathy: myositis-specific autoantibodies define useful homogeneous patient groups. Med (Baltimore). (1991) 70(6):360–74. doi: 10.1097/00005792-199111000-00002
13. Betteridge Z, Tansley S, Shaddick G, Chinoy H, Cooper RG, New RP, et al. Frequency, mutual exclusivity and clinical associations of myositis autoantibodies in a combined European cohort of idiopathic inflammatory myopathy patients. J Autoimmun (2019) 101:48–55. doi: 10.1016/j.jaut.2019.04.001
14. Canhão H, Faustino A, Martins F, Fonseca JE. Reuma.pt - the rheumatic diseases portuguese register. Acta Reumatol Port (2011) 36(1):45–56.
15. Chinoy H, Fertig N, Oddis CV, Ollier WER, Cooper RG. The diagnostic utility of myositis autoantibody testing for predicting the risk of cancer-associated myositis. Ann Rheum Dis (2007) 66(10):1345–9. doi: 10.1136/ard.2006.068502
16. Gonzalez-Lopez L, Gamez-Nava JI, Sanchez L, Rosas E, Suarez-Almazor M, Cardona-Muñoz C, et al. Cardiac manifestations in dermato-polymyositis. Clin Exp Rheumatol (1996) 14(4):373–9.
17. Damoiseaux J, Vulsteke J-B, Tseng C-W, Platteel ACM, Piette Y, Shovman O, et al. Autoantibodies in idiopathic inflammatory myopathies: Clinical associations and laboratory evaluation by mono- and multispecific immunoassays. Autoimmun Rev (2019) 18(3):293–305. doi: 10.1016/j.autrev.2018.10.004
18. Cavagna L, Castañeda S, Sciré C, Gonzalez-Gay MA. Antisynthetase syndrome or what else? different perspectives indicate the need for new classification criteria. Ann Rheum Dis (2018) 77(8):e50. doi: 10.1136/annrheumdis-2017-212368
19. Martins P, Dourado E, Melo AT, et al. Clinical characterisation of a multicentre nationwide cohort of patients with antisynthetase syndrome. ARP Rheumatol (2022) 1(ARP Rheumatology, no3 2022):190–6.
20. Hengstman GJD, ter Laak HJ, Vree Egberts WTM, Lundberg IE, Moutsopoulos HM, Vencovsky J, et al. Anti-signal recognition particle autoantibodies: marker of a necrotising myopathy. Ann Rheum Dis (2006) 65(12):1635–8. doi: 10.1136/ard.2006.052191
21. Ma X, Bu B-T. Anti-SRP immune-mediated necrotizing myopathy: A critical review of current concepts. Front Immunol (2022) 13:1019972. doi: 10.3389/fimmu.2022.1019972
22. Arouche-Delaperche L, Allenbach Y, Amelin D, Preusse C, Mouly V, Mauhin W, et al. Pathogenic role of anti-signal recognition protein and anti-3-Hydroxy-3-methylglutaryl-CoA reductase antibodies in necrotizing myopathies: Myofiber atrophy and impairment of muscle regeneration in necrotizing autoimmune myopathies. Ann Neurol (2017) 81(4):538–48. doi: 10.1002/ana.24902
Keywords: idiopathic inflammatory myopathies, cardiac involvement, myocarditis, risk factors, biomarkers, predictors
Citation: Bandeira M, Dourado E, Melo AT, Martins P, Fraga V, Ferraro JL, Saraiva A, Sousa M, Parente H, Soares C, Correia AM, Almeida DE, Dinis SP, Pinto AS, Oliveira Pinheiro F, Rato MS, Beirão T, Samões B, Santos B, Mazeda C, Chícharo AT, Faria M, Neto A, Lourenço MH, Brites L, Rodrigues M, Silva-Dinis J, Dias JM, Araújo FC, Martins N, Couto M, Valido A, Santos MJ, Barreira SC, Fonseca JE and Campanilho-Marques R (2023) Predictors of cardiac involvement in idiopathic inflammatory myopathies. Front. Immunol. 14:1146817. doi: 10.3389/fimmu.2023.1146817
Received: 17 January 2023; Accepted: 24 February 2023;
Published: 08 March 2023.
Edited by:
Chris Wincup, King’s College Hospital NHS Foundation Trust, United KingdomReviewed by:
Eleni Tiniakou, Johns Hopkins University, United StatesNatasa Isailovic, Humanitas University, Italy
James B. Lilleker, The University of Manchester, United Kingdom
Corinna Preuße, Charité Universitätsmedizin Berlin, Germany
Copyright © 2023 Bandeira, Dourado, Melo, Martins, Fraga, Ferraro, Saraiva, Sousa, Parente, Soares, Correia, Almeida, Dinis, Pinto, Oliveira Pinheiro, Rato, Beirão, Samões, Santos, Mazeda, Chícharo, Faria, Neto, Lourenço, Brites, Rodrigues, Silva-Dinis, Dias, Araújo, Martins, Couto, Valido, Santos, Barreira, Fonseca and Campanilho-Marques. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matilde Bandeira, MjcyMTlAY2hsbi5taW4tc2F1ZGUucHQ=
†These authors have contributed equally to this work and share first authorship
‡ORCID: Matilde Bandeira, orcid.org/0000-0001-8312-4532
Eduardo Dourado, orcid.org/0000-0003-2186-2833