 Antonio Vitale1,2†
Antonio Vitale1,2† Valeria Caggiano1,2†
Valeria Caggiano1,2† Abdurrahman Tufan3
Abdurrahman Tufan3 Gaafar Ragab4,5
Gaafar Ragab4,5 Ezgi Deniz Batu6
Ezgi Deniz Batu6 Piero Portincasa7
Piero Portincasa7 Emma Aragona8
Emma Aragona8 Jurgen Sota1,2
Jurgen Sota1,2 Giovanni Conti9
Giovanni Conti9 Amato De Paulis10,11
Amato De Paulis10,11 Donato Rigante12,13Alma Nunzia Olivieri14Ali Şahin15
Donato Rigante12,13Alma Nunzia Olivieri14Ali Şahin15 Francesco La Torre16
Francesco La Torre16 Giuseppe Lopalco17Marco Cattalini18
Giuseppe Lopalco17Marco Cattalini18 Maria Cristina Maggio19
Maria Cristina Maggio19 Antonella Insalaco20
Antonella Insalaco20 Petros P. Sfikakis21
Petros P. Sfikakis21 Elena Verrecchia13,22
Elena Verrecchia13,22 Derya Yildirim3Hamit Kucuk3
Derya Yildirim3Hamit Kucuk3 Riza Can Kardas3Ahmed Hatem Laymouna4
Riza Can Kardas3Ahmed Hatem Laymouna4 Mahmoud Ghanema4
Mahmoud Ghanema4 Moustafa Ali Saad4
Moustafa Ali Saad4 Seher Sener6
Seher Sener6 Hulya Ercan Emreol6
Hulya Ercan Emreol6 Seza Ozen6
Seza Ozen6 Nour Jaber7
Nour Jaber7 Mohamad Khalil7
Mohamad Khalil7 Agostino Di Ciaula7
Agostino Di Ciaula7 Carla Gaggiano1,2Giuseppe Malizia8Andrea Affronti8
Carla Gaggiano1,2Giuseppe Malizia8Andrea Affronti8 Serena Patroniti9
Serena Patroniti9 Meri Romeo9Jessica Sbalchiero1,2Francesca Della Casa10
Meri Romeo9Jessica Sbalchiero1,2Francesca Della Casa10 Ilaria Mormile10
Ilaria Mormile10 Sara Silvaroli23Maria Francesca Gicchino14Neşe Çabuk Çelik15Maria Tarsia2,24
Sara Silvaroli23Maria Francesca Gicchino14Neşe Çabuk Çelik15Maria Tarsia2,24 Anastasios Karamanakos25
Anastasios Karamanakos25 José Hernández-Rodríguez26
José Hernández-Rodríguez26 Paola Parronchi27
Paola Parronchi27 Daniela Opris-Belinski28Patrizia Barone29
Daniela Opris-Belinski28Patrizia Barone29 Andreas Recke30,31Stefania Costi32
Andreas Recke30,31Stefania Costi32 Paolo Sfriso33
Paolo Sfriso33 Henrique A. Mayrink Giardini34Stefano Gentileschi1,2Ewa Wiesik-Szewczyk35
Henrique A. Mayrink Giardini34Stefano Gentileschi1,2Ewa Wiesik-Szewczyk35 Ibrahim Vasi3
Ibrahim Vasi3 Roberta Loconte16
Roberta Loconte16 Karina Jahnz-Różyk35
Karina Jahnz-Różyk35 Eduardo Martín-Nares36Jiram Torres-Ruiz36Alberto Cauli37Alessandro Conforti38
Eduardo Martín-Nares36Jiram Torres-Ruiz36Alberto Cauli37Alessandro Conforti38 Giacomo Emmi39,40
Giacomo Emmi39,40 Francesca Li Gobbi41Giovanni Rosario Biasi1,2Riccardo Terribili1,2
Francesca Li Gobbi41Giovanni Rosario Biasi1,2Riccardo Terribili1,2 Piero Ruscitti42
Piero Ruscitti42 Emanuela Del Giudice43
Emanuela Del Giudice43 Samar Tharwat44,45
Samar Tharwat44,45 Antonio Luca Brucato46
Antonio Luca Brucato46 Benson Ogunjimi47,48,49,50Andrea Hinojosa-Azaola36Alberto Balistreri51
Benson Ogunjimi47,48,49,50Andrea Hinojosa-Azaola36Alberto Balistreri51 Claudia Fabiani2,52Bruno Frediani1,2
Claudia Fabiani2,52Bruno Frediani1,2 Luca Cantarini1,2*
Luca Cantarini1,2*- 1Department of Medical Sciences, Surgery and Neurosciences, Research Center of Systemic Autoinflammatory Diseases and Behçet’s Disease Clinic, University of Siena, Siena, Italy
- 2Azienda Ospedaliero-Universitaria Senese [European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA) Center], Siena, Italy
- 3Gazi University Hospital, Department of Internal Medicine, Division of Rheumatology, Ankara, Türkiye
- 4Internal Medicine Department, Rheumatology and Clinical Immunology Unit, Faculty of Medicine, Cairo University, Giza, Egypt
- 5Faculty of Medicine, Newgiza University, 6th of October City, Giza, Egypt
- 6Division of Pediatric Rheumatology, Department of Pediatrics, Hacettepe University School of Medicine, Ankara, Türkiye
- 7Clinica Medica “A. Murri”, Division of Internal Medicine, Department of Precision and Regenerative Medicine and Ionian Area (DiMePre-J), University of Bari Aldo Moro, Bari, Italy
- 8Division of Gastroenterology, Ospedali Riuniti Villa Sofia-Vincenzo Cervello, Palermo, Italy
- 9Pediatric Nephrology and Rheumatology Unit, Azienda Ospedaliera Universitaria (AOU), “G. Martino”, Messina, Italy
- 10Department of Translational Medical Sciences, Section of Clinical Immunology, University of Naples Federico II, Naples, Italy
- 11Center for Basic and Clinical Immunology Research (CISI), WAO Center of Excellence, University of Naples Federico II, Naples, Italy
- 12Department of Life Sciences and Public Health, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
- 13Rare Diseases and Periodic Fevers Research Center, Università Cattolica del Sacro Cuore, Rome, Italy
- 14Department of Woman, Child and of General and Specialized Surgery, University of Campania “Luigi Vanvitelli”, Naples, Italy
- 15Division of Rheumatology, Department of Internal Medicine, Sivas Cumhuriyet University Medical Faculty, Sivas, Türkiye
- 16Department of Pediatrics, Pediatric Rheumatology Center, Giovanni XXIII Pediatric Hospital, University of Bari, Bari, Italy
- 17Department of Precision and Regenerative Medicine and Ionian Area (DiMePRe-J) Policlinic Hospital, University of Bari, Bari, Italy
- 18Pediatrics Clinic, University of Brescia and Spedali Civili of Brescia, [European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA) Center], Brescia, Italy
- 19University Department of Health Promotion, Mother and Child Care, Internal Medicine and Medical Specialties (PROMISE) “G. D’Alessandro”, University of Palermo, Palermo, Italy
- 20Division of Rheumatology, Ospedale Pediatrico Bambino Gesù, IRCCS [European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA) Center], Rome, Italy
- 21Joint Academic Rheumatology Program, Medical School, National and Kapodistrian University of Athens, [European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA) Center], Athens, Greece
- 22Department of Aging, Neurological, Orthopedic and Head and Neck Sciences, Fondazione Policlinico Universitario Agostino Gemelli Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy
- 23Department of Pediatric Surgery, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
- 24Clinical Pediatrics, Department of Molecular Medicine and Development, University of Siena, Siena, Italy
- 25Department of Rheumatology, “Evangelismos” General Hospital, Athens, Greece
- 26Department of Autoimmune Diseases, Institut d’Investigacions Biomèdiques August Pi I Sunyer (IDIBAPS), Hospital Clínic of Barcelona [European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA) Center], University of Barcelona, Barcelona, Spain
- 27Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy
- 28Rheumatology and Internal Medicine Department, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania
- 29Pediatric Rheumatology Unit, Department of integrated Maternal-Child and Reproduction Activity AOU “Policlinico-San Marco”, Catania, Italy
- 30Department of Dermatology, Allergology and Venerology, University Hospital Schleswig-Holstein, Lübeck, Germany
- 31Autoinflammatory and Autoimmune Diseases (RITA) Center, European Reference Network (ERN) for Rare Immunodeficiency, Lübeck, Germany
- 32Department of Clinical Sciences and Community Health, Research Center for Adult and Pediatric Rheumatic Diseases, University of Milan, Milan, Italy
- 33Rheumatology Unit, Department of Medicine, University of Padua, Padua, Italy
- 34Rheumatology Division, Faculdade de Medicina, Hospital das Clínicas, Universidade de São Paulo, São Paulo, Brazil
- 35Department of Internal Medicine, Pneumonology, Allergology and Clinical Immunology, Central Clinical Hospital of the Ministry of National Defense, Military Institute of Medicine, National Research Institute, Warsaw, Poland
- 36Department of Immunology and Rheumatology, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 37Rheumatology Unit, Department of Medical Sciences, University and AOU of Cagliari, Cagliari, Italy
- 38Ospedale San Paolo di Civitavecchia, U.O. Medicina Generale, ASL Roma 4, Civitavecchia, Rome, Italy
- 39Department of Medical, Surgical and Health Sciences, University of Trieste, Italy, and Clinical Medicine and Rheumatology Unit, Cattinara University Hospital, Trieste, Italy
- 40Centre for Inflammatory Diseases, Department of Medicine, Monash Medical Centre, Monash University, Clayton, VIC, Australia
- 41Rheumatology Unit, Hospital S. Giovanni di Dio, Azienda USL-Toscana Centro, Florence, Italy
- 42Rheumatology Unit, Department of Biotechnological and Applied Clinical Sciences, University of L’Aquila, L’Aquila, Italy
- 43Pediatric and Neonatology Unit, Department of Maternal Infantile and Urological Sciences, Sapienza University of Rome, Latina, Italy
- 44Rheumatology and Immunology Unit, Internal Medicine Department, Mansoura University, Mansoura, Egypt
- 45Department of Internal Medicine, Faculty of Medicine, Horus University, New Damietta, Egypt
- 46Department of Biomedical and Clinical Sciences, Fatebenefratelli Hospital, Università di Milano, Milan, Italy
- 47Antwerp Unit for Data Analysis and Computation in Immunology and Sequencing, University of Antwerp, Antwerp, Belgium
- 48Antwerp Center for Translational Immunology and Virology, Vaccine and Infectious Disease Institute, University of Antwerp, Antwerp, Belgium
- 49Department of Pediatrics, Antwerp University Hospital, Antwerp, Belgium
- 50Center for Health Economics Research and Modeling Infectious Diseases, Vaccine and Infectious Disease Institute, University of Antwerp, Antwerp, Belgium
- 51Bioengineering and Biomedical Data Science Lab, Department of Medical Biotechnologies, University of Siena, Siena, Italy
- 52Ophthalmology Unit, Department of Medicine, Surgery and Neurosciences, University of Siena, Siena, Italy
Objective: Inflammation has been associated with an increased risk for cancer development, while innate immune system activation could counteract the risk for malignancies. Familial Mediterranean fever (FMF) is a severe systemic inflammatory condition and also represents the archetype of innate immunity deregulation. Therefore, the aim of this study is to investigate the risk for cancer development in FMF.
Methods: The risk ratio (RR) for malignancies was separately compared between FMF patients and fibromyalgia subjects, Still’s disease patients and Behçet’s disease patients. Clinical variables associated with cancer development in FMF patients were searched through binary logistic regression.
Results: 580 FMF patients and 102 fibromyalgia subjects, 1012 Behçet’s disease patients and 497 Still’s disease patients were enrolled. The RR for the occurrence of malignant neoplasms was 0.26 (95% Confidence Interval [CI.] 0.10-0.73, p=0.006) in patients with FMF compared to fibromyalgia subjects; the RR for the occurrence of malignant cancer was 0.51 (95% CI. 0.23-1.16, p=0.10) in FMF compared to Still’s disease and 0.60 (95% CI. 0.29-1.28, p=0.18) in FMF compared to Behçet’s disease. At logistic regression, the risk of occurrence of malignant neoplasms in FMF patients was associated with the age at disease onset (β1 = 0.039, 95% CI. 0.001-0.071, p=0.02), the age at the diagnosis (β1 = 0.048, 95% CI. 0.039-0.085, p=0.006), the age at the enrolment (β1 = 0.05, 95% CI. 0.007-0.068, p=0.01), the number of attacks per year (β1 = 0.011, 95% CI. 0.001- 0.019, p=0.008), the use of biotechnological agents (β1 = 1.77, 95% CI. 0.43-3.19, p=0.009), the use of anti-IL-1 agents (β1 = 2.089, 95% CI. 0.7-3.5, p=0.002).
Conclusions: The risk for cancer is reduced in Caucasic FMF patients; however, when malignant neoplasms occur, this is more frequent in FMF cases suffering from a severe disease phenotype and presenting a colchicine-resistant disease.
Introduction
Familial Mediterranean fever (FMF) represents the archetype of autoinflammatory diseases. It is caused by mutations in the MEFV gene, which encodes for the pyrin protein, an essential component of the NLRP3-inflammasome, an intracellular multiprotein complex responsible for the activation of the pro-inflammatory cytokines interleukin (IL)-1 and IL-18 (1, 2). It is clinically characterized by recurrent fever attacks typically lasting less than 72 hours and variably associated with serositis, severe abdominal pain (owing to peritonitis), arthritis, and erysipela-like erythema. However, many other tissues may be involved with inflammation leading to different phenotypes (3). Inflammatory attacks are associated with a pronounced increase in the laboratory inflammatory markers, especially serum amyloid A (4). Amyloidosis develops in not adequately treated patients over time (5).
Inflammation may be highly linked to cancer development, while IL-1 has been found to be correlate with the advanced and aggressive nature of some neoplasms (6). In this perspective, FMF should be burdened by an increased risk for malignancies. On the other side, NLRP3 inflammasome–mediated inflammatory cytokines may have a protective role in some cancers, including colorectal cancer, hepatocellular carcinoma and melanoma (7). Therefore, assuming an increased risk of cancer in FMF patients based solely on the inflammatory nature of this disease could be an incorrect hypothesis. Actually, some studies based on national enrolment have disclosed a reduced risk for cancer in FMF patients (8–10). The present study is thought to investigate this condition at a supranational level using data collected from the international AutoInflammatory Disease Alliance (AIDA) Network registry dedicated to monogenic autoinflammatory diseases (11). This approach aims to overcome influences related to the living environment and different social behavior. In addition, this study is also thought to assess the risk for cancer compared to diseased controls with other systemic inflammatory disorders.
Material and methods
Data related to FMF patients, including demographics, clinical and laboratory aspects, therapeutic information and neoplasms history, were drawn from the international AIDA Network registry dedicated to monogenic autoinflammatory diseases (11).
Patients with Still’s disease and Behçet’s disease were included as controls affected by different systemic inflammatory disorders and their data were drawn from the international AIDA Network registries dedicated to Still’s disease and Behçet’s disease, respectively (12, 13). Consecutive fibromyalgia subjects not affected by other systemic inflammatory conditions were chosen as control group, taking care to include patients of different ethnicities, and matching for the sex with FMF patients. This choice was determined by the need to compare patients with FMF to individuals affected by a clinical condition completely devoid of inflammatory disorders.
The follow-up period ranged from the start of FMF, Still’s disease and Behçet’s disease to the last visit collected in the AIDA Network registries (up to January 2024). Consequently, this is an ambidirectional cohort study.
The primary aim of the study was to describe the frequency of malignant neoplasms in FMF patients and then to compare the risk versus fibromyalgia subjects, Still’s disease and Behçet’s disease. The secondary aim was to assess variables associated with the risk of neoplasms in the subgroup of FMF patients developing malignant cancer.
The endpoint of the study was the occurrence of malignant neoplasms during the whole follow-up period; the occurrence of neoplasms was reported in the AIDA network registries according to the international classification of diseases, version 10 (ICD-10).
Inclusion criteria for patients with FMF consisted of the identification of at least one pathogenic or likely pathogenic MEFV variant together with the fulfillment of the Eurofever classification criteria for FMF (14); alternatively, patients had to fulfill clinical diagnostic criteria for FMF proposed by Livneh et al. (15). Pathogenicity of MEFV variants was derived from Infevers, an online database for autoinflammatory mutations. Copyright. Available at https://infevers.umai-montpellier.fr/ (16–19).
Still’s disease patients fulfilled the classification criteria proposed by Yamaguchi et al. (20) and/or Fautrel et al. (21), while Behçet’s disease fulfilled the International Study Group criteria (22) and/or the International Criteria for Behçet’s disease (23). Classification criteria for pediatric Behçet’s disease were also applied to patients aged < 16 years (24). Fibromyalgia was classified according to either the American College of Rheumatology 1990 Criteria or American College of Rheumatology preliminary diagnostic criteria proposed by Wolfe et al. (25).
All patients included in this study gave their informed consent to participate. The study protocol was conformed to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the Azienda Ospedaliero-Universitaria Senese, Siena, Italy in June 2019 (Ref. N. 14951).
Data analysis included the following descriptive statistics: sample sizes, percentages, frequency counts, mean, median, standard deviations and interquartile range calculations. The relative risk (RR) for cancer development between study groups and the corresponding 95% confidence intervals (95% CI.) were calculated by using the Episheet software considering the number of patients with cancer (cases) and the total number of observations among patients with FMF (exposed group) and controls (unexposed groups) (26). The Chi-square test or the Fisher exact test were used for pairwise comparisons of qualitative data; the Kruskall-Wallis test was used for multiple comparisons of quantitative data after having proved their non-gaussian distribution with the Shapiro-Wilk test. The t-test or the Mann-Whitney U test were used, as required, for investigating pairwise comparisons for quantitative data and for post-hoc analysis; in this last case, Bonferroni correction was also applied. Univariate binomial logistic regression was used to investigate any association between neoplasm development and the following variables: age at disease onset, age at diagnosis, age at enrollment, disease duration at diagnosis, tabagism, specific MEFV mutations, amyloidosis development, signs and symptoms during fever attacks (thoracic pain, pericarditis, pleuritis, abdominal pain, arthritis, spondylarthritis, skin manifestations, lymphadenopathy), colchicine treatment duration, use of biotechnological agents and use of anti-IL-1 agents. The β0 and β1 estimates were provided from logistic regressions with the exponential of β0 corresponding to the odds of cancer development when the variable is equal to zero. The corresponding RR were also calculated using the inverse-logit function of (β0 + β1) divided by the inverse-logit function of β0. Two-tailed statistical analyses were conducted, with a type I error set at 0.05 (p < 0.05), using RStudio software version 4.3.0.
Results
In total, 580 FMF patients were enrolled; their demographic and clinical data are summarized in Tables 1, 2. In addition, 102 fibromyalgia subjects, 1012 Behçet’s disease patients and 497 Still’s disease patients were enrolled as controls.
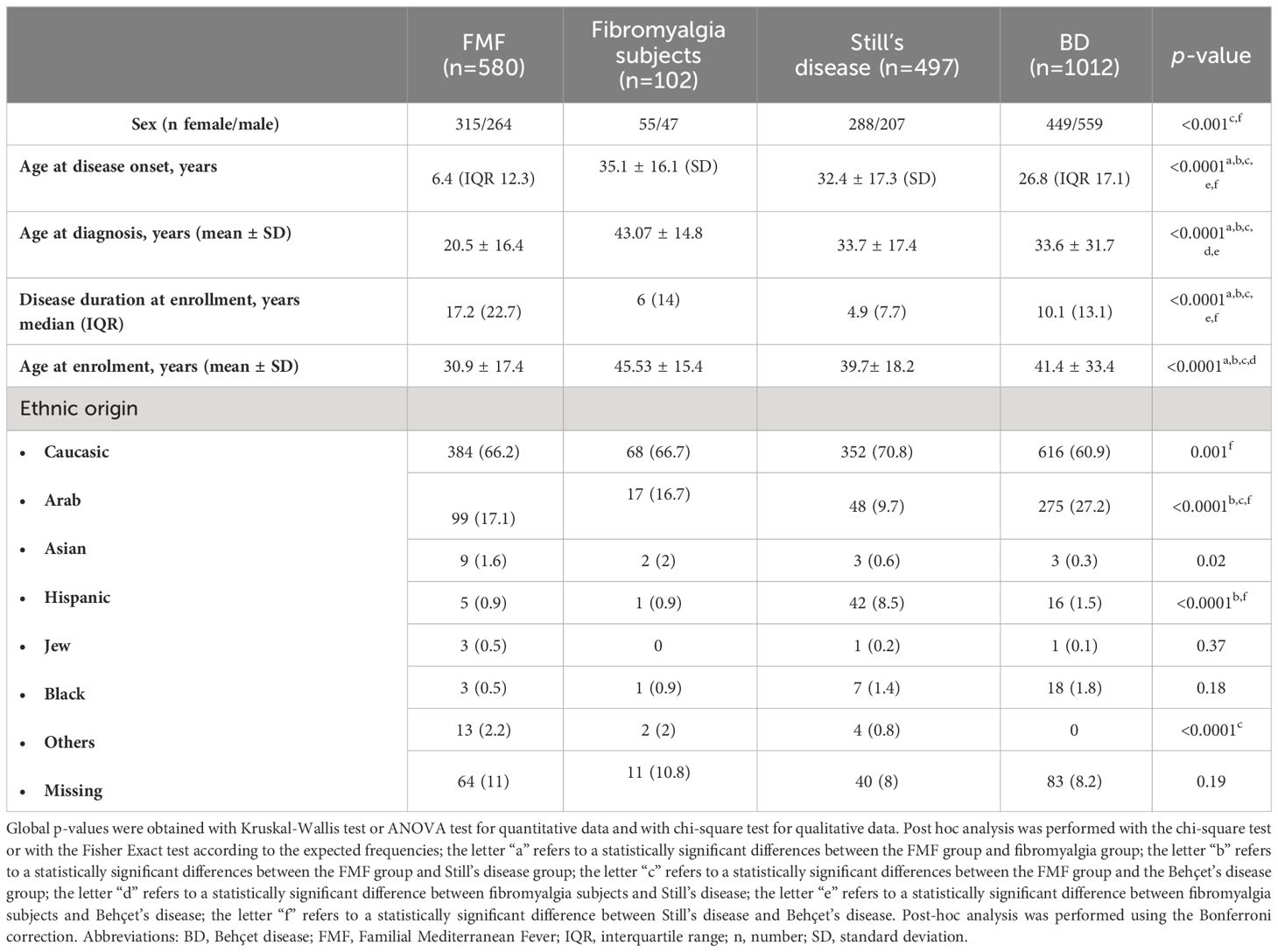
Table 1 Demographics of patients enrolled, distinguished according to the specific diseases they suffer from.
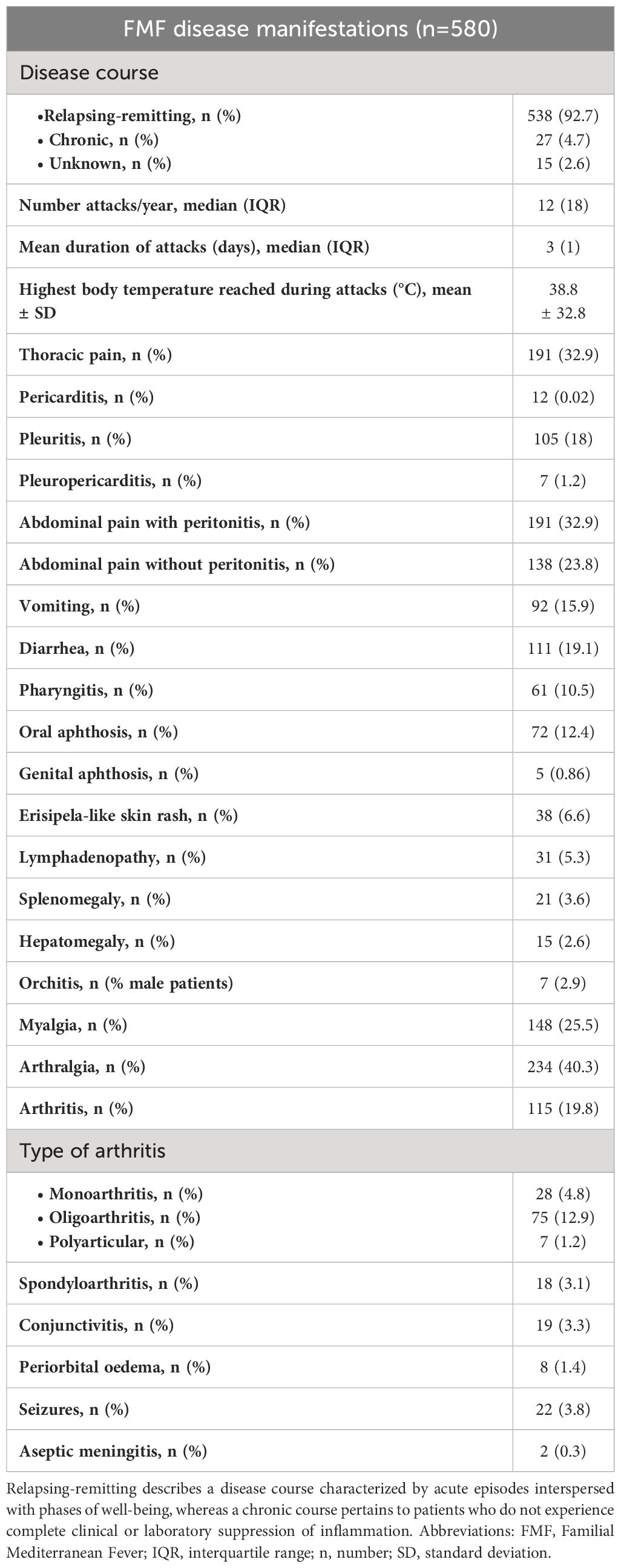
Table 2 Frequency of clinical features associated to entire cohort of patients affected by Familial Mediterranean Fever (FMF) disease.
In 14 (2.4%) FMF patients the following neoplasms were reported: monoclonal gammopathy (n=3), melanoma (n=3), thyroid carcinoma (n=3), basal cell carcinoma of skin (n=2), a benign neoplasm of transverse colon, a malignant neoplasm of testis, an adenocarcinoma of the cervix, one angiomyolipoma, one hepatic hemangioma, one uterine myoma, one prolactinoma. Eight neoplasms could be considered benign (monoclonal gammopathy, angiomyolipoma, hepatic hemangioma, uterine myoma, prolactinoma, in addition to the benign neoplasm of transverse colon). Three out of the 14 patients with tumors suffered from 5 different neoplasms; in particular, 2 patients with monoclonal gammopathy also suffered from other neoplasms (basal cell carcinoma and thyroid carcinoma); the patient with benign neoplasm of transverse colon also suffered from melanoma. Demographic, clinical and therapeutic details from the 9 patients with malignancies are reported in Table 3.
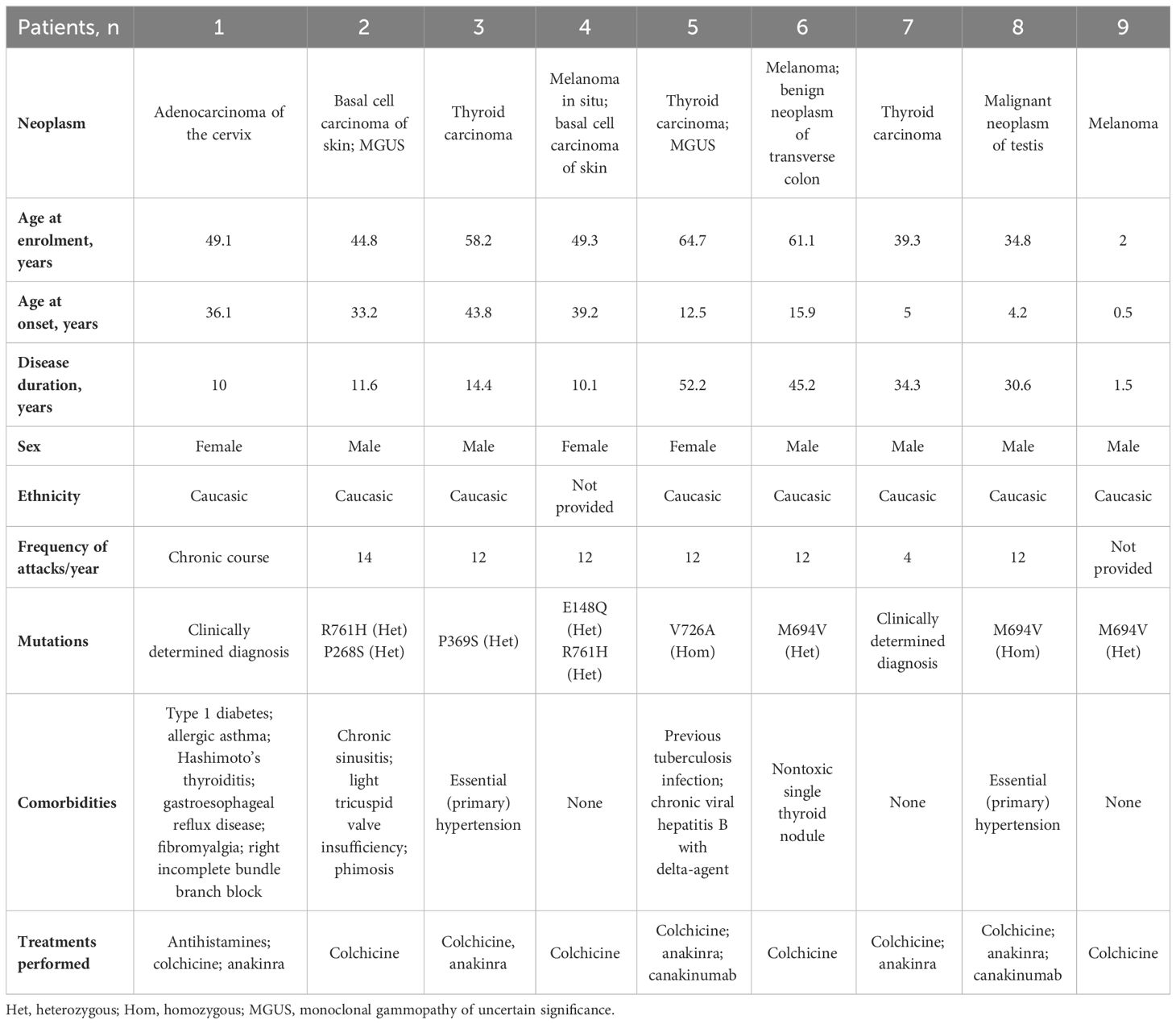
Table 3 demographic, clinical, genetic and treatment information from the nine familial mediterranean fever patients with malignancies.
Table 4 details the MEFV mutations observed in the patients with cancer in the current cohort of FMF; in 2 patients the diagnosis was clinically determined according to Livneh criteria (15).
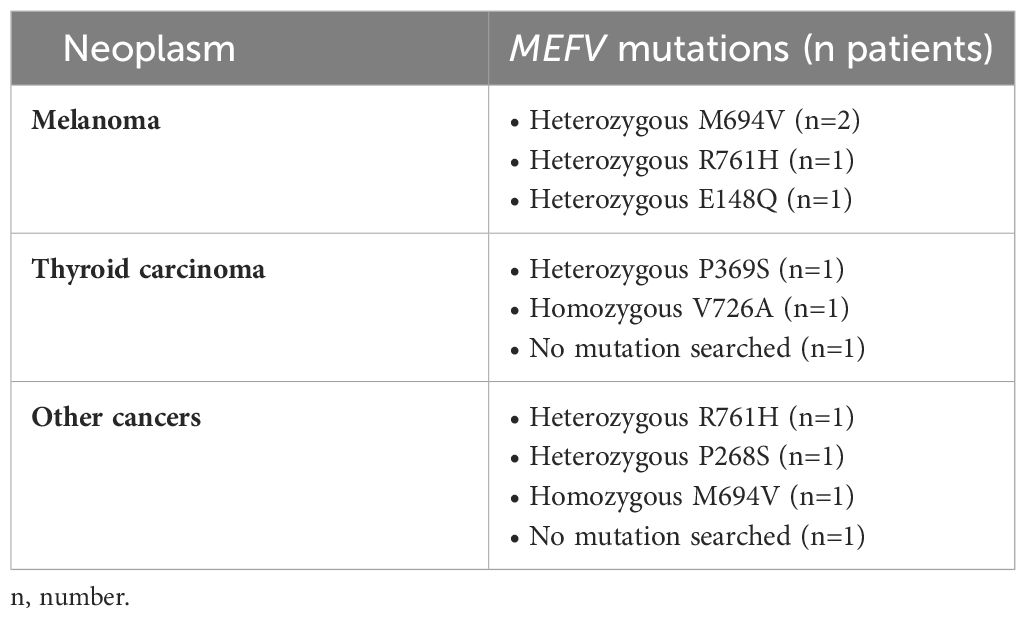
Table 4 MEFV gene mutations observed in familial Mediterranean fever patients who have developed the two more frequent cancers and the other malignant neoplasms in the current FMF cohort.
Six (5.9%) neoplasms were observed among fibromyalgia subjects, 19 (3.8%) among Still’s disease patients (4 of which to be considered benign), 43 (4.2%) among Behçet’s disease patients (17 of which to be considered benign).
The RR to observe a malignant neoplasm was 0.26 (95% CI. 0.10-0.73, p=0.006) in FMF patients compared to fibromyalgia subjects, 0.51 (95% CI. 0.23-1.16, p=0.10) in FMF patients compared to Still’s disease and 0.60 (95% CI. 0.29-1.28, p=0.18) in FMF patients compared to Behçet’s disease. Figure 1 shows the RR adjusted for the age of patients at enrolment, tabagism and treatment with biotechnological agents.
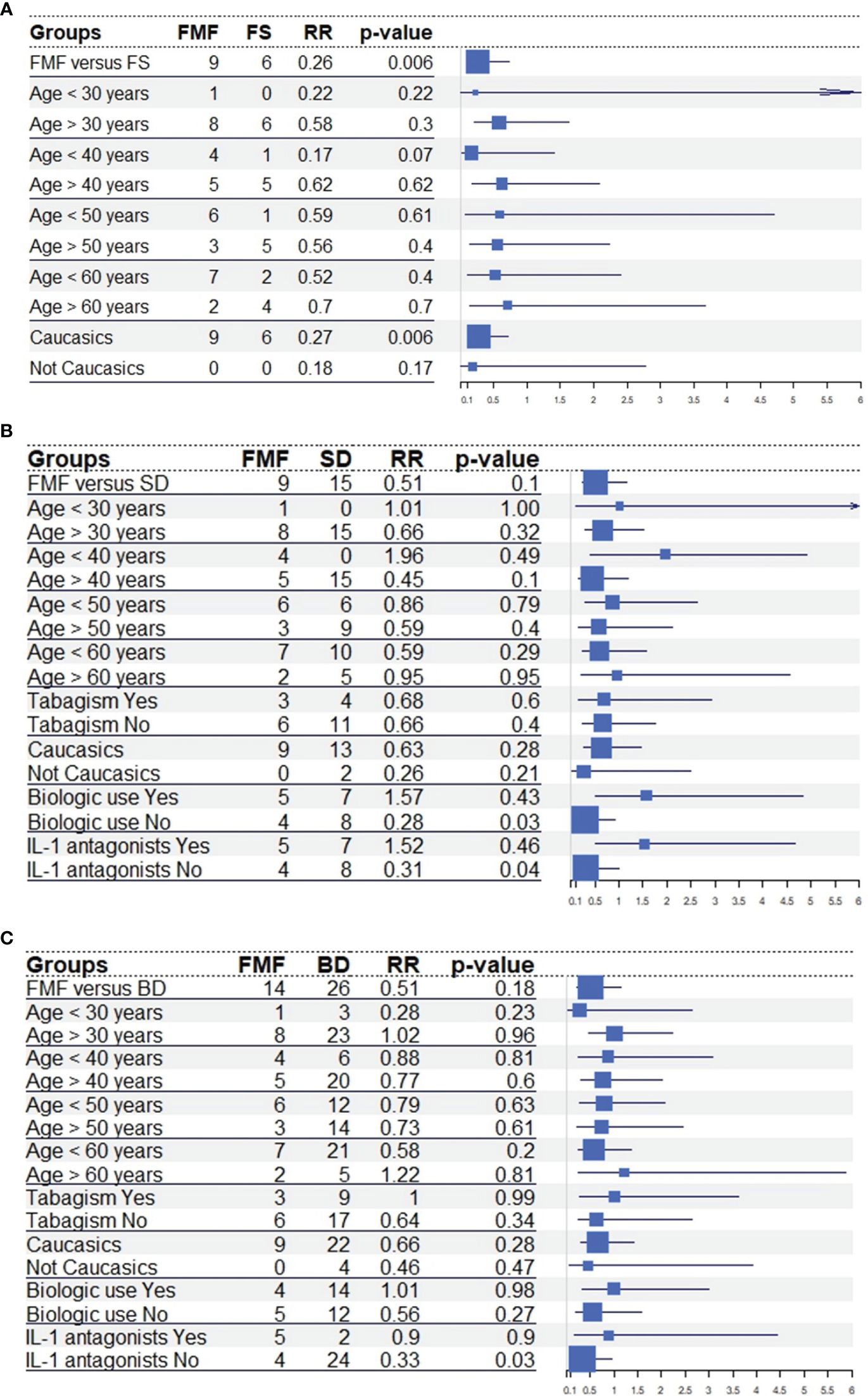
Figure 1 Forestplots illustrating the risk ratio (RR) for malignant cancers between familial Mediterranean fever patients and fibromyalgia subjects (A), Behçet’s disease (B) and Still’s disease (C) in the total number of patients, in different age groups and according to the smoking habit and the use of biotechnological agents. Tabagism was not investigated toward fibromyalgia subjects due to the lack of this information in patients with fibromyalgia; biotechnological agents and anti-interleukin-1 agents were not investigated in patients with Behçet’s disease as patients with familial Mediterranean fever were primarily treated with anti-IL-1 agents, while Behçet’s disease was predominantly treated with tumor necrosis factor inhibitors. Risk Ratios and 95% confidence intervals were calculated with Episheet software; the p-value were obtained with the chi-square test or the Fisher exact test, as appropriate. Abbreviations: BD, Behçet’s disease; FMF, familial mediterranean fever; FS, fibromyalgia subjects; IL-1, interleukin-1; RR, risk ratio; SD, Still’s disease.
At univariate binary logistic regression, the occurrence of malignant neoplasia was associated with the age at disease onset (β1 = 0.039, 95% CI. 0.001-0.071, p=0.02), the age at the diagnosis (β1 = 0.048, 95% CI. 0.039-0.085, p=0.006), the age at the enrolment (β1 = 0.05, 95% CI. 0.007-0.068, p=0.01), the number of attacks per year (β1 = 0.011, 95% CI. 0.001- 0.019, p=0.008), the use of biotechnological agents (β1 = 1.77, 95% CI. 0.43-3.19, p=0.009), and the use of anti-IL-1 agents (β1 = 2.089, 95% CI. 0.7-3.5, p=0.002). In this last regard, patients requiring the use of biotechnological agents due to colchicine effectiveness issues were 4 out of 9 among FMF patients with malignant cancer development and 71 out of 571 among patients with no cancer occurrence (p=0.02). All FMF patients with malignant neoplasms and treated with biotechnological agents during their history had experienced cancer before starting biologic drugs.
Table 5 presents β0 estimates from univariate binary logistic regression for variables significantly associated with the occurrence of malignant neoplasms, along with the corresponding RR values and their interpretation. Table 6 displays β1 estimates and p-values for additional variables evaluated in this study, which, however, did not reach statistical significance. Table 7 provides information about biotechnological treatment in enrolled patients.
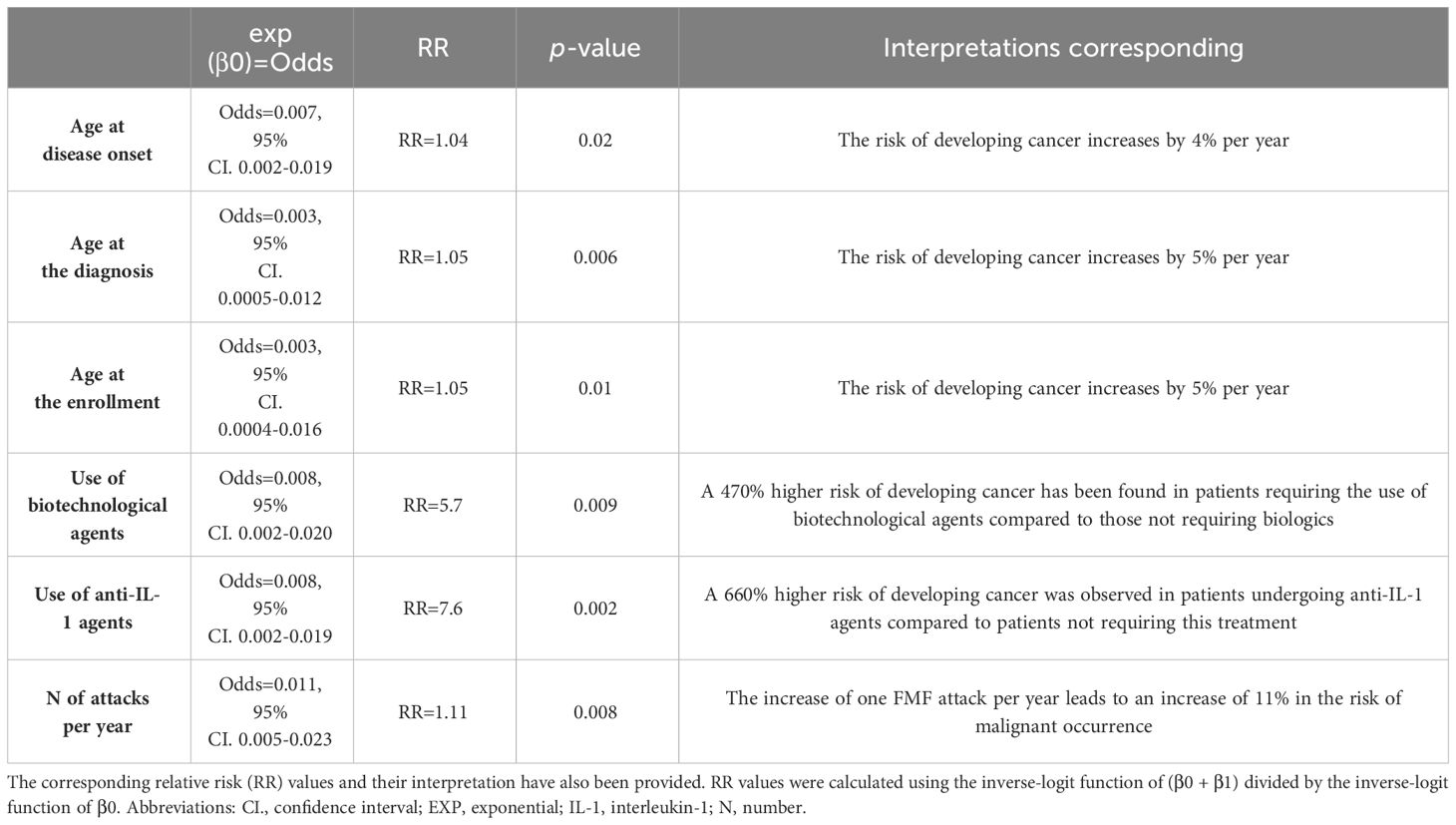
Table 5 The exponential of β0 estimates obtained from the univariate binomial logistic regression for variables significantly associated with malignancy in familial Mediterranean fever (FMF) patients.
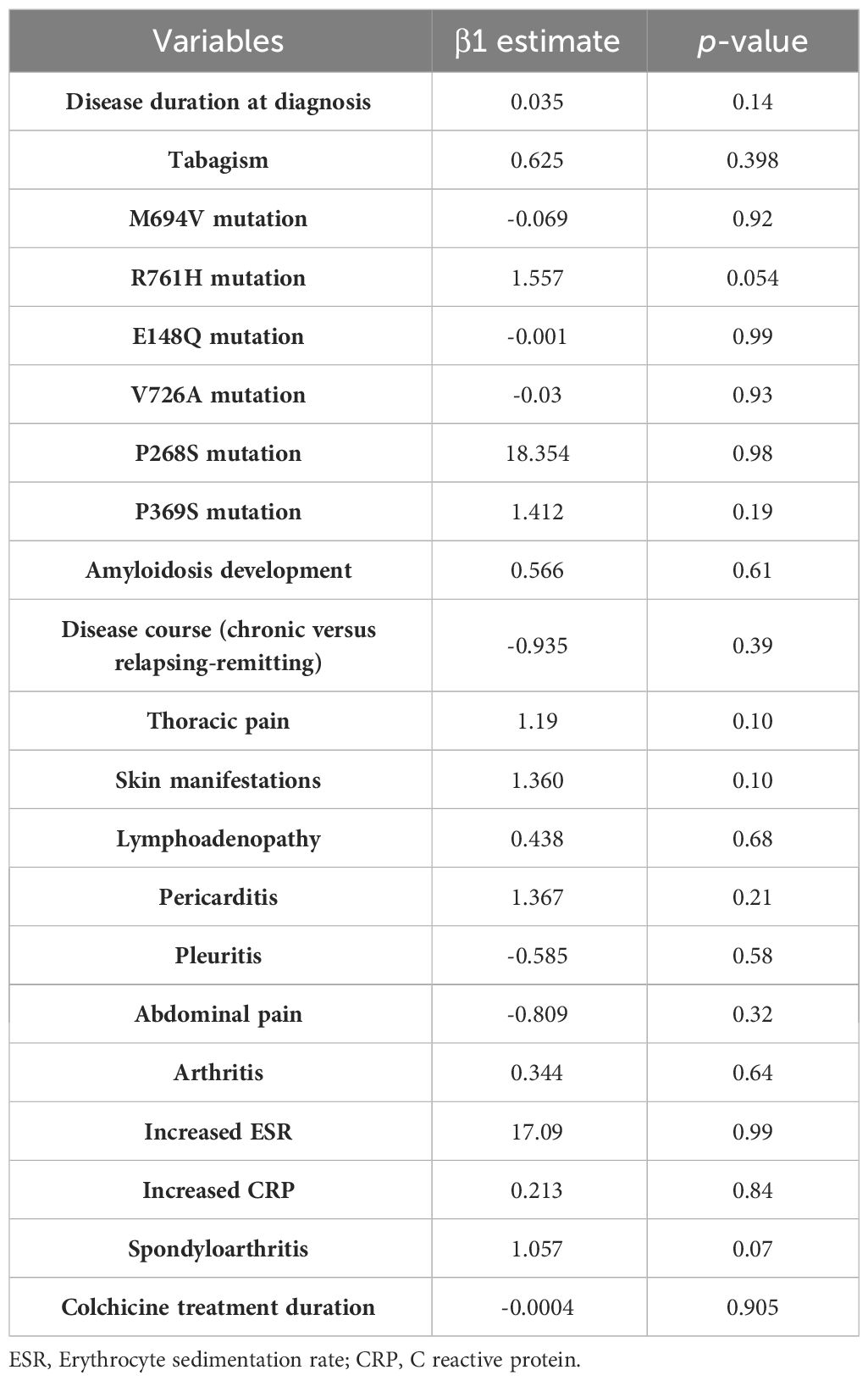
Table 6 The β1 estimates obtained from univariate binary logistic regression for variables assessed in this study, but without reaching statistical significance.
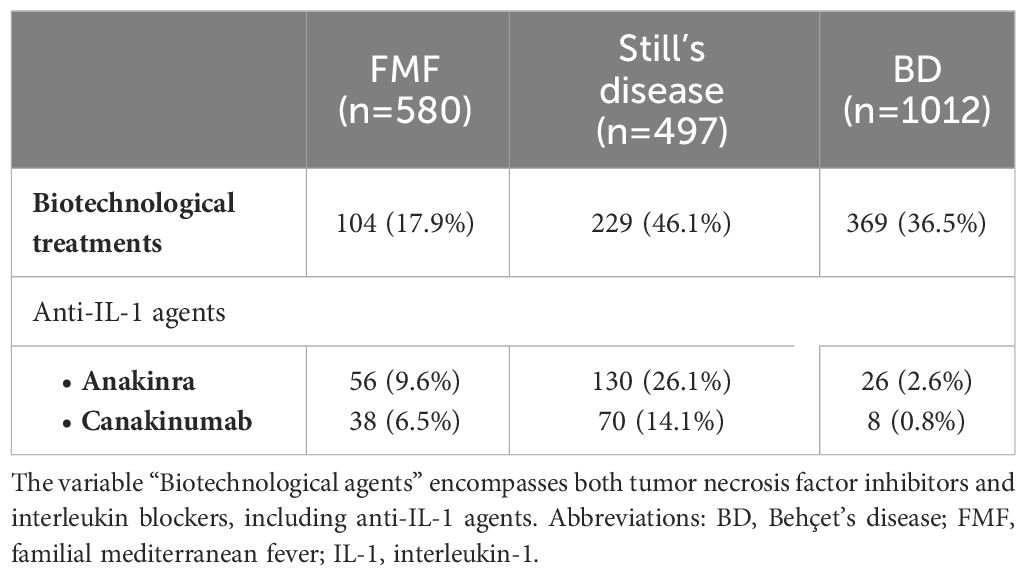
Table 7 Use of biotechnological agents in enrolled patients.
Discussion
The link between chronic inflammation and cancer is supported by strong evidence (27). On the other hand, innate immunity has been also described as a potential weapon against neoplasms, particularly through natural killer cells, macrophages, and eosinophils (28). In this scenario, FMF proves to be both a typical example of a systemic inflammatory disorder and the archetype of autoinflammatory diseases, precisely caused by dysregulation of the innate immune system (29, 30). For this reason, studying the oncological risk in FMF patients is particularly intriguing, as there is both a potential increase in cancer risk due to the chronic exposure to systemic inflammation and a possible decrease related to the hyperactivation of the innate immune system. In this regard, previous studies specifically assessing Turkish and Israelian populations have found a significant decrease in the cancer risk compared to general population (8–10). Accordingly, based on a multicentric data collection, the present study confirms a low frequency of neoplasms in FMF patients, which was equal to 1.5%. This frequency was even lower than that reported by Brenner et al. (8), corresponded to that reported by Baspinar et al. (9), and was slightly higher than that identified by Bilgin et al. (10).
Conversely, Twig et al. did not find a statistically significant difference in the hazard ratio for the occurrence of malignant disease of any type in FMF patients to control group; however, the analysis was performed in men subjects before the age of 50 years, among which the frequency of neoplasms was quite low in FMF patients (roughly 1%) (31).
The RR for cancer was reduced in FMF in all cases, both after comparison with fibromyalgia subjects and after comparison with controls affected by inflammatory diseases. However, statistical significance was achieved only towards fibromyalgia subjects as an example of non-inflammatory condition; in this case, the RR for malignant cancer was reduced of up to 74%. Nevertheless, the overall risk of encountering malignant neoplasms was reduced even when FMF was compared to controls suffering from inflammatory disorders, with a non-statistically significant risk reduction of 49% versus Still’s disease and 40% versus Behçet’s disease. Noteworthy, based on ethnic stratification in our data analysis, it appears that this phenomenon exhibits a stronger manifestation in Caucasian patients compared to individuals of other ethnic backgrounds. However, this discrepancy could be attributed to either real ethnic disparities or the limited representation of non-Caucasic patients in our study cohort. To address this ambiguity, we advocate for conducting a further study specifically focused on non-Caucasic patients in the near future. This would allow for a more comprehensive understanding of the phenomenon across diverse ethnic groups.
The presence of inflammation does not seem to increase the risk of malignant neoplasms in FMF, but the activity and severity of FMF might influence oncological risk. In this regard, logistic regression disclosed a significant association of malignant neoplasms in FMF patients with the age at disease onset and the number of inflammatory attacks per year. This seems to suggest that more severe phenotypes, frequently occurring in earlier stages of life with a higher frequency of attacks (32–35), may increase oncological risk among FMF patients. In this framework, the significant association between the occurrence of neoplasms and the use of biotechnological agents, including IL-1 inhibitors (Figure 1), observed towards Still’s disease and Behçet’s disease may lie. Indeed, neoplasms described in this study occurred before starting biotechnological agents in all FMF cases, while colchicine was associated to biotechnological agents due to effectiveness issues in roughly a half of patients with malignancy. This suggests that individuals necessitating biotechnological agents due to disease activity with treatment resistance are the same exhibiting a higher exposure to neoplasms. Indeed, although neoplasms could have occurred both before and after the potential use of biotechnological agents, neoplasms occurred only before the use of biologics in this cohort of FMF patients enrolled regardless of the use of specific therapies. This further corroborates data about the excellent safety profile with IL-1 inhibitors in FMF patients and provides more information about the increased rate of incident malignancy among patients treated with biotechnological agents as a controversial topic (36, 37).
The reduced incidence of neoplasms in patients with FMF is not currently easy to explain. A role has been suggested for colchicine (38, 39), which represents the first-line therapy in FMF. However, we cannot analyze this hypothesis, as all FMF patients included in the study have taken colchicine throughout their clinical history. Therefore, obtaining a comparison group is not feasible. Nevertheless, we have investigated an association between neoplasms and the duration of colchicine therapy, without identifying statistically significant associations. Of note, in the relationship between the pro-oncogenic risk posed by systemic inflammation and the potential anti-tumoral action of the innate immunity, the latter component could play a predominant role in FMF patients. However, excessive disease activity seems to play a contrary role, favoring a greater tendency towards oncogenesis among the group of FMF patients. In this regard, the recurrent nature of inflammatory attacks, particularly when accompanied by colchicine resistance, could result in a sustained inflammatory environment that in turn could contribute to carcinogenesis. In particular, specific laboratory studies should be conducted to understand whether sustained release of IL-1β can promote tumor progression.
In addition to the age at disease-onset, both the age at diagnosis and the age at the enrolment positively associated with malignant cancer development. Therefore, FMF patients, fibromyalgia subjects and controls with inflammatory diseases were stratified according to the different ages at which they were enrolled in the study. Considering the variations in RR by age groups, the age at the enrolment seems to work as an effect modifier rather than a confounding factor. Specifically, the progression of the age at enrolment generally led to an increased risk of neoplasia when comparing FMF to fibromyalgia subjects, as expected. Conversely, the reduction in the risk of tumors was less pronounced in younger age groups when comparing FMF and Still’s disease patients below the age of 60; the same effect was observed when comparing FMF and Behçet’s disease patients aged 40-60 years. On the other hand, tabagism showed to be a mediator of neoplasm development, especially when comparing FMF and Behçet’s disease patients.
Of note, mesothelioma has been described as associated with FMF in the past years (40–44); nevertheless, mesothelioma did not appear among neoplasms observed in our cohort of patients. Conversely, monoclonal gammopathy was observed in 3 out of the 14 patients with benign and malignant cancer. This aligned with what was previously studied regarding the identification of a high frequency of MEFV gene mutations in patients with hematological neoplasms (45–47).
Limitations of the study include the relatively limited number of FMF patients enrolled and the lack of an extensive adjustment for all cancer-related health habits. In additions, control groups may appear quite different in their demographic features. This last issue is mainly related to the well-known early age at FMF disease onset compared to the onset of other diseases chosen as control groups. This also affects the disease duration, the age at the diagnosis, and the age at the enrolment into the study. However, we ruled out any influence by the age of patients at the time of the enrolment by adjusting the results for different ages of patients. “Furthermore, the median disease duration at the time of enrollment in the study (more than 17 years) was significantly longer among FMF patients compared to the control groups. This shows a longer exposure to inflammation and the diseased status for FMF subjects. If a pro-tumorigenic role of FMF were to emerge in FMF patients, this would be highlighted precisely due to the prolonged exposure. In any case, this study provides further evidence regarding the risk of neoplasms in FMF patients, particularly among Caucasians, while also examining differences with fibromyalgia subjects and controls with other inflammatory diseases.
In conclusion, the present study confirms that the risk for neoplasms is reduced in Caucasic FMF patients; considering the subgroup of FMF subjects with cancer, the occurrence of tumors is more pronounced among patients showing a severe disease phenotype and those with a colchicine-resistant disease.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Azienda Ospedaliero Universitaria Senese. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AV: Writing – review & editing, Writing – original draft. VC: Writing – original draft, Writing – review & editing. AT: Writing – review & editing, Supervision. GR: Supervision, Writing – review & editing. EB: Supervision, Writing – review & editing. PPo: Writing – review & editing. EA: Writing – review & editing. JS: Writing – review & editing. GC: Writing – review & editing. ADP: Writing – review & editing. DR: Writing – review & editing. AO: Writing – review & editing. AŞ: Writing – review & editing. FL: Writing – review & editing. GL: Writing – review & editing. MC: Writing – review & editing. MM: Writing – review & editing. AI: Writing – review & editing. PPS: Writing – review & editing. EV: Writing – review & editing. DY: Writing – review & editing. HK: Writing – review & editing. RK: Writing – review & editing. AL: Writing – review & editing. MG: Writing – review & editing. MS: Writing – review & editing. SSe: Writing – review & editing. HE: Writing – review & editing. SO: Writing – review & editing. NJ: Writing – review & editing. MK: Writing – review & editing. ADC: Writing – review & editing. CG: Writing – review & editing. GM: Writing – review & editing. AA: Writing – review & editing. SP: Writing – review & editing. MR: Writing – review & editing. JS: Writing – review & editing. FD: Writing – review & editing. IM: Writing – review & editing. SSi: Writing – review & editing. MFG: Writing – review & editing. NÇ: Writing – review & editing. MT: Writing – review & editing. AK: Writing – review & editing. JH-R: Writing – review & editing. PPa: Writing – review & editing. DO-B: Writing – review & editing. PB: Writing – review & editing. AR: Writing – review & editing. SC: Writing – review & editing. PS: Writing – review & editing. HG: Writing – review & editing. SG: Writing – review & editing. EW-S: Writing – review & editing. İV: Writing – review & editing. RL: Writing – review & editing. KJ-R: Writing – review & editing. EM: Writing – review & editing. JT: Writing – review & editing. ACa: Writing – review & editing. ACo: Writing – review & editing. GE: Writing – review & editing. FL: Writing – review & editing. GB: Writing – review & editing. RT: Writing – review & editing. PR: Writing – review & editing. ED: Writing – review & editing. ST: Writing – review & editing. ABr: Writing – review & editing. BO: Writing – review & editing. AH-A: Writing – review & editing. ABa: Writing – review & editing. CF: Writing – review & editing. BF: Writing – review & editing. LC: Writing – review & editing, Project administration, Supervision.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We thank the University of Siena for the financial support in supporting the open access fees.
Acknowledgments
This research is supported (not financially) by the European Reference Network (ERN) for Rare Immunodeficiency, Autoinflammatory and Autoimmune Diseases (RITA). Thirteen of the authors of this publication [AV, VC, JS, MT, SG, MC, AI, CG, PS, JS, JH-R, AR, FB, CF, and LC] belong to institutes that are members of the ERN RITA [Azienda Ospedaliero-Universitaria Senese of Siena; University of Brescia and Spedali Civili of Brescia, Ospedale Pediatrico Bambino Gesù, Laiko General Hospital of Athens; Hospital Clínic of Barcelona, University Hospital Schleswig-Holstein].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
Abbreviations: AIDA, AutoInflammatory Disease Alliance; BD Behçet’s disease; CI, confidence intervals; CRP, C reactive protein; ESR, erythrocyte sedimentation rate; EXP exponential; FMF, Familial Mediterranean fever; FS, fibromyalgia subjects; ICD-10, international classification of diseases-version 10; IL, interleukin; IQR, interquartile range; n, number; RR, relative risk; SD, standard deviation.
References
1. Bernot A, da Silva C, Petit JL, Cruaud C, Caloustian C, Castet V, et al. Non-founder mutations in the MEFV gene establish this gene as the cause of familial Mediterranean fever (FMF). Hum Mol Genet. (1998) 7:1317–25. doi: 10.1093/hmg/7.8.1317
2. Ben-Chetrit E. Old paradigms and new concepts in familial Mediterranean fever (FMF): an update 2023. Rheumatol (Oxford). (2024) 63:309–18. doi: 10.1093/rheumatology/kead439
3. Cantarini L, Vitale A, Lucherini OM, De Clemente C, Caso F, Costa L, et al. The labyrinth of autoinflammatory disorders: a snapshot on the activity of a third-level center in Italy. Clin Rheumatol. (2015) 34:17–28. doi: 10.1007/s10067-014-2721-0
4. Cantarini L, Rigante D, Brizi MG, Lucherini OM, Sebastiani GD, Vitale A, et al. Clinical and biochemical landmarks in systemic autoinflammatory diseases. Ann Med. (2012) 44:664–73. doi: 10.3109/07853890.2011.598546
5. Siligato R, Gembillo G, Calabrese V, Conti G, Santoro D. Amyloidosis and glomerular diseases in familial Mediterranean fever. Medicina (Kaunas). (2021) 57:1049. doi: 10.3390/medicina57101049
6. Liu X, Yin L, Shen S, Hou Y. Inflammation and cancer: paradoxical roles in tumorigenesis and implications in immunotherapies. Genes Dis. (2021) 10:151–64. doi: 10.1016/j.gendis.2021.09.006
7. Hamarsheh S, Zeiser R. NLRP3 inflammasome activation in cancer: A double-edged sword. Front Immunol. (2020) 11:1444. doi: 10.3389/fimmu.2020.01444
8. Brenner R, Ben-Zvi I, Shinar Y, Liphshitz I, Silverman B, Peled N, et al. Familial Mediterranean fever and incidence of cancer: an analysis of 8,534 Israeli patients with 258,803 person-years. Arthritis Rheumatol. (2018) 70:127–33. doi: 10.1002/art.40344
9. Baspinar SN, Kilic B, Azman FN, Guler Y, Gunay UB, Tanin MK, et al. Cancer incidence in Familial Mediterranean Fever: A retrospective analysis. Semin Arthritis Rheumatol. (2023) 63:152284. doi: 10.1016/j.semarthrit.2023.152284
10. Bilgin E, Dizdar Ö, Güven DC, Ceylan S, Aybi Ö, Fırlatan B, et al. Cancer incidence in familial Mediterranean fever patients: a retrospective analysis from central Anatolia. Rheumatol Int. (2019) 39:1045–51. doi: 10.1007/s00296-019-04311-x
11. Gaggiano C, Vitale A, Tufan A, Ragab G, Aragona E, Wiesik-Szewczyk E, et al. The Autoinflammatory Diseases Alliance Registry of monogenic autoinflammatory diseases. Front Med (Lausanne). (2022) 9:980679. doi: 10.3389/fmed.2022.980679
12. Vitale A, Della Casa F, Lopalco G, Pereira RM, Ruscitti P, Giacomelli R, et al. Development and implementation of the AIDA international registry for patients with still’s disease. Front Med (Lausanne). (2022) 9:878797. doi: 10.3389/fmed.2022.878797
13. Vitale A, Della Casa F, Ragab G, Almaghlouth IA, Lopalco G, Pereira RM, et al. Development and implementation of the AIDA International Registry for patients with Behçet’s disease. Intern Emerg Med. (2022) 17:1977–86. doi: 10.1007/s11739-022-03038-1.
14. Gattorno M, Hofer M, Federici S, Vanoni F, Bovis F, Aksentijevich I, et al. Classification criteria for autoinflammatory recurrent fevers. Ann Rheum Dis. (2019) 78:1025–32. doi: 10.1136/annrheumdis-2019-215048.
15. Livneh A, Langevitz P, Zemer D, Zaks N, Kees S, Lidar T, et al. Criteria for the diagnosis of familial Mediterranean fever. Arthritis Rheumatol. (1997) 40:1879–85. doi: 10.1002/art.1780401023
16. Van Gijn ME, Ceccherini I, Shinar Y, Carbo EC, Slofstra M, Arostegui JI, et al. New workflow for classification of genetic variants’ pathogenicity applied to hereditary recurrent fevers by the International Study Group for Systemic Autoinflammatory Diseases (INSAID). J Med Genet. (2018) 55:530–7. doi: 10.1136/jmedgenet-2017-105216
17. Milhavet F, Cuisset L, Hoffman HM, Slim R, El-Shanti H, Aksentijevich I, et al. The infevers autoinflammatory mutation online registry: update with new genes and functions. Hum Mutat. (2008) 29:803–8. doi: 10.1002/humu.20720
18. Touitou I, Lesage S, McDermott M, Cuisset L, Hoffman H, Dode C, et al. Infevers: an evolving mutation database for auto-inflammatory syndromes. Hum Mutat. (2004) 24:194–8. doi: 10.1002/humu.20080
19. Sarrauste de Menthière C, Terrière S, Pugnère D, Ruiz M, Demaille J, Touitou I. INFEVERS: the Registry for FMF and hereditary inflammatory disorders mutations. Nucleic Acids Res. (2003) 31:282–5. doi: 10.1093/nar/gkg031
20. Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still’s disease. J Rheumatol. (1992) 19:424–30.
21. Fautrel B, Zing E, Golmard JL, Le Moel G, Bissery A, Rioux C, et al. Proposal for a new set of classification criteria for adult-onset still disease. Med (Baltimore). (2002) 81:194–200. doi: 10.1097/00005792-200205000-00003
22. Criteria for diagnosis of Behçet’s disease. International Study Group for Behçet’s Disease. Lancet. (1990) 335:1078–80.
23. International Team for the Revision of the International Criteria for Behçet’s Disease (ITR-ICBD). The International Criteria for Behçet’s Disease (ICBD): a collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. (2014) 28:338–47. doi: 10.1111/jdv.12107
24. Koné-Paut I, Shahram F, Darce-Bello M, Cantarini L, Cimaz R, Gattorno M, et al. Consensus classification criteria for pediatric Behçet’s disease from a prospective observational cohort: PEDBD. Ann Rheum Dis. (2016) 75:958–64. doi: 10.1136/annrheumdis-2015-208491
25. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Häuser W, Katz RL, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. (2016) 46:319–29. doi: 10.1016/j.semarthrit.2016.08.012
26. Rothman K. Episheet. 2015 . Available online at: https://www.rtihs.org/sites/default/files/2022-04/Episheet.xls.
27. Singh N, Baby D, Rajguru JP, Patil PB, Thakkannavar SS, Pujari VB. Inflammation and cancer. Ann Afr Med. (2019) 18:121–6. doi: 10.4103/aam.aam_56_18
28. Demaria O, Cornen S, Daëron M, Morel Y, Medzhitov R, Vivier E. Publisher Correction: Harnessing innate immunity in cancer therapy. Nature. (2019) 576:E3. doi: 10.1038/s41586-019-1758-2
29. Ancient missense mutations in a new member of the RoRet gene family are likely to cause familial Mediterranean fever. The International FMF Consortium. Cell. (1997) 90:797–807. doi: 10.1016/S0092-8674(00)80539-5
30. Lancieri M, Bustaffa M, Palmeri S, Prigione I, Penco F, Papa R, et al. An update on familial Mediterranean fever. Int J Mol Sci. (2023) 24:9584. doi: 10.3390/ijms24119584
31. Twig G, Livneh A, Vivante A, Afek A, Shamiss A, Derazne E, et al. Mortality risk factors associated with familial Mediterranean fever among a cohort of 1.25 million adolescents. Ann Rheum Dis. (2014) 73:704–9. doi: 10.1136/annrheumdis-2012-202932
32. Tanatar A, Karadağ ŞG, Çakan M, Sönmez HE, Ayaz NA. Age of onset as an influencing factor for disease severity in children with familial Mediterranean fever. Mod Rheumatol. (2021) 31:219–22. doi: 10.1080/14397595.2020.1719594
33. Özdel S, Özçakar ZB, Kunt SŞ, Elhan AH, Yalçınkaya F. Late-onset disease is associated with a mild phenotype in children with familial Mediterranean fever. Clin Rheumatol. (2016) 35:1837–40. doi: 10.1007/s10067-016-3196-y
34. Mor A, Shinar Y, Zaks N, Langevitz P, Chetrit A, Shtrasburg S, et al. Evaluation of disease severity in familial Mediterranean fever. Semin Arthritis Rheumatol. (2005) 35:57–64. doi: 10.1016/j.semarthrit.2005.02.002
35. Bodur H, Yurdakul FG, Çay HF, Uçar Ü, Keskin Y, Sargın B, et al. Familial Mediterranean fever: assessment of clinical manifestations, pregnancy, genetic mutational analyses, and disease severity in a national cohort. Rheumatol Int. (2020) 40:29–40. doi: 10.1007/s00296-019-04443-0
36. Gülez N, Makay B, Sözeri B. Long-term effectiveness and safety of canakinumab in pediatric familial Mediterranean fever patients. Mod Rheumatol. (2020) 30:166–71. doi: 10.1080/14397595.2018.1559488
37. Koker O, Sahin S, Adrovic A, Yildiz M, Barut K, Gulle B, et al. A controversial topic in juvenile idiopathic arthritis: Association between biologic agents and Malignancy. Int J Rheum Dis. (2020) 23:1210–8. doi: 10.1111/1756-185X.13906
38. Kumar A, Sharma PR, Mondhe DM. Potential anticancer role of colchicine-based derivatives: an overview. Anticancer Drugs. (2017) 28:250–62. doi: 10.1097/CAD.0000000000000464
39. Kumar A, Singh B, Mahajan G, Sharma PR, Bharate SB, Mintoo MJ, et al. A novel colchicine-based microtubule inhibitor exhibits potent antitumor activity by inducing mitochondrial mediated apoptosis in MIA PaCa-2 pancreatic cancer cells. Tumor Biol. (2016) 37:13121–36. doi: 10.1007/s13277-016-5160-5
40. Talerico R, Cardillo C, De Vito F, Schinzari F, Soldato M, Giustiniani MC, et al. Mesothelioma in familial Mediterranean fever with colchicine intolerance: A case report and literature review. Front Immunol. (2020) 11:889. doi: 10.3389/fimmu.2020.00889
41. Eryilmaz MK, Mutlu H, Tazegul G, Eryılmaz R, Müsri FY, Salim DK, et al. Multiple pelvic cysts in a patient with familial Mediterranean fever: Benign cystic mesothelioma. J Cancer Res Ther. (2017) 13:1047–9. doi: 10.4103/jcrt.JCRT_125_16
42. Hershcovici T, Chajek-Shaul T, Hasin T, Aamar S, Hiller N, Prus D, et al. Familial Mediterranean fever and peritoneal Malignant mesothelioma: a possible association? Isr Med Assoc J. (2006) 8:509–11.
43. Curgunlu A, Karter Y, Tüfekci IB, Tunckale A, Karahasanoglu T. Benign cystic mesothelioma: a rare cause of ascites in a case with familial Mediterranean fever. Clin Exp Rheumatol. (2003) 21:S41–3.
44. Gentiloni N, Febbraro S, Barone C, Lemmo G, Neri G, Zannoni G, et al. Peritoneal mesothelioma in recurrent familial peritonitis. J Clin Gastroenterol. (1997) 24:276–9. doi: 10.1097/00004836-199706000-00023
45. Oktenli C, Sayan O, Celik S, Erikci AA, Tunca Y, Terekeci HM, et al. High frequency of MEFV gene mutations in patients with myeloid neoplasm. Int J Hematol. (2010) 91:758–61. doi: 10.1007/s12185-010-0577-x
46. Celik S, Erikci AA, Tunca Y, Sayan O, Terekeci HM, Umur EE, et al. The rate of MEFV gene mutations in hematolymphoid neoplasms. Int J Immunogenet. (2010) 37:387–91. doi: 10.1111/j.1744-313X.2010.00938.x
Keywords: autoinflammatory diseases, FMF, tumor, neoplasm, rare diseases, treatment
Citation: Vitale A, Caggiano V, Tufan A, Ragab G, Batu ED, Portincasa P, Aragona E, Sota J, Conti G, De Paulis A, Rigante D, Olivieri AN, Şahin A, La Torre F, Lopalco G, Cattalini M, Maggio MC, Insalaco A, Sfikakis PP, Verrecchia E, Yildirim D, Kucuk H, Kardas RC, Laymouna AH, Ghanema M, Saad MA, Sener S, Ercan Emreol H, Ozen S, Jaber N, Khalil M, Di Ciaula A, Gaggiano C, Malizia G, Affronti A, Patroniti S, Romeo M, Sbalchiero J, Della Casa F, Mormile I, Silvaroli S, Gicchino MF, Çelik NÇ, Tarsia M, Karamanakos A, Hernández-Rodríguez J, Parronchi P, Opris-Belinski D, Barone P, Recke A, Costi S, Sfriso P, Giardini HAM, Gentileschi S, Wiesik-Szewczyk E, Vasi I, Loconte R, Jahnz-Różyk K, Martín-Nares E, Torres-Ruiz J, Cauli A, Conforti A, Emmi G, Li Gobbi F, Biasi GR, Terribili R, Ruscitti P, Del Giudice E, Tharwat S, Brucato AL, Ogunjimi B, Hinojosa-Azaola A, Balistreri A, Fabiani C, Frediani B and Cantarini L (2024) Risk for cancer development in familial Mediterranean fever and associated predisposing factors: an ambidirectional cohort study from the international AIDA Network registries. Front. Immunol. 15:1397890. doi: 10.3389/fimmu.2024.1397890
Received: 08 March 2024; Accepted: 22 April 2024;
Published: 10 May 2024.
Edited by:
Ozgur Kasapcopur, Istanbul University-Cerrahpasa, TürkiyeReviewed by:
Sezgin Sahin, Istanbul University-Cerrahpasa, TürkiyeOya Koker, Istanbul University, Türkiye
Copyright © 2024 Vitale, Caggiano, Tufan, Ragab, Batu, Portincasa, Aragona, Sota, Conti, De Paulis, Rigante, Olivieri, Şahin, La Torre, Lopalco, Cattalini, Maggio, Insalaco, Sfikakis, Verrecchia, Yildirim, Kucuk, Kardas, Laymouna, Ghanema, Saad, Sener, Ercan Emreol, Ozen, Jaber, Khalil, Di Ciaula, Gaggiano, Malizia, Affronti, Patroniti, Romeo, Sbalchiero, Della Casa, Mormile, Silvaroli, Gicchino, Çelik, Tarsia, Karamanakos, Hernández-Rodríguez, Parronchi, Opris-Belinski, Barone, Recke, Costi, Sfriso, Giardini, Gentileschi, Wiesik-Szewczyk, Vasi, Loconte, Jahnz-Różyk, Martín-Nares, Torres-Ruiz, Cauli, Conforti, Emmi, Li Gobbi, Biasi, Terribili, Ruscitti, Del Giudice, Tharwat, Brucato, Ogunjimi, Hinojosa-Azaola, Balistreri, Fabiani, Frediani and Cantarini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Cantarini, Y2FudGFyaW5pbHVjYUBob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work