 Miguel Ángel Prieto del Prado
Miguel Ángel Prieto del Prado Francesc Fernández Avilés
Francesc Fernández Avilés- 1Hematology Department, Hospital Universitario de Melilla, Melilla, Spain
- 2Hematology Department, Bone Marrow Transplantation Unit, Instituto del Cáncer y Enfermedades de la Sangre (ICAMS), Hospital Clínic, Barcelona, Spain
Autologous stem-cell transplantation (ASCT) is the standard of care for the management of multiple myeloma and has a well-established role in the treatment of some types of lymphoma. Over the last decades, the number of ASCT performed has increased significantly, leading to elevated pressure and cost for healthcare services. Conventional model of ASCT includes the admission of patients to a specialized Transplant Unit at any stage of the procedure. To optimize healthcare provision, ambulatory (outpatient/at-home) setting should be the focus moving forward. Thus, ambulatory ASCT model permits reducing average hospital stays and pressures on healthcare services, with significant cost-saving benefits and high degree of patient and caregiver satisfaction. In addition, it facilitates the bed resource for other complex procedures such as allografts or CAR-T cell therapy. The aim of this systematic review is to document the health impact, feasibility and safety of the outpatient/at-home ASCT models, which are increasingly being applied around the world.
Introduction
Hospital-at-home involves the provision of clinical care in the patient’s home, their natural environment, rather than in the hospital. The reasons for this paradigm shift, which we are already witnessing, lie in different factors such as the increase in the consumption of health services, their costs, and the rationalization of the use of hospital beds (1). The evidence is limited by the few controlled and randomized trials (2–4), by the difficulty in patient selection, or by the small sample size. Most studies show that this type of care is feasible and effective, which is confirmed in a meta-analysis (5) on home hospitalization programs.
Ambulatory ASCT model was recognized for its positive results in terms of effectiveness and safety since the end of the last century (6), reducing length of stay, nosocomial infections, costs, and generating greater comfort for patients. However, this model also shows associated risks (3, 7–10).
With the exponential increase in autografts performed in developed countries, and the consequent increase in care costs, the optimization of ambulatory care provision was established as a strategic objective on the basis of the results of health-care and quality of life of patients (11–13). However, these models are still not routine procedures for different reasons, which the Italian Group for Stem-Cell Transplantation (GITMO) (14) have analyzed, highlighting three essential elements: the identification of the selection criteria for candidates for ambulatory ASCT, the definition of a standard procedure, and the characterization of the criteria for hospital admission during the aplastic phase.
Likewise, the advent of CAR-T platforms, with an increased range of indications and more limited toxicity, has increased interest in early patient discharge in the ambulatory setting while maintaining close patient monitoring. It appears that the future of CAR-T therapy is outpatient management with a careful planning to optimize patient safety.
The review of home hospitalization focused on ASCT, presented below, aims to highlight the potential impact of the model in optimizing care delivery. And this in terms of health results, in aspects such as the perception of the user and caregiver, economic costs or in the use of new technologies, in contrast to conventional and exclusive hospital management.
Methodology
A systematic review to document the health impact, feasibility and safety of the ambulatory ASCT models, which are increasingly being applied around the world, was conducted.
Data sources and searches
PubMed is used as a search engine to identify relevant and quality bibliography. Published articles in the PubMed database as at February 1, 2024 were searched by two investigators, using a search strategy developed for PubMed that included a combination of appropriate keywords, MeSH (Medical Subject Headings) and non- MeSH terms. No language or time restrictions were applied.
The descriptors used were autologous stem-cell transplantation, hospital at home, outpatient transplantation, at-home transplantation, and ambulatory transplantation. And “and” was used as a Boolean operator. Additional S1 File illustrates the search strategy details. An effort to identify additional eligible studies was made by reviewing the references of the included studies. The full text of the selected articles was accessed through different means. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) was used to improve transparency in our findings. The PRISMA checklist is available in S2 File.
Inclusion and exclusion criteria
We looked for home hospitalization studies focused on ASCT, to highlight the possible impact of the model in optimizing health results, in contrast to conventional hospital management. Therefore, we sought models of care that aimed to avoid or reduce hospitalization duration and pressures on healthcare services. Studies carried out on the pediatric population were excluded, as well as duplicates articles, irrelevant studies to autologous stem-cell transplantation or without comparison between outpatient and inpatient settings. The PRISMA Flow Diagram is available in S3 File.
Study selection: data collection process and data items
We then proceeded to critically read each and every one of the selected publications, which are reflected later, as they are original articles that show the experience of researchers in the area of ASCT, in diseases basically onco-hematological with non-hospital models.
Two authors screened titles and when the information provided in the title was inconclusive, the abstract was consulted for eligibility, followed by full-text review to be considered.
Details pertaining to author, publication year, country, study characteristics and design, study sample, outpatient interventions scheme, and reported outcomes were extracted using a spreadsheet software, Microsoft Excel, because Excel is a powerful tool for data analysis, as it allows users to manipulate and analyze large amounts of data quickly and easily.
Results
Feasibility of a hospital-at-home program for ASCT
Currently, home hospitalization presents a great diversity of care models (1). It entails a modality of health care capable of carrying out diagnostic and therapeutic procedures and care at home similar to those provided in hospitals. Its characteristics are set out in Table 1.
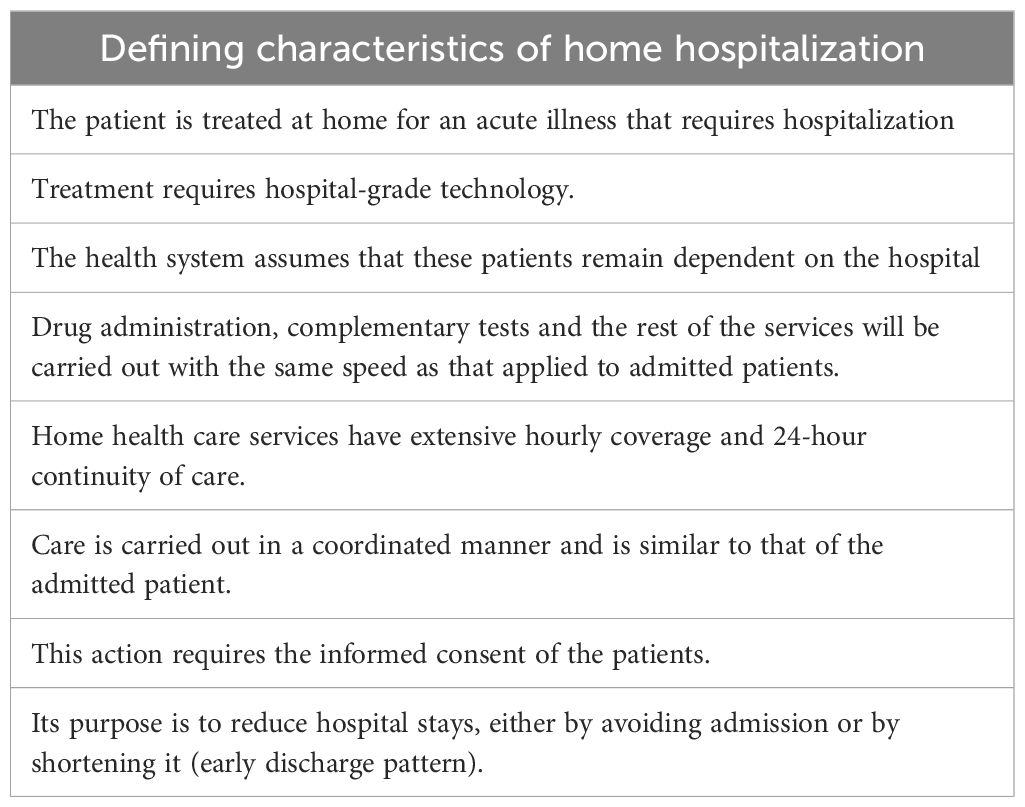
Table 1 Characteristics of hospitalization at home units.
Ambulatory ASCT programs have been favored by the improvement of antimicrobial prophylaxis and therapy, the prevention of mucositis, technological advances, adequate infrastructure and the existence of an experienced multidisciplinary team, among other aspects. The selected patients share requirements such as living in a geographical area less than 60 minutes distant from the hospital, suffering from a disease whose evolution is in a phase that fully justifies admission to the hospital, having a person who performs the functions of caregiver, and, finally, to have the consent of the patient and their families.
The establishment of an ambulatory ASCT program improves health care for patients who require this procedure in the natural history of their hematological process (10, 12, 13).
Most autologous transplants are performed for hematological malignancies; specifically, they are the standard in the management of multiple myeloma and also have a well-established role in the treatment of Hodgkin and non-Hodgkin lymphomas. The advantages of home hospitalization are evident from several points of view (7–10):
✔ For the patient: personalized assistance in their family environment, better perception of patient care, greater ability to carry out activities of daily living. In short, high patient satisfaction.
✔ For the family: unnecessary trips are avoided, greater comfort is reached.
✔ For the hospital: resources are optimized by saving hospital stays, lower risk of nosocomial infections, fewer clinical complications such as confusional and agitation disorders, etc. Ultimately, it reduces healthcare pressure and the waiting list for ASCT. On the other hand, this innovative activity gives “prestige” to the hospital.
✔ For healthcare managers: it clearly represents economic savings in healthcare, mainly due to the reduction in hospitalization and greater patient-bed rotation, without there being any difference in mortality and readmission rates.
Ambulatory ASCT models
Various studies have evaluated the safety, effectiveness, and feasibility of ambulatory ASCT, in its different models, as an optimal approach to the management of hospital stays, with the consequent potential savings in healthcare resources and costs (Table 2).
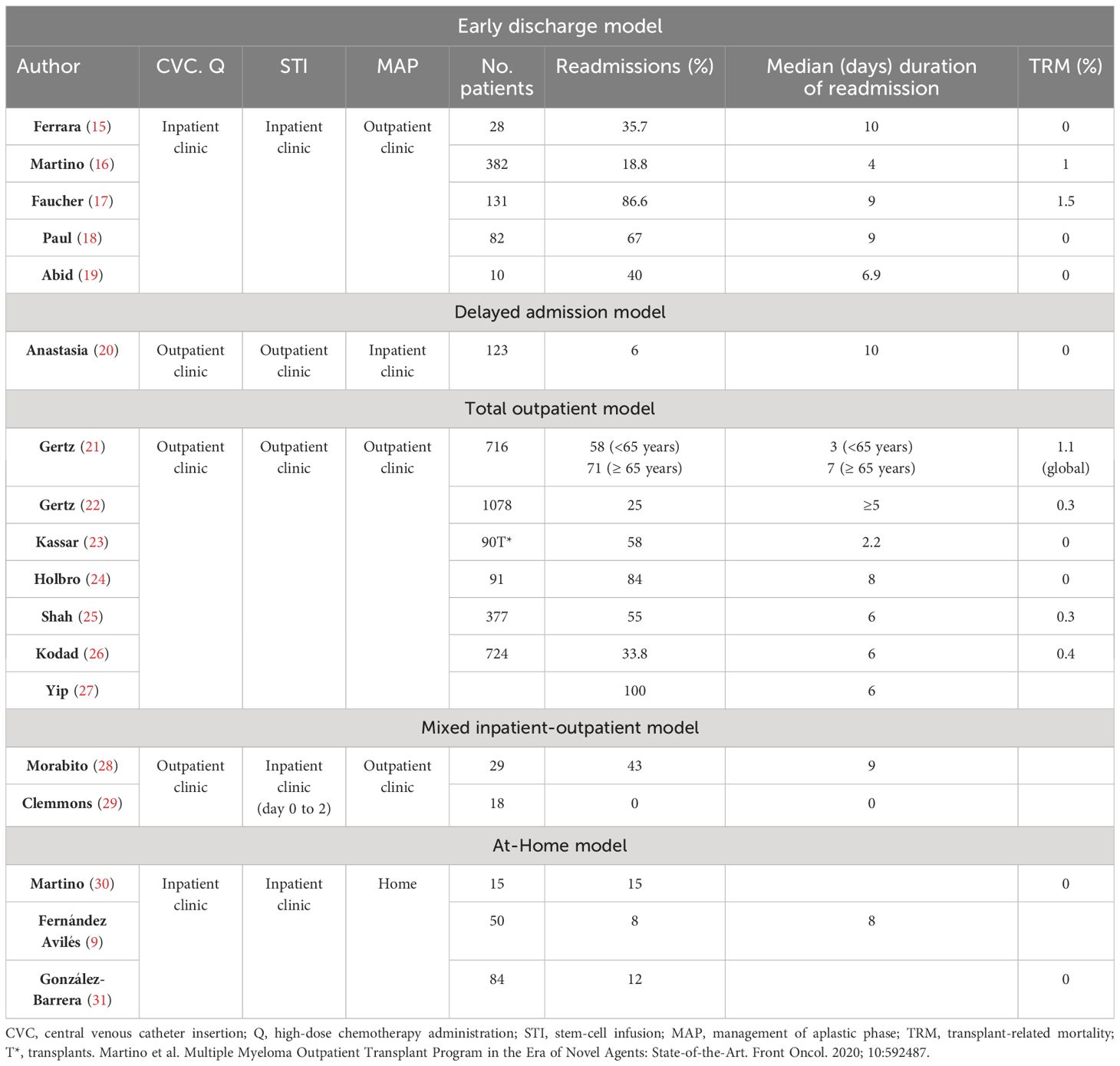
Table 2 Ambulatory ASCT models.
Different publications are shown on the different existing models, with the patients included in each case and the main clinical and health results that determine hospital bed resource they consume.
Patient selection
Patient selection is the key to achieving successful ambulatory ASCT. The inclusion and exclusion criteria used in studies published over recent decades reflect common aspects, although they show differences in their values and in the number of conditions required (10, 13, 14, 17) (Table 3).
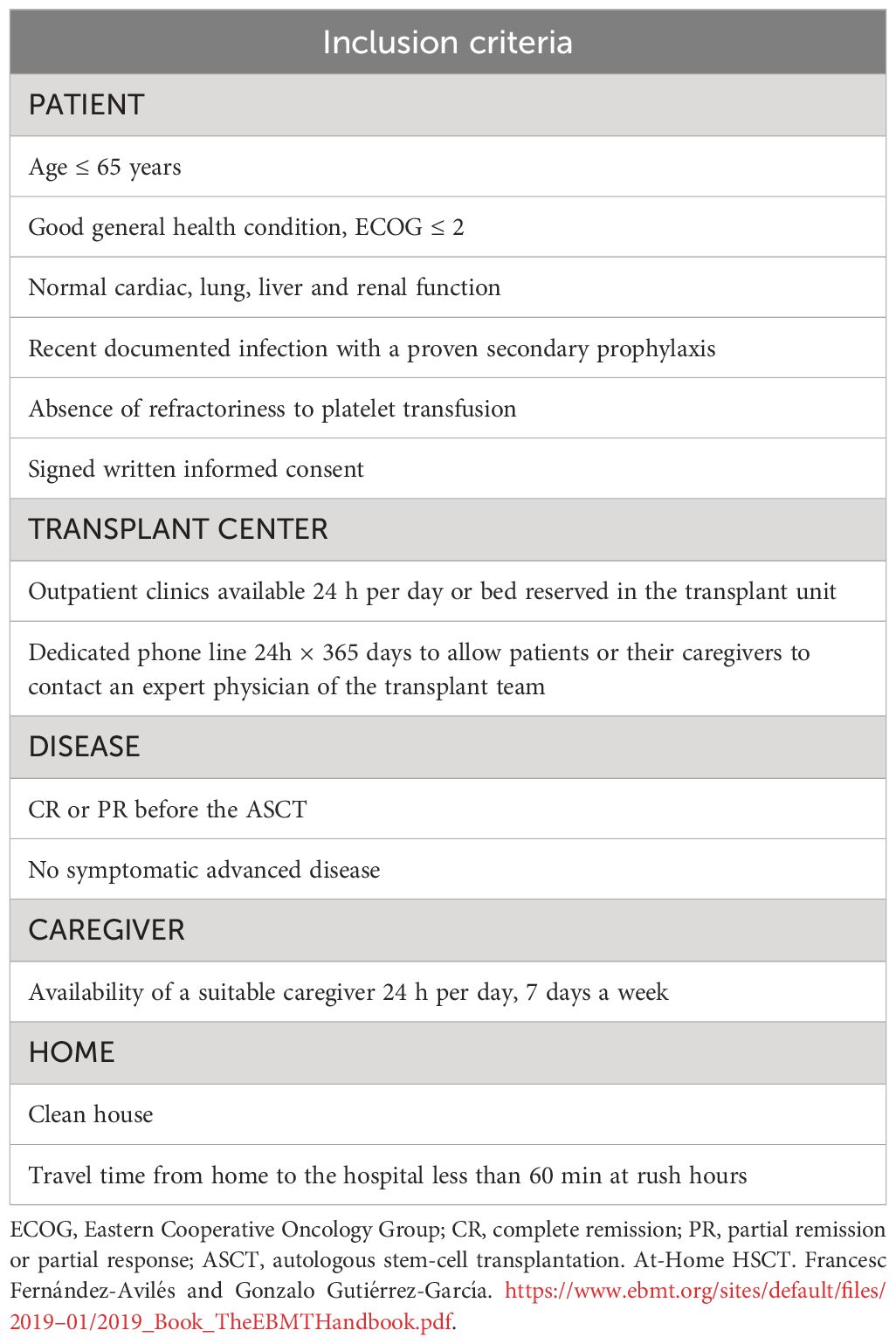
Table 3 Inclusion criteria for ambulatory ASCT.
Incidence of complications
The incidence of the most common complications in patients treated in a home environment varies widely depending on the series. Fever is, by far, the most common complication. Febrile neutropenia is the most frequent cause of hospital readmission in ambulatory care programs for patients treated with ASCT. It shows a wide range, between 20–86%, although lower percentages respond to the use of parenteral antibacterial prophylaxis. A recent study showed that the use of piperacillin/tazobactam and fluoroquinolone prophylaxis may effectively prevent episodes of neutropenic fever and hospitalizations in lymphoma patients managed in our at-home ASCT care model (32). However, it is possible that, sometimes, the febrile episodes may have a non-infectious etiology, and engraftment syndrome could play a more significant role. The study by Rodríguez-Lobato et al. (33) found that, for patients with multiple myeloma in at-home ASCT, the avoidance of G-CSF and the addition of primary prophylaxis with corticosteroids after ASCT minimizes the incidence rates of neutropenic fever and engraftment syndrome.
Mucositis varies between 6–100% (some authors focus on grade 2–3 mucositis, while others also include grade 1 mucositis), while gastrointestinal disorders range between 17–53%. The values of the different series are shown in Table 4.
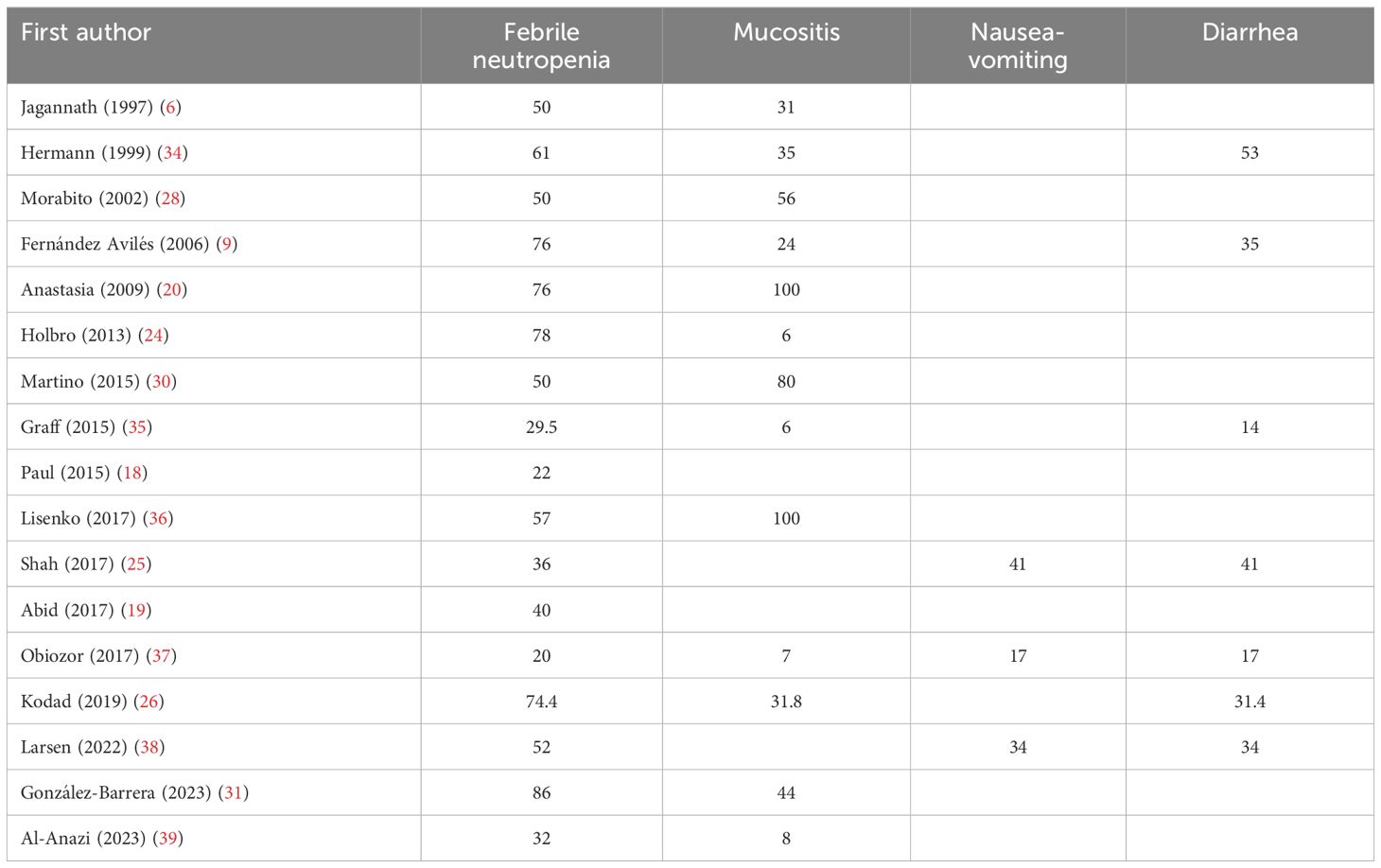
Table 4 Incidence (%) of the main complications in ambulatory ASCT.
Causes of hospital readmissions
Hospital readmission is a frequent occurrence in patients with ASCT on an ambulatory model. It happens in a very wide range, which oscillates between 8–90% due to the disparity and laxity of criteria recorded in the different published series. The causes are very varied, highlighting the patient’s or caregiver’s own will or claudication, hemodynamic instability, persistent fever, cardiorespiratory disorders, altered level of consciousness, uncontrolled nausea/vomiting or diarrhea, or mucositis oral requiring total parenteral nutrition and opioid analgesics, among other reasons.
Quality of life
The general belief that patients treated on an ambulatory basis perceive greater physical and psychological well-being is controversial. A similar pattern in quality of life is observed in both outpatients and inpatients, worsening between days 4–6 post-transplant and improving on day 12–16, when in most cases recovery of neutrophil values occurs, and extramedullary toxicity is overcome.
The few studies that provide data on the quality of life of the patient treated in an outpatient/home ASCT model have important limitations; they are observational, non-randomized studies, in which the patient chooses the transplant modality, which makes the results often inconsistent, contradictory, and influenced by the initial choice, or not finding statistically significant differences with respect to the conventional model (9, 13, 40, 41).
Summers et al. (42) found that emotional, social and physical well-being, as well as quality of life, were significantly better in ambulatory than in hospitalized patients. Fernández Avilés et al. (9) used an anonymous questionnaire after completing the procedure. All patients and caregivers felt safe at home and almost all indicated that they would choose the home model again and recommend it to another patient.
On the other hand, Martino et al. (40) confirmed that global quality of life was not significantly different between ambulatory and hospitalized patients during the transplant period. In conclusion, the ambulatory ASCT model did not improve or affect the patient’s overall quality of life compared to the hospital standard.
The use of telemedicine in the Hematopoietic Transplant environment allows equitable and universal healthcare, accessible to the most disadvantaged sectors or from geographical areas that are difficult to access. They can positively affect the physical and psychological state of patients and, therefore, their overall quality of life. But the clinical experience of telemedicine in this area is very limited. The pilot study carried out by Nawas et al. (43) found a high rate of satisfaction among patients, but not among the responsible clinician, due to technological barriers that caused delays and a suboptimal physical examination as the main causes of their dissatisfaction. The study by Mussetti et al. (44), in Hospitalet (Spain), with transplant patients during the COVID19 pandemic, confirmed the obvious advantages for doctors and patients that these technologies provided, although technological problems still represent a challenge, especially for patients who live alone or without caregivers. González Sierra et al. (31), at the University Hospital of Granada, uses a mixed post-transplant care model: the patient goes to the outpatient clinic 2–3 days a week for analytical monitoring and physical examination, and on the rest of the days they have a mobile application that ensures direct daily doctor-patient communication.
The use of this technology is a complementary tool in the management of hematopoietic transplantation that can improve the physical and psychological state of both patients and their caregivers, but it must be adapted to their capabilities to avoid technological limitations.
Impact of caregivers on home ASCT results
Most hospitals offering ambulatory transplantation require “twenty-four seven” availability of a caregiver, at least for the duration of the aplastic phase. Caregivers play a crucial role in the success of the ambulatory procedure, spending most of their time with the patient, affecting them in multiple facets of their life, and carrying a very significant physical and emotional burden. The profile of the caregiver would be the patient’s couple, an active worker in half of the cases, with a high academic level, female, and aged around 54 years (45).
Several trials showed better overall survival in patients with availability of a caregiver compared to those undergoing ASCT without such support. Likewise, the decrease in readmissions, with the consequent reduction in costs, and the feasibility associated with the ambulatory approach seem to be mediated mainly by the effort of the caregivers. Furthermore, the lack of a caregiver was the most frequent cause of patient refusal to participate in an outpatient/at-home program (40, 42, 46, 47).
Therefore, rigorous studies are needed to evaluate better the emotional, economic-labor burden and quality of life of caregivers, their impact on the results and quality of life of patients undergoing an ambulatory or home transplant.
Costs and impact on health services
Numerous studies have indicated that ambulatory ASCT is cost-effective, mainly due to the shorter length of hospital stay, which ranges between 3 and 17 days (5–7, 9, 10, 12, 13, 17, 19, 29–31). It offers specialized medical care to patients in their homes for diseases that normally require hospitalization (13, 41). All articles that compare costs between ambulatory and hospital care confirm a reduction in favor of the ambulatory model, ranging between 19.32% and 53% (Table 5). However, the limitations of these publications are important. Therefore, selection criteria for hospitalization of ambulatory patients, which differ between studies, and the variability of the models, may make the comparison of the results very complicated. Only one randomized clinical trial was found in our review, Faucher´s one (17). There is a lack of studies with an appropriate design that evaluate the real savings obtained with outpatient/home ASCT programs. It is known that more than half of the total costs billed by autologous transplant correspond to expenses for hospital admissions, which has a significant effect on health systems. However, other factors involved in the expense should be considered, such as the outpatient/home model used, with or without a bed freed up during out-of-hospital follow-up, the hospital readmission rate of each program, the different existing health and economic models or other relevant expenses (drugs, laboratory, healthcare personnel fees, sick leave).
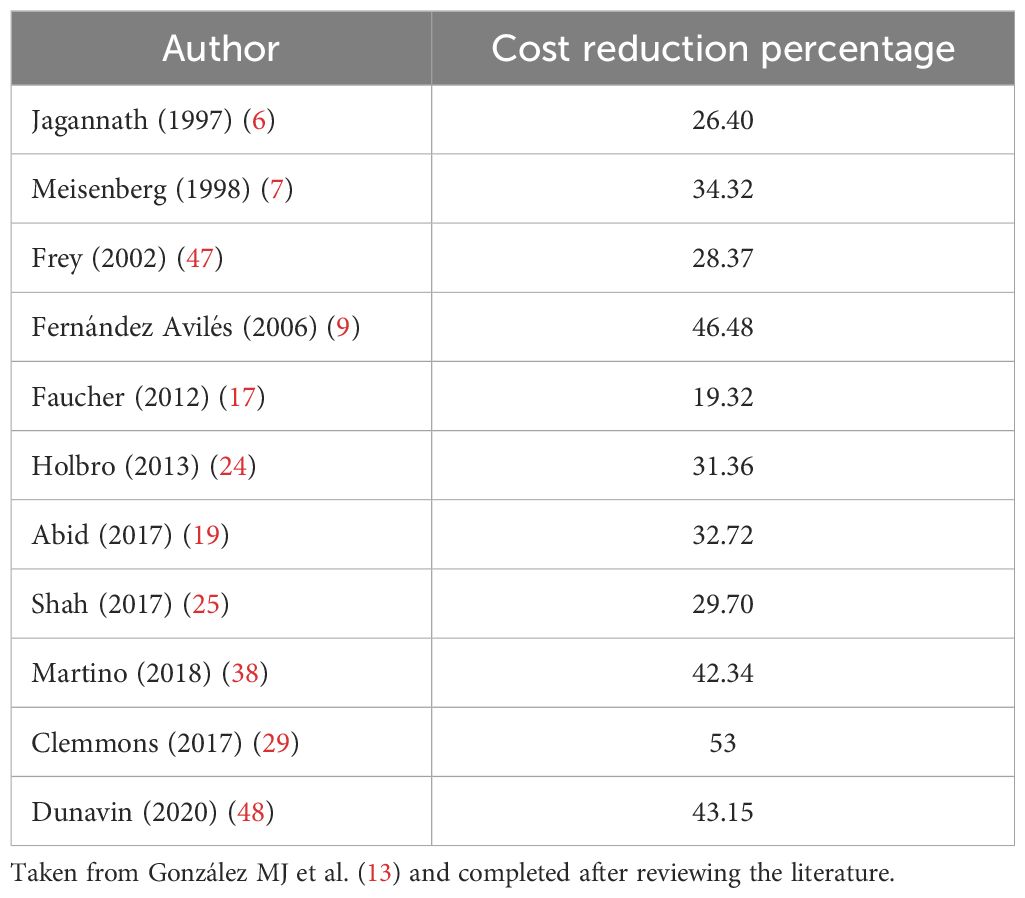
Table 5 Cost reduction of the ambulatory vs. hospital model in ASCT.
Worldwide distribution of published clinical studies of home ASCT
Although different researchers (10, 13, 41, 49) have focused on studying the impact of the ambulatory model in stem-cell transplantation, the overall comparative effects have not yet been systematically evaluated. Table 6 shows the publications from different continents that analyze the evidence on the effects of ambulatory treatment, in terms of health results, costs and experience in care.
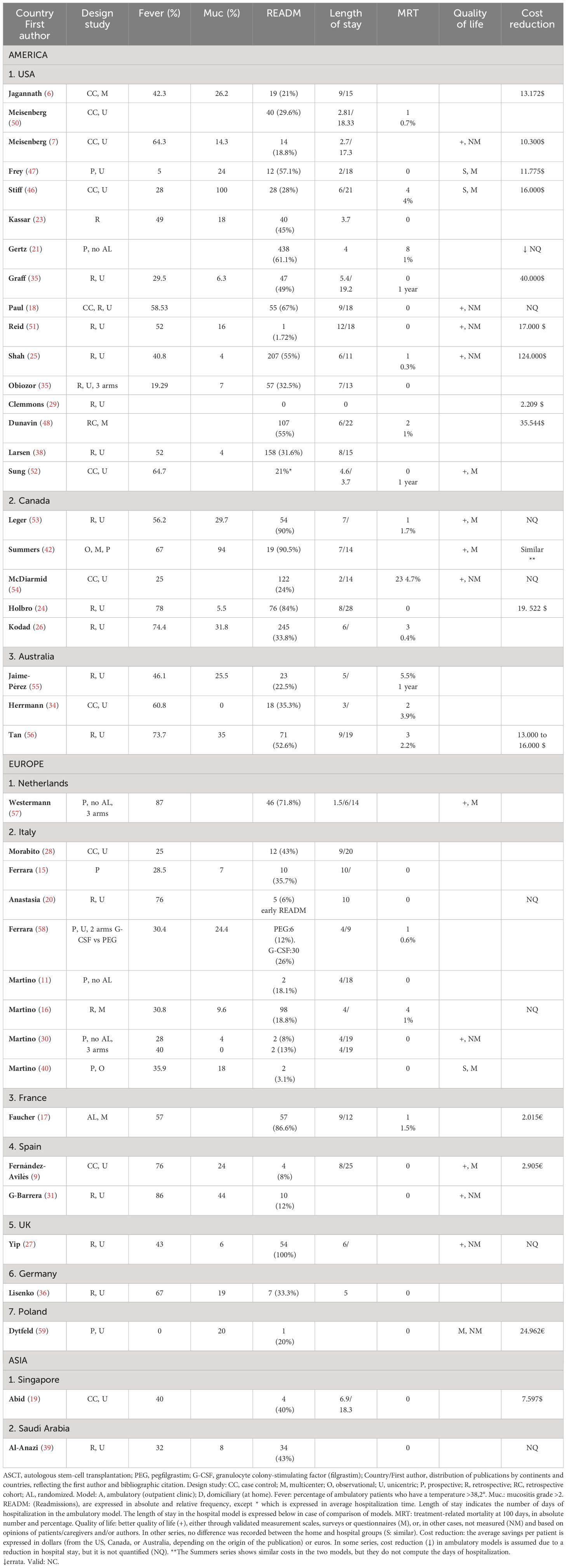
Table 6 Worldwide distribution of ambulatory ASCT for hematological malignancies.
It is worth highlighting certain limitations of the studies that are set out in Table 6 and which we briefly summarize: 1. Health outcome data show wide variability between the different series. 2. Regarding quality of life, only some studies use validated measurement scales or satisfaction questionnaires. 3. To evaluate costs, it must be taken into account that the financing of health systems is highly variable in different countries. 4. It must also be reflected that the savings recorded in most studies are based only on the reduction in hospital length of stay while other economic aspects of the procedure are not included. 5. The designs of the studies are heterogeneous, with many being retrospective, without a comparison group; others are prospective, with several arms, but are not randomized; few have a case-control design and sufficient sample size, and we only have one randomized, multicenter clinical trial, therefore with greater methodological rigor.
Discussion
Several studies have confirmed the feasibility and safety of ambulatory ASCT, reinforcing it as an alternative to standard hospitalization. Its potential benefits in terms of health outcomes and quality of life for the patient, or savings of healthcare resources for organizations, are obvious.
The systematic review and meta-analysis by Owattanapanich et al. (10), which included nine studies with a rigorous design, showed a significantly lower probability of developing febrile neutropenia and septicemia in patients undergoing ambulatory management compared to those who received an ASCT as inpatients, with the Ib level of evidence. In addition, it reported lower costs and higher levels of patient satisfaction in that group. We also have a single, randomized, multicenter clinical trial that found a shorter hospital stay, as well as a lower cost of the procedure in the group of home patients (17) (evidence Ib).
These data should facilitate broader implementation of the ambulatory strategy. However, it has not yet been established as a routine procedure, and many hospital centers are reluctant to adopt this approach, probably due to lack of adequate infrastructure.
Over the last decades, other studies have also shown that the home model improves the quality perceived by the patient and their families, reduces the duration of hospitalization, the waiting list for hematopoietic transplant, and minimizes exposure to nosocomial microorganisms. In short, it optimizes healthcare resources and clearly represents financial savings in healthcare, without any difference in mortality rates with respect to the hospital model. However, many of them are non-prospective and non-randomized studies and, therefore, this methodology limits the validity of the results, with level III evidence.
In our systematic review, most of the patient populations undergoing transplantation suffered from multiple myeloma. Generally, high-dose melphalan conditioning (140–200 mg/m2), administered in one or two consecutive days, was chosen as cytoreductive regimen in these patients and may be more suitable for a fully outpatient management. The second patient population is Hodgkin and non-Hodgkin lymphomas receiving BEAM as conditioning. BEAM is administered for six consecutive days, even with two components given every 12 hours, making it difficult to administer on an ambulatory basis.
On the other hand, the incidence of early adverse events, such as neutropenic fever and oral/gastrointestinal mucositis, was much lower in patients with multiple myeloma who received an ASCT.
Due to the ease of administration of high-dose melphalan and the relatively low extra-hematological toxicity, patients with multiple myeloma are ideal candidates for ambulatory ASCT.
The current systematic review found positive results among patients underwent an ambulatory ASCT than among those who had an inpatient ASCT. This could be an appealing reason to utilize the first strategy in addition to its reported better cost-effectiveness, and higher patient satisfaction levels. However, given the methodological heterogeneity of existing publications, and the limited validity of the observational nature of the included studies, future controlled and randomized studies are still needed to confirm the potential benefit of the ambulatory procedure, in terms of health outcomes, cost-effectiveness, or quality of life. In relation to the cost studying, other factors involved in the expense should be considered in addition to the clinical aspects, such as the outpatient/home model used, the different existing health and economic models, or other expenses (role of the caregivers, drugs, laboratory, healthcare personnel fees…).
Conclusions
The ambulatory ASCT is safe, feasible, and cost-effective, even in patients over 65 years of age and with certain non-limiting comorbidities, especially in work groups with consolidated outpatient projects. So, it seems to us that we are in a position to propose certain inclusion criteria to be candidates for ambulatory ASCT, especially for teams that want to start an outpatient ASCT program: multiple myeloma patients, age less than or equal to 65 years, good performance status (ECOG ≤ 2), favorable comorbidity profile (normal cardiac, lung, liver and renal function), availability of a suitable and full-time empowered caregiver and travel time from home to the hospital less than 60 min at rush hours. The main advantages reported of performing this ambulatory procedure include saving beds, reducing hospital costs, and lowering the rates of infections. These aspects should be considered by healthcare providers. Due to the difficulty to carry out randomized and controlled trials in this setting, specific and rigorous inclusion and exclusion selection criteria are required for the routine use of the ambulatory ASCT model.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
MP: Writing – review & editing, Writing – original draft, Visualization, Software, Methodology, Investigation, Formal analysis. FF: Writing – review & editing, Visualization, Supervision, Project administration, Methodology, Investigation, Formal analysis, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1419186/full#supplementary-material
References
1. Cuxart Mèlich A, Estrada Cuxart O. Hospital at home: an opportunity for change. Med Clin (Barc). (2012) 138:355–60. doi: 10.1016/j.medcli.2011.04.008
2. Shepperd S, Iliffe S, Doll HA, Clarke MJ, Kalra L, Wilson AD, et al. Admission avoidance hospital at home. Cochrane Database Syst Rev. (2016) 9:CD007491. doi: 10.1002/14651858.CD007491.pub2
3. Leff B. Defining and disseminating the hospital-at-home model. Can Med Assoc J. (2009) 180:156–7. doi: 10.1503/cmaj.081891
4. Leff B, Burton L, Mader SL, Naughton B, Burl J, Inouye SK, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med. (2005) 143:798–808. doi: 10.7326/0003-4819-143-11-200512060-00008
5. Shepperd S, Doll H, Angus RM, Clarke MJ, Iliffe S, Kalra L, et al. Avoiding hospital admission through provision of hospital care at home: a systematic review and meta-analysis of individual patient data. CMAJ. (2009) 180:175–82. doi: 10.1503/cmaj.081491
6. Jagannath S, Vesole DH, Zhang M, Desikan KR, Copeland N, Jagannath M, et al. Feasibility and cost-effectiveness of outpatient autotransplants in multiple myeloma. Bone Marrow Transpl. (1997) 20:445–50. doi: 10.1038/sj.bmt.1700900
7. Meisenberg B, Ferran K, Hollenbach K, Brehm T, Jollon J, Piro L. Reduced charges and costs associated with outpatient autologous stem-cell transplantation. Bone Marrow Transpl. (1998) 21:927–32. doi: 10.1038/sj.bmt.1701191
8. Glück S, des Rochers C, Cano C, Dorreen M, Germond C, Gill K, et al. High-dose chemotherapy followed by autologous blood cell transplantation: a safe and effective outpatient approach. Bone Marrow Transpl. (1997) 20:431–34. doi: 10.1038/sj.bmt.1700901
9. Fernández-Avilés F, Carreras E, Urbano-Ispizua A, Rovira M, Martínez C, Gaya A, et al. Case-control comparison of at-home to total hospital care for autologous stem-cell transplantation for hematologic Malignancies. J Clin Oncol. (2006) 24:4855–61. doi: 10.1200/JCO.2006.06.4238
10. Owattanapanich W, Suphadirekkul K, Kunacheewa C, Ungprasert P, Prayongratana K. Risk of febrile neutropenia among patients with multiple myeloma or lymphoma who undergo inpatient versus outpatient autologous stem-cell transplantation: a systematic review and meta-analysis. BMC Cancer. (2018) 18:1126–35. doi: 10.1186/s12885-018-5054-6
11. Martino M, Pellicano G, Moscato T, Massara E, Fedele R, Console G, et al. At-home management of aplastic phase following high-dose melphalan and autologous haematopoietic stem-cell transplantation for multiple myeloma patients: A pilot study. Blood. (2011) 118:4497. doi: 10.1182/blood.V118.21.4497.4497
12. Martino M, Montanari M, Bruno B, Console G, Irrera G, Messina G, et al. Autologous hematopoietic progenitor cell transplantation for multiple myeloma through an outpatient program. Expert Opin Biol Ther. (2012) 12:1449–62. doi: 10.1517/14712598.2012.707185
13. González MJ, Urizar E, Urtaran-Laresgoiti M, Nuño-Solinís R, Lázaro-Pérez E, Vázquez L, et al. Hospital and outpatient models for Hematopoietic Stem-Cell Transplantation: A systematic review of comparative studies for health outcomes, experience of care and costs. PLoS One. (2021) 16:e0254135. doi: 10.1371/journal.pone.0254135
14. Martino M, Lemoli RM, Girmenia C, Castagna L, Bruno B, Cavallo F, et al. Italian consensus conference for the outpatient autologous stem-cell transplantation management in multiple myeloma. Bone Marrow Transpl. (2016) 51:1032–40. doi: 10.1038/bmt.2016.79
15. Ferrara F, Palmieri S, Viola A, Copia C, Schiavone EM, De Simone M, et al. Outpatient-based peripheral blood stem-cell transplantation for patients with multiple myeloma. Hematol J. (2004) 5:222–6. doi: 10.1038/sj.thj.6200349
16. Martino M, Montanari M, Ferrara F, Ciceri F, Scortechini I, Palmieri S, et al. Very low rate of readmission after an early discharge outpatient model for autografting in multiple mieloma patients: an Italian multicenter retrospective study. Biol Blood Marrow Transplant. (2014) 20:1026–32. doi: 10.1016/j.bbmt.2014.03.027
17. Faucher C, Le Corroller Soriano AG, Esterni B, Vey N, Stoppa AM, Chabannon C, et al. Randomized study of early hospital discharge following autologous blood SCT: medical outcomes and hospital costs. Bone Marrow Transpl. (2012) 47:549–55. doi: 10.1038/bmt.2011.126
18. Paul TM, Liu SV, Chong EA, Luger SM, Porter DL, Schuster SJ, et al. Outpatient autologous stem-cell transplantation for patients with myeloma. Clin Lymphoma Myeloma Leuk. (2015) 15:536–40. doi: 10.1016/j.clml.2015.05.006
19. Abid MB, Christopher D, Abid MA, Poon ML, Tan LK, Koh LP, et al. Safety and cost-effectiveness of outpatient autologous transplantation for multiple myeloma in Asia: single-center perspective from Singapore. Bone Marrow Transplant. (2017) 52:1044–6. doi: 10.1038/bmt.2017.77
20. Anastasia A, Giglio F, Mazza R, Sarina B, Todisco E, Bramanti S, et al. Early discharge after high-dose melphalan and peripheral blood stem-cell reinfusion in patients with hematological and non-hematological disease. Leuk Lymphoma. (2009) 50:80–4. doi: 10.1080/10428190802535098
21. Gertz MA, Ansell SM, Dingli D, Dispenzieri A, Buadi FK, Elliott MA, et al. Autologous stem-cell transplant in 716 patients with multiple myeloma: low treatment-related mortality, feasibility of outpatient transplant, and effect of a multidisciplinary quality initiative. Mayo Clin Proc. (2008) 83:1131–5. doi: 10.4065/83.10.1131
22. Gertz MA, Buadi FK, Hayman SR, Lacy MQ, Dispenzieri A, Dingli D, et al. Safety outcomes for autologous stem-cell transplant in multiple myeloma. Mayo Clin Proc. (2018) 93:56–8. doi: 10.1016/j.mayocp.2017.09.012
23. Kassar M, Medoff E, Seropian S, Cooper DL. Outpatient high dose melphalan in multiple myeloma patients. Transfusion. (2007) 47:115–9. doi: 10.1111/j.1537-2995.2007.01073.x
24. Holbro A, Ahmad I, Cohen S, Roy J, Lachance S, Chagnon M, et al. Safety and cost-effectiveness of outpatient autologous stem-cell transplantation in patients with multiple myeloma. Biol Blood Marrow Transpl. (2013) 19:547–51. doi: 10.1016/j.bbmt.2012.12.006
25. Shah N, Cornelison AM, Saliba R, Ahmed S, Nieto YL, Bashir Q, et al. Inpatient vs outpatient autologous hematopoietic stem-cell transplantation for multiple myeloma. Eur J Haematol. (2017) 99:532–35. doi: 10.1111/ejh.12970
26. Kodad SG, Sutherland H, Limvorapitak W, Abou Mourad Y, Barnett MJ, Forrest D, et al. Outpatient autologous stem-cell transplants for multiple myeloma: analysis of safety and outcomes in a tertiary care center. Clin Lymphoma Myeloma Leuk. (2019) 19:784–90. doi: 10.1016/j.clml.2019.09.619
27. Yip HM, Yong K, De-Silva D, Rabin N. Assessing the safety of autologous stem-cell transplant pathway via ambulatory care for patients with multiple myeloma. Hematol Oncol Stem-Cell Ther. (2021) 14:160–2. doi: 10.1016/j.hemonc.2020.01.001
28. Morabito F, Martino M, Stelitano C, Oliva E, Kropp M, Irrera G, et al. Feasibility of a mixed inpatient-outpatient model of peripheral blood stem-cell transplantation for multiple myeloma. Haematologica. (2002) 87(11):1192–9.
29. Clemmons AB, Anderegg S. Mixed outpatient-inpatient autologous stem-cell transplant for multiple myeloma: A cost-saving initiative in a resource constrained environment. J Oncol Pharm Pract. (2017) 23:384–88. doi: 10.1177/1078155216639753
30. Martino M, Russo L, Martinello T, Gallo GA, Fedele R, Moscato T, et al. A home-care, early discharge model after autografting in multiple myeloma: results of a three-arm prospective, non-randomized study. Leuk Lymphoma. (2015) 56:801–4. doi: 10.3109/10428194.2014.931952
31. González-Barrera S, Martín-Sánchez G, Parra-Jordán JJ, Fernández-Luis S, Calvo JA, Lobeira R, et al. Feasibility of a hospital-at-home program for autologous hematopoietic stem-cell transplantation. Transplant Cell Ther. (2023) 29:111.e1–7. doi: 10.1016/j.jtct.2022.11.018
32. Rodríguez-Lobato LG, Martínez-Roca A, Moreno DF, Gutiérrez-García G, Suárez-Lledó M, Rovira M, et al. Impact of intensifying primary antibiotic prophylaxis in at-home autologous stem-cell transplantation program for lymphoma patients. Leuk Lymphoma. (2020) 61(7):1565–74. doi: 10.1080/10428194.2020.1742901
33. Rodríguez-Lobato LG, Martínez-Roca A, Castaño-Díez S, Palomino-Mosquera A, Gutiérrez-García G, Pedraza A, et al. The avoidance of G-CSF and the addition of prophylactic corticosteroids after autologous stem-cell transplantation for multiple myeloma patients appeal for the at-home setting to reduce readmission for neutropenic fever. PloS One. (2020) 15(11):e0241778. doi: 10.1371/journal.pone.0241778
34. Herrmann RP, Trent M, Cooney J, Cannell PK. Infections in patients managed at home during autologous stem-cell transplantation for lymphoma and multiple myeloma. Bone Marrow Transpl. (1999) 24:1213–7. doi: 10.1038/sj.bmt.1702044
35. Graff TM, Singavi AK, Schmidt W, Eastwood D, Drobyski WR, Horowitz M, et al. Safety of outpatient autologous hematopoietic cell transplantation for multiple myeloma and lymphoma. Bone Marrow Transpl. (2015) 50:947–53. doi: 10.1038/bmt.2015.46
36. Lisenko K, Sauer S, Bruckner T, Egerer G, Goldschmidt H, Hillengass J, et al. High-dose chemotherapy and autologous stem-cell transplantation of patients with multiple myeloma in an outpatient setting. BMC Cancer. (2017) 17:151–61. doi: 10.1186/s12885-017-3137-4
37. Obiozor C, Subramaniam DP, Divine C, Shune L, Singh AK, Lin TL, et al. Evaluation of performance status and hematopoietic cell transplantation specific comorbidity index on unplanned admission rates in patients with multiple myeloma undergoing outpatient autologous stem-cell transplantation. Biol Blood Marrow Transpl. (2017) 23:1641–45. doi: 10.1016/j.bbmt.2017.06.001
38. Larsen K, Spencer H, Mohan M, Bailey C, Hill K, Kottarathara M, et al. Feasibility of outpatient stem-cell transplantation in multiple myeloma and risk factors predictive of hospital admission. J Clin Med. (2022) 11:1640–48. doi: 10.3390/jcm11061640
39. Al-Anazi KA, Alshami A, Mutahar E, Abduljalil O, Kanfer S, Kaloyannidis P, et al. Outcome of outpatient autologous hematopoietic stem-cell transplantation in patients with multiple myeloma and relapsed and refractory Hodgkin lymphoma. The experience of king fahad specialist hospital in Dammam, Saudi Arabia. J Stem-Cell Ther Transpl. (2023) 7:003–15. doi: 10.29328/journal.jsctt.1001030
40. Martino M, Ciavarella S, De Summa S, Russo L, Meliambro N, Imbalzano L, et al. A comparative assessment of quality of life in patients with multiple myeloma undergoing autologous stem-cell transplantation through an outpatient and inpatient model. Biol Blood Marrow Transpl. (2018) 24:608–13. doi: 10.1016/j.bbmt.2017.09.021
41. Martino M, Paviglianiti A, Memoli M, Martinelli G, Cerchione C. Multiple myeloma outpatient transplant program in the era of novel agents: state-of-the-art. Front Oncol. (2020) 10:592487. doi: 10.3389/fonc.2020.592487
42. Summers N, Dawe U, Stewart D. A comparison of inpatient and outpatient ASCT. Bone Marrow Transpl. (2000) 26:389–95. doi: 10.1038/sj.bmt.1702534
43. Nawas MT, Landau HJ, Sauter CS, Featherstone CA, Kenny SA, Rodriguez ES, et al. Pilot study of telehealth evaluations in patients undergoing hematopoietic cell transplantation. Biol Blood Marrow Transpl. (2020) 26:e135–7. doi: 10.1016/j.bbmt.2020.02.004
44. Mussetti A, Salas MQ, Condom M, Antonio M, Ochoa C, Ivan I, et al. Use of telehealth for domiciliary follow-up after hematopoietic cell transplantation during the COVID-19 pandemic: prospective pilot study. JMIR Form Res. (2021) 5:e26121. doi: 10.2196/26121
45. Martino M, Pitino A, Tripepi G, Paviglianiti A, Russo L, Cusumano G, et al. The burden in caregivers of multiple myeloma patients undergoing outpatient autologous stem-cell transplantation compared to inpatient transplantation. Clin Lymphoma Myeloma Leuk. (2021) 21:e402–9. doi: 10.1016/j.clml.2020.11.011
46. Stiff P, Mumby P, Miler L, Rodriguez T, Parthswarthy M, Kiley K, et al. Autologous hematopoietic stem-cell transplants that utilize total body irradiation can safely be carried out entirely on an outpatient basis. Bone Marrow Transpl. (2006) 38:757–64. doi: 10.1038/sj.bmt.1705525
47. Frey P, Stinson T, Siston A, Knight S, Ferdman E, Traynor A, et al. Lack of caregivers limits use of outpatient hematopoietic stem-cell transplant program. Bone Marrow Transpl. (2002) 30:741–8. doi: 10.1038/sj.bmt.1703676
48. Dunavin N, Mau LW, Meyer CL, Divine C, Abdallah AO, Leppke S, et al. Health care reimbursement, service utilization, and outcomes among medicare beneficiaries with multiple myeloma receiving autologous hematopoietic cell transplantation in inpatient and outpatient settings. Biol Blood Marrow Transpl. (2020) 26:805–13. doi: 10.1016/j.bbmt.2019.12.772
49. Khouri J, Majhail NS. Advances in delivery of ambulatory autologous stem- cell transplantation for multiple myeloma. Curr Opin Support Palliat Care. (2017) 11:361–5. doi: 10.1097/SPC.0000000000000305
50. Meisenberg BR, Miller WE, McMillan R, Callaghan M, Sloan C, Brehm T, et al. Outpatient high-dose chemotherapy with autologous stem-cell rescue for hematologic and nonhematologic Malignancies. J Clin Oncol. (1997) 15:11–7. doi: 10.1200/JCO.1997.15.1.11
51. Reid RM, Baran A, Friedberg JW, Phillips GL 2nd, Liesveld JL, Becker MW, et al. Outpatient administration of BEAM conditioning prior to autologous stem-cell transplantation for lymphoma is safe, feasible, and cost-effective. Cancer Med. (2016) 5:3059–67. doi: 10.1002/cam4.879
52. Sung AD, Giri VK, Tang H, Nichols KR, Lew MV, Bohannon L, et al. Home-based hematopoietic cell transplantation in the United States. Transplant Cell Ther. (2022) 28:207.e1–8. doi: 10.1016/j.jtct.2022.01.015
53. Leger C, Sabloff M, McDiarmid S, Bence-Bruckler I, Atkins H, Bredeson C, et al. Outpatient autologous hematopoietic stem-cell transplantation for patients with relapsed follicular lymphoma. Ann Hematol. (2006) 85:723–9. doi: 10.1007/s00277-006-0149-6
54. McDiarmid S, Hutton B, Atkins H, Bence-Bruckler I, Bredeson C, Sabri E, et al. Performing allogeneic and autologous hematopoietic SCT in the outpatient setting: effects on infectious complications and early transplant outcomes. Bone Marrow Transpl. (2010) 45:1220–6. doi: 10.1038/bmt.2009.330
55. Jaime-Pérez JC, Hernández-Coronado M, Picón-Galindo E, Salazar-Cavazos L, Gutiérrez-Aguirre CH, Gómez-Almaguer D. Results of a completely outpatient autologous stem-cell transplant program for lymphoma patients receiving reduced-intensity conditioning. Leuk Lymphoma. (2021) 62:1619–28. doi: 10.1080/10428194.2021.1876870
56. Tan XN, Yew CY, Ragg SJ, Harrup RA, Johnston AM. Outpatient autologous stem-cell transplantation in Royal Hobart Hospital, Tasmania: a single-centre, retrospective review in the Australian setting. Intern Med J. (2022) 52:1242–50. doi: 10.1111/imj.15334
57. Westermann AM, Holtkamp MM, Linthorst GA, van Leeuwen L, Willemse EJ, van Dijk WC, et al. At home management of aplastic phase following high-dose chemotherapy with stem-cell rescue for hematological and non-hematological Malignancies. Ann Oncol. (1999) 10:511–7. doi: 10.1023/A:1026427724108
58. Ferrara F, Izzo T, Criscuolo C, Riccardi C, Viola A, Delia R, et al. Comparison of fixed dose pegfilgrastim and daily filgrastim after autologous stem-cell transplantation in patients with multiple myeloma autografted on an outpatient basis. Hematol Oncol. (2011) 29:139–43. doi: 10.1002/hon.978
59. Dytfeld D, Łojko-Dankowska A, Nowicki A, Matuszak M, Wache A, Gil L. Safety and cost effectiveness of outpatient autologous hematopoietic stem-cell transplantation for multiple mieloma- single-center experience of a pilot Early Discharge Program. Acta Haematologica Polonica. (2021) 52:178–81. doi: 10.5603/AHP.a2021.0029
Keywords: autologous hematopoietic stem-cell transplantation, outpatient transplantation, quality of life, hospital-at-home, ambulatory
Citation: Prieto del Prado MÁ and Fernández Avilés F (2024) Ambulatory models for autologous stem-cell transplantation: a systematic review of the health impact. Front. Immunol. 15:1419186. doi: 10.3389/fimmu.2024.1419186
Received: 17 April 2024; Accepted: 02 July 2024;
Published: 16 July 2024.
Edited by:
Giuseppe Milone, University Hospital Polyclinic Vittorio Emanuele, ItalyReviewed by:
Filippo Antonio Canale, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, ItalyPranali Shah, Brigham and Women’s Hospital, and Harvard Medical School, United States
Copyright © 2024 Prieto del Prado and Fernández Avilés. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesc Fernández Avilés, ZmZlcm5hbmRAY2xpbmljLmNhdA==