 Victor M. Cnossen1*
Victor M. Cnossen1* Paula C. Leao Moreira1
Paula C. Leao Moreira1 Othmar G. Engelhardt2
Othmar G. Engelhardt2 Jerzy Samolej2Geert H. Groeneveld3,4
Jerzy Samolej2Geert H. Groeneveld3,4 Simon P. Jochems3
Simon P. Jochems3 Wesley Huisman3
Wesley Huisman3 Gabriel K. Pedersen5
Gabriel K. Pedersen5 Katharina Wørzner5Lukas Recek6
Katharina Wørzner5Lukas Recek6 Giulia Piccini7
Giulia Piccini7 Claudia M. Trombetta7,8Amy Aspelund9Alaura Hoag9Manfred Reiter9Carrie Wick9Thomas Muster9
Claudia M. Trombetta7,8Amy Aspelund9Alaura Hoag9Manfred Reiter9Carrie Wick9Thomas Muster9 Ingrid Maria Catharina Kamerling1,3
Ingrid Maria Catharina Kamerling1,3- 1Centre for Human Drug Research, Leiden, Netherlands
- 2Medicines and Healthcare Products Regulatory Agency, Potters Bar, United Kingdom
- 3Leiden University Center for Infectious Diseases (LU-CID), Leiden University Medical Center, Leiden, Netherlands
- 4Department of Internal Medicine - Acute Internal Medicine, Leiden University Medical Center, Leiden, Netherlands
- 5Center for Vaccine Research, Statens Serum Institut, Copenhagen, Denmark
- 6MediTox S.R.O., Konárovice, Czechia
- 7VisMederi S.r.l., Siena, Italy
- 8Department of Molecular and Developmental Medicine, University of Siena, Siena, Italy
- 9Vivaldi Biosciences, Vienna, Austria
Influenza is a significant global health problem, causing disease and hospitalisations in elderly individuals and infants. While updated vaccines are available every year, their effectiveness is moderate at best. FLUniversal is a European Union funded consortium, aiming to develop a universal influenza vaccine by bringing together partners with expertise in different areas of vaccine development. An intranasal live attenuated vaccine, DeltaFLU, will be produced using an innovative platform; preclinical assessment in animal models and clinical studies using a controlled human infection model (CHIM) will be conducted for assessment of safety, immunogenicity and protective efficacy; and finally, comprehensive immunological analysis of blood and nasal mucosa will elucidate vaccine responses and potential new correlates of protection (CoPs). In addition to a universal influenza vaccine, listed as a top priority by the EU, FLUniversal seeks to deliver an enhanced vaccine manufacturing technology that is superior in terms of efficiency, production costs and production speed - especially critical in the face of a potential new pandemic. Moreover, an influenza CHIM with a focus on harmonisation of clinical procedures and assays will be established to generate translatable and reproducible data. Newly generated knowledge on mechanisms of protection, CoPs and new molecular analysis tools may significantly contribute to our knowledge on influenza infection and influenza vaccines. In conclusion, FLUniversal is an innovative and ambitious public-private partnership, aiming to present a new development pathway for influenza vaccines, and maximising impact by bringing together leading partners from academy and industry with a shared purpose of collaboration and innovation.
Introduction
Influenza is a leading worldwide cause of disease and hospitalisations, affecting elderly and infants most severely (1, 2). Approximately 3 to 5 million severe influenza cases occur each year, and annual deaths are estimated to be up to 600,000 worldwide. Moreover, up to 10% of the general population is affected annually, resulting in lost workdays and a significant economic burden (3). In temperate regions incidence is predominantly seasonal, with outbreaks in the northern hemisphere generally beginning after November, and peaks subsiding before April (4, 5). Currently, several seasonal influenza vaccines are available across a variety of vaccine platforms. However, vaccine effectiveness is moderate at best. Also, vaccine strains need to be updated every year as the haemagglutinin (HA) protein that is the main antigenic target of influenza vaccines, is highly changeable and its evolution is unpredictable (6, 7).
The design for a new influenza vaccine every year is costly and time-consuming. The most widely used production platforms take approximately 6 months; the possibility of a mismatch between available vaccines and circulating strains remains (8). Moreover, clinical evaluation of efficacy is often performed in trials focusing on vaccine immunogenicity to the HA, relying on historic immunological assays predictive of protective efficacy that are possibly inadequate for candidates developed through new platforms (9). Assessing clinical vaccine efficacy in patients is generally complex and expensive: due to the unpredictability of influenza virus circulation, trials often are conducted in multiple geographic locations, and may require up to tens of thousands of participants (10). In addition, these populations are often monitored over multiple influenza seasons, which may further delay vaccine availability and increase the risk of mismatch with newly emerging strains.
Many research teams have been working on the development of universal influenza vaccines, to circumvent the need for yearly updates and to protect against potential future influenza pandemics. This has resulted in the development of new platforms and the design of various vaccine candidates, but major breakthroughs have not been achieved (11). The FLUniversal consortium is developing a vaccine platform consisting of innovative preclinical models, an influenza controlled human infection model (CHIM) to produce results akin to wild-type infection as well as clinical samples, and integrated complex immunological analyses. The platform provides synergy, aids in identifying molecular signatures of protection, and reducing the timeline and risks involved in the clinical development of next-generation vaccines. Using this platform, FLUniversal will develop, manufacture and test an influenza vaccine with the aim of achieving universal or broad cross-protective immunity. Reducing timelines in vaccine design, manufacturing and clinical testing is not only beneficial for the current influenza landscape but also amounts to preparedness for possible future pandemics (12).
CHIMs are innovative clinical trials in which a study population (usually) consisting of healthy volunteers is exposed to the target pathogen and may also be given a vaccine or therapeutic. Conducting a CHIM study facilitates rapid vaccine testing in a relatively small population of healthy volunteers, under safe and controlled circumstances. CHIM studies have been performed for decades; while historically focusing on disease characteristics and immunology, they are increasingly conducted to evaluate new vaccines or therapeutics (13, 14). Clinical endpoints such as protection against virus infection or symptomatic disease are valuable additions to vaccine safety and immunogenicity. In addition, CHIMs can be used to study disease characteristics and immunological endpoints in a thorough and standardised manner (13).
The FLUniversal consortium
FLUniversal is a public-private partnership funded by the European Union’s Horizon Europe research and innovation programme, which started in June 2023. The consortium consists of 8 partners and brings together leading scientific and academic institutions with partners from industry. A vast amount of experience is shared in the consortium, from all aspects of vaccine development: partners have expertise in vaccine design and manufacturing, (pre-)clinical evaluation, CHIMs, standardisation of assays and immunological assessment of vaccines and influenza infection (15). The partners, goals and methods of FLUniversal are comprehensively outlined at https://www.fluniversal.eu/. In this paper, we outline the different areas of innovation that FLUniversal will contribute to.
Areas of innovation
DeltaFLU
FLUniversal aims to advance DeltaFLU, a vaccine containing live replication-deficient influenza strains lacking the NS1 protein. The influenza NS1 protein acts as an interferon antagonist; the attenuated influenza strains lacking NS1 induce an interferon response and lead to durable protection through the induction of memory T and B cells (16–18). DeltaFLU is to be administered intranasally, thus inducing mucosal (IgA and tissue-resident memory mediated) immunity resulting in local protection and prevention of further virus transmission. The vaccine is designed to protect against all influenza virus strains; it targets all viral antigens and induces effective T cell-mediated immunity against conserved internal proteins, and B cell-mediated immunity against the conserved stem structure of the HA, which is typically poorly immunogenic. This broad cross-protection will be achieved using a prime-boost immunisation (PBI) regimen to direct the immune responses to conserved regions of the virus. The PBI regimen is a combination of the DeltaFLU influenza strains lacking NS1, paired with wild-type HA proteins that all have different head regions but homologous stalk regions. This combination is expected to also induce HA stalk directed antibodies, which may confer broad cross-protection against influenza, as the HA stalk region is highly conserved across wild-type influenza strains. Vaccines containing isolated stalk regions generally induce poor immune responses, and are often unstable when combined with other, more immunogenic HA regions. The PBI strategy is a simple yet innovative regimen, with the aim to overcome these challenges in achieving universal protection against influenza. FLUniversal will primarily test the PBI regimen with influenza A group 2 HA proteins (H3 and H7), which have been generated and have met all testing criteria to be manufactured for use in clinical trials in 2025. In parallel, combinations including also influenza A group 1 and B HA proteins are being developed separately from the consortium.
Vaccine strain production
Most current influenza vaccines consist of inactivated influenza viruses produced in embryonated chicken eggs. Commonly, three or four influenza strains are selected; selected influenza A viruses are usually reassorted with the master strain A/Puerto Rico/8/34. These hybrid viruses are then inoculated into the eggs, from which the virus can be harvested, purified, chemically inactivated or split, and formulated to produce an inactivated vaccine. Licensed live attenuated vaccines, based on influenza virus strains with multiple cold-adapted and other function-modulating point mutations, also are produced on embryonated chicken eggs. The time between strain selection and vaccine distribution is approximately 6 months. This time gap may sometimes result in a mismatch between the available vaccine and circulating influenza strains, if the latter have acquired antigenically relevant amino acid substitutions in the HA during this period. The mismatch may increase when mutations occur during the egg-based manufacturing, or when the development process is delayed by one of several recognised potential hurdles (19). Several emerging vaccine technologies, such as mRNA-based vaccines, viral vector systems and nanoparticle-based platforms, are being explored for universal vaccine development (11). Table 1 provides an overview of several of these cross-protective vaccine technologies in development.

Table 1. Strategies/platforms for developing cross-protective vaccines.
FLUniversal partner Vivaldi Biosciences, based in Austria, has developed an alternative vaccine production platform: a Vero cell-based manufacturing system, more flexible compared to egg-based development with a lower risk of changes in the HA protein throughout the process. In addition, the platform used to produce DeltaFLU is readily scalable, with a virtually unlimited substrate – making it preferable to egg-based systems in the event of a pandemic. Technologies improving strain growth and vaccine purity and potency result in a high downstream yield of the influenza vaccine strains lacking NS1. The increased efficiency of the platform amounts to a production time of seven weeks, which is significantly shorter than timelines in conventional influenza vaccine production.
Preclinical evaluation
Preclinical assessment of DeltaFLU toxicity, safety and tolerability will be performed in ferret models at MediTox S.R.O., based in Czech Republic. After vaccination, ferrets will be extensively assessed for toxicity, including neuro- and immunotoxicity, as well as shedding and biodistribution of the different vaccine strains. Immunology will focus also on nasal IgA levels, and the functional activity of vaccine-induced antibodies against H1N1, H3N2 and influenza B viruses, to demonstrate the universal protection induced by the immunisation strategy. Finally, ferrets will be challenged with highly divergent H1N1, H3N2 and influenza B wild-type strains, in a placebo-controlled setting, to demonstrate protective efficacy of the vaccine.
In addition, immunogenicity of the vaccine will be assessed in a Syrian golden hamster model at the Statens Serum Institute (SSI), based in Denmark. Recent studies highlight that Syrian hamsters are sensitive to influenza viruses, including recent H3N2 strains, without adaptation (20). While hamsters do not resemble human influenza infection as closely as ferrets, they are easier to handle and allow for a wide variety of immunological analyses (21). The hamster model has already been established at SSI using the A/Brisbane/10/07 H3N2 virus, and DeltaFLU will be assessed in the model parallel to the clinical trials. After intranasal vaccination, single-cell-RNA sequencing will be performed on blood, and local secretory IgA responses will be assessed. The vaccinated hamsters will also be challenged with wild-type viruses in a placebo-controlled setting; nasal-associated lymphoid tissue will be evaluated for various cellular responses and correlated with protection against influenza infection. This cutting-edge animal model provides an innovative platform for preclinical vaccine testing.
Early clinical vaccine evaluation
Following preclinical evaluation, the Centre for Human Drug Research (CHDR) will test the universal DeltaFLU in a first-in-human, phase 1 clinical trial, focusing on safety and immunogenicity for influenza type A group 2. Subsequently, a CHIM study will be conducted in which additional safety data will be collected and protective efficacy will be evaluated in a randomised, placebo-controlled setting. Clinical endpoints (e.g., safety parameters and symptom scores) will be combined with virological and immunological analyses, performed on nasal and blood samples.
For our CHIM, the reverse genetics influenza virus strain A/Texas/71/2017 (H3N2) will be used as a challenge agent. This influenza strain was manufactured according to Good Manufacturing Practice (GMP) in the United States and tested in a dose-titration CHIM at the US National Institute of Allergy and Infectious Diseases (NIAID) to assess safety and infection rate in healthy volunteers (22). An acknowledged issue in the design and execution of CHIMs is the variability in infection rate between continents and study centres, even when identical challenge strains and doses are used. This can be attributed to variability between challenge lots and stability over time, heterogeneity of handling, transport, QC procedures, type and quality of performed assays, sampling techniques and differences in background immunity between regions (23). As a consequence, an important step in the clinical evaluation is to establish a CHIM using the A/Texas/71/2017 strain at the Centre for Human Drug Research (CHDR), based in The Netherlands. In this first implementation trial, 10 healthy volunteers will be inoculated with the challenge strain, without administration of the vaccine. The validation of the challenge agent as well as the harmonisation of clinical procedures (e.g., virus administration, nasal sampling techniques, and virological and immunological analyses) will be the most important focus points of this trial, which is planned to be performed in 2025.
The principal innovative aspect of a CHIM in the context of vaccine development is the ability to evaluate protective efficacy early in clinical development in a smaller trial compared to conventional phase 2 and 3 studies (24). The WHO endorses the use of influenza CHIMs for vaccine development, as they are generally safe and can provide a wide array of insights (25). While the protective efficacy of a vaccine, as assessed by a CHIM, may not be entirely translatable to a real-world setting, a CHIM can provide the basis for an early go/no-go decision to move a vaccine candidate to the next clinical testing stage. Although CHIMs generally cannot replace conventional real-world efficacy trials, they can nevertheless allow vaccine candidates to ‘fail fast’, i.e., to show a lack of efficacy early in clinical testing, leading to early termination and saving significant time and costs when compared to the conventional pathway of vaccine development. With a pipeline with several vaccine candidates, using a CHIM to gain preliminary information on protective efficacy is highly valuable, as illustrated in Figure 1.
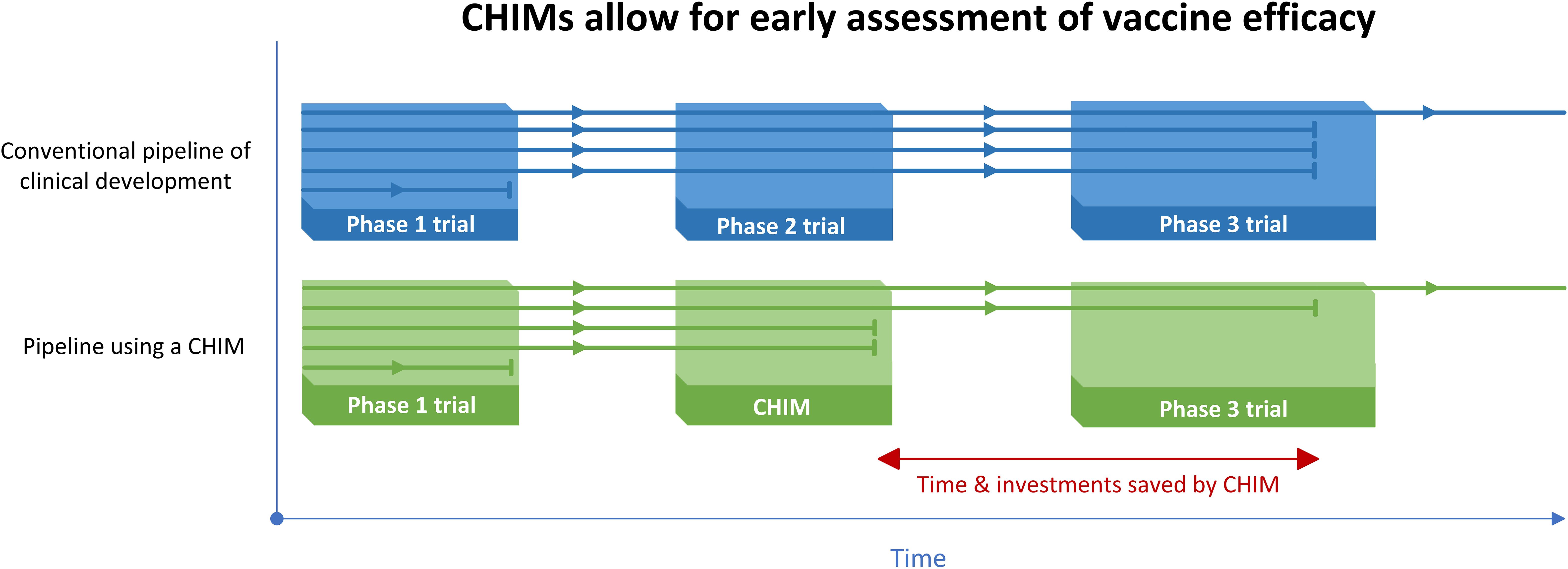
Figure 1. Illustration of the value of using a CHIM with multiple vaccine candidates in the pipeline, with each horizontal line representing a vaccine candidate going through different clinical testing phases. CHIMs allow ineffective vaccines to ‘fail fast’, compared to the conventional vaccine development pathway. This way, resources are saved and pursuing of more promising candidates can be ‘de-risked’ (26).
The combination of a CHIM implementation study, a conventional phase 1 study, and a placebo-controlled vaccine CHIM study, will provide a comprehensive set of clinical, pharmacological and immunological data on DeltaFLU. Data collected in the influenza CHIM, thoughtfully implemented and validated and with use of harmonised clinical and laboratory procedures, will provide valuable preliminary data on vaccine efficacy, at an early stage in clinical development.
Immunology and correlates of protection
After the clinical trials assessing DeltaFLU, a substantial collection of clinical samples will be available for immunological analysis. CHIMs can be useful not only for testing of new vaccines and therapeutics, but also to study disease characteristics and to identify immunological factors contributing to and indicative of protection against clinical disease. These correlates of protection (CoPs) are relevant for estimating the protective efficacy of vaccines in an early clinical development stage. CoPs are relatively well established for some pathogens (e.g. serum neutralising antibodies against SARS-CoV-2), while for other pathogens no clear CoP has been established (e.g. respiratory syncytial virus (RSV)) (27, 28). For influenza, a CoP was identified already in 1970s: a virus-specific haemagglutination inhibition (HAI) titre of 1:40 is associated with 50% protection against virus infection, and protection increases as HAI titres rise (29).
Currently, approval of influenza vaccines is based on their ability to increase HAI titres in healthy adults or in older adults; the extensive track record of the HAI assay in trials studying vaccine immunogenicity has eliminated the need for large, costly and time-consuming efficacy trials for a large group of vaccine candidates (12, 30). However, the HAI assay sometimes fails to predict a vaccine’s protective efficacy. There are several aspects of the assay that lead to this limitation: first, the HAI assay is a marker of systemic immunity, providing little information on the local nasal immunity associated with mucosal IgA antibodies (31). Second, it is not representative of cellular immunological processes contributing to protection against infection, which are associated with broader protective immunity and hypothesised to play a significant role in adult immunity against influenza (32). Third, it demonstrates a broad estimate of functional activity of all available HAI-active antibodies and cannot distinguish between antibodies with relatively high or low virus neutralising capacity. Finally, the correlation with protective efficacy is variable or even absent for some vaccine types and technologies, including universal vaccines (9, 33–35).
FLUniversal aims to identify new CoPs for influenza that may circumvent some of these limitations. Using state of the art minimally-invasive approaches to collect upper respiratory tract samples, we will be able to also investigate both humoral (Nasosorptions) and cellular immunity (nasal FLOQswabs) at the site of infection (36–41). These minimally-invasive nasal and blood samples (38), collected during the influenza CHIM, will be analysed using a wide variety of assays: virus neutralising antibodies, HAI antibodies and ELISA antibodies reacting with the whole HA protein, HA subunits and epitopes of the HA stalk; mucosal assays to detect virus neutralising and IgG/IgA antibodies, cytokines and nasal tissue-resident memory T-cells (37). On top of that, spectral flow cytometry will be used to detect and characterise in-depth antigen-specific CD8+ and CD4+ T-cells from nasal samples and PBMCs, whereas memory B-cells (42) will be additionall investigatedin peripheral blood mononuclear cells (PBMCs). Performing the analyses on both blood and nasal mucosa samples allows to understand the effect of compartmentalisation in the context of nasal vaccination. We expect that the combination of mucosal immune measurements with a large number of CHIM samples has the ability to define correlates of protection against influenza infection, which we will then assess also in animal models. FLUniversal aims to use harmonised immunological assays and biological standards to allow comparison within the consortium, and externally (43–45). Immune assays will be performed by the Leiden University Medical Centre (LUMC), The Netherlands; Medicines and Healthcare products Regulatory Agency (MHRA), United Kingdom; and VisMederi, Italy.
The clinical outcomes of the influenza CHIM will be integrated with pre-challenge immunological assay results to identify potential CoPs. Advanced machine learning approaches will be employed to explore relationships between clinical and immunological data, with feature selection performed using Elastic Net regularisation to identify the most predictive immune markers (46, 47) and random forest algorithms (48) to capture complex interactions between immune responses and protection. Transcriptional data will be analysed using mixOmics feature selection (49) to identify key molecular signatures associated with protection. Furthermore, datasets from the clinical study will be compared with protection data from preclinical animal models to establish a comprehensive and robust framework for identifying CoPs.
Discussion
FLUniversal addresses the critical global health priority of developing new and improved vaccines, particularly universal influenza vaccines. The consortium combines a replication-deficient live attenuated influenza vaccines platform based on deletion of NS1, with innovative technologies for vaccine design, production and immunisation, and state-of-the-art methodologies for preclinical, clinical and immunological evaluation. The progression of DeltaFLU through various stages of vaccine research within a multidisciplinary consortium, integrating complementary areas of expertise, provides significant advantages in enhancing both the effectiveness and efficiency of the vaccine development process.
This initiative is driven by the urgent need for innovative approaches to overcome scientific, logistical, and societal challenges. The need for a universal influenza vaccine is well recognised, and the use of existing vaccine platforms has not yet led to success, shifting the focus towards new technologies as shown in Table 1 (11). These technologies each face challenges in achieving universal protection: vaccines targeting broadly conserved regions of influenza viruses often require innovative delivery systems or adjuvants to compensate for their poor immunogenicity (50); multivalent vaccines are highly immunogenic and can induce broad protection, yet face challenges in manufacturing scalability and consistency (51, 52); use of genetic platforms such as mRNA and viral vector-based vaccines confer strong but relatively short-lasting immunogenicity, but face limitations in technological requirements for production and storage (53, 54). These novel technologies increasingly gain attention, and combining platforms (e.g., prime-boost regimens targeting conserved T and B cell epitopes), could offer a promising path toward universal or broadly cross-protective protection against influenza (11, 55). Moreover, the definition of a universal influenza vaccine has been topic of discussion: ideally, these vaccines should protect against all influenza A and B viruses, as well as existing or emergent zoonotic viruses with pandemic potential (56). However, it is recognised that this may not be achievable at all, and the WHO has published a Proposed Product Characteristic for universal or broad cross-protective vaccines (57). These discussions, as well as the high failure rate of previous attempts underscore the challenges inherent in vaccine development; an example is the Multimeric-001 vaccine, which failed to show clinical efficacy in a large phase 3 trial, despite robust T-cell responses in earlier trials (58–60). This highlights the importance of early indications of vaccine efficacy, where CHIMs have proven to be particularly advantageous.
CHIMs have emerged as invaluable tools in vaccine research, significantly reducing the risks associated with clinical vaccine testing and potentially avoiding substantial investments in ineffective candidates. Unlike large field trials, which rely on the unpredictable occurrence of natural infections to assess vaccine efficacy, CHIMs provide robust preliminary data on protective efficacy using smaller cohorts and shorter timelines. Historically, CHIMs have successfully accelerated vaccine development for diseases such as cholera, typhoid and malaria, enabling researchers to quickly identify promising candidates and eliminate ineffective ones early on (61–64). CHIMs offer additional advantages: the harmonised timing and collection of samples, coupled with safe and controlled conditions, produce reliable data on virological and immunological processes associated with infection and protection. The establishment of an influenza CHIM at CHDR enables a swift preliminary assessment of DeltaFLU’s protective efficacy; moreover, it provides a comprehensive platform to test future vaccine candidates targeting circulating influenza strains or potential pandemic pathogens. The expertise gained in standardised clinical procedures and harmonised sampling and immunological analyses is adaptable to a wide range of pathogens.
Other international projects focusing on influenza research and vaccines include the Collaborative Influenza Vaccine Innovation Centers (CIVICs) (65) funded by NIAID, and Inno4Vac, funded by the Innovative Medicines Initiative (IMI) (66). Beyond research and development projects, international collaboration is also supported by initiatives such as assay harmonisation—a field where the IMI-funded FLUCOP consortium has made significant contributions (43, 44) – open science, and improved data management. Aligning with these global efforts, FLUniversal aims to promote reproducibility, transparency, and global accessibility of scientific data and methodologies in vaccine development.
In conclusion, the FLUniversal consortium intends not only to develop a universal influenza vaccine, but also to deliver an innovative and versatile vaccine platform, based on novel technologies in vaccine production, as well as an efficient pathway for the (pre)clinical evaluation of vaccine candidates and identification of correlates of protection. This way, FLUniversal can support meeting a critical global health need, contribute to pandemic preparedness and leave a lasting legacy in the form of a versatile and efficient platform for vaccine development.
Ethics statement
The FLUniversal consortium established an external Ethics Advisory Board (EAB) to provide advice and oversight for the research programs to be carried out by the consortium. The EAB consists of fully independent board members with experience in ethical topics related to the various aspects of the FLUniversal activities. The appointed experts provide the consortium the latest information about ethics and regulations, ensure that the existing rules are adhered to, monitor the work performed by the consortium and advise it when ethics issues arise that are not governed by the ethics routines installed. Potential ethical concerns are reported periodically or ad hoc to the EAB. In addition, advice can be sought from the Department of Ethics of FLUniversal partner LUMC, in case this is needed for human studies within FLUniversal. All ethics approvals, measures and considerations will comply with requirements of HCT (for human cells), animal experiments, and authorisations for relevant facilities (i.e., security classification of laboratory, GMO authorisation). A report by the EAB must be submitted at the end of each reporting period of the consortium.
The protocols of the clinical trials to be conducted in the FLUniversal consortium will be submitted for approval by the Dutch Central Committee on Research Involving Human Subjects (CCMO), and the Scientific Advisory Board of CHDR. The studies will be conducted in full compliance with the principles of the Declaration of Helsinki and ICH GCP guidelines. For every participant, written informed consent will be obtained before any study procedures take place. Changes to the protocol regarding trial design and/or safety of participants will only be implemented after approval by the CCMO. FLUniversal aims to involve former challenge trial participants during the writing of the CHIM study protocol(s); either by analysing previously gathered data or by active involvement of initiatives such as 1Day Sooner (https://www.1daysooner.org/). The results of the individual studies will be reported to the Ethics Committee and EAB shortly after the end of the study. In accordance with standard editorial and ethical practice, the results of the studies will be published. Guidelines regarding (co-)authorship, such as the Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals, will be followed.
Author contributions
VC: Conceptualization, Investigation, Visualization, Writing – original draft, Writing – review & editing. PL: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. OE: Writing – review & editing. JS: Writing – review & editing. GG: Writing – review & editing. SJ: Writing – review & editing. WH: Writing – review & editing. GPe: Resources, Writing – review & editing. KW: Writing – review & editing. LR: Writing – review & editing. GPi: Writing – review & editing. CT: Writing – review & editing. AA: Writing – review & editing. AH: Writing – review & editing. MR: Writing – review & editing. CW: Writing – review & editing. TM: Supervision, Writing – review & editing. IK: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the European Union (grant agreement No.101080692).
Conflict of interest
Author LR was employed by company MediTx S.R.O. Author GPi and CT were employed by the company VisMederi S.r.l. Authors AA, AH, MR, CW and TM were employed by company Vivaldi Biosciences.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
Views and opinions expressed are those of the author(s) only and do not necessarily reflect those of the European Union or the European Health and Digital Executive Agency (HADEA). Neither the European Union nor HADEA can be held responsible for them.
References
1. Cromer D, van Hoek AJ, Jit M, Edmunds WJ, Fleming D, and Miller E. The burden of influenza in England by age and clinical risk group: A statistical analysis to inform vaccine policy. J Infect. (2014) 68:363–71. doi: 10.1016/j.jinf.2013.11.013
3. Gasparini R, Amicizia D, Lai PL, and Panatto D. Clinical and socioeconomic impact of seasonal and pandemic influenza in adults and the elderly. Hum Vacc Immunother. (2012) 8:21–8. doi: 10.4161/hv.8.1.17622
4. Monto AS. Epidemiology of influenza. Vaccine. (2008) 26:D45–8. doi: 10.1016/j.vaccine.2008.07.066
5. Monto AS and Kioumehr F. The tecumseh study of respiratory illness: IX. Occurrence of influenza in the community, 1966–19711. Am J Epidemiol. (1975) 102:553–63. doi: 10.1093/oxfordjournals.aje.a112193
6. Sekiya T, Ohno M, Nomura N, Handabile C, Shingai M, Jackson DC, et al. Selecting and using the appropriate influenza vaccine for each individual. Viruses. (2021) 13:971. doi: 10.3390/v13060971
7. Kim SS, Flannery B, Foppa IM, Chung JR, Nowalk MP, Zimmerman RK, et al. Effects of prior season vaccination on current season vaccine effectiveness in the United States flu vaccine effectiveness network, 2012–2013 through 2017–2018. Clin Infect Dis. (2021) 73:497–505. doi: 10.1093/cid/ciaa706
8. de Jong JC, Rimmelzwaan GF, Fouchier RAM, and Osterhaus ADME. Influenza virus: a master of metamorphosis. J Infect. (2000) 40:218–28. doi: 10.1053/jinf.2000.0652
9. Cowling BJ, Lim WW, Perera RAPM, Fang VJ, Leung GM, Peiris JSM, et al. Influenza hemagglutination-inhibition antibody titer as a mediator of vaccine-induced protection for influenza B. Clin Infect Dis. (2019) 68:1713–7. doi: 10.1093/cid/ciy759
10. Papi A, Ison MG, Langley JM, Lee DG, Leroux-Roels I, Martinon-Torres F, et al. Respiratory syncytial virus prefusion F protein vaccine in older adults. N Engl J Med. (2023) 388:595–608. doi: 10.1056/NEJMoa2209604
11. Wang WC, Sayedahmed EE, Sambhara S, and Mittal SK. Progress towards the development of a universal influenza vaccine. Viruses. (2022) 14(8):1684. doi: 10.3390/v14081684
12. He X, Zhang T, Huan S, and Yang Y. Novel influenza vaccines: from research and development (R&D) challenges to regulatory responses. Vaccines. (2023) 11(10):1573. doi: 10.3390/vaccines11101573
13. Habibi MS and Chiu C. Controlled human infection with RSV: The opportunities of experimental challenge. Vaccine. (2017) 35:489–95. doi: 10.1016/j.vaccine.2016.08.086
14. Choy RKM, Bourgeois AL, Ockenhouse CF, Walker RI, Sheets RL, and Flores J. Controlled human infection models to accelerate vaccine development. Clin Microbiol Rev. (2022) 35:e0000821. doi: 10.1128/cmr.00008-21
15. FLUniversal. Available online at: https://www.fluniversal.eu/ (Accessed January 30, 2025).
16. García-Sastre A, Egorov A, Matassov D, Brandt S, Levy DE, Durbin JE, et al. Influenza A virus lacking the NS1 gene replicates in interferon-deficient systems. Virology. (1998) 252:324–30. doi: 10.1006/viro.1998.9508
17. Diebold SS, Montoya M, Unger H, Alexopoulou L, Roy P, Haswell LE, et al. Viral infection switches non-plasmacytoid dendritic cells into high interferon producers. Nature. (2003) 424:324–8. doi: 10.1038/nature01783
18. Mueller SN, Langley WA, Carnero E, García-Sastre A, and Ahmed R. Immunization with live attenuated influenza viruses that express altered NS1 proteins results in potent and protective memory CD8+ T-cell responses. J Virol. (2010) 84:1847–55. doi: 10.1128/jvi.01317-09
19. Wong SS and Webby RJ. Traditional and new influenza vaccines. Clin Microbiol Rev. (2013) 26:476–92. doi: 10.1128/CMR.00097-12
20. Paterson J, Ryan KA, Morley D, Jones NJ, Yeates P, Hall Y, et al. Infection with seasonal H1N1 influenza results in comparable disease kinetics and host immune responses in ferrets and golden Syrian hamsters. Pathogens. (2023) 12(5):668. doi: 10.3390/pathogens12050668
21. Iwatsuki-Horimoto K, Nakajima N, Ichiko Y, Sakai-Tagawa Y, Noda T, Hasegawa H, et al. Syrian hamster as an animal model for the study of human influenza virus infection. J Virol. (2018) 92. doi: 10.1128/JVI.01693-17
22. A Multicenter, Blinded, Randomized, Placebo-Controlled, Dose-Ranging Influenza Challenge Study in Healthy Adult Volunteers to Determine the Optimal Infection Dose and Safety of a Recombinant H3N2 (A/Texas/71/2017 (H3N2), Clade 3C3a) Influenza Challenge Virus (202). Available online at: https://clinicaltrials.gov/study/NCT04978454 (Accessed August 19, 2021).
23. Balasingam S and Wilder-Smith A. Randomized controlled trials for influenza drugs and vaccines: a review of controlled human infection studies. Int J Infect Dis. (2016) 49:18–29. doi: 10.1016/j.ijid.2016.05.013
24. Roestenberg M, Kamerling IMC, and De Visser SJ. Controlled human infections as a tool to reduce uncertainty in clinical vaccine development. Front Med. (2018) 5:297. doi: 10.3389/fmed.2018.00297
25. World Health Organization. WHO guidance on the ethical conduct of controlled human infection studies (2021). Available online at: https://www.who.int/publications/i/item/9789240037816 (Accessed January 30, 2025).
26. Cnossen VM, van Leeuwen RP, Mazur NI, Vernhes C, Voorde ten W, Burggraaf J, et al. From setbacks to success: lessons from the journey of RSV vaccine development. Ther Adv Vacc Immunother. (2024) 12:25151355241308305. doi: 10.1177/25151355241308305
27. Goldblatt D, Alter G, Crotty S, and Plotkin SA. Correlates of protection against SARS-CoV-2 infection and COVID-19 disease. Immunol Rev. (2022) 310:6–26. doi: 10.1111/imr.13091
28. Mazur NI, Terstappen J, Baral R, Bardají A, Beutels P, Buchholz UJ, et al. Respiratory syncytial virus prevention within reach: the vaccine and monoclonal antibody landscape. Lancet Infect Dis. (2023) 23:e2–e21. doi: 10.1016/S1473-3099(22)00291-2
29. Black S, Nicolay U, Vesikari T, Knuf M, Giudice Del G, Cioppa Della G, et al. Hemagglutination inhibition antibody titers as a correlate of protection for inactivated influenza vaccines in children. Pediatr Infect Dis J. (2011) 30. Available at: https://journals.lww.com/pidj/fulltext/2011/12000/hemagglutination_inhibition_antibody_titers_as_a.14.aspx (Accessed January 30, 2025).
30. Wijnans L and Voordouw B. A review of the changes to the licensing of influenza vaccines in Europe. Influenza Other Resp Virus. (2016) 10:2–8. doi: 10.1111/irv.12351
31. Gould VMW, Francis JN, Anderson KJ, Georges B, Cope AV, and Tregoning JS. Nasal igA provides protection against human influenza challenge in volunteers with low serum influenza antibody titre. Front Microbiol. (2017) 8:900. doi: 10.3389/fmicb.2017.00900
32. McElhaney JE, Xie D, Hager WD, Barry MB, Wang Y, Kleppinger A, et al. T cell responses are better correlates of vaccine protection in the elderly. J Immunol. (2006) 176:6333–9. doi: 10.4049/jimmunol.176.10.6333
33. Barrett PN, Berezuk G, Fritsch S, Aichinger G, Hart MK, El-Amin W, et al. Efficacy, safety, and immunogenicity of a Vero-cell-culture-derived trivalent influenza vaccine: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet. (2011) 377:751–9. doi: 10.1016/S0140-6736(10)62228-3
34. Dunning Andrew J, DiazGranados Carlos A, Voloshen T, Hu B, Landolfi VA, and Keipp TH. Correlates of protection against influenza in the elderly: results from an influenza vaccine efficacy trial. Clin Vacc Immunol. (2016) 23:228–35. doi: 10.1128/CVI.00604-15
35. Ward BJ, Pillet S, Charland N, Trepanier S, Couillard J, and Landry N. The establishment of surrogates and correlates of protection: Useful tools for the licensure of effective influenza vaccines? Hum Vacc Immunother. (2018) 14:647–56. doi: 10.1080/21645515.2017.1413518
36. van Dorst MMAR, Azimi S, Wahyuni S, Amaruddin A, Sartono E, Wammes LJ, et al. Differences in bacterial colonization and mucosal responses between high and low SES children in Indonesia. Pediatr Infect Dis J. (2022) 41. Available at: https://journals.lww.com/pidj/fulltext/2022/06000/differences_in_bacterial_colonization_and_mucosal.13.aspx (Accessed January 30, 2025).
37. Roukens AHE, Pothast CR, König M, Huisman W, Dalebout T, Tak T, et al. Prolonged activation of nasal immune cell populations and development of tissue-resident SARS-CoV-2-specific CD8+ T cell responses following COVID-19. Nat Immunol. (2022) 23:23–32. doi: 10.1038/s41590-021-01095-w
38. Jochems SP, Piddock K, Rylance J, Adler H, Carniel BF, Collins A, et al. Novel analysis of immune cells from nasal microbiopsy demonstrates reliable, reproducible data for immune populations, and superior cytokine detection compared to nasal wash. PloS One. (2017) 12:e0169805. doi: 10.1371/journal.pone.0169805
39. Carniel BF, Marcon F, Rylance J, German EL, Zaidi S, Reiné J, et al. Pneumococcal colonization impairs mucosal immune responses to live attenuated influenza vaccine. JCI Insight. (2021) 6(4):e141088. doi: 10.1172/jci.insight.141088
40. Lim JME, Tan AT, and Bertoletti A. Protocol to detect antigen-specific nasal-resident T cells in humans. STAR Protoc. (2023) 4:101995. doi: 10.1016/j.xpro.2022.101995
41. de Silva TI, Gould V, Mohammed NI, Cope A, Meijer A, Zutt I, et al. Comparison of mucosal lining fluid sampling methods and influenza-specific IgA detection assays for use in human studies of influenza immunity. J Immunol Methods. (2017) 449:1–6. doi: 10.1016/j.jim.2017.06.008
42. Prins MLM, Roozen GVT, Pothast CR, Huisman W, Binnendijk van R, Hartog den G, et al. Immunogenicity and reactogenicity of intradermal mRNA-1273 SARS-CoV-2 vaccination: a non-inferiority, randomized-controlled trial. NPJ Vacc. (2024) 9:1. doi: 10.1038/s41541-023-00785-w
43. Begue S, Waerlop G, Salaun B, Janssens M, Bellamy D, Cox RJ, et al. Harmonization and qualification of intracellular cytokine staining to measure influenza-specific CD4+ T cell immunity within the FLUCOP consortium. Front Immunol. (2022) 13. doi: 10.3389/fimmu.2022.982887
44. Waldock J, Zheng L, Remarque EJ, Civet A, Hu B, Jalloh SL, et al. Assay harmonization and use of biological standards to improve the reproducibility of the hemagglutination inhibition assay: a FLUCOP collaborative study. mSphere. (2021) 6. doi: 10.1128/msphere.00567-21
45. Waerlop G, Leroux-Roels G, Pagnon A, Begue S, Salaun B, Janssens M, et al. Proficiency tests to evaluate the impact on assay outcomes of harmonized influenza-specific Intracellular Cytokine Staining (ICS) and IFN-γ Enzyme-Linked ImmunoSpot (ELISpot) protocols. J Immunol Methods. (2023) 523:113584. doi: 10.1016/j.jim.2023.113584
46. Kurtovic L, Feng G, Hysa A, Haghiri A, O'Flaherty K, Wines BW, et al. Antibody mechanisms of protection against malaria in RTS,S-vaccinated children: a post-hoc serological analysis of phase 2 trial. Lancet Microbe. (2024) 5:100898. doi: 10.1016/S2666-5247(24)00130-7
47. Ehrenberg PK, Shangguan S, Issac B, Alter G, Geretz A, Izumi T, et al. A vaccine-induced gene expression signature correlates with protection against SIV and HIV in multiple trials. Sci Trans Med. (2019) 11:eaaw4236. doi: 10.1126/scitranslmed.aaw4236
48. McIlwain DR, Chen H, Rahil Z, Aghaeepour N, Tucker SN, Nolan GP, et al. Human influenza virus challenge identifies cellular correlates of protection for oral vaccination. Cell Host Microbe. (2021) 29:1828–1837.e5. doi: 10.1016/j.chom.2021.10.009
49. Rohart F, Gautier B, Singh A, and Lê Cao KA. mixOmics: An R package for ‘omics feature selection and multiple data integration. PloS Comput Biol. (2017) 13:e1005752. doi: 10.1371/journal.pcbi.1005752
50. Jazayeri SD and Poh CL. Development of universal influenza vaccines targeting conserved viral proteins. Vaccines. (2019) 7(4):169. doi: 10.3390/vaccines7040169
51. Uno N and Ross TM. Multivalent next generation influenza virus vaccines protect against seasonal and pre-pandemic viruses. Sci Reports. (2024) 14:1440. doi: 10.1038/s41598-023-51024-0
52. Shinde V, Cho I, Plested JS, Agrawal S, Fiske J, Cai R, et al. Comparison of the safety and immunogenicity of a novel Matrix-M-adjuvanted nanoparticle influenza vaccine with a quadrivalent seasonal influenza vaccine in older adults: a phase 3 randomised controlled trial. Lancet Infect Dis. (2022) 22:73–84. doi: 10.1016/S1473-3099(21)00192-4
53. Gote V, Bolla PK, Kommineni N, Butreddy A, Nukala PK, Palakurthi SSP, et al. A comprehensive review of mRNA vaccines. Int J Mol Sci. (2023) 24(3):2700. doi: 10.3390/ijms24032700
54. Bahl K, Senn JJ, Yuzhakov O, Bulychev A, Brito LA, Hassett KJ, et al. Preclinical and Clinical Demonstration of Immunogenicity by mRNA Vaccines against H10N8 and H7N9 Influenza Viruses. Mol Ther. (2017) 25:1316–27. doi: 10.1016/j.ymthe.2017.03.035
55. Ullah S and Ross TM. Next generation live-attenuated influenza vaccine platforms. Expert Rev Vacc. (2022) 21:1097–110. doi: 10.1080/14760584.2022.2072301
56. Taaffe J, Ostrowsky JT, Mott J, Goldin S, Friede M, Gsell P, et al. Advancing influenza vaccines: A review of next-generation candidates and their potential for global health impact. Vaccine. (2024) 42:126408. doi: 10.1016/j.vaccine.2024.126408
57. World Health Organization. WHO Preferred Product Characteristics for next Generation Influenza Vaccines. Geneva, Switzerland: World Health Organization (2017). Available at: https://iris.who.int/handle/10665/258767.
58. Atsmon J, Caraco Y, Ziv-Sefer S, Shaikevich D, Abramov E, Volokhov I, et al. Priming by a novel universal influenza vaccine (Multimeric-001)—A gateway for improving immune response in the elderly population. Vaccine. (2014) 32:5816–23. doi: 10.1016/j.vaccine.2014.08.031
59. Atmar RL, Bernstein DI, Winokur P, Frey SE, Angelo LS, Bryant C, et al. Safety and immunogenicity of Multimeric-001 (M-001) followed by seasonal quadrivalent inactivated influenza vaccine in young adults – A randomized clinical trial. Vaccine. (2023) 41:2716–22. doi: 10.1016/j.vaccine.2023.03.023
60. BiondVax Pharmaceuticals Ltd. BiondVax Announces Topline Results from Phase 3 Clinical Trial of the M-001 Universal Influenza Vaccine Candidate (2020). Available online at: https://www.prnewswire.com/news-releases/biondvax-announces-topline-results-from-phase-3-clinical-trial-of-the-m-001-universal-influenza-vaccine-candidate-301158876.html (Accessed January 30, 2025).
61. Chen WH, Cohen MB, Kirkpatrick BD, Brady RC, Galloway D, Gurwith M, et al. Single-dose live oral cholera vaccine CVD 103-hgR protects against human experimental infection with vibrio cholerae O1 el tor. Clin Infect Dis. (2016) 62:1329–35. doi: 10.1093/cid/ciw145
62. Meiring JE, Giubilini A, Savulescu J, Pitzer VE, and Pollard AJ. Generating the evidence for typhoid vaccine introduction: considerations for global disease burden estimates and vaccine testing through human challenge. Clin Infect Dis. (2019) 69:S402–7. doi: 10.1093/cid/ciz630
63. Matuschewski K and Borrmann S. Controlled Human malaria Infection (CHMI) Studies: Over 100 Years of Experience with Parasite Injections. In: Ariey F, Gay F, and Ménard R, editors. Malaria Control and Elimination. Springer, New York (2019). p. 91–101. doi: 10.1007/978-1-4939-9550-9_7
64. Hodgson SH, Juma E, Salim A, Magiri C, Njenga D, Molyneux S, et al. Lessons learnt from the first controlled human malaria infection study conducted in Nairobi, Kenya. Malaria J. (2015) 14:182. doi: 10.1186/s12936-015-0671-x
65. CIVICs - Collaborative Influenza Vaccine Innovation Centers. Available online at: https://www.niaidcivics.org/ (Accessed January 30, 2025).
66. Inno4vac. CHIMICHURRI - ST2 Controlled Human Infection Models (CHIMs) . Available online at: https://www.inno4vac.eu/st2chimichurri (Accessed January 30, 2025).
67. Mohsen MO and Bachmann MF. Virus-like particle vaccinology, from bench to bedside. Cell Mol Immunol. (2022) 19:993–1011. doi: 10.1038/s41423-022-00897-8
68. Schwartzman LM, Cathcart AL, Pujanauski LM, Qi L, Kash JC, and Taubenberger JK. An intranasal virus-like particle vaccine broadly protects mice from multiple subtypes of influenza A virus. mBio. (2015) 6. doi: 10.1128/mbio.01044-15
69. FDA News Release. FDA Approves Nasal Spray Influenza Vaccine for Self- or Caregiver-Administration (2024). Available online at: https://www.fda.gov/news-events/press-announcements/fda-approves-nasal-spray-influenza-vaccine-self-or-caregiver-administration (Accessed January 30, 2025).
70. European Medicines Agency. Fluenz (2024). Available online at: https://www.ema.europa.eu/en/medicines/human/EPAR/fluenz (Accessed January 30, 2025).
71. de Vries RD and Rimmelzwaan GF. Viral vector-based influenza vaccines. Hum Vacc Immunother. (2016) 12:2881–901. doi: 10.1080/21645515.2016.1210729
72. Liebowitz D, Gottlieb K, Kolhatkar NS, Garg SJ, Asher JM, Nazareno J, et al. Efficacy, immunogenicity, and safety of an oral influenza vaccine: a placebo-controlled and active-controlled phase 2 human challenge study. Lancet Infect Dis. (2020) 20:435–44. doi: 10.1016/S1473-3099(19)30584-5
73. The IVR initiative. Universal Influenza Vaccine Technology Landscape (2025). Available online at: https://ivr.cidrap.umn.edu/universal-influenza-vaccine-technology-landscape (Accessed January 30, 2025).
74. Lutz J, Lazzaro S, Habbeddine M, Schmidt KE, Baumhof P, Mui BL, et al. Unmodified mRNA in LNPs constitutes a competitive technology for prophylactic vaccines. NPJ Vacc. (2017) 2:29–9. doi: 10.1038/s41541-017-0032-6
75. Bezbaruah R, Chavda VP, Nongrang L, Alom S, Deka K, Kalita T, et al. Nanoparticle-based delivery systems for vaccines. Vaccines. (2022) 10(11):1946. doi: 10.3390/vaccines10111946
Keywords: influenza, vaccine, universal influenza vaccine, FLUniversal, controlled human infection model, public-private partnerships, correlate of protection
Citation: Cnossen VM, Moreira PCL, Engelhardt OG, Samolej J, Groeneveld GH, Jochems SP, Huisman W, Pedersen GK, Wørzner K, Recek L, Piccini G, Trombetta CM, Aspelund A, Hoag A, Reiter M, Wick C, Muster T and Kamerling IMC (2025) Development of an intranasal, universal influenza vaccine in an EU-funded public-private partnership: the FLUniversal consortium. Front. Immunol. 16:1568778. doi: 10.3389/fimmu.2025.1568778
Received: 30 January 2025; Accepted: 29 April 2025;
Published: 23 May 2025.
Edited by:
Ralph A. Tripp, University System of Georgia, United StatesReviewed by:
Victor C. Huber, University of South Dakota, United StatesValentina Di Salvatore, University of Catania, Italy
Baik Lin Seong, Yonsei University, Republic of Korea
Copyright © 2025 Cnossen, Moreira, Engelhardt, Samolej, Groeneveld, Jochems, Huisman, Pedersen, Wørzner, Recek, Piccini, Trombetta, Aspelund, Hoag, Reiter, Wick, Muster and Kamerling. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victor M. Cnossen, dmNub3NzZW5AY2hkci5ubA==