 Yufeng Li1,2,3
Yufeng Li1,2,3 Ruizi Ni2
Ruizi Ni2 Yajing An2
Yajing An2 Ling Yang2
Ling Yang2 Zhaoyang Ye2
Zhaoyang Ye2 Li Zhuang2
Li Zhuang2 Linsheng Li2
Linsheng Li2 Liang Wang2,3*
Liang Wang2,3* Wenping Gong1,2*
Wenping Gong1,2*- 1Institute of Tuberculosis, Senior Department of Tuberculosis, the Eighth Medical Center of PLA General Hospital, Beijing, China
- 2Graduate school, Hebei North University, Zhangjiakou, Hebei, China
- 3Department of Geriatrics, the Eighth Medical Center of PLA General Hospital, Beijing, China
Background: The synergistic epidemic of diabetes mellitus and tuberculosis (DM-TB) has created a dual disease burden, challenging global health systems with complex pathophysiological interactions and suboptimal treatment outcomes. To decode the evolving research landscape, this study presents the latest comprehensive bibliometric analysis mapping the intellectual architecture of DM-TB research over three decades.
Methods: We systematically analyzed 791 peer-reviewed articles from the Web of Science Core Collection (1995-2023) using CiteSpace, VOSviewer, and Bibliometrix. Advanced metrics including co-citation networks, keyword burst detection, and institutional collaboration patterns were employed to identify paradigm-shifting trends.
Results: Three distinct growth phases were observed: initial stagnation (1995-2007, <10 annual publications), exponential growth (2008-2019), and research diversification (2020-2023). The United States dominated scientific output (27.3% of total publications), while the London School of Hygiene & Tropical Medicine emerged as the central hub for international collaborations (TLS=176). Keyword evolution revealed three transformative phases: (1) Pathomechanistic exploration (1995-2016): Focused on hyperglycemia-immunity interplay and epidemiological surveillance; (2) Translational innovation (2017-2020): Shifted to preclinical models, pharmacokinetic optimization, and multidrug resistance; (3) Precision medicine era (2021-2023): Emerging hotspots in latent TB screening (burst strength=6.82), metformin-mediated immunomodulation, and AI-driven diagnostic biomarkers.
Conclusion: Beyond delineating historical trajectories, this study identifies critical knowledge gaps in inflammation-resolution mechanisms and insulin resistance pathways, proposing a roadmap for targeted biomarker discovery and global health policy formulation. The constructed knowledge framework empowers strategic resource allocation for combating the DM-TB syndemic.
1 Introduction
Diabetes mellitus (DM) is a group of metabolic disorders characterized by persistent hyperglycemia due to defects in insulin secretion or impaired insulin action. This chronic hyperglycemic state is closely associated with long-term damage, dysfunction, and failure of various organs, posing a significant threat to human health (1). According to estimates by the International Diabetes Federation (IDF), in 2021, the global number of people with diabetes reached 537 million, with diabetes-related health expenditures amounting to USD 966 billion, and this figure is projected to exceed USD 1,054 billion by 2045, highlighting the immense economic burden of diabetes on global healthcare systems (2). The Global Burden of Disease (GBD) report indicates that the prevalence of DM is rising at an alarming rate, with an estimated over 1.31 billion people expected to be affected by 2050 (3). Hyperglycemia negatively impacts immune responses, making diabetic patients more susceptible to infections (4).
Tuberculosis (TB) is a pulmonary infectious disease caused by Mycobacterium tuberculosis (MTB) (5). The World Health Organization (WHO) Global Tuberculosis Report 2024 reveals that in 2023, there were an estimated 10.8 million new TB cases globally, with 1.25 million deaths, underscoring TB as a major public health challenge worldwide (6, 7). Existing research indicates a close association between DM and TB (8), TB can lead to abnormal glucose metabolism, becoming a significant factor in poor glycemic control, while hyperglycemia weakens immune defenses, promoting the growth and proliferation of MTB, thereby creating a vicious cycle (9, 10). A meta-analysis indicates that the global prevalence of diabetes mellitus complicated with tuberculosis (DM-TB) co-occurrence reaches 13.73% (11). The increase in DM-TB poses a serious threat to human life and health and imposes a significant economic burden on global healthcare systems.
Despite extensive research focusing on DM-TB, particularly in terms of its epidemiology, treatment management, and pathogenesis (12–14), the relationship between DM and TB remains incompletely understood. Bibliometric analysis is a method involving the statistical analysis of research literature related to a specific domain or topic, providing insights into the current state of research and its temporal trends, thus offering researchers macro-level information (15). It helps researchers understand progress trends and key areas of research, clarify research directions, and explore new research foci (16). This study employs bibliometric methods to analyze the overall status of DM-TB research, examining current hotspots and trends in DM-TB research.
2 Materials and methods
2.1 Data sources and retrieval strategy
This study conducted data retrieval from the Web of Science Core Collection (WoSCC) database, which provides the document formats required for bibliometric analysis software such as CiteSpace, VOSviewer, and Bibliometrix R package, making it one of the most widely used databases in bibliometric studies (17). We selected the Science Citation Index Expanded (SCI-E) from the WoSCC database as the primary source of literature. Since only publicly available data from the WoSCC database was used in this study, there are no ethical approval issues. Detailed retrieval strategies are provided in the Supplementary Material Box 1. The document types were restricted to Articles and Reviews, with the time span set from January 1, 1995, to December 31, 2023. As of September 23, 2024, an independent literature search was conducted, identifying a total of 791 related papers, and all retrieved documents were exported and saved in TXT format for subsequent bibliometric analysis. The complete retrieval process is detailed in Figure 1.
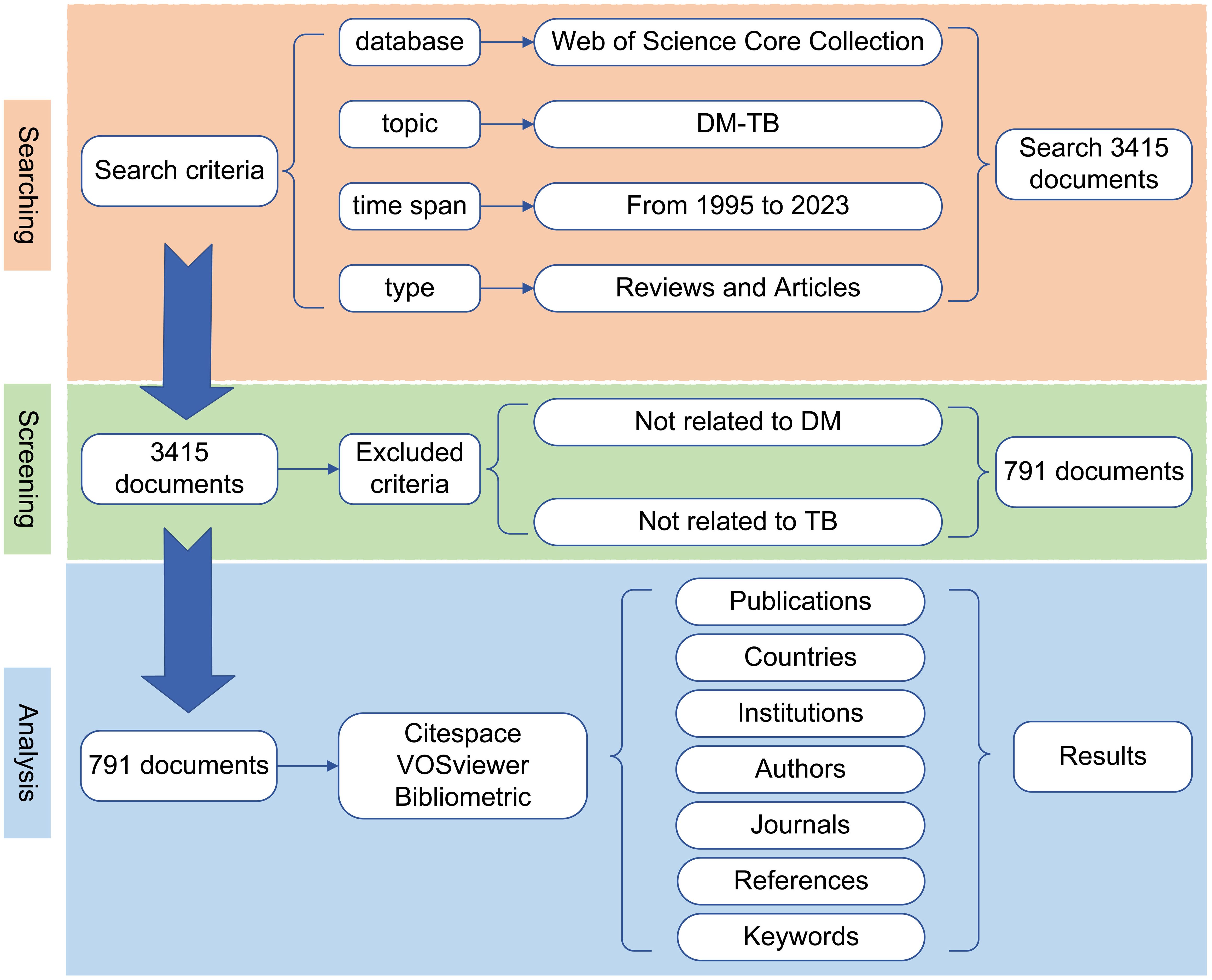
Figure 1. Search strategy and flowchart. Employing the aforementioned search strategy in the Web of Science Core Collection (SCI-Expanded) database, a total of 791 publications were retrieved and subsequently exported to VOSviewer, CiteSpace, and Bibliometrix for bibliometric analysis.
2.2 Inclusion and exclusion criteria
Inclusion criteria: (1) Papers indexed in the SCI-E database between 1995 and 2023; (2) Research papers related to DM-TB. Exclusion criteria: (1) Papers unrelated to DM-TB; (2) Non-scholarly articles such as conference papers, news reports, book chapters and so on. (3) Duplicate publications, where the same research results are reported in different journals or conferences.
2.3 Data visualization and analysis
The downloaded data was imported into Microsoft Office Excel 2021, CiteSpace, VOSviewer, Bibliometrix and OriginPro 2024 for analysis to extract meaningful information. Specifically, Microsoft Office Excel 2021 was employed for publication trend statistics, data collation and related tables. VOSviewer (version 1.6.20) was used to construct visualization maps for collaboration networks, co-citation analysis, and keyword co-occurrence analysis among countries/regions, institutions, journals, and cited journals (18). CiteSpace (version 6.3.R1) was employed for journal dual-map overlay analysis, centrality of countries, citation clustering and burst analysis, and keyword clustering and burst analysis (19). Additionally, R studio desktop software (2024.04.2) was used to connect R software Bibliometrix (version 4.4.1) for visual analysis of annual publications, author analysis, journal analysis country distribution and collaboration networks, and thematic evolution analysis (20). OriginPro 2024 was used to construct lollipop charts of author publication output.
3 Results
3.1 Annual publication output analysis
From 1995 to 2023, a total of 791 papers were published in the field of DM-TB, comprising 702 original articles and 89 reviews. These publications involved 4,062 authors across 1,430 institutions from 100 different countries/regions. Figure 2 illustrates the annual publication volume of DM-TB related articles. The number of publications generally showed an upward trend from 1995 to 2023, despite minor fluctuations. Three distinct phases were identified: Phase I (1995-2007), Phase II (2008-2019), and Phase III (2020-2023). Phase I maintained annual publications <10, representing the initial stage of DM-TB research; Phase II demonstrated substantial growth with an average of 37 publications per year; Phase III sustained steady growth in annual output, peaking at 97 publications in 2022. The Mean Total Citation per Year (MeanTCperYear) was used to evaluate the impact of publications. MeanTCperYear is defined as the total citation count of a publication divided by the cumulative years since its publication year. From 1995 to 2006, the MeanTCperYear remained below 5, indicating relatively stable impact. In 2008, the index peaked at 9.61, showing a significant increase in publication impact at that time. However, a declining trend was observed subsequently, with the MeanTCperYear dropping to 1.18 by 2023, reflecting a need for more impactful and high-quality research in this field.
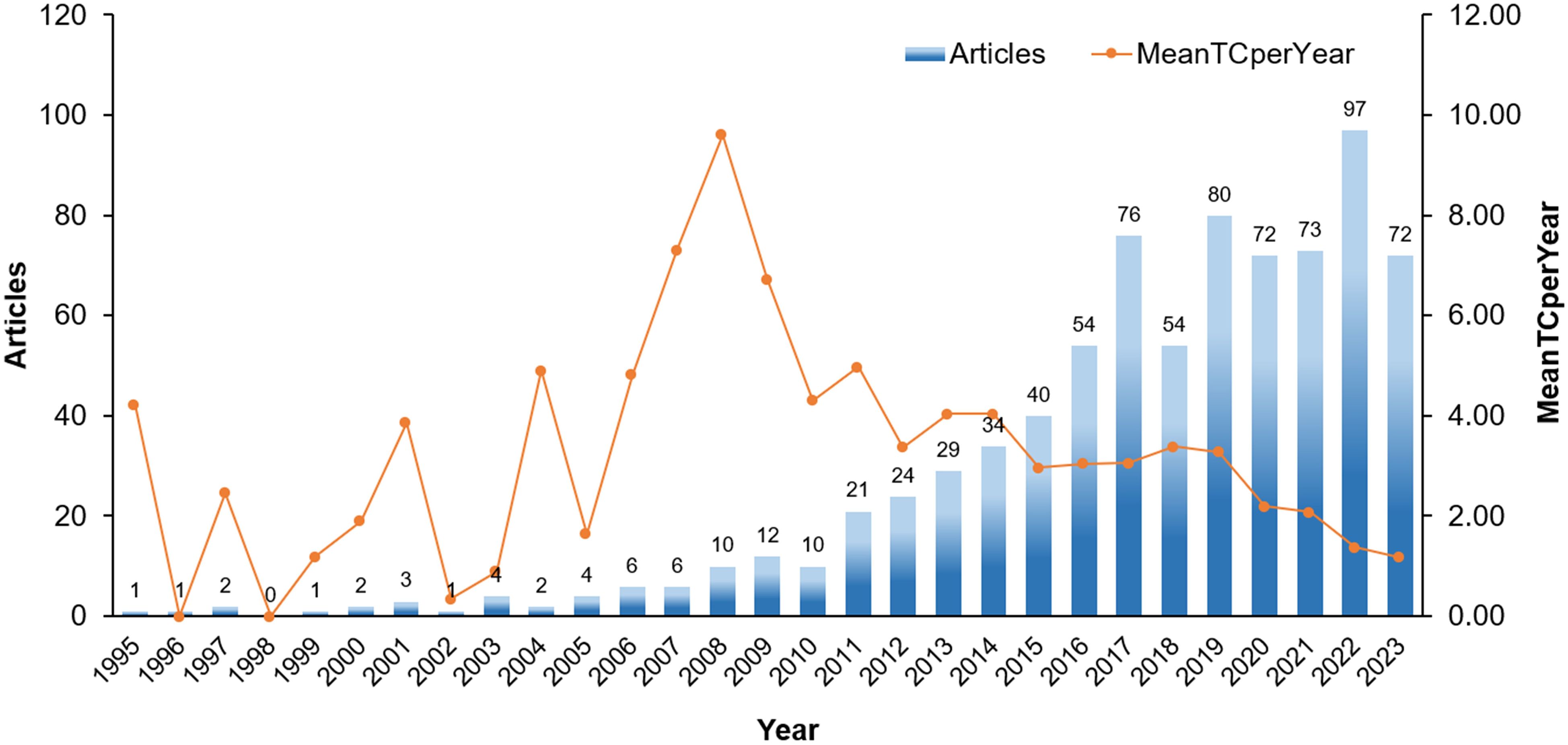
Figure 2. Growth trend of publications. Temporal trends in DM-TB research publication growth (1995-2023): Annual publication volume and mean total citations per year.
3.2 Country or region analysis
A total of 100 countries/regions have conducted research on DM-TB. Table 1 lists the top 10 countries/regions in terms of publication volume, with the United States leading (216 articles), followed by China (145 articles), India (116 articles), the United Kingdom (103 articles), and Mexico (66 articles). Betweenness centrality (BC) quantifies a node’s frequency of occurring on shortest network paths, assessing its topological significance, with values exceeding 0.1 designating pivotal nodes (21). Five countries had BC values greater than 0.1: the United States (0.33), the United Kingdom (0.29), South Africa (0.14), Denmark (0.12), and France (0.11), indicating their crucial role in research in this field. The United States led in publication volume (216 articles), BC (0.33), and citation count (8,970), significantly surpassing other countries/regions. Although China and India ranked highly, their BC was relatively low. Figure 3A maps out the collaborative relationships between major countries/regions. The width of the connecting lines represents the strength of collaboration, with wider lines indicating stronger partnerships. The United States is the most frequent initiator and participant in collaborations, particularly with India, the United Kingdom, China, Mexico, Brazil, Peru, South Africa, and Australia. Figure 3B illustrates the collaboration network for countries/regions with a minimum of five publications. Additionally, the node colors in Figure 3C represent the year each country first appeared in this research field, with yellow nodes indicating more recent entry. Since 2020, some countries/regions have entered this research area, showing increasing global interest in the field.
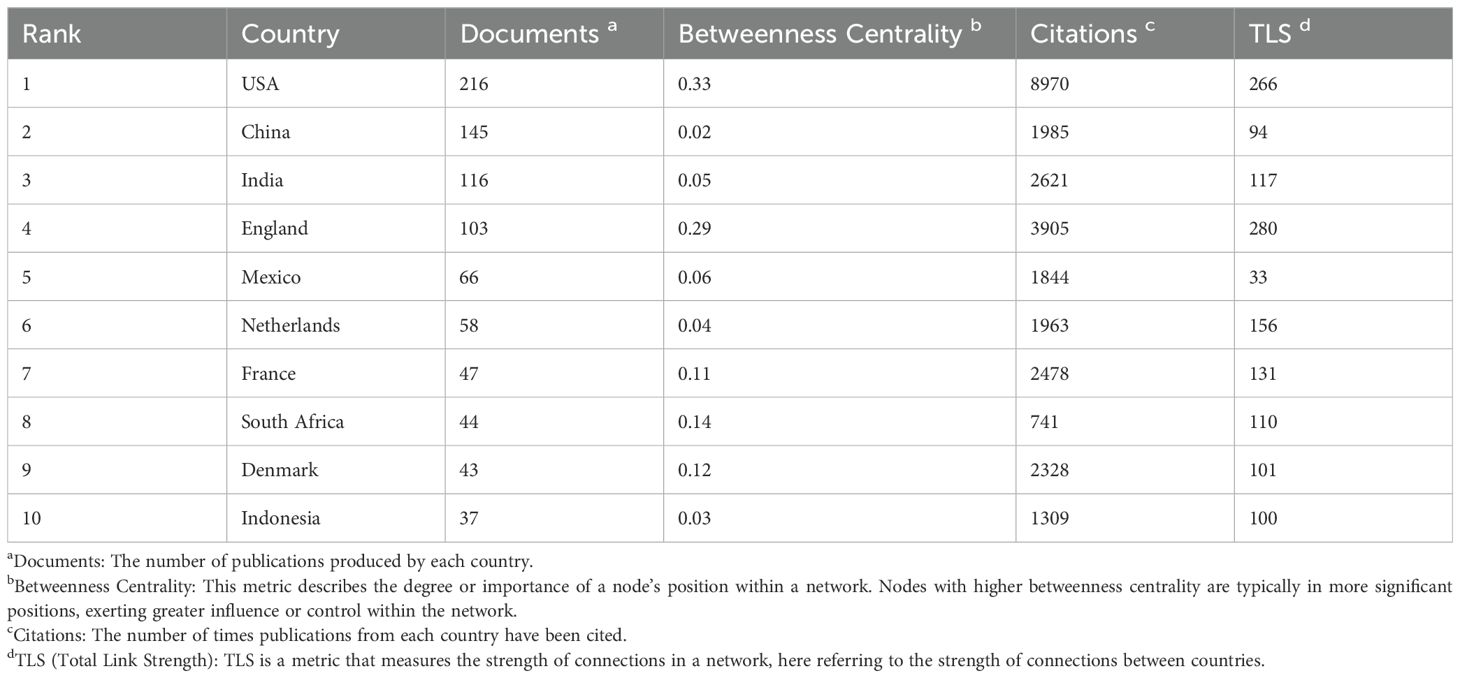
Table 1. Ten countries with the most publications.
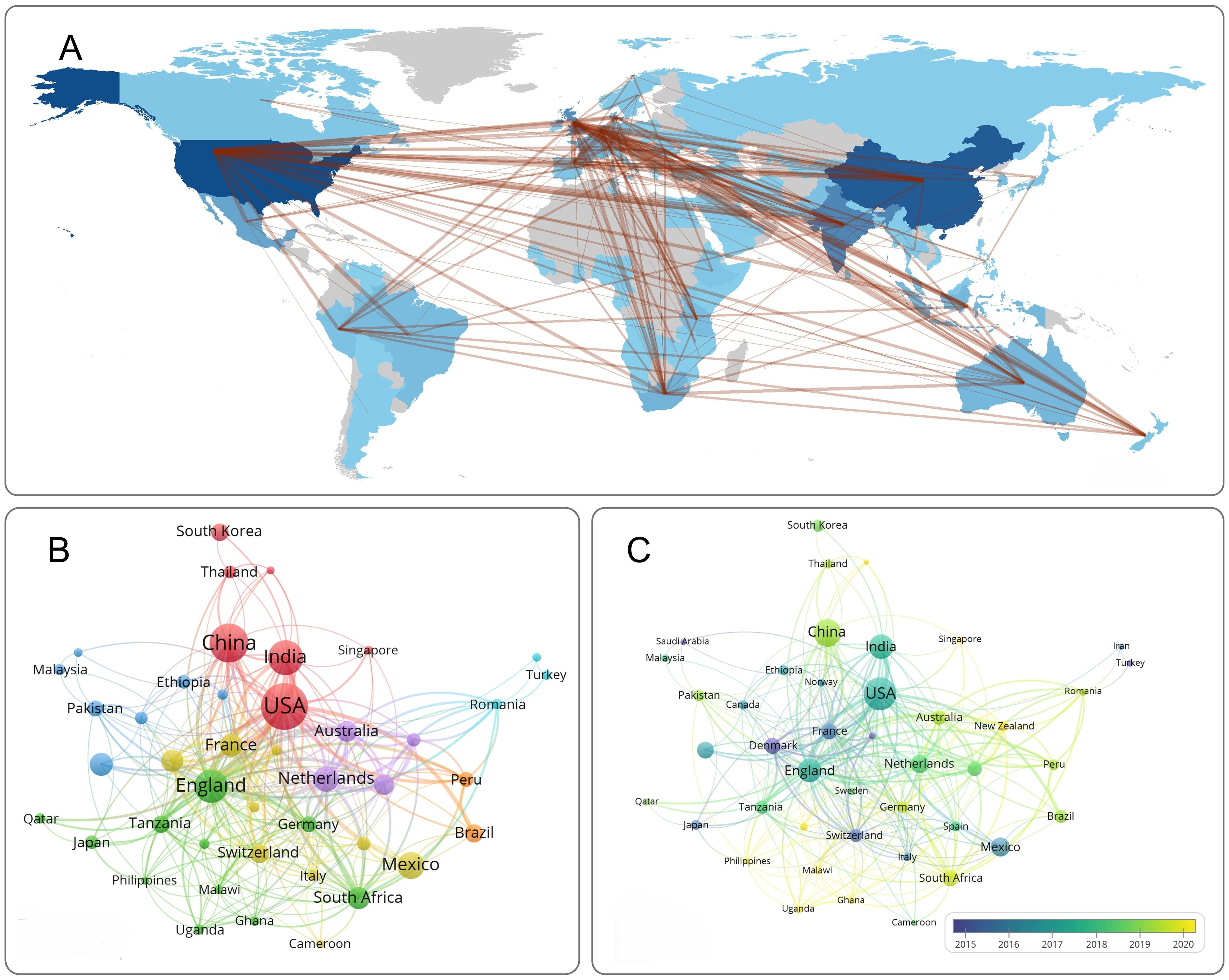
Figure 3. Visualization of countries/regions analysis. (A) Country collaboration map. The colors of the map’s regions indicate the number of published articles, with darker shades corresponding to a higher volume of articles contributed by each country/region. (B) Network visualization of countries. (C) Overlay visualization of countries. Nodes represent countries/regions, with node size corresponding to publication count. Connections between nodes indicate collaborative partnership.
3.3 Institutional and collaborative institution analysis
A total of 1,430 institutions conducted research on DM-TB. Table 2 lists the top ten institutions by publication volume, with the London School of Hygiene & Tropical Medicine (52 articles), International Union Against TB and Lung Disease (33 articles), and University of Massachusetts (32 articles) ranking as the top three. Analyzing collaboration intensity, the top three institutions in total link strength (TLS) were London School of Hygiene & Tropical Medicine (176), International Union Against TB and Lung Disease (111), and St George’s, University of London (108). Notably, the London School of Hygiene & Tropical Medicine stood out with significantly higher citation frequency and TLS than the other two, indicating its leading impact in publications.
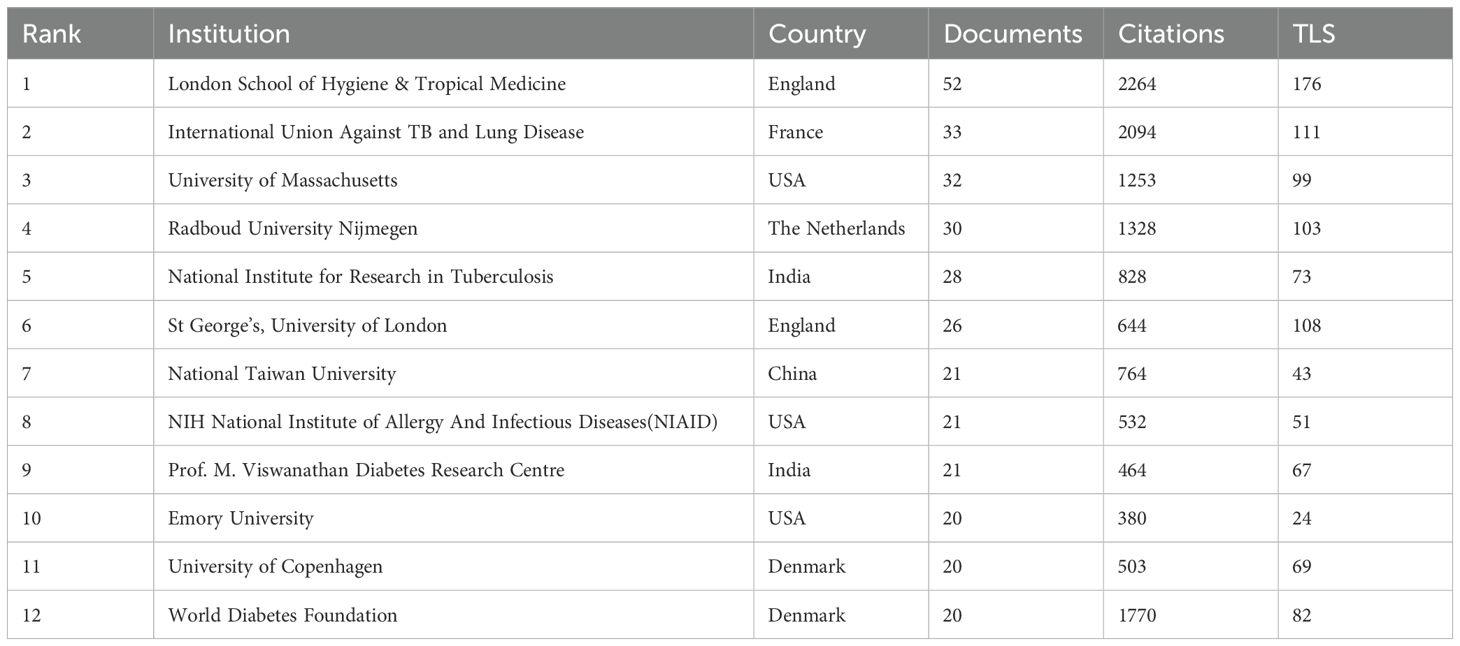
Table 2. Ten institutions with the most publications.
Co-occurrence analysis on institutions with more than five publications is shown in Figure 4A, where apparent close collaborations exist among these institutions. Institutions like London School of Hygiene & Tropical Medicine, Radboud University Nijmegen, and University of Copenhagen have gradually formed self-centered collaborative networks. In Figure 4B, nodes predominantly purple, such as International Union Against TB and Lung Disease, indicate early entry into the field, while nodes primarily yellow, like University of Queensland, Fundação Oswaldo Cruz, and University of Virginia, indicate later entry. The largest yellow node, St George’s, University of London, suggests it might be an emerging research institution in the field, potentially leading future developments and becoming a key force.
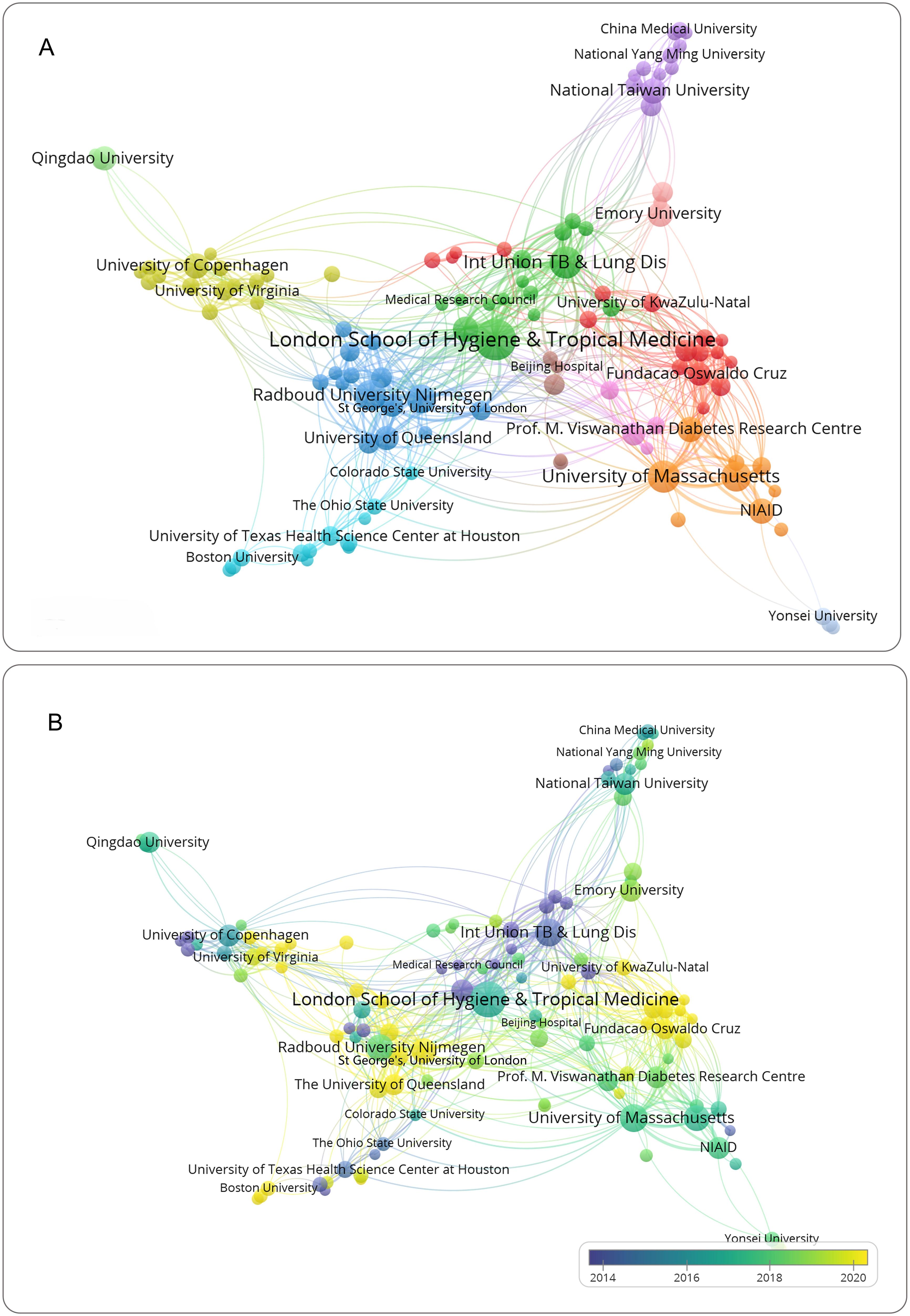
Figure 4. Visualization of institutions analysis. (A) Network visualization of institutions. (B) Overlay visualization of institutions. Nodes represent institutions, with node size corresponding to publication count. Connections between nodes indicate collaborative partnership.
3.4 Author analysis
A total of 4,062 authors have conducted research on DM-TB. Supplementary Table S1 and Figure 5A provide information about the top ten authors with the most publications. The H-index, G-index and M-index are comprehensive quantitative indicators considering both the quantity and quality of academic output, used to assess academic impact (22–24). Among them, Kornfeld, Hardy has the highest publication count (30 articles), higher H-index (18), and highest G-index (30). In contrast, Kapur, Anil achieves the highest H-index (20) and total citation count (1,829), with a marginally higher M-index (1.25 vs. 1.0). These metrics collectively establish that Kornfeld, Hardy represents the most prolific author with dominant core paper impact in DM-TB research, while Kapur, Anil demonstrates the highest comprehensive academic influence. This discrepancy may be attributed to Kapur’s institutional leadership as Chair of the World Diabetes Foundation, which enhances academic visibility through frequent conference participation, collaborative networks, and sustained research engagement. Figure 5B compares authors’ publication output over time, with Kornfeld, Hardy having the most papers, and Van Crevel, Reinout, Restrepo, Blanca I and Alisjahbana Bachti starting research earliest and having the longest duration. Recently, Critchley, Julia A and Van Crevel, Reinout have made greater contributions. Figure 5C uses a three-field plot to illustrate authors’ publishing patterns in different related topics and journals. The top 10 authors’ main research keywords include “tuberculosis”, “diabetes mellitus”, “pulmonary tuberculosis”, “tb”, “screening”, “mycobacterium tuberculosis”, “metformin”, “risk factors”. Their work is typically published in journals like the International Journal of Tuberculosis and Lung Disease, BMC Infectious Diseases, Tuberculosis and Plos One.
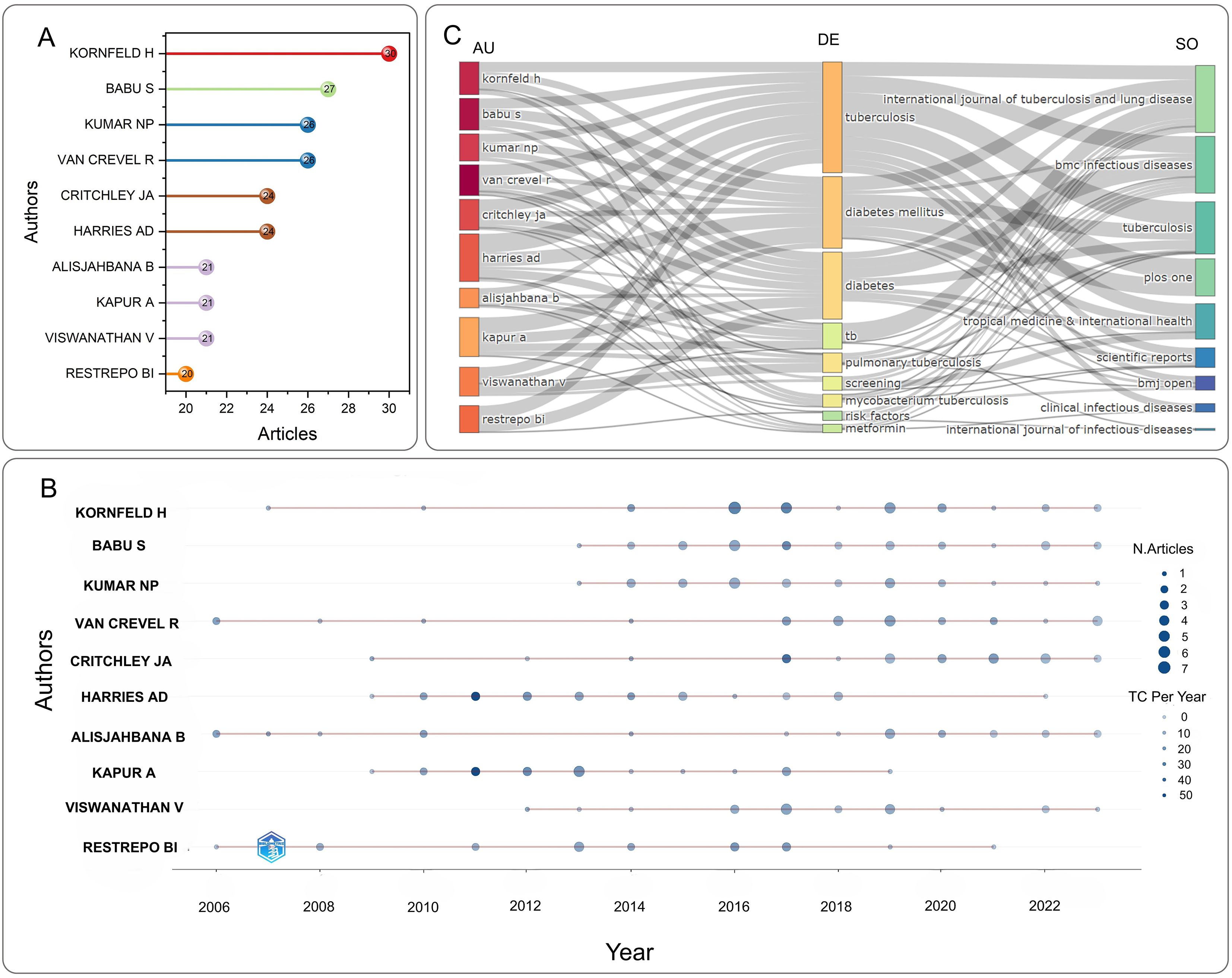
Figure 5. Visualization of authors analysis. (A) Top 10 most relevant authors in the field of DM-TB. (B) Authors’ production over time. Node size corresponds to publication count, and color denotes annual total citation counts per author (C) Three-field plot illustrating interconnections among AU (Author), DE (Keyword), and SO (Journal).
3.5 Journal and cited journal analysis
The 791 publications related to DM-TB spanned 263 journals and 4,790 co-cited journals. Supplementary Tables S2 and S3 list the top ten journals by publication volume and citation frequency, respectively. The journals with the most publications are International Journal of Tuberculosis and Lung Disease (60 articles) and PLOS ONE (60 articles), followed by BMC Infectious Diseases (39 articles). The highest impact factor (IF) among them belongs to Clinical Infectious Diseases at 8.2. A journal’s impact largely depends on its citation frequency, as citations reflect the extent to which scholars and researchers in the field refer to its articles. PLOS ONE has the highest citation frequency (1574 times), followed by International Journal of Tuberculosis and Lung Disease (1,379 times) and Clinical Infectious Diseases (824 times), with six journals in the Q1 category, indicating significant impact in the field. Figure 6A shows cumulative publications from the top five journals. Before 2013, the International Journal of Tuberculosis and Lung Disease led in publications; after 2013, publication volumes for various journals increased markedly, with International Journal of Tuberculosis and Lung Disease and PLOS ONE taking the lead.
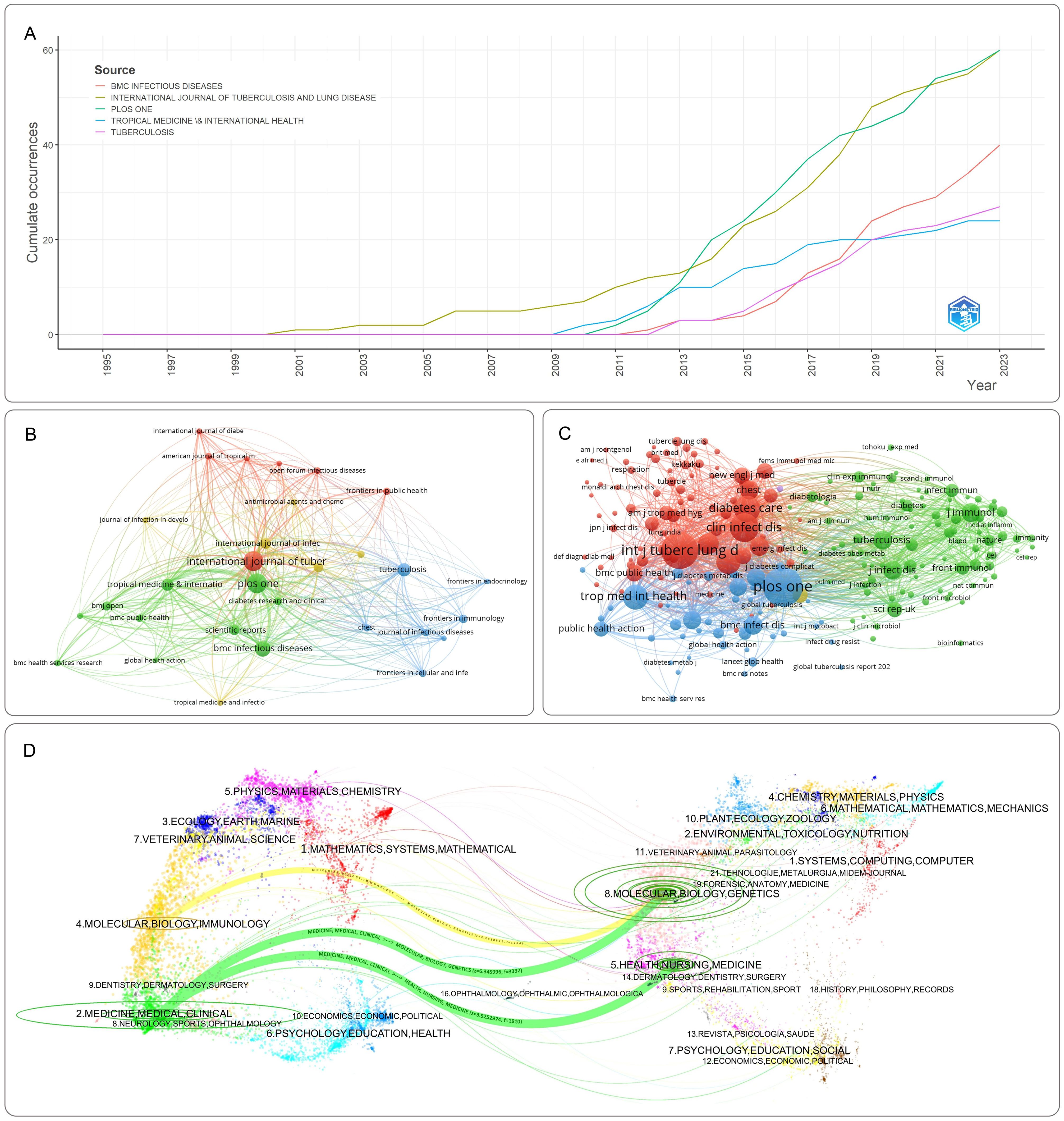
Figure 6. Visualization of journal analysis. (A) Top 10 journals’ production over time. (B) Network visualization of journals. (C) Network visualization of co-cited journals. Nodes represent journals or co-cited journals, with node size corresponding to publication count. Connections between nodes indicate collaborative partnership. (D) The dual-map overlay of journal publishing research. The citing journals mainly focus on molecular, biology, immunology, medicine, medical and clinical studies; the cited journals primarily focus on health, nursing, medicine, molecular biology, and genetics.
Cluster analysis of journals and co-cited journals is presented in Figures 6B, C, visually displaying collaboration among journals and co-cited journals. Dual-map overlay of journals illustrates the relationship between citing and cited journals, with research areas of citing journals on the left and cited journals on the right. As shown in Figure 6D, the map identifies three main citation paths, including one orange path and two green paths. The orange path indicates that journals from the fields of molecular, biology and genetics are most likely to be cited by journals in the fields of molecular, biology and immunology. The green path suggests that publications related to molecular, biology and genetics, as well as health, nursing, and medicine fields are more likely to be cited by journals in the fields of medicine, medical and clinical.
3.6 Co-cited references analysis
Supplementary Table S4 lists the top ten most cited articles among the 791 publications. These articles systematically investigated the bidirectional relationship between DM-TB, including DM’s elevated risk of developing TB, its impacts on therapeutic responses and clinical outcomes, as well as their epidemiological interactions and clinical management strategies (25–34). “Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies” is the most cited article (416 times). This paper systematically reviews and meta-analyzes observational studies evaluating the association between DM and TB, finding that DM is associated with increased TB risk, and indicating that TB control should consider interventions targeting DM patients (25). The second most cited article (272 times), “The impact of diabetes on tuberculosis treatment outcomes: a systematic review” systematically reviews 33 observational studies on DM patients receiving TB treatment, finding that DM increases the risk of treatment failure, death, and relapse in TB patients. This study highlights the need for increased attention to the treatment of TB in diabetic patients, potentially including testing for suspected DM, improving glycemic control, and enhancing clinical and treatment monitoring (26). “Tuberculosis and diabetes mellitus: convergence of two epidemics” is the third most cited article (211 times). It reviews the epidemiology of TB and DM, and outlines the role of DM in TB susceptibility, clinical manifestation, and treatment response. Additionally, it reviews the potential mechanisms by which DM leads to TB, the impact of TB on DM control, and pharmacokinetic issues related to the co-management of DM and TB (27).
Co-citation analysis of cited articles using VOSviewer is shown in Figure 7A, with the minimum citation threshold set to 20. Network clustering of literature relationships using CiteSpace is depicted in Figure 7B, with the first seven clusters shown. The parameters were configured as follows: temporal scope spanning 1995–2023 with 1-year slices, node type defined as references, g-index standardization (k=25), and pruning disabled. The Modularity Q value of the clustering map is 0.6465, and the Weighted Mean Silhouette S value is 0.8522, confirming the reliability of the clustering structure. Cluster #0: “metformin” is the largest cluster, indicating its extensive citation. Followed by clusters such as “inflammation” (#1), “glucose metabolism” (#2), “T cells” (#3), “China” (#4), and “body mass index” (#5). Other important clusters include “cellular immune responses” (#6). The cluster timeline diagram in Figure 7C illustrates the evolution of research directions, with nodes representing cited articles, different shades representing research evolution, and curves between nodes indicating co-citation relationships. Reference burst analysis enables quick identification of the most influential cited documents, facilitating a clear understanding of the DM-TB research backdrop and current frontlines and emerging trends. Reference burst analysis is shown in Figure 7D, where higher burst strength values indicate explosive increases in citations during specific periods. Jeon CY et al.’s study (25) shows the highest burst strength, confirming the association between DM and increased TB risk, significantly impacting the DM-TB field. Recent studies by Workneh MH (35), AI-Rifai RH (36), Huangfu P (37), and Noubiap JJ (38) are the latest, exploring the prevalence and mortality of DM-TB.
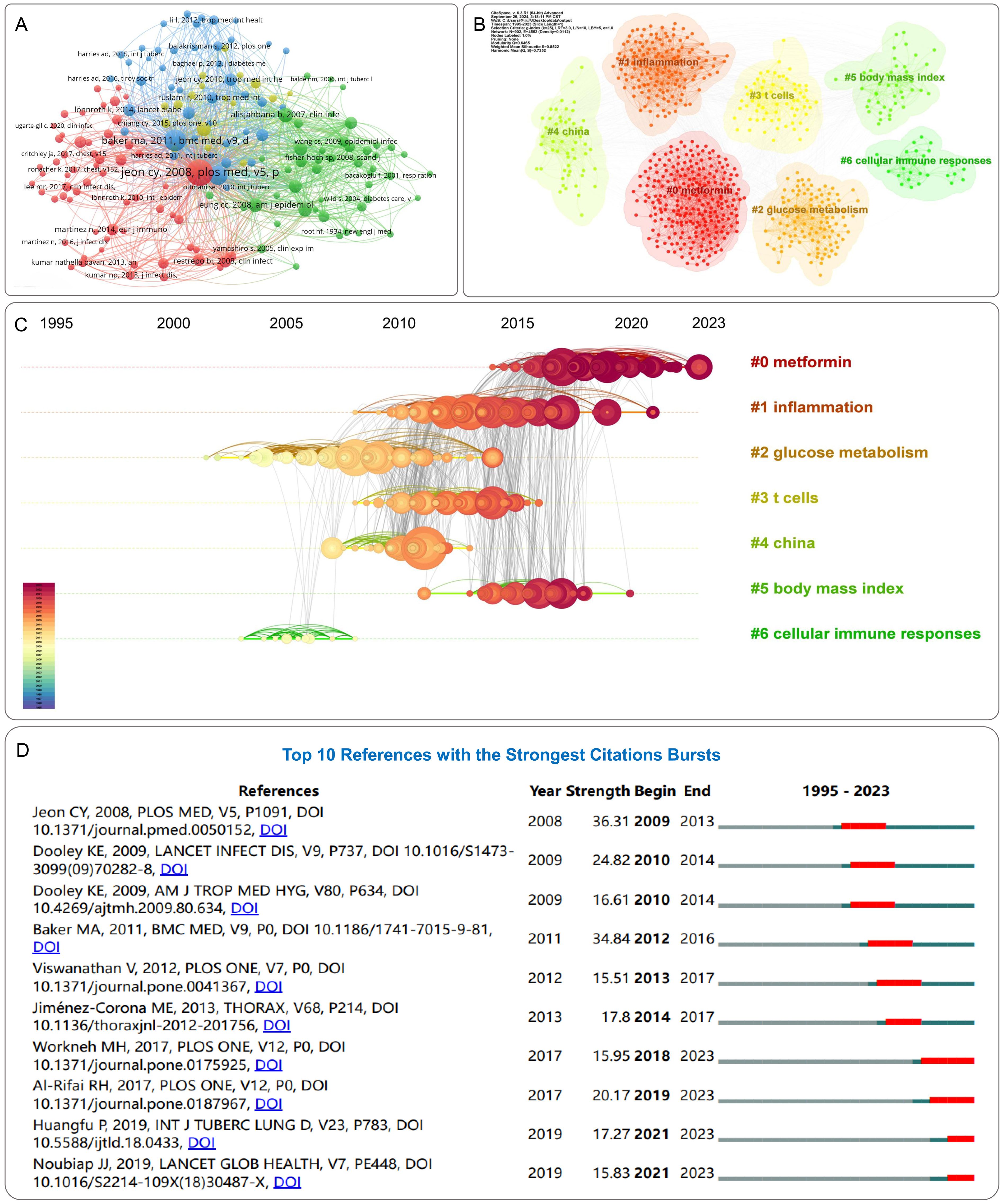
Figure 7. Visualization of reference analysis. (A) Network visualization of references. (B) Clusters of references. (C) Reference timeline view. Nodes represent cited references, where the diameter proportionally correlates with citation frequency. A chromatic temporal gradient from blue (1995) to red (2023) visually encodes the publication timeline across nodes. (D) Top 10 references with the strongest citation bursts. Red bars represent the duration of burst periods. The burst strength demonstrates the significance of this study to the research field.
3.7 Keywords analysis
To understand the core content and hotspots in the DM-TB field, we analyzed author keywords in the retrieved literature. We extracted 2,030 keywords from 791 publications, and conducted a synonym merge to improve readability. A density map of the top 50 most frequent keywords was plotted using VOSviewer, as shown in Figure 8A. These keywords include “diabetes mellitus,” “tuberculosis,” “risk factors,” “pulmonary tuberculosis,” “prevalence,” “impact,” “Mycobacterium tuberculosis,” “treatment outcomes,” “infection,” “immunity,” “association,” “disease,” “type 2 diabetes,” “expression,” “latent tuberculosis,” “epidemiology” and so on. These keywords represent the focal points of research in the field. CiteSpace was used for clustering of keywords, as shown in Supplementary Table S5 and Figure 8B, which displays eight clusters for visualizing emerging trends in the DM-TB field. The parameters were configured as follows: temporal scope spanning 1995–2023 with 1-year slices, node type defined as keywords, g-index standardization (k=25), and pruning disabled. The cluster network includes 578 nodes and 3,227 links, with Modularity Q = 0.3982 (>0.3), indicating significance and credibility. Weighted Mean Silhouette S = 0.7564 (>0.7) signals homogeneity among clusters, demonstrating a reliable network. The eight clusters are: “multidrug-resistant tuberculosis (MDR-TB),” “murine model,” “cells,” “population pharmacokinetics,” “risk factors,” “T2DM,” “transient hyperglycemia” and “outcomes (show as outcm in figure).”
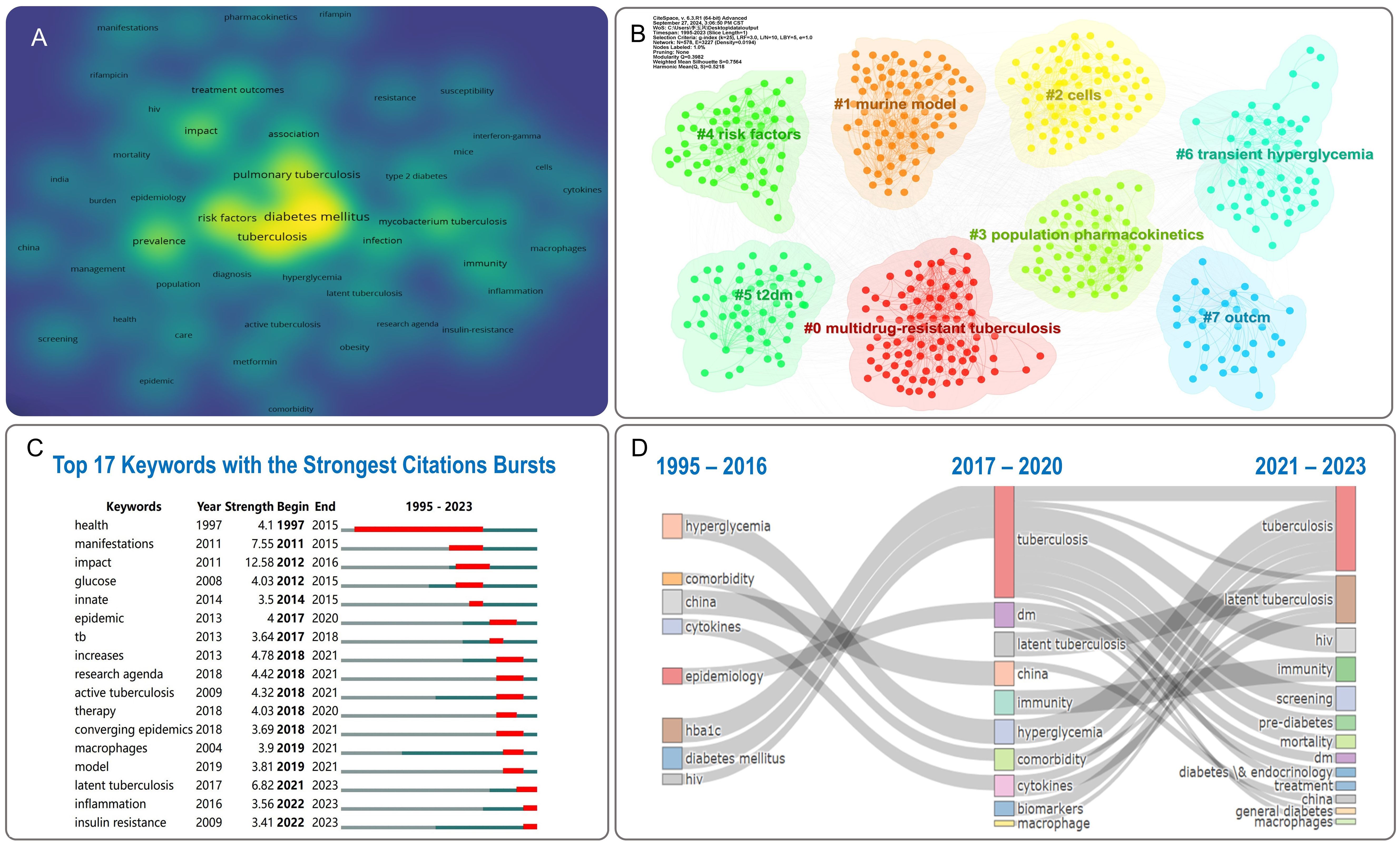
Figure 8. Visualization of keywords analysis. (A) Density visualization of keywords. (B) Clusters of keywords. (C) Top 17 keywords with the strongest citation bursts. Red bars represent the duration of burst periods. The burst strength demonstrates the significance of this study to the research field. (D) Thematic evolution of DM-TB: temporal dynamics of Keywords.
The top 17 keywords in the DM-TB research burst analysis are shown in Figure 8C. Burst strength is calculated by combining keyword frequency with time aspects, where higher strength signifies a sudden or explosive increase in prevalence over a specified period. “Impact” is the most prominent keyword, followed by “manifestations” and “latent tuberculosis.” Notably, the keyword “health” had the longest burst duration. Recently burst keywords in the past three years include “latent tuberculosis,” “inflammation,” and “insulin resistance,” indicating these subjects currently constitute research frontiers in the field. As displayed in Figure 8D, the thematic evolution diagram depicting horizontal spatial shifts of nodes constitutes a comprehensive timeline of initial appearances and evolution processes of relevant keywords in academic literature, highlighting shifts in research directions over time and providing insights into the research process. Between 1995 and 2016, research themes focused on hyperglycemia, comorbidities, cytokines, and epidemiology, evolving to tuberculosis, diabetes, as well as latent tuberculosis, immunity, biomarkers, and macrophages from 2017 to 2020. From 2021 to 2023, themes shifted to tuberculosis, latent tuberculosis, HIV, screening, and prediabetes, reflecting the dynamic evolution of DM-TB research.
4 Discussion
The incidence of DM-TB has been rising steadily, becoming a focal point in global public health. This study employed bibliometric methods to analyze literature related to DM-TB published between 1995 and 2023, aiming to uncover research hotspots and thematic trends in this field. The analysis encompassed 791 papers published by 1,430 institutions across 100 countries/regions in 263 journals, providing a macro perspective on the current research status and forecasting future trends.
The increasing annual number of publications highlights the robust development. The low research output during 1995–2007 reflects limited academic understanding of the DM-TB association. The marked increase in publications post-2008 may be attributed to studies demonstrating DM elevates TB risk (27), which prompted global enhancements in comorbid disease screening. During the COVID-19 pandemic, shifted research priorities and resource allocation led to reduced DM-TB research output compared to previous periods, accompanied by declining citation rates (39). However, the peak publication volume in 2022 likely reflects concentrated recovery of previously suppressed scientific activities as pandemic management transitioned into routine phases. The United States emerged as a key contributor in terms of publication volume, BC, total link strength, and citation numbers, indicating its strong international influence in this research field. This phenomenon may be attributed to the significant advantages of the U.S. scientific research system. The United States boasts a large number of widely distributed research institutions, and its highly developed economic system provides a solid material foundation for scientific research activities. In contrast, as developing countries and high TB burden countries defined by the WHO, China and India face more complex public health challenges. In recent years, with the growing prominence of DM-TB issues, research investment in the field of DM-TB in these countries has increased significantly. According to data released by the WHO, most high TB burden countries are low- and middle-income nations, where relatively weak healthcare systems, poor nutritional status, and suboptimal living conditions interact, further exacerbating the prevalence of DM-TB (40). Therefore, research on the epidemiology, clinical management, and prevention strategies of DM-TB is particularly critical in these countries.
At the institutional level, the London School of Hygiene & Tropical Medicine and the International Union Against TB and Lung Disease published the highest number of papers on DM-TB research. The London School of Hygiene & Tropical Medicine’s outstanding performance in publication volume, citation frequency, and TLS reflects its leading role and extensive collaborative relationships in this field. At the author level, prolific authors such as Kornfeld, Hardy, Babu, Subash, and Kumar, Nathella Pavan demonstrate marked activity and output, while the significant citation frequency and H-index of Kapur, Anil showcases the major impact of his scientific contributions. These authors form distinct clusters with stable collaborations, providing robust support for research advancements in the field.
In terms of journals, the International Journal of Tuberculosis and Lung Disease and PLOS ONE rank among the top in publication volume and citation frequency, highlighting their authority and influence in the field. Particularly, PLOS ONE’s open-access model offers unrestricted access and citation of research results to scholars worldwide, promoting the widespread dissemination of academic findings. Additionally, the top ten cited publications are all reviews, mainly addressing the epidemiology of DM-TB, the association between DM and TB, and the impact of DM on TB clinical manifestations and treatment outcomes. These areas form the foundation of DM-TB-related research and foster deeper development in the field. Notably, in recent years, themes related to “metformin” have been prominent among co-cited references in the DM-TB research field, becoming a persistent research theme. Studies indicate that metformin may enhance innate immunity against MTB through direct mechanisms or by modulating corticosteroid hormones (41), and its therapeutic use has been associated with reduced mortality rates among patients with DM-TB comorbidity (42).
Through high-frequency keyword extraction and clustering analysis, we identified research hotspots in DM-TB between 1995 and 2023 and predicted future trends in this research field. Clustering analysis indicates that MDR-TB, animal models, cellular and molecular mechanisms, pharmacokinetics, and risk factors are the current research hotspots. Notably, the sudden increase in keywords such as “latent tuberculosis,” “inflammation,” and “insulin resistance” suggests significant potential for future research development in these areas.
Emerging evidence highlights that MDR-TB has evolved into a major public health challenge. Accumulating clinical evidence demonstrates DM serves as an independent risk factor for developing MDR-TB and predicts suboptimal clinical outcomes (43). While advancements in pharmacokinetic modeling have revolutionized tuberculosis drug development, novel therapeutic paradigms focusing on host-pathogen interactions (HPI) are gaining prominence. These host-directed therapies (HDT) represent a promising frontier for optimizing bacterial clearance while preventing post-tuberculosis pulmonary sequelae (44). Similarly, adjunctive therapeutic strategies utilizing natural products have shown potential clinical value. Current evidence confirms that mulberry extracts facilitate glucose absorption, enhance insulin biosynthesis/secretion, and demonstrate antioxidative/anti-inflammatory properties (45). Polyphenolic compounds including quercetin, curcumin, and resveratrol exert therapeutic effects through mitigating intracellular oxidative stress and attenuating chronic low-grade inflammation (46). However, the clinical translation of these interventions faces critical scientific challenges, necessitating implementation of hyperspectral imaging technology for authentication of natural product integrity (47). Thematic trajectory analysis reveals an important paradigm shift in DM-TB research: from initial clinical characterization of disease manifestations to current mechanistic investigations at molecular levels. Notably, the precise pathogenesis of TB in individuals with DM remains poorly delineated. Capitalizing on recent breakthroughs in multi-omics technologies, priority should be given to interdisciplinary research integrating metabolic profiling, immune phenotyping, and transcriptomic signatures to establish predictive biomarkers and therapeutic targets (48). These studies not only enhance our understanding of the pathophysiological mechanisms of DM-TB but also provide a solid theoretical foundation for developing more effective prevention, diagnosis, and treatment strategies.
Despite offering a macro perspective on the research status and future trends within the DM-TB field through bibliometric methods, this study has certain limitations. The research data is solely sourced from the WoSCC database, possibly overlooking relevant studies from other databases. Additionally, the bibliometric tools used may introduce data processing bias. Lastly, the time constraints of the study might lead to the omission of some high-quality articles. Future research should delve deeper into data analysis, extract more valuable information, consider future research directions, and propose concrete suggestions and outlooks. Despite these limitations, the research directions established in this study will contribute to the continuous advancement of the DM-TB field.
5 Conclusions
The bibliometric analysis of literature from 1995 to 2023 revealed significant growth in the DM-TB field, with a peak in research activity noted in 2022. The United States and China are major contributors to this research domain, with institutions like the London School of Hygiene & Tropical Medicine standing out. Open-access journals such as PLOS ONE have facilitated the wide dissemination of research findings. Research hotspots focus on areas like MDR-TB, animal models, and pharmacokinetics, indicating future research directions.
While this study highlights the research dynamics and future trends in the DM-TB field, it is limited by data sources and temporal scope. Future studies should aim to deepen data analysis and explore new research directions. These findings are anticipated to further propel the DM-TB field’s development, positively impacting global public health.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author/s.
Author contributions
YL: Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft. RN: Investigation, Methodology, Writing – review & editing. YA: Investigation, Methodology, Writing – review & editing. LY: Investigation, Methodology, Writing – review & editing. ZY: Investigation, Methodology, Writing – review & editing. LZ: Investigation, Methodology, Writing – review & editing. LL: Investigation, Methodology, Writing – review & editing. LW: Conceptualization, Writing – review & editing. WG: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the Special Topics in Health Care (24BJZ34). We sincerely thank the reviewers and editors who provided review and editing services for this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1571123/full#supplementary-material
Abbreviations
DM, diabetes mellitus; TB, tuberculosis; MTB, Mycobacterium tuberculosis; DM-TB, Diabetes Mellitus Complicated with Tuberculosis; IDF, International Diabetes Federation; GBD, Global Burden of Disease; WHO, World Health Organization; SCI-E; Science Citation Index Expanded; WoSCC, Web of Science Core Collection; MeanTCperYear, The Mean Total Citation per Year; BC, Betweenness centrality; TLS, total link strength; IF, impact factor; MDR-TB, multidrug-resistant tuberculosis; T2DM, type 2 diabetes mellitus; HPI, host-pathogen interactions; HDT, host-directed therapies.
References
1. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. (2013) 36 Suppl 1:S67–74. doi: 10.2337/dc13-S067
2. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
3. GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. (2023) 402:203–34. doi: 10.1016/s0140-6736(23)01301-6
4. Holt RIG, Cockram CS, Ma RCW, Luk AOY. Diabetes and infection: review of the epidemiology, mechanisms and principles of treatment. Diabetologia. (2024) 67:1168–80. doi: 10.1007/s00125-024-06102-x
5. Furin J, Cox H, Pai M. Tuberculosis. Lancet. (2019) 393:1642–56. doi: 10.1016/s0140-6736(19)30308-3
7. Chen Z, Wang T, Du J, Sun L, Wang G, Ni R, et al. Decoding the WHO global tuberculosis report 2024: A critical analysis of global and chinese key data. Zoonoses. (2025) 5:1. doi: 10.15212/zoonoses-2024-0061
8. Ye Z, Li L, Yang L, Zhuang L, Aspatwar A, Wang L, et al. Impact of diabetes mellitus on tuberculosis prevention, diagnosis, and treatment from an immunologic perspective. Explor (Beijing). (2024) 4:20230138. doi: 10.1002/EXP.20230138
9. Boadu AA, Yeboah-Manu M, Osei-Wusu S, Yeboah-Manu D. Tuberculosis and diabetes mellitus: The complexity of the comorbid interactions. Int J Infect Dis. (2024) 146:107140. doi: 10.1016/j.ijid.2024.107140
10. Ssekamatte P, Sande OJ, van Crevel R, Biraro IA. Immunologic, metabolic and genetic impact of diabetes on tuberculosis susceptibility. Front Immunol. (2023) 14:1122255. doi: 10.3389/fimmu.2023.1122255
11. Li M, Chen T, Hua Z, Yan H, Wang D, Li Z, et al. Global, regional, and national prevalence of diabetes mellitus in patients with pulmonary tuberculosis: a systematic review and meta-analysis. Diabetol Metab Syndr. (2021) 13:127. doi: 10.1186/s13098-021-00743-3
12. Ugarte-Gil C, Alisjahbana B, Ronacher K, Riza AL, Koesoemadinata RC, Malherbe ST, et al. Diabetes mellitus among pulmonary tuberculosis patients from 4 tuberculosis-endemic countries: the TANDEM study. Clin Infect Dis. (2020) 70:780–8. doi: 10.1093/cid/ciz284
13. Khattak M, Rehman AU, Muqaddas T, Hussain R, Rasool MF, Saleem Z, et al. Tuberculosis (TB) treatment challenges in TB-diabetes comorbid patients: a systematic review and meta-analysis. Ann Med. (2024) 56:2313683. doi: 10.1080/07853890.2024.2313683
14. Ngo MD, Bartlett S, Bielefeldt-Ohmann H, Foo CX, Sinha R, Arachchige BJ, et al. Blunted GPR183/oxysterol axis during dysglycemia results in delayed recruitment of macrophages to the lung during mycobacterium tuberculosis infection. J Infect Dis. (2022) 225:2219–28. doi: 10.1093/infdis/jiac102
15. Ninkov A, Frank JR, Maggio LA. Bibliometrics: Methods for studying academic publishing. Perspect Med Educ. (2022) 11:173–6. doi: 10.1007/s40037-021-00695-4
16. Thompson DF, Walker CK. A descriptive and historical review of bibliometrics with applications to medical sciences. Pharmacotherapy. (2015) 35:551–9. doi: 10.1002/phar.1586
17. Zhang L, Yao Q, Hu J, Qiu B, Xiao Y, Zhang Q, et al. Hotspots and trends of microglia in Alzheimer’s disease: a bibliometric analysis during 2000-2022. Eur J Med Res. (2024) 29:75. doi: 10.1186/s40001-023-01602-9
18. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
19. Synnestvedt MB, Chen C, Holmes JH. CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. (2005) 2005:724–8.
20. Oyewola DO, Dada EG. Exploring machine learning: a scientometrics approach using bibliometrix and VOSviewer. SN Appl Sci. (2022) 4:143. doi: 10.1007/s42452-022-05027-7
21. Lee J, Lee Y, Oh SM, Kahng B. Betweenness centrality of teams in social networks. Chaos. (2021) 31:061108. doi: 10.1063/5.0056683
22. Mondal H, Deepak KK, Gupta M, Kumar R. The h-Index: Understanding its predictors, significance, and criticism. J Family Med Prim Care. (2023) 12:2531–7. doi: 10.4103/jfmpc.jfmpc_1613_23
23. Kosmulski M. Generalized g-index. Scientometrics. (2025) 130:531–6. doi: 10.1007/s11192-024-05221-x
24. Nocera AP, Boudreau H, Boyd CJ, Tamhane A, Martin KD, Rais-Bahrami S. Correlation between H-index, M-index, and academic rank in urology. Urology. (2024) 189:150–5. doi: 10.1016/j.urology.2024.04.041
25. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. (2008) 5:e152. doi: 10.1371/journal.pmed.0050152
26. Baker MA, Harries AD, Jeon CY, Hart JE, Kapur A, Lönnroth K, et al. The impact of diabetes on tuberculosis treatment outcomes: a systematic review. BMC Med. (2011) 9:81. doi: 10.1186/1741-7015-9-81
27. Dooley KE, Chaisson RE. Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. (2009) 9:737–46. doi: 10.1016/s1473-3099(09)70282-8
28. Alisjahbana B, Sahiratmadja E, Nelwan EJ, Purwa AM, Ahmad Y, Ottenhoff TH, et al. The effect of type 2 diabetes mellitus on the presentation and treatment response of pulmonary tuberculosis. Clin Infect Dis. (2007) 45:428–35. doi: 10.1086/519841
29. Jiménez-Corona ME, Cruz-Hervert LP, García-García L, Ferreyra-Reyes L, Delgado-Sánchez G, Bobadilla-Del-Valle M, et al. Association of diabetes and tuberculosis: impact on treatment and post-treatment outcomes. Thorax. (2013) 68:214–20. doi: 10.1136/thoraxjnl-2012-201756
30. Leung CC, Lam TH, Chan WM, Yew WW, Ho KS, Leung GM, et al. Diabetic control and risk of tuberculosis: a cohort study. Am J Epidemiol. (2008) 167:1486–94. doi: 10.1093/aje/kwn075
31. Ponce-De-Leon A, Garcia-Garcia-Md-Mde L, Garcia-Sancho MC, Gomez-Perez FJ, Valdespino-Gomez JL, Olaiz-Fernandez G, et al. Tuberculosis and diabetes in southern Mexico. Diabetes Care. (2004) 27:1584–90. doi: 10.2337/diacare.27.7.1584
32. Stevenson CR, Forouhi NG, Roglic G, Williams BG, Lauer JA, Dye C, et al. Diabetes and tuberculosis: the impact of the diabetes epidemic on tuberculosis incidence. BMC Public Health. (2007) 7:234. doi: 10.1186/1471-2458-7-234
33. Dooley KE, Tang T, Golub JE, Dorman SE, Cronin W. Impact of diabetes mellitus on treatment outcomes of patients with active tuberculosis. Am J Trop Med Hyg. (2009) 80:634–9. doi: 10.4269/ajtmh.2009.80.634
34. Jeon CY, Harries AD, Baker MA, Hart JE, Kapur A, Lönnroth K, et al. Bi-directional screening for tuberculosis and diabetes: a systematic review. Trop Med Int Health. (2010) 15:1300–14. doi: 10.1111/j.1365-3156.2010.02632.x
35. Workneh MH, Bjune GA, Yimer SA. Prevalence and associated factors of tuberculosis and diabetes mellitus comorbidity: A systematic review. PLoS One. (2017) 12:e0175925. doi: 10.1371/journal.pone.0175925
36. Al-Rifai RH, Pearson F, Critchley JA, Abu-Raddad LJ. Association between diabetes mellitus and active tuberculosis: A systematic review and meta-analysis. PLoS One. (2017) 12:e0187967. doi: 10.1371/journal.pone.0187967
37. Huangfu P, Ugarte-Gil C, Golub J, Pearson F, Critchley J. The effects of diabetes on tuberculosis treatment outcomes: an updated systematic review and meta-analysis. Int J tuberculosis Lung disease: Off J Int Union against Tuberculosis Lung Dis. (2019) 23:783–96. doi: 10.5588/ijtld.18.0433
38. Noubiap JJ, Nansseu JR, Nyaga UF, Nkeck JR, Endomba FT, Kaze AD, et al. Global prevalence of diabetes in active tuberculosis: a systematic review and meta-analysis of data from 2·3 million patients with tuberculosis. Lancet Global Health. (2019) 7:e448–60. doi: 10.1016/s2214-109x(18)30487-x
39. Sohrabi C, Mathew G, Franchi T, Kerwan A, Griffin M, Soleil CDMJ, et al. Impact of the coronavirus (COVID-19) pandemic on scientific research and implications for clinical academic training - A review. Int J Surg. (2021) 86:57–63. doi: 10.1016/j.ijsu.2020.12.008
40. Portnoy A, Yamanaka T, Nguhiu P, Nishikiori N, Garcia Baena I, Floyd K, et al. Costs incurred by people receiving tuberculosis treatment in low-income and middle-income countries: a meta-regression analysis. Lancet Glob Health. (2023) 11:e1640–7. doi: 10.1016/s2214-109x(23)00369-8
41. Gonzalez-Muñiz OE, Rodriguez-Carlos A, Santos-Mena A, Jacobo-Delgado YM, Gonzalez-Curiel I, Rivas-Santiago C, et al. Metformin modulates corticosteroids hormones in adrenals cells promoting Mycobacterium tuberculosis elimination in human macrophages. Tuberculosis (Edinb). (2024) 148:102548. doi: 10.1016/j.tube.2024.102548
42. Chung E, Jeong D, Mok J, Jeon D, Kang HY, Kim H, et al. Relationship between metformin use and mortality in tuberculosis patients with diabetes: a nationwide cohort study. Korean J Intern Med. (2024) 39:306–17. doi: 10.3904/kjim.2023.303
43. Saktiawati AMI, Subronto YW. Influence of diabetes mellitus on the development of multi drug resistant-tuberculosis in yogyakarta. Acta Med Indones. (2018) 50:11–7.
44. Zhao L, Fan K, Sun X, Li W, Qin F, Shi L, et al. Host-directed therapy against mycobacterium tuberculosis infections with diabetes mellitus. Front Immunol. (2023) 14:1305325. doi: 10.3389/fimmu.2023.1305325
45. Wei H, Liu S, Liao Y, Ma C, Wang D, Tong J, et al. Systematic review of the medicinal potential of mulberry in treating diabetes mellitus. Am J Chin Med. (2018) 46:1743–70. doi: 10.1142/s0192415x1850088x
46. Zhao Y, Chen B, Shen J, Wan L, Zhu Y, Yi T, et al. The beneficial effects of quercetin, curcumin, and resveratrol in obesity. Oxid Med Cell Longev. (2017) 2017:1459497. doi: 10.1155/2017/1459497
47. Shang Y, Bao L, Bi H, Guan S, Xu J, Gu Y, et al. Authenticity discrimination and adulteration level detection of camellia seed oil via hyperspectral imaging technology. Food Analytical Methods. (2024) 17:450–63. doi: 10.1007/s12161-024-02577-x
48. Wang Y, He X, Zheng D, He Q, Sun L, Jin J. Integration of metabolomics and transcriptomics reveals major metabolic pathways and potential biomarkers involved in pulmonary tuberculosis and pulmonary tuberculosis-complicated diabetes. Microbiol Spectr. (2023) 11:e0057723. doi: 10.1128/spectrum.00577-23
Keywords: bibliometrics, diabetes mellitus, tuberculosis, diabetes mellitus complicated with tuberculosis (DM-TB), research trends
Citation: Li Y, Ni R, An Y, Yang L, Ye Z, Zhuang L, Li L, Wang L and Gong W (2025) Bibliometric analysis and knowledge mapping of diabetes mellitus combined with tuberculosis research: trends from 1995 to 2023. Front. Immunol. 16:1571123. doi: 10.3389/fimmu.2025.1571123
Received: 05 February 2025; Accepted: 14 March 2025;
Published: 04 April 2025.
Edited by:
Tao Yi, Hong Kong Baptist University, Hong Kong SAR, ChinaReviewed by:
Kun Liu, Air Force Medical University, ChinaNingning Song, Shandong Second Medical University, China
Copyright © 2025 Li, Ni, An, Yang, Ye, Zhuang, Li, Wang and Gong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liang Wang, V2FuZ2wzMDlAc2luYS5jb20=; Wenping Gong, Z3dwODkxMDE1QHdodS5lZHUuY24=