 Lóránt Varju1,2
Lóránt Varju1,2 Zsuzsa Bagoly3,4
Zsuzsa Bagoly3,4 Éva Ajzner5
Éva Ajzner5 Rita Orbán-Kálmándi3,4Anna Zsófia Kádár3,4Judit Nevelős5
Rita Orbán-Kálmándi3,4Anna Zsófia Kádár3,4Judit Nevelős5 Péter Ilonczai1*
Péter Ilonczai1*- 1Department of Hematology, Szabolcs-Szatmár-Bereg County Teaching Hospitals, András Jósa Hospital, Nyíregyháza, Hungary
- 2Kálmán Laki Doctorate School, University of Debrecen, Debrecen, Hungary
- 3Division of Clinical Laboratory Science, Department of Laboratory Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 4Lendület “Momentum” Hemostasis and Stroke Research Group of the Hungarian Academy of Sciences, Debrecen, Hungary
- 5Central Laboratory, Szabolcs-Szatmár-Bereg County Teaching Hospitals, András Jósa Hospital, Nyíregyháza, Hungary
Introduction: Antiphospholipid syndrome (APS) is an autoimmune disease characterized by a hypercoagulable state and recurrent thromboembolism (TE). Patients with triple-positive antiphospholipid antibodies (APAs) are at the highest risk of TE. As standard treatment for these patients, oral anticoagulation therapy (OAT) with vitamin K antagonists (VKAs) is widely used, but inaccurate International Normalized Ratio (INR) measurement due to APA interference can complicate monitoring.
Case: Here we report the case of a 19-year-old male patient, with a history of submassive pulmonary embolism at the age of 13. Thrombophilia investigations confirmed type II antithrombin deficiency (Budapest 3 heterozygous) combined with triple-positive APS. He received sustained VKA (warfarin) therapy, but his INR values showed strikingly different results when monitored in two different laboratories (INR 3–4 vs. INR >8 on multiple occasions). Therefore, we aimed to investigate the impact of different thromboplastin reagents on INR values in this triple-positive APS patient receiving VKA therapy. INR measurements were performed using animal-derived (rabbit brain-derived) and recombinant thromboplastins. The effect of purified patient IgG concentrates was examined on INR values using antiphospholipid antibody-negative plasma mixtures. Chromogenic FXa activity (CFXa) was also measured to assess the true anticoagulant effect of VKA.
Conclusions: INR values measured using recombinant thromboplastin reagent were consistently higher and less reliable in high APA-titer conditions compared to rabbit brain-derived reagent. CFXa results were more consistent with INR values obtained using rabbit brain-derived thromboplastin. Rabbit brain-derived thromboplastin, less sensitive to APA interference, provided reliable INR monitoring for this high-risk patient. We recommend choosing thromboplastin reagents without interference to APAs, to optimize OAT monitoring in similar cases of patients with high APA-titers.
Introduction
Antiphospholipid syndrome (APS) is an autoimmune disease characterized by recurrent thromboembolism (TE) and obstetric complications. The revised Sapporo criteria for APS require at least one clinical criterion (vascular thrombosis and/or pregnancy morbidity) and one laboratory criterion, which can be any of the following: lupus anticoagulant (LA), anticardiolipin (aCL) IgG or IgM, or anti-β2-glycoprotein I (aβ2GPI) IgG or IgM, confirmed on two or more occasions, at least 12 weeks apart (1–3). In the 2023 American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) APS classification criteria, the type of laboratory parameters remain essentially unchanged compared with the updated Sapporo classification criteria, but aCL and aβ2GPI measurement are restricted to enzyme-linked immunosorbent assays (ELISAs) with moderate and high titer aPL thresholds defined as 40 and 80 Units (4). It must be noted, that the ACR/EULAR classification criteria, having excellent specificity, are meant for participant inclusion in studies and trials to study homogeneous populations of patients, and in general, laboratory detection for APS diagnosis in daily practice remain broader, meant to diagnose each APS patient to optimize their management (3, 4). In APS, thromboses are caused by APA-induced vascular cell activation, inhibition of natural anticoagulants and the fibrinolytic system, and complement activation (2, 5). The triple-positive form of APS presents the highest TE risk, which is characterized by the simultaneous occurrence of LA, ACL and aB2GP1 (6), and is often associated with catastrophic APS and pregnancy loss (7). The risk of recurrent TE is the highest in the triple-positive group of APS patients (8, 9). Secondary TE prevention is the primary goal in APS patients (10, 11). Although direct oral anticoagulants (DOACs) have been investigated, their safety and efficacy in APS are debated, and are not recommended for triple-positive APS (12–14). Instead, vitamin K antagonists (VKAs) remain the cornerstone anticoagulation therapy (15).
INR monitoring in APS patients can be challenging due to LA interference, which affects thromboplastin reagents differently (16, 17). If a TE event occurs despite VKA therapy, the thromboplastin reagent’s LA sensitivity should be reviewed, and confirmatory testing (e.g., FXa amidolytic assays) should be performed (11).
Case description
We report the case of a 19-year-old male with a history of deep vein thrombosis (DVT) at the age of 12 and submassive pulmonary embolism (PE) at 13 years old. Thrombophilia investigations confirmed type II antithrombin deficiency (Budapest 3 heterozygous) and triple-positive APS. Despite sustained VKA (warfarin) therapy, INR values varied significantly between two laboratories (INR 3–4 vs. INR >8). To investigate these discrepancies, we assessed the impact of different thromboplastin reagents on INR measurements using the patient’s plasma and IgG purified from the patient’s serum.
The presence of LA was confirmed based on the screening and confirmatory tests in accordance with the revised Sapporo recommendations (1). The quantitative determination of aB2GP1 IgG and IgM and ACL IgG and IgM antibodies was performed using the ELISA method (QUANTA Lite, Inova Diagnostics). IgG of the triple-positive APS patient was purified by affinity chromatography (MabTrap Kit, GE Healthcare). The protein content obtained by chromatography was measured using a Multiskan Sky photometer (Pierce BCA Protein Assay Kit, Thermo Scientific). We examined the effect of purified patient IgG concentrates on coagulation screening tests, with special regard to INR. The measurements were also performed on an aPL-negative plasma mixture with therapeutic (2.0-3.5) and above therapeutic (>3.5) range of INR. During the measurements, we used animal-derived (rabbit brain thromboplastin, Dia-PT, ISI: 1.16, Diagon, Budapest, Hungary) and recombinant thromboplastin (Innovin, ISI: 0.91, Siemens Healthcare Diagnostics, Marburg, Germany) thromboplastin reagents. As control tests, measurements were performed with the purified IgG of aPL-negative individuals. The effect of VKA was verified by chromogenic FX activity (CFXa) measurements, using a commercially available amidolytic method (Siemens Healthcare Diagnostics, Marburg, Germany).
The patient’s detailed history includes hospitalization at the age of 10 (in 2006) due to bilateral pneumonia that was treated with antibiotics and healed without further complications. Two years later he was readmitted for deep vein thrombosis (DVT) in his left lower extremity. Doppler ultrasound revealed thrombosis in the left femoral common vein, profound vein, posterior and anterior tibial veins. Laboratory results showed an elevated D-dimer level (1.17 mg FEU/L, reference threshold < 0.5 mg FEU/L). He was treated with therapeutic doses of low-molecular-weight heparin (LMWH), transitioned to warfarin (6 mg daily, corresponding to a target INR of 2-3, that was achieved and typically maintained with an INR range of 1.7-4). The patient was referred for pediatric hematology evaluation to rule out familial and/or acquired thrombophilia.
At age 13 (February 2009), the patient was hospitalized again due to weakness and exertional dyspnea. Laboratory findings included an INR of 3.36 (using rabbit brain-derived thromboplastin, Dia-PT, ISI: 1.16, Diagon, Budapest, Hungary), APTT of 73 seconds (reference range APTT: 26–36 sec) and a D-dimer level of 0.79 mg FEU/L. A chest X-ray revealed cardiomegaly, while a cardiology examination showed right heart strain, incomplete right bundle branch block, and pulmonary hypertension. Chest computed tomography (CT) identified calcification in the right main pulmonary artery, raising suspicion of thrombus presence. Pulmonary scintigraphy confirmed pulmonary embolism in the affected region. Although thrombophilia testing had been previously suggested, it was only conducted at this point. Laboratory results confirmed lupus anticoagulant (LA) positivity and type II antithrombin deficiency (Budapest 3 heterozygous).
The patient was referred to the National Institute of Cardiology (György Gottsegen Institute, Budapest, Hungary) for consideration of therapeutic embolectomy. Due to the complexity of the case, a consultation was arranged with an international center (Allgemeine Krankenhaus, Vienna, Austria) to perform the procedure. One month later, the patient underwent a successful thrombectomy in Vienna. However, in the postoperative period, a subtotal thromboembolism developed, necessitating a second thrombectomy within 48 hours. This time, antithrombin replacement and low-dose methylprednisolone therapy were administered. The patient’s oral anticoagulation regimen was switched from warfarin to acenocoumarol.
The patient was first seen in our adult hematology clinic at the age of 18 while on stable vitamin K antagonist therapy (acenocoumarol 5 mg daily). His INR was 3.72 at that visit, measured using rabbit brain-derived thromboplastin (Dia-PT, ISI: 1.16, Diagon, Budapest, Hungary). However, subsequent INR values showed considerable variability depending on the laboratory and thromboplastin reagent used (Figure 1A). To investigate this discrepancy, we performed parallel INR and chromogenic factor X (CFXa) measurements on two separate occasions, using an amidolytic method (Siemens Healthcare Diagnostics, Marburg, Germany, reference range: 70-120%), based on previous literature (18). CFXa results—reflecting the pharmacodynamic effect of VKA—aligned more closely with INR values obtained using rabbit brain-derived thromboplastin. In contrast, INR measurements with recombinant thromboplastin reagent (Innovin, ISI: 0.91, Siemens Healthcare Diagnostics, Marburg, Germany) were consistently higher and not supported by the moderately reduced FXa levels. This discrepancy was not attributed to INR calibration errors. The different INR values obtained were reproducible using the same coagulometer (BCS XP, Siemens) and the same plasma sample but different thromboplastin reagents (data not shown). This suggested that the recombinant reagent might be more susceptible to interference from antiphospholipid antibodies, leading us to further test the impact of patient-derived IgG on INR measurements with both types of thromboplastins.
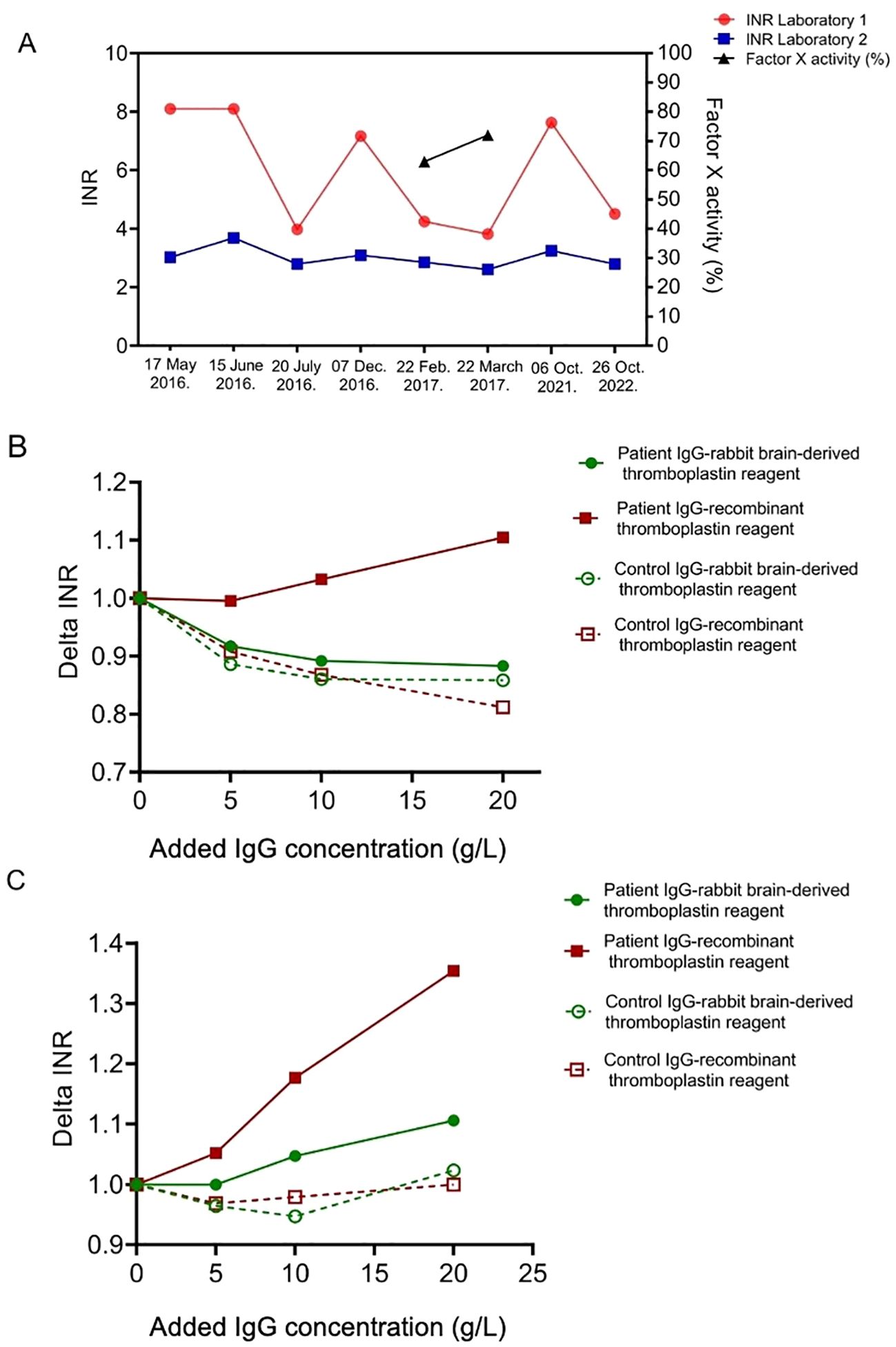
Figure 1. Impact of thromboplastin reagent type on international normalized ratio (INR) measurement in a triple-positive APS patient. (A) INR values (left axis) from the plasma sample of a triple-positive APS patient on vitamin K antagonist therapy, measured in two different laboratories (red circles and blue squares) over time. Laboratory 1 had been using recombinant thromboplastin (Innovin, ISI: 0.91, Siemens Healthcare Diagnostics, Marburg, Germany, red circles), while Laboratory 2 used animal-derived, rabbit brain thromboplastin (Dia-PT, ISI: 1.16, Diagon, Budapest, Hungary) to assess INR. Chromogenic factor X activity (%) (black triangles) is plotted on the right axis to assess anticoagulation effectiveness. The corresponding values of factor X activity, Laboratory 1 INR, and Laboratory 2 INR were as follows: 63%, 4.25 and 2.86 (February 22, 2017) and 72%, 3.82 and 2.61 (March 22, 2017), respectively. (B) Changes in INR (Delta INR) after adding increasing concentrations of purified patient IgG (solid symbols) or control IgG (open symbols) to aPL-negative control plasma, measured using either rabbit brain-derived thromboplastin (green circles) or recombinant thromboplastin (red squares). (C) Changes in INR (Delta INR) after adding increasing concentrations of purified patient IgG (solid symbols) or control IgG (open symbols) to plasma with therapeutic INR (3.5).
Repeat thrombophilia testing at the regional center (University of Debrecen, Hungary) showed persistently high INR values (>8), a prolonged APTT of 145 seconds, and an APTT-LA of 119 seconds. Additional findings included an antithrombin activity of 73%, anti-beta 2 glycoprotein 1 (anti-B2GPI) IgG levels exceeding 6100 U/ml, and anticardiolipin IgG levels surpassing 2024 U/ml. After 12 weeks, repeated antiphospholipid antibody testing confirmed extremely high APA titers, leading to a definitive diagnosis of triple-positive APS, associated with a high risk of thromboembolism. Further etiological workup revealed a congenital IgA deficiency.
INR values measured with the recombinant thromboplastin reagent were influenced in a concentration-dependent manner when purified IgG from the patient was added to aPL-negative control plasma at varying concentrations, while this effect was not observed when INR values were obtained using rabbit brain-derived thromboplastin (Figure 1B). As a control, purified IgG from aPL-negative individuals was tested, showing no significant impact on INR measurements. The purified patient IgG, in addition to the IgG concentration already present in the patient’s plasma, significantly prolonged the INR of the VKA-anticoagulated pooled plasma measured with recombinant thromboplastin reagent —an effect that was negligible when using rabbit brain-derived thromboplastin (Figure 1C). This result is of particular relevance, as FX activity did not reach the expected therapeutic range in the patient, it was therefore considered that the INR obtained by rabbit brain-derived thromboplastin may also have been affected to some extent by lupus anticoagulant interference. However, based on the above-described experiments, the extent of this interference was not considerable. Of note, prolongation of INR by the purified IgG of the patient in VKA-anticoagulated pooled plasma was particularly pronounced in therapeutic or higher INR ranges. In contrast, no such phenomenon was observed when using IgG from aPL-negative controls.
The patient’s anticoagulation therapy with vitamin K antagonists was closely monitored in a 10-year follow-up period. Anticoagulation adjustments were based on INR values from the local laboratory. INR was monitored every three months at our outpatient clinic, and values remained consistently within the therapeutic range (2.0-3.0). This approach was effective in preventing secondary TE events, as over a 10-year follow-up period, no thromboembolic or hemorrhagic complications were observed.
Discussion
The clinical significance of accurate INR monitoring in triple-positive APS patients is substantial, given their elevated risk of thromboembolic (TE) events. The primary objective in managing such patients is the prevention of secondary TE, typically achieved through VKA therapy. While direct oral anticoagulants (DOACs) have been explored, findings from the TRAPS study and subsequent follow-ups suggest that rivaroxaban is inadequate for oral anticoagulant therapy (OAT) in this high-risk subgroup (14, 19). Current evidence supports the continued use of VKAs, provided that INR monitoring is precise and unaffected by APA interference.
Commercially available thromboplastin reagents vary in their composition and sensitivity to lupus anticoagulant (LA) interference. A multinational study examined nine thromboplastin reagents, including human recombinant, human placenta-derived, and rabbit brain-derived formulations (16). The objective was to distinguish true LA-induced INR variability from calibration-related artifacts and to identify optimal reagents for OAT monitoring. Key limitations of previous investigations, such as small sample sizes and inconsistent calibration methods, were addressed in this study by implementing centralized sample processing and uniform analytical procedures. Findings indicated that among recombinant thromboplastins, only one exhibited significant LA interference, while the majority of reagents, including recombinant thromboplastin reagents showed minimal or no susceptibility. This underscores the importance of reagent selection, as INR values measured using thromboplastins with instrument-specific International Sensitivity Index (ISI) calibration were deemed reliable. However, newer thromboplastins incorporating relipidated or recombinant tissue factor components may exhibit varying degrees of LA sensitivity. Research by Della Valle et al. demonstrated that INR values measured with recombinant thromboplastins containing synthetic phospholipid components were systematically overestimated in LA-positive patients, particularly when low plasma dilutions (1:3 final dilution) were used. By contrast, reagents incorporating bovine brain-derived thromboplastins at higher plasma dilutions (1:20) yielded more accurate results. This suggests that reagent composition and dilution ratios are critical determinants of INR reliability in APS patients (20).
Consequently, LA interference should be assessed before utilizing such reagents for INR-based OAT monitoring. As an alternative, CFXa measurement may serve as a confirmatory test, albeit with limitations such as cost and prolonged turnaround times (18). It must be noted that in rare cases, a differential diagnosis to consider is lupus anticoagulant-hypoprothrombinemia syndrome (LAHS), a condition characterized by lupus anticoagulant positivity with acquired hypoprothrombinemia, often due to anti-prothrombin antibodies. LAHS can present with markedly prolonged PT/INR and is associated with both thrombotic and severe bleeding complications, making it important to recognize in anticoagulated APS patients with unexpected INR elevations (21).
In APS patients with prolonged baseline INR values prior to warfarin initiation or recurrent TE despite therapeutic INR ranges, CFXa measurement may be indispensable. The utility of CFXa in these clinical situations has been demonstrated by independent groups (18, 22–24). Some experts advocate for dual INR and CFXa monitoring during treatment stabilization, a concept referred to as CFXa-calibrated INR targeting. Supporting this approach, an Italian working group compared INR values obtained using two different thromboplastins across 16 LA-positive and 11 LA-negative patients (25). Notably, they concluded that INR values exceeding 4.0 were disproportionately observed in LA-positive samples, reinforcing the need for supplementary CFXa testing in such cases. CFXa typically shows a strong inverse correlation with INR values between 2.0 and 3.0, which supports its utility in assessing anticoagulation intensity within this therapeutic window. However, it is important to note that the interpretation of FX activity measurements becomes increasingly uncertain at supratherapeutic INR levels, particularly above 3.5. At these high INR values, the correlation between FX activity and anticoagulation intensity weakens, limiting the clinical utility of CFXa for monitoring purposes. Efthymiou et al. reported that FX activity may overestimate anticoagulant effect in such settings (18), while Rosborough et al. highlighted the reduced accuracy in patients on warfarin initiation compared with chronic warfarin administration (23). These findings suggest that FX activity results should be interpreted with caution during the initiation of warfarin treatment and when INR exceeds the upper therapeutic threshold.
Compared to prior studies that assessed thromboplastin reagent sensitivity in APS patients, our case report provides a unique combination of clinical, laboratory, and mechanistic insights. While earlier investigations primarily compared INR variability across different reagents in broader APS cohorts, our study is distinguished by its focus on a single, well-characterized triple-positive patient with extremely high APA titers and recurrent thromboembolism. Importantly, we employed patient-derived purified IgG to demonstrate a concentration-dependent interference with recombinant thromboplastin reagents—an approach rarely utilized in prior reports. Given the limited literature addressing the impact of thromboplastin reagent variability in antiphospholipid syndrome, particularly in triple-positive patients, our case report provides timely and clinically relevant insights that may assist both clinical laboratories and physicians in optimizing anticoagulation monitoring strategies. In a most recent study, pooled normal plasma and control plasma from patients on VKA (without LA) were incubated with monoclonal and isolated patient immunoglobulin G antiprothrombin and anti–beta-2-glycoprotein I antibodies that express LA activity. INR was determined before and after addition using 3 laboratory assays (Owren STA-Hepato Prest, Quick STA-NeoPTimal, and Quick STA-Neoplastine R) and 1 point-of-care test device (CoaguChek Pro II) (26). In line with our findings, the authors concluded that INR reagents that utilized recombinant human thromboplastin were more sensitive to the presence of monoclonal and patient-derived antibodies with LA activity, consequently, APS patients positive for LA were suggested to be monitored using tissue-derived thromboplastin reagents.
It should be emphasized that determining the true INR value in patients with triple-positive antiphospholipid syndrome is not merely a technical issue but a clinical imperative. Inaccurate INR readings—particularly overestimations due to reagent sensitivity—can lead to inappropriate dose adjustments, resulting in under-anticoagulation with risk of thromboembolic recurrence or over-anticoagulation with bleeding complications. Given the high thrombotic risk in these patients and the limitations of DOACs in this population, the reliability of INR measurement directly impacts patient safety and long-term outcomes. Therefore, individualized INR monitoring strategies, guided by thromboplastin reagent sensitivity and, when necessary, confirmed with CFXa assays, are essential to ensure accurate anticoagulation assessment and therapeutic efficacy. Our findings, while derived from a single-patient case study, offer a valuable starting point for future investigations and encourage methodological refinements in anticoagulation monitoring for APS patients.
Conclusions
This report highlights the importance of thromboplastin reagent selection in the INR-based monitoring of high-risk, triple-positive APS patients on VKA therapy. INR values obtained with low-plasma-diluted recombinant thromboplastins were significantly elevated compared to those measured with higher-plasma-diluted rabbit brain thromboplastins, particularly in the upper INR range. This discrepancy was not observed in aPL-negative controls. As a confirmatory test, CFXa activity measurement correlated more closely with INR values obtained using rabbit brain-derived thromboplastin, supporting its use as a reliable tool in cases of suspected LA interference within the therapeutic INR range. Given the critical implications for patient safety, we recommend prioritizing high-plasma-dilutions with animal-derived, or combined thromboplastin reagents for INR monitoring in triple-positive APS patients receiving VKAs.
Limitations
While our study provides valuable insights into INR measurement discrepancies in triple-positive APS patients, several limitations should be considered. First, our findings are based on a single high-risk patient, necessitating validation in larger cohorts to confirm the generalizability of our results. Second, variability among commercial thromboplastin reagents underscores the need for standardization in INR monitoring, as reagent composition and ISI calibration may differ across laboratories. Third, due to limited sample availability, FX activity measurement was only performed on two occasions in this study, a limitation that was beyond the control of the investigators. It must be noted that while this test may serve as a relevant confirmatory test within the therapeutic INR range, its routine clinical application is often hindered by high costs, long turnaround times, and limited accessibility in many healthcare settings. Finally, further studies are needed to explore the impact of additional confounding factors, such as coexisting prothrombotic conditions and genetic predispositions, on INR variability in APS patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Ethics Committee of the University of Debrecen, Hungary. The studies were conducted in accordance with the local legislation and institutional requirements. The participant provided their written informed consent to participate in this study. Written informed consent was obtained from the individual for the publication of any potentially identifiable data included in this article.
Author contributions
LV: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. ZB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. ÉA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. RO-K: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AK: Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. JN: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. PI: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Hungarian Society of Hematology and Transfusion, and the Lendület “Momentum” Hemostasis and Stroke Research Group of the Hungarian Academy of Sciences, Debrecen, Hungary. This research work was conducted with the support of the National Academy of Scientist Education Program of the National Biomedical Foundation under the sponsorship of the Hungarian Ministry of Culture and Innovation. Supported by the grants from the National Research, The Development and Innovation Fund (FK128582, EKÖP-24-2-DE-100 and TKP 2021 EGA-19, financed under the TKP2021-EGA funding scheme, and the HUN-REN Hungarian Research Network (HUN-REN Cerebrovascular Research Group).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. (2006) 4:295–306. doi: 10.1111/j.1538-7836.2006.01753.x
2. Chaturvedi S and McCrae KR. Diagnosis and management of the antiphospholipid syndrome. Blood Rev. (2017) 31:406–17. doi: 10.1016/j.blre.2017.07.006
3. Devreese KMJ, Bertolaccini ML, Branch DW, de Laat B, Erkan D, Favaloro EJ, et al. An update on laboratory detection and interpretation of antiphospholipid antibodies for diagnosis of antiphospholipid syndrome: guidance from the ISTH-SSC Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibodies. J Thromb Haemost. (2025) 23:731–44. doi: 10.1016/j.jtha.2024.10.022
4. Barbhaiya M, Zuily S, Naden R, Hendry A, Manneville F, Amigo MC, et al. ACR/EULAR antiphospholipid syndrome classification criteria. Ann Rheum Dis. (2023) 82(10):1258–70. doi: 10.1136/ard-2023-224609
5. Schreiber K, Sciascia S, de Groot PG, Devreese K, Jacobsen S, Ruiz-Irastorza G, et al. Antiphospholipid syndrome. Nat Rev Dis Primers. (2018) 4:17103. doi: 10.1038/nrdp.2017.103
6. Pengo V, Bison E, Zoppellaro G, Padayattil Jose S, Denas G, Hoxha A, et al. APS - Diagnostics and challenges for the future. Autoimmun Rev. (2016) 15:1031–3. doi: 10.1016/j.autrev.2016.07.028
7. Pengo V, Ruffatti A, Legnani C, Testa S, Fierro T, Marongiu F, et al. Incidence of a first thromboembolic event in asymptomatic carriers of high-risk antiphospholipid antibody profile: a multicenter prospective study. Blood. (2011) 118:4714–8. doi: 10.1182/blood-2011-03-340232
8. Ruffatti A, Tonello M, Visentin MS, Bontadi A, Hoxha A, De Carolis S, et al. Risk factors for pregnancy failure in patients with anti-phospholipid syndrome treated with conventional therapies: a multicentre, case-control study. Rheumatol (Oxford). (2011) 50:1684–9. doi: 10.1093/rheumatology/ker139
9. Pengo V, Ruffatti A, Legnani C, Gresele P, Barcellona D, Erba N, et al. Clinical course of high-risk patients diagnosed with antiphospholipid syndrome. J Thromb Haemost. (2010) 8:237–42. doi: 10.1111/j.1538-7836.2009.03674.x
10. Garcia D and Erkan D. Diagnosis and management of the antiphospholipid syndrome. N Engl J Med. (2018) 378:2010–21. doi: 10.1111/bjh.16431
11. Arachchillage DRJ and Laffan M. What is the appropriate anticoagulation strategy for thrombotic antiphospholipid syndrome? Br J Haematol. (2020) 189:216–27.
12. Dufrost V, Risse J, Reshetnyak T, Satybaldyeva M, Du Y, Yan XX, et al. Increased risk of thrombosis in antiphospholipid syndrome patients treated with direct oral anticoagulants. Results from an international patient-level data meta-analysis. Autoimmun Rev. (2018) 17:1011–21. doi: 10.1016/j.autrev.2018.04.009
13. Cohen H, Hunt BJ, Efthymiou M, Arachchillage DR, Mackie IJ, Clawson S, et al. Rivaroxaban versus warfarin to treat patients with thrombotic antiphospholipid syndrome, with or without systemic lupus erythematosus (RAPS): a randomised, controlled, open-label, phase 2/3, non-inferiority trial. Lancet Haematol. (2016) 3:e426–36. doi: 10.1016/S2352-3026(16)30079-5
14. Pengo V, Denas G, Zoppellaro G, Jose SP, Hoxha A, Ruffatti A, et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood. (2018) 132:1365–71. doi: 10.1182/blood-2018-04-848333
15. Cohen H, Efthymiou M, and Devreese KMJ. Monitoring of anticoagulation in thrombotic antiphospholipid syndrome. J Thromb Haemost. (2021) 19:892–908. doi: 10.1111/jth.15217
16. Tripodi A, Chantarangkul V, Clerici M, Negri B, Galli M, and Mannucci PM. Laboratory control of oral anticoagulant treatment by the INR system in patients with the antiphospholipid syndrome and lupus anticoagulant. Results of a collaborative study involving nine commercial thromboplastins. Br J Haematol. (2001) 115:672–8. doi: 10.1046/j.1365-2141.2001.03178.x
17. Isert M, Miesbach W, Schuttfort G, Weil Y, Tirneci V, Kasper A, et al. Monitoring anticoagulant therapy with vitamin K antagonists in patients with antiphospholipid syndrome. Ann Hematol. (2015) 94:1291–9. doi: 10.1007/s00277-015-2374-3
18. Efthymiou M, Lawrie AS, Mackie I, Arachchillage D, Lane PJ, Machin S, et al. Thrombin generation and factor X assays for the assessment of warfarin anticoagulation in thrombotic antiphospholipid syndrome. Thromb Res. (2015) 135:1191–7. doi: 10.1016/j.thromres.2015.03.030
19. Nielsen CT, Rasmussen NS, Heegaard NH, and Jacobsen S. Kill" the messenger: Targeting of cell-derived microparticles in lupus nephritis. Autoimmun Rev. (2016) 15:719–25. doi: 10.1016/j.autrev.2016.03.009
20. Della Valle P, Crippa L, Garlando AM, Pattarini E, Safa O, Vigano D'Angelo S, et al. Interference of lupus anticoagulants in prothrombin time assays: implications for selection of adequate methods to optimize the management of thrombosis in the antiphospholipid-antibody syndrome. Haematologica. (1999) 84:1065–74.
21. Nusrat S, Tewari S, and Khan O. Successful treatment of lupus anticoagulant hypoprothrombinemia syndrome with rituximab. Thromb J. (2023) 21:77. doi: 10.1186/s12959-023-00517-z
22. Rosborough TK, Jacobsen JM, and Shepherd MF. Factor X and factor II activity levels do not always agree in warfarin-treated lupus anticoagulant patients. Blood Coagul Fibrinolysis. (2010) 21:242–4. doi: 10.1097/MBC.0b013e32833581a3
23. Rosborough TK, Jacobsen JM, and Shepherd MF. Relationship between chromogenic factor X and international normalized ratio differs during early warfarin initiation compared with chronic warfarin administration. Blood Coagul Fibrinolysis. (2009) 20:433–5. doi: 10.1097/MBC.0b013e32832ca31f
24. Baumann Kreuziger LM, Datta YH, Johnson AD, Zantek ND, Shanley R, and Reding MT. Monitoring anticoagulation in patients with an unreliable prothrombin time/international normalized ratio: factor II versus chromogenic factor X testing. Blood Coagul Fibrinolysis. (2014) 25:232–6. doi: 10.1097/MBC.0000000000000030
25. Ferrazzi P, Colombo A, Di Micco P, Lodigiani C, Libre L, Rota LL, et al. Differences in the INR evaluation of two different thromboplastins in patients with positivity to lupus anticoagulant in ongoing oral anticoagulation. J Blood Med. (2010) 1:57–60. doi: 10.2147/JBM.S8938
26. Gehlen R, Moesbergen RG, Bai C, de Groot PG, Jansen AJG, Meijers JCM, et al. Interference of lupus anticoagulant causing antiprothrombin and anti-beta-2-glycoprotein I antibodies on international normalized ratio measurements: comparative analysis of international normalized ratio methods. Res Pract Thromb Haemost. (2024) 8:102470. doi: 10.1016/j.rpth.2024.102470
Keywords: triple-positive antiphospholipid syndrome, recurrent thromboembolism, case report, INR monitoring, antiphospholipid antibodies
Citation: Varju L, Bagoly Z, Ajzner É, Orbán-Kálmándi R, Kádár AZ, Nevelős J and Ilonczai P (2025) Impact of thromboplastin reagents on monitoring INR in a patient with triple-positive antiphospholipid syndrome: a case report. Front. Immunol. 16:1591029. doi: 10.3389/fimmu.2025.1591029
Received: 10 March 2025; Accepted: 09 July 2025;
Published: 31 July 2025.
Edited by:
Danieli Castro Oliveira De Andrade, University of São Paulo, BrazilReviewed by:
Koshy Nithin Thomas, Christian Medical College, IndiaChristiane Gouvea, Fleury S.A., Brazil
Copyright © 2025 Varju, Bagoly, Ajzner, Orbán-Kálmándi, Kádár, Nevelős and Ilonczai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Péter Ilonczai, aWxvbmN6YWlAbWVkLnVuaWRlYi5odQ==