 Luise Appeltshauser1†*
Luise Appeltshauser1†* Christian P. Moritz2,3†
Christian P. Moritz2,3† Lena Reinhardt1†
Lena Reinhardt1† Luisa Kreß1
Luisa Kreß1 Nurcan Üçeyler1
Nurcan Üçeyler1 François Lassablière3Anastasia Barcic1
François Lassablière3Anastasia Barcic1 Sabine Seefried1
Sabine Seefried1 Claudia Sommer1
Claudia Sommer1 Yannick Tholance4
Yannick Tholance4 Jean-Christophe Antoine2
Jean-Christophe Antoine2 Jean-Philippe Camdessanché2
Jean-Philippe Camdessanché2 Kathrin Doppler1
Kathrin Doppler1- 1Department of Neurology, University Hospital Würzburg, Würzburg, Germany
- 2Department of Neurology, CHU Saint-Etienne, Saint-Etienne, France
- 3Synaptopathies et autoanticorps (SynatAc), Institut MELIS-NeuroMyoGène, INSERM U1314/CNRS UMR 5284, Université Jean Monnet, Saint-Étienne, France
- 4Department of Biochemistry, CHU Saint-Etienne, Saint-Etienne, France
Introduction: Autoantibodies against fibroblast growth factor receptor 3 (FGFR3) have been suggested as a diagnostic marker in both sensory large and small fiber neuropathy. Yet, their clinical relevance remains unclear and no standardized protocols for antibody testing exist. Here, we evaluate an anti-FGFR3 ELISA protocol in an inter-laboratory comparison.
Methods: We performed anti-FGFR3 ELISA on 42 serum samples of patients with sensory neuronopathy (n = 18), small fiber neuropathy (n = 18), and healthy controls (n = 6) in two independent centers in France (center 1) and Germany (center 2) using identical protocols, with double immunofluorescence staining on rat dorsal root ganglion (DRG) sections as a confirmational test.
Results: Overall ELISA concordance was 34/42 (81.0%, Cohen’s kappa = 0.61, substantial agreement). Discordance occurred for sera with optical densities (OD) near the cut-off. ODs correlated (r = 0.68, p < 0.0001), but were lower at center 2 (median = 0.076 vs 0.293, p < 0.0001), indicating that cut-off values are laboratory-specific. 11/16 (68.8%) ELISA-double-positive sera stained small DRG neurons, colocalizing with commercial anti-FGFR3 antibody, while positive binding was only found in 1/20 (5%) of ELISA-negative sera (p < 0.0001). DRG-positive samples showed higher ODs than negative ones (p < 0.0001).
Discussion: We provide and evaluate a detailed ELISA protocol for anti-FGFR3 diagnostic assessment. Positive results near the threshold should be interpreted cautiously. Anti-FGFR3 DRG staining may be a useful confirmatory method and could increase diagnostic specificity. This study facilitates future studies on the diagnostic relevance of anti-FGFR3 autoantibodies in sensory neuropathies.
1 Introduction
Sensory neuropathies, encompassing both large and small fiber pathology, are debilitating diseases of the peripheral nervous system (PNS), characterized by sensory deficits, autonomic dysfunction, and/or neuropathic pain (1, 2). The etiologies are diverse, including metabolic, paraneoplastic, genetic, toxic, and autoimmune causes. Despite extensive diagnostic work-up, many cases remain idiopathic (1, 3). Identifying autoimmune etiologies among these idiopathic cases is particularly crucial, as this could have a direct impact on treatment decisions (2). Recent studies have identified autoantibodies against fibroblast growth factor receptor 3 (FGFR3) as a potential biomarker for sensory neuropathies particularly affecting the dorsal root ganglia (DRG), such as sensory neuronopathy (SNN) and small fiber neuropathy (SFN) (3–5).
FGFR3, a member of the tyrosine kinase receptor family, is suggested to be expressed in sensory neurons of the DRG and plays an important role in neuronal development and maintenance (4, 6, 7). The presence of anti-FGFR3 antibodies in SNN and SFN could indicate a possible autoimmune mechanism targeting the DRG. Still, the antibody’s ability to bind these targets and their clinical relevance remain unclear. Further, anti-FGFR3 are not exclusive for sensory neuropathies, but can also occur in other neuropathies, questioning the specificity of the test (8).
Detection of anti-FGFR3 is primarily conducted using ELISA, and normalization of serum-specific background noise by subtraction can increase the sensitivity and specificity of the assay (4, 9). Still, many studies report anti-FGFR3 test results without a published protocol or a second validation method. These inconsistencies underscore the necessity for standardized testing protocols to ensure reliable and reproducible results.
In this context, we aimed to evaluate an anti-FGFR3 ELISA protocol through an inter-laboratory comparison between two independent centers in France and Germany. By analyzing serum samples from patients with SNN, SFN, and healthy controls, we sought to assess the concordance of ELISA results and establish standardized procedures for antibody testing. Additionally, we employed double immunofluorescence staining on DRG sections, providing a complementary method to enhance diagnostic accuracy. Our findings address the critical need for standardizing anti-FGFR3 testing in sensory neuropathies.
2 Methods
2.1 Anti-FGFR3 ELISA protocol
We established and applied a protocol for FGFR3 testing from the reference laboratory (center 1) at center 2 according to previously published information only (4), and in a second step adapted the protocol to the details provided by center 1, as shown in Table 1. For center 1, cut-off values to define an anti-FGFR3-positive result had been determined as previously described from 65 healthy control sera without reported autoimmune disease, neurological disease including neuropathic pain, or malignancy (4). For center 2, these cut-off values were determined using 50 healthy controls whose sera had been recruited during previous studies (10, 11) or routine diagnostic testing.
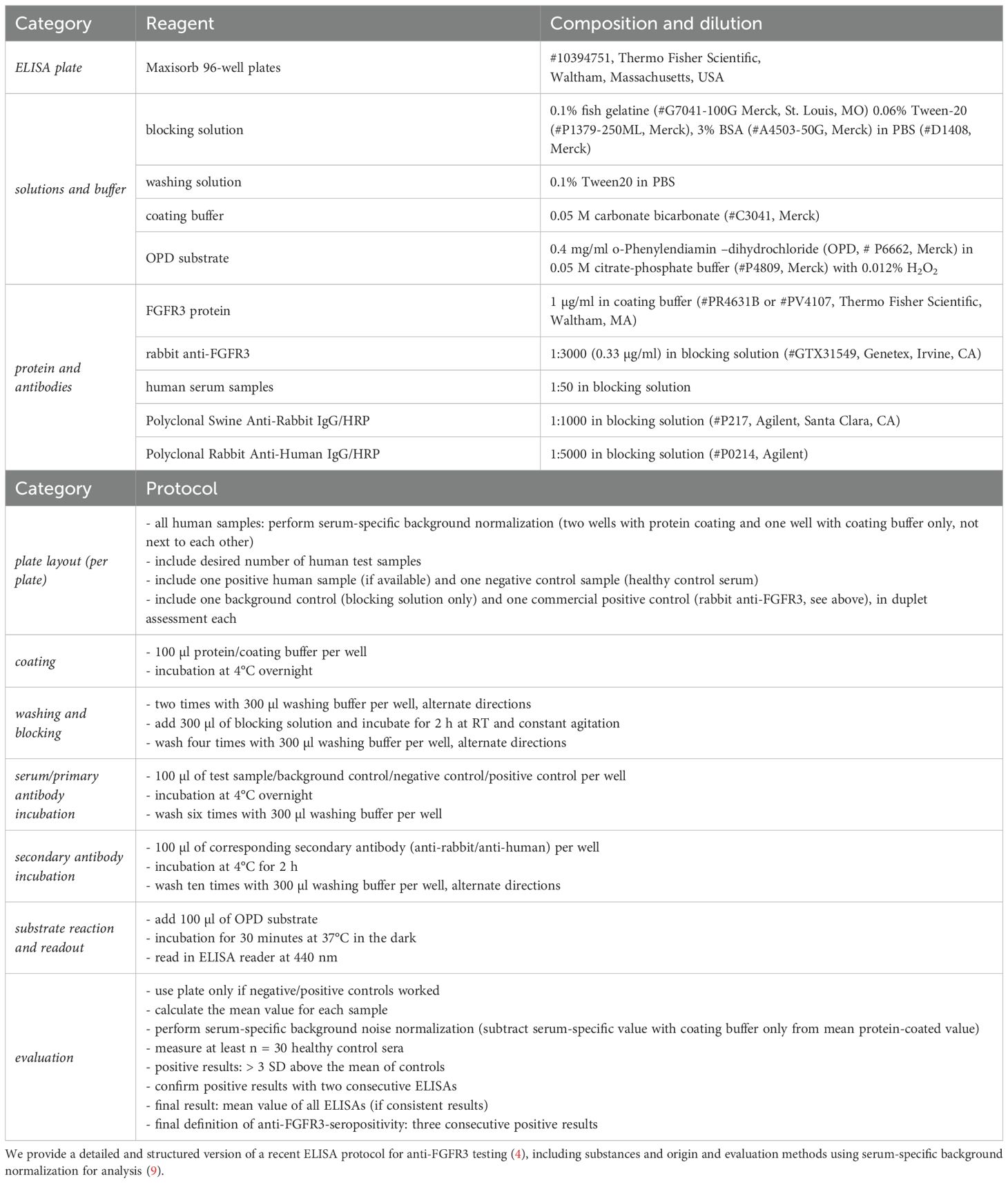
Table 1. Standardized ELISA protocol for anti-FGFR3 testing.
2.2 Patients
A schematic illustration of the study design including patient and control cohort sizes is shown in Figure 1. To screen for anti-FGFR3 antibodies at center 2, we included sera of 60 patients with SFN fulfilling the diagnostic criteria of “definite SFN” proposed bei Devigili et al. (12, 13), namely clinical symptoms of small fiber damage, exclusion of large fiber pathology by sural nerve conduction studies, and either abnormal results in quantitative sensory testing, or reduced intraepidermal nerve fiber density in skin biopsy at the ankle, or both. Further, we included sera of 17 patients with SNN who fulfilled the diagnostic criteria proposed by Camdessanché et al. (14) (n = 11 possible, n = 5 probable). As a control group, we assessed 68 patients with fibromyalgia syndrome (FMS) diagnosed according to the American College of Rheumatology (ACR) 1990 or ACR 2010 classification without further autoimmune disease, polyneuropathy, or pain of other origin as previously reported (15). Of these FMS patients, intraepidermal nerve fiber density was reduced in 33/68 (proximal) or 30/68 (distal) individuals (15).
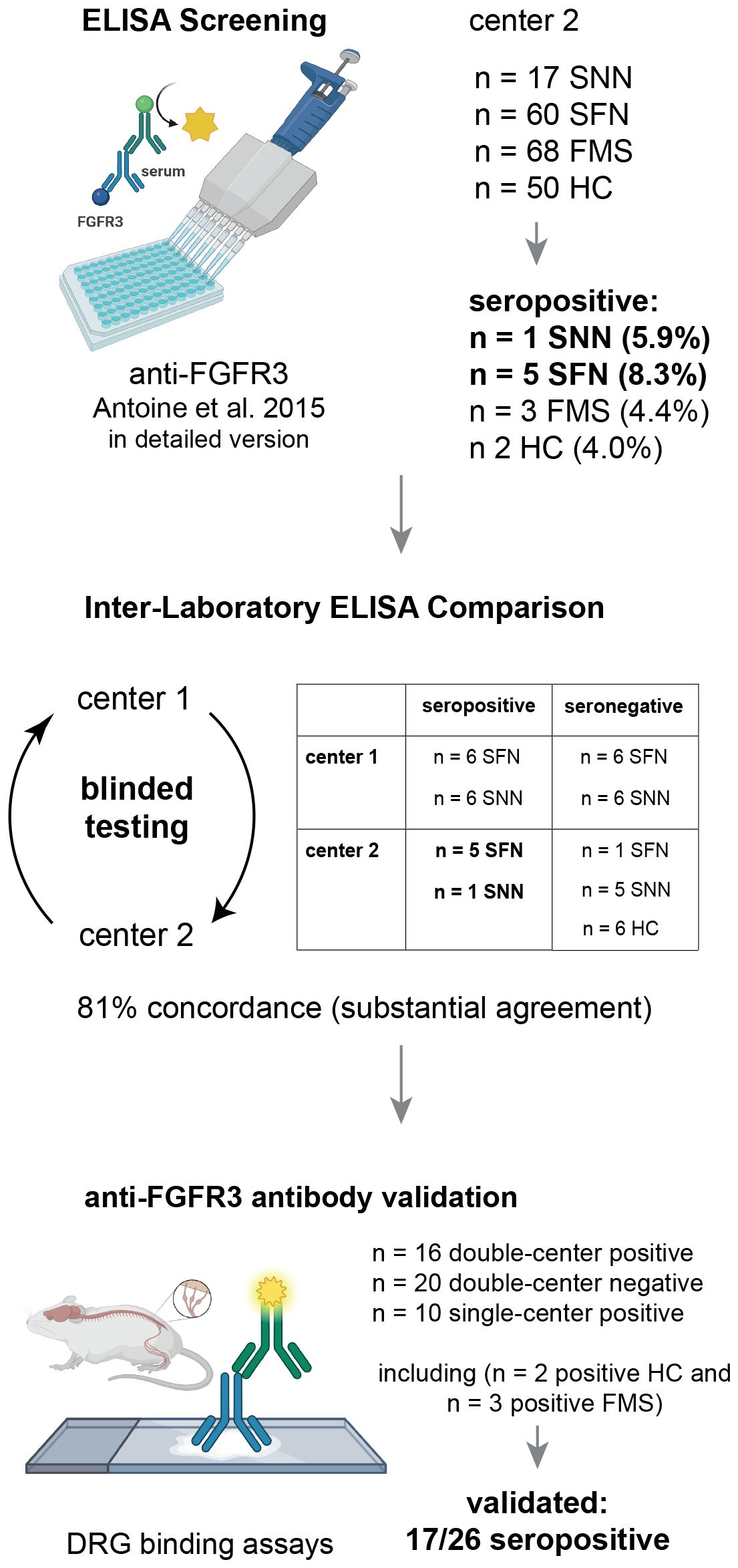
Figure 1. Schematic illustration of the study design. DRG, Dorsal Root Ganglion; FGFR3, Fibroblast Growth Factor Receptor 3; FMS, Fibromyalgia Syndrome; HC, healthy controls; pat., patients; SFN, Small Fiber Neuropathy; SNN, Sensory Neuronopathy.
For the inter-laboratory comparison study, we included all seropositive patient samples from center 2 detected by the screening assay (n = 6), and matched them with equal numbers of seronegative sera, healthy controls (n = 6), and samples from center 1 recruited in previous studies (4, 9). This resulted in a cohort of 36 patients with sensory neuropathies (18 with SFN and 18 with SNN), each fulfilling the respective diagnostic criteria (12, 14), of whom 18 had been considered seropositive and 18 had been considered seronegative. Demographic data of patients included in the inter-laboratory testing are shown in Table 2. The study was approved by the Ethics Committees of the Universities of Würzburg and St.-Étienne (reference number 220/20 and IRBN742021/CHUSTE, respectively). Patients and controls either gave informed consent or in case they were lost to follow-up, the Ethics Committee of the University of Würzburg or St.-Étienne approved the use of diagnostic serum samples and retrospective analysis of documented clinical data (reference 2021031501).
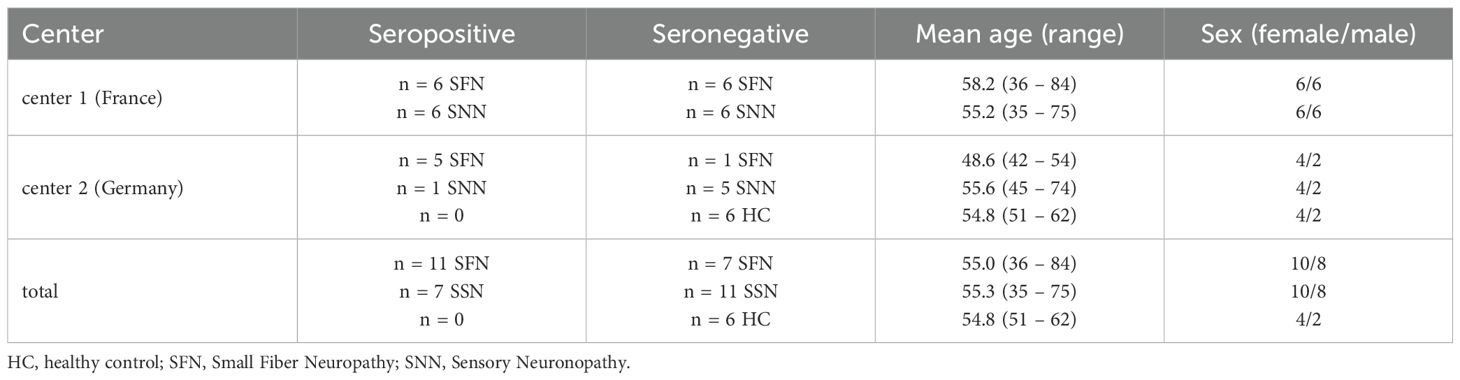
Table 2. Cohort and demographic data of patients included in the inter-laboratory validation study for an ELISA FGFR3 antibody test.
2.3 Inter-laboratory comparison of ELISA
Patient and control sera were sent to the other center on dry ice and stored at -20°C or -80°C until testing. ELISA using the protocol described in Table 1 was performed three times in independent assays with serum samples from the other center, and evaluated by blinded researchers. Sera which showed three consecutive values above 3 standard deviations (SD) of the means of controls were considered positive. The degree of positivity was assessed semi-quantitatively according to the mean optical density (OD) level (weakly positive if 3–5 SD and strongly positive if > 5 SD above the mean of controls).
2.4 Immunofluorescence staining
To confirm ELISA results for anti-FGFR3 antibodies, 41/42 sera included in the inter-laboratory validation study (n = 1 one serum missing due to insufficient volumes) as well as sera tested positive at center 2 during screening (n = 3 FMS and n = 2 healthy control, see Figure 1) were stained on 5-µm cryosections of rat DRG in center 2. After fixation for 10 minutes in acetone at -20°C and blocking with 4% normal goat serum, 4% fetal calf serum, and 0.3% Triton-X-100 in Phosphate-Buffered Saline for one hour at room temperature (RT), serum diluted 1:500 in blocking solution, rabbit Anti-FGFR3 (1:1000, # GTX31549, Genetex, Irvine, CA) and Alexa-647-labeled mouse anti-peripherin (1:1000, # sc-377093, Santa Cruz Biotechnology, Dallas, TX) were incubated overnight at 4°C. After washing, Cy3-labeled anti-human and Alexa-488-labeled anti-rabbit IgG secondary antibodies (1:300, Jackson Immuno Research, Westgrove, PA) were incubated for 1h at RT. Slides were mounted with Vecatshield Mounting Medium with DAPI 1.5 µg/ml (Vector Laboratories, Newark, CA) and assessed using a fluorescence microscope (Zeiss Axiovert 200m, Oberkochen, Germany). Cross-reaction was ruled out by performing single stainings with the respective serum/commercial antibody and by using healthy sera as controls. Staining clusters and colocalization of serum reactivity with commercial anti-FGFR3 and peripherin reactivity were assessed from photomicrographs semiquantitatively by two independent and blinded researchers. For display, identical image modification protocols were applied to photomicrographs of both patient and control sera using ImageJ (16). Further, we aimed to establish cell-based assay (CBA) using plasmids for full-length human FGFR3 and the extracellular domain of FGFR3 as previously described (4, 11), including double-staining with patient sera and commercial Anti-FGFR3 (Genetex), but results were not reliably reproducible for positive sera. Therefore, CBA was not applied as further confirmation assay in this study.
2.5 Statistics
The frequency of positive/negative results between testing via a self-established protocol and the detailed protocol (Table 1) was assessed using Fisher’s exact test. Inter-laboratory concordance of positive/negative results was calculated using Cohen’s Kappa coefficient. OD values between centers were compared using the Mann-Whitney test and Spearman correlation, or t-test depending on normal distribution. DRG binding rates were compared by Chi-square test, and ELISA sensitivity and specificity was calculated by Fisher’s exact test. Testing and display were performed using Prism V9.3.0 (GraphPad Software, San Diego, CA).
3 Results
3.1 Anti-FGFR3 testing results depend on ELISA protocol
First, we established an anti-FGFR3 ELISA at center 2 using previously published information only (4). The ELISA cut-off value from n = 50 healthy controls for a positive result was at an OD440 of 0.102 (0.020 + 3x standard deviation of 0.027). Using this self-established protocol, 1/17 (5.9%) patients with SNN and 1/60 (1.7%) patient with SFN were considered seropositive for anti-FGFR3 antibodies, but also 1/50 healthy controls (2%). We then repeated the assay using a very detailed version of the protocol provided by reference center 1, as shown in Table 1, and including three reproductions of the ELISA. The cut-off value was at an OD440 of 0.122 (0.039 + 3x standard deviation of 0.028). We still identified 1/17 seropositive patients with SNN, but now 5/60 patients with SFN (8.3%, p = 0.08 compared to first protocol), and also 2/50 healthy controls (4%, p = 0.04 compared to first protocol). The two positive controls were re-assessed, and one of them had developed malignancy (pulmonary adenocarcinoma) four years after recruitment, the other was tested positive for anti-cortactin-antibodies (17). Moreover, 3/68 (4.4%) of patients with FMS were tested seropositive (15). These three individuals had normal results in quantitative sensory testing, partially reduced intraepidermal nerve fiber density, but normal results in clinical examination, thus not fulfilling the SFN diagnostic criteria (12, 13). Thus, controls with autoimmune/malignant context and patients with FMS can also show positive FGFR3 ELISA results. Furthermore, this direct comparison of two protocol versions shows that small modifications can impact cut-off values and results.
3.2 Inter-laboratory validation of an anti-FGFR3 assay
To validate the anti-FGFR3 ELISA assay, we compared the results of 42 sera between two independent laboratories at center 1 and 2, using identical sera and protocols. Cut-off values for positive results were higher in center 1 compared to those in center 2 (OD440 0.371 vs 0.122), as well as mean ODs in general (median = 0.293 vs 0.076, p < 0.0001, Figure 2A). OD values correlated strongly between center 1 and 2 (r = 0.68, p < 0.0001, Figure 2B). In total, 34/42 samples (81%) were evaluated in concordance (13 positive, 21 negative, see Figure 2B). A Cohen’s kappa coefficient of κ = 0.61 indicated a substantial agreement (18) between both tests. Discordance occurred in one healthy control, four SFN and three SNN sera. Seropositive sera which were evaluated in concordance tended to exhibit higher ODs than sera that were rated as positive only in one center (median of 0.655 vs. 0.537 for those rated positive center 1 only, p = 0.350; median of 0.208 vs. 0.137 for those rated positive in center 2 only, p = 0.08), and 7/8 discordant sera were rated only as weakly positive. In conclusion, we could successfully validate the anti-FGFR3 assay in two independent laboratories with high levels of concordance. Still, cut-off values have to be determined separately for every lab, as mean ODs can vary among different settings.
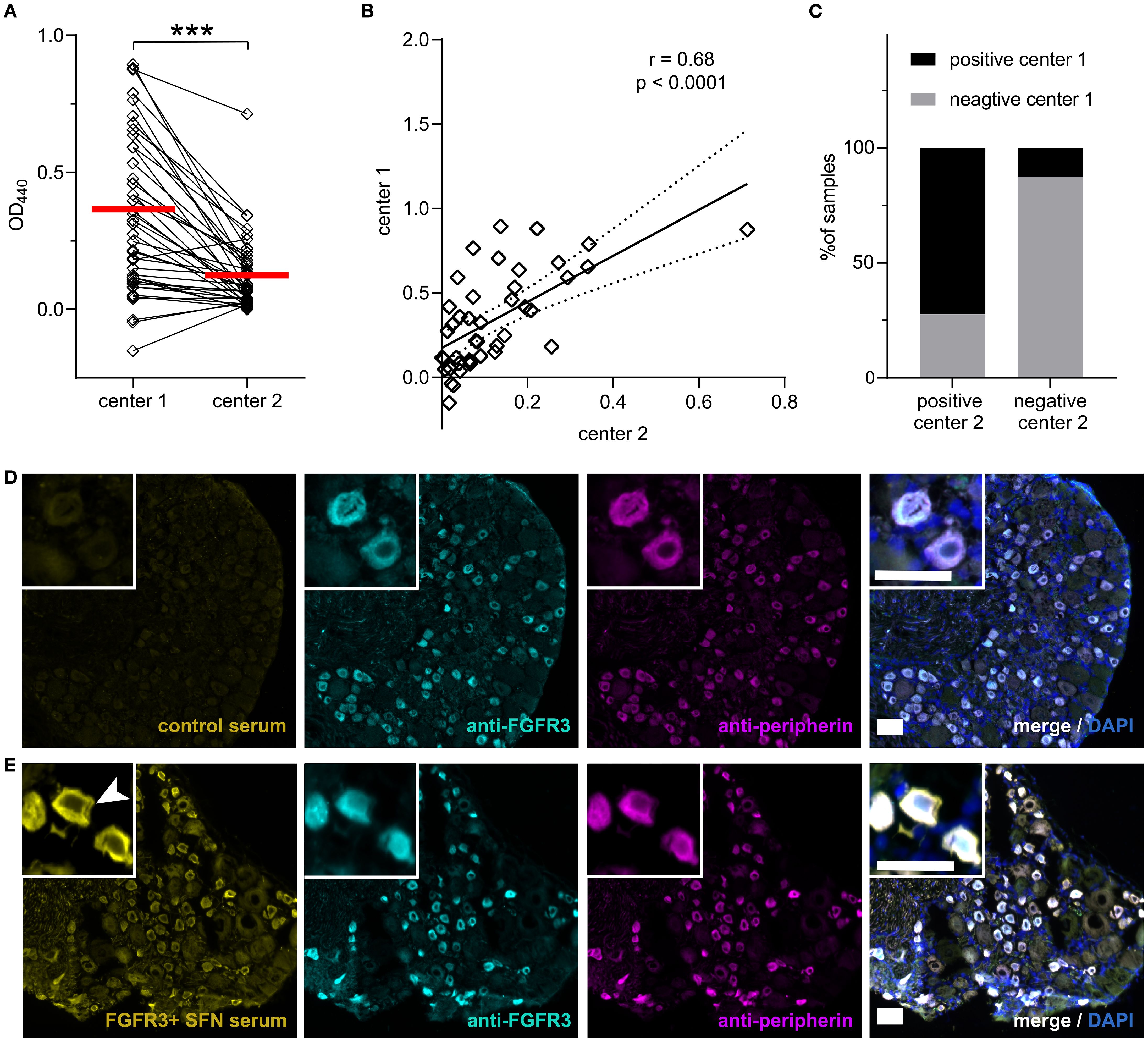
Figure 2. Inter-laboratory anti-FGFR3 ELISA validation and DRG binding. (A) Mean OD440 for the n = 42 sera included in the inter-laboratory comparison are higher in center 1 than center 2. Respective threshold values are marked in red. (B) Mean ODs correlate between the two centers. Regression line is shown as solid and 95% confidence bands as dashed lines. (C) Concordance of the overall positive/negative testing results for both centers is displayed in percentage with bar graphs. (D) No specific binding of a healthy control serum without FGFR3 antibodies to DRG sections (shown in yellow). Commercial anti-FGFR3 is shown in cyan and anti-peripherin in magenta, without serum colocalization. (E) IgG binding of an anti-FGFR3 positive serum of a patient with SFN to DRG sections. Arrowhead marks cytosol of small DRG neurons and membrane specifically bound by patient IgG. Colocalization with commercial anti-FGFR3 and anti-peripherin appears white. Scale bar = 50 µm. DRG, Dorsal Root Ganglion; FGFR3, Fibroblast Growth Factor Receptor 3; OD, optical density; SFN, Small Fiber Neuropathy. ***, p < 0.001.
3.3 Anti-FGFR3-positive sera show specific DRG binding patterns
To further validate ELISA results, we performed immunofluorescence binding assays on rat DRG sections with the sera included in the inter-laboratory validation study and FGFR3 seropositive sera from center 2 (including n = 2 positive healthy controls and n = 3 positive FMS sera). Inter-rater comparison revealed almost perfect agreement on semiquantitative assessment and classification of staining cluster regarding the stained cell type (43/46 sera, 93.5%, Cohen’s κ = 0.849). The staining pattern of DRG positive sera included staining of small, peripherin-positive DRG neurons (see Figure 2E). Triple immunofluorescence with a commercial anti-FGFR3 antibody revealed colocalized binding of serum, anti-FGFR3, and anti-peripherin on small DRG neurons, but no colocalization in anti-FGFR3 negative sera (see Figures 2D, E). While anti-peripherin and commercial anti-FGFR3 stained the cytosol, staining with patient serum also exhibited membrane localization (see Figure 2E, arrow).
11/16 (68.8%) ELISA anti-FGFR3-positive sera (confirmed by both centers) and in total 17/26 (65.4%) of single- or double-center positive sera showed binding to DRG small neurons, whereas only 1/20 (5%) sera rated as FGFR3-negative in both centers showed binding to small DRG neurons (p < 0.0001). Out of the 11 anti-FGFR3-positive sera binding small neurons, seven were rated as strongly positive in ELISA in both centers, two as strongly positive in one center (n = 1 center 1 and n = 1 center 2), and two as weakly positive in both centers. Patients with positive DRG neuron staining had higher OD values in the FGFR3 ELISA than patients without specific DRG binding (ELISA at center 1: mean 0.65 vs. 0.23, p < 0.0001; ELISA at center 2: median 0.208 vs. 0.06, p = 0.0011). In general, sera rated as anti-FGFR3-positive in only one center showed higher DRG binding rates than negative sera (3/8, 37.5% vs. 5%, p = 0.026), but a trend towards lower DRG binding-rates compared to double-confirmed positive sera (37.5% vs. 68.8%, p = 0.14). If only double positive (ELISA and DRG staining) were considered as a gold standard for anti-FGFR3 diagnostics, ELISA testing in general (including single-center positive and double-center positive results) showed a sensitivity of 93.3% and a specificity of 61.3%, with a false positive rate of 38.7% (p = 0.0004, Fisher’s exact test). Using DRG staining as a confirmation method, anti-FGFR3 antibodies were not confirmed in FMS sera (0/3 positive), and only in 1/2 healthy control sera tested positive for anti-FGFR3. All other healthy control sera (n = 7) were confirmed negative.
Thus, FGFR3 antibodies can be visualized on small DRG in most patients with high ODs in the anti-FGFR3 ELISA test. The combination of ELISA and binding assays to rat DRG could increase diagnostic specificity for anti-FGFR3 antibodies.
4 Discussion
Here, we validate a detailed protocol for an FGFR3 antibody test by ELISA, performed in two independent reference laboratories and introduce test confirmation by tissue-based assays.
This study demonstrates that ELISA is reliable for detecting anti-FGFR3 antibodies. Previous experimental and clinical studies often lacked detailed protocols for determining anti-FGFR3 antibodies, especially when tested in commercial laboratories (8, 19–22). Moreover, commercially available anti-FGFR3 antibody detection kits are costly, are not validated for diagnostic use, and do not include serum-specific background normalization (23, 24). In this study, we did therefore not include those assays for validation. Here, we present comprehensive instructions for a self-established and normalized ELISA, and only consider assays with consistent results from ≥ 3 repetitions as positive. These measures of normalization (9, 25) and repetition enhance both the sensitivity and specificity of the assay. However, our findings indicate that minor variations in the protocol can influence assay accuracy. Prior studies on inter-laboratory assessments of local, non-commercial ELISAs for antibody-mediated peripheral nerve diseases also highlight that different ELISA protocols can affect assay performance (26, 27). Therefore, the detailed protocol presented here could be used as a standard for future antibody testing if further validated in larger studies.
Still, some weakly positive samples yielded discrepant results between the two reference laboratories, indicating that values close to the threshold should be interpreted cautiously. Possible explanations for this include variations in probe handling, experimental conditions (e.g., laboratory temperature), reagent preparation, hardware-specific differences, or variations in human pipetting. Whether these discrepancies represent false positives or false negatives remains unclear, as no independent gold standard is available for anti-FGFR3 diagnostic assessment. To prevent false positive results, future ELISA protocols could include disease controls with an autoimmune context for the calculation of cut-off values and use higher-fold standard deviations for the cut-off due to variability of control values. Consequently, a positive anti-FGFR3 result should always be interpreted in a clinical context, and treatment decisions should not be solely based on antibody test results. Further, independent assays should be developed to increase diagnostic specificity.
Binding to DRG sections can help identify patients with autoantibodies and correlate with clinical symptoms, as demonstrated in previous studies involving cohorts of patients with Guillain-Barré syndrome and FMS (15, 28, 29). FGFR3 is expressed in the cytosol and the nucleus of DRG neurons, and SNN patients with high-titer FGFR3 antibodies bind to the cytoplasm when tested on cultivated rat DRG neurons (4). Here, patients with SFN and SNN strongly positive in ELISA bound to small DRG neurons in cryosections, colocalizing with a commercial anti-FGFR3 antibody, and sera binding to DRG sections showed higher ELISA values than negative sera. Samples that show low OD values in ELISA and cannot be validated by DRG binding assays might lack specificity. Tissue-based immunofluorescence assays are straightforward to perform and serve as a diagnostic standard in autoantibody-mediated neurological diseases (30). Therefore, we recommend using immunofluorescence staining on rat DRG sections as a viable method for further validating anti-FGFR3 results, as it might increase diagnostic specificity.
Although anti-FGFR3 antibodies have been recognized for a decade (4), their specificity, pathogenic role, and impact on treatment decisions in sensory neuropathies remain inconclusive. Initially described in neuropathies predominantly affecting DRG sensory neurons such as SNN and SFN (4, 5), anti-FGFR3 antibodies have now also been detected in chronic inflammatory demyelinating polyradiculoneuropathy, motor neuropathy, trigeminal neuropathy, FMS and patients with corneal neuropathic pain when using commercial anti-FGFR3 testing (8, 15, 21, 31, 32). 48% of the FMS control cohort in this study also showed reduced intraepidermal nerve fiber density as a sign of small fiber pathology, which can occur in up to 50% of patients with FMS (33–35). Still, the FGFR3 seropositive FMS patients did not fulfill diagnostic criteria for SFN, and anti-FGFR3 positive results were not confirmed using tissue-based assays. Further, we detected two control sera with a positive anti-FGFR3 ELISA result, with one of them being confirmed using tissue-based assays. Upon further investigation, these two individuals developed autoimmunity or malignancy after recruitment for this study. These findings indicate that ELISA-based anti-FGFR3 are not specific for sensory neuropathies and could occur in other conditions, but most certainly could also be due to false-positive ELISA results when no confirmation method such as tissue-based assay is applied. Thus, confirmation tests using DRG binding assays could enhance specificity also in other conditions than sensory neuropathies.
Although FGFRs play a crucial role in neuronal development, functioning, and survival (6), and different functional anti-FGFR3 binding epitopes are related to clinical subtypes of SNN (36), no conclusions can be made on a potential pathogenicity of antibodies against FGFR3 in sensory neuropathies. With our current knowledge, anti-FGFR3 antibodies could only be considered a possible marker of an underlying autoimmune context, similar to anti-argonaute antibodies in SNN (37–39). Similarly, the significance of further antibodies in SFN, such as anti-PlexinD1 and anti-trisulfated heparan disaccharide (TS-HDS) (20, 40), is still under investigation, and future studies could benefit from methodological standardization similar to this study before concluding their significance.
Immunomodulatory treatment in patients with anti-FGFR3 and anti-TS-HDS antibodies has not shown any beneficial effect for patients with SFN in a pilot study, with similar results for anti-FGFR3 in retrospective analyses (5, 22, 41). Still, antibody detection methods were not always specified, with a possible impact on the study results.
Here, we provide a standardized and validated protocol for anti-FGFR3 antibody detection, and offer a method for antibody confirmation, thus paving the way for more accurate testing and multicenter investigations to understand the clinical relevance of anti-FGFR3 antibodies in sensory neuropathies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committees of the Universities of Würzburg (reference number 220/20) and St.-Étienne (reference number IRBN742021/CHUSTE). The studies were conducted in accordance with the local legislation and institutional requirements. Patients and controls either gave informed consent or in case they were lost to follow-up, the Ethics Committee of the University of Würzburg or St.-Étienne approved the use of diagnostic serum samples and retrospective analysis of documented clinical data (reference 2021031501). The animal study was not separately reviewed, as according to German law, a formal animal experiment application is not required if tissue is collected from animals killed for other purposes (experiments previously approved by Bavarian State authorities, license number: 55.2.2-2532-2-593-17).
Author contributions
LA: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CM: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Validation, Writing – review & editing. LR: Formal Analysis, Investigation, Methodology, Validation, Writing – review & editing. LK: Investigation, Resources, Writing – review & editing. NÜ: Investigation, Resources, Writing – review & editing. FL: Investigation, Methodology, Writing – review & editing. AB: Investigation, Writing – review & editing. SS: Investigation, Writing – review & editing. CS: Resources, Writing – review & editing. YT: Investigation, Methodology, Resources, Writing – review & editing. J-CA: Methodology, Resources, Supervision, Writing – review & editing. J-PC: Methodology, Resources, Supervision, Writing – review & editing. KD: Project administration, Resources, Supervision, Writing – review & editing.
Funding
The authors declare financial support was received for the research, and/or publication of this article. LA was supported by the Interdisciplinary Center of Clinical Research (IZKF) of the Faculty of Medicine, University of Würzburg (#ZZ-32). KD, CS, and NÜ received funding from the German Research Foundation for the Clinical Research Unit ResolvePain. NÜ received funding from the German Research Foundation (UE171/3-1). Parts of the study were funded by the Association Française contre les Myopathies (AFM-MyoNeurALP 2), the GROUPAMA Foundation, the Centre Hospitalier Universitaire of Saint-Étienne, the BETPSY project (reference ANR-18-RHUS-0012) and the Fondation pour la Recherche Médicale (FRM, DQ20170336751). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
We thank Barbara Reuter for her excellent technical assistance (center 2) and Karine Ferraud for her assistance in clinical data management (center 1). J-PC and J-CA are members of the European Reference Network for Rare Neuromuscular Diseases, 75013 Paris, France.
Conflict of interest
CPM submitted a patent application for the application of AGO antibodies as biomarkers for autoimmune neurologic diseases. JPC holds a patent on anti-FGFR3 antibodies (EP2880449B1, US10539577B2) and submitted a patent application for AGO antibodies as biomarkers for autoimmune neurologic diseases. JCA holds a patent on anti-FGFR3 antibodies (EP2880449B1, US10539577B2) and has submitted a patent application for the application of AGO antibodies as biomarkers for autoimmune neurologic diseases.
The remaining author(s) declare(s) that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Antoine JC. Sensory neuronopathies, diagnostic criteria and causes. Curr Opin Neurol October. (2022) 35:553–61. doi: 10.1097/WCO.0000000000001105
2. Sghirlanzoni A, Pareyson D, and Lauria G. Sensory neuron diseases. Lancet Neurol June. (2005) 4:349–61. doi: 10.1016/S1474-4422(05)70096-X
3. Morelli L, Serra L, Ricciardiello F, Gligora I, Donadio V, Caprini M, et al. The role of antibodies in small fiber neuropathy: a review of currently available evidence. Rev Neurosci. (2024) 35:877–93. doi: 10.1515/revneuro-2024-0027
4. Antoine JC, Boutahar N, Lassabliere F, Reynaud E, Ferraud K, Rogemond V, et al. Antifibroblast growth factor receptor 3 antibodies identify a subgroup of patients with sensory neuropathy. J Neurol Neurosurg Psychiatry. (2015) 86:1347–55. doi: 10.1136/jnnp-2014-309730
5. Tholance Y, Moritz CP, Rosier C, Ferraud K, Lassabliere F, Reynaud-Federspiel E, et al. Clinical characterisation of sensory neuropathy with anti-FGFR3 autoantibodies. J Neurol Neurosurg Psychiatry. (2020) 91:49–57. doi: 10.1136/jnnp-2019-321849
6. Latko M, Czyrek A, Porębska N, Kucińska M, Otlewski J, Zakrzewska M, et al. Cross-talk between fibroblast growth factor receptors and other cell surface proteins. Cells. (2019) 8:455. doi: 10.3390/cells8050455
7. Jungnickel J, Gransalke K, Timmer M, and Grothe C. Fibroblast growth factor receptor 3 signaling regulates injury-related effects in the peripheral nervous system. Mol Cell Neurosci. (2004) 25:21–9. doi: 10.1016/j.mcn.2003.09.014
8. Kovvuru S, Cardenas YC, Huttner A, Nowak RJ, and Roy B. Clinical characteristics of fibroblast growth factor receptor 3 antibody-related polyneuropathy: a retrospective study. Eur J Neurol. (2020) 27:1310–8. doi: 10.1111/ene.14180
9. Moritz CP, Tholance Y, Lassabliere F, Camdessanche JP, and Antoine JC. Reducing the risk of misdiagnosis of indirect ELISA by normalizing serum-specific background noise: The example of detecting anti-FGFR3 autoantibodies. J Immunol Methods March. (2019) 466:52–6. doi: 10.1016/j.jim.2019.01.004
10. Doppler K, Appeltshauser L, Kramer HH, Ng JK, Meinl E, Villmann C, et al. Contactin-1 and neurofascin-155/-186 are not targets of auto-antibodies in multifocal motor neuropathy. PloS One. (2015) 10:e013:4274. doi: 10.1371/journal.pone.0134274
11. Doppler K, Appeltshauser L, Wilhelmi K, Villmann C, Dib-Hajj SD, Waxman SG, et al. Destruction of paranodal architecture in inflammatory neuropathy with anti-contactin-1 autoantibodies. J Neurol Neurosurg Psychiatry. (2015) 86:720–8. doi: 10.1136/jnnp-2014-309916
12. Devigili G, Tugnoli V, Penza P, Camozzi F, Lombardi R, Melli G, et al. The diagnostic criteria for small fibre neuropathy: from symptoms to neuropathology. Brain. (2008) 131:1912–25. doi: 10.1093/brain/awn093
13. Devigili G, Rinaldo S, Lombardi R, Cazzato D, Marchi M, and Salvi E. Diagnostic criteria for small fibre neuropathy in clinical practice and research. Brain. (2019) 142:3728–36. doi: 10.1093/brain/awz333
14. Camdessanché JP, Jousserand G, Ferraud K, Vial C, Petiot P, Honnorat J, et al. pattern and diagnostic criteria of sensory neuronopathy: a case-control study. The Brain. (2009) 132:1723–33. doi: 10.1093/brain/awp136
15. Seefried S, Barcic A, Grijalva Yepez MF, Reinhardt L, Appeltshauser L, Doppler K, et al. Autoantibodies in patients with fibromyalgia syndrome. Pain. (2025) 166:1922–33. doi: 10.1097/j.pain.0000000000003535
16. Abramoff M, Magalhães P, and Ram SJ. Image processing with imageJ. Biophotonics Int. (2003) 11:36–42.
17. Doppler K, Hemprich A, Haarmann A, Brecht I, Franke M, and Kröger S. Autoantibodies to cortactin and agrin in sera of patients with myasthenia gravis. J Neuroimmunol. (2021) 356:577588. doi: 10.1016/j.jneuroim.2021.577588
18. Landis GG Jr Fau - Koch and Koch GG. The measurement of observer agreement for categorical data. Biometrics. March. (1977) 33:159–74.
19. Zeidman LA and Kubicki K. Clinical features and treatment response in immune-mediated small fiber neuropathy with trisulfated heparin disaccharide or fibroblast growth factor receptor 3 antibodies. J Clin Neuromuscul Dis June. (2021) 22:192–9. doi: 10.1097/CND.0000000000000355
20. Trevino JA and Novak P. TS-HDS and FGFR3 antibodies in small fiber neuropathy and Dysautonomia. Muscle Nerve. July. (2021) 64:70–6. doi: 10.1002/mus.27245
21. Samara V, Sampson J, and Muppidi S. FGFR3 antibodies in neuropathy: what to do with them? J clin neuromuscul dis. 2018/08/21 Aufl. September. (2018) 20:35–40. doi: 10.1097/CND.0000000000000221
22. Gibbons CH, Rajan S, Senechal K, Hendry E, McCallister B, and Levine TD. A double-blind placebo-controlled pilot study of immunoglobulin for small fiber neuropathy associated with TS-HDS and FGFR-3 autoantibodies. Muscle Nerve. (2023) 67:363–70. doi: 10.1002/mus.27745
23. CellTrend GmbH. EIA for Quantitative Determination of anti-FGFR3-Antibodies (2025). Available online at: https://www.celltrend.de/wp-content/uploads/2020/09/FGFR3-Ab-Produktinfo-engl-2020-09.pdf (Accessed February 17, 2025).
24. Eagle Biosciences. Anti-FGFR-3 autoantibodies ELISA (2025). Available online at: https://eaglebio.com/product/anti-fgfr-3-autoantibodies-elisa/ (Accessed February 17, 2025)
25. Haberland A, Müller J, Wallukat G, and Wenzel K. Antigen-free control wells in an ELISA set-up for the determination of autoantibodies against G protein-coupled receptors-a requisite for correct data evaluation. Anal Bioanal Chem August. (2018) 410:5101–5. doi: 10.1007/s00216-018-1172-x
26. Willison HJ, Veitch J, Swan AV, Baumann N, Comi G, Gregson NA, et al. Inter-laboratory validation of an ELISA for the determination of serum anti-ganglioside antibodies. Eur J Neurol. (1999) 6:71–7. doi: 10.1046/j.1468-1331.1999.610071.x
27. Lleixà C, Titulaer M, Rohrbacher S, Mgbachi V, Halstead S, and Fehmi J. Inter-laboratory validation of nodal/paranodal antibody testing. J Peripher Nerv Syst JPNS. (2025) 30:e70000. doi: 10.1111/jns.70000
28. Lleixà C, Martín-Aguilar L, Pascual-Goñi E, Franco T, Caballero M, and de Luna N. Autoantibody screening in Guillain-Barré syndrome. . J Neuroinflamm. (2021) 18:251. doi: 10.1186/s12974-021-02301-0
29. Krock E, Morado-Urbina CE, Menezes J, Hunt MA, Sandström A, and Kadetoff D. Fibromyalgia patients with elevated levels of anti-satellite glia cell immunoglobulin G antibodies present with more severe symptoms. Pain. 1. (2023) 164:1828–40. doi: 10.1097/j.pain.0000000000002881
30. Prüss H. Autoantibodies in neurological disease. Nat Rev Immunol Dezember. (2021) 21:798–813. doi: 10.1038/s41577-021-00543-w
31. Nagarajan E, Kang SA, Holmes C, and Govindarajan R. Clinical features with anti fibroblast growth factor receptor 3 (FGFR3) antibody-related polyneuropathy: a retrospective study. BMC Neurol. (2021) 21:74. doi: 10.1186/s12883-021-02090-2
32. Bayraktutar BN, Atocha V, Farhad K, Soto O, and Hamrah P. Autoantibodies against trisulfated heparin disaccharide and fibroblast growth factor receptor-3 may play a role in the pathogenesis of neuropathic corneal pain. Cornea. July. (2023) 42:821–8. doi: 10.1097/ICO.0000000000003142
33. Evdokimov D, Frank J, Klitsch A, Unterecker S, Warrings B, Serra J, et al. Reduction of skin innervation is associated with a severe fibromyalgia phenotype. Ann Neurol. (2019) 86:504–16. doi: 10.1002/ana.25565
34. Farhad K. Current diagnosis and treatment of painful small fiber neuropathy. Curr Neurol Neurosci Rep. (2019) 19:103. doi: 10.1007/s11910-019-1020-1
35. Marshall A, Rapteas L, Burgess J, Riley D, Anson M, Matsumoto K, et al. Small fibre pathology, small fibre symptoms and pain in fibromyalgia syndrome. Sci Rep. (2024) 14:3947. doi: 10.1038/s41598-024-54365-6
36. Tholance Y, Antoine JC, Mohr L, Jung M, Reynaud-Federspiel E, and Ferraud K. Anti-FGFR3 antibody epitopes are functional sites and correlate with the neuropathy pattern. J Neuroimmunol. (2021) 361:577757. doi: 10.1016/j.jneuroim.2021.577757
37. Do LD, Moritz CP, Muñiz-Castrillo S, Pinto AL, Tholance Y, Brugiere S, et al. Argonaute autoantibodies as biomarkers in autoimmune neurologic diseases. Neurol Neuroimmunol Neuroinflamm. (2021) 8:e1032. doi: 10.1212/NXI.0000000000001032
38. Moritz CP, Tholance Y, Vallayer PB, Do LD, Muñiz-Castrillo S, Rogemond V, et al. Anti-AGO1 antibodies identify a subset of autoimmune sensory neuronopathy. Neurol Neuroimmunol Neuroinflamm. (2023) 10:e200105. doi: 10.1212/NXI.0000000000200105
39. Antoine JC. Antibodies in immune-mediated peripheral neuropathies. Where are we in 2024. Rev Neurol (Paris). (2024) 180:876–87. doi: 10.1016/j.neurol.2024.09.002
40. Fujii T, Yamasaki R, Iinuma K, Tsuchimoto D, Hayashi Y, Saitoh BY, et al. A novel autoantibody against plexin D1 in patients with neuropathic pain. Ann Neurol. (2018) 84:208–24. doi: 10.1002/ana.25279
Keywords: fibroblast growth factor receptor 3, ELISA, autoantibodies, sensory neuropathy, sensory neuronopathy, small fiber neuropathy, dorsal root ganglion
Citation: Appeltshauser L, Moritz CP, Reinhardt L, Kreß L, Üçeyler N, Lassablière F, Barcic A, Seefried S, Sommer C, Tholance Y, Antoine J-C, Camdessanché J-P and Doppler K (2025) Inter-laboratory comparison of a serum fibroblast growth factor receptor 3 (FGFR3) antibody test in sensory neuropathies. Front. Immunol. 16:1604456. doi: 10.3389/fimmu.2025.1604456
Received: 01 April 2025; Accepted: 23 September 2025;
Published: 10 October 2025.
Edited by:
Jan Stępniak, Medical University of Lodz, PolandReviewed by:
Luana Morelli, IRCCS Institute of Neurological Sciences of Bologna (ISNB), ItalyJerome Devaux, Délégation Languedoc Roussillon (CNRS), France
Copyright © 2025 Appeltshauser, Moritz, Reinhardt, Kreß, Üçeyler, Lassablière, Barcic, Seefried, Sommer, Tholance, Antoine, Camdessanché and Doppler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luise Appeltshauser, QXBwZWx0c2hhdV9MQHVrdy5kZQ==
†These authors share first authorship