 Cheng Tong
Cheng Tong Yue Wu
Yue Wu Renzhao Wu
Renzhao Wu- 1First People’s Hospital of Linping District, Hangzhou, China
- 2The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, China
- 3The Key Laboratory of Research and Development of Chinese Medicine of Zhejiang Province, Zhejiang Academy of Traditional Chinese Medicine, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, China
The treatment of tumors remains one of the most challenging issues in modern medicine. For a long time, surgical intervention and radiochemotherapy were the primary methods employed to combat tumors; however, the therapeutic outcomes often fell short of expectations. Immunotherapy offers a promising alternative by enhancing the patient’s immune system’s ability to recognize and eliminate tumor cells while minimizing damage to normal cells and tissues. This advancement has brought new hope for cancer patients. In recent years, significant progress has been made in tumor immunotherapy with immune checkpoint inhibitors (ICIs), particularly Programmed Cell Death Protein-1 (PD-1)/Programmed Cell Death-Ligand 1 (PD-L1) inhibitors. An increasing number of researchers have discovered that combination therapy involving PD-1/PD-L1 inhibitors alongside chemotherapeutic agents or other types of ICIs yields more pronounced effects compared to monotherapy. Nevertheless, there remains a considerable risk of developing resistance and experiencing various adverse events. Traditional Chinese medicine (TCM) is frequently utilized as an adjunctive treatment for tumors due to its potential to enhance overall immune function in patients. Recent studies indicate that combining TCM with PD-1/PD-L1 inhibitors can significantly improve median survival times for patients, undoubtedly providing new directions for cancer treatment, however, there remains a lack of sufficient large-sample prospective controlled studies to provide evidence supporting the combined treatment of traditional Chinese medicine and immune checkpoint inhibitors for tumors. This study summarizes recent research on the combined use of PD-1/PD-L1 inhibitors with chemotherapeutic drugs, other ICIs, or TCM in cancer therapy. The aim is to explore their synergistic mechanisms and clinical application value while drawing greater attention from scholars to the significant value of traditional Chinese medicine in the combined treatment strategies for tumors. Additionally, this research provides insights into future prospects for anti-tumor research within TCM.
Introduction
Currently, cancer remains one of the most challenging diseases to cure. The treatment of cancer has undergone a lengthy evolution; prior to the 21st century, surgical resection was the predominant method employed for cancer treatment. However, since most cancers are already advanced or have metastasized to adjacent tissues and organs by the time they are diagnosed, surgery often cannot achieve complete eradication. Consequently, targeted therapeutic approaches such as radiotherapy and chemotherapy have been developed (1). Chemotherapy agents can directly inhibit the DNA synthesis of tumor cells, thereby interfering with their growth and differentiation. Radiotherapy employs high doses of high-energy radiation to damage the DNA of tumor cells, achieving a similar effect. It is worth noting that for an extended period, even up to the present day, radiochemotherapy has significantly enhanced the survival rates of certain cancer patients due to its pronounced antitumor effects, establishing it as one of the first-line treatment modalities for cancer. However, the cytotoxic effects associated with radiochemotherapy also impact normal cells, often disrupting the homeostasis of the patient’s immune system and leading to a series of severe complications. Consequently, further exploration into safe and effective therapeutic approaches has become a crucial direction in anticancer research.
Research indicates that during tumor development, T cells undergo exhaustion. The T cells that should be activated exhibit a high expression of certain surface molecules that inhibit their activation. These include Programmed Cell Death Protein-1 (PD-1), Cytotoxic T-Lymphocyte Antigen 4 (CTLA-4), and Lymphocyte Activation Gene-3 (LAG-3). Collectively, these molecules are referred to as immune checkpoints (2). Research has shown that immune checkpoints play a crucial role in the regulation of immune homeostasis and are highly expressed on the surfaces of tumor cells as well as various immune cell types (3). The binding of immune checkpoints to their ligands can inhibit certain signaling pathways, serving the purpose of maintaining immune tolerance. However, tumor cells often exploit these mechanisms to evade immune surveillance, a phenomenon commonly referred to as “immune evasion” (4). In this research context, the investigators discovered that immune checkpoint inhibitors (ICIs) can prevent the binding of immune checkpoints to their ligands or interfere with their functional activities post-binding, thereby achieving anti-tumor effects. This led to the introduction of the concept of immunotherapy. Immunotherapy enhances the body’s ability to recognize tumor cells and utilize the immune system to eliminate them. It has garnered widespread attention and is gradually becoming a primary approach in anti-tumor treatment (5) (6). The PD-1/PD-L1 inhibitors, as a class of ICIs, play a significant role in restoring T cell-mediated anti-tumor immune responses. They have demonstrated remarkable efficacy in the treatment of various cancer types, including melanoma, lung cancer, and gastrointestinal tumors (7, 8). However, clinical evidence indicates that the use of PD-1/PD-L1 inhibitors as monotherapy for tumor treatment is associated with notable limitations. These include a low objective response rate, an increased likelihood of secondary resistance development, and potential risks of adverse toxic effects (9–11). This review systematically examines the critical clinical challenges inherent in PD-1/PD-L1 inhibitor monotherapy and highlights recent advances in combination therapies involving chemotherapy regimens, other ICIs, and active components of traditional Chinese medicine (TCM). The aim is to clarify the synergistic mechanisms underlying enhanced efficacy and reduced toxicity across different combination strategies, as well as their translational significance in clinical practice.
This review conducted a systematic search in PubMed, China National Knowledge Infrastructure (CNKI), and Wanfang Database. The search strategies employed included: “(PD-1/PD-L1 inhibitors) AND (combination)”, “(Bevacizumab) AND (combination)”, “(Nivolumab) AND (combination)”, “(Atezolizumab) AND (combination)”, “(PD-1/PD-L1 inhibitors) AND (traditional Chinese medicine)”, “(PD-1/PD-L1 inhibitors) AND (decoction)”, “(PD-1/PD-L1 inhibitors) AND (injection solution)”, “(PD-1/PD-L1 inhibitors) AND (compound preparations)”, “(ICIs) AND (chemotherapy)” etc. The keywords used included: tumor, cancer, combination therapy, traditional Chinese medicine, ICIs, among others. Studies published from 2015 to 2025 that met the criteria were retrieved.
Interactions between PD-1 and PD-L1, and their inhibitors
PD-1 is an immune checkpoint receptor that is expressed on the surface of various immune cells, including macrophages, dendritic cells, B lymphocytes, and tumor-specific activated T cells (12, 13). PD-L1 is one of the natural receptors for PD-1, primarily expressed on antigen-presenting cells and tumor cells (14). When researchers explore the occurrence and development of tumors, it is essential to address the concept of “T cell exhaustion.” Under sustained antigenic stimulation, activated specific CD8+ T cells gradually lose their potent effector functions. This process leads to the expression of various inhibitory receptors, such as PD-1, resulting in the inability of the immune system to eliminate antigens effectively (15).
Recent studies have demonstrated that the primary mechanism of anti-tumor activity associated with PD-1/PD-L1 inhibitors involves PD-1+ TCF-1+ stem-like CD8+ T cells, specifically the exhausted CD8+ T cells (Tpex). During tumor progression, blocking PD-1 pathway leads to providing proliferative burst of (transitory) effector-like CD8 T cells from stem-like CD8 T cells, which subsequently differentiate into effector-like CD8+ T cells. These effector-like cells engage in the tumor immune microenvironment, exhibiting characteristics typical of effectors and migrating to key sites of tumor development. Ultimately, thereby exerting control over tumor progression (15–17).
Furthermore, research has revealed that the activation of PD-L1 leads to the phosphorylation of PD-1 by protein tyrosine kinases. Subsequently, Src homology region 2 domain-containing phosphatase (SHP-2) is recruited, resulting in the dephosphorylation of T cell receptors (TCR). This process significantly inhibits TCR signaling pathways (18). The PD-1 receptor can transmit inhibitory signals through the immunoreceptor tyrosine-based inhibition motif and the immunoreceptor tyrosine-based activation motif, thereby inhibiting the RAS/MEK/ERK and PI3K/AKT signaling pathways. This results in a reduction of T cell proliferation and cytokine secretion (19).
The PD-1 and PD-L1 inhibitors can bind to PD-1 and PD-L1, respectively, thereby inhibiting their interaction (Figure 1). When PD-1/PD-L1 inhibitors exert their effects, they lead to a failure in the phosphorylation of PD-1 while suppressing the dephosphorylation of TCR. As a result, activation signals generated by antigen-presenting cells can be effectively transmitted downstream through TCR pathways. This stimulation promotes T cell proliferation and differentiation, thereby enhancing the immune system’s surveillance capabilities and facilitating the destruction of tumor cells (20).
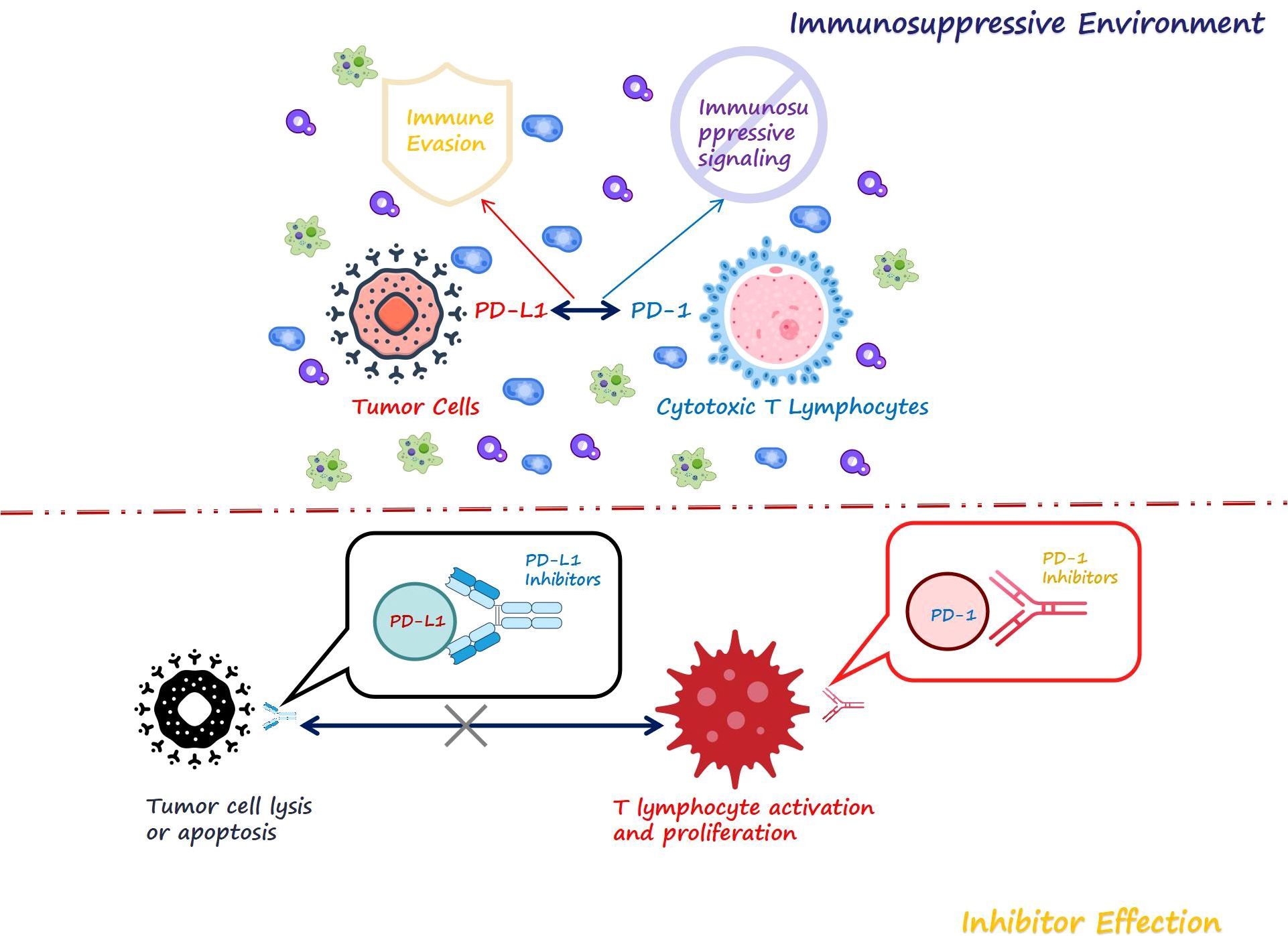
Figure 1. The immune microenvironment and the mechanism of ICIs.
Challenges of monotherapy with PD-1/PD-L1 inhibitors
Despite the fact that currently approved PD-1/PD-L1 inhibitors have benefited some patients and significantly improved survival rates, 50%-60% of patients still exhibit low responsiveness or no response at all (21). Furthermore, numerous studies have reported on the resistance to PD-1/PD-L1 inhibitors as well as immune-related adverse events (irAEs) (Table 1). In immunotherapy, many patients, despite meeting the treatment criteria, exhibit an inherent lack of responsiveness to the drugs due to their tumor cells’ primary resistance. For instance, a deficiency in immunogenicity is one of the potential reasons for the development of resistance during monotherapy (22). A study on metastatic urothelial carcinoma has demonstrated that transforming growth factor β (TGF-β) can inhibit T lymphocytes, particularly CD8+ T lymphocytes, thereby affecting the antitumor efficacy of PD-L1 inhibitors (23). Additionally, research has indicated that the intensity of IFNγ signaling within tumor cells is positively correlated with their responsiveness to PD-1 inhibitors. Different phenotypes of tumor cells exhibit varying sensitivities to PD-1 inhibitors, which may be related to the strength of IFNγ signaling. In other words, low levels of IFNγ signaling could be one of the contributing factors leading to primary resistance (24). Tumor cells can secrete certain inhibitors, such as VEGF or IL-10, which lead to a reduction in the number of normal mature dendritic cells. As a result, effector T cells are not effectively activated during the antigen presentation process (25). Some patients initially exhibit favorable therapeutic responses; however, over the course of treatment, they gradually develop tolerance to the medication, resulting in tumor progression and acquired resistance. The mechanism of acquired drug resistance is highly complex and may involve multiple factors, including the tumor immune microenvironment (TIME), genetic mutations, and alterations in the gut microbiota. Tumor cells, together with various immune cells such as T cells, regulatory T cells (Tregs), myeloid-derived suppressor cells (MDSCs), and stromal cells, collaboratively establish an immunosuppressive TIME, which protects tumor cells from immune-mediated clearance (26, 27). Proteomics and RNA analysis have revealed that collagen in tumors exerts its effects through the LAIR1 receptor, leading to the exhaustion and functional impairment of CD8+ T cells. This phenomenon results in patient resistance to PD-1 inhibitors. However, reducing the deposition of collagen in tumor cells can restore this resistance. Consequently, collagen and LAIR1 are considered potential biomarkers for predicting the efficacy of PD-1 inhibitors (28). In non-small cell lung cancer (NSCLC), the Stk11/Lkb1 gene is subject to deletions and mutations, which contribute to the resistance of tumor patients to PD-1/PD-L1 inhibitors (29). The resistance to PD-1/PD-L1 inhibitors can also be attributed to abnormalities in the composition of gut microbiota. Research has shown that patients who are resistant to PD-1/PD-L1 inhibitors often experience alterations in their gut microbiome structure due to antibiotic use, which disrupts the homeostasis of gut flora. In animal experiments, fecal transplants from mice sensitive to PD-1/PD-L1 inhibitors into the intestines of resistant mice resulted in a significant restoration of sensitivity to these inhibitors. Metagenomic analysis indicated that this phenomenon is associated with the relative abundance of Akkermansia muciniphila (30).
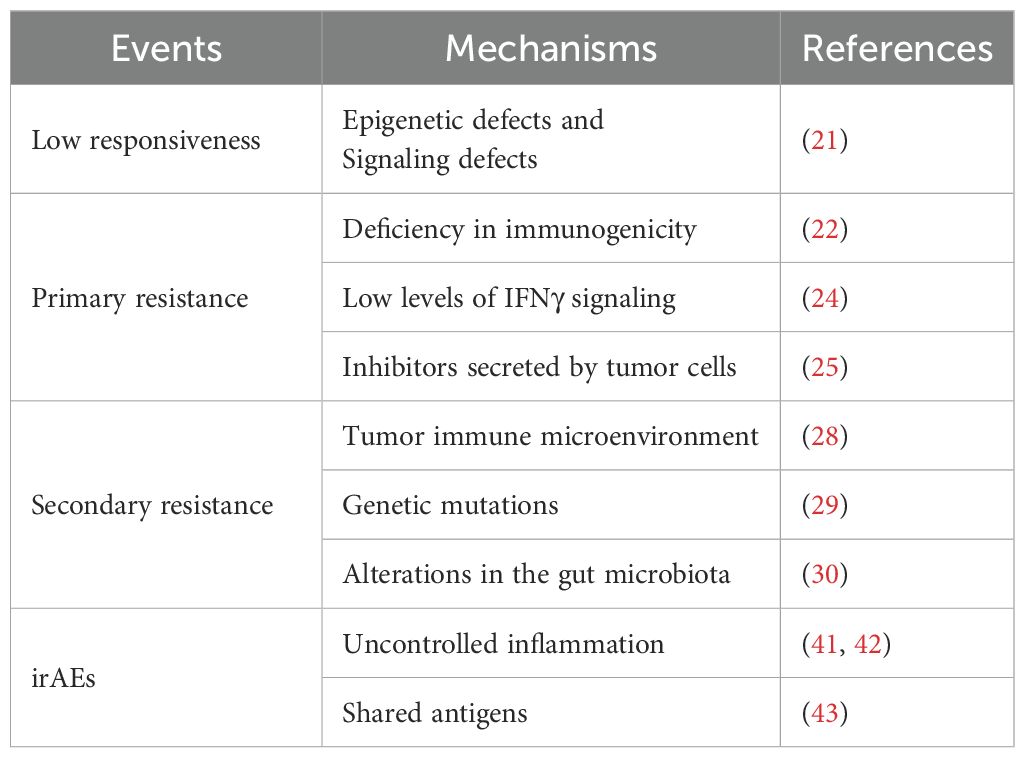
Table 1. The ICI monotherapy dilemma.
Long-term use of ICIs continuously stimulates the immune system, which may lead to the occurrence of irAEs (31, 32). Numerous studies have demonstrated that the use of PD-1/PD-L1 inhibitors alone in the treatment of various types of cancer patients is associated with a significantly elevated risk of irAEs, with this incidence typically reaching 20% to 30% (33–35), including risks associated with drug toxicity-related mortality and inflammatory responses in target organs (36, 37). For patients who have previously experienced irAEs, the risk of developing irAEs again upon re-treatment with PD-1/PD-L1 inhibitors rises to 34.2% (38). This risk is also associated with factors such as the type of medication used and the specific tumor type involved (39, 40). The uncontrolled inflammation and shared antigens may be the primary causes of irAEs. Researchers have observed that following the administration of PD-1/PD-L1 inhibitors, there is a significant infiltration of T cells into both tumor tissues and even normal tissues. This phenomenon can lead to the release of numerous inflammatory factors, resulting in adverse reactions (41). Patients with melanoma often experience gastrointestinal adverse reactions such as diarrhea or colitis following the use of PD-1 inhibitors. Notably, serum levels of IL-10 and IL-17 in these patients are frequently significantly elevated, with serum IL-10 also serving as a potential predictor for melanoma recurrence (42). In patients with NSCLC, nine antigens identical to those found in human skin tissue have been identified on the surface of tumor cells. This suggests that while patients undergo monotherapy immunotherapy, normal skin tissue may also be affected (43).
It is evident that, despite the groundbreaking advancements achieved with PD-1/PD-L1 inhibitors in tumor immunotherapy, monotherapy still presents certain limitations. To enhance efficacy and overcome resistance, exploring combination therapy strategies has become an inevitable trend.
Therapeutic strategies based on the combination of PD-1/PD-L1 inhibitors and chemotherapeutic agents
Although PD-L1 inhibitors may demonstrate significant efficacy in patients with advanced NSCLC who exhibit high levels of PD-L1 expression (44), they can also accelerate tumor progression in a subset of these patients (45). Chemotherapy agents can delay the growth of tumor cells by stimulating immune responses, inhibiting DNA replication, and interfering with cellular metabolism and the cell cycle (46, 47). Therefore, chemotherapy remains a high-priority treatment option for most cancers. In recent years, clinical trials have been conducted to investigate the efficacy of combining PD-1/PD-L1 inhibitors with chemotherapy drugs, aiming to determine whether this combination therapy can achieve improved therapeutic outcomes. In experiments involving lung cancer gene mice treated with low-dose Apatinib in combination with PD-L1 inhibitors, it was observed that the concurrent administration of low-dose Apatinib and anti-PD-L1 significantly delayed tumor growth. The researchers confirmed that low-dose Apatinib enhances the infiltration of CD8+ T cells while reducing the recruitment of tumor-associated macrophages within the tumor microenvironment, thereby optimizing its conditions (48). Triple-negative breast cancer is characterized by high heterogeneity, aggressive behavior, and a lack of specific therapeutic targets, which often results in limited efficacy of chemotherapy. This has posed a significant challenge in the field of breast cancer treatment. However, it is noteworthy that researchers have discovered that the combination therapy of PD-L1 inhibitors with paclitaxel can yield satisfactory outcomes (49). Subsequently, further studies have confirmed that this approach is not restricted to its use with paclitaxel; combinations of doxorubicin or cisplatin with PD-1/PD-L1 inhibitors also represent promising therapeutic strategies for triple-negative breast cancer (50). Similarly, the underlying cause of this phenomenon can also be attributed to alterations in the tumor immune microenvironment (51).
The combination therapy for NSCLC has also become a research focus. A phase III clinical study revealed that, compared to chemotherapy alone, the use of PD-1 inhibitors in conjunction with standard chemotherapy significantly improves the overall survival rate of patients with non-small cell lung cancer (52). The combination immunotherapy involving PD-L1 inhibitors, such as atezolizumab and bevacizumab, has garnered significant attention. When used in conjunction with carboplatin and paclitaxel for the treatment of NSCLC, these therapies have demonstrated notable therapeutic efficacy and are regarded as a first-line treatment option for NSCLC (53–55). The current evidence regarding the enhanced efficacy of combining chemotherapy agents with ICIs in amplifying the antitumor effects of monotherapy remains limited. We propose that this synergy may be attributed to the complementary mechanisms of action between the two treatment modalities. Firstly, chemotherapy agents can promote the release and presentation of tumor antigens, thereby enhancing T cell recognition and attack capabilities against tumors. Concurrently, ICIs serve to restore T cell immune function further. Secondly, chemotherapy can eliminate immunosuppressive cells within the tumor microenvironment, thereby altering it to facilitate a more effective response when ICIs are employed to reinstate immune system functionality.
However, although the combination therapy of chemotherapy agents with PD-1/PD-L1 inhibitors can significantly enhance therapeutic efficacy, issues such as resistance and irAEs persist. Research has indicated that Galectin-3 (Gal-3) plays a role in drug resistance. Numerous patients with lung adenocarcinoma and melanoma who exhibit resistance to PD-L1 inhibitors have been identified, characterized by a high expression of Gal-3 in their tumor cells (56, 57). Gal-3 binding to the glycosylation on PD-L1 can lead to a decreased affinity of atezolizumab for its receptor, resulting in impaired therapeutic efficacy and the development of resistance. However, when the glycosylation is removed from PD-1, the tumor’s sensitivity to the drug is restored (58), and the combined use of GB1211 (a Gal-3 inhibitor) with PD-L1 inhibitors can effectively eliminate Gal-3-induced resistance to pembrolizumab and atezolizumab, thereby enhancing their therapeutic effectiveness (59). The irAEs associated with combination therapy primarily include fever, skin toxicity, thyroid dysfunction, and pneumonia. The incidence of these risks has reached 68.3% (60). Furthermore, some studies have reported that approximately 1.49% of patients experienced fatal outcomes following treatment with platinum-based agents in conjunction with PD-1/PD-L1 inhibitors (61).
It is evident that the combination of PD-1/PD-L1 inhibitors with chemotherapy agents significantly enhances anti-tumor efficacy. However, the cytotoxic effects of chemotherapy drugs still pose a risk of irAEs for patients following treatment. Therefore, further exploration of effective and safe strategies for combined immunotherapy involving PD-1/PD-L1 remains a crucial research direction in cancer therapy.
Therapeutic strategies involving PD-1/PD-L1 inhibitors in combination with other ICIs
Immune checkpoint markers often play similar roles; therefore, the combination of ICIs is theoretically feasible for enhancing tumor treatment efficacy. CTLA-4 is predominantly expressed on regulatory T cells (Tregs) and activated T cells, where it exerts an inhibitory effect on T cell activation. Currently, it is established that CTLA-4 and PD-1 are co-inhibitory molecules. Evidence suggests that they inhibit T cell activation through distinct mechanisms (62). CTLA-4 binds to CD80 and CD86, thereby utilizing SHP-2 to inhibit downstream signaling induced by TCR and suppressing the PI3K-Akt pathway, which ultimately affects T cell activation (63). Besides, CTLA-4 functions at the early stage of T cell activation, specifically during the “immune initiation phase”, while PD-1/PD-L1 operates during the “effector phase” (64), this indicates that CTLA-4 and PD-1 function at different time points during T cell evolution and may have overlapping effects.
In a clinical trial involving 945 patients with stage III or IV melanoma, the survival rates of patients treated with Ipilimumab (a CTLA-4 inhibitor) and Nivolumab (a PD-1 inhibitor) in combination were investigated and compared to those receiving monotherapy with either drug. The results indicated that the median survival time for the combination therapy group exceeded 60 months, while it was 19.9 months for the Ipilimumab group and 36.9 months for the Nivolumab group. Furthermore, the five-year survival rate in the combination therapy group was also found to be the highest at 52%. However, this study also revealed that the incidence of adverse events was greatest in the combination therapy group (65). Meanwhile, the combination of these two types of ICIs demonstrates a significant advantage over standard targeted therapies or chemotherapy (66, 67). Wei et al. (68) conducted an experiment using the MC38 colon adenocarcinoma mouse model, where they analyzed the T cell phenotypes in tumor samples from mice treated with a combination of CTLA-4 and PD-1 inhibitors through mass cytometry. Their findings concluded that the efficacy of combination therapy is, in most cases, additive to that of monotherapy. Furthermore, they observed an expansion of terminally differentiated effector CD8+ T cells following combination treatment, which also led to an increased frequency of type 1 helper T cells. High-grade neuroendocrine tumors are characterized by more aggressive biological properties and low expression of somatostatin receptors, which often results in a lower response rate to chemotherapy (69). A phase 3 clinical study has demonstrated that 44% of patients with high-grade neuroendocrine tumors exhibit a favorable response to dual blockade therapy targeting CTLA-4 and PD-1. This response rate represents a significant improvement compared to chemotherapy and monotherapy with ICIs. However, the incidence of treatment-related adverse events reached 84.4%, primarily including abnormalities in thyroid and liver function, as well as symptoms such as vomiting and fatigue (70). Although these side effects are considerably milder than the consequences associated with the tumor itself, there remains a pressing need for therapeutic strategies that not only deliver substantial efficacy but also minimize adverse effects in order to enhance patients’ quality of life. However, some clinical trial results have not achieved the expected outcomes. The combination of durvalumab and tremelimumab has shown no significant improvement in treatment efficacy compared to trastuzumab in patients with metastatic urothelial carcinoma and head and neck squamous cell carcinoma (71, 72). In contrast, better therapeutic effects can be observed in patients with non-small cell lung cancer (73), it indicates that the combined immunotherapy strategies involving ICIs still require tailored approaches based on specific tumor subgroups. Furthermore, extensive foundational experiments and clinical research are necessary to develop more specialized treatment guidelines that support these therapeutic regimens.
The efficacy of combining PD-1/PD-L1 inhibitors with other ICIs, such as α-TIM-3, α-LAG-3, α-PVRIG, and α-TIGIT, is currently under investigation. Nivolumab in combination with α-PVRIG or α-TIGIT has demonstrated improved efficacy in patients with PD-L1-positive NSCLC compared to monotherapy combined with placebo groups (74). The efficacy and safety of the combination therapy with α-TIM-3 have been studied across various types of tumors. Research indicates that this combined strategy is well-tolerated by patients, with a slight enhancement in therapeutic effect. However, it is noteworthy that over half of the patients experienced adverse events. Therefore, further research is needed to refine patient selection criteria (75–77). Some scholars have proposed a treatment strategy that combines two types of ICIs with chemotherapy agents. In a mouse model experiment for intrahepatic cholangiocarcinoma, the therapeutic approach involved pre-treatment with a CTLA-4 inhibitor and platinum-based chemotherapy, followed by administration of a PD-1 inhibitor. This combination demonstrated significant survival benefits and lower incidence rates compared to monotherapy with ICIs. Further research revealed that platinum compounds could normalize the vasculature in Intrahepatic Cholangiocarcinoma (ICC), while dual blockade of CTLA-4 and PD-1 resulted in an increased population of CD8+ T cells (78). Table 2 summarizes the clinical research findings on the combination therapy of PD-1/PD-L1 inhibitors with other ICIs for cancer treatment. The majority of these studies focus on the combination with CTLA-4 inhibitors. This combined therapeutic approach holds promise for application in clinical trials, aiming to address patient resistance to single ICIs.
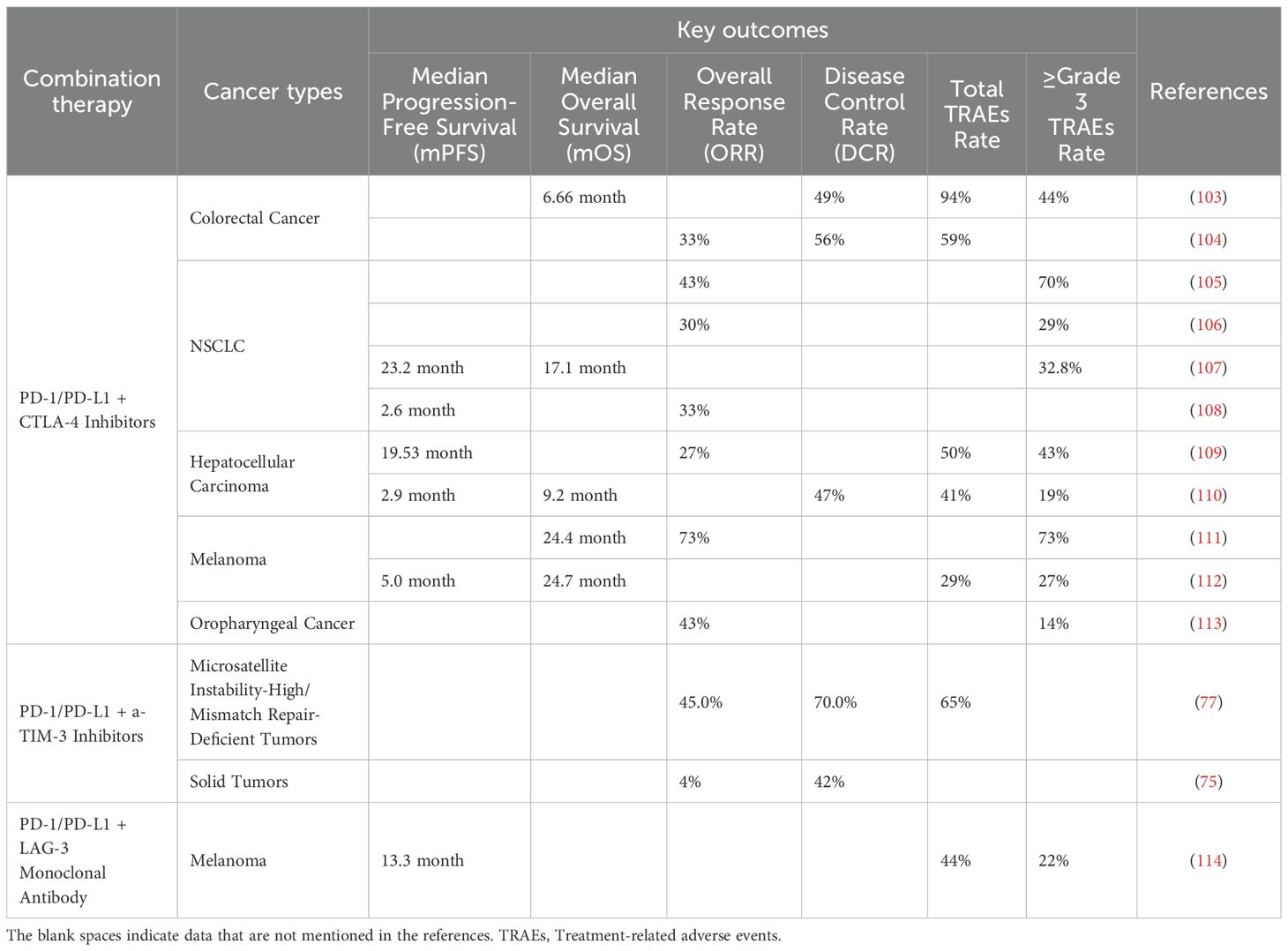
Table 2. The efficacy of PD-1/PD-L1 inhibitors in combination with other types of immune checkpoint inhibitors in cancer treatment.
However, the combinatorial strategies involving ICIs still require extensive research validation. Some studies have reported contrasting conclusions, indicating that the concurrent use of multiple ICIs for cancer treatment may lead to an earlier median onset time of irAEs without a significant enhancement in therapeutic efficacy (79). This suggests that it remains essential to further explore the mechanisms underlying the synergistic effects of ICIs and their roles across different cancer phenotypes.
TCM in tumor therapy and its comprehensive immunotherapy combined with PD-1/PD-L1 inhibitors
Currently, it is widely recognized that TCM possesses advantages in cancer treatment through multiple pathways and targets. TCM can exert its anti-tumor effects by altering the tumor immune microenvironment and enhancing the immune efficacy of T cells. Additionally, its functions include promoting the proliferation and differentiation of T cells, boosting the activity of natural killer cells, inhibiting immune checkpoints, and modulating immune signaling pathways (80, 81). In TCM, herbal remedies are often utilized as maintenance therapy for patients who have undergone surgery or received radiotherapy and chemotherapy. This approach aims to alleviate adverse reactions following treatment, thereby reducing patient suffering. Additionally, some studies have reported that adjunctive herbal therapy may extend the median survival time of certain patients (82, 83) and decrease the mortality risk associated with cancer (84). Berberine, a compound recognized in TCM, possesses the ability to regulate endocrine metabolism and improve gut microbiota. Additionally, due to its capacity to induce apoptosis in cancer cells, it is frequently employed in the fight against various cancers (85). Research has also indicated that berberine can enhance the sensitivity of tumor cells to CD8+ T cells by reducing the expression levels of PD-L1 on these cells, thereby contributing to immunotherapy efforts (86). As previously mentioned, the homeostasis of gut microbiota plays a crucial role in the body’s ability to eliminate tumor cells. Ginseng Polysaccharides can enhance the sensitivity of tumor patients who are resistant to PD-1 inhibitors by improving the gut microbiota structure in non-small cell lung cancer patients and increasing the microbial metabolite pentanoate (87). The mutations in genes of normal cells disrupt the homeostasis of the extracellular environment, thereby promoting tumor cell proliferation, metastasis, and drug resistance through various signaling pathways. This results in a complex TIME, which is one of the critical factors determining the development and characteristics of tumor cells (88). The complex components of TCM engage multiple signaling pathways, which endows it with unique advantages in cancer treatment. TCM can modulate various cytokines and immune cells within the tumor immune microenvironment TIME, thereby enhancing the body’s immune function (89). Huangqi, a traditional Chinese medicinal herb with a long history, is commonly utilized as one of the herbal components in various bioactive TCM formulas. It has been shown to directly combat tumor cell proliferation and promote apoptosis in tumor cells, thereby reducing tumor volume and inhibiting metastasis. Additionally, Huangqi can enhance immune response by activating macrophages and T cells within the TIME to target and eliminate tumors (90). The Yiyi Fuzi Baijiang Decoction is a TCM formula used for the treatment of gastrointestinal diseases. It has been demonstrated to possess significant efficacy in the management of gastrointestinal tumors. This decoction can alter the gut microbiota structure in ApcMin/+ mice and regulate the Treg/Th17 ratio to control cellular carcinogenesis. Additionally, it inhibits the proliferation and development of intestinal tumor cells in ApcMin/+ mice (91).
TCM emphasizes enhancing the body’s overall immunity to improve its anti-tumor capabilities, which aligns closely with contemporary mainstream concepts of tumor immunotherapy. Additionally, the combined use of TCM and anti-tumor drugs can significantly enhance therapeutic efficacy while reducing side effects, thereby playing a crucial role in improving the survival rates of cancer patients. Numerous studies have reported that TCM can serve as a sensitizer for PD-1/PD-L1 inhibitors by modulating the TIME and improving gut microbiota, thus strengthening anti-tumor immune responses. A meta-analysis conducted an in-depth examination of the effects of TCM combined with PD-1/PD-L1 inhibitors on various tumor subgroups. The findings revealed that, following the combination treatment of TCM and PD-1/PD-L1 inhibitors, there was a significant reduction in both tumor weight and volume compared to treatment with PD-1/PD-L1 inhibitors alone. Additionally, patients experienced a notable extension in survival time, accompanied by a marked increase in the activity of CD4+ T lymphocytes and various growth factors (92). The mice with intestinal tumors treated with a combination of Gegen Qinlian Decoction and PD-1 inhibitors exhibited a significant upregulation of IL-2 levels compared to those treated solely with PD-1 inhibitors. This indicates that the combined therapy is beneficial for restoring T cell function. Furthermore, this study found an increase in the abundance of gut Bacteroides in mice receiving the combined treatment, which can enhance the intestinal immune inflammatory environment and exert immunomodulatory effects by releasing extracellular bacterial DNA (93). The Shenmai injection primarily adjusts the tumor immune microenvironment by inducing the infiltration of NK cell subpopulations. Furthermore, its synergistic effect in combating NSCLC when used in conjunction with PD-1 inhibitors is superior to that of PD-1 inhibitors alone. Ultimately, this combination therapy prolongs the survival time of cancer patients and highlights that NK cell-mediated apoptosis of tumor cells is one of the key synergistic mechanisms underlying this combined treatment approach (94). The combination of demethoxycurcumin and PD-L1 inhibitors can activate the functionality of CD8+ T cells while simultaneously suppressing MDSCs, thereby enhancing the immune defense against tumor cells (95). Table 3 summarizes several clinical studies on the combination of TCM with PD-1/PD-L1 inhibitors in cancer treatment. However, research in this area remains limited, and most studies have primarily focused on Asian populations. Nevertheless, it is evident from these investigations that the combined use of TCM and PD-1/PD-L1 inhibitors not only demonstrates a favorable anti-tumor effect but also presents a relatively low risk of adverse reactions (even though these data are derived from small sample sizes). This underscores the need for further in-depth exploration into the integration of traditional and modern medical approaches for cancer treatment. Table 4 provides a brief introduction to the traditional Chinese medicine mentioned above.
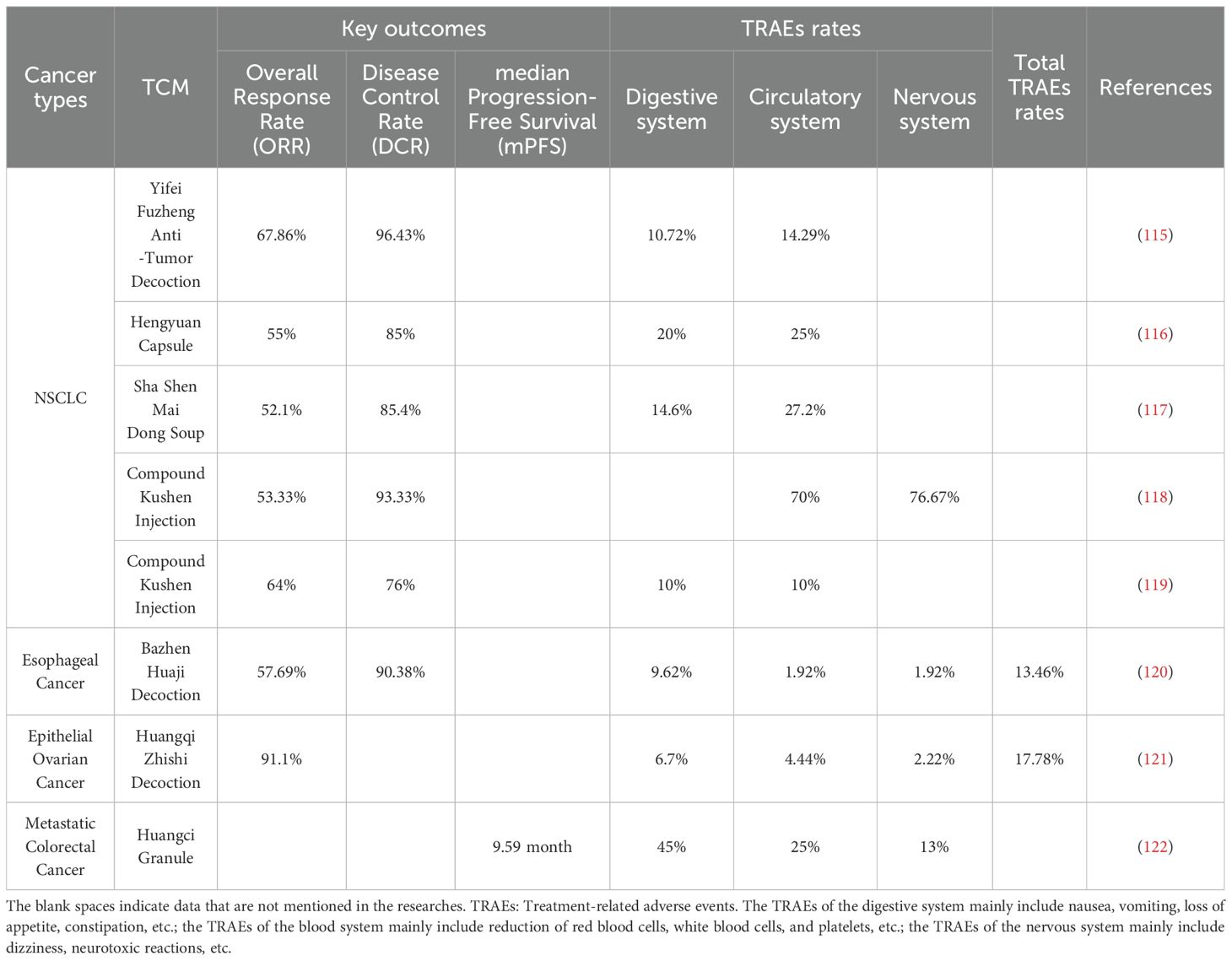
Table 3. The efficacy of traditional Chinese medicine combined with PD-1/PD-L1 inhibitors in the treatment of cancer.
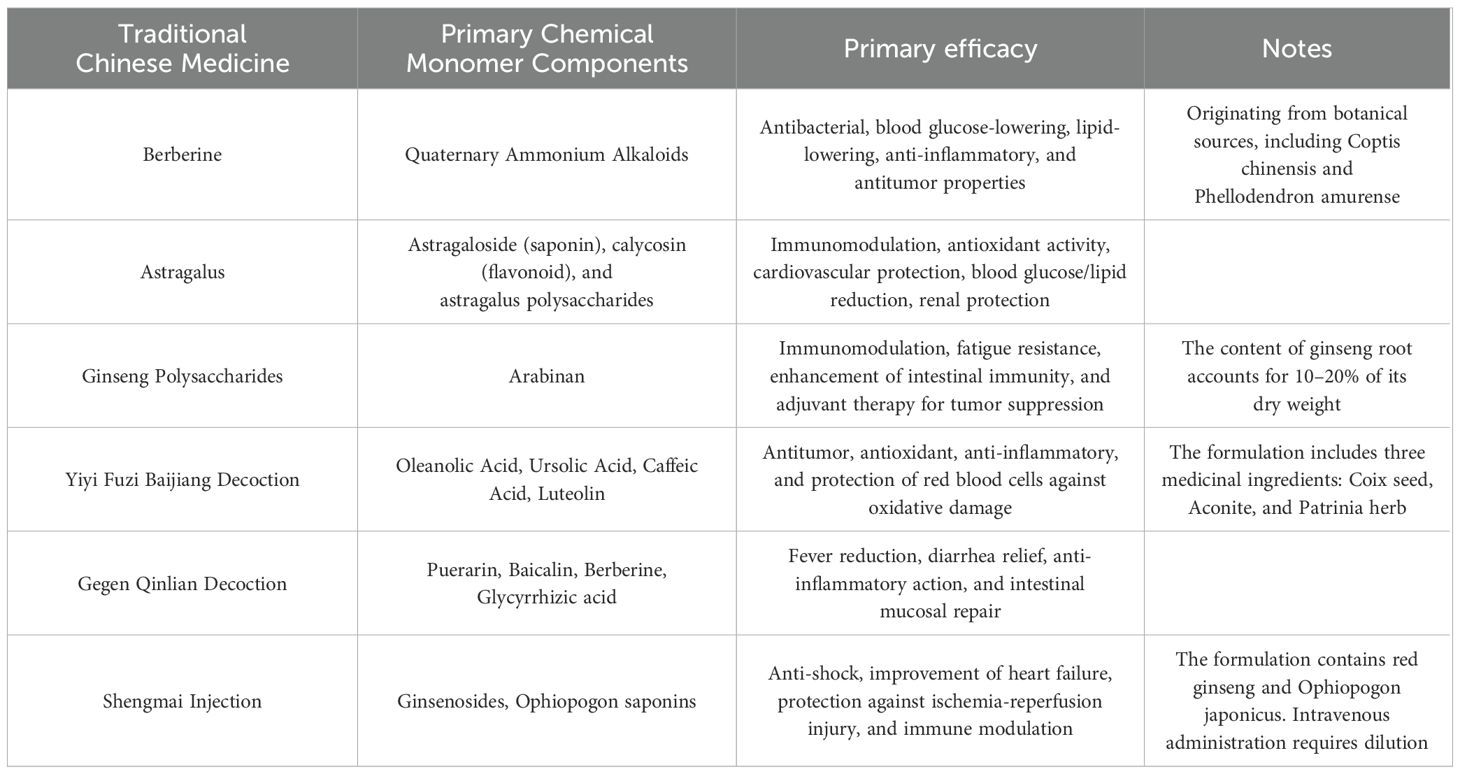
Table 4. A brief description of the TCM mentioned in this review.
The combination of TCM with PD-1/PD-L1 inhibitors in comprehensive immunotherapy offers new perspectives and strategies for cancer treatment. Existing research indicates that TCM, through its multi-component and multi-target mechanisms, can modulate the tumor microenvironment, enhance immune cell functionality, and exert a synergistic anti-tumor effect when used alongside PD-1/PD-L1 inhibitors. However, several issues remain to be addressed urgently, such as the identification of specific active components in TCM, a deeper elucidation of their mechanisms of action, and the establishment of standardized protocols for combination therapy. Nevertheless, with the ongoing advancement in integrative studies between Western and TCM, this comprehensive immunotherapy holds promise for providing new therapeutic hope to more cancer patients and advancing the field of tumor immunotherapy further.
Perspective and conclusion
PD-1/PD-L1 inhibitors represent a revolutionary class of drugs in tumor immunotherapy, demonstrating significant efficacy across various malignancies. However, monotherapy still faces challenges such as low response rates, resistance, and irAEs, the existing combination strategies continue to face a dual challenge of efficacy and toxicity: the combination of these inhibitors with chemotherapy agents or multiple ICIs has been shown to enhance therapeutic efficacy to some extent and has become the preferred treatment option for certain tumors; nevertheless, issues related to resistance and irAEs remain unresolved and may potentially increase toxic side effects. In contrast to chemotherapy agents, TCM is characterized by its multi-component, multi-targeted approach that promotes holistic regulation while causing minimal damage to normal cells. TCM can exert unique advantages in anti-tumor activity and immune modulation. Recent studies have increasingly indicated that certain herbal medicines can synergistically enhance the anti-tumor effects of PD-1/PD-L1 inhibitors through mechanisms such as modulating the tumor microenvironment, enhancing immune cell function, and inhibiting PD-1/PD-L1 expression.
This study not only summarizes the use of PD-1/PD-L1 inhibitors in combination with other Western medical approaches for cancer treatment but also conducts an in-depth review of relevant research on their concurrent application with TCM. The aim is to explore the feasibility of combined anti-tumor therapies from a TCM perspective. Traditional Chinese medicine can reshape the immune microenvironment through multi-target mechanisms, reduce irAEs, and optimize the anti-tumor effects of ICIs. Numerous herbal formulas and active components, such as astragalus polysaccharides and cordycepin, have been shown to modulate the tumor immune microenvironment through multi-target actions: promoting dendritic cell maturation, enhancing T/NK cell functions, inhibiting regulatory T cells/myeloid-derived suppressor cells activity, downregulating immunosuppressive factors (such as TGF-β and IL-10), and even directly or indirectly regulating PD-1/PD-L1 expression. These mechanisms hold promise for reversing immunosuppressive states and enhancing the efficacy of PD-1/PD-L1 inhibitors (96–99). Compared to chemotherapy or dual immunotherapy, traditional Chinese medicine demonstrates unique and significant advantages in terms of “toxicity reduction.” Clinical practices and some studies have indicated that traditional Chinese medicine can alleviate toxic reactions such as rashes, diarrhea, pneumonia, and hepatitis. Additionally, it has the potential to improve overall patient symptoms (such as fatigue, loss of appetite, and sleep disturbances), thereby enhancing quality of life and treatment tolerance (100–102).
However, it is essential to recognize that there are significant deficiencies in the current research on the combination of traditional Chinese medicine with PD-1/PD-L1 inhibitors for cancer treatment. The majority of existing evidence stems from small-sample retrospective analyses, case reports, or basic research, lacking rigorously designed and large-sample prospective randomized controlled trials (RCTs) that can provide high-level evidence in evidence-based medicine. Looking ahead, it is crucial to elucidate the underlying mechanisms of action when combining PD-1/PD-L1 inhibitors with TCM. Identifying and optimizing the best combinations of these therapies will be essential. Conducting high-quality clinical research will provide a comprehensive assessment of the safety and efficacy of combination regimens while further exploring the potential for integrating TCM with various ICIs in cancer treatment. This endeavor holds promise as an important area for leveraging TCM in anti-tumor strategies.
Author contributions
CT: Writing – review & editing, Writing – original draft. YW: Supervision, Writing – review & editing. RW: Writing – review & editing, Writing – original draft, Funding acquisition.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was supported by funds from the Zhejiang Provincial Science and Technology Department Research Institute and research project (No.2023TD001), and Linping District Medical and Health Technology Project (LPWJ2024-03-77).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CTLA-4, Cytotoxic T-Lymphocyte Antigen 4; Gal-3, Galectin-3; ICIs, immune checkpoint inhibitors; irAEs, immune-related adverse events; LAG-3, Lymphocyte Activation Gene-3; MDSCs, myeloid-derived suppressor cells; NSCLC, non-small cell lung cancer; PD-1, Programmed Cell Death Protein-1; PD-L1, Programmed Cell Death-Ligand 1; SHP-2, Src homology region 2 domain-containing phosphatase; TCM, Traditional Chinese medicine; TCR, T cell receptor; TGF-β, transforming growth factor β; TIME, tumor immune microenvironment; Tregs, regulatory T cells.
References
1. Rui R, Zhou L, and He S. Cancer immunotherapies: advances and bottlenecks. Front Immunol. (2023) 14:1212476. doi: 10.3389/fimmu.2023.1212476
2. Dolina JS, Van Braeckel-Budimir N, Thomas GD, and Salek-Ardakani S. Cd8(+) T cell exhaustion in cancer. Front Immunol. (2021) 12:715234. doi: 10.3389/fimmu.2021.715234
3. Attanasio J and Wherry EJ. Costimulatory and coinhibitory receptor pathways in infectious disease. Immunity. (2016) 44:1052–68. doi: 10.1016/j.immuni.2016.;4.022
4. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. (2012) 12:252–64. doi: 10.1038/nrc3239
5. Peng L, Sferruzza G, Yang L, Zhou L, and Chen S. Car-T and car-nk as cellular cancer immunotherapy for solid tumors. Cell Mol Immunol. (2024) 21:1089–108. doi: 10.1038/s41423-024-01207-0
6. Ghosh C, Luong G, and Sun Y. A snapshot of the pd-1/pd-L1 pathway. J Cancer. (2021) 12:2735–46. doi: 10.7150/jca.57334
7. Ortega MA, Boaru DL, De Leon-Oliva D, Fraile-Martinez O, García-Montero C, Rios L, et al. Pd-1/pd-L1 axis: implications in immune regulation, cancer progression, and translational applications. J Mol Med (Berl). (2024) 102:987–1000. doi: 10.1007/s00109-024-02463-3
8. Hossain MA, Liu G, Dai B, Si Y, Yang Q, Wazir J, et al. Reinvigorating exhausted cd8(+) cytotoxic T lymphocytes in the tumor microenvironment and current strategies in cancer immunotherapy. Med Res Rev. (2021) 41:156–201. doi: 10.1002/med.21727
9. Chen L and Han X. Anti-pd-1/pd-L1 therapy of human cancer: past, present, and future. J Clin Invest. (2015) 125:3384–91. doi: 10.1172/jci80011
10. Yu YX, Wang S, Liu ZN, Zhang X, Hu ZX, Dong HJ, et al. Traditional chinese medicine in the era of immune checkpoint inhibitor: theory, development, and future directions. Chin Med. (2023) 18:59. doi: 10.1186/s13020-023-00751-7
11. Kaptein P, Jacoberger-Foissac C, Dimitriadis P, Voabil P, de Bruijn M, and Brokamp S. et al. Addition of Interleukin-2 Overcomes Resistance to Neoadjuvant Ctla4 and Pd1 Blockade in Ex Vivo Patient Tumors. Sci Transl Med. (2022) 14:eabj9779. doi: 10.1126/scitranslmed.abj9779
12. Jalili-Nik M, Soltani A, Mashkani B, Rafatpanah H, and Hashemy SI. Pd-1 and pd-L1 inhibitors foster the progression of adult T-cell leukemia/lymphoma. Int Immunopharmacol. (2021) 98:107870. doi: 10.1016/j.intimp.2021.107870
13. Nakamura T, Sato T, Endo R, Sasaki S, Takahashi N, Sato Y, et al. Sting agonist loaded lipid nanoparticles overcome anti-pd-1 resistance in melanoma lung metastasis via nk cell activation. J Immunother Cancer. (2021) 9. doi: 10.1136/jitc-2021-002852
14. Zuo H and Wan Y. Inhibition of myeloid pd-L1 suppresses osteoclastogenesis and cancer bone metastasis. Cancer Gene Ther. (2022) 29:1342–54. doi: 10.1038/s41417-022-00446-5
15. Hashimoto M, Ramalingam SS, and Ahmed R. Harnessing cd8 T cell responses using pd-1-il-2 combination therapy. Trends Cancer. (2024) 10:332–46. doi: 10.1016/j.trecan.2023.11.008
16. Utzschneider DT, Charmoy M, Chennupati V, Pousse L, Ferreira DP, Calderon-Copete S, et al. T cell factor 1-expressing memory-like cd8(+) T cells sustain the immune response to chronic viral infections. Immunity. (2016) 45:415–27. doi: 10.1016/j.immuni.2016.07.021
17. Im SJ, Hashimoto M, Gerner MY, Lee J, Kissick HT, Burger MC, et al. Defining cd8+ T cells that provide the proliferative burst after pd-1 therapy. Nature. (2016) 537:417–21. doi: 10.1038/nature19330
18. Sitaram P, Uyemura B, Malarkannan S, and Riese MJ. Beyond the cell surface: targeting intracellular negative regulators to enhance T cell anti-tumor activity. Int J Mol Sci. (2019) 20. doi: 10.3390/ijms20235821
19. Shi J, He C, Chen L, Xing X, Wei W, and Zhang J. Targeting pd-1 post-translational modifications for improving cancer immunotherapy. Cell Insight. (2025) 4:100248. doi: 10.1016/j.cellin.2025.100248
20. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, et al. Pd-1 blockade induces responses by inhibiting adaptive immune resistance. Nature. (2014) 515:568–71. doi: 10.1038/nature13954
21. Morad G, Helmink BA, Sharma P, and Wargo JA. Hallmarks of response, resistance, and toxicity to immune checkpoint blockade. Cell. (2021) 184:5309–37. doi: 10.1016/j.cell.2021.09.020
22. Kawakami Y, Ohta S, Sayem MA, Tsukamoto N, and Yaguchi T. Immune-resistant mechanisms in cancer immunotherapy. Int J Clin Oncol. (2020) 25:810–7. doi: 10.1007/s10147-019-01611-x
23. Mariathasan S, Turley SJ, Nickles D, Castiglioni A, Yuen K, Wang Y, et al. Tgfβ Attenuates tumour response to pd-L1 blockade by contributing to exclusion of T cells. Nature. (2018) 554:544–8. doi: 10.1038/nature25501
24. Bullock BL, Kimball AK, Poczobutt JM, Neuwelt AJ, Li HY, Johnson AM, et al. Tumor-intrinsic response to ifnγ Shapes the tumor microenvironment and anti-pd-1 response in nsclc. Life Sci Alliance. (2019) 2. doi: 10.26508/lsa.201900328
25. Wang Z and Wu X. Study and analysis of antitumor resistance mechanism of pd1/pd-L1 immune checkpoint blocker. Cancer Med. (2020) 9:8086–121. doi: 10.1002/cam4.3410
26. Hanahan D and Coussens LM. Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell. (2012) 21:309–22. doi: 10.1016/j.ccr.2012.02.022
27. Liu C, Zheng S, Wang Z, Wang S, Wang X, Yang L, et al. Kras-G12d mutation drives immune suppression and the primary resistance of anti-pd-1/pd-L1 immunotherapy in non-small cell lung cancer. Cancer Commun (Lond). (2022) 42:828–47. doi: 10.1002/cac2.12327
28. Peng DH, Rodriguez BL, Diao L, Chen L, Wang J, Byers LA, et al. Collagen promotes anti-pd-1/pd-L1 resistance in cancer through lair1-dependent cd8(+) T cell exhaustion. Nat Commun. (2020) 11:4520. doi: 10.1038/s41467-020-18298-8
29. Skoulidis F, Goldberg ME, Greenawalt DM, Hellmann MD, Awad MM, Gainor JF, et al. Stk11/lkb1 mutations and pd-1 inhibitor resistance in kras-mutant lung adenocarcinoma. Cancer Discov. (2018) 8:822–35. doi: 10.1158/2159-8290.Cd-18-0099
30. Routy B, Le Chatelier E, Derosa L, Duong CPM, Alou MT, Daillère R, et al. Gut microbiome influences efficacy of pd-1-based immunotherapy against epithelial tumors. Science. (2018) 359:91–7. doi: 10.1126/science.aan3706
31. Alghamdi EA, Aljohani H, Alghamdi W, and Alharbi F. Immune checkpoint inhibitors and potential risk of thromboembolic events: analysis of the who global database of individual case safety reports. Saudi Pharm J. (2022) 30:1193–9. doi: 10.1016/j.jsps.2022.06.010
32. Chhabra N and Kennedy J. A review of cancer immunotherapy toxicity: immune checkpoint inhibitors. J Med Toxicol. (2021) 17:411–24. doi: 10.1007/s13181-021-00833-8
33. Sonpavde GP, Grivas P, Lin Y, Hennessy D, and Hunt JD. Immune-related adverse events with pd-1 versus pd-L1 inhibitors: A meta-analysis of 8730 patients from clinical trials. Future Oncol. (2021) 17:2545–58. doi: 10.2217/fon-2020-1222
34. Zhang Q, Wang W, Yuan Q, Li L, Wang YC, Chi CZ, et al. Correlation between immune-related adverse events and the efficacy of pd-1/pd-L1 inhibitors in the treatment of non-small cell lung cancer: systematic review and meta-analysis. Cancer Chemother Pharmacol. (2022) 89:1–9. doi: 10.1007/s00280-021-04375-2
35. Shi Y, Duan J, Guan Q, Xue P, and Zheng Y. Effectivity and safety of pd-1/pd-L1 inhibitors for different level of pd-L1-positive, advanced nsclc: A meta-analysis of 4939 patients from randomized controlled trials. Int Immunopharmacol. (2020) 84:106452. doi: 10.1016/j.intimp.2020.106452
36. Wolchok JD, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J Clin Oncol. (2022) 40:127–37. doi: 10.1200/jco.21.02229
37. Shoushtari AN, Friedman CF, Navid-Azarbaijani P, Postow MA, Callahan MK, Momtaz P, et al. Measuring toxic effects and time to treatment failure for nivolumab plus ipilimumab in melanoma. JAMA Oncol. (2018) 4:98–101. doi: 10.1001/jamaoncol.2017.2391
38. Zafar A, Rashid AA, Moeed A, Tahir MJ, Khan AJ, Shrateh ON, et al. Safety and efficacy of pd-1/pd-L1 immune checkpoint inhibitors in patients with pre-treated advanced stage Malignant mesothelioma: A systematic review and meta-analysis. BMC Cancer. (2024) 24:1353. doi: 10.1186/s12885-024-13127-3
39. Bertrand A, Kostine M, Barnetche T, Truchetet ME, and Schaeverbeke T. Immune related adverse events associated with anti-ctla-4 antibodies: systematic review and meta-analysis. BMC Med. (2015) 13:211. doi: 10.1186/s12916-015-0455-8
40. Wang Y, Zhou S, Yang F, Qi X, Wang X, Guan X, et al. Treatment-related adverse events of pd-1 and pd-L1 inhibitors in clinical trials: A systematic review and meta-analysis. JAMA Oncol. (2019) 5:1008–19. doi: 10.1001/jamaoncol.2019.0393
41. Geisler AN, Phillips GS, Barrios DM, Wu J, Leung DYM, Moy AP, et al. Immune checkpoint inhibitor-related dermatologic adverse events. J Am Acad Dermatol. (2020) 83:1255–68. doi: 10.1016/j.jaad.2020.03.132
42. Tarhini AA, Zahoor H, Lin Y, Malhotra U, Sander C, Butterfield LH, et al. Baseline circulating il-17 predicts toxicity while tgf-β1 and il-10 are prognostic of relapse in ipilimumab neoadjuvant therapy of melanoma. J Immunother Cancer. (2015) 3:39. doi: 10.1186/s40425-015-0081-1
43. Berner F, Bomze D, Diem S, Ali OH, Fässler M, Ring S, et al. Association of checkpoint inhibitor-induced toxic effects with shared cancer and tissue antigens in non-small cell lung cancer. JAMA Oncol. (2019) 5:1043–7. doi: 10.1001/jamaoncol.2019.0402
44. Sholl LM. Biomarkers of response to checkpoint inhibitors beyond pd-L1 in lung cancer. Mod Pathol. (2022) 35:66–74. doi: 10.1038/s41379-021-00932-5
45. Wang X, Wang F, Zhong M, Yarden Y, and Fu L. The biomarkers of hyperprogressive disease in pd-1/pd-L1 blockage therapy. Mol Cancer. (2020) 19:81. doi: 10.1186/s12943-020-01200-x
46. Gotwals P, Cameron S, Cipolletta D, Cremasco V, Crystal A, Hewes B, et al. Prospects for combining targeted and conventional cancer therapy with immunotherapy. Nat Rev Cancer. (2017) 17:286–301. doi: 10.1038/nrc.2017.17
47. Zhu H, Shan Y, Ge K, Lu J, Kong W, and Jia C. Oxaliplatin induces immunogenic cell death in hepatocellular carcinoma cells and synergizes with immune checkpoint blockade therapy. Cell Oncol (Dordr). (2020) 43:1203–14. doi: 10.1007/s13402-020-00552-2
48. Zhao S, Ren S, Jiang T, Zhu B, Li X, Zhao C, et al. Low-dose apatinib optimizes tumor microenvironment and potentiates antitumor effect of pd-1/pd-L1 blockade in lung cancer. Cancer Immunol Res. (2019) 7:630–43. doi: 10.1158/2326-6066.Cir-17-0640
49. Dirix LY, Takacs I, Jerusalem G, Nikolinakos P, Arkenau HT, Forero-Torres A, et al. Avelumab, an anti-pd-L1 antibody, in patients with locally advanced or metastatic breast cancer: A phase 1b javelin solid tumor study. Breast Cancer Res Treat. (2018) 167:671–86. doi: 10.1007/s10549-017-4537-5
50. De Santis P, Perrone M, Guarini C, Santoro AN, Laface C, Carrozzo D, et al. Early-stage triple negative breast cancer: the therapeutic role of immunotherapy and the prognostic value of pathological complete response. Explor Target Antitumor Ther. (2024) 5:232–50. doi: 10.37349/etat.2024.00215
51. Voorwerk L, Slagter M, Horlings HM, Sikorska K, van de Vijver KK, de Maaker M, et al. Immune induction strategies in metastatic triple-negative breast cancer to enhance the sensitivity to pd-1 blockade: the tonic trial. Nat Med. (2019) 25:920–8. doi: 10.1038/s41591-019-0432-4
52. Novello S, Kowalski DM, Luft A, Gümüş M, Vicente D, Mazières J, et al. Pembrolizumab plus chemotherapy in squamous non-small-cell lung cancer: 5-year update of the phase iii keynote-407 study. J Clin Oncol. (2023) 41:1999–2006. doi: 10.1200/jco.22.01990
53. Schmid P, Rugo HS, Adams S, Schneeweiss A, Barrios CH, Iwata H, et al. Atezolizumab plus nab-paclitaxel as first-line treatment for unresectab le, locally advanced or metastatic triple-negative breast cancer (Impassion130): updated efficacy results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. (2020) 21:44–59. doi: 10.1016/s1470-2045(19)30689-8
54. West H, McCleod M, Hussein M, Morabito A, Rittmeyer A, Conter HJ, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (Impower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. (2019) 20:924–37. doi: 10.1016/s1470-2045(19)30167-6
55. Zhang Y, Zhou H, and Zhang L. Which is the optimal immunotherapy for advanced squamous non-small-cell lung cancer in combination with chemotherapy: anti-pd-1 or anti-pd-L1? J Immunother Cancer. (2018) 6:135. doi: 10.1186/s40425-018-0427-6
56. Capalbo C, Scafetta G, Filetti M, Marchetti P, and Bartolazzi A. Predictive biomarkers for checkpoint inhibitor-based immunotherapy: the galectin-3 signature in nsclcs. Int J Mol Sci. (2019) 20. doi: 10.3390/ijms20071607
57. Kim JS, Kim S, Koh J, Kim M, Keam B, Kim TM, et al. Predictive role of galectin-3 for immune checkpoint blockades (Icbs) in advanced or metastatic non-small cell lung cancer: A potential new marker for icb resistance. J Cancer Res Clin Oncol. (2023) 149:2355–65. doi: 10.1007/s00432-022-04275-9
58. Liu K, Tan S, Jin W, Guan J, Wang Q, Sun H, et al. N-glycosylation of pd-1 promotes binding of camrelizumab. EMBO Rep. (2020) 21:e51444. doi: 10.15252/embr.202051444
59. Mabbitt J, Holyer ID, Roper JA, Nilsson UJ, Zetterberg FR, Vuong L, et al. Resistance to anti-pd-1/anti-pd-L1: galectin-3 inhibition with gb1211 reverses galectin-3-induced blockade of pembrolizumab and atezolizumab binding to pd-1/pd-L1. Front Immunol. (2023) 14:1250559. doi: 10.3389/fimmu.2023.1250559
60. Iwama S, De Remigis A, Callahan MK, Slovin SF, Wolchok JD, and Caturegli P. Pituitary expression of ctla-4 mediates hypophysitis secondary to administration of ctla-4 blocking antibody. Sci Transl Med. (2014) 6:230ra45. doi: 10.1126/scitranslmed.3008002
61. Zhou X, Yao Z, Bai H, Duan J, Wang Z, Wang X, et al. Treatment-related adverse events of pd-1 and pd-L1 inhibitor-based combination therapies in clinical trials: A systematic review and meta-analysis. Lancet Oncol. (2021) 22:1265–74. doi: 10.1016/s1470-2045(21)00333-8
62. Willsmore ZN, Coumbe BGT, Crescioli S, Reci S, Gupta A, Harris RJ, et al. Combined anti-pd-1 and anti-ctla-4 checkpoint blockade: treatment of melanoma and immune mechanisms of action. Eur J Immunol. (2021) 51:544–56. doi: 10.1002/eji.202048747
63. Qureshi OS, Zheng Y, Nakamura K, Attridge K, Manzotti C, Schmidt EM, et al. Trans-endocytosis of cd80 and cd86: A molecular basis for the cell-extrinsic function of ctla-4. Science. (2011) 332:600–3. doi: 10.1126/science.1202947
64. Nandi D, Pathak S, Verma T, Singh M, Chattopadhyay A, Thakur S, et al. T cell costimulation, checkpoint inhibitors and anti-tumor therapy. J Biosci. (2020) 45. doi: 10.1007/s12038-020-0020-2
65. Hodi FS, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Cowey CL, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (Checkmate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. (2018) 19:1480–92. doi: 10.1016/s1470-2045(18)30700-9
66. Baas P, Scherpereel A, Nowak AK, Fujimoto N, Peters S, Tsao AS, et al. First-line nivolumab plus ipilimumab in unresect able Malignant pleural mesothelioma (Checkmate 743): A multicentre, randomised, open-label, phase 3 trial. Lancet. (2021) 397:375–86. doi: 10.1016/s0140-6736(20)32714-8
67. Yau T, Kang YK, Kim TY, El-Khoueiry AB, Santoro A, Sangro B, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the checkmate 040 randomized clinical trial. JAMA Oncol. (2020) 6:e204564. doi: 10.1001/jamaoncol.2020.4564
68. Wei SC, Anang NAS, Sharma R, Andrews MC, Reuben A, Levine JH, et al. Combination anti-ctla-4 plus anti-pd-1 checkpoint blockade utilizes cellular mechanisms partially distinct from monotherapies. Proc Natl Acad Sci U.S.A. (2019) 116:22699–709. doi: 10.1073/pnas.1821218116
69. Strosberg J, El-Haddad G, Wolin E, Hendifar A, Yao J, Chasen B, et al. Phase 3 trial of (177)Lu-dotatate for midgut neuroendocrine tumors. N Engl J Med. (2017) 376:125–35. doi: 10.1056/NEJMoa1607427
70. Patel SP, Othus M, Chae YK, Giles FJ, Hansel DE, Singh PP, et al. A phase ii basket trial of dual anti-ctla-4 and anti-pd-1 blockade in rare tumors (Dart swog 1609) in patients with nonpancreatic neuroendocrine tumors. Clin Cancer Res. (2020) 26:2290–6. doi: 10.1158/1078-0432.Ccr-19-3356
71. Powles T, van der Heijden MS, Castellano D, Galsky MD, Loriot Y, Petrylak DP, et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectab le, locally advanced or metastatic urothelial carcinoma (Danube): A randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. (2020) 21:1574–88. doi: 10.1016/s1470-2045(20)30541-6
72. Ferris RL, Haddad R, Even C, Tahara M, Dvorkin M, Ciuleanu TE, et al. Durvalumab with or without tremelimumab in patients with recurrent or metastatic head and neck squamous cell carcinoma: eagle, a randomized, open-label phase iii study. Ann Oncol. (2020) 31:942–50. doi: 10.1016/j.annonc.2020.04.001
73. Goldman JW, Dvorkin M, Chen Y, Reinmuth N, Hotta K, Trukhin D, et al. Durvalumab, with or without tremelimumab, plus Platinum-Etoposide Versus Platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (Caspian): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. (2021) 22:51–65. doi: 10.1016/s1470-2045(20)30539-8
74. Cho BC, Abreu DR, Hussein M, Cobo M, Patel AJ, Secen N, et al. Tiragolumab plus atezolizumab versus placebo plus atezolizumab as a first-line treatment for pd-L1-selected non-small-cell lung cancer (Cityscape): primary and follow-up analyses of a randomised, double-blind, phase 2 study. Lancet Oncol. (2022) 23:781–92. doi: 10.1016/s1470-2045(22)00226-1
75. Harding JJ, Moreno V, Bang YJ, Hong MH, Patnaik A, Trigo J, et al. Blocking tim-3 in treatment-refractory advanced solid tumors: A phase ia/B study of ly3321367 with or without an anti-pd-L1 antibody. Clin Cancer Res. (2021) 27:2168–78. doi: 10.1158/1078-0432.Ccr-20-4405
76. Curigliano G, Gelderblom H, Mach N, Doi T, Tai D, Forde PM, et al. Phase I/ib clinical trial of sabatolimab, an anti-tim-3 antibody, alone and in combination with spartalizumab, an anti-pd-1 antibody, in advanced solid tumors. Clin Cancer Res. (2021) 27:3620–9. doi: 10.1158/1078-0432.Ccr-20-4746
77. Hollebecque A, Chung HC, de Miguel MJ, Italiano A, Machiels JP, Lin CC, et al. Safety and antitumor activity of α-pd-L1 antibody as monotherapy or in combination with α-tim-3 antibody in patients with microsatellite instability-high/mismatch repair-deficient tumors. Clin Cancer Res. (2021) 27:6393–404. doi: 10.1158/1078-0432.Ccr-21-0261
78. Chen J, Amoozgar Z, Liu X, Aoki S, Liu Z, Shin SM, et al. Reprogramming the intrahepatic cholangiocarcinoma immune microenvironment by chemotherapy and ctla-4 blockade enhances anti-pd-1 therapy. Cancer Immunol Res. (2024) 12:400–12. doi: 10.1158/2326-6066.Cir-23-0486
79. Sugai M, Amino Y, Fujishima S, Nibuya K, Iso H, Ito M, et al. Impact of immune-related adverse event severity on overall survival in patients with advanced nsclc receiving immune checkpoint inhibitors therapy, with a focus on combination regimens. Lung Cancer. (2025) 204:108555. doi: 10.1016/j.lungcan.2025.108555
80. Wang X, Li J, Chen R, Li T, and Chen M. Active ingredients from chinese medicine for combination cancer therapy. Int J Biol Sci. (2023) 19:3499–525. doi: 10.7150/ijbs.77720
81. Yang C, Li D, Ko CN, Wang K, and Wang H. Active ingredients of traditional chinese medicine for enhancing the effect of tumor immunotherapy. Front Immunol. (2023) 14:1133050. doi: 10.3389/fimmu.2023.1133050
82. Wang Y, Zhang Q, Chen Y, Liang CL, Liu H, Qiu F, et al. Antitumor effects of immunity-enhancing traditional chinese medicine. BioMed Pharmacother. (2020) 121:109570. doi: 10.1016/j.biopha.2019.109570
83. Lin S, An X, Guo Y, Gu J, Xie T, Wu Q, et al. Meta-analysis of astragalus-containing traditional chinese medicine combined with chemotherapy for colorectal cancer: efficacy and safety to tumor response. Front Oncol. (2019) 9:749. doi: 10.3389/fonc.2019.00749
84. Chen Y, Han H, Cheng J, Cheng Q, Zhu S, Zhan P, et al. Efficacy and safety of anti-pd-1/pd-L1-based dual immunotherapies versus pd-1/pd-L1 inhibitor alone in patients with advanced solid tumor: A systematic review and meta-analysis. Cancer Immunol Immunother. (2024) 73:155. doi: 10.1007/s00262-024-03734-1
85. Vlavcheski F, O’Neill EJ, Gagacev F, and Tsiani E. Effects of berberine against pancreatitis and pancreatic cancer. Molecules. (2022) 27. doi: 10.3390/molecules27238630
86. Liu Y, Liu X, Zhang N, Yin M, Dong J, Zeng Q, et al. Berberine diminishes cancer cell pd-L1 expression and facilitates antitumor immunity via inhibiting the deubiquitination activity of csn5. Acta Pharm Sin B. (2020) 10:2299–312. doi: 10.1016/j.apsb.2020.06.014
87. Huang J, Liu D, Wang Y, Liu L, Li J, Yuan J, et al. Ginseng polysaccharides alter the gut microbiota and kynurenine/tryptophan ratio, potentiating the antitumour effect of antiprogrammed cell death 1/programmed cell death ligand 1 (Anti-pd-1/pd-L1) immunotherapy. Gut. (2022) 71:734–45. doi: 10.1136/gutjnl-2020-321031
88. Xie J, Huang H, Li X, Ouyang L, Wang L, Liu D, et al. The role of traditional chinese medicine in cancer immunotherapy: current status and future directions. Am J Chin Med. (2023) 51:1627–51. doi: 10.1142/s0192415x2350074x
89. Wu X, Xia J, Wang Z, Xu Z, Liu K, Fu X, et al. Feiyanning downregulating cxcls/cxcr2 axis to suppress tans infiltration in the prevention of lung cancer metastasis. J Ethnopharmacol. (2022) 295:115277. doi: 10.1016/j.jep.2022.115277
90. Li S, Sun Y, Huang J, Wang B, Gong Y, Fang Y, et al. Anti-tumor effects and mechanisms of astragalus membranaceus (Am) and its specific immunopotentiation: status and prospect. J Ethnopharmacol. (2020) 258:112797. doi: 10.1016/j.jep.2020.112797
91. Feng X, Li Z, Guo W, and Hu Y. The effects of traditional chinese medicine and dietary compounds on digestive cancer immunotherapy and gut microbiota modulation: A review. Front Immunol. (2023) 14:1087755. doi: 10.3389/fimmu.2023.1087755
92. Li J, Fan S, Li H, Hu Z, and Hu Q. Evaluation of efficacy, safety and underlying mechanism on traditional chinese medicine as synergistic agents for cancer immunotherapy: A preclinical systematic review and meta-analysis. J Ethnopharmacol. (2025) 338:119035. doi: 10.1016/j.jep.2024.119035
93. Deng L, Shi Y, Liu P, Wu S, Lv Y, Xu H, et al. Gegen qinlian decoction alleviate influenza virus infectious pneumonia through intestinal flora. BioMed Pharmacother. (2021) 141:111896. doi: 10.1016/j.biopha.2021.111896
94. Yu D, Yang P, Lu X, Huang S, Liu L, and Fan X. Single-cell rna sequencing reveals enhanced antitumor immunity after combined application of pd-1 inhibitor and shenmai injection in non-small cell lung cancer. Cell Commun Signal. (2023) 21:169. doi: 10.1186/s12964-023-01184-3
95. Shao Y, Zhu W, Da J, Xu M, Wang Y, Zhou J, et al. Bisdemethoxycurcumin in combination with α-pd-L1 antibody boosts immune response against bladder cancer. Onco Targets Ther. (2017) 10:2675–83. doi: 10.2147/ott.S130653
96. Xu Q, Cheng W, Wei J, Ou Y, Xiao X, and Jia Y. Synergist for antitumor therapy: astragalus polysaccharides acting on immune microenvironment. Discov Oncol. (2023) 14:179. doi: 10.1007/s12672-023-00798-w
97. Li Q, Zhang C, Xu G, Shang X, Nan X, Li Y, et al. Astragalus polysaccharide ameliorates cd8(+) T cell dysfunction through stat3/gal-3/lag3 pathway in inflammation-induced colorectal cancer. BioMed Pharmacother. (2024) 171:116172. doi: 10.1016/j.biopha.2024.116172
98. Rong Y, Wang J, Hu T, Shi Z, Lang C, Liu W, et al. Ginsenoside Rg1 Regulates Immune Microenvironment and Neurological Recovery after Spinal Cord Injury through Mycbp2 Delivery Via Neuronal Cell-Derived Extracellular Vesicles. Adv Sci (Weinh). (2024) 11:e2402114. doi: 10.1002/advs.202402114
99. Wei J, Liu Z, He J, Liu Q, Lu Y, He S, et al. Traditional chinese medicine reverses Cancer Multidrug Resistance and Its Mechanism. Clin Transl Oncol. (2022) 24:471–82. doi: 10.1007/s12094-021-02716-4
100. Zhang X, Qiu H, Li C, Cai P, and Qi F. The Positive Role of Traditional chinese medicine as an adjunctive therapy for cancer. Biosci Trends. (2021) 15:283–98. doi: 10.5582/bst.2021.01318
101. Shao G, Liu Y, Lu L, Wang L, Ji G, and Xu H. Therapeutic potential of traditional chinese medicine in the prevention and treatment of digestive inflammatory cancer transformation: portulaca oleracea L. As a promising drug. . J Ethnopharmacol. (2024) 327:117999. doi: 10.1016/j.jep.2024.117999
102. Luo H, Vong CT, Chen H, Gao Y, Lyu P, Qiu L, et al. Naturally occurring anti-cancer compounds: shining from chinese herbal medicine. Chin Med. (2019) 14:48. doi: 10.1186/s13020-019-0270-9
103. Song D, Hou S, Ma N, Yan B, and Gao J. Efficacy and safety of pd-1/pd-L1 and ctla-4 immune checkpoint inhibitors in the treatment of advanced colorectal cancer: A systematic review and meta-analysis. Front Immunol. (2024) 15:1485303. doi: 10.3389/fimmu.2024.1485303
104. Jin C, Zhu X, Huang X, Gong T, Wei Z, and You J. Efficacy and safety of pd-1/pd-L1 and ctla-4 immune checkpoint inhibitors in colorectal cancer: A meta-analysis. J Comp Eff Res. (2022) 11:203–12. doi: 10.2217/cer-2021-0134
105. Hellmann MD, Rizvi NA, Goldman JW, Gettinger SN, Borghaei H, Brahmer JR, et al. Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (Checkmate 012): results of an open-label, phase 1, multicohort study. Lancet Oncol. (2017) 18:31–41. doi: 10.1016/s1470-2045(16)30624-6
106. Ready N, Hellmann MD, Awad MM, Otterson GA, Gutierrez M, Gainor JF, et al. First-line nivolumab plus ipilimumab in advanced non-small-cell lung cancer (Checkmate 568): outcomes by programmed death ligand 1 and tumor mutational burden as biomarkers. J Clin Oncol. (2019) 37:992–1000. doi: 10.1200/jco.18.01042
107. Hellmann MD, Paz-Ares L, Bernabe Caro R, Zurawski B, Kim SW, Carcereny Costa E, et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. (2019) 381:2020–31. doi: 10.1056/NEJMoa1910231
108. Antonia SJ, López-Martin JA, Bendell J, Ott PA, Taylor M, Eder JP, et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (Checkmate 032): A multicentre, open-label, phase 1/2 trial. Lancet Oncol. (2016) 17:883–95. doi: 10.1016/s1470-2045(16)30098-5
109. Kaseb AO, Hasanov E, Cao HST, Xiao L, Vauthey JN, Lee SS, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resect able hepatocellular carcinoma: A randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. (2022) 7:208–18. doi: 10.1016/s2468-1253(21)00427-1
110. Alden SL, Lim M, Kao C, Shu D, Singal AG, Noonan A, et al. Salvage ipilimumab plus nivolumab after anti-pd-1/pd-L1 therapy in advanced hepatocellular carcinoma. Cancer Res Commun. (2023) 3:1312–7. doi: 10.1158/2767-9764.Crc-23-0072
111. Amaria RN, Reddy SM, Tawbi HA, Davies MA, Ross MI, Glitza IC, et al. Neoadjuvant immune checkpoint blockade in high-risk resect able melanoma. Nat Med. (2018) 24:1649–54. doi: 10.1038/s41591-018-0197-1
112. Olson DJ, Eroglu Z, Brockstein B, Poklepovic AS, Bajaj M, Babu S, et al. Pembrolizumab plus ipilimumab following anti-pd-1/L1 failure in melanoma. J Clin Oncol. (2021) 39:2647–55. doi: 10.1200/jco.21.00079
113. Zhang L, Sun L, Zhou Y, Yu J, Lin Y, Wasan HS, et al. Association of survival and immune-related adverse events with anti-pd-1/pd-L1 and anti-ctla-4 inhibitors, alone or their combination for the treatment of cancer: A systematic review and meta-analysis of 13 clinical trials. Front Oncol. (2021) 11:575457. doi: 10.3389/fonc.2021.575457
114. Hamid O, Lewis KD, Weise A, McKean M, Papadopoulos KP, Crown J, et al. Phase I study of fianlimab, a human lymphocyte activation gene-3 (Lag-3) monoclonal antibody, in combination with cemiplimab in advanced melanoma. J Clin Oncol. (2024) 42:2928–38. doi: 10.1200/jco.23.02172
115. Mi S, Chen Z, Luo J, and Zheng W. Clinical effect analysis of yifei fuzheng anti -tumor decoction combined with sintilizumab and pemetrexed in the treatment of advanced non - squamous non-small cell lung cancer. China Modern Doctor. (2021) 59:87–91.
116. Zhang C, Fang C, and Zhu L. Clinical efficacy of 7hengyuan capsule combined with sintilimab in treatment of advanced non-small cell lung cancer. Jiangsu Med J. (2022) 48:586–9.
117. Li X, Cui Y, Yao Z, and Li Q. Clinical study on Replenishing qi and nourishing yin method combined with sintilizumab injection and chemotherapy in the treatment of advanced non-small cell lung cancer. Guangming J Chin Med. (2022) 37:2675–8.
118. Liu M and Ma Y. Clinical effect and safety of compound kushen injection combined with atilizumab in the second-line treatment of advanced non-squamous carcinoma non-small cell lung cancer. Chin J Clin National Drug Use. (2022) 15:15–8.
119. Liu S, Yuan K, and You J. Clinical study of compound kushen injection combined with navulizumab in treatment of advanced non-small cell lung cancer. Drugs Clinic. (2025) 40:161–5.
120. Zhu S, Zhang T, and Wang J. Clinical efficacy of bazhen huaji decoction combined with camrelizumab in the treatment of advanced esophageal cancer. Acta Chin Med Pharmacol. (2025) 53:77–82.
121. Guo L, Wang J, Feng W, and Lin R. Clinical observation of bevacizumab combined with huangqi zhishi decoction in treating ovarian epithelial carcinoma. CHINA’S NATUROPATHY. (2023) 31:84–7.
Keywords: immune checkpoint, combination therapy, PD-1/PD-L1, traditional Chinese medicine (TCM), immune-related adverse events (IRAE)
Citation: Tong C, Wu Y and Wu R (2025) New dimensions of PD-1/PD-L1 inhibitor combination therapy in cancer treatment: current advances and future perspectives. Front. Immunol. 16:1616872. doi: 10.3389/fimmu.2025.1616872
Received: 23 April 2025; Accepted: 14 August 2025;
Published: 27 August 2025.
Edited by:
Zhongbao Zhou, Capital Medical University, ChinaReviewed by:
Chang Liu, University of Rhode Island, United StatesSatomi Ando, Cincinnati Children’s Hospital Medical Center, United States
Copyright © 2025 Tong, Wu and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renzhao Wu, V3VmZW5nMDNAMTI2LmNvbQ==
†These authors have contributed equally to this work and share first authorship