 Jia-Jing Zheng
Jia-Jing Zheng Zhi-Fei Wu1
Zhi-Fei Wu1 Yi-Bing Hu
Yi-Bing Hu- 1Department of Pediatrics, Beilun District People’s Hospital, Ningbo, Zhejiang, China
- 2Department of Gastroenterology, Affiliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang, China
Background: Children with inflammatory bowel disease (IBD) have a higher risk of cancer due to prolonged exposure to chronic inflammation and immunosuppressive therapies.
Methods: A comprehensive review of extant literature was performed. Findings: The cancer landscape in pediatric IBD is complex, with colorectal cancer, small intestine cancer, lymphoma, cholangiocarcinoma/hepatocellular carcinoma, and skin cancer being predominant concerns. The underlying pathogenic mechanisms involve genomic instability induced by chronic inflammation, carcinogenic effects of immunosuppressants, and environmental factors (e.g., high-fat diet and air pollution). Effective cancer surveillance is crucial in mitigating risk. Strategies include early endoscopic monitoring for high-risk populations, routine dermatological assessments, and clinical monitoring for tumor-related symptoms.
Conclusion: This review synthesizes current evidence on the epidemiological characteristics, pathogenic mechanisms, and clinical management strategies for IBD-related malignancies in children. An in-depth characterization of the mechanisms by which pediatric IBD contributes to tumorigenesis is essential for developing surveillance protocols and advancing research to reduce tumor-associated morbidity.
Introduction
Inflammatory bowel disease (IBD) refers to a group of chronic, immune-mediated inflammatory disorders, primarily Crohn’s disease (CD) and ulcerative colitis (UC), which can affect multiple organ systems and tissues in the body (1, 2). Despite the advances in management, IBD remains incurable, and the disease course is marked by recurrent episodes of remission and relapse (3). The persistent or progressive inflammation associated with IBD can lead to various complications beyond the gastrointestinal tract, with malignancy being a major concern (4). The incidence of pediatric IBD has shown a steady increase in recent years, and younger age at onset is associated with a heavier disease burden (5). Consequently, the risk of malignancy in pediatric IBD patients is a major concern. Compared to adults with IBD, children are exposed to chronic inflammation for a longer duration, predisposing them to an increased risk of tumor development (6). In addition, pediatric patients often require prolonged and more intensive treatment regimens, potentially contributing to carcinogenesis. Pediatric IBD-associated malignancies include gastrointestinal malignancies (such as colorectal tumors, small intestinal tumors, and cholangiocarcinoma) and extraintestinal malignancies (such as lymphoma and skin cancer) (7–9). The present review aims to enhance the awareness among clinicians, particularly pediatric specialists, regarding the diagnosis and management of malignancies in children with IBD. It systematically summarizes the epidemiological characteristics and potential pathogenic mechanisms underlying IBD-associated malignancies in pediatric patients. A comprehensive overview of preventive and therapeutic strategies is also provided to facilitate clinical decision-making and improve patient outcomes.
Cancer risk in pediatric patients with IBD
Colorectal cancer
Epidemiology
Colorectal cancer (CRC) is the most common malignancy in pediatric IBD, mirroring trends observed in adults, where IBD confers a 1.40–1.70-fold higher risk due to chronic inflammation (10) (Figure 1). A meta-analysis of 20 studies (40,547 patients, 1965–2008) reported CRC as the most frequent malignancy in CD, with an incidence rate of 0.50 per 1,000 person-years—2–3 times higher than in the general population and occurring ~20 years earlier (mean age: 51.5 years), though still lower than in UC (11). There is a relative paucity of data on children in this regard.
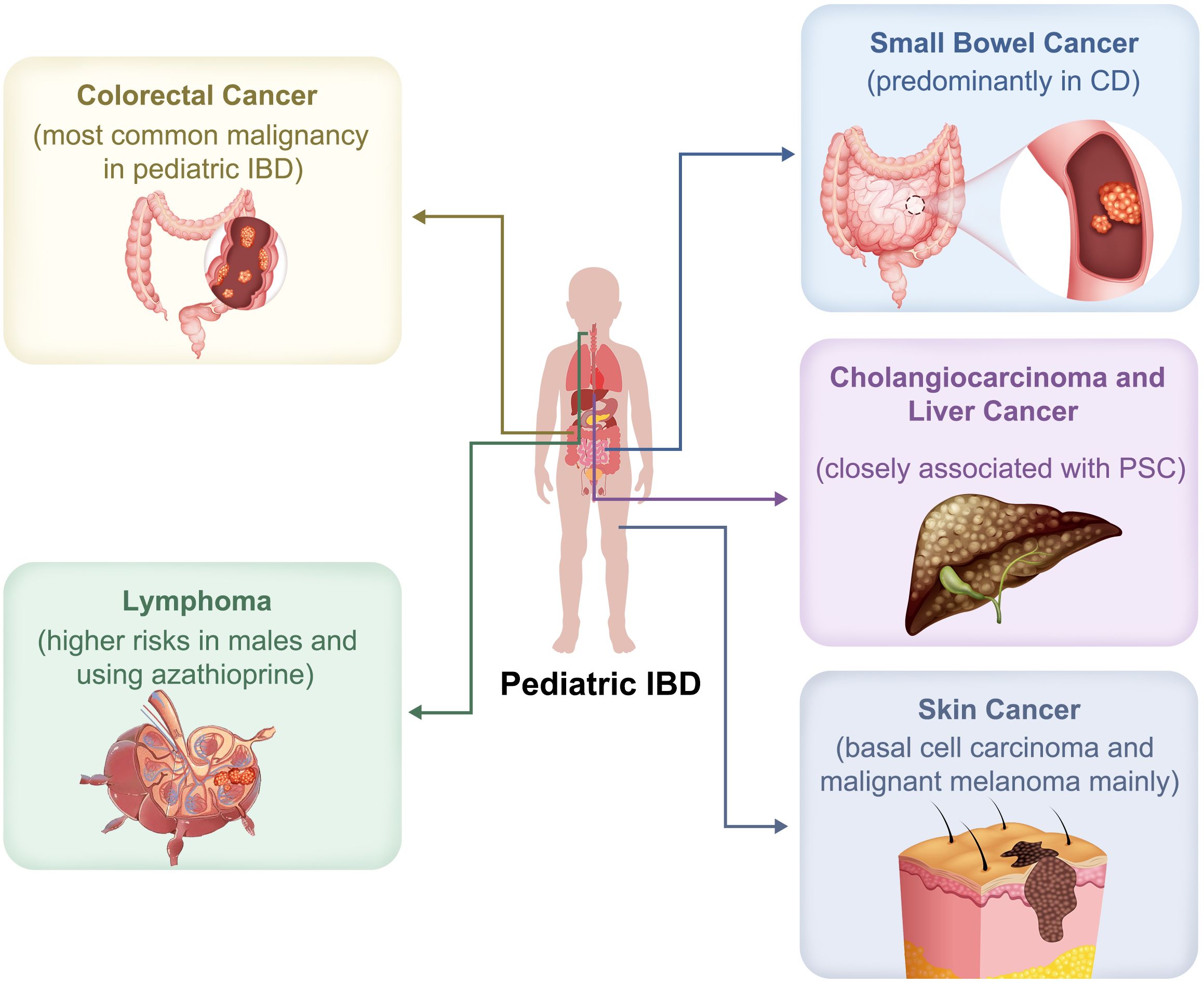
Figure 1. Spectrum of malignancies associated with pediatric inflammatory bowel disease (IBD). Pediatric IBD is associated with an increased risk of various malignancies. Colorectal cancer is the most common. Small bowel cancer occurs predominantly in Crohn’s disease (CD). Lymphoma risk is especially increased in males and those receiving azathioprine. Cholangiocarcinoma and liver cancer are closely linked to primary sclerosing cholangitis (PSC). Skin cancers associated with pediatric IBD include basal cell carcinoma and malignant melanoma.
Risk factors
A Swedish nationwide cohort study of 9,405 pediatric-onset IBD patients (1964–2014) found a markedly elevated gastrointestinal cancer risk (HR: 18.00, 95% CI: 14.40–22.70), particularly CRC (HR: 33.30 for UC, 5.08 for CD), which did not decline over time (12). Long-standing colitis and coexisting primary sclerosing cholangitis (PSC) were key risk factors (12). In a follow-up study, pediatric-onset UC was associated with a significantly higher CRC risk (adjusted HR [aHR]: 37.00 [95% CI: 25.10–54.40]) compared to adult-onset UC (HR: 1.32–1.88) (13). Similar findings have been reported for pediatric-onset CD (14). A Danish–Swedish registry study (1969–2017) involving 6,937 CD patients and 8,514 UC patients (<18 years) showed CRC risk ratios of 6.46 (95% CI: 3.95–10.60) in CD and 32.50 (95% CI: 23.00–45.90) in UC. Risk was highest in colonic CD (L2) (HR: 17.90) and extensive UC (E3/E4) (HR: 36.30, 95% CI: 22.80–57.80), especially with comorbid PSC or younger IBD onset. However, the absence of endoscopic and laboratory data and small CRC case numbers limit these findings (15). Another large cohort study (Pediatric PSC Consortium; n = 509) assessed CRC/dysplasia in pediatric PSC-UC or unclassified IBD (IBD-U) patients (16). The incidence was 2.80 CRC/dysplasia cases per 1,000 person-years (cumulative probability: 0.80% at 5 years and 4.80% at 10 years). Eight patients (1.60%) developed CRC or dysplasia; five were detected via surveillance colonoscopy, and three post-colectomy due to refractory colitis. Half of these patients had very early-onset IBD (VEO-IBD, <6 years), with a significantly higher incidence (5.80 vs. 1.80 per 1,000 person-years, HR: 3.40), underscoring the need for intensified CRC surveillance in this subgroup.
Onset time and cancer types
A Korean retrospective study (2000–2020) of 443 pediatric IBD patients reported four CRC cases (all male) (incidence: 1.29 per 1,000 person-years) (17). Median age at IBD and CBC diagnoses were 11.50 years and 18.50 years, respectively. Most tumors arose in the sigmoid colon (3/4), with histological types including adenocarcinoma (n = 2), mucinous adenocarcinoma (n = 1), and signet-ring cell carcinoma (n = 1). All patients had received azathioprine (AZA, median: 2.27 years); one also received a TNF-α inhibitor. One patient developed peritoneal metastasis and died post-chemotherapy, while the remaining three had early-stage CRC managed surgically. The authors noted that early CRC onset may reflect prolonged inflammation and disease duration, though small sample size and lack of a control group limit conclusions.
Small bowel cancer
Epidemiology
Small bowel cancer is a rare but significant complication of IBD, predominantly affecting patients with CD (Figure 1). The exact etiology remains unclear (18). Laukoetter et al. (11) reported it as the second most common CD-associated malignancy (0.30/1,000 person-years). However, the true incidence may be underestimated due to subclinical presentation and limited access to small bowel imaging. A Danish–Swedish cohort (1969–2017) showed a markedly elevated risk in CD (aHR: 9.09) and mortality (aHR: 6.59), while UC patients had a lower, but still increased risk (aHR: 1.85 for incidence; 1.57 for mortality) (19). Limited data analysis exists regarding children.
Risk factors and cancer types
Among the CD patients, adenocarcinoma predominated (aHR: 15.80), especially in the ileum and jejunum (50% of cases), followed by neuroendocrine tumors (aHR: 5.51) and sarcomas (aHR: 4.04). Early-onset CD was a key risk factor. A meta-analysis of national registries from Sweden, Denmark, and Finland reported a significantly higher risk in pediatric-onset IBD (relative risk [RR]: 16.20), though the absolute incidence remained low (0.10/1,000 person-years) (20). Subgroup analyses were limited by small sample size and a focus on high-income Western countries. In a French cohort (n = 698), nine malignancies were reported, including one incidentally-detected small bowel carcinoid tumor following pathological examination of the appendectomy specimen (21). A 23-year study in Denmark and Finland (n=6,689) found an elevated standardized incidence ratio (SIR) for small bowel cancer (SIR: 21.80), especially in CD (SIR: 32.60); the increased risk in UC (SIR: 13.30) was not statistically significant. Only three small bowel cancer cases were reported, limiting broader conclusions (22).
Lymphoma
Epidemiology
Lymphoma, a heterogeneous group of lymphoproliferative disorders, can be classified into subtypes based on lymphocyte origin, clinical presentation, and prognosis (23). Available evidence suggests a higher risk of lymphoma in IBD patients, particularly those with CD, likely due to persistent, uncontrolled inflammation (Figure 1) (24, 25). A meta-analysis reported a significantly elevated risk of hematologic malignancies in pediatric IBD (RR: 3.10 [95% CI: 1.88–5.10]) compared to the general pediatric population (20), particularly in thiopurine-exposed patients and males (RR: 3.23), while the increased risk in females was not statistically significant (RR: 2.45). However, the findings were limited by a low proportion of thiopurine users and a Western-centric population. A nationwide cohort study in Israel (n = 3,944) reported four non-Hodgkin lymphoma (NHL) cases in pediatric IBD patients (incidence: 1.69 per 10,000 person-years), yielding an RR of 4.40 (95% CI: 1.00–19.60; p = 0.06) (26). CD patients had a significantly elevated risk (RR: 10.00, 95% CI: 1.03–100, p = 0.04), whereas UC patients did not. Overall, data pertaining to the pediatric population remains scarce.
Risk factors and cancer types
Thiopurine monotherapy or combination therapy with anti-TNFα agents was not found to be significantly associated with NHL risk. No hepatosplenic T-cell lymphoma (HSTCL) cases were reported. In contrast, a retrospective multicenter study by the Porto Pediatric IBD Working Group (2006–2011) across 20 European countries and Israel identified 18 malignancy cases in 44 pediatric IBD cases—67% with CD and 22% with UC (27). Hematologic malignancies predominated (n = 12), including HSTCL (three cases), Epstein-Barr virus (EBV)-associated lymphoma (three cases), Hodgkin lymphoma (four cases), and leukemia (two cases). Six cases were linked to long-term thiopurine use (>12 months), suggesting a potential therapy-related risk. Differences in study design and underreporting may explain inconsistencies with the previous Israeli study (27).
Cholangiocarcinoma and liver cancer
Epidemiology
Cholangiocarcinoma is a highly lethal malignancy with limited treatment options (28). Kaj-Carbaidwala et al. (29) investigated the timeline and clinical significance of cholangiocarcinoma development in pediatric-onset PSC patients with IBD. Out of 21 patients who developed cholangiocarcinoma, 38% were diagnosed within two years of the second diagnosis (PSC or IBD), and 75% within 14 years (median: 6.95 years). Nearly half (47%) were diagnosed between the ages of 14 and 25, highlighting the need for enhanced screening during the transition to adult care. However, these findings were partly based on retrospective case reports, warranting prospective validation.
Risk factors and cancer types
A Danish–Finnish case-control study (n = 6,689) identified seven cholangiocarcinoma cases among pediatric IBD patients—six in UC (mostly pancolitis), and one in CD with ileocecal disease (30). PSC was identified as a significant risk factor, present in 25% of cholangiocarcinoma cases versus 3.6% in controls. Use of immunosuppressants or biologics was not associated with increased risk. According to the International Agency for Research on Cancer (IARC), liver cancer remains a major global health burden (31). In pediatric-onset IBD, the relative risk of liver cancer is strikingly elevated (RR: 55.45 [95% CI: 19.59–156.99]), surpassing that of CRC (pRR = 20.29) and small intestinal cancer (pRR = 16.20), likely due to its association with PSC. Despite the low absolute incidence of liver cancer, the extraordinarily high RR underscores the need for close surveillance. However, a notable limitation of the study was the lack of distinction between hepatocellular carcinoma and cholangiocarcinoma subtypes, highlighting the need for further research to elucidate the specific risks and mechanisms involved (Figure 1) (20).
Skin cancer
Epidemiology
Skin involvement in IBD, presenting as extra-intestinal manifestations (EIM), has been linked to an increased risk of skin cancers, such as malignant melanoma and non-melanoma skin cancer (Figure 1) (32). A French study of 698 pediatric-onset IBD patients reported a 1.30% cancer incidence rate, in which two cases of basal cell carcinoma (BCC), which were primarily located on the abdomen and face, required local excision (21).
Risk factors and cancer types
A Danish–Finnish study found a 4.20-fold higher risk of skin cancer in pediatric IBD patients compared to the general population (SIR: 2.40–6.70), with significantly increased risk in CD (SIR: 6.70), but not UC (SIR: 2.20) (22). Of 17 total skin cancer cases, 10 were melanomas—predominantly in CD (n=7)—and 7 were BCCs (5 in CD, 2 in UC). A nationwide Danish cohort further confirmed elevated risks for both melanoma (HR: 2.01 [95% CI: 1.19–3.42]) and non-melanoma skin cancer (HR: 2.21 [95% CI: 1.49–3.28]) in pediatric-onset IBD (33). No association was observed with IBD subtype, thiopurine or TNF-α therapy, PSC, or history of colectomy.
Potential mechanisms of tumor risk
Chronic inflammation-driven carcinogenesis
Chronic inflammation promotes carcinogenesis by inducing variants and epigenetic alterations in key regulatory genes, disrupting normal cellular growth control (Figure 2) (34). Many basic experiments have corroborated these results. Chronic inflammation also drives oxidative stress and excessive lipid peroxidation, leading to elevated oxidase activity and increased production of reactive oxygen species (ROS) and reactive nitrogen species (RNS). These reactive intermediates cause DNA and mitochondrial damage, impair repair pathways, and inactivate tumor suppressor genes, thereby facilitating tumor development (35).
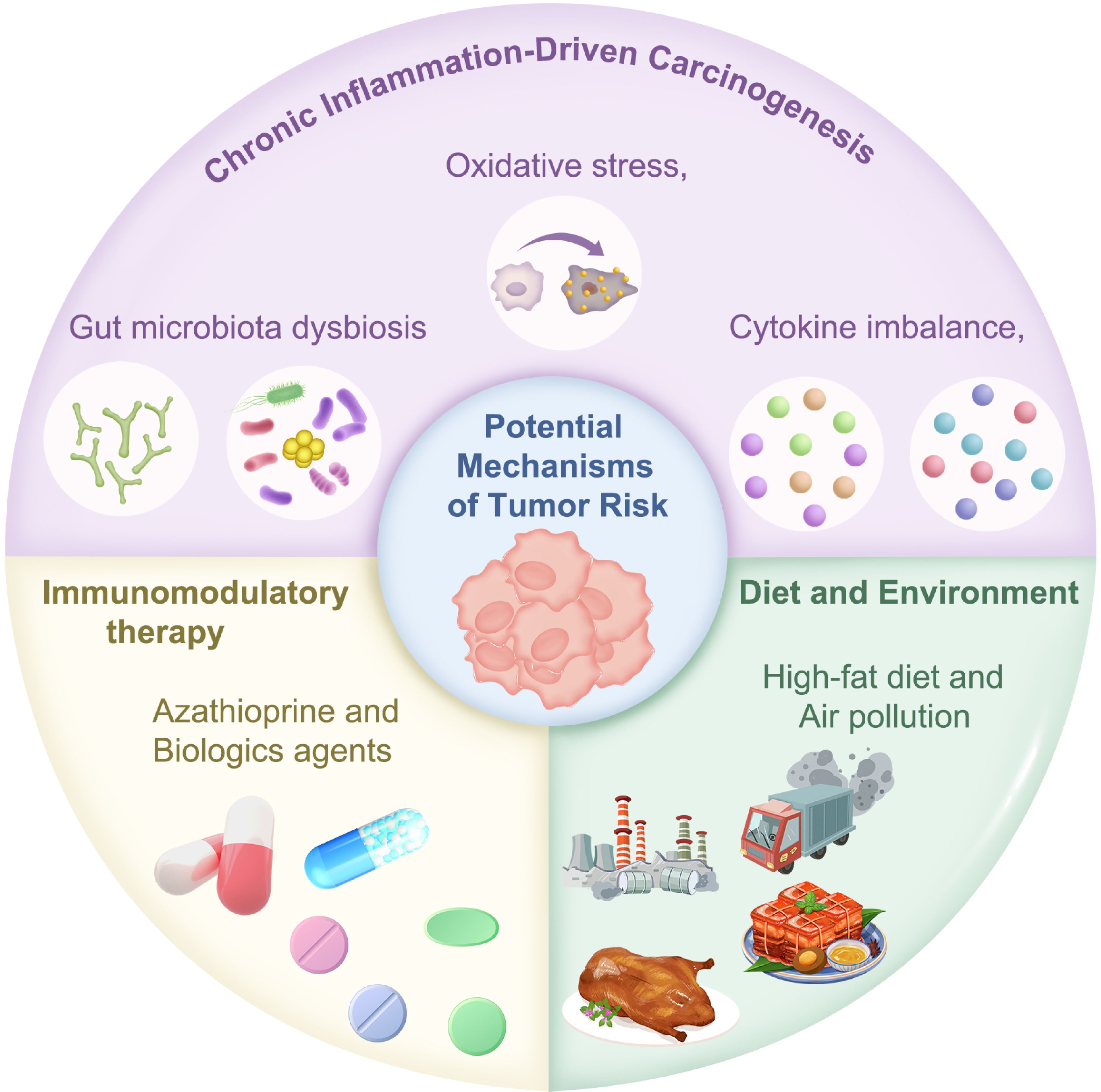
Figure 2. Potential mechanisms underlying tumor risk in pediatric inflammatory bowel disease (IBD). The pathogenesis of cancer in IBD involves genetic variants induced by chronic inflammation, carcinogenic effects of immunosuppressive agents, and environmental factors.
Inflammatory cytokines contribute to cancer development by inhibiting apoptosis, inducing angiogenesis, and disrupting normal inflammatory signaling (36). Chronic inflammation is marked by immune cell infiltration, which drives cytokine release and stress protein production, forming a microenvironment conducive to cancer development (37–39).
Key inflammatory mediators include proteases, arachidonic acid, cyclooxygenase, IL-4, IL-7, NF-κB, TNF-α, IFN-α, IL-1β, IL-8, and coagulation factors (40–42). Major stress proteins involved are heat shock proteins (HSPs) and glucose-regulated proteins (GRPs). Together, these molecules support tumor cell proliferation, survival, and metastasis, underpinning cancer initiation and progression (43–45).
The tumor suppressor gene p53 plays a central role in colitis-associated cancer (CAC), with early dysplastic changes commonly detected in colitis biopsies (46). These findings have been corroborated by numerous clinical studies. A meta-analysis of 19 studies by Lu et al. (47) reported a significantly higher p53 expression in UC patients compared to normal controls (OR: 3.14, p = 0.001), with higher expression in patients with dysplasia compared to those without dysplasia (OR: 10.76, p < 0.001). Although less pronounced, a significant difference in p53 expression was observed between UC cancer patients and patients with dysplasia (OR: 1.69, p = 0.035). Phosphoinositide 3-kinase (PI3K), a key signaling mediator in tumorigenesis, enhances cell migration, proliferation, and survival. Colon biopsies from UC and CAC patients revealed PI3K pathway activation, particularly involving the IL23R rs10889677 variant (c.309C>A), which was highly prevalent. Alterations in interleukin-12 receptor beta 1 (IL12Rβ1) were also detected in 20% of samples (48, 49). Other inflammation-driven carcinogenic pathways implicated in UC include Toll-like receptors, cyclooxygenases, carbonic anhydrases 2/9, and microRNAs (miRNAs), all contributing to neoplastic transformation (50–53). These findings have been obtained from clinical studies.
Regulatory T cells (Tregs) suppress excessive immune activation and self-inflicted tissue injury (54). However, Tregs exhibit plasticity, converting into Th17 cells that exacerbate inflammation. In UC, Tregs can paradoxically produce IL-1 and IL-6, serving as effector cells that contribute to UC and CAC pathogenesis (55, 56). Another mechanism involves neutrophil extracellular traps (NETs), formed via NETosis—a distinct cell death pathway triggered by pathogens, immune complexes, and ROS. This process involves the activation of NADPH oxidase, myeloperoxidase (MPO), and neutrophil elastase (NE), leading to chromatin decondensation and NET formation. UC patients show elevated levels of peptidyl arginine deiminase 4 (PAD4), MPO, and NE in the colonic mucosa, suggesting the important role of NETs in UC-related inflammation (57). Additionally, autophagy and macrophage-mediated immune regulation have been linked to the transition from chronic colitis to colon cancer (58).
Gut microbiota alterations contribute significantly to colitis-associated carcinogenesis. Probiotic modulation using Clostridium butyricum (CB) and Akkermansia muciniphila (AKK) reduced weight loss in a dextran sodium sulfate (DSS)-induced IBD mouse model. Furthermore, in the azoxymethane (AOM)/DSS-induced CAC mouse model, the combined probiotic treatment reduced tumor burden and Ki67 expression (a proliferation marker). Treatment also increased Caspase-3 activity (an apoptosis marker) and decreased CD8+ T cell and macrophage infiltration, enhancing anti-PD-L1 therapy efficacy (59). Xu et al. (60) identified Achromobacter pulmonis (A. pulmonis), isolated from mesenteric adipose tissue of CD patients, as a colitis-aggravating bacterium in mice. Its type III secretion system (T3SS) gene cluster induced macrophage and epithelial cell necrosis via the effector protein AopD, independent of caspase activation. Clinical studies have shown similar findings. Fecal samples from CD patients showed a significant abundance of Achromobacter and T3SS core genes compared to healthy individuals and patients with UC/CRC. Saussurea costus (SC) also showed therapeutic potential in a UC mouse model, alleviating weight loss, fecal occult blood, and colon shortening. SC restored colonic architecture, reduced inflammation, and modulated the gut microbiota, decreasing the abundance of harmful bacteria, such as Proteobacteria, and increasing beneficial bacteria, including Lactobacillus (lactic acid bacteria) and Firmicutes. This shift in microbial community structure suggested that the therapeutic effects of SC may be partly attributed to its ability to restore gut microbiota homeostasis (61).
Carcinogenic effects of immunosuppressive therapy
Immunomodulators (e.g., azathioprine [AZA], 6-mercaptopurine) and biologics, particularly TNF-α inhibitors, are cornerstone treatments for pediatric IBD (62–64). However, prolonged use of these medications may increase the risk of malignant tumors (Figure 2). Several results have been obtained from clinical studies.
AZA, an imidazole derivative of 6-mercaptopurine, suppresses nucleic acid biosynthesis and cell proliferation, potentially causing DNA damage. It is widely used for long-term IBD maintenance therapy, as it reduces disease activity, steroid dependence, relapse rates, and postoperative recurrence (65–67). However, the association between long-term AZA use and cancer risk remains debated. The following studies link AZA to fatal malignancies, including colorectal, skin, and hematologic cancers (68). A meta-analysis of 18 studies involving adult populations found that AZA significantly increases lymphoma risk, particularly in current users, with males having a higher risk than females. Thus, due caution should be exercised during long-term AZA treatment in elderly patients (>50 years) and young males (<30 years). Notably, 56% of lymphoma cases were EBV-positive, implicating immunosuppression-induced EBV reactivation as a possible mechanism (69). In contrast, a single-center retrospective study of 1,374 pediatric and young adult IBD patients identified only two lymphoma cases over 6,624 patient-years, both in males treated with thiopurines, but not biologics. No significant increase in lymphoma risk was observed in the subgroup of pediatric patients treated with thiopurine drugs (70). To some extent, lymphoma risk may reflect underlying IBD severity, with treatment benefits potentially outweighing the disease risks. Another meta-analysis of 27 studies (95,397 patients) found that AZA use was associated with a decreased risk of CRC. The analysis revealed a significant risk reduction, with case-control studies showing a 51% decrease in risk, and cohort studies revealing a slight 4% risk reduction. These data are derived from adult populations. Notably, AZA exhibited a chemopreventive effect in high-risk CRC patients with a longer disease course (>8 years). However, no protective effect was observed in patients with extensive colitis or concomitant PSC (71). Nonetheless, another meta-analysis revealed that AZA did not prevent progression from mild atypical dysplasia to severe atypical dysplasia or CRC in IBD patients (72). Since most of the present evidence is based on studies involving adult cohorts, more robust research is required to better characterize the carcinogenic effects of thiopurine drugs in pediatric populations.
TNF-α-inhibitors, such as infliximab and adalimumab, have revolutionized IBD treatment, enabling the achievement of clinical remission in patients with CD and UC (73, 74). These drugs neutralize pro-inflammatory TNF-α molecules, modulate intestinal immune responses, and promote mucosal healing (75). However, their long-term safety—particularly the potential malignancy risk in pediatric patients—remains a concern. A 2008 U.S. FDA report documented malignancies in children who received anti-TNF therapy for immune-related diseases (including IBD), prompting reduced AZA use in pediatric patients. Among 31 reported pediatric malignancy cases post-infliximab, 24 involved IBD patients. Notably, nine developed fatal HSTCL, while others developed NHL, Hodgkin lymphoma, or leukemia. Most IBD patients (20 of 24 patients) had received thiopurines; only four received methotrexate in combination (76). In contrast, basic research suggests that infliximab may reduce cancer risk. In a DSS-induced colitis mouse model, early intervention with infliximab significantly reduced CRC incidence from 75–80% to 16.7% (77). Supporting this, a 20-year U.S. cohort study (1999–2020) found that TNF antagonist use was associated with a significantly lower risk of CRC in IBD patients (adjusted OR: 0.69 for CD; 0.78 for UC) (78). A recent meta-analysis of 55 studies (57,518 patients) found no significant increase in overall cancer risk with TNF-α inhibitors—including adalimumab, infliximab, etanercept, certolizumab, and golimumab—in both interventional and observational studies (79). Although a trend toward increased risk emerged with long-term follow-up, most studies had short follow-up periods, highlighting the need for high-quality, long-term prospective studies to better assess malignancy risk and optimize adverse event monitoring (79).
Carcinogenic effects of diet and the environment
Environmental factors, such as diet, lifestyle, and air pollution, have also been implicated in the development of IBD (Figure 2). Long-term high-fat diet (HFD) consumption disrupts intestinal barrier homeostasis in mice, accelerating CRC progression by promoting a chronic inflammatory microenvironment (80). HFD-induced inflammation not only drives malignant transformation but may also create a self-sustaining pro-cancer loop. Animal experiments have demonstrated that prolonged HFD exposure induces low-grade chronic intestinal inflammation, impairs mucosal barrier function, and increases IBD risk (81). Epidemiological data further support a positive correlation between excessive fat intake and CAC incidence. Experimental models to elucidate the molecular pathways linking diet and CAC remain limited. Activation of the STAT3 transcription factor plays a crucial role in CAC by upregulating anti-apoptotic proteins like Bcl-2, correlating with the clinical and pathological features of CAC (82). Clinical studies have revealed increased levels of phosphorylated STAT3 (pSTAT3) in the intestinal epithelial cells of patients with CAC (83). While the mechanisms by which HFD exacerbates CRC via STAT3 remain unclear, cross-disease evidence suggests STAT3 signaling is central to HFD-induced tumorigenesis. Specifically, the amplification of STAT3-mediated pro-cancer signaling cascades warrants further exploration. Furthermore, HFDs contribute to CAC by altering gut microbiota’s butyrate metabolism. Research has demonstrated that HFDs reduce the abundance of butyrate-producing bacteria (e.g., Clostridiaceae), and lower intestinal butyrate levels, correlating with increased polyp formation (p = 0.007) and reduced ZO-1 expression (p = 0.004), a marker of epithelial barrier integrity. Notably, these carcinogenic effects were reversed by broad-spectrum antibiotics or butyrate supplementation, suggesting the microbiota’s role in CAC pathogenesis and supporting dietary or microbial interventions in high-risk IBD patients (84). A recent preclinical study demonstrated the anti-cancer properties of Bacteroides plebeius, a gut symbiont that degrades algal polysaccharides (85). In AOM/DSS-induced CRC mice, oral administration of B. plebeius reduced tumor number and size by 50% (p < 0.01), with less inflammatory infiltration in colon tissues. The proposed mechanism involves modulation of gut microbiota (increasing beneficial bacteria and decreasing pathogenic bacteria) and increased production of anti-cancer metabolites (e.g., propionate and ursodeoxycholic acid [UDCA]) (85).
The increasing incidence of IBD in newly industrialized countries is linked to environmental factors, particularly air pollution. Mendelian randomization analysis identified PM2.5 as a significant UC risk factor (86). A UK Bio-bank study of 453,199 individuals found that increased exposure to nitrogen oxides (Nox), nitrogen dioxide (NO2), PM2.5, and a composite pollution score increased UC risk by 20–26% per each interquartile range (IQR) increment, with stronger risk in populations with high genetic risk, unhealthy diets, smoking, obesity, or alcohol use. Epigenetic analysis revealed significant associations between UC risk and methylation changes in the CXCR2 gene (chemokine receptor), and the MHC III region (e.g., AGPAT1 and DDAH2). These changes were validated in colonic tissues and correlated with gene expression regulation (87). The latter two genes play a crucial role in colitis and CAC (88).
Screening and prevention strategies
Colorectal cancer surveillance
The incidence of dysplasia and CRC in pediatric patients with UC has been underreported, resulting in the lack of data to inform a defined CRC screening protocol. Moreover, discrepancies exist in screening recommendations among various guidelines. The ECCO-ESPGHAN guidelines recommend initiating endoscopic surveillance at 8-10 years after disease onset, based on individual risk factors (89), using chromoendoscopy performed by experienced gastroenterologists. While optimal surveillance intervals remain undefined, ECCO-ESPGHAN recommends universal screening at 10 years after disease onset, whereas Dutch guidelines recommend screening only in children with extensive colitis (89, 90). Due to the scarcity of pediatric data, CRC surveillance guidelines for children with UC are extrapolated from adult studies. In adults, routine surveillance is not recommended for ulcerative proctitis, given the comparable CRC risk to the general population (91, 92). However, pediatric guidelines remain inconsistent due to limited evidence. PSC is an established independent risk factor for dysplasia and CRC in children with UC. Consequently, both pediatric and adult UC guidelines recommend annual or biennial surveillance colonoscopies starting from the diagnosis of PSC (Figure 3) (89–91).
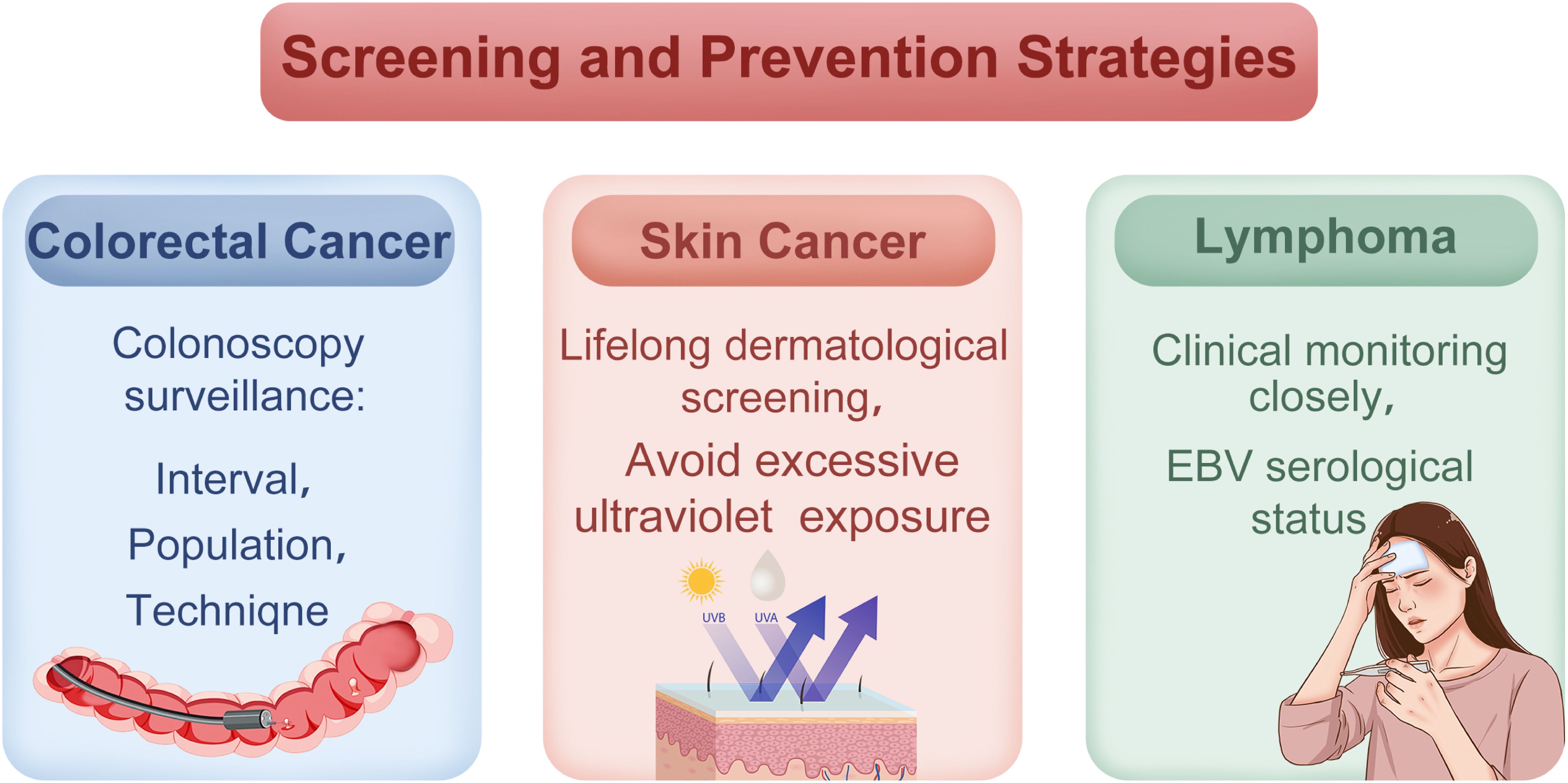
Figure 3. Cancer screening and prevention strategies in pediatric inflammatory bowel disease (IBD). Surveillance strategies include early colonoscopic monitoring, regular dermatological evaluations, and clinical monitoring for lymphoma-related symptoms in high-risk pediatric IBD patients.
Chromoendoscopy is the preferred surveillance method per guidelines, but limited access and expertise may hinder its use. As alternatives, the European guidelines recommend high-definition or white-light endoscopy combined with random biopsies as a suitable alternative. Furthermore, the Dutch adult IBD guidelines recommend white-light endoscopy with targeted biopsies (89, 91). Given technical limitations in pediatric settings, collaboration with experienced gastroenterologists is recommended. For high-risk groups, such as those with VEO-IBD or concurrent PSC, earlier and more frequent surveillance may be warranted.
Skin cancer surveillance
Given the elevated risk of skin cancer in pediatric IBD patients, especially those who have received AZA, anti-TNF therapies, or combination therapies, some researchers have recommended lifelong dermatological screening. Given the scarcity of data on the pediatric population, adult guidelines are used as a reference. The primary focus should be screening for basal cell carcinoma, melanoma, and non-melanoma skin cancers, with emphasis on ultraviolet (UV) protection (e.g., sunscreen use, minimizing UV exposure) (Figure 3) (21). Danish researchers suggest incorporating skin cancer surveillance into standard care, particularly for male patients. However, the optimal frequency and methods for screening remain undefined (22, 33).
Lymphoma surveillance
Adolescent males and patients on multiple immunosuppressants (e.g., AZA + anti-TNF) require close monitoring for lymphoma. Due to limited data on children, guidelines for adult populations are referenced. Persistent fever, lymphadenopathy, hepatosplenomegaly, or cytopenia warrant evaluation for lymphoma, with the diagnosis confirmed through imaging (e.g., computed tomography [CT]) and bone marrow biopsy (Figure 3) (27). EBV serology (IgM/IgG) should be assessed before and during treatment, as AZA may heighten lymphoma risk in EBV-positive patients (20, 26). For EBV-negative patients, EBV screening is recommended before initiating immunosuppressive therapy to assess lymphoma risk (26). Although no standardized protocol exists, regular clinical assessments are recommended every 6-12 months, with shorter intervals for high-risk groups.
Conclusion
Children with IBD have a significantly increased risk of developing malignancies due to chronic inflammation and immunosuppressive therapies. The incidence of cancer in this population is trending towards a younger onset. Common cancers include CRC (highest incidence, especially with PSC or extensive colitis), small bowel cancer (mainly in CD), lymphoma (notably in males and AZA users), cholangiocarcinoma/hepatocellular carcinoma (linked to PSC), and skin cancers (primarily basal cell carcinoma and malignant melanoma). The pathogenesis of cancer in IBD involves genetic variants induced by chronic inflammation, carcinogenic effects of immunosuppressive agents, and environmental factors (e.g., HFD and air pollution). Chronic inflammation drives tumorigenesis through oxidative stress, cytokine network imbalance, and gut microbiota dysbiosis, while immunomodulatory therapy, though effective in controlling inflammation, may increase the risk of lymphoma and other cancers. Early surveillance—colonoscopy, dermatologic exams, and lymphoma screening—is essential for high-risk groups, such as those with early-onset IBD or coexisting PSC. Most existing data are from small Western cohorts, highlighting the need for larger, prospective studies to refine cancer prevention and treatment strategies tailored to children with IBD.
Author contributions
J-JZ: Conceptualization, Data curation, Writing – original draft. Z-FW: Visualization, Writing – original draft. Y-BH: Writing – review & editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Science and Technology Plan Project of Jinhua Municipal Central Hospital (JY2020-6-06 to Yi-Bing Hu).
Acknowledgments
We thank Medjaden Inc. for scientific editing of this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Le Berre C, Honap S, and Peyrin-Biroulet L. Ulcerative colitis. Lancet. (2023) 402:571–84. doi: 10.1016/s0140-6736(23)00966-2
2. Dolinger M, Torres J, and Vermeire S. Crohn’s disease. Lancet. (2024) 403:1177–91. doi: 10.1016/s0140-6736(23)02586-2
3. Chauhan G and Rieder F. The pathogenesis of inflammatory bowel diseases. Surg Clin North Am. (2025) 105:201–15. doi: 10.1016/j.suc.2024.10.008
4. Gros B and Kaplan GG. Ulcerative colitis in adults: A review. Jama. (2023) 330:951–65. doi: 10.1001/jama.2023.15389
5. Kuenzig ME, Fung SG, Marderfeld L, Mak JWY, Kaplan GG, Ng SC, et al. Twenty-first century trends in the global epidemiology of pediatric-onset inflammatory bowel disease: systematic review. Gastroenterology. (2022) 162:1147–59.e4. doi: 10.1053/j.gastro.2021.12.282
6. El-Matary W and Bernstein CN. Cancer risk in pediatric-onset inflammatory bowel disease. Front Pediatr. (2020) 8:400. doi: 10.3389/fped.2020.00400
7. Faye AS, Holmer AK, and Axelrad JE. Cancer in inflammatory bowel disease. Gastroenterol Clin North Am. (2022) 51:649–66. doi: 10.1016/j.gtc.2022.05.003
8. Fanizza J, Bencardino S, Allocca M, Furfaro F, Zilli A, Parigi TL, et al. Inflammatory bowel disease and colorectal cancer. Cancers (Basel). (2024) 16:2943. doi: 10.3390/cancers16172943
9. Conceição D, Saraiva MR, Rosa I, and Claro I. Inflammatory bowel disease treatment in cancer patients-A comprehensive review. Cancers (Basel). (2023) 15:3130. doi: 10.3390/cancers15123130
10. Derks MEW, Te Groen M, van Lierop LMA, Murthy S, Rubin DT, Bessissow T, et al. Management of colorectal neoplasia in IBD patients: current practice and future perspectives. J Crohns Colitis. (2024) 18:1726–35. doi: 10.1093/ecco-jcc/jjae071
11. Laukoetter MG, Mennigen R, Hannig CM, Osada N, Rijcken E, Vowinkel T, et al. Intestinal cancer risk in Crohn’s disease: a meta-analysis. J Gastrointest Surg. (2011) 15:576–83. doi: 10.1007/s11605-010-1402-9
12. Olén O, Askling J, Sachs MC, Frumento P, Neovius M, Smedby KE, et al. Childhood onset inflammatory bowel disease and risk of cancer: a Swedish nationwide cohort study 1964-2014. Bmj. (2017) 358:j3951. doi: 10.1136/bmj.j3951
13. Olén O, Erichsen R, Sachs MC, Pedersen L, Halfvarson J, Askling J, et al. Colorectal cancer in ulcerative colitis: a Scandinavian population-based cohort study. Lancet. (2020) 395:123–31. doi: 10.1016/s0140-6736(19)32545-0
14. Olén O, Erichsen R, Sachs MC, Pedersen L, Halfvarson J, Askling J, et al. Colorectal cancer in Crohn’s disease: a Scandinavian population-based cohort study. Lancet Gastroenterol Hepatol. (2020) 5:475–84. doi: 10.1016/s2468-1253(20)30005-4
15. Everhov ÅH, Ludvigsson JF, Järås J, Erichsen R, Pedersen L, Halfvarson J, et al. Colorectal cancer in childhood-onset inflammatory bowel disease: A scandinavian register-based cohort study, 1969-2017. J Pediatr Gastroenterol Nutr. (2022) 75:480–4. doi: 10.1097/mpg.0000000000003574
16. El-Matary W, Guthery SL, Amir AZ, DiGuglielmo M, Draijer LG, Furuya KN, et al. Colorectal dysplasia and cancer in pediatric-onset ulcerative colitis associated with primary sclerosing cholangitis. Clin Gastroenterol Hepatol. (2021) 19:1067–70.e2. doi: 10.1016/j.cgh.2020.04.055
17. Kim MJ, Ko JS, Shin M, Hahn JW, Moon SY, Kim HY, et al. Colorectal Cancer associated with pediatric inflammatory bowel disease: a case series. BMC Pediatr. (2021) 21:504. doi: 10.1186/s12887-021-02966-9
18. Faggiani I, D’Amico F, Furfaro F, Zilli A, Parigi TL, Cicerone C, et al. Small bowel cancer in crohn’s disease. Cancers (Basel). (2024) 16:2901. doi: 10.3390/cancers16162901
19. Axelrad JE, Olén O, Sachs MC, Erichsen R, Pedersen L, Halfvarson J, et al. Inflammatory bowel disease and risk of small bowel cancer: a binational population-based cohort study from Denmark and Sweden. Gut. (2021) 70:297–308. doi: 10.1136/gutjnl-2020-320945
20. Elmahdi R, Lemser CE, Thomsen SB, Allin KH, Agrawal M, and Jess T. Development of cancer among patients with pediatric-onset inflammatory bowel disease: A meta-analysis of population-based studies. JAMA Netw Open. (2022) 5:e220595. doi: 10.1001/jamanetworkopen.2022.0595
21. Peneau A, Savoye G, Turck D, Dauchet L, Fumery M, Salleron J, et al. Mortality and cancer in pediatric-onset inflammatory bowel disease: a population-based study. Am J Gastroenterol. (2013) 108:1647–53. doi: 10.1038/ajg.2013.242
22. Malham M, Jakobsen C, Paerregaard A, Virta LJ, Kolho KL, and Wewer V. The incidence of cancer and mortality in paediatric onset inflammatory bowel disease in Denmark and Finland during a 23-year period: a population-based study. Aliment Pharmacol Ther. (2019) 50:33–9. doi: 10.1111/apt.15258
23. Farooqi HA, Saffi Ullah M, Raza A, Sadiq Z, Shaikh WA, Muhammad R, et al. Efficacy and safety of polatuzumab-vedotin plus bendamustine and rituximab in patients with relapsed/refractory diffuse large B-cell lymphoma: A systematic review and meta-analysis. Crit Rev Oncol Hematol. (2025) 207:104611. doi: 10.1016/j.critrevonc.2024.104611
24. Stasik K and Filip R. The complex relationship between mechanisms underlying inflammatory bowel disease, its treatment, and the risk of lymphomas: A comprehensive review. Int J Mol Sci. (2024) 25:4241. doi: 10.3390/ijms25084241
25. Biancone L, Armuzzi A, Scribano ML, Castiglione F, D’Incà R, Orlando A, et al. Cancer risk in inflammatory bowel disease: A 6-year prospective multicenter nested case-control IG-IBD study. Inflammation Bowel Dis. (2020) 26:450–9. doi: 10.1093/ibd/izz155
26. Atia O, Harel S, Ledderman N, Greenfeld S, Kariv R, Dotan I, et al. Risk of Cancer in Paediatric onset Inflammatory Bowel Diseases: A Nation-wide Study From the epi-IIRN. J Crohns Colitis. (2022) 16:786–95. doi: 10.1093/ecco-jcc/jjab205
27. de Ridder L, Turner D, Wilson DC, Koletzko S, Martin-de-Carpi J, Fagerberg UL, et al. Malignancy and mortality in pediatric patients with inflammatory bowel disease: a multinational study from the porto pediatric IBD group. Inflammation Bowel Dis. (2014) 20:291–300. doi: 10.1097/01.MIB.0000439066.69340.3c
28. Moris D, Palta M, Kim C, Allen PJ, Morse MA, and Lidsky ME. Advances in the treatment of intrahepatic cholangiocarcinoma: An overview of the current and future therapeutic landscape for clinicians. CA Cancer J Clin. (2023) 73:198–222. doi: 10.3322/caac.21759
29. Kaj-Carbaidwala B, Fevery J, Adler DG, Bergquist A, de Ridder L, Deneau M, et al. Determining the time to cholangiocarcinoma in pediatric-onset PSC-IBD. J Pediatr Gastroenterol Nutr. (2025) 80:450–4. doi: 10.1002/jpn3.12443
30. Malham M, Jansson S, Malmborg P, Olén O, Paerregaard A, Virta LJ, et al. Risk factors of cancer in pediatric-onset inflammatory bowel disease in Denmark and Finland. J Pediatr Gastroenterol Nutr. (2023) 77:55–61. doi: 10.1097/mpg.0000000000003781
31. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
32. Zhao Y, Shao Y, Zhou J, Pei J, Chong J, Lu C, et al. Erythema nodosum, Malignant melanoma and non-melanoma skin cancer in relation to inflammatory bowel disease: a Mendelian randomization study. Sci Rep. (2025) 15:1369. doi: 10.1038/s41598-025-85249-y
33. Kjærgaard VS, Jensen CB, Elmahdi R, Burisch J, Allin KH, and Jess T. Cancer risk in pediatric-onset inflammatory bowel disease: A population-based danish cohort study. Gastroenterology. (2020) 159:1609–11. doi: 10.1053/j.gastro.2020.06.030
34. Shahgoli VK, Noorolyai S, Ahmadpour Youshanlui M, Saeidi H, Nasiri H, Mansoori B, et al. Inflammatory bowel disease, colitis, and cancer: unmasking the chronic inflammation link. Int J Colorectal Dis. (2024) 39:173. doi: 10.1007/s00384-024-04748-y
35. Wen Y, Zhu Y, Zhang C, Yang X, Gao Y, Li M, et al. Chronic inflammation, cancer development and immunotherapy. Front Pharmacol. (2022) 13:1040163. doi: 10.3389/fphar.2022.1040163
36. Hajishengallis G, Netea MG, and Chavakis T. Trained immunity in chronic inflammatory diseases and cancer. Nat Rev Immunol. (2025) 497–514. doi: 10.1038/s41577-025-01132-x
37. Rubin R. White blood cells might provide clues to breast cancer risk. Jama. (2020) 323:1123. doi: 10.1001/jama.2020.2457
38. Hsu AY, Huang Q, Pi X, Fu J, Raghunathan K, Ghimire L, et al. Neutrophil-derived vesicles control complement activation to facilitate inflammation resolution. Cell. (2025) 188:1623–41.e26. doi: 10.1016/j.cell.2025.01.021
39. Li L, Xu T, and Qi X. Balanced regulation of ROS production and inflammasome activation in preventing early development of colorectal cancer. Immunol Rev. (2025) 329:e13417. doi: 10.1111/imr.13417
40. Cui L, Liu R, Han S, Zhang C, Wang B, Ruan Y, et al. Targeting arachidonic acid metabolism enhances immunotherapy efficacy in ARID1A-deficient colorectal cancer. Cancer Res. (2025) 85:925–41. doi: 10.1158/0008-5472.Can-24-1611
41. Dai T, Jia Y, and Zhang Y. Genetic evidence for the causal link between coagulation factors and the risk of ovarian cancer: A two-sample mendelian randomization study. Int J Womens Health. (2024) 16:1947–57. doi: 10.2147/ijwh.S482359
42. Rees PA, Castle J, Clouston HW, Lamb R, Singh U, Duff SE, et al. The effects of coagulation factors and their inhibitors on proliferation and migration in colorectal cancer. Cancer Med. (2023) 12:17184–92. doi: 10.1002/cam4.6332
43. Zhang H, Shi Y, Lin C, He C, Wang S, Li Q, et al. Overcoming cancer risk in inflammatory bowel disease: new insights into preventive strategies and pathogenesis mechanisms including interactions of immune cells, cancer signaling pathways, and gut microbiota. Front Immunol. (2023) 14:1338918. doi: 10.3389/fimmu.2023.1338918
44. Zhao R, Zhu X, Wei W, and Zhen L. The role of HSPA14 in breast cancer: implications for tumorigenesis, immune response modulation, and personalized therapies. Int J Hyperthermia. (2025) 42:2452922. doi: 10.1080/02656736.2025.2452922
45. Chierichetti M, Cristofani R, Crippa V, Ferrari V, Cozzi M, Casarotto E, et al. Small heat shock protein B8: from cell functions to its involvement in diseases and potential therapeutic applications. Neural Regener Res. (2025) 20:2872–86. doi: 10.4103/nrr.Nrr-d-24-00517
46. Gené M, Cuatrecasas M, Amat I, Veiga JA, Fernández Aceñero MJ, Fusté Chimisana V, et al. Alterations in p53, microsatellite stability and lack of MUC5AC expression as molecular features of colorectal carcinoma associated with inflammatory bowel disease. Int J Mol Sci. (2023) 24:8655. doi: 10.3390/ijms24108655
47. Lu X, Yu Y, and Tan S. p53 expression in patients with ulcerative colitis - associated with dysplasia and carcinoma: a systematic meta-analysis. BMC Gastroenterol. (2017) 17:111. doi: 10.1186/s12876-017-0665-y
48. Razali NN, Raja Ali RA, Muhammad Nawawi KN, Yahaya A, and Mokhtar NM. Targeted sequencing of cytokine-induced PI3K-related genes in ulcerative colitis, colorectal cancer and colitis-associated cancer. Int J Mol Sci. (2022) 23:11472. doi: 10.3390/ijms231911472
49. Yin Y, Wan J, Yu J, and Wu K. Molecular pathogenesis of colitis-associated colorectal cancer: immunity, genetics, and intestinal microecology. Inflammation Bowel Dis. (2023) 29:1648–57. doi: 10.1093/ibd/izad081
50. Lai CY, Yeh KY, Liu BF, Chang TM, Chang CH, Liao YF, et al. MicroRNA-21 plays multiple oncometabolic roles in colitis-associated carcinoma and colorectal cancer via the PI3K/AKT, STAT3, and PDCD4/TNF-α Signaling pathways in zebrafish. Cancers (Basel). (2021) 13:5565. doi: 10.3390/cancers13215565
51. Andoh A, Fujiyama Y, Yoshioka U, Sasaki M, Araki Y, Tsujikawa T, et al. Elevated serum anti-carbonic anhydrase II antibodies in patients with ulcerative colitis. Int J Mol Med. (2002) 9:499–502. doi: 10.3892/ijmm.9.5.499
52. Singer II, Kawka DW, Schloemann S, Tessner T, Riehl T, and Stenson WF. Cyclooxygenase 2 is induced in colonic epithelial cells in inflammatory bowel disease. Gastroenterology. (1998) 115:297–306. doi: 10.1016/s0016-5085(98)70196-9
53. Rafa H, Benkhelifa S, AitYounes S, Saoula H, Belhadef S, Belkhelfa M, et al. All-trans retinoic acid modulates TLR4/NF-κB signaling pathway targeting TNF-α and nitric oxide synthase 2 expression in colonic mucosa during ulcerative colitis and colitis associated cancer. Mediators Inflamm. (2017) 2017:7353252. doi: 10.1155/2017/7353252
54. Khalil RG, Mohammed DA, Hamdalla HM, and Ahmed OM. The possible anti-tumor effects of regulatory T cells plasticity/IL-35 in the tumor microenvironment of the major three cancer types. Cytokine. (2025) 186:156834. doi: 10.1016/j.cyto.2024.156834
55. Miyao T, Floess S, Setoguchi R, Luche H, Fehling HJ, Waldmann H, et al. Plasticity of Foxp3(+) T cells reflects promiscuous Foxp3 expression in conventional T cells but not reprogramming of regulatory T cells. Immunity. (2012) 36:262–75. doi: 10.1016/j.immuni.2011.12.012
56. Parang B, Barrett CW, and Williams CS. AOM/DSS model of colitis-associated cancer. Methods Mol Biol. (2016) 1422:297–307. doi: 10.1007/978-1-4939-3603-8_26
57. Dinallo V, Marafini I, Di Fusco D, Laudisi F, Franzè E, Di Grazia A, et al. Neutrophil extracellular traps sustain inflammatory signals in ulcerative colitis. J Crohns Colitis. (2019) 13:772–84. doi: 10.1093/ecco-jcc/jjy215
58. Jin X, You L, Qiao J, Han W, and Pan H. Autophagy in colitis-associated colon cancer: exploring its potential role in reducing initiation and preventing IBD-Related CAC development. Autophagy. (2024) 20:242–58. doi: 10.1080/15548627.2023.2259214
59. Hua D, Yang Q, Li X, Zhou X, Kang Y, Zhao Y, et al. The combination of Clostridium butyricum and Akkermansia muciniphila mitigates DSS-induced colitis and attenuates colitis-associated tumorigenesis by modulating gut microbiota and reducing CD8(+) T cells in mice. mSystems. (2025) 10:e0156724. doi: 10.1128/msystems.01567-24
60. Xu J, Li P, Li Z, Liu S, Guo H, Lesser CF, et al. Gut bacterial type III secretion systems aggravate colitis in mice and serve as biomarkers of Crohn’s disease. EBioMedicine. (2024) 107:105296. doi: 10.1016/j.ebiom.2024.105296
61. Pang WL, Li TG, Wang YY, Song LY, Li L, Li XY, et al. Saussurea costus alleviates ulcerative colitis by regulating the gut microbiota and improving intestinal barrier integrity. Front Cell Infect Microbiol. (2025) 15:1528578. doi: 10.3389/fcimb.2025.1528578
62. Colman RJ, Solitano V, MacDonald JK, Ma C, Griffiths AM, Jairath V, et al. Operating properties of disease activity indices in pediatric inflammatory bowel disease: A systematic review. Inflammation Bowel Dis. (2025) 31:220–45. doi: 10.1093/ibd/izae060
63. Roncoroni L, Gori R, Elli L, Tontini GE, Doneda L, Norsa L, et al. Nutrition in patients with inflammatory bowel diseases: A narrative review. Nutrients. (2022) 14:751. doi: 10.3390/nu14040751
64. Olbjørn C, Rove JB, and Jahnsen J. Combination of biological agents in moderate to severe pediatric inflammatory bowel disease: A case series and review of the literature. Paediatr Drugs. (2020) 22:409–16. doi: 10.1007/s40272-020-00396-1
65. Timmer A, McDonald JW, and Macdonald JK. Azathioprine and 6-mercaptopurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. (2007) 24:Cd000478. doi: 10.1002/14651858.CD000478.pub2
66. Chatterjee A, Bhatia P, Sinha SK, Singh AK, Mandavdhare HS, Shah J, et al. Effectiveness and safety of thiopurines in inflammatory bowel disease patients with NUDT15 polymorphism: a real-world retrospective study. Expert Rev Clin Pharmacol. (2025) 18:175–83. doi: 10.1080/17512433.2025.2465425
67. Strigáč A, Caban M, Małecka-Wojciesko E, and Talar-Wojnarowska R. Safety and effectiveness of thiopurines and small molecules in elderly patients with inflammatory bowel diseases. J Clin Med. (2024) 13:4678. doi: 10.3390/jcm13164678
68. Kreuz M, Cardoso JCO, Sobreira LER, Cavalcanti Souza ME, Campos LE, Kelly FA, et al. Azathioprine and risk of non-melanoma skin cancers in organ transplant recipients: a systematic review and update meta-analysis. Clin Transl Oncol. (2025) 27:3100–9. doi: 10.1007/s12094-024-03839-0
69. Kotlyar DS, Lewis JD, Beaugerie L, Tierney A, Brensinger CM, Gisbert JP, et al. Risk of lymphoma in patients with inflammatory bowel disease treated with azathioprine and 6-mercaptopurine: a meta-analysis. Clin Gastroenterol Hepatol. (2015) 13:847–58.e4. doi: 10.1016/j.cgh.2014.05.015
70. Ashworth LA, Billett A, Mitchell P, Nuti F, Siegel C, and Bousvaros A. Lymphoma risk in children and young adults with inflammatory bowel disease: analysis of a large single-center cohort. Inflammation Bowel Dis. (2012) 18:838–43. doi: 10.1002/ibd.21844
71. Zhu Z, Mei Z, Guo Y, Wang G, Wu T, Cui X, et al. Reduced risk of inflammatory bowel disease-associated colorectal neoplasia with use of thiopurines: a systematic review and meta-analysis. J Crohns Colitis. (2018) 12:546–58. doi: 10.1093/ecco-jcc/jjy006
72. Zeng J, Meng ZM, Huang XL, and Gan HT. Effects of 5-aminosalicylates or thiopurines on the progression of low-grade dysplasia in patients with inflammatory bowel disease: a systematic review and meta-analysis. Int J Colorectal Dis. (2021) 36:11–8. doi: 10.1007/s00384-020-03735-3
73. Yang X, He M, Tang Q, Wang Z, Jin D, Wu X, et al. Assessment of anti-inflammatory efficacy of acupuncture in patients with inflammatory bowel disease: A systematic review and meta-analysis. Complement Ther Med. (2023) 74:102946. doi: 10.1016/j.ctim.2023.102946
74. Souza RF, Caetano MAF, Magalhães HIR, and Castelucci P. Study of tumor necrosis factor receptor in the inflammatory bowel disease. World J Gastroenterol. (2023) 29:2733–46. doi: 10.3748/wjg.v29.i18.2733
75. Gareb B, Otten AT, Frijlink HW, Dijkstra G, and Kosterink JGW. Review: local tumor necrosis factor-α Inhibition in inflammatory bowel disease. Pharmaceutics. (2020) 12:539. doi: 10.3390/pharmaceutics12060539
76. Diak P, Siegel J, La Grenade L, Choi L, Lemery S, and McMahon A. Tumor necrosis factor alpha blockers and Malignancy in children: forty-eight cases reported to the Food and Drug Administration. Arthritis Rheumatol. (2010) 62:2517–24. doi: 10.1002/art.27511
77. Kim YJ, Hong KS, Chung JW, Kim JH, and Hahm KB. Prevention of colitis-associated carcinogenesis with infliximab. Cancer Prev Res (Phila). (2010) 3:1314–33. doi: 10.1158/1940-6207.Capr-09-0272
78. Alkhayyat M, Abureesh M, Gill A, Khoudari G, Abou Saleh M, Mansoor E, et al. Lower rates of colorectal cancer in patients with inflammatory bowel disease using anti-TNF therapy. Inflammation Bowel Dis. (2021) 27:1052–60. doi: 10.1093/ibd/izaa252
79. Driscoll CB, Rich JM, Isaacson D, Nicolas J, Jiang Y, Mi X, et al. Tumor necrosis factor-alpha inhibitor use and Malignancy risk: A systematic review and patient level meta-analysis. Cancers (Basel). (2025) 17:390. doi: 10.3390/cancers17030390
80. Schulz MD, Atay C, Heringer J, Romrig FK, Schwitalla S, Aydin B, et al. High-fat-diet-mediated dysbiosis promotes intestinal carcinogenesis independently of obesity. Nature. (2014) 514:508–12. doi: 10.1038/nature13398
81. van der Logt EM, Blokzijl T, van der Meer R, Faber KN, and Dijkstra G. Westernized high-fat diet accelerates weight loss in dextran sulfate sodium-induced colitis in mice, which is further aggravated by supplementation of heme. J Nutr Biochem. (2013) 24:1159–65. doi: 10.1016/j.jnutbio.2012.09.001
82. Pandurangan AK and Esa NM. Signal transducer and activator of transcription 3 - a promising target in colitis-associated cancer. Asian Pac J Cancer Prev. (2014) 15:551–60. doi: 10.7314/apjcp.2014.15.2.551
83. Li Y, de Haar C, Chen M, Deuring J, Gerrits MM, Smits R, et al. Disease-related expression of the IL6/STAT3/SOCS3 signalling pathway in ulcerative colitis and ulcerative colitis-related carcinogenesis. Gut. (2010) 59:227–35. doi: 10.1136/gut.2009.184176
84. Shao X, Liu L, Zhou Y, Zhong K, Gu J, Hu T, et al. High-fat diet promotes colitis-associated tumorigenesis by altering gut microbial butyrate metabolism. Int J Biol Sci. (2023) 19:5004–19. doi: 10.7150/ijbs.86717
85. Chen HL, Hu PY, Chen CS, Lin WH, Hsu DK, Liu FT, et al. Gut colonization of Bacteroides plebeius suppresses colitis-associated colon cancer development. Microbiol Spectr. (2025) 13:e0259924. doi: 10.1128/spectrum.02599-24
86. Wen J, Zhang J, Zhang H, Zhang N, Lei R, Deng Y, et al. Large-scale genome-wide association studies reveal the genetic causal etiology between air pollutants and autoimmune diseases. J Transl Med. (2024) 22:392. doi: 10.1186/s12967-024-04928-y
87. Chen J, Zhang H, Fu T, Zhao J, Nowak JK, Kalla R, et al. Exposure to air pollution increases susceptibility to ulcerative colitis through epigenetic alterations in CXCR2 and MHC class III region. EBioMedicine. (2024) 110:105443. doi: 10.1016/j.ebiom.2024.105443
88. Katoh H, Wang D, Daikoku T, Sun H, Dey SK, and Dubois RN. CXCR2-expressing myeloid-derived suppressor cells are essential to promote colitis-associated tumorigenesis. Cancer Cell. (2013) 24:631–44. doi: 10.1016/j.ccr.2013.10.009
89. Turner D, Ruemmele FM, Orlanski-Meyer E, Griffiths AM, de Carpi JM, Bronsky J, et al. Management of paediatric ulcerative colitis, part 1: ambulatory care-an evidence-based guideline from european crohn’s and colitis organization and european society of paediatric gastroenterology, hepatology and nutrition. J Pediatr Gastroenterol Nutr. (2018) 67:257–91. doi: 10.1097/mpg.0000000000002035
90. Oliva S, Thomson M, de Ridder L, Martín-de-Carpi J, Van Biervliet S, Braegger C, et al. Endoscopy in pediatric inflammatory bowel disease: A position paper on behalf of the porto IBD group of the european society for pediatric gastroenterology, hepatology and nutrition. J Pediatr Gastroenterol Nutr. (2018) 67:414–30. doi: 10.1097/mpg.0000000000002092
91. Maaser C, Sturm A, Vavricka SR, Kucharzik T, Fiorino G, Annese V, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. (2019) 13:144–64. doi: 10.1093/ecco-jcc/jjy113
Keywords: pediatric, inflammatory bowel disease, cancer, inflammation, immunosuppressive
Citation: Zheng J-J, Wu Z-F and Hu Y-B (2025) Pediatric inflammatory bowel disease and cancer. Front. Immunol. 16:1624177. doi: 10.3389/fimmu.2025.1624177
Received: 07 May 2025; Accepted: 08 August 2025;
Published: 27 August 2025.
Edited by:
Li-Tung Huang, Kaohsiung Chang Gung Memorial Hospital, TaiwanReviewed by:
Juan Carlos Núñez-Enríquez, Mexican Social Security Institute, MexicoHirokazu Kanegane, Tokyo Medical and Dental University, Japan
Copyright © 2025 Zheng, Wu and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi-Bing Hu, WWliaW5nX2h1OTBAMTYzLmNvbQ==