 David Gandara1*
David Gandara1* Miranda Gogishvili2
Miranda Gogishvili2 Ahmet Sezer3Tamta Makharadze4Mahmut Gümüş5
Ahmet Sezer3Tamta Makharadze4Mahmut Gümüş5 Cong Zhu6
Cong Zhu6 Eric Yan6,7Giuseppe Gullo6Petra Rietschel6Ruben G. W. Quek6
Eric Yan6,7Giuseppe Gullo6Petra Rietschel6Ruben G. W. Quek6- 1Division of Hematology/Oncology, Department of Medicine, UC Davis Comprehensive Cancer Center, Sacramento, CA, United States
- 2High Technology Medical Centre, University Clinic Ltd, Tbilisi, Georgia
- 3Department of Medical Oncology, Başkent University, Adana, Türkiye
- 4LTD High Technology Hospital Med Center, Batumi, Georgia
- 5Department of Medical Oncology, School of Medicine, Istanbul Medeniyet University, Istanbul, Türkiye
- 6Regeneron Pharmaceuticals, Inc., Tarrytown, NY, United States
- 7Cyan Global Inc., San Diego, CA, United States
Introduction: There is potential clinical utility in using patient-reported outcomes (PROs) to predict survival in patients with advanced non-small cell lung cancer. We assessed the prognostic value of PROs for survival in two phase 3 cemiplimab studies in advanced non-small cell lung cancer.
Methods: Data from EMPOWER-Lung 1 and EMPOWER-Lung 3 Part 2, two global, randomized phase 3 clinical trials, were used. Patients with advanced non-small cell lung cancer and programmed cell death-ligand 1 expression ≥50% received cemiplimab monotherapy (n=283), and patients with no EGFR, ALK, or ROS1 genomic aberrations received cemiplimab plus chemotherapy (n=312). PROs were assessed using the European Organization for Research and Treatment of Cancer Core Quality of Life and Quality of Life Lung Cancer 13 questionnaires. Association between baseline PROs and survival was analyzed, and the C-statistic was used to assess the prognostic value of PROs in comparison with the Eastern Cooperative Oncology Group performance status (ECOG PS) scale.
Results: Twenty-five PROs were evaluated, of which 15 were significantly associated (P<0.05) with overall survival and were better predictors than ECOG PS. Fourteen PROs were significantly associated (P<0.05) with progression-free survival; of these, 13 had better prognostic value than ECOG PS. Patient-reported dyspnea and physical functioning had the highest prognostic values for overall survival (c=0.635 and c=0.619, respectively) and progression-free survival (c=0.593 and c=0.583, respectively). Stratifying physical functioning into high, medium, and low categories showed that patients with high physical functioning at baseline had significantly better overall survival (high vs low; HR, 0.41; 95% CI, 0.23-0.71; P=0.001), resulting in a 59% reduction in the risk of death. Similarly, patients in the high physical functioning category had significantly favorable progression-free survival (high vs low; HR, 0.44, 95% CI, 0.29-0.66; P<0.001) and a 56% reduction in the risk of death.
Conclusion: Baseline PROs, including dyspnea and physical functioning, have significant prognostic value for survival for patients with advanced non-small cell lung cancer.
1 Introduction
The therapeutic landscape in advanced non-small-cell lung cancer (NSCLC) has changed rapidly in recent years. For the majority of patients with non−oncogene-driven cancers, immune checkpoint inhibitor (ICI) therapy has revolutionized therapeutic decision-making. ICI therapeutic options vary widely; these include anti-programmed cell death-1 (PD-1)/programmed cell death-ligand 1 (PD-L1) agent monotherapy, combination therapy with radiotherapy or chemotherapy, and immunotherapy combinations (anti–PD-1/PD-L1 plus anti−cytotoxic T-lymphocyte antigen 4) (1–4).
Cemiplimab (a PD-1 inhibitor) is approved internationally as a first-line treatment for patients with advanced NSCLC with a PD-L1 expression level of ≥50%, as well as in combination with platinum-based chemotherapy for patients with advanced NSCLC with no epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), or c-ros oncogene 1 (ROS1) genomic aberrations (5–8). The approval of cemiplimab was based on published data from two pivotal phase 3 trials, EMPOWER-Lung 1 (NCT03088540) and EMPOWER-Lung 3 Part 2 (NCT03409614) (Supplementary Table S1) (9–13). Results from these studies showed clinically meaningful and statistically significant improvement in overall survival (OS) and progression-free survival (PFS) with first-line cemiplimab ± chemotherapy compared with platinum-doublet chemotherapy in patients with advanced NSCLC (9, 13). The safety results of cemiplimab in EMPOWER-Lung 1 and EMPOWER-Lung 3 were generally consistent with that of other immunotherapy-based trials in first-line treatment of advanced NSCLC (9, 13).
Patient-reported outcomes (PROs) in advanced NSCLC have previously also been examined for first-line cemiplimab (as monotherapy and in combination with chemotherapy) in EMPOWER Lung 1 and EMPOWER Lung 3 (14, 15); significant overall improvement in symptoms and delayed time to definitive clinically meaningful deterioration in cancer-related and lung cancer–specific symptoms and functions were observed.
Most recently, PROs have shown promise in their prognostic value for survival (16); however, no studies have assessed the prognostic performance of PROs in patients with advanced NSCLC initiating first-line cemiplimab-based therapy. Quality-of-life data have also been underutilized in a significant number of phase 3 lung cancer trials (17, 18). This study therefore aimed to evaluate the prognostic value of PROs for survival in patients from the two pivotal phase 3 cemiplimab trials, EMPOWER-Lung 1 and EMPOWER-Lung 3, in advanced NSCLC.
The physician-reported Eastern Cooperative Oncology Group performance status (ECOG PS) scale is influenced by several factors, such as the burden of the disease itself, the presence of comorbidities, and global frailty of elderly people (16), and relying on ECOG PS alone as a prognostic clinical marker may be insufficient. Patient-reported physical function has been shown to be a tumor-agnostic predictor of OS, which in several analyses has been more prognostic than physician-assessed ECOG PS (19–24). This study therefore aimed to further evaluate the prognostic value of patient-reported risk-stratified physical functioning in patients with advanced NSCLC initiating first-line cemiplimab-based therapy.
2 Methods
2.1 Inclusion criteria and trial description
The study designs have been described previously (9, 10). Briefly, patients with advanced NSCLC were included in the cemiplimab monotherapy and cemiplimab plus chemotherapy treatment arms for the EMPOWER-Lung 1 and EMPOWER-Lung 3 Part 2 phase 3 clinical trials. Both trials included patients aged ≥18 years with squamous and non-squamous advanced NSCLC; however, EMPOWER-Lung 1 included patients with PD-L1 expression ≥50% and EMPOWER-Lung 3 Part 2 included patients with no EGFR, ALK, or ROS1 genomic aberrations (9, 10).
2.2 Predictor and patient-reported outcome measures
The physician-defined ECOG PS scale is widely used to assess the functional status of patients with cancer, including their ability to self-care, ability to perform daily activities, physical ability (ie, walking and working), and ability to tolerate treatment. ECOG PS scores range from 0 (fully active) to 5 (dead); higher scores represent poorer functioning (25).
PROs were assessed using the European Organization for Research and Treatment of Cancer (EORTC) Core Quality of Life (QLQ-C30) and Quality of Life Lung Cancer 13 (QLQ-LC13) questionnaires. The QLQ-C30 questionnaire assesses functioning (physical, role, cognitive, emotional, and social), symptoms (fatigue, pain, nausea, vomiting, dyspnea, appetite loss, insomnia, constipation, and diarrhea), global health, and quality of life (26). As a supplementary module to the QLQ-C30, the QLQ-LC13 questionnaire measures lung-cancer–associated symptoms (coughing, hemoptysis, dyspnea, and pain) and side effects from conventional chemotherapy and radiotherapy (hair loss, neuropathy, sore mouth, and dysphagia) (27).
The EORTC QLQ-C30 and QLQ-LC13 questionnaires were scored per the instrument scoring manual (28). For both questionnaires, scores range from 0 to 100; higher scores on functioning and global health/quality of life scales indicate better outcomes, and higher scores on symptom scales indicate worse outcomes, from a patient perspective (26, 27, 29–31).
2.3 Statistical analysis
Individual patient data from cemiplimab-based therapy in the EMPOWER-Lung 1 and EMPOWER-Lung 3 Part 2 studies were utilized to evaluate the association between baseline PROs and survival by Cox proportional hazard regression, stratified by treatment, histology, and PD-L1 level. Statistically significant results were reported with HRs and 95% CIs, and statistical significance was pre-defined at P<0.05. HRs were based on a 10-point increase in the EORTC QLQ-C30 and QLQ-LC13 scales.
The prediction performance of PROs was assessed using Harrell’s concordance statistic, or C-statistic, which measures the concordance between PROs and OS (32). The higher the C-statistic, the better the model predicts OS outcomes (33).
For patient-reported physical functioning, the prognostic performance was also compared against the ECOG PS scale. The association between survival outcomes and baseline physical functioning was assessed by Kaplan–Meier analysis (stratified by low, intermediate, and high categories per EORTC QLQ-C30 Lung Cancer Stage III/IV (34)–specified interquartile definitions with thresholds being: low, <46.7; intermediate, ≥46.7–≤86.7; and high, >86.7).
C-statistic computations were performed using R programming language (GNU Project); SAS version 9.4 (SAS Institute Inc) was used for all other statistical analyses.
2.4 Ethical consideration
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and the International Conference on Harmonization Good Clinical Practice guidelines. All patients provided written informed consent (9, 10).
3 Results
3.1 Patient population
In the pooled cohort, 283 patients with advanced NSCLC and PD-L1 expression ≥50% were treated with cemiplimab monotherapy, and 312 patients with advanced NSCLC and no EGFR, ALK, or ROS1 genomic aberrations were treated with cemiplimab plus chemotherapy (9, 10). Supplementary Table S2 summarizes the baseline patient characteristics by treatment arms, which were broadly similar. For every cycle from baseline to Cycle 27, ≥90% of patients who received cemiplimab monotherapy and ≥90% of patients who received cemiplimab plus chemotherapy completed at least one question on each of the EORTC QLQ-C30 and QLQ-LC13 questionnaires.
3.2 Patient-reported outcomes
Out of the 25 PROs analyzed, 15 were significantly associated with OS (P<0.05) and had greater prognostic value than physician-reported ECOG PS. Patient-reported dyspnea (per EORTC QLQ-LC13; c=0.635) and physical functioning (per EORTC QLQ-C30; c=0.619) had the highest predictability for OS (Table 1).
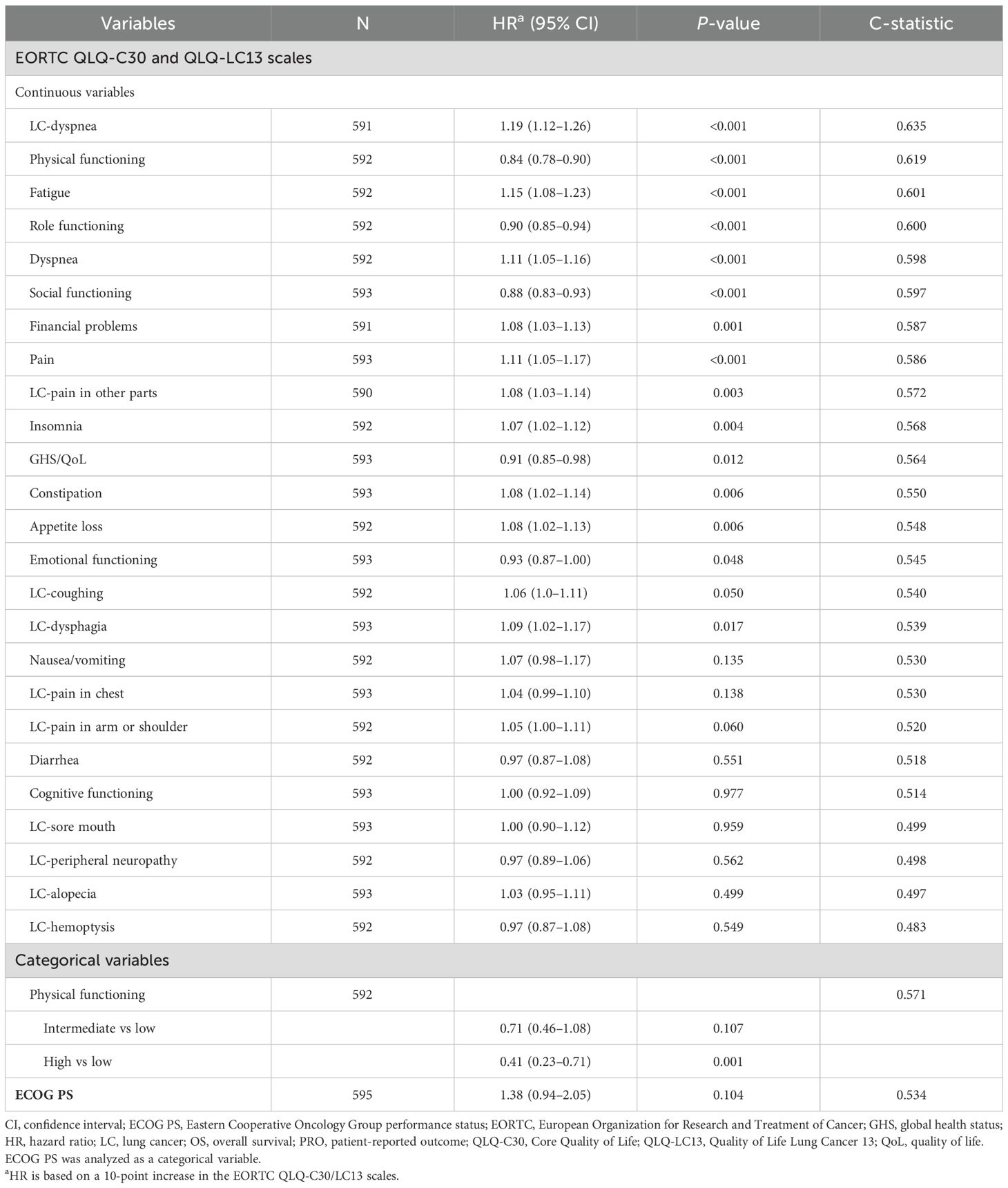
Table 1. Rank summary of the prognostic value of PROs for OS for patients in the overall population.
Fourteen out of 25 PROs were significantly associated with PFS (P<0.05), and 13 of the statistically significant PROs had higher prognostic performance than the ECOG PS. For PFS, patient-reported dyspnea (per EORTC QLQ-LC13; c=0.593) and physical functioning (per EORTC QLQ-C30; c=0.583) had the highest predictability (Table 2).
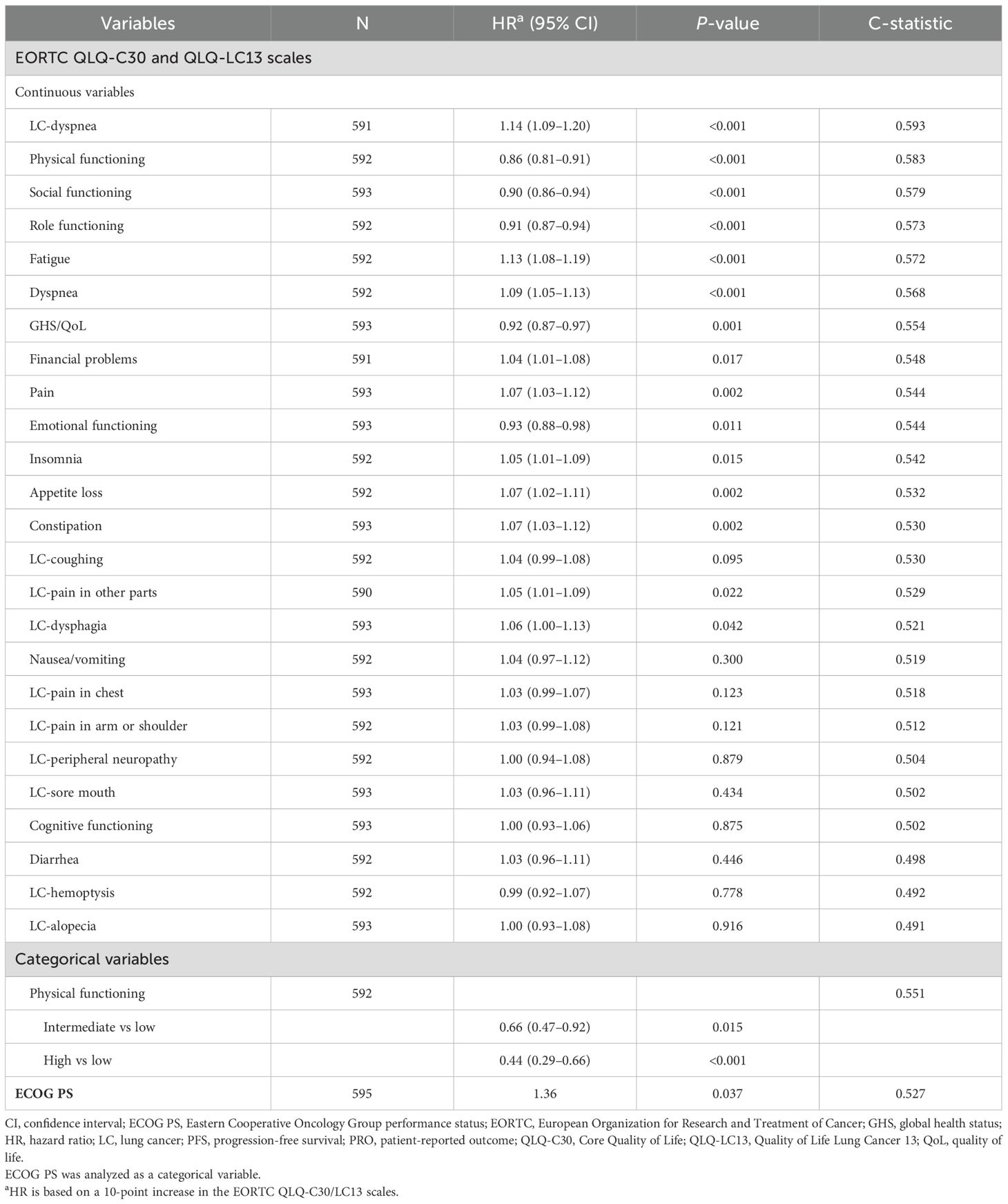
Table 2. Rank summary of the prognostic value of PROs for PFS for patients in the overall population.
When baseline physical functioning was stratified by low, intermediate, and high categories, results from the survival analyses showed that patients with high baseline physical functioning had significantly more favorable OS than those with low physical functioning (high vs low; HR, 0.41; 95% CI, 0.23–0.71; P=0.001) (Figure 1), representing a predicted 59% reduction in the risk of death.
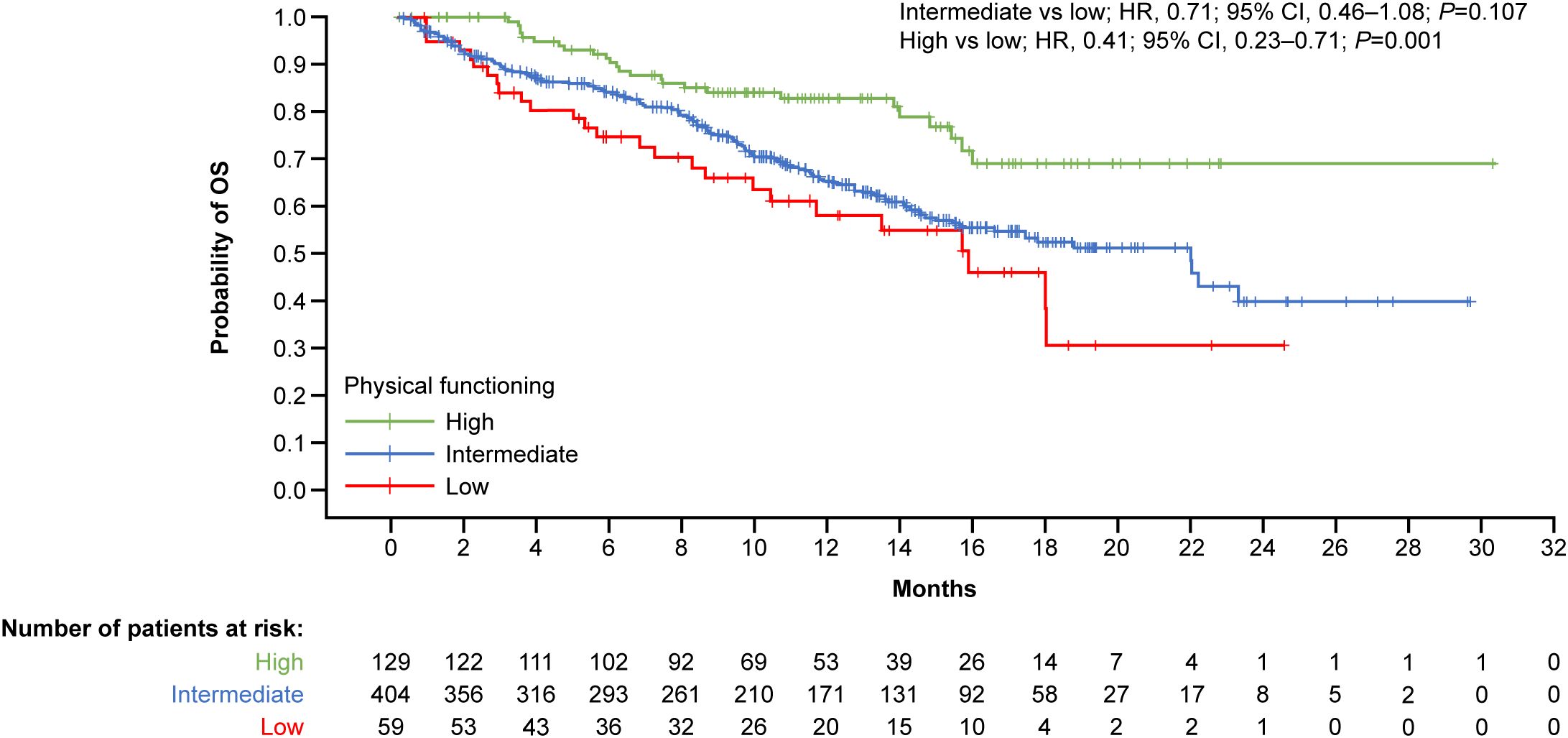
Figure 1. Kaplan–Meier curves by physical functioning at baseline for OS. Physical functioning baseline scores per EORTC QLQ-C30 Lung Cancer Model – Stage III/IV interquartile categories: low, <46.7; intermediate, ≥46.7–≤86.7; high, >86.7. CI, confidence interval; EORTC, European Organization for Research and Treatment of Cancer; HR, hazard ratio; OS, overall survival; QLQ-C30, Core Quality of Life.
Likewise, patients with high baseline physical functioning had significantly more favorable PFS than those with low physical functioning (high vs low; HR, 0.44; 95% CI, 0.29-0.66; P<0.001) (Figure 2), representing a predicted 56% reduction in the risk of death.
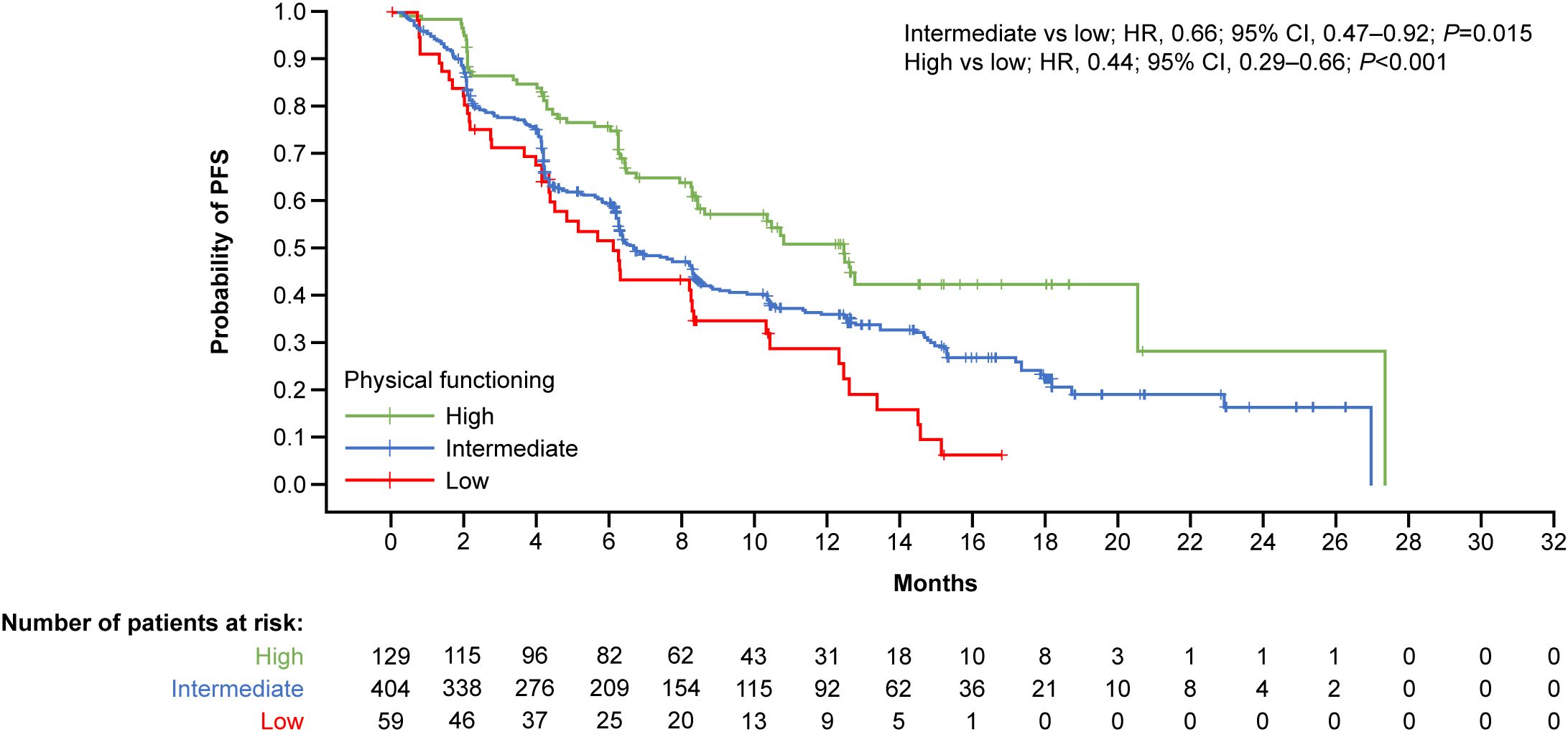
Figure 2. Kaplan–Meier curves by physical functioning at baseline for PFS. Physical functioning baseline scores per EORTC QLQ-C30 Lung Cancer Module – stage III/IV interquartile categories: low, <46.7; intermediate, ≥46.7–≤86.7; high, >86.7. CI, confidence interval; EORTC, European Organization for Research and Treatment of Cancer; HR, hazard ratio; PFS, progression-free survival; QLQ-C30, Core Quality of Life.
4 Discussion
While recent studies have increasingly incorporated PROs into cancer clinical trial design and interpretation, there remains wide variability in the actual measures and analytic approaches employed (35). Most importantly, studies have found discordance between physician and patient perspectives, including underreporting of toxicities by physicians (36, 37). Further, studies of ECOG PS have shown that 40–50% of physicians overestimate patients’ performance status (36, 38). In our study, 15 and 14 out of 25 baseline PROs had better prognostic performance for OS and PFS, respectively, than physician-defined ECOG PS (0–1) in patients with advanced NSCLC initiating first-line cemiplimab-based therapy. The two baseline PROs with the highest predictability for OS and PFS were patient-reported dyspnea and physical functioning. Stratification at baseline for high versus low physical functioning categories revealed significant separation between patients, creating low-risk and high-risk patient groups.
The US Food and Drug Administration and other regulatory bodies have acknowledged the added value of incorporating PRO symptom and functional scales into clinical trial assessments. A set of key PROs that may contribute to a patient’s health-related quality of life and may provide a more sensitive measure of the effects of disease and treatment has been previously explored (39). More recently, the US Food and Drug Administration expanded on this concept by publishing guidance recommending the collection of specific core PROs in cancer clinical trials; these include disease-related symptoms, physical function, and role function (40).
In our analysis, PROs with functioning scales (e.g. physical) and select disease-related symptom scales (e.g. dyspnea) showed better prognostic performance for OS and PFS than ECOG PS. These may help clinicians prioritize select PROs with the most meaningful and measurable outcomes that predict OS and PFS in advanced NSCLC, thereby minimizing the burden on the patient and increasing the quality of collected data. This could help streamline PRO assessments in clinical trials and increase the regulatory utility of PRO data.
Furthermore, the prognostic value of PROs for survival could be useful in an increasingly patient-centered clinical setting. For example, the Enhancing Oncology model requires participating practices to collect and monitor PRO data (41). Such tools can increase patients’ self-awareness of symptoms and involvement in their care, better identify patient needs, inform treatment decisions, and improve cancer outcomes (41). The Centers for Medicare & Medicaid Services have outlined several domains for inclusion in PRO surveys, including symptom, functioning, and behavioral scales, such as the EORTC quality of life questionnaires (41).
Larger-scale studies designed to assess the prognostic value of PROs are needed to confirm these results. This analysis only included data from patients with advanced NSCLC who received first-line cemiplimab-based treatment and results may not be generalizable to other tumor and treatment types; future research should explore the validity of our results among patients receiving other therapies. Our study included patients from open-label trials (EMPOWER-Lung 1 and EMPOWER-Lung 3 Part 2), and the PRO results presented may be subject to patient biases. Of note, there is a lack of clear empirical evidence that such biases are sufficient to meaningfully affect the results of clinical trials (42). PROs collected from patients with advanced NSCLC in a real-world setting would be warranted to validate these results; especially among patients with ECOG PS >1 as our research is limited to patients with ECOG PS 0–1. Future analyses should explore interaction analyses and sensitivity analyses such as imputation methods to assess effects on the research outcomes. Future studies in a real-world setting that include patients with ECOG PS >1 (e.g. the CEMI-LUNG observational study [NCT05363319]) (43) should also be explored to evaluate the generalizability of our results.
5 Conclusions
In patients with advanced NSCLC who received first line cemiplimab based therapy, baseline PROs such as dyspnea and physical functioning have clinical utility in predicting patient survival in advanced NSCLC. These results suggest PROs have significant worth in oncology clinical practice and research trials of ICIs.
Data availability statement
The datasets presented in this article are not readily available because data will be made available by request. Qualified researchers may request access to study documents (including the clinical study report, study protocol with any amendments, blank case report form and statistical analysis plan) that support the methods and findings reported in this article. Individual anonymized participant data will be considered for sharing once the product and indication has been approved by major health authorities (eg, US Food and Drug Administration, European Medicines Agency, Pharmaceuticals and Medical Devices Agency, etc.), if there is legal authority to share the data and there is not a reasonable likelihood of participant re-identification. Requests to access the datasets should be directed to https://vivli.org/.
Ethics statement
The studies involving humans were approved by the appropriate institutional review board or independent ethics committee at each participating study site. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DG: Investigation, Writing – review & editing. MGo: Investigation, Writing – review & editing. AS: Investigation, Writing – review & editing. TM: Investigation, Writing – review & editing. MGü: Investigation, Writing – review & editing. CZ: Formal Analysis, Methodology, Validation, Writing – review & editing. EY: Conceptualization, Formal Analysis, Methodology, Validation, Writing – review & editing. GG: Conceptualization, Writing – review & editing. PR: Conceptualization, Writing – review & editing. RQ: Conceptualization, Formal Analysis, Methodology, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by Regeneron Pharmaceuticals, Inc. The sponsor was involved in the study design and in the collection, analysis, and interpretation of data, as well as checking of data and information provided in the manuscript. This manuscript, including the description of the study design, methods and results, has been independently reviewed and approved by five external academic authors. Furthermore, the data analysis was independently reviewed by another statistician within Regeneron Pharmaceuticals, Inc. Authors were included based on ICMJE authorship criteria. The authors had unrestricted access to study data, were responsible for all content and editorial decisions, and received no honoraria related to the development of this publication.
Acknowledgments
The authors thank the patients, their families, all other investigators, and all investigational site members involved in this study. The authors also thank the contributions of Xuanyao He, former employee of Regeneron Pharmaceuticals, Inc. Medical writing support was provided by Adrienn Teraz-Orosz, PhD, and editorial support was provided by Elke Sims, MLangTrans, both of Alpha (a division of Prime, Knutsford, UK), funded by Regeneron Pharmaceuticals, Inc. and Sanofi.
Conflict of interest
Authors CZ, EY, GG, PR, and RGWQ were employed by the company Regeneron Pharmaceuticals, Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Regeneron Pharmaceuticals, Inc. The funder had the following involvement in the study: involvement in the study design and in the collection, analysis, and interpretation of data, as well as checking of data and information provided in the manuscript. This manuscript, including the description of the study design, methods and results, has been independently reviewed and approved by five external academic authors. Furthermore, the data analysis was independently reviewed by another statistician within Regeneron Pharmaceuticals, Inc. Authors were included based on ICMJE authorship criteria. The authors had unrestricted access to study data, were responsible for all content and editorial decisions, and received no honoraria related to the development of this publication.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1640595/full#supplementary-material
References
1. Tang S, Qin C, Hu H, Liu T, He Y, Guo H, et al. Immune checkpoint inhibitors in non-small cell lung cancer: Progress, challenges, and prospects. Cells. (2022) 11:320. doi: 10.3390/cells11030320
2. Tian Y, Xu L, Li X, Li H, and Zhao M. SMARCA4: Current status and future perspectives in non-small-cell lung cancer. Cancer Lett. (2023) 554:216022. doi: 10.1016/j.canlet.2022.216022
3. Yao Y, Fareed R, Zafar A, Saleem K, Huang T, Duan Y, et al. State-of-the-art combination treatment strategies for advanced stage non-small cell lung cancer. Front Oncol. (2022) 12:958505. doi: 10.3389/fonc.2022.958505
4. Insa A, Martin-Martorell P, Di Liello R, Fasano M, Martini G, Napolitano S, et al. Which treatment after first line therapy in NSCLC patients without genetic alterations in the era of immunotherapy? Crit Rev Oncol Hematol. (2022) 169:103538. doi: 10.1016/j.critrevonc.2021.103538
5. US Food and Drug Administration. FDA approves cemiplimab-rwlc for non-small cell lung cancer with high PD-L1 expression (2021). Available online at: https://www.fda.gov/drugs/resources-information-approveddrugs/fda-approves-cemiplimab-rwlc-non-small-cell-lung-cancer-high-pd-l1-expression (Accessed August 2, 2021).
6. US Food and Drug Administration. FDA approves cemiplimab-rwlc in combination with platinum-based chemotherapy for non-small cell lung cancer (2022). Available online at: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-cemiplimab-rwlc-combination-platinum-based-chemotherapy-non-small-cell-lung-cancer (Accessed February 8, 2023).
7. European Medicines Agency. LIBTAYO EPAR (2023). Available online at: https://www.ema.europa.eu/en/documents/product-information/libtayo-epar-product-information_en.pdf (Accessed August 22, 2023).
8. Health Canada. Libtayo™ injection solution for infusion, 50 mg/mL. Product monograph (2023). Available online at: https://pdf.hres.ca/dpd_pm/00070427.pdf (Accessed May 18, 2023).
9. Makharadze T, Gogishvili M, Melkadze T, Baramidze A, Giorgadze D, Penkov K, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in advanced NSCLC: 2-year follow-up from the phase 3 EMPOWER-Lung 3 Part 2 trial. J Thorac Oncol. (2023) 18:755–68. doi: 10.1016/j.jtho.2023.03.008
10. Sezer A, Kilickap S, Gümüş M, Bondarenko I, Özgüroğlu M, Gogishvili M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomized, controlled trial. Lancet. (2021) 397:592–604. doi: 10.1016/s0140-6736(21)00228-2
11. US Food and Drug Administration. LIBTAYO (cemiplimab) prescribing information. Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761097s007lbl.pdf (Accessed March 21, 2024).
12. Gogishvili M, Melkadze T, Makharadze T, Giorgadze D, Dvorkin M, Penkov K, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: A randomized, controlled, double-blind phase 3 trial. Nat Med. (2022) 28:2374–80. doi: 10.1038/s41591-022-01977-y
13. Özgüroğlu M, Kilickap S, Sezer A, Gümüş M, Bondarenko I, Gogishvili M, et al. First-line cemiplimab monotherapy and continued cemiplimab beyond progression plus chemotherapy for advanced non-small-cell lung cancer with PD-L1 50% or more (EMPOWER-Lung 1): 35-month follow-up from a multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. (2023) 24:989–1001. doi: 10.1016/S1470-2045(23)00329-7
14. Gümüş M, Chen C-I, Ivanescu C, Kilickap S, Bondarenko I, Özgüroğlu M, et al. Patient-reported outcomes with cemiplimab monotherapy for first-line treatment of advanced non-small cell lung cancer with PD-L1 of ≥50%: the EMPOWER-Lung 1 study. Cancer. (2023) 129:118–29. doi: 10.1002/cncr.34477
15. Makharadze T, Quek RGW, Melkadze T, Gogishvili M, Ivanescu C, Giorgadze D, et al. Quality of life with cemiplimab plus chemotherapy for first-line treatment of advanced non-small cell lung cancer: Patient-reported outcomes from phase 3 EMPOWER-Lung 3. Cancer. (2023) 129:2256–65. doi: 10.1002/cncr.34687
16. Badaoui S, Shahnam A, McKinnon RA, Abuhelwa AY, Sorich MJ, and Hopkins AM. The predictive utility of patient-reported outcomes and performance status for survival in metastatic lung cancer patients treated with chemoimmunotherapy. Transl Lung Cancer Res. (2022) 11:432–9. doi: 10.21037/tlcr-21-938
17. Reale ML, De Luca E, Lombardi P, Marandino L, Zichi C, Pignataro D, et al. Quality of life analysis in lung cancer: A systematic review of phase III trials published between 2012 and 2018. Lung Cancer. (2020) 139:47–54. doi: 10.1016/j.lungcan.2019.10.022
18. Kalantri S, Sainatham C, Gaddipati GN, Tallapalli JR, Singh R, and Kloecker GH. Patient-centered perspectives: Examining quality-of-life integration in recent phase III lung cancer trials (2019–2023). J Cancer Policy. (2025) 44:100566. doi: 10.1016/j.jcpo.2025.100566
19. Mierzynska J, Piccinin C, Pe M, Martinelli F, Gotay C, Coens C, et al. Prognostic value of patient-reported outcomes from international randomised clinical trials on cancer: a systematic review. Lancet Oncol. (2019) 20:e685–e98. doi: 10.1016/s1470-2045(19)30656-4
20. Quinten C, Coens C, Mauer M, Comte S, Sprangers MA, Cleeland C, et al. Baseline quality of life as a prognostic indicator of survival: a meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. (2009) 10:865–71. doi: 10.1016/s1470-2045(09)70200-1
21. Kerrigan K, Patel SB, Haaland B, Ose D, Weinberg Chalmers A, Haydell T, et al. Prognostic significance of patient-reported outcomes in cancer. JCO Oncol Pract. (2020) 16:e313–e23. doi: 10.1200/jop.19.00329
22. Seow H, Tanuseputro P, Barbera L, Earle C, Guthrie D, Isenberg S, et al. Development and validation of a prognostic survival model with patient-reported outcomes for patients with cancer. JAMA Netw Open. (2020) 3:e201768. doi: 10.1001/jamanetworkopen.2020.1768
23. Trejo MJ, Bell ML, Dhillon HM, and Vardy JL. Baseline quality of life is associated with survival among people with advanced lung cancer. J Psychosoc Oncol. (2020) 38:635–41. doi: 10.1080/07347332.2020.1765065
24. Gotay CC, Kawamoto CT, Bottomley A, and Efficace F. The prognostic significance of patient-reported outcomes in cancer clinical trials. J Clin Oncol. (2008) 26:1355–63. doi: 10.1200/jco.2007.13.3439
25. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. (1982) 5:649–55. doi: 10.1097/00000421-198212000-00014
26. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. (1993) 85:365–76. doi: 10.1093/jnci/85.5.365
27. Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, and Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. (1994) 30A:635–42. doi: 10.1016/0959-8049(94)90535-5
28. European Organisation for Research and Treatment of Cancer. EORTC QLQ-C30 scoring manual (2001). Available online at: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf (Accessed July 23, 2025).
29. Osoba D, Rodrigues G, Myles J, Zee B, and Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. (1998) 16:139–44. doi: 10.1200/JCO.1998.16.1.139
30. Cocks K, King MT, Velikova G, Fayers PM, and Brown JM. Quality, interpretation and presentation of European Organisation for Research and Treatment of Cancer quality of life questionnaire core 30 data in randomised controlled trials. Eur J Cancer. (2008) 44:1793–8. doi: 10.1016/j.ejca.2008.05.008
31. King MT. The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual Life Res. (1996) 5:555–67. doi: 10.1007/BF00439229
32. Harrell FE Jr., Califf RM, Pryor DB, Lee KL, and Rosati RA. Evaluating the yield of medical tests. JAMA. (1982) 247:2543–6. doi: 10.1001/jama.1982.03320430047030
33. Guo C, So Y, and Jang W. Evaluating predictive accuracy of survival models with PROC PHREG (2017). Available online at: https://support.sas.com/resources/papers/proceedings17/SAS0462-2017.pdfpage=13&zoom=100,96,98 (Accessed April 19, 2024).
34. Scott NW, Fayers P, Aaronson NK, Bottomley A, de Graeff A, Groenvold M, et al. EORTC QLQ-C30 reference values (2008). Available online at: https://www.eortc.org/app/uploads/sites/2/2018/02/reference_values_manual2008.pdf (Accessed October 31, 2023).
35. Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, and Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. (2018) 9:353–67. doi: 10.2147/PROM.S156279
36. Ando M, Ando Y, Hasegawa Y, Shimokata K, Minami H, Wakai K, et al. Prognostic value of performance status assessed by patients themselves, nurses, and oncologists in advanced non-small cell lung cancer. Br J Cancer. (2001) 85:1634–9. doi: 10.1054/bjoc.2001.2162
37. Ooki A, Morita S, Tsuji A, Iwamoto S, Hara H, Tanioka H, et al. Disagreement between patient- and physician-reported outcomes on symptomatic adverse events as poor prognosis in patients treated with first-line cetuximab plus chemotherapy for unresectable metastatic colorectal cancer: Results of Phase II QUACK trial. Cancer Med. (2020) 9:9419–30. doi: 10.1002/cam4.3564
38. Sørensen JB, Klee M, Palshof T, and Hansen HH. Performance status assessment in cancer patients. An inter-observer variability study. Br J Cancer. (1993) 67:773–5. doi: 10.1038/bjc.1993.140
39. Kluetz PG, Slagle A, Papadopoulos EJ, Johnson LL, Donoghue M, Kwitkowski VE, et al. Focusing on core patient-reported outcomes in cancer clinical trials: symptomatic adverse events, physical function, and disease-related symptoms. Clin Cancer Res. (2016) 22:1553–8. doi: 10.1158/1078-0432.CCR-15-2035
40. US Food & Drug Administration. Core patient-reported outcomes in cancer clinical trials (2024). Available online at: https://www.fda.gov/media/149994/download (Accessed January 3, 2024).
41. Centers for Medicare and Medicaid Services. EOM electronic patient-reported outcomes guide (2024). Available online at: https://www.cms.gov/priorities/innovation/media/document/eom-elec-pat-rpt-outcomes (Accessed January 6, 2025).
42. Atkinson TM, Wagner J-S, and Basch E. Trustworthiness of patient-reported outcomes in unblinded cancer clinical trials. JAMA Oncol. (2017) 3:738–9. doi: 10.1001/jamaoncol.2016.3328
43. An observational study to assess the effectiveness and safety of cemiplimab based regimen in patients with advanced Non-small Cell Lung Cancer (NSCLC) in routine clinical practice settings in Europe (CEMI-LUNG) (2022). Available online at: https://clinicaltrials.gov/study/NCT05363319. (Accessed September 22, 2025)
Keywords: non-small cell lung cancer, immunotherapy, patient-reported outcomes, immune checkpoint inhibitors, cemiplimab, quality of life
Citation: Gandara D, Gogishvili M, Sezer A, Makharadze T, Gümüş M, Zhu C, Yan E, Gullo G, Rietschel P and Quek RGW (2025) Prognostic value of patient-reported outcomes for survival in patients with advanced lung cancer receiving immune checkpoint inhibitors. Front. Immunol. 16:1640595. doi: 10.3389/fimmu.2025.1640595
Received: 03 June 2025; Accepted: 03 October 2025;
Published: 21 October 2025.
Edited by:
Cleber Machado-Souza, Pelé Pequeno Príncipe Research Institute, BrazilReviewed by:
Lingyun Zhao, King Abdullah University of Science and Technology, Saudi ArabiaYang Zhi, Chengdu Fifth People’s Hospital, China
Shreyas Kalantri, University of Louisville, United States
Copyright © 2025 Gandara, Gogishvili, Sezer, Makharadze, Gümüş, Zhu, Yan, Gullo, Rietschel and Quek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Gandara, ZHJnYW5kYXJhQHVjZGF2aXMuZWR1