 Leyi Wang
Leyi Wang Changdong Wu
Changdong Wu Ming Hou
Ming Hou Zhiwei Li
Zhiwei Li- 1People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, China
- 2Clinical Laboratory Center, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, China
Sepsis and cancer interact in a complex, bidirectional manner that significantly impacts patient prognosis, with metabolic reprogramming being a key factor. Sepsis-induced immune dysregulation and metabolic changes promote immunosuppression, tumor growth, metastasis, and resistance to immunotherapy. Cancer patients, especially those on immunosuppressive therapies, are more vulnerable to sepsis, complicating treatment and worsening outcomes. An integrated approach combining immunotherapy, metabolic interventions, and antimicrobial strategies is essential, alongside identifying biomarkers for personalized care. Recent advancements emphasize the need to integrate molecular insights, immunotherapy, and drug sensitivity analysis. This review explores how sepsis-driven metabolic reprogramming affects cancer immunotherapy and metastasis, providing a foundation for future integrated treatment strategies. Further research should focus on developing precise therapies that regulate metabolism, immunity, and the microbiome.

Graphical Abstract. The interaction between sepsis and cancer presents significant clinical challenges, as illustrated in the graphical abstract. (A) Sepsis disrupts the tumor microenvironment by triggering inflammation and immune suppression, promoting tumor growth and immune escape through mechanisms like PD-L1 expression. (B) Sepsis alters tumor cell metabolism, increasing ROS production and metabolic stress, which accelerates tumor growth and complicates cancer treatment. (C) Sepsis in cancer patients often presents with atypical symptoms like fever and organ dysfunction, making early diagnosis difficult. Timely detection using biomarkers and advanced imaging is essential. (D) Effective treatment strategies involve combining immunotherapy, antibiotics, and antitumor drugs, with emerging therapies like engineered bacteria and exosome-based nanomedicine offering innovative dual-targeting approaches. Multidisciplinary collaboration and precision medicine are key to improving outcomes in this high-risk population.
1 The basic theory of sepsis and tumor interaction
1.1 Pathological mechanisms and impact on the tumor microenvironment
Sepsis is a life-threatening condition characterized by a dysregulated immune response to infection, leading to systemic inflammation, immune dysfunction, and multiorgan failure (1). A hallmark is the cytokine storm, primarily driven by TNF-α, IL-1β, and IL-6, which induces endothelial damage, vascular leakage, coagulopathy, and subsequent immunosuppression through lymphocyte apoptosis and impaired antigen presentation (2). T cell exhaustion in the septic TME is characterized by elevated expression of inhibitory receptors (PD-1, CTLA-4, TIM-3, LAG-3) on CD8+ T cells, driven by chronic antigen exposure and sustained NF-κB/STAT3 signaling (3). Transcription factors such as TOX, TOX2, and NR4A family members maintain the epigenetic and transcriptional programs underlying exhaustion (4, 5). Pathogen-associated molecular patterns (PAMPs), such as LPS, activate Toll-like receptors (TLRs) on TME-resident cells, amplifying NF-κB/STAT3 signaling and promoting tumor survival and metastasis (3). Tumor cells contribute to systemic inflammation by secreting pro-inflammatory cytokines (e.g., IL-1β, IL-6) and chemokines (e.g., CCL2), which intensify immune dysregulation (6). Glioma-derived CCL2 and CCL7 facilitate monocytic-MDSC migration via CCR2+/CX3CR1+ signaling, reinforcing local immunosuppression (7). Sepsis induced extracellular matrix (ECM) remodeling, mediated by matrix metalloproteinases (MMPs), promotes tumor motility, invasiveness, and angiogenesis, facilitating dissemination (8). The interaction between sepsis and the tumor microenvironment (TME) is bidirectional; although acute infection may temporarily enhance anti-tumor immunity, chronic sepsis contributes to immunosuppression, metabolic reprogramming, and tissue remodeling. Recent studies have demonstrated that tumor-derived apoptotic extracellular vesicles promote metastasis and stemness through TME-mediated communication, unveiling a novel mechanism by which tumors exploit sepsis-induced alterations (9). This emerging paradigm warrants further mechanistic investigation.
1.2 Immunological basis of tumor associated sepsis
Cancer patients, especially those receiving cytotoxic therapies, face elevated sepsis risk due to therapy-induced immunosuppression (10). Sepsis exacerbates immune dysfunction and accelerates tumor progression, partly through the expansion of granulocytic myeloid-derived suppressor cells (G-MDSCs), which inhibit T cell responses via arginase-1, nitric oxide, and reactive oxygen species (11). In sepsis-induced tumor models, TLR4/MyD88 signaling boosts G-MDSC survival and function, promoting tumor growth. Sepsis also causes lymphopenia, T cell exhaustion (PD-1, TIM-3, LAG-3), and dendritic cell dysfunction, impairing tumor surveillance and reducing immunotherapy effectiveness (12, 13). Immune checkpoint inhibitor (ICI) resistance remains a major obstacle. Calreticulin-expressing liposomal nanoparticles (CRT-NPs) have reversed anti-CTLA-4 resistance in colon cancer by inducing immunogenic cell death, enhancing T cell activity, and reducing regulatory T cells (14). In gastric cancer, a low VEGF-A121/VEGF-A165 ratio was associated with improved progression-free survival, suggesting predictive value for ICI response. In clear cell renal cell carcinoma (ccRCC), resistance to combined anti-PD-1/CTLA-4 therapy was linked to myeloid-driven immunosuppression and alternative checkpoint pathways beyond PD-1 and CTLA-4 (15, 16). These findings highlight the multifactorial nature of immune resistance within the tumor–sepsis axis, emphasizing the need for personalized, targeted immunotherapies to overcome complex immunosuppressive networks.
1.3 Interaction between sepsis and tumor cell metabolism
Cancer cells exhibit metabolic reprogramming, notably the Warburg effect, characterized by elevated glycolysis despite sufficient oxygen availability, which supports cellular proliferation (17). Sepsis induces systemic metabolic disturbances, including hyperglycemia and insulin resistance, which affect both immune and tumor cell metabolism (18). In its early stages, sepsis enhances glycolysis and mitochondrial respiration in immune cells, augmenting anti-tumor activity. However, prolonged sepsis leads to metabolic exhaustion and immune dysfunction, fostering a tumor-permissive environment (19). Macrophage-targeted autophagy may mitigate this dysregulation by promoting inflammation resolution and tissue repair (20). Lactate, a glycolysis byproduct elevated in both cancer and sepsis, suppresses immune responses by impairing dendritic and T cell function and promoting Treg and MDSC expansion. Lactate also stabilizes Tregs via MOESIN lactylation, enhancing TGF-β/SMAD3 signaling and reinforcing immunosuppression.
Sepsis-induced oxidative stress further supports tumor survival through DNA damage, activation of PI3K/Akt and MAPK pathways, and oncogenic transformation (21). The impact of sepsis on tumor progression is context-dependent. In murine models, polymicrobial sepsis inhibited tumor growth via TLR4-mediated NK cell activation, suggesting that sepsis-induced innate immunity can have anti-tumor effects under certain conditions (22). GLUT1 upregulation promotes glycolysis and NF-κB-driven inflammation in macrophages; inhibiting it impairs cytokine production and mitochondrial function, indicating similar reprogramming in tumor-associated macrophages (23). Moreover, the upregulation of CPT1A, linked to enhanced lipid metabolism and tumor suppression in colitis-associated cancer models, may be disrupted during sepsis, altering the tumor’s energy balance (24). This intricate metabolic crosstalk offers opportunities for therapeutic intervention, such as exercise-induced adipokine secretion, which regulates tumor metabolic reprogramming and may enhance immunotherapy efficacy when combined with exercise interventions under septic conditions (25–27) (Figure 1).
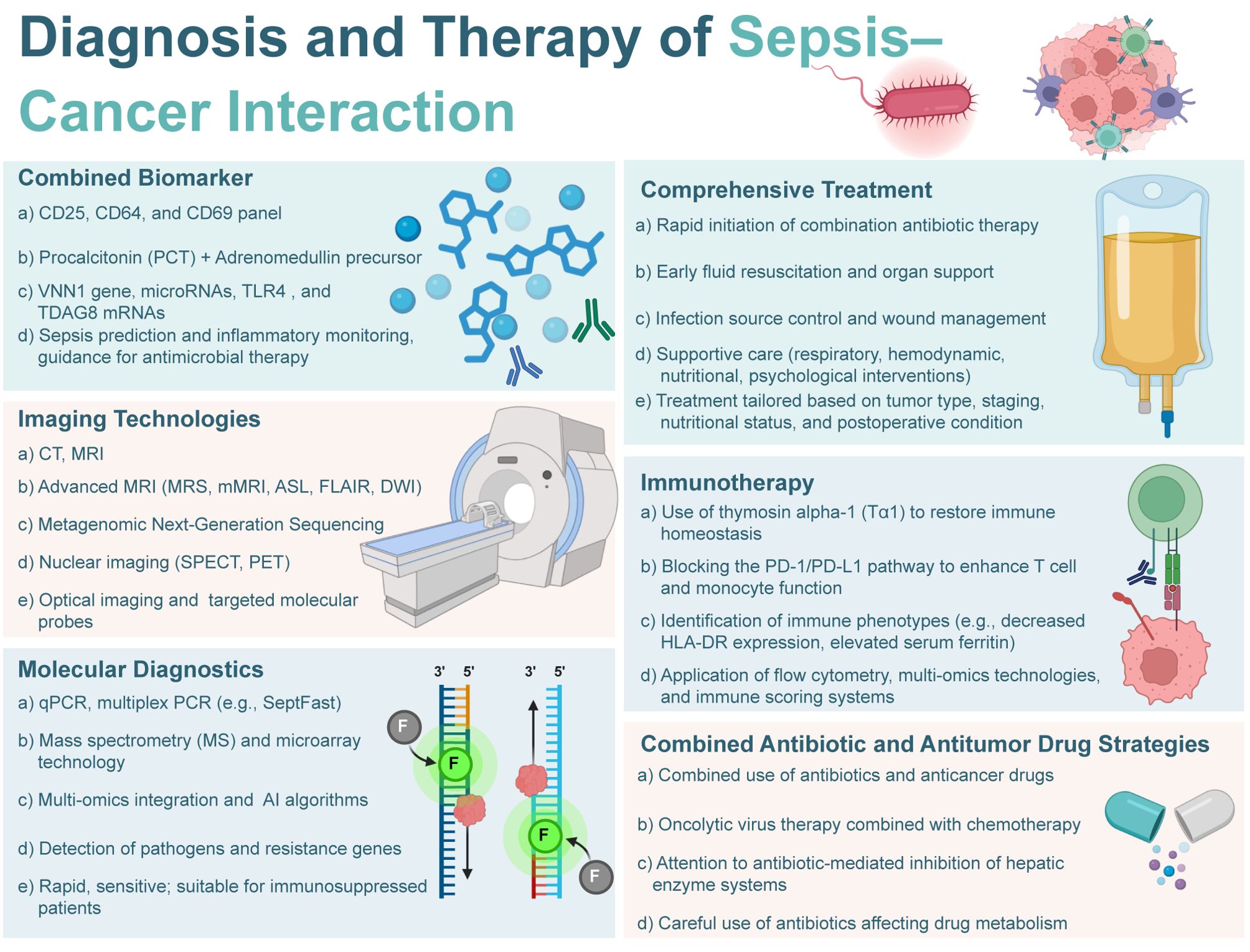
Figure 1. Diagnosis and therapy of sepsis-cancer interaction. The image provides an overview of various approaches and technologies used in the management of sepsis in cancer patients.
2 Epidemiology of sepsis and tumor interaction
2.1 Incidence and mortality of sepsis in cancer patients
Sepsis, a life threatening consequence of dysregulated host responses to infection, presents a major clinical challenge in oncology (28).Due to malignancy induced immunosuppression and aggressive anticancer therapies, cancer patients face a significantly higher risk of sepsis incidence and mortality compared to the general population (29). Contributing factors include tumor-induced immune evasion, disruption of anatomical barriers by invasive tumor growth, and immunosuppression resulting from cytotoxic therapies (30). Notably, despite their anti-inflammatory properties, statins did not confer a protective effect against sepsis in cancer patients, indicating complex immunopathological mechanisms beyond inflammation alone. Cancer stem cells further exacerbate immune evasion under septic conditions by enhancing metastatic potential and promoting drug resistance (31). Although sepsis-related mortality among cancer patients has declined in recent years—reflecting advances in oncologic care—certain subgroups remain disproportionately vulnerable (32). Hematologic malignancies, such as acute myeloid leukemia and multiple myeloma, confer particularly high sepsis risk due to severe neutropenia and bone marrow failure (33). The rising threat of antimicrobial resistance, especially infections caused by carbapenem-resistant Gram-negative bacteria, further complicates sepsis management, elevating mortality and constraining effective treatment options (34).
2.2 Impact of cancer type on sepsis incidence
Sepsis risk varies significantly by cancer type, tumor biology, and treatment modality (35). Solid tumors and hematologic malignancies exhibit distinct infection profiles (36). Recent Mendelian randomization studies have established a causal link between specific malignancies, particularly lung cancer (squamous cell carcinoma, adenocarcinoma, and small cell carcinoma), and increased sepsis susceptibility (37). This association is consistent with local tissue destruction, chronic inflammation, and opportunistic infections common in pulmonary cancers. In addition to tumor type, patient-specific factors such as advanced age, comorbidities, recurrent infections, and previous hospitalizations also contribute to an increased risk of sepsis (38). Anatomical patterns also emerge: solid tumors are often linked to intra-abdominal infections (e.g., post-surgical complications), while hematologic cancers predispose to bloodstream and pulmonary infections due to systemic immunosuppression (39). Iatrogenic factors, such as central venous catheters, chemotherapy-induced neutropenia, and mucosal barrier injury from radiotherapy, further exacerbate sepsis risk (40).
2.3 Correlation between sepsis and cancer patient prognosis
Beyond its acute mortality, sepsis exerts profound long-term effects on cancer outcomes, potentially accelerating tumor progression, promoting relapse, and reducing survival (41). Prognostic studies have identified key markers, including the neutrophil to lymphocyte ratio (NLR), brain natriuretic peptide (BNP), fluid balance, and SOFA scores, as predictors of short-term mortality in patients with sepsis and cancer (42).These markers offer promising avenues for early risk stratification and individualized management. However, the prognostic impact of sepsis is context dependent (43). For instance, in advanced epithelial ovarian cancer, sepsis did not significantly affect progression-free or overall survival, suggesting that host immune competence and tumor biology modulate outcomes (44). Notably, exercise-induced interleukin-15 (IL-15) has emerged as a potential prognostic biomarker in this setting, with serum levels positively correlating with tumor inhibition (45). This observation underscores the potential of exercise-mediated immune modulation as a therapeutic adjunct in septic oncology patients. Nonetheless, accumulating evidence supports the hypothesis that postoperative sepsis fosters tumor recurrence and worsens survival by inducing immune exhaustion and promoting tumor microenvironmental changes conducive to metastasis and angiogenesis (46). Clinically, these findings advocate for integrating sepsis prevention and rapid intervention into oncologic care protocols, emphasizing infection control, antimicrobial stewardship, and immune modulation (47).
3 Clinical manifestations of sepsis and tumor interaction
3.1 Typical clinical manifestations of sepsis in cancer patients
Sepsis, a life-threatening organ dysfunction from a dysregulated host response to infection, is particularly severe in cancer patients due to tumor- and treatment-induced immunosuppression (48). Compared to the general population, cancer patients exhibit higher sepsis incidence and 30-day mortality, driven by advanced disease, comorbidities, and immune dysfunction (49).A retrospective study of 435 ICU-admitted cancer patients identified metastatic disease, elevated serum lactate, and need for advanced life support as key mortality predictors, indicating severe physiological compromise (50). Classic signs of sepsis, including fever, leukocytosis or leukopenia, and coagulopathy, may be absent or atypical in immunocompromised patients, thereby complicating the diagnostic process (51). Hypothermia or afebrile presentations can obscure early signs, while viral endothelial injury exacerbates coagulopathy via platelet activation (52). Chronic tumor-related inflammation can further mask sepsis, requiring individualized assessment. Cancer therapies (chemotherapy, radiotherapy, targeted agents) impair immunity, while tumor invasion and surgeries disrupt barriers, facilitating infections. Infection patterns vary by cancer type: abdominal infections are common in solid tumors, and pulmonary and bloodstream infections are common in hematologic malignancies, often due to neutropenia (53). Cancer patients also face higher rates of hospital-acquired infections (HAIs), exacerbated by prolonged hospitalization, invasive procedures, and broad-spectrum antibiotics, leading to multidrug resistance (54, 55).
3.2 Diagnostic challenges of sepsis in cancer patients
Timely and accurate diagnosis of sepsis is critical in cancer patients, but oncologic care presents substantial diagnostic challenges (56). Traditional markers (e.g., CRP, PCT, leukocyte counts) have reduced sensitivity and specificity, particularly in those receiving chemotherapy or immunotherapy (57). The high prevalence of neutropenia and leukopenia further limits the diagnostic utility of conventional inflammatory parameters (58). Prior anticancer treatments further confound clinical assessment. Immunotherapy can trigger immune-related adverse events that mimic infection, while corticosteroids may suppress overt inflammatory signs (59). Additionally, paraneoplastic effects in certain cancers can distort biomarker levels, leading to false findings (60). High colonization rates, especially with indwelling devices or mucositis, increase the risk of culture contamination. These challenges underscore the need for cancer-specific diagnostic criteria for sepsis. Multifactorial strategies integrating tumor type, treatment history, immune status, infection risk, and organ function are essential (61). Combined biomarker panels (e.g., CRP, PCT, IL-6, sTREM-1) show promise, but require further validation (62). Machine learning and clinical decision support systems in electronic health records may improve early detection and risk assessment (63).
3.3 Analysis of sepsis related complications in cancer patients
Sepsis in cancer patients is associated with high rates of acute and chronic complications, contributing to poor short- and long-term outcomes (64). Multiple organ dysfunction syndrome (MODS), particularly post-surgery, is a major sequela (65). Surgical stress induces transient immunosuppression, increasing infection risk and potentially promoting tumor recurrence by impairing immune surveillance (66). Gram-negative and polymicrobial infections, often resulting from gut translocation or nosocomial sources, were prevalent, thereby complicating antimicrobial management (67). Infection profiles evolve with immunosuppression: bacterial pathogens dominate early neutropenic phases, while fungal infections (e.g., Candida, Aspergillus) emerge later (68). Antibiotic resistance and superinfections complicate therapy, necessitating a balance between empirical and targeted approaches (69). For instance, oral hydrogels may counter antibiotic-induced immunosuppression by modulating the gut microbiota–immune axis (70). The complex cancer–sepsis interplay demands individualized, multidisciplinary management (71). Collaboration among oncologists, infectious disease specialists, intensivists, and microbiologists is essential to improve outcomes (72).
4 Diagnostic technologies for the interaction between sepsis and cancer
4.1 Research on combined biomarkers for sepsis and cancer
Diagnosing sepsis in cancer patients is challenging due to overlapping tumor-related inflammatory responses (73). Traditional biomarkers like CRP and PCT lack specificity in oncology settings due to tumor-associated factors (74). To address this, combined biomarker panels have been developed. For instance, a panel including CD25, CD64, and CD69 achieved an AUC of 0.978, outperforming individual markers (Figure 2) (75). At the molecular level, VNN1 and microRNAs (miR-146a, miR-155, miR-223) are promising biomarkers (76). VNN1, involved in oxidative stress and immune modulation, correlates with both sepsis and cancer outcomes (77). MicroRNAs help differentiate septic from tumor-related inflammation (78). Emerging multi-omics approaches, integrated with machine learning, are set to enhance diagnostic strategies and individualized treatment (79–81).
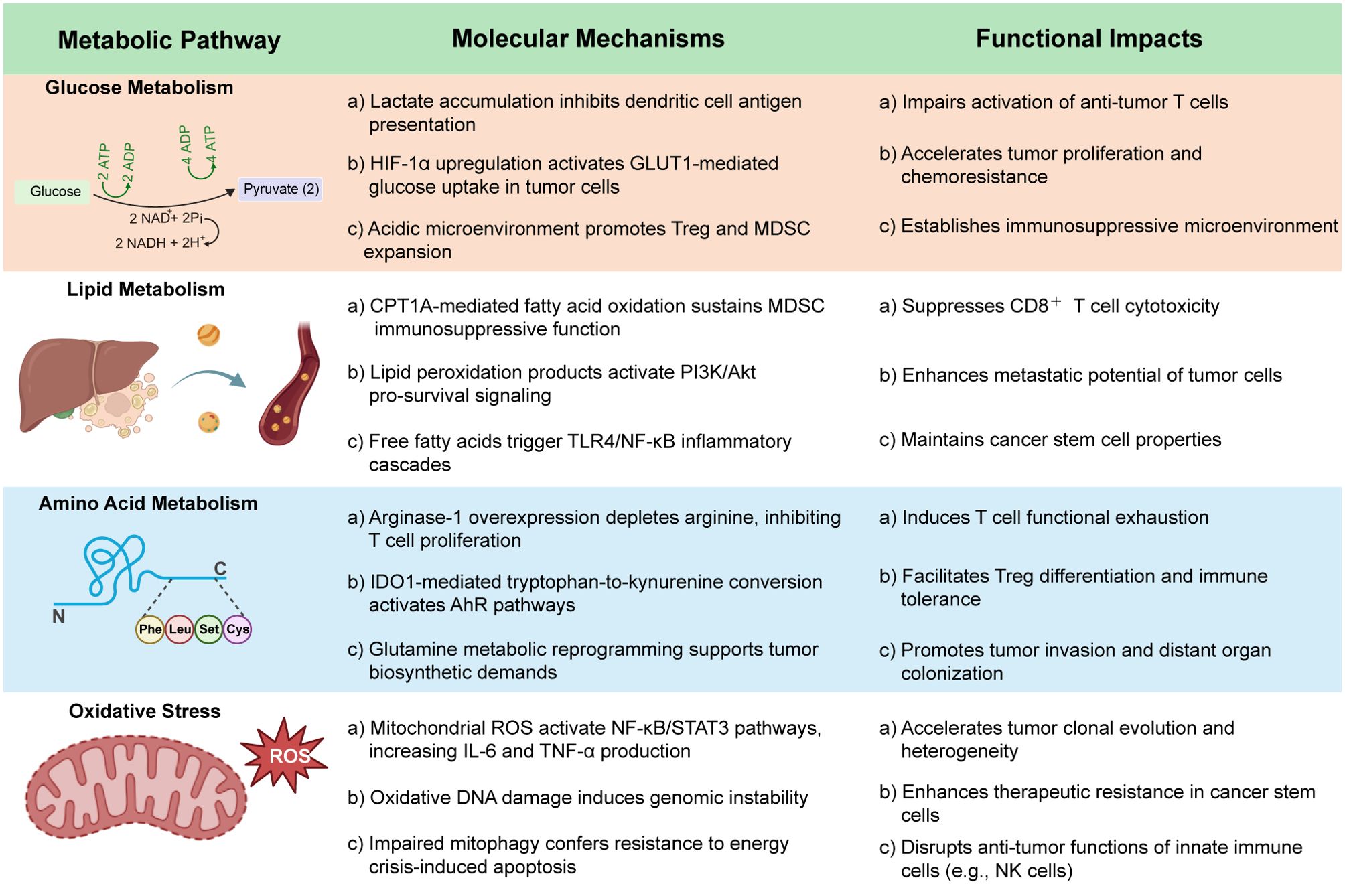
Figure 2. Sepsis-induced metabolic reprogramming in cancer immunosuppression and progression.
4.2 Application of imaging techniques in the diagnosis of sepsis and cancer
Imaging remains indispensable for the detection and management of sepsis and malignancy (79). Advanced magnetic resonance imaging (MRI) techniques, including magnetic resonance spectroscopy (MRS), molecular MRI (mMRI), arterial spin labeling (ASL), fluid-attenuated inversion recovery (FLAIR), and diffusion-weighted imaging (DWI), enable early detection of sepsis-associated encephalopathy (SAE), particularly in oncology patients whose neurological symptoms may be atypical or obscured by treatment effects (Figure 1) (82, 83). FLAIR and DWI are sensitive to white matter changes and cytotoxic edema, while MRS provides metabolic insights, facilitating timely neuroprotective interventions (84). Beyond neuroimaging, plasma metagenomic next-generation sequencing (mNGS) demonstrates superior pathogen detection compared to conventional blood cultures, which is critical in cancer patients with atypical infections (85). Advances in optical imaging, employing fluorescent and bioluminescent probes targeting bacterial structures, allow real time visualization of microbial burden, enhancing surgical and therapeutic decision making (86). Moreover, molecular diagnostics have markedly improved the sensitivity, specificity, and speed of infectious and oncologic disease detection (87).In sepsis, multi-omics approaches have identified transcriptomic, proteomic, and metabolomic signatures that define distinct disease subtypes and prognostic trajectories, promoting a shift toward precision diagnostics (88). PCR based technologies, including multiplex assays like SeptFast, allow rapid, simultaneous pathogen and resistance gene detection, significantly reducing time to treatment despite challenges such as contamination risk and limited detection of novel organisms(Figure 2) (89). Meanwhile, microarrays and nanotechnology based biosensors facilitate high throughput, point of care testing, critical for intensive care and oncology settings (90–92).The integration of multi-omics data with artificial intelligence (AI) and machine learning is an emerging frontier (93). Predictive models based on large datasets can uncover complex disease patterns, forecast therapeutic responses, and guide individualized treatment plans, greatly enhancing clinical decision making in patients navigating both cancer and sepsis (94).
5 Sepsis and cancer: integrated treatment strategies and future perspectives
5.1 Multidisciplinary approaches for managing sepsis in cancer patients
The coexistence of sepsis and cancer presents a major clinical challenge, requiring dynamic management strategies to address immune, metabolic, and physiological disruptions (95). Treatment must focus on infection control, tumor progression, immune stabilization, and preserving physiological function. Early intervention is critical, as delays in antibiotics worsen outcomes (Figure 2) (96). Multifunctional composite hydrogels offer synergistic benefits for sepsis in bone metastasis, combining immunomodulatory and osteogenic effects (97). Supportive therapies, including fluid resuscitation, hemodynamic management, respiratory support, nutrition, and psychological care, should be tailored to individual patient needs. A multidisciplinary team of intensivists, oncologists, and other specialists is essential for optimizing patient survival and care (98).
5.2 Emerging immunotherapeutic and pharmacological innovations
Advances in immunotherapy have opened new avenues for addressing the immune dysregulation inherent in both sepsis and cancer (Figure 1) (99). Non-invasive physical stimulation can enhance immune cell infiltration and mitigate T-cell depletion by altering the tumor microenvironment (100). Agents such as thymosin α-1 improve immune competence and survival in sepsis, while immune checkpoint inhibitors (ICIs) reverse T-cell exhaustion and enhance antigen presentation (101). Preclinical data indicate that anti-PD-1/PD-L1 antibodies function through Fcγ receptor-dependent mechanisms, although FcγR-independent variants may be more effective in immunocompromised settings, underscoring the need to optimize ICI formats (102). Immunotherapies also influence immune cell metabolism, particularly glycolysis and mitochondrial oxidative phosphorylation, which are critical during sepsis. Given the heterogeneity of immune status in sepsis, biomarkers like mHLA-DR and ferritin can help identify candidates for immunometabolic therapy (103). T cell therapies targeting oncogenic viral antigens may overcome antigen presentation deficits induced by sepsis, with efficacy enhanced by metabolic modulation, such as reducing lactate and promoting fatty acid oxidation. CD4+ T cells in sepsis exhibit persistent mitochondrial dysfunction and elevated glycolysis, leading to IL-17 dysregulation and impaired secondary responses (104). Targeting these pathways may restore T cell function post-sepsis. Novel delivery platforms, such as engineered bacteria, bacterial vesicles, and exosome-based systems, enable targeted delivery of metabolic modulators (e.g., NAD+ precursors, AMPK activators, and short-chain fatty acids) to immunosuppressive sites. These strategies address mitochondrial dysfunction and energy depletion characteristic of late-stage sepsis (105–109).
5.3 Personalization of therapy and optimization of drug interactions
Polypharmacy in septic cancer patients significantly increases the risk of drug–drug interactions, particularly through the modulation of cytochrome P450 enzymes by antibiotics and antifungals, thereby altering the pharmacokinetics and toxicity profiles of chemotherapeutic agents (110). To address these complexities, strategies such as therapeutic drug monitoring, pharmacogenetic testing, computer-aided drug design techniques, and AI-driven clinical decision support systems are needed (Figure 1) (111). Moreover, the transition toward personalized medicine, guided by immunophenotyping, transcriptomics, and dynamic biomarker monitoring, holds considerable promise for both sepsis and oncology care (112).Tailored treatment plans that incorporate genetic, metabolic, and immune profiles may enhance therapeutic efficacy while minimizing adverse effects, particularly in vulnerable patient populations. Prospective validation of precision-based protocols is crucial to fully realize the potential of individualized therapy in improving outcomes for patients confronting the dual burden of sepsis and malignancy.
6 Future perspectives on the interaction between sepsis and cancer
Advances in biomedical engineering, systems biology, and molecular diagnostics have propelled sepsis and cancer research (113). Technologies like high-resolution biosensors improve early detection, while CRISPR/Cas9 aids targeted drug discovery (114). Next-generation sequencing enhances pathogen identification, and AI revolutionizes risk stratification in oncologic sepsis (115, 116). These innovations drive precision diagnostics and individualized treatments. Therapeutic targets such as inflammatory caspases, PDGFB, TLR4, and PD-1/PD-L1 are being explored for their roles in immune modulation and tumor growth (117). However, ethical issues arise, particularly around consent in acute sepsis (118) and concerns over patient privacy with AI and big data (119). Addressing these is vital for equitable healthcare (120).
7 Conclusion
In conclusion, the bidirectional relationship between sepsis and cancer complicates patient management, as sepsis-induced immune dysfunction and metabolic reprogramming hinder cancer progression, impair immunotherapy, and promote metastasis. These metabolic shifts in cancer and immune cells worsen the disease, resulting in a more aggressive clinical course. To improve outcomes, integrated therapies addressing both immune and metabolic disturbances are essential. Combining immunotherapy, metabolic interventions, and antimicrobial treatments, along with identifying relevant biomarkers, could significantly enhance personalized cancer care. Ongoing research is expected to lead to better management strategies and improved prognosis for cancer patients at risk of sepsis.
Author contributions
LW: Conceptualization, Visualization, Resources, Formal Analysis, Project administration, Investigation, Methodology, Writing – review & editing, Writing – original draft, Software. CW: Investigation, Writing – original draft, Validation, Formal Analysis, Writing – review & editing, Methodology. MH: Formal Analysis, Writing – original draft, Conceptualization, Validation, Methodology, Investigation, Writing – review & editing. ZL: Conceptualization, Writing – review & editing, Supervision, Writing – original draft, Software, Visualization, Project administration.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liu Z, Ting Y, Li M, Li Y, Tan Y, and Long Y. From immune dysregulation to organ dysfunction: understanding the enigma of Sepsis. Front Microbiol. (2024) 15:1415274. doi: 10.3389/fmicb.2024.1415274
3. Dajon M, Iribarren K, and Cremer I. Toll-like receptor stimulation in cancer: A pro- and anti-tumor double-edged sword. Immunobiology. (2017) 222:89–100. doi: 10.1016/j.imbio.2016.06.009
4. Seo H, Chen J, González-Avalos E, Samaniego-Castruita D, Das A, Wang YH, et al. TOX and TOX2 transcription factors cooperate with NR4A transcription factors to impose CD8+ T cell exhaustion. Proc Natl Acad Sci USA. (2019) 116:12410–5. doi: 10.1073/pnas.1905675116
5. Huang YJ, Ngiow SF, Baxter AE, Manne S, Park SL, Wu JE, et al. Continuous expression of TOX safeguards exhausted CD8 T cell epigenetic fate. Sci Immunol. (2025) 10:eado3032. doi: 10.1126/sciimmunol.ado3032
6. Atretkhany K-SN, Drutskaya MS, Nedospasov SA, Grivennikov SI, and Kuprash DV. Chemokines, cytokines and exosomes help tumors to shape inflammatory microenvironment. Pharmacol Ther. (2016) 168:98–112. doi: 10.1016/j.pharmthera.2016.09.011
7. Takacs GP, Kreiger CJ, Luo D, Tian G, Garcia JS, Deleyrolle LP, et al. Glioma-derived CCL2 and CCL7 mediate migration of immune suppressive CCR2+/CX3CR1+ M-MDSCs into the tumor microenvironment in a redundant manner. Front Immunol. (2023) 13:993444. doi: 10.3389/fimmu.2022.993444
8. Kessenbrock K, Plaks V, and Werb Z. Matrix metalloproteinases: regulators of the tumor microenvironment. Cell. (2010) 141:52–67. doi: 10.1016/j.cell.2010.03.015
9. He X, Ma Y, Wen Y, Zhang R, Zhao D, Wang G, et al. Tumor-derived apoptotic extracellular vesicle-mediated intercellular communication promotes metastasis and stemness of lung adenocarcinoma. Bioact Mater. (2024) 36:238–55. doi: 10.1016/j.bioactmat.2024.02.026
10. Boucher J and Carpenter D. Sepsis: symptoms, assessment, diagnosis, and the hour-1 bundle in patients with cancer. CJON. (2020) 24:99–102. doi: 10.1188/20.CJON.99-102
11. Talmadge JE. Pathways mediating the expansion and immunosuppressive activity of myeloid-derived suppressor cells and their relevance to cancer therapy. Clin Cancer Res. (2007) 13:5243–8. doi: 10.1158/1078-0432.CCR-07-0182
12. Wu D-D, Li T, and Ji X-Y. Dendritic cells in sepsis: pathological alterations and therapeutic implications. J Immunol Res. (2017) 2017:1–9. doi: 10.1155/2017/3591248
13. Llitjos J-F, Auffray C, Alby-Laurent F, Rousseau C, Merdji H, Bonilla N, et al. Sepsis-induced expansion of granulocytic myeloid-derived suppressor cells promotes tumour growth through Toll-like receptor 4: Sepsis-induced MDSC and tumour growth. J Pathol. (2016) 239:473–83. doi: 10.1002/path.4744
14. Chandrasekar SV, Singh A, and Ranjan A. Overcoming resistance to immune checkpoint inhibitor therapy using calreticulin-inducing nanoparticle. Pharmaceutics. (2023) 15:1693. doi: 10.3390/pharmaceutics15061693
15. Hamada Y, Tanoue K, Arigami T, Yamakuchi M, Okawa M, Matsushita D, et al. The vascular endothelial growth factor-A121/vascular endothelial growth factor-A165 ratio as a predictor of the therapeutic response to immune checkpoint inhibitors in gastric cancer. Cancers. (2024) 16:3958. doi: 10.3390/cancers16233958
16. Peighambari A, Huang H, Metzger P, Adlesic M, Zodel K, Schäfer S, et al. Characterisation of an autochthonous mouse ccRCC model of immune checkpoint inhibitor therapy resistance. Sci Rep. (2025) 15:19818. doi: 10.1038/s41598-025-04917-1
17. Kooshan Z, Cárdenas-Piedra L, Clements J, and Batra J. Glycolysis, the sweet appetite of the tumor microenvironment. Cancer Lett. (2024) 600:217156. doi: 10.1016/j.canlet.2024.217156
18. Andersen SK, Gjedsted J, Christiansen C, and Tønnesen E. The roles of insulin and hyperglycemia in sepsis pathogenesis. J Leukoc Biol. (2004) 75:413–21. doi: 10.1189/jlb.0503195
19. Mirouse A, Vigneron C, Llitjos J-F, Chiche J-D, Mira J-P, Mokart D, et al. Sepsis and cancer: an interplay of friends and foes. Am J Respir Crit Care Med. (2020) 202:1625–35. doi: 10.1164/rccm.202004-1116TR
20. Wang E, Wu M-Y, Ren Z, Zheng Y, Ye RD, Tan CSH, et al. Targeting macrophage autophagy for inflammation resolution and tissue repair in inflammatory bowel disease. Burns Trauma. (2023) 11:tkad004. doi: 10.1093/burnst/tkad004
21. Gu J, Zhou J, Chen Q, Xu X, Gao J, Li X, et al. Tumor metabolite lactate promotes tumorigenesis by modulating MOESIN lactylation and enhancing TGF-β signaling in regulatory T cells. Cell Rep. (2022) 39:110986. doi: 10.1016/j.celrep.2022.110986
22. Vigneron C, Mirouse A, Merdji H, Rousseau C, Cousin C, Alby-Laurent F, et al. Sepsis inhibits tumor growth in mice with cancer through Toll-like receptor 4-associated enhanced Natural Killer cell activity. OncoImmunology. (2019) 8:e1641391. doi: 10.1080/2162402X.2019.1641391
23. Cornwell A, Ziółkowski H, and Badiei A. Glucose transporter glut1-dependent metabolic reprogramming regulates lipopolysaccharide-induced inflammation in RAW264.7 macrophages. Biomolecules. (2023) 13:770. doi: 10.3390/biom13050770
24. Zhang J, Huang D, Dai Y, and Xia Y-F. Sinomenine ameliorates colitis-associated cancer by modulating lipid metabolism via enhancing CPT1A expression. Metabolites. (2022) 12:946. doi: 10.3390/metabo12100946
25. Agustiningsih D and Wibawa T. Demystifying roles of exercise in immune response regulation against acute respiratory infections: A narrative review. Sports Med Health Sci. (2024) 6:139–53. doi: 10.1016/j.smhs.2024.01.004
26. Qian Y, Bu Z, Qin Y, Qian S, Qin L, Zhou S, et al. Exploring the role of adipokines in exercise-induced inhibition of tumor growth. Sports Med Health Sci. (2025) 7:143–56. doi: 10.1016/j.smhs.2024.03.006
27. Liu J, Liu W, Wan Y, and Mao W. Crosstalk between exercise and immunotherapy: current understanding and future directions. Research. (2024) 7:360. doi: 10.34133/research.0360
28. Bode C, Weis S, Sauer A, Wendel-Garcia P, and David S. Targeting the host response in sepsis: current approaches and future evidence. Crit Care. (2023) 27:478. doi: 10.1186/s13054-023-04762-6
29. Nates JL, Pène F, Darmon M, Mokart D, Castro P, David S, et al. Septic shock in the immunocompromised cancer patient: a narrative review. Crit Care. (2024) 28:285. doi: 10.1186/s13054-024-05073-0
30. Fang J, Lin L, Cao Y, Tan J, Liang Y, Xiao X, et al. Targeting the CD24-siglec10 axis: A potential strategy for cancer immunotherapy. BIOI. (2024) 5:e997. doi: 10.15212/bioi-2023-0022
31. Dakal TC, Bhushan R, Xu C, Gadi BR, Cameotra SS, Yadav V, et al. Intricate relationship between cancer stemness, metastasis, and drug resistance. MedComm. (2024) 5:e710. doi: 10.1002/mco2.710
32. Hensley MK, Donnelly JP, Carlton EF, and Prescott HC. Epidemiology and outcomes of cancer-related versus non–cancer-related sepsis hospitalizations*. Crit Care Med. (2019) 47:1310–6. doi: 10.1097/CCM.0000000000003896
33. Rosenberg PS. The incidence of leukemia and mortality from sepsis in patients with severe congenital neutropenia receiving long-term G-CSF therapy. Blood. (2006) 107:4628–35. doi: 10.1182/blood-2005-11-4370
34. Kaye KS and Pogue JM. Infections caused by resistant gram-negative bacteria: epidemiology and management. Pharmacotherapy. (2015) 35:949–62. doi: 10.1002/phar.1636
35. Shvetsov YB, Ogino MH, Glibetic N, Asato CB, Wilkens LR, Le Marchand L, et al. Association of sepsis mortality with specific cancer sites and treatment type: the multiethnic cohort study. JPM. (2021) 11:146. doi: 10.3390/jpm11020146
36. Marin M, Gudiol C, Ardanuy C, Garcia-Vidal C, Calvo M, Arnan M, et al. Bloodstream infections in neutropenic patients with cancer: Differences between patients with haematological Malignancies and solid tumours. J Infect. (2014) 69:417–23. doi: 10.1016/j.jinf.2014.05.018
37. Cheng H, Wang X, Yao J, Guo N, and Liu J. Assessing the causal relationship between non-small cell lung cancer and sepsis: a Mendelian randomization study. BMC Cancer. (2024) 24:1233. doi: 10.1186/s12885-024-13003-0
38. Perdikouri EIA, Arvaniti K, Lathyris D, Apostolidou Kiouti F, Siskou E, Haidich AB, et al. Infections due to multidrug-resistant bacteria in oncological patients: insights from a five-year epidemiological and clinical analysis. Microorganisms. (2019) 7:277. doi: 10.3390/microorganisms7090277
39. Rolston KVI. Infections in cancer patients with solid tumors: A review. Infect Dis Ther. (2017) 6:69–83. doi: 10.1007/s40121-017-0146-1
40. O’Brien SN, Blijlevens NMA, Mahfouz TH, and Anaissie EJ. Infections in patients with hematological cancer: recent developments. Hematology. (2003) 2003:438–72. doi: 10.1182/asheducation-2003.1.438
41. Williams JC, Ford ML, and Coopersmith CM. Cancer and sepsis. Clin Sci. (2023) 137:881–93. doi: 10.1042/CS20220713
42. Jain PK, Seval M, Meena V, and Meena DK. Predictive value of neutrophil-to-lymphocyte ratio in in-hospital mortality in sepsis patients: A cross-sectional study. J Acute Dis. (2024) 13:106–10. doi: 10.4103/jad.jad_63_24
43. Knaus WA, Wagner DP, Harrell FE, Draper EA, and Reinhart K. What Determines Prognosis in Sepsis? Evidence for a Comprehensive Individual Patient Risk Assessment Approach to the Design and Analysis of Clinical Trials. In: Eyrich K and Sprung C, editors. Sepsis. Update in Intensive Care and Emergency Medicine. Springer Berlin Heidelberg, Berlin, Heidelberg (1994). p. 23–37. doi: 10.1007/978-3-642-85036-3_3
44. Said SA, De Hullu JA, van der Aa MA, Walraven JEW, Bekkers RLM, Slangen BFM, et al. Impact of sepsis on the oncologic outcomes of advanced epithelial ovarian cancer patients: A multicenter observational study. Cancers. (2023) 15:4642. doi: 10.3390/cancers15184642
45. Luo Z, He Z, Qin H, Chen Y, Qi B, Lin J, et al. Exercise-induced IL-15 acted as a positive prognostic implication and tumor-suppressed role in pan-cancer. Front Pharmacol. (2022) 13:1053137. doi: 10.3389/fphar.2022.1053137
46. Cheng X, Zhang H, Hamad A, Huang H, and Tsung A. Surgery-mediated tumor-promoting effects on the immune microenvironment. Semin Cancer Biol. (2022) 86:408–19. doi: 10.1016/j.semcancer.2022.01.006
47. Shelton B, Stanik-Hutt J, Kane J, and Jones R. Implementing the surviving sepsis campaign in an ambulatory clinic for patients with hematologic Malignancies. CJON. (2016) 20:281–8. doi: 10.1188/16.CJON.281-288
48. Hattori Y, Hattori K, Suzuki T, and Matsuda N. Recent advances in the pathophysiology and molecular basis of sepsis-associated organ dysfunction: Novel therapeutic implications and challenges. Pharmacol Ther. (2017) 177:56–66. doi: 10.1016/j.pharmthera.2017.02.040
49. Liu MA, Bakow BR, Hsu T-C, Chen J-Y, Su K-Y, Asiedu EK, et al. Temporal trends in sepsis incidence and mortality in patients with cancer in the US population. Am J Crit Care. (2021) 30:e71–9. doi: 10.4037/ajcc2021632
50. Awad WB, Nazer L, Elfarr S, Abdullah M, and Hawari F. A 12-year study evaluating the outcomes and predictors of mortality in critically ill cancer patients admitted with septic shock. BMC Cancer. (2021) 21:709. doi: 10.1186/s12885-021-08452-w
51. McCreery RJ, Florescu DF, and Kalil AC. Sepsis in immunocompromised patients without human immunodeficiency virus. J Infect Dis. (2020) 222:S156–65. doi: 10.1093/infdis/jiaa320
52. Martio AE, Soares PDMR, Karam OR, Padua WL, Manzato LB, and Mesquita Filho PM. Intracranial hemorrhage and Covid-19: A retrospective analysis of 1675 hospitalized Covid-19 Brazilian patients. Brain Hemorrhages. (2023) 4:57–64. doi: 10.1016/j.hest.2023.01.002
53. Bodey GP. Infection in cancer patients: A continuing association. Am J Med. (1986) 81:11–26. doi: 10.1016/0002-9343(86)90510-3
54. Mayhall CG, Craven DE, Steger KA, and Hirschhorn LR. Nosocomial colonization and infection in persons infected with human immunodeficiency virus. Infect Control Hosp Epidemiol. (1996) 17:304–18. doi: 10.1086/647300
55. Cornejo-Juárez P, Vilar-Compte D, Pérez-Jiménez C, Ñamendys-Silva SA, Sandoval-Hernández S, and Volkow-Fernández P. The impact of hospital-acquired infections with multidrug-resistant bacteria in an oncology intensive care unit. Int J Infect Dis. (2015) 31:31–4. doi: 10.1016/j.ijid.2014.12.022
56. Gotts JE and Matthay MA. Sepsis: pathophysiology and clinical management. BMJ. (2016) 353:i1585. doi: 10.1136/bmj.i1585
57. Ebihara Y, Kobayashi K, Ishida A, Maeda T, Takahashi N, Taji Y, et al. Diagnostic performance of procalcitonin, presepsin, and C-reactive protein in patients with hematological Malignancies. Clin Lab Anal. (2017) 31:e22147. doi: 10.1002/jcla.22147
58. Dubinina YN, Sarzhevskii VO, and Melnichenko V. Role of biochemical inflammatory markers in patients with chemotherapy-induced neutropenia. Клиническая онкогематология. (2019) 12:101–7. doi: 10.21320/2500-2139-2019-12-4-461-467
59. Fishman JA, Hogan JI, and Maus MV. Inflammatory and infectious syndromes associated with cancer immunotherapies. Clin Infect Dis. (2019) 69:909–20. doi: 10.1093/cid/ciy1025
60. Luzak A, Schnell-Inderst P, Bühn S, Mayer-Zitarosa A, and Siebert U. Clinical effectiveness of cancer screening biomarker tests offered as self-pay health service: a systematic review. Eur J Public Health. (2016) 26:498–505. doi: 10.1093/eurpub/ckv227
61. Pomakova D and Segal BH. Prevention of Infection in Cancer Patients. In: Stosor V and Zembower TR, editors. Infectious Complications in Cancer Patients. Cancer Treatment and Research. Springer International Publishing, Cham (2014). p. 485–511. doi: 10.1007/978-3-319-04220-6_16
62. Kofoed K, Andersen O, Kronborg G, Tvede M, Petersen J, Eugen-Olsen J, et al. Use of plasma C-reactive protein, procalcitonin, neutrophils, macrophage migration inhibitory factor, soluble urokinase-type plasminogen activator receptor, and soluble triggering receptor expressed on myeloid cells-1 in combination to diagnose infections: a prospective study. Crit Care. (2007) 11:R38. doi: 10.1186/cc5723
63. Gomathy DCK, Bathrinathan SR, and Sripada SKA. STUDY ON MACHINE LEARNING IN ENHANCING CLINICAL DECISION SUPPORT SYSTEMS. IJSREM. (2023) 07:1–11. doi: 10.55041/IJSREM26769
64. Danai PA, Moss M, Mannino DM, and Martin GS. The epidemiology of sepsis in patients with Malignancy. Chest. (2006) 129:1432–40. doi: 10.1378/chest.129.6.1432
65. Barie PS and Hydo LJ. Epidemiology of multiple organ dysfunction syndrome in critical surgical illness. Surg Infect. (2000) 1:173–86. doi: 10.1089/109629600750018105
66. Hogan BV, Peter MB, Shenoy HG, Horgan K, and Hughes TA. Surgery induced immunosuppression. Surgeon. (2011) 9:38–43. doi: 10.1016/j.surge.2010.07.011
67. MacFie J, O’Boyle C, Mitchell CJ, Buckley PM, Johnstone D, and Sudworth P. Gut origin of sepsis: a prospective study investigating associations between bacterial translocation, gastric microflora, and septic morbidity. Gut. (1999) 45:223–8. doi: 10.1136/gut.45.2.223
68. Wingard JR. Stem Cell Transplantation. In: Kleinberg M, editor. Managing Infections in Patients With Hematological Malignancies. Humana Press, Totowa, NJ (2009). p. 211–31. doi: 10.1007/978-1-59745-415-5_8
69. Karam G, Chastre J, Wilcox MH, and Vincent J-L. Antibiotic strategies in the era of multidrug resistance. Crit Care. (2016) 20:136. doi: 10.1186/s13054-016-1320-7
70. Li L, He S, Liao B, Wang M, Lin H, Hu B, et al. Orally administrated hydrogel harnessing intratumoral microbiome and microbiota-related immune responses for potentiated colorectal cancer treatment. Research. (2024) 7:364. doi: 10.34133/research.0364
71. Gudiol C, Albasanz-Puig A, Cuervo G, and Carratalà J. Understanding and managing sepsis in patients with cancer in the era of antimicrobial resistance. Front Med. (2021) 8:636547. doi: 10.3389/fmed.2021.636547
72. Nassar AP, Dettino ALA, Amendola CP, Dos Santos RA, Forte DN, and Caruso P. Oncologists’ and intensivists’ Attitudes toward the care of critically ill patients with cancer. J Intensive Care Med. (2019) 34:811–7. doi: 10.1177/0885066617716105
73. Gunsolus IL, Sweeney TE, Liesenfeld O, and Ledeboer NA. Diagnosing and managing sepsis by probing the host response to infection: advances, opportunities, and challenges. J Clin Microbiol. (2019) 57:e00425–19. doi: 10.1128/JCM.00425-19
74. Moschetti G, Markovic U, Carco D, Iachelli V, Guardo P, Milone GA, et al. Utility of procalcitonin and interleukin-6 as severe infection biomarkers in adulthematological and oncological patients. Real-life single center prospective observational study. Blood. (2022) 140:12931–2. doi: 10.1182/blood-2022-166369
75. Liu Y, Hou J, Li Q, Chen K, Wang S-N, and Wang J. Biomarkers for diagnosis of sepsis in patients with systemic inflammatory response syndrome: a systematic review and meta-analysis. SpringerPlus. (2016) 5:2091. doi: 10.1186/s40064-016-3591-5
76. Aziz F. The emerging role of miR-223 as novel potential diagnostic and therapeutic target for inflammatory disorders. Cell Immunol. (2016) 303:1–6. doi: 10.1016/j.cellimm.2016.04.003
77. Qin W, Kang M, Li C, Zheng W, and Guo Q. VNN1 overexpression in pancreatic cancer cells inhibits paraneoplastic islet function by increasing oxidative stress and inducing β−cell dedifferentiation. Oncol Rep. (2023) 49:120. doi: 10.3892/or.2023.8557
78. Shomali N, Mahmoodpoor A, Abbas Abad AN, Marofi F, Akbari M, Xu H, et al. The relationship between extracellular/intracellular microRNAs and TLRs may be used as a diagnostic and therapeutic approach in sepsis. Immunol Investig. (2022) 51:154–69. doi: 10.1080/08820139.2020.1817067
79. Ahmed Z, Mohamed K, Zeeshan S, and Dong X. Artificial intelligence with multi-functional machine learning platform development for better healthcare and precision medicine. Database. (2020) 2020):baaa010. doi: 10.1093/database/baaa010
80. Dar MA, Arafah A, Bhat KA, Khan A, Khan MS, Ali A, et al. Multiomics technologies: role in disease biomarker discoveries and therapeutics. Briefings Funct Genomics. (2023) 22:76–96. doi: 10.1093/bfgp/elac017
81. Huang J, Chen Y, Guo Z, Yu Y, Zhang Y, Li P, et al. Prospective study and validation of early warning marker discovery based on integrating multi-omics analysis in severe burn patients with sepsis. Burns Trauma. (2023) 11:tkac050. doi: 10.1093/burnst/tkac050
82. Young GB. Encephalopathy of infection and systemic inflammation. J Clin Neurophysiol. (2013) 30:454–61. doi: 10.1097/WNP.0b013e3182a73d83
83. Tang P, Liu Y, Peng S, Cai Z, Tang G, Zhou Z, et al. Cerebral [18F]AIF-FAPI-42-based PET imaging of fibroblast activation protein for non-invasive quantification of fibrosis after ischemic stroke. Transl Stroke Res. (2025) 16:848–58. doi: 10.1007/s12975-024-01269-2
84. Lin A, Ross BD, Harris K, and Wong W. Efficacy of proton magnetic resonance spectroscopy in neurological diagnosis and neurotherapeutic decision making. Neurotherapeutics. (2005) 2:197–214. doi: 10.1602/neurorx.2.2.197
85. Schulz E, Grumaz S, Hatzl S, Gornicec M, Valentin T, Huber-Kraßnitzer B, et al. Pathogen detection by metagenomic next-generation sequencing during neutropenic fever in patients with hematological Malignancies. Open Forum Infect Dis. (2022) 9:ofac393. doi: 10.1093/ofid/ofac393
86. Jiang T, Bai X, and Li M. Advances in the development of bacterial bioluminescence imaging. Annu Rev Anal Chem. (2024) 17:265–88. doi: 10.1146/annurev-anchem-061622-034229
87. Liu Q, Jin X, Cheng J, Zhou H, Zhang Y, and Dai Y. Advances in the application of molecular diagnostic techniques for the detection of infectious disease pathogens (Review). Mol Med Rep. (2023) 27:104. doi: 10.3892/mmr.2023.12991
88. Reinhart K, Bauer M, Riedemann NC, and Hartog CS. New approaches to sepsis: molecular diagnostics and biomarkers. Clin Microbiol Rev. (2012) 25:609–34. doi: 10.1128/CMR.00016-12
89. Tziolos N and Giamarellos-Bourboulis EJ. Contemporary approaches to the rapid molecular diagnosis of sepsis. Expert Rev Mol Diagn. (2016) 16:1201–7. doi: 10.1080/14737159.2016.1246958
90. Noah NM and Ndangili PM. Current trends of nanobiosensors for point-of-care diagnostics. J Anal Methods Chem. (2019) 2019:1–16. doi: 10.1155/2019/2179718
91. Tang H, Pouri H, Lu C, and Zhang J. Rapid detection of spermine by using a cost-effective carbon nanostructured aptasensor. Nano TransMed. (2024) 3:100037. doi: 10.1016/j.ntm.2024.100037
93. He X, Liu X, Zuo F, Shi H, and Jing J. Artificial intelligence-based multi-omics analysis fuels cancer precision medicine. Semin Cancer Biol. (2023) 88:187–200. doi: 10.1016/j.semcancer.2022.12.009
94. Liu AC, Patel K, Vunikili RD, Johnson KW, Abdu F, Belman SK, et al. Sepsis in the era of data-driven medicine: personalizing risks, diagnoses, treatments and prognoses. Briefings Bioinf. (2020) 21:1182–95. doi: 10.1093/bib/bbz059
95. Thirumala R, Ramaswamy M, and Chawla S. Diagnosis and management of infectious complications in critically ill patients with cancer. Crit Care Clinics. (2010) 26:59–91. doi: 10.1016/j.ccc.2009.09.007
96. Liu VX, Fielding-Singh V, Greene JD, Baker JM, Iwashyna TJ, Bhattacharya J, et al. The timing of early antibiotics and hospital mortality in sepsis. Am J Respir Crit Care Med. (2017) 196:856–63. doi: 10.1164/rccm.201609-1848OC
97. He Y, Luo Z, Wan R, Lin J, Lu S, Li F, et al. An injectable multi-functional composite bioactive hydrogel for bone regeneration via immunoregulatory and osteogenesis effects. Adv Compos Hybrid Mater. (2024) 8:128. doi: 10.2139/ssrn.4909774
98. Biskup E, Cai F, Vetter M, and Marsch S. Oncological patients in the intensive care unit: prognosis, decision-making, therapies and end-of-life care. Swiss Med Wkly. (2017) 147:w14481. doi: 10.4414/smw.2017.14481
99. Davies R, O’Dea K, and Gordon A. Immune therapy in sepsis: Are we ready to try again? J Intensive Care Soc. (2018) 19:326–44. doi: 10.1177/1751143718765407
100. Guo Z, Saw PE, and Jon S. Non-invasive physical stimulation to modulate the tumor microenvironment: unveiling a new frontier in cancer therapy. BIOI. (2024) 5:e986. doi: 10.15212/bioi-2024-0012
101. Payen D, Monneret G, and Hotchkiss R. Immunotherapy - a potential new way forward in the treatment of sepsis. Crit Care. (2013) 17:118. doi: 10.1186/cc12490
102. Dahan R, Sega E, Engelhardt J, Selby M, Korman AJ, and Ravetch JV. FcγRs modulate the anti-tumor activity of antibodies targeting the PD-1/PD-L1 axis. Cancer Cell. (2015) 28:543. doi: 10.1016/j.ccell.2015.09.011
103. Venet F, Lukaszewicz A-C, Payen D, Hotchkiss R, and Monneret G. Monitoring the immune response in sepsis: a rational approach to administration of immunoadjuvant therapies. Curr Opin Immunol. (2013) 25:477–83. doi: 10.1016/j.coi.2013.05.006
104. Assis PA, Allen RM, Schaller MA, Kunkel SL, and Bermick JR. Metabolic reprogramming and dysregulated IL-17 production impairs CD4 T cell function post sepsis. iScience. (2024) 27:110114. doi: 10.1016/j.isci.2024.110114
105. Xu G, Li J, Zhang S, Cai J, Deng X, Wang Y, et al. Two-dimensional nano-biomaterials in regulating the tumor microenvironment for immunotherapy. Nano TransMed. (2024) 3:100045. doi: 10.1016/j.ntm.2024.100045
106. Liang H, Lu Q, Yang J, and Yu G. Supramolecular biomaterials for cancer immunotherapy. Research. (2023) 6:211. doi: 10.34133/research.0211
107. Wang H, Zhang W, Sun Y, Xu X, Chen X, Zhao K, et al. Nanotherapeutic strategies exploiting biological traits of cancer stem cells. Bioact Mater. (2025) 50:61–94. doi: 10.1016/j.bioactmat.2025.03.016
108. Li G, Jin Q, Xia F, Fu S, Zhang X, Xiao H, et al. Smart stimuli-responsive carrier-free nanoassembly of SN38 prodrug as efficient chemotherapeutic nanomedicine. Acta Materia Med. (2023) 2:54–63. doi: 10.15212/AMM-2023-0003
109. Grewal AK and Salar RK. Chitosan nanoparticle delivery systems: An effective approach to enhancing efficacy and safety of anticancer drugs. Nano TransMed. (2024) 3:100040. doi: 10.1016/j.ntm.2024.100040
110. Mani S, Ghalib M, Chaudhary I, and Goel S. Alterations of chemotherapeutic pharmacokinetic profiles by drug–drug interactions. Expert Opin Drug Metab Toxicol. (2009) 5:109–30. doi: 10.1517/17425250902753212
111. Wu Z, Chen S, Wang Y, Li F, Xu H, Li M, et al. Current perspectives and trend of computer-aided drug design: a review and bibliometric analysis. Int J Surg. (2024) 110:3848–78. doi: 10.1097/JS9.0000000000001289
112. Drury SK, Wallet SM, Maile R, Efron PA, Mohr AM, and Bible L. Current updates in precision and personalized medicine in sepsis and trauma. Surgery. (2024) 176:541–3. doi: 10.1016/j.surg.2024.03.048
113. Schenz J, Weigand MA, and Uhle F. Molecular and biomarker-based diagnostics in early sepsis: current challenges and future perspectives. Expert Rev Mol Diagn. (2019) 19:1069–78. doi: 10.1080/14737159.2020.1680285
114. Jacinto FV, Link W, and Ferreira BI. CRISPR/Cas9-mediated genome editing: From basic research to translational medicine. J Cell Mol Medi. (2020) 24:3766–78. doi: 10.1111/jcmm.14916
115. Li F, Wang S, Gao Z, Qing M, Pan S, Liu Y, et al. Harnessing artificial intelligence in sepsis care: advances in early detection, personalized treatment, and real-time monitoring. Front Med. (2025) 11:1510792. doi: 10.3389/fmed.2024.1510792
116. Sharma R and Malviya R. Modifying the electrical, optical, and magnetic properties of cancer cells: A comprehensive approach for cancer management. Med Adv. (2024) 2:3–19. doi: 10.1002/med4.51
117. Yang Y, Chen M, Qiu Y, Li X, Huang Y, and Zhang W. The Apelin/APLNR system modulates tumor immune response by reshaping the tumor microenvironment. Gene. (2022) 834:146564. doi: 10.1016/j.gene.2022.146564
118. Luce JM. Research ethics and consent in the intensive care unit. Curr Opin Crit Care. (2003) 9:540–4. doi: 10.1097/00075198-200312000-00013
119. Murdoch B. Privacy and artificial intelligence: challenges for protecting health information in a new era. BMC Med Ethics. (2021) 22:122. doi: 10.1186/s12910-021-00687-3
Keywords: sepsis, cancer, metabolic reprogramming, immunotherapy, metastasis, biomarkers
Citation: Wang L, Wu C, Hou M and Li Z (2025) Sepsis-driven metabolic reprogramming shapes cancer immunotherapy efficacy, metastatic potential, and drug sensitivity. Front. Immunol. 16:1642477. doi: 10.3389/fimmu.2025.1642477
Received: 06 June 2025; Accepted: 12 August 2025;
Published: 01 September 2025.
Edited by:
Qi Zhang, Yale University, United StatesReviewed by:
Mahmood Al-Maqbali, Rosalind Franklin University Health System, United StatesDawei Chen, University of Liège, Belgium
Copyright © 2025 Wang, Wu, Hou and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhiwei Li, bGl6aGl3ZWlAeGpybXl5LmNvbQ==; Ming Hou, MTg3MzQ3MzEwQHFxLmNvbQ==