 Martin Schmidauer1
Martin Schmidauer1 Klaus Berek1
Klaus Berek1 Michael Auer1
Michael Auer1 Gabriel Bsteh2,3
Gabriel Bsteh2,3 Paola Cavalla4
Paola Cavalla4 Franziska Di Pauli1
Franziska Di Pauli1 Massimiliano Di Filippo5
Massimiliano Di Filippo5 Florian Deisenhammer1
Florian Deisenhammer1 Andreja Emeršič6,7Fabian Föttinger2
Andreja Emeršič6,7Fabian Föttinger2 Lorenzo Gaetani5Michaela Hassler8
Lorenzo Gaetani5Michaela Hassler8 Nik Krajnc2,3
Nik Krajnc2,3 Dejan Milosavljevic8
Dejan Milosavljevic8 Markus Ponleitner2,3
Markus Ponleitner2,3 Thor Petersen9Stefan Presslauer10
Thor Petersen9Stefan Presslauer10 Igal Rosenstein11Uroš Rot6,7Caroline Winther Tørring12
Igal Rosenstein11Uroš Rot6,7Caroline Winther Tørring12 Domizia Vecchio13
Domizia Vecchio13 Marco Vercellino4
Marco Vercellino4 Tobias Zrzavy2,3
Tobias Zrzavy2,3 Anne Zinganell1
Anne Zinganell1 Janette Walde14
Janette Walde14 Harald Hegen1*
Harald Hegen1*- 1Department of Neurology, Medical University of Innsbruck, Innsbruck, Austria
- 2Department of Neurology, Medical University of Vienna, Vienna, Austria
- 3Comprehensive Center for Clinical Neurosciences and Mental Health, Medical University of Vienna, Vienna, Austria
- 4Multiple Sclerosis Center and Neurologia I U, Department of Neuroscience and Mental Health, Azienda Ospedaliero - Universitaria (AOU) Città della Salute e della Scienza di Torino, Torino, Italy
- 5Section of Neurology, Department of Medicine and Surgery, University of Perugia, Perugia, Italy
- 6Department of Neurology, University Medical Center Ljubljana, Ljubljana, Slovenia
- 7Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia
- 8FH Campus Wien, University of Applied Sciences, Vienna, Austria
- 9Sygehus Sønderjylland, Department of Regional Health Research, University Hospital of Southern Denmark, Hadersleben, Denmark
- 10Department of Neurology, Klinikum Ottakring, Vienna, Austria
- 11Department of Clinical Neuroscience, Institute of Neuroscience and Physiology at Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 12Department of Neurology, Aarhus University Hospital, Aarhus, Denmark
- 13Neurology Unit, Department of Translational Medicine, Maggiore della Carità University Hospital, Novara, Italy
- 14Department of Statistics, Faculty of Economics and Statistics, University of Innsbruck, Innsbruck, Austria
Background: The kappa free light chain (κ-FLC) index is a well-established biomarker in multiple sclerosis (MS). While the prognostic value of the κ-FLC index has been demonstrated in early relapsing–remitting MS, its prognostic value in primary progressive MS (PPMS) has not yet been investigated.
Methods: In this multicenter, retrospective cohort study, patients diagnosed with PPMS with diagnostic lumbar puncture and clinical follow-up of at least 12 months were recruited from nine MS centers across five countries. At baseline, age, sex, disease duration, and the number of T2 hyperintense (T2L) and contrast-enhancing T1 lesions (CEL) on MRI were determined. κ-FLC was measured using nephelometry/turbidimetry, and the κ-FLC index was calculated as (CSF κ-FLC/serum κ-FLC)/albumin quotient. At follow-up, the occurrence of disability progression and the administration of disease-modifying treatment (DMT) were registered. The primary endpoint was time to disability progression.
Results: A total of 121 PPMS patients were included with a median age of 53 years (25th–75th percentile: 46–59) and a balanced sex distribution (48.8% female). Multivariable Cox regression analysis revealed no significant association between the κ-FLC index and disability progression [hazard ratio (HR) 1.0, p = 0.950]. Prior use of DMT (HR 0.60, p = 0.023) and brain T2L > 9 at baseline (HR 2.22, p = 0.026) were significantly associated with disability progression. The remaining covariates, including age, sex, disease duration, and CEL, showed no significant associations.
Conclusion: The κ-FLC index does not predict disability progression in PPMS, contrasting its growing role as a prognostic biomarker in relapsing MS. This highlights phenotypic differences in MS pathophysiology and underscores the need for prognostic biomarkers in PPMS.
Introduction
The kappa free light chain (κ-FLC) index is a well-established biomarker for intrathecal immunoglobulin synthesis, included in the 2024 revision of the diagnostic criteria for multiple sclerosis (MS) (1–3). κ-FLC are produced by B cells in excess of intact immunoglobulins and accumulate in the intrathecal compartment in case of inflammatory disorders of the central nervous system (4). It is well-established that the κ-FLC index offers comparable diagnostic sensitivity and specificity as oligoclonal bands (OCB) for the diagnosis of both relapsing–remitting MS (RRMS) and primary progressive MS (PPMS) (5–7). Furthermore, the determination of κ-FLC offers significant advantages over OCB detection, as it can be easily measured using nephelometry/turbidimetry with high reliability (8–10).
In RRMS, several studies have demonstrated the prognostic value of the κ-FLC index. Higher values at disease onset were associated with shorter time to relapse, new MRI activity, disability progression, or cognitive disturbance (11–16). Whether the κ-FLC index also has prognostic value in patients with PPMS has not been investigated so far, which is why we performed the present study.
Methods
Patients with PPMS from a previous study (6) who had a diagnostic lumbar puncture (LP) and results of cerebrospinal fluid (CSF) analysis, including κ-FLC index, were eligible for inclusion. Additional patients meeting these inclusion criteria were identified by participating centers (Supplementary Figure S1). The diagnosis of PPMS was made based on the diagnostic criteria applicable at the time of LP. Furthermore, the 2017 revised McDonald criteria were applied to the whole cohort (17). None of the patients had a history of relapses.
At baseline, age, sex, disease duration, Expanded Disability Status Scale (EDSS), the number of T2 hyperintense (T2L) and contrast-enhancing T1 lesions (CEL) on cerebral MRI, the number of T2L on spinal MRI, and CSF-restricted OCB were determined. During follow-up, disability was assessed using EDSS scores, and disease-modifying treatment (DMT) was recorded at routine clinical visits, in accordance with each center’s routine practice. Due to the heterogeneity in data collection between centers, the EDSS scores were retrieved every 2 years (± 12 months) during follow-up.
Cerebrospinal fluid analysis
All CSF samples were collected via LP, and serum samples concomitantly within 30 min via venipuncture. All samples were centrifuged at 2,000 g for 10 min at room temperature before storage at either −20°C or −80°C (18). CSF analysis was performed for routine diagnostic purposes, including OCB detection by each center using isoelectric focusing followed by IgG immunoblotting/IgG fixation. A detailed description of the methods is provided in Supplementary Table S1.
Determination of κ-FLC index
κ-FLC concentrations in CSF and serum were measured at each center via either nephelometry or turbidimetry using the N Latex kappa FLC (Siemens, Erlangen, Germany) or the Freelite MX™ Kappa Kit (The Binding Site Group Ltd., Birmingham, UK) (19–21).
According to the manufacturer, the lower limit of detection in CSF was 0.034 mg/L for the N Latex kappa FLC Kit. Inter- and intra-assay coefficients of variation (CoV) were <3.3% and <5.5%, respectively. The lot-to-lot variation was ≤4.8%. Linearity was <14.7%. Further details can be found in the work of Velthuis et al. and Pretorius et al. (19, 22). For the Freelite MX™ Kappa Kit, the lower limit of detection was 0.33 mg/L. Inter- and intra-assay CoVs were <7.3% and <4.6%, respectively, according to the manufacturer. The lot-to-lot variation was up to ~20% (23, 24). Further details can be found in the work of Bradwell et al. and White-Al Habeeb et al. (21, 25). The overview of the used methods per center is shown in Supplementary Table S1 and previous publications (6, 26–33).
Intrathecal κ-FLC synthesis was calculated using the following formula.
A κ-FLC index >6.1 was considered “positive”, and a κ-FLC index ≤6.1 was considered “negative” (5).
Magnetic resonance imaging
Brain and spinal MRI scans were obtained as part of the routine diagnostic work-up. The number of T2L (>/≤ 9) and CEL (≥1/0) of brain MRI, as well as the number of T2L of spinal MRI (≥2/<2), were retrieved from the respective databases of the specialized MS centers. MRI scans were performed on 1.5- or 3-Tesla MRI scanners and rated by experienced local (neuro)radiologists. MRI protocols included contrast-enhanced T1 sequences as well as T2 sequences.
Definition of disability progression
Disability progression was defined as an EDSS score increase of ≥1.5 for an EDSS baseline score of 0, ≥1.0 for EDSS baseline scores ≥1.0 and ≤5.5, or ≥0.5 for EDSS baseline scores of >5.5 (34), confirmed after 6 months.
Statistical analysis
Categorical variables were expressed as frequencies and percentages, and continuous variables were displayed as median and 25th–75th percentile, as appropriate. Univariate comparisons were performed using chi-square, Fisher’s test, and the Mann–Whitney U test.
Multivariable Cox regression was employed using time to disability progression as the dependent variable and age (continuous), sex (binary), disease duration (continuous), brain T2L (binary, >/≤ 9), brain CEL (binary, ≥1/0), DMT (binary), and κ-FLC index (continuous) as independent variables.
To visualize the effect of the κ-FLC index, we computed the estimated Cox regression survival probabilities separately for high (>100) and low (≤100) κ-FLC index values (12). We used the median of these high and low κ-FLC index values to plug into the Cox regression to compute the graph.
An a priori power analysis for the Cox regression with a significance level of 5%, a power of 80%, and a hazard ratio of two (12) revealed a necessary sample size of 100 patients. We considered a proportion of patients with disability progression of 0.6, and we considered a shorter observation time for patients with disability progression (ratio of observation time in patients with and without disability progression of 0.7).
A p-value <0.05 was considered statistically significant. In Cox regression analysis, according to one-sided hypotheses, that is, increased risk for disability progression, e.g., by higher MRI activity (T2L and CEL) (35) and a lowered risk by DMT (34), one-sided hypothesis testing was used. Thus, a one-sided 95% confidence interval (CI), that is, the lower limit (LL) or upper limit (UL), was shown as appropriate.
All statistical analyses were performed in R (36).
Ethics statement
The studies involving humans were approved by local ethics committees of participating centers. The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired as part of previous studies for which ethical approval was obtained (Supplementary Table S2). Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Results
A total of 121 PPMS patients with a median age of 53 years (46–59) and a balanced sex ratio (48.8% female) were included in the study. All patients fulfilled the 2017 revised McDonald criteria. The patients had a disease duration of 3 (1–6) years and an EDSS score at baseline of 4 (3–5). Brain MRI showed high lesion load (>9 T2L) in 83.6% of patients, and CEL were present in 15.5%. OCB were positive in 108 (89.3%) patients. The median κ-FLC index was 40.0 (14.6–87.8) and considered positive (>6.1) in 112 (92.6%) patients. None of the patients was on DMT at the time of LP; however, DMT was started in 53 (43.8%) patients thereafter. Median follow-up was 5 (3–8) years; i.e., 89.3% of patients had follow-up of at least 2 years.
The details on demographics, clinical characteristics, MRI, and CSF findings are displayed in Table 1 and Supplementary Tables S3 and S4.
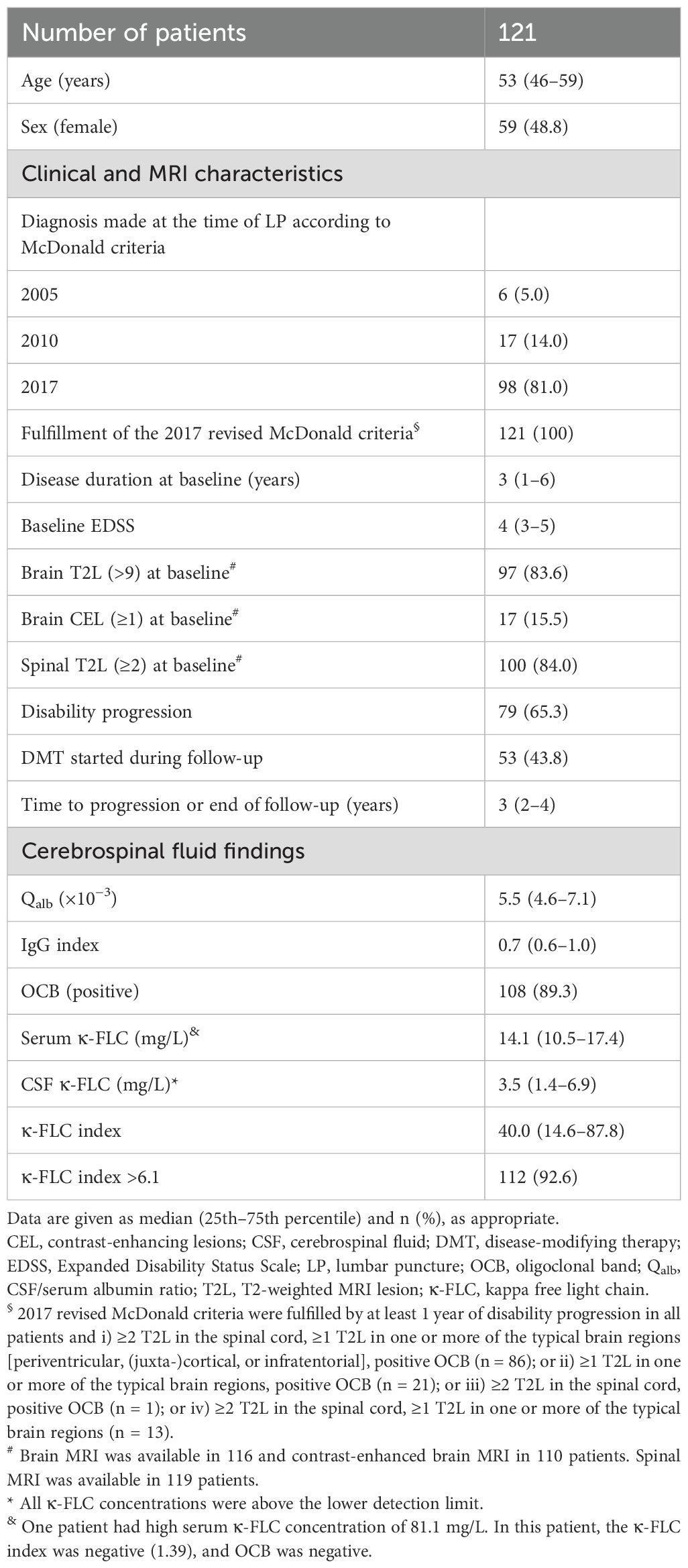
Table 1. Demographics, clinical characteristics, MRI, and CSF findings.
Progressive vs. stable patients
A total of 79 (65.3%) patients had disability progression during follow-up. In univariate analyses, age, sex, disease duration, EDSS, T2L, and CEL at baseline were similar between progressive and stable PPMS patients. The proportion of patients on DMT during follow-up was comparable between the two groups (Table 2). The median κ-FLC index determined at baseline was numerically higher in progressive patients (43.7; 15.5–108.2) compared to the stable group (26.1; 13.9–75.8); however, this difference did not reach statistical significance (p = 0.328; Table 2).
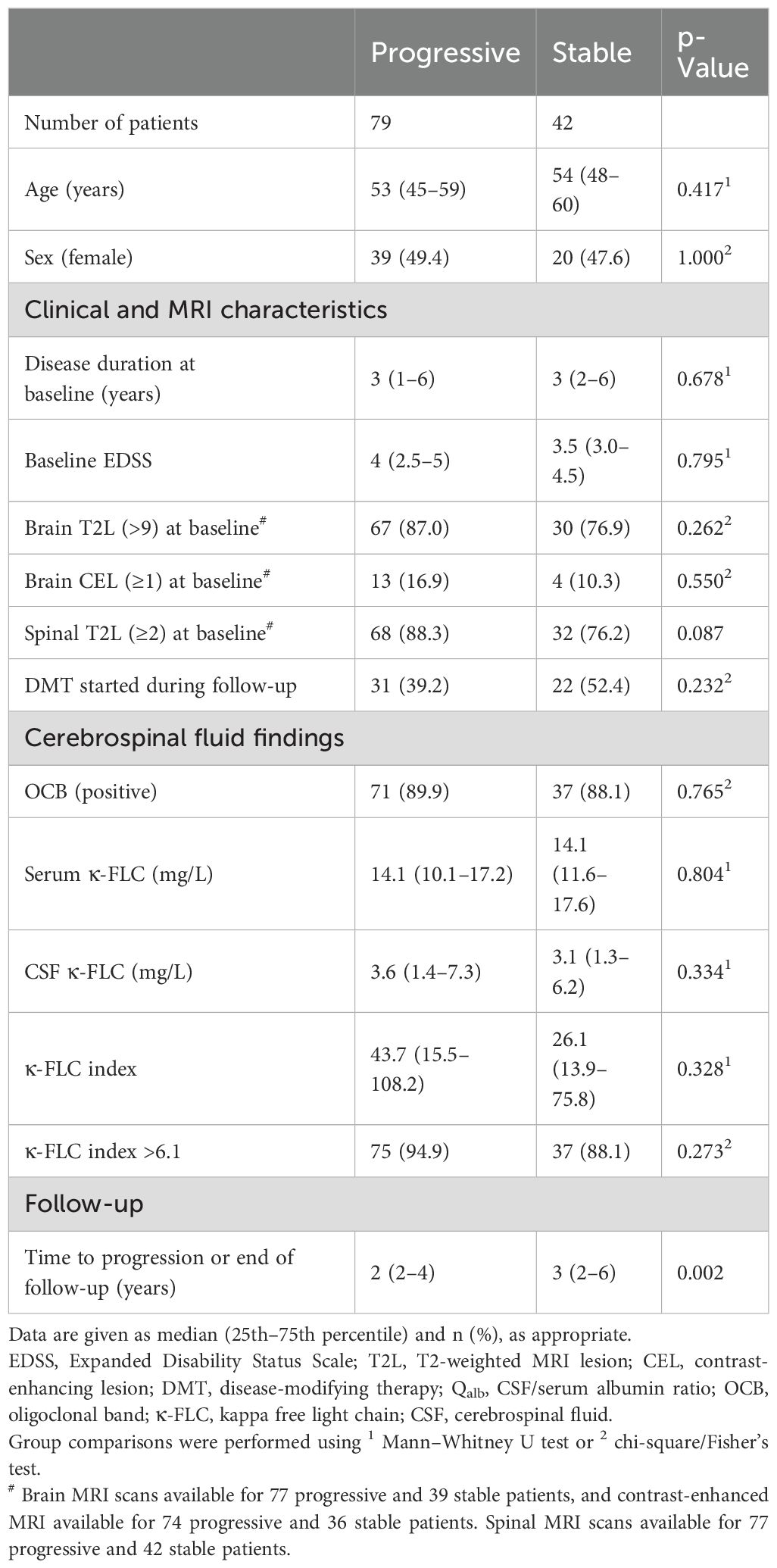
Table 2. Demographics, clinical characteristics, MRI, and CSF findings in progressive and stable PPMS patients.
κ-FLC index does not predict disability progression in PPMS
Multivariable Cox regression analysis showed that the κ-FLC index was not a statistically significant predictor of time to disability progression [hazard ratio (HR) 1.0, p = 0.950]. In contrast, DMT use (HR 0.60, UL-CI: 0.91, p = 0.023) and brain MRI T2L at baseline (HR 2.22, LL-CI: 1.13, p = 0.026) were predictors of disability progression. The remaining variables, age, sex, disease duration, and CEL showed no statistically significant association (Figure 1, Table 3). Further analyses, also including OCB status (Supplementary Table S5) and T2L on spinal MRI (Supplementary Table S6), yielded qualitatively the same results.
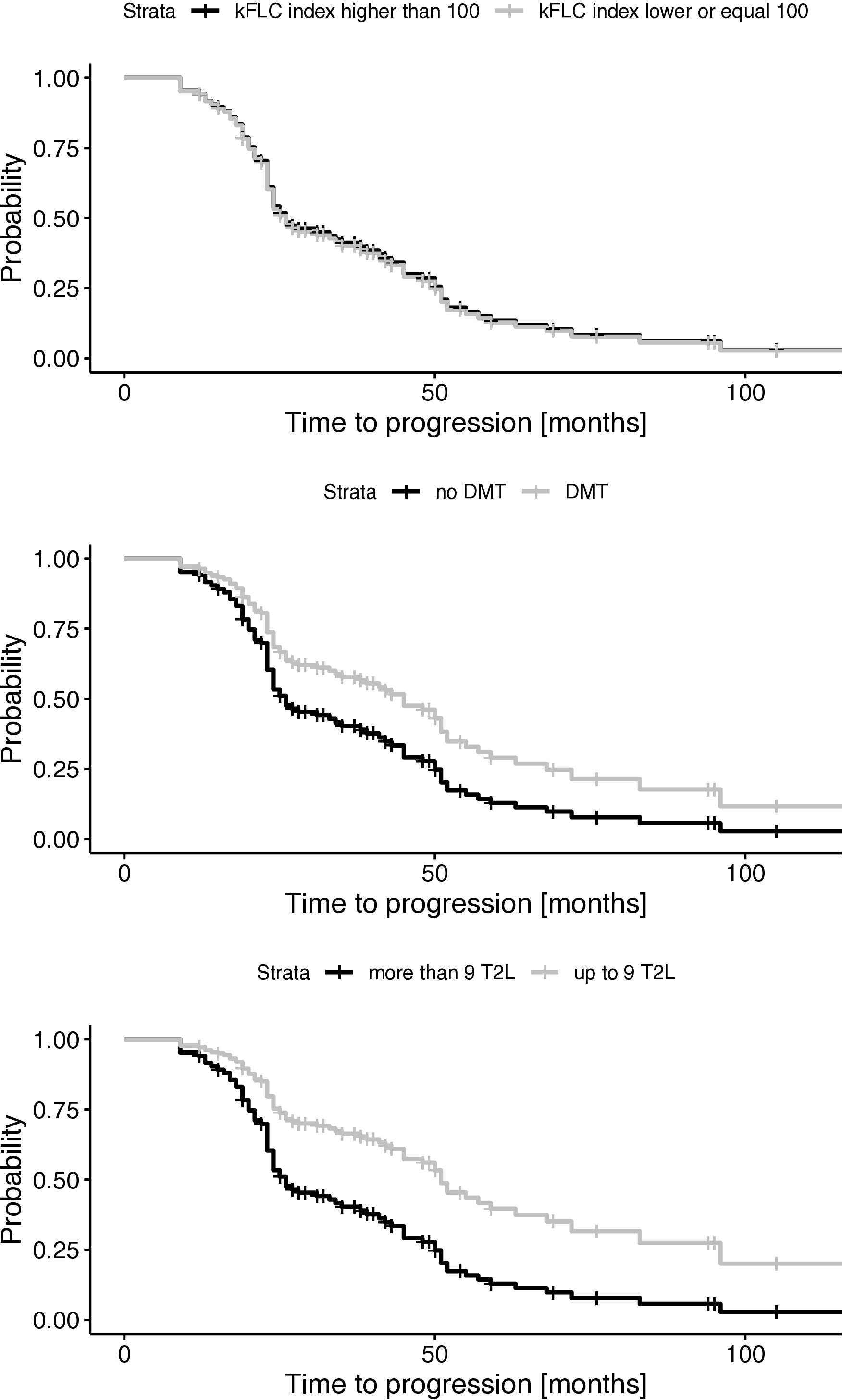
Figure 1. Probability of disability progression dependent on κ-FLC index, DMT, and MRI lesion load. FLC, free light chain; DMT, disease-modifying therapy; T2L, hyperintense lesion on T2-weighted MRI; κ-FLC, kappa free light chain.
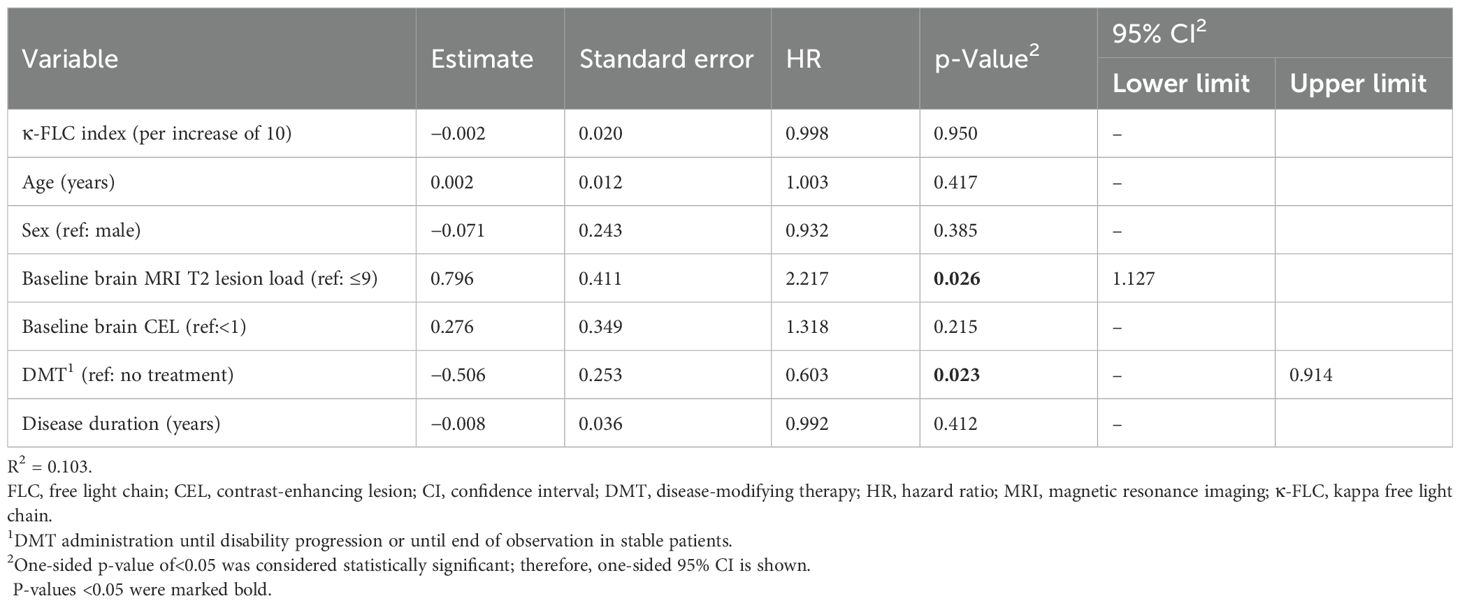
Table 3. Cox regression analysis identifying predictors of disability progression.
Discussion
Here, we investigated whether the κ-FLC index, a quantitative biomarker of intrathecal inflammation, predicts disability progression in patients with PPMS. Our study, including a total of 121 patients, revealed no significant association, even after adjusting for established covariates.
The prognostic value of intrathecal inflammation has been shown by a multitude of studies in relapsing–remitting MS through both the κ-FLC index and OCB (4). In PPMS, the prognostic value of the κ-FLC index has not yet been investigated, and previous studies using OCB have not found any association with the disease course (37, 38).
A possible explanation why intrathecal inflammation, as determined by OCB, was not prognostic in PPMS, but is a clear predictor in RRMS, could be that the inflammatory extent and its contribution to disease evolution are lower in PPMS compared to RRMS (39). We had hypothesized that the κ-FLC index, in contrast to OCB, could exert some prognostic capabilities in PPMS due to the previously reported superiority of the κ-FLC index over OCB in terms of the prognosis of MS disease course (12). While OCB were detected in 95% of patients with relapses during follow-up, OCB were also positive in 86% of non-relapsing patients. The κ-FLC index, as a continuous variable, overcame the weak performance of OCB by further stratification. In the subgroup of OCB-positive patients only, the κ-FLC index was still statistically significantly higher in patients with relapses compared to those without relapses, and testing for log-likelihood reduction by including either the κ-FLC index or OCB in the prognostic model clearly confirmed the superior prognostic value of the κ-FLC index (12). Furthermore, OCB only detect intrathecal IgG production (40), while the κ-FLC index captures intrathecal synthesis from IgG, IgA, and IgM (41, 42). It could have been that this broader spectrum enhanced sensitivity to intrathecal immune responses, as a prognostic value of IgM OCB in PPMS has been reported (37).
Ultimately, we did not observe a statistically significant prognostic value of the κ-FLC index in patients with PPMS (Figure 1A). A priori, we performed a power analysis for the Cox regression (as specified in detail in the methods), considering a power of 80% and a hazard ratio of two. The effect size of the κ-FLC index in RRMS was usually high (12), and for other variables, i.e., DMT and MRI T2L, we did observe a difference between progressing and non-progressing patients in the present analysis (Figures 1B, C) (34, 35). Of course, we cannot exclude that having more patients would have uncovered minor prognostic effects of the κ-FLC index.
Interestingly, the κ-FLC index was higher in patients with CEL (43.7) compared to patients without CEL (31.5) by univariate analysis (p = 0.049). An interaction effect in the Cox regression model between CEL and κ-FLC index was considered in order to investigate whether the κ-FLC index provides additional prognostic value; e.g., only in patients with contrast enhancement it did not show any effect. However, for this analysis, the number of patients (with CEL, n = 17) was too small. Future studies could explore κ-FLC’s utility in PPMS patients with concomitant inflammatory activity. The stratification of patients, those with CEL and high κ-FLC index, may gain further utility, for example, for the evaluation of treatment response, as it is known that patients with inflammatory activity benefit more from B-cell depletion therapies (34).
Our study has several limitations that warrant consideration. It was a retrospective study with all inherent attributes, e.g., the inclusion of patients depended on the availability of samples and follow-up data. Furthermore, time intervals between consecutive clinical visits and MRI protocols used for the determination of baseline T2L and the presence of CEL differed between centers, too. Differences in sampling handling (e.g., processing of fresh versus thawed samples) and laboratory methods used for κ-FLC detection (nephelometry vs. turbidimetry, or polyclonal vs. monoclonal detection antibody) may have led to variability in absolute κ-FLC values, although the calculation of the κ-FLC index does minimize this effect (43). While after frozen sample storage, some decreases in absolute κ-FLC concentrations in CSF and serum have been observed, these changes are evened out using CSF/serum ratios of κ-FLC (and albumin) when calculating the κ-FLC index (43). Also, OCB positivity may vary due to different detection methods (e.g., IgG immunoblotting vs. silver staining). Notably, none of the patients had received DMT at the time of LP, thereby eliminating potential confounding effects of immunomodulatory treatment on κ-FLC index levels (44–46). We also would like to state that disability progression was based solely on the EDSS. The assessments of upper extremity function or cognition were not available. Including further modalities that increase sensitivity for the detection of disability progression may influence the assessment of the prognostic value of the κ-FLC index. Furthermore, we could not consider longitudinal changes of MRI lesions for our analysis, as follow-up MRIs were not regularly performed. Investigation of the prognostic value of the κ-FLC index using a more sensitive endpoint, such as MRI activity, should be addressed by further research. This would also allow us to consider progression independent of MRI activity.
Although the κ-FLC index did not demonstrate a significant prognostic value in PPMS, this study provides a relevant piece of evidence for the interpretation of the κ-FLC index, a biomarker that is already used in clinical routine.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by local ethic committees of participating centers. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because this was a re-analysis of existing data collected from different centers. Every sub-study was approved by the local ethics committee of the respective center.
Author contributions
MS: Writing – original draft, Formal analysis, Data curation, Writing – review & editing. KB: Writing – review & editing. MA: Writing – review & editing. GB: Writing – review & editing. PC: Data curation, Writing – review & editing. FDP: Writing – review & editing. MD: Data curation, Writing – review & editing. FD: Writing – review & editing. AE: Writing – review & editing, Data curation. FF: Data curation, Writing – review & editing. LG: Writing – review & editing, Data curation. MH: Data curation, Writing – review & editing. NK: Data curation, Writing – review & editing. DM: Data curation, Writing – review & editing. MP: Data curation, Writing – review & editing. TP: Data curation, Writing – review & editing. SP: Writing – review & editing, Data curation. IR: Data curation, Writing – review & editing. UR: Writing – review & editing, Data curation. CW: Data curation, Writing – review & editing. DV: Writing – review & editing, Data curation. MV: Data curation, Writing – review & editing. TZ: Writing – review & editing, Data curation. AZ: Writing – review & editing. JW: Writing – review & editing, Formal analysis. HH: Writing – review & editing, Formal analysis, Writing – original draft, Data curation, Conceptualization.
Funding
The author(s) declare no financial support was received for the research and/or publication of this article.
Conflict of interest
MS has participated in meetings sponsored by or received travel grants from Novartis, Sanofi-Genzyme, and Amgen. KB has participated in meetings sponsored by and received travel funding or speaker honoraria from Roche, Teva, Merck, Biogen, Sanofi, and Novartis. He is an associate editor of Frontiers in Immunology/Neurology, Section Multiple Sclerosis and Neuroimmunology. MA has received speaker honoraria and/or travel grants from Biogen, Merck, Novartis, Sanofi-Genzyme, Horizon Therapeutics/Amgen, and Zentiva. GB has participated in meetings sponsored by and received speaker honoraria or travel funding from Biogen, BMS, Janssen, Lilly, Medwhizz, Merck, Neuraxpharm, Novartis, Roche, Sanofi, and Teva; and received honoraria for consulting from Adivo Associates, Biogen, BMS, Janssen, Merck, Novartis, Roche, Sanofi, and Teva. He has received unrestricted research grants from BMS and Novartis. He serves on the Executive Committee of the European Committee for Treatment and Research in Multiple Sclerosis ECTRIMS and the Board of Directors of the International Multiple Sclerosis Visual System Consortium IMSVISUAL. PC has received research funding and speaker fees from Merck Serono, Roche, Novartis, Biogen, and Sanofi. FDP has participated in meetings sponsored by and received honoraria lectures, advisory boards, and consultations or travel funding from Bayer, Biogen, Celgene, BMS, Merck, Novartis, Sanofi-Genzyme, Teva, and Roche. Her institution has received research grants from Roche. MD participated on advisory boards and steering committees for and received speaker or writing honoraria, research support, and funding for travelling from Alexion, Amgen, BMS, Bayer, Biogen Idec, Genzyme, Horizon, Janssen, Merck, Mylan, Novartis, Roche, Siemens Healthineers, Teva, and Viatris. FD has participated in meetings sponsored by or received honoraria for acting as an advisor/speaker for Alexion, Almirall, Biogen, Celgene, Merck, Novartis, Roche, and Sanofi-Genzyme. His institution received scientific grants from Biogen and Sanofi-Genzyme. AE received travel grants and participated in meetings sponsored by Novartis and Eli Lilly and Company. FF has participated in meetings sponsored by and received speaker honoraria and/or travel funding from Novartis, Biogen, and Merck. LG has participated in advisory boards for and received writing or speaker honoraria and travel grants from Almirall, Biogen, Eisai, Euroimmun, Fujirebio, Lilly, Merck, Mylan, Novartis, Roche, Sanofi, Siemens Healthineers, and Teva. NK has participated in meetings sponsored by and received speaker honoraria or travel funding from Alexion, BMS, Janssen, Merck, Neuraxpharm, Novartis, Roche, and Sanofi; and held a grant for a Multiple Sclerosis Clinical Training Fellowship Programme from the European Committee for Treatment and Research in Multiple Sclerosis ECTRIMS. MP has received speaker or consulting honoraria from Amicus, Sanofi-Aventis, and Novartis; and participated in meetings sponsored by and received travel funding from Amicus, Merck, Novartis, and Sanofi-Genzyme, as well as a grant for clinical and research fellowships awarded by the European Academy of Neurology EAN. TP has received research grants and travel support from Novartis, Roche, and Genzyme. SP has received travel funding and speaker honoraria from Bayer, Biogen, Merck, Novartis, Sanofi-Genzyme, Teva, and The Binding Site.
IR has received compensation for lectures from Biogen, Novartis, Merck, and Sanofi and has served on advisory boards for Sanofi. UR has received speaker and consulting honoraria from Biogen, Bayer, Novartis, Teva, Merck, Sanofi, Lek, Roche, Janssen, Salus, and Swixx, as well as research support from Biogen and Novartis. CW Tørring has received/participated in travel funding and sponsored meetings from Biogen, Merck, Novartis, Roche, and Sanofi-Genzyme. DV has received travel grants from Merck, Sanofi-Genzyme, Almirall, and Novartis and research grants from Merck and FISM. MV has received research funding and speaker fees from Merck Serono, Roche, Novartis, Biogen, and Sanofi. TZ received/participated in travel funding/sponsored meetings from Biogen, Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. AZ has participated in meetings sponsored by and received speaking honoraria or travel funding from Biogen, Merck, Novartis, Sanofi-Genzyme, Janssen, Bristol Myers Squibb, and Teva. HH has participated in meetings sponsored by and received speaker honoraria or travel funding from Amgen, Bayer, Biogen, Bristol Myers Squibb, Janssen, Merck, Novartis, Sanofi-Genzyme, Siemens, and Teva; and received honoraria for acting as a consultant for Biogen, Bristol Myers Squibb, Novartis, Roche, Sanofi-Genzyme, and Teva.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1658182/full#supplementary-material
References
1. Hegen H, Arrambide G, Gnanapavan S, Kaplan B, Khalil M, Saadeh R, et al. Cerebrospinal fluid kappa free light chains for the diagnosis of multiple sclerosis: A consensus statement. Mult Scler J. (2023) 29:182–95. doi: 10.1177/13524585221134217
2. Montalban X, Lebrun-Frénay C, Oh J, Arrambide G, Moccia M, Amato MP, et al. Diagnosis of multiple sclerosis: 2024 revisions of the McDonald criteria. Lancet Neurol. (2025) 24:850–65. doi: 10.1016/S1474-4422(25)00270-4
3. Deisenhammer F, Hegen H, Arrambide G, Banwell BL, Coetzee T, Gnanapavan S, et al. Positive cerebrospinal fluid in the 2024 McDonald criteria for multiple sclerosis. eBioMedicine. (2025) 120:105905. doi: 10.1016/j.ebiom.2025.105905
4. Filippo M, Gaetani L, Centonze D, Hegen H, Kuhle J, Teunissen C, et al. Fluid biomarkers in multiple sclerosis: from current to future applications. Lancet Reg Health - Eur. (2024) 44:101009. doi: 10.1016/j.lanepe.2024.101009
5. Hegen H, Walde J, Berek K, Arrambide G, Gnanapavan S, Kaplan B, et al. Cerebrospinal fluid kappa free light chains for the diagnosis of multiple sclerosis: A systematic review and meta-analysis. Mult Scler J. (2023) 29:169–81. doi: 10.1177/13524585221134213
6. Hegen H, Berek K, Cavalla P, Christiansen M, Emeršič A, Di Filippo M, et al. Diagnostic value of kappa free light chain index in patients with primary progressive multiple sclerosis - a multicentre study. Front Immunol. (2023) 14:1327947. doi: 10.3389/fimmu.2023.1327947
7. Konen FF, Hannich MJ, Schwenkenbecher P, Grothe M, Gag K, Jendretzky KF, et al. Diagnostic cerebrospinal fluid biomarker in early and late onset multiple sclerosis. Biomedicines. (2022) 10:1629. doi: 10.3390/biomedicines10071629
8. Konen FF, Wurster U, Schwenkenbecher P, Gerritzen A, Groß CC, Eichhorn P, et al. Oligoclonal bands and kappa free light chains: Competing parameters or complementary biomarkers? Autoimmun Rev. (2025) 24:103765. doi: 10.1016/j.autrev.2025.103765
9. Hegen H, Schmidauer M, Auer M, Di Pauli F, Berek K, Walde J, et al. Kappa free light chain index in the real world—Do we miss clinically relevant information by skipping oligoclonal banding? Eur J Neurol. (2025) 32:e70355. doi: 10.1111/ene.70355
10. Hegen H, Berek K, and Deisenhammer F. Cerebrospinal fluid kappa free light chains as biomarker in multiple sclerosis-from diagnosis to prediction of disease activity. Wien Med Wochenschr 1946. (2022) 172:337–45. doi: 10.1007/s10354-022-00912-7
11. Hegen H, Berek K, Bsteh G, Auer M, Altmann P, Di Pauli F, et al. Kappa free light chain and neurofilament light independently predict early multiple sclerosis disease activity-a cohort study. EBioMedicine. (2023) 91:104573. doi: 10.1016/j.ebiom.2023.104573
12. Berek K, Bsteh G, Auer M, Di Pauli F, Grams A, Milosavljevic D, et al. Kappa-free light chains in CSF predict early multiple sclerosis disease activity. Neurol Neuroimmunol Neuroinflamm. (2021) 8:e1005. doi: 10.1212/NXI.0000000000001005
13. Levraut M, Gavoille A, Landes-Chateau C, Cohen M, Bresch S, Seitz-Polski B, et al. Kappa free light chain index predicts disease course in clinically and radiologically isolated syndromes. Neurol Neuroimmunol Neuroinflamm. (2023) 10:e200156. doi: 10.1212/NXI.0000000000200156
14. Rosenstein I, Axelsson M, Novakova L, Rasch S, Blennow K, Zetterberg H, et al. High levels of kappa free light chain synthesis predict cognitive decline in relapsing-remitting multiple sclerosis. Front Immunol. (2023) 14:1106028/full. doi: 10.3389/fimmu.2023.1106028/full
15. Rosenstein I, Axelsson M, Novakova L, Malmeström C, Blennow K, Zetterberg H, et al. Intrathecal kappa free light chain synthesis is associated with worse prognosis in relapsing-remitting multiple sclerosis. J Neurol. (2023) 270:4800–11. doi: 10.1007/s00415-023-11817-9
16. Berek K, Schmidauer M, Bsteh G, Auer M, Barket R, Berger T, et al. Kappa free light chain index predicts long-term disease activity and disability accrual in multiple sclerosis. Mult Scler J. (2025) 31:1187–94. doi: 10.1177/13524585251344807
17. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
18. Teunissen CE, Petzold A, Bennett JL, Berven FS, Brundin L, Comabella M, et al. A consensus protocol for the standardization of cerebrospinal fluid collection and biobanking. Neurology. (2009) 73:1914–22. doi: 10.1212/WNL.0b013e3181c47cc2
19. Velthuis HT, Knop I, Stam P, van den Broek M, Bos HK, Hol S, et al. N Latex FLC - new monoclonal high-performance assays for the determination of free light chain kappa and lambda. Clin Chem Lab Med. (2011) 49:1323–32. doi: 10.1515/CCLM.2011.624
20. Hoedemakers RMJ, Pruijt JFM, Hol S, Teunissen E, Martens H, Stam P, et al. Clinical comparison of new monoclonal antibody-based nephelometric assays for free light chain kappa and lambda to polyclonal antibody-based assays and immunofixation electrophoresis. Clin Chem Lab Med. (2011) 50:489–95. doi: 10.1515/CCLM.2011.793
21. Bradwell AR, Carr-Smith HD, Mead GP, Tang LX, Showell PJ, Drayson MT, et al. Highly sensitive, automated immunoassay for immunoglobulin free light chains in serum and urine. Clin Chem. (2001) 47:673–80. doi: 10.1093/clinchem/47.4.673
22. Pretorius CJ, Klingberg S, Tate J, Wilgen U, and Ungerer JPJ. Evaluation of the N Latex FLC free light chain assay on the Siemens BN analyser: precision, agreement, linearity and variation between reagent lots. Ann Clin Biochem. (2012) 49:450–5. doi: 10.1258/acb.2012.011264
23. Tate J, Mollee P, Dimeski G, Carter A, and Gill D. Analytical performance of serum free light-chain assay during monitoring of patients with monoclonal light-chain diseases. Clin Chim Acta Int J Clin Chem. (2007) 376:30–6. doi: 10.1016/j.cca.2006.07.011
24. Handley SA, Barnes S, Jenkins N, and Wanandy T. Performance of the Binding Site cerebrospinal fluid kappa free light chains assay. Ann Clin Biochem. (2025) 62:505–9. doi: 10.1177/00045632251337616
25. White-Al Habeeb NMA, Earle T, Spencer M, and Blasutig IM. Evaluation of the N-latex serum free light chain assay on the Siemens BNII analyzer and agreement with The Binding Site FreeLite assay on the SPAPlus. Clin Biochem. (2018) 51:90–6. doi: 10.1016/j.clinbiochem.2017.05.009
26. Cavalla P, Caropreso P, Limoncelli S, Bosa C, Pasanisi MB, Schillaci V, et al. Kappa free light chains index in the differential diagnosis of Multiple Sclerosis from Neuromyelitis optica spectrum disorders and other immune-mediated central nervous system disorders. J Neuroimmunol. (2020) 339:577122. doi: 10.1016/j.jneuroim.2019.577122
27. Emersic A, Anadolli V, Krsnik M, and Rot U. Intrathecal immunoglobulin synthesis: The potential value of an adjunct test. Clin Chim Acta Int J Clin Chem. (2019) 489:109–16. doi: 10.1016/j.cca.2018.12.006
28. Rosenstein I, Rasch S, Axelsson M, Novakova L, Blennow K, Zetterberg H, et al. Kappa free light chain index as a diagnostic biomarker in multiple sclerosis: A real-world investigation. J Neurochem. (2021) 159:618–28. doi: 10.1111/jnc.15500
29. Christiansen M, Gjelstrup MC, Stilund M, Christensen T, Petersen T, and Jon Møller H. Cerebrospinal fluid free kappa light chains and kappa index perform equal to oligoclonal bands in the diagnosis of multiple sclerosis. Clin Chem Lab Med. (2018) 57:210–20. doi: 10.1515/cclm-2018-0400
30. Presslauer S, Milosavljevic D, Brücke T, Bayer P, and Hübl W. Elevated levels of kappa free light chains in CSF support the diagnosis of multiple sclerosis. J Neurol. (2008) 255:1508–14. doi: 10.1007/s00415-008-0954-z
31. Presslauer S, Milosavljevic D, Huebl W, Aboulenein-Djamshidian F, Krugluger W, Deisenhammer F, et al. Validation of kappa free light chains as a diagnostic biomarker in multiple sclerosis and clinically isolated syndrome: A multicenter study. Mult Scler Houndmills Basingstoke Engl. (2016) 22:502–10. doi: 10.1177/1352458515594044
32. Vecchio D, Bellomo G, Serino R, Virgilio E, Lamonaca M, Dianzani U, et al. Intrathecal kappa free light chains as markers for multiple sclerosis. Sci Rep. (2020) 10:20329. doi: 10.1038/s41598-020-77029-7
33. Gaetani L, Di Carlo M, Brachelente G, Valletta F, Eusebi P, Mancini A, et al. Cerebrospinal fluid free light chains compared to oligoclonal bands as biomarkers in multiple sclerosis. J Neuroimmunol. (2020) 339:577108. doi: 10.1016/j.jneuroim.2019.577108
34. Montalbán X, Hauser SL, Kappos L, Arnold DL, Bar-Or A, Comi G, et al. Ocrelizumab versus placebo in primary progressive multiple sclerosis. New Engl J Med. 376:209–20. doi: 10.1056/NEJMoa1606468
35. Sastre-Garriga J, Ingle GT, Rovaris M, Téllez N, Jasperse B, Altmann DR, et al. Long-term clinical outcome of primary progressive MS: predictive value of clinical and MRI data. Neurology. (2005) 65:633–5. doi: 10.1212/01.wnl.0000173061.12776.1f
36. RStudio Team. RStudio: Integrated Development for R (2020). PBC, Boston, MA: RStudio. Available online at: http://www.rstudio.com/.
37. Villar LM, Casanova B, Ouamara N, Comabella M, Jalili F, Leppert D, et al. Immunoglobulin M oligoclonal bands: biomarker of targetable inflammation in primary progressive multiple sclerosis. Ann Neurol. (2014) 76:231–40. doi: 10.1002/ana.24190
38. Lourenco P, Shirani A, Saeedi J, Oger J, Schreiber WE, and Tremlett H. Oligoclonal bands and cerebrospinal fluid markers in multiple sclerosis: associations with disease course and progression. Mult Scler J. (2013) 19:577–84. doi: 10.1177/1352458512459684
39. Nowak-Kiczmer M, Niedziela N, Czuba ZP, Sowa P, Wierzbicki K, Lubczyński M, et al. A comparison of serum inflammatory parameters in progressive forms of multiple sclerosis. Mult Scler Relat Disord. (2023) 79:105004. doi: 10.1016/j.msard.2023.105004
40. Freedman MS, Thompson EJ, Deisenhammer F, Giovannoni G, Grimsley G, Keir G, et al. Recommended standard of cerebrospinal fluid analysis in the diagnosis of multiple sclerosis: A consensus statement. Arch Neurol. (2005) 62:865–70. doi: 10.1001/archneur.62.6.865
41. Hannich MJ, Dressel A, Budde K, Petersmann A, Nauck M, and Süße M. Kappa free light chains in the context of blood contamination, and other igA- and igM-related cerebrospinal fluid disease pattern. Cells. (2021) 10:616. doi: 10.3390/cells10030616
42. Hegen H, Milosavljevic D, Schnabl C, Manowiecka A, Walde J, Deisenhammer F, et al. Cerebrospinal fluid free light chains as diagnostic biomarker in neuroborreliosis. Clin Chem Lab Med. (2018) 56:1383–91. doi: 10.1515/cclm-2018-0028
43. Schmidauer M, Berek K, Bsteh G, Auer M, Barket R, Di Pauli F, et al. Effect of long-term frozen storage on stability of kappa free light chain index. Clin Chem Lab Med CCLM. (2025) 63:1786–91. doi: 10.1515/cclm-2025-0125/html
44. Süße M, Konen FF, Schwenkenbecher P, Budde K, Nauck M, Grothe M, et al. Decreased intrathecal concentrations of free light chains kappa in multiple sclerosis patients taking very high effective disease-modifying treatment. Diagnostics. (2022) 12:720. doi: 10.3390/diagnostics12030720
45. Konen FF, Wurster U, Witte T, Jendretzky KF, Gingele S, Tumani H, et al. The impact of immunomodulatory treatment on kappa free light chains as biomarker in neuroinflammation. Cells. (2020) 9:842. doi: 10.3390/cells9040842
Keywords: cerebrospinal fluid, kappa free light chain, primary progressive, multiple sclerosis, prognostic biomarker
Citation: Schmidauer M, Berek K, Auer M, Bsteh G, Cavalla P, Di Pauli F, Di Filippo M, Deisenhammer F, Emeršič A, Föttinger F, Gaetani L, Hassler M, Krajnc N, Milosavljevic D, Ponleitner M, Petersen T, Presslauer S, Rosenstein I, Rot U, Tørring CW, Vecchio D, Vercellino M, Zrzavy T, Zinganell A, Walde J and Hegen H (2025) Prognostic value of kappa free light chain index in patients with primary progressive multiple sclerosis. Front. Immunol. 16:1658182. doi: 10.3389/fimmu.2025.1658182
Received: 02 July 2025; Accepted: 24 October 2025;
Published: 07 November 2025.
Edited by:
Silvia Romano, Sapienza University of Rome, ItalyReviewed by:
Franz Felix Konen, Hannover Medical School, GermanyMassimo Pieri, University of Rome Tor Vergata, Italy
Copyright © 2025 Schmidauer, Berek, Auer, Bsteh, Cavalla, Di Pauli, Di Filippo, Deisenhammer, Emeršič, Föttinger, Gaetani, Hassler, Krajnc, Milosavljevic, Ponleitner, Petersen, Presslauer, Rosenstein, Rot, Tørring, Vecchio, Vercellino, Zrzavy, Zinganell, Walde and Hegen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Harald Hegen, aGFyYWxkLmhlZ2VuQGktbWVkLmFjLmF0