 E. Elefante1†
E. Elefante1† D. Schilirò1†
D. Schilirò1† M. L. Manca2
M. L. Manca2 C. Stagnaro1
C. Stagnaro1 D. Zucchi1
D. Zucchi1 C. Cardelli1V. Signorini1M. Maffi1G. Cascarano1R. Zas3L. Carli1
C. Cardelli1V. Signorini1M. Maffi1G. Cascarano1R. Zas3L. Carli1 F. Ferro1
F. Ferro1 C. Tani1M. Mosca1*
C. Tani1M. Mosca1*- 1Rheumatology Unit, University of Pisa, Pisa, Italy
- 2Department of Clinical and Experimental Medicine and Department of Mathematics, University of Pisa, Pisa, Italy
- 3Rheumatology Department, Instituto de Investigación Hospital 12 de Octubre, Madrid, Spain
Objectives: To describe different clinical phenotypes of severe flares in a monocentric cohort of SLE patients and to compare treatment and outcomes.
Material and methods: Retrospective study of prospectively collected data on 122 severe flares occurred in 110 patients, between 2018 and 2023, and followed up for 12 months after the flare. Baseline characteristics included disease activity assessment by SELENA-SLEDAI and BILAG 2004 scores, demographic and laboratory data. A hierarchical unsupervised segmentation method was applied to cluster flares based on baseline features. Treatments and outcomes according to LLDAS, DORIS Remission and SRI definitions, were compared among clusters at different timepoints.
Results: We identified 3 clusters, 2 composed mainly by extra-renal, and one by renal flares. Among non-renal clusters, cluster 1 was characterized by severe constitutional symptoms, serositis and arthritis occurring in younger patients, associated with hyper-inflammatory biomarkers and multiple autoantibodies specificities. Cluster 2 included flares with more BILAG B scores and mainly mucocutaneous and musculoskeletal manifestations, and overlapping antiphospholipid syndrome (APS). Cluster 3 was the renal flares cluster. Cluster 1 and the renal cluster were treated more frequently with glucocorticoid (GC) pulses and mycophenolate mofetil (MMF) and presented higher daily and cumulative GCs doses at 12 months (t12). These two clusters also shared similar percentage of attainment of LLDAS (about 50%) and remission (about 35% both) at t12, compared to 73% of LLDAS and 53% of remission in cluster 2 at t12.
Conclusions: We described three different clusters of severe flares in SLE in a real-life setting, identifying a hyper-inflammatory flare phenotype, that shares a comparable proportion of unsatisfying response to treatment as renal flares. Our results may represent a clinical starting point, in the context of precision medicine, for better characterization of severe non-renal disease of SLE, with the final aim of setting up early tailored treatment strategies.
Introduction
Systemic Lupus Erythematosus (SLE) is characterized by a relapsing-remitting course, alternating quiescent phases and relapses, and by a complex and proteiform clinical picture. Disease flares may be characterized by mild and limited manifestations or present severe and multi-organ forms, up to very aggressive clinical events with organ- and life-threatening manifestations (1). Classically, renal and neuropsychiatric involvement are considered “major” organ involvements and the most severe disease manifestations, with a negative impact on disease outcomes and prognosis (2, 3).
With the availability of new therapeutic options and the implementation of a treat-to-target strategy in the management of SLE, a better definition of different phenotypes of disease flares might support a more personalized and tailored treatment. This is even more important with the advent of new biological drugs for SLE and the possibility of a combined treatment strategy when poor prognostic factors are identified.
In this context, in the latest EULAR recommendations for the management of SLE, it was proposed that early combination therapy, for example with belimumab on top of standard immunosuppressive drugs (IS), ‘should be considered’ in all adult patients with active lupus nephritis, that is by default a severe disease (4). However, it is more difficult to identify aggressive phenotypes and poor prognostic factors for more heterogeneous extra-renal disease.
We have previously demonstrated in our cohort, among extra-renal flares in an outpatient setting, that mucocutaneous flares still represent an unmet need in the management of SLE patients (5).
The aim of the present study was to identify different phenotypes of severe flares, defined according to The Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA)-SLEDAI flare index (SFI) (6), among hospitalized SLE patients regularly followed at our Unit.
Materials and methods
Study population
This is a retrospective study of prospectively collected data from a monocentric cohort of adult SLE patients, in regular follow-up at the Lupus Clinic of the University of Pisa, Italy.
All patients enrolled in the study fulfilled the following inclusion criteria:
- patients who met the 2012 SLICC (7) or 2019 EULAR-ACR classification criteria for SLE (8);
- patients who were hospitalized between 2018 and 2023 at our Unit, due to a severe disease flare, according to the SELENA-SLEDAI flare index (SFI) definition (6);
- patients with at least 12 months of regular follow-up available after the SLE flare.
Patients with concomitant infections, oncologic and onco-hematologic diseases were excluded.
For each patient demographic data (sex, ethnicity, age at hospital admission), comorbidities, disease duration, cumulative SLE manifestations and treatments, overlap with Sjogren’s syndrome (SSj) (according to the 2016 ACR/EULAR classification criteria) (9) and antiphospholipid syndrome (APS) (according to the revised Sapporo classification criteria) (10), were retrieved from inpatients’ clinical charts.
The moment of hospitalization due to disease flare was considered as the baseline (t0).
At t0, for each flare the following data were collected: clinical manifestations, immunologic profile, laboratory, imaging and histopathology (if performed during hospitalization), ongoing treatment at admission and therapeutic management of the flare. Particularly, among laboratory routine tests, complete blood cells count, complement factors C3 and C4, immunoglobulins percentage on total serum proteins and IgA, IgG, IgM classes values, inflammatory biomarkers as C reactive protein (CRP), erythrocyte sedimentation rate (ESR), fibrinogen and ferritin were reported.
Lymphadenopathies were assessed by ultrasound.
Biopsy-proven lupus nephritis, when present, was classified according to the International Society of Nephrology/Renal Pathology Society (ISN/RPS) classification (11).
For each flare, disease activity was assessed according to the SELENA-SLEDAI (12) and British Isles Lupus Assessment Group 2004 (BILAG 2004) (13).
After each flare included in the study, we collected data for one year of follow-up. The following time points for disease outcomes and treatment evaluation were set at 3-, 6-, and 12-months of follow-up (reported as t3, t6, and t12).
At each timepoint, disease activity status was assessed according to the Lupus Low Disease Activity State (LLDAS) (14) and Definition Of Remission In SLE (DORIS) (15), and response to treatment was evaluated using the SLE responder index (SRI) criteria (16).
With respect to the therapeutic management, ongoing treatments and therapeutic variations, if any, were collected at t3, t6, and t12. As far as the glucocorticoid (GC) treatment is concerned, we recorded at baseline the GC pulses, if performed, the daily and the cumulative doses of oral prednisone (PDN) administered to treat the flare, and taken by the patient at 1-, 3-, 6- and 12-months’ time-points.
Organ damage was expressed by the Systemic Lupus International Collaborating Clinics Damage Index (SLICC-DI) (17) and assessed at baseline and at t12.
Statistical analysis
For descriptive analysis, patients and flares characteristics were reported in terms of frequency and percentages for categorical variables and mean and standard deviation or median and interquartile range (based on whether the probability distribution is normal or not) for continuous variables.
Clustering analysis methodology
A k-means clustering analysis was performed on the SLE flares selected according to the above inclusion criteria. The analysis utilized Euclidean distance as the similarity metric and included all baseline clinical, laboratory, and immunological features. To determine the optimal number of clusters, we tested solutions with 2, 3, and 4 clusters and compared their performance using silhouette score analysis. The 3-cluster solution was selected based on the highest silhouette score and clinical interpretability of the resulting clusters. No imputation was performed for missing data; complete case analysis was conducted for variables with missing values.
Post-hoc analysis
The following post-hoc elaborations, 1-way analysis of variance with Bonferroni test for quantitative variables, and Chi square test for qualitative variables, were performed to estimate any statistically significant differences between the clusters.
P-values <0.05 were considered statistically significant.
Data processing was performed with the STATA software package and R statistical software.
This study was conducted according to the Declaration of Helsinki and was approved by the Ethics Committee “Area Vasta Nord Ovest” (CEAVNO) with the number 14478.
Results
122 severe SLE flares occurring in 110 consecutive patients in the period between 2018 and 2023, fulfilled the inclusion criteria and were considered for the analysis. Overall flares’ characteristics at baseline are summarized in the Supplementary Table and briefly reported below.
Baseline patients’ and flares’ characteristics
Most flares occurred in female patients (83%) of White ethnicity (89%). The mean age and disease duration at the moment of the flare were 39.2 ± 12.3 years, and 8.2 ± 8.6 years, respectively. 22 flares (18%) represented the onset of the disease. The median SELENA-SLEDAI at baseline was 10.5 (IQR 11-16) and more than half of flares (65%) were characterized by “BILAG A” disease manifestations. According to the BILAG definitions, the most frequent active disease manifestations at baseline were renal (46%), followed by musculoskeletal (33%), constitutional (32%) and hematologic (22%). At the moment of hospitalization, 60 cases (49%) were already under treatment with immunosuppressants (IS); 94 cases (77%) were on hydroxychloroquine (HCQ) alone or in combination with IS, and 31 (25%) were not on GC treatment.
Management, follow-up and outcomes
Glucocorticoids were used in the management of most flares (78%) with pulses administered in 66 cases (54%); 33 flares were treated without introducing (25/33) or modifying the dosage of GCs (8/33), but only introducing an immunosuppressant (the most frequently used were: Mycophenolate Mofetil, Methotrexate, Azathioprine, Rituximab, without a clear predominance of one drug over another). Of note, 4 patients in this group were treated with intravenous immunoglobulins, underlining that they were frail patients at an elevated infectious risk. Compared to GCs-treated flares, the “no-GCs” flares presented more active cutaneous involvement (39% vs 15%; p=0.00) and less frequent renal (24% vs 56%; p=0.002) and cardiopulmonary (p=0.05) active manifestations, significantly lower SLEDAI scores (10.59 ± 6.78 vs 13.9 ± 7.16, p=0.05), and less BILAG A scores in active domains (80% vs 20%; p=0.001).
In 104 flares (85%), ongoing therapy was modified by adding or changing one or more IS. Overall, remission was achieved in almost one third of the cases at 6 and 12 months (26% and 34%, respectively) and LLDAS in almost half of the cases (45% at 6 months and 50% at 12 months).
Cluster analysis
All 122 flares were considered for the clusterization process. 3 clusters were identified, composed of 40, 34 and 48 flares respectively. Only 10 patients had more than 1 flare; for each of them repeated flares belonged to the same cluster. Cluster 3 included patients with a renal flare, while cluster 1 and 2 were characterized by extra-renal manifestations.
In Table 1 we summarized the different clinical characteristics, SELENA-SLEDAI and BILAG scores of the three clusters.
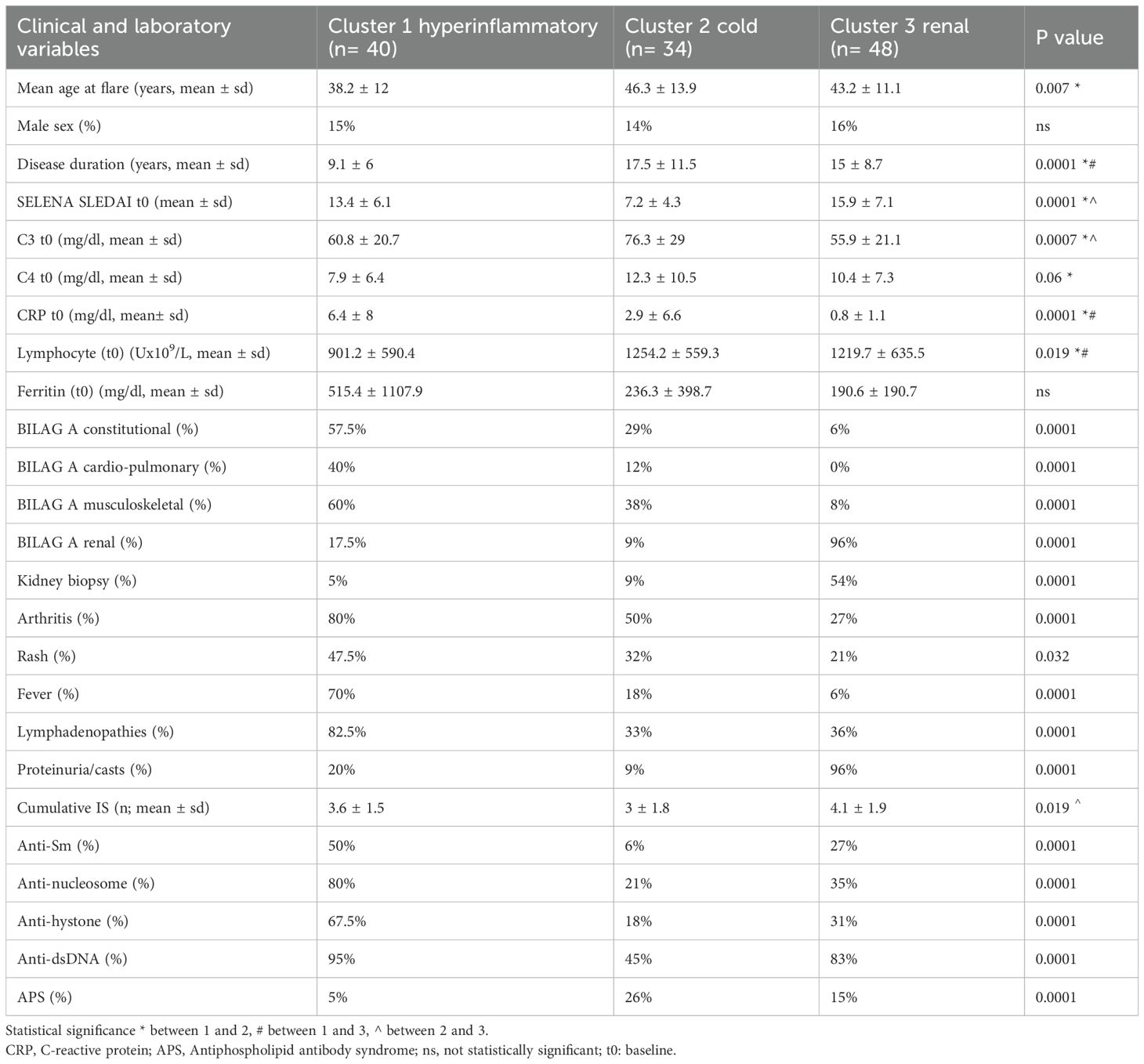
Table 1. Clusters’ baseline and laboratory features.
Clinical and laboratory features of the three clusters at baseline
Cluster 1 included flares that occurred in younger patients (mean age 38.2 ± 12 years), with shorter disease duration (9.1 ± 6 years). Overall, arthritis (80% vs 50% and 27%), fever (70% vs 18% and 6%) and lymphadenopathies (82.5% vs 33% and 36%) resulted significantly more frequent in this cluster compared to the others. Constitutional involvement appeared significantly associated with this cluster, also characterizing the past medical history of patients (74% vs 47% and 37% cluster 2 and 3 respectively; p= 0.003). No significant differences in other cumulative disease manifestations were found between clusters. 2 kidney biopsies were performed in Cluster 1, showing one class II and one class IV lupus nephritis.
As far as laboratory parameters is concerned, cluster 1 included flares characterized by marked CRP elevation (6.4 ± 8 vs 2.9 ± 6.6 and 0.8 ± 1.1 mg/dL, p=0.000), a trend for higher ferritin serum levels and lymphopenia (901.2 ± 590.4 vs 1254.2 ± 559.3 and 1219.7 ± 635.5 Ux109/L, p=0.000) compared to the other clusters. Cluster 1 was also characterized by a higher number of different SLE-specific autoantibodies (anti-histone, anti-Sm, anti-nucleosome and anti-dsDNA antibodies) than cluster 2 and 3 (p=0.000). Interestingly, despite a shorter disease duration, this cluster presented a number of cumulative previous IS comparable to cluster 3.
Considering the most prevalent clinical and laboratory features of flares belonging to cluster 1, we named it the “hyper-inflammatory” cluster.
Cluster 2 included flares presenting lower disease activity (Table 1), and less severe clinical manifestations, mainly in the mucocutaneous and musculoskeletal domains, reporting more “BILAG B” scores compared to the other clusters (59% vs 28% and 19%; p=0.000). In three cases, a kidney biopsy was required, showing one class III, one class II and one class IV lupus nephritis.
In line with a “milder” clinical profile, flares in cluster 2 presented higher values of complement C3 (76.3 ± 29 vs 60.8 ± 20.7 and 55.9 ± 21.1 mg/dL; p=0.000). Patients belonging to this cluster were older, with longer disease duration with respect to cluster 1 (p=0.000), requiring fewer cumulative IS in their history with respect to cluster 3 (3 ± 1.8 vs 4.1 ± 1.9, p=0.019). Moreover, a significant higher percentage of patients in this cluster presented a secondary APS (26% vs 5% and 15%; p=0.000) compared to cluster 1 and 3. However, no significant differences emerged between the clusters regarding the positivity of the different antiphospholipid antibodies.
We named cluster 2 the “cold” cluster to suggest a lower severity of flares and a different clinical and laboratory phenotype in contrast to that of cluster 1.
Cluster 3 included most flares with active renal involvement presenting a BILAG score A in the renal domains (96% vs 17.5% and 9%, p= .0001). As expected, more than a half of cases in this cluster (26/48 flares) underwent a renal biopsy, and histologic examination showed a proliferative glomerulonephritis in most of the cases: 18/26 (70%) were class III or IV; in 4/26 (15%) cases, class III or IV was in combination with class V.
As far as serology is concerned, a clear prevalence of anti-dsDNA positivity compared to other autoantibodies was observed.
Cluster 3 was named the “renal” cluster.
Therapeutic management of flares in the three clusters
The therapeutic management of the three clusters at t0 is summarized in Table 2.
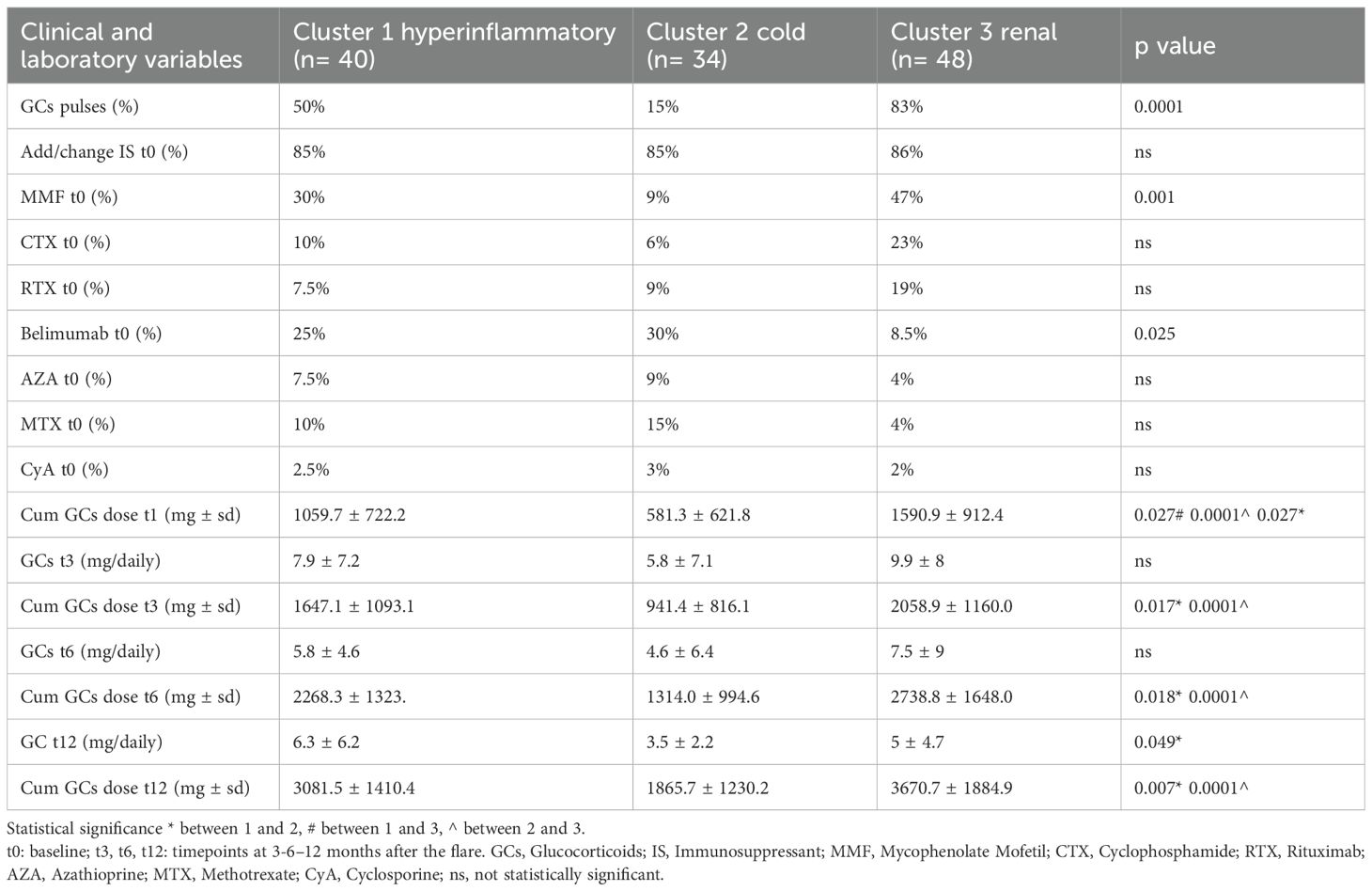
Table 2. Therapeutic management in the three clusters.
A significant difference was observed in the administration of GC pulses which were more commonly used to treat flares in clusters 1 and 3. No differences emerged between clusters as for the number of flares treated without GC (data not shown). About 85% of flares in each cluster required a modification of therapy by adding or changing an IS. MMF was the most used drug in clusters 1 and 3.
Belimumab was added in 25% and 30% of flares in clusters 1 and 2 reflecting the fact that most flares included in our study occurred before the approval of BLM for lupus nephritis. No significant differences emerged with respect to other therapies.
At t12 cluster 1 and cluster 3 had been treated with significantly higher GC cumulative doses compared to cluster 2. Interestingly, cluster 1 presented the highest daily GC dose at t12 (6.3 ± 6 mg/daily vs 3.5 ± 2 and 5 ± 4.7 in clusters 2 and 3, respectively) (Table 2).
Disease outcomes in the three clusters
We finally compared the attainment of treatment targets after flare in the three clusters.
In the cluster 2 an early achievement of LLDAS and remission at t3 was observed in a statistically significant higher percentage of cases compared to the clusters 1 and 3 (p= 0.0001 and 0.0014, respectively). Flares in the clusters 1 and 3 showed a similar course during follow-up, presenting a comparable and quite low percentage of patients that achieved LLDAS and remission at the different timepoints. Particularly, only about one third of flares reached remission at t12 in both clusters 1 and 3 (35%) (Table 3).
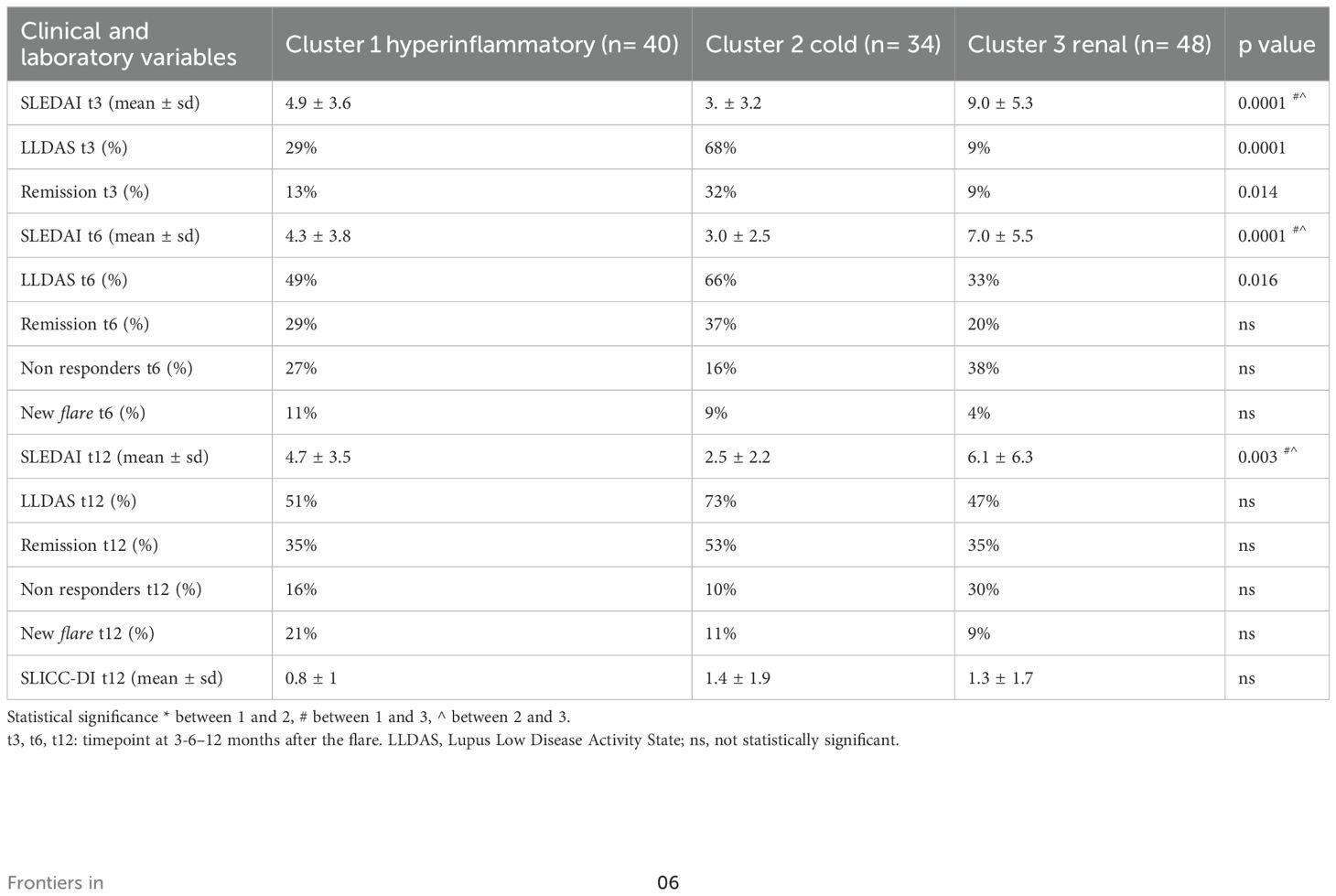
Table 3. Outcomes in the three clusters.
No significant differences were observed between clusters in the percentage of non-responders and new disease flares at t6 and t12.
Finally, no significant differences between clusters were found as far as damage accrual after one year of follow-up is concerned. In particular, 76 flares (62%) had no damage at t0. Among them, 15 (20%) developed damage at t12, 4 belonging to cluster 1, 2 to cluster 2 and 9 to cluster 3 (p=0.2). Moreover, at baseline 48 flares (40%) already presented a SLICC-DI score ≥ 1, with a mean value of 1.95 ± 1, and at t12 this percentage rose to 50% of flares with a mean SLICC-DI value of 2.03 ± 1.5, with no significant differences between clusters. Overall, at t12, 27 flares presented a damage accrual, without differences between clusters.
Discussion
The main objective of this study was to identify different phenotypes of severe flares in a monocentric cohort of SLE patients. Among 122 consecutive SLE flares requiring hospitalization at our Unit between 2018 and 2023, we identified three distinct clinical and biological clusters of severe flares: one cluster constituted mainly by “renal flares” (cluster 3), and two by extra-renal flares: cluster 1, characterized by “hyperinflammatory flares”, and cluster 2, by milder and “cold flares”.
In the current literature, several studies have tried to identify different subsets of SLE patients, underlining the complexity of SLE and the need for physicians to stratify the therapeutic strategies according to the different patients’ characteristics. Pisetzky and colleagues have recently introduced the concept of two different types of SLE: Type 1 SLE characterized by the classical inflammatory symptoms of the disease, and Type 2 SLE characterized by symptoms such as fatigue, widespread body pain, neuropsychiatric symptoms, and sleep disturbance that are often unrelated to disease activity (18).
Overall, starting from the immunological profile or from the cumulative clinical features of the disease in large US, European and Asian cohorts, currently available data seem to converge on the existence of some subsets of patients. Particularly, patients with dominant proliferative nephritis present anti-dsDNA positivity and a higher risk of damage accrual, while patients with anti-RNP positivity seem to have lower probability of renal involvement and an association with extra-renal manifestations, like myositis and anemia. Patients with associated Sjogren’s syndrome are mainly female and seem to have milder clinical manifestations of SLE, while patients with anti-phospholipid antibodies are clearly at higher risk of vascular complications, neurological involvement and damage accrual (19–21).
Recently, in a very large multicenter cohort of SLE patients in China, three different subgroups were identified among “serologically active clinically quiescent (SACQ)” patients: cluster 1 consisted of elderly males with a history of major organ involvement and the highest risk of severe flares and damage accrual; cluster 2 was characterized by milder disease and a lower risk of organ damage, with 30.8% of patients in this cluster who successfully discontinued low-dose glucocorticoids; cluster 3 presented the highest proportion of lupus nephritis and a moderate risk of organ damage (22).
To the best of our knowledge, our study is the first one performing a clustering-analysis focusing on clinical, laboratory and immunologic features of severe SLE flares, defined according to the SFI criteria. The clustering analysis, performed on flares instead of cumulative clinical features, proved to be a useful approach to understanding the heterogeneity of severe SLE flares. By moving beyond traditional clinical classifications, we were able to reveal distinct phenotypes that share underlying biological and clinical characteristics. This method allowed for a more nuanced characterization of disease severity, potentially paving the way for more targeted therapeutic strategies.
As expected, and in line with literature data (21, 23, 24), one of the identified clusters included flares with prevalent renal expression, thus characterized by active lupus nephritis associated with a prevalent positivity of anti-dsDNA antibodies. More interestingly, two other distinct clusters of non-renal severe flares emerged in our study.
Cluster 1, which we called the “hyperinflammatory” cluster, included younger patients with a shorter disease duration and was characterized, from a clinical point of view, by constitutional manifestations (such as fever and lymphadenopathies), severe arthritis and cardiopulmonary manifestations. Moreover, from a biological point of view, it was characterized by hyperinflammatory response with marked elevation of CRP and ferritin levels, lymphopenia, and multiple SLE specific autoantibodies positivity.
Historically, high CRP levels in SLE are considered more suggestive of infection rather than disease activity (25), although a moderate elevation of CRP has been associated with specific SLE manifestations, namely arthritis and serositis (26, 27). However, our results outlined a more definite phenotype of SLE flare for which a marked elevation of all the inflammatory biomarkers represents the hallmark of disease activity and is associated with a severe clinical picture and with a quite complex disease history, rather than with a single disease manifestation.
Cluster 2, the other extra-renal cluster, which we called the “cold” cluster, was characterized by milder clinical manifestations, mainly mucocutaneous and articular, and by a higher prevalence of APS. Despite this apparent benign presentation, all the flares in this cluster should also be considered severe, as they required hospitalization and/or therapeutic escalation.
As already stated, renal involvement represents the prototype of a severe SLE manifestation and current literature offers a great amount of data on its therapeutic management and treatment targets. On the contrary, less is known with respect to other severe disease phenotypes.
Interestingly, in our study, several similarities emerged between the hyperinflammatory and the renal clusters in terms of clinical severity, therapeutic choices, and outcomes.
At baseline, these two clusters presented similar total SLEDAI score and complement consumption, and they shared analogous therapeutic attitude in the use of GCs. The hyperinflammatory flares required high doses of GCs, with pulses needed in half of the cases. During the follow-up, no differences emerged in terms of cumulative GC doses, at the different timepoints, between hyperinflammatory and renal flares. Moreover, MMF was the most frequently used IS to treat flares in both clusters. Interestingly, BLM was the second drug administered in the hyperinflammatory cluster (25%), suggesting that biological drugs could represent a valuable option for this disease phenotype. In the renal subgroup, BLM was less used as most of the flares included in the study occurred before its approval for lupus nephritis.
As for the response to treatment at the different timepoints during the follow-up, the hyperinflammatory and the renal clusters presented a comparable and quite low percentage of flares that achieved the targets of LLDAS and remission; in particular, at t12, only about one-third of flares in both clusters had reached remission. Of course, our study presents some limitations. First, the limited follow-up period of 12 months compromised the possibility to draw conclusions on longer-term outcomes in terms of response to treatment and, above all, damage accrual in the different clusters. Another limitation is that most of the flares included in the study occurred before the approval of belimumab for lupus nephritis and all of them occurred before the approval of anifrolumab for non-renal SLE. So, maybe the therapeutic approach to flares included in the study, nowadays, could have been changed according to the latest EULAR recommendations for the management of SLE.
It is interesting to underline that some of the clinical and laboratory features that we described for the “hyperinflammatory” flares, have been associated, according to recent literature data, with a high interferon (IFN) signature, particularly fever, lymphopenia, hypocomplementemia, multiple autoantibodies positivity and resistance to glucocorticoids (28–30). So, we could only speculate whether the “hyperinflammatory” flares identify a subset of IFN-driven SLE flares that may benefit from an early introduction of targeted anti-IFN treatment.
Finally, the relatively small size of each cluster did not allow us to perform subanalysis to evaluate the response to different treatments within each flare phenotype.
We also believe that our study presents some points of strength. First, a large amount of data for each flare, with few missing, was collected in a homogeneous and prospective way despite the retrospective design of the study. Moreover, we believe that the monocentric design of the study ensures a homogeneous approach in the management of these flares. In conclusion, this study describes three different phenotypes of severe flares in SLE in a real-life setting. In particular, we identified a kind of non-renal flare presenting with fever, arthritis and serositis associated with a hyperinflammatory response. These flares appeared to be as severe as the “classical” severe renal flares, deserving similar aggressive therapeutic strategies and burdened by a comparable proportion of unsatisfying response to treatment.
In the era of precision medicine, a better phenotyping of SLE patients and flares appears of utmost importance, especially for non-renal manifestations, for the early identification of flares with poor prognostic factors deserving early aggressive treatments. In this context, the advent of biological drugs and early combined treatment strategies could help in the management of severe flares, improving the attainment of treatment targets and disease outcomes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by Ethics Committee “Area Vasta Nord Ovest” (CEAVNO). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
EE: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. DS: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MMan: Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. CS: Investigation, Writing – review & editing. DZ: Investigation, Writing – review & editing. CC: Investigation, Writing – review & editing. VS: Investigation, Writing – review & editing. MMaf: Data curation, Investigation, Writing – review & editing. GC: Data curation, Investigation, Writing – review & editing. RZ: Investigation, Writing – review & editing. LC: Investigation, Writing – review & editing. FF: Investigation, Writing – review & editing. CT: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. MMos: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1673350/full#supplementary-material
References
1. Zucchi D, Silvagni E, Elefante E, Signorini V, Cardelli C, Trentin F, et al. Systemic lupus erythematosus: one year in review 2023. Clin Exp Rheumatol. (2023) 41:997–1008. doi: 10.55563/clinexprheumatol/4uc7e8
2. Zirkzee EJM, Huizinga TWJ, Bollen ELEM, van Buchem MA, Middelkoop H a. M, van der Wee NJA, et al. Mortality in neuropsychiatric systemic lupus erythematosus (NPSLE). Lupus. (2014) 23:31–8. doi: 10.1177/0961203313512540
3. Umeda R, Ogata S, Hara S, Takahashi K, Inaguma D, Hasegawa M, et al. Comparison of the 2018 and 2003 International Society of Nephrology/Renal Pathology Society classification in terms of renal prognosis in patients of lupus nephritis: a retrospective cohort study. Arthritis Res Ther. (2020) 22:260. doi: 10.1186/s13075-020-02358-x
4. Fanouriakis A, Kostopoulou M, Andersen J, Aringer M, Arnaud L, Bae SC, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis. (2024) 83:15–29. doi: 10.1136/ard-2023-224762
5. Maffi M, Tani C, Cascarano G, Scagnellato L, Elefante E, Stagnaro C, et al. Which extra-renal flare is “difficult to treat” in systemic lupus erythematosus? A one-year longitudinal study comparing traditional and machine learning approaches. Rheumatol Oxf Engl. (2024) 63:376–84. doi: 10.1093/rheumatology/kead166
6. Petri M, Kim MY, Kalunian KC, Grossman J, Hahn BH, Sammaritano LR, et al. Combined oral contraceptives in women with systemic lupus erythematosus. N Engl J Med. (2005) 353:2550–8. doi: 10.1056/NEJMoa051135
7. Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. (2012) 64:2677–86. doi: 10.1002/art.34473
8. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheum Dis. (2019) 78:1151–9. doi: 10.1136/annrheumdis-2018-214819
9. Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, et al. 2016 American college of rheumatology/european league against rheumatism classification criteria for primary sjögren’s syndrome: A consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheumatol Hoboken NJ. (2017) 69:35–45. doi: 10.1002/art.39859
10. Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost JTH. (2006) 4:295–306. doi: 10.1111/j.1538-7836.2006.01753.x
11. Bajema IM, Wilhelmus S, Alpers CE, Bruijn JA, Colvin RB, Cook HT, et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. (2018) 93:789–96. doi: 10.1016/j.kint.2017.11.023
12. Gladman DD, Ibañez D, and Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. (2002) 29:288–91.
13. Isenberg DA, Rahman A, Allen E, Farewell V, Akil M, Bruce IN, et al. BILAG 2004. Development and initial validation of an updated version of the British Isles Lupus Assessment Group’s disease activity index for patients with systemic lupus erythematosus. Rheumatol Oxf Engl. (2005) 44:902–6. doi: 10.1093/rheumatology/keh624
14. Franklyn K, Lau CS, Navarra SV, Louthrenoo W, Lateef A, Hamijoyo L, et al. Definition and initial validation of a Lupus Low Disease Activity State (LLDAS). Ann Rheum Dis. (2016) 75:1615–21. doi: 10.1136/annrheumdis-2015-207726
15. van Vollenhoven R, Voskuyl A, Bertsias G, Aranow C, Aringer M, Arnaud L, et al. A framework for remission in SLE: consensus findings from a large international task force on definitions of remission in SLE (DORIS). Ann Rheum Dis. (2017) 76:554–61. doi: 10.1136/annrheumdis-2016-209519
16. Luijten KMa.C, Tekstra J, Bijlsma JWJ, and Bijl M. The Systemic Lupus Erythematosus Responder Index (SRI); a new SLE disease activity assessment. Autoimmun Rev. (2012) 11:326–9. doi: 10.1016/j.autrev.2011.06.011
17. Gladman D, Ginzler E, Goldsmith C, Fortin P, Liang M, Urowitz M, et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheumatol. (1996) 39:363–9. doi: 10.1002/art.1780390303
18. Pisetsky DS, Clowse MEB, Criscione-Schreiber LG, and Rogers JL. A novel system to categorize the symptoms of systemic lupus erythematosus. Arthritis Care Res. (2019) 71:735–41. doi: 10.1002/acr.23794
19. To CH and Petri M. Is antibody clustering predictive of clinical subsets and damage in systemic lupus erythematosus? Arthritis Rheumatol. (2005) 52:4003–10. doi: 10.1002/art.21414
20. Mariette F, Le Guern V, Nguyen Y, Yelnik C, Morel N, Hachulla E, et al. Cluster analysis of clinical manifestations assigns systemic lupus erythematosus-phenotype subgroups: A multicentre study on 440 patients. Joint Bone Spine. (2024) 91:105760. doi: 10.1016/j.jbspin.2024.105760
21. Font J, Cervera R, Ramos-Casals M, García-Carrasco M, Sents J, Herrero C, et al. Clusters of clinical and immunologic features in systemic lupus erythematosus: analysis of 600 patients from a single center. Semin Arthritis Rheumatol. (2004) 33:217–30. doi: 10.1053/S0049-0172(03)00133-1
22. Ding Y, Zhou Y, Zhan F, Xu J, Duan X, Luo H, et al. Phenotypic subgroup in serologically active clinically quiescent systemic lupus erythematosus: A cluster analysis based on CSTAR cohort. Med N Y N. (2024) 5:1266–1274.e3. doi: 10.1016/j.medj.2024.06.005
23. Li PH, Wong WHS, Lee TL, Lau CS, Chan TM, Leung AMH, et al. Relationship between autoantibody clustering and clinical subsets in SLE: cluster and association analyses in Hong Kong Chinese. Rheumatol Oxf Engl. (2013) 52:337–45. doi: 10.1093/rheumatology/kes261
24. Artim-Esen B, Çene E, Şahinkaya Y, Ertan S, Pehlivan Ö, Kamali S, et al. Cluster analysis of autoantibodies in 852 patients with systemic lupus erythematosus from a single center. J Rheumatol. (2014) 41:1304–10. doi: 10.3899/jrheum.130984
25. Firooz N, Albert DA, Wallace DJ, Ishimori M, Berel D, and Weisman MH. High-sensitivity C-reactive protein and erythrocyte sedimentation rate in systemic lupus erythematosus. Lupus. (2011) 20:588–97. doi: 10.1177/0961203310393378
26. Kim HA, Jeon JY, An JM, Koh BR, and Suh CH. C-reactive protein is a more sensitive and specific marker for diagnosing bacterial infections in systemic lupus erythematosus compared to S100A8/A9 and procalcitonin. J Rheumatol. (2012) 39:728–34. doi: 10.3899/jrheum.111044
27. Gaitonde S, Samols D, and Kushner I. C-reactive protein and systemic lupus erythematosus. Arthritis Rheumatol. (2008) 59:1814–20. doi: 10.1002/art.24316
28. Gómez-Bañuelos E, Goldman DW, Andrade V, Darrah E, Petri M, and Andrade F. Uncoupling interferons and the interferon signature explains clinical and transcriptional subsets in SLE. Cell Rep Med. (2024) 5:101569. doi: 10.1016/j.xcrm.2024.101569
29. Shirahama Y, Hashimoto A, Ono N, Takeyama Y, Maruyama A, Inoue T, et al. Relationships between Type 1 interferon signatures and clinical features of the new-onset lupus patients in Japan. Mod Rheumatol. (2024) 34:346–51. doi: 10.1093/mr/road015
Keywords: systemic lupus - erythematosus, lupus flares, cluster analysis, disease outcomes, lupus phenotypes
Citation: Elefante E, Schilirò D, Manca ML, Stagnaro C, Zucchi D, Cardelli C, Signorini V, Maffi M, Cascarano G, Zas R, Carli L, Ferro F, Tani C and Mosca M (2025) Different phenotypes of severe flares in patients with systemic lupus erythematosus: results of a clustering analysis in a monocentric cohort. Front. Immunol. 16:1673350. doi: 10.3389/fimmu.2025.1673350
Received: 25 July 2025; Accepted: 03 November 2025;
Published: 21 November 2025.
Edited by:
Yu-Jih Su, Kaohsiung Chang Gung Memorial Hospital, TaiwanReviewed by:
Silvia Scriffignano, University of Molise, ItalyDaliya Pencheva, University Hospital St. Ivan Rilski, Bulgaria
Copyright © 2025 Elefante, Schilirò, Manca, Stagnaro, Zucchi, Cardelli, Signorini, Maffi, Cascarano, Zas, Carli, Ferro, Tani and Mosca. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. Mosca, bWFydGEubW9zY2FAdW5pcGkuaXQ=
†These authors have contributed equally to this work