 Léa-Sophie Dreveton1,2,3*
Léa-Sophie Dreveton1,2,3* Jakob Joachim Spencker3
Jakob Joachim Spencker3 Hector Rincon-Arevalo1,2,3,4Arman Aue2,3,5
Hector Rincon-Arevalo1,2,3,4Arman Aue2,3,5 Bilgin Osmanodja3
Bilgin Osmanodja3 Annika Wiedemann1,2
Annika Wiedemann1,2 Franziska Szelinski1,2Gerhard Krönke1,2
Franziska Szelinski1,2Gerhard Krönke1,2 Thomas Dörner1,2
Thomas Dörner1,2 Eva Schrezenmeier2,3
Eva Schrezenmeier2,3 Ana-Luisa Stefanski1,2
Ana-Luisa Stefanski1,2- 1Department of Rheumatology and Clinical Immunology, Charité- Universitätsmedizin Berlin, Berlin, Germany
- 2Deutsches Rheumaforschungszentrum (DRFZ), Berlin, Germany
- 3Department of Nephrology and Medical Intensive Care, Charité- Universitätsmedizin Berlin, Berlin, Germany
- 4Grupo de Inmunología Celular e Inmunogenética, Facultad de Medicina, Instituto de Investigaciones Médicas, Universidad de Antioquia UdeA., Medellín, Colombia
- 5Immanuel Krankenhaus Berlin Buch, Klinik für Rheumatologie und Klinische Immunologie, Berlin, Germany
Background: Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by systemic inflammation and the involvement of multiple organ systems. The disease’s heterogeneity challenges clinical assessment, highlighting the need for personalized diagnostics and therapies. Soluble immune checkpoint molecules (sICPs) have emerged as potential biomarkers for predicting disease activity in other autoimmune diseases. However, the role of sICPs in SLE has not yet been delineated.
Methods: In this study serum concentrations of soluble co-stimulatory (sCD25, sCD27, sCD40L, s4-1BB and sCD86) and co-inhibitory checkpoint molecules (sCTLA-4, sPD-1, sPD-L1, sPD-L2, sTim-3, sGal-9 and sLAG-3) were measured by bead-based assay in 235 SLE patients. sICPs were analyzed in relation to clinical data (SLEDAI, organ involvement, C3, C4, anti-dsDNA, Siglec- 1, and sustained DORIS/LLDAS remission). Analyses included Wilcoxon rank-sum tests, multivariable logistic regressions, receiver operating characteristic (ROC) analyses, cluster analyses, and correlation matrices.
Results: Higher concentrations of sCD25, sTim-3, and sGal-9 were associated with active SLE disease (SLEDAI > 4). Cluster analysis identified highest concentrations in a SLE subgroup with more severe disease (median SLEDAI 10). These molecules correlated strongly with each other and were specifically elevated in patients with renal involvement and/ or anemia, but not with APS, skin, or joint manifestations. Low sCD25 levels were associated with sustained DORIS/LLDAS remission.
Conclusion: This study highlights sCD25, sTim-3, and sGal-9 as biomarkers for active SLE and renal and hematologic involvement. Low sCD25 levels were associated with achieving long-term DORIS and LLDAS remission, underscoring the potential of sCD25 as a predictive and sensitive biomarker mandating further clinical validation.
Introduction
Systemic lupus erythematosus (SLE) is a highly heterogenous chronic inflammatory autoimmune disease, characterized by multiple organ manifestations, mainly affecting women of childbearing age. SLE can result in severe organ damage with kidneys, nervous and vascular system, and especially joints and skin frequently affected (1). The disease process involves abnormal cellular activity of innate and adaptive immunity connected to elevated cytokine and autoantibody production together with immune complex formation all able to maintain chronic inflammatory reactions, ultimately leading to multiorgan damage accrual (2). Overall, current concepts consider a breakdown of immune homeostasis and loss of self-tolerance as key which results in abnormalities of T and B cell interaction within a milieu of extensive secretion of certain pro-inflammatory cytokines (i.e. type I and II interferon, IL-6, BAFF, APRIL) (3).
The main goal of SLE therapy is to achieve remission, as defined by the DORIS criteria (Definitions of Remission in SLE (4)) or at least to achieve a stable state of low disease activity (LLDAS), defined by minimal or controlled clinical activity on/off immunosuppression and minimal systemic glucocorticoid requirement (5). This therapeutic objective is crucial, as shown in the Systemic Lupus International Collaborating Clinics (SLICC) inception cohort, where both DORIS remission and LLDAS significantly reduce the accumulation of irreversible organ damage, enhance the patient’s quality of life and lower the overall disease burden (6). However, despite advances in diagnosis and therapy, SLE remains a heterogeneous disease with highly variable disease courses and therapeutic responses. This diversity not only complicates the clinical assessment of disease activity, but also presents a challenge and necessity for the development of personalized treatment approaches.
Given the wide variability in symptoms and disease progression together with the rising prevalence of SLE (7), early diagnosis and the systematic tracking of disease activity and progression through immunological biomarkers are becoming increasingly important to enable better disease management, individualized therapy and improve patients’ quality of life (8). Soluble immune checkpoint molecules (sICPs) were recently identified as biomarkers associated with the development, prognosis, and treatment of autoimmune disease like rheumatoid arthritis (RA) (9), systemic sclerosis (sSc) (10, 11) and (ANCA)-associated vasculitis (AAV) (12–14). Immune checkpoints represent a group of co-stimulatory and co-inhibitory molecules, which control interactions between B and T cells during an inflammatory response and play a pivotal role in the initiation, maintenance and duration of inflammatory processes triggered by (auto)immune antigens. Immune checkpoint inhibitors are known to induce immune-related adverse events (IRAEs), which mimic autoimmune diseases (15), suggesting a dysregulated immune balance as part of autoimmune pathogenesis (16–18). Moreover, agonistic modulation of inhibitory checkpoint molecules such as CTLA-4 and PD-1 has already shown efficacy in certain autoimmune diseases and is currently under investigation, highlighting their potential as promising therapeutic targets (19–21).
The aim of this study is to assess the contribution of soluble co-inhibitory and co-stimulatory checkpoint molecules in SLE and to identify potential predictive biomarkers for disease activity, specific organ manifestations and treatment outcomes in SLE patients.
Methods
Study design and data collection
We performed a retrospective study including all patients with a confirmed diagnosis of systemic lupus erythematosus (SLE), according to the classification criteria of EULAR/ACR 20 (8). The patients presented at the Department for Rheumatology and Clinical Immunology or the Department of Nephrology at Charité Universitätsmedizin Berlin between January 2016 and February 2023. Serum samples were collected from all patients and stored after obtaining written informed consent (EA1/002/16, EA1/302/16), EA1/009/17, EA1/215/18). A total of 235 patients and 416 patient visits were identified. Clinical data and individual blood values were extracted from medical records and electronic entries. Clinical data included disease activity via SLEDAI (Systemic Lupus Erythematosus Disease Activity Index) (22) and specific organ involvement. Laboratory values included autoantibody profile, complement factors C3, C4, serologic and urine findings and Siglec-1 expression on monocytes (a surrogate maker for the type I interferon signature (23)). To provide a comprehensive overview of the collected data, a detailed summary of all data recorded of the cohort is listed in Supplementary Table 1. Biobank samples per patient are summarized in Supplementary Table 2.
Analyte detection
Serum concentrations of soluble co-stimulatory sCD25, sCD27, sCD40L, s4-1BB and sCD86 and co-inhibitory checkpoint molecules sCTLA-4 (soluble Cytotoxic T-Lymphocyte Activation Gene-3), sPD-1 (soluble Programmed Cell Death Protein 1), sPD-L1 (soluble programmed Death-Ligand 1), sPD-L2 (soluble programmed Death-Ligand 2), sTim-3 (soluble T-cell Immunoglobulin and Mucine-domain containing-3), sGal-9 (soluble Galectin-9) and sLAG-3 (soluble Lymphocyte Activation Gene-3) were determined using bead-based LEGENDplex multiplex analysis (BioLegend). Type I interferon (IFN) proteins IFN-α, IFN-ß, IFN-λ1 and IFN-λ2/3, as well as sAPRIL (soluble A Proliferation-Inducing Ligand) and BAFF (soluble B-cell activation factor), known cytokines involved into the pathophysiology of SLE (3, 24), were also assessed with the same bead-based method. All tests were conducted in accordance with the manufacturer´s protocol (25).
Measurements were performed on the BD FACSCanto (BD Biosciences). The results were analyzed using FlowJo software 10.7.1 (TreeStar) and Prism GraphPad Prism Version 9 (GraphPad software).
Statistical analysis
For 235 participants, 416 blood samples were available. Descriptive statistics were applied to describe the sample regarding unique clinical characteristics of each participant (time since diagnosis, remission status, kidney involvement, associated antiphospholipid antibody syndrome) and at each time point when samples were obtained (e.g., active disease defined as SLEDAI > 4, anemia, skin involvement, articular involvement). These characteristics served as the basis for further analysis as grouping discriminants. Wilcoxon-rank-sum-test was applied to investigate the levels of sICPs between patient subgroups. For non-time-dependent variables, one representative time point per patient was included. For time-dependent variables, all available visits were used. This pragmatic approach was chosen to maximize data use while avoiding artificial inflation of patient numbers for fixed variables. More complex longitudinal models such as generalized estimating equations (GEE) were not applied, as our primary objective was to identify cross-sectional associations between biomarker levels and clinical phenotypes. The following clinical considerations were applied: for kidney involvement, the sample closest to the time of maximum creatinine was chosen; for remission and APS, the first recorded time point was used. For disease activity, anemia, skin involvement, and articular involvement, all recorded values were included in the analysis. Subsequently, multivariable logistic regression models were performed for each sICP showing significant differences in the location test. Thereby, the respective discriminant factor was set as dependent variable. To account for potential confounding, age, sex, and current daily prednisolone dose were included as covariates in all multivariable logistic regression models. If a multivariable model shows a significant fit, a univariate logistic regression model was performed with the respective sICPs as independent variable. The Receiver-Operating-Characteristic (ROC) was plotted and the area under the curve (AUC) calculated.
Besides, an unsupervised cluster analysis of certain sICPs with significant higher levels in the group of samples with a SLEDAI > 4 was conducted. Established biomarkers for SLE-Activity (anti-dsDNA, C3, C4 and SIGLEC-1) were also included. The k-mean method was chosen to investigate the possible deviating tendency of sICPs compared to established biomarkers.
Spearman coefficients were calculated between selected sICPs and the following biomarkers/clinical factors: SLEDAI; anti-dsDNA; proteinuria; creatinine; hemoglobin concentration (Hb); complement factor 3 (C3); complement factor 4 (C4); and CD163/SIGLEC-1 expressed on peripheral CD14+ monocytes. All statistical analyses were performed by using R 4.4.2 (R Foundation for Statistical Computing), utilizing packages including dplyr (v1.1.4), gtsummary (v2.2.0), broom (v1.0.8), pROC (V1.18.5), openxlsx (v4.2.8), broom.helpers (v1.20.0), ggplot2 (v3.5.1), tibble (v3.2.1), readxl (v1.4.5), purrr (v1.0.2), tidyr (v1.3.1), stringr (v1.5.1), forcats (v1.0.0), scales (v1.3.0), RColorBrewer (v1.1-3), corrplot (v0.95), pheatmap (v1.0.12), survival (v3.7-0), stats (v4.4.2), utils (v4.4.2) (26). A final spelling check was performed using ChatGPT (OpenAI).
Results
Cohort characteristics
According to the EULAR/ACR classification criteria 2019, we identified 235 SLE patients being followed at Charité Universitätsmedizin Berlin during 416 time points between January 2016 and February 2023. As typical for SLE, the majority of the patients were women (90%) and the median age was 38 years. The mean disease duration was 8 years and varied among patients: 17% had been diagnosed within the past 3 years, 42% between 3 to 10 years, and (41%) diagnosed over 10 years ago. Taking this into account, patients were retrospectively classified based on available longitudinal data regarding long-term remission according to DORIS and LLDAS criteria (4, 5). A total of 98 patients (41%) achieved LLDAS (mean disease duration of 13 years), of whom 60 patients (25%) (mean disease duration of 13 years) also met the criteria for DORIS remission. In contrast, 137 patients (57%) showed a rather remission-relapsing phenotype and did not achieve either DORIS or LLDAS long-term remission (mean disease duration of 11 years).
Regarding organ manifestations, kidney involvement was present in 38% of patients, with a small fraction experiencing kidney failure in our observation period (0.5%). Anemia was observed in 33% of patients, followed by the presence of an antiphospholipid syndrome (APS, 23%), skin (12%) and articular manifestations (6%). The SLE patients in our cohort received individual treatment regimes, so medication changed over time according to their disease activity. At the first presentation in our clinic during the observational period, most of the patients received hydroxychloroquine (58%) and prednisolone (45%, mean dose per day was 4,8 mg/d) followed by azathioprine (23%) and mycophenolate mofetil (14%) as well as initial biologics (belimumab in 5%, rituximab in 6%). Demographic and clinical characteristics as well as treatment regimen for all study participants are summarized in Table 1.
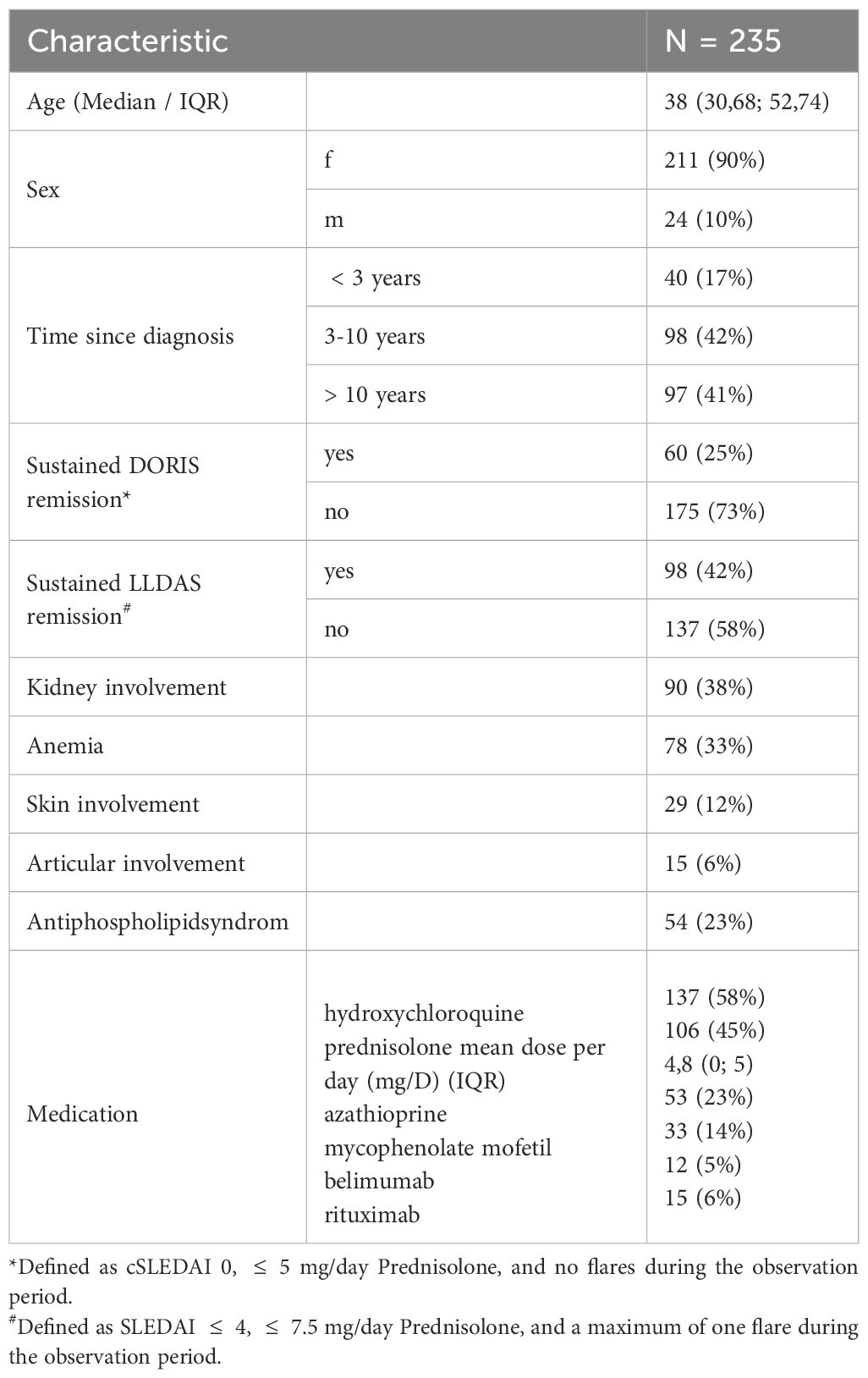
Table 1. Demographic and clinical characteristics.
Higher levels of sCD25, sTim-3 and sGal-9 are characteristic of active SLE
In a first step, we wanted to identify possible biomarkers for SLE activity. Therefore, the study participants were categorized at each time point of their presentation in our clinic as either inactive or active according to a SLEDAI score above 4. All recorded time points were included in this analysis. First, we performed a Wilcoxon rank sum test using the median values of checkpoint molecules and identified significant higher levels of sCD25, sCTLA-4, sGal-9, sLAG-3, sPD-1, sPD-L1, sTim-3, and sCD27 in active compared to inactive patients (Supplementary Table 3).
To rule out possible confounders and to evaluate the odds of disease activity in relation to the levels of these checkpoint molecules, we conducted a multivariable logistic regression analysis. We defined prednisolone dose, age and sex as possible confounder and adjusted accordingly. Interestingly, higher concentrations of sCD25, sTim-3 and sGal-9 were associated with active disease (Figure 1A), confirming these three molecules as the most robust ones related to higher lupus activity. The prednisolone dose appeared to be the most significant confounder when comparing active versus inactive patients in our system, as it is administered in higher doses or as a pulse therapy in active patients. We assessed the predictive performance of these molecules for active SLE using univariate logistic regression and ROC analysis. Interestingly, the ROC curve for sCD25 demonstrated an AUC value of 0.650, sGal-9 0.653 and sTim-3 an AUC value of 0.626 (Figure 1B).
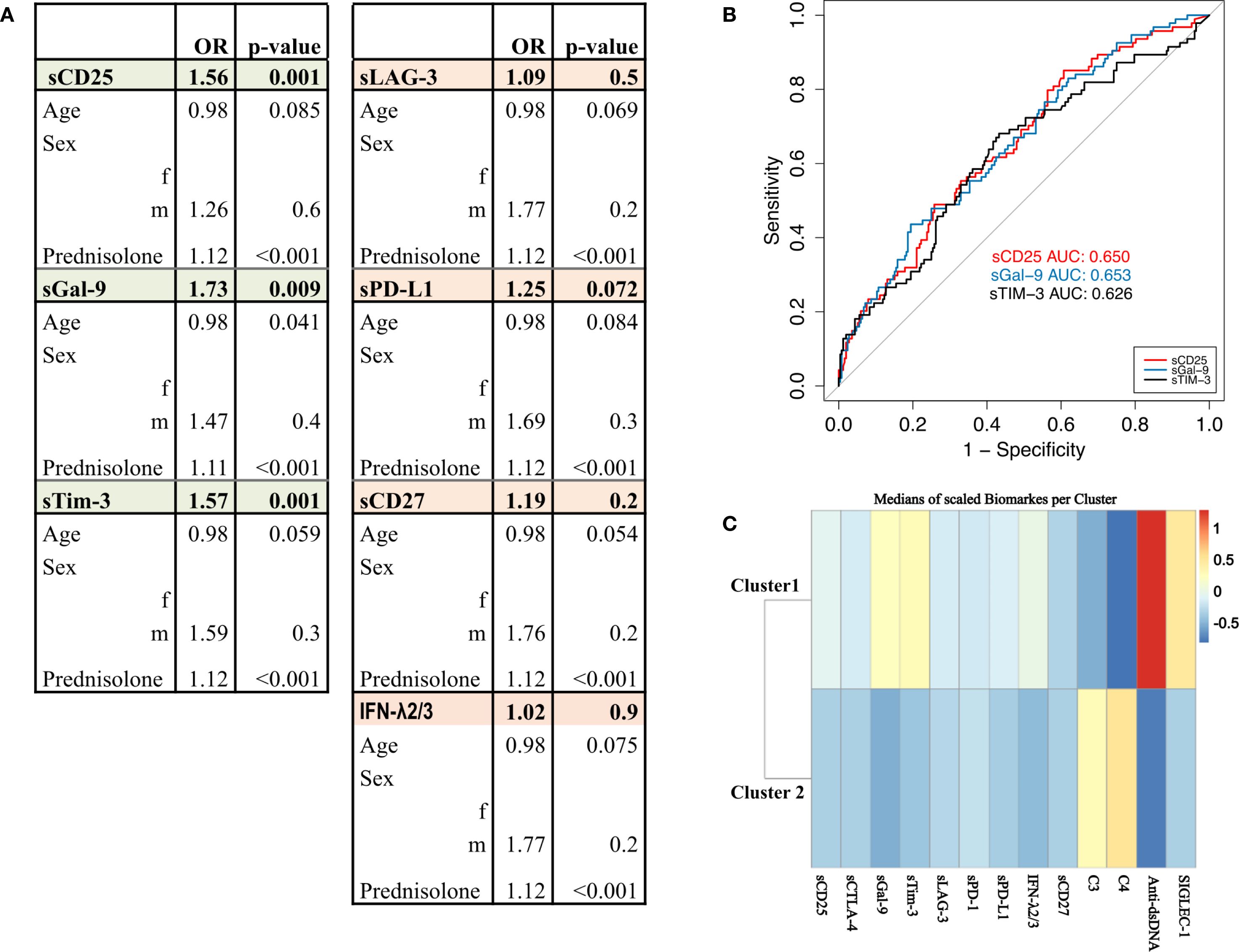
Figure 1. SLEDAI. (A) Circulating levels of sCD25, sTim-3 and sGal-9 are higher in the disease group (SLEDAI > 4) compared with patients in remission or LLDAS (SLEDAI ≤ 4). Multivariable logistic regression model adjusted for age, sex, and prednisolone dose. Significant results (p<0.05) are highlighted in green, non-significant results are shown in orange. (B) ROC curves displaying the predictive performance of univariate logistic regression models for biomarkers sCD25 (red), sTim-3 (black), and sGal-9 (blue) differentiate SLEDAI active vs. inactive states. (C) Cluster analysis of biomarker levels identifies two groups based on similarities in biomarker expression. The analysis represents the median values of biomarkers per cluster, with higher biomarker levels shown in red and lower levels in blue. Highlighting patterns of biomarker distribution across the cluster.
Cluster analysis
To identify potential subgroups of patients with similar biomarker profiles, we conducted an unsupervised cluster analysis of all patients with active SLE (SLEDAI > 4) including classical biomarkers, such as anti-dsDNA titer, complement C3, C4 levels and CD169/Siglec-1 expression related to type I IFN as well as the most identified sICPs (sCD25, sGal-9, sTim-3, sPD-L1, IFN-λ2/3 and sCD27) (Figure 1C). The resulting plot illustrates the mean values of the biomarkers within the different clusters. Two main clusters were identified: cluster 1 containing 26 patients and cluster 2 containing 39 patients. Detailed characteristics of the patients in each cluster are given in Supplementary Table 4.
Cluster 1 included SLE patients with significantly higher disease activity (median SLEDAI 10) compared to Cluster 2 (median SLEDAI 6). In addition to higher anti-dsDNA titers and hypocomplementemia, patients in cluster 1 exhibited also significantly higher levels of Siglec-1, sCD25, sTim-3, and sGal-9 compared to those in Cluster 2, along with higher levels of IFN-λ2/3. The clustering indicates that within the active SLE cohort, there is a subgroup with known conventional lupus activity markers as well as elevated checkpoint molecule levels. This pattern suggests a subgroup with high disease activity and elevated checkpoint molecules, potentially linked to more severe manifestations.
Soluble checkpoint molecules as biomarkers for renal and hematologic SLE manifestations
Given the heterogeneity of the disease, we aimed to identify in a next step, the role of sICPs in specific organ manifestations of SLE. According to the cohort characteristics, we focused on renal, hematologic (anemia), skin and articular manifestations as well as the presence of an associated APS. Therefore, we compared the group of patients with increased disease activity in one specific organ system with patients who never experienced activity in this organ system, respectively. Using Wilcoxon rank sum tests, we observed significantly higher levels of sCD25, sTim-3, sGal-9 and sPD-1 in patients with renal involvement (Supplementary Table 5). To account for potential confounders such as age, sex, prednisolone dose, we performed multivariable logistic regression and ROC curve analysis. This evaluation revealed sCD25, sTim-3 and sGal-9 as the most robust soluble checkpoint molecules related to renal manifestations (Figures 2A, B, Supplementary Figure 1). In patients presenting with anemia, Wilcoxon rank sum tests also revealed elevated serum concentrations of 4-1BB, sCD25, sCTLA-4, sGal-9, sPD-L1, sTim-3, IFN-α2, sCD27 and BAFF compared to patients without anemia (Supplementary Table 6). Multivariable logistic regression and ROC curve analysis confirmed these associations only for sCD25, sGal-9, sTim-3 and BAFF (Figures 2C, D). A detailed analysis of the patient distribution showed that 38% of the patients with kidney involvement also presented concomitantly with anemia.
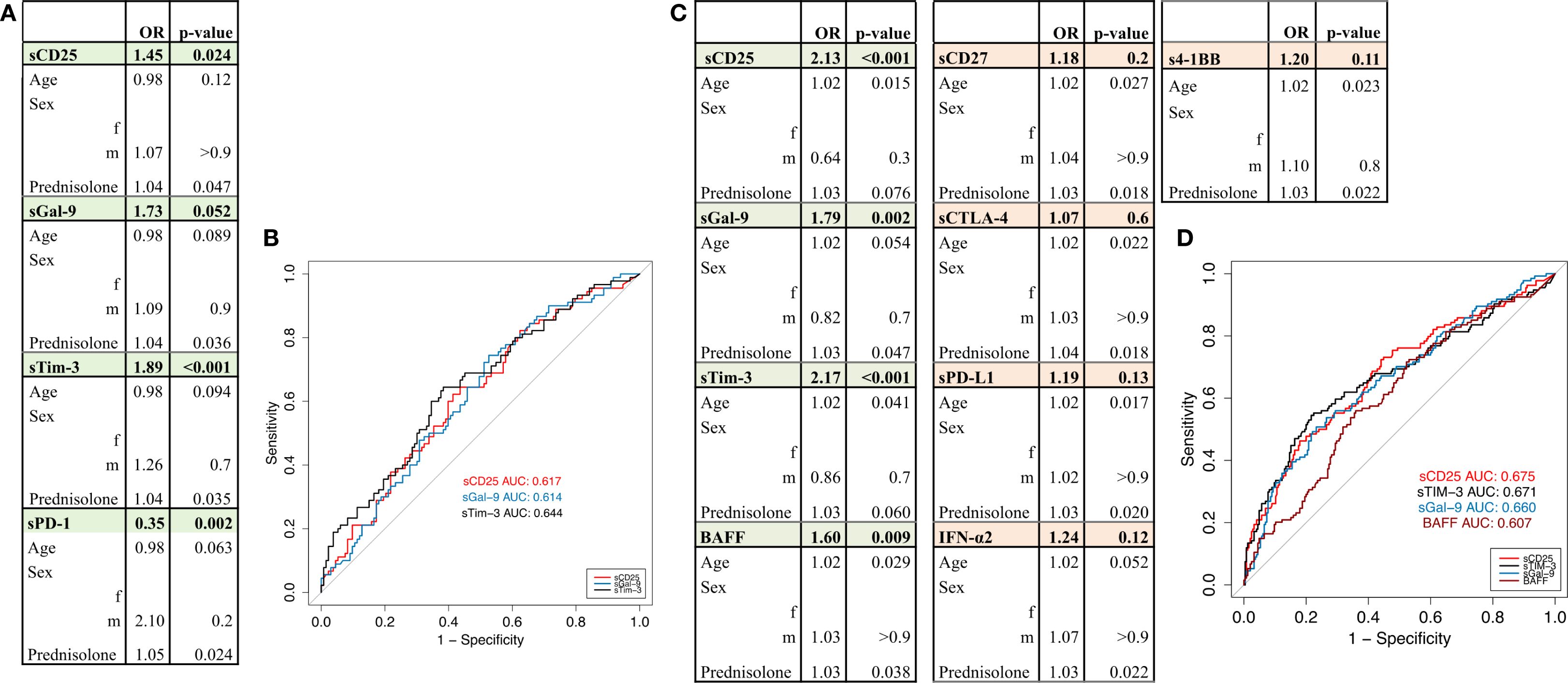
Figure 2. Kidney involvement and anemia. (A) Circulating levels of sCD25, sTim-3, sGal-9 and sPD-1 are higher in patients with renal involvement compared to patients without renal involvement. Multivariable logistic regression model adjusted for age, sex, and prednisolone dose. Significant results (p<0.05) are highlighted in green, non-significant results are shown in orange. (B) ROC curves displaying the predictive performance of univariate logistic regression models for biomarkers sCD25 (red), sTim-3 (black), and sGal-9 (blue) in differentiating patients with and without renal involvement. (C) Circulating levels of sCD25, sTim-3, sGal-9 and BAFF are higher in patients with anemia compared to patients without anemia. Multivariable logistic regression model adjusted for age, sex, and prednisolone dose. Significant results (p< 0.05) are highlighted in green, non-significant results are shown in orange. (D) ROC curve displaying the predictive performance of univariate logistic regression models for sCD25 (red), sTim-3 (black), sGal-9 (blue) and BAFF (brown) in differentiating patients with versus without anemia.
Differences in sICPs levels were observed in patients with skin manifestation in univariable analysis for IFN-λ2/3 (Supplementary Table 7), but not in the multivariable model (Supplementary Table 8). Interestingly, no significant differences of sICPs level were found in patients with skin (Supplementary Tables 7, 8) or articular manifestations (Supplementary Table 9) or associated APS (Supplementary Table 10), respectively.
To evaluate the relationship between the checkpoint molecules and clinical parameters, we performed a correlation matrix (Figures 3A, B): strong positive correlations between sCD25, sTim-3, and sGal-9 were found suggesting that they are likely involved in interrelated pathophysiologic mechanisms driving their upregulation and appearance in the circulation. With respect to clinical data, a direct correlation was seen between sTim-3 level and proteinuria. Notably, no correlation was observed between the significant sICPs and Siglec-1 expression on peripheral CD14+ monocytes suggesting that these molecules are probably independent of type I IFN upregulation.
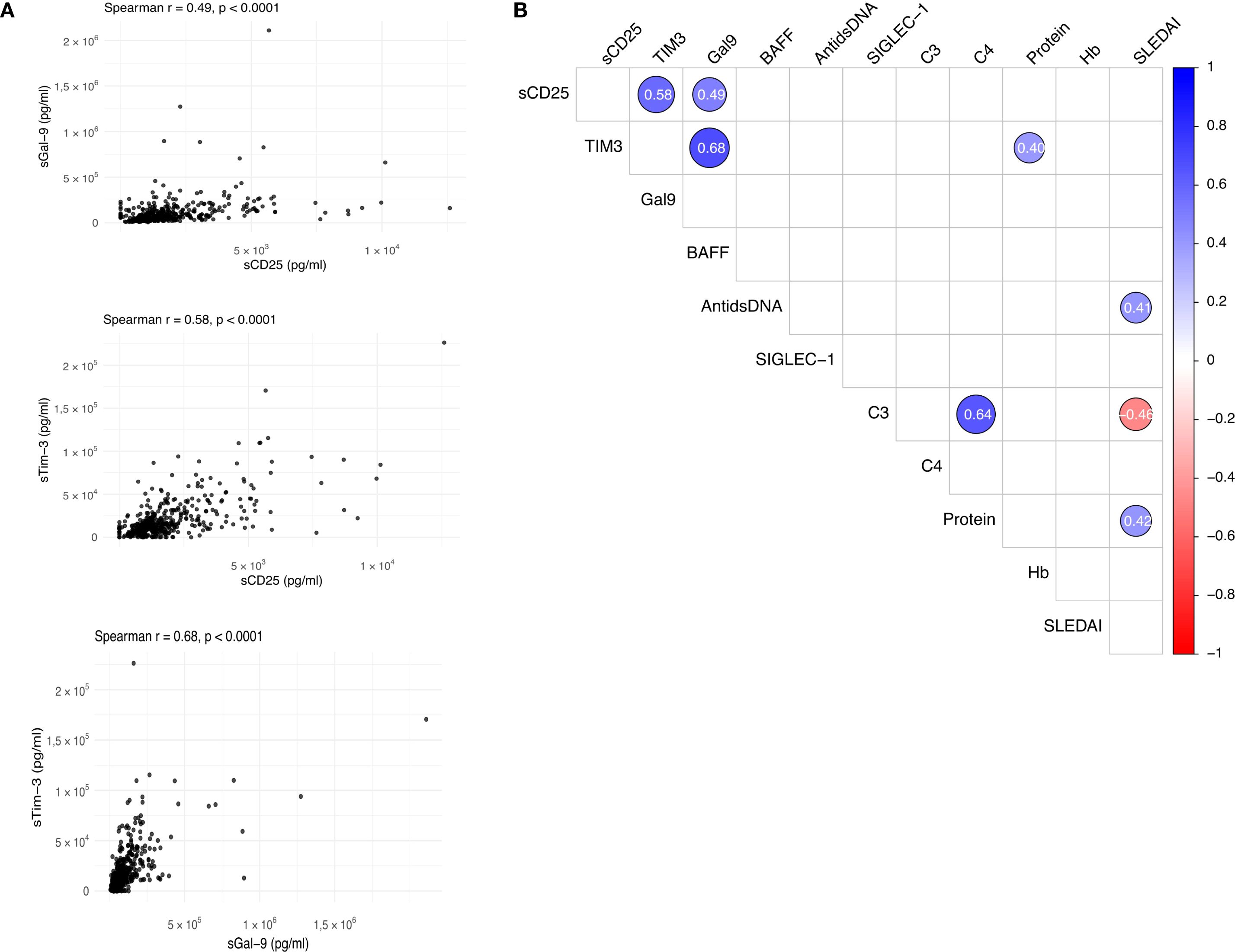
Figure 3. Correlation. (A) Scatter plots showing correlations between sCD25, sTim-3 and sGal-9. Pearson correlation coefficients (r) and p-values are provided for each comparison. (B) Correlation matrix displaying associations between biomarkers (sCD25, sTim-3 and sGal-9 and BAFF) and other parameters (anti-dsDNA, SIGLEC-1, C3, C4 Proteinuria, Hb, SLEDAI and cSLEDAI). Correlation coefficients are represented by color intensity, with blue indicating positive and red negative correlations.
Low sCD25 levels as robust biomarkers for sustained remission.
To assess long-term remission in patients with SLE, we evaluated their status based on established criteria for DORIS and LLDAS during the observational period. A total of 98 out of 235 patients (42%) met the criteria for LLDAS, of whom 60 patients (25%) also fulfilled the criteria for DORIS remission.
Patients were retrospectively classified into four distinct groups: those achieving DORIS remission, those achieving LLDAS remission, those achieving LLDAS remission but not DORIS, and those who did not achieve either DORIS or LLDAS remission. In an initial step, Wilcoxon rank sum tests revealed that patients in sustained DORIS or LLDAS remission displayed significantly lower levels of sCD25 and sTim-3 (Supplementary Tables 11, 13, 14). Multivariable logistic regression (Supplementary Table 12, Figure 4) revealed that lower concentrations of sCD25 were consistently associated with a higher likelihood of achieving both DORIS and LLAS remission. In contrast, patients who did not achieve either DORIS or LLDAS remission exhibited significantly elevated levels of sCD25 and sTim-3. (Supplementary Table 11, Figures 4A, C).
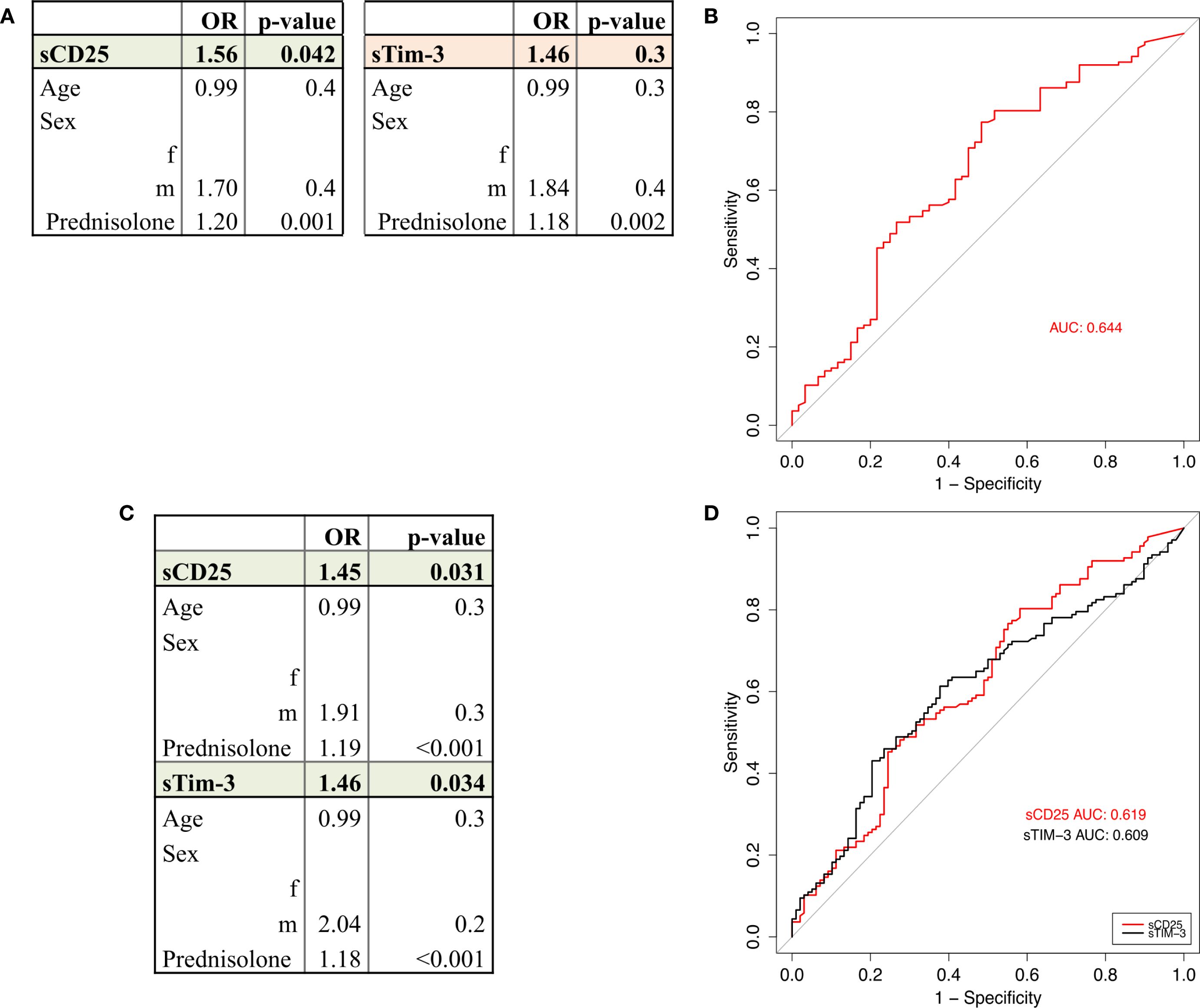
Figure 4. DORIS remission and LLDAS remission. (A) Circulating levels of sCD25 and sTim-3 are lower in patients in DORIS Remission compared to those neither in DORIS nor in LLDAS. Multivariable logistic regression model adjusted for age, sex, and prednisolone dose. Significant results (p<0.05) of sCD25 are highlighted in green, non-significant results (sTIM-3) are shown in orange. (B) ROC curves displaying the predictive performance of univariate logistic regression models for biomarker sCD25 (red). (C) Circulating levels of sCD25 and sTim-3 are lower in patients in LLDAS remission compared to those not in LLDAS. Multivariable logistic regression model adjusted for age, sex, and prednisolone dose. Significant results (p< 0.05) are highlighted in green, non-significant results are shown in orange. (D) ROC curve displaying the predictive performance of univariate logistic regression models for sCD25 (red) and sTim-3 (black).
The prednisolone dose appeared to be the most influential confounder in comparing remission and non-remission groups, as it is administered in higher doses or as pulse therapy in patients with active disease who fail to achieve DORIS or LLDAS remission. (Supplementary Table 11, Figures 4A, B). None of the investigated molecules could differentiate between patients in DORIS remission and patients fulfilling LLDAS criteria without DORIS remission.
To further evaluate the predictive power of sCD25 and sTim-3, univariate models were calculated, and receiver operating characteristics (ROC) analyses were performed. The predictive performance of sCD25 was particularly strong in the DORIS vs. neither DORIS nor LLDAS comparison (AUC=0.619) (Figure 4B), while sTim-3 added predictive values in the LLDAS vs. non-LLDAS comparison (AUC=0.609) (Figure 4D).
Discussion
In this study, we investigated the role of various immune checkpoint molecules in relation to disease activity, specific organ manifestations and long-term outcome in patients with SLE. We included molecules belonging to different co-stimulatory and co-inhibitory pathways, to be able to assess the inflammatory orchestration related to their immunobiology mechanisms. To understand dynamic changes during disease progression, we analyzed data at multiple time points to identify potential temporal dynamics in SLE.
As key findings, higher serum concentration of the co-stimulatory molecule sCD25 as well as of the co-inhibitory molecules, sTim-3 and sGal-9 were characteristic in active SLE patients, specifically in patients with kidney involvement and/or anemia. However, although skin and joint manifestations are components of SLEDAI, organ specific analyses did not reveal independent associations with cutaneous and articular involvement or presence of APS, supporting the hypothesis that specific sICPs may play different roles in certain organ manifestations. Moreover, these molecules together with the conventional activity markers (anti-ds-DNA titers and hypocomplementemia) identified a more severe disease phenotype, consistent with our unsupervised cluster analysis. sCD25 was uniquely associated with sustained DORIS/LLDAS remission, indicating its potential role as a biomarker for identifying patients eligible for treatment de-escalation and reduced pharmacologic exposure.
Although membrane-bound immune checkpoint molecules are well characterized, the origin and function of their circulating soluble forms remains incompletely understood. In addition to proteolytic cleavage by metalloproteases and/or alternative pre-mRNA splicing (27), they may also arise from passive release during enhanced lymphocyte death or fragility, a phenomenon observed in SLE (28). In our cohort, however, leukocyte counts did not correlate with sCD25, sTim-3, or sGal-9 (Supplementary Figure 3), supporting shedding and/or splicing as the more likely predominant sources.
sCD25 also known as sIL-2R (soluble interleukin 2 receptor), is a key co-stimulatory receptor for the human immune system, playing a crucial role for an adequate T cell response (via proliferation of effector T cells) as well as in immune tolerance and regulation of CD4+ T lymphocytes (via T regulatory cells/Treg (29),). Elevated sCD25 values are known to be present in patients with granulomatous lesions and are included in the classification criteria for sarcoidosis (30) and hemophagocytic lymphohistiocytosis (HLH) (31). In SLE, acquired interleukin-2 (IL-2) deficiency disrupts the balance between Treg and pathogenic effector/memory CD4+ T cells, impairing Treg homeostasis and promoting autoreactive T-cell activity and chronic inflammation (32). Accordingly, low-dose IL-2 approaches have shown immunomodulatory effects in SLE, including Treg expansion in early studies (33, 34), however, clinical efficacy remains uncertain (35). In this context, higher circulating levels of sCD25 may indicate an inefficient or abnormal immune regulation, potentially compensating impaired Treg dysfunction and IL-2 deficiency. In a clinical context, elevated levels of sCD25 in SLE have been reported to be associated with higher disease activity and with lupus nephritis (36). In our cohort, we could furthermore identify low sCD25 as a key biomarker for long-term DORIS and LLDAS remission.
The next identified significant sICPs Tim-3 and Gal-9, describe a receptor-ligand interrelationship. Tim-3 is a unique inhibitory receptor, being largely restricted to terminally differentiated, inflammatory IFN-γ-producing T helper 1 (Th1) CD4+ and CD8 T cells (37). IFN-γ is a central driver of SLE pathogenesis, particularly in lupus nephritis, and remains insufficiently controlled by current therapies (38, 39). At the same time, IFN-γ regulates multiple inhibitory checkpoint molecules including Tim-3/Gal-9 and PD-1/PD-L1 pathways (40, 41). Tim-3, initially identified as a marker of IFN-γ-producing CD4+ and CD8+ T cells (40), has been reported to have multiple different ligands, whereby the interaction with galectin 9 (Gal-9) seems to reflect the main inhibitory pathway, leading to T cell exhaustion and ultimately to cell death (42). In line with this, several subsets of T and B cells in SLE exhibit signs of functional exhaustion or remain in a post-activated state (43–45), a phenotype, which may be linked to enhanced activation of inhibitory immune checkpoints (46). Soluble Tim-3 is supposed to be mainly a result of metalloproteinase-dependent cleavage that facilitates its shedding from the cell surface (47) and has functionally the ability to reduce IL-2 production by T cells (48). In this context, higher levels of sTim-3 may reflect an inefficient attempt to counterbalance the continuous immune activation in SLE, by simultaneously accentuating the IL-2 deficiency. Our study highlights the role of the Tim-3 – Gal-9 pathway in SLE and goes in line with previous work showing increased Tim-3 expression upon SLE CD3+CD4+ T cells (49) as well as higher values of sTim-3 in SLE compared with healthy controls (50). Our association of sTim-3 with SLE kidney involvement underlines the previous observation of Tim-3 expression in the renal interstitial and tubular epithelial cells from lupus nephritis patients (51). An observation of our cohort is the association of increased sTim-3 and anemia that is undergoing further delineation.
With respect to Gal-9, there is evidence that it may be induced by Tim-3 as an inhibitory feedback mechanism (37), and can also exert Tim-3-independent effects (42). Previous studies have reported significantly higher sGal-9 levels in SLE patients compared to healthy controls, including a correlation with lupus disease activity (52, 53). Our data provide additional evidence towards a relationship between Gal-9 levels with specific organ manifestations like kidney involvement and anemia. Interestingly, although sTim-3 and sGal-9 showed strong associations with active SLE, particularly with renal and hematologic manifestations, they were not linked to sustained DORIS/LLDAS remission. Further research it needed to elucidate the molecular mechanism underlying sustained remission. While sPD-1 showed a significant association with renal involvement in both univariable and multivariable logistic regression analyses, its poor discriminatory performance in ROC analysis (AUC 0.369) suggests that sPD-1 lacks clinically utility as a biomarker in this context.
BAFF, also known as BlyS (B-lymphocyte stimulator), is a cytokine belonging to the tumor necrosis factor (TNF) family and plays a key role in B-cell activation, differentiation and survival (24). In our study, BAFF was significantly associated with anemia in SLE patients. The underlying mechanism resulting in increased BAFF may comprise increased cleavage and/or production. As there is only a moderate effect of belimumab, a monoclonal antibody targeting BAFF, on anemia (54), the current finding provides the basis for further mechanistic studies.
To sum up, our findings indicate that certain checkpoint molecules are intimately associated with increased disease activity, specific clinical manifestations and able to predict long-term outcome. The strong correlations between sCD25, sTim-3, and sGal-9 levels suggest their involvement in shared immune T/B abnormalities possibly related to increased IFNγ.
The main limitation of this study is its retrospective nature including lack of standardized data collection and various patient observation periods. Additionally, treating each time point as an independent data source rather than analyzing time-course data of individual patients precluded more stringent data assessments. Individual overlap of organ manifestations may be another significant confounder of the current analyses.
Our study identified a significant diagnostic value for sCD25, sTim-3, sGal-9 and BAFF as biomarkers for subsets of SLE patients and predicting outcome. The results enhance our understanding of the role certain CPM for disease activity and candidate for innovative diagnostic and therapeutic biomarkers. Most notably, low sCD25 levels were particularly associated with long-term DORIS and LLDAS remission, highlighting its potential as a marker for sustained disease control and potentially holding promise to guide safely treatment de-escalation or discontinuation. Nevertheless, translation into clinical practice will require assay standardization, validation in independent cohorts, and longitudinal studies to confirm its relevance as a biomarker guiding personalized therapeutic strategies in SLE.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethic committee at the Charité University Hospital Berlin. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LD: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. JS: Formal analysis, Writing – review & editing. HR: Methodology, Writing – review & editing, Data curation. AA: Writing – review & editing. BO: Formal analysis, Writing – review & editing. AW: Data curation, Writing – review & editing. FS: Data curation, Writing – review & editing. GK: Writing – review & editing. TD: Data curation, Funding acquisition, Resources, Supervision, Writing – review & editing. ES: Data curation, Project administration, Supervision, Writing – review & editing. AS: Data curation, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Funding TD: Funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) projects Do491/7-5, 11-1, 12-1, 14-1 (KFO BECAUSE-Y, P7). TD/ALS: CURE-ME Project WP3 funded by BMBF (Federal Ministery of Education and Research, Germany) ALS: Rahel-Hirsch scholarship of Universitätsklinik Charité, Berlin, Germany.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. A final spelling check was performed using ChatGPT (OpenAI).
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1685275/full#supplementary-material
References
1. Crow MK. Pathogenesis of systemic lupus erythematosus: risks, mechanisms and therapeutic targets. Ann Rheumatic Diseases. (2023) 82:999. doi: 10.1136/ard-2022-223741
2. Dorner T and Lipsky PE. The essential roles of memory B cells in the pathogenesis of systemic lupus erythematosus. Nat Rev Rheumatol. (2024) 20:770–82. doi: 10.1038/s41584-024-01179-5
3. Hoi A, Igel T, Mok CC, and Arnaud L. Systemic lupus erythematosus. Lancet. (2024) 403:2326–38. doi: 10.1016/S0140-6736(24)00398-2
4. van Vollenhoven RF, Bertsias G, Doria A, Isenberg D, Morand E, Petri MA, et al. 2021 DORIS definition of remission in SLE: final recommendations from an international task force. Lupus Sci Med. (2021) 80, 181–2. doi: 10.1136/annrheumdis-2021-eular.1192
5. Franklyn K, Lau CS, Navarra SV, Louthrenoo W, Lateef A, Hamijoyo L, et al. Definition and initial validation of a Lupus Low Disease Activity State (LLDAS). Ann Rheum Dis. (2016) 75:1615–21. doi: 10.1136/annrheumdis-2015-207726
6. Ugarte-Gil MF, Hanly J, Urowitz M, Gordon C, Bae SC, Romero-Diaz J, et al. Remission and low disease activity (LDA) prevent damage accrual in patients with systemic lupus erythematosus: results from the Systemic Lupus International Collaborating Clinics (SLICC) inception cohort. Ann Rheum Dis. (2022) 81:1541–8. doi: 10.1136/ard-2022-222487
7. Duarte-García A, Hocaoglu M, Valenzuela-Almada M, Osei-Onomah SA, Dabit JY, Sanchez-Rodriguez A, et al. Rising incidence and prevalence of systemic lupus erythematosus: a population-based study over four decades. Ann Rheum Dis. (2022) 81:1260–6. doi: 10.1136/annrheumdis-2022-222276
8. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European league against rheumatism/American college of rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. (2019) 71:1400–12. doi: 10.1002/art.40930
9. Sun J, Sui Y, Wang Y, Song L, Li D, Li G, et al. Galectin-9 expression correlates with therapeutic effect in rheumatoid arthritis. Sci Rep. (2021) 11:5562. doi: 10.1038/s41598-021-85152-2
10. Yanaba K, Hayashi M, Yoshihara Y, and Nakagawa H. Serum levels of soluble programmed death-1 and programmed death ligand-1 in systemic sclerosis: Association with extent of skin sclerosis. J Dermatol. (2016) 43:954–7. doi: 10.1111/1346-8138.13339
11. Fukasawa T, Yoshizaki A, Ebata S, Nakamura K, Saigusa R, Miura S, et al. Contribution of soluble forms of programmed death 1 and programmed death ligand 2 to disease severity and progression in systemic sclerosis. Arthritis Rheumatol. (2017) 69:1879–90. doi: 10.1002/art.40164
12. Yoon T, Ahn SS, Jung SM, Song JJ, Park YB, and Lee SW. Serum soluble programmed cell death protein 1 could predict the current activity and severity of antineutrophil cytoplasmic antibody-associated vasculitis: a monocentric prospective study. Clin Exp Rheumatol. (2019) 37 Suppl 117:116–21.
13. Pyo JY, Yoon T, Ahn SS, Song JJ, Park Y-B, and Lee S-W. Soluble immune checkpoint molecules in patients with antineutrophil cytoplasmic antibody-associated vasculitis. Sci Rep. (2022) 12:21319. doi: 10.1038/s41598-022-25466-x
14. Gamerith G, Mildner F, Merkel PA, Harris K, Cooney L, Lim N, et al. Association of baseline soluble immune checkpoints with the risk of relapse in PR3-ANCA vasculitis following induction of remission. Ann Rheum Dis. (2023) 82:253–61. doi: 10.1136/ard-2022-222479
15. Das R, Bar N, Ferreira M, Newman AM, Zhang L, Bailur JK, et al. Early B cell changes predict autoimmunity following combination immune checkpoint blockade. J Clin Invest. (2018) 128:715–20. doi: 10.1172/JCI96798
16. Stefanski AL and Dörner T. Immune checkpoints and the multiple faces of B cells in systemic lupus erythematosus. Curr Opin Rheumatol. (2021) 33:592–7. doi: 10.1097/BOR.0000000000000825
17. Vendel AC, Jaroszewski L, Linnik MD, and Godzik A--. and T-lymphocyte attenuator in systemic lupus erythematosus disease pathogenesis. Clin Pharmacol Ther. (2024) 116:247–56. doi: 10.1002/cpt.3282
18. Burke KP, Patterson DG, Liang D, and Sharpe AH. Immune checkpoint receptors in autoimmunity. Curr Opin Immunol. (2023) 80:102283. doi: 10.1016/j.coi.2023.102283
19. Mohammadi P, Hesari M, Chalabi M, Salari F, and Khademi F. An overview of immune checkpoint therapy in autoimmune diseases. Int Immunopharmacol. (2022) 107:108647. doi: 10.1016/j.intimp.2022.108647
20. Tuttle J, Drescher E, Simón-Campos JA, Emery P, Greenwald M, Kivitz A, et al. A phase 2 trial of peresolimab for adults with rheumatoid arthritis. New Engl J Med. (2023) 388:1853–62. doi: 10.1056/NEJMoa2209856
21. AnaptysBio I. Anaptys Announces Positive Rosnilimab Data Updated Through Six Months in Phase 2b Trial in RA. San Diego, CA: AnaptysBio, Inc (2025). Available online at: https://ir.anaptysbio.com/news-releases/news-release-details/anaptys-announces-positive-rosnilimab-data-updated-through-six (Accessed August 27, 2025).
22. Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH, and Derivation of the SLEDAI. A disease activity index for lupus patients. The Committee on Prognosis Studies in SLE. Arthritis Rheumatol. (1992) 35:630–40. doi: 10.1002/art.1780350606
23. Rose T, Grützkau A, Hirseland H, Huscher D, Dähnrich C, Dzionek A, et al. IFNα and its response proteins, IP-10 and SIGLEC-1, are biomarkers of disease activity in systemic lupus erythematosus. Ann Rheum Dis. (2013) 72:1639–45. doi: 10.1136/annrheumdis-2012-201586
24. Möckel T, Basta F, Weinmann-Menke J, and Schwarting A. B cell activating factor (BAFF): Structure, functions, autoimmunity and clinical implications in Systemic Lupus Erythematosus (SLE). Autoimmun Rev. (2021) 20:102736. doi: 10.1016/j.autrev.2020.102736
25. BioLegend. LEGENDplex™ HU Immune Checkpoint Panel 1 Manual. San Diego, CA: BioLegend. Available online at: https://www.biolegend.com/Files/Images/media_assets/pro_detail/datasheets/750000504_HU_Immune_Checkpoint_Panel_1_Manual_R01.pdf.
26. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2021). Team RC, editor.
27. Bailly C, Thuru X, and Quesnel B. Soluble programmed death ligand-1 (sPD-L1): A pool of circulating proteins implicated in health and diseases. Cancers (Basel). (2021) 13(12):3034. doi: 10.3390/cancers13123034
28. Fayyaz A, Igoe A, Kurien BT, Danda D, James JA, Stafford HA, et al. Hematological manifestations of lupus. Lupus Sci Med. (2015) 2:e000078. doi: 10.1136/lupus-2014-000078
29. Damoiseaux J. The IL-2 – IL-2 receptor pathway in health and disease: The role of the soluble IL-2 receptor. Clin Immunol. (2020) 218:108515. doi: 10.1016/j.clim.2020.108515
30. Vanmaris RMM and Rijkers GT. Biological role of the soluble interleukin-2 receptor in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. (2017) 34:122–9. doi: 10.36141/svdld.v34i2.5369
31. Henter J-I, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. (2007) 48:124–31. doi: 10.1002/pbc.21039
32. Ohmes J, Comdühr S, Akbarzadeh R, Riemekasten G, and Humrich JY. Dysregulation and chronicity of pathogenic T cell responses in the pre-diseased stage of lupus. Front Immunol. (2022) 13. doi: 10.3389/fimmu.2022.1007078
33. He J, Zhang X, Wei Y, Sun X, Chen Y, Deng J, et al. Low-dose interleukin-2 treatment selectively modulates CD4(+) T cell subsets in patients with systemic lupus erythematosus. Nat Med. (2016) 22:991–3. doi: 10.1038/nm.4148
34. Humrich JY, Cacoub P, Rosenzwajg M, Pitoiset F, Pham HP, Guidoux J, et al. Low-dose interleukin-2 therapy in active systemic lupus erythematosus (LUPIL-2): a multicenter, double-blind, randomized and placebo-controlled phase II trial. Ann Rheum Dis. (2022) 81:1685–94. doi: 10.1136/ard-2022-222501
35. Nektar Therapeutics. Nektar therapeutics announces phase 2 topline data for rezpegaldesleukin in patients with systemic lupus erythematosus(2023). Available online at: https://www.prnewswire.com/news-releases/nektar-therapeutics-announces-phase-2-topline-data-for-rezpegaldesleukin-in-patients-with-systemic-lupus-erythematosus-301754953.html (Accessed August 27, 2025).
36. Zhang RJ, Zhang X, Chen J, Shao M, Yang Y, Balaubramaniam B, et al. Serum soluble CD25 as a risk factor of renal impairment in systemic lupus erythematosus — a prospective cohort study. Lupus. (2018) 27:1100–6. doi: 10.1177/0961203318760993
37. Wolf Y, Anderson AC, and Kuchroo VK. TIM3 comes of age as an inhibitory receptor. Nat Rev Immunol. (2020) 20:173–85. doi: 10.1038/s41577-019-0224-6
38. Chasset F and Arnaud L. Targeting interferons and their pathways in systemic lupus erythematosus. Autoimmun Rev. (2018) 17:44–52. doi: 10.1016/j.autrev.2017.11.009
39. Moneta GM, Bracaglia C, Caiello I, Farroni C, Pires Marafon D, Carlomagno R, et al. Persistently active interferon-γ pathway and expansion of T-bet+ B cells in a subset of patients with childhood-onset systemic lupus erythematosus. Eur J Immunol. (2023) 53:2250319. doi: 10.1002/eji.202250319
40. Dixon KO, Lahore GF, and Kuchroo VK. Beyond T cell exhaustion: TIM-3 regulation of myeloid cells. Sci Immunol. (2024) 9:eadf2223. doi: 10.1126/sciimmunol.adf2223
41. Chen G, Huang AC, Zhang W, Zhang G, Wu M, Xu W, et al. Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature. (2018) 560:382–6. doi: 10.1038/s41586-018-0392-8
42. Zhu C, Anderson AC, Schubart A, Xiong H, Imitola J, Khoury SJ, et al. The Tim-3 ligand galectin-9 negatively regulates T helper type 1 immunity. Nat Immunol. (2005) 6:1245–52. doi: 10.1038/ni1271
43. Schrezenmeier E, Weißenberg SY, Stefanski A-L, Szelinski F, Wiedemann A, Lino AC, et al. Postactivated B cells in systemic lupus erythematosus: update on translational aspects and therapeutic considerations. Curr Opin Rheumatol. (2019) 31:175–84. doi: 10.1097/BOR.0000000000000576
44. Wang K, Zhao J, Feng X, He S, Li J, Sun F, et al. PD-1/PD-L1 governed cross-talk of exhausted CD8(+) T and memory B cells in systemic lupus erythematosus. RMD Open. (2024) 10:e003503. doi: 10.1136/rmdopen-2023-003503
45. Guo C, Liu Q, Zong D, Zhang W, Zuo Z, Yu Q, et al. Single-cell transcriptome profiling and chromatin accessibility reveal an exhausted regulatory CD4+ T cell subset in systemic lupus erythematosus. Cell Rep. (2022) 41(6):111606. doi: 10.1016/j.celrep.2022.111606
46. Khan AR, Hams E, Floudas A, Sparwasser T, Weaver CT, and Fallon PG. PD-L1hi B cells are critical regulators of humoral immunity. Nat Commun. (2015) 6:5997. doi: 10.1038/ncomms6997
47. Möller-Hackbarth K, Dewitz C, Schweigert O, Trad A, Garbers C, Rose-John S, et al. A disintegrin and metalloprotease (ADAM) 10 and ADAM17 are major sheddases of T cell immunoglobulin and mucin domain 3 (Tim-3) *. J Biol Chem. (2013) 288:34529–44. doi: 10.1074/jbc.M113.488478
48. Gonçalves Silva I, Yasinska IM, Sakhnevych SS, Fiedler W, Wellbrock J, Bardelli M, et al. The tim-3-galectin-9 secretory pathway is involved in the immune escape of human acute myeloid leukemia cells. EBioMedicine. (2017) 22:44–57. doi: 10.1016/j.ebiom.2017.07.018
49. Jiao Q, Qian Q, Zhao Z, Fang F, Hu X, An J, et al. Expression of human T cell immunoglobulin domain and mucin-3 (TIM-3) and TIM-3 ligands in peripheral blood from patients with systemic lupus erythematosus. Arch Dermatol Res. (2016) 308:553–61. doi: 10.1007/s00403-016-1665-4
50. Asano T, Matsuoka N, Fujita Y, Matsumoto H, Temmoku J, Yashiro-Furuya M, et al. Serum levels of T cell immunoglobulin and mucin-domain containing molecule 3 in patients with systemic lupus erythematosus. J Clin Med. (2020) 9:3563. doi: 10.3390/jcm9113563
51. Guo L, Yang X, Xia Q, Zhen J, Zhuang X, and Peng T. Expression of human T cell immunoglobulin domain and mucin-3 (TIM-3) on kidney tissue from systemic lupus erythematosus (SLE) patients. Clin Exp Med. (2014) 14:383–8. doi: 10.1007/s10238-013-0264-3
52. Matsuoka N, Fujita Y, Temmoku J, Furuya MY, Asano T, Sato S, et al. Galectin-9 as a biomarker for disease activity in systemic lupus erythematosus. PLoS One. (2020) 15:e0227069. doi: 10.1371/journal.pone.0227069
53. van den Hoogen LL, van Roon JAG, Mertens JS, Wienke J, Lopes AP, de Jager W, et al. Galectin-9 is an easy to measure biomarker for the interferon signature in systemic lupus erythematosus and antiphospholipid syndrome. Ann Rheum Dis. (2018) 77:1810–4. doi: 10.1136/annrheumdis-2018-213497
Keywords: SLE, biomarker, soluble immune checkpoints, remission, activity, SLEDAI
Citation: Dreveton L-S, Spencker JJ, Rincon-Arevalo H, Aue A, Osmanodja B, Wiedemann A, Szelinski F, Krönke G, Dörner T, Schrezenmeier E and Stefanski A-L (2025) Soluble checkpoint molecules as predictive biomarker for disease activity and long-term outcome in SLE. Front. Immunol. 16:1685275. doi: 10.3389/fimmu.2025.1685275
Received: 13 August 2025; Accepted: 03 September 2025;
Published: 25 September 2025.
Edited by:
Emanuele Bizzi, Vita-Salute San Raffaele University, ItalyReviewed by:
Mohammad Malekan, Mazandaran University of Medical Sciences, IranAndrew Vendel, Eli Lilly & Co, United States
Copyright © 2025 Dreveton, Spencker, Rincon-Arevalo, Aue, Osmanodja, Wiedemann, Szelinski, Krönke, Dörner, Schrezenmeier and Stefanski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Léa-Sophie Dreveton, bGVhc29waGllLmRyZXZldG9uQGdvb2dsZW1haWwuY29t