 Li Zhang
Li Zhang Ge Peng
Ge Peng Mingyue Wang
Mingyue Wang François Niyonsaba
François Niyonsaba Xinghua Gao
Xinghua Gao- 1Department of Dermatology, The First Hospital of China Medical University, Liaoning, China
- 2Key Laboratory of Immunodermatology, Ministry of Education and National Health Commission, National Joint Engineering Research Center for Theranostics of Immunological Skin Diseases, Liaoning, China
- 3Atopy (Allergy) Research Center, Juntendo University Graduate School of Medicine, Tokyo, Japan
- 4Faculty of International Liberal Arts, Juntendo University, Tokyo, Japan
Current atopic dermatitis treatments have been revolutionized by systemic targeted therapies that modulate inflammatory cytokine signaling pathways. While agents such as Janus kinase inhibitors and interleukin-4/interleukin-13 pathway inhibitors have shown significant efficacy, unmet needs persist. These needs include challenges in achieving stable disease control and remission, addressing nonresponders, managing potential side effects, and alleviating the ongoing struggle with pruritus. Future directions will focus on developing dual/multitarget drugs, creating longer-acting formulations, improving administration convenience, reducing dosing frequency, identifying novel therapeutic targets, and incorporating patient-reported outcomes in clinical assessments.
1 Introduction
Atopic dermatitis (AD) is a prevalent chronic inflammatory skin condition, which are not associated with autoimmune diseases but are instead linked to IgE-mediated conditions such as asthma, rhinitis, conjunctivitis, and food allergy (1). In the United Kingdom alone, approximately one in five children and one in ten adults are affected by AD (2), whereas in developed countries overall, the prevalence of AD is estimated to range from 15 to 20% (3). Clinically, AD is characterized by dry, intensely itchy skin, often accompanied by redness (erythema) and thickening of the skin (lichenification), which significantly impair patients’ quality of life. Relentless itch and visible skin changes often result in sleep disturbances, anxiety, depression, social isolation, and reduced productivity, highlighting the broader psychosocial toll of the disease (4, 5).
The intricate pathophysiology of AD involves a complex interplay of genetic predisposition, immune dysregulation, skin barrier dysfunction, and environmental factors (5–8). A dysregulated T helper 2 (Th2) immune response plays a central role, triggering the overproduction of type 2 cytokines such as interleukin (IL)-4, IL-5, IL-13, IL-31 and thymic stromal lymphopoietin (TSLP), as well as histamine release and eosinophilic infiltration (9). These cytokines not only drive characteristic pruritus and inflammation but also perpetuate epidermal barrier impairment. In chronic AD, immune polarization often shifts toward the Th1 and Th17 pathways, contributing to sustained inflammation and epidermal hyperplasia (7). Notably, many of the abovementioned cytokines exert their biological effects through the Janus kinase/signal transducer and activator of transcription (JAK/STAT) signaling cascade, which plays a pivotal role in amplifying and sustaining the inflammatory milieu in patients with AD (10, 11). The identification of these specific immune pathways and their driving cytokines has been pivotal for understanding AD pathogenesis, paving the way for the development of targeted therapeutic agents (Figure 1).
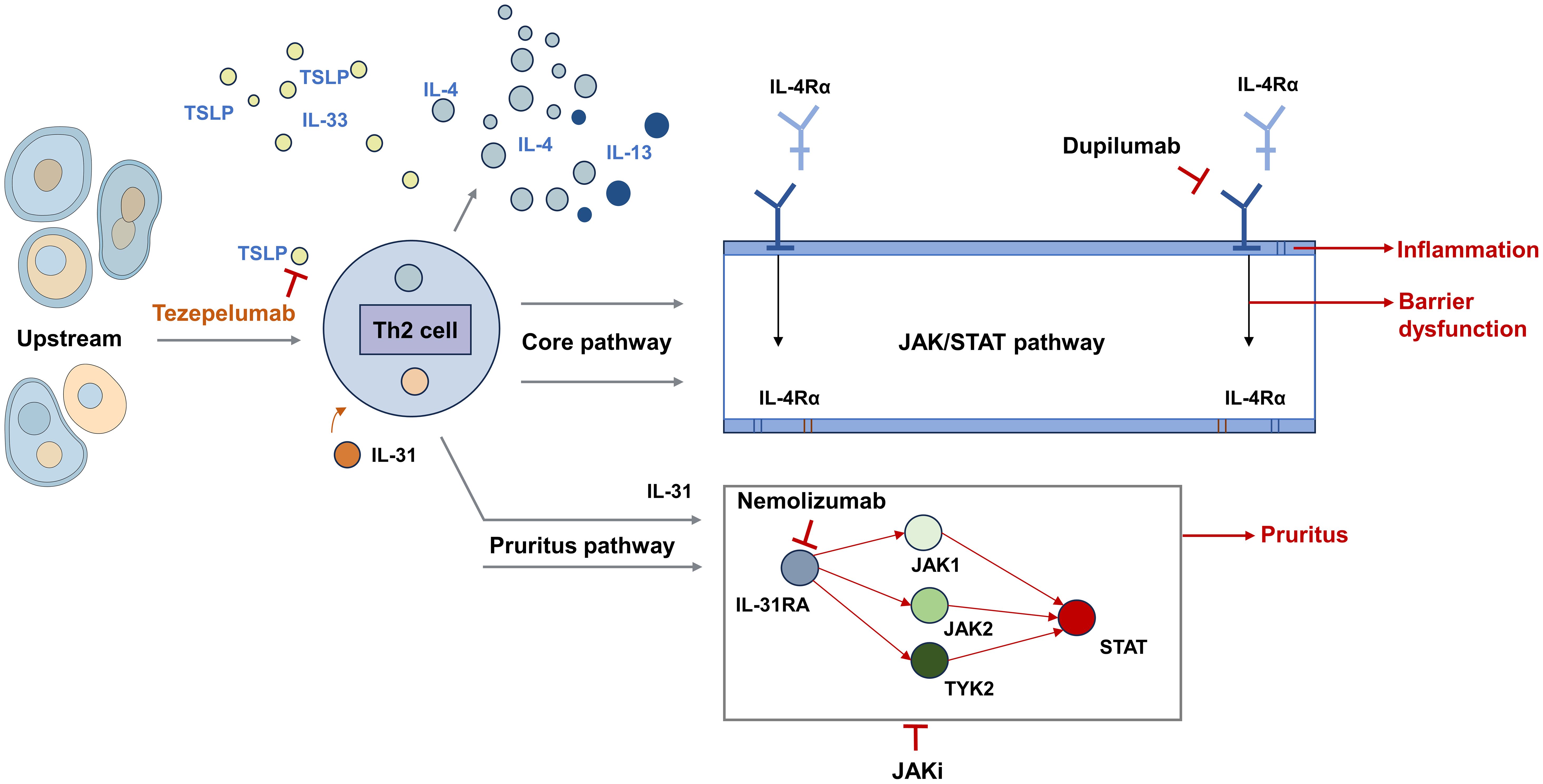
Figure 1. Key pathogenic pathways and therapeutic targets in AD.
Recent years have witnessed a paradigm shift in AD treatment, which has transitioned from nonspecific immunosuppressive to targeted therapies, including both biologic agents and small-molecule inhibitors. These therapies include both biologic agents targeting extracellular cytokines and their receptors, as well as small-molecule inhibitors, particularly JAK inhibitors, that act intracellularly to block multiple cytokine signals simultaneously, providing more effective and safer treatment options for patients with moderate-to-severe disease who do not respond adequately to conventional topical therapies or for whom such treatments are contraindicated (12, 13). While the development of novel topical agents is also a rapidly advancing field, this review will focus primarily on the progress, unmet needs, and future directions of systemic targeted therapies for patients with moderate-to-severe AD.
2 Current targeted therapies for AD: an overview
The current therapeutic landscape of AD has undergone a major transformation with the advent of targeted therapies designed to modulate key immune pathways involved in disease pathogenesis. These therapies primarily include small-molecule JAK inhibitors and monoclonal antibodies targeting specific ILs and their receptors (Table 1) (12, 14).
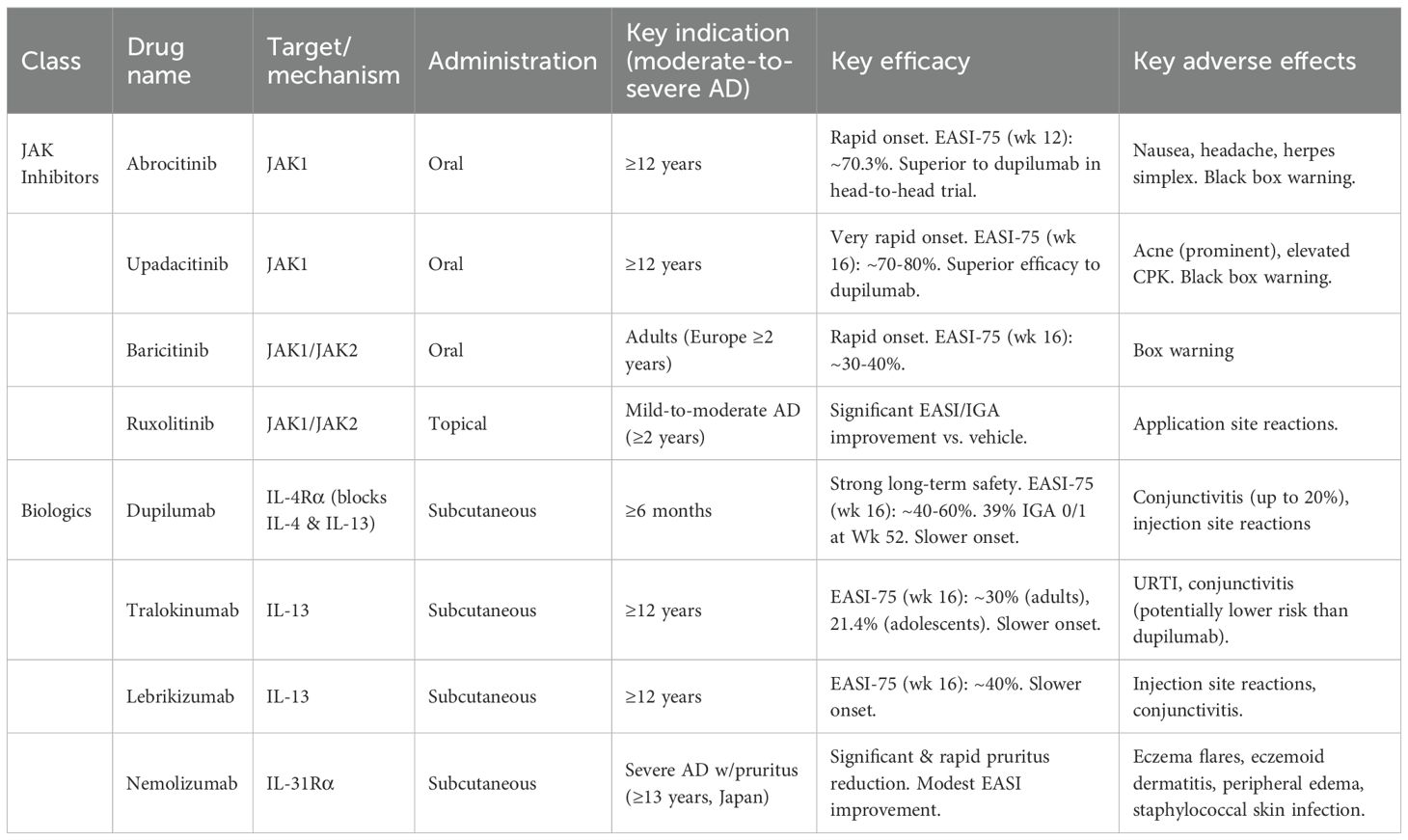
Table 1. Approved targeted therapies for AD.
2.1 JAK inhibitors
JAK inhibitors are a class of small-molecule drugs that have shown significant efficacy in the treatment of moderate-to-severe AD (12). They function by inhibiting the JAK/STAT signaling pathway, which is essential for the signaling of most ILs involved in the progression of AD (15). Four JAK family members, namely, JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2), have been identified and form homodimers and heterodimers to mediate cytokine signaling. By blocking the activity of these kinases, JAK inhibitors can simultaneously interfere with the signaling of multiple proinflammatory cytokines, including IL-4, IL-13, IL-31, IL-17, IL-22, and interferon-gamma, which are involved in AD (16). This broad inhibition helps to modulate the Th2 cell- and Th17-mediated inflammation, epidermal barrier dysfunction, and itch signaling that are characteristics of AD.
The clinical application of JAK inhibitors has revolutionized the treatment of AD by offering effective systemic and topical options. Oral selective JAK1 inhibitors, such as abrocitinib and upadacitinib, provide rapid and profound symptom relief (17). In the JADE DARE head-to-head trial, abrocitinib (200 mg) was superior to dupilumab in achieving a 75% improvement in Eczema Area and Severity Index (EASI-75) response (70.3% vs 58.1%) and itch relief at week 12 (18). Similarly, upadacitinib (30 mg) has shown trends toward superior efficacy compared to dupilumab (12). Furthermore baricitinib, a JAK1/JAK2 inhibitor, has been approved in Europe for use in pediatric patients aged two years and older (19). Additionally, ruxolitinib is approved for patients aged 12 years and older for oral formulations used in the treatment of graft-versus-host disease and for topical use in vitiligo. Recently, the topical formulation (Opzelura) has been approved by the FDA for use in pediatric patients aged 2 years and older for AD, with the caveat that its safety and efficacy have not been established in children under 2 years of age (20, 21). Clinical trials have consistently demonstrated that both oral and topical JAK inhibitors can rapidly ease itching, reduce inflammation, and improve EASI scores (22).
Despite their high efficacy, the primary challenge of JAK inhibitors lies in their safety profile. Common adverse events include nausea, headache (more common with abrocitinib), acne (prominent with upadacitinib), and elevated creatine phosphokinase (CPK) levels (17). More significant concerns relate to the “black box” warnings issued by regulatory agencies for increased risks of serious infections (including herpes zoster), malignancy, major adverse cardiovascular events, and venous thromboembolism (22, 23). However, it is important to contextualize this risk: studies have suggested that the elevated risk for serious adverse events (including major adverse cardiovascular events, malignancy, and venous thromboembolism) is predominantly observed in patients with pre-existing risk factors, such as older age and a history of cardiovascular disease (24). Therefore, the potential for adverse events necessitates a careful consideration of the risk–benefit profile of each patient before initiating treatment with a JAK inhibitor.
2.2 IL-4 and IL-13 pathway inhibitors
IL-4 and IL-13 are key drivers of type 2 inflammation in AD. IL-4 is considered an orchestrator of Th2 cell polarization and immunoglobulin (Ig) E class switching, whereas IL-13 plays a major role in driving inflammation at the tissue level, particularly in the skin. Several targeted therapies have been developed to inhibit signaling by these cytokines, offering effective treatments for moderate-to-severe AD (16).
Dupilumab and stapokibart are two fully human monoclonal antibodies that target IL-4 receptor (IL-4R), thereby blocking the signaling of both IL-4 and IL-13 (25). In contrast, tralokinumab and lebrikizumab selectively inhibit IL-13 signaling, and both drugs have been approved for use in adolescents and adults aged 12 years and above with AD (26, 27). These inhibitors of the IL-4 and/or IL-13 pathways have shown significant efficacy in achieving clearer skin, improving skin barrier function, and reducing the intense itching associated with AD. Their safety profiles are generally favorable, with common adverse reactions being injection site reactions. However, a notable limitation associated specifically with IL-4Rα blockade (dupilumab) is a significantly higher incidence of conjunctivitis, which can affect up to 20% of patients (28). While generally mild to moderate, this conjunctivitis requires monitoring and ophthalmic management (25). Tralokinumab and lebrikizumab also carry a risk of conjunctivitis, though some data suggest it may be less frequent than with dupilumab (26, 29).
As the first biologic agent approved for AD, dupilumab has significantly altered the treatment paradigm for patients whose disease is not adequately controlled with topical therapies (30, 31). By blocking IL-4R, dupilumab effectively inhibits the signaling pathways of both IL-4 and IL-13, two key cytokines that drive type 2 inflammation in AD. This dual blockade leads to a downregulation of type 2 inflammatory gene expression, a reduction in epidermal hyperplasia, and the restoration of skin barrier function (32). Importantly, dupilumab does not act as classical immunosuppressants, thereby avoiding the broad effects on the immune system typically associated with traditional systemic therapies. Extensive clinical trial data have consistently demonstrated the significant efficacy of dupilumab in treating moderate-to-severe AD (33, 34). For example, in the foundational LIBERTY AD CHRONOS trial, 39% of adults receiving dupilumab (300 mg) with topical corticosteroids (TCS) achieved IGA 0/1 (clear or almost clear skin) at week 52, compared to 12% in the placebo + TCS group (28). Importantly, long-term studies have shown that the efficacy and safety of dupilumab can be sustained for up to five years with continuous treatment (30, 31). The newer IL-13 inhibitors also show robust efficacy; tralokinumab, in the ECZTRA 6 trial for adolescents, demonstrated an EASI-75 response of 21.4% (vs 4.3% placebo) at week 16 (29), and lebrikizumab has shown similar results (26). Additionally, treatment with dupilumab has been associated with reductions in the frequency of AD exacerbations and the need for hospitalization, further supporting its role in long-term disease control. Dupilumab has been approved for the treatment of patients with moderate-to-severe AD for more than six months in multiple countries (13). Compared with JAK inhibitors, anti-IL-4Rα therapies may have a slower onset of action but are generally preferred for patients who require a well-characterized long-term safety profile.
2.3 IL-31 receptor antagonists
IL-31 is a cytokine that has been identified as a key player in the induction of pruritus, the hallmark symptom of AD (35). Elevated levels of IL-31 are correlated with the severity of AD and the intensity of itching. Nemolizumab is a humanized monoclonal antibody that acts as an antagonist of the IL-31 receptor, specifically blocking the IL-31 receptor (IL-31R), which forms a heterodimeric complex with the oncostatin M receptor. By targeting IL-31, nemolizumab helps disrupt the itch–scratch cycle that significantly contributes to the exacerbation of AD (36). Apart from its approval in Japan, nemolizumab has now also been approved for the treatment of moderate-to-severe AD in the United Kingdom, the European Union, Switzerland, and the United States (36–40). Clinical trials have demonstrated its efficacy in reducing pruritus and improving overall disease severity, as measured by EASI scores. Reported adverse events associated with nemolizumab include eczema flares, eczemoid dermatitis, peripheral edema, and staphylococcal skin infection, but overall tolerability remains acceptable in most patients (36).
2.4 TSLP inhibitors
TSLP is an epithelial cell-derived cytokine that acts as an upstream initiator of type 2 immune responses by activating dendritic cells, mast cells and Th2 lymphocytes. Moreover, high TSLP expression has been observed in both the skin lesions and serum of patients with AD, indicating that TSLP is a promising therapeutic target (6, 41). Tezepelumab, a human IgG2 monoclonal antibody, inhibits circulating TSLP by blocking its interaction with the TSLP receptor, thus suppressing downstream inflammatory cascades (42). While tezepelumab has shown some efficacy in achieving an EASI-50 response in a phase 2a trial, it did not reach statistical significance for other key disease endpoints (43). Additionally, small-molecule inhibitors of the TSLP receptor are under development as potential topical therapeutic options for AD.
3 Comparative analysis of targeted therapies for AD
With the increasing number of targeted therapies available for AD, comparing their efficacy and safety profiles is crucial to guide treatment decisions and identify optimal strategies for patients with different profiles.
3.1 Contrasting efficacy and safety profiles of biologics and JAK inhibitors
Network meta-analyses have been conducted to compare the efficacy of different biologics and JAK inhibitors in the treatment of AD. These analyses suggest that compared with other therapies, upadacitinib, an oral JAK inhibitor, is often noted for having the fastest onset of action, providing rapid symptom relief, and may present the most favorable response estimates for achieving high levels of skin clearance (EASI-90, EASI-75, and IGA 0/1), but it may be associated with higher rates of adverse events (44). Tralokinumab, an IL-13 inhibitor, may be particularly effective at alleviating pruritus (40), and it is important to highlight nemolizumab, which targets the IL-31 receptor, for its strong and specific efficacy in reducing pruritus, the hallmark symptom of AD. Dupilumab, which targets both IL-4 and IL-13, consistently has better outcomes than the placebo does across various measures of disease severity in pediatric patients (13, 30).
Real-world evidence comparing oral JAK inhibitors and dupilumab in adult patients suggests that while oral JAK inhibitors do not appear to increase the risks of major adverse cardiovascular events, venous thromboembolism, renal events, or malignancies in AD patients, they may be associated with higher risks of skin and subcutaneous tissue infections, herpes infections, and acne than dupilumab (45). Conversely, the use of dupilumab may increase the risk of ophthalmic complications. These comparative data highlight a landscape of crucial therapeutic trade-offs. The “optimal” drug varies depending on the specific outcome prioritized. For example, regarding efficacy, some network meta-analyses suggest oral JAK inhibitors like upadacitinib may provide the highest rates of skin clearance (e.g., EASI-90) (44), whereas other biologics like tralokinumab may be particularly effective for the specific outcome of pruritus relief (40). This variation extends to safety profiles, where a patient and clinician must weigh distinct risks: real-world evidence suggests oral JAK inhibitors may carry higher risks of certain infections (like herpes infections or acne) (45), which must be balanced against the increased risk of ophthalmic complications, such as conjunctivitis, associated with dupilumab (45). Therefore, these findings indicate that while dupilumab remains a highly effective and well-established treatment option (46), the selection of newer JAK inhibitors and other biologics must be tailored to different patient profiles based on their specific symptoms (e.g., predominant itch vs. skin lesions) and tolerance for different safety considerations (46).
3.2 Identifying optimal treatment strategies based on patient profiles
Clinical guidelines for AD management such as the AAD and EuroGuiDerm guidelines strongly recommend biologics and JAK inhibitors as first-line systemic options for moderate-to-severe AD when standard topical therapies have failed (47–49). However, the selection of the most appropriate targeted therapy must be based on a comprehensive assessment of the individual patient’s profile, including efficacy expectations, speed of onset, safety considerations, comorbidities, age, and personal preferences (50). For instance, in patients with severe, highly symptomatic disease requiring rapid control of skin lesions and intense pruritus, oral JAK inhibitors (especially high doses) may be advantageous. A head-to-head clinical trial (Heads Up) demonstrated that upadacitinib (30 mg) was superior to dupilumab for achieving EASI-75 at week 16 (71.0% vs 61.1%) (51), and showed significant advantages in speed of onset, with superior itch improvement as early as week 1 (51) Network meta-analyses also support that high-dose upadacitinib and abrocitinib demonstrate the highest relative efficacy (50, 52). This efficacy advantage, however, must be balanced against their safety profile. JAK inhibitors carry “black box” warnings (21), and have shown higher rates of serious infections, eczema herpeticum, and herpes zoster in clinical trials (51, 53). Therefore, for patients with a history of recurrent herpes infections, high risk of serious infection, cardiovascular risk factors, or a history of malignancy, a biologic with a well-established long-term safety profile (30, 31), such as dupilumab, is often the preferred first-line targeted therapy.
Comorbidities are another critical factor influencing selection. For example, the most common adverse event associated with dupilumab is conjunctivitis (51, 54); thus, for patients with pre-existing severe ocular disease, clinicians may prefer other IL-13 specific inhibitors (e.g., tralokinumab or lebrikizumab) (26, 27) or a JAK inhibitor. Age and patient preferences are also key determinants. Dupilumab is approved for infants (≥6 months) (13), whereas baricitinib is approved for children (≥2 years) in Europe (19), and specific guideline recommendations must be consulted for special populations such as pregnant or breastfeeding women (47). Furthermore, the convenience of oral JAK inhibitors (45, 55) compared to the subcutaneous injections required for biologics (56, 57) is an important factor in shared decision-making. Additionally, real-world data show that a substantial disease burden remains even for patients on the most widely used systemic therapies like dupilumab (58). For these patients with an inadequate response, the primary strategy is often switching treatment [e.g., to a JAK inhibitor (51)]. If the response remains insufficient after switching, combination therapy (59) may then be considered as a subsequent strategy for more refractory cases. Ultimately, a shared decision-making process between the clinician and the patient is crucial for determining the optimal treatment approach that balances efficacy, safety, and patient preferences.
4 Unmet medical needs in the management of AD
Despite the significant advancements in AD treatment with targeted therapies, several unmet medical needs persist, and further research and development are needed to optimize patient outcomes and quality of life.
4.1 Pruritus management
Chronic pruritus is a hallmark symptom of AD and is a major contributor to the disease burden and reduced quality of life (60). While targeted therapies often lead to itch reduction, many patients continue to experience persistent or inadequately controlled pruritus. The complex pathophysiology of AD-related itch, involving skin barrier dysfunction, immune dysregulation, and nerve sensitization, makes targeted treatment with single-mechanism therapies challenging. An urgent need exists for highly effective and targeted antipruritic therapies with minimal side effects. Future directions should include mechanistically targeted agents (e.g., neuroimmune modulators) and combination strategies to disrupt the itch–scratch cycle more effectively (16).
4.2 Disease control and remission
While current systemic targeted therapies significantly improve symptoms in many patients with moderate-to-severe AD, a substantial proportion (approximately 40–60%) do not achieve adequate disease control (22, 33). Furthermore, 30% of patients fail to reach optimal treatment goals, such as complete or near-complete skin clearance (IGA 0/1) or EASI-90 (61).
A critical distinction must be made between clinical control and true disease remission. Current trial endpoints, such as EASI-75 or IGA 0/1 (51, 62), represent successful disease suppression while the patient is on active therapy. However, a more profound unmet need is the induction of deep and therapy-free remission (TFR)—a state where disease control is maintained long-term even after the treatment— is discontinued (63).
Achieving TFR is exceptionally challenging because AD is a chronic disease with deep-seated immunological and structural persistence. The primary barrier to TFR is the establishment of a “disease memory” within the skin. Groundbreaking research has shown that even after long-term treatment with IL-4Rα blockade (dupilumab) and apparent clinical resolution, pathogenic immune cell populations persist in the resolved skin. These include mature dendritic cells and specialized T helper cells (e.g., TH2A cells) which are absent in healthy controls (64). These lingering cells, along with Staphylococcus aureus-specific tissue-resident memory T cells (65), remain primed to reactivate the inflammatory cascade, explaining why disease recurrence upon treatment cessation is so common (64).
This persistent immune memory explains why most current treatments, including biologics and JAK inhibitors, function as highly effective “disease-suppressing” rather than “disease-modifying” agents (63). Patients often require long-term, even lifelong, treatment to maintain control, and symptoms frequently recur upon cessation of therapy (16). Therefore, the development of true disease-modifying therapies that can erase this immune memory, promote immune tolerance, and induce sustained TFR remains one of the most critical unmet needs in AD management (16, 63).
Most current treatments focus on disease suppression rather than the induction of sustained remission. Patients often require long-term, even lifelong treatment, and symptoms frequently recur upon the cessation of therapy. Disease-modifying therapies that not only control symptoms but also alter the natural course of AD, promote immune tolerance, and induce sustained remission or even a functional cure are critically needed (16).
4.3 Needs of specific populations
Treatments for AD must be tailored to the unique needs of specific populations. Although dupilumab has extended therapeutic options for children as young as six months, many targeted agents remain unapproved or understudied in pediatric populations, particularly infants and toddlers (13). Moreover, disparities in clinical manifestation, genetic predisposition, and treatment response across racial and ethnic groups are being increasingly recognized. However, most clinical trials underrepresent nonwhite populations, limiting the generalizability of the findings (17). Addressing these gaps requires the intentional inclusion of diverse populations in clinical research and the development of culturally and biologically tailored therapeutic strategies.
4.4 Therapeutic inertia
Therapeutic inertia—the delay or failure to escalate treatment when therapeutic goals are not met—is a prevalent obstacle in real-world AD management. Despite the availability of effective targeted therapies, clinicians may hesitate to adjust treatment plans because of concerns about adverse effects, a lack of confidence in newer agents, or the absence of clear escalation protocols (66). This delay in appropriate intervention often results in prolonged patient suffering, poor disease control, and reduced quality of life. Addressing therapeutic inertia will require improved education, updated clinical guidelines, and decision-support tools to facilitate timely treatment optimization.
4.5 Cost and accessibility
The high cost of targeted therapies often restricts their accessibility to a broader patient population. Biologic agents and JAK inhibitors remain unaffordable for many patients, particularly in low-resource settings or where insurance coverage is limited. This substantial financial burden may lead to treatment discontinuation or nonadherence, undermining long-term outcomes. Efforts to improve accessibility should include the development of cost-effective therapeutic alternatives, the expansion of biosimilar markets, and policy-level interventions to reduce the economic burden on patients and healthcare systems (55).
4.6 Unmet needs in patient-centered care
Despite the increasing clinical understanding of AD pathophysiology and treatment options, patient-centered approaches for AD management remain insufficiently addressed (59). Treatment decisions often prioritize clinical signs and investigator assessments while underemphasizing patient-reported outcomes (PROs), such as itch severity, sleep disruption, fatigue, and emotional distress. Integrating PROs into clinical practice and research is essential for aligning therapeutic goals with patients’ lived experiences. Additionally, real-world evidence (RWE) derived from observational data and routine practice complements findings from randomized clinical trials (RCTs), providing insights into treatment effectiveness, safety, and adherence in diverse patient populations (67). We urge researchers to prioritize the collection and analysis of PROs as primary or secondary endpoints in clinical trials to better address the needs of AD patients. Furthermore, we advocate for the establishment of AD patient registries to collect longitudinal clinical data, including PROs and RWE, to improve our understanding of the natural course of AD, the long-term effects and safety of different treatments, and patterns of disease recurrence. Drawing inspiration from established registries for diseases such as psoriasis, AD registries could provide valuable data to enhance patient care, guide clinical research, and inform the development of more effective treatment strategies (68).
5 Future directions in AD therapeutics
The therapeutic landscape of AD is rapidly evolving, driven by ongoing research focused on addressing unmet needs and further improving treatment outcomes. Several promising future directions are currently being explored (Table 2).
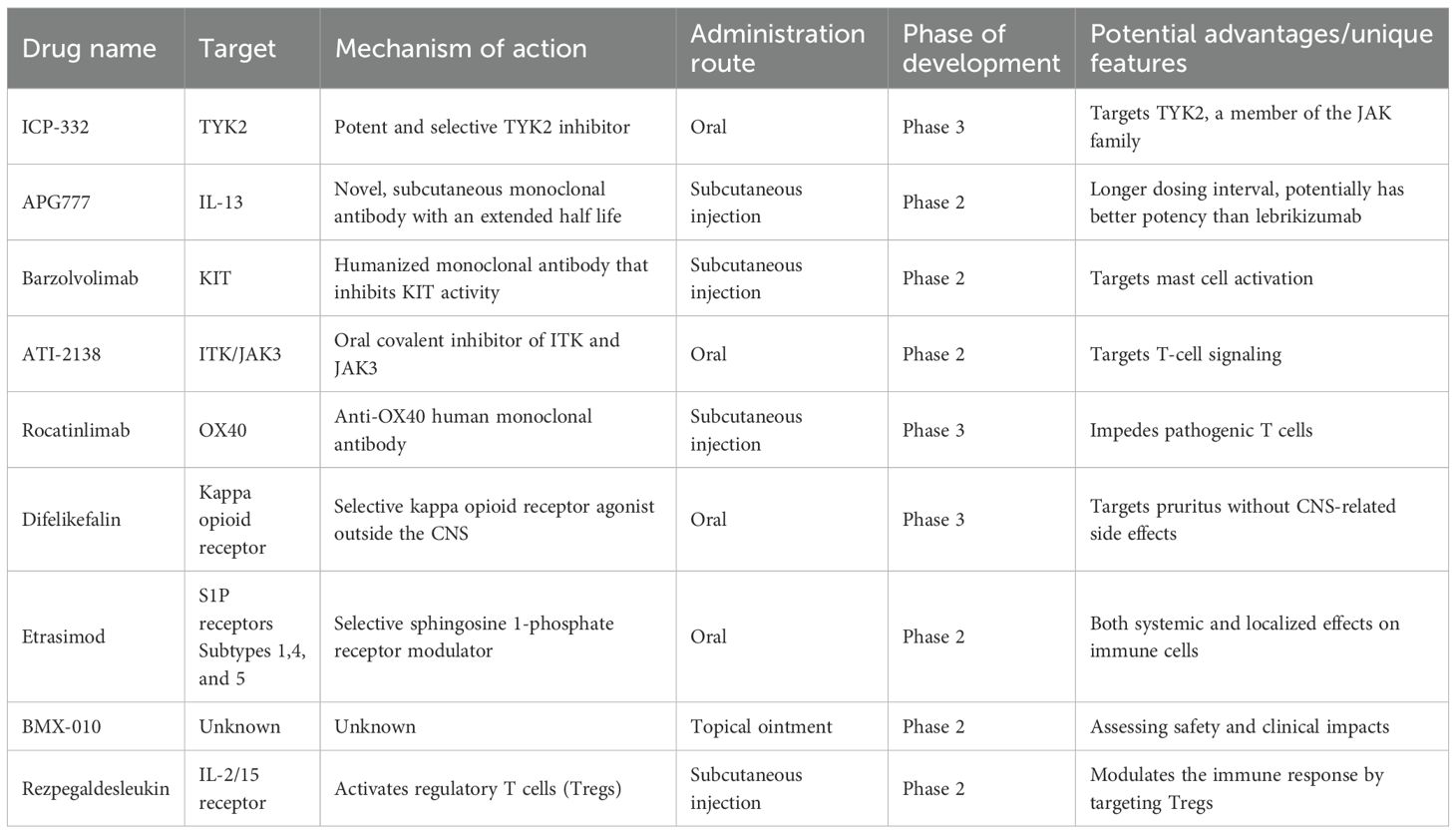
Table 2. Key investigational targeted therapies for AD in late-stage clinical trials.
5.1 Development of dual-target and multitarget agents
One exciting avenue of research is the development of dual-target and multitarget agents, particularly bispecific antibodies that can simultaneously target multiple pathogenic pathways. For example, GB12–09 is a bispecific antibody targeting both IL-4Rα and IL-31Rα (69), whereas NM26–2198 targets IL-4Rα and IL-31, effectively modulating both type 2 inflammation and pruritus (70). These approaches may increase clinical efficacy by overcoming the limitations of single-cytokine blockade, particularly in patients with heterogeneous inflammatory profiles or partial responses to existing monotherapies. Dual or multicytokine blockade may also reduce the likelihood of inflammatory pathway compensation, potentially achieving more sustained disease control.
5.2 Exploring longer-acting formulations for improved patient convenience and adherence
Frequent dosing remains a significant barrier to long-term adherence in patients with chronic diseases such as AD. Accordingly, the development of longer-acting formulations of targeted therapies is a key area of innovation. One such agent, APG777, a novel half-life-extended IL-13 monoclonal antibody that is currently in phase 2 clinical trials for AD, has a prolonged half-life of up to 77 days (71). The development of such longer-acting formulations may significantly improve treatment adherence and patient satisfaction by reducing the injection frequency and minimizing the healthcare burden. These formulations are particularly beneficial in pediatric populations and in patients requiring maintenance therapy over extended periods.
5.3 Advancements in convenient administration routes
The availability of convenient administration routes is crucial for patient comfort and adherence. While subcutaneous injections are the primary route for most approved biologic therapies, such as dupilumab, stapokibart, tralokinumab, and lebrikizumab, oral JAK inhibitors, such as abrocitinib, upadacitinib, and baricitinib, offer a more convenient oral route of administration. Ongoing research has focused on exploring oral formulations for other targeted therapies as well. For instance, difelikefalin, an oral kappa-opioid receptor agonist, is in phase 3 clinical trials for the treatment of pruritus in patients with AD (72). Similarly, etrasimod, an oral sphingosine 1-phosphate receptor modulator, is undergoing a phase 2 trial for AD (73). The availability of both subcutaneous and oral options provides greater flexibility in treatment selection, allowing clinicians to tailor the route of administration to individual patient preferences and needs, potentially improving treatment adherence and overall satisfaction.
5.4 Identification and validation of novel therapeutic targets
Continuous research efforts are focused on identifying and validating novel therapeutic targets involved in the pathogenesis of AD, including exploring targets beyond the canonical type 2 cytokines. For instance, the OX40/OX40 ligand (OX40L) interaction, filaggrin replacement, and modulation of the skin microbiome are areas of active investigation (74). Several therapies targeting other cytokines and receptors, such as IL-22 (e.g., fezakinumab), IL-33, and the components of the IL-23/IL-17 axis, as well as oncostatin M β, are under investigation (75). The drug development pipeline for AD is robust, with numerous investigational drugs targeting various mechanisms of action currently being studied in different phases of clinical trials. These drugs include TYK2 inhibitors (e.g., ICP-332) (76) and ITK/JAK3 inhibitors (e.g., ATI-2138) (56, 57). Additionally, novel approaches such as rezpegaldesleukin, which aims to activate regulatory T cells to suppress inflammation, are being explored (77). The identification and validation of these novel therapeutic targets hold significant promise for the development of new treatments that can address the limitations of current therapies, potentially leading to more effective and personalized approaches for managing AD.
5.5 Advancing precision medicine and personalized therapies
A major paradigm shift anticipated in the future of AD management is the move towards precision medicine, transitioning away from the current largely “trial-and-error” approach to selecting systemic therapies (78, 79). AD is increasingly recognized not as a single entity but as a complex syndrome with significant heterogeneity in clinical presentation and underlying molecular mechanisms, referred to as endotypes (80, 81). This heterogeneity explains why patient responses to specific targeted therapies can vary considerably (78).
The development and validation of reliable biomarkers are crucial for realizing the potential of precision medicine in AD (11, 82). Currently, the selection between therapies like IL-4/IL-13 pathway inhibitors (e.g., dupilumab) and JAK inhibitors often relies on clinical factors and shared decision-making, rather than objective biological predictors (78). Future research is intensively focused on identifying predictive biomarkers that can guide therapeutic choices.
Serum biomarkers: Measuring levels of specific cytokines (e.g., IL-13, IL-22, TSLP), chemokines (e.g., CCL17/TARC), or cellular components like eosinophils in peripheral blood holds promise for stratifying patients (83). For example, higher baseline levels of Th2-related markers might predict a better response to IL-4/IL-13 blockade, whereas elevated Th17/Th22 markers could suggest potential benefit from broader-acting JAK inhibitors (80).
Skin transcriptomics and other omics: Analyzing the gene expression profile (transcriptome) directly from skin biopsies allows for a deeper understanding of the patient’s specific inflammatory signature (84). Distinguishing between a predominantly Th2-driven endotype versus a mixed phenotype involving significant Th1, Th17, or Th22 pathway activation could become key for selecting the most appropriate targeted agent (80, 81). Integration with other omics data (epigenomics, proteomics, metabolomics) may further refine these endotypes (84).
Recognizing distinct AD endotypes is fundamental to this personalized approach. Significant differences have been observed across populations. For instance, the “Asian AD phenotype” often exhibits a stronger Th17/Th22 signature compared to the typically Th2-dominant profile seen in European-American patients (13, 85). Other proposed endotypes differentiate based on IgE levels (extrinsic vs. intrinsic AD) or filaggrin mutation status (80, 85). Such distinctions imply that future treatment algorithms may need to be tailored; for example, strongly Th2-skewed patients might benefit most from IL-4/IL-13 pathway inhibitors, while those with mixed inflammatory profiles might respond better to JAK inhibitors or potentially therapies targeting IL-17 or IL-22 (75, 80).
Ultimately, precision medicine aims to transform the AD treatment paradigm from the conventional “step-care” approach (where treatments are escalated based on failure) to a biomarker-guided, personalized strategy (78, 86) By leveraging individual patients’ biological profiles, clinicians could select the most effective first-line targeted therapy, improving outcomes, minimizing exposure to ineffective treatments, and optimizing resource utilization (79, 87).
6 Clinical guidelines and expert consensus on AD treatment
Clinical practice guidelines and expert consensus statements play vital roles in providing clinicians with evidence-based recommendations for the management of AD, including the use of targeted therapies.
6.1 Current recommendations for the use of targeted therapies
The American Academy of Dermatology (AAD) guidelines strongly recommend the use of dupilumab, tralokinumab, abrocitinib, baricitinib, and upadacitinib for the treatment of AD (33). These guidelines reflect the growing body of evidence supporting the efficacy and safety of these targeted agents. Similarly, European guidelines also incorporate dupilumab and other targeted therapies into their recommendations. Expert consensus statements emphasize the increasing importance of biological therapies in the management of pediatric patients with moderate-to-severe AD. A general consensus exists that systemic therapy, including targeted agents, should be considered for patients with moderate-to-severe AD when optimized topical therapy has proven inadequate for controlling the disease (88). These guidelines and consensus statements provide a valuable framework for clinicians in making informed decisions about when and how to incorporate targeted therapies into their treatment algorithms for AD.
6.2 Emerging trends and future research priorities highlighted by experts
Experts in the field advocate for setting higher treatment goals in AD management, such as achieving EASI-90 (90% improvement in skin clearance) and a numeric rating scale (NRS) score of 0 or 1 for itch, indicating near-clear skin and minimal to no itch (34). The need to overcome therapeutic inertia by proactively adjusting treatment strategies when patients are not meeting these optimal targets has also been emphasized. Future research priorities include the continued development of disease-modifying therapies that can potentially alter the long-term course of AD, as well as investigating recurrence rates upon the cessation of current treatments. These emerging trends and research priorities underscore the ongoing commitment to further optimize AD management and improve the long-term outcomes of patients.
7 Conclusions
Targeted therapies have ushered in a new era in the treatment of AD, offering significant advancements in efficacy and safety, particularly for patients with moderate-to-severe disease. However, despite these remarkable achievements, critical unmet needs persist. A substantial proportion of patients continue to experience inadequate responses to current treatments or unstable disease control. Moreover, the potential for side effects, although generally less severe than traditional immunosuppressants, remains a concern. An inadequate response to existing therapies, residual pruritus, and treatment-limiting side effects underscore the need for improved therapeutic options. Furthermore, therapeutic options for children, especially infants, and for individuals with mild AD are still relatively limited. The persistent burden of pruritus also highlights the need for more targeted antipruritic therapies.
The future of AD therapeutics holds immense promise. The development of dual and multitarget agents, longer-acting formulations, and convenient administration routes are poised to further increase treatment efficacy and support patient convenience. The ongoing identification and validation of novel therapeutic targets have the potential to address the limitations of current therapies and provide new avenues for intervention. The increasing integration of patient-reported outcomes into clinical assessments is crucial for a more holistic evaluation of treatment success, and the growing emphasis on personalized medicine will allow therapeutic strategies to be tailored individual patient profiles and disease endotypes. As researchers continue to elucidate the complex pathogenesis of AD, the field is on the cusp of further breakthroughs that will undoubtedly improve the lives of individuals living with this chronic and often debilitating condition.
Author contributions
LZ: Conceptualization, Writing – original draft. GP: Conceptualization, Writing – original draft. MW: Writing – review & editing, Conceptualization. FN: Conceptualization, Writing – review & editing. XG: Conceptualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was funded by National Key R&D Program of China (2023YFC2508200). Medical writing was supported by Dr. Paul Zhang of MedSci and was funded by Sanofi.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Savva M, Papadopoulos NG, Gregoriou S, Katsarou S, Papapostolou N, Makris M, et al. Recent advancements in the atopic dermatitis mechanism. Front Biosci (Landmark Ed). (2024) 29:84. doi: 10.31083/j.fbl2902084
2. Caffarelli C, Giannetti A, Giannì G, and Ricci G. Anti-inflammatory and biologic drugs for atopic dermatitis: a therapeutic approach in children and adolescents. Front Med (Lausanne). (2023) 10:1214963. doi: 10.3389/fmed.2023.1214963
3. Yamamura Y, Nakashima C, and Otsuka A. Interplay of cytokines in the pathophysiology of atopic dermatitis: insights from Murin models and human. Front Med (Lausanne). (2024) 11:1342176. doi: 10.3389/fmed.2024.1342176
4. Wang J, Zhou Y, Zhang H, Hu L, Liu J, Wang L, et al. Pathogenesis of allergic diseases and implications for therapeutic interventions. Signal Transduct Target Ther. (2023) 8:138. doi: 10.1038/s41392-023-01344-4
5. Pappa G, Sgouros D, Theodoropoulos K, Kanelleas A, Bozi E, Gregoriou S, et al. The IL-4/-13 axis and its blocking in the treatment of atopic dermatitis. J Clin Med. (2022) 11(19):5633. doi: 10.3390/jcm11195633
6. Luo J, Zhu Z, Zhai Y, Zeng J, Li L, Wang D, et al. The role of TSLP in atopic dermatitis: from pathogenetic molecule to therapeutical target. Mediators Inflammation. (2023) 2023:7697699. doi: 10.1155/2023/7697699
7. Adhikary PP, Idowu T, Tan Z, Hoang C, Shanta S, Dumbani M, et al. Disrupting TSLP-TSLP receptor interactions via putative small molecule inhibitors yields a novel and efficient treatment option for atopic diseases. EMBO Mol Med. (2024) 16:1630–56. doi: 10.1038/s44321-024-00085-3
8. Chiricozzi A, Maurelli M, Peris K, and Girolomoni G. Targeting IL-4 for the treatment of atopic dermatitis. Immunotargets Ther. (2020) 9:151–6. doi: 10.2147/ITT.S260370
9. Orfali RL and Aoki V. Blockage of the IL-31 pathway as a potential target therapy for atopic dermatitis. Pharmaceutics. (2023) 15:577. doi: 10.3390/pharmaceutics15020577
10. Guttman-Yassky E, Irvine AD, Brunner PM, Kim BS, Boguniewicz M, Parmentier J, et al. The role of Janus kinase signaling in the pathology of atopic dermatitis. J Allergy Clin Immunol. (2023) 152:1394–404. doi: 10.1016/j.jaci.2023.07.010
11. Schuler C, Billi AC, Maverakis E, Tsoi LC, and Gudjonsson JE. Novel insights into atopic dermatitis. J Allergy Clin Immunol. (2023) 151:1145–54. doi: 10.1016/j.jaci.2022.10.023
12. Zhang L, Xu J, Gu C, Zheng M, Pan M, Li L, et al. Efficacy and safety of upadacitinib through 140 weeks in Chinese adult and adolescent patients with moderate-to-severe atopic dermatitis: Post hoc analysis of the phase 3 Measure Up 1 and AD Up clinical trials. Chin Med J (Engl). (2025) 138:1633–4. doi: 10.1097/cm9.0000000000003595
13. Wang M, Gao XH, and Zhang L. A review of dupilumab in the treatment of atopic dermatitis in infants and children. Drug Des Devel Ther. (2024) 18:941–51. doi: 10.2147/dddt.S457761
14. Yoon S, Kim K, Shin K, Kim HS, Kim B, Kim MB, et al. The safety of systemic Janus kinase inhibitors in atopic dermatitis: A systematic review and meta-analysis of randomized controlled trials. J Eur Acad Dermatol Venereol. (2024) 38:52–61. doi: 10.1111/jdv.19426
15. Huang IH, Chung WH, Wu PC, and Chen CB. JAK-STAT signaling pathway in the pathogenesis of atopic dermatitis: An updated review. Front Immunol. (2022) 13:1068260. doi: 10.3389/fimmu.2022.1068260
16. Alska E, Łaszczych D, Napiórkowska-Baran K, Szymczak B, Rajewska A, Rubisz AE, et al. Advances in biologic therapies for allergic diseases: current trends, emerging agents, and future perspectives. J Clin Med. (2025) 14:1079. doi: 10.3390/jcm14041079
17. Wang M, Gao X, and Zhang L. Efficacy and safety of Janus kinase selective inhibitors in the treatment of atopic dermatitis: A systematic review and meta-analysis. Allergy Asthma Proc. (2025) 46:88–97. doi: 10.2500/aap.2025.46.240113
18. Das S, Vishakha K, Banerjee S, Nag D, and Ganguli A. Tetracycline-loaded magnesium oxide nanoparticles with a potential bactericidal action against multidrug-resistant bacteria: In vitro and in vivo evidence. Colloids Surf B Biointerf. (2022) 217:112688. doi: 10.1016/j.colsurfb.2022.112688
19. David E, Ungar B, Renert-Yuval Y, Facheris P, Del Duca E, and Guttman-Yassky E. The evolving landscape of biologic therapies for atopic dermatitis: Present and future perspective. Clin Exp Allergy. (2023) 53:156–72. doi: 10.1111/cea.14263
20. Hoy SM. Ruxolitinib cream 1.5%: A review in mild to moderate atopic dermatitis. Am J Clin Dermatol. (2023) 24:143–51. doi: 10.1007/s40257-022-00748-2
21. Incyte. Incyte announces additional FDA approval of opzelura (Ruxolitinib) cream in children ages 2–11 with atopic dermatitis®(2025). Available online at: https://www.businesswire.com/news/home/20250918551027/en/Incyte-Announces-Additional-FDA-Approval-of-Opzelura-Ruxolitinib-Cream-in-Children-Ages-2-11-with-Atopic-Dermatitis.
22. Eichenfield LF, Simpson EL, Papp K, Szepietowski JC, Blauvelt A, Kircik L, et al. Efficacy, safety, and long-term disease control of ruxolitinib cream among adolescents with atopic dermatitis: pooled results from two randomized phase 3 studies. Am J Clin Dermatol. (2024) 25:669–83. doi: 10.1007/s40257-024-00855-2
23. Schlosser AR, Nijman L, Schappin R, Nijsten TEC, and Hijnen D. Long-term outcomes of new systemic agents in atopic dermatitis: drug survival analyses and treatment patterns in daily practice. Acta Derm Venereol. (2025) 105:adv41504. doi: 10.2340/actadv.v105.41504
24. Samuel C, Cornman H, Kambala A, and Kwatra SG. A review on the safety of using JAK inhibitors in dermatology: clinical and laboratory monitoring. Dermatol Ther (Heidelb). (2023) 13:729–49. doi: 10.1007/s13555-023-00892-5
25. Thibodeaux Q, Smith MP, Ly K, Beck K, Liao W, and Bhutani T. A review of dupilumab in the treatment of atopic diseases. Hum Vaccin Immunother. (2019) 15:2129–39. doi: 10.1080/21645515.2019.1582403
26. Stingeni L, Ferrucci S, Amerio P, Foti C, Patruno C, and Girolomoni G. Lebrikizumab: a new anti-IL-13 agent for treating moderate-to-severe atopic dermatitis. Expert Opin Biol Ther. (2025) 25:15–20. doi: 10.1080/14712598.2024.2435427
27. Paller AS, Flohr C, Cork M, Bewley A, Blauvelt A, Hong HC, et al. Efficacy and safety of tralokinumab in adolescents with moderate to severe atopic dermatitis: the phase 3 ECZTRA 6 randomized clinical trial. JAMA Dermatol. (2023) 159:596–605. doi: 10.1001/jamadermatol.2023.0627
28. Sanfilippo F, Johnson C, Bellavia D, Morsolini M, Romano G, Santonocito C, et al. Mitral regurgitation grading in the operating room: A systematic review and meta-analysis comparing preoperative and intraoperative assessments during cardiac surgery. J Cardiothorac Vasc Anesth. (2017) 31:1681–91. doi: 10.1053/j.jvca.2017.02.046
29. Kim HG and Hong S. Influence of land cover, point source pollution, and granularity on the distribution of metals, metalloids, and organic matter in the river and stream sediments in the Republic of Korea. Environ Sci pollut Res Int. (2023) 30:65129–40. doi: 10.1007/s11356-023-27080-4
30. Seegräber M, Srour J, Walter A, Knop M, and Wollenberg A. Dupilumab for treatment of atopic dermatitis. Expert Rev Clin Pharmacol. (2018) 11:467–74. doi: 10.1080/17512433.2018.1449642
31. Senner S, Seegräber M, Frey S, Kendziora B, Eicher L, and Wollenberg A. Dupilumab for the treatment of adolescents with atopic dermatitis. Expert Rev Clin Immunol. (2020) 16:641–50. doi: 10.1080/1744666x.2020.1801420
32. Berni Canani R, Caminati M, Carucci L, and Eguiluz-Gracia I. Skin, gut, and lung barrier: Physiological interface and target of intervention for preventing and treating allergic diseases. Allergy. (2024) 79:1485–500. doi: 10.1111/all.16092
33. Blauvelt A, de Bruin-Weller M, Gooderham M, Cather JC, Weisman J, Pariser D, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet. (2017) 389:2287–303. doi: 10.1016/s0140-6736(17)31191-1
34. Reich K, Thyssen JP, Blauvelt A, Eyerich K, Soong W, Rice ZP, et al. Efficacy and safety of abrocitinib versus dupilumab in adults with moderate-to-severe atopic dermatitis: a randomised, double-blind, multicentre phase 3 trial. Lancet. (2022) 400:273–82. doi: 10.1016/s0140-6736(22)01199-0
35. Akhtar S, Ahmad F, Alam M, Ansari AW, Uddin S, Steinhoff M, et al. Interleukin-31: the inflammatory cytokine connecting pruritus and cancer. Front Biosci (Landmark Ed). (2024) 29:312. doi: 10.31083/j.fbl2909312
36. Kwatra SG, Yosipovitch G, Legat FJ, Reich A, Paul C, Simon D, et al. Phase 3 trial of nemolizumab in patients with prurigo nodularis. N Engl J Med. (2023) 389:1579–89. doi: 10.1056/NEJMoa2301333
37. National Eczema Association. Breaking news: FDA approves two new treatments for atopic dermatitis: biologic nemluvio and topical cream vtama(2025). Available online at: https://nationaleczema.org/blog/breaking-news-fda-approves-two-new-treatments-for-atopic-dermatitis-biologic-nemluvio-and-topical-cream-vtama/ (Accessed October 28, 2025).
38. Galderma. Nemluvio® (nemolizumab) approved in the European Union for moderate-to-severe atopic dermatitis and prurigo nodularis Zug, Switzerland(2025). Available online at: https://www.medthority.com/news/2025/2/european-commission-approves-nemluvio-nemolizumab–to-treat–moderate-to-severe-atopic-dermatitis-and-prurigo-nodularis.–galderma:~:text=Nemluvio%20is%20now%20approved%20for%20subcutaneous%20use%20for,prurigo%20nodularis%20who%20are%20candidates%20for%20systemic%20therapy (Accessed October 28, 2025).
39. Medicines and Healthcare products Regulatory Agency. Nemolizumab approved to treat prurigo nodularis and atopic dermatitis (eczema) for patients in the UK(2025). Available online at: https://www.gov.uk/government/news/nemolizumab-approved-to-treat-prurigo-nodularis-and-atopic-dermatitis-eczema-for-patients-in-the-uk (Accessed October 28, 2025).
40. Duggan S. Tralokinumab: first approval. Drugs. (2021) 81:1657–63. doi: 10.1007/s40265-021-01583-1
41. Tatsuno K, Fujiyama T, Yamaguchi H, Waki M, and Tokura Y. TSLP directly interacts with skin-homing th2 cells highly expressing its receptor to enhance IL-4 production in atopic dermatitis. J Invest Dermatol. (2015) 135:3017–24. doi: 10.1038/jid.2015.318
42. Matera MG, Rogliani P, Calzetta L, and Cazzola M. TSLP inhibitors for asthma: current status and future prospects. Drugs. (2020) 80:449–58. doi: 10.1007/s40265-020-01273-4
43. Simpson EL, Parnes JR, She D, Crouch S, Rees W, Mo M, et al. Tezepelumab, an anti-thymic stromal lymphopoietin monoclonal antibody, in the treatment of moderate to severe atopic dermatitis: A randomized phase 2a clinical trial. J Am Acad Dermatol. (2019) 80:1013–21. doi: 10.1016/j.jaad.2018.11.059
44. Lax SJ, Van Vogt E, Candy B, Steele L, Reynolds C, Stuart B, et al. Topical anti-inflammatory treatments for eczema: network meta-analysis. Cochrane Database Syst Rev. (2024) 8:Cd015064. doi: 10.1002/14651858.CD015064.pub2
45. Chu AWL, Wong MM, Rayner DG, Guyatt GH, Díaz Martinez JP, Ceccacci R, et al. Systemic treatments for atopic dermatitis (eczema): Systematic review and network meta-analysis of randomized trials. J Allergy Clin Immunol. (2023) 152:1470–92. doi: 10.1016/j.jaci.2023.08.029
46. Manzar D, Suntres E, Nair N, Patel Y, and Abu-Hilal M. Elevation of creatine phosphokinase in moderate-to-severe atopic dermatitis is associated with the use of JAK inhibitors but not dupilumab: A systematic review and meta-analysis. J Am Acad Dermatol. (2024) 91:168–9. doi: 10.1016/j.jaad.2024.03.027
47. Wollenberg A, Kinberger M, Arents B, Aszodi N, Avila Valle G, Barbarot S, et al. European guideline (EuroGuiDerm) on atopic eczema - part II: non-systemic treatments and treatment recommendations for special AE patient populations. J Eur Acad Dermatol Venereol. (2022) 36:1904–26. doi: 10.1111/jdv.18429
48. Davis DMR, Drucker AM, Alikhan A, Bercovitch L, Cohen DE, Darr JM, et al. Guidelines of care for the management of atopic dermatitis in adults with phototherapy and systemic therapies. J Am Acad Dermatol. (2024) 90:e43–56. doi: 10.1016/j.jaad.2023.08.102
49. Wollenberg A, Kinberger M, Arents B, Aszodi N, Avila Valle G, Barbarot S, et al. European guideline (EuroGuiDerm) on atopic eczema: part I - systemic therapy. J Eur Acad Dermatol Venereol. (2022) 36:1409–31. doi: 10.1111/jdv.18345
50. Drucker AM, Lam M, Prieto-Merino D, Malek R, Ellis AG, Yiu ZZN, et al. Systemic immunomodulatory treatments for atopic dermatitis: living systematic review and network meta-analysis update. JAMA Dermatol. (2024) 160:936–44. doi: 10.1001/jamadermatol.2024.2192
51. Blauvelt A, Teixeira HD, Simpson EL, Costanzo A, De Bruin-Weller M, Barbarot S, et al. Efficacy and safety of upadacitinib vs dupilumab in adults with moderate-to-severe atopic dermatitis: A randomized clinical trial. JAMA Dermatol. (2021) 157:1047–55. doi: 10.1001/jamadermatol.2021.3023
52. Drucker AM, Morra DE, Prieto-Merino D, Ellis AG, Yiu ZZN, Rochwerg B, et al. Systemic immunomodulatory treatments for atopic dermatitis: update of a living systematic review and network meta-analysis. JAMA Dermatol. (2022) 158:523–32. doi: 10.1001/jamadermatol.2022.0455
53. Chovatiya R and Paller AS. JAK inhibitors in the treatment of atopic dermatitis. J Allergy Clin Immunol. (2021) 148:927–40. doi: 10.1016/j.jaci.2021.08.009
54. Halling AS, Loft N, Silverberg JI, Guttman-Yassky E, and Thyssen JP. Real-world evidence of dupilumab efficacy and risk of adverse events: A systematic review and meta-analysis. J Am Acad Dermatol. (2021) 84:139–47. doi: 10.1016/j.jaad.2020.08.051
55. Langan SM, Irvine AD, and Weidinger S. Atopic dermatitis. Lancet. (2020) 396:345–60. doi: 10.1016/s0140-6736(20)31286-1
56. Kaul A, Hope H, Xu C, Basavalingappa R, Binz SK, Boily C, et al. Characterization of the dual ITK/JAK3 small molecule covalent inhibitor ATI-2138. J Pharmacol Exp Ther. (2025) 392:100054. doi: 10.1016/j.jpet.2024.100054
57. Silverberg JI, Eichenfield LF, Hebert AA, Simpson EL, Stein Gold L, Bissonnette R, et al. Tapinarof cream 1% once daily: Significant efficacy in the treatment of moderate to severe atopic dermatitis in adults and children down to 2 years of age in the pivotal phase 3 ADORING trials. J Am Acad Dermatol. (2024) 91:457–65. doi: 10.1016/j.jaad.2024.05.023
58. Eyerich K, Gooderham MJ, Silvestre JF, Shumack SP, Mendes-Bastos P, Aoki V, et al. Real-world clinical, psychosocial and economic burden of atopic dermatitis: Results from a multicountry study. J Eur Acad Dermatol Venereol. (2024) 38:340–53. doi: 10.1111/jdv.19500
59. Müller S, Maintz L, and Bieber T. Treatment of atopic dermatitis: Recently approved drugs and advanced clinical development programs. Allergy. (2024) 79:1501–15. doi: 10.1111/all.16009
60. Choo ZY, Mehlis SL, and Joyce JC. Updates in atopic dermatitis for the primary care physician: A review of advances in the understanding and treatment of atopic dermatitis. Dis Mon. (2024) 70:101687. doi: 10.1016/j.disamonth.2024.101687
61. Patruno C, Lauletta G, Pezzolo E, Boccaletti V, Rossi M, Caroppo F, et al. Effectiveness and safety of upadacitinib for adolescents with atopic dermatitis in a real-world setting. Clin Drug Investig. (2024) 44:629–34. doi: 10.1007/s40261-024-01382-y
62. Paller AS, Simpson EL, Siegfried EC, Cork MJ, Wollenberg A, Arkwright PD, et al. Dupilumab in children aged 6 months to younger than 6 years with uncontrolled atopic dermatitis: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. (2022) 400:908–19. doi: 10.1016/s0140-6736(22)01539-2
63. Bieber T. Disease modification in inflammatory skin disorders: opportunities and challenges. Nat Rev Drug Discov. (2023) 22:662–80. doi: 10.1038/s41573-023-00735-0
64. Bangert C, Rindler K, Krausgruber T, Alkon N, Thaler FM, Kurz H, et al. Persistence of mature dendritic cells, T(H)2A, and Tc2 cells characterize clinically resolved atopic dermatitis under IL-4Rα blockade. Sci Immunol. (2021) 6:eabe2749. doi: 10.1126/sciimmunol.abe2749
65. Braun C, Badiou C, Guironnet-Paquet A, Iwata M, Lenief V, Mosnier A, et al. Staphylococcus aureus-specific skin resident memory T cells protect against bacteria colonization but exacerbate atopic dermatitis-like flares in mice. J Allergy Clin Immunol. (2024) 154:355–74. doi: 10.1016/j.jaci.2024.03.032
66. Boguniewicz M, Fonacier L, Guttman-Yassky E, Ong PY, Silverberg J, and Farrar JR. Atopic dermatitis yardstick: Practical recommendations for an evolving therapeutic landscape. Ann Allergy Asthma Immunol. (2018) 120:10–22 e2. doi: 10.1016/j.anai.2017.10.039
67. Simpson EL, Gadkari A, Worm M, Soong W, Blauvelt A, Eckert L, et al. Dupilumab therapy provides clinically meaningful improvement in patient-reported outcomes (PROs): A phase IIb, randomized, placebo-controlled, clinical trial in adult patients with moderate to severe atopic dermatitis (AD). J Am Acad Dermatol. (2016) 75:506–15. doi: 10.1016/j.jaad.2016.04.054
68. Baumrin E, Shin DB, Mitra N, Pidala J, El Jurdi N, Lee SJ, et al. Patient-reported outcomes and mortality in cutaneous chronic graft-vs-host disease. JAMA Dermatol. (2024) 160:393–401. doi: 10.1001/jamadermatol.2023.6277
69. Deng F, Qiu Y, Zhang X, Guo N, Hu J, Yang W, et al. GB12-09, a bispecific antibody targeting IL4Rα and IL31Rα for atopic dermatitis therapy. Antib Ther. (2024) 7:77–87. doi: 10.1093/abt/tbad032
70. Tietz J, Gunde T, Warmuth S, Weinert C, Brock M, Simonin A, et al. A bispecific, tetravalent antibody targeting inflammatory and pruritogenic pathways in atopic dermatitis. JID Innov. (2024) 4:100258. doi: 10.1016/j.xjidi.2024.100258
71. Yilmaz O and Torres T. Extended half-life antibodies: A narrative review of a new approach in the management of atopic dermatitis. Dermatol Ther (Heidelb). (2024) 14:2393–406. doi: 10.1007/s13555-024-01253-6
72. Fishbane S, Jamal A, Munera C, Wen W, and Menzaghi F. A phase 3 trial of difelikefalin in hemodialysis patients with pruritus. N Engl J Med. (2020) 382:222–32. doi: 10.1056/NEJMoa1912770
73. Silverberg JI, Bissonnette R, Kircik L, Murrell DF, Selfridge A, Liu K, et al. Efficacy and safety of etrasimod, a sphingosine 1-phosphate receptor modulator, in adults with moderate-to-severe atopic dermatitis (ADVISE). J Eur Acad Dermatol Venereol. (2023) 37:1366–74. doi: 10.1111/jdv.18914
74. Guttman-Yassky E, Simpson EL, Reich K, Kabashima K, Igawa K, Suzuki T, et al. An anti-OX40 antibody to treat moderate-to-severe atopic dermatitis: a multicentre, double-blind, placebo-controlled phase 2b study. Lancet. (2023) 401:204–14. doi: 10.1016/s0140-6736(22)02037-2
75. Guttman-Yassky E, Brunner PM, Neumann AU, Khattri S, Pavel AB, Malik K, et al. Efficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by conventional treatments: A randomized, double-blind, phase 2a trial. J Am Acad Dermatol. (2018) 78:872–81.e6. doi: 10.1016/j.jaad.2018.01.016
76. Liu Q, Xia Y, Liu L, Zhou Y, and Li Y. Recent progress in tyrosine kinase 2 inhibitors for atopic dermatitis. Expert Opin Investig Drugs. (2024) 33:1001–7. doi: 10.1080/13543784.2024.2391825
77. Bempegaldesleukin stimulates immune response. Cancer Discov. (2019) 9:OF1. doi: 10.1158/2159-8290.Cd-nb2019-036
78. Bakker D, de Bruin-Weller M, Drylewicz J, van Wijk F, and Thijs J. Biomarkers in atopic dermatitis. J Allergy Clin Immunol. (2023) 151:1163–8. doi: 10.1016/j.jaci.2023.01.019
79. Bieber T, D’Erme AM, Akdis CA, Traidl-Hoffmann C, Lauener R, Schäppi G, et al. Clinical phenotypes and endophenotypes of atopic dermatitis: Where are we, and where should we go? J Allergy Clin Immunol. (2017) 139:S58–s64. doi: 10.1016/j.jaci.2017.01.008
80. Czarnowicki T, He H, Krueger JG, and Guttman-Yassky E. Atopic dermatitis endotypes and implications for targeted therapeutics. J Allergy Clin Immunol. (2019) 143:1–11. doi: 10.1016/j.jaci.2018.10.032
81. Fyhrquist N, Yang Y, Karisola P, and Alenius H. Endotypes of atopic dermatitis. J Allergy Clin Immunol. (2025) 156:24–40.e4. doi: 10.1016/j.jaci.2025.02.029
82. Park CO, Kim SM, Lee KH, and Bieber T. Biomarkers for phenotype-endotype relationship in atopic dermatitis: a critical review. EBioMedicine. (2024) 103:105121. doi: 10.1016/j.ebiom.2024.105121
83. Ogulur I, Pat Y, Ardicli O, Barletta E, Cevhertas L, Fernandez-Santamaria R, et al. Advances and highlights in biomarkers of allergic diseases. Allergy. (2021) 76:3659–86. doi: 10.1111/all.15089
84. Iturria-Medina Y, Adewale Q, Khan AF, Ducharme S, Rosa-Neto P, O’Donnell K, et al. Unified epigenomic, transcriptomic, proteomic, and metabolomic taxonomy of Alzheimer’s disease progression and heterogeneity. Sci Adv. (2022) 8:eabo6764. doi: 10.1126/sciadv.abo6764
85. Tokura Y and Hayano S. Subtypes of atopic dermatitis: From phenotype to endotype. Allergol Int. (2022) 71:14–24. doi: 10.1016/j.alit.2021.07.003
86. Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease. Nat Rev Drug Discov. (2022) 21:21–40. doi: 10.1038/s41573-021-00266-6
87. Chu DK, Schneider L, Asiniwasis RN, Boguniewicz M, De Benedetto A, Ellison K, et al. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on Practice Parameters GRADE- and Institute of Medicine-based recommendations. Ann Allergy Asthma Immunol. (2024) 132:274–312. doi: 10.1016/j.anai.2023.11.009
Keywords: atopic dermatitis, targeted therapies, biologics, JAK inhibitors, blockade
Citation: Zhang L, Peng G, Wang M, Niyonsaba F and Gao X (2025) Beyond the blockade: unmet needs in systemic targeted atopic dermatitis therapy. Front. Immunol. 16:1712757. doi: 10.3389/fimmu.2025.1712757
Received: 25 September 2025; Accepted: 11 November 2025; Revised: 04 November 2025;
Published: 27 November 2025.
Edited by:
Marco Casciaro, University Hospital of Policlinico G. Martino, ItalyReviewed by:
Mario Di Gioacchino, University of Studies G. d’Annunzio Chieti and Pescara, ItalyHemali Shah, University of Pittsburgh Medical Center, United States
Copyright © 2025 Zhang, Peng, Wang, Niyonsaba and Gao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: François Niyonsaba, ZnJhbmNvaXNAanVudGVuZG8uYWMuanA=; Xinghua Gao, eGhnYW9AY211LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship