 Laure Bastide1*
Laure Bastide1* Gaetano Perrotta1
Gaetano Perrotta1 Valentina Lolli2
Valentina Lolli2 Céline Mathey3
Céline Mathey3 Ortensa-Irina Vierasu3Serge Goldman3
Ortensa-Irina Vierasu3Serge Goldman3 Frédéric Vandergheynst4
Frédéric Vandergheynst4- 1Department of Neurology, CUB Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
- 2Department of Radiology, CUB Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
- 3Department of Nuclear Medicine, CUB Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
- 4Department of Internal Medicine, CUB Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
Background: Only a few cases of acute disseminated encephalomyelitis (ADEM) following coronavirus disease 19 (COVID-19) vaccination have been described since the beginning of the vaccination campaign.
Results: Here we report the first case of central nervous system (CNS) demyelination with systemic inflammatory findings on whole body 19-fluorodeoxyglucose positron emission tomography with computed tomography (FDG-PET/CT) following the ChAdOx1 nCoV-19 vaccine.
Conclusions: Clinicians should stay aware of potential new adverse events after immunization.
Introduction
Since the beginning of the pandemic, vaccines were produced in record time. Real-world studies indicated an excellent safety profile. Despite these studies, the scientific community must stay aware of rare but severe complications and report them. This allows more accuracy of the real-world safety profile of the vaccine. We can take appropriate measures, as we did with the AztraZaneca vaccine (ChAdOx1 nCoV-19) and its thromboembolic complications (1). The ChAdOx1 nCoV-19 is a vaccine based on a recombinant adenoviral vector encoding the spike protein of SARS-CoV-2 (2). Acute disseminated encephalomyelitis (ADEM) is an immune-mediated inflammatory disorder of the central nervous system (CNS) that occurs after an antigenic challenge. The post-vaccine etiology represents 5% of all ADEM cases and the annual incidence of ADEM ranges from 1 to 10 per million (3). Here we report the first case of central nervous system (CNS) demyelination with systemic inflammatory findings on whole body 19-fluorodeoxyglucose positron emission tomography with computed tomography (FDG-PET/CT) following the ChAdOx1 nCoV-19 vaccine.
Case report
A previously healthy 49-year-old female received her first dose of ChAdOx1 nCoV-19 vaccine. She experienced mild flu-like symptoms during the following 48 h. One week later, the patient presented another episode of flu-like symptoms with fever, fatigue, neck pain, followed over the next few days by rapidly progressive sensitive symptoms including paresthesia in both legs, up to the chest, Lhermitte's phenomenon and sphincter dysfunction. In April, the patient came to the neurological consultation at another hospital. During the examination a hypoesthesia with a thoracic (Th) 8 level was noticed with a sensory ataxia. A full spine magnetic resonance imaging (MRI) was normal but somatosensory evoked potentials (SSEPs) showed abnormal conduction above the sensory decussation in the lower brainstem. Four weeks later, the patient came to our neurological outpatient clinic. Her symptoms had worsened with sensory symptoms now involving her hands, worsening sensory ataxia and of sphincter dysfunction. Her neurological examination showed normal strength, hypoesthesia to all modalities with a Th 8 level, absent plantar response, impaired tandem walking and the presence of a Romberg sign.
An MRI of the brain was obtained and revealed large, ill-defined T2 fluid attenuated inversion recovery (FLAIR) hyperintensities of periventricular and deep white matter, along with smaller lesions infratentorially (Figure 1, part1). Subcortical U fibers were spared, and so were the cortex and deep gray matter. Lesions showed mildly increased diffusivity and were mostly non-enhancing. They exerted no mass effect. No meningeal enhancement was noted. MRI of the spinal cord revealed the appearance of numerous contiguous short-segment cervical and thoracic lesions, showing variably increased T2 signal intensity and contrast enhancement (Figure 1, part 2). The spinal cord was moderately swollen. Nerve conductive studies were normal. A lumbar puncture showed a mild pleocytosis with 8 white blood cells, elevated protein levels (101 mg/dL), normal IgG/albumin index and identical oligoclonal bands in the cerebrospinal fluid (CSF) and serum (type 4 pattern). Based on the clinical history and the radiological aspects an inflammatory origin was retained. Our differential diagnosis workup was mainly focused on an infectious or an auto-immune causes. An infectious panel was negative. An exhaustive blood investigation was done with the intention to exclude auto-immune systemic diseases, no relevant findings were found. A screening for antibodies targeting antigens associated with demyelinating disorders of the CNS (MOG antibody disease and NMO spectrum) remained negative (Table 1).
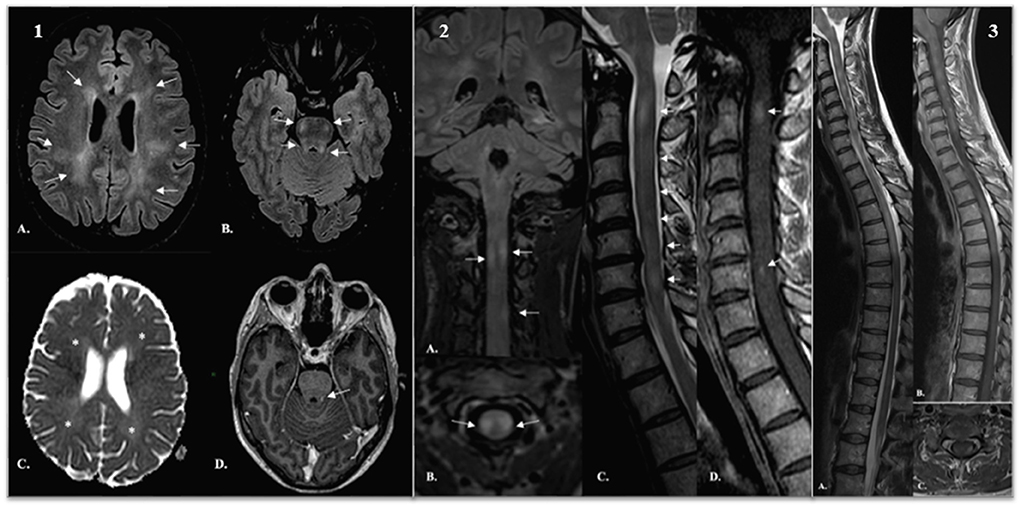
Figure 1. Part 1: (A,B) Axial T2 FLAIR-weighted images demonstrated extensive, asymmetric involvement of periventricular and deep white matter [arrows in (A)]. Smaller lesions were observed in the ponto-mesencephalic tegmentum, superior and middle cerebellar peduncles [arrows in (B)]. (C) Lesions were mildly hyperintense on ADC cartography, revealing increased diffusivity (*). (D) A small focus of contrast enhancement was demonstrated in the left superior cerebellar peduncle (arrow). Part 2: (A–C) Reformatted coronal (A) and axial (B) T2 FLAIR-weighted images and sagittal T2-weighted images and sagittal T2 weighted image (C) reveal multiple short-segment hyperintensities (arrows). Lesions are asymmetric and excentrically located and involve both white and gray matter. Signal intensity is variable, from midly to markedly increased. (D) Sagittal post-gadolinium T1-weighted image shows scattered foci of enhancement (arrows). Part 3: (A–C) Sagittal T2 (A) and post-contrast sagittal (B) and axial (C) T1-weighted images demonstrate progression of disease. We found lesions on the entire spinal cord. FLAIR, fluid attenuated inversion recovery; ADC, apparent diffusion coefficient.
Table 1. Clinical evolution and complementary assessments done during patient follow-up.
Based on the exclusion of CNS infection or other autoimmune disorders, the diagnosis of atypical ADEM was made. The patient was treated with an intravenous course of methylprednisolone (1 g/day for 5 days). Her condition stabilized and she was transferred to a rehabilitation center.
Three weeks after discharge, she was readmitted because of a clinical deterioration. Neurological evaluation showed a new paraparesis, evaluated at 2/5 in the right leg and 3/5 in the left leg, complete loss of pallesthesia up to the iliac crests, a sensory Th 5 level, and a severe sensory ataxia requiring walking aids.
Six weeks afterwards, on July 14, an MRI showed an increase in the number and size of spinal cord lesions and the appearance of new foci of contrast enhancement (Figure 1, part 3). Brain findings were unchanged. She was treated with 5 sessions of plasma exchange. She improved and was discharged again to a rehabilitation center. Three weeks later, her weakness worsened. A new MRI showed there were new enhancing lesions in the brain stem and cervical spinal cord.
Because of the atypical course of the disease, the diagnosis of ADEM was reconsidered. Whole body fluorodeoxyglucose positron emission tomography with computed tomography (FDG-PET/CT) was obtained with the aim of excluding systemic inflammation, namely sarcoidosis despite negative biological markers. Results revealed increased glucose uptake not only in the spinal cord but also in the thyroid, the thoracic aorta walls and the lumbar spinous processes (Figure 2).
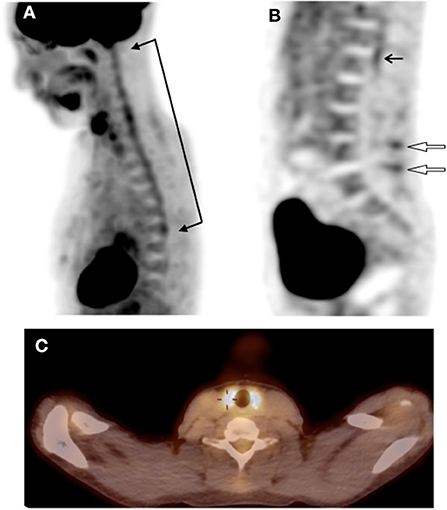
Figure 2. (A) sagittal view of FDG-PET/CT showing hypermetabolism of the spinal cord at the cervicothoracic level (between arrows). (B) sagittal view of FDG-PET/CT showing hypermetabolism of the spinal cord at the lumbosacral level (black arrow) and an interspinous hypermetabolism at two level of the lumbar spine (open arrows). (C) fused FDG-PET/CT image on the transverse plane showing a marked and diffuse hypermetabolism of the thyroid gland. FDG-PET/CT, whole body 19-fluorodeoxyglucose positron emission tomography with computed tomography.
She did not have any complaints about osteo-articular or vascular systems. Further thyroid testing with echography, hormone levels and autoantibodies were normal. She received IV rituximab (1 g and another after 15 days) and another course of IV methylprednisolone (1 g/day for 5 days). Over the next 2 months, she progressively improved. At last follow-up, strength in her right and left lower limbs was evaluated at 3+/5 and 4+/5, respectively, the sensory level had dropped to the level of Th12 and she could take a few steps without aid. Another MRI showed stability or regression of most lesions.
On repeat whole body FDG-PET/CT (13 weeks after the first one), thyroid uptake had disappeared but other regions' abnormal uptake had decreased and new areas of increased uptake had appeared at the level of the scapular and pelvic girdles, ischiatic and great trochanters.
Discussion
This case report raises two important points: the association between ChAdOx1 nCoV-19 and ADEM and the meaning of incidental findings in the FDG PET-CT.
A review of the SARS-CoV-2 vaccine and ADEM literature showed 13 reported cases of ADEM following the administration of a COVID-19 vaccine, which are summarized in Table 2 (4–14).
Table 2. Clinical and demographic characteristics of the 6 cases reporting with an ADEM post COVID vaccine.
In comparison to prior cases except maybe one who had a pseudo relapse (14), our patient had a more protracted course, which evolved in two subsequent worsening phases until improvement 8 months later. These phases occurred each time after treatment cessation and there was no relapse after the symptomatic nadir which occurred in August (Table 1). Therefore, we conclude that these recurrences are part of the same monophasic course.
Also, the MRI evolution of the lesions is atypical for several reasons: the sub-acute evolution (longer than 3 months), the discordance between brain and spinal cord lesions in terms of how they evolved and their aspects, and the limited resolution on the last MRI after 7 months of follow-up. As some studies have described, some lesions could take up to 18 months to disappear (15) or persisted on follow-up imaging (16). We did have the information of the MRI evolution from only 3 previously reported cases as shown in Table 2: one with a complete resolution in 1 month (4) and the other two with a partial resolution at follow-up of 30 and 66d (6, 11). We retained the diagnosis of ADEM according to Sejvar et al. (17) but determined it atypical because of these particular findings.
It is the first reported case of post-ChAdOx1 nCoV-19 vaccination ADEM in which FDG-PET/CT was performed. The observed pulmonary nodules' hypercaption were very small (<5 mm) with a reduction of the glucose uptake at the FDG-PET/CT control. A basic control will be performed at one year with a CT.
The increased glucose uptake observed in the thyroid on the first FDG-PET/CT is difficult to interpret in our clinical setting. Mild FDG uptake by the thyroid is likely physiological and a normal variant but moderate-to-intense diffuse uptake is usually associated with elevated TSH, thyroiditis, hyperthyroidism or Graves' disease (18). One interesting study reported aortic and thyroid unexpected hypermetabolism without clinical relevance in a cohort of patients with anti-neutrophil cytoplasmic antibodies-associated vasculitis (19). In our case the complementary analysis and also the control FDG-PET/CT were normal, leading to the conclusion that the initial thyroid finding had no clinical relevance.
The increased uptake of the thoracic aorta and the lumbar spinous processes interspaces associated with the increased uptake of the scapular and pelvic girdles, ischiatic and great trochanters in the second FDG-PET/CT raised the question of polymyalgia rheumatic associated with a giant cell arteritis (PMR-GCA) diagnosis. Again, in our case we did not have any clinical correlation and our patient is substantially younger (40 years old) than the median age (70 years old) of diagnosis for this PMR-GCA entity (20). We did not find any description in the literature of the association of ADEM with vasculitis, in particular giant-cell arteritis. Large-vessel vasculitis is not classically associated with extensive myelitis. We only found a case report of NMO spectrum disorder which is a demyelinating auto-immune disease of the CNS, associated with Takayasu arteritis (21). The possibility of CNS and systemic vasculitis, triggered by the vaccination in our case, should be raised. Recent literature reports cases of vasculitis as cutaneous vasculitis (22), hypersensitivity angiitis, IgA vasculitis (23) and ANCA-associated vasculitis (24) following ChAdOx1 nCoV-19 vaccine and one case of eosinophilic granulomatosis with polyangiitis after the Moderna vaccine (25). We also found one reported case of CNS vasculitis following BNT162b2, Pfizer/BioN-Tech vaccine (26) but without FDG-PET/CT done. Vasculitis was described as a complication during COVID-19 because of direct endothelial damage (27) and ChAdOx1 nCoV-19 vaccine is associated with immune thrombosis and thrombocytopenia. To date, current data do not strongly support a causative link between vaccination and most of vasculitis (28). The hypothesis of two autoimmune disorders coexistence' rather than a large-vessel vasculitis with CNS involvement could also be raised and it is a situation already described in the literature (29, 30). In our case, the lack of clinical corresponding symptoms to the FDG-PET/CT findings does not allow to confirm a specific diagnosis. For all these reasons we will remain for now with the diagnosis of atypical ADEM with systemic inflammation without a clear diagnosis.
Conclusions
We report the first case of post-ChAdOx1 nCoV-19 vaccination atypical ADEM with incidental findings on the FDG-PET/CT consistent with a large-vessel vasculitis, in particular GCA given the hypermetabolism of scapular and pelvic girdles and typical of polymyalgia rheumatica. Their relevance remains debatable at this stage given the lack of corresponding symptoms. Clinicians should stay aware of potential new adverse events after immunization.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by Comité d'Ethique de l'Hopital Erasme—CUB. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
LB wrote the first draft of the manuscript. VL, SG, MC, and VO-I wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ADEM, acute disseminated encephalomyelitis; Coronavirus disease 19, COVID-19; CNS, central nervous system; FDG-PET/CT, whole body 19-fluorodeoxyglucose positron emission tomography with computed tomography; Th, thoracic; MRI, magnetic resonance imaging; SSEPs, somatosensory evoked potentials; FLAIR, fluid attenuated inversion recovery; ADC, apparent diffusion coefficient PMR-GCA, polymyalgia rheumatic associated with a giant cell arteritis.
References
1. Greinacher A, Thiele T, Warkentin TE, Weisser K, Paul A. Kyrle, Eichinger S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med. (2021) 384:2092–101. doi: 10.1056/NEJMoa2104840
2. Voysey M, Clemens SAC, Madhi SA, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. (2021) 397:99–111. doi: 10.1016/S0140-6736(20)32661-1
3. Pellegrino P, Carnovale C, Perrone V, et al. Acute disseminated encephalomyelitis onset: evaluation based on vaccine adverse events reporting systems. PLoS ONE. (2013) 8:e77766. doi: 10.1371/journal.pone.0077766
4. Cao L, Ren L. Acute disseminated encephalomyelitis after severe acute respiratory syndrome coronavirus 2 vaccination: a case report. Acta Neurol Belg. (2021) 1:1–3. doi: 10.1007/s13760-021-01608-2
5. Ozgen Kenangil G, Ari BC, Guler C, Demir MK. Acute disseminated encephalomyelitis-like presentation after an inactivated coronavirus vaccine. Acta Neurol Belg. (2021) 121:1089–91. doi: 10.1007/s13760-021-01699-x
6. Raknuzzaman M, Jannaty T, Hossain MB, Saha B, Dey SK, Shahidullah M. Post Covid19 vaccination acute disseminated encephalomyelitis: a case report in Bangladesh. Int J Med Sci Clin Res Stud. (2021) 1:31–6.
7. Vogrig A, Janes F, Gigli GL, Curcio F, Negro ID, D'Agostini S, et al. Acute disseminated encephalomyelitis after SARS-CoV-2 vaccination. Clin Neurol Neurosurg. (2021) 208:106839. doi: 10.1016/j.clineuro.2021.106839
8. Kania K, Ambrosius W, Tokarz Kupczyk E, Kozubski W. Acute disseminated encephalomyelitis in a patient vaccinated against SARS-CoV-2. Ann Clin Transl Neurol. (2021) 8:2000–3. doi: 10.1002/acn3.51447
9. Rinaldi V, Bellucci G, Romano A, Bozzao A, Salvetti M. ADEM after ChAdOx1 nCoV-19 vaccine: A case report. Mult Scler. (2021) 28:1151–4. doi: 10.1177/13524585211040222
10. Permezel F, Borojevic B, Lau S, de Boer HH. Acute disseminated encephalomyelitis (ADEM) following recent Oxford/AstraZeneca COVID-19 vaccination. Forensic Sci Med Pathol. (2022) 18:74–9. doi: 10.1007/s12024-021-00440-7
11. Shimizu M, Ogaki K, Nakamura R, Kado E, Nakajima S, Kurita N, et al. An 88-year-old woman with acute disseminated encephalomyelitis following messenger ribonucleic acid-based COVID-19 vaccination. eNeurologicalSci. (2021) 25:100381. doi: 10.1016/j.ensci.2021.100381
12. Al-Quliti K, Qureshi A, Quadri M, Abdulhameed B, Alanazi A, Alhujeily R. Acute demyelinating encephalomyelitis post-COVID-19 vaccination: a case report and literature review. Diseases. (2022) 10:13. doi: 10.3390/diseases10010013
13. Nagaratnam SA, Ferdi AC, Leaney J, Lee RLK, Hwang YT, Heard R. Acute disseminated encephalomyelitis with bilateral optic neuritis following ChAdOx1 COVID-19 vaccination. BMC Neurol. (2022) 22:54. doi: 10.1186/s12883-022-02575-8
14. Ancau M, Liesche-Starnecker F, Niederschweiberer J, et al. Case series: acute hemorrhagic encephalomyelitis after SARS-CoV-2 vaccination. Front Neurol. (2021) 12:820049. doi: 10.3389/fneur.2021.820049
15. Honkaniemi J, Dastidar P, Kähärä V, Haapasalo H. Delayed MR imaging changes in acute disseminated encephalomyelitis. AJNR Am J Neuroradiol. (2001) 22:1117–24.
16. van der Knaap MS, Valk J eds. Acute disseminated encephalomyelitis and acute hemorrhagic encephalomyelitis. In: Magnetic Resonance of Myelination and Myelin Disorders. (2005). Berlin: Springer. p. 604–15. doi: 10.1007/3-540-27660-2_80
17. Sejvar JJ, Kohl KS, Bilynsky R, et al. Encephalitis, myelitis, and acute disseminated encephalomyelitis (ADEM): case definitions and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine. (2007) 25:5771–92. doi: 10.1016/j.vaccine.2007.04.060
18. Liu Y, Ghesani NV, Zuckier LS. Physiology and pathophysiology of incidental findings detected on FDG-PET scintigraphy. Semin Nucl Med. (2010) 40:294–315. doi: 10.1053/j.semnuclmed.2010.02.002
19. Kemna MJ, Vandergheynst F, Vöö S, Blocklet D, Nguyen T, Timmermans SAMEG, et al. Positron emission tomography scanning in anti-neutrophil cytoplasmic antibodies-associated vasculitis. Medicine (Baltimore). (2015) 94:e747. doi: 10.1097/MD.0000000000000747
20. Slart Slart RHJA; Writing group; Reviewer group; Members of EANM Cardiovascular; Members of EANM Infection & Inflammation; Members of Committees SNMMI Cardiovascular , et al. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. (2018) 45:1250–69. doi: 10.1007/s00259-018-3973-8
21. Lamartine S. Monteiro M, Lascano AM, Meunier Carus Vincent N, Seebach JD, Lalive PH, Gschwind M. AQP4 antibody-positive NMO spectrum disorder associated with Takayasu arteritis. J Neurol Sci. (2019) 396:130–2. doi: 10.1016/j.jns.2018.11.016
22. Cavalli G, Colafrancesco S, De Luca G, Rizzo N, Priori R, Conti F, et al. Cutaneous vasculitis following COVID-19 vaccination. Lancet Rheumatol. (2021) 3:e743–4. doi: 10.1016/S2665-9913(21)00309-X
23. Pottegård A, Lund LC, Karlstad Ø, Dahl J, Andersen M, Hallas J, et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. BMJ. (2021) 373:n1114. doi: 10.1136/bmj.n1114
24. Villa M, Díaz-Crespo F, Pérez de José A, Verdalles Ú, Verde E, Almeida Ruiz F, et al. A case of ANCA-associated vasculitis after AZD1222 (Oxford-AstraZeneca) SARS-CoV-2 vaccination: casualty or causality? Kidney Int. (2021) 100:937–8. doi: 10.1016/j.kint.2021.07.026
25. Ibrahim H, Alkhatib A, Meysami A. Eosinophilic Granulomatosis With Polyangiitis Diagnosed in an Elderly Female After the Second Dose of mRNA Vaccine Against COVID-19. Cureus. (2022) 14:e21176. doi: 10.7759/cureus.21176
26. Takeyama R, Fukuda K, Kouzaki Y, et al. Intracerebral hemorrhage due to vasculitis following COVID-19 vaccination: a case report. Acta Neurochir (Wien). (2022) 164:543–7. doi: 10.1007/s00701-021-05038-0
27. McGonagle D, Bridgewood C, Ramanan AV, Meaney JFM, Watad A. COVID-19 vasculitis and novel vasculitis mimics. Lancet Rheumatol. (2021) 3:e224–33. doi: 10.1016/S2665-9913(20)30420-3
28. Bonetto C, Trotta F, Felicetti P, et al. Vasculitis as an adverse event following immunization - Systematic literature review. Vaccine. (2016) 34:6641–51. doi: 10.1016/j.vaccine.2015.09.026
29. Wingerchuk DM, Weinshenker BG. The emerging relationship between neuromyelitis optica and systemic rheumatologic autoimmune disease. Mult Scler. (2012) 18:5–10. doi: 10.1177/1352458511431077
Keywords: acute disseminated encephalomyelitis (ADEM), COVID-19, vaccination, systemic inflammation, fluorodeoxyglucose positron emission tomography with computed tomography (FDG-PET/CT)
Citation: Bastide L, Perrotta G, Lolli V, Mathey C, Vierasu O-I, Goldman S and Vandergheynst F (2022) Atypical acute disseminated encephalomyelitis with systemic inflammation after a first dose of AztraZaneca COVID-19 vaccine. A case report. Front. Neurol. 13:995875. doi: 10.3389/fneur.2022.995875
Received: 16 July 2022; Accepted: 11 August 2022;
Published: 29 August 2022.
Edited by:
Hans-Peter Hartung, Heinrich Heine University of Düsseldorf, GermanyReviewed by:
Yuto Uchida, Johns Hopkins Medicine, United StatesAntonella Muroni, Azienda Ospedaliero-Universitaria Cagliari, Italy
Copyright © 2022 Bastide, Perrotta, Lolli, Mathey, Vierasu, Goldman and Vandergheynst. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laure Bastide, bGF1cmUuYmFzdGlkZUBlcmFzbWUudWxiLmFjLmJl