 Jonathan E. Attwood1,2*
Jonathan E. Attwood1,2* Izabelle Lövgren1,3
Izabelle Lövgren1,3 Rob Forsyth4Célia Demarchi5,6
Rob Forsyth4Célia Demarchi5,6 Tony Thayanandan7
Tony Thayanandan7 Lara Prisco1,2,3
Lara Prisco1,2,3 Mario Ganau1,2Rebecca Roberts2Kate Scarff2
Mario Ganau1,2Rebecca Roberts2Kate Scarff2 Julia L. Newton2
Julia L. Newton2 Gabriele C. DeLuca1,2Tim Lawrence1,2*
Gabriele C. DeLuca1,2Tim Lawrence1,2*- 1Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
- 2Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom
- 3The Podium Institute for Sports Medicine and Technology, Department of Engineering Science, University of Oxford, Oxford, United Kingdom
- 4Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom
- 5Department of Brain Sciences, Imperial College London, London, United Kingdom
- 6Children’s Neurosciences, Evelina London Children’s Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom
- 7Department of Psychiatry, University of Oxford, Oxford, United Kingdom
Outcomes following paediatric mild traumatic brain injury (mTBI) are extremely heterogenous. While emerging biomarkers promise enhanced prognostic accuracy, a critical question remains unanswered—which outcome measures provide the most accurate assessment of injury impact? In this article, we highlight barriers to selecting appropriate outcome measures, including variability in how outcomes are defined and the wide range of assessment tools used. With reference to the most recent literature, we summarise current evidence of adverse outcomes following paediatric mTBI and highlight emerging candidate biomarkers of these outcomes. We emphasise the unique challenges associated with interpreting outcome measures in younger patients, from the impact of developmental stage and assessment timing to the influence of injury-independent factors. We assert the need to consider these obstacles when designing and interpreting mTBI biomarker studies. To realise the potential of prognostic biomarkers, future research should prioritise establishing consensus definitions, compiling a set of accessible and comprehensive outcome measures, and capturing injury-independent factors through longitudinal study designs.
1 Introduction
Traumatic brain injury (TBI) encompasses a wide range of conditions whereby the brain is structurally or functionally altered by a mechanical insult (1). Although TBIs are a leading cause of death and disability among young people worldwide, up to 90% are classified as ‘mild’ (i.e., Glasgow Coma Scale 13–15) (2, 3). Mild TBI (mTBI) with no structural neuroimaging abnormalities is also known as concussion (4). While mTBIs are unlikely to result in death or disability, poor medium-and long-term outcomes still occur. Indeed, a significant proportion of patients with mTBI endure persistent symptoms, ranging from headache to impaired attention and mood disturbance, all of which can be debilitating and life-changing (5).
For more than 50 years, the Glasgow Coma Scale (GCS) has been central to the assessment of TBI severity, but the variability of outcomes following mTBI highlights the need for more granular classification of these injuries (6). In a statement to this unmet need, the National Institute of Neurological Disorders and Stroke recently recommended combining clinical assessment with biomarkers, imaging, and outcome modifying factors (CBI-M) in the evaluation of TBI (7). The proposed CBI-M framework promises to transform how TBI is characterised, managed, and studied (8). However, a key challenge remains: how can we utilise these evaluations in the acute phase post-injury to distinguish who is more likely to experience adverse outcomes?
Inherent to this challenge is the need for scientific accuracy. Specifically, the distinction between biomarkers and outcome measures must be recognised. Biomarkers are measurable characteristics that indicate biological processes (9), while outcome measures capture functional impacts experienced by patients (10). Short-term outcomes, such as symptom scores, may be reliable predictors of longer-term outcomes, but this does not make them biomarkers unless they relate directly to biological processes. Recognising this distinction highlights an opportunity for both biomarkers and outcome measures collected longitudinally to be integrated into dynamic prediction models.
To date, considerable research has been dedicated to identifying diagnostic and prognostic biomarkers of TBI (Figure 1) (11, 12). In contrast, relatively little attention has been given to determining which outcome measures these emerging biomarkers should be validated against, and what additional factors need to be accounted for. The latter is particularly important in paediatric TBI, where age at injury (13), time since injury (14), and neurodevelopmental stage (15) can all strongly influence observed outcomes. There is also substantial heterogeneity in the outcome assessment tools used, and little consensus on which measures are most appropriate, with tools developed for moderate–severe TBI (GCS 3–12) often lacking sensitivity to impairments experienced after mTBI.
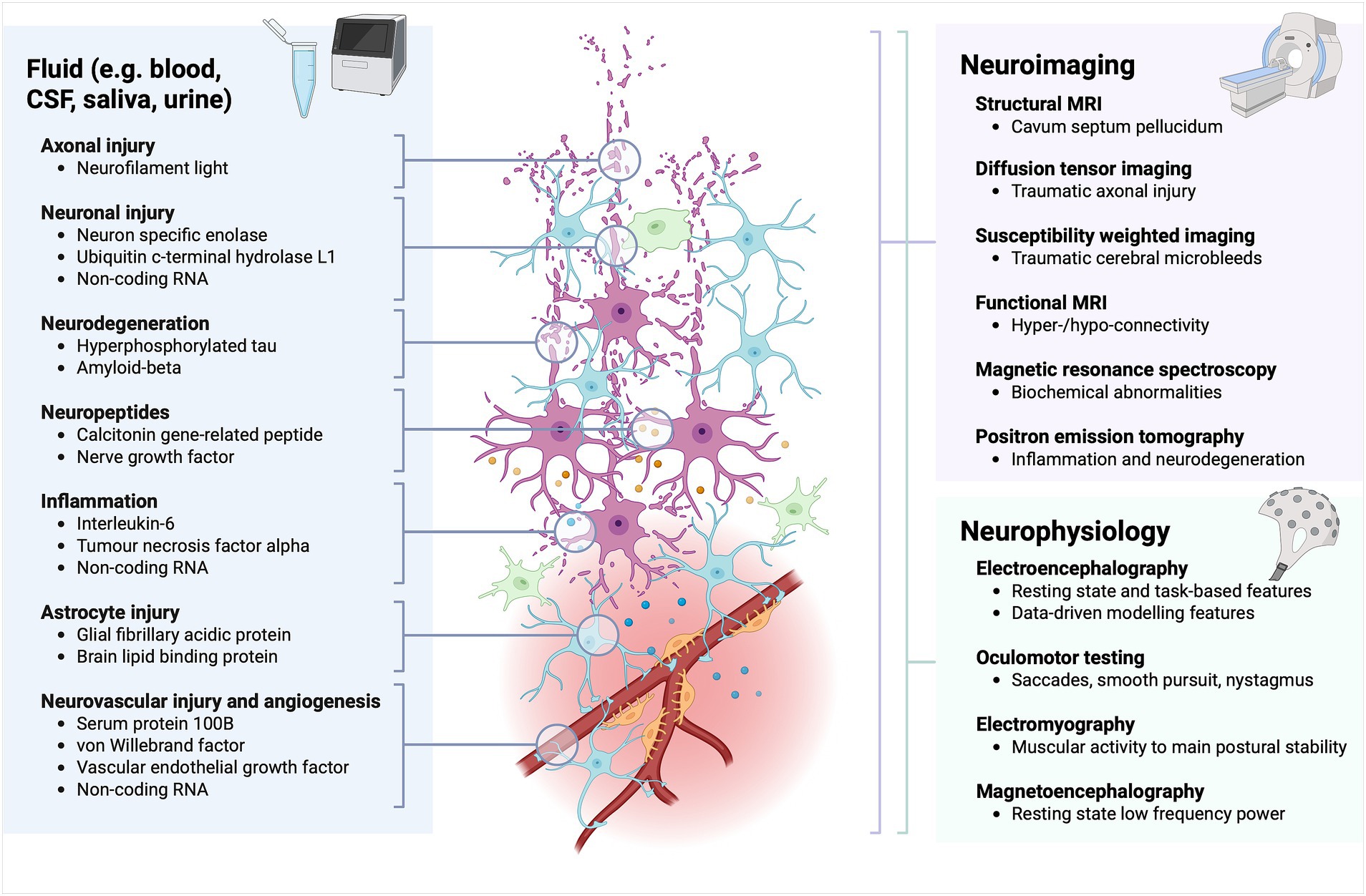
Figure 1. Emerging fluid, neuroimaging, and neurophysiological biomarkers of TBI. Fluid biomarkers are organised according to components of TBI pathophysiology. Neuroimaging and neurophysiological biomarkers are grouped by technique or modality.
To accurately validate prognostic biomarkers of mTBI, it is critical that we first understand which outcome measures provide the best assessment of the effects of an injury. In this article, we draw on the expertise of a multidisciplinary team to (i) discuss barriers to selecting outcome measures for the validation of prognostic biomarkers; (ii) summarise current evidence of adverse outcomes following paediatric mTBI and highlight emerging candidate biomarkers of these outcomes; and (iii) highlight the unique challenges in assessing and interpreting outcomes in a paediatric population. We conclude by offering recommendations for future research.
2 Barriers to selecting outcome measures for validating prognostic mTBI biomarkers
2.1 Variability in definitions across the literature
The terminology used to describe and classify brain injuries continues to pose fundamental challenges. In 2023, a consensus definition and diagnostic criteria for mTBI were published by the American Congress of Rehabilitation Medicine (ACRM), while separately the definition of sport-related concussion (SRC) was updated (4, 16). The definition of SRC still lacks diagnostic criteria, and both the meaning and relevance of the term ‘sport-related’ remains unclear. Moreover, the terms ‘mTBI’ and ‘concussion’ continue to be conflated in the literature, and the corresponding criteria used to recruit participants into studies are not always clear, limiting comparability and generalisability. Reaching consensus on an operational definition that encompasses both terms is vital to make progress in the field.
Considering outcomes, a clear definition of what constitutes abnormally prolonged recovery following mTBI is also essential to enable comparisons between studies and meta-analyses. Currently, temporal thresholds for abnormally prolonged recovery are inconsistent across the literature, spanning from 3 weeks to 3 months (17). Additionally, the domains by which recovery is assessed vary between studies, ranging from self-reported symptom resolution or resumption of usual activities to return to baseline assessment scores, among others. Given that approximately one in eight children remain symptomatic 3 months after mTBI (5), a consensus definition of abnormally prolonged recovery needs to be established. Terms used to describe this condition, including post-concussion syndrome (PCS) and persistent post-concussion symptoms (PPCS) must also be harmonised (17–19).
While diagnostic criteria for prolonged recovery have not been validated in children, a working paediatric definition has been proposed (17), nevertheless, the optimal temporal cut-off for prolonged recovery remains a key area of uncertainty, stressing the need for a better understanding of the natural evolution of mTBI in young people (20). Overcoming barriers to the long-term follow-up of paediatric patients will be central to sustaining the longitudinal studies needed to gain these insights.
2.2 Heterogeneity of assessment tools
mTBI can produce a broad range of symptoms, and as such, those in whom symptoms persist may present to various specialties, including neurology, neuropsychology, psychiatry, and sport and exercise medicine (21). Each specialty prioritises different outcomes according to their perspective and skillset, and different specialties often employ distinct methods to measure similar outcomes (Figure 2) (22).
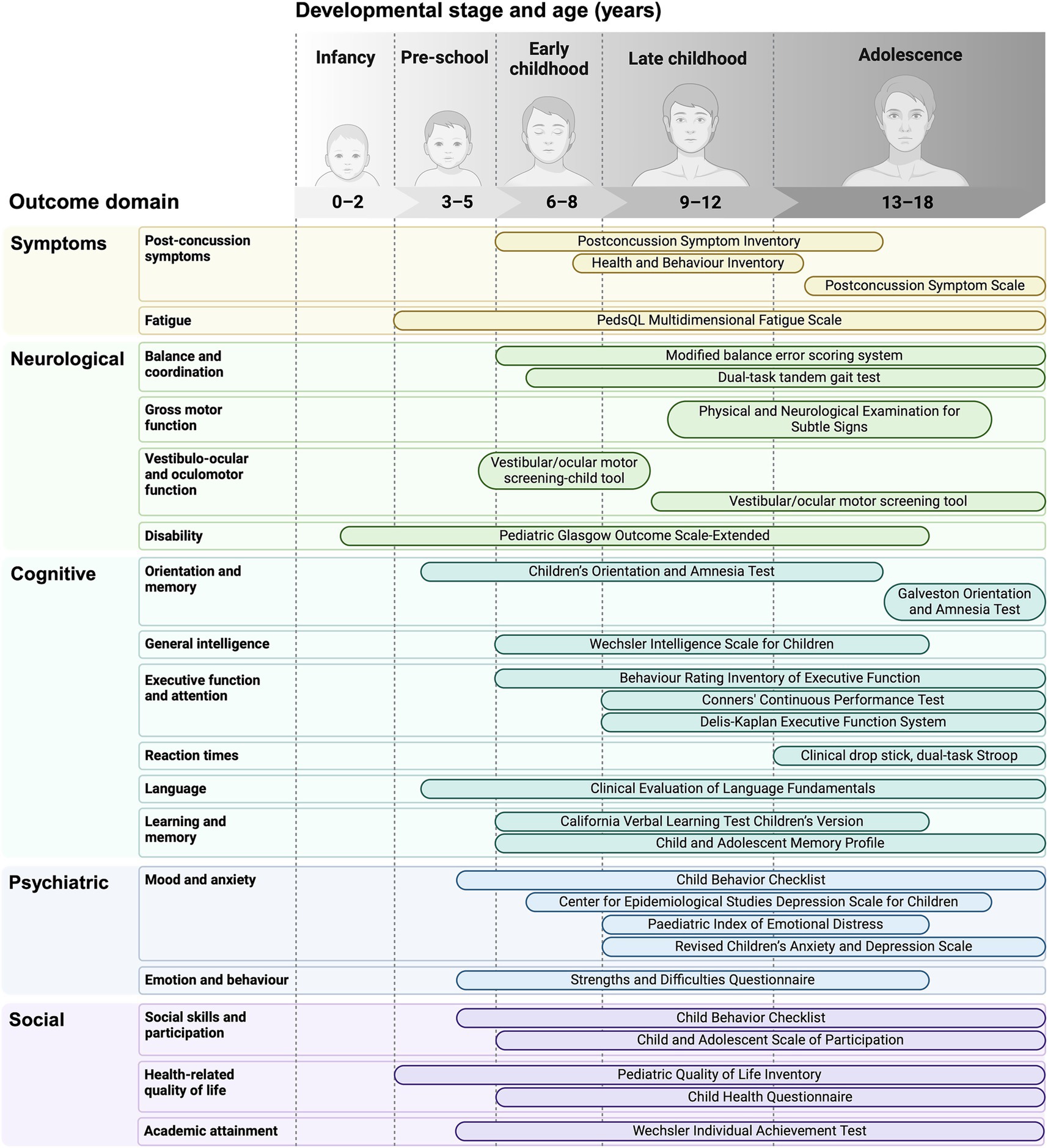
Figure 2. A selection of tools used throughout childhood to assess the spectrum of domains affected by mild TBI.
Even within a specialty, different sites use different tools to assess the same domains, leading to considerable heterogeneity in both clinical practice and research. Assessment tools that were originally designed for clinical use, such as the immediate post-concussion assessment and cognitive test (ImPACT), are increasingly used as outcome measures in research (23). While these tools can help to measure symptom resolution and return to baseline cognitive performance, there is limited evidence to support their use beyond the acute phase (24).
Pragmatically, the choice of tool is often guided by practical constraints, which limit the applicability of lengthy, costly, or highly technical assessments. A consensus needs to be reached about which assessment tools should be used to provide a comprehensive view of meaningful outcomes, while minimising time and resource burden to ensure they can be feasibly implemented in both clinical and research settings.
3 Current evidence of adverse outcomes following paediatric mTBI and emerging candidate biomarkers
Having highlighted the barriers posed by variable injury and outcome definitions and the heterogeneity of outcome assessment tools, in this section we summarise the range of adverse outcomes that have been demonstrated following paediatric mTBI to highlight opportunities for the development of prognostic biomarkers.
3.1 Neurological outcomes
Post-traumatic headache (PTH), which often resembles migraine or tension-type headache, is a common feature of prolonged recovery from mTBI, affecting over half of children with persistent symptoms (25, 26). While the pathophysiology of PTH is not fully understood, neuropeptides implicated in migraine (e.g., calcitonin gene-related peptide and nerve growth factor) have emerged as candidate biomarkers of headache after mTBI (27, 28). As no paediatric definition of PTH exists, studies validating prognostic biomarkers for PTH should use the most recent International Classification of Headache Disorders definition as their primary outcome (29). This defines PTH as headache reported to have developed within 7 days of mTBI, and persistent PTH as headache developing with 7 days and persisting for more than 3 months.
Other frequent neurological sequelae include vestibulo-ocular and oculo-motor dysfunction, resulting in dizziness, vertigo, nausea, and blurred vision (30, 31). These symptoms affect approximately one in four children with concussion and two out of three children with persistent post-concussion symptoms (30). Smooth pursuit, saccade, and vestibulo-ocular reflex abnormalities may be identifiable on examination, and could be utilised as objective outcomes measures alongside self-reported symptoms (32). Additionally, gross motor deficits including postural instability, impaired balance, and gait abnormalities, may persist up to 12 months post-injury after mTBI (33, 34).
3.2 Cognitive outcomes
While cognitive symptoms often arise following mTBI, there is currently no evidence of a lasting effect on intellectual abilities (23, 35, 36). Other cognitive domains, including executive function, reaction time, working memory, processing speed, and attention are variably affected in children with TBI across the spectrum of injury severity (37, 38). The balance of evidence currently suggests that these impairments tend to recover after a single mTBI, with the possible exception of executive function (23, 37, 38). In adults, a history of three or more mTBIs has been linked with impaired executive function, working memory, processing speed, and attention later in life (39, 40). However, the long-term cognitive effects of multiple mTBIs in children and young adults remains poorly understood, highlighting an important area for future research.
Advanced neuroimaging may be more apt than fluid biomarkers to predict cognitive impairments arising from altered brain network performance following mTBI. For example, volumetric abnormalities in grey and white matter structures are associated with greater cognitive difficulties after moderate–severe TBI in children (41). In adults affected by TBI, fMRI reveals hypo-connectivity within the default mode network (DMN) during performance of choice-reaction cognitive tasks, with a compensatory hyper-connectivity at rest (42). Using magnetic resonance spectroscopy (MRS), it has also been shown that frontal lobe gamma-aminobutyric acid (GABA) levels are associated with impaired working memory after mTBI (43), and subcortical levels of N-acetyl aspartate (NAA) are associated with cognitive outcomes up to 1 year after injury in children (44).
3.3 Psychiatric outcomes
According to parental reports, up to a quarter of young people experience significant psychological distress following mTBI (45). Children with mTBI are also more likely to exhibit internalising symptoms (e.g., anxiety, depression) and externalising symptoms (e.g., inattention, hyperactivity, aggression) compared to uninjured children (46). Longitudinal data suggest that the risk of affective and behavioural disorders, psychiatric hospitalisation, and self-harm may remain elevated for years following paediatric mTBI, compared to children with orthopaedic injuries (46, 47). Systematic reviews have found that a history of multiple mTBIs and pre-existing psychiatric illness are strong predictors of adverse psychiatric outcomes, and also highlight the importance of distinguishing between mental health symptoms and psychiatric diagnoses, noting that children with mTBI may experience symptoms which not reach diagnostic thresholds (46, 48).
There is currently limited evidence to suggest that fluid biomarkers can predict psychiatric outcomes following TBI in adults. For example, in a trial of targeted interventions for chronic psychological issues following TBI, response to treatment (measured by post-traumatic stress and overall psychological health) was predicted by composite pre-intervention serum levels of glial fibrillary acidic protein (GFAP), ubiquitin c-terminal hydrolase L1 (UCH-L1), von Willebrand factor (vWF), brain lipid-binding protein (BLBP), and vascular endothelial growth factor A (VEGF-A) (49). In terms of neuroimaging, structural abnormalities in frontal white matter are associated with novel psychiatric disorders up to 2 years after mTBI in children aged 5–14 years (50). Traumatic axonal injury (TAI) detected by diffusion tensor imaging (DTI) has been associated with psychiatric disorders following severe TBI (51), but fMRI and positron emission tomography (PET) detect alterations associated with new-onset depression and post-traumatic stress disorder (PTSD) following mTBI, with many of these studies being performed in young adults (52).
3.4 Social outcomes
Approximately one in eight children affected by mTBI experience persistently reduced health-related quality of life beyond one-year post-injury, and a subgroup do not return to full levels of participation in their community or school (53, 54). While a single mTBI is associated with only transiently reduced academic performance (55, 56) and no long-term effect on educational attainment, employment, or material standard of living (57), the effects of multiple mTBIs on social outcomes are not well understood. It is also important to consider whether conventional measures of these outcomes, such as academic performance, are sufficiently sensitive to injury-related impairments. Given that social disruption can have a significant and long-lasting effect on an individual’s life, further research into these outcomes is needed. Identifying robust associations between biomarkers and such complex outcomes may seem to be challenging. For example, a longitudinal study of structural brain development after mTBI in children aged 10–12 years found no differences in the thickness of cortical regions involved in social behaviour compared to uninjured controls (58). However, a recent study of military TBI in adults found that unemployment was associated with elevated plasma GFAP levels 8 years after injury (59). Further research is required to determine whether this relationship exists in paediatric mTBI cohorts.
3.5 Neurodegenerative outcomes
Numerous large meta-analyses have confirmed that a lifetime history of TBI is associated with a greater risk of dementia, although the risk associated with mTBI specifically remains unclear (60–63). Studies investigating the association between TBI and a post-mortem diagnosis of neurodegenerative disease have produced inconsistent findings (64). The neuropathological features of chronic traumatic encephalopathy (CTE) can be identified among former professional athletes and other individuals exposed to multiple mTBIs and repetitive head impacts (RHIs) (65–68). The duration of exposure to RHIs is associated with the extent of CTE pathology (69). However, the strength of this association is difficult to interpret in such highly selected cohorts, and the prevalence of individuals without CTE pathology after significant RHI exposure remains unclear (70, 71). Nevertheless, in one study, over 40% of brain donors aged under 30 with contact sports exposure displayed CTE pathology (72, 73). The paucity of human post-mortem material from children with RHI and mTBI limits our understanding of pathological changes in younger age groups. Including younger participants in prospective lifelong studies is therefore crucial to ensure that advances in the diagnosis and prediction of neurodegenerative outcomes are applicable across all age groups who may be at risk. Levels of hyperphosphorylated tau (p-tau) in the plasma and cerebrospinal fluid (CSF) are potential fluid biomarkers of Alzheimer’s disease (AD) and CTE (74, 75). The relation of neuroimaging biomarkers to CTE is also under investigation (76, 77).
4 Challenges in assessing and interpreting outcomes of paediatric mTBI
4.1 The impact of developmental stage and assessment timing
When assessing a paediatric population, it is essential to consider which outcomes are most relevant at different developmental stages, and to use age-appropriate assessment tools, as shown in Figure 2. In children, age at injury can significantly influence outcomes (13). Brain development is neither uniform nor linear, with different regions maturing at different rates at each developmental stage (i.e., peri-natal, infancy, pre-school, early childhood, middle childhood, late childhood, adolescence) (78). Adolescence, for example, is a time of complex neurobiological maturation (e.g., synaptic pruning, myelination) that coincides with fluctuating biological (e.g., hormonal) and psychosocial (e.g., identity formation) variables (79).
Relatively little is known about how the timing of brain injury affects these processes, or how this may differ between sexes (80–82). However, epidemiological studies support the notion that cognitive abilities are most vulnerable during critical periods of development (83). For example, infancy and middle childhood appear to be when intellectual and behavioural domains are most vulnerable to disruption by TBI, while injury during early childhood or adolescence may be more likely to affect executive function (84–88). To capture the evolution of outcomes across developmental milestones, and examine deviations as they progress over time, longitudinal studies with long follow-up periods will be needed.
4.2 Capturing the influence of other injury-independent factors
Clinical evaluation of injury severity is currently the mainstay of predicting adverse outcomes following mTBI (89). For instance, a higher initial symptom burden is associated with longer time to recovery (defined by return to usual activities) (13, 14, 90). However, a wide range of factors beyond injury severity can influence mTBI outcomes (17, 21). These modifying factors include the circumstances surrounding the injury, such as the degree of emotional distress experienced, as well as a wide range of injury-independent factors, including: (i) patient factors (e.g., age, developmental stage, sex, ethnicity, education, coping style, premorbid conditions and medical history) (13, 91, 92), (ii) management factors (e.g., rest, graduated return to activities, social isolation, screen time) (93–95), and (iii) environmental factors (e.g., socioeconomic status, peer relationships, family function, and other social determinants of health) (36, 96, 97).
The impact of these factors appears to accumulate over time, contributing to greater variability in cognitive, psychiatric, and social outcomes in studies with longer time since injury (21, 53, 97–99). Unless sufficiently accounted for, modifying factors are likely to confound any attempt to predict adverse outcomes following mTBI. This is particularly relevant to children and young adults, who face unique developmental challenges, often have less autonomy and capacity for self-advocacy, and may be more sensitive to environmental factors such as family functioning.
New approaches to TBI evaluation, such as the CBI-M framework, emphasise the importance of considering modifying factors at the initial assessment (100). While integrating clinical findings, biomarkers, and modifying factors entails a high degree of complexity, machine learning approaches are emerging as promising solutions (101, 102). However, further work is needed to identify the most influential modifying factors, which should then be systematically accounted for in studies seeking to validate predictive mTBI biomarkers, with reference to common data elements (21, 37, 103).
5 Discussion
While emerging biomarkers hold great promise for enhancing our ability to predict adverse outcomes following mTBI, careful consideration must first be given to selecting the outcome measures against which these emerging biomarkers are validated. To this end, future priorities include: (i) harmonising terminology used to describe brain injury and establishing consensus definitions and diagnostic criteria for prolonged recovery from mTBI through Delphi consensus processes; (ii) compiling a standardised set of accessible, comprehensive, and complementary outcome measure assessment tools, and (iii) developing effective methods to capture injury-independent factors in longitudinal study designs. Addressing these priorities will be essential to advance care and improve outcomes for young people affected by mTBI.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
JA: Visualization, Writing – original draft, Project administration, Conceptualization, Writing – review & editing. IL: Conceptualization, Writing – review & editing, Writing – original draft, Visualization. RF: Writing – review & editing, Writing – original draft, Conceptualization. CD: Conceptualization, Writing – review & editing, Writing – original draft. TT: Writing – original draft, Conceptualization, Writing – review & editing. LP: Visualization, Conceptualization, Writing – review & editing. MG: Writing – review & editing, Visualization, Conceptualization. RR: Conceptualization, Writing – review & editing. KS: Writing – review & editing, Conceptualization. JN: Conceptualization, Writing – review & editing. GD: Conceptualization, Writing – review & editing. TL: Writing – review & editing, Conceptualization, Supervision, Visualization, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. JA acknowledges funding from the MRC (MR/Y001850/1), IL acknowledges funding from the Podium Institute for Sports Medicine and Technology at the University of Oxford, RF acknowledges funding from the NIHR Efficacy and Mechanism Evaluation Programme, LP acknowledges funding from an NIHR Doctoral Research Fellowship (NIHR300741), and GD acknowledges funding from the NIHR Oxford BRC, UK MS Society, Oxford-Quinnipiac-Trinity Health Partnership, and Oxford University Clinical Academic Graduate School.
Acknowledgments
The authors would like to thank Sheikh Momin for reviewing the manuscript. Figures were created in BioRender (Figure 1: https://BioRender.com/b04f552, Figure 2: https://BioRender.com/z68i348).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
References
1. Menon, DK, Schwab, K, Wright, DW, and Maas, AI. Demographics and clinical assessment working Group of the International and Interagency Initiative toward common data elements for research on traumatic brain injury and psychological health. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. (2010) 91:1637–40. doi: 10.1016/j.apmr.2010.05.017
2. Hyder, AA, Wunderlich, CA, Puvanachandra, P, Gururaj, G, and Kobusingye, OC. The impact of traumatic brain injuries: a global perspective. Neuro Rehabilitation. (2007) 22:341–53. doi: 10.3233/NRE-2007-22502
3. Clark, D, Joannides, A, Adeleye, AO, Bajamal, AH, Bashford, T, Biluts, H, et al. Casemix, management, and mortality of patients receiving emergency neurosurgery for traumatic brain injury in the global Neurotrauma outcomes study: a prospective observational cohort study. Lancet Neurol. (2022) 21:438–49. doi: 10.1016/S1474-4422(22)00037-0
4. Silverberg, ND, Iverson, GL, Cogan, A, Dams-O-Connor, K, Delmonico, R, Graf, MJP, et al. The American congress of rehabilitation medicine diagnostic criteria for mild traumatic brain injury. Arch Phys Med Rehabil. (2023) 104:1343–55. doi: 10.1016/j.apmr.2023.03.036
5. Barlow, KM, Crawford, S, Stevenson, A, Sandhu, SS, Belanger, F, and Dewey, D. Epidemiology of postconcussion syndrome in pediatric mild traumatic brain injury. Pediatrics. (2010) 126:e374–81. doi: 10.1542/peds.2009-0925
6. Wilson, L, Newcombe, VFJ, Whitehouse, DP, Mondello, S, Maas, AIR, Menon, DK, et al. Association of early blood-based biomarkers and six-month functional outcomes in conventional severity categories of traumatic brain injury: capturing the continuous spectrum of injury. EBioMedicine. (2024) 107:105298. doi: 10.1016/j.ebiom.2024.105298
7. Manley, GT, Dams-O’Connor, K, Awwad, HO, Doperalski, A, Umoh, N, Maas, AIR, et al. Marking a new age in characterization of acute traumatic brain injury: the National Institute of Neurological Disorders and Stroke traumatic brain injury classification and nomenclature initiative. J Neurotrauma. (2025) 42:1021–e1242. doi: 10.1089/neu.2025.0134
8. Manley, GT, Dams-O’Connor, K, Alosco, ML, Awwad, HO, Bazarian, JJ, Bragge, P, et al. A new characterisation of acute traumatic brain injury: the NIH-NINDS TBI classification and nomenclature initiative. Lancet Neurol. (2025) 24:512–23. doi: 10.1016/S1474-4422(25)00154-1
9. FDA-NIH Biomarker Working Group. BEST (Biomarkers, Endpoint S, and other Tools) Resource. Silver Spring, MD: Food and Drug Administration (US) (2016).
10. Califf, RM. Biomarker definitions and their applications. Exp Biol Med (Maywood). (2018) 243:213–21. doi: 10.1177/1535370217750088
11. Wang, KK, Yang, Z, Zhu, T, Shi, Y, Rubenstein, R, Tyndall, JA, et al. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert Rev Mol Diagn. (2018) 18:165–80. doi: 10.1080/14737159.2018.1428089
12. Friberg, S, Lindblad, C, Zeiler, FA, Zetterberg, H, Granberg, T, Svenningsson, P, et al. Fluid biomarkers of chronic traumatic brain injury. Nat Rev Neurol. (2024) 20:671–84. doi: 10.1038/s41582-024-01024-z
13. Cuff, S, Maki, A, Feiss, R, Young, J, Shi, J, Hautmann, A, et al. Risk factors for prolonged recovery from concussion in young patients. Br J Sports Med. (2022) 56:1345–52. doi: 10.1136/bjsports-2022-105598
14. Putukian, M, Purcell, L, Schneider, KJ, Black, AM, Burma, JS, Chandran, A, et al. Clinical recovery from concussion-return to school and sport: a systematic review and meta-analysis. Br J Sports Med. (2023) 57:798–809. doi: 10.1136/bjsports-2022-106682
15. Kooper, CC, van der Zee, CW, Oosterlaan, J, Plötz, FB, and Königs, M. Prediction models for neurocognitive outcome of mild traumatic brain injury in children: a systematic review. J Neurotrauma. (2023) 40:1263–73. doi: 10.1089/neu.2022.0369
16. Patricios, JS, Schneider, KJ, Dvorak, J, Ahmed, OH, Blauwet, C, Cantu, RC, et al. Consensus statement on concussion in sport: the 6th international conference on concussion in sport–Amsterdam, October 2022. Br J Sports Med. (2023) 57:695–711. doi: 10.1136/bjsports-2023-106898
17. Barlow, KM. Postconcussion syndrome: a review. J Child Neurol. (2016) 31:57–67. doi: 10.1177/0883073814543305
18. Silverberg, ND, and Iverson, GL. Etiology of the post-concussion syndrome: Physiogenesis and psychogenesis revisited. Neuro Rehabilitation. (2011) 29:317–29. doi: 10.3233/NRE-2011-0708
19. Ewing-Cobbs, L, Cox, CS, Clark, AE, Holubkov, R, and Keenan, HT. Persistent Postconcussion symptoms after injury. Pediatrics. (2018) 142:e20180939. doi: 10.1542/peds.2018-0939
20. McKinlay, A, Dalrymple-Alford, JC, Horwood, LJ, and Fergusson, DM. Long term psychosocial outcomes after mild head injury in early childhood. J Neurol Neurosurg Psychiatry. (2002) 73:281–8. doi: 10.1136/jnnp.73.3.281
21. Beauchamp, MH, Dégeilh, F, and Rose, SC. Improving outcome after paediatric concussion: challenges and possibilities. Lancet Child Adolescent Health. (2023) 7:728–40. doi: 10.1016/S2352-4642(23)00193-1
22. McCauley, SR, Wilde, EA, Anderson, VA, Bedell, G, Beers, SR, Campbell, TF, et al. Recommendations for the use of common outcome measures in pediatric traumatic brain injury research. J Neurotrauma. (2012) 29:678–705. doi: 10.1089/neu.2011.1838
23. Goh, MSL, Looi, DSH, Goh, JL, Sultana, R, Goh, SSM, Lee, JH, et al. The impact of traumatic brain injury on neurocognitive outcomes in children: a systematic review and Meta-analysis. J Neurol Neurosurg Psychiatry. (2021) 92:847–53. doi: 10.1136/jnnp-2020-325066
24. Alsalaheen, B, Stockdale, K, Pechumer, D, and Broglio, SP. Validity of the immediate post concussion assessment and cognitive testing (ImPACT). Sports Med. (2016) 46:1487–501. doi: 10.1007/s40279-016-0532-y
25. Kuczynski, A, Crawford, S, Bodell, L, Dewey, D, and Barlow, KM. Characteristics of post-traumatic headaches in children following mild traumatic brain injury and their response to treatment: a prospective cohort. Dev Med Child Neurol. (2013) 55:636–41. doi: 10.1111/dmcn.12152
26. Ashina, H, Iljazi, A, Al-Khazali, HM, Ashina, S, Jensen, RH, Amin, FM, et al. Persistent post-traumatic headache attributed to mild traumatic brain injury: deep phenotyping and treatment patterns. Cephalalgia. (2020) 40:554–64. doi: 10.1177/0333102420909865
27. Scher, AI, McGinley, JS, Van Dam, LR, Campbell, AM, Chai, X, Collins, B, et al. Plasma calcitonin gene–related peptide and nerve growth factor as headache and pain biomarkers in recently deployed soldiers with and without a recent concussion. Headache J. Head Face Pain. (2023) 63:1240–50. doi: 10.1111/head.14635
28. Kamins, JL, Karimi, R, Hoffman, A, Prins, ML, and Giza, CC. Biomarkers and Endophenotypes of post-traumatic headaches. Curr Pain Headache Rep. (2024) 28:1185–93. doi: 10.1007/s11916-024-01255-1
29. Scotton, WJ, Botfield, HF, Westgate, CS, Mitchell, JL, Yiangou, A, and Uldall, MS. Headache classification Committee of the International Headache Society (IHS) the international classification of headache disorders. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
30. Ellis, MJ, Cordingley, D, Vis, S, Reimer, K, Leiter, J, and Russell, K. Vestibulo-ocular dysfunction in pediatric sports-related concussion. J Neurosurg Pediatr. (2015) 16:248–55. doi: 10.3171/2015.1.PEDS14524
31. Kaae, C, Cadigan, K, Lai, K, and Theis, J. Vestibulo-ocular dysfunction in mTBI: utility of the VOMS for evaluation and management - a review. Neuro Rehabilitation. (2022) 50:279–96. doi: 10.3233/NRE-228012
32. Crampton, A, Schneider, KJ, Grilli, L, Chevignard, M, Katz-Leurer, M, Beauchamp, MH, et al. Characterizing the evolution of oculomotor and vestibulo-ocular function over time in children and adolescents after a mild traumatic brain injury. Front Neurol. (2022) 13:904593. doi: 10.3389/fneur.2022.904593
33. Gagnon, I, Swaine, B, Friedman, D, and Forget, R. Visuomotor response time in children with a mild traumatic brain injury. J Head Trauma Rehabil. (2004) 19:391–404. doi: 10.1097/00001199-200409000-00004
34. Stephens, J, Salorio, C, Denckla, M, Mostofsky, S, and Suskauer, S. Subtle motor findings during recovery from pediatric traumatic brain injury: a preliminary report. J Mot Behav. (2017) 49:20–6. doi: 10.1080/00222895.2016.1204267
35. Chadwick, L, Peckham, SB, and Yeates, KO. Adult cognitive outcomes following childhood mild traumatic brain injury: a scoping review. J Head Trauma Rehabil. (2022) 37:285–92. doi: 10.1097/HTR.0000000000000782
36. Ware, AL, McLarnon, MJW, Lapointe, AP, Brooks, BL, Bacevice, A, Bangert, BA, et al. IQ after pediatric concussion. Pediatrics. (2023) 152:e2022060515. doi: 10.1542/peds.2022-060515
37. Babikian, T, and Asarnow, R. Neurocognitive outcomes and recovery after pediatric TBI: Meta-analytic review of the literature. Neuropsychology. (2009) 23:283–96. doi: 10.1037/a0015268
38. Karr, JE, Areshenkoff, CN, and Garcia-Barrera, MA. The neuropsychological outcomes of concussion: a systematic review of meta-analyses on the cognitive sequelae of mild traumatic brain injury. Neuropsychology. (2014) 28:321–36. doi: 10.1037/neu0000037
39. Frencham, KAR, Fox, AM, and Maybery, MT. Neuropsychological studies of mild traumatic brain injury: a meta-analytic review of research since 1995. J Clin Exp Neuropsychol. (2005) 27:334–51. doi: 10.1080/13803390490520328
40. Lennon, MJ, Brooker, H, Creese, B, Thayanandan, T, Rigney, G, Aarsland, D, et al. Lifetime traumatic brain injury and cognitive domain deficits in late life: the PROTECT-TBI cohort study. J Neurotrauma. (2023) 40:1423–435. doi: 10.1089/neu.2022.0360
41. Bourke, NJ, Demarchi, C, De Simoni, S, Samra, R, Patel, MC, Kuczynski, A, et al. Brain volume abnormalities and clinical outcomes following paediatric traumatic brain injury. Brain. (2022) 145:2920–34. doi: 10.1093/brain/awac130
42. Sharp, DJ, Beckmann, CF, Greenwood, R, Kinnunen, KM, Bonnelle, V, De Boissezon, X, et al. Default mode network functional and structural connectivity after traumatic brain injury. Brain. (2011) 134:2233–47. doi: 10.1093/brain/awr175
43. Friedman, SD, Poliakov, AV, Budech, C, Shaw, DW, Breiger, D, Jinguji, T, et al. GABA alterations in pediatric sport concussion. Neurology. (2017) 89:2151–6. doi: 10.1212/WNL.0000000000004666
44. Holshouser, B, Pivonka-Jones, J, Nichols, JG, Oyoyo, U, Tong, K, Ghosh, N, et al. Longitudinal metabolite changes after traumatic brain injury: a prospective pediatric magnetic resonance spectroscopic imaging study. J Neurotrauma. (2019) 36:1352–60. doi: 10.1089/neu.2018.5919
45. Brooks, BL, Plourde, V, Beauchamp, MH, Tang, K, Yeates, KO, Keightley, M, et al. Predicting psychological distress after pediatric concussion. J Neurotrauma. (2019) 36:679–85. doi: 10.1089/neu.2018.5792
46. Gornall, A, Takagi, M, Morawakage, T, Liu, X, and Anderson, V. Mental health after paediatric concussion: a systematic review and meta-analysis. Br J Sports Med. (2021) 55:1048–58. doi: 10.1136/bjsports-2020-103548
47. Ledoux, A-A, Webster, RJ, Clarke, AE, Fell, DB, Knight, BD, Gardner, W, et al. Risk of mental health problems in children and youths following concussion. JAMA Netw Open. (2022) 5:e221235. doi: 10.1001/jamanetworkopen.2022.1235
48. Emery, CA, Barlow, KM, Brooks, BL, Max, JE, Villavicencio-Requis, A, Gnanakumar, V, et al. A systematic review of psychiatric, psychological, and Behavioural outcomes following mild traumatic brain injury in children and adolescents. Can J Psychiatr. (2016) 61:259–69. doi: 10.1177/0706743716643741
49. Eagle, SR, Svirsky, SE, Puccio, AM, Borrasso, A, Edelman, K, Beers, S, et al. Predictive blood biomarkers of targeted intervention for chronic mental health symptoms following traumatic brain injury. J Neurotrauma. (2024) 42:e454–60. doi: 10.1089/neu.2024.0245
50. Max, JE, Friedman, K, Wilde, EA, Bigler, ED, Hanten, G, Schachar, RJ, et al. Psychiatric disorders in children and adolescents 24 months after mild traumatic brain injury. JNP. (2015) 27:112–20. doi: 10.1176/appi.neuropsych.13080190
51. Aldossary, NM, Kotb, MA, and Kamal, AM. Predictive value of early MRI findings on neurocognitive and psychiatric outcomes in patients with severe traumatic brain injury. J Affect Disord. (2019) 243:1–7. doi: 10.1016/j.jad.2018.09.001
52. Mayer, AR, and Quinn, DK. Neuroimaging biomarkers of new-onset psychiatric disorders following traumatic brain injury. Biol Psychiatry. (2022) 91:459–69. doi: 10.1016/j.biopsych.2021.06.005
53. Fineblit, S, Selci, E, Loewen, H, Ellis, M, and Russell, K. Health-related quality of life after pediatric mild traumatic brain injury/concussion: a systematic review. J Neurotrauma. (2016) 33:1561–8. doi: 10.1089/neu.2015.4292
54. Resch, C, Renaud, MI, Marzolla, MC, Catsman-Berrevoets, CE, and Lambregts, S. Participation 1.5 years after mild traumatic brain injury in children and adolescents. Dev Neurorehabil. (2024) 27:273–82. doi: 10.1080/17518423.2024.2398160
55. Russell, K, Hutchison, MG, Selci, E, Leiter, J, Chateau, D, and Ellis, MJ. Academic outcomes in high-school students after a concussion: a retrospective population-based analysis. PLoS One. (2016) 11:e0165116. doi: 10.1371/journal.pone.0165116
56. Rozbacher, A, Selci, E, Leiter, J, Ellis, M, and Russell, K. The effect of concussion or mild traumatic brain injury on school grades, National Examination Scores, and school attendance: a systematic review. J Neurotrauma. (2017) 34:2195–203. doi: 10.1089/neu.2016.4765
57. De Netto, RK, and McKinlay, A. Impact of childhood traumatic brain injury on educational outcomes and adult standard of living. Disabil Rehabil. (2020) 42:2444–50. doi: 10.1080/09638288.2019.1637948
58. Dégeilh, F, von Soest, T, Ferschmann, L, Beer, JC, Gaubert, M, Koerte, IK, et al. Social problems and brain structure development following childhood mild traumatic brain injury. Cortex. (2023) 162:26–37. doi: 10.1016/j.cortex.2023.02.003
59. Graham, NS, Blissitt, G, Zimmerman, K, Orton, L, Friedland, D, Coady, E, et al. Poor long-term outcomes and abnormal neurodegeneration biomarkers after military traumatic brain injury: the ADVANCE study. J Neurol Neurosurg Psychiatry. (2025) 96:105–13. doi: 10.1136/jnnp-2024-333777
60. Li, Y, Li, Y, Li, X, Zhang, S, Zhao, J, Zhu, X, et al. Head injury as a risk factor for dementia and Alzheimer’s disease: a systematic review and Meta-analysis of 32 observational studies. PLoS One. (2017) 12:e0169650. doi: 10.1371/journal.pone.0169650
61. Gu, D, Ou, S, and Liu, G. Traumatic brain injury and risk of dementia and Alzheimer’s disease: a systematic review and Meta-analysis. Neuroepidemiology. (2022) 56:4–16. doi: 10.1159/000520966
62. Gardner, RC, Bahorik, A, Kornblith, ES, Allen, IE, Plassman, BL, and Yaffe, K. Systematic review, Meta-analysis, and population attributable risk of dementia associated with traumatic brain injury in civilians and veterans. J Neurotrauma. (2023) 40:620–34. doi: 10.1089/neu.2022.0041
63. Mavroudis, I, Kazis, D, Petridis, FE, Balmus, I-M, Papaliagkas, V, and Ciobica, A. The association between traumatic brain injury and the risk of cognitive decline: an umbrella systematic review and Meta-analysis. Brain Sci. (2024) 14:1188. doi: 10.3390/brainsci14121188
64. Graham, NS, and Sharp, DJ. Understanding neurodegeneration after traumatic brain injury: from mechanisms to clinical trials in dementia. J Neurol Neurosurg Psychiatry. (2019) 90:1221–33. doi: 10.1136/jnnp-2017-317557
65. Brett, BL, Nader, AM, Kerr, ZY, Chandran, A, Walton, SR, DeFreese, JD, et al. Disparate associations of years of football participation and a metric of head impact exposure with neurobehavioral outcomes in former collegiate football players. J Int Neuropsychol Soc. (2022) 28:22–34. doi: 10.1017/S1355617721000047
66. Roberts, AL, Pascual-Leone, A, Speizer, FE, Zafonte, RD, Baggish, AL, Taylor, H, et al. Exposure to American football and neuropsychiatric health in former National Football League Players: findings from the football players health study. Am J Sports Med. (2019) 47:2871–80. doi: 10.1177/0363546519868989
67. Montenigro, PH, Alosco, ML, Martin, BM, Daneshvar, DH, Mez, J, Chaisson, CE, et al. Cumulative head impact exposure predicts later-life depression, apathy, executive dysfunction, and cognitive impairment in former high school and college football players. J Neurotrauma. (2017) 34:328–40. doi: 10.1089/neu.2016.4413
68. Bieniek, KF, Cairns, NJ, Crary, JF, Dickson, DW, Folkerth, RD, Keene, CD, et al. The second NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. J Neuropathol Exp Neurol. (2021) 80:210–9. doi: 10.1093/jnen/nlab001
69. McKee, AC, Stein, TD, Huber, BR, Crary, JF, Bieniek, K, Dickson, D, et al. Chronic traumatic encephalopathy (CTE): criteria for neuropathological diagnosis and relationship to repetitive head impacts. Acta Neuropathol. (2023) 145:371–94. doi: 10.1007/s00401-023-02540-w
70. Smith, DH, Johnson, VE, and Stewart, W. Chronic neuropathologies of single and repetitive TBI: substrates of dementia? Nat Rev Neurol. (2013) 9:211–21. doi: 10.1038/nrneurol.2013.29
71. Iverson, GL, Gardner, AJ, McCrory, P, Zafonte, R, and Castellani, RJ. A critical review of chronic traumatic encephalopathy. Neurosci Biobehav Rev. (2015) 56:276–93. doi: 10.1016/j.neubiorev.2015.05.008
72. McKee, AC, Stern, RA, Nowinski, CJ, Stein, TD, Alvarez, VE, Daneshvar, DH, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. (2013) 136:43–64. doi: 10.1093/brain/aws307
73. McKee, AC, Mez, J, Abdolmohammadi, B, Butler, M, Huber, BR, Uretsky, M, et al. Neuropathologic and clinical findings in Young contact sport athletes exposed to repetitive head impacts. JAMA Neurol. (2023) 80:1037–50. doi: 10.1001/jamaneurol.2023.2907
74. Turk, KW, Geada, A, Alvarez, VE, Xia, W, Cherry, JD, Nicks, R, et al. A comparison between tau and amyloid-β cerebrospinal fluid biomarkers in chronic traumatic encephalopathy and Alzheimer disease. Alz Res Therapy. (2022) 14:28. doi: 10.1186/s13195-022-00976-y
75. Miner, AE, Groh, JR, Tripodis, Y, Adler, CH, Balcer, LJ, Bernick, C, et al. Examination of plasma biomarkers of amyloid, tau, neurodegeneration, and neuroinflammation in former elite American football players. Alzheimers Dement. (2024) 20:7529–46. doi: 10.1002/alz.14231
76. Alosco, ML, Mariani, ML, Adler, CH, Balcer, LJ, Bernick, C, Au, R, et al. Developing methods to detect and diagnose chronic traumatic encephalopathy during life: rationale, design, and methodology for the DIAGNOSE CTE research project. Alz Res Therapy. (2021) 13:136. doi: 10.1186/s13195-021-00872-x
77. Bergauer, A, Van Osch, R, Van Elferen, S, Gyllvik, S, Venkatesh, H, and Schreiber, R. The diagnostic potential of fluid and imaging biomarkers in chronic traumatic encephalopathy (CTE). Biomed Pharmacother. (2022) 146:112602. doi: 10.1016/j.biopha.2021.112602
78. Mills, KL, Goddings, A-L, Clasen, LS, Giedd, JN, and Blakemore, S-J. The developmental mismatch in structural brain maturation during adolescence. Dev Neurosci. (2014) 36:147–60. doi: 10.1159/000362328
79. Casey, BJ, Getz, S, and Galvan, A. The adolescent brain. Dev Rev. (2008) 28:62–77. doi: 10.1016/j.dr.2007.08.003
80. Forsyth, RJ. Back to the future: rehabilitation of children after brain injury. Arch Dis Child. (2010) 95:554–9. doi: 10.1136/adc.2009.161083
81. Forsyth, R, and Kirkham, F. Predicting outcome after childhood brain injury. CMAJ. (2012) 184:1257–64. doi: 10.1503/cmaj.111045
82. Atkinson, TB, and Forsyth, RJ. It’s easier to relearn gross motor skills than learn them for the first time after injury: empirical evidence informing the age at injury debate. Eur J Paediatr Neurol. (2023) 47:67–71. doi: 10.1016/j.ejpn.2023.09.001
83. Ewing-Cobbs, L, Prasad, MR, Landry, SH, Kramer, L, and DeLeon, R. Executive functions following traumatic brain injury in Young children: a preliminary analysis. Dev Neuropsychol. (2004) 26:487–512. doi: 10.1207/s15326942dn2601_7
84. Anderson, V, Spencer-Smith, M, Leventer, R, Coleman, L, Anderson, P, Williams, J, et al. Childhood brain insult: can age at insult help us predict outcome? Brain. (2009) 132:45–56. doi: 10.1093/brain/awn293
85. Varier, S, Kaiser, M, and Forsyth, R. Establishing, versus maintaining, brain function: a neuro-computational model of cortical reorganization after injury to the immature brain. J Int Neuropsychol Soc. (2011) 17:1030–8. doi: 10.1017/S1355617711000993
86. Crowe, LM, Catroppa, C, Babl, FE, Rosenfeld, JV, and Anderson, V. Timing of traumatic brain injury in childhood and intellectual outcome. J Pediatr Psychol. (2012) 37:745–54. doi: 10.1093/jpepsy/jss070
87. Krasny-Pacini, A, Chevignard, M, Lancien, S, Escolano, S, Laurent-Vannier, A, De Agostini, M, et al. Executive function after severe childhood traumatic brain injury – age-at-injury vulnerability periods: the TGE prospective longitudinal study. Ann Phys Rehabil Med. (2017) 60:74–82. doi: 10.1016/j.rehab.2016.06.001
88. Resch, C, Anderson, VA, Beauchamp, MH, Crossley, L, Hearps, SJC, van Heugten, CM, et al. Age-dependent differences in the impact of paediatric traumatic brain injury on executive functions: a prospective study using susceptibility-weighted imaging. Neuropsychologia. (2019) 124:236–45. doi: 10.1016/j.neuropsychologia.2018.12.004
89. Dasic, D, Morgan, L, Panezai, A, Syrmos, N, Ligarotti, GKI, Zaed, I, et al. A scoping review on the challenges, improvement programs, and relevant output metrics for neurotrauma services in major trauma centers. Surg Neurol Int. (2022) 13:171. doi: 10.25259/SNI_203_2022
90. Zemek, R, Barrowman, N, Freedman, SB, Gravel, J, Gagnon, I, McGahern, C, et al. Clinical risk score for persistent Postconcussion symptoms among children with acute concussion in the ED. JAMA. (2016) 315:1014–25. doi: 10.1001/jama.2016.1203
91. Asarnow, RF, Newman, N, Weiss, RE, and Su, E. Association of Attention-Deficit/hyperactivity disorder diagnoses with pediatric traumatic brain injury: a Meta-analysis. JAMA Pediatr. (2021) 175:1009–16. doi: 10.1001/jamapediatrics.2021.2033
92. Maldonado, J, Huang, JH, Childs, EW, and Tharakan, B. Racial/ethnic differences in traumatic brain injury: pathophysiology, outcomes, and future directions. J Neurotrauma. (2023) 40:502–13. doi: 10.1089/neu.2021.0455
93. Asken, BM, Bauer, RM, Guskiewicz, KM, McCrea, MA, Schmidt, JD, Giza, CC, et al. Immediate removal from activity after sport-related concussion is associated with shorter clinical recovery and less severe symptoms in collegiate student-athletes. Am J Sports Med. (2018) 46:1465–74. doi: 10.1177/0363546518757984
94. Cairncross, M, Yeates, KO, Tang, K, Madigan, S, Beauchamp, MH, Craig, W, et al. Early Postinjury screen time and concussion recovery. Pediatrics. (2022) 150:e2022056835. doi: 10.1542/peds.2022-056835
95. Leddy, JJ, Burma, JS, Toomey, CM, Hayden, A, Davis, GA, Babl, FE, et al. Rest and exercise early after sport-related concussion: a systematic review and meta-analysis. Br J Sports Med. (2023) 57:762–70. doi: 10.1136/bjsports-2022-106676
96. Venturini, S, Still, MEH, Hutchinson, PJ, and Gwinnutt, JM. Is pre-injury socioeconomic status associated with outcomes in patients with traumatic brain injury? A Systematic Review. J Neurotrauma. (2024) 41:789–806. doi: 10.1089/neu.2022.0341
97. Hunt, TN, Roberts, K, Taylor, EM, Quintana, CP, and Kossman, MK. The effect of social determinants of health on clinical recovery following concussion: a systematic review. J Sport Rehabil. (2024) 34:28–36. doi: 10.1123/jsr.2023-0068
98. Anderson, V, Godfrey, C, Rosenfeld, JV, and Catroppa, C. Predictors of cognitive function and recovery 10 years after traumatic brain injury in Young children. Pediatrics. (2012) 129:e254–61. doi: 10.1542/peds.2011-0311
99. Beauchamp, MH, Aglipay, M, Yeates, KO, Désiré, N, Keightley, M, Anderson, P, et al. Predictors of neuropsychological outcome after pediatric concussion. Neuropsychology. (2018) 32:495–508. doi: 10.1037/neu0000419
100. NINDS TBI Classification and Nomenclature Workshop|National Institute of Neurological Disorders and Stroke. Available online at: https://www.ninds.nih.gov/news-events/events/ninds-tbi-classification-and-nomenclature-workshop (accessed September 28, 2024).
101. Iyer, KK, Zalesky, A, Barlow, KM, and Cocchi, L. Default mode network anatomy and function is linked to pediatric concussion recovery. Annal. Clin Transl Neurol. (2019) 6:2544–54. doi: 10.1002/acn3.50951
102. Fedorchak, G, Rangnekar, A, Onks, C, Loeffert, AC, Loeffert, J, Olympia, RP, et al. Saliva RNA biomarkers predict concussion duration and detect symptom recovery: a comparison with balance and cognitive testing. J Neurol. (2021) 268:4349–61. doi: 10.1007/s00415-021-10566-x
Keywords: paediatric mild traumatic brain injury, prognostic biomarkers, validation, outcomes assessment, neurodevelopment
Citation: Attwood JE, Lövgren I, Forsyth R, Demarchi C, Thayanandan T, Prisco L, Ganau M, Roberts R, Scarff K, Newton JL, DeLuca GC and Lawrence T (2025) Selecting outcome measures to validate prognostic biomarkers of paediatric mild traumatic brain injury: challenges and priorities. Front. Neurol. 16:1620178. doi: 10.3389/fneur.2025.1620178
Edited by:
Karen L. Lankford, Yale University, United StatesReviewed by:
Kryshawna Beard, Traumatic Brain Injury Center of Excellence, United StatesFares Komboz, University Medical Center Göttingen, Germany
Copyright © 2025 Attwood, Lövgren, Forsyth, Demarchi, Thayanandan, Prisco, Ganau, Roberts, Scarff, Newton, DeLuca and Lawrence. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonathan E. Attwood, am9uYXRoYW4uYXR0d29vZEBuZGNuLm94LmFjLnVr; Tim Lawrence, dGltLmxhd3JlbmNlQG5kY24ub3guYWMudWs=