 Aydın Talip Yıldoğan1*
Aydın Talip Yıldoğan1* Ramazan Şencan2Gizem Türker Yıldoğan3Gözde Öngün4
Ramazan Şencan2Gizem Türker Yıldoğan3Gözde Öngün4 Bekir Sıtkı Said Ulusoy5Fettah Eren6Abdurrahman Neyal7
Bekir Sıtkı Said Ulusoy5Fettah Eren6Abdurrahman Neyal7- 1Department of Neurology, Faculty of Medicine, Nigde Omer Halis Demir University, Nigde, Türkiye
- 2Neurology Clinic, Gaziantep 25 Aralık State Hospital, Gaziantep, Türkiye
- 3Department of Biochemistry, Faculty of Medicine, Gaziantep University, Gaziantep, Türkiye
- 4Neurology Clinic, İstinye University Hospital, Istanbul, Türkiye
- 5Radiology Clinic, Gaziantep City Hospital, Gaziantep, Türkiye
- 6Department of Neurology, Faculty of Medicine, Selcuk University, Konya, Türkiye
- 7Department of Neurology, Faculty of Medicine, GIBTU University, Gaziantep, Türkiye
Background: This study aimed to investigate the association between the monocyte-to-high density lipoprotein (HDL) cholesterol ratio (MHR) and the presence and severity of white matter hyperintensities (WMHs) in patients with migraine.
Methods: A total of 153 patients diagnosed with migraine and 90 age- and sex-matched healthy controls were included. Serum monocyte and HDL levels, and MRI findings were evaluated. WMHs severity was graded using the Fazekas scale. Serum parameters were compared and evaluated between the patient and control groups. In addition, the relationship between migraine clinical characteristics and MHR levels was examined.
Results: MHR values were significantly higher in migraine patients than in controls (p < 0.001). Higher Fazekas scores were associated with increased MHR and monocyte levels, and decreased HDL levels. Receiver operating characteristic (ROC) analysis indicated that an MHR > 13.37 predicted the presence of WMHs with 88.50% sensitivity and 98% specificity (AUC = 0.918, p < 0.001).
Conclusion: MHR appears to be a promising inflammatory biomarker reflecting cerebral microvascular changes in migraine patients, even among young adults. These results support the contribution of low-grade systemic inflammation to migraine-associated white matter lesions.
Introduction
Migraine is a prevalent primary headache disorder influenced by both genetic and environmental factors. It is now widely accepted as a neurovascular condition, with activation of the trigeminovascular pain pathway that has a central role in its pathophysiology (1, 2).
Although brain imaging is typically normal in most migraine patients, white matter hyperintensities (WMHs) are frequently observed, especially on magnetic resonance imaging (MRI) (3, 4). WMHs are among the most common structural abnormalities in the white matter, usually detecting as small, punctate, non-mass lesions on T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences (5).
The exact pathogenesis of WMHs remains unclear, but they are believed to result from chronic ischemic processes linked to small vessel disease. In addition, WMHs are known to increase with aging (6, 7). Several recent studies have detected that WMHs are significantly more prevalent in migraine patients compared to healthy individuals (3, 4, 8). Although migraine subtype, disease duration, and attack frequency have been suggested as factors that may contribute to the occurrence and burden of WMH in migraine patients, the findings are not conclusive (3, 9).
Proposed mechanisms underlying WMH formation in migraine include regional hypoperfusion, ischemic microvascular injury, hypercoagulability, and endothelial dysfunction (10, 11). Oxidative stress, present during both ictal and interictal periods, may also contribute to WMH development (3, 12).
The monocyte-to-HDL cholesterol ratio (MHR) has recently been reported as a novel biomarker of inflammation and endothelial dysfunction. Higher MHR indicates a pro-inflammatory and pro-atherogenic state and it is associated with various conditions such as coronary artery disease, ischemic stroke, and schizophrenia (13–15). Based on the relationship between MHR and vascular dysfunction, it has been suggested that MHR may be a potential biomarker in migraine. However, MHR is not only associated with migraine; it is also linked to systemic inflammatory and cardiometabolic states, including insulin resistance and increased cardiovascular risk in rheumatoid arthritis and the inflammatory processes observed in gout (16, 17). It was reported that there was an association between MHR and WMHs in migraine patients, and that a positive correlation was also detected with Visual Analog Scale (VAS) and Migraine Disability Assessment Scale (MIDAS) scores (18). Similarly, Increased MHR was significantly associated with cerebral small vessel disease markers, including WMHs, lacunes, and microbleeds (19).
Although the Fazekas scale is widely used for semiquantitative WMH assessment few studies have explored the relationship between MHR and WMH in migraine populations (5). WMHs severity using the Fazekas classification was evaluated in our study. In addition, the relationship between this score and serum parameters were evaluated in migraine.
This study aimed to evaluate the association between MHR and WMH severity using Fazekas scale in patients with migraine. We sought to elucidate the inflammatory and vascular mechanisms contributing to migraine pathophysiology.
Materials and methods
Study design and population
This cross-sectional observational study was conducted from May 1, 2024, to November 1, 2024, at the Neurology Department of Dr. Ersin Arslan Training and Research Hospital. A total of 153 patients diagnosed with migraine according to the International Headache Society (IHS) criteria and 90 healthy controls were included (20). Inclusion criteria for this study were age between 18 and 65 years, anddiagnosis of migraine based on IHS criteria. Exclusion criteria were determined as history of hypertension, diabetes, stroke, or cardiovascular disease; renal, endocrine, or metabolic disorders; central nervous system (CNS) disease or malignancy; smoking; pregnancy, alcohol or substance use; and the last inability to complete assessments due to sociocultural or cognitive limitations. The control group was recruited from hospital volunteers during the same study period. Participants with a confirmed migraine diagnosis were included in the migraine group, and those with a migraine diagnosis were excluded from the control group. Beyond this distinction, the same inclusion and exclusion criteria were applied to both groups. Controls were matched with migraine patients by gender, age and body mass index (BMI). Most of the controls presented with nonspecific, mild complaints such as tension-type headache or transient dizziness that did not meet migraine criteria, and subsequent evaluations revealed no underlying organic pathology.
Clinical and demographic assessment
All migraine patients completed a structured headache questionnaire and the MIDAS scale (21). Clinical data included headache type, duration, frequency, and aura status. Control subjects were matched by age and gender.
Neuroimaging protocol
All participants underwent brain MRI using a 1.5 Tesla scanner (Siemens, Germany). WMHs were evaluated on axial FLAIR sequences. Imaging was interpreted by a neuroradiologist blinded to the clinical and laboratory data. WMH severity was graded using the Fazekas scale. Fazekas scalewere grouped as Fazekas 0: No lesions; Fazekas 1: Mild lesions; Fazekas 2: Moderate lesions; Fazekas 3: Large confluent areas (5).
Serum assessment
Venous blood samples were collected to determine: All these parameters were detected monocyte count (cells/μL), HDL cholesterol (mg/dL) and MHR was calculated with formulation as (monocyte count/HDL). Additional parameters included complete blood count, C reactive protein (CRP), glucose, triglycerides, and low-density lipoprotein (LDL) cholesterol.
Statistical analysis
Data were analyzed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA) and MedCalc software. Continuous variables were expressed as mean ± standard deviation or median (interquartile range), and categorical variables as counts and percentages. Normality was assessed using the Shapiro–Wilk test. The Mann–Whitney U and Kruskal-Wallis tests were used for between-group comparisons. Chi-square tests were used for categorical data. Receiver operating characteristic (ROC) curves analyses were constructed for MHR, and optimal cut-off values were calculated. Binary and multinomial logistic regression analyses were performed to evaluate the impact of variables on WMH presence and severity. A p-value <0.05 was considered statistically significant.
Results
Clinical and laboratory characteristics
There were no significant differences between migraine patients (n = 153) and healthy controls (n = 90) in terms of age, sex, BMI, lymphocyte and neutrophil counts, glucose, LDL, hemoglobin, platelet count, or CRP levels (p > 0.05). However, monocyte count, HDL, MHR, triglycerides, and WBC levels showed significant differences (p < 0.05). Migraine patients had higher monocyte counts, MHR, triglyceride levels, and WBCs, while HDL levels were higher in the control group (Table 1).

Table 1. Clinical and laboratory characteristics of patients and controls.
Clinical and laboratory parameters according to Fazekas score
Migraine patients were categorized into three groups based on WMH severity (Fazekas 0, 1, and 2). No significant differences were found among these groups in terms of age, BMI, lymphocyte/neutrophil counts, glucose, LDL, WBC, hemoglobin, platelet count, CRP, or headache duration (p > 0.05). However, monocyte count, HDL, MHR, and aura status differed significantly across the groups (p < 0.05) (Table 2).

Table 2. Clinical and laboratory parameters by Fazekas score.
Monocyte count and MHR were positive correlated with Fazekas scores (p < 0.001, r = 0.496). HDL levels were negative correlated with Fazekas scores (p < 0.001, r = −0.512). Aura was more common in patients with higher Fazekas scores (p < 0.001).
WMH presence vs. absence
Patients were divided into WMH-negative (Fazekas 0) and WMH-positive (Fazekas 1 + 2) groups. No differences were observed in age, BMI, headache duration, lymphocyte/neutrophil counts, glucose, LDL, triglycerides, WBC, hemoglobin, platelet count, or CRP (p > 0.05). However, monocyte count, HDL, MHR, and aura status showed significant differences (p < 0.05) (Table 3).
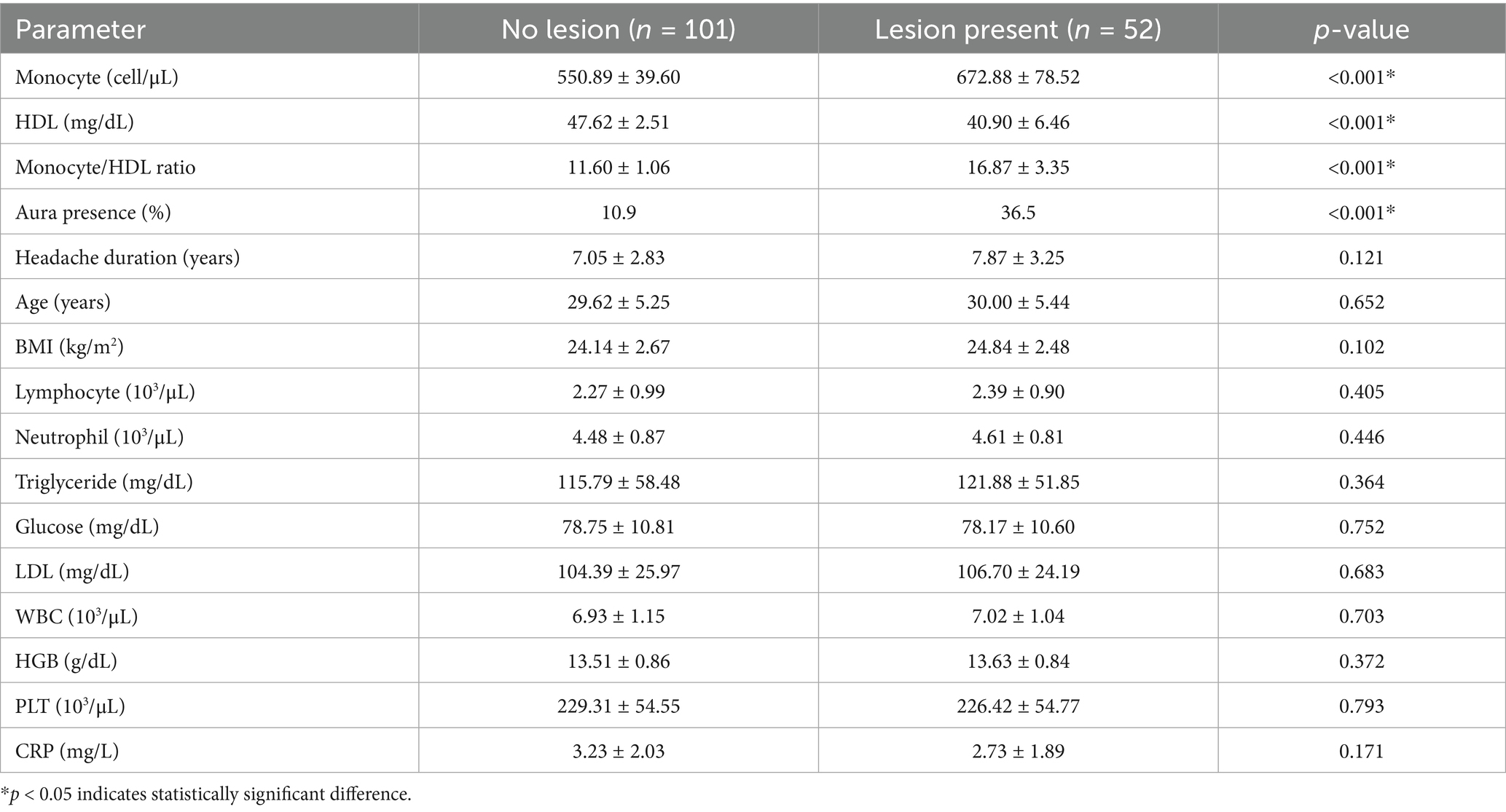
Table 3. Clinical and laboratory characteristics of migraine patients with and without lesions.
WMH-positive patients had higher monocyte counts and MHR (p < 0.001). HDLwas lower in WMH-positive patients (p < 0.001). Aura was more frequent in the WMH-positive group (p < 0.001).
Receiver operating characteristic analysis
An ROC analysis was performed to assess the predictive value of the monocyte-to-HDL cholesterol ratio (MHR) for WMH presence. The ROC curve (Figure 1) demonstrated an area under the curve (AUC) of 0.918 (95% confidence interval: 0.851–0.984; p < 0.001), with a sensitivity of 88.50% and specificity of 98.00% at an optimal MHR cut-off point of 13.37. These results suggest that MHR may serve as a reliable biomarker for identifying WMH in migraine patients.

Figure 1. Receiver operating characteristic (ROC) curve showing the predictive accuracy of the monocyte-to-HDL cholesterol ratio (MHR) for the presence of white matter hyperintensities (WMH). The blue curve represents the diagnostic performance of the MHR in predicting WMH, while the diagonal orange line indicates the no-discrimination reference line (chance level). The optimal cut-off point was 13.37, the area under the curve (AUC) was 0.918 (95% confidence interval: 0.851–0.984; p < 0.001), the sensitivity was 88.50%, and the specificity was 98.00%.
Logistic regression analysis
Longer disease duration was significantly associated with Fazekas 1 grade. Higher MHR levels were significantly associated with increasing WMH severity. Age and sex were also included as covariates in the regression analyses but did not reach statistical significance. Both binary and multiple logistic regression models were statistically significant (p < 0.01) (Table 4).

Table 4. Analysis of regression models according to the Fazekas scale in migraine patients.
Discussion
This study examined the association between the monocyte-to-HDL cholesterol ratio (MHR) and white matter hyperintensities (WMHs) in migraine patients. Our results demonstrated that MHR was significantly higher in migraine patients compared to healthy controls and a positive correlation was observed with both the presence and severity of WMHs. Higher Fazekas scores were associated with increased MHR values, indicating a potential link between systemic inflammation and cerebral microangiopathy in migraine.
These findings are consistent with Ulusoy et al. (18) who reported a positive correlation between MHR and WMHs in migraine patients. Similarly, Nam et al. (19) reported an association between elevated MHR and cerebral small vessel disease markers, including WMHs, lacunes, and microbleeds. Our findings extend this association to a younger cohort (mean age ~29.5 years), suggesting that inflammation-related cerebral changes may occur even in early adulthood. Additionally, Schramm et al. (22) reported that in an older population-based cohort (mean age 60.9 ± 13 years), a significant association between headache history and WMH volume was observed in women but not in men. In contrast, our cohort was significantly younger (migraine: 29.7 ± 5.3 years; control: 29.0 ± 5.2 years) and free of vascular comorbidities such as hypertension, diabetes, or cardiovascular disease; these were applied as exclusion criteria rather than statistical covariates. Sex-stratified analyses in our sample showed a significantly higher prevalence of WMHs in both female and male migraineurs compared with controls. These findings suggest that, in contrast to the female-specific association observed by Schramm et al. (22) migraine may be associated with increased WMH burden in both sexes in younger, healthy populations. However, the absence of WMHs in our healthy control group limits our ability to disentangle the relative contribution of gender and migraine to WMH occurrence, and future studies with larger participants and more diverse cohorts are required.
In contrast, Tekeşin and Tunç (23) did not reported a significant association between MHR and WMHs in migraine. However, methodological limitations, including the absence of Fazekas grading or confounder adjustment, may explain these results.
Monocytes contribute to inflammation and endothelial activation, while HDL has anti-inflammatory and antioxidant features (24, 25). Thus, an elevated MHR represents a pro-inflammatory state conducive to cerebral microvascular damage (18, 19). It’s important to note that elevated MHR may not be specific to migraine. Previous studies have shown increased MHR levels in systemic inflammatory and cardiometabolic disorders, particularly rheumatoid arthritis, which is associated with insulin resistance and cardiovascular risk, and gout, which is characterized by chronic inflammation. Therefore, elevated MHR in migraineurs may reflect not only migraine-related mechanisms but also broader systemic inflammatory activity (16, 17).
Longitudinal studies have shown that WMHs in migraine patients may progress over time (26–29). Identifying MHR as a marker of WMH burden may enable early detection of microvascular involvement and inform long-term management strategies.
The strengths of this study are as follows: First, the use of Fazekas-based MRI evaluation; second, exclusion of major comorbidities, and comprehensive inflammatory diseases. Third, WMH-related inflammation was evident even in young adults without overt systemic disease.
Limitations of study
First, the cross-sectional design, which precludes causal inferences. Second, unmeasured factors such as diet or genetics may influence MHR levels. Additionally, lesion location, morphometric features, and the presence of cerebral microbleeds or lacunes were not analyzed and broader inflammatory markers (e.g., IL-6, TNF-α) were not included. Finally, none of the healthy controls, male or female, exhibited Fazekas ≥1 WMH, likely reflecting the younger age and absence of vascular comorbidities in this group. Consequently, although we observed a significantly higher WMH burden in migraineurs of both sexes, our ability to determine the relative contribution of the migraine-sex relationship to WMH occurrence was limited. Larger, older control cohorts will be needed to clarify these sex-specific associations. The p-value of 0.005 obtained for Hosmer-Lemeshow in Table 4 may indicate a statistical limitation in model calibration. This finding may be related to statistical sensitivity arising from the strong association between MHR and Fazekas score and is noted as a methodological limitation. Additionally, Correction for Multiple Comparisons was not applied in this study, which is a methodological limitation.
Conclusion
MHR is significantly associated with the presence and severity of WMHs in migraine patients. Higher Fazekas scores associated with higher MHR and monocyte levels and lower HDL levels. An MHR > 13.37 strongly predicted WMH presence with high sensitivity and specificity. These results suggest that MHR may serve as a feasible and accessible biomarker for identifying microvascular involvement in migraine, even among younger patients. Further prospective studies are needed to validate its clinical applicability.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was obtained from the Clinical Research Ethics Committee of Gaziantep University (date: 17.04.2024, no: 2024/109). All participants provided written informed consent prior to enrollment. The study was conducted in accordance with local legislation and institutional requirements.
Author contributions
AY: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. RŞ: Supervision, Writing – review & editing. GY: Formal analysis, Investigation, Writing – review & editing. GÖ: Conceptualization, Writing – original draft. BU: Data curation, Writing – review & editing. FE: Writing – review & editing. AN: Data curation, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ashina, M, Katsarava, Z, Do, TP, Buse, DC, Pozo-Rosich, P, Özge, A, et al. Migraine: epidemiology and systems of care. Lancet. (2021) 397:1485–95. doi: 10.1016/S0140-6736(20)32160-7
2. Dodick, DW. A phase-by-phase review of migraine pathophysiology. Headache. (2018) 58:4–16. doi: 10.1111/head.13300,
3. Al-Hashel, JY, Alroughani, R, Gad, K, Al-Sarraf, L, and Ahmed, SF. Risk factors of white matter hyperintensities in migraine patients. BMC Neurol. (2022) 22:159. doi: 10.1186/s12883-022-02680-8,
4. Negm, M, Housseini, AM, Abdelfatah, M, and Asran, A. Relation between migraine pattern and white matter hyperintensities in brain magnetic resonance imaging. Egypt J Neurol Psych Neurosurg. (2018) 54:24. doi: 10.1186/s41983-018-0027-x,
5. Fazekas, F, Chawluk, JB, Alavi, A, Hurtig, HI, and Zimmerman, RA. MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging. Am J Roentgenol. (1987) 149:351–6. doi: 10.2214/ajr.149.2.351,
6. Dupré, N, Drieu, A, and Joutel, A. Pathophysiology of cerebral small vessel disease: a journey through recent discoveries. J Clin Invest. (2024) 134:1–13. doi: 10.1172/JCI172841,
7. Wardlaw, J. M., Valdés Hernández, M. C., and Muñoz-Maniega, S. What are white matter hyperintensities made of? Relevance to vascular cognitive impairment. J Am Heart Assoc (2015). 4:e001140. doi: 10.1161/JAHA.114.001140
8. Dobrynina, LA, Suslina, AD, Gubanova, MV, Belopasova, AV, Sergeeva, AN, Evers, S, et al. White matter hyperintensity in different migraine subtypes. Sci Rep. (2021) 11:10881. doi: 10.1038/s41598-021-90341-0,
9. Gaist, D, Garde, E, Blaabjerg, M, Nielsen, HH, Krøigård, T, Østergaard, K, et al. Migraine with aura and risk of silent brain infarcts and white matter hyperintensities: an MRI study. Brain. (2016) 139:2015–23. doi: 10.1093/brain/aww099,
10. Tietjen, GE, and Collins, SA. Hypercoagulability and migraine. Headache. (2018) 58:173–83. doi: 10.1111/head.13044,
11. Zhang, W, Cheng, Z, Fu, F, and Zhan, Z. Prevalence and clinical characteristics of white matter hyperintensities in migraine: a meta-analysis. Neuroimage. (2023) 37:103312. doi: 10.1016/j.nicl.2023.103312,
12. Sparaco, M, Feleppa, M, Lipton, RB, Rapoport, AM, and Bigal, ME. Mitochondrial dysfunction and migraine: evidence and hypotheses. Cephalalgia. (2006) 26:361–72. doi: 10.1111/j.1468-2982.2005.01059.x
13. Bolayir, A, Gokce, SF, Cigdem, B, Bolayir, HA, Yildiz, OK, Bolayir, E, et al. Monocyte/high-density lipoprotein ratio predicts the mortality in ischemic stroke patients. Neurol Neurochir Pol. (2018) 52:150–5. doi: 10.1016/j.pjnns.2017.08.011,
14. Canpolat, U, Çetin, EH, Cetin, S, Aydin, S, Akboga, MK, Yayla, C, et al. Association of Monocyte-to-HDL cholesterol ratio with slow coronary flow is linked to systemic inflammation. Clin Appl Thromb Hemost. (2016) 22:476–82. doi: 10.1177/1076029615594002,
15. Sahpolat, M, Ayar, D, Ari, M, and Karaman, MA. Elevated monocyte to high-density lipoprotein ratios as an inflammation markers for schizophrenia patients. Clin Psychopharmacol. Neurosci. (2021) 19:112–6. doi: 10.9758/cpn.2021.19.1.112,
16. Romo-Cordero, A, González-Sierra, M, Quevedo-Abeledo, JC, Quevedo-Rodríguez, A, Gómez-Bernal, F, de Vera-González, A, et al. The ratio of monocytes to HDL-cholesterol is associated with cardiovascular risk and insulin resistance in patients with rheumatoid arthritis. Life. (1995) 2023, 13:1–11. doi: 10.3390/life13101995
17. Mi, L, He, X, Gao, J, and Xu, K. Monocyte-to-HDL cholesterol ratio (MHR) as a novel Indicator of gout risk. Sci Rep. (2025) 15:12188. doi: 10.1038/s41598-025-97373-w,
18. Ulusoy, EK. Correlations between the monocyte to high-density lipoprotein cholesterol ratio and white matter hyperintensities in migraine. Neurol Res. (2020) 42:126–32. doi: 10.1080/01616412.2019.1710406,
19. Nam, KW, Kwon, HM, Jeong, HY, Park, JH, and Min, K. Monocyte to high-density lipoprotein cholesterol ratio is associated with cerebral small vessel diseases. BMC Neurol. (2024) 24:18. doi: 10.1186/s12883-023-03524-9,
20. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
21. Stewart, WF, Lipton, RB, Dowson, AJ, and Sawyer, J. Development and testing of the migraine disability assessment (MIDAS) questionnaire to assess headache-related disability. Neurology. (2001) 56:S20–8. doi: 10.1212/WNL.56.suppl_1.S20
22. Schramm, SH, Tenhagen, I, Jokisch, M, Gronewold, J, Moebus, S, Caspers, S, et al. Migraine or any headaches and white matter hyperintensities and their progression in women and men. J Headache Pain. (2024) 25:78. doi: 10.1186/s10194-024-01782-7,
23. Tekeşin, A, and Tunç, A. Evaluation of inflammatory markers in patients with migraine. Arch. Clin. Exp. Med. (2019) 4:37–40. doi: 10.25000/acem.494415
24. Greco, R, Bighiani, F, Demartini, C, Zanaboni, A, Francavilla, M, Facchetti, R, et al. Expression of miR-155 in monocytes of people with migraine: association with phenotype, disease severity and inflammatory profile. J Headache Pain. (2024) 25:138. doi: 10.1186/s10194-024-01842-y
25. Uygur-Kucukseymen, E, and Akca, G. Serum lipid profile in migraine and its association with clinical characteristics. Neurol Res. (2023) 45:57–61. doi: 10.1080/01616412.2022.2119723,
26. Biscetti, L, De Vanna, G, Cresta, E, Bellotti, A, Corbelli, I, Letizia Cupini, M, et al. Immunological findings in patients with migraine and other primary headaches: a narrative review. Clin Exp Immunol. (2022) 207:11–26. doi: 10.1093/cei/uxab025,
27. Erdélyi-Bótor, S, Aradi, M, Kamson, DO, Kovács, N, Perlaki, G, Orsi, G, et al. Changes of migraine-related white matter hyperintensities after 3 years: a longitudinal MRI study. Headache. (2015) 55:55–70. doi: 10.1111/head.12459,
28. Ha, WS, and Chu, MK. Altered immunity in migraine: a comprehensive scoping review. J Headache Pain. (2024) 25:95. doi: 10.1186/s10194-024-01800-8,
Keywords: migraine, white matter hyperintensities, Fazekas scale, monocyte-to-HDL ratio (MHR), inflammation
Citation: Yıldoğan AT, Şencan R, Yıldoğan GT, Öngün G, Ulusoy BSS, Eren F and Neyal A (2025) Association between monocyte-to-HDL ratio and Fazekas-scaled white matter hyperintensities in migraine patients: a cross-sectional MRI-based study. Front. Neurol. 16:1664839. doi: 10.3389/fneur.2025.1664839
Edited by:
Claudia Altamura, Fondazione Policlinico Campus Bio-Medico, ItalyReviewed by:
Lars Neeb, Brandenburg Medical School Theodor Fontane, GermanyDaniel Tozer, University of Cambridge, United Kingdom
Hongtao Li, Eastern Mennonite University, United States
Copyright © 2025 Yıldoğan, Şencan, Yıldoğan, Öngün, Ulusoy, Eren and Neyal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aydın Talip Yıldoğan, eWlsZG9nYW5heWRpbnRhbGlwQGdtYWlsLmNvbQ==