 Xiaoying Zhang
Xiaoying Zhang Jianjun Li1,2,3,4,5*
Jianjun Li1,2,3,4,5*- 1School of Rehabilitation Medicine, Capital Medical University, Beijing, China
- 2Beijing Key Laboratory of Neural Injury and Rehabilitation, China Rehabilitation Research Center, Beijing, China
- 3Center of Neural Injury and Repair, Beijing Institute for Brain Disorders, Beijing, China
- 4Department of Psychology, Music Therapy Center, China Rehabilitation Research Center, Beijing, China
- 5Chinese Institute of Rehabilitation Science, Beijing, China
- 6Key Laboratory of Behavioral Science, Institute of Psychology, Chinese Academy of Sciences (CAS), Beijing, China
- 7Departments of Psychology, University of Chinese Academy of Sciences, Beijing, China
Melodic intonation therapy (MIT) is a melodic musical training method that could be combined with language rehabilitation. However, some of the existing literature focuses on theoretical mechanism research, while others only focus on clinical behavioral evidence. Few clinical experimental studies can combine the two for behavioral and mechanism analysis. This review aimed at systematizing recent results from studies that have delved explicitly into the MIT effect on non-fluent aphasia by their study design properties, summarizing the findings, and identifying knowledge gaps for future work. MIT clinical trials and case studies were retrieved and teased out the results to explore the validity and relevance of these results. These studies focused on MIT intervention for patients with non-fluent aphasia in stroke recovery period. After retrieving 128 MIT-related articles, 39 valid RCT studies and case reports were provided for analysis. Our summary shows that behavioral measurements at MIT are excessive and provide insufficient evidence of MRI imaging structure. This proves that MIT still needs many MRI studies to determine its clinical evidence and intervention targets. The strengthening of large-scale clinical evidence of imaging observations will result in the clear neural circuit prompts and prediction models proposed for the MIT treatment and its prognosis.
Introduction
Aphasia is a language disorder generally caused by stroke-related damage to the dominant hemisphere. It describes a multitude of acquired language impairment as a consequence of brain damage (Go et al., 2014; WHO, 2015; Benjamin et al., 2017; Koleck et al., 2017). In relation to localization, it is possible to make a division between fluent and non-fluent aphasia. Oral expression of non-fluent aphasia is characterized by low speech volume, lack of grammar, and pronunciation dysphonia. According to the American Hearing Language Association's classification of aphasia, the types of non-fluent aphasia include motor aphasia, complete aphasia, transcortical motor aphasia, and transcortical mixed aphasia (Kim et al., 2016; Gerstenecker and Lazar, 2019; Hoover, 2019). According to the survey data from WHO on stroke prevention in 2019, about 2.6 to 4.7 million people suffer from stroke-related aphasia yearly, significantly impacting their quality of life (WHO, 2015; Wang et al., 2019). Aphasia affects the patient's linguistic skills and daily communication. As the course of the disease is prolonged, it will also impede patients' quality of life.
Due to the lack of targeted surgery and efficacious treatment regimens, speech therapy is a general method to train patients with aphasia. The mechanism of speech therapy is mainly based on the language function centers located in the dominant left hemisphere (Kamath et al., 2019). Several studies have demonstrated that music therapy for non-fluent aphasia is used to treat patients who have lost their speaking ability after a stroke or accident. It is reported that the right hemispheric regions are more active during singing (Jeffries et al., 2003; Callan et al., 2006; Ozdemir et al., 2006). Music therapy involving melodic elements is deemed to be a potential treatment for non-fluent aphasia, as singing potentially activates patients' right hemisphere to compensate for their lesioned left hemisphere (Zipse et al., 2009; Schlaug et al., 2010). Aside from singing, many other music therapy techniques have also been attempted, and the effectiveness of some methods has been revealed.
Melodic intonation therapy (MIT) is one of the verified effective methods of aphasia by the American Academy of Neurology (AAN) (Helm-Estabrooks and Albert, 2004). MIT is an intonation-based treatment method for non-fluent or dysfluent aphasic patients developed in response to the observation that severely aphasic patients can often produce well-articulated, linguistically accurate words while singing but not during a speech (Albert et al., 1973; Sparks et al., 1974). MIT is a hierarchically structured treatment that utilizes intoned (sung) patterns that exaggerate the typical melodic content of speech across three levels of increasing difficulty. At the elementary level, patients need to complete 1–2 syllables of melodic intonation in oral expression, such as “hello,” “thank you,” “goodbye,” etc. At the intermediate level, patients need to complete oral expressions of melodic intonation of 3–5 syllables, such as “I love you,” “I am thirsty (hungry),” “I have to rest,” etc. to express daily needs. At the advanced level, patients need to express sentences of 6–10 words or more, such as “I am going to train today,” “It is 10 a.m. in the morning,” etc. The original explanation of MIT is to utilize the musical and language output region in the right hemisphere, in which the mechanism differs from the left hemisphere (Albert et al., 1973; Sparks et al., 1974). An assumption raised by Albert and Sparks is that music can be effective by discovering music to language connections between the right and the left hemisphere in an interactive way or by using either reserved music/language functional area in the two hemispheres to speak. MIT combines melodic and rhythmic aspects of sentence intonation with language (Albert et al., 1973; Sparks et al., 1974; Sparks and Holland, 1976; Helm-Estabrooks et al., 1989; Cohen and Masse, 1993; Boucher et al., 2001; Norton et al., 2009). It can mobilize the auditory musical area on the right and the language area in the left hemisphere. The goal of MIT is namely to elicit the sound of the language (or spontaneous speech) by exaggerating the melody and rhythm of the language. The implementation process of MIT is musical, activating the right hemisphere mechanism that is not commonly used in daily language expression.
However, according to the currently published MIT studies, there is an excessive number of reviews and mechanism analysis studies. Still, there is a scarce number of randomized controlled trials (RCT), cross-over studies, cohort studies, and case studies. In experimental researches, the evidence is accentuated over language behavior measurements, and there are very few studies that use multimodal imaging observation to verify behavioral, neural mechanisms. In the assessment results of the language scale, the brain areas observed by MRI imaging are scattered, and the target areas of symptoms remain unclear. According to the results of existing mechanism analysis and scale evaluation, there are many possible narratives for the mechanism of MIT, but its underlying mechanism remains unclear as of yet (Breier et al., 2010; van de Sandt-Koenderman et al., 2010; Merrett et al., 2014; Zumbansen et al., 2014b). Therefore, the purpose of our review is to (1) retrieve the evidence and effectiveness of MIT for non-fluent aphasia after strokes, determine the superior performance of melody intonation therapy-related interventions in behavioral measurement results, and summarize our findings. (2) From a meager amount of MRI evidence, determine which areas the onset mechanism is more focused in, identify more targeted brain areas and circuits, and find a more feasible mechanism direction for the treatment of aphasia by MIT, thus providing the groundwork for future research.
Materials and Methods
Selection of Studies
We have planned and analyzed literature from reviews, systematic reviews, randomized controlled trials (RCT), clinical-controlled trials (CCT), cross-over studies, cohort studies, self-control, and case studies, regarding aphasia and music therapy. A literature search was conducted on four electronic databases: PubMed, Bing Scholar, Google Scholar, and Medline. The included articles are in English, French, Italian, Spanish, German, Korean, and Japanese. The publication timeframe was from January 1970 to July 2021. The keywords of “stroke,” “aphasia,” “music,” “melody,” “rhythmic,” “intonation,” “melodic intonation therapy,” “music therapy,” “music and aphasia,” and “rhythm and aphasia” were searched. The search was free and followed PRISMA's recommendations (Liberati et al., 2009; Higgins and Green, 2011), with a reference list of articles attached.
Randomized controlled trials (RCT), clinical-controlled trials (CCT), cross-over design, self-control, and case studies were subsequently recruited, with the omission of reviews. In accordance with the PICOS principle in evidence-based medicine, this review defines the criteria for inclusion.
(1) Participants: In participant's inclusion, all studies concerned only human adults (≥18 years) in stroke recovery period with non-fluent aphasia, including ischemic and hemorrhagic stroke, and the time since stroke was more than 2 weeks. (2) Intervention: The intervention group followed musical supported MIT such as melodic intonation therapy (MIT), modified MIT, rhythmic syllables therapy (RST), spoken language stimuli, singing therapy (ST), rhythmic therapy (RT), prosody perception task (PPT), sung-spoken story recall task, melodic cueing, melodic singing, and rhythmic cueing. (3) Comparison: The MIT intervention dose ranges from 1 to 4 times per week, and the duration ranges from 1 to 12 weeks. The control group was followed by speech therapy or blank control in the same dose and duration. (4) Outcomes: Using behavioral evaluation scales and fMRI to evaluate the results, the primary outcomes with a p < 0.5 are meaningful. (5) Study design: Methods are a randomized controlled study of MIT and speech therapy, or a self-controlled study of MIT, or a cross-design study of modified MIT and speech therapy, case reports of MIT, etc.
We compared speech therapy and melodic intonation therapy, combined with commonly integrated rehabilitation, and evaluated clinical outcomes.
Data Sources and Search Strategy
After searching for relevant literature in 4 databases, a total of 128 works of literature about melodic intonation (induced) therapy were retrieved, and 2 was from another website. It was found that 90 articles were repeated in each database after reviewing the titles, indicating high reliability. After a quick review of the literature, 10 MIT literature reviews, 5 abstracts, and 4 qualitative analyses were excluded. The remaining 71 articles contain complete quantitative analysis and case studies. After careful examination of these articles, it was found that the data of 5 brief articles were published as spotlight, and 11 papers were presented as the original form; without statistical analysis, the statistical correlation could not be obtained. Thirteen articles did not belong to melodic intonation therapy and relative therapy. Three papers were for patients with a cognitive impairment not relevant to aphasia intervention. Finally, 39 quantitative experimental types of research and case studies of aphasia rehabilitation of typical MIT were identified. The risk of bias assessment was based on the handbook of Cochrane review methods (Higgins and Green, 2011; Figure 1).
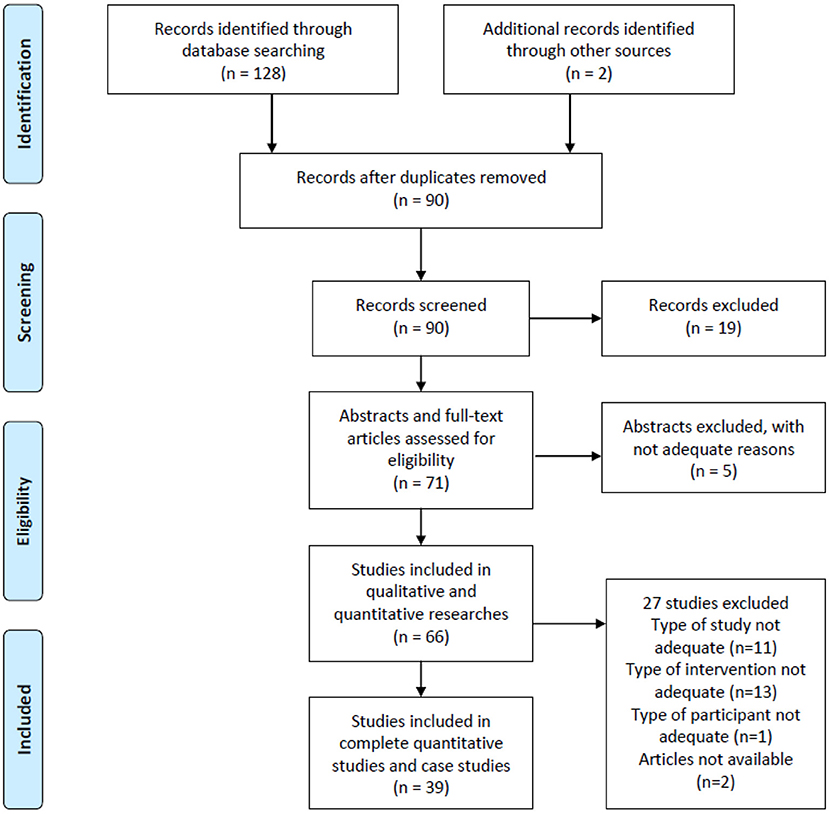
Figure 1. Flow diagram of article identification and inclusion.
The principle behind selecting these clinical studies as a systematic review is that these studies have applied MIT to clinical patients to observe the actual effects. Secondly, internationally standard measures were performed before and after the clinical trial to compare the results. Eleven of the experiments were accompanied by imaging tests. The intervention was a melodic musical form, accomplished by the therapist. Therefore, the above three points align with the therapy standards and principles proposed at the beginning of standard melodic intonation therapy.
Main Results of Clinical Trials of MIT to Aphasia
This review summarizes all MIT studies with non-fluent aphasia patients since 1970 (Table 1). Since MIT was established in the 1970s as a more effective supplementary treatment for non-fluency aphasia, clinical trials on MIT have gradually garnered widespread attention. MIT clinical trials have the following characteristics: (1) In the research before the Twentieth century, the behavioral observation records of patients with MIT were more detailed; (2) Comparative case studies, self-controlled studies, and small sample experiments were more numerous; (3) Most of them used subjective language assessment scales for result evaluation. After the Twentieth century, with the advancement of imaging medicine, researchers conducted large sample experiments while focusing on behavioral measurements. They were more concerned about the evidence yielded by the brain imaging structure. The assessment tool was taken as a classification feature. Twenty-two MIT clinical trials evaluated using language ability scales and 11 clinical trials using imaging measurements; all the 33 pieces of research are listed in Table 1.

Table 1. The clinical trials of MIT for the aphasia of stroke.
The Effects of MIT on 15–40 Sample Trials: The Most Assessment Tools Are Subjective Measurement Scales
In these MIT clinical trials, 13 experiments use various language assessment scales for evaluation, accounting for the majority. Melodic interventions are the selected essential factors, but evaluation criteria are equally important. There are mainly two evaluation criteria in the quantitative studies, one is various standard language test scales, which include the Boston Diagnostic Aphasia Examination (BDAE), the Western Aphasia Battery (WAB) in different language versions, the Aphasia Quotient (AQ), the Aachen Aphasia Test (AAT), amongst others. The other is imaging check, which includes functional magnetic resonance imaging (fMRI), magnetic resonance (MR), and diffusion tensor imaging (DTI), which are usually applied in a one-time assessment.
RCT Studies Evaluated Using Standard Language Test Scales Showed Consistent Results in Behavioral Measurement Results (Without Imaging)
Of the more than 15 MIT RCT studies selected in this review, seven valuable clinical trials used the language assessment scale to evaluate the results. Conklyn et al. (2012); Lim et al. (2013); Van der Meulen et al. (2014); Van Der Meulen et al. (2016); Raglio et al. (2015); Kasdan and Kiran (2018); Haro-Martínez et al. (2019); Leo et al. (2019), and Zhang et al. (2016, 2021) all used various language scales to assess two groups of patients with aphasia. The results demonstrated that whether it was only one observation of the immediate treatment effect or the cumulative treatment effect for up to 12 weeks, compared with the speech therapy group, the MIT group was better in understanding (Haro-Martínez et al., 2019), retelling (Haro-Martínez et al., 2019), and oral task response time (Lim et al., 2013), and oral memory time and retelling phrase length (Kasdan and Kiran, 2018) have been markedly improved. Regarding spontaneous expression, most of the target languages trained by MIT are short sentences of varying lengths, while the content of melody training is fixed. Therefore, in addition to improving the level of training items, patients receiving MIT can also enhance the spontaneous speech of untrained items. This is particularly conspicuous in the test of story retelling (Van der Meulen et al., 2014; Van Der Meulen et al., 2016). These meaningful behavioral measurement results are reflected in the scores of different dimensions of various language test scales.
Among the specific results, Haro-Martínez et al. (2019) found that after MIT, the MIT group improved communicative activity log (CAL), but no significant difference was noted in comprehension and repetition. Leo et al. (2019) found that after singing melody in the MIT group, the aphasic patients recalled longer in the singing rather than the speaking task and also with chunk length in the singing task. Kasdan and Kiran (2018) compared 1-h immediate effect after MIT and then found that patients with standard MIT conspicuously improved phrase length. Zumbansen et al. (2014a) conducted a crossover study on 3 aphasia patients for 6 weeks to compare MIT. The results showed that all of the 3 patients in MIT training improved clarity of syllables significantly. Stahl et al. (2013) did a similar crossover study of 3 aphasia patients, and it turns out the MT group improved significantly in repetition. In 2014, Van der Meulen et al. (2014) and Van Der Meulen et al. (2016), conducted an MIT crossover study on 27 aphasia patients, among which 16 patients received MIT for 6 weeks, and 11 patients in the control group received MIT after weeks. It was revealed that compared to the control group, the MIT group improved the repetition (AAT) in both trained items and untrained items. He then ran the same MIT crossover study in 2016 and found MIT group improved repetition in trained items and spontaneous sentences in untrained items. Raglio's et al. RCT study (Conklyn et al., 2012; Lim et al., 2013; Raglio et al., 2015) also proved that MIT improved repetition, listening comprehension, spontaneous speech, naming, and responsive items 2–3 score. Vian (Vines et al., 2011) turns out that applying anodal-tDCS during MIT produced a significantly greater improvement in verbal fluency.
Case Studies and Small Sample Studies Have the Characteristics of Complete Specific Treatment Interventions
There are 6 clinical trials with sample sizes between 1 and 6 patients. These studies mostly use the patient's control or crossover design to observe the effectiveness of MIT intervention. Due to the small sample size, these studies reflect the characteristics of a more detailed record of the intervention process and a more evident division of music elements in MIT. In the MIT intervention conducted by Van der Meulen et al. (2012) for 2 patients, a dedicated MIT therapist carried out the implementation process. Although in the MIT study conducted by Racette (2006), Kim and Tomaino (2008), Stahl et al. (2013), Zumbansen et al. (2014b), and Cortese et al. (2015), the implementer of the intervention process was realized by a speech therapist. Still, because the case study can record the detailed procedure, they compared the difference between melody and rhythm and found that the melody is dominant. The prognostic score will display more positive results. In the case report by Slavin and Fabus (2018), the therapist trained in NMT who performed MIT treatment also showed positive results. Although the samples in the above studies are generally small, the results are similar to the RCT study of more than 15 people, and the intervention process tends to be more musical.
The Advantages and Disadvantages of RCT Studies of Using Medical Imaging or Computers for Evaluation
In the clinical trials reviewed, most of the studies using MRI have the following characteristics: (i) case studies are dominant; (ii) the number of subjects is inferior or equal to 6; (iii) in case of large sample size, MRI observation should only be used before and once after MIT intervention to provide an immediate comparison. The above three characteristics are in an either-or relationship and will not appear simultaneously in the same study. In addition, we also found that the number of MIT musical interventions directly leads to different imaging results.
Among the RCT studies searched for, eight types of research used MRI to compare the effect before and after treatment. Orellana et al. (2014) compared an immediate impact on 20 aphasia patients before and after once MIT. After the intervention, fMRI and 3T MR scans showed that MIT increased activation in the left-lateralized in the SMG, IPL, STG, and SFG. Right-lateralized activation was seen in the insula, rolandic operculum, and pars opercularis of the inferior frontal gyrus. Akanuma et al. (2015) used positron emission tomography (PET) to conduct a self-control study in 10 chronic aphasia patients. The results demonstrated that 5 patients exhibited improvements after singing intervention; all indicated intact right basal ganglia and left temporal lobes. Norton et al. (2009), Schlaug et al. (2009), and Zipse et al. (2012) performed DTI to analyze structural changes in both hemispheres in 7 patients before and after MIT intervention. It turns out that all 7 patients showed a substantial increase in the absolute number of fibers in the right arcuate fasciculus (AF) comparing post-vs. pre-treatment DTI studies (paired t-test, p = 0.04) and also an increase in the fiber length, although omitting to mention the professional music therapists. It is worth noting that their melodic intervention time all exceeded 8 weeks, 75 courses of treatment. Al-Janabi et al. (2014) observed patients with functional magnetic resonance imaging after 6 days of MIT intervention and found that the left BA44 and right BA44 of the patients who received MIT had a significant increase in the activity. But Breier et al. (2010) compared two patients with chronic aphasia and came up with contradictory results. He showed a steady decrease in activation in the right hemisphere of both treatment areas, resulting in strong left hemisphere lateralization of MEG activity. However, Jungblut used his case studies through fMRI to argue that the limitation of this study is that activation changes were not measured by image acquisition before and after treatment (Jungblut et al., 2014). Cortese et al. (2015) found that in Italian MIT, all phonemic structure, speech automatism, prosody, communication, correct repetition, naming, and comprehension improved, while the adaptation of the MIT in the French language was developed by Belin et al. (1991).
Case Studies
Because the case study method is more meticulous and concentrated, the examination and evaluation method of MRI plus scale is more common.
Van der Meulen et al. (2012) compared MIT interventions with those of two patients. After 6 weeks, patients with MIT improved 35 scores in repetition trained phrases, 50 scores in repetition, 7 scores in action naming, and 9 scores in comprehension (AAT). Seven scores were improved in Amsterdam Nijmegen Everyday Language Test (ANELT); 22.5 scores were improved in Sabadel Story Retell Task. Slavin and Fabus (2018) conducted a before-after MIT intervention in a 63-year-old man with chronic aphasia for 10 years. Unlike other studies, Slavin teamed up with a professional music therapist to intervene. The results found that MIT improved auditory comprehension skills, question answering, and repetition of BDAE after listening to the paragraphs. Breier et al. (2010) compared two patients with chronic aphasia with an average age of 53 and an average duration of 3.5 years. Using MR to observe hemisphere structural changes, patient 1 with MIT exhibited a significant increase in CIUs (>35%) after the first block of treatment. Patient 1 showed lateralization in the right hemisphere of MEG activity. Al-Janabi et al. (2014) used transcranial magnetic stimulation (rTMS) and MIT to intervene two aphasia patients with an average duration of 15 months and using MR to the before-and-after comparison. The results revealed that patients with MIT revealed significant activity increase in left BA44 and a decrease in right BA44. Patient 2 revealed significant activity increase in left BA44, right BA44, and left BA45. Tabei et al. (2016) used fMRI to observe a 48-year-old patient with a 3-year history of chronic aphasia before and after 9 days of intensive MIT. The results showed in fMRI that the patient had a significant activation of the medial frontal gyrus, inferior frontal gyrus, superior temporal gyrus, lentiform nucleus, and lingual gyrus of the right hemisphere.
In the Research Using fMRI Measurement, the Main Concentrated Region of Interest in Brain
Through summarizing the studies in Table 1 which used fMRI to support MIT, we used the software BrainNet Viewer to locate the brain ROI (regions of interest). BrainNet Viewer is a brain network visualization tool for imaging connect omics. It can help researchers to visualize topological patterns of structural and to find functional brain networks derived from different imaging modalities (Xia et al., 2013). Using the BrainNet Viewer to locate the occurrence sites, it was found that all MIT-supported patients had more activation ROI in the right hemisphere than in the left hemisphere. The concentrated areas of ROI are the precentral gyrus, precentral sulcus, postcentral gyrus, middle frontal gyrus, superior temporal gyrus, superior temporal sulcus, middle temporal gyrus, inferior temporal sulcus, lingual gyrus, angular gyrus, etc. (Figure 2).
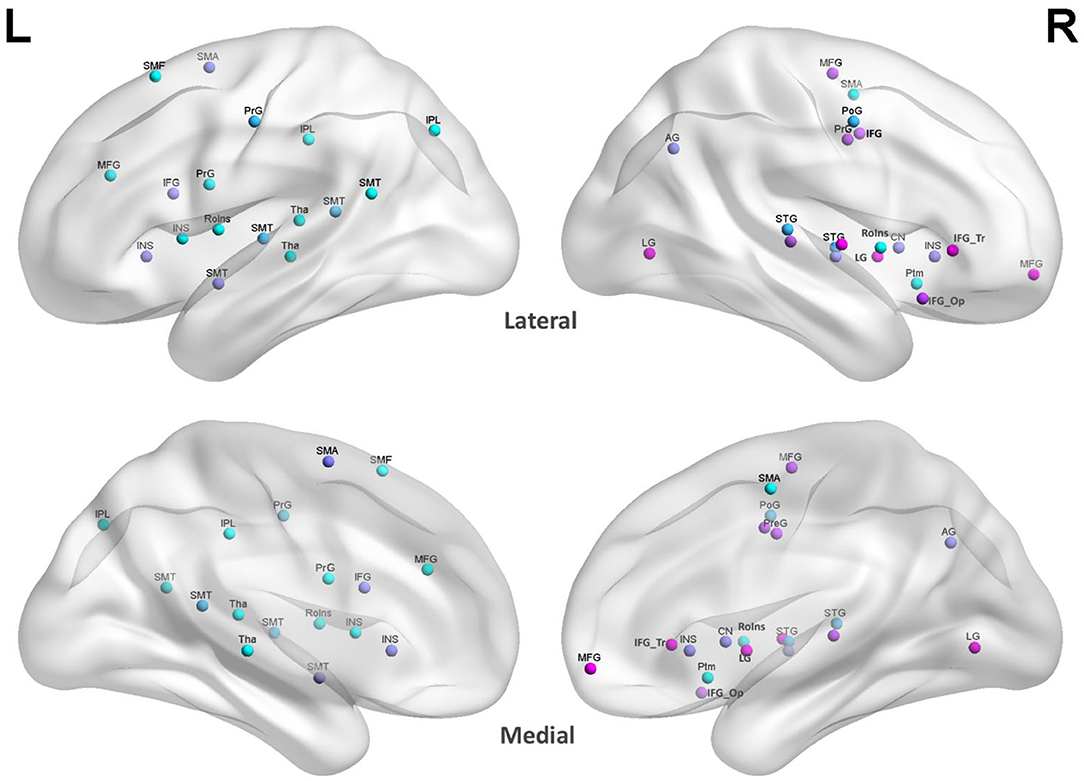
Figure 2. ROI in MIT-supported studies. The site colors were randomly generated to distinguish different ROI regions at the same site to prevent color overlap. L, left hemisphere; R, right hemisphere; Lateral, lateral cerebral hemisphere; Medial, medial cerebral hemisphere; SMT, superior and middle temporal gyrus; SMA, supplementary motor area; SMF, superior and middle frontal gyrus; PrG, pre-central gyrus; PoG, post-central gyrus; IPL, inferior parietal lobule; IFG, inferior frontal gyrus; INS, insula; MFG, middle frontal gyrus; RoIns, rolandic operculum insula; Tha, thalamus; LG, lingual gyrus; AG, angular gyrus; LN, lentiform nucleus; IFG_Tr, inferior frontal gyrus pars triangularis; IFG_Op, inferior frontal gyrus pars opercularis.
Discussions
Our review selected 39 typical effective MIT experimental studies from 127 studies. Their common feature is the use of musical melody to intervene in aphasia, accompanied by effective evaluation. This analysis and discussion are based on the analysis of the intervention methods, evaluations, and effects of these studies.
Feasibility Differences in Measurement Methods Between Clinical Trials With More Subjects and Case Studies
In these RCT studies with relatively more subjects, we found that objective imaging observation was not used as a primary means of effective monitoring. There may be some correlations to the therapeutic way of MIT. The one-to-one treatment and evaluation method will increase the working load of clinicians. If every participant is involved in the medical imaging test, the clinical workload, patient compliance, and financial support will all influence factors. Therefore, in more than 6 subjects of RCT studies in the past 10 years, only two articles with imaging observations were found. However, all of the RCT findings, including the two objective tests, confirmed the effectiveness of the subjective measurement scale of MIT. Because MIT requires individualized intervention and a long course of treatment, language assessment scales are the most convenient way of assessment. Compared with the high-cost evaluation of functional MRI, the scale evaluation of more than 15 patients with aphasia is easy to operate on and easy to compare before and after. In these MIT studies using MRI detection, the changes in cortical white matter and fiber bundles are apparent, which provide substantial evidence for the therapeutic effect of MIT and lay a foundation for the study of neural mechanisms.
However, due to the time-consuming, labor-intensive, and cost-intensive MRI examinations, most of these MIT's RCT studies have the following shortcomings: (i) there are some studies (Orellana et al., 2014) that could perform long-term MIT intervention experiments, and the imaging examinations are meticulous. Still, the number of samples is too small. Most of the samples comprised 6 participants; (ii) although there are 4 studies (Schlaug et al., 2009; Stahl et al., 2013; Zumbansen et al., 2014a; Cortese et al., 2015) that can match the minimum number of statistical subjects, there is no long-term intervention for comparison; therefore, the cumulative effect cannot be observed. The only one-time immediate effect is not enough to explain the mechanism. Therefore, in the future, how to ensure that both the demand for sample size and the long-term intervention of MRI detection can be achieved is matter of pressing academic concern.
The Number of Musical Factors in the MIT Intervention Is Directly Linked to the Imaging Results
Previous literature has demonstrated several effective clinical results related to the recovery of musical melody-induced speech in the treatment of post-stroke aphasia. MIT (Albert et al., 1973), formally proposed by the American Academy of Neurology in 1973, is used to treat aphasia. In the early clinical treatment of non-fluency aphasia, Sparks et al. (1974) recorded the use of spectrum examples when training patients, with “Sprechgesang” as the core, requiring patients to follow the written melody. Zipse et al. (2012), Orellana et al. (2014), and Tabei et al. (2016), and others tend to use MIT treatment under more musical intervention, so their imaging results all show more features of active right hemisphere area. Moreover, although Zipse et al. (2012), Schlaug et al. (2014), Akanuma et al. (2015), and others used MIT recordings or provided MIT by general therapists, their intervention processes were all over 8 weeks. The natural melody factor in MIT makes the imaging results they obtained also reflected the active characteristics of the right hemisphere. Therefore, in the existing MIT experimental research, it is found that musical factors and the cumulative effect of time will directly affect the evidence that the right hemisphere of the brain participates in activities. Although rhythm is part of the music, as the rhythm is unpitched, we did not find a clear trend of activating the right hemisphere in the MIT intervention under the guidance of rhythm or language.
It is reported that the effects of the musical rhythm are observed in the left brain areas (Chen et al., 2008) and listening to musical rhythms recruits motor regions of the brain (Limb Charles et al., 2006; Limb et al., 2006; Thaut et al., 2014). However, these studies only focus on the music listening of healthy individuals or the rhythm perception of musicians. They are not the observation of MIT on patients with aphasia caused by stroke in the left hemisphere. Therefore, in the case of damage to the language center of the left hemisphere, patients treated with MIT can have correct oral speech output. This phenomenon confirms the mechanism of musical pitch from one side. But its brain mechanism still needs further study.
The Neural Mechanism of MIT Based on Music
In the evidence summarized in previous MIT experimental studies, we found that the ROIs activated by MIT were the central anterior gyrus, central anterior sulcus, central posterior gyrus, middle frontal gyrus, superior temporal gyrus, superior temporal sulcus, middle temporal gyrus, inferior temporal gyrus, lingual gyrus, and angular gyrus of the right hemisphere. These areas include the frontal motor cortex (including Broca's area and ventral anterior motor cortex), which connects speech sensation and output, auditory cortex (including superior temporal gyrus and middle temporal gyrus), and parietal cortex (including angular gyrus and gyrus). MIT based on music activities, that is, MIT provided by professional music therapists, whether extracting lyrics from familiar songs or learning new fixed-pitch short melody for patients, affects the white matter structure of the auditory-motor neural circuit compensation to promote the ability to encode and integrate verbal information. This trans-hemisphere “mirror effect” has an important mechanism for the language recovery of patients with aphasia.
Valuable Findings in Case Studies
It is found in literature retrieval that the evaluation methods of case studies are generally comprehensive and meticulous. Such qualitative studies reflecting the therapeutic effects of satisfactory MIT have more profound clinical implications for the brain regions it may activate. In the case reports retrieved in this paper, the evaluation criteria of early studies were generally international scales, mostly subjective scoring methods, and language recovery competence was based on scoring in different dimensions. In the recent 10 years of research, some medical imaging evidence of changes in brain structure at MIT to aphasia patients is easier to find in case reports (Schlaug et al., 2009; Al-Janabi et al., 2014; Tabei et al., 2016; Martzoukou et al., 2021). Besides, in the case study, whether the language assessment scale or fMRI was used, the subjective measurement and objective monitoring of patients have received sufficient concertation. Evidence of structural changes in patients' brain regions before and after also provides a factual neurological basis for MIT. It provides a realistic basis for the treatment of clinical aphasia.
The Importance of Music Therapist at MIT
In the literature we reviewed, only 5 studies mentioned the participation of music therapists. Although MIT originated in speech therapy, MIT's guidance is melodic. It should be necessary for a correct rehabilitative approach by MIT to have specific training. For instance, the accuracy of melodic language needs a musical or music therapy formation. The rest of the literature does not mention the credentials of speech therapists and whether they have music learning experience. In fact, in MIT, treatment performed by music therapists includes instrumental accompaniment, melodic guidance, and songs inducement. Therefore, in the process of activating the vocabulary encoding of patients with aphasia, the instrument accompaniment, the professional, accurate melodic pitch, and the guidance from music therapists to play and sing are all combined to activate the melodic “lyrics” of the episodic memory network and promote the output of spoken language.
Expectations for Future MIT Development
Through MIT's RCT studies, the left and right brains were found to have different processing advantages. The functional areas responsible for music melody processing and memory retrieval are more concentrated in the auditory cortex of the right brain temporal lobe. Therefore, it is speculated that the left brain is more responsible for language functions. After damage sustained by the dominant hemisphere, MIT may activate the auditory cortex corresponding to music processing in the right brain and activate the right brain language motor area corresponding to the Broca's area of the left brain through the conduction of the right arcuate track to achieve compensation and guide the patient's language output, to achieve the purpose of language communication (Merrett et al., 2014). However, 90% of the literature we reviewed so far was RCT studies on Western language aphasia; only 10% of the literature comes from East Asian language aphasia (Japanese and Korean), while the MIT intervention in Chinese Mandarin aphasia trials has not been found in internationally registered clinical trials. Compared with Western languages, East Asian languages, as a tonal language (including four or more tones), have a more bilateral distribution of brain nerve circuits than Western languages represented by English (Liang and Du, 2018). However, despite this, the neural mechanism of the effect of MIT on East Asian languages has not been verified by a large sample of experiments.
It should be noted that, according to the high incidence of aphasia. However, relatively effective treatment methods were developed. A large amount of imaging evidence has not supported MIT, nor has it been endorsed by large cohort studies. This may be due to factors such as MIT's over-reliance on therapists, its unitary approach, lack of computerization, and individual patient differences. From existing evidence, MIT is effective and has positive results of scale testing. In the future, researchers should try the use of technology to develop music artificial intelligence evaluation and training tools, streamline and step the operation of MIT, reduce the human cost, and, on this basis, cooperate with imaging detection, and then conduct large sample experiments, so that the clinical and scientific value of MIT will be maximized in the future.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This research received a grant from Scientific Research Project of Establishment of the Winter Olympics Sports Injury Rehabilitation Diagnosis and Treatment System and Green Channel Demonstration, No. 2018YFF0301104 (to JL).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank YD for the guidance, advice, encouragement, and assistance for this review, and Teng Wen-Jia for the analysis in BrainNet Viewer.
References
Akanuma, K., Meguro, K., Satoh, M., Tashiro, M., and Itoh, M. (2015). Singing can improve speech function in aphasics associated with intact right basal ganglia and preserve right temporal glucose metabolism: Implications for singing therapy indication. Int. J. Neurosci. 126, 39–45. doi: 10.3109/00207454.2014.992068
Albert, M. L., Sparks, R. W., and Helm, N. A. (1973). Melodic intonation therapy for aphasia. Arch. Neurol. 29, 130–131. doi: 10.1001/archneur.1973.00490260074018
Al-Janabi, S., Nickels, L. A., Sowman, P. F., Burianová, H., Merrett, D., and Thompson, B. (2014). Augmenting melodic intonation therapy with non-invasive brain stimulation to treat impaired left-hemisphere function two case studies. Front. Psychol. 5:37. doi: 10.3389/fpsyg.2014.00037
Baker, F. (2000). Modifying the Melodic Intonation Therapy Program for Adults With Severe Non-fluent Aphasia. Music Therapy Perspectives (2000), Vol. 18. New York, NY: American Music Therapy Association.
Belin, P., Van Eeckhout, P., Zilbovicius, M., Remy, P., François, C., Guillaume, S., et al. (1996). Recovery from nonfluent aphasia after melodic intonation therapy: a PET study. Neurology 47, 1504-1511. doi: 10.1212/wnl.47.6.1504
Belin, P., Van Eeckhout, P., Zilbovicius, M., Remy, P., FranFois, C., Guillaume, S., et al. (1991). Recovery from nonfluent aphasia after melodic intonation therapy. Hum. Mov. Sci. 10, 315–334.
Benjamin, E. J., Blaha, M. J., Chiuve, S. E., Cushman, M., Das, S. R., Deo, R., et al. (2017). Heart disease and stroke statistics-−2017 update: a report from the American heart association. Circulation 135, e146–e603. doi: 10.1161/CIR.0000000000000485
Bonakdarpour, B., Eftekharzadeh, A., and Ashayeri, H. (2003). Melodic intonation therapy in Persian aphasic patients. Aphasiology. 17, 75–95. doi: 10.1080/729254891
Boucher, V., Garcia, L. J., Fleurant, J., and Paradis, J. (2001). Variable efficacy of rhythm and tone in melody-based interventions: implications for the assumption of a right-hemisphere facilitation in nonfluent aphasia. Aphasiology 15, 131–149. doi: 10.1080/02687040042000098
Breier, J. I., Randle, S., Maher, L. M., and Papanicolaou, A. C. (2010). Changes in maps of language activity activation following melodic intonation therapy using magnetoencephalography: two case studies. J. Clin. Exp. Neuropsychol. 32, 309–314. doi: 10.1080/13803390903029293
Callan, D. E., Tsytsarev, V., Hanakawa, T., Callan, A. M., Katsuhara, M., Fukuyama, H., et al. (2006). Song and speech: brain regions involved with perception and covert production. Neuroimage 31, 1327–1342. doi: 10.1016/j.neuroimage.2006.01.036
Chen, J. L., Penhune, V. B., and Zatorre, R. J. (2008). Moving on time: brain network for auditory-motor synchronization is modulated by rhythm complexity and musical training. J. Cogn. Neurosci. 20, 226–239. doi: 10.1162/jocn.2008.20018
Cohen, N. S., and Masse, R. (1993). The application of singing and rhythmic instruction as a therapeutic intervention for persons with neurogenic communication disorders. J. Music Ther. 30, 81–99. doi: 10.1093/jmt/30.2.81
Conklyn, D., Novak, E., Boissy, A., Bethoux, F., and Chemali, K. (2012). The effects of modified melodic intonation therapy on nonfluent aphasia: a pilot study. J. Speech Lang. Hear. Res. 55:1463. doi: 10.1044/1092-4388(2012/11-0105)
Cortese, M., Riganello, F., and Arcuri, F. (2015). Rehabilitation of aphasia: application of melodic-rhythmic therapy to the Italian language. Front. Hum. Neurosci. 9:520. doi: 10.3389/fnhum.2015.00520
Gerstenecker, A., and Lazar, R. (2019). Language recovery following stroke. Clin. Neuropsychol. 33, 928–947. doi: 10.1080/13854046.2018.1562093
Go, A. S., Mozaffarian, D., Roger, V. L., Benjamin, E. J., Berry, J. D., Blaha, M. J., et al. (2014). Executive summary: Heart disease and stroke statistics – 2014 update: a report from the American heart association. Circulation 129, 399–410. doi: 10.1161/01.cir.0000442015.53336.12
Goldfarb, R., and Bader, E. (1979). Espousing melodic intonation therapy in aphasia rehabilitation: a case study. Int. J. Rehabil. Res. 2, 333–42. doi: 10.1097/00004356-197909000-00002
Goodglass, H., and Kaplan, E. (1972). The Assessment of Aphasia and Related Disorders. London: Henry Klimpton.
Haro-Martínez, A. M., Lubrini, G., Madero-Jarabo, R., Díez-Tejedor, E., and Fuentes, B. (2019). Melodic intonation therapy in post-stroke nonfluent aphasia: a randomized pilot trial. Clin. Rehabil. 33, 44–53. doi: 10.1177/0269215518791004
Helm-Estabrooks, N., and Albert, M. (2004). Manual of Aphasia and Aphasia Therapy, 2nd Edn. Austin, TX: PRO-ED, Inc.
Helm-Estabrooks, N., Nicholas, M., and Morgan, A. (1989). Melodic Intonation Therapy. Austin, TX: PRO-ED, Inc.
Higgins, J. P. T., and Green, S. (2011). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. Available online at: www.handbook.Cochrane.org.
Hough, M. S. (2010). Melodic intonation therapy and aphasia: another variation on a theme. Aphasiology 24, 775–786. doi: 10.1080/02687030903501941
Jeffries, K. J., Fritz, J. B., and Braun, A. R. (2003). Words in melody: an H(2)15O PET study of brain activation during the singing and speaking. Neuroreport 14, 749–754. doi: 10.1097/00001756-200304150-00018
Jungblut, M., Huber, W., Mais, C., and Schnitker, R. (2014). Paving the way for speech: voice-training-induced plasticity in chronic aphasia and apraxia of speech—three single cases. Neural Plast. 2014, 1–14. doi: 10.1155/2014/841982
Kamath, V., Sutherland, E. R., and Chaney, G.-A. (2019). A meta-analysis of neuropsychological functioning in the logopenic variant of primary progressive aphasia: comparison with the semantic and non-fluent variants. J. Int. Neuropsychol. Soc. 26, 322–330. doi: 10.1017/S1355617719001115
Kasdan, A., and Kiran, S. (2018). Please don't stop the music: song completion in patients with aphasia. J. Commun. Disord. 75, 72–86. doi: 10.1016/j.jcomdis.2018.06.005
Kim, G., Min, D., Lee, E. O., and Kang, E. K. (2016). Impact of co-occurring dysarthria and aphasia on functional recovery in post-stroke patients. Ann. Rehabil. Med. 40, 1010–1017. doi: 10.5535/arm.2016.40.6.1010
Kim, M., and Tomaino, C. M. (2008). Protocol evaluation for effective music therapy for persons with nonfluent aphasia. Top. Stroke Rehabil. 15, 555–569. doi: 10.1310/tsr1506-555
Koleck, M., Gana, K., Lucot, C., Darrigrand, B., Mazaux, J. M., and Glize, B. (2017). Quality of life in aphasic patients 1 year after a first stroke. Qual. Life Res. 26, 45–54. doi: 10.1007/s11136-016-1361-z
Laine, M., Tuomainen, J., and Ahonen, A. (1994). Changes in hemispheric brain perfusion elicited by Melodic Intonation Therapy: A preliminary experiment with single photon emission computed tomography (SPECT). Cham: Scandinavian University Press.
Leo, V., Sihvonen, A. J., Linnavalli, T., Tervaniemi, M., Laine, M., Soinila, S., et al. (2019). Cognitive and neural mechanisms underlying the mnemonic effect of songs after stroke. NeuroImage Clin. 24:101948. doi: 10.1016/j.nicl.2019.101948
Liang, B., and Du, Y. (2018). The functional neuroanatomy of lexical tone perception: an activation likelihood estimation meta-analysis. Front. Neurosci. 12:495. doi: 10.3389/fnins.2018.00495
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700. doi: 10.1136/bmj.b2700
Lim, K. B., Kim, Y. K., Lee, H. J., Yoo, J., Hwang, J. Y., Kim, J. A., et al. (2013). The therapeutic effect of neurologic music therapy and speech-language therapy in post-stroke aphasic patients. Ann. Rehabil. Med. 37:556. doi: 10.5535/arm.2013.37.4.556
Limb Charles, J., Stefan, K., Eric, O. B., Sherin, R., and Allen, B. R. (2006). Left hemispheric lateralization of brain activity during passive rhythm perception in musicians. Anat. Rec. A Discov. Mol. Cell. Evol. Biol. 288, 382–389. doi: 10.1002/ar.a.20298
Limb, C. J., Kemeny, S., Ortigoza, E. B., Rouhani, S., and Braun, A. R. (2006). Left hemispheric lateralization of brain activity during passive rhythm perception in musicians. Cereb. Cortex 18, 2844–2854.
Marshall, N., and Holtzapple, P. (1976). Medodic Intonation Therapy: variations on a theme. Audiology and Speech pathology service veterans administration hospital, Bew Orleans, Louisianna.
Martínez, A. H., Lubrini, G., Madero-Jarabo, R., Díez-Tejedor, E., and Fuentes, B. (2018). Melodic intonation therapy in post-stroke nonfluent aphasia: a randomized pilot trial. Clin. Rehabili. 33, 44–53.
Martzoukou, M., Nousia, A., Nasios, G., and Tsiouris, S. (2021). Adaptation of melodic intonation therapy to greek: a clinical study in broca's aphasia with brain perfusion spect validation. Front. Aging Neurosci. 13:664581. doi: 10.3389/fnagi.2021.664581
Merrett, D. L., Peretz, I., and Wilson, S. J. (2014). Neurobiological, cognitive, and emotional mechanisms in melodic intonation therapy. Front. Hum. Neurosci. 8:401. doi: 10.3389/fnhum.2014.00401
Naeser, M. A., and Helm-Estabrooks, N. (1985). Ct scan lesion localization and response to melodic intonation therapy with nonfluent aphasia cases. Cortex 21, 203–223.
Norton, A., Zipse, L., Marchina, S., and Schlaug, G. (2009). Melodic intonation therapy. Ann. N. Y. Acad. Sci. 1169, 431–436. doi: 10.1111/j.1749-6632.2009.04859.x
Orellana, M. C. P., van de Sandt-Koenderman, M. E., Saliasi, E., van der Meulen, I., Klip, S., van der Lugt, A., et al. (2014). Insight into the neurophysiological processes of melodically intoned language with functional MRI. Brain Behav. 4, 615–625. doi: 10.1002/brb3.245
Ozdemir, E., Norton, A., and Schlaug, G. (2006). Shared and distinct neural correlates of singing and speaking. Neuroimage 33, 628–635. doi: 10.1016/j.neuroimage.2006.07.013
Popovic, A., and Boniver, J. (1992). Cause of death determined at autopsy in the University Hospital of Liège. Developments from 1878 to 1986. Rev. Med. Liege. 47, 618–23.
Racette, A. (2006). Making non-fluent aphasics speak: sing along! Brain 129, 2571–2584. doi: 10.1093/brain/awl250
Raglio, A., Oasi, O., Gianotti, M., Rossi, A., Goulene, K., and Stramba-Badiale, M. (2015). Improvement of spontaneous language in stroke patients with chronic aphasia treated with music therapy: a randomized controlled trial. Int. J. Neurosci. 126, 235–242. doi: 10.3109/00207454.2015.1010647
Schlaug, G., Marchina, S., and Kumar, S. (2014). Study design for the fostering eating after stroke with transcranial direct current stimulation trial: a randomized controlled intervention for improving Dysphagia after acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 24, 511–520. doi: 10.1016/j.jstrokecerebrovasdis.2014.09.027
Schlaug, G., Marchina, S., and Norton, A. (2008). From singing to speaking: why singing may lead to recovery of expressive language function in patients with broca's aphasia. Music Percep. 25, 315–323.
Schlaug, G., Marchina, S., and Norton, A. (2009). Evidence for plasticity in white-matter tracts of patients with chronic Broca's aphasia undergoing intense intonation-based speech therapy. Ann. N. Y. Acad. Sci. 1169, 385–394. doi: 10.1111/j.1749-6632.2009.04587.x
Schlaug, G., Norton, A., and Marchina, S. (2010). From singing to speaking: facilitating recovery from non-fluent aphasia. Fut. Neurol. 5, 657–665. doi: 10.2217/fnl.10.44
Slavin, D., and Fabus, R. (2018). A case study using a multimodal approach to melodic intonation therapy. Am. J. Speech Lang. Pathol. 27, 1352–1362. doi: 10.1044/2018_AJSLP-17-0030
Sparks, R. W., Helm, N. A., and Albert, M. L. (1974). Aphasia rehabilitation resulting from melodic intonation therapy. Cortex 10, 303–316. doi: 10.1016/S0010-9452(74)80024-9
Sparks, R. W., and Holland, A. L. (1976). Method: melodic intonation therapy for aphasia. J. Speech Hear. Disord. 41, 287–297. doi: 10.1044/jshd.4103.287
Springer, L., Willmes, K., and Haag, E. (1993). Training in the use of wh-questions and prepositions in dialogues: A comparison of two different approaches in aphasia therapy. Aphasiology 7, 251–270, doi: 10.1080/02687039308249509
Stahl, B., Henseler, I., Turner, R., Geyer, S., and Kotz, S. A. (2013). How to engage the right brain hemisphere in aphasics without even singing: evidence for two paths of speech recovery. Front. Hum. Neurosci. 7:35. doi: 10.3389/fnhum.2013.00035
Tabei, K. I., Satoh, M., Nakano, C., Ito, A., Shimoji, Y., Kida, H., et al. (2016). Improved neural processing efficiency in a chronic aphasia patient following melodic intonation therapy: a neuropsychological and functional MRI study. Front. Neurol. 7:148. doi: 10.3389/fneur.2016.00148
Thaut, M. H., Trimarchi, P. D., and Parsons, L. M. (2014). Human brain basis of musical rhythm perception: common and distinct neural substrates for meter, tempo, and pattern. Brain Sci. 4, 428–452. doi: 10.3390/brainsci4020428
van de Sandt-Koenderman, M., Smits, M., van der Meulen, I., Visch-Brink, E., van der Lugt, A., and Ribbers, G. (2010). A case study of melodic intonation therapy (MIT) in the subacute stage of aphasia: early re-re activation of left hemisphere structures. Proc. Soc. Behav. Sci. 6, 241–243. doi: 10.1016/j.sbspro.2010.08.121
Van Der Meulen, I., De Sandt-Koenderman, V., Mieke, W. M. E., Heijenbrok, M. H., Visch-Brink, E., and Ribbers, G. M. (2016). Melodic intonation therapy in chronic aphasia: evidence from a pilot randomized controlled trial. Front. Hum. Neurosci. 10:533. doi: 10.3389/fnhum.2016.00533
Van der Meulen, I., Sandt-Koenderman, V., and Ribbers, G. M. (2012). Melodic intonation therapy: present controversies and future opportunities. Arch. Phys. Med. Rehabil. 93, S46–S52. doi: 10.1016/j.apmr.2011.05.029
Van der Meulen, I., van de Sandt-Koenderman, W. M. E., Heijenbrok-Kal, M. H., Visch-Brink, E. G., and Ribbers, G. M. (2014). The efficacy and timing of melodic intonation therapy in subacute aphasia. Neurorehabil. Neural Repair 28, 536–544. doi: 10.1177/1545968313517753
Vines, B. W., Norton, A. C., and Schlaug, G. (2011). Non-invasive brain stimulation enhances the effects of melodic intonation therapy. Front. Psychol. 2:230. doi: 10.3389/fpsyg.2011.00230
Wang, L. D., Liu, J. M., Yang, Y., Peng, B., and Wang, Y. L. (2019). Stroke prevention in china still faces huge challenges-summary of “stroke prevention report 2018 in China. China Circul. J. 34, 105–119.
WHO (2015). World Report on Aging and Health. Available online at: http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf?ua=1 (accessed April 11, 2017).
Wilson, SJ., Parsons, K., and Reutens, D. C. (2006). Preserved Singing In Aphasia: A Case Study Of The Efficacy Of Melodic Intonation Therapy. Music Perception: An Interdisciplinary Journal, Vol. 24, No. 1. p. 23–36.
Xia, M., Wang, J., and He, Y. (2013). BrainNet viewer: a network visualization tool for human brain connectomics. PLoS ONE 8:e68910. doi: 10.1371/journal.pone.0068910
Zhang, X., Wang, C., and Liu, S. (2016). Case study of melodic intonation therapy and therapeutic singing in the treatment of motor aphasia after stroke. Chin. J. Stroke 11, 791–794. doi: 10.3969/j.issn.1673-5765.2016.09.016
Zhang, X. Y., Yu, W. Y., Teng, W. J., Lu, M. Y., Wu, X. L., Yang, Y. Q., et al. (2021). Effectiveness of melodic intonation therapy in chinese mandarin on non-fluent aphasia in patients after stroke: a randomized control trial. Front. Neurosci. 15:648724. doi: 10.3389/fnins.2021.648724
Zipse, L., Norton, A., Marchina, S., and Schlaug, G. (2009). Singing versus speaking in nonfluent aphasia. Neuroimage 47:S119. doi: 10.1016/S1053-8119(09)71121-8
Zipse, L., Norton, A., Marchina, S., and Schlaug, G. (2012). When right is all that is left: plasticity of righthemisphere tracts in a young aphasic patient. Ann. N. Y. Acad. Sci. 1252, 237–245. doi: 10.1111/j.1749-6632.2012.06454.x
Zumbansen, A., Peretz, I., and Harbert, S. (2014a). The combination of rhythm and pitch can account for the beneficial effect of melodic intonation therapy on connected speech improvements in Broca’s aphasia. Front. Hum. Neurosci. 8:592. doi: 10.3389/fnhum.2014.00592
Keywords: melodic intonation therapy, music therapy, non-fluent aphasia, speech therapy, stroke
Citation: Zhang X, Li J and Du Y (2022) Melodic Intonation Therapy on Non-fluent Aphasia After Stroke: A Systematic Review and Analysis on Clinical Trials. Front. Neurosci. 15:753356. doi: 10.3389/fnins.2021.753356
Received: 04 August 2021; Accepted: 07 December 2021;
Published: 27 January 2022.
Edited by:
Mary Miu Yee Waye, The Chinese University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Xiaoyu Xia, The Military General Hospital of Beijing PLA, ChinaFrancesco Riganello, Sant'Anna Crotone Institute, Italy
Copyright © 2022 Zhang, Li and Du. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianjun Li, bGludGFveml4eXpfMTIyOEBob3RtYWlsLmNvbQ==; Y3JyY2xpampAMTYzLmNvbQ==