 Adrian Schulz
Adrian Schulz Eric Dragendorf
Eric Dragendorf Katharina Wendt
Katharina Wendt André Schomakers
André Schomakers Eva Bültmann
Eva Bültmann Dominik Wolff
Dominik Wolff- 1Peter L. Reichertz Institute for Medical Informatics of TU Braunschweig and Hannover Medical School, Hannover Medical School, Hannover, Germany
- 2Institute of Diagnostic and Interventional Neuroradiology, Hannover Medical School, Hannover, Germany
Introduction: For brain maturity assessment of infants aged above 6 months, T2-weighted MRI scans are recommended. Prior to automated brain tissue analysis, skull stripping is typically applied. However, most skull stripping tools neither focus on T2-weighted scans nor on pediatric cohorts. Here, we present the evaluation results of seven common skull stripping tools in a comparably large pediatric cohort.
Methods: This study is based on 199 T2-weighted scans of children under the age of 5 years retrospectively acquired from the clinical routine at Hannover Medical School. We established a manually labeled ground truth under quality control of a senior neuroradiologist specialized in pediatric neuroradiology and evaluated seven skull stripping tools (BET, ROBEX, HD-BET, HD-BET-fast, SynthStrip, SynthStrip-noCSF and d-SynthStrip). Segmentation performance (Dice score, 95th percentile Hausdorff distance, sensitivity, specificity) and computation time were assessed on non-preprocessed and preprocessed scans (zero padding, contrast enhancement, artifact removal and normalization) as well as in different brain regions. For the best performing model, we manually assessed the top and bottom quartile of segmentations with respect to the integrity of different anatomical brain structures.
Results: Only BET, HD-BET, HD-BET-fast profited from data preprocessing. Considering this, all models had median Dice scores between 0.88 and 0.96, with SynthStrip performing best. All models segmented most accurately in the middle axial slices of the brain. Resampling lowered the performance of all models, except ROBEX. Mean computing times ranged from 2 s (BET) to 132 s (HD-BET) with SynthStrip requiring 7 s. per scan. SynthStrip was prone to not entirely including the Sinus sagittalis superior, the upper Cerebrum, the temporal pole, the Cerebellum and the Chiasma opticum/pituitary gland. In contrast, the petrous bone and the skull in the middle axial slices have often been partly included.
Discussion: Due to its robustness and quick computation time, we recommend SynthStrip for skull stripping of pediatric T2-weighted MRI scans. We attribute the observed segmentation errors to the partial volume effect, which should be addressed in future research. Limitations of our study include the monocentric setting, the exclusion of pathological cases and the skewed age distribution in our cohort.
1 Introduction
By analyzing cerebral magnetic resonance images, an individual’s brain age can be derived. For children, the focus lays on the development of the brain (Morita et al., 2022). The maturation of the brain is a complex process involving structural and functional changes (Lenroot and Giedd, 2006; Stiles and Jernigan, 2010) that correlate with an infant’s development. For tracking anatomical brain changes, such as myelination status as well as changes in volume and cortical thickness, magnetic resonance imaging (MRI) is the imaging modality of choice (Allen et al., 2005; Stiles and Jernigan, 2010). Dragendorf et al. (2024) suggested the automation of pediatric brain age prediction based on MRI scans in the clinical routine through the application of artificial intelligence (AI). For this, skull stripping is a crucial preprocessing step (Bernal et al., 2019; Fatima et al., 2020). Skull stripping, also referred to as brain extraction, removes non-brain tissue from scans. This way, potential age-related covariates, like the skull thickness in children, are removed, which allows age predictions solely based on relevant tissue.
Over several decades, a variety of skull stripping methods have been introduced. There has been a shift from the initial conventional image-processing-based methods toward machine learning (ML) and deep learning (DL) (Fatima et al., 2020). The conventional methods can be further subcategorized into five groups (Kalavathi and Prasath, 2016): mathematical morphology-based, intensity-based, deformable surface-based, atlas/template-based and hybrid models. According to Bernal et al. (2019), two frequently used conventional skull stripping tools are BET and ROBEX.
BET (Brain Extraction Tool) belongs to the group of deformable surface-based models, which performs skull stripping in a two-step approach (Smith, 2002). It identifies the center of the brain and, from there, grows a triangle mesh until it reaches the brain’s contours. For finding the center, BET applies a histogram-derived binarization threshold leading to a rough separation of the head from the background. Within the binarized volume, the center of gravity (COG) is calculated, which approximately corresponds to the brain’s center. For initializing a spherical triangle mesh around the COG, a reasonably small radius must be defined that allows the mesh to grow and, thus, adapt to the brain’s surface from the inside of the organ. To determine this radius, a sphere centered at the COG is fitted to the head voxels of the binarized scan. Since it risks exceeding the brain’s boundaries, its radius is halved. The result is a small sphere in the middle of the brain, that serves as the initialization of a mesh within the non-binarized scan. Growing the mesh is an iterative process of minimally altering the triangles’ tips (vertices) until they reach voxels with intensities below a locally calculated threshold. By this, BET relies on the change in intensity at the boundary from brain to cerebrospinal fluid (CSF).
ROBEX (Robust, Learning-Based Brain Extraction System) is considered a conventional hybrid tool (Kalavathi and Prasath, 2016), although it combines two ML models: a Random Forrest Classifier (RFC) as a discriminative model and a Point Distribution Model (PDM) as a generative model (Iglesias et al., 2011). For each voxel in an intensity-standardized scan, the RFC determines whether it is part of the brain outline, thus creating a single brain shape within a scan. Ten voxel features, which are linked to the voxels’ location (x-, y-, and z-coordinates) and intensity context (application of edge detection filters), serve as input to the RFC. The resulting brain shape is highly individual but might overshoot and not always be realistic. In contrast to the RFC, the PDM can generate a multitude of brain shapes by deforming a mean brain shape established from training data. The degree of deformation is restricted, which on the one hand prevents the PDM from creating unrealistic shapes, but on the other hand also prevents the shapes from perfectly matching an individual brain. ROBEX finds a compromise between the two ML methods by fitting a PDM shape to the RFC shape.
In contrast to conventional methods, such as BET and ROBEX, there are more modern approaches based on DL, such as HD-BET (Isensee et al., 2019). Its core component is a special type of convolutional neural net, the U-Net (Ronneberger et al., 2015). U-Net consists of a contracting path and an expansive part that are connected through skip-connections resulting in a u-shaped network scheme. The contracting path abstracts the image to its semantic essence by applying convolutions and thus reducing the feature map size. The gain in semantic information is paid for with a loss of localization information. In the expansive path, feature maps are enlarged again while adding previously lost localization information via the skip-connections to generate the image mask. During the training of HD-BET with a total of 1,500 scans, a five-fold cross-validation was performed, which resulted in five different U-Net models forming an ensemble for the brain mask prediction. HD-BET applies test time augmentation (TTA). This technique uses modified copies of the input image and their associated predicted masks to finetune and generate the final brain mask. As an alternative to the U-Net ensemble with TTA, HD-BET can be limited to using a single U-Net without TTA (referred to as HD-BET-fast in this paper).
SynthStrip is another U-Net-based model for skull stripping (Hoopes et al., 2022). Compared to HD-BET, it has a fundamentally different approach concerning its training data. With 80 T1-weighted MRI scans, only a very limited set of training data was used. But the data was vastly augmented during model training. The dynamic augmentation included translation, rotation, scaling and non-linear deformation to different degrees, which were randomly performed in each epoch. Further, 46 distinct anatomical regions within the scan were assigned randomly chosen voxel intensities and bias fields were introduced to varying extents. Additionally, the overall brightness of the scans was altered, and a Gaussian blur was introduced. Moreover, half of the time, the scans were randomly cropped and down sampled. This data augmentation strategy even led to unrealistic training images with the aim of creating a robust model for various input modalities. A specialized pediatric version, developmental SynthStrip (d-SnythStrip), was trained on a mixture of 57 T1-weighted (T1W) and T2-weighted (T2W) scans of children under the age of 4.5 years (Kelley et al., 2024). SynthStrip includes CSF in its brain masks by default. This behavior can be adapted for receiving segmentations without CSF (referred to as SynthStrip-noCSF). The immutable default of d-SynythStrip does not include any CSF in the brain masks.
Although required in the context of brain maturity assessment in children, few of the available skull stripping tools target pediatric populations (Das et al., 2023; Kelley et al., 2024). More specifically, for brain age predictions in children over the age of 6 months, T2-weighted MRI scans are recommended (Barkovich and Barkovich, 2018). However, the brain stripping tools mentioned above have not been evaluated on T2W pediatric scans. The only exception is d-SynthStrip, whose testing dataset included 39 scans of that kind. Rehman et al. (2020) pointed out that the performance of brain extraction tools may deteriorate when applied to different datasets and that there was a need for tools suited for modalities such as T2W scans.
Here, we investigate in a pediatric cohort the performance of seven open-source skull stripping models (BET, ROBEX, HD-BET, HD-BET-fast, SynthStrip, SynthStrip-noCSF, d-SynthStrip). For this, we use 199 clinical routine T2W MRI scans of children under the age of 5 years with normal brain development retrospectively retrieved at Hannover Medical School. By analyzing both the overall and regional segmentation performance, we provide researchers and clinical users in the field with a reliable recommendation. To our knowledge, there is yet no such evaluation, while other studies have focused on different aspects, such as neonatal populations (Vaz et al., 2024) or T1W scans (Das et al., 2023).
2 Materials and methods
2.1 Cohort
We acquired all available T2W MRI scans matching the inclusion criteria from the clinical routine at the Institute of Diagnostic and Interventional Neuroradiology of Hannover Medical School (MHH) between 2011 and 2023. Inclusion criteria were normal brain development, absence of any pathologies, age under 5 years and parental informed consent to the secondary data use for research purposes. Scans were checked by a senior neuroradiologist specialized in pediatric neuroradiology (EB) and excluded in case of relevant motion artifacts. The cohort included 199 children (94 female, 105 male) who had been scanned for the assessment of their brain development in general anesthesia or sedation. The age range in the cohort spanned from four to 1791 days (4.9 years) with a median age of 1.4 years, a mean (M) of 1.8 years and a standard deviation (SD) of 1.4 years (Figure 1). The research was approved by the ethics committee at MHH (Nr. 11658_BO_K_2024).

Figure 1. Distribution of age and sex within the cohort (n = 199).
2.2 MRI protocol
All scans were T2W scans with from either a Siemens Magnetom Verio 3 Tesla or a Siemens Avanto 1.5 Tesla MRI scanner. Due to the infants differing head sizes, the number of axial slices ranged from 24 to 44. Since all data originate from the clinical routine there is no consistent protocol. 162 scans had a voxel size of 0.43 mm × 0.43 mm × 4.00 mm and 4.00 mm spacing between slices. The remaining 37 scans had varying voxel dimensions and slice spacings (Supplementary Table A). Echo times ranged from 127 ms to 131 ms, repetition times from 2,860 ms to 9,010 ms, and flip angles from 120° to 150°.
2.3 Data preparation
We extracted the MRI scans from the PACS at MHH as DICOM files and converted them to NIFTI format with dcm2niix (version v1.0.20211006). Using Lanczos3 as a resampling filter from MeVisLab (version 3.7.0.14), we resampled the 37 scans with varying dimensions according to the voxel size and slice spacing of the other 162 scans (Figure 2). Based on these unified scans, referred to as “original” in this paper, we performed manual segmentation.

Figure 2. Curation of the original and the preprocessed dataset from the same 199 scans.
Data preprocessing was implemented in Python (version 3.12) and included four steps: resizing, contrast enhancement, artifact removal and normalization. By zero padding, we adjusted all scans to the size of the largest scan (484 voxels × 596 voxels × 40 voxels). For contrast enhancement, we applied an image specific threshold based on the triangle method. We handled artifacts by detecting objects through region property detection and only keeping the largest object in the image, which is the patient’s head including the skull (Figure 3). Finally, we min-max normalized the scans.

Figure 3. Axial slice of a T2-weighted MRI scan before (left) and after (right) artifact removal.
2.4 Ground truth
A medical student (ED) performed manual labeling of the scans using 3D Slicer (version 5.4.0) (Fedorov et al., 2012) and a neuroradiologist specialized in pediatric neuroradiology (EB) quality checked all manual segmentations, which were, if necessary, refined accordingly. The segmentation process was carried out in the axial plane according to the following rules. The segmentation of the outer boundary covers the entire cranial content. Therefore, voxels with partial volume sections (e.g., bone and parenchyma) are included. The cranial part of the Sinus sagittalis superior is only included if brain parenchyma is present within the slice. The frontobasal area, including the CSF around the olfactory nerve, is segmented. Further, all components of the Sinus durae matris and spaces containing CSF are included. The caudal segmentation includes the entire Cerebellum. The Medulla oblongata is included down to the level of the caudal edge of the cerebellar tonsils.
2.5 Segmentation models
In this paper, we assess seven open source skull stripping models, namely BET1 (version 6.0.7.14 as part of the FSL library), ROBEX2 (version 1.2), HD-BET and HD-BET-fast3 (both version 1.0), as well as SynthStrip, SynthStrip-noCSF and d-SynthStrip4 (as part of Freesurfer version 7.4.1, the pth-file containing weights and biases for d-SynthStrip was manually downloaded on December 17, 2024), on both the original and the preprocessed data. We ran all models on a NVIDIA A100 GPU with 40 GB VRAM on a Rocky Linux System (version 9.4). For all models, we monitored the computing time per scan.
2.6 Evaluation
For comparing the automated segmentations (S) with the manually established ground truth (GT), we calculated the Dice score, 95th percentile Hausdorff distance (HD95), sensitivity and specificity as evaluation metrics. Using the Dice score and HD95, we evaluated for each model whether data preprocessing should be applied. Based on that, we compared the models’ performance (Dice score and HD95) in whole scans and applied statistical testing. We used the Shapiro–Wilk test to check for normality in the metrics’ distributions. Then, we applied the Friedman test as a non-parametric test for related samples. A two-sided Wilcoxon signed-rank test served as a post-hoc test. The significance level was set to α = 0.05, and the p-values were adjusted based on the Bonferroni correction. For comparing the best with all competing models, we visualized the respective Dice score differences in Bland–Altman plots. Analog to Vaz et al. (2024), we analyzed the evaluation metrics in different brain regions by splitting the scans. With their 22 neonates, Vaz et al. (2024) defined fixed slice number ranges to distinguish three regions along the longitudinal scan axis. Since our cohort contains children of different ages and, therefore, scans with varying slice numbers, we based our splits on the dimensions of the corresponding ground truth masks. In the longitudinal direction, we performed three splits of equal size (superior, central and inferior axial slices). Additionally, we divided the brain along the transversal axis into its left and right sagittal slices. Along the sagittal axis, it was subdivided into the anterior and posterior coronal slices. In addition, a medical student (ED) and a physician (AS) manually assessed the integrity of different anatomical structures in the top and the lowest quartile of segmentations of the best performing model with 3D Slicer (Fedorov et al., 2012). Finally, we evaluated resampling, sex and age as potential covariates for the models’ overall performance. For each model, Dice score and HD95 distributions of the resampled and non-resampled cases were tested for normality with a Shapiro–Wilk test. Subsequently, we used the two-sided Brunner Munzel test as a non-parametric test, which tolerates unequal sample sizes to test Dice scores as well as HD95 in the 37 resampled scans against the 167 non-resampled ones for each model. The significance level was set to α = 0.05, and the p-values were adjusted based on the Bonferroni correction. The correlation of age and segmentation performance was quantified using the Pearson correlation coefficient (PCC) with |PCC| > 0.1 indicating a weak, |PCC| > 0.4 indicating a moderate and |PCC| > 0.7 indicating a strong correlation (Schober et al., 2018). For comparison, the Dice scores of each model were visualized as violin plots. The violins’ range is limited to the actual data range and the violins’ maximum width is constant. All calculations and visualizations were performed with Python (version 3.11). We use the reporting guideline STARE-HI (STAtement on the Reporting of Evaluation studies in Health Informatics) by Talmon et al. (2009) and provide the checklist in the supplements.
3 Results
A total of seven skull stripping models were evaluated on the original as well as the preprocessed dataset. We compared their segmentation results to the manually labeled ground truth by calculating different evaluation metrics (Figure 4 and Supplementary Table B). Median Dice scores were between 0.884 and 0.961, while the value ranges showed larger differences, especially due to data preprocessing.
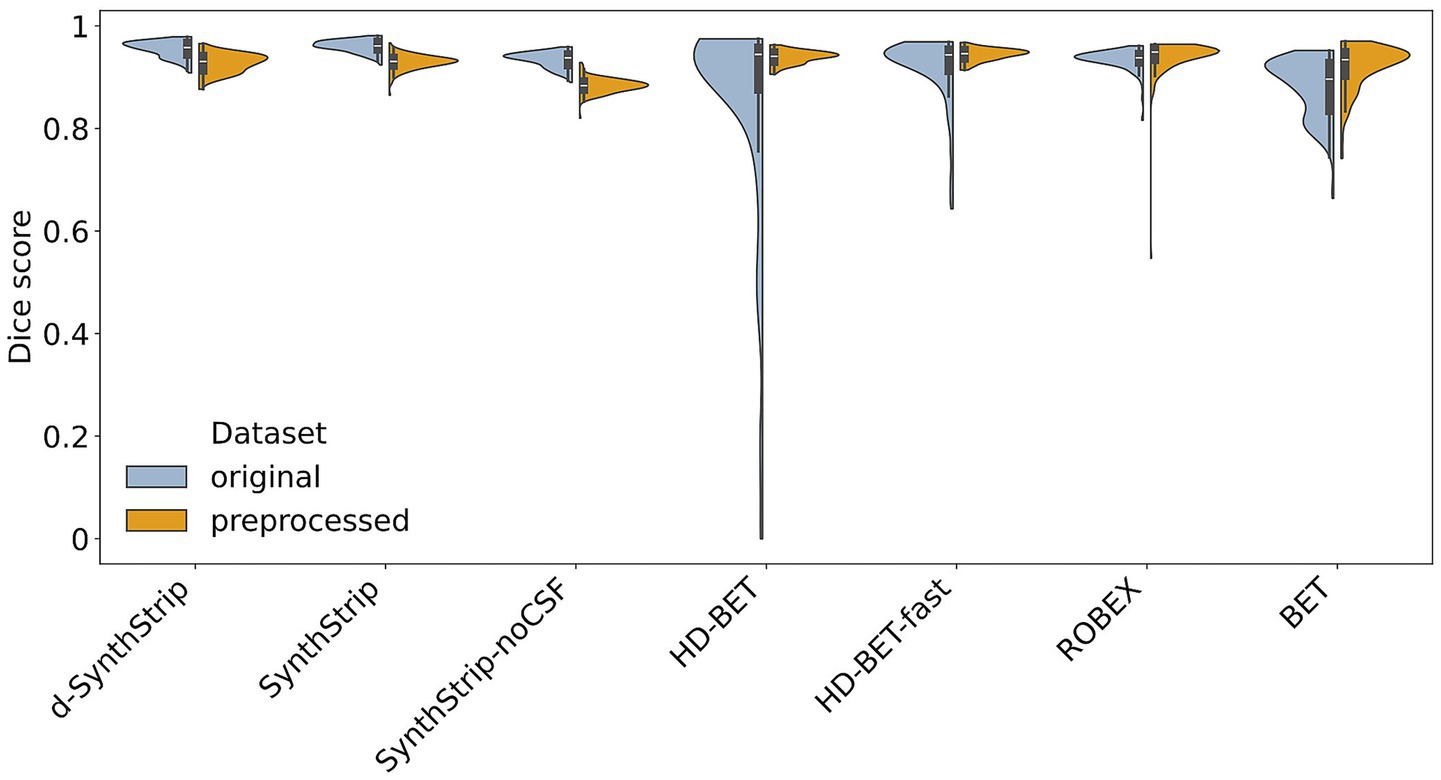
Figure 4. Performances of skull stripping models (Dice score) based on the original and the preprocessed scans of all 199 cases.
3.1 Data preprocessing influences the models’ segmentation results
Data preprocessing had varying effects on the models’ performances. BET was positively affected (Δ median Dice score = 0.038, Δ median HD95 score = −3.7 mm) including a narrower value range in both metrics. Although both HD-BET and HD-BET-fast had slightly higher median Dice scores and a smaller median HD95 on the original dataset, their value ranges drastically improved through preprocessing. The positive influence of preprocessing on ROBEX was limited to the median Dice score, whereas the HD95 and the respective value ranges deteriorated. Preprocessing negatively affected all of SynthStrip-related models, lowering their median Dice score by up to 0.054 and increasing the median HD95 by 2.9 mm – 8.0 mm, while broadening their respective value ranges. Thus, only three models, namely BET, HD-BET-fast and HD-BET, were improved by data preprocessing.
3.2 Skull stripping models differ in their segmentation performance
To compare the skull-stripping models, we used each model’s best-performing data preprocessing configuration (original vs. preprocessed dataset). SynthStrip achieved the highest median Dice score (0.961, [0.924–0.981]) and the smallest median HD95 (4.0 mm, [2.3 mm – 8.0 mm]) followed by d-SynthStrip. The lowest median Dice score (0.934, [0.742–0.970]) and the largest median HD95 (12.3 mm, [4.0 mm – 44.4. mm]) were observed using BET. ROBEX also had a low Dice score performance. In contrast, concerning their sensitivity, ROBEX and BET had the highest median values (0.993 and 0.942), whereas SynthStrip-noCSF and HD-BET were the least sensitive models (0.885 and 0.892). The median specificity of all models was remarkably high with ROBEX and BET being the only models below 0.99.
All model comparisons apart from three exceptions (SynthStrip-noCSF vs. BET, ROBEX vs. SynthStrip-noCSF, ROBEX vs. HD-BET) showed statistically significant Dice score and HD95 differences (Supplementary Table C). Thus, the performance advantage of SynthStrip over all other tools is most likely not based on chance. Bland–Altman plots (Figure 5) reveal, that the elevation of SynthStrip’s mean Dice score by 0.01 to 0.04 in comparison to the other skull stripping models is also reflected on an individual level. BET and d-SynthStrip achieved higher Dice scores in 17% of the cases and the remaining models outperformed SynthStrip in only under 10% of the scans. The margin by which models outperformed SynthStrip in these cases was small compared to the margin in the majority of cases, where they underperformed. When comparing SynthStrip to BET as well as ROBEX, this margin clearly increased with the decrease in combined mean performance. This tendency is also visible in the comparison to d-SynthStrip and SynthStrip-noCSF.

Figure 5. Bland–Altman plots comparing the segmentation performance (Dice score) of SynthStrip on all 199 cases to the segmentation performances of the six other skull stripping models.
With a mean computation time per scan of 7 s (SD = 0.90), SynthStrip was among the faster models with only BET being considerably quicker (M = 2.4 s, SD = 0.62), whereas ROBEX (M = 40.8 s, SD = 2.38) and HD-BET (M = 132 s, SD = 0.83) had a substantially higher computing time (Table 1).

Table 1. Descriptive statistics of the models’ computing time in seconds over all 199 cases.
3.3 Regional segmentation performances
Along the longitudinal scan axis, all models performed better in the central region compared to the inferior one (Δ median Dice scores = [0.036–0.063], Δ median HD95 = [−3.2 mm – −0.4 mm]). With the single exception of BET, this was also observed when comparing the central to the superior region (Figure 6 and Supplementary Table D). In the central region, all models’ median Dice scores lay above 0.961 and the median HD95 below 8.0 mm with SynthStrip achieving the best values (median Dice score = 0.985, median HD95 = 1.4 mm). The comparison of the left and right hemisphere (Supplementary Figure E and Supplementary Table E) did not reveal any considerable differences (Δ median Dice scores ≤ 0.01, Δ median HD95 ≤ 1.0 mm). The only model clearly showing better values for both the Dice score and the HD95 in the posterior region compared to the anterior one was SynthStrip-noCSF (Δ median Dice scores = 0.036, Δ median HD95 = 3.3 mm) (Supplementary Figure F and Supplementary Table F).

Figure 6. Regional skull stripping performances (Dice score) along the longitudinal scan axis in the superior (A), central (B) and inferior region (C).
Regarding the best performing model, SynthStrip, in about one third of the highest and lowest quartiles of segmentations, the Cerebellum was not entirely detected (Table 2). In about two thirds of these cases, the Sinus sagittalis superior, the Chisma opticum/pituitary gland and the pole of the temporal lobe were partially missing. With only four exceptions, the upper axial slices of the cerebrum were not fully segmented (Figure 7). In the central slices in over 90% of these cases, anterior and lateral CSF was missing, whereas parts of the posterior and lateral skull were included. Parts of the petrous bone were also included in 81%.

Table 2. Manual assessment of multiple anatomical brain structures in the highest and lowest quartiles of SynthStrip segmentations with respect to the Dice score.

Figure 7. Exemplary SynthStrip segmentations (blue) and the corresponding ground truth (red). The percentiles refer to the Dice score distribution of all 199 cases.
3.4 Potential covariates
All SynthStrip-related models dropped statistically significant in their segmentation performance regarding both Dice score and HD95 when comparing the 162 non-resampled scans to the 37 resampled ones (Table 3 and Supplementary Figure G and Supplementary Table G). For HD-BET-fast only the Dice score difference was statistically significant. Sex did not alter the segmentation performance of any model (Supplementary Figure H and Supplementary Table H). The segmentation performance of BET showed a strong correlation with the covariate age with a PCC of −0.734 (Figure 8). Its median Dice score gradually decreased from 0.950 under the age of one until it was 0.857 during the fifth year of life (Supplementary Table J). Contrarily, all SynthStrip-related models as well as HD-BET-fast showed a performance increase of 0.015 to 0.027 over the same age span with a moderate correlation (PCCs between 0.564 and 0.633).

Table 3. Segmentation performance metrics on 37 resampled MRI scans and 162 non-resampled scans.

Figure 8. Linear regression analysis of segmentation performance (Dice score) in relation to infants’ age for all 199 cases (PCC: Pearson correlation coefficient).
4 Discussion
Rehman et al. (2020) postulate a gap between the use of skull stripping tools in research and their use in clinical routine. Robustness, computing time and user-friendly application were considered the main obstacles to overcome. We hope to narrow the implementation gap through the evaluation of different skull stripping tools in pediatric T2W MRI scans. Although not trained with a focus on this use case, all models exhibited decent median segmentation performances. Nevertheless, we recommend SynthStrip since it is the most robust model with a quick computational time.
In our study, SynthStrip achieved the highest Dice score, which measures the overall agreement between ground truth and segmentation but potentially underrepresents the contour of the brain. SynthStrip also had the highest HD95 score, which is solely based on the brain’s contour. Therefore, the model segments both the inner structures and the outer shape of the brain more reliably than the other models. Varying margins in the Bland–Altman plots indicate that SynthStrip handles cases well when other models’ segmentations are less satisfactory. The observed differences were statistically significant. For interpreting the results of the statistical tests, our study setting should be taken into consideration. Usually, power calculations are used to determine adequate cohort sizes for detecting an anticipated effect without involving too many subjects, which can be connected to ethical as well as economic implications (Kang, 2021). Since our study was carried out retrospectively on clinical routine data, it was not affected by these implications. Therefore, we used all available data from the clinical routine resulting in a considerably large cohort. This generally leads to more reliable results, but at the same time to statistical significance even though differences observed are small (“overpowered” setting).
The developers of SynthStrip (Hoopes et al., 2022) published comparisons to ROBEX as well as BET on three adult T2W MRI datasets: IXI5, FSM (Greve et al., 2021) and QIN (Mamonov and Kalpathy-Cramer, 2016). In the three datasets, SynthStrip had mean Dice scores of 0.96, 0.98 and 0.95, respectively, and outperformed ROBEX as well as BET. The two models were also outperformed by HD-BET in its original publication (Isensee et al., 2019) when tested on T1W scans. This is in concordance with our findings and the notion that deep learning models outperform classical skull stripping methods (Fatima et al., 2020).
In contrast to our study, Vaz et al. (2024) found that SynthStrip was outperformed by HD-BET by approximately 1% in T2W pediatric scans. Possible explanations include their small cohort and a differing age distribution (22 premature neonates). The finding of Kelley et al. (2024), that d-SynthStrip outperforms SynthStrip on pediatric T2W MRI scans, is also not supported by our results. Kelley et al. investigated the models’ performances on two pediatric cohorts with T2W scans, which led to median Dice scores of 0.97 and 0.96 for SynthStrip, whereas d-SynthStrip showed median Dice scores of approximately 0.98 in both cohorts. Although the performance of SynthStrip in these cohorts aligns with our measurements, the median Dice score of d-SynthStrip is 0.02 lower in our setting. The most likely explanation is the exclusion of CSF by Kelley et al., whereas in our study CSF was included. This explanation is supported by the segmentation performance difference between SynthStrip and SynthStrip-noCSF in our research which was also 0.02. Generally, the lack of fixed segmentation rules is an obstacle to standardized skull stripping tools. Using SynthStrip, the inclusion and exclusion of CSF can easily be switched through the noCSF-parameter.
The fact that SynthStrip can compete with the pediatric model d-SynthStrip, shows that its data augmentation strategy compensates for the difference in training data. d-SynthStrip was trained on a mixture of 57 T1W and T2W scans of children under the age of 4.5 years, whereas the training data of SynthStrip exclusively included T1W scans and only 10 out of 80 scans belonged to infants which were all under the age of 1.5 years. The success of the data augmentation strategy is also evident in the comparison of SynthStrip and HD-BET, which both have U-Net-based architectures. HD-BET was trained on as many as 6,586 MRI sequences with a fifth of them being T2-weighted but did not yield better results than SynthStrip.
The robustness of SynthStrip, reflected by its narrow value range, has also been observed in T1W pediatric MRI scans. Das et al. (2023) observed that SynthStrip provided good results where other models (BET, Freesurfer) failed. However, their finding that SynthStrip leaves the frontal lobe and other brain structures in T1-weighted scans intact, differs from our experience with T2W scans. Despite its high overall performance, SynthStrip has shortcomings. We found that parts of the upper brain slices, the temporal poles and the Cerebellum were prone to be omitted, which may be linked to the partial volume effect (PVE) at their borders. The PVE describes the phenomenon of capturing multiple tissues within a voxel and is known to impair the accuracy of brain segmentations (Tohka, 2014). Eventually, the PVE is also the reason why the petrous bone has, on the other hand, often been included. Albeit not being included in the brain regions SynthStrip was trained on, the Chiasma opticum/pituitary gland as well as the Sinus sagittalis superior were segmented in about one third of the cases. But this rate is not sufficient for using the tool in diagnostics linked to these structures (e.g., adenoma of the pituitary gland or thrombosis of the Sinus sagittalis superior). In alignment with the research by Vaz et al. (2024), SynthStrip performed best in the middle slices of the brain. Nevertheless, we witnessed errors in the skull exclusion and CSF inclusion in these slices. Due to the small size of the affected area, this did not lead to a considerable Dice score decrease.
Generally, the SynthStrip-related models are the computationally most efficient models. Although BET is faster, it requires time-consuming data preprocessing, which nullifies its advantage. In contrast, SynthStrip-related models can be directly applied to data from the clinical routine. The reason why Vaz et al. (2024) measured a computation time of SynthStrip almost 40 times above ours, is the usage of superseded consumer grade hardware for the calculations (a laptop from 2015).
For ML applications that require skull stripped MRI scans with standardized input dimensions, scans need to be resampled. In these cases, we recommend skull stripping before resampling to obtain the best possible brain segmentation. Although, we did not analyze the segmentation performance before and after resampling on the same scans, the comparison of the 162 non-resampled scans to the 37 resampled ones showed a drop in performance. Drai et al. (2022) did not recognize any age-dependent alterations in the performance of HD-BET or BET. For the latter, there was a steady performance decrease in correlation with the infants’ age in our study, whereas the performance of SynthStrip as well as d-SynthStrip increased. To our knowledge, there is no literature investigating the impact of age on the performance of SynthStrip or d-SynthStrip. Still, the influence could be derived from the drastic brain changes taking place within the first 6 years of life. During this period, the brain volume expands and changes in voxel intensity occur due to the process of myelination. In the younger, less myelinated brains, the contrast is lower making it more difficult to distinguish different anatomical structures from one another (Phan et al., 2018).
A limitation of our study is its monocentric design, which could cause selection bias. Further, the dataset used is skewed toward younger children with ages under 1 year. Since SynthStrip had its lowest performance in that age group and most of the other models did not show age-related performance alterations, this should be negligible regarding model comparisons. The fact that there are only subjects with non-pathological scans in the cohort is also a limitation. Therefore, the skull stripping performance when bleedings, cancer, or other pathologies are present, could not be assessed. Our assessment of regional segmentation performances is based on splits derived from the dimensions of the ground truth masks. Although, the assessment is therefore limited to brought areas of the brain, it aligns well with the manual findings. For directly linking segmentations performances to distinct anatomical structures extensive labeling would be required.
On the other hand, our study has several strengths. The cohort size (n = 199) is comparably large in the field of brain segmentation, where small sample sizes are frequent. Vaz et al. (2024) with a cohort of n = 22 cited multiple publications with test datasets of an equal or smaller size (Shattuck et al., 2001; Péporté et al., 2011; Eskildsen et al., 2012; Mahapatra, 2012; Serag et al., 2016; Kobashi and Udupa, 2013). According to them, the time-consuming manual segmentation is a reason for the small cohorts. In our study, we invested considerable resources in creating ground truth masks, which were quality-checked by a senior expert in the field.
In this study, we evaluated different skull stripping tools in pediatric T2W MRI scans. Generally, all tools lead to acceptable results in most cases, although some require prior data preprocessing. However, we recommend SynthStrip and its application prior to any resampling, if needed. SynthStrip showed the most stable segmentation performance on non-preprocessed (“original”) data and a small computation time, which are two requirements formulated by Rehman et al. (2020) for skull stripping tools. The third requirement, a user-friendly application, is also met with only a single line command necessary to execute the model. Especially for clinicians, it would be even more user-friendly, if a graphical user interface, such as an extension to 3D Slicer (Fedorov et al., 2012), was available. In the future, brain extraction assessment should be expanded to multicenter settings, also including pathological cases. Furthermore, future research should address the partial volume effect, as it has led to segmentation inaccuracies.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: a publication of pediatric MRI scans is not possible due to privacy concerns. Requests to access these datasets should be directed to QnVlbHRtYW5uLkV2YUBtaC1oYW5ub3Zlci5kZQ==.
Ethics statement
The studies involving humans were approved by Ethics Committee of Hannover Medical School. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
ASchu: Conceptualization, Formal analysis, Investigation, Software, Visualization, Writing – original draft. ED: Data curation, Formal analysis, Writing – review & editing. KW: Data curation, Software, Visualization, Writing – review & editing. AScho: Software, Writing – original draft. EB: Conceptualization, Data curation, Investigation, Supervision, Writing – review & editing. DW: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft.
Funding
The author(s) declared that financial support was received for this work and/or its publication. The study was carried out as part of the project “Interoperable and eXplainable clinical decision support (iXplain_CDS)” funded by the German Federal Ministry of Education and Research (BMBF) (grant no. 01ZZ2021).
Conflict of interest
The author(s) declared that this work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declared that Generative AI was not used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2025.1715514/full#supplementary-material
Abbreviations
AI, artificial intelligence; COG, center of gravity; CSF, cerebrospinal fluid; DL, deep learning; GT, ground truth; HD95, 95th percentile Hausdorff distance; M, mean; MHH, Hannover Medical School; ML, machine learning; SD, standard deviation; PCC, Pearson correlation coefficient; PVE, partial volume effect; T1W, T1-weighted; T2W, T2-weighted; TTA, test time augmentation.
Footnotes
1.^BET:https://fsl.fmrib.ox.ac.uk/fsl/docs/structural/bet.html, last access November 12, 2025.
2.^ROBEX:https://www.nitrc.org/projects/robex, last access November 12, 2025.
3.^HD-BET&HD-BET-fast:https://github.com/MIC-DKFZ/HD-BET, last access November 12, 2025.
4.^SynthStrip,SynthStrip-noCSFandd-SynthStrip:https://surfer.nmr.mgh.harvard.edu/docs/synthstrip/, last access November 12, 2025.
5.^IXI-Dataset:https://brain-development.org/ixi-dataset/, last accessed August 25, 2025.
References
Allen, J. S., Bruss, J., Brown, C. K., and Damasio, H. (2005). Normal neuroanatomical variation due to age: the major lobes and a parcellation of the temporal region. Neurobiol. Aging 26, 1245–1260. doi: 10.1016/j.neurobiolaging.2005.05.023,
Barkovich, A. J., and Barkovich, M. J. (2018). “Normal development of the fetal, neonatal, and infant brain, skull, and spine – milestones” in Pediatric neuroimaging. ed. S. Zinner. Sixth ed (Philadelphia: Wolters Kluwer).
Bernal, J., Kushibar, K., Asfaw, D. S., Valverde, S., Oliver, A., Martí, R., et al. (2019). Deep convolutional neural networks for brain image analysis on magnetic resonance imaging: a review. Artif. Intell. Med. 95, 64–81. doi: 10.1016/j.artmed.2018.08.008,
Das, A., Duarte, K. T. N., Wong, S., Mamoun, Y., and Bento, M. (2023). “Comparative skull stripping techniques on pediatric magnetic resonance imaging” in 2023 19th International Symposium on Medical Information Processing and Analysis (SIPAIM), 1–4.
Dragendorf, E., Bültmann, E., and Wolff, D. (2024). Quantitative assessment of neurodevelopmental maturation: a comprehensive systematic literature review of artificial intelligence-based brain age prediction in pediatric populations. Front. Neuroinform. 18:1496143. doi: 10.3389/fninf.2024.1496143
Drai, M., Testud, B., Brun, G., Hak, J. F., Scavarda, D., Girard, N., et al. (2022). Borrowing strength from adults: transferability of AI algorithms for paediatric brain and tumour segmentation. Eur. J. Radiol. 151:110291. doi: 10.1016/j.ejrad.2022.110291,
Eskildsen, S. F., Coupé, P., Fonov, V., Manjón, J. V., Leung, K. K., Guizard, N., et al. (2012). BEaST: brain extraction based on nonlocal segmentation technique. NeuroImage 59, 2362–2373. doi: 10.1016/j.neuroimage.2011.09.012,
Fatima, A., Shahid, A. R., Raza, B., Madni, T. M., and Janjua, U. I. (2020). State-of-the-art traditional to the machine- and deep-learning-based skull stripping techniques, models, and algorithms. J. Digit. Imaging 33, 1443–1464. doi: 10.1007/s10278-020-00367-5,
Fedorov, A., Beichel, R., Kalpathy-Cramer, J., Finet, J., Fillion-Robin, J. C., Pujol, S., et al. (2012). 3D slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 30, 1323–1341. doi: 10.1016/j.mri.2012.05.001,
Greve, D. N., Billot, B., Cordero, D., Hoopes, A., Hoffmann, M., Dalca, A. V., et al. (2021). A deep learning toolbox for automatic segmentation of subcortical limbic structures from MRI images. NeuroImage 244:118610. doi: 10.1016/j.neuroimage.2021.118610,
Hoopes, A., Mora, J. S., Dalca, A. V., Fischl, B., and Hoffmann, M. (2022). SynthStrip: skull-stripping for any brain image. NeuroImage 260:119474. doi: 10.1016/j.neuroimage.2022.119474,
Iglesias, J. E., Liu, C.-Y., Thompson, P. M., and Zhuowen, T. (2011). Robust brain extraction across datasets and comparison with publicly available methods. IEEE Trans. Med. Imaging 30, 1617–1634. doi: 10.1109/TMI.2011.2138152,
Isensee, F., Schell, M., Pflueger, I., Brugnara, G., Bonekamp, D., Neuberger, U., et al. (2019). Automated brain extraction of multisequence MRI using artificial neural networks. Hum. Brain Mapp. 40, 4952–4964. doi: 10.1002/hbm.24750,
Kalavathi, P., and Prasath, V. B. S. (2016). Methods on skull stripping of MRI head scan images—a review. J. Digit. Imaging 29, 365–379. doi: 10.1007/s10278-015-9847-8,
Kang, H. (2021). Sample size determination and power analysis using the G*power software. J. Educ. Eval. Health Prof. 18, 1–12. doi: 10.3352/jeehp.2021.18.17,
Kelley, W., Ngo, N., Dalca, A. V., Fischl, B., Zöllei, L., and Hoffmann, M. (2024). “Boosting skull-stripping performance for pediatric brain images” in 2024 IEEE International Symposium on Biomedical Imaging (ISBI), 1–5.
Kobashi, S., and Udupa, J.K. (2013) Fuzzy connectedness image segmentation for newborn brain extraction in MR images, in. 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), 7136–7139.
Lenroot, R. K., and Giedd, J. N. (2006). Brain development in children and adolescents: insights from anatomical magnetic resonance imaging. Neurosci. Biobehav. Rev. 30, 718–729. doi: 10.1016/j.neubiorev.2006.06.001,
Mahapatra, D. (2012). Skull stripping of neonatal brain MRI: using prior shape information with graph cuts. J. Digit. Imaging 25, 802–814. doi: 10.1007/s10278-012-9460-z,
Mamonov, A. B., and Kalpathy-Cramer, J. (2016). Data from QIN GBM treatment response. United States: The Cancer Imaging Archive.
Morita, R., Ando, S., Fujita, D., Ishikawa, S., Onoue, K., Ando, K., et al. (2022) Quantification of pediatric brain development with X-ray CT images using 3D-CNN, in. 2022 Joint 12th International Conference on Soft Computing and Intelligent Systems and 23rd International Symposium on Advanced Intelligent Systems (SCIS & ISIS), 1–3.
Péporté, M., Ghita, D. E. I., Twomey, E., and Whelan, P. F. (2011). “A hybrid approach to brain extraction from premature infant MRI” in Image Analysis. eds. A. Heyden and F. Kahl (Berlin, Heidelberg: Springer), 719–730.
Phan, T. V., Smeets, D., Talcott, J. B., and Vandermosten, M. (2018). Processing of structural neuroimaging data in young children: bridging the gap between current practice and state-of-the-art methods. Dev. Cogn. Neurosci. 33, 206–223. doi: 10.1016/j.dcn.2017.08.009,
Rehman, H. Z. U., Hwang, H., and Lee, S. (2020). Conventional and deep learning methods for skull stripping in brain MRI. Appl. Sci. 10:1773. doi: 10.3390/app10051773
Ronneberger, O., Fischer, P., and Brox, T. (2015). “U-net: convolutional networks for biomedical image segmentation” in Medical image computing and computer-assisted intervention – MICCAI 2015. eds. N. Navab, et al. (Cham: Springer International Publishing), 234–241.
Schober, P., Boer, C., and Schwarte, L. A. (2018). Correlation coefficients: appropriate use and interpretation. Anesth. Analg. 126, 1763–1768. doi: 10.1213/ANE.0000000000002864,
Serag, A., Blesa, M., Moore, E. J., Pataky, R., Sparrow, S. A., Wilkinson, A. G., et al. (2016). Accurate learning with few atlases (ALFA): an algorithm for MRI neonatal brain extraction and comparison with 11 publicly available methods. Sci. Rep. 6:23470. doi: 10.1038/srep23470,
Shattuck, D. W., Sandor-Leahy, S. R., Schaper, K. A., Rottenberg, D. A., and Leahy, R. M. (2001). Magnetic resonance image tissue classification using a partial volume model. NeuroImage 13, 856–876. doi: 10.1006/nimg.2000.0730,
Smith, S. M. (2002). Fast robust automated brain extraction. Hum. Brain Mapp. 17, 143–155. doi: 10.1002/hbm.10062,
Stiles, J., and Jernigan, T. L. (2010). The basics of brain development. Neuropsychol. Rev. 20, 327–348. doi: 10.1007/s11065-010-9148-4,
Talmon, J., Ammenwerth, E., Brender, J., Dekeizer, N., Nykanen, P., and Rigby, M. (2009). STARE-HI—statement on reporting of evaluation studies in health informatics. Int. J. Med. Inform. 78, 1–9. doi: 10.1016/j.ijmedinf.2008.09.002,
Tohka, J. (2014). Partial volume effect modeling for segmentation and tissue classification of brain magnetic resonance images: a review. World J. Radiol. 6, 855–864. doi: 10.4329/wjr.v6.i11.855,
Keywords: evaluation, skull stripping, magnetic resonance imaging, T2-weighted, pediatrics, dice score, retrospective studies
Citation: Schulz A, Dragendorf E, Wendt K, Schomakers A, Bültmann E and Wolff D (2025) Skull stripping tools in pediatric T2-weighted MRI scans: a retrospective evaluation of segmentation performance. Front. Neurosci. 19:1715514. doi: 10.3389/fnins.2025.1715514
Edited by:
Laura Cabral, University of Pittsburgh, United StatesReviewed by:
Yuchuan Zhuang, AbbVie, United StatesNegar Noorizadeh, College of Medicine, University of Tennessee Health Science Center (UTHSC), United States
Copyright © 2025 Schulz, Dragendorf, Wendt, Schomakers, Bültmann and Wolff. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adrian Schulz, YWRyaWFuLnNjaHVsekBwbHJpLmRl
†These authors have contributed equally to this work