Explore article hub
 Mariona Estapé Senti1
Mariona Estapé Senti1 Alexandre Ceccaldi2
Alexandre Ceccaldi2 Marta Luciani1
Marta Luciani1 Nadine Saber1
Nadine Saber1 Paul J. L. Schurmann3
Paul J. L. Schurmann3 Maurits W. Geerlings4
Maurits W. Geerlings4 Peter Holig5Joel de Beer6Michael Hannus7
Peter Holig5Joel de Beer6Michael Hannus7 Fred Campbell8Martin Winter9Wim van Hoeve10Maurits Westerik11Kim D. Dorst-Mooiman12
Fred Campbell8Martin Winter9Wim van Hoeve10Maurits Westerik11Kim D. Dorst-Mooiman12 Jan Dekker12
Jan Dekker12 Sabine Fuchs3
Sabine Fuchs3 Floor Wolbers13
Floor Wolbers13 Tim Segers14,15,16
Tim Segers14,15,16 Maarten IJzerman17
Maarten IJzerman17 Hanna MG Barriga18
Hanna MG Barriga18 Marie L. De Bruin19
Marie L. De Bruin19 Sven Even Borgos20Molly M. Stevens18,21
Sven Even Borgos20Molly M. Stevens18,21 Pieter Cullis22
Pieter Cullis22 Raymond M. Schiffelers1,23*
Raymond M. Schiffelers1,23*- 1Central Diagnostic Laboratory (CDL) Research, University Medical Center (UMC) Utrecht, Utrecht, Netherlands
- 2European Technology Platform Nanomedicine (ETPN), Paris, France
- 3Metabolic Diseases, Wilhelmina Children’s Hospital, UMC Utrecht, Utrecht, Netherlands
- 4CelluTx Inc, Wayne, PA, United States
- 5Lipoid GmbH, Ludwigshafen, Germany
- 6Anjarium Biosciences AG, Schlieren, Switzerland
- 7siTOOLS GmbH, Planegg, Germany
- 8NanoVation Therapeutics UK Ltd†, Didcot, United Kingdom
- 9Curevac, Tübingen, Germany
- 10Solstice Pharmaceuticals bv, Enschede, Netherlands
- 11Leiden Academic Centre for Drug Research, Leiden University, Leiden, Netherlands
- 12Hospital Pharmacy, UMC Utrecht, Utrecht, Netherlands
- 13Applied Nanotechnology Research Group, Saxion University of Applied Sciences, Enschede, Netherlands
- 14BIOS/Lab on a Chip Group, University of Twente, Enschede, Netherlands
- 15Max-Planck Center Twente for Complex Fluid Dynamics, University of Twente, Enschede, Netherlands
- 16MESA+ Institute for Nanotechnology, University of Twente, Enschede, Netherlands
- 17Erasmus School of Health Policy & Management, Erasmus University Rotterdam, Rotterdam, Netherlands
- 18Department of Medical Biochemistry and Biophysics, Karolinska Institute, Stockholm, Sweden
- 19Pharmacoepidemiology & Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences (UIPS), Department of Pharmaceutical Sciences, Utrecht University, Utrecht, Netherlands
- 20Department of Biotechnology and Nanomedicine, SINTEF Industry, Trondheim, Norway
- 21Kavli Institute for Nanoscience Discovery, Department of Physiology, Anatomy and Genetics, and Department of Engineering Science, University of Oxford, Oxford, United Kingdom
- 22Life Sciences Centre (LSC), University of British Columbia, Vancouver, BC, Canada
- 23Nanocell Therapeutics, Inc, Wayne, PA, United States
Abstract
The NANOSPRESSO project is a pioneering response to the complex challenge of treating orphan diseases, which, despite affecting millions of people globally, have only scant therapeutic options. This initiative represents a paradigm shift by decentralizing the production of personalized nucleic acid nanomedicines. Integrating advanced microfluidic technology with lipid nanoparticle engineering platforms—validated by their efficacy in COVID-19 messenger (m)RNA vaccines—the NANOSPRESSO model enables hospital pharmacists to seamlessly assemble tailored therapeutic cartridges for gene/RNA therapy administration at the patient’s bedside. This innovative model subverts the traditional constraints of high-cost, intricate manufacturing and the instability of nucleic acid-based treatments, offering a streamlined. localized, flexible, and patient-centric alternative. Inspired by the traditional art of compounding in pharmacy, NANOSPRESSO strives to democratize access to innovative treatments for rare diseases, challenging the conventional, monolithic medical approach. Alongside its technological breakthroughs, the project also engages in proactive dialogue with regulatory authorities to ensure compliance with stringent quality, safety, and efficacy standards, applying an array of analytical techniques recently developed for nucleic acid nanomedicines. Orchestrated by an extensive European consortium of multidisciplinary experts, NANOSPRESSO embodies the collaborative spirit driving the next wave of healthcare innovation, placing patients at the center of a precision medicine revolution. This article conveys the core mission of NANOSPRESSO: to redefine the reach and impact of nanomedicine, heralding a future in which personalized therapy for rare and orphan diseases—and potentially other conditions—is a reality, available to patients and affordable by public health systems. We outline the scientific and technological basis for this model, explore various regulatory, legal, economic, and societal implications and challenges, and advocate for interdisciplinary solutions across the research and innovation ecosystem.
Key points
- Nucleic acid therapeutics could offer high-precision treatments targeting the protein anomalies underlying many conditions, with applications spanning noncommunicable diseases, such as cancer and rare “orphan” diseases, and vaccines with high adaptability, as evidenced by the mRNA vaccine responses to COVID-19 variants.
- Despite their unique adaptability and high precision for personalized care, nucleic acid therapeutics have been held back by pharmaceutical challenges, commercial disincentives in rare orphan diseases, the approval and reimbursement landscape, and their high costs.
- Nucleic acid therapeutics (involving essentially the same molecule, differing only in length and sequence) are uniquely qualified for platform-based personalized production in local hospital pharmacies, echoing the bespoke approach needed for orphan diseases.
- Novel nanomedicine platforms that encapsulate nucleic acids within lipid nanoparticles deliver these therapeutics to their intracellular sites of action and are suitable for small-scale manufacturing, mirroring the versatility required to address the myriad presentations of orphan diseases.
- The NANOSPRESSO model fuses nucleic acid therapeutics and nanomedicine delivery platforms to offer a flexible new paradigm of rapid, personalized therapeutics produced at the point of care—democratizing access to these innovative therapies, particularly for orphan diseases and low-income regions.
- Interdisciplinary and intersectoral collaboration between scientists, engineers, entrepreneurs, healthcare providers, policymakers, regulators, payers, and patients is pivotal to realizing the full potential of these innovative therapies while ensuring their financial sustainability and accessibility.
Introduction
Nucleic acid therapeutics are revolutionizing medicine, offering significant potential to treat an array of diseases. Nucleic acid therapeutics represent a leap forward in our capacity to combat diseases (1) from infectious outbreaks, such as COVID-19, to the complex challenges posed by multifactorial noncommunicable diseases, such as cancer (2, 3). This is because nucleic acids can interfere precisely with the synthesis of proteins, which is at the root of virtually all diseases. Nucleic acids can encode missing or mutated proteins, as well as proteins produced at suboptimal levels, e.g., a tumor-suppressive protein in cancer or a functioning enzyme in patients suffering from metabolic diseases due to a non-functional mutated enzyme, such as methylmalonic acidemia (MMA). Conversely, if too much of a pathogenic protein is being produced, nucleic acids can silence their production (e.g., a pro-inflammatory protein in auto-immune diseases or a mutated protein causing plaques in hereditary transthyretin amyloidosis). The promise of nucleic acid therapeutics is particularly strong in the field of orphan diseases, where traditional pharmacological interventions have often fallen short (4–6). Although each orphan disease affects only a small population—defined by the European Medicines Agency (EMA) as no more than 5 in 10,000 people—there are 5000–8000 such diseases and hence the total population of affected patients is enormous. About 36 million of the 449 million people living in the European Union alone suffer from a rare disease (7, 8).
At their core, nucleic acid therapeutics are based on the fundamental building blocks of life—the nucleic acids DNA and RNA—which encode and modulate the genetic information of all living organisms. The increased availability of molecular biology tools over the past decades has reshaped our understanding of and approach to cell biology, genetic engineering, disease modelling, and therapeutic interventions. Nucleic acid therapeutics redefine the possibilities for patient care, from the pioneering use of antisense oligonucleotides (ASOs) to block messenger RNAs (mRNAs) and produce disease causing proteins (9–12) to the advanced genome-editing capabilities of clustered regularly spaced short palindromic repeats (CRISPR)/CRISPR-associated endonuclease (Cas9) (13–15).
Despite their potential, nucleic acid therapeutics have encountered formidable barriers to their development and accessibility, rooted in economic and pharmaceutical constraints. High costs, complex manufacturing processes, and stringent regulatory requirements have historically impeded the progress of nucleic acid-based treatments, particularly for orphan diseases affecting small patient populations (6, 16). The medical use of nucleic acids is hampered by their large size and strong negative charge, which differ markedly from conventional therapeutics. In addition, their site of activity is within the diseased cell. To get such a large and charged molecule across the essentially impermeable membrane that protects every cell is a major challenge (17, 18). In 2018, a breakthrough nanotechnology-based medicine emerged, achieving the delivery of nucleic acid therapeutics into cells (19, 20). The same nanomedicine recipe was essential for the success of the COVID-19 mRNA vaccines (21, 22). These are clear examples of the great potential and clinical impact nanomedicine has shown in recent years to better diagnose, treat, and monitor patients suffering from a wide range of diseases (23).
This convergence of nucleic acid therapeutics and advanced nanomedicine delivery systems sets the stage for a new intervention paradigm, particularly impactful for orphan diseases. The NANOSPRESSO project (www.nanospresso.eu) exemplifies a vision where hospitals locally produce personalized nucleic acid treatments directly at the patient’s bedside. This disruptive model leverages the uniform molecular nature of nucleic acids—varying only in sequence and length—with a dedicated nanomedicine platform technology to streamline development and allow for rapid, tailored treatment strategies that address the pressing unmet needs in orphan diseases. Drawing inspiration from the convenience and customization of modern coffee brewing, the NANOSPRESSO model envisions a future where nucleic acid therapeutics are crafted at the point of care, akin to espresso capsules tailored to individual preferences, or, in this case, individual patient needs. Moreover, the quality of the final product is certified by the process and is easily achievable by non-expert users. This approach not only represents an innovative leap in personalizing pharmaceutical care but also embodies the democratization of access to nucleic acid therapeutics, signifying a revolution for personalized medicine.
This article outlines the scientific and technological foundation of this paradigm, detailing both the challenges and the state-of-the-art platforms embodied by the NANOSPRESSO model. We explore the potential benefits of this technology, the research and innovation ecosystem necessary to implement and expand it, and the associated regulatory, legal, economic, and wide societal implications.
Nucleic acid therapeutics: current status and future prospects
Introduction and principles
Discovery of the DNA double-helix structure in 1953 (24) and mRNA in 1961 (25) laid the molecular biology groundwork leading to the creation of pivotal technologies, including recombinant DNA and polymerase chain reaction (PCR). These advancements have enabled gene manipulation outside their natural settings, fueling significant strides in genetic engineering—from the creation of recombinant proteins to the development of genetically modified organisms (26, 27). Subsequent innovations, such as PCR for DNA amplification (28) and advanced sequencing technologies, not only enabled the decoding of the human genome but also revealed its predominantly noncoding nature (Figure 1) (29–34). These developments have revealed new therapeutic targets and strategies, including CRISPR gene editing, mRNA-based protein replacement therapies, and ASOs for gene silencing (Table 1, Figures 2A, B). The ongoing study of genomic regulation and epigenetic modification continues to enhance our ability to diagnose and treat diseases at the genetic level (34).
Figure 1
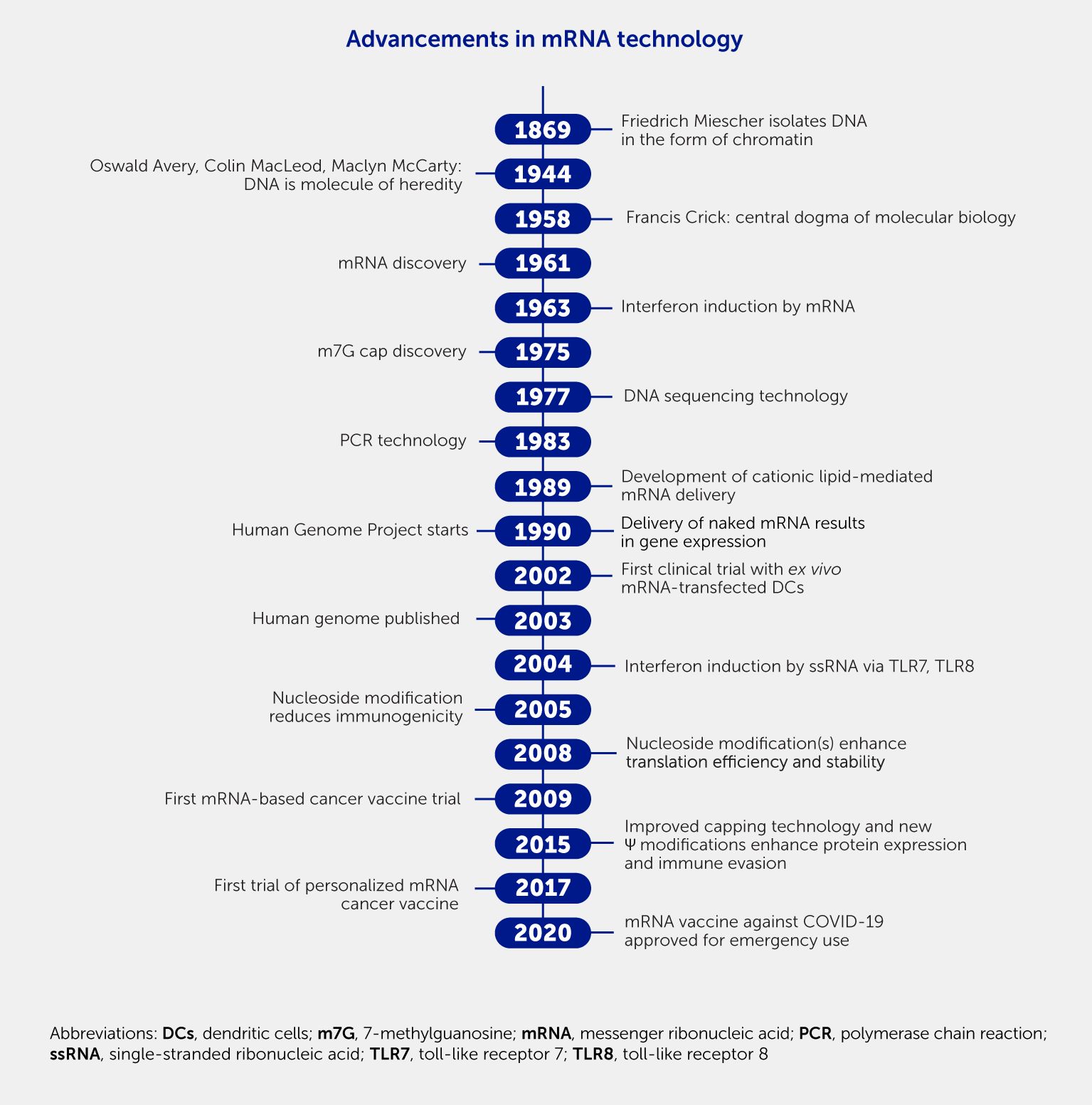
Figure 1. Landmark advances in molecular biology that enabled messenger RNA (mRNA) therapeutics to reach the market in 2020. Chronological figure showing the most important discoveries in molecular biology that have been crucial to the development of nucleic acid therapeutics.
Table 1
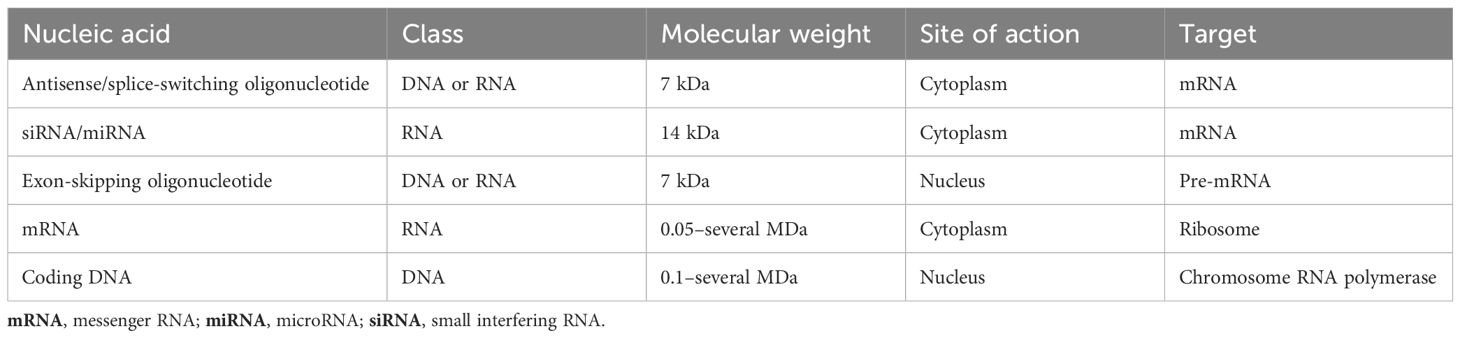
Table 1. Characteristics of different classes of approved nucleic acid therapeutics.
Figure 2
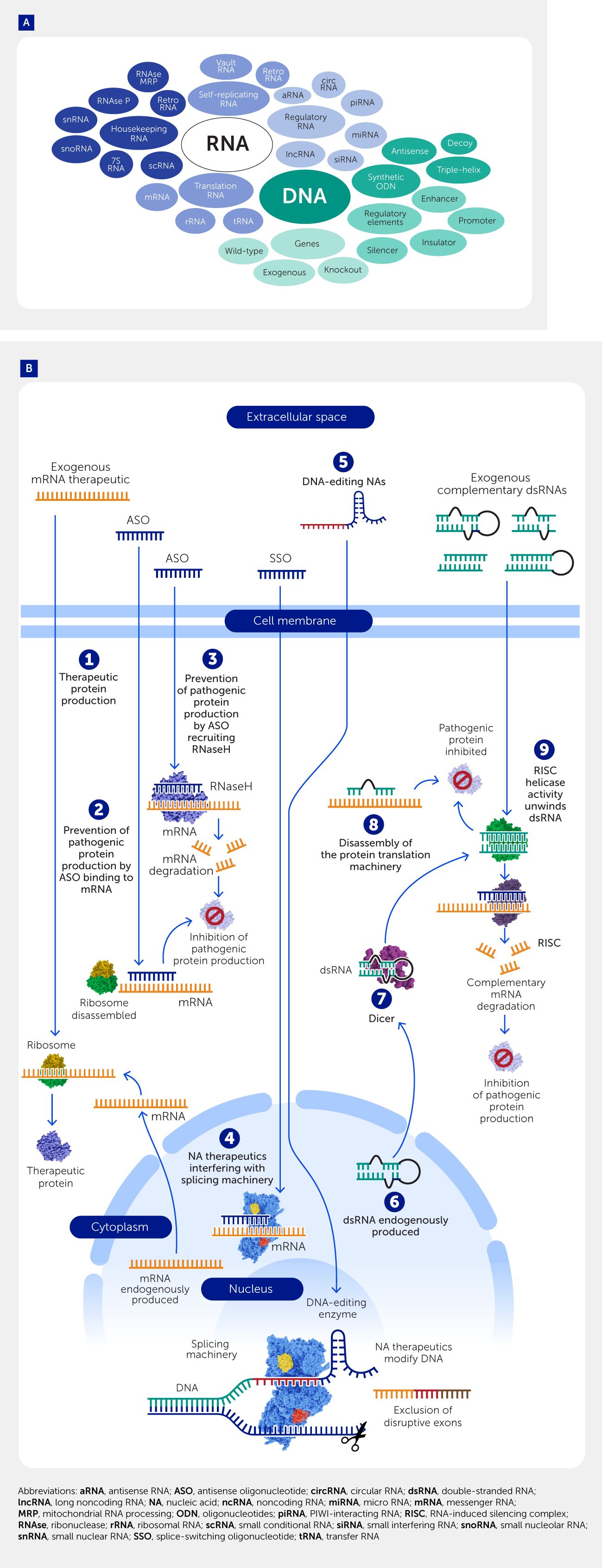
Figure 2. Nucleic acid landscape. (A) To date, tens of thousands of long (i.e., >200 nucleotides) noncoding RNAs (lncRNAs) have been discovered. LncRNAs can modulate chromatin function, regulate the assembly and function of nuclear bodies, alter the stability and translation of cytoplasmic messenger RNAs (mRNAs), and interfere with signaling pathways, depending on their localization. They are functionally different from shorter (generally 20–30 nucleotides long) RNA species, such as microRNAs (miRNAs), short interfering RNAs (siRNAs), and PIWI-interacting RNAs (piRNAs) that regulate gene expression, and small nucleolar RNAs (snoRNAs), which interact with proteins and other RNAs. Circular RNAs (circRNAs) have diverse functions, such as acting as scaffolds for proteins, binding other RNAs, and regulating gene expression. New functions continue to be discovered. (B) Mechanism of action of various nucleic acid therapeutics. 1) mRNA can be endogenously produced in the nucleus or exogenously added to produce a (therapeutic) protein via interaction with ribosomes. 2) Antisense oligonucleotides (ASOs) can bind complementary mRNA and stall ribosomes, preventing the production of pathogenic proteins. 3) When the ASO is able to recruit ribonuclease H (RNaseH), the complementary mRNA is enzymatically degraded, stopping pathogenic protein production. 4) Some nucleic acid therapeutics act in the nucleus. Splice-switching oligonucleotides can interact with mRNA and interfere with the splicing machinery, for example to restore a partially functional truncated protein by excluding disruptive exons. 5) Nucleic acid therapeutics can also modify DNA. Gene editing can be achieved, for example using guide RNAs or prime editors. 6) Double-stranded RNAs (dsRNA) can be produced endogenously. These are mostly short hairpin RNAs that are not perfectly complementary; after enzymatic processing, they become 19–25 nucleotide long miRNAs. 7) The imperfect binding to mRNA results in disassembly of the protein translation machinery, inhibiting pathogenic protein production. 8) Perfectly complementary dsRNAs are mostly exogenous. They recruit an enzyme that degrades the complementary mRNA.
Nucleic acid therapeutics go beyond simply synthesizing or inhibiting proteins; instead, they use subtler methods, such as exon-skipping oligonucleotides that alter splicing patterns (35) or antagomirs that inhibit gene-regulating micro RNAs (miRNAs) (Figure 2B) (36, 37). Recent developments in DNA editing are now entering clinical trials and expanding the toolkit for genetic intervention, including CRISPR/Cas9 and the newer Cas13, which makes temporary RNA edits (38) (Figure 3) (39–42). Innovations such as mRNA-encoded zinc finger nucleases are pushing boundaries in epigenetic editing (43).
Figure 3
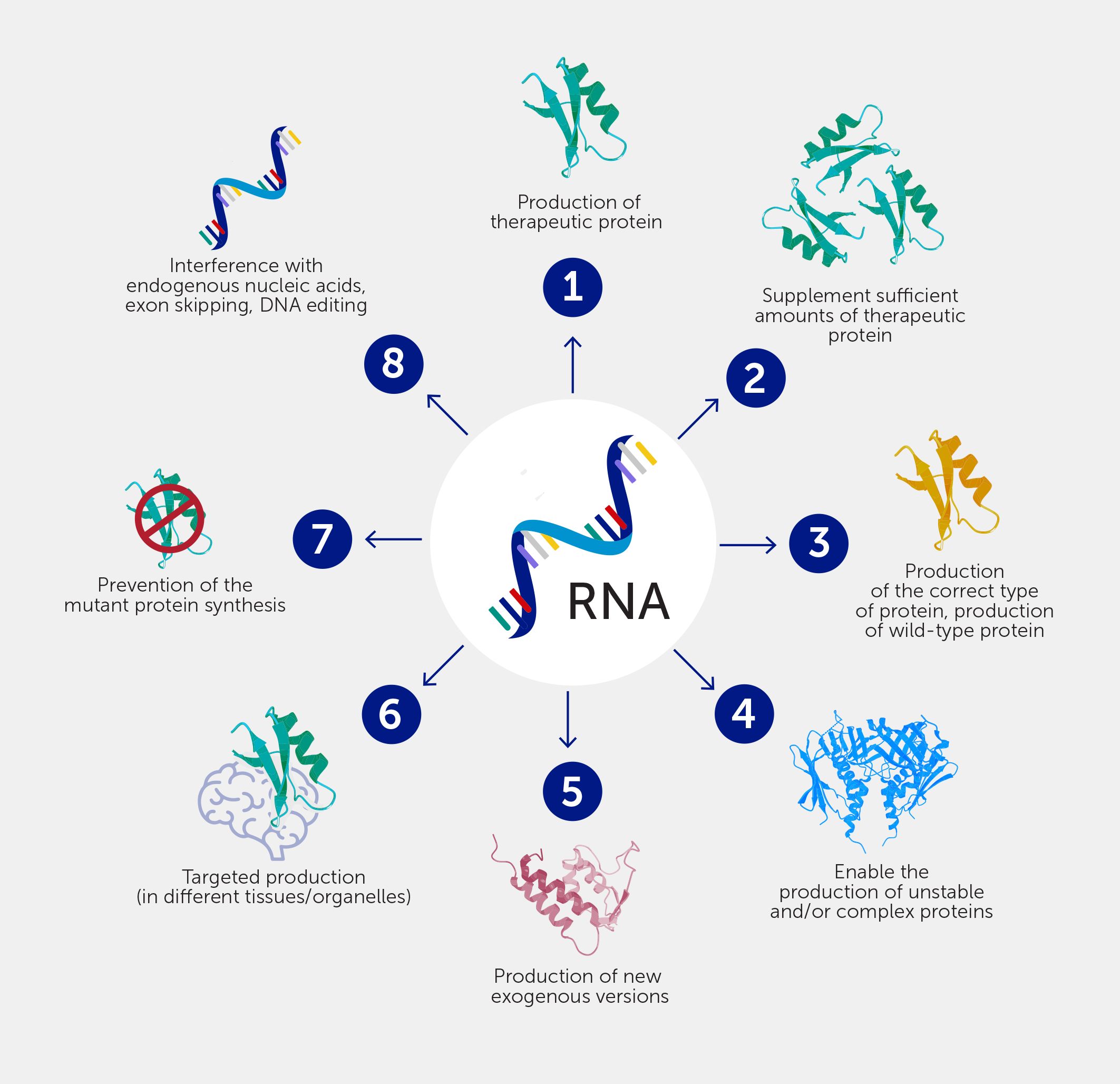
Figure 3. Nucleic acids offer exciting opportunities for new therapeutic interventions. 1) A therapeutic protein can be made when a patient fails to express it. 2) More of a therapeutic protein can be made when patients make insufficient amounts. 3) The correct protein can be made, e.g., to replace mutant proteins. 4) Proteins that are difficult to produce ex vivo (e.g., because of insufficient stability) can be made. 5) New therapeutic strategies can be developed based on exogenous proteins, e.g., by encoding for CRISPR-associated (Cas)9 protein, which in combination with a guide RNA can edit DNA. 6) Proteins can be made at locations where they are not normally produced. 7) Production of a pathogenic protein can be blocked. 8) Interference with normal processing of endogenous nucleic acids can be achieved, for example for exon-skipping.
Introducing non-natural genes enables additional functionalities, such as chimeric antigen receptor (CAR)-T cells that recognize and destroy cancer cells, highlighting the versatility of nucleic acid therapeutics (44–47). This approach could revolutionize treatment for diseases currently beyond the reach of conventional drugs, tapping into the vast potential of previously unexplored therapeutic targets (48, 49).
Approved products
Nucleic acid therapeutics have matured over decades from initial concepts, such as ASOs, into marketable drugs (Table 2). For example, fomivirsen, which targets cytomegalovirus in the eye by binding mRNA encoding the essential immediate-early 2 (IE2) protein, was approved in 1998 (12, 50, 51). Development timelines of about two decades are common, as seen for example with eteplirsen, which was approved for Duchenne’s muscular dystrophy in 2016 (52), inclisiran for familial hypercholesterolemia in 2021 (53), and patisiran for transthyretin-mediated amyloidosis in 2018 (54)—all rooted in late 20th-century discoveries (55–57).
Table 2
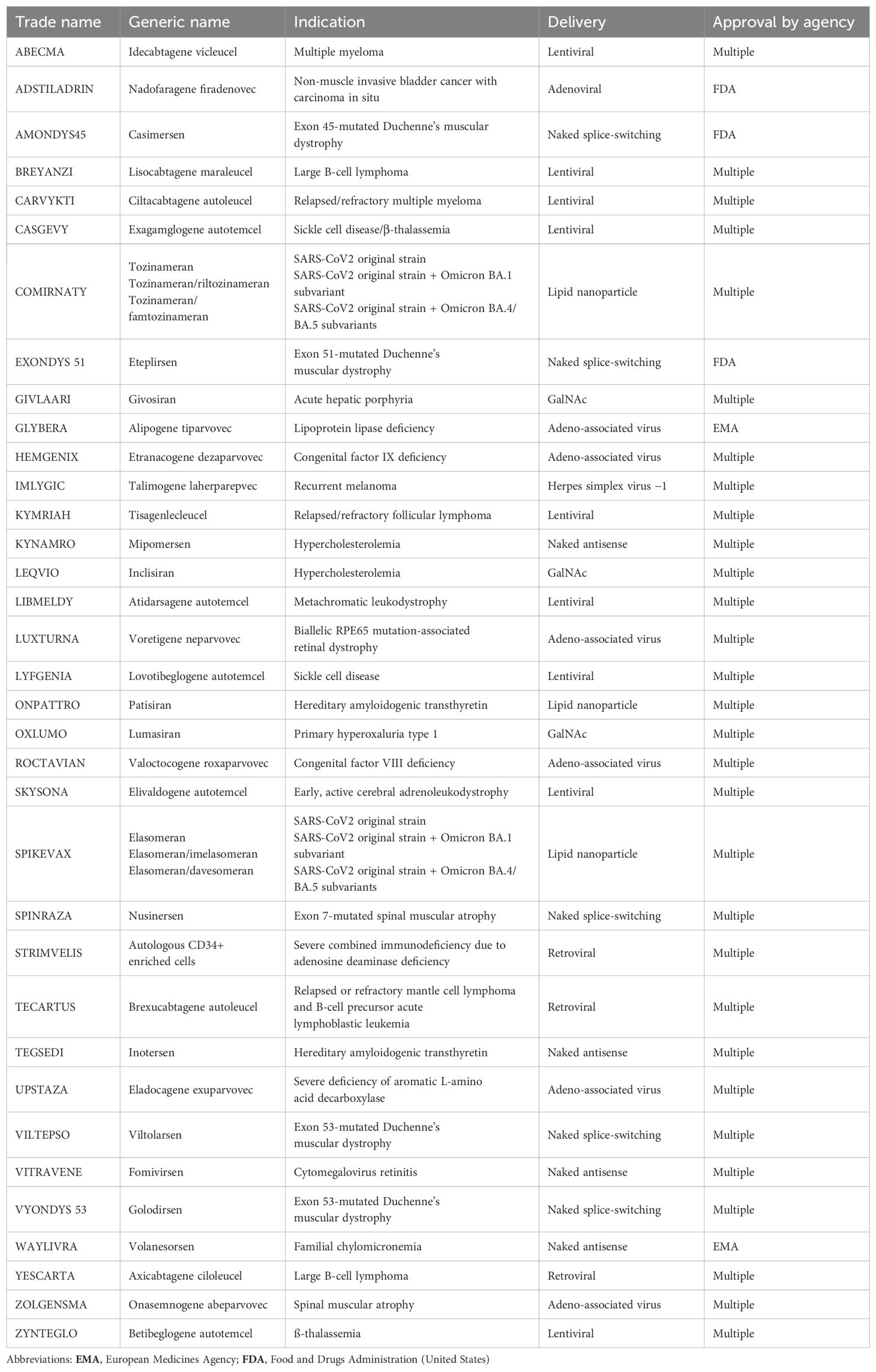
Table 2. Approved nucleic acid therapeutics.
The prominence of nucleic acid therapeutics soared in 2020 with the swift development and worldwide distribution of mRNA-based COVID-19 vaccines, showcasing their potential (Figure 1) (58–60). This spurred further research into broader applications, including in malignant and cardiovascular diseases (1). In oncology, mRNA therapeutics customize immune responses by generating cancer-specific antigens (61–63) or modulating immune functions within the tumor environment (62–65), highlighting their versatility in precision medicine (66).
In December 2023, the Food and Drug Administration (FDA) approval of the first cell-based gene therapy using CRISPR/Cas9 for sickle cell disease marked a significant advancement in genetic-based treatments (40, 41). Further, emerging technologies such as Cas13 for temporary RNA edits (38) and sophisticated gene editing methods (67, 68) continue to expand the precision and scope of these therapies.
Nucleic acid therapeutics are especially effective for orphan diseases, offering targeted interventions that align with the unique genetic profiles of these conditions. This platform technology supports the rapid, cost-effective development of new treatments, improving access for patients with rare genetic disorders.
Challenges for nucleic acid therapeutics
While nucleic acid therapeutics offer considerable potential, their therapeutic application faces major challenges. Crucially, their negative charge, high water solubility, and high molecular weight (Table 2) (69, 70) make their spontaneous translocation through the lipophilic cell membrane virtually impossible. They can also be immunogenic, particularly when present extracellularly, triggering immune pathways through pro-inflammatory components such as Toll-like receptors (TLRs) (71–73). For example, phage RNA polymerases can inadvertently generate immunogenic double-stranded RNA by-products (74, 75) that induce unwanted immune responses via TLR3 (18, 71). Among other approaches, substituting uridine with pseudouridine in RNA sequences can mitigate such responses (76). The limited stability of nucleic acids is also problematic, especially for mRNA or plasmid DNA. For mRNA, even aqueous storage at –80°C causes activity loss within weeks owing to hydrolysis. Nucleic acids can also be rapidly degraded in biological environments by nucleases (77, 78). Finally, nucleic acid therapeutics are costly to prepare: oligonucleotides require stepwise synthesis protocols with increasing amounts of non-full-length product impurities, while longer nucleic acids need enzymatic biological production with purification challenges. However, these costs are expected to decrease as production scales up and processes become more efficient (79).
Lipid nanoparticle delivery of nucleic acid therapeutics
The challenges of nucleic acid therapeutics necessitate an efficient delivery method for their clinical use. Strategies are centered on maximizing therapeutic exposure and ensuring intact arrival at the site of action within cells. The goal is to engineer carriers that can navigate through biological barriers and release their cargo precisely where the therapeutic activity is needed. This section explores lipid nanoparticles (LNPs), the drug delivery platform selected for the NANOSPRESSO project. The Supplementary Material includes a section outlining other platforms used in clinical settings for nucleic acid therapeutic delivery (Supplementary Section 1).
Initial lipid-based delivery systems grappled with challenges related to nucleic acid complexation, cellular uptake, and safety. Whereas viral vectors require a nucleic acid payload close in size and class to the original viral genome, synthetic nanoparticles offer a greater degree of freedom. This strategy can be applied to both short and long RNA and DNA molecules. It formed the basis for the COVID-19 vaccines (80, 81). The speed by which lead candidates for nucleic acid therapeutics can be generated remains unsurpassed in drug development: the first phase I COVID-19 vaccine clinical trial commenced just 42 days after SARS-CoV-2 was sequenced, and mass vaccinations began less than a year after the World Health Organization declared COVID-19 a pandemic (82, 83).
This ultrafast development would have been impossible without the decades of research on the delivery of nucleic acids with nanoparticles (82). First-generation excipients for nucleic acid delivery were cationic compounds, such as calcium ions in the early 1970s. In the 1980s, these were largely replaced by neutral or negatively charged lipid-based systems (84). An important step was achieved with cationic lipids, such as dioctadecenyl trimethylammonium propane, that coupled efficient complexation of nucleic acids to effective uptake by cells in vitro (17, 18, 84). On this theme, a range of structural variants have been added, such as dioctadecylamidoglycylspermine. However, their inherent toxicity and instability in vivo limited their use until the development of ionizable alternatives. Subsequent developments included the use of helper lipids, pivotal in optimizing the fusogenic capacity of LNPs and significantly enhancing the delivery efficacy by promoting endosomal escape (18, 85) and the covalent conjugation of lipids to polyethylene glycol (PEG) to enhance colloidal stability (17, 18). The flexibility, biocompatibility, and straightforward self-assembly of LNPs have brought them to the forefront of nucleic acid delivery.
Ionizable lipids and detachable PEG coatings emerged as two major breakthroughs, directly addressing the need for LNPs that were safe and effectively taken up by cells (17, 18, 84, 86). The shift from permanently cationic to ionizable lipids was crucial in reducing adverse interactions with biological components. Cationic LNPs carry a net positive surface charge and hence their interaction with negatively charged cell surfaces and biological molecules can cause cell aggregation—for example, red blood cell aggregation upon intravenous injection can lead to thrombotic events such as lung embolism (87). Ionizable lipids are cationic at low pH conditions during the loading of the nucleic acid into the LNP, ensuring a tight packaging of the therapeutic material and allowing for effective encapsulation. Raising the pH of the LNP suspension to physiological values causes this charge to be lost, providing a near-neutral surface charge—an important asset that avoids aggregation. In the acidifying endosome, the charge returns, providing an interactive surface for interaction with the organelle membrane (18, 86, 88). A second innovation was the introduction of PEG lipids with a short C14-acyl chain that can leave the particle surface upon dilution in vivo. This sheddable PEG coating provides colloidal stability in the pharmaceutical formulation while ensuring a controlled surface opsonization in vivo. In particular, apolipoprotein E is an important opsonin that allows interaction with many cell types displaying the low-density lipoprotein (LDL) receptor (89).
While PEGylation has improved stability and circulation time, its potential immunogenicity has led to considerations on dosage and frequency of treatments to minimize adverse immune reactions and prompted the exploration of alternative polymers for future LNP designs (90). Recent studies highlight the ongoing research to mitigate this PEG-related immunogenicity in LNPs, even before the widespread use of COVID-19 vaccines (91–96). This ongoing research signals a commitment to advancing successful LNP technology while ensuring patient safety.
Reflecting these advances, the first RNA-based therapeutic to be marketed, patisiran—a small interfering (si)RNA formulated as a LNP—contains both an ionizable lipid and a sheddable PEG coating. This blueprint was also instrumental for COVID vaccines and has been adopted by CRISPR/Cas9 gene editing platforms (22, 97).
Precision mixing: the convergence of LNPs and RNA
LNPs are the current clinical frontrunners in nucleic acid-based therapeutics. At present, the preferred recipe consists of an ionizable lipid, cholesterol, helper lipid, and a PEG lipid (Figure 4A) to form ~100 nm LNPs used to reach liver hepatocytes (e.g., for patisiran) after intravenous administration (18, 98, 99).
Figure 4
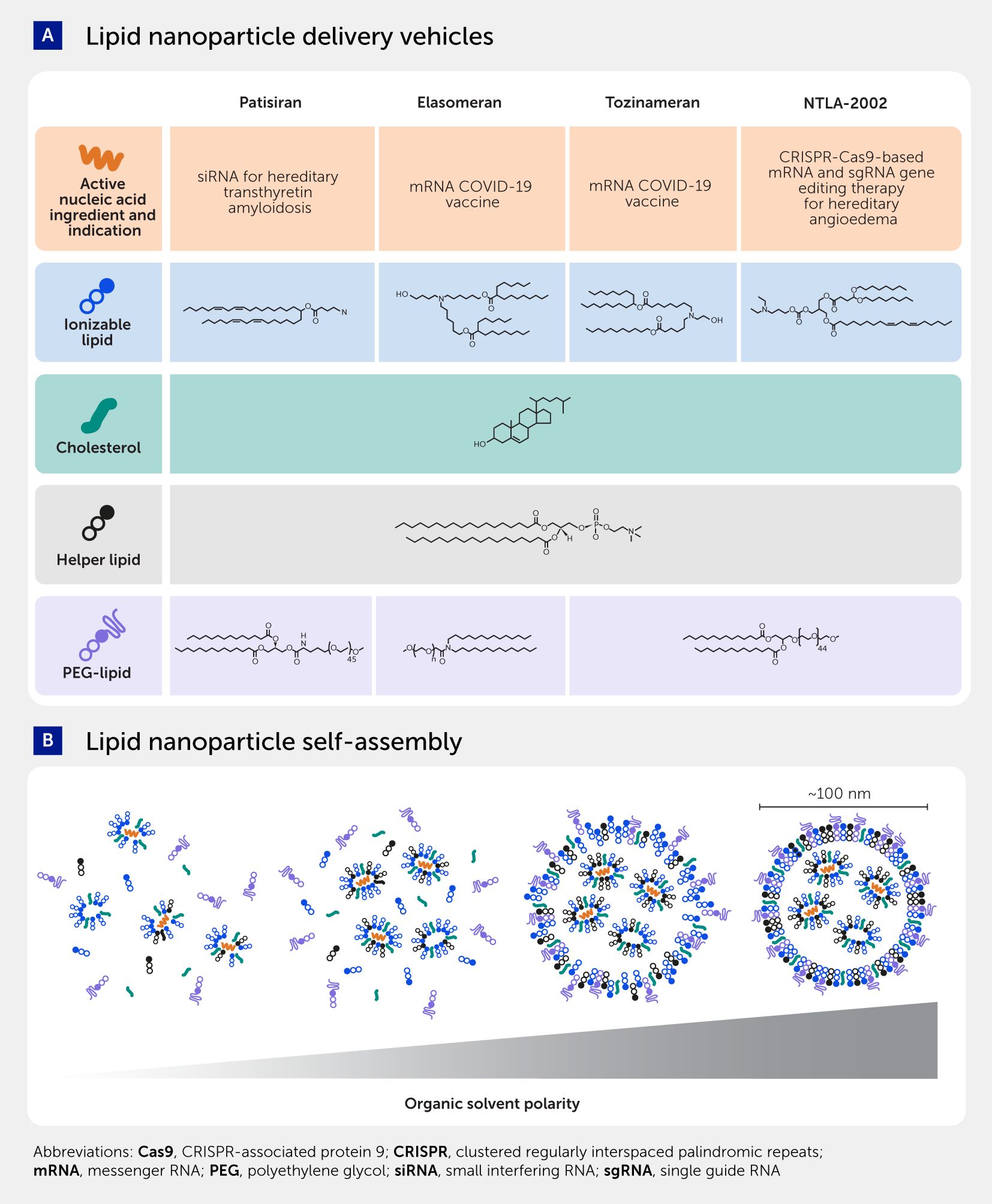
Figure 4. Lipid nanoparticle platform. (A) Several lipid nanoparticles have reached the clinical stage. The different nucleic acid therapeutics shown—i.e., small interfering RNA in patisiran, messenger RNA in Spikevax/Comirnaty, and CRISPR-associated (Cas)9 mRNA with single-guide (sg)RNA in NTLA-2002—use the same delivery recipe mixing four lipid types: ionizable lipid, helper phospholipid, cholesterol, and polyethylene glycol (PEG)-conjugated lipids. (B) Rapid mixing methods are used to reproduce complex nucleic acids in lipid nanoparticles. Lipids in organic solvent are mixed with an acidic aqueous solution of nucleic acids. The acidity ensures protonation of the ionizable lipid, enabling electrostatic binding to the nucleic acids. As the polarity of the medium increases during mixing, the other lipids are forced into hydrophobic interactions, building the nanoparticle. Owing to the hydrophilicity of the polymer, the PEG lipid forms the final layer, coating the surface of the particle and ensuring colloidal stability.
The performance of these nanomedicines depends highly on reproducible manufacturing within tight nanomedicine specifications, necessitating the development of platform technologies to achieve this. Consistent and rapid mixing of lipids in organic solvent and the aqueous nucleic acid solution is crucial to create nanoparticles with a narrow size distribution of around 100 nm. The electrostatic interactions and increase in solvent polarity drive the self-assembly of the nanomedicines. The first interactions to occur, upon mixing the ethanol and aqueous streams, are those between the ionizable lipids being charged by the acidic pH of the nucleic acid solution. Subsequently, these lipids electrostatically bind the negatively charged nucleic acids. As the solvent polarity increases, hydrophobic interactions cause cholesterol and helper lipids to drop out of the solution and form the core of the nanomedicine. Finally, the most polar lipid, i.e., the PEG lipid, coats the surface of the nanoparticles (Figure 4B) (88, 100). The design and parameters of the mixing play a crucial role in controlling the size and homogeneity of the resulting nanoparticles. Factors such as lipid and nucleic acid concentrations, buffer composition, flow rates, channel dimensions, and mixing angles and energies can be optimized to achieve desired nanomedicine characteristics (88, 101, 102).
The method of choice for COVID-19 vaccine manufacturing has been impingement jet mixing (103, 104). An impingement jet mixer consists of two or more liquid channels that converge at a high-speed collision point. When lipids and nucleic acids collide at high velocities within such a system, they experience significant shear stress and turbulence. This leads to the disruption and reformation of lipid structures, facilitating the encapsulation of the RNA molecules within the LNPs. The intense mixing provided by impingement jet mixing ensures dispersion and distribution of the components. The technique proved to be easily adaptable to accommodate larger volumes, allowing COVID-19 vaccine production on a billion-dose scale (104–106). Although impingement jet mixing and other rapid-mixing variants are ideal to accommodate large volumes at an industrial scale, this often overshoots the need, especially in the field of orphan diseases with limited numbers of patients. Other platform solutions now provide precise, rapid mixing at small scales. For example, microfluidic manufacture offers exact control over the mixing of two fluid streams at scales suitable for small clinical trials and even single-patient therapeutics (102, 105).
Research progress means the future of LNPs looks promising, with the potential to unlock new frontiers in personalized medicine through even safer and more efficient delivery systems.
Convergence of nucleic acid platform technologies to tackle unmet clinical needs
As described above, a recipe seems to have been found for new nucleic acid interventions in specific applications, such as vaccines (Figure 4A). The success of mRNA vaccine recipes during the SARS-CoV-2 pandemic is likely to have forever changed our approach to future pathogens with pandemic potential. For SARS-CoV-2, a month elapsed between the first patient being hospitalized and publication of the viral genome (82, 83). This publication already predicted the crucial role of the spike protein on the viral surface for entry into the cell based on structural similarities and differences to other related viruses (107–109). The deployment of mRNA COVID-19 vaccines was hence expedited through extraordinary global scientific collaboration and proactive regulatory strategies, such as “rolling reviews”, resulting in swift market authorization amid a crisis. Models suggest that these vaccines cut global mortality by two-thirds in their first year, yet over 7 million deaths occurred worldwide (110), highlighting the stark impact of the pandemic (111). This experience has fueled speculation on pre-emptively halting future pandemics through rapid genomic analysis to identify mRNA vaccine targets. Advancing multi-RNA LNP vaccines could curb the emergence of resistant variants. Moreover, the COVID-19 vaccine rollout has underscored the necessity for robust storage solutions and equitable distribution frameworks, particularly in resource-limited settings, to improve vaccination access.
As described, delivering nucleic acid therapeutics in clinical settings requires both biological insight and a mastery of engineering, especially when it comes to the precise formulation of LNPs. Addressing the challenge of systematically applying such sophisticated engineering to rare diseases with small patient populations has led to the advent of NANOSPRESSO. This project transcends these barriers with its innovative, onsite production capability, making personalized treatments a reality for those battling rare diseases.
NANOSPRESSO: producing personalized nucleic acid nanomedicines at the point of care
RNA-LNP local production “at the bedside”
The development and integration of the technological innovations outlined above marks a transformative shift in healthcare from a generalized to a personalized approach, profoundly impacting how medical treatments are developed and administered. We are moving from one-size-fits-all industrial approaches to individual treatments that are designed, developed, and produced locally.
Analysis of a patient’s unique genetic makeup points to the cause of the disease, and bioinformatic tools allow us to identify the modality of the nucleic acid-based intervention. Local production of the nucleic acid and local microfluidic mixing with the lipid excipients could provide small amounts of therapy to treat the handful of patients in the vicinity of the local care institution.
NANOSPRESSO: democratizing personalized nucleic acid nanomedicines
The proposed paradigm shift in pharmaceutical production resembles Nespresso’s revolution in coffee brewing—aiming to provide high-quality, personalized beverages with convenience, directly at home. In parallel, NANOSPRESSO seeks to offer high-quality, personalized nucleic acid therapeutics, manufactured conveniently at local healthcare facilities. We envision a future in which a personalized cartridge (analogous to the coffee capsule) is made on demand according to an individual’s “taste” (i.e., with the precisely designed personalized nucleic acid therapeutics provided at the right dose and right excipients matched to an individual’s disease and genotype) to be inserted in a microfluidic mixer (analogous to the coffee machine) in a local hospital pharmacy. Prototypes of the individual components in this system are currently operational, bringing this concept tantalizingly close to application (105, 112). Blisters can be loaded with the lipids on one side and nucleic acids on the other and mounted on a cartridge. These blisters can be emptied using defined pressures to carefully introduce the compounds into microfluidic channels that allow precise mixing to form lipid nanoparticles with onboard purification and sterile end filtration (Figures 5A, B, Supplementary Figure 1). Such an automated closed cartridge system has been successfully used to make radiolabeled peptides and proteins in a hospital pharmacy with complete on-board process validation.
Figure 5
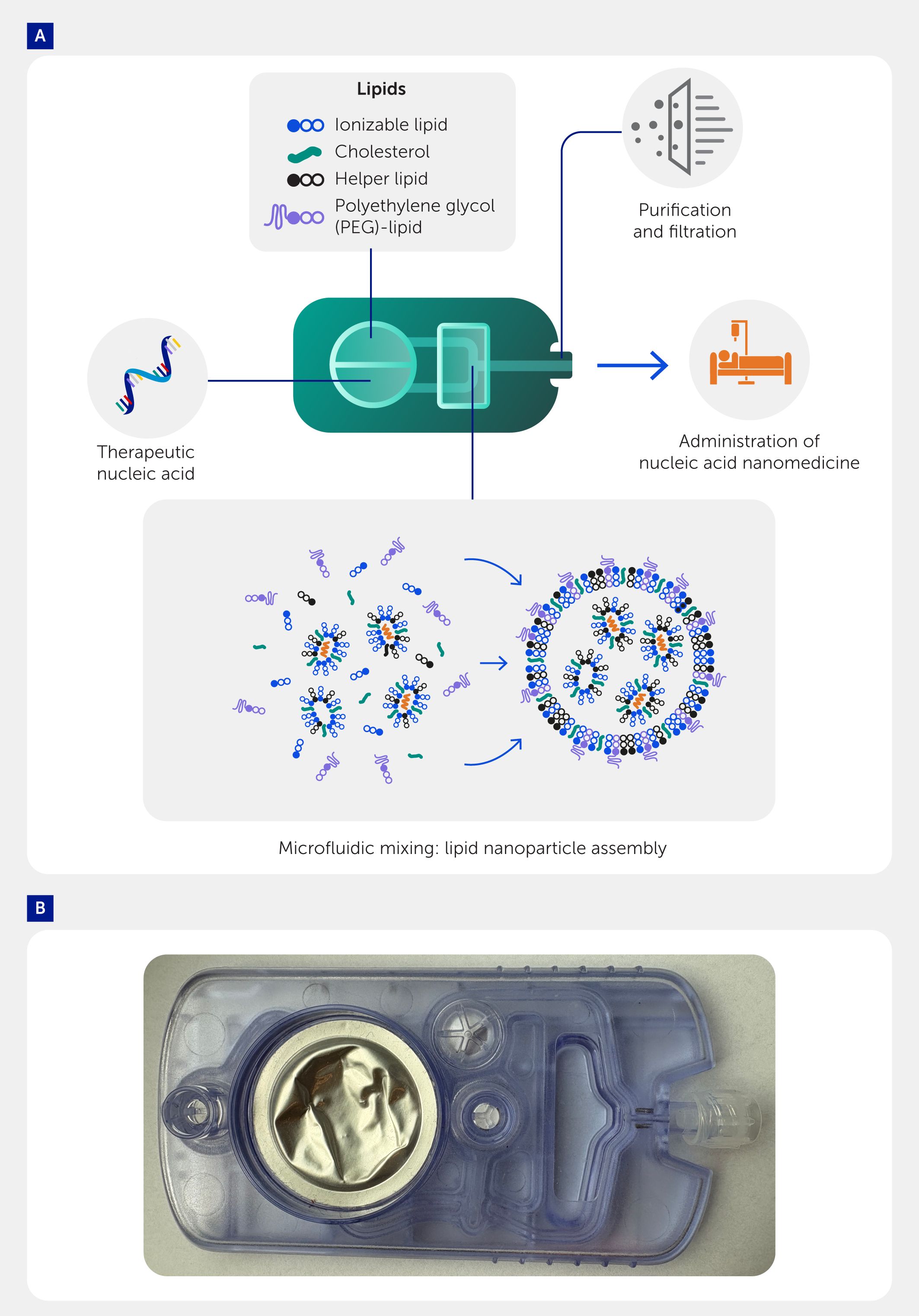
Figure 5. NANOSPRESSO platform technology. We envision a future where personalized cartridges are created on demand, tailored to individual needs. (A) These cartridges will contain the necessary therapeutic nucleic acids and the appropriate lipid excipients, customized to the patient’s specific disease and genotype. In a local hospital pharmacy, the cartridge will be inserted into a microfluidic mixer, allowing the lipid and nucleic acid phases to be precisely combined to form lipid nanoparticles. Additionally, each cartridge will include an onboard sterile end filtration system to ensure the highest quality and safety of the final product. (B) Prototype of cartridge undergoing testing and optimization.
Pharmacists once personalized medicines through compounding, but today, pharmaceuticals are mass-produced at centralized facilities, raising concerns over supply chains and environmental impact (113). While efficient for frequently used, high-volume, “one-size-fits-all” medicines, such as vaccines and painkillers, this model fails for orphan and ultra-orphan diseases, where high development costs (~US$1 billion) (114) and the small market size force extreme pricing, sometimes leading to market failures, as seen with Glybera, a treatment for the rare inherited disorder lipoprotein lipase deficiency (LPLD) (115). A systematic review showed that, among all personalized medicines, gene therapy brings the most significant improvements in health with much increased incremental quality-adjusted life-years (QALYs) for patients. However, these benefits often come at a very high cost, which is higher than the monetary value of the QALY gains, leading to a net loss (116). NANOSPRESSO aims to disrupt this by enabling local production of small batches, circumventing the economic and logistical constraints that often leave rare diseases untreated.
Finally, new therapies for rare diseases face significant challenges in generating clinical evidence for market approval, as they often rely on single-arm trials due to the absence of standard comparators. Local NANOSPRESSO manufacture would bypass these major hurdles and therefore mark a future with true personalization of pharmaceutical care and democratization of access to nucleic acid therapeutics.
Personalization and agility
While the NANOSPRESSO concept represents a versatile toolbox particularly suited to orphan disease therapy, its potential applications extend beyond this field, for example to personalized/precision oncology and tackling emerging pathogens.
In oncology, for example, therapeutic interventions are more and more dictated by the genetic make-up of the patient’s tumor. This could, for example, be exploited to raise an immune response to an endogenous antigen on tumor cells. Moderna has initiated a Phase III clinical trial of mRNA-4157, a personalized mRNA that encodes up to 34 different patient-specific neoantigens (117–119). Locally manufacturing the optimal mRNA coding for the exact mix of neoantigens and adjuvants prescribed based on genetic testing of individual patients would make this a truly personalized intervention.
The ability to rapidly respond to emerging therapeutic needs is another significant advantage of magistral preparation. Unlike industrial manufacturing, which often involves long lead times and regulatory hurdles, compounding allows for quicker adaptation to new discoveries. In the case of mRNA vaccines, for instance, a compounding-based approach enables the swift production of customized vaccines to combat novel local variants of a pathogen. For example, an Ebola virus outbreak in 2014 killed over 10,000 people in a short period and within a small geographic area in West Africa (120). Such outbreaks may be prevented by a switch to local mRNA-based vaccines.
Magistral preparation: design advantages and pharmaceutical implications
The switch to magistral preparation also has implications for the pharmaceutical applications and field. There is often a perception that, since nucleic acid therapeutics are already complicated to manufacture at large industrial scales, need intricate quality control, and possess challenging stability and shelf-lives, alternative small-scale production methods are even less feasible. We challenge this perception: local production would circumvent many issues that currently limit widespread roll-out of centrally produced nanomedicines.
The NANOSPRESSO solution nicely exemplifies two major principles of “good industrial design” as articulated by Nam P. Suh’s axiomatic design theory (121). It achieves this through (i) functional decoupling, as by separating the functional requirements—encapsulation efficacy of LNPs and therapeutic potency of RNA—NANOSPRESSO enables rapid adaptation to different diseases or requirements without needing to redesign the entire platform; and (ii) user simplicity, as the final user, typically a hospital pharmacist, does not need extensive nanomedicine expertise to encapsulate nucleic acid therapeutics efficiently and safely. The complexity of the process is contained within the pre-engineered capsule, ensuring ease of use and reliability in a clinical setting. This design aligns with Suh’s principle that the best designs minimize the information required by the user, streamlining the operation and enhancing usability (121).
Pharmaceutical stability
Nucleic acid nanomedicines are complex and costly to produce and distribute, with challenges largely stemming from the need for long shelf-lives required for global distribution under centralized manufacturing models. The COVID-19 vaccines illustrate this well. International distribution after centralized preparation of the mRNA vaccines necessitated an (ultra)low temperature of transport and storage for over 6 months, which presents a significant logistical challenge (122). In contrast, a stability of up to 24 hours has been reported at room temperature, which supports their local manufacture and administration.
Industrial manufacturing may also limit the optimal LNP formulation. Asymmetric lipids seem to outperform their symmetric counterparts in preclinical rodent and nonhuman primate models (123, 124). Studies have reported that LNPs with asymmetrical amino lipids display enhanced endosomal escape, as well as improved amino lipid clearance and tolerability (124, 125). However, symmetric excipients are used in currently marketed formulations because asymmetric lipid formulations exhibit physical instability owing to Ostwald ripening, a process where smaller lipid particles dissolve and larger ones grow, limiting their shelf life (126, 127). Ostwald ripening, a process that occurs over a period of months, is incompatible with global distribution and storage and yet is perfectly acceptable for local magistral preparation, where immediate use is possible.
Quality
Nucleic acid LNPs have a complex structure (100) heavily dependent on composition and production parameters; small deviations can significantly affect structure and stability. While pharmaceutical companies excel in producing high-quality medications at scale, they currently lack the capacity to manufacture patient-specific products. On the other hand, treatment centers and hospital pharmacies possess detailed knowledge specific to the diseases and techniques involved in these personalized products, potentially more so than the industry. Safety concerns of compounding are often mentioned as a disadvantage, with a perceived reduction in quality control stringency. However, this view is primarily influenced by incidents such as a fungal meningitis outbreak in the United States, where 750 out of 14,000 exposed individuals fell ill (128) and 64 died from a contaminated epidural steroid (129, 130). It is important to note that this example of mass production does not conform to the definition of magistral preparation, which is typically reserved for individual patients when no registered alternative exists. In Europe, such magistral preparations are often the only alternative, and large-scale compounders are regularly inspected by health authorities such as the Inspectie Gezondheidszorg en Jeugd (IGJ; Health and Youth Care Inspectorate) in the Netherlands, to ensure high quality. Also, effective risk management requires addressing two dimensions: probability and impact. In a magistral preparation, the direct link between patient, prescriber, and pharmacist makes any problem with the product completely traceable and confined to one patient, in sharp contrast to industrially prepared and globally distributed drugs.
Furthermore, while industrial manufacturing strives to minimize batch variability through stringent quality standards dictated by pharmacopeial requirements, challenges in maintaining uniformity can still arise due to variations in raw materials or production conditions. Compounding, while typically executed on a smaller scale, adheres to high-quality standards, with meticulous quality control processes in place to minimize product variability, ensuring that each preparation meets the specific needs of individual patients.
Nevertheless, this issue underscores the need for stringent quality control processes in the production of magistral nanomedicines. Critical quality attributes of LNP nanomedicines and their measurement continue to be refined, as discussed in recent studies that highlight the importance of orthogonal analytical techniques for ensuring product consistency and reliability (131, 132). These techniques evaluate chemical composition, drug loading, particle size, stability, and morphology, linking these properties to therapeutic efficacy and safety. Key physical parameters to be analyzed include size, size distribution, surface charge, encapsulation efficiency, and aggregation propensity. These will be evaluated using batch dynamic light scattering (DLS) and nanoparticle tracking analysis (NTA), with further verification through field flow fractionation with multi-angle light scattering (FFF-MALS), zeta potential measurements, and nucleic acid quantification. Furthermore, the chemical composition of the nanoparticles will be verified using high-resolution mass spectrometry, along with an assessment of mRNA payload integrity (131). We will perform both bulk and single particle analysis using single particle automated Raman trapping analysis (SPARTA). This method provides high-resolution insights into the chemical composition, structure, and uniformity of individual nanoparticles. By combining optical trapping and Raman spectroscopy, SPARTA enables non-invasive, label-free characterization of nanoparticles, making it an ideal tool for evaluating critical properties such as lipid composition, mRNA encapsulation, and batch consistency. Its single-particle precision is particularly valuable for ensuring the quality and reproducibility of LNP formulations (133). Moreover, given the ongoing efforts by regulators to clearly define the regulatory requirements for nanomedicines in general, as well as biologics-based nanomedicines, we aim to collaborate with regulators to publish insights on the translation process into clinical practice and the associated regulatory requirements. This will benefit future European nanomedicine developers.
This evolving landscape calls for a “renaissance” of the pharmacist’s role in production, emphasizing the importance of their deep understanding of these quality attributes. By developing specialized skills in manufacturing nucleic acid nanomedicines, pharmacists can contribute to the innovation and enhancement of quality standards, fostering a dynamic ecosystem for new clinical developments.
Cost-saving
Compounding/magistral preparation offers potential cost savings compared with large-scale industrial manufacturing. The manufacturing method chosen by NANOSPRESSO, microfluidics, saves on material and molecular consumption costs (134). More importantly, the capital-intensive nature of industrial facilities, including specialized equipment and stringent regulatory requirements, can significantly drive-up costs. In contrast, local compounding facilities are relatively more accessible and cost-effective, as they only produce upon prescription by the local physician, making them suitable for smaller research institutions, clinics, or even local pharmacies, in particular in the context of orphan drugs for rare diseases (135). This affordability could enhance the availability and affordability of nucleic acid therapeutics, especially in resource-limited settings, potentially making these therapies accessible for low- and middle-income countries. Importantly, this approach is primarily advocated for when registered products do not provide solutions tailored to individual patient needs.
Research and innovation ecosystem
The NANOSPRESSO project exemplifies the fusion of nucleic acid therapeutics with nanoparticle-mediated delivery systems in a microfluidic manufacturing setup, creating a dynamic platform for personalized medicine. This integration promotes close collaboration between hospital pharmacies, clinicians, and researchers, accelerating the translation from academic research to clinical settings (Supplementary Figure 2). For instance, emerging treatments such as circular RNAs, still in preclinical stages (136–138), can swiftly move into clinical trials facilitated by existing NANOSPRESSO infrastructure with minimal adjustments required for delivery to targeted tissues.
Continuous feedback from clinical trials can be quickly integrated into the manufacturing process to enhance the efficacy and safety of the formulations. This new model is even more relevant in the current context of national centers of clinical excellence (and their networks of collaboration), where most of the patients suffering from orphan diseases are treated by the same specialized clinicians and caregivers.
The model mirrors the evolution seen in CAR-T cell therapies, which transitioned from centralized to local production. Technologies such as the CliniMACS Prodigy® system (Miltenyi Biotec) system have simplified CAR-T cell manufacturing at the point of care, automating the entire process from cell activation to reinfusion, thus reducing risks and delivery times crucial for rapidly progressing diseases (139–141).
Regulatory changes are anticipated to keep pace with these technological advances, encouraging collaboration across the healthcare spectrum to balance innovation with affordability. Globally, NANOSPRESSO’s local production capability is poised to enhance access to cutting-edge treatments in lower-income countries and provide vital responses to local health emergencies like viral outbreaks.
Moreover, the framework supports equitable healthcare distribution by facilitating technology and data sharing on a unified platform, where blockchain technology could ensure secure and consistent data across the network. This could lead to enhanced treatment protocols and better patient outcomes worldwide, demonstrating the potential of decentralized manufacturing in a global healthcare setting.
Regulatory and legal implications
A tale of two diseases: methylmalonic acidemia and Crigler-Najjar syndrome
Currently, mRNA LNPs are being clinically developed by a biotechnology company for the treatment of MMA, a disease affecting approximately 1/50,000 individuals. It is a seemingly straightforward approach in which mRNA-3705 encodes the missing methylmalonyl-CoA mutase. The LNPs closely follow the patisiran recipe to deliver this mRNA to hepatocytes, the cells that predominantly express this enzyme in healthy individuals (142, 143). The well-understood etiology of the disease, recipe for delivery to the target cell, availability of predictive mouse models, and straightforward design of the active mRNA make this an attractive choice for pharmaceutical development. At the same time, it is expected that such treatments will be premium-priced, as the investments in industrial development and clinical testing need to be recouped from their use within a small patient population, taking them out of reach for many patients in less affluent countries.
The situation for Crigler-Najjar syndrome, a rarer condition with a prevalence of <1/1,000,000 in Europe, is even more difficult. Despite a similarly clear understanding of the potential treatment—a mRNA encoding the crucial uridine 5’-diphospho-glucuronosyltransferase enzyme delivered to hepatocytes (144, 145)—there is limited industrial commitment to developing this drug (146). This gap between medical knowledge and its application in drug development is not just disappointing, it is also frustrating for patients and their families. They are painfully aware that a feasible solution exists, yet it remains out of reach, trapped between pharmaceutical prioritizations.
By maximizing the platform potency of nucleic acid therapeutics, it could be envisioned that an mRNA produced under good manufacturing practice (GMP), with a similar sequence and modifications (such as pseudouridine), encoding methylmalonyl-CoA mutase mixed with the same GMP-grade lipids used in clinical trials using a NANOSPRESSO-like device, would provide a high-quality nucleic acid nanomedicine that could be prescribed to an individual patient with MMA. In principle, this mRNA could be replaced by a different mRNA to correct another enzyme defect, e.g., to treat Crigler-Najjar syndrome, for delivery via the same nanomedicine platform (Figure 5). This would dramatically reduce the development costs of new therapeutics and present a business model where low-profit margin blister pouches are filled with mRNA and excipients on demand and assembled into a personalized cartridge in a plug-and-play approach for manufacture in the local hospital pharmacy. The regulatory and intellectual property implications of such a change are discussed below.
Regulation
The regulatory landscape surrounding nucleic acid therapeutics is continually evolving. Compounding/magistral preparation offers greater regulatory flexibility compared with industrial manufacturing, which often necessitates lengthy and expensive approval processes. Regulatory agencies have recognized the importance of tailored therapies and have created pathways to support compounding practices for patient-specific needs. In the European Union (EU), Article 3 of Directive 2001/83/EC (147) exempts two types of pharmacy preparation to which the Directive does not apply: the magistral formula, referring to pharmacy preparation following prescription for an individual patient; and the officinal formula, referring to stock preparation of a drug in accordance with a pharmacopeia and delivered to customers of the pharmacy. Since the EU legislation does not apply to these preparations, member states can establish local regulations (148, 149). For an example of what compounding via these exemptions entails in practice, see the work of Polak and colleagues (150). They describe how they ensured their active ingredients, excipients, and compounded product complied with the requirements of the European pharmacopeia and Dutch law (150).
In addition to the magistral and officinal exemptions, the European Pharmaceutical legislation also has an exemption for advanced therapy medicinal products (ATMPs) (see Article 28, Regulation 1394/2007/EC) (151). The Hospital Exemption (HE) allows non-routine preparation of ATMPs in a hospital setting upon prescription for an individual patient in accordance with specified quality standards. Specific requirements to obtain an HE license differ between member states (152). This regulatory flexibility allows for timely and individualized patient access to nucleic acid therapeutics without compromising safety or efficacy.
Compounding/magistral preparation fosters a culture of research and innovation within the medical community. By enabling local research institutions, academic centers, and small-scale biotech companies to develop and test novel LNP formulations, compounding encourages scientific exploration and fosters collaboration. This decentralized approach to development can lead to breakthrough discoveries and advancements in the field of nucleic acid therapeutics, expanding the horizon of treatment options available to patients.
Notably, the proposed revision to the EU pharmaceutical legislation aims to increase medicine availability, introducing expansions to pharmacy compounding exemptions and a more comprehensive regime for hospitals to prepare and use ATMPs, which include nucleic acid therapeutics. The Enhanced Pharmacy Exemption allows pharmacies to prepare limited stocks of magistral formula products in advance. Also, the HE for ATMPs, detailed in the draft Directive (153), outlines strict regulatory requirements for manufacturing and monitoring ATMPs under this exemption. Although these outlines are strict, they also provide much-needed guidance that could lead to a more systematic (albeit non-routine) approach to producing cell and gene therapies and tissue-engineered products in hospitals. If patients and health systems are to benefit optimally from the NANOSPRESSO’s nucleic acid-LNP platform approach, a (multistakeholder) discussion with regulators is required to explore its advantages and potential applications, as compared with the forced early lock-in of technology during conventional pharmaceutical product development and regulation. NANOSPRESSO is especially well positioned to initiate such a dialogue, as it is driven by a unique consortium of European partners, with its core group in the Netherlands. This 6-year multidisciplinary project unites a full ecosystem of health technology developers, clinicians, engineers, regulators, public researchers, innovative small and medium-sized enterprises (SMEs), and many more in a concerted effort to deliver a groundbreaking nanomedicine solution to real societal needs, with a clear dedication to fostering the availability of new therapies for patients with orphan diseases.
Patents
The Hospital and Pharmacy Exemption mentioned above is governed by the legal frameworks around the development and application of personalized (nano)medicines. These patent laws, operational in most countries, provide specific exemptions for therapeutic interventions prepared for individual patients, shielding them from infringement claims. This legal stipulation presents a unique opportunity to accelerate the pace of translational medicine in the context of personalized medicine. By falling under this exemption, the approach allows for the real-time incorporation of the latest advancements in nucleic acid sequences, excipients, and manufacturing techniques without the encumbrance of legal repercussions. This not only expedites the development process but also ensures that patients receive the most cutting-edge treatments available. The incorporation of novel designs and materials can significantly enhance the therapeutic index, delivery efficiency, and biocompatibility of these personalized nanomedicines.
Consequently, this specific legal framework not only has implications for rapid clinical translation but also serves as a catalyst for fostering innovation in the design and production of next-generation treatments.
There is notable resistance from pharmaceutical companies—key stakeholders often considered as innovators in the market—who argue that a wider use of these exemptions will disrupt the market. While the concerns of innovative pharmaceutical companies are valid in a competitive market context, the role of hospital and pharmacy exemptions in compounding medicines is to address gaps in patient care that the broader pharmaceutical market does not fill. These exemptions are vital for patient-centered care, driving innovation, and ensuring that all patients, regardless of the rarity or complexity of their conditions, have access to effective treatments.
Economic considerations and reimbursement
The specific nature of orphan diseases, combined with the complexities of delivering personalized nucleic acid nanomedicines, potentially disrupts the current procedures used by national health technology assessment (HTA) agencies. Decisions to reimburse particular therapies are now largely based on metrics such as the incremental cost-effectiveness ratio (ICER), which computes the ratio between the incremental cost of a new treatment and the associated gain in (quality-adjusted) survival. Estimation of the ICER is usually based on clinical trial-based evidence supported by data about healthcare resource use (staff time, equipment, patient travel, etc.). This evidence is not easy to obtain for rare diseases. In addition, because listed prices for orphan disease products are usually high, the resulting ICER is not favorable despite long-term health gains (154). Unlike traditional, “one-size-fits-all” pharmaceuticals, personalized nanomedicines require a tailored and specialized hospital-based approach that incurs additional costs. However, because hospital pharmacies are not-for-profit, the pricing strategy may be a cost-plus approach. This is in contrast to the industrial use of a dynamic price range to maximize company revenues, often including a “premium for innovation”. The downside, however, is two-fold. First, healthcare payers may be reticent to underwrite these therapies without robust evidence demonstrating their superior efficacy and cost-effectiveness over existing treatments, which is difficult to collect in a hospital setting. Also, decisions to reimburse new therapies are usually made at a national level. However, the therapies may be limited to specialized centers, particularly if they are used to treat orphan diseases. These specific conditions may therefore need decisions about restricted access and a price–volume arrangement for selected hospitals. Policymakers will in such instances request therapies be available for all patients and that action should be taken to ensure access at national level. Given this complexity, interdisciplinary collaborations between scientists, healthcare providers, policymakers, and funders are pivotal for realizing the full potential of these innovative therapies while ensuring their financial sustainability and accessibility.
Societal implications
The advent of nucleic acid therapeutics promises to revolutionize medicine, yet it also raises important societal questions that extend beyond the realm of clinical efficacy. These therapies have the potential to modify or correct genetic anomalies, thereby opening the door to treatments for a myriad of previously incurable conditions. However, this capability also triggers ethical considerations around gene editing and the potential for “designer” traits, with implications for social equity and human diversity. Furthermore, the high cost of developing and producing these therapeutics may exacerbate existing healthcare disparities, concentrating these advanced treatments in high-income populations or countries unless measures are taken to democratize access. The permanence of some nucleic acid interventions also generates new dimensions of patient consent and long-term impact, including unforeseeable off-target effects or ecological impacts should modified organisms be released into the environment. Therefore, as nucleic acid therapeutics continue to evolve, it is imperative that societal, ethical, and environmental considerations are woven into the fabric of both regulatory oversight and public discourse to guide responsible development and application.
The implications of nucleic acid therapeutics extend beyond the medical field, as it is related to developments in both the fourth and fifth industrial revolutions. Nucleic acid therapeutics epitomize the convergence seen in the fourth industrial revolution, characterized by the fusion of physical, digital, and biological systems. They leverage computational biology for drug design, digital technology for patient-specific customization, and advanced manufacturing techniques for production. The result is a highly integrated, data-driven approach to healthcare that is congruent with Industry 4.0 objectives. Looking toward the fifth industrial revolution, which emphasizes the coexistence of humans and intelligent machines, nucleic acid therapeutics could become a cornerstone in bio-augmentation and personalized healthcare models. These therapies have the potential to interact seamlessly with wearable technologies for real-time health monitoring and adjustment of treatment parameters, thus harmonizing human health with technological innovation. Importantly, as we advance through these industrial stages, ethical considerations around data privacy, accessibility, and social justice will become increasingly salient, necessitating multidisciplinary dialogues to navigate the complex landscape of benefits and challenges.
Conclusions
Patient perspectives, especially from those battling conditions such as MMA and Crigler-Najjar syndrome, highlight the dire need for readily available and effective treatments. Manifesting from an early age, these diseases severely compromise the quality of life through debilitating symptoms such as fatigue, blindness, and dementia, leading to premature mortality. The promise shown by ongoing clinical trials for gene therapies brings a beacon of hope, positioning NANOSPRESSO as a crucial platform to enable bedside delivery of these life-altering treatments.
Combining genomic sequencing with bioinformatics to identify therapeutic targets, along with state-of-the-art delivery methods, represents a robust strategy, particularly vital for orphan diseases. The ability to decode the human genome and conduct patient-specific genetic profiling allows for the crafting of bespoke therapeutics, exemplifying the essence of precision medicine and marking a new chapter in addressing diseases with previously limited treatment avenues.
NANOSPRESSO’s innovative approach transforms the landscape of nano-enabled ATMPs. By tackling the regulatory challenges intrinsic to such a pioneering paradigm, it paves the way for regulatory frameworks that embrace the intricacies of nanomedicine and personalized care. This initiative is more than a scientific venture; it is a collaborative push toward shaping the future of medical innovation.
Nanomedicine’s versatility extends beyond generic applications and could encompass drug delivery systems to reduce the side effects or improve the efficacy of chemotherapy, enhance radiotherapy, or improve the detection of elusive metastases, holding the potential to revolutionize gene therapy and personalized medicine. The NANOSPRESSO platform underscores this by facilitating the engineering flexibility to swiftly adapt components on the research side and manufacture the final therapy at bedside, without necessitating complex nanotechnology expertise from the manufacturing hospital. This localized, lab-scale approach not only simplifies quality control but also significantly reduces costs compared with traditional large-scale clinical trials.
As we acknowledge the multitude of scientific, technical, medical, regulatory, and economic challenges ahead, we invite all interested parties to join us on this journey. NANOSPRESSO represents not just a leap forward in therapeutic delivery but a call to action for collaborative innovation. Together, we can navigate the complexities of this new frontier in healthcare, making personalized nanomedicine a tangible reality for patients in need.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsci.2025.1458636/full#supplementary-material
Statements
Author contributions
MES: Visualization, Writing – original draft, Writing – review & editing.
AC: Writing – original draft, Writing – review & editing.
ML: Writing – original draft, Writing – review & editing.
NS: Writing – original draft, Writing – review & editing.
PS: Writing – original draft, Writing – review & editing.
MG: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
PH: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
JB: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
MH: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
FC: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
MWi: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
WH: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
MWe: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
KD-M: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
JD: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
SF: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
FW: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
TS: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
MI: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
HB: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
MB: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
SE: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
MMS: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
PC: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing.
RS: Conceptualization, Funding acquisition, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. further inquiries can be directed to the corresponding author.
Funding
The authors declared financial support was received for the research presented in this article. The project NANOSPRESSO-NL received funding from the Netherlands Science Agenda-Netherlands Organization for Scientific Research Grant No NWA.1389.20.096. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of interest
MG is CEO of CelluTx Inc.
PH is employed by Lipoid GmbH.
JB is employed by Anjarium Biosciences AG.
MH is employed by siTOOLS GmbH.
FC is employed by NanoVation Therapeutics™ UK Ltd Research.
MWi is employed by Curevac.
WH is CEO of Solstice Pharmaceuticals BV.
HMGB was employed part time by NanoVation TherapeuticsTM UK Ltd Research (NanoVation Therapeutics) from 2022–2024.
MMS is the founder of Sparta Biosciences Ltd and advisor to NanoVation Therapeutics, NanoCell, OutFox Bio, and Sensible Biotechnologies.
PC is the founder of Acuitas Therapeutics, Integrated Nanotherapeutics, Precision NanoSystems, and NanoVation Therapeutics.
RS is employed by Nanocell Therapeutics, Inc.
Neither these companies nor the funders mentioned above were involved in the study design, data collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication. The companies mentioned above also did not provide funding for the work.
The remaining authors declared that this work was conducted in the absence of financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declared that no generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kulkarni JA, Witzigmann D, Thomson SB, Chen S, Leavitt BR, Cullis PR, et al. The current landscape of nucleic acid therapeutics. Nat Nanotechnol (2021) 16(6):630–43. doi: 10.1038/s41565-021-00898-0
2. Tambuyzer E, Vandendriessche B, Austin CP, Brooks PJ, Larsson K, Miller Needleman KI, et al. Therapies for rare diseases: therapeutic modalities, progress and challenges ahead. Nat Rev Drug Discov (2020) 19(2):93–111. doi: 10.1038/s41573-019-0049-9
3. Opalinska JB and Gewirtz AM. Nucleic-acid therapeutics: basic principles and recent applications. Nat Rev Drug Discov (2002) 1(7):503–14. doi: 10.1038/nrd837
4. Chung CCY, Hong Kong Genome Project, Chu AT, and Chung BH. Rare disease emerging as a global public health priority. Front Public Health (2022) 10:1028545. doi: 10.3389/fpubh.2022.1028545
5. Iyer VR, Praveen P, Kaduskar BD, Moharir SC, and Mishra RK. mRNA biotherapeutics landscape for rare genetic disorders. J Biosci (2024) 49:33. doi: 10.1007/s12038-023-00415-6
6. Martini PGV and Guey LT. A new era for rare genetic diseases: messenger RNA therapy. Hum Gene Ther (2019) 30(10):1180–9. doi: 10.1089/hum.2019.090
7. Health TL. The landscape for rare diseases in 2024. Lancet Glob Health (2024) 12(3):e341. doi: 10.1016/S2214-109X(24)00056-1
8. Cavaller-Bellaubi M, Hughes-Wilson W, Kubinová Š, Van de Casteele M, Van Lente EJ, Degortes E, et al. Patients, payers and developers of orphan medicinal products: lessons learned from 10 years’ multi-stakeholder dialogue on improving access in Europe via MoCA. Orphanet J Rare Dis (2023) 18(1):144. doi: 10.1186/s13023-023-02774-7
9. Hammond SM, Bernstein E, Beach D, and Hannon GJ. An RNA-directed nuclease mediates post-transcriptional gene silencing in Drosophila cells. Nature (2000) 404(6775):293–6. doi: 10.1038/35005107
10. Southwell AL, Skotte NH, Bennett CF, and Hayden MR. Antisense oligonucleotide therapeutics for inherited neurodegenerative diseases. Trends Mol Med (2012) 18(11):634–43. doi: 10.1016/j.molmed.2012.09.001
11. Holt JT, Redner RL, and Nienhuis AW. An oligomer complementary to c-myc mRNA inhibits proliferation of HL-60 promyelocytic cells and induces differentiation. Mol Cell Biol (1988) 8(2):963–73. doi: 10.1128/mcb.8.2.963-973.1988
12. Stephenson ML and Zamecnik PC. Inhibition of Rous sarcoma viral RNA translation by a specific oligodeoxyribonucleotide. Proc Natl Acad Sci USA (1978) 75(1):285–8. doi: 10.1073/pnas.75.1.285
13. Moon SB, Kim DY, Ko J-H, and Kim Y-S. Recent advances in the CRISPR genome editing tool set. Exp Mol Med (2019) 51(11):1–11. doi: 10.1038/s12276-019-0339-7
14. Adli M. The CRISPR tool kit for genome editing and beyond. Nat Commun (2018) 9(1):1911. doi: 10.1038/s41467-018-04252-2
15. Liu G, Lin Q, Jin S, and Gao C. The CRISPR-Cas toolbox and gene editing technologies. Mol Cell (2022) 82(2):333–47. doi: 10.1016/j.molcel.2021.12.002
16. Khorkova O, Hsiao J, and Wahlestedt C. Nucleic acid-based therapeutics in orphan neurological disorders: recent developments. Front Mol Biosci (2021) 8:643681. doi: 10.3389/fmolb.2021.643681
17. Hald Albertsen CH, Kulkarni JA, Witzigmann D, Lind M, Petersson K, and Simonsen JB. The role of lipid components in lipid nanoparticles for vaccines and gene therapy. Adv Drug Delivery Rev (2022) 188:114416. doi: 10.1016/j.addr.2022.114416
18. Estapé Senti M, García Del Valle L, and Schiffelers RM. mRNA delivery systems for cancer immunotherapy: lipid nanoparticles and beyond. Adv Drug Delivery Rev (2024) 206:115190. doi: 10.1016/j.addr.2024.115190
19. Akinc A, Maier MA, Manoharan M, Fitzgerald K, Jayaraman M, Barros S, et al. The Onpattro story and the clinical translation of nanomedicines containing nucleic acid-based drugs. Nat Nanotechnol (2019) 14(12):1084–7. doi: 10.1038/s41565-019-0591-y
20. Jayaraman M, Ansell SM, Mui BL, Tam YK, Chen J, Du X, et al. Maximizing the potency of siRNA lipid nanoparticles for hepatic gene silencing in vivo. Angew Chem Int Ed Engl (2012) 51(34):8529–33. doi: 10.1002/anie.201203263
21. Schoenmaker L, Witzigmann D, Kulkarni JA, Verbeke R, Kersten G, Jiskoot W, et al. mRNA-lipid nanoparticle COVID-19 vaccines: structure and stability. Int J Pharm (2021) 601:120586. doi: 10.1016/j.ijpharm.2021.120586
22. Suzuki Y and Ishihara H. Difference in the lipid nanoparticle technology employed in three approved siRNA (Patisiran) and mRNA (COVID-19 vaccine) drugs. Drug Metab Pharmacokinet (2021) 41:100424. doi: 10.1016/j.dmpk.2021.100424
23. Germain M, Caputo F, Metcalfe S, Tosi G, Spring K, Åslund AKO, et al. Delivering the power of nanomedicine to patients today. J Control Release (2020) 326:164–71. doi: 10.1016/j.jconrel.2020.07.007
24. Watson JD and Crick FH. Molecular structure of nucleic acids: a structure for deoxyribose nucleic acid. Nature (1953) 171(4356):737–8. doi: 10.1038/171737a0
25. Zimmermann RA and Levinthal C. Messenger RNA and RNA transcription time. J Mol Biol (1967) 30(2):349–70. doi: 10.1016/S0022-2836(67)80044-5
26. Galambos L and Sturchio JL. Pharmaceutical firms and the transition to biotechnology: a study in strategic innovation. Bus Hist Rev (1998) 72(2):250–78. doi: 10.2307/3116278
27. Steinberg FM and Raso J. Biotech pharmaceuticals and biotherapy: an overview. J Pharm Pharm Sci (1998) 1(2):48–59. doi: 10.70392/9akkzg37
28. Mullis KB. The unusual origin of the polymerase chain reaction. Sci Am (1990) 262(4):56–61, 64. doi: 10.1038/scientificamerican0490-56
29. Goodwin S, McPherson JD, and McCombie WR. Coming of age: ten years of next-generation sequencing technologies. Nat Rev Genet (2016) 17(6):333–51. doi: 10.1038/nrg.2016.49
30. Levy SE and Myers RM. Advancements in next-generation sequencing. Annu Rev Genomics Hum Genet (2016) 17(1):95–115. doi: 10.1146/annurev-genom-083115-022413
31. Rhoads A and Au KF. Pacbio sequencing and its applications. Genom Proteom Bioinform (2015) 13(5):278–89. doi: 10.1016/j.gpb.2015.08.002
32. Lander ES, Linton LM, Birren B, Nusbaum C, Zody MC, Baldwin J, et al. Initial sequencing and analysis of the human genome. Nature (2001) 409(6822):860–921. doi: 10.1038/35057062
33. Mu XJ, Lu ZJ, Kong Y, Lam HYK, and Gerstein MB. Analysis of genomic variation in non-coding elements using population-scale sequencing data from the 1000 Genomes Project. Nucleic Acids Res (2011) 39(16):7058–76. doi: 10.1093/nar/gkr342
34. Boland CR. Non-coding RNA: it’s not junk. Dig Dis Sci (2017) 62(5):1107–9. doi: 10.1007/s10620-017-4506-1
35. Järver P, O’Donovan L, and Gait MJ. A chemical view of oligonucleotides for exon skipping and related drug applications. Nucleic Acid Ther (2014) 24(1):37–47. doi: 10.1089/nat.2013.0454
36. Krützfeldt J, Rajewsky N, Braich R, Rajeev KG, Tuschl T, Manoharan M, et al. Silencing of microRNAs in vivo with ‘antagomirs’. Nature (2005) 438(7068):685–9. doi: 10.1038/nature04303
37. Yang M and Mattes J. Discovery, biology and therapeutic potential of RNA interference, microRNA and antagomirs. Pharmacol Ther (2008) 117(1):94–104. doi: 10.1016/j.pharmthera.2007.08.004
38. Zhang F. Development of CRISPR-Cas systems for genome editing and beyond. Q Rev Biophys (2019) 52:e6. doi: 10.1017/S0033583519000052
39. Frangoul H, Altshuler D, Cappellini MD, Chen Y-S, Domm J, Eustace BK, et al. CRISPR-Cas9 gene editing for sickle cell disease and β-thalassemia. N Engl J Med (2021) 384(3):252–60. doi: 10.1056/NEJMoa2031054
40. Frangoul H, Locatelli F, Sharma A, Bhatia M, Mapara M, Molinari L, et al. Exagamglogene autotemcel for severe sickle cell disease. Blood (2023) 142(Suppl 1):1052. doi: 10.1182/blood-2023-190139
41. Hoy SM. Exagamglogene autotemcel: first approval. Mol Diagn Ther (2024) 28(2):133–9. doi: 10.1007/s40291-024-00696-z
42. Gillmore JD, Gane E, Taubel J, Kao J, Fontana M, Maitland ML, et al. CRISPR-Cas9 in vivo gene editing for transthyretin amyloidosis. N Engl J Med (2021) 385(6):493–502. doi: 10.1056/NEJMoa2107454
43. Cappelluti MA, Mollica Poeta V, Valsoni S, Quarato P, Merlin S, Merelli I, et al. Durable and efficient gene silencing in vivo by hit-and-run epigenome editing. Nature (2024) 627(8003):416–23. doi: 10.1038/s41586-024-07087-8
44. Barrett DM, Singh N, Porter DL, Grupp SA, and June CH. Chimeric antigen receptor therapy for cancer. Annu Rev Med (2014) 65:333–47. doi: 10.1146/annurev-med-060512-150254
45. June CH and Sadelain M. Chimeric antigen receptor therapy. N Engl J Med (2018) 379(1):64–73. doi: 10.1056/NEJMra1706169
46. Sadelain M, Brentjens R, and Rivière I. The basic principles of chimeric antigen receptor design. Cancer Discov (2013) 3(4):388–98. doi: 10.1158/2159-8290.CD-12-0548
47. Sterner RC and Sterner RM. CAR-T cell therapy: current limitations and potential strategies. Blood Cancer J (2021) 11(4):69. doi: 10.1038/s41408-021-00459-7
48. Dixon SJ and Stockwell BR. Identifying druggable disease-modifying gene products. Curr Opin Chem Biol (2009) 13(5–6):549–55. doi: 10.1016/j.cbpa.2009.08.003
49. Landry Y and Gies J-P. Drugs and their molecular targets: an updated overview. Fundam Clin Pharmacol (2008) 22(1):1–18. doi: 10.1111/j.1472-8206.2007.00548.x
50. Zamecnik PC and Stephenson ML. Inhibition of Rous sarcoma virusrous sarcoma virus replication and cell transformation by a specific oligodeoxynucleotide. Proc Natl Acad Sci USA (1978) 75(1):280–4. doi: 10.1073/pnas.75.1.280
51. Roehr B. Fomivirsen approved for CMV retinitis. J Int Assoc Phys AIDS Care (1998) 4(10):14–6. doi: 10.1177/1545109798004001003
52. Syed YY. Eteplirsen: first global approval. Drugs (2016) 76(17):1699–704. doi: 10.1007/s40265-016-0657-1
54. Hoy SM. Patisiran: first global approval. Drugs (2018) 78(15):1625–31. doi: 10.1007/s40265-018-0983-6
55. Dominski Z and Kole R. Restoration of correct splicing in thalassemic pre-mRNA by antisense oligonucleotides. Proc Natl Acad Sci USA (1993) 90(18):8673–7. doi: 10.1073/pnas.90.18.8673
56. Fire A, Xu S, Montgomery MK, Kostas SA, Driver SE, and Mello CC. Potent and specific genetic interference by double-stranded RNA in Caenorhabditis elegans. Nature (1998) 391(6669):806–11. doi: 10.1038/35888
57. Elbashir SM, Harborth J, Lendeckel W, Yalcin A, Weber K, and Tuschl T. Duplexes of 21-nucleotide RNAs mediate RNA interference in cultured mammalian cells. Nature (2001) 411(6836):494–8. doi: 10.1038/35078107
58. Parhiz H, Atochina-Vasserman EN, and Weissman D. mRNA-based therapeutics: looking beyond COVID-19 vaccines. Lancet (2024) 403(10432):1192–204. doi: 10.1016/S0140-6736(23)02444-3
59. Chavda VP, Hossain MK, Beladiya J, and Apostolopoulos V. Nucleic acid vaccines for COVID-19: a paradigm shift in the vaccine development arena. Biologics (2021) 1(3):337–56. doi: 10.3390/biologics1030020
60. Hogan MJ and Pardi N. mRNA vaccines in the COVID-19 pandemic and beyond. Annu Rev Med (2022) 73:17–39. doi: 10.1146/annurev-med-042420-112725
61. Blass E and Ott PA. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat Rev Clin Oncol (2021) 18(4):215–29. doi: 10.1038/s41571-020-00460-2
62. Miao L, Zhang Y, and Huang L. mRNA vaccine for cancer immunotherapy. Mol Cancer (2021) 20(1):41. doi: 10.1186/s12943-021-01335-5
63. Sobhani N, Scaggiante B, Morris R, Chai D, Catalano M, Tardiel-Cyril DR, et al. Therapeutic cancer vaccines: from biological mechanisms and engineering to ongoing clinical trials. Cancer Treat Rev (2022) 109:102429. doi: 10.1016/j.ctrv.2022.102429
64. Hewitt SL, Bai A, Bailey D, Ichikawa K, Zielinski J, Karp R, et al. Durable anticancer immunity from intratumoral administration of IL-23, IL-36γ, and OX40L mRNAs. Sci Transl Med (2019) 11(477):eaat9143. doi: 10.1126/scitranslmed.aat9143
65. Hewitt SL, Bailey D, Zielinski J, Apte A, Musenge F, Karp R, et al. Intratumoral IL12 mRNA therapy promotes TH1 transformation of the tumor microenvironment. Clin Cancer Res (2020) 26(23):6284–98. doi: 10.1158/1078-0432.CCR-20-0472
66. Anderson WF. September 14, 1990: the beginning. Hum Gene Ther (1990) 1(4):371–2. doi: 10.1089/hum.1990.1.4-371
67. Li T, Yang Y, Qi H, Cui W, Zhang L, Fu X, et al. CRISPR/Cas9 therapeutics: progress and prospects. Signal Transduct Target Ther (2023) 8(1):36. doi: 10.1038/s41392-023-01309-7
68. Anzalone AV, Randolph PB, Davis JR, Sousa AA, Koblan LW, Levy JM, et al. Search-and-replace genome editing without double-strand breaks or donor DNA. Nature (2019) 576(7785):149–57. doi: 10.1038/s41586-019-1711-4
69. Ghose AK, Viswanadhan VN, and Wendoloski JJ. A knowledge-based approach in designing combinatorial or medicinal chemistry libraries for drug discovery. 1. A qualitative and quantitative characterization of known drug databases. J Comb Chem (1999) 1(1):55–68. doi: 10.1021/cc9800071
70. Dagle JM, Andracki ME, DeVine RJ, and Walder JA. Physical properties of oligonucleotides containing phosphoramidate-modified internucleoside linkages. Nucleic Acids Res (1991) 19(8):1805–10. doi: 10.1093/nar/19.8.1805
71. Sahin U, Karikó K, and Türeci Ö. mRNA-based therapeutics–developing a new class of drugs. Nat Rev Drug Discov (2014) 13(10):759–80. doi: 10.1038/nrd4278
72. Diebold SS, Kaisho T, Hemmi H, Akira S, and Reis e Sousa C. Innate antiviral responses by means of TLR7-mediated recognition of single-stranded RNA. Science (2004) 303(5663):1529–31. doi: 10.1126/science.1093616
73. Heil F, Hemmi H, Hochrein H, Ampenberger F, Kirschning C, Akira S, et al. Species-specific recognition of single-stranded RNA via toll-like receptor 7 and 8. Science (2004) 303(5663):1526–9. doi: 10.1126/science.1093620
74. Pardi N, Muramatsu H, Weissman D, and Karikó K. In vitro transcription of long RNA containing modified nucleosides. Methods Mol Biol (2013) 969:29–42. doi: 10.1007/978-1-62703-260-5_2
75. Karikó K, Muramatsu H, Ludwig J, and Weissman D. Generating the optimal mRNA for therapy: HPLC purification eliminates immune activation and improves translation of nucleoside-modified, protein-encoding mRNA. Nucleic Acids Res (2011) 39(21):e142. doi: 10.1093/nar/gkr695
76. Karikó K, Buckstein M, Ni H, and Weissman D. Suppression of RNA recognition by toll-like receptors: the impact of nucleoside modification and the evolutionary origin of RNA. Immunity (2005) 23(2):165–75. doi: 10.1016/j.immuni.2005.06.008
77. Uddin MN and Roni MA. Challenges of storage and stability of mRNA-based COVID-19 vaccines. Vaccines (Basel) (2021) 9(9):1033. doi: 10.3390/vaccines9091033
78. Houseley J and Tollervey D. The many pathways of RNA degradation. Cell (2009) 136(4):763–76. doi: 10.1016/j.cell.2009.01.019
79. Roberts TC, Langer R, and Wood MJA. Advances in oligonucleotide drug delivery. Nat Rev Drug Discov (2020) 19(10):673–94. doi: 10.1038/s41573-020-0075-7
80. Wilson B and Geetha KM. Lipid nanoparticles in the development of mRNA vaccines for COVID-19. J Drug Delivery Sci Technol (2022) 74:103553. doi: 10.1016/j.jddst.2022.103553
81. Khurana A, Allawadhi P, Khurana I, Allwadhi S, Weiskirchen R, Banothu AK, et al. Role of nanotechnology behind the success of mRNA vaccines for COVID-19. Nano Today (2021) 38:101142. doi: 10.1016/j.nantod.2021.101142
82. Fauci AS. The story behind COVID-19 vaccines. Science (2021) 372(6538):109. doi: 10.1126/science.abi8397
83. Carvalho T, Krammer F, and Iwasaki A. The first 12 months of COVID-19: a timeline of immunological insights. Nat Rev Immunol (2021) 21(4):245–56. doi: 10.1038/s41577-021-00522-1
84. Cullis PR and Hope MJ. Lipid nanoparticle systems for enabling gene therapies. Mol Ther (2017) 25(7):1467–75. doi: 10.1016/j.ymthe.2017.03.013
85. Kulkarni JA, Witzigmann D, Leung J, Tam YYC, and Cullis PR. On the role of helper lipids in lipid nanoparticle formulations of siRNA. Nanoscale (2019) 11(45):21733–9. doi: 10.1039/c9nr09347h
86. Hou X, Zaks T, Langer R, and Dong Y. Lipid nanoparticles for mRNA delivery. Nat Rev Mater (2021) 6(12):1078–94. doi: 10.1038/s41578-021-00358-0
87. Sakurai F, Nishioka T, Yamashita F, Takakura Y, and Hashida M. Effects of erythrocytes and serum proteins on lung accumulation of lipoplexes containing cholesterol or DOPE as a helper lipid in the single-pass rat lung perfusion system. Eur J Pharm Biopharm (2001) 52(2):165–72. doi: 10.1016/s0939-6411(01)00165-5
88. Evers MJW, Kulkarni JA, van der Meel R, Cullis PR, Vader P, and Schiffelers RM. State-of-the-art design and rapid-mixing production techniques of lipid nanoparticles for nucleic acid delivery. Small Methods (2018) 2(9):1700375. doi: 10.1002/smtd.201700375
89. Akinc A, Querbes W, De S, Qin J, Frank-Kamenetsky M, Jayaprakash KN, et al. Targeted delivery of RNAi therapeutics with endogenous and exogenous ligand-based mechanisms. Mol Ther (2010) 18(7):1357–64. doi: 10.1038/mt.2010.85
90. Abu Lila AS, Kiwada H, and Ishida T. The accelerated blood clearance (ABC) phenomenon: clinical challenge and approaches to manage. J Control Release (2013) 172(1):38–47. doi: 10.1016/j.jconrel.2013.07.026
91. Hoang Thi TT, Pilkington EH, Nguyen DH, Lee JS, Park KD, and Truong NP. The importance of poly(ethylene glycol) alternatives for overcoming PEG immunogenicity in drug delivery and bioconjugation. Polymers (Basel) (2020) 12(2):298. doi: 10.3390/polym12020298
92. Szebeni J. Complement activation-related pseudoallergy: a stress reaction in blood triggered by nanomedicines and biologicals. Mol Immunol (2014) 61(2):163–73. doi: 10.1016/j.molimm.2014.06.038
93. Mohamed M, Abu Lila AS, Shimizu T, Alaaeldin E, Hussein A, Sarhan HA, et al. PEGylated liposomes: immunological responses. Sci Technol Adv Mater (2019) 20(1):710–24. doi: 10.1080/14686996.2019.1627174
94. Szebeni J, Storm G, Ljubimova JY, Castells M, Phillips EJ, Turjeman K, et al. Applying lessons learned from nanomedicines to understand rare hypersensitivity reactions to mRNA-based SARS-CoV-2 vaccines. Nat Nanotechnol (2022) 17(4):337–46. doi: 10.1038/s41565-022-01071-x
95. Besin G, Milton J, Sabnis S, Howell R, Mihai C, Burke K, et al. Accelerated blood clearance of lipid nanoparticles entails a biphasic humoral response of B-1 followed by B-2 lymphocytes to distinct antigenic moieties. Immunohorizons (2019) 3(7):282–93. doi: 10.4049/immunohorizons.1900029
96. Tenchov R, Sasso JM, and Zhou QA. Pegylated lipid nanoparticle formulations: immunological safety and efficiency perspective. Bioconjug Chem (2023) 34(6):941–60. doi: 10.1021/acs.bioconjchem.3c00174
97. Kazemian P, Yu S-Y, Thomson SB, Birkenshaw A, Leavitt BR, and Ross CJD. Lipid-nanoparticle-based delivery of CRISPR/Cas9 genome-editing components. Mol Pharm (2022) 19(6):1669–86. doi: 10.1021/acs.molpharmaceut.1c00916
98. Tenchov R, Bird R, Curtze AE, and Zhou Q. Lipid nanoparticles─from liposomes to mRNA vaccine delivery, a landscape of research diversity and advancement. ACS Nano (2021) 15(11):16982–7015. doi: 10.1021/acsnano.1c04996
99. Qiu M, Li Y, Bloomer H, and Xu Q. Developing biodegradable lipid nanoparticles for intracellular mRNA delivery and genome editing. Acc Chem Res (2021) 54(21):4001–11. doi: 10.1021/acs.accounts.1c00500
100. Kulkarni JA, Darjuan MM, Mercer JE, Chen S, van der Meel R, Thewalt JL, et al. On the formation and morphology of lipid nanoparticles containing ionizable cationic lipids and siRNA. ACS Nano (2018) 12(5):4787–95. doi: 10.1021/acsnano.8b01516
101. Xu L, Wang X, Liu Y, Yang G, Falconer RJ, and Zhao C-X. Lipid nanoparticles for drug delivery. Adv Nanobio Res (2022) 2(2):2100109. doi: 10.1002/anbr.202100109
102. Maeki M, Uno S, Niwa A, Okada Y, and Tokeshi M. Microfluidic technologies and devices for lipid nanoparticle-based RNA delivery. J Control Release (2022) 344:80–96. doi: 10.1016/j.jconrel.2022.02.017
103. Bourla A. Moonshot: inside Pfizer’s nine-month race to make the impossible possible. New York: Harper Business (2022)
104. King ML. How manufacturing won or lost the COVID-19 vaccine race. Vaccine (2024) 42(5):1004–12. doi: 10.1016/j.vaccine.2023.12.031
105. O’Brien Laramy MN, Costa AP, Cebrero YM, Joseph J, Sarode A, Zang N, et al. Process robustness in lipid nanoparticle production: a comparison of microfluidic and turbulent jet mixing. Mol Pharm (2023) 20(8):4285–96. doi: 10.1021/acs.molpharmaceut.3c00390
106. Costa AP, Xu X, Khan MA, and Burgess DJ. Liposome formation using a coaxial turbulent jet in co-flow. Pharm Res (2016) 33(2):404–16. doi: 10.1007/s11095-015-1798-8
107. Li J, Lai S, Gao GF, and Shi W. The emergence, genomic diversity and global spread of SARS-CoV-2. Nature (2021) 600(7889):408–18. doi: 10.1038/s41586-021-04188-6
108. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet (2020) 395(10224):565–74. doi: 10.1016/S0140-6736(20)30251-8
109. Tan W, Zhao X, Ma X, Wang W, Niu P, Xu W, et al. A novel coronavirus genome identified in a cluster of pneumonia cases - Wuhan, China 2019-2020. China CDC Wkly (2020) 2(4):61–2. doi: 10.46234/ccdcw2020.017
110. World Health Organization. COVID-19 epidemiological update – 24 December 2024 [online] (2024). Available at: https://www.who.int/publications/m/item/covid-19-epidemiological-update---24-december-2024
111. Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, and Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis (2022) 22(9):1293–302. doi: 10.1016/S1473-3099(22)00320-6
112. van Hoeve W, de Vargas Serrano M, Te Winkel L, Forsberg F, Dave JK, Sarkar K, et al. Improved sensitivity of ultrasound-based subharmonic aided pressure estimation using monodisperse microbubbles. J Ultrasound Med (2022) 41(7):1781–9. doi: 10.1002/jum.15861
113. Karliner J, Slotterback S, Boyd R, Ashby B, Steele K, and Wang J. Health care’s climate footprint: the health sector contribution and opportunities for action. Eur J Public Health (2020) 30(Supplement_5):ckaa165–843. doi: 10.1093/eurpub/ckaa165.843
114. Wouters OJ, McKee M, and Luyten J. Estimated research and development investment needed to bring a new medicine to market, 2009–2018. JAMA (2020) 323(9):844–53. doi: 10.1001/jama.2020.1166
115. Senior M. After Glybera’s withdrawal, what’s next for gene therapy? Nat Biotechnol (2017) 35(6):491–2. doi: 10.1038/nbt0617-491
116. Vellekoop H, Versteegh M, Huygens S, Corro Ramos I, Szilberhorn L, Zelei T, et al. The net benefit of personalized medicine: a systematic literature review and regression analysis. Value Health (2022) 25(8):1428–38. doi: 10.1016/j.jval.2022.01.006
117. Dolgin E. Personalized cancer vaccines pass first major clinical test. Nat Rev Drug Discov (2023) 22(8):607–9. doi: 10.1038/d41573-023-00118-5
118. Terai M and Sato T. Individualised neoantigen cancer vaccine therapy. Lancet (2024) 403(10427):590–1. doi: 10.1016/S0140-6736(23)02463-7
119. Weber JS, Carlino MS, Khattak A, Meniawy T, Ansstas G, Taylor MH, et al. Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): a randomised, phase 2b study. Lancet (2024) 403(10427):632–44. doi: 10.1016/S0140-6736(23)02268-7
120. Elston JWT, Cartwright C, Ndumbi P, and Wright J. The health impact of the 2014–15 Ebola outbreak. Public Health (2017) 143:60–70. doi: 10.1016/j.puhe.2016.10.020
122. Sun J, Zhang M, Gehl A, Fricke B, Nawaz K, Gluesenkamp K, et al. Dataset of ultralow temperature refrigeration for COVID 19 vaccine distribution solution. Sci Data (1990) 9(1):67. doi: 10.1038/s41597-022-01167-y
123. Stanton MG, Budzik BW, Beutner GL, and Liao H. Low molecular weight cationic lipids for oligonucleotide delivery. [U.S. Patent Publication No. 9669097]. United States Patent and Trademark Office (2017)
124. Suzuki Y, Hyodo K, Suzuki T, Tanaka Y, Kikuchi H, and Ishihara H. Biodegradable lipid nanoparticles induce a prolonged RNA interference-mediated protein knockdown and show rapid hepatic clearance in mice and nonhuman primates. Int J Pharm (2017) 519(1–2):34–43. doi: 10.1016/j.ijpharm.2017.01.016
125. Suzuki Y and Ishihara H. Structure, activity and uptake mechanism of siRNA-lipid nanoparticles with an asymmetric ionizable lipid. Int J Pharm (2016) 510(1):350–8. doi: 10.1016/j.ijpharm.2016.06.124
126. Gindy ME, Feuston B, Glass A, Arrington L, Haas RM, Schariter J, et al. Stabilization of Ostwald ripening in low molecular weight amino lipid nanoparticles for systemic delivery of siRNA therapeutics. Mol Pharm (2014) 11(11):4143–53. doi: 10.1021/mp500367k
127. Suzuki Y, Hyodo K, Tanaka Y, and Ishihara H. siRNA-lipid nanoparticles with long-term storage stability facilitate potent gene-silencing in vivo. J Control Release (2015) 220(A):44–50. doi: 10.1016/j.jconrel.2015.10.024
128. Kainer M, Wiese AD, Benedict K, Braden C, Brandt M, Harris J, et al. Multistate outbreak of fungal infection associated with injection of methylprednisolone acetate solution from a single compounding pharmacy - United States, 2012. Morb Mortal Wkly Rep (2012) 61(41):839–42. doi: 10.1001/jama.2012.64944
129. Smith RM, Schaefer MK, Kainer MA, Wise M, Finks J, Duwve J, et al. Fungal infections associated with contaminated methylprednisolone injections. N Engl J Med (2013) 369(17):1598–609. doi: 10.1056/NEJMoa1213978
130. Centers for Disease Control and Prevention. Multistate outbreak of fungal meningitis and other infections – case count. Centres for Disease Control and Prevention (2024). Available at: https://archive.cdc.gov/#/details?url=https://www.cdc.gov/hai/outbreaks/meningitis-map-large.html
131. Parot J, Mehn D, Jankevics H, Markova N, Carboni M, Olaisen C, et al. Quality assessment of LNP-RNA therapeutics with orthogonal analytical techniques. J Control Release (2024) 367:385–401. doi: 10.1016/j.jconrel.2024.01.037
132. Barriga HMG, Pence IJ, Holme MN, Doutch JJ, Penders J, Nele V, et al. Coupling lipid nanoparticle structure and automated single-particle composition analysis to design phospholipase-responsive nanocarriers. Adv Mater (2022) 34(26):e2200839. doi: 10.1002/adma.202200839
133. Penders J, Pence IJ, Horgan CC, Bergholt MS, Wood CS, Najer A, et al. Single particle automated raman trapping analysis. Nat Commun (2018) 9(1):4256. doi: 10.1038/s41467-018-06397-6
134. Weaver E, O’Hagan C, and Lamprou DA. The sustainability of emerging technologies for use in pharmaceutical manufacturing. Expert Opin Drug Delivery (2022) 19(7):861–72. doi: 10.1080/17425247.2022.2093857
135. Simoens S, Cassiman D, Picavet E, and Dooms M. Are some orphan drugs for rare diseases too expensive? A study of purchase versus compounding costs. Drugs Ther Perspect (2011) 27(10):24–6. doi: 10.2165/11601640-000000000-00000
136. Vo JN, Cieslik M, Zhang Y, Shukla S, Xiao L, Zhang Y, et al. The landscape of circular RNA in cancer. Cell (2019) 176(4):869–881.e13. doi: 10.1016/j.cell.2018.12.021
137. Chen R, Wang SK, Belk JA, Amaya L, Li Z, Cardenas A, et al. Engineering circular RNA for enhanced protein production. Nat Biotechnol (2023) 41(2):262–72. doi: 10.1038/s41587-022-01393-0
138. Santer L, Bär C, and Thum T. Circular RNAs: a novel class of functional RNA molecules with a therapeutic perspective. Mol Ther (2019) 27(8):1350–63. doi: 10.1016/j.ymthe.2019.07.001
139. Zhang W, Jordan KR, Schulte B, and Purev E. Characterization of clinical grade CD19 chimeric antigen receptor T cells produced using automated Clinimacs prodigy system. Drug Des Devel Ther (2018) 12:3343–56. doi: 10.2147/DDDT.S175113
140. Zhu F, Shah NN, Xu H, Schneider D, Orentas R, Dropulic B, et al. CAR-T cell production using the Clinimacs® prodigy system. Blood (2016) 128(22):5724. doi: 10.1182/blood.V128.22.5724.5724
141. Fernández L, Fernández A, Mirones I, Escudero A, Cardoso L, Vela M, et al. GMP-compliant manufacturing of NKG2D CAR memory T cells using CliniMACS prodigy. Front Immunol (2019) 10:2361. doi: 10.3389/fimmu.2019.02361
142. An D, Frassetto A, Jacquinet E, Eybye M, Milano J, DeAntonis C, et al. Long-term efficacy and safety of mRNA therapy in two murine models of methylmalonic acidemia. EBiomedicine (2019) 45:519–28. doi: 10.1016/j.ebiom.2019.07.003
143. An D, Schneller JL, Frassetto A, Liang S, Zhu X, Park J-S, et al. Systemic messenger RNA therapy as a treatment for methylmalonic acidemia. Cell Rep (2017) 21(12):3548–58. doi: 10.1016/j.celrep.2017.11.081
144. Ebrahimi A and Rahim F. Crigler-Najjar syndrome: current perspectives and the application of clinical genetics. Endocr Metab Immune Disord Drug Targets (2018) 18(3):201–11. doi: 10.2174/1871530318666171213153130
145. Strauss KA, Ahlfors CE, Soltys K, Mazareigos GV, Young M, Bowser LE, et al. Crigler-Najjar syndrome type 1: pathophysiology, natural history, and therapeutic frontier. Hepatology (2020) 71(6):1923–39. doi: 10.1002/hep.30959
146. Dhawan A, Lawlor MW, Mazariegos GV, McKiernan P, Squires JE, Strauss KA, et al. Disease burden of Crigler-Najjar syndrome: systematic review and future perspectives. J Gastroenterol Hepatol (2020) 35(4):530–43. doi: 10.1111/jgh.14853
147. European Commission. Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use [Document 32001L0083]. European Commission (2001). Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32001L0083&qid=1748446672656
148. Scheepers HPA, Neerup Handlos V, Walser S, Schutjens MDB, and Neef C. Impact of the council of Europe Resolution on quality and safety assurance requirements for medicinal products prepared in pharmacies for the special needs of patients. Eur J Hosp Pharm (2017) 24(4):218–23. doi: 10.1136/ejhpharm-2016-001017
149. Scheepers HP, Langedijk J, Neerup Handlos V, Walser S, Schutjens MH, and Neef C. Legislation on the preparation of medicinal products in European pharmacies and the Council of Europe Resolution. Eur J Hosp Pharm (2017) 24(4):224–9. doi: 10.1136/ejhpharm-2016-001016
150. Polak Y, Jacobs BAW, and Kemper EM. Pharmacy compounded medicines for patients with rare diseases: lessons learned from chenodeoxycholic acid and cholic acid. Front Pharmacol (2021) 12:758210. doi: 10.3389/fphar.2021.758210
151. European Commission. Regulation (EC) No 1394/2007 of the European Parliament and of the Council of 13 November 2007 on advanced therapy medicinal products and amending Directive 2001/83/EC and Regulation (EC) No 726/2004 [Document 32007R1394]. European Commission (2007). Available at: https://eur-lex.europa.eu/eli/reg/2007/1394/oj/eng.
152. Coppens DG, Gardarsdottir H, Bruin MLD, Meij P, Gm Leufkens H, and Hoekman J. Regulating advanced therapy medicinal products through the hospital exemption: an analysis of regulatory approaches in nine EU countries. Regener Med (2020) 15(8):2015–28. doi: 10.2217/rme-2020-0008.
153. European Commission. Proposal for a directive of the European Parliament and of the council on the union code relating to medicinal products for human use, and repealing Directive 2001/83/EC and Directive 2009/35/EC [COM/2023/192 final]. European Commission (2023). Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:52023PC0192.
Keywords: nanomedicine, nucleic acid therapeutics, mRNA, siRNA, gene editing, orphan diseases, lipid nanoparticles, precision medicine
Citation: Estapé Senti M, Ceccaldi A, Luciani M, Saber N, Schurmann PJL, Geerlings MW, Holig P, de Beer J, Hannus M, Campbell F, Winter M, van Hoeve W, Westerik M, Dorst-Mooiman KD, Dekker J, Fuchs S, Wolbers F, Segers T, IJzerman M, Barriga HMG, De Bruin ML, Borgos SE, Stevens MM, Cullis P and Schiffelers RM. NANOSPRESSO: toward personalized, locally produced nucleic acid nanomedicines. Front Sci (2025) 3:1458636. doi: 10.3389/fsci.2025.1458636
Received: 02 July 2024; Accepted: 12 May 2025;
Published: 26 June 2025.
Edited by:
Thomas Anchordoquy, University of Colorado Anschutz Medical Campus, United StatesReviewed by:
Claes Wahlestedt, University of Miami, United StatesHoracio Cabral, The University of Tokyo, Japan
Copyright © 2025 Estapé Senti, Ceccaldi, Luciani, Saber, Schurmann, Geerlings, Holig, de Beer, Hannus, Campbell, Winter, van Hoeve, Westerik, Dorst-Mooiman, Dekker, Fuchs, Wolbers, Segers, IJzerman, Barriga, De Bruin, Borgos, Stevens, Cullis and Schiffelers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raymond M. Schiffelers, ci5zY2hpZmZlbGVyc0B1bWN1dHJlY2h0Lm5s
†Now OutFox Bio Ltd