 Feihong Zhang
Feihong Zhang Yang Wu1,†
Yang Wu1,† Li Zhang
Li Zhang Bin Xia
Bin Xia- 1Department of Pediatrics, West China Second Hospital, Sichuan University, Chengdu, China
- 2Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Ministry of Education, Chengdu, China
The coexistence of congenital diaphragmatic hernia and esophageal atresia with or without tracheoesophageal fistula is extremely rare; only 36 cases have been reported. We report a case of a preterm male newborn infant with left congenital diaphragmatic hernia, esophageal atresia, and tracheoesophageal fistula and review 27 related cases.
Introduction
Congenital diaphragmatic hernia (CDH) is a developmental defect in the diaphragm that occurs in approximately 1 in 3,300 live births (1). A defect in the diaphragm causes herniation of the abdominal organs into the chest and compression of the lungs, which results in respiratory insufficiency after birth and persistent pulmonary hypertension of the newborn (2). Esophageal atresia (EA) and tracheoesophageal fistula (TEF) are some of the most common congenital abnormalities of the gastrointestinal tract, affecting 1 in 3,000–4,500 live births (3). The co-occurrence of CDH and EA with TEF is very rare and carries a high fatality rate of 51.9%. The fatality rates of right and left CDH and EA with TEF were estimated to be 60% and 44.4%, respectively, while that of left CDH with EA was 80%. Surgery is the only method to correct these deformities. Cases of early postoperative survival have been reported since 1993. However, there is no unified method to treat these two deformities. We report a case of a premature infant with left CDH, EA, TEF and a right aortic arch.
Case report
A male infant weighing 2,350 g with an antenatal diagnosis of left CDH and right aortic arch since the 24-week gestation period was born by cesarean section at 35+2 weeks of gestation. No abnormality was found in amniotic fluid low density gene chip at 21 weeks of gestation. The left CDH was revealed by systematic fetal ultrasound and targeted ultrasound at 24 weeks of gestation. The size of the right lung in the cross section was about 2.4 × 1.57 cm and the lung-to-head ratio (LHR) was about 1.64. Follow-up targeted fetal echocardiography and fetal chest MRI suggested right aortic arch. Fetal ultrasound at 26 weeks of gestation showed polyhydramnios (amniotic fluid: 8.4 cm, amniotic fluid index: 26.0 cm). Targeted ultrasound at 34 weeks of pregnancy showed that the lung-to-head ratio was 1.93.
The baby had mild respiratory distress at birth, with Apgar scores of 5 and 8 at 1 and 5 min, respectively. Immediately after birth, the infant was intubated and admitted to the neonatal intensive care unit (NICU). Attempts to pass a nasogastric tube (NGT) were unsuccessful, and EA was suspected. Chest radiography confirmed the presence of left CDH with multiple air-filled loops of the bowel in the thoracic cavity, which suggested the possibility of EA and TEF with a U-shaped NGT in the middle mediastinum. Emergency surgery was performed after the evaluation. The spleen, stomach, and most of the intestines were returned to the abdominal cavity via a transverse incision of the left upper abdomen, and a 3 × 3 cm defect of the left posterolateral diaphragm was observed(Defect B according to CDH Study Group Staging System). The diaphragmatic defect was intermittently sutured using a non-absorbable suture. It was difficult to maintain the infant's breathing under high-frequency ventilation (HFV); therefore, we did not attempt to perform a thoracotomy to ligate the fistula. A gastrostomy was performed to prevent gastrointestinal flatulence caused by mechanical ventilation. After the first operation, the infant suffered severe pulmonary hypertension and underwent treatment with high-frequency oscillatory ventilation, nitric oxide inhalation, and cetuximab. His blood oxygen saturation under HFV was normal. Subsequently, pulmonary hemorrhage occurred, and a hemodynamically significant patent ductus arteriosus (HsPDA) was considered. Ibuprofen was used for the closure of the PDA. After these treatments, the patient underwent thoracotomy via the left posterolateral incision on day of life (DOL) 16. Due to a large amount of pleural effusion in the pleural cavity and evident mediastinal edema, only the TEF was ligated and divided. Esophageal anastomosis was performed on DOL 39; the distance between the proximal and distal ends was 2.5 cm.
The patient was fed through a gastrostomy tube on DOL 20. No signs of esophageal stricture or gastroesophageal reflux were found on esophagography 10 days after esophageal anastomosis. Unfortunately, the patient developed intestinal failure-associated liver disease due to long-term parenteral nutrition. Biochemical indices, such as liver enzymes and serum conjugated bilirubin, returned to normal after treatment with fish oil monotherapy. The patient was on oral total enteral feeding when he was discharged from the hospital at the age of 3 months. On follow-up at the age of 6 months, the patient was able to raise his head steadily and turn his body over.
Discussion
To the best of our knowledge, 36 cases of CDH, EA, and TEF have been reported to date. We included a total of 27 cases with detailed information (Table 1) in this literature review. There were 17 cases of left CDH, EA, and TEF; 5 cases of left CDH and EA; and 5 cases of right CDH, EA, and TEF. No cases of right CDH or EA have been reported to date. Most reported cases were accompanied by other malformations, the most common of which was a cardiovascular malformation (22.2%), such as a patent ductus arteriosus, atrial septal defect, interruption of the inferior vena cava, right aortic arch, or common arterial trunk. Other malformations included lung agenesis (18.5%), Meckel's diverticulum (14.8%), renal dysplasia (11.1%), trisomy 18 (7.4%), spinal deformities (7.4%), and facial deformities (3.7%). CDH, EA, and TEF are fatal deformities in children; however, surgery has been the key to saving their lives since 1970 (4).
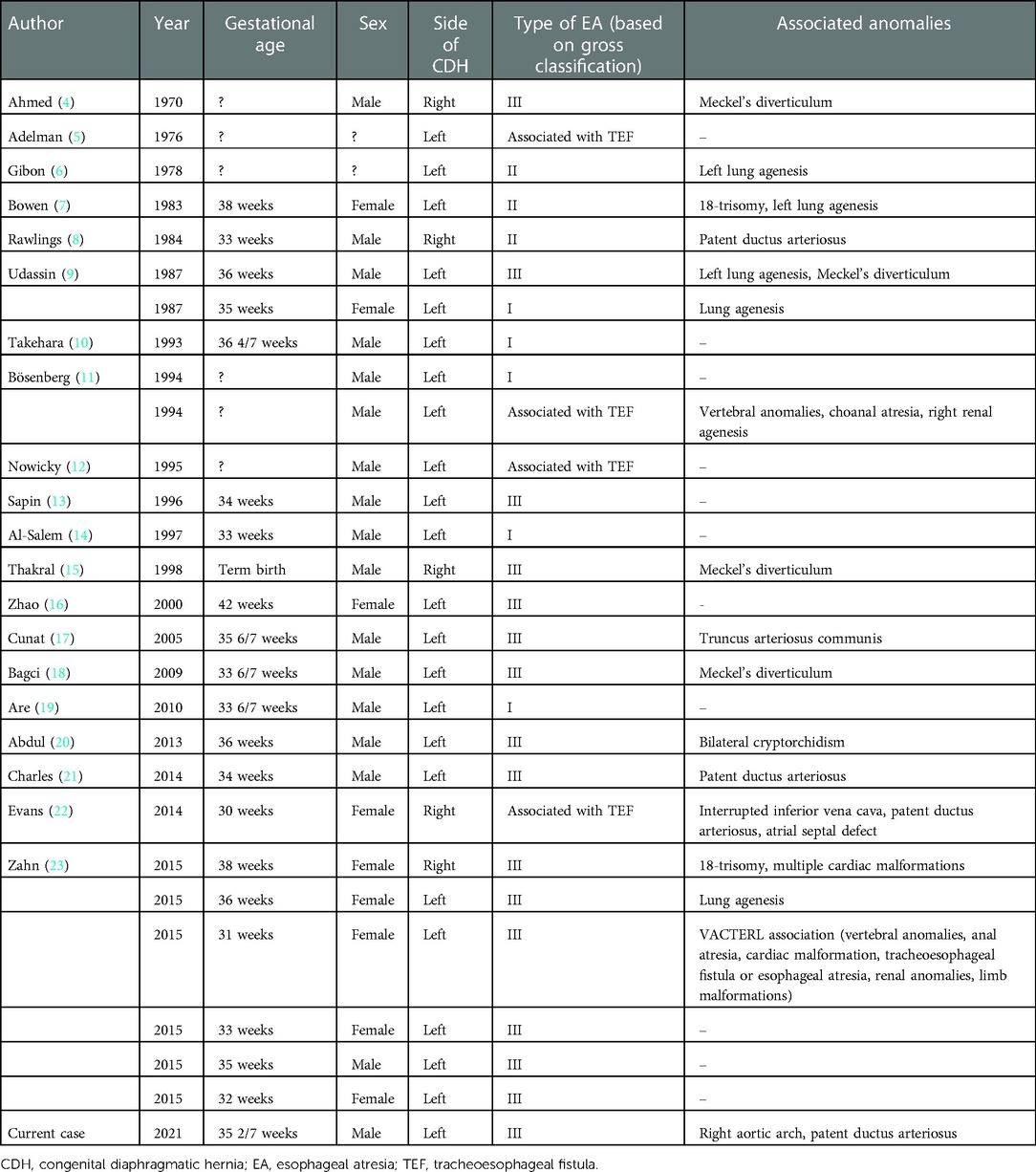
Table 1. Summary of findings of CDH associated with EA or EA and TEF.
Treatment of left CDH, EA, and TEF
Left CDH with EA and TEF is the most common combination of deformities, and our review includes a total of 17 cases with this combination (Table 1). Among them, 13 of the cases had relevant surgical records (Table 2). In 8 cases of staged surgeries, CDH was repaired through an abdominal incision followed by esophageal anastomosis through a right thoracotomy, and a total of 4 patients survived. On average, the diaphragmatic hernia was repaired on DOL 1, and the TEF and EA were repaired between DOL 10 and DOL 14. The shortest discharge time was DOL 48, and the longest was 6.5 months. One of the patients that survived underwent diaphragmatic hernia repair on DOL 1, ligation and division of the TEF on DOL 13, and repair of the EA on DOL 49, with a total discharge time of 4 months after birth. Our patient also underwent three surgeries and was discharged at the age of 3 months. The repair of EA and TEF was performed on DOL 1 in only one reported cases (5). He was discharged at the age of 4 months and started to develop normally at 10 months old (5). In addition, two patients underwent a one-stage operation (13, 23). One died on DOL 113 due to chronic pulmonary insufficiency. The other was discharged at the age of 3 months. In general, both one-stage surgery and staged surgery seem to be reasonable choices. One-stage operation is taken into consideration only if the patient's condition permits. Interestingly, although most surgeons believed that the repair of diaphragmatic hernia should be put in the first place in staged surgery, repairing the EA first does not seem to have much to do with the survival rate(5). Therefore, we believed that the first stage of surgery should be more individualized according to the patient's condition.
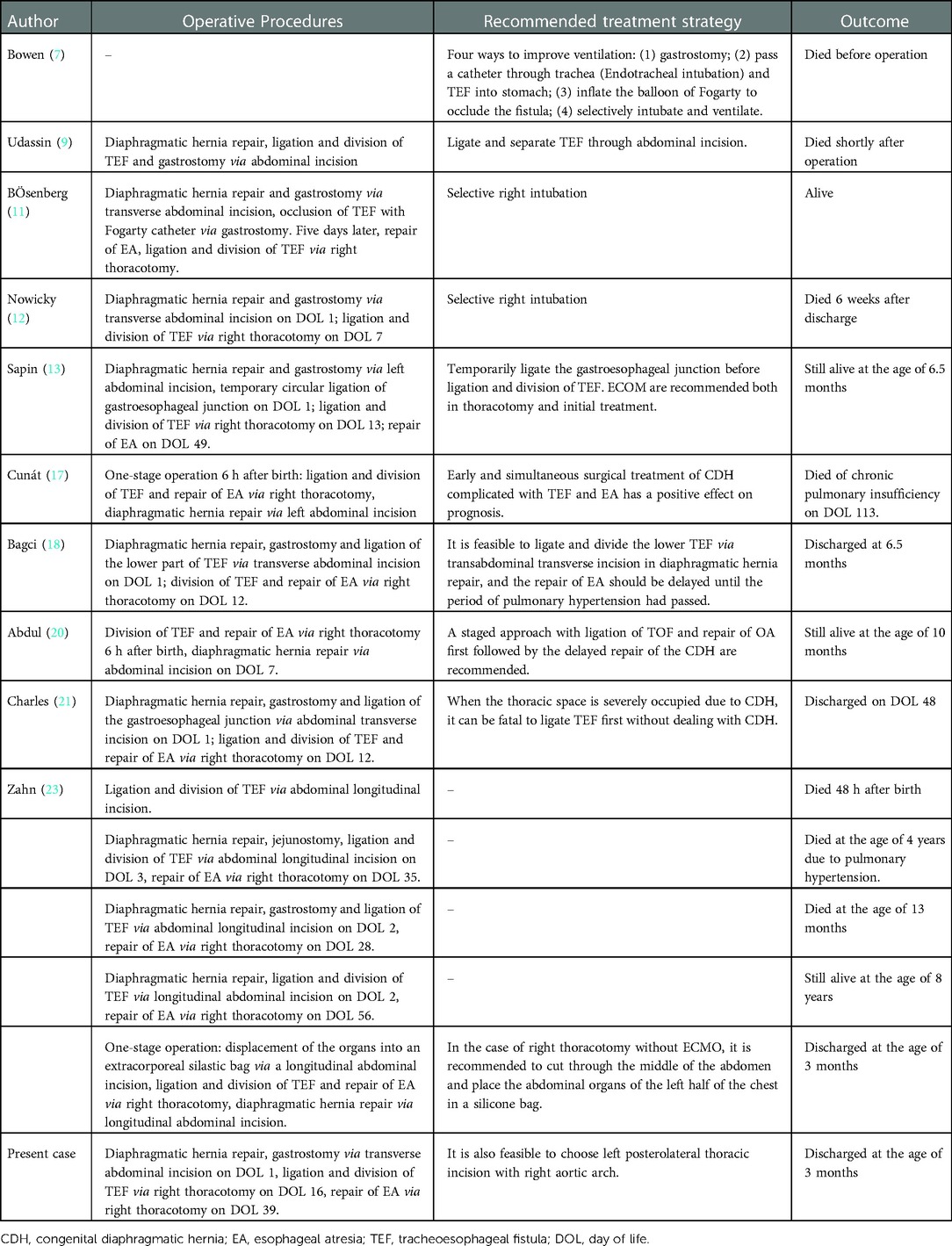
Table 2. Summary of treatments of left CDH associated with EA or EA and TEF.
Sapin et al. (13) believed that gastrostomy was the most effective way to solve progressive flatulence caused by TEF in the gastrointestinal tract. Almost all surgical patients underwent a gastrostomy. Early gastrostomy stabilized the respiratory state and created conditions for subsequent EA and TEF repair. In three reported cases, in addition to gastrostomy, circular ligation was performed at the gastroesophageal junction to reduce air leakage caused by TEF (13, 21, 23). Among these cases, one patient reported by Zahn et al. (23) had an obvious esophageal stricture at the ligation site. Therefore, circular ligation of the gastroesophageal junction should be performed cautiously. Notably, in three cases of staged surgery, the TEF was repaired in the first stage of the operation (23). A longitudinal abdominal incision made it possible to ligate and divide the TEF in the operation of diaphragmatic hernia. Early closure of the fistula improves ventilation function by preventing gas from leaking into the intestines through the trachea, and this may have the same effect as a gastrostomy. Therefore, we recommend that TEF be repaired in the first stage of the operation as much as possible.
Treatment of right CDH, EA, and TEF
Similar to surgical procedures for a left CDH, the routine operation for patients with right CDH with EA and TEF is transabdominal repair of diaphragmatic hernia, ligation, and separation of the TEF and EA repair via a right thoracic incision. Of the five reported cases of right CDH with EA and TEF, four patients underwent surgery (Table 3). Two patients died shortly after diaphragmatic hernia repair, ligation, and division of TEF. The other two patients who underwent one-stage surgery survived during follow-up. In summary, one-stage surgery seems to be a reasonable choice for patients with right-sided CDH complicated by EA and TEF.
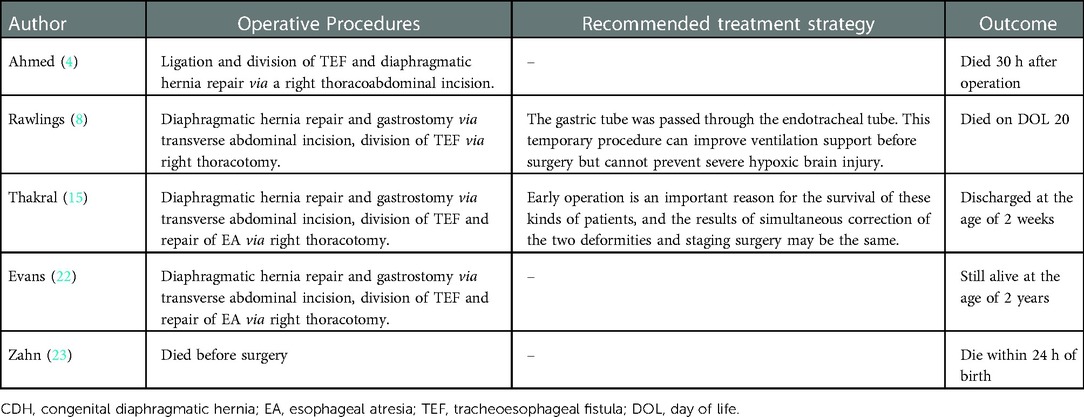
Table 3. Summary of treatments of right CDH associated with EA or EA and TEF.
Treatment of left CDH and EA
Among the five patients with CDH and EA, two died within 24–48 h due to severe persistent hypoxemia after diaphragmatic hernia repair (with or without esophagogastric anastomosis) (Table 4). Two patients underwent diaphragmatic hernia repair on DOL 3 and esophageal anastomosis on DOL 10 or 15. Although all patients died of septicemia at an advanced stage, some surgeons still believe that diaphragmatic hernia repair can be performed initially, and EA repair can be delayed while pulmonary hypertension resolves (9, 14). Only one patient survived during follow-up. In this case, EA with a low esophageal end was confirmed before surgery; therefore, a chevron incision was used to correct both deformities at the same time. Three months after discharge, the patient was still alive. Owing to the small number of cases, there is no unified surgical method for addressing combined deformities.
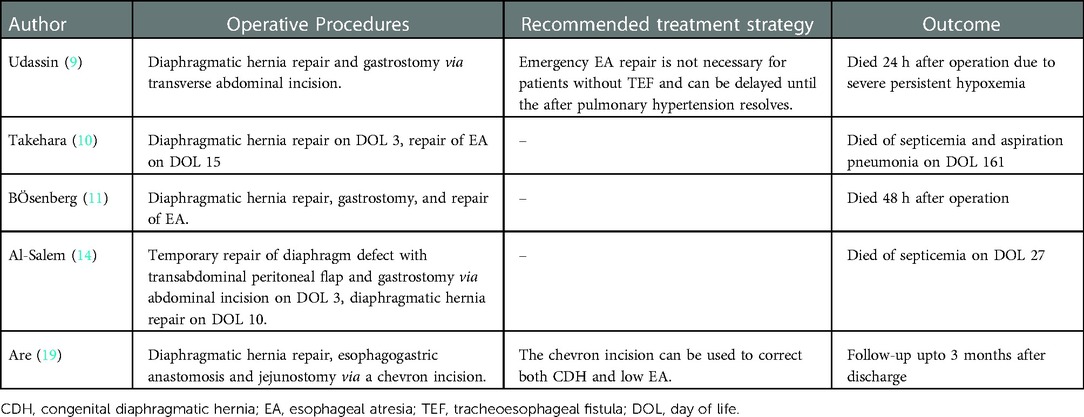
Table 4. Summary of treatments of left CDH associated with EA.
Conclusion
For patients with a left or right CDH with EA and TEF, a one-stage surgery is possible when the patient's breathing is stable. In staged surgery, in addition to gastrostomy, early ligation and division of the TEF are also important for stabilizing the respiratory state of patients. In patients with left CDH with EA, some surgeons recommend staged surgery to repair the EA after correcting for pulmonary hypertension, while others use a chevron incision to correct both deformities in a one-stage surgery.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
The Author Contributions section is mandatory for all articles, including articles by sole authors. If an appropriate statement is not provided on submission, a standard one will be inserted during the production process. The Author Contributions statement must describe the contributions of individual authors referred to by their initials and, in doing so, all authors agree to be accountable for the content of the work. Please see here for full authorship criteria. All authors contributed to the article and approved the submitted version.
Acknowledgments
This is a short text to acknowledge the contributions of specific colleagues, institutions, or agencies that aided the efforts of the authors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Canadian Congenital Diaphragmatic Hernia Collaborative, Puligandla PS, Skarsgard ED, Offringa M, Adatia I, Baird R, et al. Diagnosis and management of congenital diaphragmatic hernia: a clinical practice guideline. CMAJ. (2018) 190:E103–12. doi: 10.1503/cmaj.170206
2. Gien J, Palmer C, Liechty K, Kinsella JP. Early abnormalities in gas exchange in infants with congenital diaphragmatic hernia. J Pediatr. (2022) 243:188–92. doi: 10.1016/j.jpeds.2021.12.009
3. Way C, Wayne C, Grandpierre V, Harrison BJ, Travis N, Nasr A. Thoracoscopy vs. thoracotomy for the repair of esophageal atresia and tracheoesophageal fistula: a systematic review and meta-analysis. Pediatr Surg Int. (2019) 35:1167–84. doi: 10.1007/s00383-019-04527-9
4. Ahmed S. Right-sided Bochdalek hernia associated with esophageal atresia and tracheo-esophageal fistula. J Pediatr Surg. (1970) 5:256. doi: 10.1016/0022-3468(70)90284-8
5. Haium AAA, Sim SW, Ong LY, Rajadurai VS. Congenital diaphragmatic hernia associated with oesophageal atresia and tracheooesophageal fistula in a low birth weight infant. BMJ Case Rep. (2013) 2013:bcr2013200014. doi: 10.1136/bcr-2013-200014
6. Sapin E, Berg A, Raynaud P, Lapeyre G, Seringe R, Helardot PG. Coexisting left congenital diaphragmatic hernia and esophageal atresia with tracheoesophageal fistula: successful management in a premature neonate. J Pediatr Surg. (1996) 31:989–91. doi: 10.1016/s0022-3468(96)90432-7
7. Zahn KB, Scherf S, Schaible T, Wessel LM, Hagl CI. Single-staged surgical approach in congenital diaphragmatic hernia associated with esophageal atresia. J Pediatr Surg. (2015) 50:1418–24. doi: 10.1016/j.jpedsurg.2015.04.015
8. Charles EJ, Judge JM, Vergales BD, Randall AH, Kane BJ, McGahren ED, et al. Managing concomitant congenital diaphragmatic hernia, esophageal atresia, and tracheoesophageal fistula: a case report of a premature infant that achieved survival. J Pediatr Surg Case Rep. (2014) 2:239–42. doi: 10.1016/j.epsc.2014.04.009
9. Udassin RZOP, Zamir O, Peleg O, Lernau OZ. Coexisting left diaphragmatic hernia and esophageal atresia. Pediatr Surg Int. (1987) 2:301–3. doi: 10.1007/BF00176204
10. Al-Salem AH, Qaisruddin S, Varma KK. Concurrent left congenital diaphragmatic hernia and esophageal atresia: case report and review of the literature. J Pediatr Surg. (1997) 32:772–4. doi: 10.1016/s0022-3468(97)90032-4
11. Adelman S, Benson CD. Bochdalek hernias in infants: factors determining mortality. J Pediatr Surg. (1976) 11:569–73. doi: 10.1016/s0022-3468(76)80015-2
12. Gibon Y, Borde J, Mitrofanoff P, Lefort J. [Association of left diaphragmatic hernia, lung agenesia and esophageal atresia (author’s transl)]. Chir Pediatr. (1978) 19:261–7.737826
13. Bowen A. The ventilatory dilemma of coexisting diaphragmatic hernia, esophageal atresia, and tracheoesophageal fistula. Crit Care Med. (1983) 11:390–1. doi: 10.1097/00003246-198305000-00017
14. Rawlings JS, Shetler PL, Fill WL, Cathcart CF. Concurrent right diaphragmatic hernia and Type C Tracheoesophogeal fistula. A case report. Clin Pediatr. (1984) 23:518–20. doi: 10.1177/000992288402300917
15. Takehara H, Komi N, Okada A, Nishi M, Masamune K. Left diaphragmatic hernia associated with lower esophageal atresia. Pediatr Surg Int. (1993) 8:339–40. doi: 10.1007/BF00173360
16. Bösenberg AT, Mickel RE, Hadley GP. Management of oesophageal atresia in association with congenital diaphragmatic hernia. Pediatr Anesth. (1994) 4:263–6. doi: 10.1111/j.1460-9592.1994.tb00176.x
17. Nowicky DJ. Simultaneous Bochdalek hernia and type C tracheoesophageal fistula. J S C Med Assoc. (1995) 91:303–4.7658682
18. Thakral CL, Sajwani MJ. Concurrent right diaphragmatic hernia and esophageal atresia. Pediatr Surg Int. (1998) 14:96–7. doi: 10.1007/s003830050448
19. Meijian Zhao QMWL. Congenital esophageal atresia and tracheoesophageal fistula complicated with congenital diaphragmatic hernia: a case report. Tianjin Med. (2001) 1:61.
20. Cunát V, Stranák Z, Pýcha K, Tláskal T, Melichar J, Miletín J, et al. Congenital diaphragmatic hernia associated with esophageal atresia, tracheoesophageal fistula, and truncus arteriosus in a premature newborn. Pediatr Surg Int. (2005) 21:684–6. doi: 10.1007/s00383-005-1443-4
21. Bagci S, Müller A, Heydweiller A, Bachour H, Petersen C, Heep A, et al. Temporary banding of a lower tracheoesophageal fistula in an infant with left congenital diaphragmatic hernia and esophageal atresia. Eur J Pediatr Surg. (2009) 19:260–3. doi: 10.1055/s-2008-1038960
22. Are NK, Nagarjuna K, Kannaiyan L. A rare association of congenital diaphragmatic hernia with lower esophageal atresia and perforation. Int J Pediatr. (2010) 2010:738546. doi: 10.1155/2010/738546
Keywords: congenital abnormalities, diaphragm defect, deformities, premature infants, surgery
Citation: Zhang F, Wu Y, Zhang L and Xia B (2022) Case Report: Congenital diaphragmatic hernia associated with esophageal atresia and tracheoesophageal fistula. Front. Surg. 9:1061951. doi: 10.3389/fsurg.2022.1061951
Received: 5 October 2022; Accepted: 7 December 2022;
Published: 4 January 2023.
Edited by:
Lucas Wessel, University Medical Centre Mannheim, University of Heidelberg, GermanyReviewed by:
Dick Tibboel, Erasmus Medical Center, NetherlandsAntti Koivusalo, Helsinki University Central Hospital, Finland
Laura Valfrè, Bambino Gesù Children’s Hospital (IRCCS), Italy
© 2023 Zhang, Wu, Zhang and Xia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bin Xia eGlhYmluMTk3MkAxNjMuY29t
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Pediatric Surgery, a section of the journal Frontiers in Surgery
Abbreviations CDH, congenital diaphragmatic hernia; EA, esophageal atresia; TEF, tracheoesophageal fistula; NICU, neonatal intensive care unit; NGU, nasogastric tube; HFV, high-frequency ventilation; HFOV, high-frequency oscillatory ventilation; PDA, patent ductus arteriosus; DOL, day of life.