 Ruben J. Hoepelman1,†
Ruben J. Hoepelman1,† Fabrizio Minervini2*†
Fabrizio Minervini2*† Frank J. P. Beeres3
Frank J. P. Beeres3 Bas van Wageningen4
Bas van Wageningen4 Frank F. IJpma5Nicole M. van Veelen3Koen W. W. Lansink6Jochem M. Hoogendoorn7Mark. C. P. van Baal1
Frank F. IJpma5Nicole M. van Veelen3Koen W. W. Lansink6Jochem M. Hoogendoorn7Mark. C. P. van Baal1 Rolf H. H. Groenwold8,9Roderick M. Houwert1on behalf of the NEXT study group1
Rolf H. H. Groenwold8,9Roderick M. Houwert1on behalf of the NEXT study group1
- 1Department of Trauma Surgery, University Medical Center Utrecht, Utrecht, Netherlands
- 2Department of Thoracic Surgery, Luzerner Kantonsspital, Lucerne, Switzerland
- 3Department of Orthopedics and Trauma Surgery, Luzerner Kantonsspital, Lucerne, Switzerland
- 4Department of Trauma Surgery, Radboud University Medical Center Utrecht, Nijmegen, Netherlands
- 5Department of Trauma Surgery, University Medical Center Groningen, Groningen, Netherlands
- 6Department of Trauma Surgery, Elisabeth-Tweesteden Hospital, Tilburg, Netherlands
- 7Department of Trauma Surgery, Haaglanden Medical Center, Hague, Netherlands
- 8Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, Netherlands
- 9Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, Netherlands
Introduction: Most studies about rib fractures focus on mortality and morbidity. Literature is scarce on long term and quality of life (QoL) outcomes. Therefore, we report QoL and long-term outcomes after rib fixation in flail chest patients.
Methods: A prospective cohort study of clinical flail chest patients admitted to six level 1 trauma centres in the Netherlands and Switzerland between January 2018 and March 2021. Outcomes included in-hospital outcomes and long-term outcomes, such as QoL measurements 12 months after hospitalization using the EuroQoL five dimensions (EQ-5D) questionnaire.
Results: Sixty-one operatively treated flail chest patients were included. Median hospital length of stay was 15 days and intensive care length of stay was 8 days. Sixteen (26%) patients developed pneumonia and two (3%) died. One year after hospitalization the mean EQ5D score was 0.78. Complication rates were low and included hemothorax (6%) pleural effusion (5%) and two revisions of the implant (3%). Implant related irritation was commonly reported by patients (n = 15, 25%).
Conclusions: Rib fixation for flail chest injuries can be considered a safe procedure and with low mortality rates. Future studies should focus on quality of life rather than solely short-term outcomes.
Trial registration: Registered in the Netherlands Trial Register NTR6833 on 13/11/2017 and the Swiss Ethics Committees Registration Number 2019-00668
Introduction
Thoracic trauma is a potentially life-threatening injury which often result in rib fractures (1). Patients with rib fractures represent a heterogenous group of patients among whom injury severity, morbidity, and mortality differ significantly (2). Distinction between patients with and without a flail chest is paramount, as flail chest injuries are associated with higher morbidity and mortality (1, 2).
Historically, patients with rib fractures were treated nonoperatively, however, since the introduction of the dedicated plating systems, rib fixation has become a routinely performed procedure in many trauma centers (3). Indications for rib fixation include flail chest injuries, failure to wean from mechanical ventilation, severe thorax deformity and inadequately manageable pain through conservative measures. Although rib fixation has not proven beneficial in all patients with multiple rib fractures, it has shown to improve in-hospital outcomes in flail chest patients (2, 4–6). The essence of rib fixation is creating a stable chest wall in order to facilitate adequate ventilation and reduce fracture related pain, caused by paradoxical movement of the chest wall. There are several different methods for rib fixation of which plate osteosynthesis is most widely used (7).
Rib fixation should be performed as soon as possible (preferable within 72 h) after admission, however treatment strategy and timing should still be evaluated for each individual patient, as flail chest patients often suffer from serious intra-and extra-thoracic injuries as well (8).
Mortality after multiple rib fractures has steadily declined in the last decades (1, 9). This is mainly due to the vast improvements in trauma care and intensive care management in general. Therefore, focus in trauma research has shifted from mortality to morbidity and Quality of Life (QoL) (10, 11). Nonetheless, most studies on rib fixation in flail chest patients are still focused on in-hospital outcomes, while studies reporting long term outcomes and quality of life are limited. Therefore, the aim of this study was to report short and long-term outcomes of a cohort of operatively treated flail chest patients.
Methods
In this study we focus solely on patients with flail chest injuries who received operative treatment. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (12).
Patients and study design
This was a multicentre prospective cohort study conducted in five level 1 trauma centres in the Netherlands and one in Switzerland. All patients 18 years and older with computerized tomography (CT) scan confirmed flail chest injuries, which is defined as clinically visible paradoxical movement of a portion of the chest wall and three or more consecutive ribs broken, each in at least two places, were eligible for inclusion. Patients were excluded in case of cognitive impairment, non-traumatic rib fractures, and rib fractures due to cardiopulmonary resuscitation. The study was registered in the Netherlands Trial Registry (NTR6833). Approval from the institutional review board was obtained at every study site. Informed consent was obtained from all participants.
Rib fixation
Rib fixation was always performed or supervised by a senior thoracic and/or orthopaedic trauma surgeon with experience in surgical treatment of rib fractures. Preoperative planning was done using a chest CT scan with 3D reconstruction. Prophylactic preoperative antibiotic therapy (2 g Cefazolin i.v.) was administered to all patients. The surgical approaches were performed as described by Taylor et al. (6). After reduction, ideally internal fixation was performed using at least three bicortical screws on each side of the fracture and the MatrixRIB system (Depuy Synthes). The number of ribs fixated was left to the discretion of the attending surgeon, with the goal of achieving a stable thorax. Consequently, not all fractured ribs associated with the flail segment were always stabilized.
Patient characteristics
Patient characteristics measured at hospital admission included age, sex, body mass index (BMI), American Society of Anaesthesiologist (ASA) score, presence of chronic obstructive pulmonary disease (COPD), smoking status, trauma mechanism, abbreviated injury scale (AIS) score (13), injury severity score (ISS), number of fractured ribs, concomitant injuries (i.e., pulmonary contusion, pneumothorax, haemothorax, sternum, and/or clavicle fracture), and laboratory results (specifically venous blood pH and base excess) (14, 15).
Outcomes
Outcomes included: Intensive care unit length of stay (ILOS), hospital length of stay (HLOS), duration of mechanical ventilation (DMV), need for tracheostomy, pneumonia rate and other in-hospital complications, in-hospital mortality rate, and general pain [measured using a numeric rating scale (NRS)]. Mid- and long-term outcomes were measured at the outpatient clinic visit at 6 weeks and using telephone interviews after 12 months. These measures included pain with breathing and coughing (measured using the NRS), quality of life (measured using the EQ5D), dyspnoea burden [measured using the modified Medical Research Council (mMRC) dyspnoea scale], and return to work and sports in weeks. Surgery-specific complications included fracture-related infection, symptomatic non-union, and implant removal (assessed using Hulsmans et al.'s algorithm) (16, 17). Pneumonia was defined as clinical signs or symptoms (two or more present; temperature > 38.5°C, auscultation with suspicion for infiltrate, or purulent sputum) and/or additional tests (thoracic radiographs with signs of infiltrate, leucocytosis, elevated C-reactive protein,) for which antimicrobial therapy was needed. Acute respiratory distress syndrome (ARDS) was defined according to the Berlin definition (18). Fracture-related infections were diagnosed according to the FRI consensus definition (16). Symptomatic non-union was defined as the presence of unsuccessfully healed ribs, confirmed by CT scan, at least 6 months after trauma, with clinical evidence of pain. The EQ5D-5L is a standardized instrument for generic health status measurements to assess the quality of life (19). The mMRC is a five-category scale that characterizes the level of dyspnoea with physical activity (20).
Statistical analyses
Data were analyzed using SPSS version 28.0 (SPSS, Chicago, USA). Missing values were not imputed. Continuous variables were presented as mean with standard deviation or median with interquartile ranges (IQR). Categorical data were presented as frequencies and percentages. A one-sample T-test was used to compare the EQ5D index score to the population norm (0.84) (21).
Results
Patients
From January 2018 to March 2021, 87 patients with clinical flail chest injuries were included of whom 61 were treated operatively. Follow-up was completed March 2022, with a completion rate of 77% (Figure 1). Mean age was 60.8 ± 15.9, 43 patients (71%) were male and 67% of patients were classified as ASA 1 or 2. Most patients were polytrauma patients with a mean ISS of 26.4 ± 11.9 and a mean Thorax trauma severity score (TTSS) of 12.8 ± 3.5. The median number of rib fractures was 10 (8–12.5), and 52.5% had bilateral fractures. The rate of concomitant thoracic injuries was high; 91.8% had a pneumothorax, 60.7% a haemothorax and 57.4% a pulmonary contusion (Table 1).
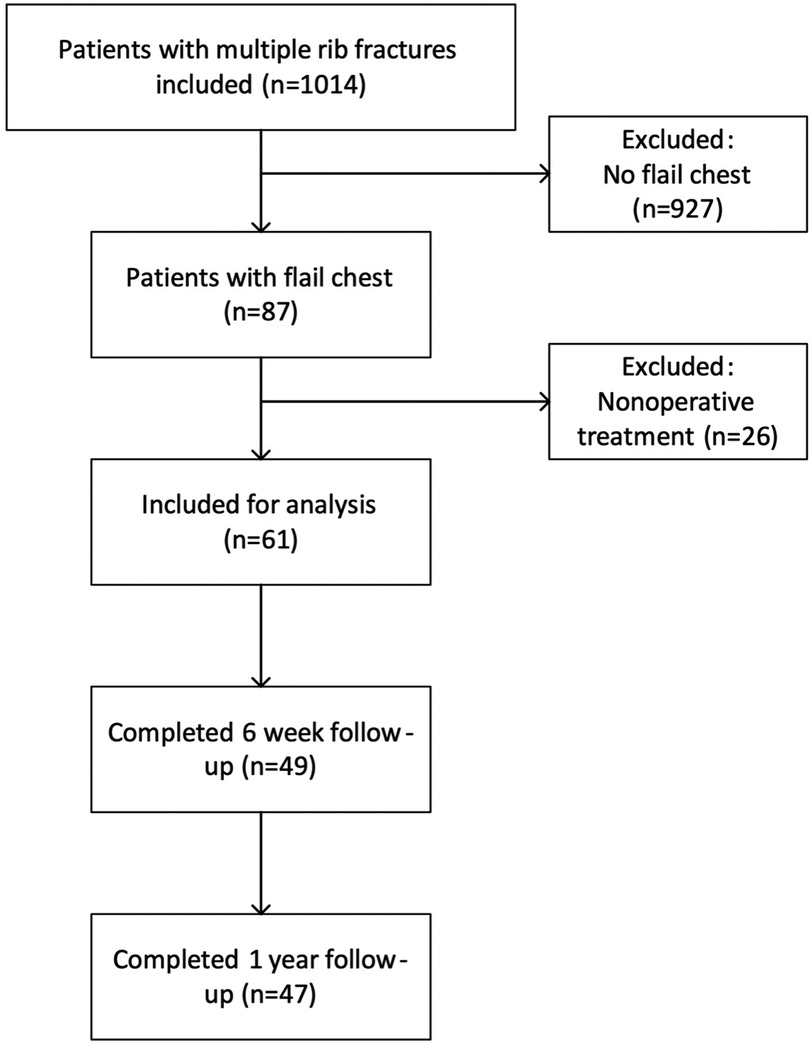
Figure 1. Flow diagram of inclusion and follow-up.
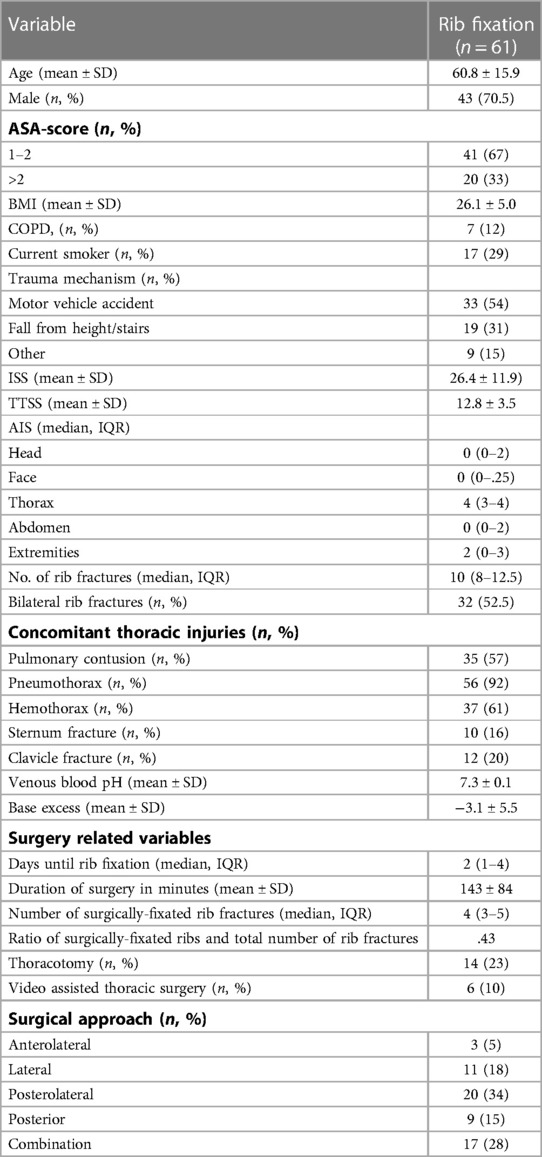
Table 1. Baseline characteristics of operatively treated patients with flail chest injuries.
Surgery related information
The median number of days to surgery was 2 (1–4) days with a mean duration of surgery of 143 ± 84 min. The median number of fixated ribs was 4 (3–5), which was a proportion of 0.43 of the number of fractured ribs. Video assisted thoracic surgery was performed in 6 patients (10%) aiming to better localize the fractures or identify/treat other thoracic injuries. In total there were two implant related complications (3.3%) for which revisions were performed. One implant dislocated during the initial in-patient stay, while the second dislocation was detected during follow-up. There were no infections nor symptomatic non-unions.
Primary and secondary outcomes
The median hospital length of stay was 15 (10–28) days. Fourtyseven (77%) patients were admitted to the ICU with a median duration of ICU stay of 8 (3–14) days. Mechanical ventilation was necessary in 38 patients (62%) with a median duration of 6.5 days. Sixteen patient (26%) developed pneumonia; the rate of other (respiratory) complications was low. Two patients died during admission (3.3%), one patient developed pneumonia and died due to respiratory failure. The second patient died due to unrelated causes. All outcomes are available in Table 2.

Table 2. Outcomes of operatively treated patients with flail chest injuries.
Mid- and long-term outcomes
Quality of life measured using the EQ5D score was median 0.71 (0.58–0.80) after six weeks and 0.78 (0.57–0.90) after one year, while the median EQ5D VAS score was 70 (40–70) at the six week follow-up and 70 (60–75) at one year. The complication rate was low at six weeks (pneumonia 3% (n = 2), pleural effusion 3% (n = 2)), while implant irritation after one year was high; 15 patients (24.6%) reported irritation and two patients (3.3%) had the implants removed prior to the one year follow-up. One patient had died prior to the one year follow-up due to causes unrelated to the thoracic trauma. Median return to work was 14 (6.5–19.5) weeks and return to sports was 23 (9.75–32.5) weeks among patients that performed these activities before injury.
Discussion
This study describes the clinical and long-term outcomes of a prospective cohort of operatively treated flail chest patients. Although all patients were severely injured, mortality rate (3%) and surgery-related complications (3%) were low. Quality of life as measured by the EQ5D was 0.78 (0.6–0.9) after one year and 26% of the patients experienced implant related irritation.
Comparison to previous literature
There are several previously published prospective studies and trials that report on flail chest patients (22–28). Although comparison of studies is complicated by heterogeneity in inclusion criteria and different definitions of flail chests, most studies report benefits after rib fixation compared to nonoperative treatment in flail chest patients. Advantages are mostly observed in patient who were ventilated at the time of rib fixation.
The results of our study closely resemble those of the operative group of the most recently published RCT on the subject (23). Patients' characteristics and outcomes are remarkably similar, most likely due to similar indications for rib fixation. They conclude a potential advantage with operative treatment in the subgroup of patients who were ventilated at the time of randomization, but not in those that were not ventilated.
Our study adds to current literature as one of the few studies to report 1-year outcomes. Most studies focus on in-hospital or short-term outcomes, which is also demonstrated by Supplementary Material Table S1. Marasco et al. reports QoL after 6 months (21). They reported no difference between operative and nonoperative treatment in SF-36 scores (21), although the reported scores were lower compared to population's norms. Caragounis et al. reports an excellent EQ5D score of 0.93 after rib fixation (28). It is difficult to compare this to our or other studies as they give limited information about their cohort and no in-hospital information. Walters et al. report QoL as well, with varying time to follow-up (mean 17.6 SD 9.5 months) (25). They did not find any differences between their groups, however, interestingly their EQ5D-5l scores are much lower compared to our cohort (0.66 vs. 0.78). It is not readily apparent why this is the case. EQ5D population norms are generally lower in the UK compared to the Netherlands and Switzerland and their reported return rate was 65% (n = 36) for the operative group which makes it more susceptible to selection bias compared to the return rate of 77% (n = 48) in our cohort (29). TheEQ5D value of 0.78 in our study is also significantly (p < 0.001) lower than population norms in the Netherlands (21). However, this is common after trauma and whether this is a clinically important difference remains up to debate (11, 30).
We do consider rib fixation a safe procedure. There were no symptomatic non-unions nor infections and only two (3.3%) implant related complications for which additional surgery was required. These low rates are supported by literature, with complication rates between 1.3–3% (31, 32). Overall surgery related complication rates lie between 10%–16%, but most being minor and not requiring immediate reinterventions (31, 33). Similar good outcomes were reported by De Palma et al. in a retrospective analysis which included 27 patients who underwent surgical stabilization of the thoracic wall for traumatic and non traumatic chest wall disease (34).
Finally, implant irritation is not often reported in studies, but can be a burden to patients. In our study the rate was 26%. Implant irritation predisposes a patient to implant removal. Interestingly, previous research from one of our participating hospitals found plate related irritation rates 53% (33). Whether this decrease is due to more experience (as these results from the prior study were from 6 to 10 years ago), different plating systems or other reasons is unknown. When deciding which patients to operate both the low complication rate and the high implant irritation rate should be kept in mind, as preventing a secondary operation is not only cost effective it also improves trauma patient care.
Limitations
Several limitations should be acknowledged. The noncomparative design of our study doesn't allow for comparison to other treatment methods (notably nonoperative treatment). However, our study adds to current literature in reporting prospectively gathered long-term outcomes, which are scarce. Second, our follow up does not allow to accurately measure long-term implant removal rate, as follow-up was limited to one year.
Third, EQ5D-5L and mMRC are subjective questionnaires and assess general health and not specifically thorax-related problems. The vast majority of the patients described in this cohort were polytrauma patients; therefore, concomitant injuries but also comorbidities could have influenced the outcome. Lastly, the transition from hospital to home is a critically vulnerable period for patients, which is also dependent on health care system and social class of patients. As there is limited literature on this transition period among trauma patients we do not know how this could have influenced for instance quality of life in our population. For future studies, applying a biopsychosocial model might be able to provide more insight into the matter.
Conclusion
Flail chest remains a severe injury, however, mortality has declined spectacularly compared to a decade ago. Rib fixation can be considered a safe procedure, but the injury and treatment still impact rehabilitation and quality of life of the patient. Future studies should therefore shift their focus to these aspects to further improve trauma patients care.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by regional Medical Research Ethics Committee UMC Utrecht. All participants have given written permission/informed consent for participations in this study.
Author contributions
RJH and FM: were responsible for the conceptualization of this study. NV, RJH, and FJPB: collected the data. RJH and RHHG: performed the data analysis. The first draft of the manuscript was written by RJH and FM and all authors commented on previous versions of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was financially supported by the DePuy Synthes (grant number DPS-TCMF-2017-036). The organization was not involved in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. All researchers are independent from the funder. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgments
This work was part of the activities of the Natural Experiments Study Group (www.next-studygroup.org).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Peek J, Ochen Y, Saillant N, Groenwold RHH, Leenen LPH, Uribe-Leitz T, et al. Traumatic rib fractures: a marker of severe injury. A nationwide study using the national trauma data bank. Trauma Surg Acute Care Open. (2020) 5:e000441. doi: 10.1136/tsaco-2020-000441
2. Beks RB, Peek J, de Jong MB, Wessem KJP, Öner CF, Hietbrink F, et al. Fixation of flail chest or multiple rib fractures: current evidence and how to proceed. A systematic review and meta-analysis. Eur J Trauma Emerg Surg. (2019) 45:631–44. doi: 10.1007/s00068-018-1020-x
3. Marasco SF, Nguyen Khuong J, Fitzgerald M, Summerhayes R, Sekandarzad MW, Varley V, et al. Flail chest injury—changing management and outcomes. Eur J Trauma Emerg Surg. (2022). doi: 10.1007/s00068-022-02152-1. [Epub ahead of print]
4. Marasco SF, Balogh ZJ, Wullschleger ME, Hsu J, Patel B, Fitzgerald M, et al. Rib fixation in non-ventilator-dependent chest wall injuries: a prospective randomized trial. J Trauma Acute Care Surg. (2022) 92:1047–53. doi: 10.1097/TA.0000000000003549
5. Hoepelman RJ, Beeres Frank JP, Beks RB, Sweet AAR, Ijpma FF, Lansink KWW, et al. Non-operative vs. Operative treatment for multiple rib fractures after blunt thoracic trauma: a multicenter prospective cohort study. Eur J Trauma Emerg Surg. (2022) 49:461–71. doi: 10.1007/s00068-022-02093-9
6. Leinicke JA, Elmore L, Freeman BD, Colditz GA. Operative management of rib fractures in the setting of flail chest: a systematic review and meta-analysis. Ann Surg. (2013) 258:914–21. doi: 10.1097/SLA.0b013e3182895bb0
7. Divisi D, Mucilli F, Leonardo GD, Zaccagna G, De Vico A, Camplese P, et al. Plates versus struts versus an extracortical rib fixation in flail chest patients: two-center experience. Injury. (2021) 52(2):235–42. doi: 10.1016/j.injury.2020.09.018
8. Pieracci FM, Coleman J, Ali-Osman F, Mangram A, Majercik S, White TW, et al. A multicenter evaluation of the optimal timing of surgical stabilization of rib fractures. J Trauma Acute Care Surg. Lippincott Williams and Wilkins (2018) 84(1):1–10. doi: 10.1097/TA.0000000000001729
9. Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the elderly. The Journal of Trauma: Injury, Infection and Critical Care (J Trauma). (2000) 48(6):1040–7. doi: 10.1097/00005373-200006000-00007.
10. Hietbrink F, Houwert RM, van Wessem KJP, Simmermacher RKJ, Govaert GAM, de Jong MB, et al. The evolution of trauma care in The Netherlands over 20 years. Eur J Trauma Emerg Surg. (2020) 46:329–35. doi: 10.1007/s00068-019-01273-4
11. van der Vliet QMJ, Bhashyam AR, Hietbrink F, Houwert RM, Öner FC, Leenen LPH. Routine incorporation of longer-term patient-reported outcomes into a Dutch trauma registry. Qual Life Res. (2019) 28:2731–9. doi: 10.1007/s11136-019-02211-y
12. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Br Med J. (2007) 335:806–8. doi: 10.1136/bmj.39335.541782.AD
13. Association for the Advancement of Automotive Medicine. Abbreviated injury scale: 2015 revision. 6th edn. Chicago, IL. (2018). https://www.aaam.org/abbreviated-injury-scale-ais/
14. Abouleish AE, Leib ML, Cohen NH. ASA Provides examples to each ASA physical Status class. ASA Newsl. (2015) 79:38–49 doi: 10.1097/ALN.0000000000001541.
15. Boyd CR, Tolson MA, Copes WS. Evaluating trauma care: the TRISS method. Trauma score and the injury severity score. J Trauma. (1987) 27:370–8. doi: 10.1097/00005373-198704000-00005
16. Metsemakers WJ, Morgenstern M, McNally MA, Moriarty TF, McFadyen I, Scarborough M, et al. Fracture-related infection: a consensus on definition from an international expert group. Injury. (2018) 49:505–10. doi: 10.1016/j.injury.2017.08.040
17. Hulsmans MHJ, van Heijl M, Houwert RM, Hammacher ER, Meylaerts SAG, Verhofstad MHJ, et al. High irritation and removal rates after plate or nail fixation in patients with displaced midshaft clavicle fractures. Clin Orthop Relat Res. (2017) 475:532–9. doi: 10.1007/s11999-016-5113-8
18. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. (2012) 307:2526–33. doi: 10.1001/jama.2012.5669
19. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol group. Ann Med. (2001) 33:337–43. doi: 10.3109/07853890109002087
20. Rajala K, Lehto JT, Sutinen E, Kautiainen H, Myllärniemi M, Saarto T. mMRC dyspnoea scale indicates impaired quality of life and increased pain in patients with idiopathic pulmonary fibrosis. ERJ Open Res. (2017) 3:00084–2017. doi: 10.1183/23120541.00084-2017
21. Versteegh MM, Vermeulen KM, Evers MAAS, de Wit GA, Prenger R, Stolk EA. Dutch Tariff for the five-level version of EQ-5D. Value Health. (2016) 19:343–52. doi: 10.1016/j.jval.2016.01.003
22. Marasco SF, Davies AR, Cooper J, Varma D, Bennett V, Nevill R, et al. Prospective randomized controlled trial of operative rib fixation in traumatic flail chest. J Am Coll Surg. (2013) 216:924–32. doi: 10.1016/j.jamcollsurg.2012.12.024
23. Pieracci FM, Lin Y, Rodil M, Synder M, Herbert B, Tran DK, et al. A prospective, controlled clinical evaluation of surgical stabilization of severe rib fractures. JTrauma Acute Care Surg. Lippincott Williams and Wilkins (2016) 80(2):187–94. doi: 10.1097/TA.0000000000000925
24. Dehghan N, Nauth A, Schemitsch E, Vicente M, Jenkinson R, Kreder H, et al. Operative vs nonoperative treatment of acute unstable chest wall injuries. JAMA Surg. (2022) 157(11):983–90. doi: 10.1001/jamasurg.2022.4299
25. Liu T, Liu P, Chen J, Xie J, Yang F, Liao Y. A randomized controlled trial of surgical rib fixation in polytrauma patients with flail chest. J Surg Res. (2019) 242:223–30. doi: 10.1016/j.jss.2019.04.005
26. Walters ST, Craxford S, Russell R, Khan T, Nightingale J, Moran CG, et al. Surgical stabilization improves 30-day mortality in patients with traumatic flail chest: a comparative case series at a Major trauma center. J Orthop Trauma. (2019) 33:15–22. doi: 10.1097/BOT.0000000000001344
27. Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. The Journal of Trauma: Injury, Infection and Critical Care (J Trauma). (2002) 57:727–32. doi: 10.1097/00005373-20020400-00020.
28. Granetzny A, El-Aal MA, Emam ER, Shalaby A, Boseila A. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interact Cardiovasc Thorac Surg. (2005) 4:583–7. doi: 10.1510/icvts.2005.111807
29. Caragounis EC, Fagevik Olsén M, Pazooki D, Granhed H. Surgical treatment of multiple rib fractures and flail chest in trauma: a one-year follow-up study. World J Emerg Surg. (2016) 11:27. doi: 10.1186/s13017-016-0085-2
30. Szende A, Janssen B, Cabases J. In: Szende A, Janssen B, Cabases J, editors. Self-Reported population health: An international perspective based on EQ-5D. Dordrecht: Springer Netherlands (2014). doi: 10.1007/978-94-007-7596-1
31. Peek J, Beks RB, Hietbrink F, Heng M, de Jong MB, Beeres FJP, et al. Complications and outcome after rib fracture fixation: a systematic review. J Trauma Acute Care Surg. (2020) 89:411–8. doi: 10.1097/TA.0000000000002716
32. Beks RB, de Jong MB, Houwert RM, Sweet AAR, de Bruin IGJM, Govaert GAM, et al. Long-term follow-up after rib fixation for flail chest and multiple rib fractures. Eur J Trauma Emerg Surg. (2019) 45:645–54. doi: 10.1007/s00068-018-1009-5
33. Uchida K, Miyashita M, Kaga S, Noda T, Nishimura T, Yamamoto H, et al. Long-term outcomes of surgical rib fixation in patients with flail chest and multiple rib fractures. Trauma Surg Acute Care Open. (2020) 5:e000546. doi: 10.1136/tsaco-2020-000546
Keywords: rib fixation, flail chest, rib fracture, quality of life, thoracic trauma
Citation: Hoepelman RJ, Minervini F, Beeres FJP, van Wageningen B, IJpma FF, van Veelen NM, Lansink KWW, Hoogendoorn JM, van Baal MCP, Groenwold RHH and Houwert RM (2023) Quality of life and clinical outcomes of operatively treated patients with flail chest injuries: A multicentre prospective cohort study. Front. Surg. 10:1156489. doi: 10.3389/fsurg.2023.1156489
Received: 1 February 2023; Accepted: 27 February 2023;
Published: 15 March 2023.
Edited by:
Savvas Lampridis, Hammersmith Hospital, United KingdomReviewed by:
Claudia Bardoni, University of Milan, ItalyAndrea De Vico, Azienda Usl Teramo, Italy
Paolo Albino Ferrari, Ospedale Oncologico Armando Businco, Italy
Angela De Palma, University of Bari Medical School, Italy
© 2023 Hoepelman, Minervini, Beeres, van Wageningen, IJpma, van Veelen, Lansink, Hoogendoorn, van Baal, Groenwold and Houwert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabrizio Minervini ZmFicml6aW9taW5lcnZpbmlAaG90bWFpbC5jb20=
†These authors share first authorship
Specialty Section: This article was submitted to Thoracic Surgery, a section of the journal Frontiers in Surgery