 Josias Olutobi Ahamidé1*
Josias Olutobi Ahamidé1* Charles Jérôme Sossa1Yolande Sissinto2Edmond Yétongnon3,4Edgard-Marius Ouendo1
Charles Jérôme Sossa1Yolande Sissinto2Edmond Yétongnon3,4Edgard-Marius Ouendo1- 1Regional Institute of Public Health, University of Abomey-Calavi, Ouidah, Benin
- 2Faculty of Health Sciences, University of Abomey-Calavi, Cotonou, Benin
- 3Laboratory of Analysis of Social Dynamics and Development, Faculty of Agronomic Sciences, University of Abomey-Calavi, Abomey-Calavi, Benin
- 4Department of Educational Foundations and Practices, Research Group on Psychosocial Maladjustment in Children (GRIP-ULaval), Laval University, Quebec, Canada
Background: The persistent endemicity of bilharziasis (schistosomiasis) in the districts of Aguégués (Agué) and N’dali underscores the need for targeted intervention. This study assessed the impact of a health education programme grounded in the behaviour change communication (BCC) framework aimed at improving awareness of health risks associated with poor hygiene practices.
Objective: To implement and evaluate an integrated communication model designed to promote behaviour change and reduce the incidence of urinary bilharzia in two endemic communities.
Methods: A quasi-experimental study was conducted involving 106 households, divided equally into control (n=53) and experimental (n=53) groups, with school-aged children (8–14 years). The intervention, delivered from January to June 2023, applied an integrated communication model based on Ajzen’s theory of planned behaviour. Community health relays conducted biweekly awareness sessions over 6 months to educate households. Data were collected using KoboCollect and analysed through logistic regression and multivariate analysis in STATA. Urine samples were collected for laboratory analysis using Plouvier’s filtration sensitivity test. Descriptive statistics and confidence intervals were calculated using Student’s t-test in SPSS. Relative risk was assessed based on an estimation of incidence among the separate groups.
Results: Overall, the incidence within the exposed group was estimated as 11.32%, compared to 24.53% within the non-exposed group. Reinfection rates were significantly associated with sex across study groups. Compared to girls, boys had higher reinfection rates in both the exposed group (boys: 7.54%; girls: 3.77%) and non-exposed group (boys: 18.87%; girls: 5.66%). The qualitative variables “duration of communication sessions,” “frequency of communication sessions,” “topics of communication sessions,” “past behaviour of the household,” and “household intention for behaviour change” were statistically significant (p < 0.01) and had an effect on reducing the incidence of bilharzia in the experimental municipalities of Aguégués and N’Dali. Furthermore, the intention of the target population of N’dali and Aguégués to adopt the expected behaviour was studied using a prediction test, with an estimated relative risk of 0.46 and a confidence interval (CI) [0.48-0.52].
Conclusion: The study proved effective in promoting health-related behaviour change and reducing bilharzia incidence. The model is recommended for broader implementation in bilharzia-endemic areas.
1 Introduction
Bilharzia, a neglected tropical disease (NTD), is a major public health concern given its endemic nature in many parts of Benin; similar concerns regarding NTDs exist in many other West African countries. A mapping of the national master plan for neglected tropical diseases carried out over the period 2016–2020 highlighted the many municipalities affected by the disease, with rates ranging from 0.40% to 91% depending on the area, including Sô Ava, Aguégués, and N’dali (1). Similarly, sub-Saharan African countries such as Nigeria, Benin, Togo, Ghana, Côte d’Ivoire, Senegal, Mali, Mauritania and others, in view of the spread and persistence of outbreaks of the disease, have set up control strategies with the help of institutional authorities such as the World Health Organisation (WHO), the Global Alliance for Vaccines and Immunization (GAVI), Family Health International (FHI 360), and the Schistosomiasis Consortium for Operational Research and Evaluation (SCORE). However, these strategies focus mainly on chemotherapy through mass treatments, with the goal of reducing the ever-growing prevalence rates (2).
Epidemiological data clearly show that schistosomiasis, despite the extensive control strategies implemented, continues to spread in several countries around the world and, due to its virulence, infects humans. Schistosoma mansoni and Schistosoma haematobium are present in Africa and the Middle East, while S. mansoni is present in America. S. japonicum is found in Asia, mainly in the Philippines and China. S. mekongi and S. guineensis are transmitted primarily in East and Central Africa (3). Data from 24 studies conducted in Africa have shown combined random risk ratios of 2.4 and 2.6 for urinary and intestinal schistosomiasis, respectively, among people living near dam reservoirs. This implies that the development and management of water resources is an important factor, the lack of care for which dramatically increases the prevalence of schistosomiasis in endemic countries. The findings of studies conducted by SCORE in five countries, including Zanzibar, have shown that the elimination of schistosomiasis will require the combined and integrated use of several actions, including the application of several methods such as chemotherapy, but in particular snail control, health education strategies to change behaviour, access to safe drinking water, and the construction of sanitation infrastructure to promote good hygiene practices. In the longer term, the development of a prophylactic vaccine to prevent transmission may also be necessary (4). However, the living conditions of populations affected by the disease—poverty, poor hygiene coupled with unsanitary living conditions, the persistence and emergence of endemic bilharziasis from local sources, the tendency of populations to ignore the instructions of health authorities and hygiene standards, the resistance of communities to adopt good hygiene behaviours to reduce the rate of contamination, and finally the resurgence of new cases and outbreaks of contamination—are all factors that hinder the regression of bilharziasis. Complications from bilharziasis include hydroceles, urethritis, prostatitis, spermatocystitis, vaginal lesions, sterility, bladder cancer and schistosomiasis–HIV co-infection, hepatic periportal fibrosis, and blood eosinophilia during the invasion phase. An epidemiological study carried out from May 5–22, 2022, on the sociodemographic and economic factors associated with bilharziasis, which has prevalences of 34.53%, 11.88%, and 13.53% in the communes of Aguégués, Sô Ava, and N’dali in Benin, respectively (5), and on the knowledge, attitudes, and practices of adults in their relationship with and use of water, provided evidence of the persistence and/or emergence of certain endemic outbreaks representing major public health concerns (6).
Considering the social and health situation observed in the communities affected by NTDs on the one hand, and referring to the conclusions of the survey on knowledge, attitudes, and practices (KAP) carried out among the populations of N’dali and Aguégués who were receptive to behaviour change, we felt it was necessary to carry out a health communication intervention. Among other things, this would enable us to increase public knowledge and awareness of this health problem, influence behaviours and attitudes, and demonstrate practices for the benefit of behaviour change in public health outcomes. In addition, should such an intervention be successful, the implementation of such a health policy through a thematically structured plan centred on this phenomenon may improve outcomes (7, 8). Health communication, as a professional field, has contributed to a better understanding of individual health, making a relevant diagnosis for effective therapy, and informing and influencing individual and community decisions (9, 10). Thus, the problem of essential community action within these populations prompted the implementation of a behaviour change intervention in the two communes with the highest prevalence (Aguégués and N’dali), which seems to be an effective solution for raising awareness of good hygiene practices. Godin’s (2002) integrated model is used to understand how the combined use of several theories, including the theory of planned behaviour (TPB) previously developed by Ajzen and Fishbein to complement their theory of reasoned action, can facilitate behaviour change. This model is represented by the perception of behavioural control (PBC) and persuasive communication theory, which postulates that human behaviour, to be effective, must first be decided upon and then planned (11–13). Behavioural decision-making involves the intervention of three types of factors: judgements about the appropriateness of the behaviour and its consequences (behavioural attitudes); considerations about the influence and opinion of others on the behaviour (social norms); and beliefs about the subject’s ability to perform the behaviour successfully (14–17). The communication model implemented in this research focuses on raising community awareness to promote good hygiene practices and habits and contribute to reducing the incidence of urinary bilharziasis.
2 Objectives
The strategic axis of this study involved a general objective, which is broken down into two specific objectives.
2.1 General objective
The general objective was to measure the effects of implementing an integrated behaviour change communication approach in the communities of Aguégués and N’dali in Benin.
2.2 Specific objectives
i. Carry out an intervention study for behaviour change over a period of 6 months in the districts of Aguégués and N’dali;
ii. Raise awareness centred on an integrated model of communication to promote good hygiene practices among populations;
iii. Determine the incidence of bilharzia in the targeted localities.
3 Materials and study method
3.1 Study design
This is a cohort study with analytical and descriptive purposes based on two components: observation and use of an integrated communication model for behaviour change. The study took place from January to June 2023.
3.2 Characteristics of the study population
This study targeted two groups of individuals from the districts of Aguégués and N’dali who participated in an epidemiological study on schistosomes from May 5–19, 2022 (5).
3.2.1 Description of the criteria for the control and experimental groups
The characteristics of the study population are described as follows in line with the criteria for the control and experimental groups outlined in Table 1.
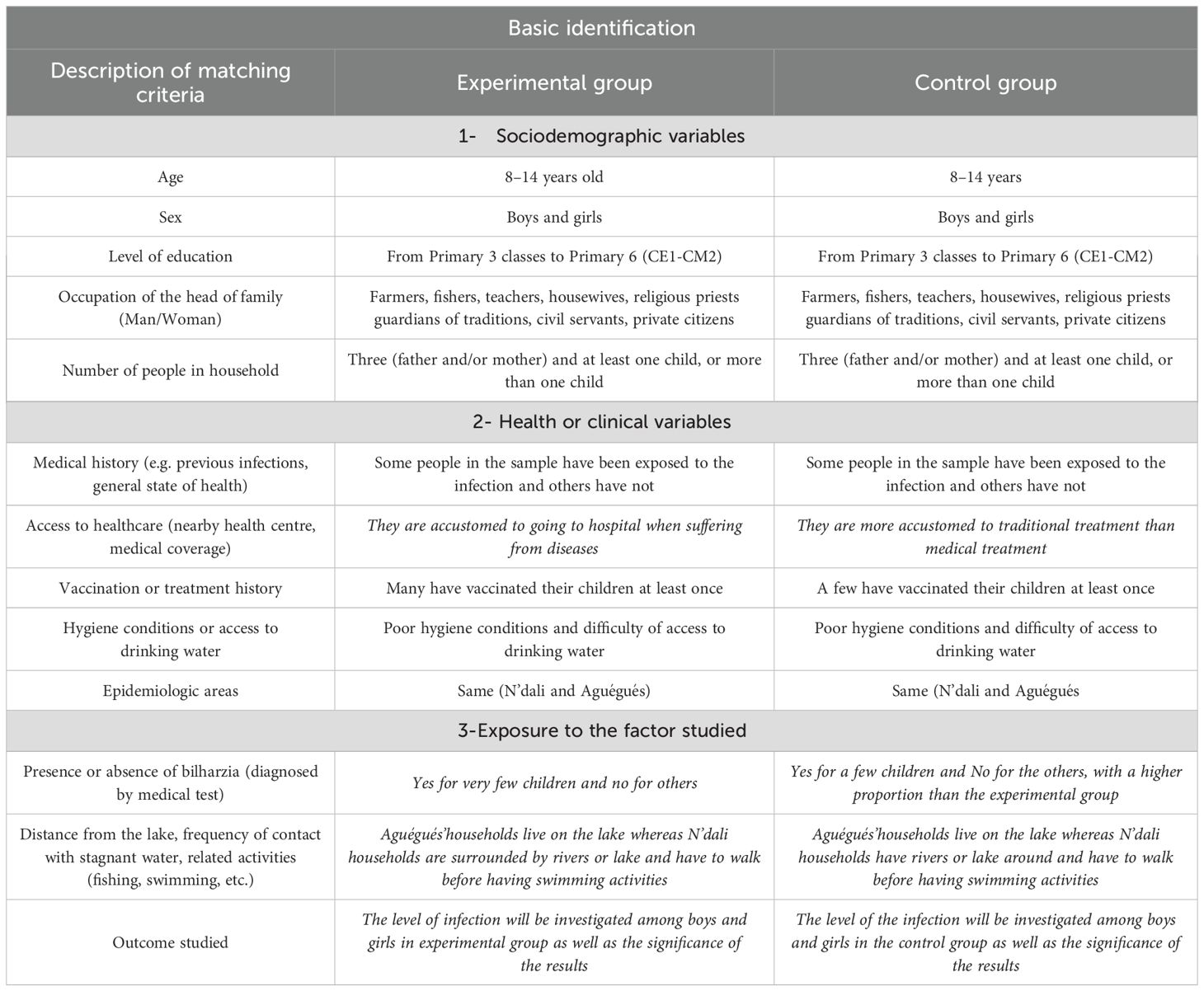
Table 1. Summary table showing description of the criteria for the control and experimental groups.
3.2.2 CONSORT flow diagram for the control and experimental groups
The details about the following quasi-experimental design is illustrated by a CONSORT flow Diagram in Figure 1 showing how control and experimental groups are matched.
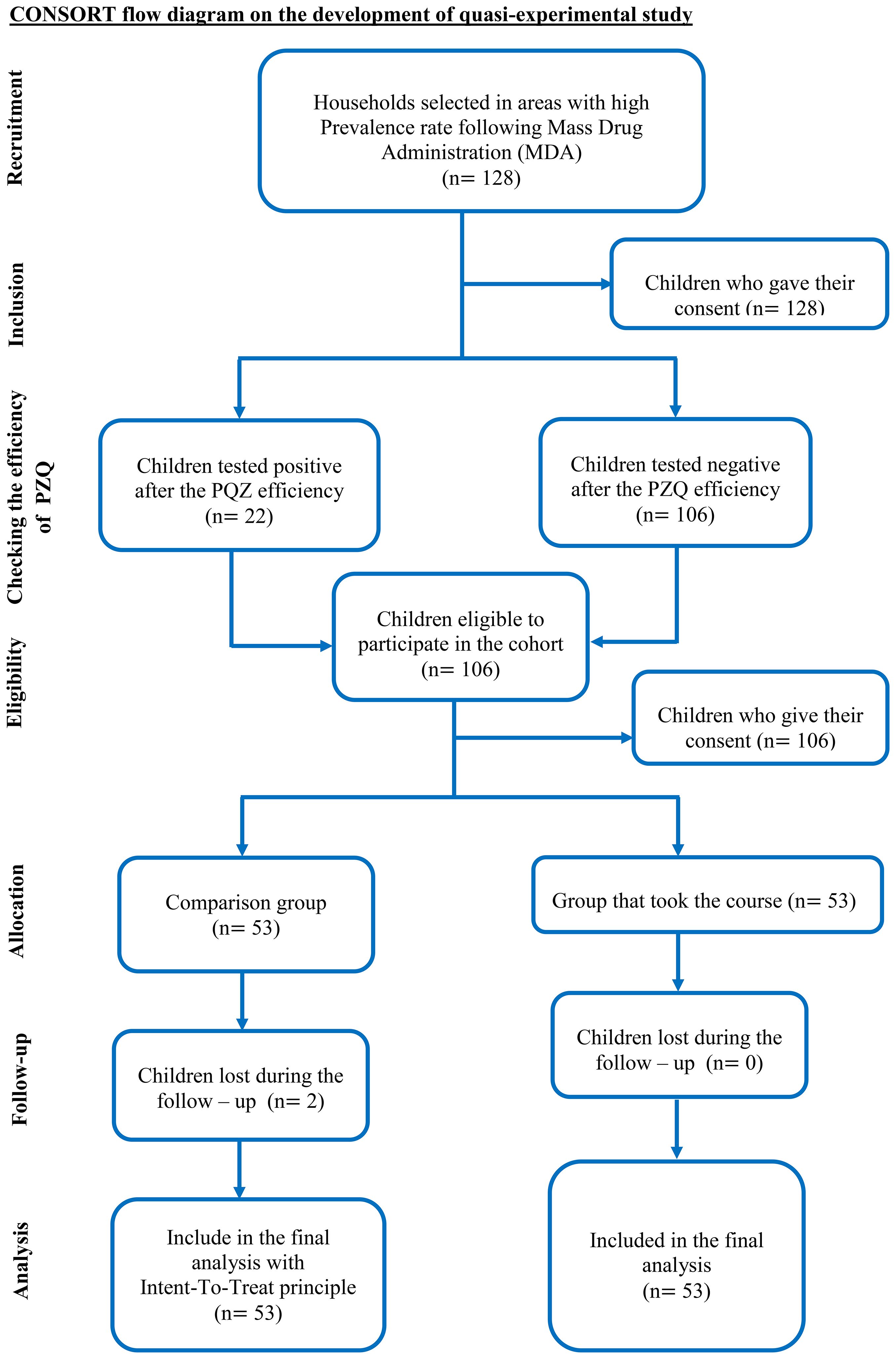
Figure 1. CONSORT flow diagram on the development of the quasi-experimental study.
3.3 Inclusion criteria
The study included households with children aged 8–14 years, from Primary 3 classes to Primary 6, who had participated in the study of the prevalence of bilharzia carried out in May 2022 and who had received preventive and/or curative treatment with praziquantel. The control and experimental sites were located sufficiently far apart from each other.
3.3.1 Non-inclusion criteria
Households that did not meet the above criteria or did not provide informed consent were excluded from the study.
3.3.2 Exclusion criteria
The exclusion criteria for the study were:
a. households that did not live in the districts during the study period;
b. households whose children did not live in the study area and had not participated in previous prevalence studies or in preventive and/or curative treatment with praziquantel; and
c. households lost to follow-up during the cohort.
3.4 Principles, process, and sampling technique
The districts of N’dali, located in northern Benin and comprising 11,492 farming households, and Aguégués, located in southern Benin, were chosen following an epidemiological study on the sociodemographic and economic factors associated with bilharzia. They have a poverty index of 78.3, with populations engaged in agriculture, fishing and hunting (18). Mass drug administration (MDA) was carried out. Sampling was globally probabilistic with multi-stage cluster random sampling to select eligible households for the cohort composed of heads of household from the two communities. A global sample of 128 schoolchildren from 128 randomly selected households in two endemic communities, following the efficiency assessment three months after one week of mass treatment with praziquantel. At the first stage: random sampling of the departments of Ouémé/Borgou; at the second stage: random sampling of the municipalities of N’dali and Aguégués; the third stage selected arrondissements through random sampling; at the fourth stage: primary public and private schools were selected with random sampling; and the fifth stage was a random sampling of school-aged children in the municipalities of N’dali and Aguégués. The Plouvier filtration test revealed 22 children who were positive and 106 who tested negative. This second group of children were eligible for a communication intervention. The study had an equal distribution of 53 children in each group: the experimental group and the control group, chosen by probabilistic sampling. Students’ parents were contacted by the president of the parents’ association with the collaboration of school directors who participated in the prevalence study. Eight schools were potentially eligible for the cohort, including two pairs of experimental groups (exposed) represented by the sites of EPP Bembè 2 and EPP Houinta/A in the district of Agué; the sites of EPP Bori and EPP Pouraparé in the district of N’dali. Two pairs of control groups (unexposed) were identified with the EPP Kindji and EPP Étoiles des Marges in the district of Agué, as well as the sites of the EPP Bahounkpo and EPP “Mon Avenir” in the district of N’dali. The study population belongs to the same cohort and has the same characteristics: environmental factors linked to endemicity, the epidemiological nature (demographic, cultural factors and occupational exposures) (5), and the same age range of children (8–14 years) from primary school in a classroom situation. Only disease-free individuals were eligible for the cohort for a period of six (6) months. To avoid interconnecting biases, each pair of districts chosen was separated from each other by 25–50 km, or approximately 1 hour–1 hour 30 minutes. The “intent-to-treat principle” (19–21) was used to increase the comparability of different groups of children, increase the power of the statistical test and minimise attrition bias. At the end of the cohort, the incidences were calculated for each group on the basis of new cases in the two groups. The relative risk (RR) was also calculated to evaluate the protective power of the exposure factor.
3.5 Procedures and practical arrangements
The organisational chart includes (1) a general supervisor; (2) two external supervisors; (3) four general coordinators of the activity, represented by post chiefs and majors; (4) eight zone coordinators, represented by school principals; and (5) focal points, which are the four community relays, the main architects of communication. The communication sessions took place in focus groups with parents and children eligible for the host cohort who received visits from facilitators. The duration of communication was 1 hour 30 minutes. They were punctuated by a teaching section and a debate section (questions and answers). Each household in the cohort was entitled to a teaching session once a fortnight.
An evaluation of the system was carried out in the middle (end of the first trimester) in two parts. The first part was the subject of a working session with the organisational chart of the intervention to study the inadequacies of the system and the strengths and weaknesses to increase its performance to achieve the set objectives. The second part involved a behavioural change prediction survey carried out among beneficiaries.
3.6 Study variables
The variables defined in the study are dependent and independent.
Dependent variable: incidence of schistosomiasis (only new cases of contamination among the individuals previously selected and who tested negative for bilharziasis)
Independent variables: cohort intervention areas
These factors are related to the analysis of parameters within the experimental group that underwent the intervention. For this purpose, seven variables, broken down into several sections, were considered: (1) duration of communication sessions; (2) frequency of communication sessions; (3) topics of communication sessions; (4) household attitudes and practices; (5) household social norms; (6) past behaviour of the household; and (7) the intention of the household to change behaviour.
3.7 Collection tools (qualitative and quantitative data)
- Qualitative data with interview guide.
The GPS-assisted Kobocollect application, v 2021.2.4, was used as a free Android data collection tool to collect qualitative data using a digitised interview guide through focus groups and interviews with the heads of household. The strategy for implementing integrated communication combined theories, including those of persuasive communication (PC) with the use of image boxes, the health belief model (HBM), and Godin’s integrative model involving Ajzen’s theory of planned behaviour (TPB) approach based on social constructs. The image boxes were designed to carry messages in six (6) themes focused on bilharziasis. The first defined bilharziasis and discussed its causes and mode of transmission. The second discussed symptoms and manifestations. The third discussed consequences and complications. The fourth addressed the socioeconomic impact of bilharzia on children’s physical development. The fifth theme discussed preventive measures used against bilharzia in relationships and uses with water, and the sixth discussed what to do in the event of suspicion or diagnosis of schistosomiasis in a subject.
- Quantitative data: urine collection for bilharzia screening.
At the end of the intervention, quantitative data represented by urine samples were collected at both the experimental and control sites in line with the guidelines of the Plouvier filtration technique (19–24). Data were digitised and collected using a questionnaire to obtain sociodemographic information (age, sex, level of education, socio-professional activity). Children were given water and asked to exercise (fast walking, running, jumping) to move the eggs to the bladder (18, 22, 25). A 10 ml sample of urine was collected in a sterile bottle from all selected pupils. The urine was then examined in the laboratory with test strips that showed the presence of a microscopic haematoma characteristic of genital schistosomiasis. The sample was then passed through a 13 mm diameter millipore filter (20 µm, Sefar AG, Switzerland), which retained any schistosome eggs, which were then counted under a binocular microscope. The test and reading were performed extemporaneously (22, 26–28). The detection of S. haematobium eggs is generally performed by urine microscopy. The eggs are released in urine, and after concentration of the sample by sedimentation, centrifugation, or filtration, eggs can be detected under the microscope. Urine test strips for detection of blood (haematuria) in the urine can also be used as an indicator of potential infection in patients living in endemic areas (29, 30) Gray et al., 2011).
3.8 Data analysis process
Qualitative data were analysed by logistic regression with multivariate analysis using STATA version 15 software for Likert scale data, and quantitative data were analysed with Student’s t-test for descriptive analysis by SPSS version 20 and logistic regression with multivariate analysis by STATA version 15 software for relative risk (RR).
3.9 Ethical considerations
The study was approved by Benin’s National Committee for Ethics and Health Research (CNERS) under ethical opinion No. 22 of June 21, 2021, and was registered under No. 91/MS/DC/SGM/CNERS/SA. In addition, free and informed consent was signed by all schoolchildren and parents of schoolchildren, and the expected objectives of the study were explained to all participants, as well as the benefits and risks.
We would like to mention that the research was strictly conducted according to the Helsinki research protocols and standards, under which we received an ethical opinion from our national ethics committee. We were also instructed by the board of the ethics committee to develop consent forms during our survey in line with the guidelines of the Helsinki considerations and standards. Our national ethics board usually refers research protocols to the updated version of the 2013 Declaration published at the 75th meeting of Helsinki in October 2024, which focuses on informed consent and requires researchers to provide detailed information about clinical trials, including their purpose, risks, and benefits. Participants must be informed of their rights, including the right to withdraw at any time.
4 Results
Table 2 presents descriptive statistics for the overall sample of households recruited for the cohort study. The sample consisted of 128 children (enumeration areas (EAs) selected from eight schools, including four from the commune of Aguégués and four from the commune of N’dali, each from one household, for a total of 128 households.
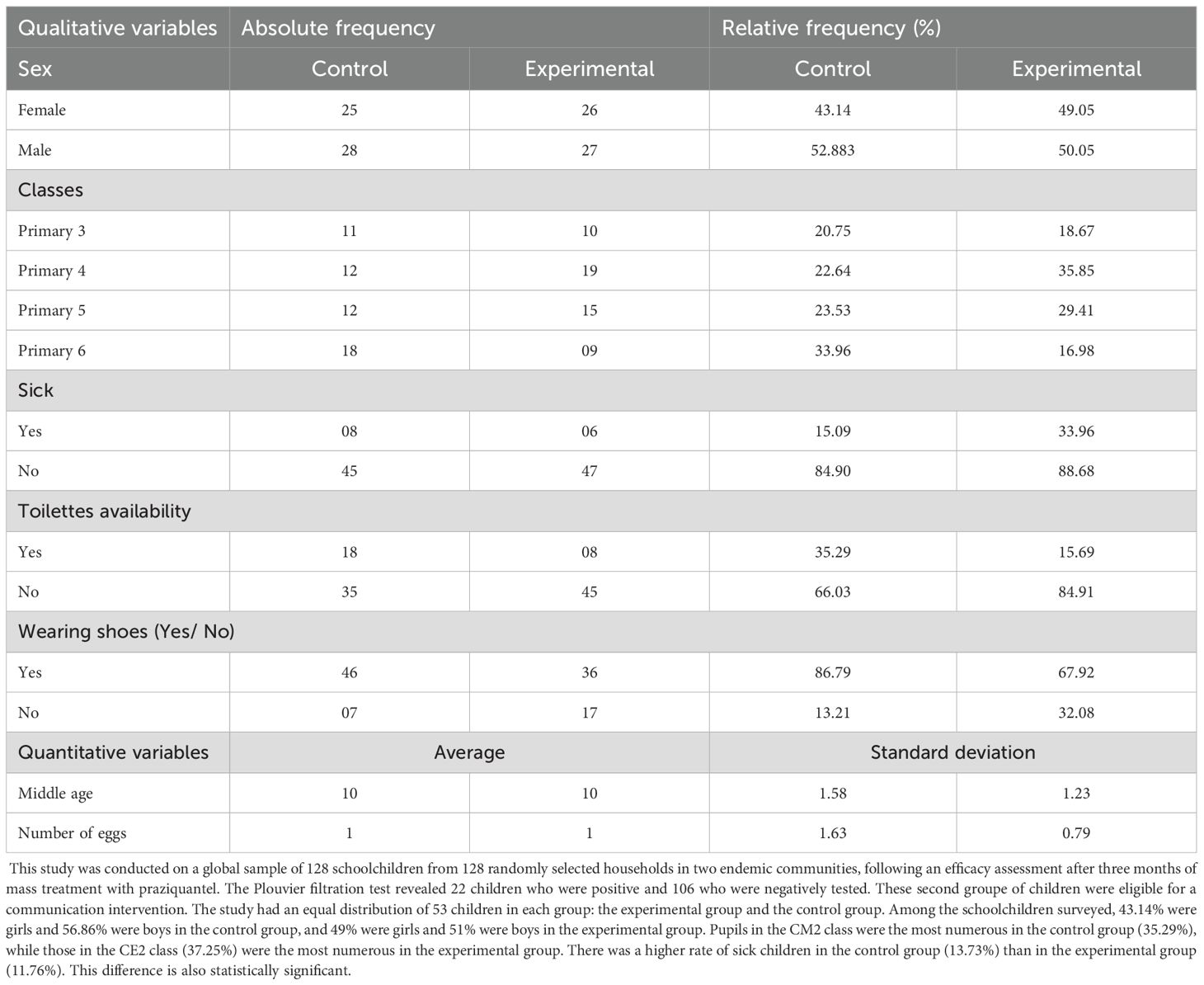
Table 2. Descriptive statistics.
In terms of frequency, the children surveyed were girls (47.17%) and boys (52.883%) at the control level. The experimental students included girls (49.05%) and boys (50.05%). Schoolchildren belonging to the CM2 class were the most dominant among the controls (33.96%), and those belonging to the CE2 class (35.8%) were the most dominant among the experimental students. The rate of infection was higher in the control group (15.09%) than in the experimental group (11.32%).
The controls included 43.14% girls and 52.88% boys, with an average parasitaemia rate of 1.63. The experimental group was represented by girls and boys in proportions of 49.05% and 50.05%, respectively, with an average parasitaemia rate of 0.79. The mean ages of the control and experimental groups were 1.58 and 1.23, respectively. The average number of sick individuals was 15.09 and 33.95 for the control and experimental groups, respectively.
Table 3 presents epidemiological data showing 22 children who tested positive for schistosomiasis after mass drug treatment (MDT). A total of 106 tested negative and were admitted to the cohort. Two groups were then formed, with 53 households in the exposed group and 53 in the non-exposed group. The proportion of negative cases was greater in the experimental (30.18%) and control (29.24%) groups in N’dali than in the experimental (19.81%) and control (29.24%) groups in Aguégués.
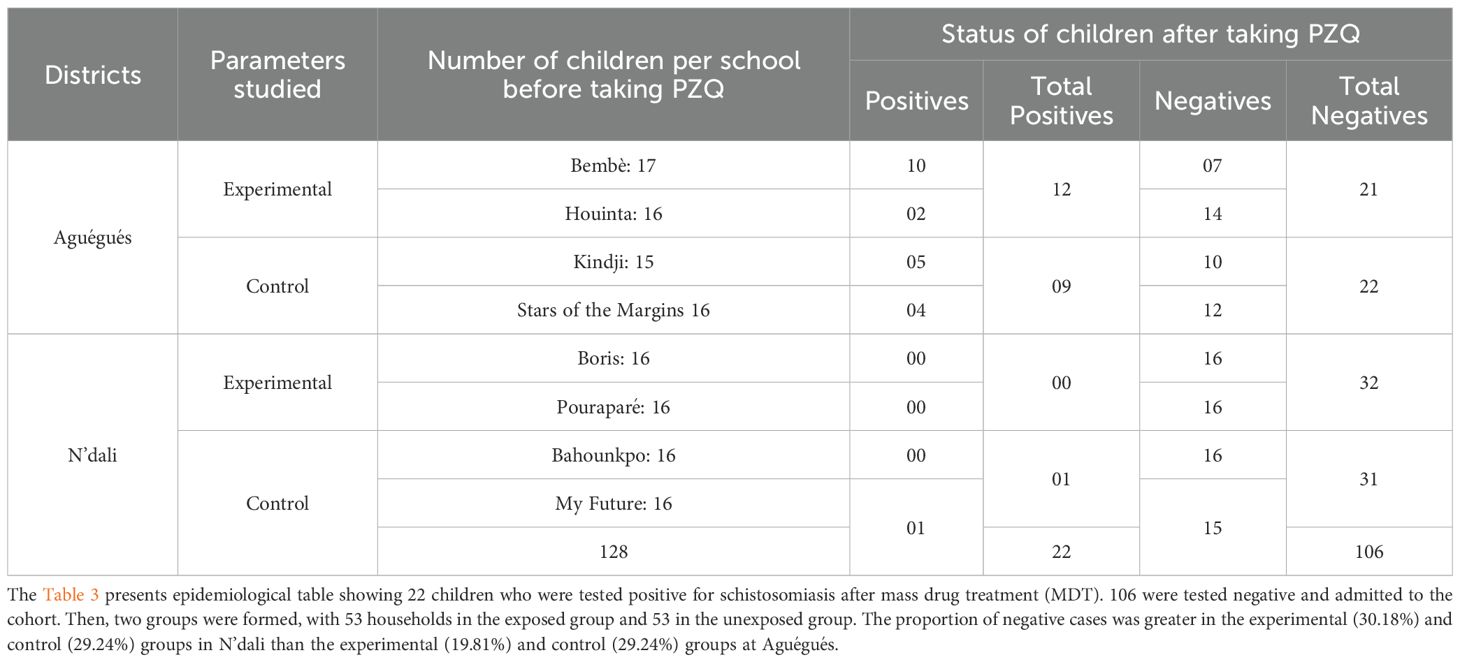
Table 3. Epidemiological profile “before intervention”.
The estimated model is globally significant at the 1% threshold (p = 0.000), as shown in the table below.
Table 4 presents a summary of the TPB-based behaviour change intention prediction survey. Five variables—TCS (p<0.01), FCS (p<0.01), DCS (p<0.01), HIBC (p<0.01), and HPB (p<0.01)—highlight the degree of predictability of household intention to change behaviour, in contrast to the variables HAP (p>0.01) and NSM (p>0.01). We also note the possibility of incidence variability, with a proportion of 59.62% at the end of the intervention.
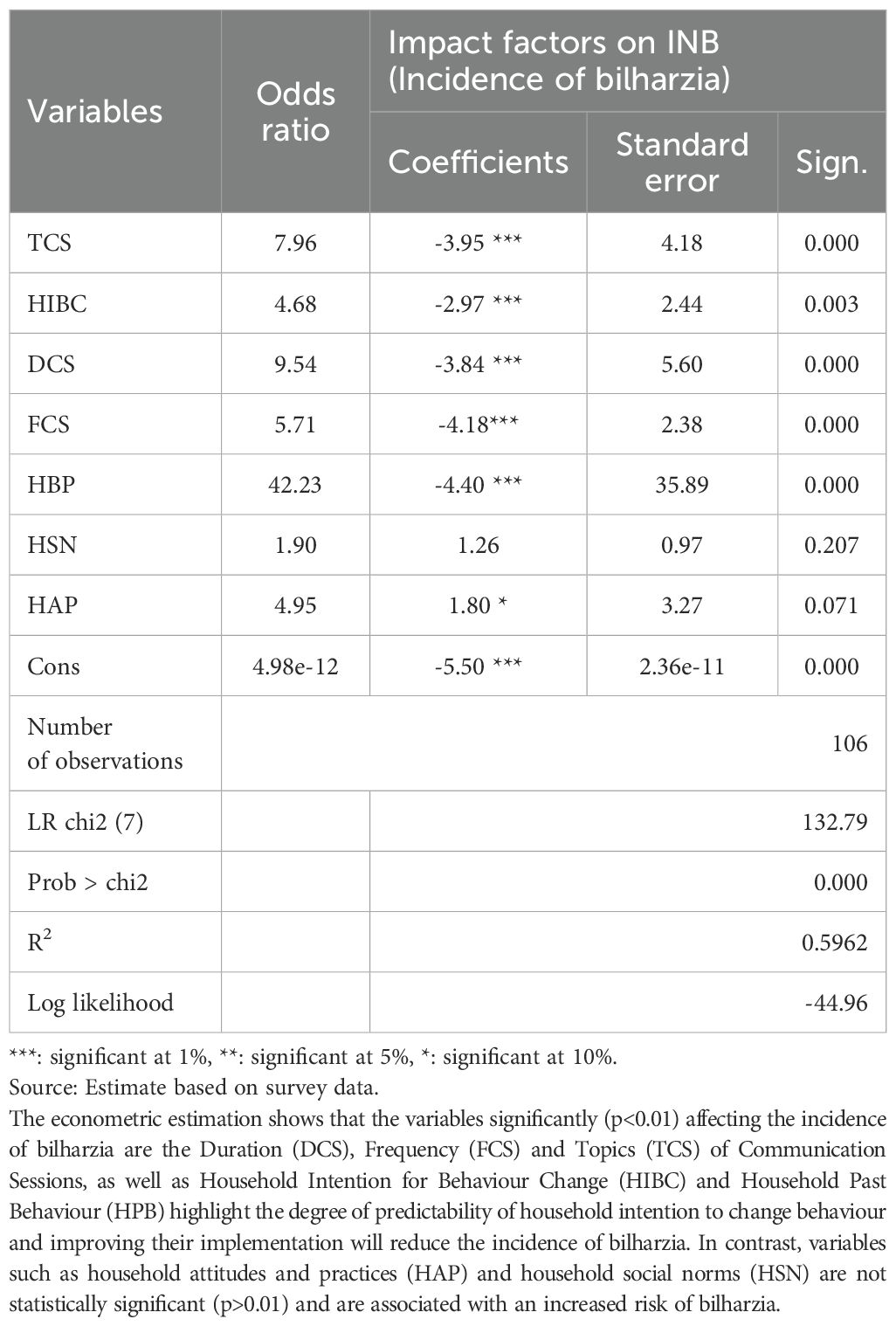
Table 4. Logit model estimation results for the AJZEN approach showing the analysis of the relationship between the incidence of bilharzia and specific determining factors.
Table 5 presents the contingency table showing that incidences were higher in the non-exposed (Nexp) group than in the exposed (Exp) group.
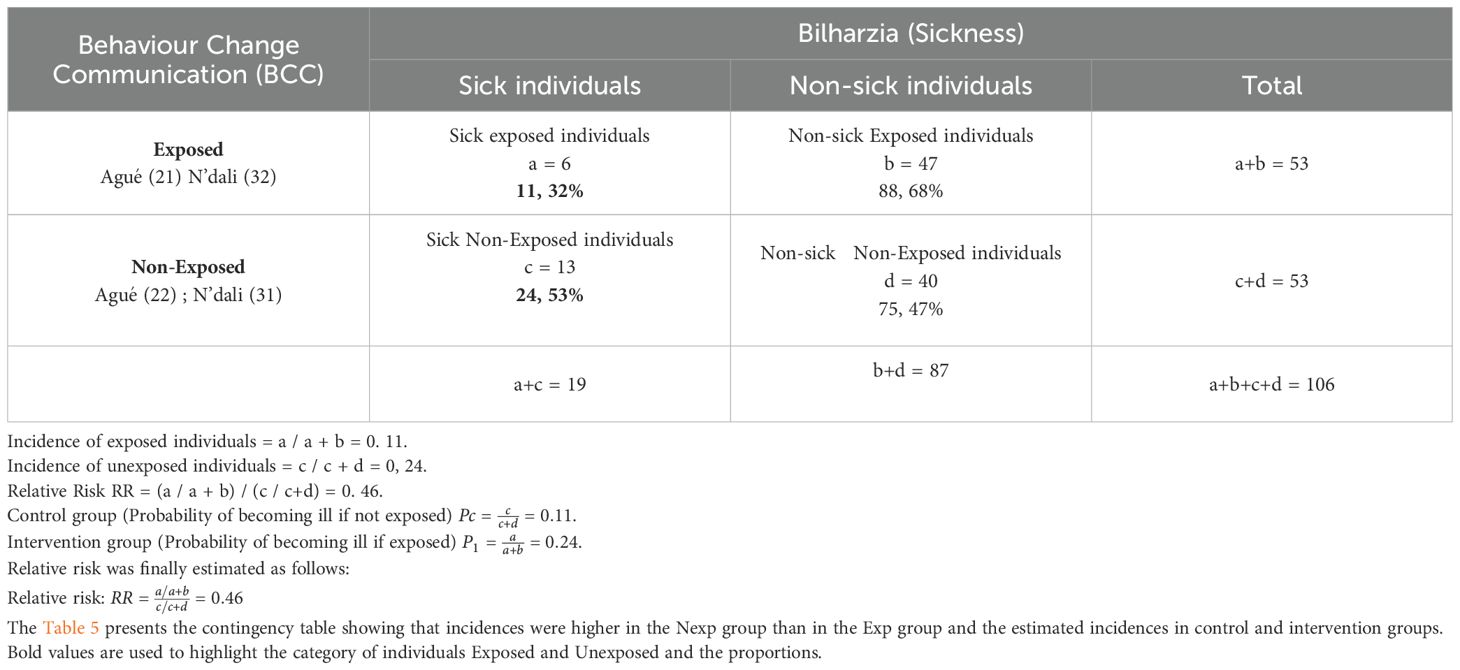
Table 5. Contingency table.
Table 6 shows households by study group of exposed and non-exposed individuals, broken down by gender. Bilharzia was observed in both exposed and non-exposed individuals, but the incidence was higher in boys than in girls. Moreover, the incidence was higher in the exposed group than in the unexposed group.
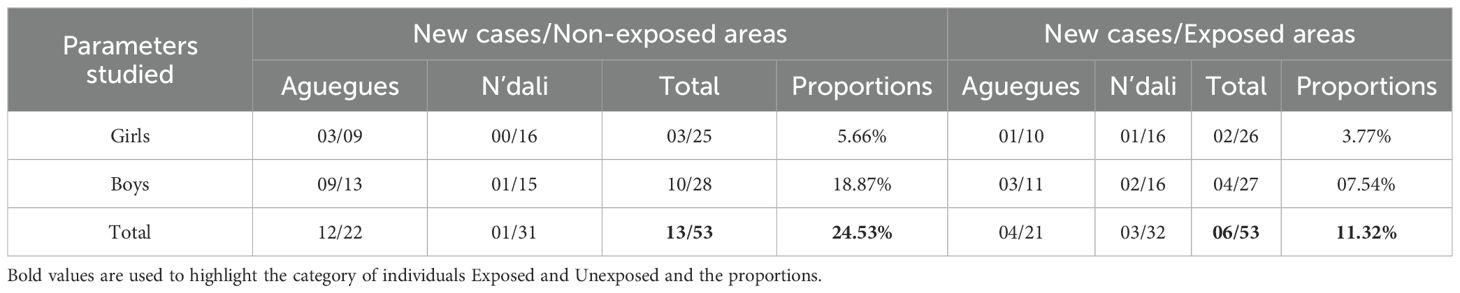
Table 6. Statistical distribution and proportions of new cases by groups and sex.
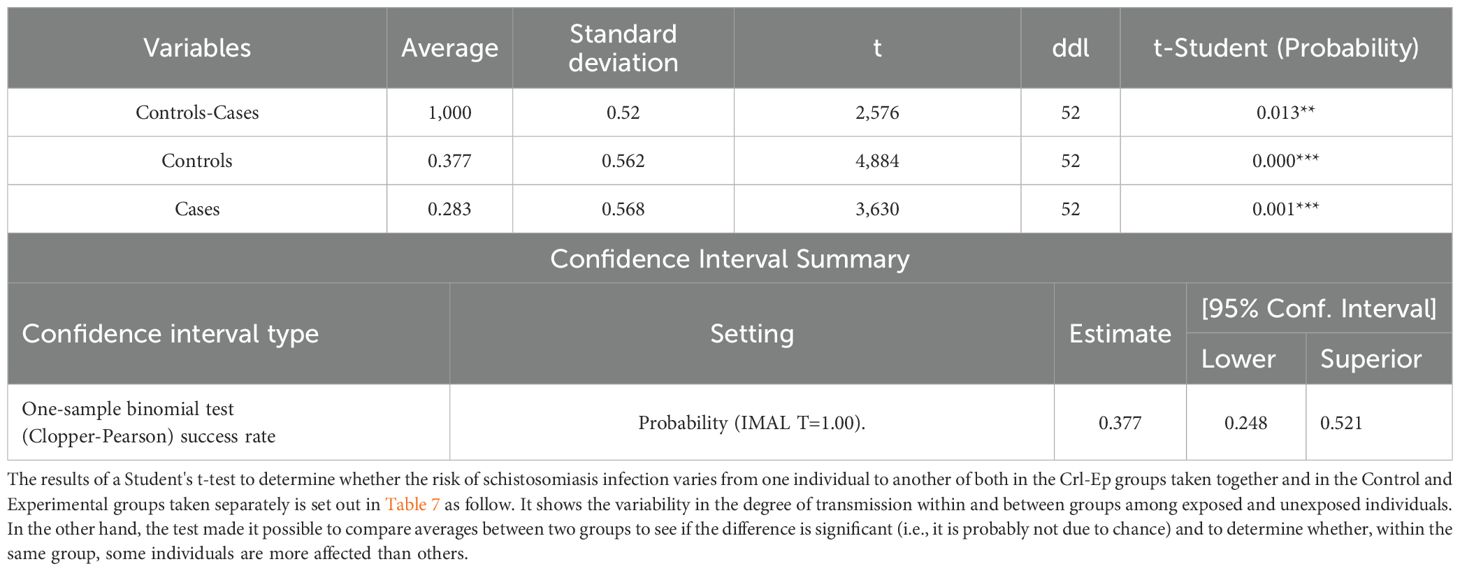
Table 7. Student's t-test for intergroup and intragroup contamination and Confidence Interval.

Table 8. Student's t-test showing the overall significance of prevalence in the study group.
Finally, the test made it possible to determine the confidence interval that places the estimated value to outline the Relative Risk.
This table shows the results of a Student’s t-test, which was performed to determine whether the risk of schistosomiasis infection varies from one individual to another. This was examined in two different ways: first, the control and experimental groups were considered together; then, the control and experimental groups were considered separately. It illustrates the variability of infection within and between groups.
4.1 Outcomes of interviews carried out with some households in the targeted population
The sections devoted to communication provided an opportunity for interesting exchanges, debates, and the sharing of experiences and knowledge between participants and trainers. This was the main point we can take from the comments made by some of the participants below. The communication sections were occasions for discussions, debates, and the sharing of experiences and knowledge between participants and instructors.
Before the sections started, many people were uninformed about the causes of the disease, as illustrated below. A cultural group designated as Fulani from the village of Ouenou in N’dali classified bilharzia in three categories in these terms:
“There are several Ketou. I know “Ketou Suwan” (Red urine in N’dali town’s local name of bilharzia), Ketou Kpika (urine with a white liquid in N’dali town’s local name of bilharzia). If you like women too much, you are often contaminated by the white colour” (P4, 28 years old, Ouénou in N’dali) (5)
A traditional healer speaks of it in these themes:
“If someone’s wife has this if you’ve sexual intercourse with her you can grab this and that’s what comes out a white liquid” (Crépin, 54, Sô-Ava) (5)
Family and health professional perceptions, such as interviews carried out with caregivers.
“ In my opinion, schistosomiasis, above all, is an infectious disease to tell you more precisely a parasitic disease that is caught if I can say so and transmitted during swimming, generally in fresh water” (Sémiou, 30 years old, N’dali) (5)
From the words of Semiou residing in N’dali, we understand that schistosomiasis is of parasitic origin and is transmitted through the skin in contact with water. Christian’s point of view contrasts with the assertion of the caregiver Semiou and testifies to the transmission of schistosomiasis by different sources of contamination in the Aguégués region:
“Adovè (Aguégués town’s local name of bilharzia), people say that this disease which occurs when a person urinates in the water of the river, there is a microbe which penetrates the genital apparatus of the man or the woman and gives this disease; people advise us not to urinate in the river water” (Christian, 30 years old, mechanic by profession in Aguégués) (5)
At the end of the sessions, the following comment illustrates the satisfaction of some participants:
“We have really appreciated the courses during the sections. the instructors help us to understand more about bilharzia. We now know that bilharzia is transmitted when swimming in dirty rivers, streams/ponds or in slakes that contain larvae of bilharzia. We are looking forwards to having other interested awareness sections to ask more questions. We are also asking favour to health authorities and the government drinking water and toilets. We really enjoyed the lessons given during the sessions. The lecturers helped us to better understand bilharzia. We now know that bilharzia is transmitted when people swim in dirty rivers and streams/ponds containing bilharzia larvae. We are looking forward to further awareness-raising sessions so that we can ask more questions. We are also asking the health authorities and the government to provide us with clean water and toilets.” (John the saver Local Authority and traditional Healer, 50 years old. in Aguégués)
An interview after the health intervention with a community relay who took part in awareness-raising activities and communication sessions was recorded as follows:
Euhhh…….Dear Doctor, the job was very exciting. On my own behalf and on behalf of my colleagues, I would like to thank you so much for this wonderful programme centred on bilharzia, its causes and consequences for human beings. I am extremely grateful to you. My concern now is that. When are we going to meet again? What is the plan for the follow-up with the local authorities? We need to make sure that we can continue to help our parents and children to fight against that killer disease and keep the incidence of bilharzia levels low. (El Hadj Wabi Inoussa, 45 years old. Trader and community relays in Aguégués)
5 Discussion
This study aimed to measure the impact of a communication model in the Aguégués and N’dali communities after a 6-month period of implementation to reduce the incidence of urinary bilharziasis. We found that the proportion of sick children was higher in the control group (15.09) compared to the experimental group (11.32), which was statistically significant (p value to be inserted). The rate of infection was significantly higher among the controls (15.09) than among the experimental participants (11.32) (Table 2). These results indicate that the incidence of bilharzia infection in households by study group (control and experimental) and by class was highly significant at the 5% threshold (p=0.03<0.05).A cross-analysis shows a greater proportion of negative cases in the experimental (30.18%) and control (29.24%) groups in N’dali than in the experimental (19.81%) and control (20.75%) groups in Agué, which suggests that the PZQ administered was more effective for the children of N’dali, who were less likely to be infected than those of Agué (Table 3).
The behavioural change intention prediction survey based on TPB carried out following the Ajzen approach (13, 14, 31) revealed that five explanatory variables—TCS (p<0.01), FCS (p<0.01), DCS (p<0.01), HIBC (p<0.01), and HBP (p<0.01)—were statistically significant, thus highlighting the degree of predictivity of the intention of households to change behaviour. In contrast, the variables HSN (p>0.01) and HAP (p>0.01), although presenting as factors impacting the incidence of bilharzia, were not statistically significant (Table 4). Furthermore, these results indicate the possibility of variability in incidence, with a proportion of 59.62% at the end of the intervention (Table 4).
These results of predictivity of intention generally converge with the trends obtained from surveys by Koffi Philippe Houmè at the University of Lomé, which revealed, through the attitudes of students, a good prediction of intention. Despite the absence of a link between the variables “social norms” and “intention,” social norms and perception of control explained 47% of the variance in the intention of their perseverance to remain in studies throughout the year in the natural sciences. This confirms Ajzen’s hypothesis, which postulates that a person’s attitude towards adopting a behaviour, their perception of social norms, and their control over the behaviour determine their intention to adopt the said behaviour, and that the intention in turn facilitates the realisation of the intended action (19–21).
Amadou Sow, during an evaluation of the determinants of intention in the Dakar region of Senegal (22), also highlighted 54% of the variance in the intention of boyfriends of sex workers (SWs) to use condoms as a means of preventing STIs and HIV/AIDS during the next sexual relationship with a SW’s friend. The data from the prediction survey carried out in the first quarter on the HSN, HIBC, HBP, and HAP essential variables of our study, although not all statistically significant, were useful to study the respondents’ ability to accept the message for transmission and the probability of achieving the expected results during the communication intervention period. This intervention was intended to work on personal convictions to contribute to behavioural change in relation to bathing activities.
The preparedness of our target group to change their behaviour, in the light of the conclusions of the prediction survey, was in line with the outcomes obtained by assimilating the concepts learned during the awareness sessions: a reduction in the incidence of urinary bilharzia in the exposed group as opposed to the unexposed group.
A distribution by group and sex of our sample showed an overall rate of 24.52% in the Nexp group compared with 13.20% in the Exp group (Table 5). This suggests that the topics taught during the communication sessions were understood, with beneficiaries demonstrating positive changes in terms of good hygienic behaviour in general and, in particular, in relation to their interactions with and use of water.
Although the literature review reveals that almost no studies have implemented an intervention protocol following the protocol of our research (1 – prevalence study; 2 – administration of PZQ; 3 – pharmacological control; 4 – cohort “Exp–Nexp”; 5 – Ajzen approach based on TPB; 6 – calculation of incidences) with determination of incidences in the Exp and Nexp groups, the investigations of Carlos A. et al. (23) in a systematic review identified 19 interventions (chemotherapy and pharmacological control) carried out for CC with a view to eliminating schistosomiasis, of which 94.73% focused on PZQ, 42.10% evaluated the impact of PZQ, 78.89% studied prevalence, and only 5.26% conducted an incidence study “before and after intervention” (32–50).
Indeed, this incidence study revealed that interventions focused on the introduction of well drilling resulted in a significant reduction in the use of high-risk water for drinking, cooking, and washing dishes. However, despite the methodology adopted—coupled with chemotherapy—the incidence of schistosomiasis infection remained at 21–28% (28). These proportions, which are significantly higher than those in the Exp group of our study, could be linked either to the type of model implemented, the monitoring of beneficiaries, or the content of the themes taught.
In an awareness-raising activity aimed at KAP carried out on 577 individuals in Kenya, Garba A. et al. reported that only 33% of individuals in the intervention zone were favourable to a behavioural change (51). The study also revealed a statistically significant difference at the 5% threshold (p=0.013<0.05) of bilharzia infection in households by study group (Cl-Ep) but with a more remarkable effect on sex workers who had not been exposed. The same applies to the reduction in the incidence of bilharziasis in relation to sex in the Exp group at the threshold of 5% (p=0.000<0.05), with a more pronounced effect in boys.In addition, reinfection with schistosomiasis was highly significant according to sex at the level of the two Exp groups among the controls at the threshold of 5% (p=0.000<0.05 and p=0.001<0.05), and we observed that boys were more affected than girls at the Exp level compared with the control level (Table 6). Furthermore, boys in the Exp (7.54%) and Nexp (18.87%) groups were in much higher proportions than girls in the Exp (3.77%) and Nexp (5.66%) groups, respectively (Table 6), which testifies to the vulnerability of boys. This is linked to their greater participation in swimming activities, unlike girls, whose lower proportion is related not only to their presence alongside their mothers for domestic activities but also to puberty, which requires them to maintain their privacy.
Our research is in accordance with the findings of Rudge et al., as cited by Knopp et al., regarding the micro-epidemiology of schistosomiasis in Zanzibar. The study revealed that boys were more commonly and severely infected than girls, resulting in mean exposure scores that were statistically significantly higher for boys. There is indeed a significant association between bilharzia infection and swimming activities, including washing and bathing, with the risk of contamination being higher for boys than for girls (odds ratio [OR] = 3.01, 95% confidence interval [CI] = 1.36–6.67) (37, 52).
Thus, it is possible to conclude that the estimation result is effective, with a determination coefficient R2 =0.5962, indicating that 59.62% of the variability in the incidence of bilharzia is explained by the independent variables. This demonstrates the good prediction quality of the model. Logistic regression estimation revealed that only the variables TCS, DCS, FCS, HIBC, and HPB were statistically significant and represented positive effects that influence the incidence of bilharzia by reducing new cases of contamination, with a RR = 0.46 and a CI [0.25–0.52], presenting our exposure factor as a “protective factor.”
The research shows an inhibitory effect, reducing the incidence of bilharzia. In other words, the periodic implementation of communication activities, with the willingness of households to follow the sessions and to change—driven by reconsideration of HPB—has an inducing effect on the reduction in incidence and could contribute to the eradication of schistosomiasis in endemic areas. Communication and awareness-raising sessions in the N'dali and Aguégués districts areas are illustrated on pictures of Figure 2.

Figure 2. Illustrative photos of communication and awareness-raising sessions in the N’dali and Aguégués districts.
The integrated approach used in the present study, centred on Godin’s model with the behaviour change method, was tested successfully. The study, based on an adapted version of Godin’s integrative model, is the result of various theoretical approaches, including TPB, HBM, and TPC (10–13). It helped to raise awareness among the target populations with a view to changing their behaviour in terms of their relationship with and use of the water sources that generate schistosomiasis.
However, a comparative analysis of Godin’s model, Green and Kreuter’s model, and the adapted Godin model shows that combining several models could further optimise results in the implementation of the CCC. Green and Kreuter’s communicative approach favours behaviour change through health education aimed at promoting nutritional health (53–56). However, the work of Aloys Hakizimana on the national Communication for Social and Behavioural Change (CSBC) strategy for health promotion, which is based on the Green and Kreuter approach (57), highlights some of Godin’s inadequacies due to its specificity in using behavioural and environmental diagnoses in the development of a communication strategy.
Indeed, the Green and Kreuter tool, unlike that of Godin, does not provide a behaviour prediction device in its methodology but is intended to be more holistic because it is derived from the PRECEDE–PROCEED (53) model of planning, implementation, and monitoring and evaluation in health promotion (56), making it possible to identify the communicational and environmental determinants of behaviours to promote health integrity. PRECEDE-PROCEED (36), developed by Green and Kreuter, thus appears as a social, epidemiological, behavioural and environmental, educational and ecological (organisational), administrative, and political diagnostic framework—a means of planning, implementing, and monitoring and evaluating health promotion programmes (56).
Sossa et al., through their studies on the early detection of the predictive value of lipoprotein ratios responsible for cardiovascular disease in adults, have already demonstrated the importance of intervention studies—particularly communication for behavioural change—in preventing cardiovascular disease (58–60).
Dale Weston et al., in addition to supporting Sossa and citing Rosentock and Rogers on the benefits of communication via interventions for behavioural change, noted in a systematic literature review on the application of behaviour change theories in the context of infectious diseases that “behavioural science can play a vital role in combating the effects of an infectious disease epidemic or public health emergency such as the COVID-19 pandemic” (14, 57, 61, 62).
Ultimately, the analysis of Green and Kreuter’s communication instrument for social change in behaviour compared with Godin’s integrated model allows us to deduce that the “adapted Godin model” used in our study suggests that the effects induced by a communication tool would be much more perceptible (i.e., lower incidences of a disease) if it had a more globalised character. Its performance should take into account elements of basic epidemiological diagnosis (analysis of the health situation of the population by determining the prevalence) alongside social diagnosis (perceptions and opinions), behavioural and environmental diagnoses, and the stages of planning, implementation, and monitoring–evaluation.
This intervention study is based on Godin’s TCP model on the one hand, and on the other hand, it incorporates the different stages of behaviour change represented by “self-awareness”, which was evaluated through the prediction survey based on the Ajzen approach to study the intention of our population to change their behaviour. “Awareness” was achieved through persuasive communication delivered in teaching sessions. “Motivation” was fostered through social empowerment. “Orientation” was linked to the perception of PBC (perceived behavioural control). “Action” was demonstrated by actual behavioural control, resulting in a reduction in the incidence of bilharziasis in N’dali and Aguégués. Finally, “sustainability” was marked by active community engagement.
Regarding sustainability, Garba et al., in their assessment of the impact of a health education programme and control measures for urinary bilharziasis, noted that “Changes of behaviour are slow to take place. As such, activities of health education must be sustained throughout a long period of time for sustainable profits of control to occur’’ (53). Therefore, it is vital for health authorities—particularly the Ministry of Health—to maintain and strengthen the measures introduced during our communication intervention to further reduce schistosomiasis transmission.
In summary, this cohort study involved the populations of Aguégués and N’dali, which are located within the same epidemiological field, and provides an overview of the two groups before and after the intervention outlined in Tables 3, 4, and summarised in the contingency table. The cohort included 128 participants, with 22 positive cases and 106 negative cases at baseline.
Before the intervention, the 106 negative cases were equally divided between the control group (53) and the experimental group (53). After the intervention, the number of sick individuals in the exposed group was 6, while the number of sick non-exposed individuals was 13.
We conclude that this health intervention was effective, with an estimated incidence of 19 new cases in a total population of 106 individuals. The exposure factor represented by health communication for behavioural change (CBC) appeared to be a « protective factor » as illustrated on the graph showing the impact of health communication on disease incidence by Figure 3.
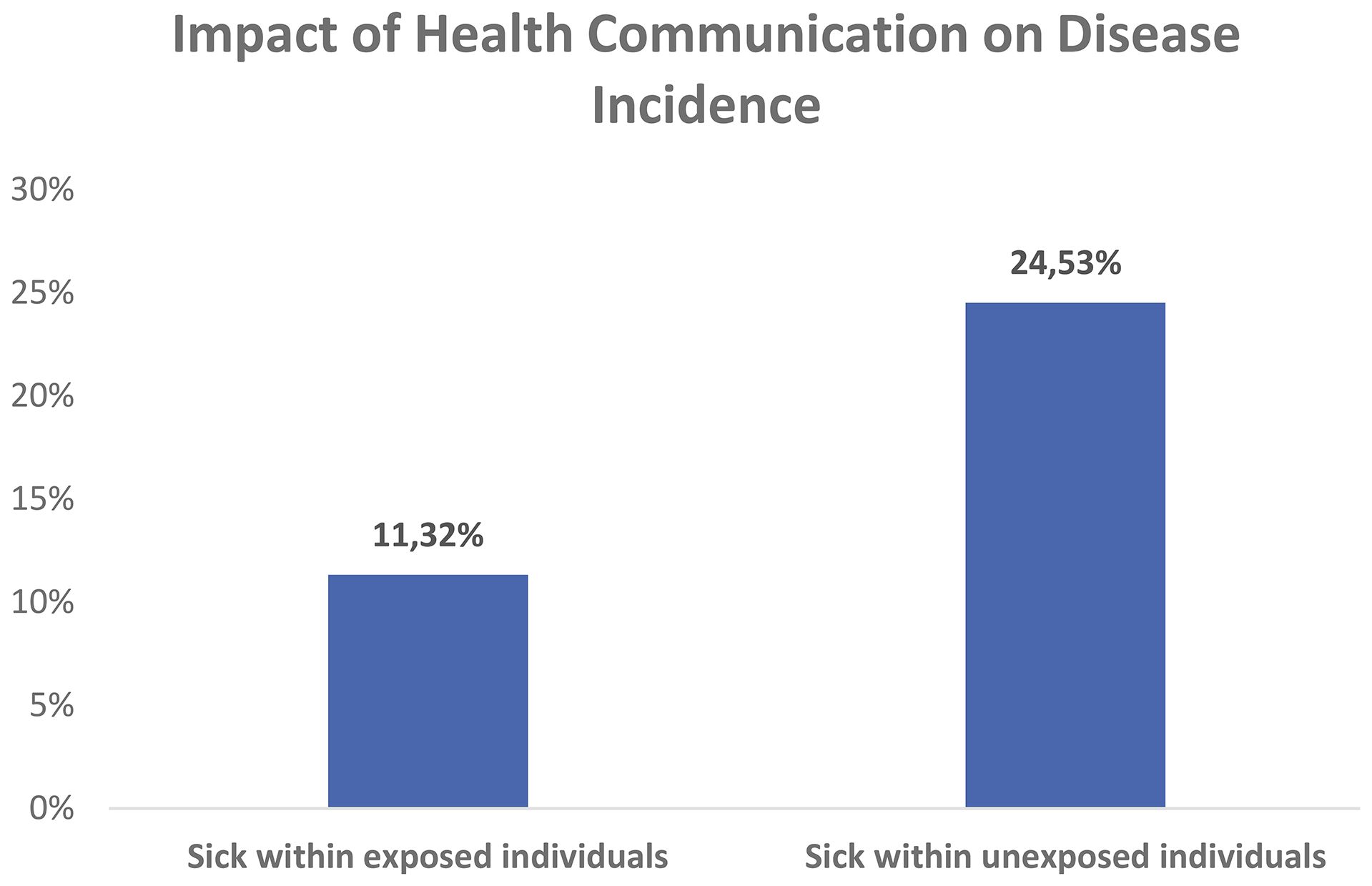
Figure 3. Graph showing incidences of the cohort study. Own fieldwork cohort in 2023.
6 “Practical implications” for public policy
In view of the relevance of these findings, we have identified the following prospects for future research and action, which could support the Ministry of Health’s policy in Benin and enable scaling of the model to other regions:
● An impact analysis of the behaviour change communication (BCC) project in the targeted localities will be necessary in the future, in view of the effects observed after the intervention with regard to a reduction in the incidence level.
● The development and promotion of health projects centred on artificial intelligence for the prediction of health-related behaviours and the management of endemic diseases, with a emphasis on the resurgence of schistosomiasis.
● Achieving excellent results will require implementing the programme in other endemic areas affected by schistosomiasis, with an increased sample size
● A comparative study with other West African countries could be carried out using the Behaviour Change Communication (BCC) model, with further experiments planned. Advocacy actions will be the main focus of this recommendation, and we will work with the Ministry of Health to redefine it. We hope to persuade partners collaborating in the fight against schistosomiasis to reallocate funds to communication activities for behavioural change. A 12- or 18-month follow-up could be used to measure relapses, sustainability, and deeper adoption by communities.
6.1 Strengths, Weaknesses, Opportunities, Threats (SWOT) analysis
Regarding the following research, a « SWOT » analysis is used as a key tool to highlight our project management, helping us to assess a project's internal Strengths and Weaknesses, as well as external Opportunities and Threats, in order to develop a strategic plan for success. As shown in Table 9 in this section, it provides a structured framework for the identification of internal factors within a project's control and external factors in its environment. This enables us as health project managers to make informed decisions, leverage advantages and mitigate risks.
6.2 The advantages of the study
An advantage of our study was our ability to diagnose children in the two communities involved in the intervention to determine whether they had the disease and to enable them to learn ways of avoiding it. The intervention was carried out over an extended period, allowing us to assess the strength and effect of the exposure factor. Cumulative model of analysis elements based on the Godin and Green Kreuter approaches. Combined model of analysis components using the Godin and Green Kreuter approaches.
6.3 Limitations of the study
This study has several limitations linked to difficulties in building a study population. Difficulties related to the funding of the study: the research was carried out using our own funds, which meant we were unable to fully pay all the stakeholders involved in data collection. The social situation of the study population—particularly those living in a lakeside environment close to neighbouring Nigeria, where a large amount of business is conducted—led to some people being lost to follow-up. However, this proportion was very small due to the epidemiological surveillance system set up by the research team. The “intent-to-treat” approach often used in epidemiological surveillance (in the case of diseases in the context of COVID-19) and the low number of unexposed participants in the cohort (individuals who tested negative for bilharzia during the efficacy control of praziquantel) enabled us to include this number in the calculations, assuming they had also been treated for the exposure factor.
Another limitation relates to potential issues with the laboratory reagents (sensitivity and specificity) and with the filters and filter holders, where manufacturing defects could cause handling errors. Such issues could lead to bias, particularly regarding compliance with the urine study protocol (communication), even if some participants had already dropped out of the cohort.
6.4 Study bias
We can cite, among others, selection bias linked to nonresponses or loss to follow-up; surveillance bias; indication or treatment bias linked to the prescription or the way the individual carried out the treatment (e.g., the children of EPP Bembè 2); information bias during data collection; bias linked to the Hawthorne effect (21, 22); confounding bias linked to the exposure factor; and bias linked to site sampling and laboratory handling (quality of reagents and inaccuracies).
7 Conclusion
This study highlighted integrated communication as a factor capable of inducing a change in behaviour within a population to reduce the incidence of schistosomiasis. The results obtained are in accordance with the objectives set, and there is no doubt that the integrated communication model implemented could be applied in other studies and promote the implementation of disease risk prevention strategies and/or reduce disease incidence.
In view of the results of this study, it seems appropriate to extend the actions developed as part of this research to other localities declared endemic for schistosomiasis, with the aim of reducing the incidence of the disease and, consequently, stopping or, as far as possible, slowing its spread. This requires public and institutional authorities to redirect financial resources traditionally allocated to chemotherapy towards awareness-raising through communication to bring about behavioural change.
Furthermore, in the hope of achieving the goal of this study, it is imperative that the Ministry of Health in general, and the health zones involved in community interventions in particular, adopt the results of this study to maintain progress in the fight against the spread of the disease.
Finally, the research department should carry out an impact study to evaluate the control strategy implemented.
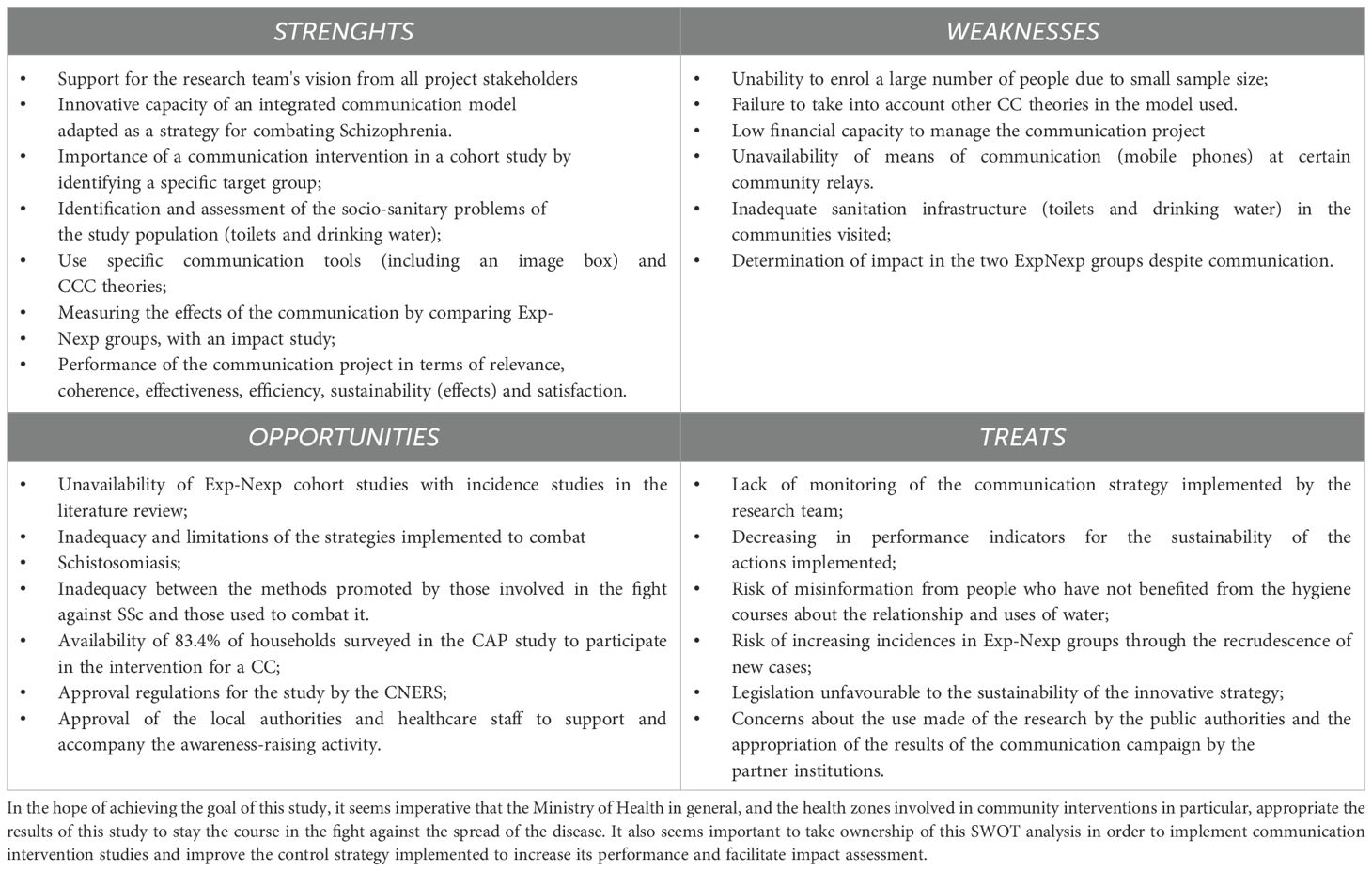
Table 9. “SWOT” analysis matrix.
Data availability statement
The datasets presented in this article are not readily available because of the regulations governing the use of health data put in place by the Ministry of Health. Requests to access the datasets should be directed to am9zaWFzYWhhbWlkZUBnbWFpbC5jb20=.
Ethics statement
The study received approval from the National Committee for Ethics and Health Research (NCEHR) of Benin under ethical opinion No. 22 of June 21, 2021, and was registered under No. 91/MS/DC/SGM/CNERS/HER. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. Written informed consent was obtained from the individual(s), and minor(s)' legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributions
JA: Supervision, Methodology, Software, Investigation, Funding acquisition, Conceptualization, Visualization, Project administration, Formal Analysis, Writing – original draft, Validation, Resources, Data curation. CS: Methodology, Supervision, Writing – original draft. YS: Project administration, Supervision, Writing – review & editing. EY: Supervision, Methodology, Conceptualization, Funding acquisition, Software, Writing – review & editing, Investigation, Formal Analysis. EO: Methodology, Writing – review & editing, Supervision.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to thank all those involved at various levels who contributed to the collection of information for this study, particularly those who substantially contributed to the scientific quality of this document. Our gratefulness is also towards the school’s principals, the central major of the municipality of Aguégués, Mr. Jules Kokoun, and all communities’ relays for their engagement and availability.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Glossary
TCS: Topics of Communication Session
DCS: Duration of Communication Sessions
FCS: Frequency of Communication Sessions
HAP: Household Attitudes and Practices
HPB: Household Past Behaviour
HSN: Household Social Norms
HIBC: Household Intention for Behaviour Change
MT: Mass Treatment
DDM: Mass Diagnosis
ITT: Intention To Treat
TPB: Theory of Planned Behaviour
TPC: theory of persuasive communication
SAC: School Aged Children
HBM: Health Belief Model
NECHR: National Ethics Committee for Health Research
PRECED: Predisposing, Reinforcing, and Enabling Constructs in Educational/Ecological Diagnosis and Evaluation
PROCEED: Policy, Regulatory, and Organizational Construct in Educational and Environment Development
PBC: Perceived Behavioural Control
PZQ: Praziquantel
PPS: Public Primary School
PrPS: Private Primary School
NTD: Neglected Tropical Disease
SW: Sex Worker
Agué: AGUEGUES
Crl: Control
Ep: Experimental
Crl-Ep: Controls and Experimental
Exp: Exposed
Non-Exposed: Nexp/Unexposed
BC: Behaviour Change
CSBC: Communication for Social and Behavioural Change
TPC: Theory of persuasive communication
References
1. National Master Plan for Integrated Control of Tropical Diseases. Ministry of health. National Public Health Department; National Control Program for communicable diseases; Benin neglected tropical diseases (NTDs) strategies(2017). Available online at: https://www.ntdenvision.org/sites/default/files/docs/Benin_plan_directeur_mtn_2016-2020_version_finale_25sept2017.pdf.
2. Steinmann P, Keiser J, Bos R, Tanner M, Utzinger J, et al. Schistosomiasis and water resources development. Systematic review, meta-analysis, and estimates of people at risk. Lancet Infectious. Dis. (2006) 6:411–25. doi: 10.1016/S1473-3099(06)70521-7
3. Colley DG, Bustinduy AL, Secor WE, and King CH. Human schistosomiasis. Lancet. (2014) 383:2253–226. doi: 10.1016/S0140-6736(13)61949-2
4. Knopp S, Mohammed KA, Ali SM, Khamis IS, Ame SM, Albonico M, et al. Study and implementation of urogenital schistosomiasis elimination in Zanzibar (Unguja and Pemba islands) using an integrated multidisciplinary approach. BMC Public Health. (2012) 12:930. doi: 10.1186/1471-2458-12-930
5. Ahamidé JO, Sossa CJ, Sissinto Y, Yétongnon E, Boko-Collins PB, Tchèbè R, et al. Sociodemographic and economic factors associated with urinary bilharzia in the municipalities of Sô-Ava, Aguégués and N’dali in Benin. PhD in Public Health in Cotonou (Benin). Open J Epidemiol. (2023) 13:342–59. doi: 10.4236/ojepi.2023.134025
6. Ahamidé J, Sossa C, and Sissinto Y. Attitudes and Practices (KAP) of adults on the uses and relationships with water in the communes of Sô-Ava, Aguégués and N’dali in Benin. PhD in Public health. J Rech. Sci Univ Lomé (Togo). (2024) 26:231–47. doi: 10.4314/jrsul.v26i1.30
7. Marshall J, Goldbart J, Pickstone C, and Roulstone S. Application of systematic reviews in speech-and-language therapy. Int J Lang Communication Disord. (2011) 46:261–72. doi: 10.3109/13682822.2011.497530
8. Morgan AT, Murray E, and Liegeois FJ. Interventions for childhood apraxia of speech. Cochrane Database Systematic Rev. (2018) 16:CD006278. doi: 10.1002/14651858.CD006278.pub37
9. Lavoie M, Macoir J, and Bier N. Effectiveness of technologies in the treatment of post-stroke anomia: A systematic review. J Communication Disord. (2017) 65:43–53. doi: 10.1016/j.jcomdis.2017.01.001
10. Salmi L-R. Lecture critique et communication médicale scientifique: Comment lire, présenter, rédiger et publier une étude clinique ou épidémiologique. In: Issy-les- Moulineaux. Elsevier Masson, France (2012).
11. The World Bank. World bank country and lending groups. Available online at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (Accessed June, 2017).
12. PATH. Advancing RSV Maternal Immunization: A Gap Analysis Report. Seattle (2018). Available online at: https://www.path.org/resources/advancing-rsv-maternalimmunization-gap-analysis-report/.
13. den Boon S, Jit M, Brisson M, Medley G, Beutels P, White R, et al. Guidelines for multi-model comparisons of the impact of infectious disease interventions. BMC Med. (2019) 17:163. doi: 10.1186/s12916-019-1403-9
14. Ajzen I. The theory of planned behavior. Organizational Behav Hum Decision Processes. (1991) 50:179–211. doi: 10.1016/0749-5978(91)90020-T
15. Fishbein M and Ajzen I. Attitudes towards objects as predictors of single and multiple behavioral criteria. Psychologica l Rev. 81:59–74.
16. Kautonen T and van Gelderen M. Predicting entrepreneurial behavior: A test of the theory of planned behavior. Appl Economics. (2013) 45:697–707. doi: 10.1080/00036846.2011.610750
17. Karim G. La Mise en Place du Brand Content par le biais des Leaders d’opinion sur les sites du Réseautage (i.e linkedIn, Viadeo, Xing et SkilledAfricans): Approche par la Théorie du Comportement Planifié. France: Thèse de doctorat, université de Poitiers (2018). Available online at: http://www.theses.fr/s93241.
18. National Review of Benin Republic Population of villages and city districts in Benin (rgph-4, 2013) RPH/INSAE Provisional results of the General Census of Population and Housing National Institute of Statistics and Economic Analysis, Benin., 18.
19. Lachin JM. Statistical considerations in the intent-to-treat principle. Controlled Clin Trials. (2000) 21:526. doi: 10.1016/S0197-2456(00)00092-1
22. WHO training course on management of NTDs at district level learner’s guide module diagnosis of NTDs with preventive chemotherapy session 9.3: diagnostic and laboratory tools for filaria, soil transmitted helminthiasis and schistosomiasis, 17–30.
23. Sow A. Les determinants de l’intention des petits amis travailleuses de sexe à utiliser le préservatif comme moyen de prevention contre les IST et le VIH/SIDA dans la region de Dakar au Sénégal. Mémoire de la faculté des études supérieures de l’université de LAVAL dans le cadre de la maîtrise en santé communautaire. In: Faculté de médecine/Faculté des sciences infirmières. Université Laval, Août (2005).
24. Torres-Vitolas CA, et al. Behaviour change interventions for the control and elimination of schistosomiasis: A systematic review of evidence from low-and middle-income countries. PloS Negl Trop Dis. (2023) 17:2–6. doi: 10.1371/journal.pntd.0011315
25. A guide for managers of control programmes(2011). Available online at: https://www.who.int/neglected_diseases/resources/9789241548267/en/. [2] World Health Organization. Schistosomiasis: progress report 2001–2011 and strategic plan 2012-2020, 2013. https://www.who.int/schistosomiasis/resources/9789241503174/en/.
26. WHO’s review. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. Geneva: World Health Organization (2018).
27. WHO’s review. Prevention and control of schistosomiasis and soil-transmitted helminthiasis. Geneva: World Health Organization (2002). Available online at: http://apps.who.int/iris/bitstream/10665/42588/1/WHO_TRS_912.pdf?ua=1.
28. World Health Organization. Preventive chemotherapy in human helminthiasis: coordinated use of anthelmintic drugs in control interventions: a manual for health professionals and programme managers. (2006) 22:49–51.
30. Gray DJ, Ross AG, Li YS, and McManus DP. Diagnosis and management of schistosomiasis. BMJ (Clinical Res Ed.). (2011) 342:d2651. doi: 10.1136/bmj.d2651
31. Poletti P, Merler S, Ajelli M, Manfredi P, Munywoki PK, Nokes DJ, et al. Evaluating vaccination strategies for reducing infant respiratory syncytial virus infection in low-income settings. BMC Med. (2015) 13:49. doi: 10.1186/s12916-015-0283-x
32. Hong Q, Yang K, Huang YX, Sun LP, Yang GJ, Gao Y, et al. Effectiveness of a comprehensive schistosomiasis japonica control program in Jiangsu province, China, from 2005 to 2008. 120:S151–57
33. Jia-Gang G, Chun-Li C, Guang-Han H, Han L, Dong L, Rong Z, et al. The role of ‘passive chemotherapy’plus health education for schistosomiasis control in China during maintenance and consolidation phase. Acta Trop. (2005) 96:177–83. doi: 10.1016/j.actatropica.2005.07.012
34. N’Diaye M, Dioukhane EM, Ndao B, Diedhiou K, Diawara L, Talla I, et al. Schistosomiasis sustained control program in ethnic groups around ninefescha (Eastern Senegal). Am J Trop Med Hyg. (2016) 95:614–22. doi: 10.4269/ajtmh.15–0125
35. Nagi M. Evaluation of a programme for control of schistosoma haematobium infection in Yemen. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit. (2005) 11:977–87.
36. Oyeyemi O, Olowookere D, Ezekiel C, Oso G, and Odaibo A. The impact of chemotherapy, education and community water supply on schistosomiasis control in a Southwestern Nigerian village. Infect Dis Health. (2018) 23:121–3. doi: 10.1016/j.idh.2018.01.004
37. Knopp S, Person B, Ame SM, Ali SM, Hattendorf J, Juma S, et al. Evaluation of integrated interventions layered on mass drug administration for urogenital schistosomiasis elimination: a cluster-randomised trial. Lancet Glob Health. (2019) 7:e1118–29. doi: 10.1016/S2214-109X(19)30189–5
38. El Kholy H, Arap Siongok TK, Koech DK, Sturrock RF, Mahmoud AF, Houser H, et al. Effects of borehole wells on water utilization in schistosoma haematobium endemic communities in coast province, Kenya. Am J Trop Med Hyg. (1989) 41:212–9. doi: 10.4269/ajtmh.1989.41.212
39. Wepnje GB, Anchang-Kimbi JK, Ndassi VD, Lehman LG, and Kimbi HK. Schistosoma haematobium infection status and its associated risk factors among pregnant women in Munyenge, South West Region, Cameroon following scale-up of communal piped water sources from 2014 to 2017: a cross-sectional study. BMC Public Health. (2019) 19:392. doi: 10.1186/s12889-019-6659–7
40. Muhumuza S, Olsen A, Katahoire A, and Nuwaha F. Reduced uptake of mass treatment for schistosomiasis control in absence of food: beyond a randomized trial. BMC Infect Dis. (2015) 15:423. doi: 10.1186/s12879-015-1158–7
41. Torres-Vitolas CA, Trienekens SCM, Zaadnoordijk W, and Gouvras ANBehaviour change for schistosomiasis control and elimination: A systematic review. PLoS Negl Trop Dis. (2023) 17:30–33. doi: 10.1371/journal.pntd.0011315
42. Chaula SA and Tarimo DS. Impact of praziquantel mass drug administration campaign on prevalence and intensity of Schistosoma haemamtobium among schoolchildren in Bahi district, Tanzania. Tanzan J Health Res. (2014) 16:1–30. doi: 10.4314/thrb.v16i1.1
43. Cline BL and Hewlett BS. Community-based approach to schistosomiasis control. Acta Trop. (1996) 61:107–19. doi: 10.1016/0001-706x(95)00118-x
44. Favre TC, Massara CL, Beck LCNH, Cabello RKSA, and Pieri OS. Adherence to diagnosis followed by selective treatment of schistosomiasis mansoni and related knowledge among schoolchildren in an endemic area of Minas Gerais, Brazil, prior to and after the implementation of educational actions. Parasite Epidemiol Control. (2021) 13:e00208. doi: 10.1016/j.parepi.2021.e00208
45. Wolmarans CT and de Kock KN. The influence of health education on the prevalence, intensity and morbidity of Schistosoma haematobium infections in children over a two-year period in the Limpopo Province, South Africa. South Afr J Epidemiol Infect. (2009) 24:13–7. doi: 10.1080/10158782.2009.11441334
46. Kosinski KC, Kulinkina AV, Abrah AFA, Adjei MN, Breen KM, Chaudhry HM, et al. A mixed-methods approach to understanding water use and water infrastructure in a schistosomiasis-endemic community: case study of Asamama, Ghana. BMC Public Health. (2016) 16:322. doi: 10.1186/s12889-016-2976–2
47. Nsowah-Nuamah NN, Mensah G, Aryeetey ME, Wagatsuma Y, and Bentil G. Urinary schistosomiasis in southern Ghana: a logistic regression approach to data from a community-based integrated control program. Am J Trop Med Hyg. (2001) 65:484–90. doi: 10.4269/ajtmh.2001.65.484
48. Hurlimann E, Silue´ KD, Zouzou F, Ouattara M, Schmidlin T, Yapi RB, et al. Effect of an integrated intervention package of preventive chemotherapy, community-led total sanitation and health education on the prevalence of helminth and intestinal protozoa infections in Coˆ te d’Ivoire. Parasit Vectors. (2018) 11:115.
49. Madon S, Malecela MN, Mashoto K, Donohue R, Mubyazi G, and Michael E. The role of community participation for sustainable integrated neglected tropical diseases and water, sanitation and hygiene intervention programs: A pilot project in Tanzania. Soc Sci Med. (1982) 2018:202:28–37. doi: 10.1016/j.socscimed.2018.02.016
50. Guang-Han H, Jia H, Kuang-Yu S, Dan-Dan L, Ju Z, Chun-Li C, et al. The role of health education and health promotion in the control of schistosomiasis: experiences from a 12-year intervention study in the Poyang Lake area. Acta Trop. (2005) 96:232–41. doi: 10.1016/j.actatropica.2005.07.016
51. Freeman MC, Clasen T, Brooker SJ, Akoko DO, and Rheingans R. The Impact of a School-Based Hygiene, Water Quality and Sanitation Intervention on Soil-Transmitted Helminth Reinfection: A Cluster-Randomized Trial. 89:875–883.
52. Rudge JW, Stothard JR, Basáñez MG, Mgeni AF, Khamis IS, Alliepo N, et al. Micro-epidemiology of urinary schistosomiasis in Zanzibar: Local risk factors associated with distribution of infections among schoolchildren and relevance for control. Acta Tropica. (2008) 105:45–54. doi: 10.1016/j.actatropica.2007.09.006
53. Garba A, Aboubacar A, Barkire A, Véra C, Sellin B, and Chippaux J-P. Cahiers d’Etudes Recherches Francophones. (2001) 11:35–42. ISSN 1157-5999.
54. Green LW and Kreuter MW. Health promotion planning: An educational and ecological approach. London, Toronto, CA: Mayfield publishing company (1999).
55. Green LW and Kreuter MW. Health promotion planning: An educational and environmental approach. CA: Mayfield publishing company: Mountain View, California (1991).
57. Weston D, Ip A, and Amlôt R. Examining the application of behaviour change theories in the context of infectious disease outbreaks and emergency response: a review of review. BMC Public Health. (2020) 20:1483. doi: 10.1186/s12889-020-09519-2
58. Charles S, Agueh V, Saizonou J, and Delisle H. Prédiction de l’insulino-résistance par les ratios de lipoprotéines chez les adultes béninois. Int J Biol Chem Sci. (2015) 9:1319–29. Available online at: http://ajol.info/index.php/ijbcs.
59. Metonnou CG, Azandjeme CS, Sossa CJ, Issiako BN, Paraïso MN, Agueh V, et al. Effects of a community-based. Intervention on the lifestyle and health of people at risk of type 2 diabetes in Benin. Food Nutr Sci. (2022) 13:842–60. doi: 10.4236/fns.2022.1310061
60. Metonnou ClémenceG, Azandjèmè C, and Sossa C. Performance Evaluation of a Communication. Plan Implementation for Behaviour Change in People at Risk of Type 2 Diabetes in the. Commune of Tchaourou in Benin. J Diabetes Mellitus. (2022) 12:224–42. Available online at: https://www.scirp.org/journal/jdm.
Keywords: bilharziasis, households, school-aged children, integrated communication model, theory of planned behaviour, quasi-experimental design
Citation: Ahamidé JO, Sossa CJ, Sissinto Y, Yétongnon E and Ouendo E-M (2025) Effects of behaviour change communication: interventions for the prevention of bilharziasis in the districts of N’dali and Aguégués in Benin. Front. Trop. Dis. 6:1622582. doi: 10.3389/fitd.2025.1622582
Received: 10 May 2025; Accepted: 04 August 2025;
Published: 23 October 2025.
Edited by:
Roberta Iatta, University of Bari Aldo Moro, ItalyReviewed by:
Leticia Gomes De Pontes, Universidade de Minas Gerais, BrazilSunny Doodu Mante, African Filariasis Morbidity Project, Ghana
Copyright © 2025 Ahamidé, Sossa, Sissinto, Yétongnon and Ouendo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josias Olutobi Ahamidé, am9zaWFzYWhhbWlkZUBnbWFpbC5jb20=