 Cristina Juan Jimenez1*†
Cristina Juan Jimenez1*† Marta Arsuaga Vicente2†María Santamaría Seijas3
Marta Arsuaga Vicente2†María Santamaría Seijas3 Mar Lago Nuñez2Marta Díaz Menéndez2Rosa de Miguel Buckley2†Fernando de la Calle-Prieto2†
Mar Lago Nuñez2Marta Díaz Menéndez2Rosa de Miguel Buckley2†Fernando de la Calle-Prieto2† Ana M. Ayuso_Alvarez4†
Ana M. Ayuso_Alvarez4† Marina Gold3†
Marina Gold3†- 1Department of International Cooperation, Anesvad Foundation, Bilbao, Spain
- 2National Referral Unit for Imported Infectious Diseases and International Health Biomedical Research Networking Center for Infectious Diseases (CIBERINFECT), Hospital La Paz-Carlos III, Madrid, Spain
- 3Department of Projects and Programs, Mundo Sano Foundation, Madrid, Spain
- 4Faculty of Political Science and Sociology, Department of Social Anthropology, University Complutense, Madrid, Spain
Background: Latin American migrants living with Chagas disease (CD) face significant healthcare challenges, including limited awareness of the disease among primary care providers and patients, undocumented status, and inflexible working conditions that hinder timely diagnosis and treatment. This study evaluates the impact of community health worker (CHW) interventions on CD patients in a hospital in Madrid and identifies key barriers within the public healthcare system.
Methods: This phenomenological study (October 2021–February 2025) involved 13 patients supported by a CHW, six unsupported patients, nine health workers, and one CHA.
Results: Most patients were Bolivian women over 41 years old working in the service and domestic roles. Health workers and the CHW had over 10 years of experience with CD. Most were diagnosed in Spain, with at least 10 individuals reporting cardiac symptoms. However, none had Chagas cardiomyopathy. They usually present with the indeterminate form, which corresponds to the chronic phase of CD. Patients had limited CD knowledge, but they generally adhered well to treatment when indicated. Key findings included misdiagnosis and lack of awareness among primary healthcare workers, leading to referrals to tropical medicine units. Barriers were administrative, geographical, work-related, financial, and cultural. The CHW improved adherence and follow-up through culturally tailored interventions. Recommendations included enhancing primary care knowledge, improving referral pathways, better integrating the CHW, and establishing a patient association in Madrid for education and support.
Conclusions: CD remains a major health issue among Latin American migrants or descendants of mothers from endemic areas, who face many obstacles in diagnosis and treatment. CHWs are key to improving treatment adherence, but their integration into the healthcare system is still ongoing. Addressing socioeconomic and cultural barriers requires collaboration, ongoing education, and stronger support networks for primary health workers and patients.
1 Introduction
Chagas disease (CD) is an infectious Neglected Tropical Disease (NTD) caused by Trypanosoma cruzi (T. cruzi), a protozoan parasite (1, 2). NTDs affect people living in poverty, with limited access to sanitation and clean water, increasing their risk of contact with vectors, domestic animals, and livestock (3, 4). One of the main difficulties in controlling CD is that fewer than 10% of people with the disease worldwide are diagnosed (5). Transmission occurs by contact with the excreta of infected bugs, mother-to-child, blood or organ donation, ingestion of contaminated food (such as açaí) or laboratory accidents (1, 3, 6). CD patients experience an initial acute phase with non-specific symptoms such as fever, headache, and muscle pain, followed by a chronic phase one to three decades later, which in some cases affects the heart, digestive system, and nervous system (1, 2, 7). Diagnosis requires at least two different serological tests, and discrepancies across countries regarding which tests are more effective present both logistical and financial challenges (2, 8). Despite the availability of two effective drugs, their efficacy declines significantly in the chronic phase, while adverse drug reactions increase with age (1, 2, 9). This explains why treatment is prescribed only in the acute phase, early chronic phase, and in cases of reactivated infection (1). However, in children, treatment is 100% effective, and treatment before pregnancy prevents vertical transmission (10).
Globally, CD affects approximately 6 to 7 million people and is predominantly endemic in 21 regions across Latin American countries, particularly in rural areas (1, 3–5, 11–13). Among these countries, Bolivia has the highest prevalence of CD (7). Nevertheless, migratory movements have led to the spread of the disease to non-endemic countries, particularly in the USA and Europe, where doctors often lack experience and underestimate its severity (3, 6, 8, 14). This new scenario presents health, economic, social, and political challenges related to human mobility (13). Spain ranks second as a destination for Latin American migrants infected with T. cruzi in childhood. They seek better job opportunities, and by the time they access the healthcare system in Spain, they are usually in the chronic phase of the disease (5, 8, 11, 15). In 2022, 79,233 Bolivian individuals were living in Spain, with at least 20% residing in the Community of Madrid, including 7,595 men and 8,774 women (16). The prevalence of CD among Bolivian individuals in Spain is estimated to be between 18.1% and 21.1% (11, 17). During the study period, the new CD diagnoses in the Community of Madrid ranged from 52 to 83 and the number of CD follow-up patients were around 300 each year.
Psychosocial and cultural determinants pose significant challenges to diagnosing and treating patients with CD, particularly due to widespread misconceptions among patients who perceive it as a terminal illness (5). This is accompanied by a lack of knowledge about the healthcare system, distrust, precarious and inflexible employment, and a limited number of specialized referral units (13, 18). In addition, individuals with CD encounter several barriers to completing treatment, including its side effects, its long duration (30 to 60 days), and challenges with patient follow-up. Furthermore, the precarious economic situation faced by many migrants poses a significant risk for delayed diagnosis, as they often prioritize work over their health (4, 13). Health studies on precarious migration (e.g., undocumented individuals or those without health insurance) emphasize the need to understand health perceptions and access strategies in such populations. To gain understanding, it is crucial to view health as part of a broader concept of well-being, including the role of social relationships (19–22).
To address these barriers, the role of the CHW has recently emerged as a key actor in supporting migrant populations, acting as a bridge between the healthcare system and the needs of vulnerable communities (5). The concept of a CHW has evolved significantly in recent years. In 2014, the World Health Organization (WHO) initially defined them as individuals chosen by their community to promote healthy practices in coordination with healthcare providers and the community, performing their work voluntarily (23, 24). Over time, this definition has been revised to include the possibility of paid positions, promoting sustainability and ensuring health systems take responsibility for integrating the role of a CHW (25). The role of the CHW has been very important in Latin America since the 1970s, especially at the community level, with outreach to impoverished and vulnerable populations and under-resourced healthcare systems (24). Given their crucial responsibility, a CHW must be adequately trained to understand both community needs and the complexities of the healthcare system (25). In this line, the Mundo Sano Foundation, an association working in the field of NTDs in Spain and other countries, began collaborating with Hospital La Paz-Carlos III (Madrid) in 2015, incorporating a CHW from its staff into the facility. As part of this collaboration, the CHW was authorized to support CD patients by providing information, guidance, mediation, counseling, social support, and assistance. In 2023, a formal agreement was signed with the Madrid Health Service to enhance this collaboration.
This study aims to qualitatively evaluate the role of a CHW in supporting CD patients in Madrid (Spain) from the perspectives of both health workers and patients. It will assess satisfaction, the effectiveness of counseling, as well as treatment and follow-up adherence, while also identifying key barriers faced by patients within the public healthcare system.
2 Methods
2.1 Setting and population
This study was carried out in Madrid (Spain) with patients affected by CD who attended consultations at the Hospital La Paz-Carlos III, health workers caring for patients with CD in three hospitals in the Community of Madrid—Hospital La Paz-Carlos III, Hospital Ramón y Cajal, and Hospital 12 de Octubre—and a CHW employed by the Mundo Sano Foundation.
In the Community of Madrid, CD is managed in both primary and hospital care, with two specialized referral units—Hospital La Paz-Carlos III and Ramón y Cajal—that accept patients without prior referral from primary care. The initial evaluation includes blood tests, PCR, cardiac exams, and digestive studies if symptoms are present. After diagnosis and organ assessment, treatment eligibility is assessed. Treated patients are monitored biweekly for two months, then at 3, 6, and 12 months after completing treatment. Follow-up visits are conducted annually or biennially. Until 2025, the two medicines for treating CD—Benznidazole (Abarax, produced by ELEA Labs in Argentina) and Nifurtimox (Lampit, produced by Bayer)—were only available as imported medications in Spain, dispensed exclusively through the pharmacy for foreign medicines.
The CHW works in multiple settings: once a week at Hospital La Paz-Carlos III to meet and follow up with patients; twice a week at the Bolivian consulate for awareness activities; and during community screenings at health centers, churches, and other events. She also occasionally supports CD patients in other Madrid hospitals upon request, despite the absence of formal agreements with these institutions.
2.2 Study design and analysis
This was a phenomenological study, carried out from October 2021 to February 2025, engaging ethnographic methodology (participant observation), semi-structured interviews (SIs), and focus groups (FGs). In both SIs and FGs, a script was developed covering the following thematic areas:
1. Access to healthcare services.
2. Previous knowledge about CD.
3. Perceptions, beliefs, and experiences regarding CD.
4. Experiences with the healthcare system.
5. Experiences with the CHW.
For healthcare interviews, the script covered the following:
1. Personal information and professional experience.
2. Roles, patient profiles, and relationships.
3. Barriers and challenges.
4. Support services, coordination, and improvements.
Participants’ inclusion criteria were:
● People over 18 years old.
● Diagnosed with CD according to WHO guidelines.
● Untreated or not under medical surveillance.
● Willing to participate in the study.
Exclusion criteria were:
● Pregnancy.
● Refusal to participate.
● Having a family member already included in the supported group.
To establish a diagnosis of T. cruzi infection following WHO criteria, at least two serological tests detecting different parasite antigens must yield positive results (e.g., ELISA, indirect immunofluorescence, or indirect hemagglutination), thereby confirming the presence of IgG antibodies in the patient’s serum. These tests can be complemented by molecular or direct parasitological diagnostic techniques, such as PCR (8). A patient was considered supported by a CHW if contact was maintained for more than one month. The inclusion criteria for health workers were experience with CD patients, current practice in Madrid, and willingness to participate. Exclusion criteria were lack of CD experience or practicing outside Madrid.
A total of 19 patients were interviewed (13 supported by a CHW and six not supported), along with nine health workers (seven doctors, one nurse, and one nursing assistant) and one CHW. A snowball sampling approach was used to identify individuals. The sample size was determined by the principle of discourse saturation, meaning that interviews continued until no new significant information emerged (26). Saturation was assessed through iterative analysis, to ensure that the categories and themes identified in the discourse were sufficiently developed and well supported by the data. A content analysis was conducted using an abductive approach. The process began with an analytical decomposition of discourse into elementary units, to identify categories that could provide meaning to the social reality studied. This was followed by a synthesis or inductive process to establish connections between the discourse, the situation of patients with CD, and the context in which the CHW operates, thereby constructing its meaning. Validation of discourse interpretation was carried out through two strategies: triangulation, in which two researchers independently analyzed the discourses and compared their respective findings (inter-subjectivity); and participant validation, in which the main findings were discussed with the interviewees.
In addition, a literature review was performed using the following keywords: Chagas and barriers, Chagas and community agent, and Chagas and CHW. Multiple sources of written and oral information were used to triangulate the results and reduce potential bias from any single source.
One set of codes detailed the interviewees’ profiles, while the others covered four key thematic macro areas:
1. Knowledge of CD.
2. Perceptions, beliefs, emotions, and experiences related to CD.
3. Healthcare system and health workers.
4. CHW support.
To simplify the analysis, some subcategories of each code were created and included as supporting material.
Two key factors were considered in the analysis:
1. Satisfaction with the CHW, measured through data collected from semi-structured interviews and patients’ experiences with the healthcare system. It was also indirectly assessed by the number of referrals satisfied patients made to family and friends, as revealed through the qualitative analysis.
2. Adherence of patients to the care and follow-up pathway was assessed based on the WHO’s 2004 definition: “The degree to which a person’s behavior corresponds with the agreed recommendations of a healthcare provider” (27). Adherence was evaluated qualitatively through interview analysis, considering whether patients continued follow-up as instructed by their physician.
Data were transcribed manually or using the transcription software Whispercpp. After revision for accuracy, they were imported and analyzed using Altas.ti qualitative data analysis v.25.0.1. Coding was performed by two independent reviewers, who discussed the codes until consensus was reached.
The research was conducted according to the principles of the Declaration of Helsinki, being the participation voluntary. Verbal consent to participate was used rather than written consent. The choice of verbal over written consent was twofold. Firstly, the low level of literacy among some participants made it difficult for them to understand written texts, and they preferred to receive the information orally. Second, due to their irregular migratory status, they were reluctant to sign documents that might place them at risk.
2.3 Ethical considerations
The study protocol received approval from the Ethics Committee for Research with Medicinal Products at the University Hospital La Paz (Spain) on 1 November 2021. HULP: PI-4971. During data processing and analysis of the data, the names of interviewers were removed to maintain their identity confidential.
3 Results
3.1 People supported by a CHW
Results regarding screening, diagnosis, and treatment coverage are presented in Table 1. Thirteen patients with CD received support from a CHW (seven women and six men). Most were from Bolivia (12), while one was from Ecuador. Their median age was 43.9 years (IQR=38.5–49.3). Their occupations included domestic work (six), service occupations (five), and dentistry (one). One person was unemployed. During childhood, they typically lived in their country of origin in houses made of natural materials (adobe, wood), as reported by 10 individuals. Nine confirmed having seen the triatomine insects known as “vinchuca”: “I lived in an adobe house, and sometimes, when I was young, I saw a strange bug. I believe it (the disease) came from there” (Patient 6).
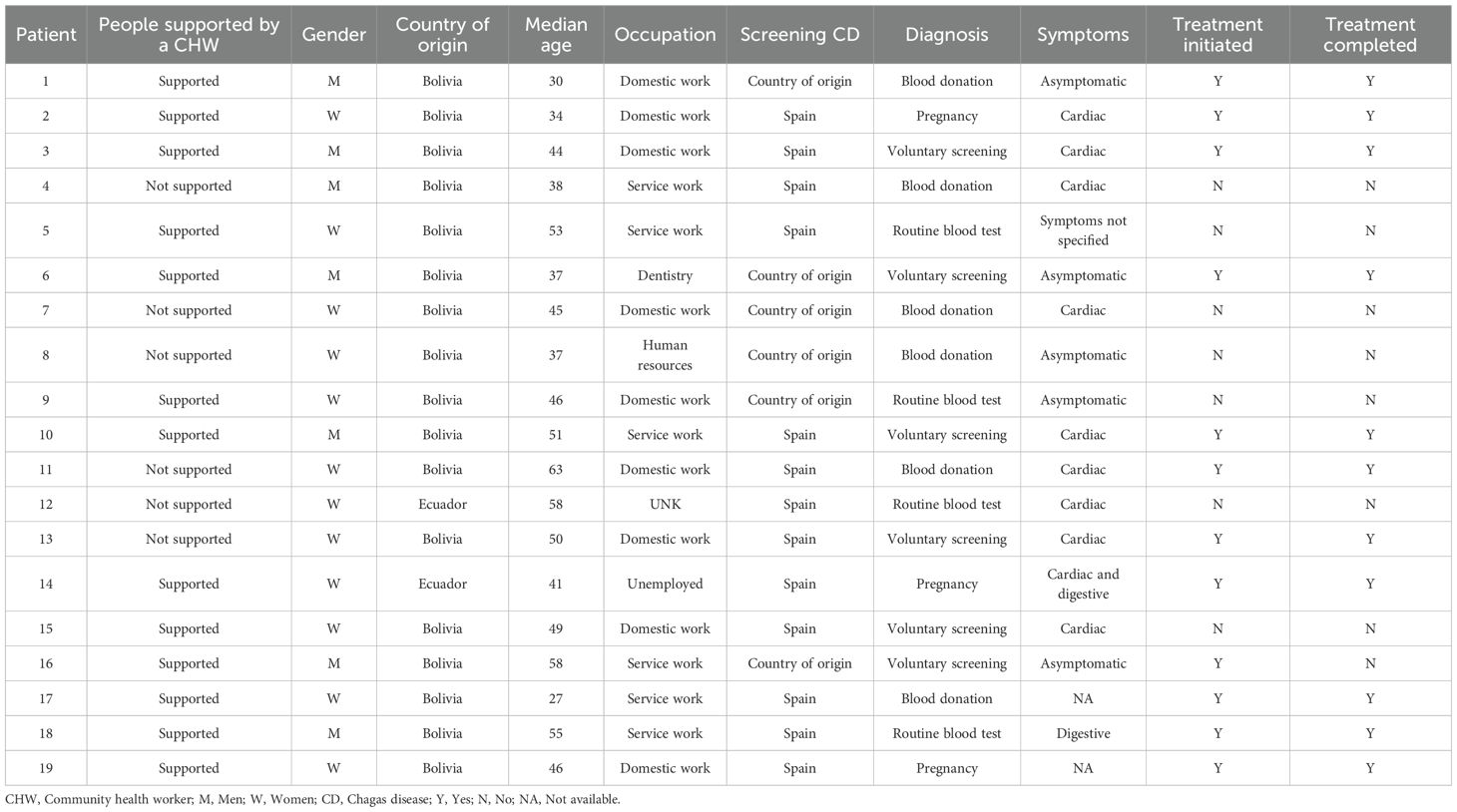
Table 1. Screening, diagnosis, and treatment coverage.
In terms of diagnosis, nine patients had been diagnosed in Spain and four in their country of origin. Patients tested positive for CD after experiencing symptoms or having a family member with CD (five), during pregnancy (three), during a routine blood test (three), or through blood donation (two). Their most common non-infectious comorbidities were hypercholesterolemia, hyperglycemia, Helicobacter pylori infection, anemia, fatty liver disease, and tumors. The most common infectious comorbidity was strongyloidiasis. Four people reported cardiac symptoms, one reported digestive symptoms, one reported both cardiac and digestive symptoms, and one mentioned symptoms without specifying which ones. Four people reported being asymptomatic. The most common cardiac symptoms were weakness, tachycardia, and fatigue. This information was missing in two interviews. Among these individuals, none had Chagas cardiomyopathy.
In analyzing family history, nine people were born to mothers with CD. Four people were unaware of their mothers’ situation, as explained in this interview: “My mother and that … since they didn’t get tested and they say they’re fine, they don’t want to get tested (Patient 1).” Twelve out of the thirteen interviewees reported having relatives with CD. Only four of the eleven who stated they had children confirmed that they had also tested their children: “My two little ones still need to get tested.—Are they in Bolivia?—Yes, they are” (Patient 15). All participants reported knowing acquaintances with CD.
Regarding knowledge of transmission, twelve individuals identified the bug bite, eight recognized mother-to-child, and three cited blood transfusions. No participant identified organ transplant or laboratory accident as routes of transmission. Knowledge of clinical symptoms was limited to cardiac (seven) and digestive (five) manifestations. Six patients cited direct contact as possible transmission route. Eight patients were aware of the availability of treatment, mentioning its “strong” side effects: “And she (the sister) is the one who did the treatment. It was very intense for three months; it made her lose weight, and my sister’s skin peeled off. She lost quite a bit of weight with the treatment because it was really strong” (Patient 15). Three patients had no knowledge of treatment. Furthermore, eight reported that CD is a incurable disease that could “sleep” or “stop,” especially after receiving treatment: “You have to undergo a long treatment, and it’s like the doctor said, we can only make the disease ‘sleep’” (Patient 5). Their primary sources of information were health workers, especially those working at Hospital La Paz-Carlos III. Four patients reported not receiving adequate information in their country of origin: “They explained a little, but as I said, they didn’t go into much detail” (Patient 1). In eight cases, family or friends also provided information, and five patients reported obtaining it online.
Ten individuals initiated treatment and nine completed it. Among this group, five reported experiencing rashes, itching, and nausea as adverse drug reactions. One person reported hearing loss as an adverse drug reaction, although this has not been previously recognized in the literature as a side effect. Additionally, one person reported no side effects. This information was missing in two interviews. Despite the side effects, patients recommended that their relatives or acquaintances get screened and treated, as evident in 11 interviews: “From there, I called my wife, then my mom. After that, I started calling my sisters, asking them to get tested” (Patient 1).
Patients of Bolivian origin and healthcare professionals with prior knowledge of CD perceived a higher risk of disease. Five participants mentioned knowing someone who had died from CD, and nine reported negative treatment experiences: “Well, someone who had that reaction said their face started itching, and then … I don’t know other things” (Patient 9). In analyzing health beliefs about CD, some patients stated that it causes death (four), only affects those over 40 (three), or could lead to cancer (two). Two interviewees mentioned an antiparasitic drug for animals, Ibome, as a treatment for CD: “And I also said there is another one, called Ibome, to deworm animals, and there is a Chinese doctor who is treating patients that come with that” (Patient 16).
Negative emotions upon CD diagnosis were mentioned in nine interviews. The most frequent emotion was fear, cited by eight patients, while others report worry, distress, disappointment, and surprise. Conversely, three people did not experience any of these negative emotions. This information was missing in one interview.
Delays in diagnosis or treatment were reported by 12 patients: “When I was pregnant they tested me and I found out I had Chagas. But after that I didn’t pay much attention to it” (Patient 2). Similarly, in 12 interviews, patients described comparable attitudes among their relatives or acquaintances. All patients indicated that trusted individuals, including work colleagues or supervisors, knew they were affected by CD.
In terms of access to screening, eight patients reported difficulties in obtaining a diagnosis, particularly in private hospitals, their countries of origin, or during pregnancy. None of the interviews specified which tests were used for screening in these cases. Regarding pathways to diagnosis, five patients were referred from primary care, while eight went directly to hospitals. One interviewee did not provide this information. Patient satisfaction with health professionals’ attitudes varied considerably. Nevertheless, all appreciated the care received at Hospital La Paz-Carlos III: “The doctors treated me very well, I was fine, they did the tests, everything, and I mentioned it, I filled in all the forms with my appointments and I’ve already had all the tests done” (Patient 3). Regarding primary care, three patients reported dissatisfaction.
Regarding the main barriers accessing the healthcare system, the findings are summarized in Table 2:
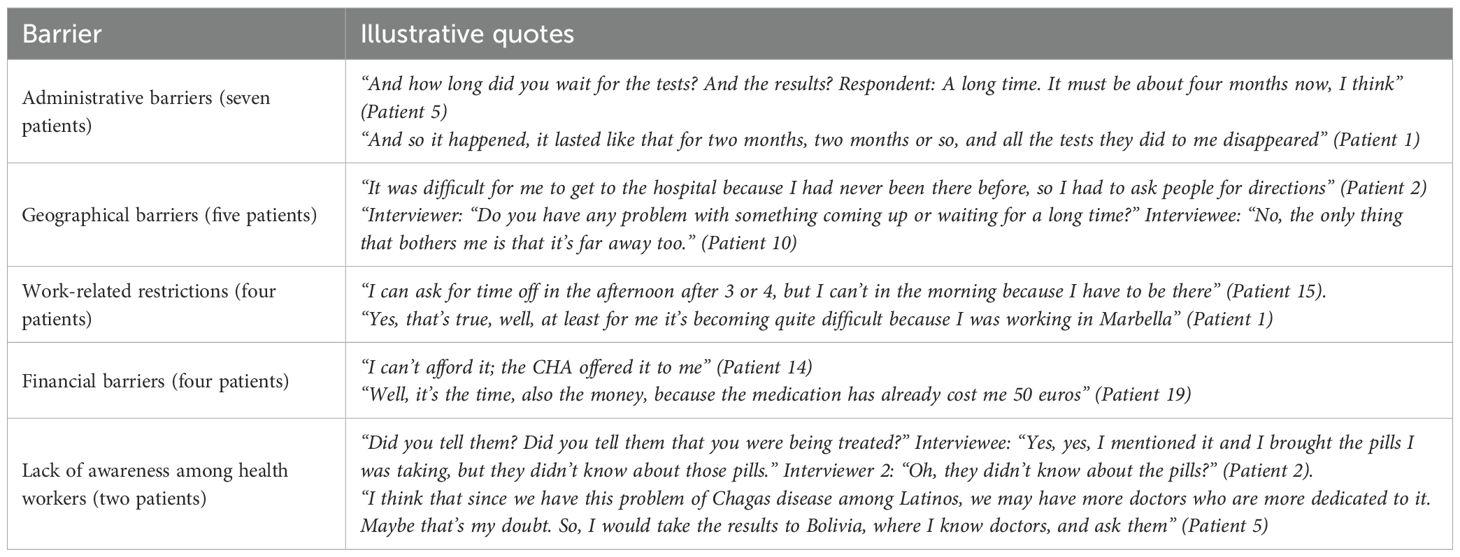
Table 2. Barriers to healthcare access in Spain for people supported by a CHW.
Administrative barriers include duplicate diagnostic tests and long waiting times; geographical barriers refer to the long distance to the hospital and to the single pharmacy in Madrid where treatment is dispensed.
The interventions performed by the CHW include assisting patients with appointments and providing information about CD, each cited by eight individuals while emotional and social support and access to medication were mentioned by seven patients each. Regarding treatment adherence, the valuable support of the CHW was cited in four interviews: “And that’s when CHW told me: don’t stop it, if what you’re experiencing is a side effect, don’t stop it” (Patient 2). All patients were very grateful for her care and support: “She is like a guardian angel who just showed up” (Patient 16). This question was not raised in one interview.
To improve the quality of care, patients suggested reducing waiting times and enhancing treatment in primary care. In addition, one patient mentioned that the role of the CHW could be helpful in treating other diseases: “I think it could be used for other treatments, not just CD—like cancers for example” (Patient 2).
3.2 People not supported by a CHW
The sample of people not supported by a CHW included six patients—five women and one man. Their median age was 48.5 years (IQR=40.0–56.9). Most were from Bolivia (five), with one from Ecuador. Their main occupations were domestic work (three), service (one), and human resources (one). This information was missing in one interview. Screening for CD was carried out in Spain (four), or in their country of origin (two). Within this group, people were diagnosed after blood donation (four), during a routine blood test (one), or through a voluntary screening (one). The most common comorbidity in this group was hypertension. Five people reported cardiac symptoms such as fatigue, tachycardia, hypertension, while one was asymptomatic. None had Chagas cardiomyopathy; their clinical presentation is the indeterminate form. In addition, two people mentioned having lived in rural areas and seeing the insects. This information was missing from the remaining interviews and focus groups. Three patients stated that their mothers also had CD. This information was missing from the other patients. Four patients mentioned having relatives with CD, and in three cases, acquaintances as well. Four patients had children, three of whom were tested, with one receiving a positive diagnosis.
They commonly knew that transmission could occur through bug bites (five) or through mother-to-child transmission (four). Only two identified blood transfusion, and none mentioned organ transplant or laboratory accident. This information was missing from one interviewee. Everyone identified cardiac symptoms of CD, but only three cited digestive symptoms: “It starts in the intestines, then it goes to the heart” (Patient 4). Knowledge of treatment was limited, and only one person mentioned its side effects. Regarding effectiveness, five recognized that taking treatment prevents disease progression: “I took the treatment to keep it sleep” (Patient 11). Their primary source of information was healthcare workers at Hospital La Paz-Carlos III. One person also mentioned searching on the internet. Two individuals started and completed the treatment. One person reported strong side effects, while the other reported none. Four patients had not been treated. Reasons for not seeking treatment included lack of time due to work (one case) and waiting for an appointment (one case). In two cases, this information was not available. Three patients advocated for the diagnosis and treatment of their relatives or acquaintances: “My mother had to be tested, my brother too” (Patient 8).
All participants reported negative feelings when they discovered that they had the disease, such as fear, anger, and sadness. Two patients noted that people in Spain do not know what CD is. They mentioned that this was also the case in Bolivia. At least four participants reported the death of a family member or relative due to CD, while three described negative experiences with treatment: “And I have it. Well, just recently, my sister also told me she has CD and is undergoing treatment there. And that’s it, the treatment … because I’m a little scared, anything can happen” (Patient 13). Regarding beliefs related to CD, four patients expressed the belief that it could be transmitted through direct contact with other people: “Of course, this is normal. If they tell you it’s a strange disease, you think, Uh, let’s see if I get infected…” (Patient 4). Additionally, two patients cited Ibome, an antiparisitic drug for animals, as an effective treatment for CD. All interviewers, except one, had delayed diagnosis or treatment: “For me, it was more like ‘I’m fine,’ so why would I do it?” (Patient 4).
All interviewees shared their diagnosis with close family and friends. Regarding the referral pathway, two were referred from primary care, while the rest went directly to tropical medicine units. All patients were very satisfied with the care received at Hospital La Paz-Carlos III: “Well, yes, if you’re listening, I am very grateful to Hospital Carlos III, to all the staff, who have cared for me and managed my Chagas treatment” (Patient 11). Four patients reported negative experiences with primary care, either related to CD or to other conditions.
The principal barriers to accessing the healthcare system faced by people not supported by a CHW are shown in Table 3:
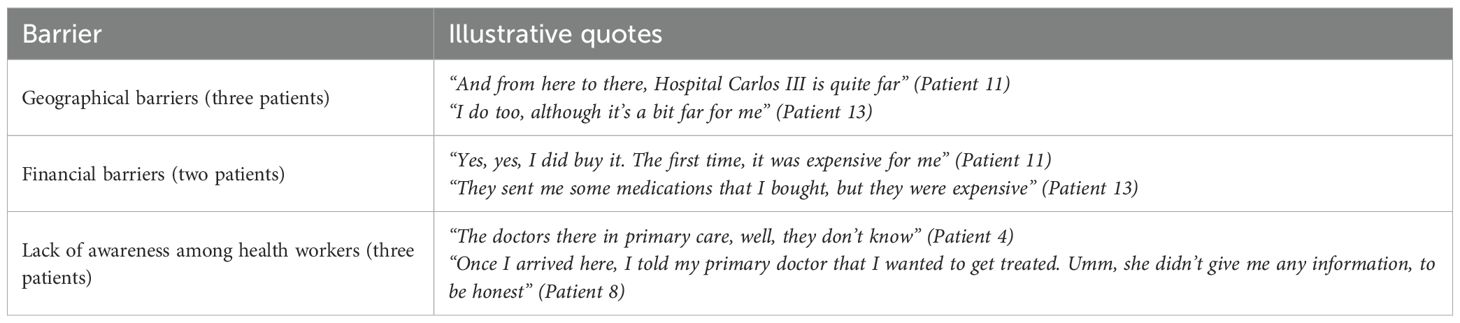
Table 3. Barriers to healthcare access in Spain for people not supported by a CHW.
Participants in this group could also have contact with the CHW, though not fulfilling criteria for full support (less than a month). Contact included information for five patients, facilitated treatment access for three, assisting one with adherence, and scheduling an appointment for another: “And it was thanks to her that she got me the appointment and everything started moving forward” (Patient 4). Four patients reported being very satisfied with the timely support provided by the CHW: “No, because if it wasn’t for them, for example, I wouldn’t have been able to do it” (Patient 4). Patients recommended that primary care workers improve their knowledge about CD (mentioned by three) and that more research be conducted on treatment options. One patient said: “I don’t know if other labs could invent new treatments. Overcoming those that cause allergies” (Patient 11).
3.3 Health workers
The sample of health workers consisted of nine individuals: seven women (78%) and two men (22%). Their median age was 46.1 years (IQR=39.8–52.3). The group included six internal medicine specialists, one cardiology specialist for CD, one nurse specialized in tropical medicine, and one auxiliary nurse. On average, these professionals had worked with imported pathologies in Spain, particularly CD, for 13.7 years. None had received specific training on CD during their academic studies. Thus, seven pursued a master’s degree or specialization in Tropical Medicine after completing their studies, while four traveled to endemic areas for international cross-border experience. Two professionals reported having no specific training on CD.
According to medical providers, patients were mainly Bolivian women aged 30–50, working in personal care and service industries, and with lower socioeconomic status. In terms of knowledge, all health workers perceived that patients had little knowledge about CD. This knowledge could increase if patients knew someone with the disease or have been referred from a tropical medicine unit: “Yes, they know, they know. I think what my colleagues in tropical medicine do, is essential; they have already explained everything to them (the patients)” (Professional 10).
Five health workers stated that they inform patients the treatment does not fully cure them, and four identified strong adverse drug reactions as a barrier leading to treatment interruption. They pointed out the patients’ primary source of information was their own family members. According to healthcare workers, patients’ reactions to diagnosis were influenced by their prior knowledge of the disease. If patients were already informed about the disease, they recognized it as a fatal disease and experienced fear, as mentioned in four interviews: “…well, you see, it’s very different with patients who come to me from tropical areas, who already know what CD is. They are afraid, very afraid” (Professional 2). When patients lacked knowledge of the disease and did not experience symptoms, they often denied having it, mainly due to stigma: “social stigma of poor people” (Professional 10).
Health providers believed that patients showed good adherence to treatment, as mentioned in four interviews. However, they recommended attending an imported tropical unit in case of any adverse reaction: “As soon as they notice itching on their body or any unusual sensation, we tell them to come here; we immediately suspend the treatment, reassess it, and if necessary, they can start another one” (Professional 4). Regarding referral pathways, health workers noted that patients arrive through primary care, donations, community screenings, or directly requesting an appointment at referral hospitals. Hospital 12 de Octubre, despite not being a specialized referral unit, also allows patients to request an appointment directly, without going through primary care: “In other words, we receive them from anywhere, (even when) and they are not sent by the general practitioner” (Professional 9). Of approximately 16 daily patients seen by the interviewed healthcare professionals, at least five had CD. During the interviews, healthcare workers emphasized their efforts to be flexible with patients, offering telephone consultations and one afternoon session per week to help overcome patients’ work-related restrictions.
From the healthcare workers’ perspective, the most common barriers to accessing the healthcare system faced by patients are summarized in Table 4.
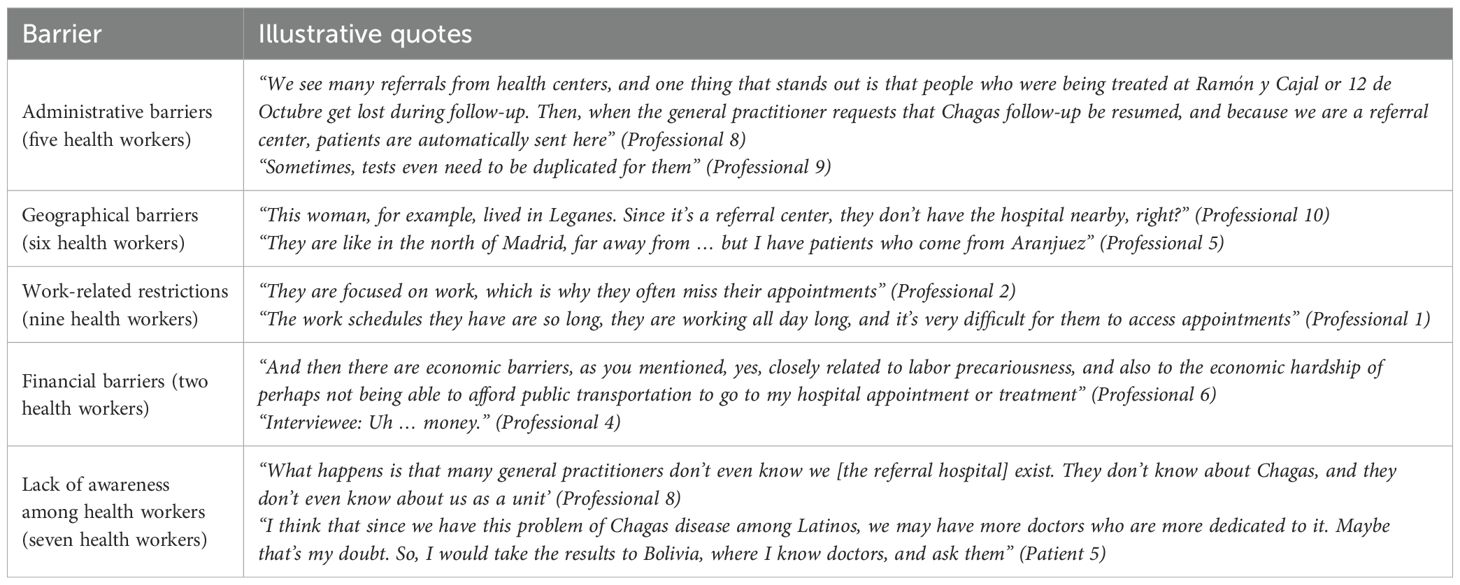
Table 4. Barriers to healthcare access in Spain from healthcare worker’s perspective.
Beyond these barriers, at least seven health workers mentioned linguistic differences: “They can’t express themselves even though they speak the same language” (Professional 8). In addition, three health providers cited cultural barriers: “There is a different concept of time and a different understanding of preventive health” (Professional 6). All healthcare professionals perceived a good relationship with patients: “They place considerable reliance on you, and you essentially act as their primary care provider” (Professional 3). While three mentioned that patients are grateful, two reported that at first, they may perceive them as somewhat “undisciplined” for not keeping their scheduled appointments—a perception that changes once they become aware of the barriers these patients face: “Sometimes it seems like they are very undisciplined patients, but actually they’re not, it’s just that they face so many obstacles to attend medical follow-ups” (Professional 7).
All healthcare providers recognized the role of the CHW, who works at the Mundo Sano Foundation. In addition, health workers knew of the Association Salud entre Culturas (five) and Médicos del Mundo (one), NGOs that conduct community screenings for CD. Regarding Salud entre Culturas, they highlighted its role in raising awareness about the disease and providing training for health workers in health facilities and universities. Some health workers participated in a working group in Madrid to develop a treatment protocol for CD, with the ai of including CD in primary care.
Service providers consistently highlighted the crucial role of the CHW in appointment management and patient support (cited in all interviews), as well as in providing essential information (mentioned by eight). In addition, one respondent mentioned the CHW’s role in providing emotional support, and three noted their role in improving access to treatment.
Five health workers believed that the CHW influenced patients’ treatment adherence, but two noted that this perception was biased: “Well, I think there’s a significant bias here, right? Maybe the people who aren’t offered support are already capable enough to adhere to the treatment on their own, you know?” (Professional 3). This points to a general tendency of people affected by CD to belong to lower socioeconomic sectors and, therefore, to be less equipped to deal with the complexities of the healthcare system in a migrant setting. Nevertheless, the role of CHWs in improving patient follow-up was acknowledged in seven interviews: “I think they contribute a lot, especially in making sure that patients keep their follow-up appointments” (Professional 5).
Health providers usually asked for the CHW’s support in providing information on CD and managing appointments for patients, who face cultural, administrative and age-related barriers. While most contacted her sporadically, one confirmed reaching out every time a CD diagnosis was made and once treatment began. This healthcare provider identified both moments as critical due to the accumulation of tests and appointments, which were sometimes incompatible with patients’ daily lives: “Because sometimes I feel like we’re here with our lab coats, and the person comes in and it’s a lot of information, because in the first consultation we tell them that they’ve been diagnosed with Chagas, what Chagas is, the tests they need to take, which are many, the treatment option, family screening, how they could have acquired it … And of course, it’s a lot of information” (Professional 8).
The Bolivian origin of the CHW was well received by health workers: “She is Bolivian, like them. It may not seem like much, but she understands, speaks their language and knows their difficulties” (Professional 3). According to all healthcare providers, the CHW role does not exist in the public health system in Madrid. However, they identified other helpers within the healthcare system in Madrid, such as volunteers or social workers, who they said could not fully meet the needs of people with CD: “There are social workers, and in La Paz we have social workers who do an excellent job, but they lack this … For example, a social worker may be very good at their job, but they don’t have that cultural understanding” (Professional 7). All health workers recognized the value of the CHW in reaching the community: “The role of CHW is like what other conditions call peer groups, in quotes, because she is a peer. She can share her experience, be part of the community, and be a success story” (Professional 6).
The main recommendations for improving the care of CD patients, made by five health workers, included community screening and training for health professionals, especially those in primary care. The aim was for primary care doctors to consider CD as a diagnostic option and refer patients to specialized hospitals: “From a support perspective, I think primary care doctors should have the opportunity to do joint sessions with them, both for training and to learn the follow-up procedures” (Professional 9). In addition, two health professionals suggested ensuring treatment availability in hospital pharmacies, not just in the pharmacy for foreign medicines, which is located in central Madrid and open only from 9 h to 14 h from Monday to Friday This limited schedule created an access barrier for both patients and practitioners, may of whom were unaware of how to obtain the medicines.
Other recommendations included reducing bureaucratic barriers for referrals and ensuring adequate health resources for patient care. Another recommedation was to integrate the CHW into the public health system (mentioned by two health workers), with the suggestion that the CHW could also work with patients suffering from other diseases: “Well, I think that … for Chagas patients, for the elderly, and I would say for people like us, because sometimes it’s really difficult with the system” (Professional 3). In one interview, a health worker suggested creating an association for people affected by CD in Madrid.
3.4 CHW
One CHW was interviewed, a 40-year-old woman of Bolivian origin with a degree as a nursing assistant. She has 10 years experience working with patients with CD. She was diagnosed as positive for CD in 2009 but did not complete the treatment. During her first pregnancy, she informed her gynecologist of her CD status and was referred to a tropical medicine unit, where she completed treatment. Her first child was screened and tested negative for CD. However, during her second pregnancy, despite her medical records, her child was not initially screened, and she had to specifically request it. Her second child also tested negative. This experience fostered her sensibility and solidarity toward others in her situation. Regarding her formal training on CD, she attended several workshops and completed specific CHW training through the School of Public Health in Valencia, which lasted approximately 300 h. The training was based on peer-to-peer learning approaches.
She described the profile of CD patients as Bolivians who grew up in rural areas and knew little about the disease. However, some had a family member who had died from CD. She oserved that some people explicitly refused to receive information about CD, while others spoke about it openly, with acceptance and resignatio their condition. She identified the main barriers faced by patients as work-related demands, administrative challenges, and a lack of awareness among primary health professionals. Additionally, she emphasized the importance of understanding patients’ circumstances: “At first, it may seem like they are not interested, but later, when you talk to the person and see their situation, it becomes understandable” (CHW).
From her perspective, her tasks include managing appointments, providing information, offering emotional and social support, and facilitating access to medication. She estimated that two to three individuals typically require her assistance each week. She also emphasized her role in promoting treatment adherence and conducting patient follow-ups: “Because I understand that sometimes it depends on the start of treatment, right? Because sometimes people let it go, forget about it, and when they want to start again, they’ve lost the papers, the prescription, and they don’t remember what they’re supposed to do” (CHW).
Regarding the barriers she faced within the healthcare system, the absence of an official collaboration agreement with certain facilities limited her formal recognition: “I go, but with the person, though I don’t introduce myself as a health agent because, at the end, if people know that you’re not family or that you’re asking for information—even if you have the person’s consent—there’s not as much trust due to data protection laws I understand that I’m not a well-known figure there” (CHW). At Hospital La Paz–Carlos III, despite the existing agreement, the CHW lacks a dedicated space to carry out her interventions, which hinders confidentiality and the ability to build greater trust with patients. Nevertheless, collaboration with some health providers is strong, particularly with auxiliary nurses who actively refer patients and coordinate efforts. Referrals with other professionals can sometimes be a challenge: “If there was a doctor in charge of reviewing patients, or if during the consultation these patients could be listed to call them or give them information” (CHW).
The CHW perceived a good relationship with patients affected by CD: “I think it’s quite good because people always appreciate having someone to talk to, even if it’s just to listen’ (CHW)”. The fact that she also has a CD has been a way for her to have a connection with patients: “It helps me; it inspires me to carry on because at some point it has affected my family” (CHW).
She recommended improving coordination with healthcare services in general, within the existing collaboration framework of the Madrid Health Service. Additionally, she emphasized the importance of recognizing her role within the healthcare system and suggested that it could be expanded to support other diseases: “The health agent could be integrated into the health system” (CHW). Finally, she repeatedly advocated for the creation of an association for people affected by Chagas in Madrid, similar to those in Murcia (AsaapechaMur) and Valencia (Achacova), with which she collaborates.
4 Discussion
The higher percentage of women with CD (63.16%) compared to men, as also perceived by health workers, aligns with findings from other studies (3, 5, 8, 28–33). This may be explained by women’s more frequent use of healthcare services (34). The median age of patients in this sample coincides with other studies, where most patients with CD were over 41 years old (5, 28, 29, 31). It could be linked to CD as a silent disease that begins to present symptoms after a long incubation period (4), or to the fact that patients in Madrid are mostly migrants in their mid-forties seeking better economic opportunities and sending remittances to their families in their home country (35).
Most participants in the study were of Bolivian origin, which is similar to other European cohorts, likely reflecting the higher prevalence of this disease in Bolivia (3, 5, 36). Some interviewees reported living in adobe houses in their country of origin which points to a likely route of CD infection (1, 12, 37). Around 50% of these migrants seek domestic and service employment, which is associated with demanding work schedules and a low socioeconomic status (4, 13, 33). This observation was also reported by health workers.
The finding that more than half of the patients (68%) were diagnosed in Spain may be linked to CD being a silent disease, which typically presenting symptoms in the chronic phase when patients arrive in the host country (4, 38, 39). Among them, diagnosis was typically made through targeted screening (whether motivated by pregnancy or not) or through donation, supporting the hypothesis that access to diagnosis in Spain is greater than in their country of origin. It should be noted that the routine CD screening for blood donors from high-endemic areas in Spain has been in place since 2005 (3). Additionally, the national consensus document for prenatal CD screening in Spain was approved in 2024 (38, 40). The fact that 63% were born to a mother with CD coincides with other studies, considering that patients come from areas with high endemicity (31). Furthermore, most patients reported having a family member or acquaintance with CD, as these close relatives also originated from endemic countries, consistent with findings from other studies (41).
The non-infectious comorbidities reported by patients with CD in this study align with the typical conditions observed in chronic patients at risk for cardiovascular disease (6). The infectious comorbidities, particularly strongyloides, may be explained by the fact that it is also a chronic infection that may remain asymptomatic for a long time and is highly prevalent in Latin American countries (42). It is worth noting that many screening campaigns in Spain test for both infectious diseases simultaneously.
Despite the higher prevalence of cardiac symptoms, the fact that none of the patients presented with Chagas cardiomyopathy is consistent with other studies, given that the indeterminate form is usually the most common clinical presentation (6, 8, 43, 44). The indeterminate form is frequently seen in the chronic phase of CD, which aligns with the median age of patients in this sample and the disease’s long incubation period (43). In addition, given the nonspecific manifestation, the diagnosis of acute CD is rarely made (6).
4.1 CD knowledge
The lack of knowledge about CD transmission beyond the vectorial route, cited by 89% of patients, and awareness of cardiac but not digestive symptoms align with findings from other studies (30, 31, 38, 44–46). In contrast, other studies reported a high level of theoretical knowledge about CD (46). This difference could be explained by prior awareness campaigns in the study area or whether it is an officially recognized endemic area, or the existence of a community health intervention program (5). In all cases, misinformation may prevent communities from adopting new health-related preventive behaviors (45). Some studies indicate that a poor understanding of CD is a major barrier to seeking care, especially in non-endemic countries where there are no general health education campaigns related to the disease (44).
Despite limited treatment knowledge, 47% of participants cited trypanocidal treatment side effects, often a barrier to beginning or completing treatment (6, 12, 18, 33, 47). Globally, around 7%–35% of adult patients with CD discontinue treatment due to the inappropriate management of side effects (6). This lack of knowledge about CD was also perceived by most health workers, confirming the absence of comprehensive information in the community and the limited perception of risk and education (30). Many programs in Latin America consider informing, educating, and communicating as strategic and essential for implementing CD community programs (13, 28, 30). This educational strategy should be culturally adapted to achieve true impact (48).
The patients pointed out that their main source of information was the staff at the Hospital La Paz–Carlos III who work in a tropical medicine unit. This may be explained by patients’ perception that primary care workers were not aware of the diagnosis, transmission, and treatment for CD, as also noted by other researchers (13, 30). This aligns with findings from a primary care study, where professionals emphasized that patients from endemic areas do not usually discuss CD with them (15). Conversely, health workers perceived family members as the primary source of information on CD for patients. Despite this discrepancy, patients reported gaining a deeper understanding of the disease after consulting specialists at the hospitals. These typical sources of information on CD—health providers and family members—are also mentioned in other studies (31).
Treatment was taken by 63% (12/19) of patients, both those supported by a CHW and those not supported. Medical opinion is divided on the circumstances in which to recommend treatment, since during the chronic phase is approximately 30%. Some studies indicated that treatment should be offered on an individual basis, and that certain patients may not be considered appropriate candidates due to age, disease severity, or comorbidities (14, 49–51). Physicians must take in account patients’ opinion. Despite 58% reporting side effects, 92% (11/12) completed treatment, demonstrating high adherence. Health workers also noted this strong adherence, linking it to greater disease awareness after appointments with patients. This perception is supported by other authors, who believe that ensuring adequate medical information and health system support will encourage patients to undergo screening and treatment (31).
By contrast, previous studies have shown that more than half of Bolivian patients with CD in Madrid did not begin or complete treatment (44). These differences may be associated with initiatives promoted in Madrid in recent years to address CD, including working groups and research, which have improved awareness of this disease among medical practitioners and patients. Strong adherence to treatment and improved awareness in recent years, could explain why 74% of patients have become advocates for the diagnosis and treatment of others in their community.
4.2 Perceptions, beliefs, emotions, and experiences related to CD
The negative feelings, especially fear, expressed by 74% of patients when diagnosed with CD are linked to stereotypical misconceptions, such as it being a rural phenomenon, affecting only the poor, and being inevitably fatal (5, 6, 18, 41, 44, 46, 52–54). The generational transfer of information, occurring only when CD is known by those around, plays an essential role in replicating behaviors and perpetuating these negative emotions (45). Experiences related to someone who has died of the disease or had a negative experience with treatment, both frequently mentioned, also reinforce rather than dispel these misconceptions. In addition, misconceptions about routes of transmission, also reported in other studies, contribute to these negative feelings (45, 55). By contrast, other studies with Bolivians with CD revealed that the disease was perceived as common and even relatively harmless, condition, given that many people are asymptomatic (56, 57). These differences may be explained by the fact that in countries with high endemicity, the presence of the disease may become normalized, with people accepting or resigning to it based on their life circumstances (18).
The fact that 89% denied the disease and delayed treatment may be linked to the stigma associated with CD, as well as to the experiences and health-related beliefs described previously (6). This stigma conveys association with death, misery, rejection, lack of hygiene, and social isolation, and has emerged as a major obstacle to receiving proper medical treatment (13, 15, 45, 52, 54, 58). This explains why most patients shared their CD status only with their closest social circle, as also reported in other studies (44). To address this stigma, some authors recommend involving social workers, mental health professionals, and community actors, including support groups (6).
4.3 Health system and health workers
Difficulties in testing availability were reported by at least 42% of patients who initially received a misdiagnosis, likely due to variability in test reliability, and the sensitivity and specificity of biomarkers, as also mentioned in other studies (14, 39, 52). Additionally, this percentage is similar to the results obtained by Gómez i Prat et al. (48), who reported an underdiagnosed rate of 56.4%. This percentage is lower than the rate in Spain in 2022 by Navarro et al. (36), which was estimated to be approximately 71%.
Healthcare in Spain is provided at two levels: hospitals and primary care facilities, where CD serological tests and treatments are available (54). The fact that 63% of patients went directly to tropical medicine units for screening, bypassing primary care, highlights the lack of CD awareness in primary care, despite its cost-effectiveness and accessibility (4, 6, 12, 13, 15, 33, 36, 44, 47). One possible explanation is that CD is often not included in traditional diagnostic and therapeutic pathways (3, 5, 33, 39). However, the ease of scheduling at hospitals facilitates sending patients directly there. Additionally, under referral pathways in Spain, blood donors and pregnant women diagnosed with CD, are always referred to a hospital facility (15).
The ratio of patients (5/16) with CD seen daily, reported by health workers, highlights CD as the most common imported parasitic infection in Spain, which has been the highest burden of the disease inEurope (11, 36). This underscores the importance of Spain’s membership in the Iberoamerican initiative for the interruption of vertical transmission of Chagas, sponsored by the Secretaria General Iberoamericana (SEGIB) (59).
The lack of specific training in CD during their studies, cited by all healthcare workers, explains why some physicians do not consider CD diagnosis, even among high-risk groups. This perception has been reported by other researchers (15, 54, 55, 57). According to Iglesias-Rus et al. (15) primary care health workers receive training focused on chronic diseases, which are commonly encountered in consultations, rather than on infectious diseases. Furthermore, there is a lack of funding for education and research on CD (14). It should be noted that for CHW, some workshops on CD may not be sufficient, as their training should be tailored to the specific tasks they are expected to perform (48). According to the Pan American Health Organization (PAHO), if these workshops addressed community needs, CHWs were considered to have received adequate training. However, CHW training needs follow up to ensure that knowledge is retained, and strategies to motivate them should also be in place (23, 24). The positive patient–provider relationships at Hospital La Paz-Carlos III reflect both the expertise of healthcare professionals and the support patients receive. This is fundamental for successful healthcare interventions, as noted in other studies (31). In contrast, 37% of patients reported negative experiences with primary care, citing the lack of knowledge and experience in this level already mentioned (15, 39, 54, 60). Training health primary workers and improving their confidence was identified as one of the main goals to be achieved (57, 60).
The most common barriers faced by patients, as reported by all interviewees and organized by prevalence, are:
1. Work-related barriers: This was identified as the most significant challenge, also cited in other studies (31, 54).
2. Lack of awareness and knowledge among healthcare workers: Lack of awareness, especially in primary care, poses a challenge for European doctors with little or no experience in detecting or managing CD (3, 9, 12, 20, 57). As cited by Iglesias-Rus et al. (15), many family physicians are unaware of the possibility of requesting a diagnosis testing, and they assume that treatment is not within the competence of primary care. In addition, they do not suspect CD in people coming from endemic countries (15). Several initiatives tried to address this barrier: the Coalition of Chagas (established in 2008), which unites stakeholders to improve CD advocacy, research, and access to diagnosis and treatment (61); the Chagas Platform (2015–2018), which focused on training primary care professionals, a key factor in scaling up interventions (7, 41, 62); and WHA Resolution 63.20 (2010), which emphasized the need to address all T. cruzi transmission routes and ensure appropriate medical care starting at the primary healthcare level (52).
3. Administrative barriers: Lengthy procedures within health systems have also been emphasized in other studies (13, 14).
4. Geographical barriers: The centralization of services, which also occurs in other countries including those in Latin America, can hinder access to diagnosis and treatment (28, 31, 33, 47, 54, 56). These barriers stem from historical inequalities, placing vulnerable groups, especially undocumented migrants, at higher risk of CD and limiting their access to healthcare (6, 12, 33, 41, 46, 52). As mentioned by Pinazo et al. (7), while centralizing care in specialized centers is more effective, it is less efficient in terms of sustainability and access. Specialized centers are limited in number and not always easily accessible from patients’ residence (7, 29).
5. Financial barriers: These have also been mentioned in other studies (14, 34, 56). In Spain, health expenditures related to treatment are partially covered by public funds, with patients paying a reduced proportion. Conversely, in many Latin American countries, including Bolivia, access to treatment is free, but patients must pay for other healthcare expenses such as doctors’ appointments and procedures in health facilities (2, 29), which result in higher overall costs. Patients from Latin America who had spent many years in Spain were usually not undocumented immigrants and therefore had access to healthcare (33).
In addition to these barriers, linguistic and cultural differences identified by health professionals are also mentioned by other authors (4, 33, 39, 46, 53, 63) highlighting the increased communication difficulties despite sharing Spanish as a language. Therefore, linguistic barriers are also influenced by class and educational differences (33). Additionally, the management of chronic diseases should move beyond biomedical approaches, considering patients’ emotional aspects to boost trust and motivation, and to avoid making them feel insecure or labeled as undisciplined (64). Social network barriers affect patients who have migrated to non-endemic countries, leaving them isolated from traditional and emotional support networks (6, 15, 18, 21). Furthermore, patients may hold perspectives on health and disease that differ considerably from the biomedical model dominant in European and US clinical settings (39). This becomes evident in the perspectives of medical providers, who evaluate patients as non-compliant—”undisciplined patients” as mentioned in the quotes above—and as reliant on the medical practitioner. There is an underlying expectation that patients should take responsibility for their own health, and those who fail to do so are labeled “undisciplined.” In Spain, health systems rarely provide support for the social and emotional challenges of living with CD (6).
The barriers faced by patients, particularly linguistic and cultural differences, encourage healthcare workers to collaborate with external resources beyond the public health system to improve service quality. Among these resources, all healthcare workers highlighted the role of the CHW from the Mundo Sano Foundation, likely due to their direct collaboration and the foundation’s active involvement with patients with CD in Spain, Latin America, and the US. The CHW aims to overcome some access barriers by engaging people who have not previously sought care, establishing cultural links, enhancing trust, and contributing to doctor–patient communication (48).
In a number of Spanish regions, such as Barcelona, community-based CD screening interventions are led by public hospitals in collaboration with private foundations or associations, as also reflected in this research (5, 54). It should be noted that, given that worldwide only approximately 10% of CD cases have been diagnosed, it is essential to establish screening protocols, focused primarily on childbearing women but also on all migrants from endemic areas, within primary health care in non-endemic countries such as Spain (11, 18).
4.4 CHW support
Considering the role of the CHW, both patients and healthcare professionals agree on its key values. The most common tasks included providing information, managing appointments, and supporting patients, all regarded as essential for the comprehensive management of CD. These tasks are similar to those described by WHO (25) and other authors, including identifying individuals and families at risk and carrying out basic interventions (24, 48, 65, 66). CHW activities vary between rural and urban areas, depending on whether they work closely with healthcare services. However, in all scenarios, the CHW requires close support and follow-up from health services, together with the collaboration of other social actors (23).
This multidisciplinary approach is essential for improving patient follow-up (5, 66). Although there was a group of individuals identified as not supported by a CHW, analysis of the interviews shows that once a patient becomes familiar with the CHW, they tend to seek occasional support to manage appointments, access treatment, or receive counseling. They benefited from the same interventions as those supported by a CHW.
Upon analyzing the patients who started treatment, a noticeable difference emerges between those supported by a CHW (69%) and those without support (33.3%). Although support is not necessary to start treatment, considering the potential bias noted by healthcare workers—who pointed out that supported patients are selected due to challenges—this highlights that for patients facing difficulties, support could make the difference between starting and not starting the treatment. These results should be interpreted considering that, in some cases, treatment may not be indicated by certain medical practitioners. Additionally, a possible explanation could be the lack of seamless integration of the CHW into the healthcare system, meaning that support during treatment (as a clinical concern) falls outside the scope of her work and depends on having a good relationship with clinical staff. Regarding follow-up adherence, the role of the CHW is clearer and indispensable, as highlighted by both patients and healthcare workers. Having made the necessary clarifications regarding the limitations of these observations, we nonetheless stress the relevance of the data emerging from this qualitative study, making a case for the importance of actors such as CHWs, who act as bridges between the healthcare system and the community.
Furthermore, in other settings, the interventions carried out by CHWs, especially at the community level, could enhance access to diagnosis (5, 7). Culturally tailored interventions—the adaptation of study designs, materials, and other components to reflect the cultural needs and preferences of a population—are most effective in increasing access to diagnosis and treatment (5, 38). These include the informal dissemination of information, and screening at community events, clubs, social organizations, waiting rooms, or embassies (52, 67).
Although healthcare providers recognize the key role of the CHW in supporting patients with CD, the process for requesting assistance remains unclear. This perception is also shared by the CHW. This may be because the CHW is not part of the public health system and there is no physical space at Hospital La Paz-Carlos III to locate her, despite the existing agreement. Some studies have also highlighted these barriers faced by CHWs, leading to the undervaluation of human capital and financial resources (24, 25). In the Community of Barcelona, the CHW role has been integrated into the public healthcare system, improving TB treatment adherence and facilitating CD diagnosis, among other outcomes (5, 68). The Bolivian origin of the CHW, who has also been diagnosed with CD, is crucial for building trust with patients as a peer counselor. Her origin also enables her to act as a cultural mediator, with an understanding of immigration and multicultural contexts.
Her strong relationship with patients, as recognized by healthcare providers and patients themselves, is based on shared experiences and histories, non-verbal communication skills, and her understanding of the Spanish context, which gives her prestige among peers. As noted by Goméz i Prat et al. (48), recruiting and selecting the most appropriate person for the CHW role is essential to ensure the sustainability, acceptability, and success of a community health strategy.
The nature of the study—a qualitative phenomenological design—prioritized depth over quantity of data. This imposes limitations on the capacity to generalize from what is a relatively small sample, determined by the network capacity of snowball sampling. However, given that the value of these data lies in its depth and multiplicity of meanings, and that it has been contextualized through comparative analysis of similar studies, the contribution it provides to understanding people’s barriers to healthcare, the role of the CHW, and healthcare providers’ perceptions of its merit are valuable contributions.
The key recommendations emerging from SIs and FGs include:
1. Facilitating access to treatment by optimizing referral pathways and improving the knowledge and involvement of primary care professionals.
2. Increasing the integration of the CHW into the public health system. Gómez i Prat et al. (48) highlighted that the CHW role can be beneficial in preventing and controlling other infectious diseases, an observation also noted in this research.
3. Creating an association of patients affected by CD in Madrid: This model has proven successful in other regions of Spain (55). Additionally, in 2009, the International Federation of Associations of People Affected by CD (FINDECHAGAS) was established, bringing together associations from the Americas, Europe, and the Western Pacific (18). These initiatives could improve patient awareness, encourage self-care, and offer social and emotional support (6, 55).
Our study has several limitations. Given its qualitative nature, participants were not randomly selected from the population, meaning the results may not be generalizable to all patients with CD. Additionally, there may have been a classification bias due to the referral process used, which could have led to differences in the profiles of patients who were accompanied by a CHW and those who were not. Recruiting people with CD, particularly those without CHW support, was challenging as the target population faced significant barriers, especially a lack of accurate information about the disease. In terms of the impact of the CHW on the initiation and adherence to treatment, the sample size was relatively small, and the supported and unsupported patients were not monitored for the same duration. Ultimately, further research is needed to gain a deeper understanding of these points.
5 Conclusion
This study confirms that CD remains a significant health problem among Latin-American populations in non-endemic countries such as Spain. The findings confirm that despite repeated information, communication, and education campaigns, knowledge of CD transmission, symptoms, and treatment among patients and primary care health workers remains limited. This reinforces the need for repeated and targeted educational interventions; as well as addressing the high prevalence of stigma, misconceptions, and negative emotions that influence delayed treatment-seeking behavior. Barriers within health systems, including administrative challenges, geographical limitations, and work-related constraints, further complicate the management of CD. These barriers often represent the most difficult obstacles for patients, as they are imbued with power relations linked to social and ethnic categories that are not easily overcome. As a cultural translator, the role of the CHW was critical in facilitating access to care, improving adherence, and providing culturally tailored support, though not specifically in patient treatment adherence. This hints at the broader implications of power relations within health systems, as well as the importance of soft skills such as empathy and shared life experiences relevant for fluid communication strategies around health-related issues. Although further studies should be conducted to gather more evidence, efforts to improve CD management should focus on strengthening primary care involvement, improving health worker training, optimizing referral pathways, and increasing CHW support within structured health programs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee for Research with Medicinal Products at the University Hospital La Paz (Spain) on 1 November 2021 (HULP: PI-4971). The studies were conducted in accordance with local legislation and institutional requirements. Participants provided their written informed consent to participate in this study.
Author contributions
CJ: Conceptualization, Investigation, Software, Formal analysis, Writing – review & editing, Validation, Methodology, Writing – original draft. MA: Conceptualization, Methodology, Validation, Writing – review & editing, Resources, Investigation. MS: Supervision, Writing – review & editing, Resources, Validation. ML: Investigation, Resources, Writing – review & editing, Conceptualization, Validation. MD: Validation, Writing – review & editing. Rd: Writing – review & editing, Validation. Fd: Validation, Writing – review & editing. AA: Validation, Supervision, Writing – review & editing, Investigation, Methodology, Formal analysis. MG: Writing – review & editing, Conceptualization, Investigation, Resources, Validation, Methodology, Supervision.
Funding
The authors declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
We extend our gratitude to the patients who participated in the study for their patience and trust, to the healthcare workers involved in the project for their dedication and confidence, and to the CHW of the Mundo Sano Foundation, whose insights were crucial to the development of this study.
Conflict of interest
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2025.1632961/full#supplementary-material
References
1. Chagas disease (2025). Available online at: https://www.who.int/news-room/fact-sheets/detail/chagas-disease-[american-trypanosomiasis (Accessed February 16, 2025).
2. Cucunubá ZM, Manne-Goehler JM, Díaz D, Nouvellet P, Bernal O, Marchiol A, et al. How universal is coverage and access to diagnosis and treatment for Chagas disease in Colombia? A health systems analysis. Soc Sci Med febrero. (2017) 175:187–98. doi: 10.1016/j.socscimed.2017.01.002
3. Castaldo M, Cavani A, Segneri MC, Costanzo G, Mirisola C, and Marrone R. Anthropological study on Chagas Disease: Sociocultural construction of illness and embodiment of health barriers in Bolivian migrants in Rome, Italy. PLoS One. (2020) 15:e0240831. doi: 10.1371/journal.pone.0240831
4. Gold M. Health, migration, and NTDs: an anthropological view. Med Anthropology. (2021) 40:491–6. doi: 10.1080/01459740.2021.1953494
5. Gómez I Prat J, Peremiquel-Trillas P, Claveria Guiu I, Choque E, Oliveira Souto I, Serre Delcor N, et al. A community-based intervention for the detection of Chagas disease in Barcelona, Spain. J Community Health. (2019) 44:704–11. doi: 10.1007/s10900-019-00684-z
6. Echeverría LE, Marcus R, Novick G, Sosa-Estani S, Ralston K, Zaidel EJ, et al. WHF IASC roadmap on Chagas disease. Glob Heart. (2020) 15:26. doi: 10.5334/gh.484
7. Pinazo MJ, Rojas-Cortez M, Saravia R, Garcia-Ruiloba W, Ramos C, Pinto Rocha JJ, et al. Results and evaluation of the expansion of a model of comprehensive care for Chagas disease within the National Health System: The Bolivian Chagas network. PLoS Negl Trop Dis. (2022) 16:e0010072. doi: 10.1371/journal.pntd.0010072
8. Pérez-Ayala A, Pérez-Molina JA, Norman F, Navarro M, Monge-Maillo B, Díaz-Menéndez M, et al. Chagas disease in Latin American migrants: a Spanish challenge. Clin Microbiol Infect. (2011) 17:1108–13. doi: 10.1111/j.1469-0691.2010.03423.x
9. Ribeiro I, Sevcsik AM, Alves F, Diap G, Don R, Harhay MO, et al. New, improved treatments for Chagas disease: from the R&D pipeline to the patients. PLoS Negl Trop Dis. (2009) 3:e484. doi: 10.1371/journal.pntd.0000484
10. Losada Galván I, Alonso-Padilla J, Cortés-Serra N, Alonso-Vega C, Gascón J, and Pinazo MJ. Benznidazole for the treatment of Chagas disease. Expert Rev Anti Infect Ther. (2021) 19:547–56. doi: 10.1080/14787210.2021.1834849
11. Navarro M, Navaza B, Guionnet A, and López-Vélez R. Chagas disease in Spain: need for further public health measures. PLoS Negl Trop Dis. (2012) 6:e1962. doi: 10.1371/journal.pntd.0001962
12. Marchiol A, Forsyth C, Bernal O, Valencia Hernández C, Cucunubá Z, Pachón Abril E, et al. Increasing access to comprehensive care for Chagas disease: development of a patient-centered model in Colombia. Rev Panam Salud Publica. (2017) 41:e153. doi: 10.26633/RPSP.2017.153
13. Avaria A, Ventura-Garcia L, Sanmartino M, and van der Laat C. Population movements, borders, and Chagas disease. Mem Inst Oswaldo Cruz. (2022) 117:e210151. doi: 10.1590/0074-02760210151
14. Manne-Goehler J, Reich MR, and Wirtz VJ. Access to care for Chagas disease in the United States: a health systems analysis. Am J Trop Med Hyg. (2015) 93:108–13. doi: 10.4269/ajtmh.14-0826
15. Iglesias-Rus L, Romay-Barja M, Boquete T, Benito A, and Blasco-Hernández T. The role of the first level of health care in the approach to Chagas disease in a non-endemic country. PLoS Negl Trop Dis. (2019) 13:e0007937. doi: 10.1371/journal.pntd.0007937
16. INE. INEbase/Demografía y población/Padrón/Estadística del Padrón continuo/Últimos datos(2024). Available online at: https://ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177012&menu=ultiDatos&idp=1254734710990 (Accessed December 14, 2024).
17. Salud Entre Culturas, Fundación Mundo Sano. Evaluación de la eficiencia de las campañas de cribado comunitario de la enfermedad de Chagas en Madrid. (2024). Available online at: https://www.saludentreculturas.es/wp-content/uploads/2024/04/Evaluacion-de-la-eficiencia-de-las-campanas-de-cribado-comunitario-de-la-enfermedad-de-chagas-en-Madrid-2014-2017-Espanol.pdf.
18. Sanmartino M, Saavedra AA, Prat J, Barba MCP, and Albajar-Viñas P. Que no tengan miedo de nosotros:el Chagas según los propios protagonistas. Interface. (2015) 19:1063–75. doi: 10.1590/1807-57622014.1170
19. Bischoff A, Schneider M, Denhaerynck K, and Battegay E. Health and ill health of asylum seekers in Switzerland: an epidemiological study. Eur J Public Health. (2009) 19:59–64. doi: 10.1093/eurpub/ckn113
20. Sangaramoorthy T. Liminal living: everyday injury, disability, and instability among migrant Mexican women in Maryland’s seafood industry. Med Anthropol Q. (2019) 33:557–78. doi: 10.1111/maq.12526
21. Gilgen D, Maeusezahl D, Salis Gross C, Battegay E, Flubacher P, Tanner M, et al. Impact of migration on illness experience and help-seeking strategies of patients from Turkey and Bosnia in primary health care in Basel. Health Place. (2005) 11:261–73. doi: 10.1016/j.healthplace.2004.04.002
22. Wild V, Zion D, and Ashcroft R. Health of migrants: approaches from a public health ethics perspective. Public Health Ethics. (2015) 8:107–9. doi: 10.1093/phe/phv017
23. Agente-comun-salud-guia-facilitador-LR.pdf(2025). Available online at: https://www3.paho.org/hq/dmdocuments/2011/Agente-Comun-Salud-Guia-Facilitador-LR.pdf (Accessed February 21, 2025).
24. Fundación EPES y Decisión de Atención Primaria. Manual de apoyo a la incorporación de agentes comunitarios en salud en los equipos de los cecosf.
25. Organización Mundial de la Salud. Directrices de la OMS sobre política sanitaria y apoyo al sistema para optimizar los programas de agentes de salud comunitarios. Ginebra: Organización Mundial de la Salud (2019). 112 p. Available online at: https://iris.who.int/handle/10665/326553 (Accessed February 21, 2025).
26. Rahimi S and Khatooni M. Saturation in qualitative research: An evolutionary concept analysis. Int J Nurs Stud Adv. (2024) 6:100174. doi: 10.1016/j.ijnsa.2024.100174
27. Organization PAH and de la Salud OM. Adherencia a los tratamientos a largo plazo: pruebas para la acción. In: Adherence to the long-term treatments: tests for the action Washington, DC: PAHO/WHO (2004). Available online at: https://iris.paho.org/handle/10665.2/41182 (Accessed December 4, 2024).
28. Monroy MC, Penados D, Pineda J, Ruiz EL, Agreda EO, Alcantara B, et al. A multidisciplinary, collaborative, inter-agency and comprehensive approach for the control of Chagas Disease as a public health problem in Guatemala. Acta Trop. (2022) 225:106157. doi: 10.1016/j.actatropica.2021.106157
29. Herazo R, Rey A, Galvão D, Camargo MM, Pinzón NJC, Sanchez ACR, et al. Analysis of the costs incurred by patients with Chagas disease: The experience in endemic municipalities in Colombia. Acta Trop. (2023) 245:106963. doi: 10.1016/j.actatropica.2023.106963
30. Herrera C, Bernabé KJ, Dumonteil E, DeCuir J, Thompson JM, Avendano M, et al. Assessment of community awareness and screening of Chagas disease in the Latin American community of greater new Orleans. Trop Med Infect Dis. (2023) 8:515. doi: 10.3390/tropicalmed8120515
31. Navarro M, Berens-Riha N, Hohnerlein S, Seiringer P, von Saldern C, Garcia S, et al. Cross-sectional, descriptive study of Chagas disease among citizens of Bolivian origin living in Munich, Germany. BMJ Open. (2017) 7:e013960. doi: 10.1136/bmjopen-2016-013960
32. Ouaarab Essadek H, Claveria Guiu I, Caro Mendivelso J, Sulleiro E, Pastoret C, Navarro M, et al. Cribado in situ de la enfermedad de Chagas con una intervención comunitaria: ¿puede mejorar la accesibilidad al diagnóstico y al tratamiento? Gaceta Sanitaria. (2017) 31:439–40. doi: 10.1016/j.gaceta.2017.04.007
33. Forsyth CJ, Hernandez S, Flores CA, Roman MF, Nieto JM, Marquez G, et al. «It’s like a phantom disease»: patient perspectives on access to treatment for Chagas disease in the United States. Am J Trop Med Hyg. (2018) 98:735–41. doi: 10.4269/ajtmh.17-0691
34. Ayuso-Álvarez A, Ortiz C, Fontán J, Rodríguez-Blázquez C, Damián J, López-Cuadrado T, et al. Predictive value of the Global Activity Limitation Indicator [GALI] on all-cause mortality. Public Health. (2024) 230:6–11. doi: 10.1016/j.puhe.2024.02.006
35. Requena-Méndez A, Bussion S, Aldasoro E, Jackson Y, Angheben A, Moore D, et al. Cost-effectiveness of Chagas disease screening in Latin American migrants at primary health-care centres in Europe: a Markov model analysis. Lancet Glob Health. (2017) 5:e439–47. doi: 10.1016/S2214-109X(17)30073-6
36. Navarro M, Reguero L, Subirà C, Blázquez-Pérez A, and Requena-Méndez A. Estimating chagas disease prevalence and number of underdiagnosed, and undertreated individuals in Spain. Travel Med Infect Dis. (2022) 47:102284. doi: 10.1016/j.tmaid.2022.102284
37. Bates BR, Carrasco-Tenezaca M, Mendez-Trivino AM, Mendoza LE, Nieto-Sanchez C, Baus EG, et al. Identifying barriers and facilitators for home reconstruction for prevention of Chagas disease: an interview study in rural Loja province, Ecuador. Trop Med Infect Dis. (2023) 8:228. doi: 10.3390/tropicalmed8040228
38. Monge-Maillo B and López-Vélez R. Challenges in the management of Chagas disease in Latin-American migrants in Europe. Clin Microbiol Infect. (2017) 23:290–5. doi: 10.1016/j.cmi.2017.04.013
39. Forsyth C, Meymandi S, Moss I, Cone J, Cohen R, and Batista C. Proposed multidimensional framework for understanding Chagas disease healthcare barriers in the United States. PloS Negl Trop Dis. (2019) 13:e0007447. doi: 10.1371/journal.pntd.0007447
40. Ministerio de Sanidad. Documento de consenso para el cribado prenatal de la enfermedad de Chagas. (2024). Available online at: https://www.sanidad.gob.es/areas/promocionPrevencion/cribado/cribadoPrenatal/enfermedadesInfecciosas/docs/Documentoconsensocribadoprenatal_enfermedadChagas.pdf.
41. Pereiro AC and Gold S. Building an innovative Chagas disease program for primary care units, in an urban non- endemic city. BMC Public Health. (2019) 19:904. doi: 10.1186/s12889-019-7248-5
42. Rodari P, Tamarozzi F, Tais S, Degani M, Perandin F, Buonfrate D, et al. Prevalence of Chagas disease and strongyloidiasis among HIV-infected Latin American immigrants in Italy – The CHILI study. Travel Med Infect Dis. (2022) 48:102324. doi: 10.1016/j.tmaid.2022.102324
43. Nascimento BR, Naback ADN, Santos BMP, Geissbühler Y, Demacq C, Quijano M, et al. Prevalence of clinical forms of Chagas disease: a systematic review and meta-analysis – data from the RAISE study. Lancet Regional Health – Americas. (2024) 30. Available online at: https://www.thelancet.com/journals/lanam/article/PIIS2667-193X[24]00008-5/fulltext (Accessed February 16, 2025).
44. Romay-Barja M, Iglesias-Rus L, Boquete T, Benito A, and Blasco-Hernández T. Key Chagas disease missing knowledge among at-risk population in Spain affecting diagnosis and treatment. Infect Dis Poverty. (2021) 10:55. doi: 10.1186/s40249-021-00841-4
45. Mora-Criollo P, Carrasco-Tenezaca M, Casapulla S, Bates BR, and Grijalva MJ. A qualitative exploration of knowledge of Chagas disease among adolescents in rural Ecuador. Rural Remote Health. (2023) 23:6796. doi: 10.22605/RRH6796
46. Iglesias Rodríguez IM, Mizukami S, Manh DH, Thuan TM, Justiniano HA, Miura S, et al. Knowledge, behaviour and attitudes towards Chagas disease among the Bolivian migrant population living in Japan: a cross-sectional study. BMJ Open. (2020) 10:e032546. doi: 10.1136/bmjopen-2019-032546
47. Klein K, Burrone MS, Alonso JP, Ares LR, Martí SG, Lavenia A, et al. Strategy to improve access to etiological treatment of Chagas disease at the first level of care in Argentina. Rev Panam Salud Publica. (2017) 41:e20. doi: 10.26633/RPSP.2017.20
48. Gómez I Prat J, Alguacil HM, Pequeño Saco S, Ouaarab Essadek H, Montero I Garcia J, Catasús I Llena O, et al. Implementation of a community-based public model for the prevention and control of communicable diseases in migrant communities in Catalonia. Trop Med Infect Dis. (2023) 8:446. doi: 10.3390/tropicalmed8090446
49. Hospital Universitario la Paz. Protocolo multidisciplinar de diagnóstico, tratamiento y seguimiento en la enfermedad de Chagas. (2016).
50. Jimenez A and Winokur EJ. Chagas disease cardiomyopathy. Dimens Crit Care Nurs. (2023) 42:202–10. doi: 10.1097/DCC.0000000000000590
51. de Sousa AS, Vermeij D, Ramos AN, and Luquetti AO. Chagas disease. Lancet. (2024) 403:203–18. doi: 10.1016/S0140-6736(23)01787-7
52. Sanmartino M, Forsyth CJ, Avaria A, Velarde-Rodriguez M, Gómez i Prat J, and Albajar-Viñas P. The multidimensional comprehension of Chagas disease. Contributions, approaches, challenges and opportunities from and beyond the Information, Education and Communication field. Mem Inst Oswaldo Cruz. (2022) 117:e200460. doi: 10.1590/0074-02760200460
53. Aith FMA, Forsyth C, and Shikanai-Yasuda MA. Chagas disease and healthcare rights in the Bolivian immigrant community of São Paulo, Brazil. Trop Med Infect Dis. (2020) 5:62. doi: 10.3390/tropicalmed5020062
54. Iglesias-Rus L, Boquete T, Romay-Barja M, Benito A, Jordan B, and Blasco-Hernández T. Diagnostic pathways of Chagas disease in Spain: a qualitative study. BMC Public Health. (2023) 23:332. doi: 10.1186/s12889-022-14938-4
55. Damasceno RF, Sabino EC, Ferreira AM, Ribeiro ALP, Moreira HF, Prates TEC, et al. Challenges in the care of patients with Chagas disease in the Brazilian public health system: A qualitative study with primary health care doctors. PLoS Negl Trop Dis. (2020) 14:e0008782. doi: 10.1371/journal.pntd.0008782
56. Pinazo MJ, Pereiro A, Herazo R, Chopita M, Forsyth C, Lenardón M, et al. Interventions to bring comprehensive care to people with Chagas disease: Experiences in Bolivia, Argentina and Colombia. Acta Trop. (2020) 203:105290. doi: 10.1016/j.actatropica.2019.105290
57. Parisi S, Navarro M, Du Plessis JD, Shock JP, Apodaca Michel B, Lucuy Espinoza M, et al. «We have already heard that the treatment doesn’t do anything, so why should we take it?»: A mixed method perspective on Chagas disease knowledge, attitudes, prevention, and treatment behaviour in the Bolivian Chaco. PloS Negl Trop Dis. (2020) 14:e0008752. doi: 10.1371/journal.pntd.0008752
58. Batista C, Forsyth CJ, Herazo R, Certo MP, and Marchiol A. A four-step process for building sustainable access to diagnosis and treatment of Chagas disease. Rev Panam Salud Publica. (2019) 43:e74. doi: 10.26633/RPSP.2019.74
59. SEGIB. Iniciativa Iberoamericana sobre Chagas Congénito: “Ningún bebé con Chagas: el camino hacia nuevas generaciones libres de Chagas”. SEGIB. Available online at: https://www.segib.org/programa/iniciativa-iberoamericana-sobre-chagas-congenito-ningun-bebe-con-chagas-el-camino-hacia-nuevas-generaciones-libres-de-chagas/ (Accessed March 2, 2025).
60. Klein K, Roberti J, Rouvier M, Belizan M, Cafferata ML, Berrueta AM, et al. Design and feasibility of an implementation strategy to address Chagas guidelines engagement focused on attending women of childbearing age and children at the primary healthcare level in Argentina: a pilot study. BMC Prim Care. (2022) 23:277. doi: 10.1186/s12875-022-01886-6
61. Coalición Chagas. Coalición Chagas(2025). Available online at: https://coalicionchagas.org/ (Accessed March 6, 2025).
62. Chagas clinical research platform | DNDi(2011). Available online at: https://dndi.org/global-networks/chagas-platform/ (Accessed March 6, 2025).
63. Burckhardt AQ, Revollo HW, Collazos Sánchez F, Visiers Würth C, and El Harrak J. La mediación intercultural sociosanitaria: implicaciones y retos. Norte Salud Ment. (2009) 8:56–66.
64. Figueredo Borda N. Compañero de vida: enfermedad crónica. Un estudio de caso. Index Enfermería. (2014) 23:46–50. doi: 10.4321/S1132-12962014000100010
65. Paula TCS, Chagas C, Noto AR, Formigoni MLOS, Pereira TV, and Ferri CP. Brief interventions for older adults [BIO] delivered by non-specialist community health workers to reduce at-risk drinking in primary care: a study protocol for a randomised controlled trial. BMJ Open. (2021) 11:e043918. doi: 10.1136/bmjopen-2020-043918
66. García GSM, de Souza EA, de Araújo VM, Macedo MSS, de Andrade RMA, Ferreira PR da S, et al. Territory, neglected diseases and the action of community and endemic combat agents. Rev Saude Publica. (2022) 56:27. doi: 10.11606/s1518-8787.2022056003730
67. Gold M, Jackson Y, and Parrat D. Chagas disease is a low health priority among high-risk Latin American migrants in Geneva, a qualitative study. J Migration Health. (2024) 10:100239. doi: 10.1016/j.jmh.2024.100239
68. El papel de los Agentes Comunitarios de Salud en el control de la tuberculosis en Barcelona – Fundacio unitat d’investigació en tuberculosis a Barcelona(2025). Available online at: https://www.uitb.cat/el-papel-de-los-agentes-comunitarios-de-salud-en-el-control-de-la-tuberculosis-en-barcelona/ (Accessed March 27, 2025).
Keywords: Chagas disease, community health workers, health system barriers, migrant health, neglected tropical diseases
Citation: Juan Jimenez C, Arsuaga Vicente M, Santamaría Seijas M, Lago Nuñez M, Díaz Menéndez M, de Miguel Buckley R, de la Calle-Prieto F, Ayuso_Alvarez AM and Gold M (2025) “A guardian angel that just appeared”: the impact of a community health worker in supporting treatment adherence and follow-up for Chagas disease patients. Front. Trop. Dis. 6:1632961. doi: 10.3389/fitd.2025.1632961
Received: 21 May 2025; Accepted: 15 September 2025;
Published: 07 October 2025.
Edited by:
Daba Abdissa, Jimma University, EthiopiaReviewed by:
Elham Kazemirad, Tehran University of Medical Sciences, IranSandra Helena Suescún Carrero, University of Boyaca, Colombia
Copyright © 2025 Juan Jimenez, Arsuaga Vicente, Santamaría Seijas, Lago Nuñez, Díaz Menéndez, de Miguel Buckley, de la Calle-Prieto, Ayuso_Alvarez and Gold. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Juan Jimenez, Y3Jpc3RpbmFqdWFuQGFuZXN2YWQub3Jn
†ORCID: Cristina Juan Jimenez, orcid.org/0000-0003-1162-9595
Marta Arsuaga Vicente, orcid.org/0000-0001-5522-3728
Rosa de Miguel Buckley, orcid.org/0000-0003-2749-818X
Fernando de la Calle-Prieto, orcid.org/0000-0003-2544-3492
Ana M. Ayuso_Alvarez, orcid.org/0000-0002-6731-0412
Marina Gold, orcid.org/0000-0002-9826-5255