Abstract
Background:
Schistosomiasis is a Neglected Tropical Disease of public health importance that is endemic in parts of Africa. With Ghana being part of such areas, it is necessary to assess knowledge, attitude, and preventive methods of schistosomiasis among nursing and midwifery students in the Hohoe Nursing and Midwifery Training College considering the endemicity of the disease in some parts of the region.
Methods:
A cross-sectional analytical design was used for the investigation knowledge, attitude, and preventive methods of schistosomiasis among nursing and midwifery college students in the Hohoe municipality. STATA 17 was used for analysis and descriptive statistics such as frequencies, proportions, percentages, averages, and standard deviation was utilized to analyze numerical data. Demographic factors associated to respondents’ knowledge, attitudes, and practices were analyzed using logistic regression.
Results:
Good knowledge was 84.1% with media being the main source of information on schistosomiasis. There was moderately good attitude of 54.6% towards schistosomiasis. However, Interest in participating in future schistosomiasis prevention and control activities was high (91.7%). Key factors significantly associated with knowledge included Age (AOR = 2.90; 95% CI: 1.60–5.20; p < 0.001), Ethnicity (AOR = 2.00; 95% CI: 1.02–3.80). Preventive practices were strong (90.6%), with Praziquantel recognized as the main treatment.
Conclusion:
While students had good knowledge and practices, attitudes were less favorable. Strengthening educational interventions within nursing and midwifery curricula and enhancing student participation in control programs could further improve schistosomiasis prevention.
Introduction
Schistosomiasis, a parasitic infection classified as a Neglected Tropical Disease (NTD), poses significant public health challenges. The disease is prevalent across 78 tropical and subtropical nations, with global estimates suggesting around 250 million infections. Notably, over 90% of these cases are concentrated in Sub-Saharan Africa (1). Schistosomiasis ranks only second to malaria amongst the most devastating human parasitic diseases and remains a public health threat in several parts of the world. This is particularly the case in sub-Saharan Africa, where schistosomiasis is the deadliest neglected tropical disease (NTD) after snakebite envenomation, killing an estimated 2,80,000 people each year. Schistosomiasis is especially prevalent in poor communities with limited access to safe water and adequate sanitation and mostly affects communities exposed to these conditions, particularly agricultural and fishing populations, as well as women doing domestic chores involving infested water, such as washing clothes and dishes. Inadequate hygiene and contact with infested water render children, in particular, vulnerable to infection (2).
Schistosomiasis has historically been endemic in parts of the Caribbean, Asia, and the Americas, with varying prevalence influenced largely by the distribution of freshwater snails that serve as intermediate hosts. In the Caribbean, cases were widespread in the early 20th century (3), while in Asia, countries such as China and the Philippines remain major foci (S. mekongi), though Japan successfully eliminated the disease through environmental management and socioeconomic development (4). In the Americas, endemic areas persist in Brazil, Venezuela, and several Caribbean islands, with risks of expansion due to the broad distribution of snail hosts (5).
In Sub-Saharan Africa, schistosomiasis is currently treated mostly through mass administration of praziquantel, and the majority of information is disseminated using this treatment model (6). In Ghana, for instance, approximately 25,000 schistosomiasis cases were reported and entered into the Ghanaian District Health Information Management System (DHIMS) in 2010. Schistosomiasis is endemic in most sub-Saharan African countries, including Ghana, where the need for effective control involving preventive chemotherapy was indicated by the WHO. Mass drug administration commenced in 2008 and has continued since then in Ghana, but the country remains highly endemic (7).
The prevention of disease depends heavily on health education for high-risk populations. As future healthcare providers, nursing and midwifery students should have sufficient knowledge about different diseases, including schistosomiasis, which is a neglected tropical disease that affects millions of people worldwide. By assessing their knowledge and attitude towards schistosomiasis, we can identify areas where they need more education and training. This study seeks to examine the knowledge, attitude, and preventive methods of schistosomiasis among nursing and midwifery students in the Hohoe Nursing and Midwifery Training College.
Methods
Study design
This study used a cross-sectional analytical quantitative study approach. This methodology was chosen because data was gathered at one point in time and utilized to assess knowledge, attitude and preventive methods of schistosomiasis among nursing and midwifery students in the Hohoe Nursing and Midwifery Training College.
Study site description
This research was carried out in the Hohoe municipality of Ghana’s Volta region. The Municipality has a total land area of 1,172 km2, which is 5.6 percent of the land area of the region. It is located at longitude 00 15’E and 00 45’E and latitude 6o 45’N and 7o 15’N and lies almost in the heart of the region. It shares borders with the Republic of Togo on the east, forming part of Ghana’s international border; on the southeast by the Afadzato district and southwest by Kpando Municipality; on the north with Jasikan district; and the northwest with the Biakoye districts. Its capital, Hohoe, is about 78 kilometers from Ho, the regional capital, and 220km from Accra, the national capital. According to Volume 3A – “Population of Regions and Districts” in the 2021 Ghana Population and Housing Census, the population of Hohoe Municipal District is 114,472 as of the 2021 census [Volta (Region, Ghana) - Population Statistics, Charts, Map and Location, n.d.] (8). Annual rainfall is between 1,016mm- 1,210mm. The presence of the Volta lake in the region is makes schistosomiasis endemic in some areas around the volta basin. There is 4-5months dry season between November and April. Temperatures are high throughout the year and range from 26°C in the coolest months to about 32°C in the hottest months. The Municipality falls within the forest-savannah transitional ecological zone (9). Hohoe Nursing and Midwifery Training College is a tertiary health institution in Ghana under the Ministry of Health and accredited by the Nurses and Midwifery Council (NMC). The College has seen rapid growth in recent years, with total student enrollment rising from 240 in 2020 to about 611 in 2023, including 267 newly matriculated students that year. It offers a wide range of programs at the basic, post-basic, and certificate levels. Basic programs include diplomas in Registered General Nursing, Registered Midwifery (females only), Registered Mental Nursing, and Registered Community Health Nursing, as well as certificates in areas such as Community Health, Environmental Health, and Clinical Health Care. Post-basic programs, often run in collaboration with other national training centers, provide specialist training in fields like ophthalmic nursing, peri-operative nursing, public health nursing, critical care, and anesthesiology. As a tertiary institution, Hohoe NMTC awards diplomas and certificates that prepare students for professional roles in nursing, midwifery, and allied health, contributing to Ghana’s broader health workforce development.
Sample size determination
The sample size proposed by Cochran was used to determine the sample size for this study, which is as follows:
An estimated prevalence rate of 50% was used to estimate the minimum sample size since the actual prevalence rate of schistosomiasis in Hohoe could not be found
where, n =sample size
Z= Reliability of coefficient corresponding to a 95% confidence interval (1.96)
P= estimated proportion of outcome of interest % = 50%
d=margin of error (0.05).
Expecting a non-response rate of 5%, n= (384×0.05) +384 = 403
Therefore, 403 respondents were recruited for this study
Sampling method
Participants were chosen using a simple random sampling method. This involved writing the numbers 1 and 2 on pieces of paper, which were then placed in a box, mixed up, and drawn at random by nursing and midwifery students. Those who selected the paper with the number 1 were recruited for data collection. This was random and anyone who picked 1 was included in the study regardless of their program or academic level till the 403 participants were selected.
Inclusion and exclusion criteria
Eligible study participants were students in the College who gave consent to participate in the study. However, students who did not give consent to be part of the study and those who were not present in school at the time of the study were excluded from the study.
Data collection procedure
A pretested structured questionnaire, using face to face interviewing technique was used to elicit information from final year nursing and midwifery students. The participants were assured of the confidentiality of their responses. The data was also be collected online using a survey tool for first and second-year nursing and midwifery students, this was because first- and second-year students were on vacation and only third year students were on campus. The first 330 online responses were selected for the study regardless of the year or program of study. All questionnaires were self-administered because all students were assumed to be literate enough at that level and google forms links were also sent to all the first- and second-year groups to be able to access the questionnaire online.
Variables and statistical analysis
Explanatory variables for Knowledge of schistosomiasis (Outcome variable) include: have you heard about schistosomiasis, source of information, knowledge on transmission of schistosomiasis, causes of schistosomiasis, common symptoms of schistosomiasis and knowledge of endemicity of schistosomiasis in area. Explanatory variables for Attitude towards schistosomiasis (Outcome variable) include: have you ever been tested for schistosomiasis, confidence in ability to recognize signs and symptoms of schistosomiasis, have you ever seen a case of schistosomiasis in your clinical practice and interest in participating in future schistosomiasis prevention and control programs. Explanatory variables for Preventive practices (Outcome variable) include: how schistosomiasis can be prevented, role of nursing and midwifery students in preventing and controlling schistosomiasis and treatment of schistosomiasis. Participants’ data was recorded into google forms and exported to STATA 17 for analysis.
In the study, the knowledge score was calculated based on participants’ responses to questions assessing their understanding of schistosomiasis. Key domains included: (1) awareness of the disease, (2) knowledge of transmission modes, (3) identification of causes (e.g., snails, contaminated water), (4) recognition of common symptoms (e.g., blood in stool/urine), and (5) awareness of local endemicity. Each correct response was assigned 1 point, while incorrect or “don’t know” responses received 0 points. A cumulative knowledge score was computed for each participant by summing these points. The total score was categorized as “good” or “poor” using a predefined threshold where ≥50% of the maximum possible score was considered good knowledge. This approach aligns with standard knowledge, attitude, and practice (KAP) survey methodologies, where correct answers to critical questions are aggregated to determine overall knowledge levels.
The attitude score was generated based on participants’ responses to a series of questions assessing their attitudes toward schistosomiasis. These questions included: (1) confidence in recognizing signs and symptoms, (2) prior involvement in schistosomiasis control programs, and (3) interest in participating in future prevention activities. Each response was assigned a numerical value (e.g., “very confident” = 2, “somewhat confident” = 1, “not confident” = 0). A composite attitude score was calculated for each participant by summing the values of their responses. The total score was then categorized as “good” or “poor” using a predefined threshold where ≥50% of the maximum possible score was considered good attitude.
The practice score was derived from participants’ responses to questions assessing their preventive behaviors and treatment knowledge related to schistosomiasis. Key items included: (1) methods of prevention (e.g., avoiding contaminated water, supporting mass drug administration), (2) perceived role in prevention (e.g., health education, screening), and (3) treatment preferences (e.g., Praziquantel vs. traditional medicine). Each correct or recommended practice (e.g., citing Praziquantel as treatment) was assigned 1 point, while incorrect responses received 0 points. A cumulative practice score was calculated for each participant by summing these points. The total score was categorized as “good” or “poor” based on a predefined threshold where ≥50% of the maximum possible score was considered good practice.
Descriptive statistics (frequencies, percentages) were used to analyze and present the results. To resolve any potential issues that arose while entering the data, a double input was made. Prior to the most recent analysis, data was cleaned using STATA 17. Descriptive statistics such as frequencies, proportions, percentages, averages, and standard deviation was utilized to examine numerical data.
Logistic regression was also utilized to analyze demographic factors associated with Knowledge of respondents, demographic factors associated with Attitude of respondents, demographic factors associated with Practices of respondents. The Crude analysis was done initially for all variables and the variables whose p-values were significant were selected for inclusion into the Adjusted analysis.
Ethical considerations
This study was conducted in full compliance with the ethical principles outlined in the World Medical Association’s Declaration of Helsinki (2024 update), which provides guidelines for medical research involving human participants. Ethical approval was given by the University of Health and Allied Sciences Research Ethics Committee (UHAS-REC A.10 [003]22-23). In accordance with the Declaration of Helsinki, all living participants provided free and informed consent prior to their inclusion in the study. Participants were informed about the study’s purpose, their right to withdraw at any time without consequences, and the confidentiality of the data collected. Anonymity was ensured by assigning unique codes to participants, and all data were kept confidential. Permission was secured from the administrator of Hohoe Nursing and Midwifery Training College before questionnaire administration. The study adhered to all relevant ethical guidelines concerning informed consent, data protection, and participant welfare as outlined in the Declaration of Helsinki.
Results
Demographic characteristic of residents
The study included 403 nursing and midwifery students, all of whom were female. The majority of respondents were between the ages of 24–31 with 18 years being the youngest and 31 being the oldest, accounting for 58.6% of the sample. Christianity was the most common religion among respondents, with 71.2% identifying as Christian and 28.5% identifying as Islamic. The majority of respondents were not married (88.8%), and the largest ethnic group was Ewe (52.1%). In terms of academic level, Year 1 and Year 2 had percentages (40.7% and 41.2%, respectively), while Year 3 had the smallest percentage (18.1%). The most common program of study among respondents was Nursing (46.7%) followed by Midwifery (43.3%) (See Table 1). Due to missing data, some variable categories are less than 403.
Table 1
| Socio-demographics | Frequency (N = 403) | Percentage (%) |
|---|---|---|
| Age mean(± SD) | 24.1(± 2.5) | |
| 18-23 | 167 | 41.4 |
| 24-31 | 236 | 58.6 |
| Sex | ||
| Female | 403 | 100 |
| Religion | ||
| Christianity | 287 | 71.2 |
| Islamic | 115 | 28.5 |
| African Traditional | 1 | 0.3 |
| Marital status | ||
| Not Married | 358 | 88.8 |
| Married | 24 | 6.0 |
| Cohabiting | 21 | 5.2 |
| Ethnic group | ||
| Akan | 114 | 28.3 |
| Ewe | 210 | 52.1 |
| Ga/Dangbe | 29 | 7.2 |
| Guan | 23 | 5.7 |
| Mole-dagbani | 27 | 6.7 |
| Academic level | ||
| Year 1 | 164 | 40.7 |
| Year 2 | 166 | 41.2 |
| Year 3 | 73 | 18.1 |
| Program of study | ||
| Midwifery | 188 | 53.3 |
| Nursing | 215 | 46.7 |
Demographic characteristics of respondents.
Knowledge of respondents on schistosomiasis
The majority of respondents (92.6%) have heard about the disease, with most of them (34.0%) getting information from the media. A large percentage (91.4%) have knowledge of the transmission of schistosomiasis, with the majority (43.4%) identifying snails as the cause of the disease. Blood in stool or urine is the most common symptom (74.3%), while only a few respondents (38.0%) know if schistosomiasis is endemic in their area (See Table 2).
Table 2
| Variable | Frequency(n=403) | Percentage (%) |
|---|---|---|
| Heard about schistosomiasis | ||
| No | 30 | 7.4 |
| Yes | 373 | 92.6 |
| Source of information | ||
| Lectures | 126 | 34.0 |
| Media | 196 | 53.0 |
| Friends/family | 51 | 14.0 |
| Knowledge on the transmission of schistosomiasis | ||
| No | 32 | 8.6 |
| Yes | 341 | 91.4 |
| Cause of schistosomiasis | ||
| Dirty water | 90 | 24.1 |
| Parasites | 107 | 28.7 |
| STI | 14 | 3.8 |
| Snails | 162 | 43.4 |
| Common symptoms of schistosomiasis | ||
| Abdominal pain and discomfort | 55 | 14.8 |
| Blood in stool or urine | 277 | 74.3 |
| Anaemia | 19 | 5.0 |
| Fatigue and weakness | 6 | 1.6 |
| itchy skin or rash | 11 | 3.0 |
| Diarrhea | 5 | 1.3 |
| Know if schistosomiasis is endemic in your area | ||
| No | 231 | 62.0 |
| Yes | 142 | 38.0 |
Knowledge of respondents on schistosomiasis.
Attitude of the respondents on schistosomiasis
All respondents have never been tested for schistosomiasis. In terms of confidence in recognizing the signs and symptoms of the disease, almost half (49.6%) are somewhat confident, while 38.3% are very confident. Most of the respondents (81.8%) have never seen a case of schistosomiasis in their clinical practice, while 60.3% have been involved in some schistosomiasis control program. Only a small percentage (8.3%) did not express interest in participating in future schistosomiasis prevention and control activities, while the majority (91.7%) expressed interested (See Table 3).
Table 3
| Variable | Frequency | Percentage % |
|---|---|---|
| Ever been tested for schistosomiasis | ||
| No | 373 | 100.0 |
| Yes | 0 | 0.0 |
| Confidence in ability to recognize the signs and symptoms of schistosomiasis | ||
| Not confident | 45 | 12.1 |
| Somehow confident | 185 | 49.6 |
| Very confident | 143 | 38.3 |
| Ever seen a case of schistosomiasis in your clinical practice | ||
| No | 305 | 81.8 |
| Yes | 68 | 18.2 |
| Ever been involved in any schistosomiasis control program | ||
| No | 148 | 39.7 |
| Yes | 225 | 60.3 |
| Interest in participating in future schistosomiasis prevention and control activities | ||
| Yes | 342 | 91.7 |
| No | 31 | 8.3 |
Attitude of the respondents on schistosomiasis.
Preventive practices of the respondents on schistosomiasis
Majority of the respondents (69.2%) believe that avoiding swimming, bathing, and washing in contaminated water is an effective way to prevent schistosomiasis. A significant percentage (16.4%) believe in mass drug administration as a preventive measure. Health education (6.4%), improving sanitation and access to clean water (7.2%), and controlling snail populations (0.8%) were also identified as preventive measures. Regarding the role of nursing and midwifery students in preventing and controlling schistosomiasis, the majority of respondents (55.8%) believe that health promotion and education are the most important roles of nursing and midwifery students in preventing and controlling schistosomiasis. Screening and diagnosis (23.6%), treatment and management (18.5%), and research (2.1%) were also identified as important roles of nursing and midwifery students in preventing and controlling schistosomiasis.
Majority of respondents (97.9%) believe that taking medication, specifically Praziquantel, is the most effective way to treat schistosomiasis, while only a few respondents (2.1%) believe in taking herbal or traditional medication (See Table 4).
Table 4
| Variable | Frequency | Percentage % |
|---|---|---|
| How schistosomiasis can be prevented | ||
| Mass drug administration | 61 | 16.4 |
| Avoid swimming, bathing and washing in contaminated water | 258 | 69.2 |
| Health education | 24 | 6.4 |
| Control snail population | 3 | 0.8 |
| Improve sanitation and access to clean water | 27 | 7.2 |
| Role of nursing and midwifery students in preventing and controlling schistosomiasis | ||
| Health promoting and education | 208 | 55.8 |
| Screening and diagnosis | 88 | 23.6 |
| Research | 8 | 2.1 |
| Treatment and management | 69 | 18.5 |
| Treatment of Schistosomiasis | ||
| Taking herbal or traditional medication | 8 | 2.1 |
| Taking Medication (Praziquantel) | 365 | 97.9 |
Preventive practices of the respondents on schistosomiasis.
According to the responses of the students, mass drug administration appears to be the most successful technique for enhancing schistosomiasis prevention and control, with 51.2% selecting this choice. The second most popular option, with 41.3% of respondents selecting it, was to increase funds for schistosomiasis control programs. Providing free education was chosen by only 4% of respondents, while research and innovation received the fewest answers, with only 3.5% selecting this choice.
The graph illustrates the learning methods that respondents believe are most successful in improving their knowledge, attitude, and practice of schistosomiasis prevention. According to the research, lectures were the most preferred technique, with 54.4% of respondents indicating they were effective. With 28.9% of respondents thinking that it will be beneficial, practical sessions were the second most chosen option. 13.7% of respondents thought educational items like brochures and posters were effective. Only 3% of those interviewed thought mobile health (mHealth) activities were useful for learning about schistosomiasis prevention.
After adjusting for potential confounders, age, cohabiting status and ethnicity were independently associated with respondents’ knowledge (Table 5). Respondents aged 24–31 years were almost three times more likely to have good knowledge compared with those aged 18–23 years (AOR = 2.90; 95% CI: 1.60–5.20; p < 0.001). Cohabiting respondents had markedly lower odds of good knowledge than those who were not married (AOR = 0.20; 95% CI: 0.10–0.50; p = 0.001). With respect to ethnicity, Ewe respondents were about twice as likely as Akan respondents to have good knowledge (AOR = 2.00; 95% CI: 1.02–3.80; p = 0.042), while no significant associations were observed for Ga/Dangbe, Guan or Mole-Dagbani groups. Marital status (married), religion, academic level and program of study did not show significant independent associations with knowledge after adjustment.
Table 5
| Variable | COR (95% CI) | P-value | AOR (95% CI) | P-value |
|---|---|---|---|---|
| Age | ||||
| 18-23 | 1 | 1 | ||
| 24-31 | 3.01(1.73-5.30) | <0.001 | 2.90(1.60-5.20) | <0.001 |
| Religion | ||||
| Christianity | 1 | |||
| Islamic/African traditional | 1.40(0.74-2.60) | 0.304 | ||
| Marital status | ||||
| Not Married | 1 | 1 | ||
| Married | 1.91(0.44-8.40) | 0.390 | 1.14(0.25-5.33) | 0.865 |
| Cohabiting | 0.23(0.10-0.60) | 0.002 | 0.20(0.10-0.50) | 0.001 |
| Ethnic group | ||||
| Akan | 1 | 1 | ||
| Ewe | 2.10(1.11-3.84) | 0.022 | 2.00(1.02-3.80) | 0.042 |
| Ga/Dangbe | 0.84(0.30-2.20) | 0.719 | 0.80(0.30-2.10) | 0.610 |
| Guan | 1.30(0.40-4.10) | 0.692 | 1.24(0.40-4.13) | 0.726 |
| Mole-dagbani | 1.20(0.40-3.42) | 0.770 | 1.00(0.31-3.00) | 0.934 |
| Academic level | ||||
| Year 1 | 1 | |||
| Year 2 | 1.11(0.61-2.04) | 0.724 | ||
| Year 3 | 0.80(0.40-1.63) | 0.529 | ||
| Program of study | ||||
| Midwifery | 1 | |||
| Nursing | 1.60(0.92-2.71) | 0.095 | ||
Univariate and multivariate analysis of demographic factors associated with knowledge of respondents.
Table 6 summarizes the multivariate logistic regression results of demographic characteristics in relation to respondents’ attitudes. Respondents aged 24–31 years were over five times more likely to report a positive attitude compared with those aged under 24 years (AOR = 5.34; 95% CI: 3.43–8.32; p < 0.001). In contrast, marital status including being married (AOR = 1.50; 95% CI: 0.60–4.01; p = 0.424) or cohabiting (AOR = 1.40; 95% CI: 0.53–3.70; p = 0.494) was not significantly associated with respondents’ attitudes. No significant associations were observed for religion, ethnicity, academic level or program of study in the adjusted model.
Table 6
| Variable | COR (95% CI) | P-value | AOR (95% CI) | P-value |
|---|---|---|---|---|
| Age | ||||
| 18-23 | 1 | 1 | ||
| 24-31 | 5.21(3.40-8.00) | <0.001 | 5.34(3.43-8.32) | <0.001 |
| Religion | ||||
| Christianity | 1 | |||
| Islamic/African traditional | 1.54(1.00-2.40) | 0.056 | ||
| Marital status | ||||
| Not Married | 1 | 1 | ||
| Married | 3.00(1.03-7.00) | 0.043 | 1.50(0.60-4.01) | 0.424 |
| Cohabiting | 1.20(0.50-3.00) | 0.717 | 1.40(0.53-3.70) | 0.494 |
| Ethnic group | ||||
| Akan | 1 | |||
| Ewe | 1.00(0.52-1.30) | 0.391 | ||
| Ga/Dangbe | 0.60(0.30-1.30) | 0.180 | ||
| Guan | 1.32(0.52-3.40) | 0.566 | ||
| Mole-dagbani | 0.60(0.24-1.31) | 0.181 | ||
| Academic level | ||||
| Year 1 | 1 | |||
| Year 2 | 0.93(0.57-1.51) | 0.760 | ||
| Year 3 | 0.57(0.32-1.03) | 0.061 | ||
| Program of study | ||||
| Midwifery | 1 | |||
| Nursing | 1.31(0.90-2.00) | 0.184 | ||
Univariate and multivariate analysis of demographic factors associated with attitude of respondents.
Table 7 presents the multivariate logistic regression results of demographic characteristics in relation to respondents’ practices.
Table 7
| Variable | COR (95% CI) | P-value | AOR (95% CI) | P-value |
|---|---|---|---|---|
| Age | ||||
| 18-23 | 1 | 1 | ||
| 24-31 | 3.02(1.50-6.10) | 0.002 | 3.70(1.64-8.20) | 0.002 |
| Religion | ||||
| Christianity | 1 | |||
| Islamic/African traditional | 1.15(0.54-2.44) | 0.724 | ||
| Marital status | ||||
| Not Married | 1 | 1 | ||
| Married | 0.93(0.21-4.20) | 0.928 | 0.41(0.10-2.14) | 0.291 |
| Cohabiting | 0.14(0.10-0.40) | <0.001 | 0.13(0.04-0.40) | <0.001 |
| Ethnic group | ||||
| Akan | 1 | 1 | ||
| Ewe | 3.62(1.70-8.00) | 0.001 | 4.14(1.74-9.90) | 0.001 |
| Ga/Dangbe | 2.70(0.60-12.33) | 0.200 | 2.60(0.52-12.72) | 0.244 |
| Guan | 1.33(0.40-5.00) | 0.667 | 1.11(0.27-4.54) | 0.887 |
| Mole-dagbani | 1.60(0.44-5.90) | 0.478 | 1.61(0.41-6.40) | 0.499 |
| Academic level | ||||
| Year 1 | 1 | |||
| Year 2 | 1.20(0.60-2.50) | 0.676 | ||
| Year 3 | 0.90(0.40-2.15) | 0.777 | ||
| Program of study | ||||
| Midwifery | 1 | 1 | ||
| Nursing | 4.20(2.00-9.10) | <0.001 | 4.90(2.10-11.30) | <0.001 |
Univariate and multivariate analysis of demographic factors associated with practices of respondents.
Respondents aged 24–31 years had significantly higher odds of appropriate practices compared with those aged 18–23 years (AOR = 3.70; 95% CI: 1.64–8.20; p = 0.002). Cohabiting status was strongly and inversely associated with appropriate practices. Cohabiting respondents were substantially less likely than unmarried respondents to report appropriate practices (AOR = 0.13; 95% CI: 0.04–0.40; p < 0.001). Being married was not significantly associated with practice (AOR = 0.41; 95% CI: 0.10–2.14; p = 0.291).
With respect to ethnicity, respondents of Ewe origin had significantly higher odds of appropriate practices compared with Akan respondents (AOR = 4.14; 95% CI: 1.74–9.90; p = 0.001). No significant associations were observed for Ga/Dangbe (AOR = 2.60; 95% CI: 0.52–12.72; p = 0.244), Guan (AOR = 1.11; 95% CI: 0.27–4.54; p = 0.887) or Mole-Dagbani (AOR = 1.61; 95% CI: 0.41–6.40; p = 0.499). Program of study was also independently associated with practice. Nursing students were nearly five times more likely to report appropriate practices compared with Midwifery students (AOR = 4.90; 95% CI: 2.10–11.30; p < 0.001).
Other variables, including religion, marital status (married), and academic level, were not independently associated with respondents’ practices after adjustment.
Discussion
The study’s results revealed good level of knowledge about schistosomiasis (84.1%) See Figure 1, with the media serving as the primary source of information. Attitudes toward the disease were only moderately positive (54.6%) See Figure 2, though interest in participating in future prevention and control activities was very high (91.7%). The study revealed strong preventive practices (90.6%) See Figure 3, including widespread recognition of Praziquantel as the main treatment. The study also found that demographic factors such as age, ethnicity, marital status, and program of study were significantly associated with the students’ knowledge, attitudes, and practices.
Figure 1
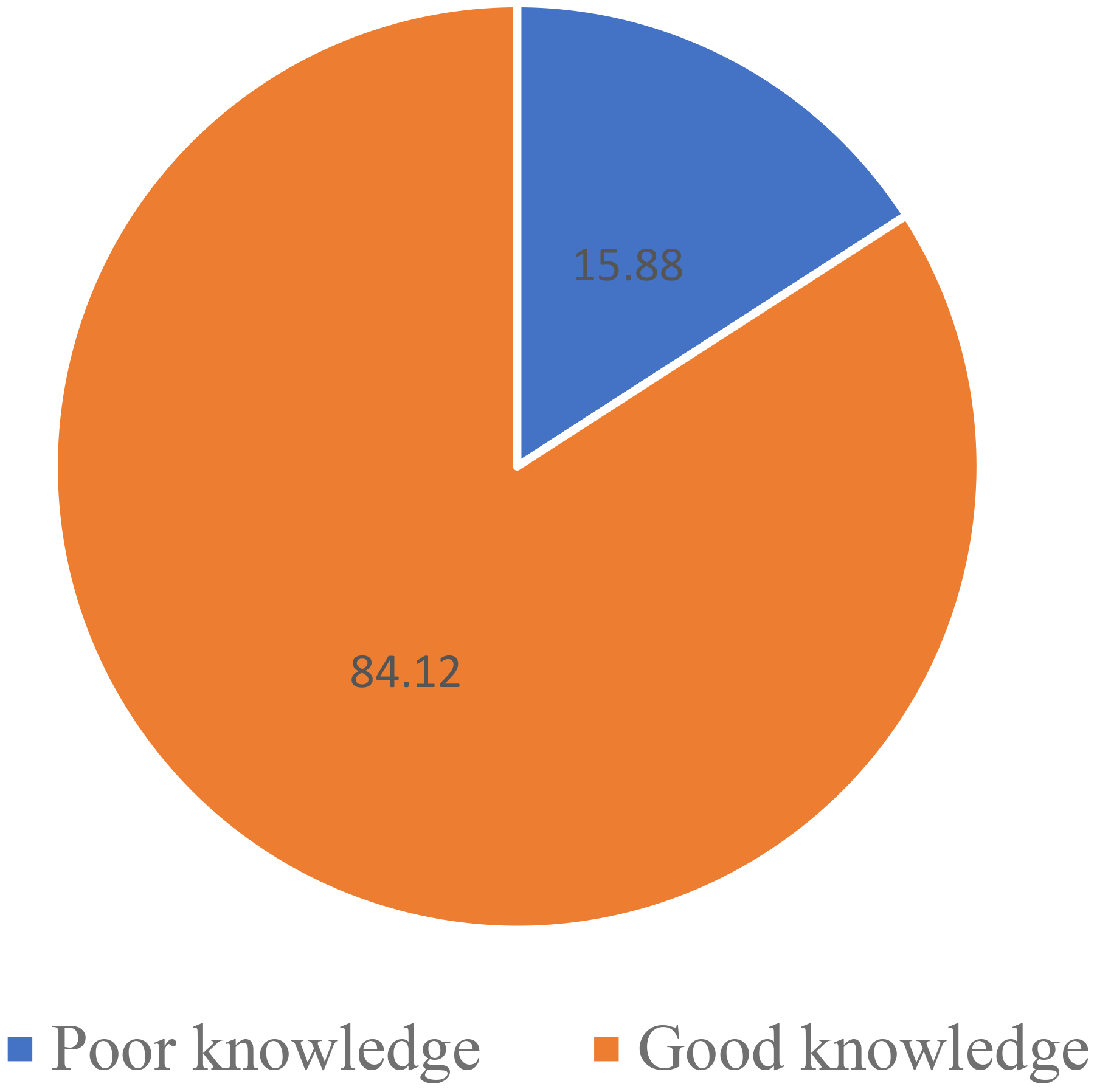
Knowledge of respondents on schistosomiasis.
Figure 2
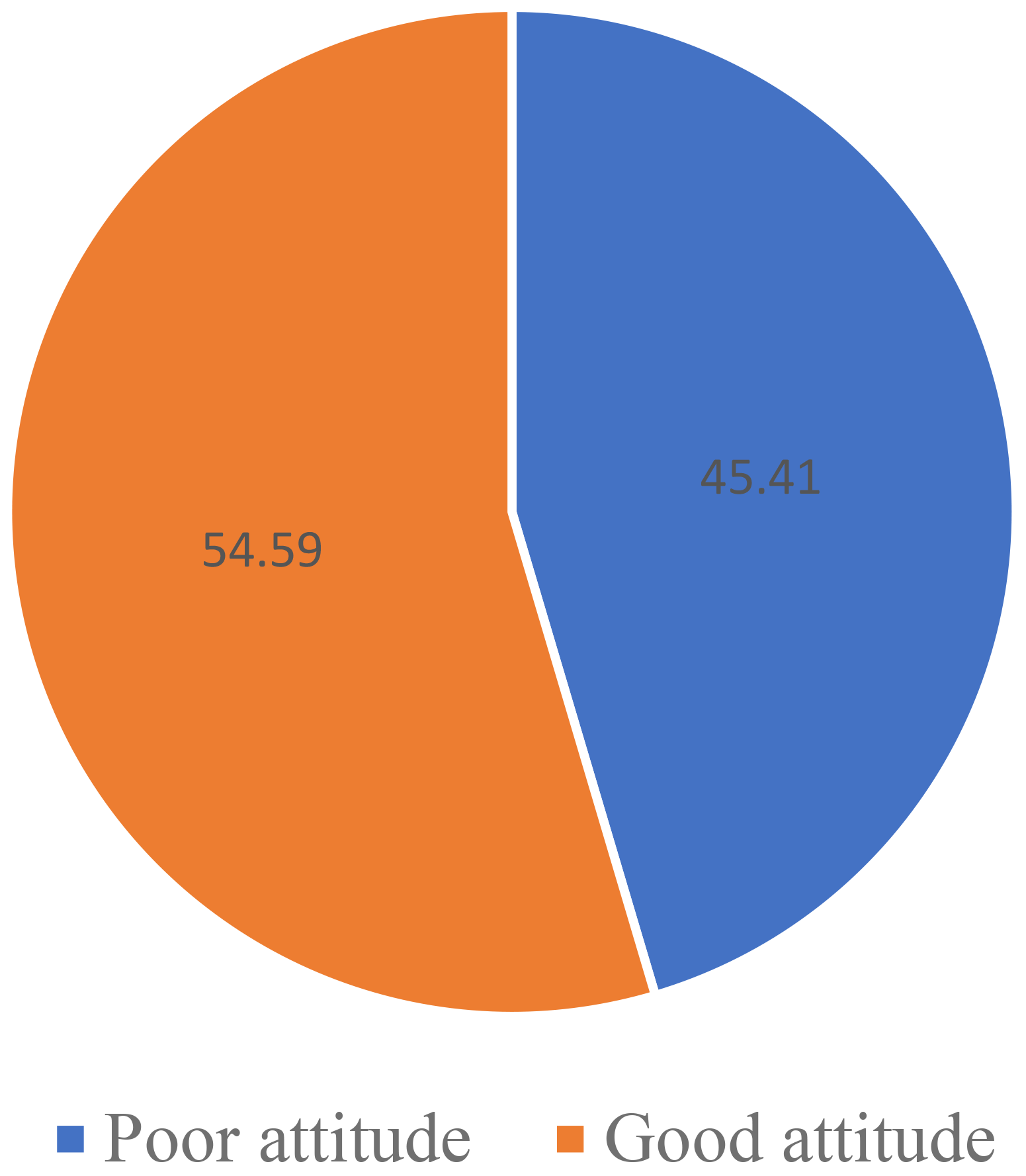
Attitude of respondents toward schistosomiasis.
Figure 3
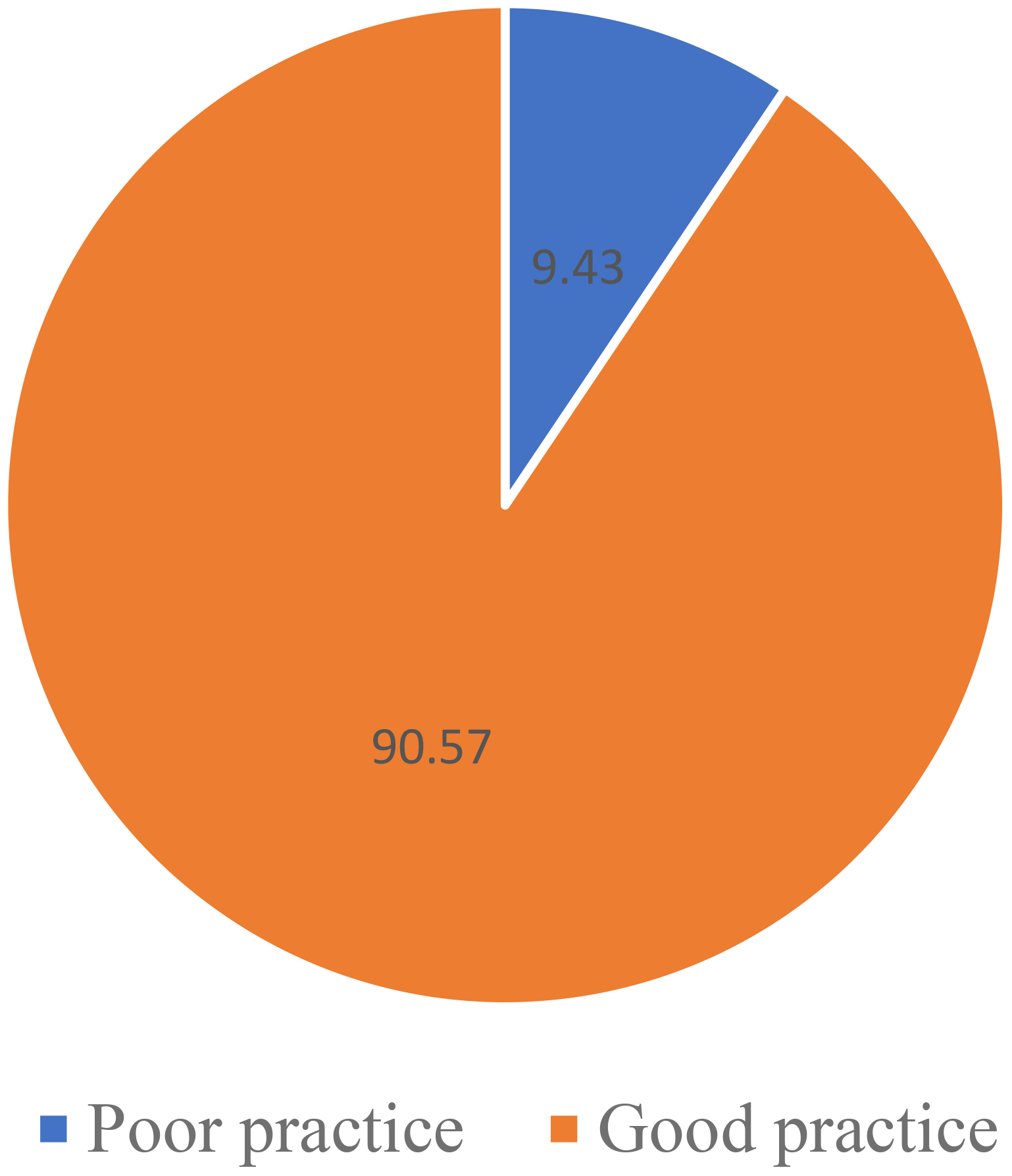
Preventive practices of respondents towards schistosomiasis.
Knowledge, attitudes and preventive practices regarding schistosomiasis
Nursing and midwifery students in Hohoe municipality have good knowledge, attitudes, and preventive practices about schistosomiasis, with 92.6%) being aware of the disease, 34.4% identifying snails as the cause, and blood in stool or urine being the most common symptom which was Consistent with findings from Dawaki et al. (10), a majority of participants in their study demonstrated familiarity with schistosomiasis, particularly its urinary form, with roughly 75% reporting prior awareness of the disease. This could be attributed to the fact that schistosomiasis is endemic in Nigeria; the high percentage of self-reported history of infection among the participants supports the endemicity of infection in these communities. In accordance, few previous reports elsewhere showed variation in the level of awareness amongst the Nigerian population; 33.8%-42.0% in Delta State, Southeastern Nigeria and 64.4% in Ogun and Niger states along the middle belt and southwestern region. In comparison with findings from other countries, poor knowledge of schistosomiasis and its causes was reported in Malawi and Kenya while a high level of awareness (80%) was reported in Zimbabwe.
According to a study by Socolo et al. (11), The results obtained from the studies reviewed indicate lack of comprehensive knowledge relating to schistosomiasis transmission, prevention and control. This is unfortunate considering that the proficiency of correct, comprehensive knowledge in promoting healthy attitudes and protective behavior has been long established. Adoka et al. (12) observed that only 3% of respondents in Lake Victoria basin could relate schistosomiasis to snails.
Regarding participants attitudes, their confidence in recognizing the signs and symptoms of the disease, the survey reveals that almost half of the respondents (49.6%) were somewhat confident, while 38.3% were very confident. When it comes to their clinical practice, the majority of respondents (81.8%) have never seen a case of schistosomiasis. However, a significant portion (60.3%) have been involved in some schistosomiasis control program. Interestingly, only a small percentage (8.3%) did not express interest in participating in future schistosomiasis prevention and control activities, while the majority (91.7%) were interested.
These findings highlight the need for further education and awareness campaigns to improve knowledge and engagement among healthcare professionals and the general population in schistosomiasis prevention and control efforts. The survey provides information on the preventive practices of the respondents towards schistosomiasis. The majority of respondents (69.2%) believe that avoiding swimming, bathing, and washing in contaminated water is an effective way to prevent schistosomiasis. A significant percentage (16.4%) believe in mass drug administration as a preventive measure. Health education, improving sanitation and access to clean water, and controlling snail populations were also identified as preventive measures.
For practices, regarding the role of nursing and midwifery students in preventing and controlling schistosomiasis, the majority of respondents (55.8%) believe that health promotion and education are the most important roles of nursing and midwifery students in preventing and controlling schistosomiasis. Screening and diagnosis, treatment and management, and research were also identified as important roles of nursing and midwifery students in preventing and controlling schistosomiasis. In terms of treatment, the majority of respondents (97.9%) believe that taking medication, specifically Praziquantel, is the most effective way to treat schistosomiasis, while only a few respondents (2.1%) believe in taking herbal or traditional medication. These findings highlight the importance of medication in treating schistosomiasis and the need for further education and awareness campaigns to promote effective preventive practices among healthcare professionals and the general population.
Association between socio-demographics and knowledge, attitude and practices
With regards to socio-demographics and knowledge, the study’s findings revealed that younger individuals that is, respondents aged 24–31 tended to be more knowledgeable than their older counterparts. The study uncovered no relation between religious affiliation and knowledge. Regarding marital status, cohabiting respondents exhibited higher knowledge compared to those who are unmarried or married. Contrary to this, studies conducted among care givers in Tanzania, Ng’weng’weta and Tarimo found that married women had significantly higher levels of schistosomiasis related knowledge compared to unmarried women (11).
With regard to ethnic background, the study found that Ewe respondents displayed a heightened knowledge of schistosomiasis as compared to their Akan counterparts. There was no relationship academic level and knowledge. This suggested that one’s academic year of study did not significantly influence their level of knowledge. Lastly, students in the midwifery program tended to have more knowledge than their counterparts in nursing. Another piece of literature showed that a significantly lower percentage of those aged below 40 years had heard about schistosomiasis compared to those aged ≥ 40 years. However, knowledge of fatigue, swollen abdomen and vomiting as symptoms of schistosomiasis was significantly higher in those aged below 40 years compared to those aged ≥ 40 years (13).
For socio-demographics and attitude, the study revealed that respondents aged 24–31 tended to exhibit more positive attitudes compared to those under 24 years old indicating a high odd of having a good attitude level when aged 24 to 31. Regarding religion, no significant associations between religious affiliation and attitudes were observed which indicated that religious beliefs did not substantially influence the attitudes of the respondents. In terms of marital status, cohabiting respondents appeared to have more positive attitudes than those who are unmarried. There were no significant associations between ethnic group and attitudes, suggesting that ethnic background does not play a significant role in shaping attitudes. Academic level did not demonstrate significant associations with attitudes. This implies that the stage of one’s academic journey does not strongly affect their attitudes. There was also no significant association between program of study and attitude towards schistosomiasis. A study by Sacolo-Gwebu et al. (14) discovered that the majority of study participants reported having inadequate attitudes on modes of transmission, prevention, and control. They stated that if modern medicine does not help them, they resort to traditional healers or utilize both treatments at the same time.
With respect to socio-demographics and practices, younger individuals, particularly those under 24 years old, had significantly better practices compared to their counterparts aged 24-31. This suggests a pattern where younger people tend to adopt more favorable practices. There were no substantial associations found between religion and individuals’ practices which implied that religious beliefs have limited influence on respondents’ practices. Marital status played a significant role, with individuals in cohabiting relationships exhibiting significantly better practices than unmarried respondents. Regarding ethnic backgrounds, the Akan ethnic group adhered to better practices as compared to the other ethnic groups. Interestingly, academic level did not have any relationship with practices which suggested that one’s academic level does not strongly impact their practices. Finally, midwifery students exhibited more favorable practices compared to their nursing counterparts.
Recommendations for improving the knowledge, attitude and practice of schistosomiasis
Based on the feedback from the students, mass drug administration is considered the most successful approach for improving schistosomiasis prevention and control, chosen by 51.2% of respondents. The second most popular choice, selected by 41.3% of participants, is increasing funding for schistosomiasis control programs. Providing free education was the preference of only 4% of those surveyed, while research and innovation garnered the least support, with only 3.5% choosing it (See Figure 4).
Figure 4
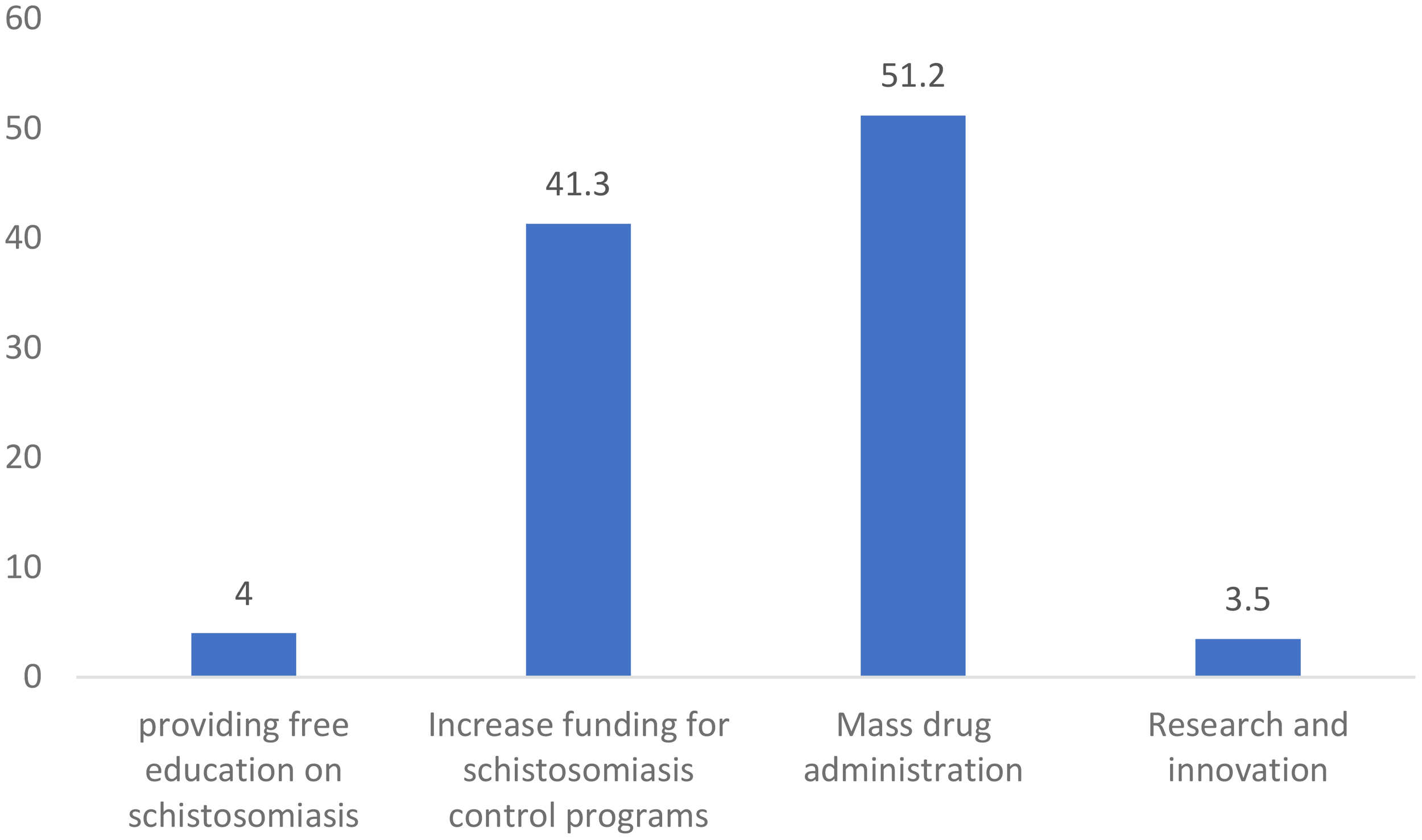
How government and health organizations can improve the prevention and control of schistosomiasis.
The survey also reveals the preferred methods for enhancing knowledge, attitude, and practice related to schistosomiasis prevention among students. Lectures are the most favored approach, with 54.4% of respondents finding them effective. Practical sessions are the second most popular choice, considered beneficial by 28.9% of participants. Educational materials such as brochures and posters were perceived as effective by 13.7% of those surveyed. Only 3% of the interviewed students believed that mobile health (mHealth) activities were useful for learning about schistosomiasis prevention (See Figure 5).
Figure 5
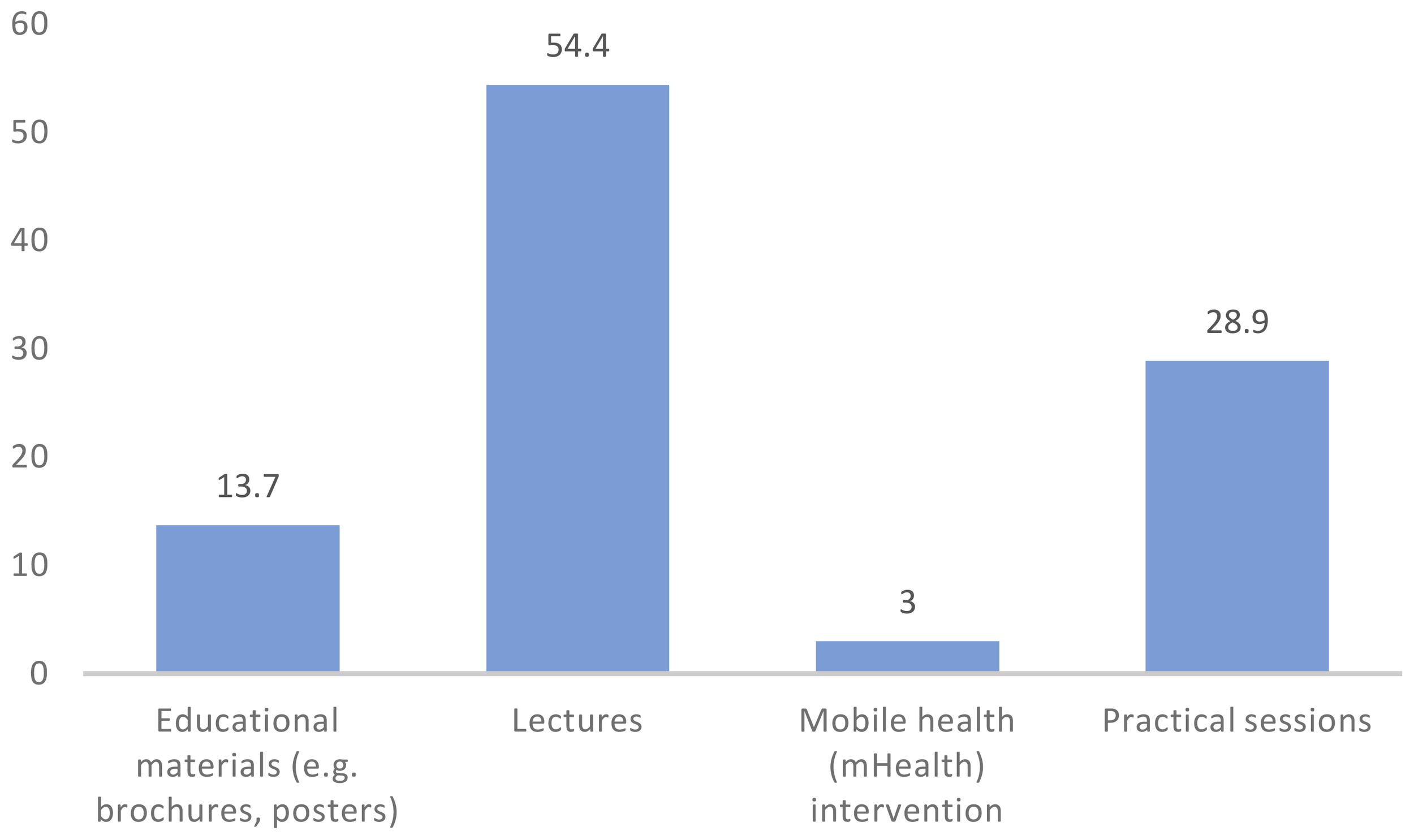
Methods of learning suggested to be most effective in improving knowledge, attitude and practice of schistosomiasis prevention.
According to Anyolitho et al. (15). there is a dire need for the government to provide clean and safe water sources and to ensure proper sanitation and hygiene among the communities. In addition, to address these barriers and bring down infection rates, there is a need to implement a more robust community-based awareness intervention that is culturally appropriate and context-specific to the community members’ deeply rooted habits and beliefs.
Integrating schistosomiasis education into mass drug administration (MDA) initiatives could enhance treatment adherence and disseminate critical knowledge across all age groups. In addition, education during school and campaigns should not be limited to talk about general characteristics of the disease, but should also highlight PMT elements, such as the constant vulnerability of each person living in high endemic settings (16).
Limitations of the study
The study has some limitations that should be acknowledged. First, its cross-sectional design restricts the ability to establish causal relationships, as it only captures data at a single point in time. Second, the sample was limited to nursing and midwifery students in a single institution, all of whom were female, which may limit the generalizability of the findings to other populations. Third, the reliance on self-reported data introduces potential biases, such as social desirability bias, where participants may overreport positive behaviors. Fourth, the study did not include actual testing for schistosomiasis, missing an opportunity to validate self-reported practices with objective infection data. Finally, while a 5% non-response rate was accounted for, any differences between participants and non-participants could still introduce bias into the results.
Conclusion
This study examined the knowledge, attitudes, and preventive practices of nursing and midwifery students regarding schistosomiasis in the Hohoe municipality. Findings showed that respondents had good knowledge, attitudes, and preventive practices towards schistosomiasis which is a positive sign of reduction in schistosomiasis. This level of knowledge, attitude and practices will gradually reduce mortalities and morbidities and will project the achievement of the Sustainable Development Goals (SDG) 3 (good health and wellbeing) and 10 (reduced inequalities).
Overall, this study contributes new knowledge to the existing body of literature on schistosomiasis and highlights the need for continued efforts to improve knowledge, attitudes, and practices towards schistosomiasis prevention and control. The study also recommends that; There is a need for increased access to schistosomiasis testing tools and treatment materials for students in the nursing and midwifery training school to familiarize themselves with. This can be done through collaboration with local health authorities to provide regular testing and treatment materials for students. Schistosomiasis control programs should be integrated into the nursing and midwifery training curriculum to increase awareness and practical knowledge of the disease among students. This can include practical training on how to diagnose and treat schistosomiasis. There should be more emphasis on the importance of participating in schistosomiasis prevention and control activities among students. This can be done through incentives such as offering extra credit or recognition for participation in such activities.
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the University of Health and Allied Sciences (UHAS-REC A.10 [003]22-23). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NT: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. DT: Data curation, Formal analysis, Investigation, Supervision, Writing – review & editing. AM: Data curation, Methodology, Project administration, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors acknowledge the support of the data collection team and are also grateful to Nursing and midwifery training college students who supported the ethical clearance and data collection processes on campus. We acknowledge the study participants for making time to respond to the research instruments. The authors are also grateful to all stakeholders for making this study successful.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
95% CI, 95% confidence interval; GIS, Gastrointestinal schistosomiasis; KAPs, Knowledge, attitude, and practices; MDA,Mass drug administration; NTDs, Neglected Tropical Diseases; OR, Odds ratio; AOR, Adjusted Odds Ratio; COR, Crude Odds Ratio; PCR, Polymerase chain reaction; SAC, School Aged Children; STH, Soil-transmitted helminths; UGS, Urogenital schistosomiasis; WASH, Water Sanitation and Hygiene; WHO, World Health Organization.
References
1
Gabaake KP Phaladze NA Lucero-Prisno DE Thakadu OT . Assessment of awareness and knowledge of schistosomiasis among school-aged children (6–13 years) in the Okavango Delta, Botswana. Global Health Research and Policy (2022) 7(1):36. doi: 10.21203/rs.3.rs-1800985/v1
2
Dejon-Agobé JC Zinsou JF Honkpehedji YJ Edoa JR Adegbité BR Beh-Mba R et al . Knowledge, attitudes and practices pertaining to urogenital schistosomiasis in Lambaréné and surrounding areas, Gabon. Parasites Vectors. (2021) 14(1):486. doi: 10.1186/s13071-021-04905-0
3
Prentice MA . Schistosomiasis and its intermediate hosts in the lesser Antillean islands of the Caribbean. Bull Pan Am Health Organ. (1980) 14(3):258–68.
4
Ross AGP Olveda RM Acosta L Harn DA Chy D Li Y et al . Road to the elimination of schistosomiasis from Asia: the journey is far from over. Microbes Infection. (2013) 15:858–65. doi: 10.1016/J.MICINF.2013.07.010
5
Noya O Katz N Pointier JP Theron A De Noya BA . Schistosomiasis in America. In: Franco-ParedesCSantos-PreciadoJI, editors. Neglected tropical diseases—Latin America and the Caribbean. Springer-Verlag Wien (2015). p. 111–37. doi: 10.1007/978-3-319-06590-7_6
6
Musuva RM Omedo M Secor WE Awiti A Ogutu M Montgomery SP et al . Community knowledge, attitudes and practices on schistosomiasis in western Kenya-the score project. Am J Trop Med Hygiene. (2014) 90:646–52. doi: 10.4269/ajtmh.13-0488
7
Boateng EM Dvorak J Ayi I Chanova M . A literature review of Schistosomiasis in Ghana: A reference for bridging the research and Control Gap. Trans R Soc Trop Med Hygiene. (2023) 117(6):407–17. doi: 10.1093/trstmh/trac134
8
Volta (Region, Ghana) - Population Statistics, Charts, Map and Location. (n.). Available online at: https://www.citypopulation.de/en/Ghana/admin/04:volta/?utm_source=chatgpt.com.
9
Simpri G Mensah EK . Ghana Statistical Service, District Analytical Report. (2010). Available online at: https://www2.statsghana.gov.gh/docfiles/2010_District_Report/Volta/Hohoe%20Mun.pdf (Accessed February 20, 2023).
10
Dawaki S Al-Mekhlafi HM Ithoi I Ibrahim J Abdulsalam AM Ahmed A et al . The menace of schistosomiasis in Nigeria: knowledge, attitude, and practices regarding schistosomiasis among rural communities in Kano state. PloS One. (2015) 10:e0143667. doi: 10.1371/journal.pone.0143667
11
Sacolo H Chimbari M Kalinda C . Knowledge, attitudes and practices on Schistosomiasis in sub-Saharan Africa: a systematic review. BMC Infect Dis. (2018) 18:46. doi: 10.1186/s12879-017-2923-6
12
Adoka S Anyona D Abuom P Dida G Karanja D Vulule J et al . Community perceptions of schistosomiasis transmission, prevalence and control in relation to aquatic habitats in the Lake Victoria basin of Kenya. East Afr Med J. (2014) 91:232–44.
13
Sady H Al-Mekhlafi HM Atroosh WM Al-Delaimy AK Nasr NA Dawaki S et al . Knowledge, attitude, and practices towards schistosomiasis among rural population in Yemen. Parasites Vectors. (2015) 8:436. doi: 10.1186/s13071-015-1050-8
14
Sacolo-Gwebu H Kabuyaya M Chimbari M . Knowledge, attitudes and practices on schistosomiasis and soil-transmitted helminths among caregivers in Ingwavuma area in uMkhanyakude district, South Africa. BMC Infect Dis. (2019) 19:1–11. doi: 10.1186/s12879-019-4253-3
15
Anyolitho MK Poels K Huyse T Tumusiime J Mugabi F Tolo CU et al . Knowledge, attitudes, and practices regarding schistosomiasis infection and prevention: A mixed-methods study among endemic communities of Western Uganda. PloS Negl Trop Dis. (2022) 16(2):e0010190. doi: 10.1371/journal.pntd.0010190
16
Parisi S Mazigo HD Kreibich S Puchner K Kasang C Mueller A . Factors associated with relevant knowledge of intestinal schistosomiasis and intention to participate in treatment campaigns: a cross-sectional survey among school children at Ijinga Island on Lake Victoria, North-Western Tanzania. BMC Public Health. (2019) 19:1–14. doi: 10.1186/s12889-019-8091-4
Summary
Keywords
schistosomiasis, knowledge, attitude, preventive practices, cross sectional study, Ghana
Citation
Naabil DT, Tsekpo D and Manyeh AK (2025) Assessing knowledge, attitude and preventive practices of schistosomiasis among nursing and midwifery students in the Hohoe nursing and midwifery training college, Ghana. Front. Trop. Dis. 6:1669964. doi: 10.3389/fitd.2025.1669964
Received
21 July 2025
Accepted
07 October 2025
Published
23 October 2025
Volume
6 - 2025
Edited by
Jean Claude Dejon Agobé, Centre de Recherche Médicales de Lambaréné, Gabon
Reviewed by
Yuzheng Huang, Jiangsu Institute of Parasitic Diseases (JIPD), China
Sunday Charles Adeyemo, Institut Superiure de Sante ISS, Niger
Updates
Copyright
© 2025 Naabil, Tsekpo and Manyeh.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Divine Tobig Naabil, noelnaabil2@gmail.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.