 Chiara Debie
Chiara Debie Laure Giberto
Laure Giberto Stéphanie Noel
Stéphanie Noel Dominique Paepe
Dominique Paepe Kris Gommeren
Kris Gommeren- 1Small Animal Department, Faculty of Veterinary Medicine, Ghent University, Merelbeke, Belgium
- 2Department of Clinical Sciences, FARAH, Faculty of Veterinary Medicine, University of Liège, Liège, Belgium
Introduction: Hypocalcemia and magnesium disturbances are linked to vasoplegia, cardiac arrhythmias, gastrointestinal ileus, and coagulopathies. In human critical care patients, these imbalances are associated with higher mortality and longer hospital stay. Little is known about such associations in companion animals. Our study assessed the prevalence of ionized calcium (iCa) and ionized magnesium (iMg) disturbances in dogs and cats with septic peritonitis at presentation, and their association with administration of antiarrhythmics, vasopressors, prokinetics, and plasma, hospitalization duration and mortality.
Methods: Medical records of patients with septic peritonitis from January 2018 to December 2023 were reviewed. Inclusion criteria were confirmed septic peritonitis and blood gas analysis with ionized calcium and magnesium values at admission. Data collected included signalment, diagnosis and cause, calcium and magnesium levels, administration of vasopressors, antiarrhythmics, prokinetics, and plasma, length of hospitalization, and survival. Comparisons were made using Chi-square, Fisher exact test, and ANOVA. Correlations were assessed with the Spearman coefficient.
Results: Sixty-one dogs and 17 cats were included. Hypocalcemia (iCa < 1.25 mmol/L in dogs; <1.10 mmol/L in cats) was diagnosed in 51.7% of dogs and 23.5% of cats. Hypomagnesemia (iMg < 0.43 mmol/L in dogs; <0.47 mmol/L in cats) was found in 13.5% of dogs and 0% of cats, and hypermagnesemia (iMg > 0.6 mmol/L in dogs; >0.7 mmol/L in cats) in 15.4% of dogs and 60% of cats. Hypocalcemia and hypermagnesemia were significantly more common in dogs and cats, respectively. Ionized hypocalcemia was associated with plasma administration in dogs (p = 0.038). No significant correlation was found between iCa and iMg disturbances and length of hospitalization in dogs (respectively p = 0.62 and p = 0.62) or cats (respectively p = 0.62 and p = 0.27). The survival rate was 50%, with no association between iCa and iMg derangements and survival in dogs (p = 0.30 and p = 0.38 respectively), nor in cats (p = 0.29 and p = 0.29 respectively). A significant difference was observed in the mean iMg values between survivors (0.49 ± 0.09 mmol/L) and non-survivors (0.55 ± 0.11 mmol/L) in dogs (p = 0.042).
Discussion: In this population with septic peritonitis, about half of the dogs and a quarter of the cats had ionized hypocalcemia. Hypo- and hypermagnesemia were rare in dogs, while hypermagnesemia was common in cats and hypomagnesemia was not seen in cats. Dogs and cats with hypocalcemia were more likely to receive plasma. Mean iMg values were lower in survived dogs than dogs that did not survive.
1 Introduction
Ionized hypocalcemia is a common electrolyte abnormality in critically ill people (1), with a prevalence described between 20 and 70% in septic patients (2, 3). The cause of ionized hypocalcemia in critically ill patients is likely multifactorial, with key pathways including parathyroid gland dysfunction (3), hypomagnesemia, acute renal failure (1–3), and calcitriol deficiency (3). Other contributing factors, such as chelation of calcium with lactate or free fatty acids (4), vitamin D deficiency (3), alkalosis (2), and acute pancreatitis (2), have also been reported. Calcium has important physiologic functions and hypocalcemia can lead to hypotension, systolic dysfunction, arrythmias, coagulopathies and functional gastro-intestinal ileus (3, 5–7). Moreover, hypocalcemia has been associated with increased mortality in critically ill people (1–3, 8).
Ionized hypocalcemia has been reported between 16 to 24% in critically ill dogs (9–11), and 59 to 93% in cats with septic peritonitis (12, 13). In critically ill dogs higher prevalences were observed with kidney disease, diabetes ketoacidosis, pancreatitis and sepsis (9). Ionized hypocalcemia in dogs has been correlated with longer hospitalization (9), and has been inconsistently associated with mortality (9–11). The study by Kellett-Gregory et al. is the only study that examined the clinical impact of ionized hypocalcemia. Their findings did not demonstrate an association between ionized hypocalcemia in cats and an increased prevalence of hypotension, coagulopathy, or arrhythmias during hospitalization (13).
Magnesium disorders have also been associated with hypotension/hypertension (14, 15), arrythmias (16–18), muscle spasms/weakness, refractory hypokalemia (19, 20), hypocalcemia (21), impaired insulin sensitivity (22, 23) or functional gastro-intestinal ileus in both human and veterinary medicine (24–27). Ionized magnesium alterations have been described in critically ill humans, with an incidence of 9.7–26% of ionized hypomagnesemia, and 15–23.6% of hypermagnesemia during hospitalization (8, 28, 29). Both hyper- and hypomagnesemia, whether present at admission or developed during hospitalization, have been associated with an increased mortality in critically ill humans (8, 28, 29).
Several studies on total serum magnesium levels in critically ill dogs found that 45–54% had hypomagnesemia and 8–13% had hypermagnesemia upon admission (11, 30). Another study investigated the prevalence of total magnesium disturbances in a specific cohort of hospitalized dogs with ionized hypocalcemia (31). This study reported a lower prevalence of total hypomagnesemia (22%) and total hypermagnesemia (3%) in this specific subgroup. Additionally, it found no correlation between ionized calcium (iCa) and total magnesium. Nevertheless, multiple studies have shown poor to moderate correlation between ionized magnesium and total magnesium, highlighting the limitations of using total magnesium as a reliable indicator of the magnesium status (28, 32–35). Moreover, in hospitalized and sick animals, the correlation between ionized magnesium and total magnesium tends to weaken (35). Studies investigating ionized magnesium levels in critically ill small animals are limited. One study examined the prevalence of ionized magnesium disturbances in critically ill dogs with parvoviral enteritis (34). In a study population of 72 dogs, a low prevalence of ionized hypomagnesemia (1.4%) was identified, while 6.9% of dogs had ionized hypermagnesemia. Another study of Murray et al. from 2023 investigated ionized magnesium disturbances in a more general population of hospitalized dogs. In this study, they identified a prevalence of 67% of ionized hypomagnesemia, and 4% of hypermagnesemia. In cats, total magnesium derangements were detected in 46% of cases (36). In both species, these derangements were associated with a longer hospital stay and higher mortality (30, 36). No study investigated the clinical impact of magnesium disturbances on the development of specific complications such as arrhythmias, hypotension or gastro-intestinal motility during hospitalization. Therapeutic value of magnesium supplementation in septic patients has not been established yet. Experimental studies in mice have demonstrated that magnesium supplementation mitigates the risk of developing sepsis (37), suggesting a potential therapeutic role for magnesium in critically ill patients during their hospitalization through its immunomodulatory effects.
The objectives of this study were to retrospectively evaluate the prevalence of ionized calcium and magnesium derangements at presentation in dogs and cats with septic peritonitis. Differences in the prevalence of calcium and magnesium derangements between dogs and cats were assessed. Additionally we investigated whether calcium and magnesium derangements at presentation were associated with increased morbidity and mortality. Our hypotheses were that ionized hypocalcemia, ionized hypermagnesemia and ionized hypomagnesemia were common in dogs and cats with septic peritonitis, and that such derangements were associated with increased vasopressor use, antiarrhythmic use, prokinetic use, plasma use, longer hospitalization and higher mortality.
2 Materials and methods
Medical records of dogs and cats presented to the emergency department of the University Veterinary Hospital of the University of Liège were searched to identify all dogs and cats with septic peritonitis between January 2018 and December 2023. Only dogs and cats with a confirmed diagnosis of septic peritonitis and with an available blood gas analysis including iCa and iMg values performed within the first 2 h upon presentation were included. The diagnosis of septic peritonitis was based on the presence of one of the following criteria: intracellular bacteria on cytology of peritoneal free fluid, bacterial growth on culture of peritoneal free fluid, or the identification of a pneumoperitoneum on abdominal ultrasound performed by a board certified imaging specialist in the absence of a history of a penetrating wound or abdominal surgery in the previous week, or identification of lesions compatible with a septic peritonitis during exploratory celiotomy (38, 39). Exclusion criteria were the administration of diuretics in the last 12 h before admission or blood products before the sample for blood gas analysis was taken.
Blood gas analysis was performed on commercial preheparinized syringes (Sarstedt Blood Gas Monovette®, Sarstedt AG & Co. KG, Nümbrecht, Germany) with a Calcium balanced lithium heparin solution. All samples were analyzed in an ion-selective electrode analyzer (Stat Profile Prime Plus® VET Critical Care Blood Gas Analyzer, Nova Biomedical, Waltham, Massachusetts, USA) within 15 min after collection. Reference intervals for ionized calcium were 1.25–1.5 mmol/L for dogs and 1.1–1.4 mmol/L for cats (40). Reference intervals for ionized magnesium were 0.43–0.6 mmol/L for dogs and 0.47–0.7 mmol/L for cats (27).
Medical records were reviewed for all included dogs and cats. Signalment, diagnosis and underlying cause of septic peritonitis, values of iCa and iMg upon admission, outcome, interventions during hospitalization and length of hospitalization were recorded. The administration of vasopressors, antiarrhythmics, prokinetics, and plasma transfusions during hospitalization were recorded, as crude markers of possible vasoplegia, cardiac arrhythmias, gastrointestinal stasis, and coagulopathies, respectively. Outcome was assessed at the time of discharge and categorized as survival or death, with the latter further classified into euthanasia and natural death. All euthanized dogs and cats were included in the prevalence and mortality analysis. However, for the morbidity analysis (association with therapeutic interventions), dogs and cats that were euthanized upon admission without undergoing hospitalization were excluded. Mean values of ionized calcium and ionized magnesium were analyzed and compared only for morbidity in dogs, as the small sample size in cats precluded statistical analysis.
2.1 Statistical analysis
Categorical variables were described using frequency tables (number and percent) and continuous variables were described using mean and standard deviation (±SD) or median and interquartile range (Q1–Q3) as appropriate. Normality of distributions was checked graphically. Comparison of categorical variables was done using Chi-square or Fisher exact test, ANOVA was used for continuous variables. Correlation was investigated using Spearman correlation coefficient. Results were considered statistically significant at 0.05 level (p < 0.05), no correction of multiple testing was applied. Analyses were conducted on the maximum number of observations, missing values were not replaced. Calculations were conducted using SAS (version 9.4) software (SAS version 9.4, SAS Institute Inc., Cary, North Carolina, USA). Boxplots were generated using R (Version 4.3.0) software (R Foundation for Statistical Computing, Vienna, Austria).
3 Results
A total of 187 records of dogs and cats with a septic abdomen were identified, of which 109 were excluded. Exclusion was due to the absence of a timely performed blood gas (98), incomplete medical records (8) or the utilization of blood products prior to blood gas analysis (3). Details of exclusion can be found in Figure 1. Therefore, 61 dogs and 17 cats were included in the study. A total of 41 male dogs and cats were included (16 intact and 25 neutered), and 37 female (11 intact and 26 neutered). Mean age across all dogs and cats was 6.3 ± 3.7 years (6.5 ± 3.4 years in dogs; 5.5 ± 4.7 years in cats). Demographic data is represented in Table 1. There were 41 different dog breeds, with the most common ones crossbreeds (9), Belgian Malinois (3) and chihuahuas (3). There were 7 different cat breeds with domestic shorthair (9) being the most frequent. Underlying causes of septic peritonitis were gastrointestinal disruption in 47 dogs and cats (60.3%, 37 dogs and 9 cats), disruption of the urogenital tract in 9 (11.5%; 6 dogs and 3 cats), trauma in 4 (5.1%; 3 dogs and 1 cat), miscellaneous in 5 (6.4%; 4 dogs and 1 cat) and unknown in 13 cases (16.7%; 11 dogs and 2 cats).
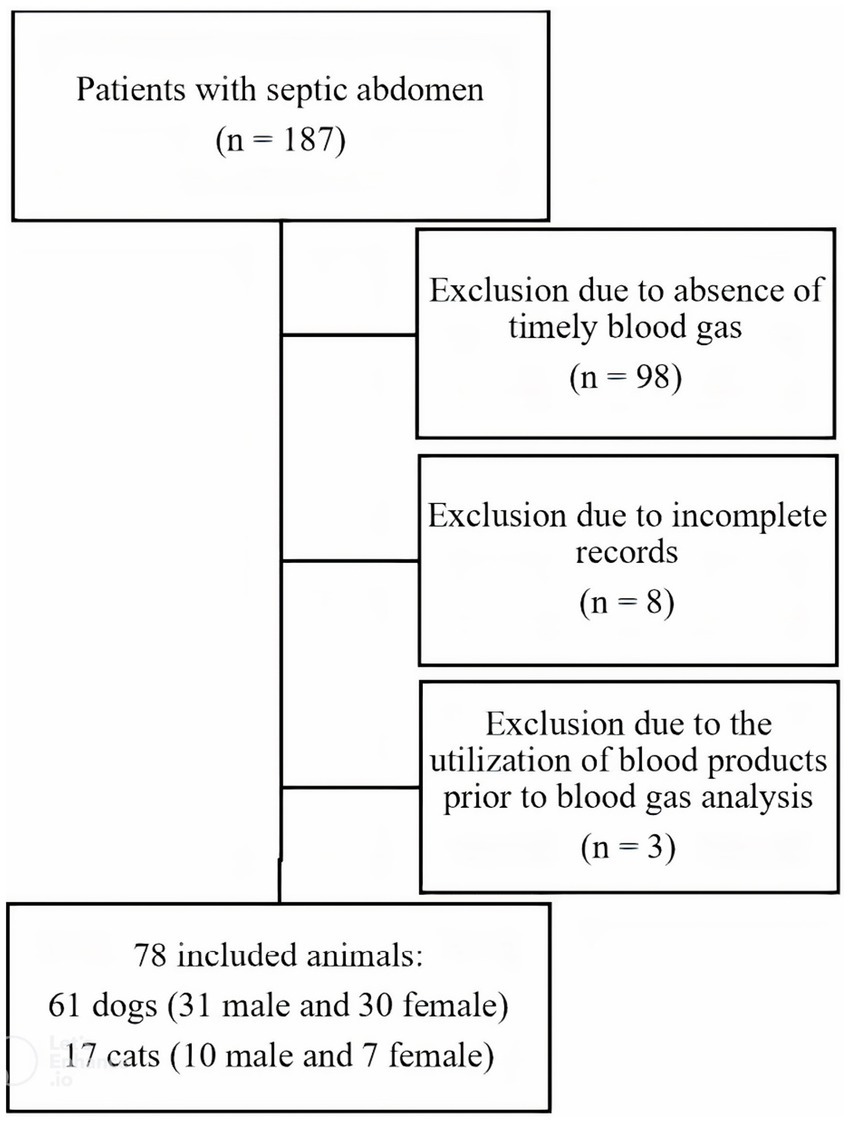
Figure 1. Flow chart representation of inclusion and exclusion process.
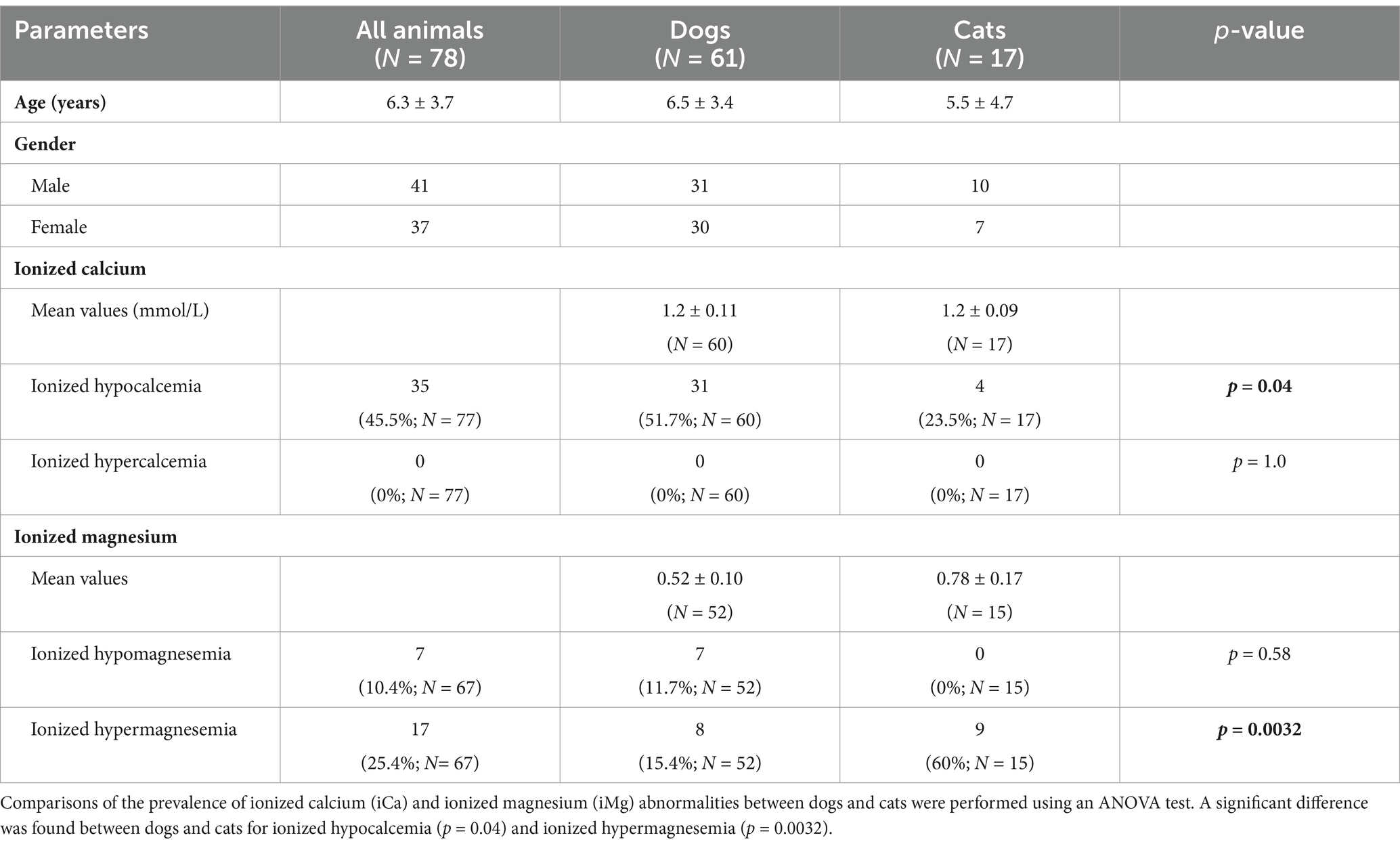
Table 1. Demographic data and prevalence of iCa and iMg disturbances in dogs and cats with septic peritonitis.
3.1 Calcium and magnesium disturbances
Calcium measurements were not available in 1 dog and magnesium measurements were not available in 9 dogs and 2 cats. The mean (±SD) iCa level was 1.2 ± 0.11 mmol/L in dogs and 1.2 ± 0.09 mmol/L in cats, with 51.7% of dogs (31/60) and 23.5% of cats (4/17) had hypocalcemia while none had ionized hypercalcemia. Ionized hypocalcemia at presentation was observed more frequently in dogs compared to cats (p = 0.040) (Figure 2). The mean (±SD) iMg level was 0.52 ± 0.10 mmol/L in dogs and 0.78 ± 0.17 in cats. 13.5% of dogs (7/52) presented with ionized hypomagnesemia, while 15.4% of dogs (8/52) presented with hypermagnesemia. No cat (0%) was presented with ionized hypomagnesemia, while 60% of cats (9/15) were presented with ionized hypermagnesemia. Ionized hypermagnesemia at presentation was observed more frequently in cats compared to dogs (p = 0.0032) (Figure 3). The prevalence of calcium and magnesium disturbances is presented in Table 1.
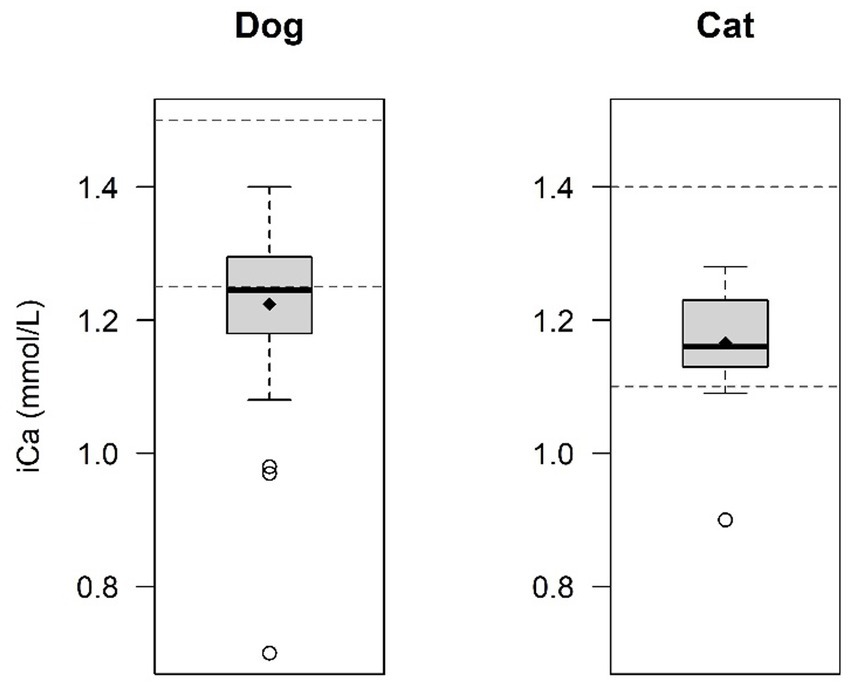
Figure 2. Comparison of ionized calcium (iCa) levels between dogs and cats. Ionized hypocalcaemia was significantly more frequent in dogs (51.7%) in comparison with cats (23.5%) (p = 0.040). The central line within each box represents the median, while the diamond represents the mean value. The box edges indicate the interquartile range (IQR; 25th-75th percentile). Whiskers extend to the smallest and largest values within 1.5x IQR, while points outside this range are considered outliers. The dashed lines indicate the normal reference range for dogs and cats.
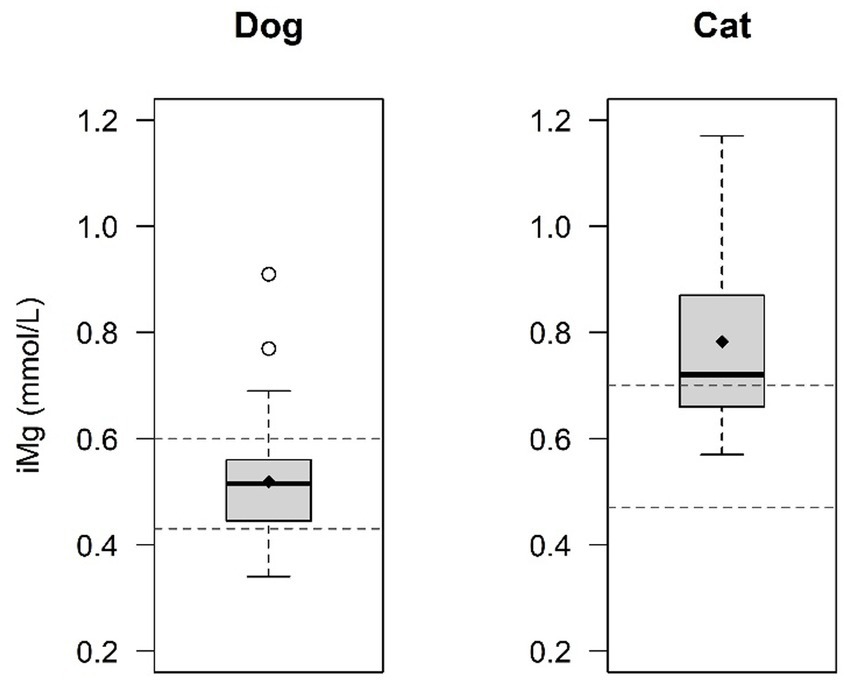
Figure 3. Comparison of ionized magnesium (iMg) levels between dogs and cats. Ionized hypermagnesemia is significantly more frequent in cats (60%) in comparison with dogs (13.3%) (p = 0.0032). The central line within each box represents the median, while the diamond represents the mean value. The box edges indicate the interquartile range (IQR; 25th-75th percentile). Whiskers extend to the smallest and largest values within 1.5x IQR, while points outside this range are considered outliers. The dashed lines indicate the normal reference range for dogs and cats.
3.2 Morbidity
The relationship between ionized calcium and ionized magnesium levels and the administration of vasopressors, antiarrhythmics, prokinetics, and plasma was analyzed in dogs, with the exclusion of dogs that were euthanized on admission. Due to the small sample size, the relationship between the presence of ionized hypocalcemia or ionized magnesium disturbances and the administration of vasopressors, antiarrhythmics, prokinetics and plasma could not be assessed in cats. In dogs, no statistically significant association was observed between the presence of hypocalcemia and the use of vasopressors (p = 0.32), antiarrhythmics (p = 0.68) or prokinetics (p = 0.72). A significant association was observed between ionized calcium levels and plasma administration during hospitalization in dogs. The prevalence of ionized hypocalcemia was higher in the plasma group, occurring in 73.3% of dogs compared to 41.2% in the group that did not receive plasma (p = 0.038). Results regarding the prevalence of ionized hypocalcemia in dogs and therapeutic interventions are represented in Table 2. The mean iCa concentration of dogs in the plasma group was 1.16 ± 0.16 mmol/L, compared to 1.25 ± 0.09 mmol/L in the group without plasma (p = 0.021). No significant difference could be found for the mean iCa concentration of dogs and the use of vasopressors (p = 0.24), antiarrhythmics (p = 0.52) and prokinetics (p = 0.60). Comparison of mean iCa values and administration of treatment during hospitalization in dogs is represented in Table 3.
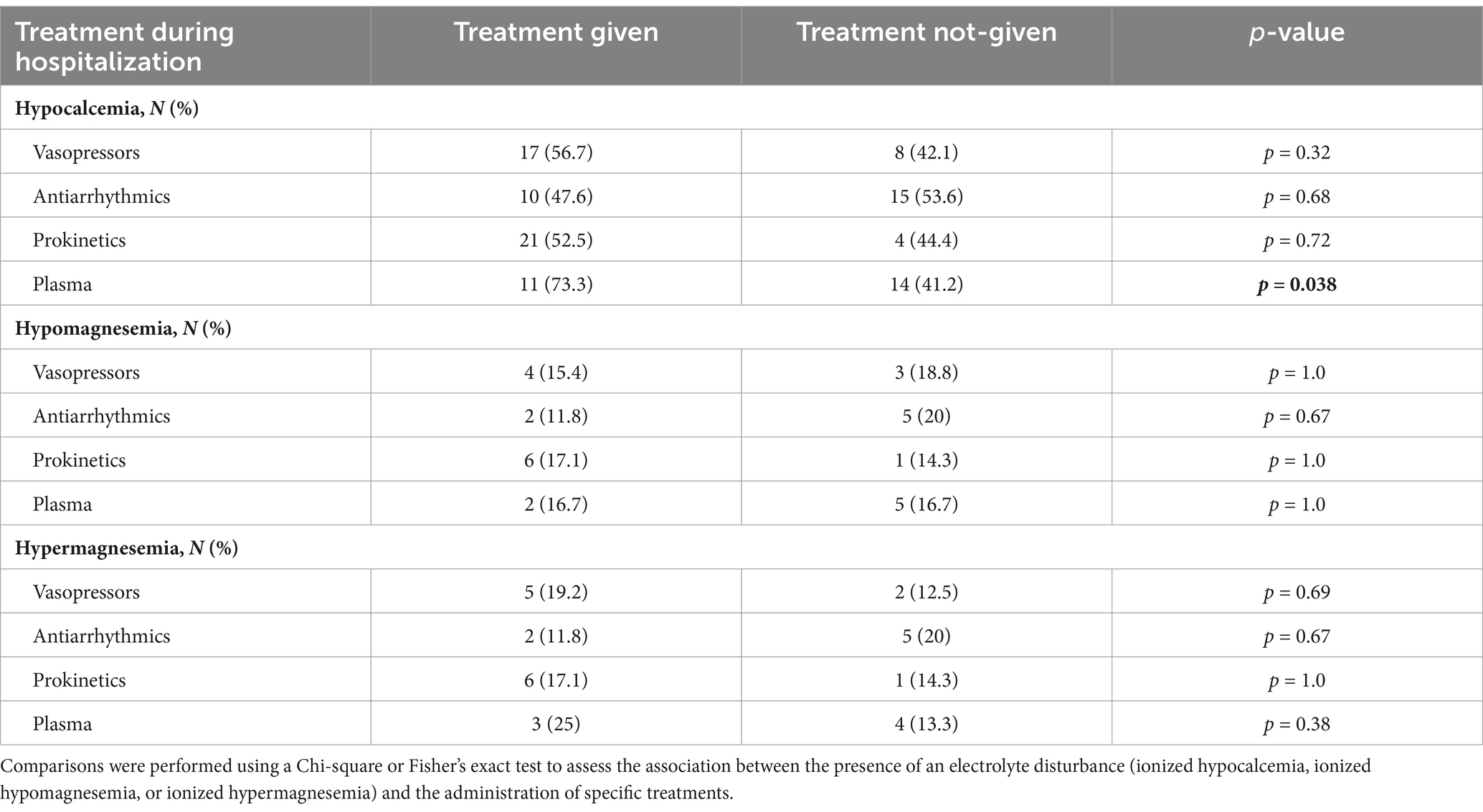
Table 2. Association of disturbances in iCa and iMg with therapy during hospitalization in dogs with septic peritonitis.
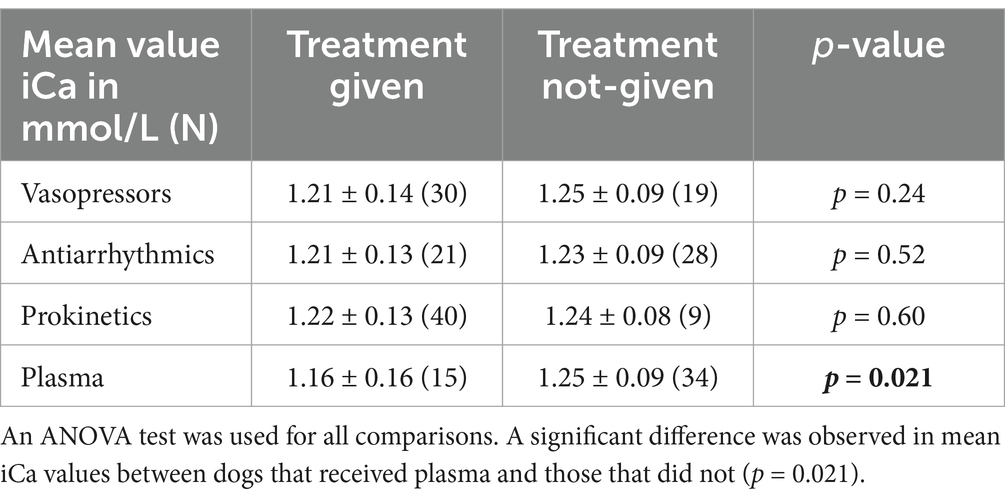
Table 3. Comparison of mean ionized calcium (iCa) values (mmol/L ± SD) in dogs and administration of treatment during hospitalization.
No significant association was found between the presence between hypo- or hypermagnesemia in dogs and the use of vasopressors (p = 1.0 and p = 0.69, respectively), antiarrhythmics (p = 0.67 and p = 0.67 respectively) prokinetics (p = 1.0 for both) or plasma (p = 1.0 and p = 0.38, respectively). Similarly, no association was found between the mean values of iMg in dogs and the use of vasopressors (p = 0.84), antiarrhythmics (p = 0.83), prokinetics (p = 0.25) and plasma (p = 0.86). Results regarding ionized hypomagnesemia or hypermagnesemia and therapeutic interventions are represented in Table 2. Comparison of mean iMg values and administration of treatment during hospitalization in dogs is represented in Table 4.
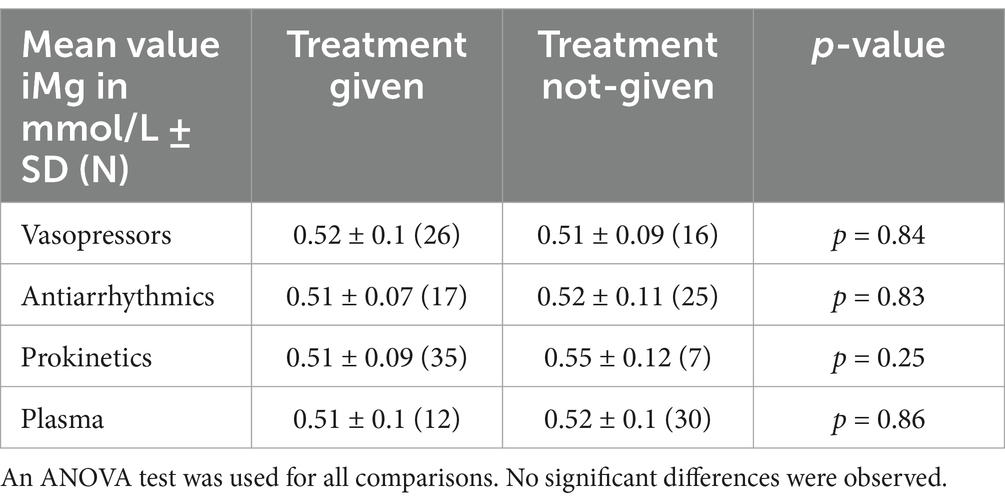
Table 4. Comparison of mean ionized magnesium (iMg) values (mmol/L ± SD) in dogs and administration of treatment during hospitalization.
There was no significant correlation between iCa and iMg values and the length of hospitalization in dogs (p = 0.62 and p = 0.62 respectively). Similarly, no significant correlation was identified between iCa and iMg values and the length of hospitalization in cats (p = 0.62 and p = 0.27 respectively).
3.3 Mortality
The survival rate of the dogs and cats included in this study was 50%. Of the 39 dogs and cats that died, 27 were euthanized (34.6%, 15 of them at presentation prior to therapeutic intervention) and 12 died due to a cardiorespiratory arrest (15.4%). Of the dogs with ionized hypocalcemia, 45.2% survived (14/31), compared to 58.6 (17/29) in dogs with normocalcemia (p = 0.30). No statistically significant difference was observed in mean iCa values between survivors and non-survivors in dogs (p = 0.59) (Table 5 and Figure 4). Among dogs with ionized hypomagnesemia, 71.4% (5/7) survived, compared to 37.5 (3/8) in the hypermagnesemic group and 46% (17/37) in the normomagnesemic group (p = 0.38). A statistically significant difference was observed when comparing the mean iMg values between survivors and non-survivor in dogs. Mean iMg was lower in the survivors group (0.49 ± 0.09 mmol/L) compared to the non-survivors group (0.55 ± 0.11 mmol/L) (p = 0.042) (Table 5 and Figure 5).
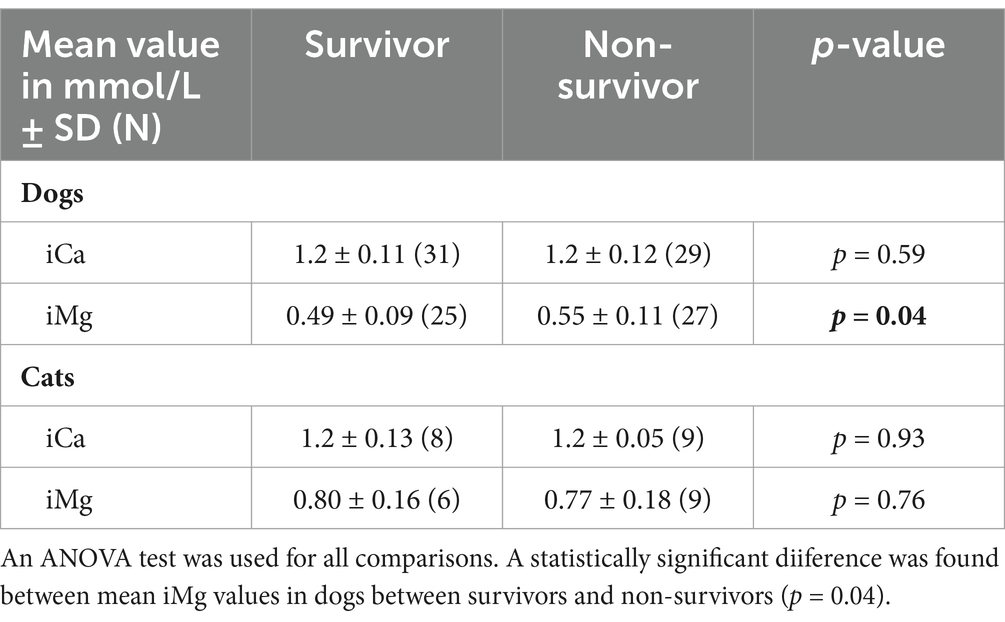
Table 5. Comparison of mean ionized calcium (iCa) and ionized magnesium (iMg) values (mmol/L ± SD) in dogs and cats between survivors and non-survivors.
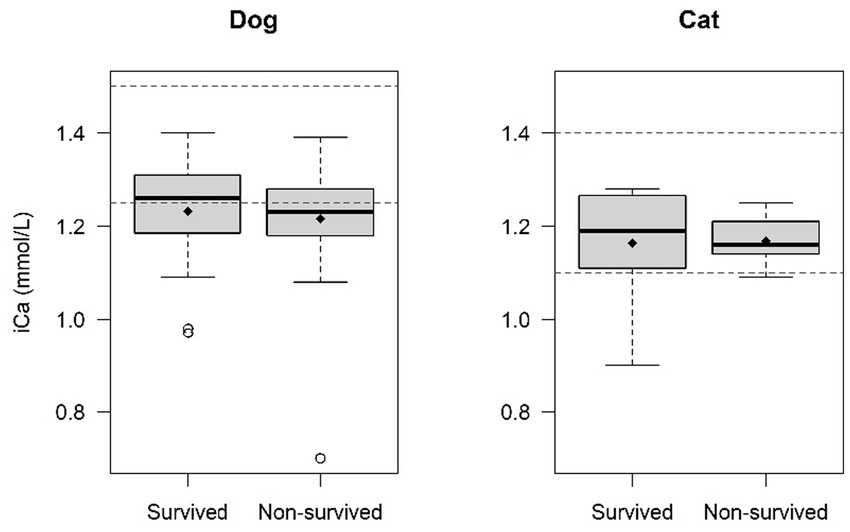
Figure 4. Comparison of ionized calcium (iCa) levels survivors and non-survivors. No statistical difference was found in mean iCa values between survivors and non-survivors in dogs (p = 0.59) and cats (p = 0.93). The central line within each box represents the median, while the diamond represents the mean value. The box edges indicate the interquartile range (IQR; 25th-75th percentile). Whiskers extend to the smallest and largest values within 1.5x IQR, while points outside this range are considered outliers. The dashed lines indicate the normal reference range for dogs and cats.

Figure 5. Comparison of ionized magnesium (iMg) levels between survivors and non-survivors. A statistically difference was found in mean iMg values between survivors and non-survivor in dogs. Mean iMg was lower in the survivors group (0.49 ± 0.09 mmol/L) compared to the non-survivors group (0.55 ± 0.11 mmol/L) (p = 0.042). No statistical difference was found in mean iMg values between survivors and non-survivors in cats (p = 0.76). The central line within each box represents the median, while the diamond represents the mean value. The box edges indicate the interquartile range (IQR; 25th-75th percentile). Whiskers extend to the smallest and largest values within 1.5x IQR, while points outside this range are considered outliers. The dashed lines indicate the normal reference range for dogs and cats.
Of the cats with ionized hypocalcemia, 75% survived (3/4), compared to 38.5% (5/13) in the 13 cats with normocalcemia (p = 0.29). Among cats with ionized hypermagnesemia, 55.6% (5/9) survived, compared to 16.7% (1/6) in the normomagnesemic group (p = 0.29). No statistically significant difference was observed in mean iCa or iMg values between survivors and non-survivors in cats (p = 0.93 and p = 0.76 respectively) (Table 5 and Figures 4, 5).
4 Discussion
In this cohort, the prevalence of ionized hypocalcemia in dogs with septic peritonitis was found to be 51.7%, which is notably higher than the previously reported prevalence of 16–24% in critically ill dogs (9–11). In contrast, the prevalence of ionized hypocalcemia in this cohort of cats with septic peritonitis was 23.5%, which is lower than previously reported values of 59–89% of cats with septic peritonitis (12, 13). Ionized hypercalcemia was not observed in the present study. The previously published studies reports on the prevalence of ionized hypocalcemia in dogs focused on all dogs admitted to the intensive care unit (ICU) (9) or dogs with parvoviral enteritis (11). With the exception for the study of Mouton et al., which solely focused on the development of sepsis during hospitalization, these studies identified an association between ionized hypocalcemia and septic conditions. The higher prevalence in this cohort of dogs with septic peritonitis compared to an overall population of critically ill dogs was therefore expected. The prevalence of ionized hypomagnesemia and ionized hypermagnesemia was 13.5% and 15.4% for dogs and 0% and 60% for cats, respectively. As previously stated, studies for iMg are mostly lacking in veterinary medicine. The prevalence of derangements in total magnesium in critically ill dogs and cats was previously reported to be 53–67% and 46%, respectively (11, 30, 36). However, studies in human medicine and in dogs have shown only poor to moderate correlation between ionized magnesium and total magnesium (28, 32, 33). The underlying hypothesis is that total magnesium levels are influenced by serum albumin concentrations. Additionally, in critically ill patients, there may be a redistribution of magnesium from the extracellular to the intracellular compartment. This shift can result in decreased total magnesium levels while preserving normal ionized magnesium concentrations (32). Any such correlation between total and ionized magnesium has been reported to be even weaker in ill rather than in healthy dogs (35). Total magnesium and ionized magnesium cannot be used interchangeably, and direct comparison of the prevalence in our cohort with these previously published data studying total magnesium levels is therefore not possible. Compared to the study of Murray et al., the prevalence of ionized hypomagnesemia is lower, while the prevalence of ionized hypermagnesemia is higher in this cohort (35). Two main factors may explain these differences. First, our study sample is larger than the previous study, which could contribute to variations in prevalence. Secondly, there is a difference in disease severity between the two populations. Murry et al. included all patients admitted for hospitalization through an emergency department, whereas our study focuses exclusively on patients with septic peritonitis. In this cohort, patients are more prone to develop sepsis and secondary consequences, which may influence magnesium metabolism and excretion. Compared to the study by Mann et al., both ionized hypo- and hypermagnesemia are more prevalent in this study, despite comparable study sample sizes and disease severity (34). Additionally, both studies even used the same reference intervals for ionized magnesium. A difference in disease severity could have explained this discrepancy; however, no direct comparison between the two studies was possible in this regard.
4.1 Morbidity
This is one of the first studies in veterinary medicine that investigates the clinical impact of disturbances in ionized calcium or ionized magnesium in dogs and cats with a septic peritonitis. In this study, a significant association was identified between ionized hypocalcemia and plasma administration during hospitalization in dogs. Plasma is commonly administered for managing hypocoagulability, and thus was used as a crude marker to explore the relationship between iCa levels and coagulopathies. Calcium (Ca2+) plays a critical role in multiple stages of the coagulation cascade (41), and hypocalcemia is associated with impaired coagulation. Plasma is also used for oncotic support in animals with hypoalbuminemia. Although hypoalbuminemia is associated with decreased total calcium levels [roughly 40% of circulating calcium is protein bound, it does not affect ionized calcium (42)].
Although both ionized calcium (iCa) and ionized magnesium (iMg) abnormalities can contribute to hypotension due to vasoplegia, cardiac arrythmias and gastrointestinal ileus, no significant association was observed between electrolyte derangements and the use of antiarrhythmics, prokinetics or vasopressors. However, we did not study whether patients demonstrated hyperemic mucous membranes or developed hypotension due to vasoplegia, nor did we assess motility via monitoring of by abdominal POCUS (43) or recording of gastric residual volume through a nasogastric feeding tube. Neither an ECG interpretation was included in this study. The administration of antiarrhythmics, vasopressors or prokinetics again served as a crude marker in an attempt to record associations between calcium and magnesium derangements and these complications.
No significant correlation was observed between iCa or iMg levels and the length of hospitalization in this study. This finding contrasts with a previous study by Holowaychuk et al., which reported a significantly longer hospitalization duration in dogs with ionized hypocalcemia (9). Similarly, a human study in critically ill paediatric patients found a significant correlation between hypocalcemia and the length of hospitalization (8). In contrast, our results align with those of Kellett-Gregory et al., who similarly found no association between iCa and iMg derangements in a disease group that is similar to ours (13). In the latter study, the authors hypothesized that variability in the administration of fluids or blood products prior to iCa measurement could have influenced results, but the design of our study appears to suggest differently.
Prior research in veterinary (36) and human medicine (8) has identified associations between iMg imbalances and hospitalization duration. However, those studies assessed iMg fluctuations throughout the entire hospitalization period. As previously stated, the evaluation of iCa and iMg during hospitalization was outside the scope of our study.
4.2 Mortality
The survival rate until discharge of the dogs and cats in this study was 50%. This is lower than or comparable to survival rates of previous studies (34.4–85%) on septic peritonitis in companion animals (13, 44–58). That said, our study included all dogs diagnosed with septic peritonitis and an available blood gas. As a consequence, the survival rate is potentially negatively impacted by the significant amount of dogs and cats euthanized after diagnosis without therapeutic intervention. Although the inclusion criteria for septic peritonitis were broad and could include dogs and cats with only a positive culture growth, more than 50% of treated dogs and cats required more than one vasopressor during hospitalization, indicating systemic involvement in our cohort. The current study did not identify an association between survival and the prevalence of iCa and iMg derangements, similarly to the papers from Holowaychuk et al. and Kellet-Gregory et al. This is in contrast with human and other veterinary medicine papers (1–3, 8, 10, 29, 30, 36, 59). In dogs, survivors had a significantly lower mean iMg concentration, although mean iMg values in both groups were within the reference range used in this study. In human studies, several hypotheses have been proposed to explain the association between elevated iMg and increased mortality. Ionized magnesium may serve as a marker of cellular damage, may indicate decreased renal perfusion, or reflect alterations due to acid–base imbalances (8, 28, 60). That said, our study was performed on a small sample, and values were only assessed upon presentation, and the clinical relevance of this observation therefore remains uncertain. Other studies additionally demonstrated an association between iCa and iMg levels during hospitalization and survival. A human paper showed higher mortality in critically ill patients that developed hypermagnesemia during hospitalization (28), whereas a study on ionized hypocalcemia in cats with septic peritonitis identified decreased survival in cats in which calcium levels failed to normalize (13). Assessing the evolution of iCa and iMg levels throughout hospitalization would have been insightful, but this was beyond the scope of the current study. A study on the evolution of these electrolytes during hospitalization would also require a larger sample size to account for the loss of patients during hospitalization and the large number of confounding factors. During the treatment of septic peritonitis numerous factors can indeed influence calcium and magnesium levels. To name a few, the administration of citrated blood products (61, 62), colloids (63) or 0.9% saline infusion can reduce iCa and iMg levels due to dilution effects or the calcium-binding properties of citrate (5, 24, 40, 64, 65).
4.3 Limitations
This study has several limitations. The reference ranges used in this study are those established by the authors institute, but were based on reference ranges in literature (40, 66). For the analyzer used in the study, the manufacturer did not establish internal reference ranges, and, to the author’s knowledge, no study has yet defined reference ranges specifically for this analyzer. The lack of an internal reference range may explain differences in prevalence rates compared to other studies. However, reference ranges in different sources based on different analyzers only show mild differences (5, 67, 68).
Due to the retrospective design of this study, blood samples were collected by multiple clinicians without standardized protocols for syringe filling, potentially introducing dilutional errors with heparin that could affect the measurements of ionized calcium (iCa) and ionized magnesium (iMg) (5, 27, 40, 66, 69). The measurement of ionized calcium (iCa) and ionized magnesium (iMg) can indeed be influenced by various factors. Proper sample collection and handling are critical, as chelation of Ca2+ and Mg2+ can occur in the presence of heparin or lactate (5, 27, 40, 66). Additionally, the presence of air bubbles in samples can affect iCa levels, as the alkalinization caused by gas exchange promotes increased protein binding of calcium, thereby reducing the ionized fraction of calcium (5, 66, 70). Our retrospective design does not allow us to exclude any of these effects on our samples.
Several comorbidities may influence iCa and iMg levels. Conditions such as trauma (71), neoplasia (72), renal failure (17, 72, 73), hyperthyroidism (64), pancreatitis (24, 74–76), hypoadrenocorticism (72), and diabetes mellitus (24, 77, 78), are known to affect iCa and iMg values. Similarly, medications such as furosemide (17, 64) and corticosteroids (5, 79) impact iCa and iMg levels. Additionally, several isotonic crystalloids, such as Lactated Ringer’s solution or Plasmalyte, contain small concentrations of calcium or magnesium (80). Dogs and cats that received these solutions from the referring veterinarian prior to arrival were not excluded from the study. In our study, several dogs and cats were affected by such conditions, or did receive treatments known to influence iCa and iMg levels. Three dogs and 1 cat had septic peritonitis secondary to trauma, 4 received long-term corticosteroid treatment, 1 received long-term furosemide therapy, and similarly there was a single patient suffering from chronic kidney disease, acute renal failure, apocrine gland anal sac adenocarcinoma, or hyperthyroidism. Previous observational studies in both human and veterinary medicine (2, 8–10, 13, 28–30, 81) did not exclude patients with these comorbidities.
An additional limitation of this study is the small sample size. The limited overall sample size may have influenced results, as some borderline findings could have reached significance with a larger sample. Caution should therefore be warranted when interpreting the potential influence of comorbidities. As there is an indication that dogs and cats might have a difference in the metabolism of calcium (82) and magnesium (83), it was decided to investigate dogs and cats as separate groups. Due to the limited sample size in cats, morbidity analysis could not be conducted. Larger prospective studies are warranted to avoid any type II error.
The possible associations between iCa and iMg disturbances and arrhythmias, vasodilatory shock, gastrointestinal ileus, and coagulation disorders were not directly assessed as our medical records did not allow to diligently track this information. Rather we recorded the use of vasopressors, anti-arrhythmics, prokinetics, and plasma transfusions and investigated their association with iCa and iMg derangements. The authors acknowledge the strong limitation of such analyses, as treatments may have been motivated by other factors, and inversely a lack of treatment does not imply an absence of the condition. Any identified association or lack thereof should therefore be confirmed in further prospective studies in which precise monitoring for such conditions seems warranted.
In conclusion, ionized hypocalcemia was significantly more common in dogs than cats with septic peritonitis and associated with an increased use of plasma during hospitalization. The prevalence of hypo- and hypermagnesemia in dogs was low, no correlation of magnesium disturbances had a significant clinical impact. Hypermagnesemia, although still rare in cats, was significantly more common than in dogs, whereas hypomagnesemia was not detected. The clinical significance of derangements at presentation in our study population seemed limited, without impact on survival to discharge.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the studies involving animals in accordance with the local legislation and institutional requirements because this is a retrospective study on available clinical data. Written informed consent was not obtained from the owners for the participation of their animals in this study because it is a retrospective study on available clinical data.
Author contributions
CD: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. LG: Conceptualization, Data curation, Writing – review & editing. SN: Conceptualization, Writing – review & editing. DP: Writing – review & editing. KG: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to acknowledge Nathalie Maes, of the Biostatistics and Research Methods Center of the University Hospital of Liège, for their statistical expertise and assistance in performing the data analysis for this study. Their contributions were important in ensuring the reliability of the statistical methods applied.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zivin, JR, Gooley, T, Zager, RA, and Ryan, MJ. Hypocalcemia: a pervasive metabolic abnormality in the critically ill. Am J Kidney Dis. (2001) 37:689–98. doi: 10.1016/S0272-6386(01)80116-5
2. Desai, TK, Carlson, RW, and Geheb, MA. Prevalence and clinical implications of hypocalcemia in acutely III patients in a medical intensive care setting. Am J Med. (1988) 84:209–14. doi: 10.1016/0002-9343(88)90415-9
3. Zaloga, GP. The multifactorial basis for hypocalcemia during Sepsis: studies of the parathyroid hormone-vitamin D Axis. Ann Intern Med. (1987) 107:36–41. doi: 10.7326/0003-4819-107-1-36
4. Cairns, CB, Niemann, JT, Pelikan, PC, and Sharma, J. Ionized hypocalcemia during prolonged cardiac arrest and closed-chest CPR in a canine model. Ann Emerg Med. (1991) 20:1178–82. doi: 10.1016/S0196-0644(05)81466-0
5. Schenck, PA, Chew, DJ, Nagode, LA, and Rosol, TJ. Disorders of Calcium: Hypercalcemia and Hypocalcemia. In: DiBartola SP, editor. Fluid, electrolyte, and acid-base disorders in small animal practice, Fourth Edition. St. Louis, Missouri: Elsevier, (2012), pp. 120–194.
6. Holowaychuk, MK. Hypocalcemia of critical illness in dogs and cats. Vet Clin North Am Small Anim Pract. (2013) 43:1299–317. doi: 10.1016/j.cvsm.2013.07.008
7. Steinhorn, DM, Sweeney, MF, and Layman, LK. Pharmacodynamic response to ionized calcium during acute sepsis. Crit Care Med. (1990) 18:851–7. doi: 10.1097/00003246-199008000-00012
8. Broner, CW, Stidham, GL, Westenkirchner, DF, and Tolley, EA. Hypermagnesemia and hypocalcemia as predictors of high mortality in critically ill pediatric patients. Crit Care Med. (1990) 18:921–8. doi: 10.1097/00003246-199009000-00004
9. Holowaychuk, MK, Hansen, BD, DeFrancesco, TC, and Marks, SL. Ionized hypocalcemia in critically ill dogs. J Vet Intern Med. (2009) 23:509–13. doi: 10.1111/j.1939-1676.2009.0280.x
10. Luschini, MA, Fletcher, DJ, and Schoeffler, GL. Retrospective study: incidence of ionized hypocalcemia in septic dogs and its association with morbidity and mortality: 58 cases (2006–2007). J Vet Emerg Crit Care. (2010) 20:406–12. doi: 10.1111/j.1476-4431.2010.00553.x
11. Mouton, A, Celliers, A, Thompson, PN, Mellanby, RJ, and Schoeman, JP. Calcium and magnesium abnormalities in puppies with parvoviral enteritis. Am J Vet Res. (2025) 86:187. doi: 10.2460/ajvr.24.07.0187
12. Costello, MF, Drobatz, KJ, Aronson, LR, and King, LG. Underlying cause, pathophysiologic abnormalities, and response to treatment in cats with septic peritonitis: 51 cases (1990–2001). J Am Vet Med Assoc. (2004) 225:897–902. doi: 10.2460/javma.2004.225.897
13. Kellett-Gregory, LM, Mittleman Boller, E, Brown, DC, and Silverstein, DC. Retrospective study: ionized calcium concentrations in cats with septic peritonitis: 55 cases (1990–2008). J Vet Emerg Crit Care. (2010) 20:398–405. doi: 10.1111/j.1476-4431.2010.00562.x
14. Nakaigawa, Y, Akazawa, S, Shimizu, R, Ishii, R, Ikeno, S, Inoue, S, et al. Effects of magnesium sulphate on the cardiovascular system, coronary circulation and myocardial metabolism in anaesthetized dogs. Br J Anaesth. (1997) 79:363–8. doi: 10.1093/bja/79.3.363
15. Nakayama, T, Nakayama, H, Miyamoto, M, and Hamlin, RL. Hemodynamic and electrocardiographic effects of magnesium sulfate in healthy dogs. J Vet Intern Med. (1999) 13:485–90. doi: 10.1111/j.1939-1676.1999.tb01467.x
16. Arsenian, MA. Magnesium and cardiovascular disease. Prog Cardiovasc Dis. (1993) 35:271–310. doi: 10.1016/0033-0620(93)90008-2
17. Tong, GM, and Rude, RK. Magnesium deficiency in critical illness. J Intensive Care Med. (2005) 20:3–17. doi: 10.1177/0885066604271539
18. Tsuji, H, Venditti, FJ, Evans, JC, Larson, MG, and Levy, D. The associations of levels of serum potassium and magnesium with ventricular premature complexes (the Framingham heart study). Am J Cardiol. (1994) 74:232–5. doi: 10.1016/0002-9149(94)90362-X
19. Shils, ME. Experimental human magnesium depletion. Medicine (Baltimore). (1969) 48:61–85. doi: 10.1097/00005792-196901000-00003
20. Whang, R, Flink, EB, Dyckner, T, Wester, PO, Aikawa, JK, and Ryan, MP. Magnesium depletion as a cause of refractory potassium repletion. Arch Intern Med. (1985) 145:1686–9. doi: 10.1001/archinte.1985.00360090162024
21. Rude, RK, Oldham, SB, and Singer, FR. Functional hypoparathyroidism and parathyroid hormone end-organ resistance in human magnesium deficiency. Clin Endocrinol. (1976) 5:209–24. doi: 10.1111/j.1365-2265.1976.tb01947.x
22. Huerta, MG, Roemmich, JN, Kington, ML, Bovbjerg, VE, Weltman, AL, Holmes, VF, et al. Magnesium deficiency is associated with insulin resistance in obese children. Diabetes Care. (2005) 28:1175–81. doi: 10.2337/diacare.28.5.1175
23. Nadler, JL, Buchanan, T, Natarajan, R, Antonipillai, I, Bergman, R, and Rude, R. Magnesium deficiency produces insulin resistance and increased thromboxane synthesis. Hypertens Dallas Tex. (1993) 21:1024–9. doi: 10.1161/01.hyp.21.6.1024
24. Ahmed, F, and Mohammed, A. Magnesium: the forgotten electrolyte—a review on hypomagnesemia. Med Sci. (2019) 7:56. doi: 10.3390/medsci7040056
25. Garcia-Lopez, JM, Provost, PJ, Rush, JE, Zicker, SC, Burmaster, H, and Freeman, LM. Prevalence and prognostic importance of hypomagnesemia and hypocalcemia in horses that have colic surgery. Am J Vet Res. (2001) 62:7–12. doi: 10.2460/ajvr.2001.62.7
26. Humphrey, S, Kirby, R, and Rudloff, E. Magnesium physiology and clinical therapy in veterinary critical care. J Vet Emerg Crit Care. (2015) 25:210–25. doi: 10.1111/vec.12253
27. Martin, LG, and Allen-Durrance, AE. Magnesium and phosphate disorders. In: Small animal critical care medicine, Third Edition. St. Louis, Missouri: Elsevier (2023), pp. 341–348.
28. Escuela, MP, Guerra, M, Anon, JM, Martinez-Vizcaino, V, Zapatero, MD, Garcia-Jalon, A, et al. Total and ionized serum magnesium in critically ill patients. Intensive Care Med. (2005) 31:151–6. doi: 10.1007/s00134-004-2508-x
29. Salem, M, Stacey, J, and Chemow, B. Ionized magnesium values un critically ill patients - a novel ion selective electrode for determining free extracellular magnesium concentrations. Crit Care Med. (1993) 21:S256. doi: 10.1097/00003246-199304001-00246
30. Martin, LG, Matteson, VL, Wingfield, WE, Van Pelt, DR, and Hackett, TB. Abnormalities of serum magnesium in critically III dogs: incidence and implications. J Vet Emerg Crit Care. (1994) 4:15–20. doi: 10.1111/j.1476-4431.1994.tb00111.x
31. Woods, GA, Oikonomidis, IL, Gow, AG, Tørnqvist-Johnsen, C, Boyé, P, Chng, Y, et al. Investigation of hypomagnesaemia prevalence and underlying aetiology in a hospitalised cohort of dogs with ionised hypocalcaemia. Vet Rec. (2021) 189:e301. doi: 10.1002/vetr.301
32. Brainard, BM, Campbell, VL, Drobatz, KJ, and Perkowski, SZ. The effects of surgery and anesthesia on blood magnesium and calcium concentrations in canine and feline patients. Vet Anaesth Analg. (2007) 34:89–98. doi: 10.1111/j.1467-2995.2006.00300.x
33. Külpmann, WR, and Gerlach, M. Relationship between ionized and total magnesium in serum. Scand J Clin Lab Invest. (1996) 56:251–8. doi: 10.3109/00365519609088645
34. Mann, FA, Boon, GD, Wagner-Mann, CC, Ruben, DS, and Harrington, DP. Ionized and total magnesium concentrations in blood from dogs with naturally acquired parvoviral enteritis. J Am Vet Med Assoc. (1998) 212:1398–401. doi: 10.2460/javma.1998.212.09.1398
35. Murray, ME, Boiron, L, Buriko, Y, Drobatz, K, and Waddell, LS. Total serum and ionized magnesium concentrations in healthy and hospitalized dogs. J Vet Emerg Crit Care. (2023) 33:427–34. doi: 10.1111/vec.13302
36. Toll, J, Erb, H, Bimbaum, N, and Schermerhorn, T. Prevalence and incidence of serum magnesium abnormalities in hospitalized cats. J Vet Intern Med. (2002) 16:217–21. doi: 10.1111/j.1939-1676.2002.tb02360.x
37. Wang, D, Zheng, J, Hu, Q, Zhao, C, Chen, Q, Shi, P, et al. Magnesium protects against sepsis by blocking gasdermin D N-terminal-induced pyroptosis. Cell Death Differ. (2020) 27:466–81. doi: 10.1038/s41418-019-0366-x
38. Ragetly, GR, Bennett, RA, and Ragetly, CA. Septic peritonitis: etiology, pathophysiology, and diagnosis. Compend Contin Educ Vet. (2011) 33:quizE7.
39. Saunders, WB, and Tobias, KM. Pneumoperitoneum in dogs and cats: 39 cases (1983–2002). J Am Vet Med Assoc. (2003) 223:462–8. doi: 10.2460/javma.2003.223.462
40. Felipe de Brito Galvao, J, Chew, DJ, and Green, TA. Calcium disorders. In: Silverstein DC, Hopper K, editors. Small animal critical care medicine, Third Edition. St. Louis, Missouri: Elsevier (2023), pp. 332–340.
41. Zou, Y, Li, H, Teng, L, Wang, Q, Wang, X, and Zhang, J. Hypocalcemia and acute traumatic coagulation disease. Int J Phys Med Rehabil. (2024) 12:734. doi: 10.35248/2329-9096.24.12.734
42. Naafs, MA. Hypocalcemia in the critically ill: a mini-review. Endocrinol Int J. (2017) 5:130. doi: 10.15406/emij.2017.05.00130
43. Sanderson, JJ, Boysen, SR, McMurray, JM, Lee, A, and Stillion, JR. The effect of fasting on gastrointestinal motility in healthy dogs as assessed by sonography. J Vet Emerg Crit Care. (2017) 27:645–50. doi: 10.1111/vec.12673
44. Abelson, AL, Buckley, GJ, and Rozanski, EA. Positive impact of an emergency department protocol on time to antimicrobial administration in dogs with septic peritonitis. J Vet Emerg Crit Care. (2013) 23:551–6. doi: 10.1111/vec.12092
45. Adams, RJ, Doyle, RS, Bray, JP, and Burton, CA. Closed suction drainage for treatment of septic peritonitis of confirmed gastrointestinal origin in 20 dogs. Vet Surg. (2014) 43:843–51. doi: 10.1111/j.1532-950X.2014.12258.x
46. Anderson, T, Beever, L, Hall, J, Moores, A, Llanos, C, Adams, R, et al. Outcome following surgery to treat septic peritonitis in 95 cats in the United Kingdom. J Small Anim Pract. (2021) 62:744–9. doi: 10.1111/jsap.13346
47. Cortellini, S, Seth, M, and Kellett-Gregory, LM. Plasma lactate concentrations in septic peritonitis: a retrospective study of 83 dogs (2007–2012). J Vet Emerg Crit Care. (2015) 25:388–95. doi: 10.1111/vec.12234
48. Craft, EM, and Powell, LL. The use of canine-specific albumin in dogs with septic peritonitis. J Vet Emerg Crit Care. (2012) 22:631–9. doi: 10.1111/j.1476-4431.2012.00819.x
49. Dayer, T, Howard, J, and Spreng, D. Septic peritonitis from pyloric and non-pyloric gastrointestinal perforation: prognostic factors in 44 dogs and 11 cats. J Small Anim Pract. (2013) 54:625–9. doi: 10.1111/jsap.12151
50. Dickinson, AE, Summers, JF, Wignal, J, Boag, AK, and Keir, I. Impact of appropriate empirical antimicrobial therapy on outcome of dogs with septic peritonitis. J Vet Emerg Crit Care. (2015) 25:152–9. doi: 10.1111/vec.12273
51. Grimes, J, Schmiedt, C, Milovancev, M, Radlinsky, M, and Cornell, K. Efficacy of serosal patching in dogs with septic peritonitis. J Am Anim Hosp Assoc. (2013) 49:246–9. doi: 10.5326/JAAHA-MS-5870
52. Hodgson, N, Llewellyn, EA, and Schaeffer, DJ. Utility and prognostic significance of neutrophil-to-lymphocyte ratio in dogs with septic peritonitis. J Am Anim Hosp Assoc. (2018) 54:351–9. doi: 10.5326/JAAHA-MS-6808
53. Lanz, O, Ellison, G, Bellah, Weichman, G, and VanGilder, J. Surgical treatment of septic peritonitis without abdominal drainage in 28 dogs. J Am Anim Hosp Assoc. (2001) 37:87–92. doi: 10.5326/15473317-37-1-87
54. Martiny, P, and Goggs, R. Biomarker guided diagnosis of septic peritonitis in dogs. Front Vet Sci. (2019) 6:208. doi: 10.3389/fvets.2019.00208
55. Parsons, KJ, Owen, LJ, Lee, K, Tivers, MS, and Gregory, SP. A retrospective study of surgically treated cases of septic peritonitis in the cat (2000–2007). J Small Anim Pract. (2009) 50:518–24. doi: 10.1111/j.1748-5827.2009.00790.x
56. Ruthrauff, CM, Smith, J, and Glerum, L. Primary bacterial septic peritonitis in cats: 13 cases. J Am Anim Hosp Assoc. (2009) 45:268–76. doi: 10.5326/0450268
57. Shipov, A, Lenchner, I, Milgram, J, Libkind, R, Klainbart, S, Segev, G, et al. Aetiology, clinical parameters and outcome in 113 dogs surgically treated for septic peritonitis (2004–2020). Vet Rec. (2023) 192:e2134. doi: 10.1002/vetr.2134
58. Staatz, AJ, Monnet, E, and Seim, HB. Open peritoneal drainage versus primary closure for the treatment of septic peritonitis in dogs and cats: 42 cases (1993–1999). Vet Surg. (2002) 31:174–80. doi: 10.1053/jvet.2002.31043
59. Chalifoux, NV, Parker, SE, and Cosford, KL. Prognostic indicators at presentation for canine parvoviral enteritis: 322 cases (2001-2018). J Vet Emerg Crit Care. (2021) 31:402–13. doi: 10.1111/vec.13052
60. Stevens, JS, Moses, AA, Nickolas, TL, Husain, SA, and Mohan, S. Increased mortality associated with Hypermagnesemia in severe COVID-19 illness. Kidney. (2021) 2:1087–94. doi: 10.34067/KID.0002592021
61. Giancarelli, A, Birrer, KL, Alban, RF, Hobbs, BP, and Liu-DeRyke, X. Hypocalcemia in trauma patients receiving massive transfusion. J Surg Res. (2016) 202:182–7. doi: 10.1016/j.jss.2015.12.036
62. Ward, RT, Colton, DM, Meade, PC, Henry, J-C, Contreras, L-M, Wilson, OM, et al. Serum levels of calcium and albumin in survivors versus nonsurvivors after critical injury. J Crit Care. (2004) 19:54–64. doi: 10.1016/j.jcrc.2004.02.011
63. Vivien, B, Langeron, O, Morell, E, Devilliers, C, Carli, PA, Coriat, P, et al. Early hypocalcemia in severe trauma. Crit Care Med. (2005) 33:1946–52. doi: 10.1097/01.CCM.0000171840.01892.36
64. Martin, LG, Wingfield, WE, Van Pelt, DR, and Hackett, TB. Magnesium in the 1990’s: implications for veterinary critical care. J Vet Emerg Crit Care. (1993) 3:106–14. doi: 10.1111/j.1476-4431.1993.tb00108.x
65. Nakamura, T, Ichikawa, S, Sakamaki, T, Sato, K, Fujie, M, Kurashina, T, et al. Effect of saline infusion on urinary calcium excretion in essential hypertension. Am J Hypertens. (1991) 4:113–8. doi: 10.1093/ajh/4.2.113
66. Wolf, J, and Silverstein, DC. Blood gas sampling. In: Silverstein DC, Hopper K, editors. In: Small animal critical care medicine, Third Edition. St. Louis, Missouri: Elsevier (2023), pp. 1153–1156.
67. Bateman, S. Disorders of magnesium: magnesium deficit and excess. In: DiBartola SP, editor. Fluid, electrolyte, and acid-base disorders in small animal practice, Fourth Edition. St. Louis, Missouri: Elsevier (2012), pp. 212–229.
68. Gilroy, C, Horney, B, Burton, S, and MacKenzie, A. Evaluation of ionized and total serum magnesium concentrations in hyperthyroid cats. Can J Vet Res. (2006) 70:137–42.
69. Hopper, K, Rezende, ML, and Haskins, SC. Assessment of the effect of dilution of blood samples with sodium heparin on blood gas, electrolyte, and lactate measurements in dogs. Am J Vet Res. (2005) 66:656–60. doi: 10.2460/ajvr.2005.66.656
70. Mazaki-Tovi, M, Topol, S, and Aroch, I. Effect of pH and storage conditions on measured ionised calcium concentration in dogs and cats. Vet Rec. (2020) 187:e72. doi: 10.1136/vr.105900
71. Holowaychuk, MK, and Monteith, G. Ionized hypocalcemia as a prognostic indicator in dogs following trauma. J Vet Emerg Crit Care. (2011) 21:521–30. doi: 10.1111/j.1476-4431.2011.00675.x
72. Messinger, JS, Windham, WR, and Ward, CR. Ionized hypercalcemia in dogs: a retrospective study of 109 cases (1998–2003). J Vet Intern Med. (2009) 23:514–9. doi: 10.1111/j.1939-1676.2009.0288.x
73. Chew, DJ, and Meuten, DJ. Disorders of calcium and phosphorus metabolism. Vet Clin North Am Small Anim Pract. (1982) 12:411–38. doi: 10.1016/S0195-5616(82)50053-8
74. Bhattacharya, SK, Luther, RW, Pate, JW, Crawford, AJ, Moore, OF, Pitcock, JA, et al. Soft tissue calcium and magnesium content in acute pancreatitis in the dog: calcium accumulation, a mechanism for hypocalcemia in acute pancreatitis. J Lab Clin Med. (1985) 105:422–7.
75. Dias, C, and Carreira, LM. Serum ionised calcium as a prognostic risk factor in the clinical course of pancreatitis in cats. J Feline Med Surg. (2015) 17:984–90. doi: 10.1177/1098612X14564203
76. Kimmel, SE, Washabau, RJ, and Drobatz, KJ. Incidence and prognostic value of low plasma ionized calcium concentration in cats with acute pancreatitis: 46 cases (1996-1998). J Am Vet Med Assoc. (2001) 219:1105–9. doi: 10.2460/javma.2001.219.1105
77. Hess, RS, Saunders, HM, Van Winkle, TJ, and Ward, CR. Concurrent disorders in dogs with diabetes mellitus: 221 cases (1993-1998). J Am Vet Med Assoc. (2000) 217:1166–73. doi: 10.2460/javma.2000.217.1166
78. Norris, CR, Nelson, RW, and Christopher, MM. Serum total and ionized magnesium concentrations and urinary fractional excretion of magnesium in cats with diabetes mellitus and diabetic ketoacidosis. J Am Vet Med Assoc. (1999) 215:1455–9. doi: 10.2460/javma.1999.215.10.1455
79. Korkor, AB, Kuchibotla, J, Arrieh, M, Gray, RW, and Gleason, WA. The effects of chronic prednisone administration on intestinal receptors for 1,25-dihydroxyvitamin D3 in the dog. Endocrinology. (1985) 117:2267–73. doi: 10.1210/endo-117-6-2267
80. Semler, MW, and Kellum, JA. Balanced crystalloid solutions. Am J Respir Crit Care Med. (2019) 199:952–60. doi: 10.1164/rccm.201809-1677CI
81. Khanna, C, Lund, EM, Raffe, M, and Armstrong, PJ. Hypomagnesemia in 188 dogs: a hospital population-based prevalence study. J Vet Intern Med. (1998) 12:304–9. doi: 10.1111/j.1939-1676.1998.tb02126.x
82. Stockman, J, Villaverde, C, and Corbee, RJ. Calcium, phosphorus, and vitamin D in dogs and cats. Vet Clin North Am Small Anim Pract. (2021) 51:623–34. doi: 10.1016/j.cvsm.2021.01.003
Keywords: ionized hypocalcemia, ionized hypermagnesemia, critical illness, calcium metabolism, septic abdomen, ionized hypomagnesemia
Citation: Debie C, Giberto L, Noel S, Paepe D and Gommeren K (2025) Ionized calcium and ionized magnesium disturbances in dogs and cats with septic peritonitis. Front. Vet. Sci. 12:1550701. doi: 10.3389/fvets.2025.1550701
Edited by:
Guillaume Laurent Hoareau, University of Utah Medical Center, United StatesReviewed by:
Giacomo Stanzani, University College London, United KingdomNoa Berlin, Tufts University, United States
Copyright © 2025 Debie, Giberto, Noel, Paepe and Gommeren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiara Debie, Y2hpYXJhLmRlYmllQHVsaWVnZS5iZQ==