 Quinn Rausch1*
Quinn Rausch1* Maryam Alhamdan2
Maryam Alhamdan2 Shane Bateman1Michelle Evason3Valli Fraser-Celin4
Shane Bateman1Michelle Evason3Valli Fraser-Celin4 Courtney Graham1Jamie Saad5Michelle Tuma4Karen Ward6
Courtney Graham1Jamie Saad5Michelle Tuma4Karen Ward6 Lauren Van Patter1
Lauren Van Patter1- 1Department of Clinical Studies, Ontario Veterinary College, University of Guelph, Guelph, ON, Canada
- 2Department of Animal Biosciences, Ontario Agricultural College, University of Guelph, Guelph, ON, Canada
- 3Antech/Mars Science & Diagnostics, Fountain Valley, CA, United States
- 4Veterinarians Without Borders North America, Ottawa, ON, Canada
- 5SPCA de Montréal, Montreal, QC, Canada
- 6Toronto Humane Society, Toronto, ON, Canada
Introduction: Many Canadians struggle to access healthcare for their animals, but little data is available from the Canadian context on how barriers to care are being addressed, and with what effects.
Methods: The aim of this research was to characterize service providing organizations, barrier mitigation tools, community partnerships, and evaluation metrics used by organizations attempting to increase access to animal healthcare in Canada. In this study, we conducted online data mining and a cross-sectional, mixed-methods organizational survey.
Results: Responses to the survey (N = 97) were received from non-profit organizations (52%), for-profit clinics (38%), and several municipal or governmental services (4%) and educational institutes (5%). Commonly reported tools included no cost or low-cost services, pop-up clinics and providing items to assist with pet transportation, with many other tools (payment plans without a credit check, services in multiple languages, availability of assistive technology) being employed by fewer than 20% of responding organizations. Only 38% of organizations used at least one tool from each of the four categories of barriers. Community involvement in programs ranged from simply accessing the service when it was available (outreach) to giving occasional feedback on their experiences (consulting), being employed or volunteering in program provision (collaborating), and community leadership partnering on initiatives (sharing leadership). Program evaluation most often involved quantitative measures of service usage with fewer organizations formally soliciting feedback from the community or looking at long-term health impacts.
Discussion: Responses demonstrate that organizations employ a wide range of tools to mitigate access to veterinary care barriers primarily along financial and geographical lines, and to a lesser extent with tools targeting cultural or disability-related barriers highlighting the importance of building capacity around addressing multiple intersecting barriers. Study findings provide a baseline characterization of current efforts by Canadian organizations to mitigate barriers to accessing animal healthcare.
1 Introduction
In Canada, an estimated 60% of individuals/families have at least one companion animal, primarily a dog or a cat (1). A significant percentage of these multi-species families in Canada experience barriers to accessing healthcare for their animals. According to extrapolations from a recent survey, at least 1.62 million families face barriers to accessing preventative care, 1.08 million face barriers to accessing sick care, and 719,000 face barriers to accessing emergency care (2). Additionally, using the Index of Care Accessibility, Neal and colleagues (2024) concluded that almost 4 million households across Canada fell within the lowest accessibility ranking. These numbers are expected to be a significant underestimation because communities most likely to face barriers, such as remote Indigenous Nations, those experiencing disability, homelessness, mental illness, and/or unemployment (3, 4), were not included in the survey. Additionally, the Yukon, Northwest Territories and Nunavut, which are the geographic areas with the most significant barriers to accessing care (5, 6) were not mapped using the Index of Care Accessibility.
Barriers to accessing animal healthcare services are diverse and often very context specific. Experiences of barriers to care have been linked to recent immigrants and young age in Canada (2) and ethnicity, low income, young age, geographic area, and lower education level in the United States (7, 8). Overall, the most prominent barriers cited in access to care literature are affordability of care (2, 3, 9–11) and geographic accessibility of care (4, 7, 8, 10–12). Other notable barriers present in the literature include limited personnel/equipment, available transportation, veterinary-client relationship or communication, client identity, appointment availability, client mental/physical circumstances, government support, cultural or language differences, and client education on animal healthcare (2–4, 7, 8, 10–12).
There are significant animal and human wellbeing threats that arise from limited or no access to animal healthcare. As summarized by Pasteur and colleagues in a recent review (2024), access to animal healthcare improves animal physical health (5, 13–24) as measured by disease prevalence (22, 23), body condition scores (20), and population control through increase in spay and neuter percentages (20). Access to care has also been shown to improve behavioral indicators of animal welfare (14, 17) measured by decreased vocalizations related to stress or nervousness (25), and decreased roaming and barking (26). Access to animal healthcare can also prevent the spread of zoonotic diseases to humans (27) and ensures that the human wellbeing benefits of pet companionship (28, 29) do not become stresses and burdens (30). Veterinary professionals are also often a trusted source for animal welfare information and heavily relied upon by animal caretakers (31–34), and lack of access can impede the sharing of best practices in animal care potentially leading to welfare issues from an animal care perspective (11).
In response to the substantial need for more accessible animal healthcare services, many grassroots organizations and multinational corporations have developed programs, employed a range of tools, or taken steps to mitigate barriers with the hopes of improving accessibility locally or for a particular underserved population (35). A notable challenge is that the success of accessible veterinary care programs might vary depending on the underserved community, their animal population and relationship with animals, geographic location, beliefs, barriers, needs, expectations, and priorities (35). Throughout the process of increasing access, it would be helpful for organizations to: (1) define and be able to measure what program success would look like [i.e., what does “access to health care” entail (11, 36)]; (2) determine where to focus their efforts [i.e., locating “veterinary care deserts” (37) or “underserved communities” (38)]; and (3) partner with their target community to understand community-specific barriers and determine tools that would most effectively and appropriately mitigate them. Unfortunately, this might not always be possible for organizations due to lack of resources, emergent situations, or lack of expertise.
To improve access to animal healthcare in Canada and support organizations working in this space, we need to better understand the current organizational landscape: How are organizations across the country attempting to address barriers to accessing animal healthcare in underserved communities? What strategies are being implemented, where, and with which communities? And how are program outcomes measured and evaluated? This paper provides baseline data to answer these questions, drawing on the findings of online data mining and a cross-sectional, mixed-methods organizational survey conducted in 2023. We report how access to veterinary care is being addressed by organizations working with diverse communities across Canada and briefly characterize the services, barrier mitigation tools, community partnerships, and evaluation metrics being used by organizations attempting to increase access to animal healthcare in Canada.
2 Materials and methods
All procedures in this study were reviewed and approved by the University of Guelph.
Research Ethics board for compliance with federal and provincial guidelines for research involving human participants (REB #23–07-031).
2.1 Data mining
Online data mining was conducted between May and August of 2023 using Google Chrome to search for and make a database of animal healthcare service providing organizations who were advertising efforts to increase financial, geographical, cultural, or physical accessibility of services. Search strings included all combinations of a region (Canada OR individual provinces OR individual cities in the 100 most populated cities according to the 2021 Canadian Census), a barrier mitigation strategy (“low-cost” OR “low cost” OR “low price” OR free OR sponsored OR subsidized OR not-for-profit OR rural OR Indigenous OR “First Nation” OR northern OR mobile OR telehealth OR virtual OR accessible OR “physically accessible” OR “community-based”) and an animal health service (“animal shelter” OR shelter OR humane society OR SPCA OR vet* clinic OR vet* services OR vet* medicine OR vet* program OR vet* treatment OR vaccination OR “spay and neuter” OR “trap neuter release” OR TNR OR animal healthcare). To be included in the database, the organization had to be located and provide services within Canada, have an email address or phone number to contact, and advertise a service or tool that increased geographical, financial, cultural, and/or physical accessibility of animal healthcare services.
2.2 Survey development
The survey consisted of 20 questions relating to organizational interventions aimed at reducing barriers to accessing animal healthcare, what tools and methods were used, which communities were targeted, and any measures of program impact that were collected. The survey took approximately 15–20 min to complete. There were single- and multiple-choice and open-ended questions with a textbox for the participant to provide a written answer. Many of the single- and multiple-choice questions had an ‘Other’ option with a textbox to add additional answers. The survey included four sections: (1) consent (information letter and one question collecting informed participant consent), (2) organizational information (four questions relating to organization type), (3) access to care information (11 questions relating to organizational priorities, perspectives, and services offered), and (4) next steps (four questions related to continued participation in other research, contact information, and any additional participant comments; see Supplementary materials for the full survey).
All questions were hypothesis driven and based on current literature on veterinary care deserts (37–41) and barriers and access to animal (4, 8, 10, 12, 42–50) and human (36, 51–55) healthcare in North America. The questionnaire was piloted and reviewed by 7 prominent researchers and practitioners in the access to veterinary care space across Canada and suggestions were incorporated prior to the launch of the survey.
2.3 Survey participant recruitment
The survey was open from December 5, 2023, to February 20, 2024. Participation was restricted to individuals 18 years of age or older with the authority to provide details on behalf of an organization offering services that address barriers to accessing animal healthcare in Canada. The online survey hosted through Qualtrics® survey software (56) so internet access was required for participation. The survey and recruitment material were offered and distributed in both English and French. The data mining portion of this project served as the initial recruitment list for the survey distribution with recruitment information sent by email to each organization individually with a follow up reminder sent 1 month after initial contact. If the organization’s email could not be found, the organization was contacted by phone. Snowball sampling techniques were then used to promote the survey further on social media and through larger organizational and regulatory bodies. This convenience sampling method relies on referral from participants and is typically utilized to reach groups of people that are otherwise difficult to access (57, 58).
Initial online advertisements, including the study description and a link to the survey, were posted on Facebook, Instagram, X/Twitter, and LinkedIn. Organizational and regulatory bodies including the Canadian Veterinary Medical Association and each provincial Veterinary Medical Association, Humane Canada, and each provincial shelter association, Canadian Animal Shelter and Community Medicine Association, PetHelpFinder, PetSmart Charities of Canada, the Canadian Kennel Club, International Fund for Animal Welfare, Canadian Companion Animal Health Surveillance Network, and each of the five Canadian veterinary schools were sent recruitment information and asked to distribute it among their members and contacts. Large pet related corporations including Communivet, Zoetis, Elanco, BI, IDEXX, Antech, True North, AHL, PDS, Hill’s, Royal Canin, Purina, and the Veterinary Practice magazine were also sent recruitment information and asked to advertise or distribute the survey to Canadian contacts.
All recruitment material encouraged sharing the survey with acquaintances or contacts who might meet the inclusion criteria. Participation in this research was voluntary, and consent was provided by respondents online through submission of the survey. No incentives were offered for completion of the survey.
2.4 Data management
The raw data were downloaded from Qualtrics® survey software and initially cleaned and reviewed in Microsoft® Excel. Any responses that met the following exclusion criteria were removed: [1] answered less than 95% of the survey (N = 38), [2] were likely to be a bot response (N = 0 based on criteria from (59)), [3] were answered from outside of Canada (N = 2), or [4] were duplicates from the same organization (the most complete response was kept, N = 3).
2.5 Quantitative analysis
Descriptive statistics were generated about participants including frequency and measures of central tendency for organizational type, location, goals, priorities, communities and species served and services offered using STATA statistical software (60).
2.6 Qualitative analysis
The open-ended question responses were analyzed using qualitative content analysis with an inductive approach (61). This grounded approach avoids initial researcher bias and allows codes to emerge naturally which encourages exploration of unanticipated insights (61–63). First, all responses were read in full by the lead author (QR) and a codebook was subsequently developed for each qualitative question. Second, all responses for each question were coded using the developed codebook for that question using NVivo 14 qualitative data analysis software (64). Entire responses or sections of responses could be coded under multiple codes. Third, coding was assessed for reliability by comparing coding agreement within NVivo (65) between the first (QR) and last (LVP) authors who both coded 100% of responses. Inter-coder reliability was conducted and yielded agreement of 94%. Any discrepancies were discussed until consensus was reached.
3 Results
3.1 Data mining
The database (N = 504) generated from online mining contained primarily for-profit clinics (54%) and non-profit organizations (39%) with some municipal or governmental services (2%) and educational institutions (<1%). Geographic accessibility barriers were predominantly mitigated through mobile private clinics (30%), telemedicine or telehealth appointment options (8%), or pop-up clinics in underserved areas (3%). Financial accessibility was mitigated through free (1%) or reduced cost (10%) spay and neuter services often accompanied by one or more other services like vaccinations or deworming. There were a few complete service clinics that reported being low (2%) or no (<1%) cost and some organizations (1%) that offered pop-up clinics for unhoused populations in large urban centers at no cost. This database will soon become part of an interactive map of organizations in Canada to help pet caretakers find accessible care locally and support organizational collaboration (See Figure 1 for the geographic distribution of organizations).
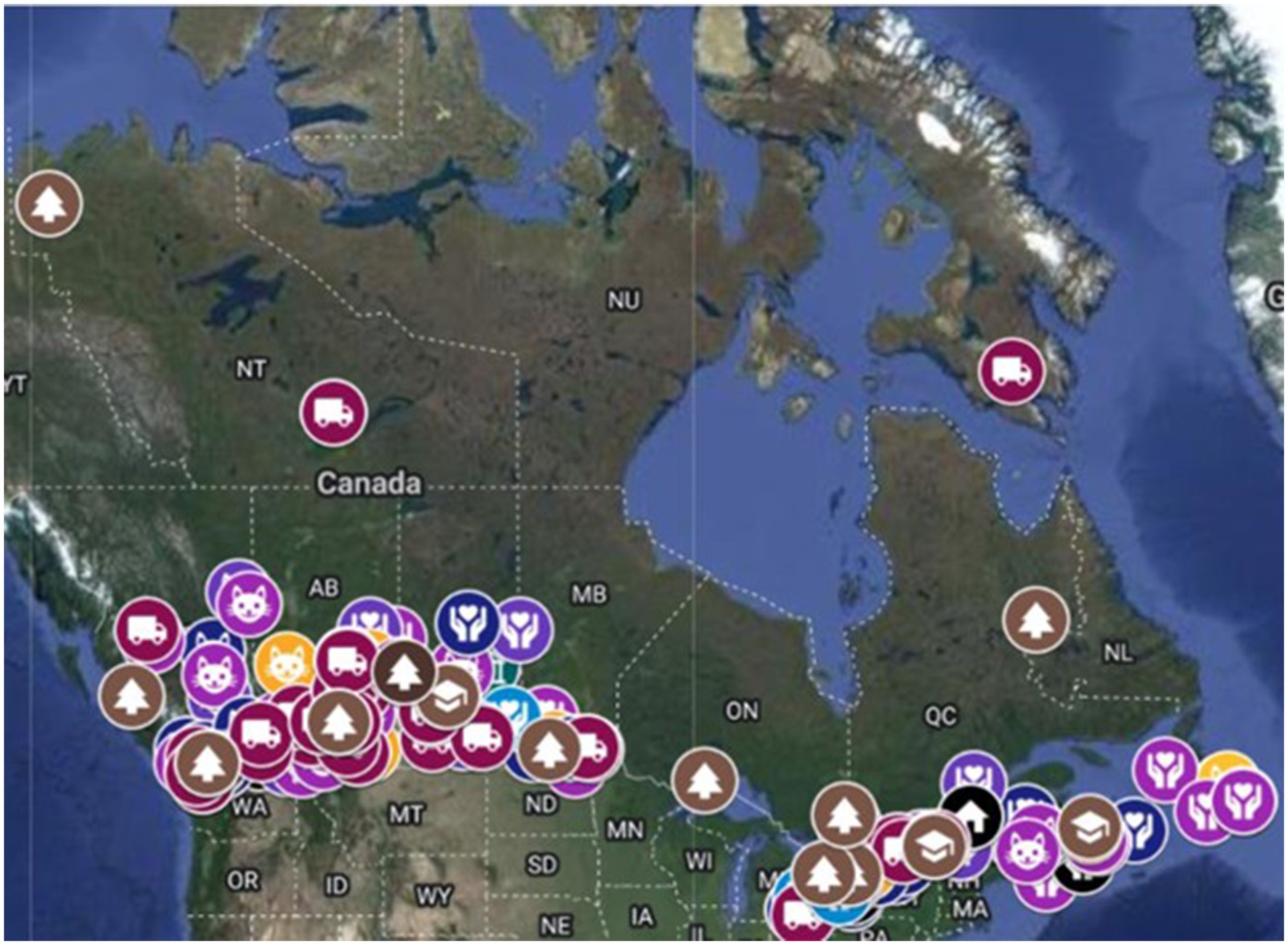
Figure 1. Map showing the geographic distribution of organizations identified offering financially or geographically accessible animal healthcare services in Canada during online data mining from May to August 2023.
3.2 Quantitative survey analysis
Survey participants (N = 97) were most commonly non-profit organizations (52%) or for-profit clinics (38%) with a few municipal or governmental services (4%) and educational institutes (5%; see Table 1 organizational descriptives). Organizations primarily offered services in Ontario (45%), British Columbia (16%), Alberta (14%), and Quebec (12%) with less than 10% in any other province and territory. Organizations primarily offered services for cats (91%) and dogs (89%) with fewer organizations offering services for other small animals (e.g., rabbits, guinea pigs; 49%), exotic animals (e.g., reptiles; 27%), and large animals (e.g., cows, horses; 12%). Participants reported that services were provided by primarily veterinarians (90%) and veterinary technicians (74%) with some organizations allowing other employees or volunteers (47%) to provide services. When organizations were asked to rank their organization’s priorities relative to one another, on average, ‘improving animal welfare’ was the top priority followed by: ‘helping people with pets’, ‘controlling animal populations’, ‘preventing zoonotic disease’, and finally ‘promoting One Health’. In open-ended textboxes asking about other organizational goals not listed above, participants noted: providing education (e.g., student training, humane education, knowledge sharing), improving community safety, rehoming unwanted animals, generating profit, and assisting animal rescue organizations. When asked about which underserved communities they worked with, the most common answer from participant organizations was low-income (66%), followed by Indigenous (51%), rural (47%), unhoused (45%) and northern (31%). Organizations worked on average with between two and three different underserved communities.
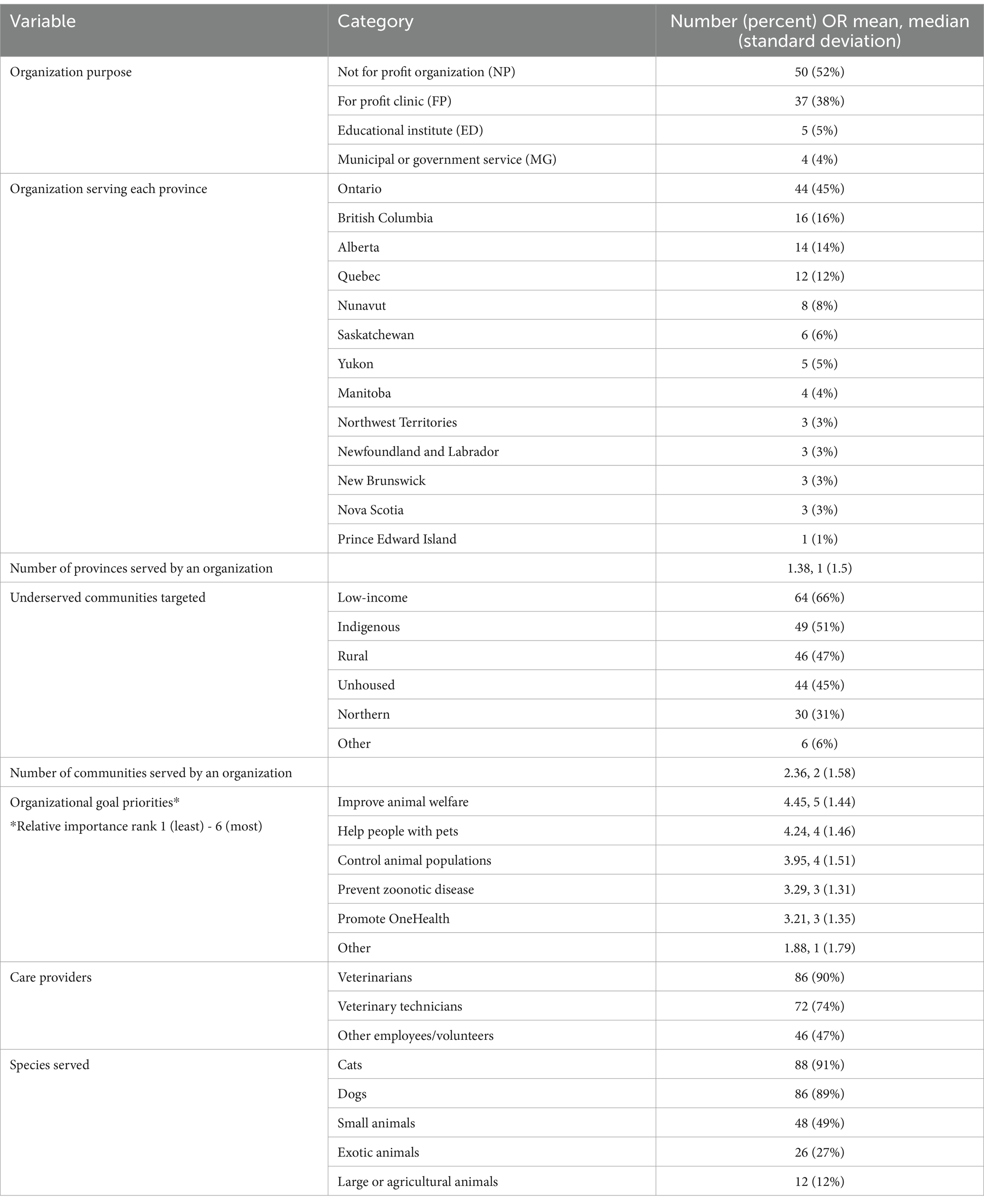
Table 1. General descriptions, frequencies and measures of central tendency of organizational characteristics collected from 97 animal healthcare providing organizations in Canada who completed the organizational survey between December 5, 2023-February 20, 2024.
The survey participants were asked which tools they use to mitigate affordability, accessibility and cultural or disability related barriers to accessing animal healthcare (see Table 2 for descriptions and frequencies of tools used). In total, only 38% of organizations used at least one tool from each of the four categories of barriers. Affordability barriers were mitigated with an average of 2.26 tools by 93% of organizations. Free (43%) and low-cost services (51%) were the most common tools. Offering funding (37%) and the use of spectrum of care (36%), offering bundled services (e.g., puppy or kitten packages, free services bundled with adoption or purchase; 20%) or payment plans with (13%) or without (15%) credit check requirements were also used by many organizations. In open-ended textboxes asking about other financial accessibility tools, participants noted using: pay what you can, unofficial payment plans, free long-term veterinary support beyond preventative care, offering discounts for particular groups (e.g., seniors, those on government assistance, shelters), free disease control programs or education, accepting volunteer donations to subsidize care for low-income clients, offering vouchers for a service, third party payment plans, reduction in certain costs when bills are high, offering discounts or free services at the veterinarian’s discretion, and staff getting a certain dollar amount per year to use for free services.
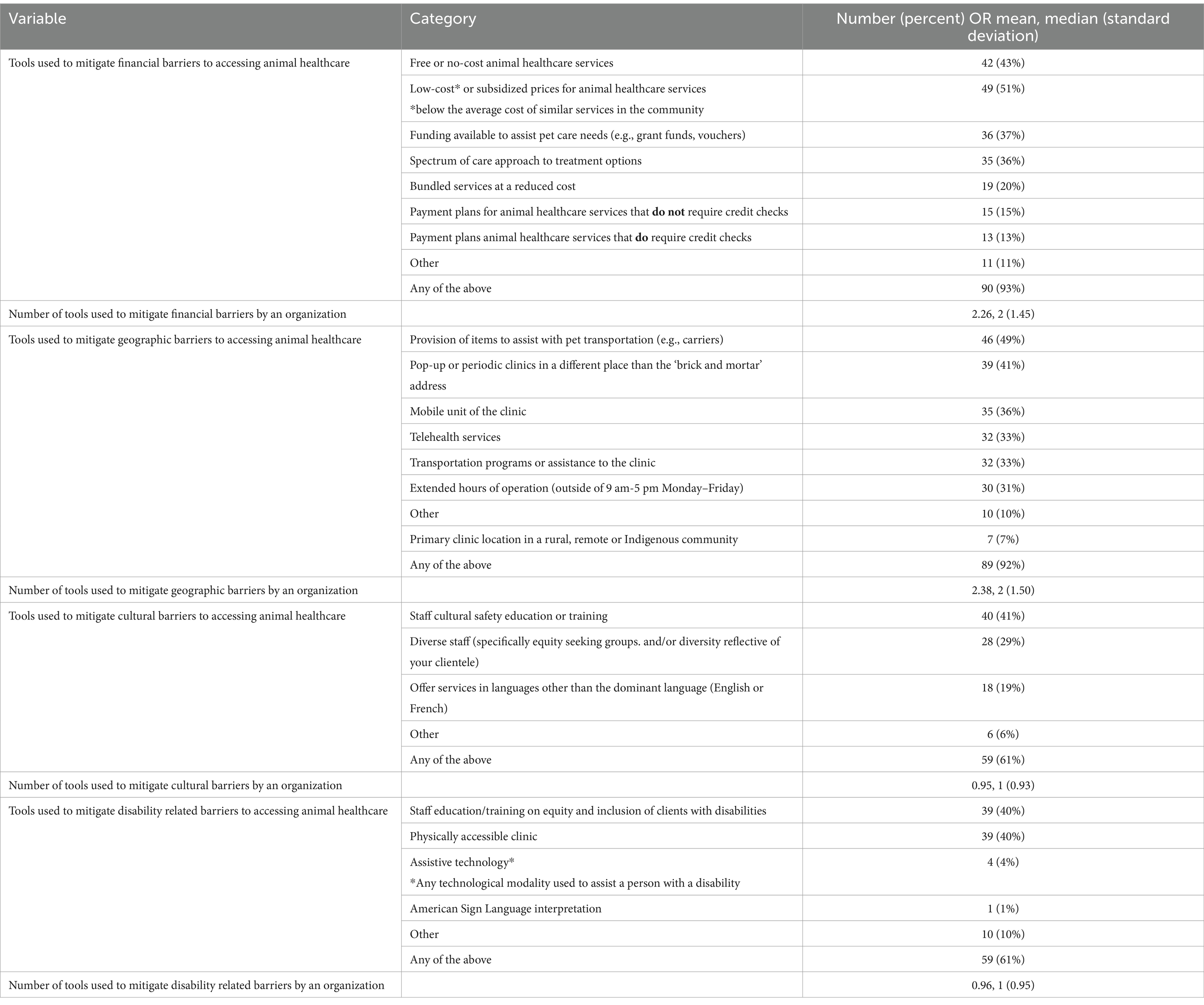
Table 2. Descriptions, frequencies and measures of central tendency for tools used to mitigate financial, geographic, cultural and disability related barriers to access animal healthcare by 97 animal healthcare providing organizations in Canada who completed the organizational survey between December 5, 2023-February 20, 2024.
Geographic accessibility tools were used by 92% of organizations with an average of 2.38 tools used per organization. The most prominent tools employed by organizations were the provision of items to assist with pet transportation (49%), pop-up or periodic clinics in an underserved area (41%), mobile units of the clinic (36%), telehealth services (33%), transportation programs (33%), and having a primary clinic location in a geographically underserved area (7%). In open-ended textboxes asking about other tools to mitigate geographic barriers, participants noted: partnering with external mobile services, facilitating client communication with one another to coordinate a communal vet visit, personal use of staff vehicles for occasional mobile services (e.g., euthanasia, pet pick-up), providing funding for travel, training community/lay vaccinators, removing animals from a community for services and returning them, dropping off medicine or food to clients, helping clients locate a closer service, telehealth consultations between organizations to reduce client travel, and setting up emergency medication pharmacy in a veterinary desert.
Cultural barriers were mitigated by 61% of organizations with the use of 0.95 tools on average used per organization. Tools included staff cultural safety training (41%), having a diverse staff (i.e., equity seeking groups and/or diversity reflective of clientele; 29%), and offering services in multiple languages other than the dominant language (19%). In open-ended textboxes asking about other tools used to mitigate cultural barriers, participants noted: access to a translator when needed, trauma-informed care training, partnering with community leadership and following cultural protocols, focusing on community-led solutions, seeking information from community leadership about needs, employing a social worker, and offering outreach services targeted at equity seeking groups.
Disability-related barriers were mitigated by 61% of organizations with an average of 0.96 tools on average used per organization. The most common tools used were staff training on equity and inclusion of clients with disabilities (40%), having a physically accessible clinic (40%) while a few organizations reported having assistive technology available (4%), and having an American Sign Language interpreter on staff (1%). In open-ended textboxes asking about other tools used to mitigate disability-related barriers, participants noted: offering various formats for filling out paperwork and consents, email correspondence, using trauma-informed and/or neurodiversity aware approaches, taking into consideration disability-related costs when measuring low-income qualification, mobile and in-home services, transportation assistance, meeting clients at vehicles, and use of Google Translate.
3.3 Qualitative survey analysis
Content coding was completed for questions 11 (barriers to care), 15 (level of community involvement) and 14 (program impact and evaluation), which are each reported separately below (see Supplementary materials for the full survey). All participant answers quoted are reported exactly as written in the survey with their participant ID directly after (FP = for-profit organization, NP = non-profit organization, MG = municipal or governmental organization, ED = educational institute). When slight clarity, spelling correction, or context was required, edits were added in square brackets.
3.3.1 Barriers to care
Perceived barriers to care fell into five general codes: care affordability, care accessibility, care availability, client situation, and client-service provider relationship (see Table 3 for Codebook with definitions and frequencies). In terms of care ‘Affordability’, many participants noted cost of care as a barrier (n = 41): “Rising cost of living and veterinary care” (FP4); “difficulty affording the cost of veterinary care” (MG1); “Pricing of larger corporate clinics” (NP24). Several specified challenges related to client disposable income (n = 19): “Finances of pet owners” (NP24); “Available money from clients” (FP23); “lack of financial resources” (FP35). Others noted the financial challenges facing organizations that provide access to veterinary care (n = 3): “Limited funds as a non-profit makes it difficult for those tough cases” (NP8); “Funding -- our organization is supported by grants and community donations” (NP45). Respondents also made links to broader systematic financial considerations (n = 3): “Poverty” (NP7); “costs of living cause financial barriers” (FP26); “the failing economy” (NP29).

Table 3. Qualitative codebook for barriers to animal healthcare including codes, sub-codes, definitions and frequencies reported in qualitative responses by 97 animal healthcare providing organizations in Canada who completed the organizational survey between December 5, 2023-February 20, 2024.
In terms of ‘Accessibility’, participants discussed barriers related to distance from care (n = 16): “Physical location of where people live, for example, in a very remote location where the closest vet is hours away” (FP27); “veterinary clinics are a plane ride [or] 6 + hour drive away” (NP48); “location/geographical distance from a veterinarian (so need for transportation and often staying in area to have pet cared for)” (NP47). Others discussed gaps in veterinary services, or veterinary ‘deserts’ (n = 13): “veterinary deserts” (NP1); “no full-time vet care available” (ED1); “Lack of services (no emergency services in [location] and only one in all of [location] region that sometimes can be at capacity)” (NP34). Finally, transportation barriers were frequently noted (n = 18): “Access to transportation” (NP6); “Lack of transportation” (NP34); “Unable to get to clinics, especially seniors” (FP29).
Participants also noted barriers in terms of veterinary care ‘Availability’, including lack of available appointments (n = 15): “Lack of veterinary clinics accepting patients (availability of for-profit clinic spaces)” (NP24); “available clinics wanting to work with rescues” (NP5); “appointment accessibility in a reasonable timeframe” (NP36). Relatedly, many respondents noted the challenges associated with the service provider shortage (n = 23): “The veterinary shortage” (NP9); “Trained veterinary staff interested and available to work in shelter medicine” (NP14); “Veterinary workforce shortage” (MG2). Respondents also noted that the high number of animals needing care impacted care availability (n = 5): “Number of animals needing care (due to overpopulation)” (NP45); “Free pets are readily available” (NP15); “number of pets” (FP5). Others noted the impacts of regulatory barriers (n = 5): “Regulatory body restrictions” (NP14); “current definition of acceptable standard of care in veterinary medicine is too high” (NP14); “the regulations of the college that create barriers to helping the general population who cannot afford the cost of care and the limitations of licensing to help organizations like shelters and not for profits who provide care to the forgotten individuals but limit our ability to reach them and provide service” (NP20).
Responses related to ‘Client situation’ acknowledged barriers related to client health and dis/abilities (n = 9): “those in more urban areas who have disabilities (physical or psychological) that make it impossible to get to a local vet” (NP13); “mobile disabilities” (FP7); “mental health barriers” (MG4). Client knowledge, both of animal health needs and of service availability, was also noted as a reason some may not access veterinary care (n = 18): “Lack of knowledge or education regarding necessary pet care” (NP15); “Education (lack of fluency in health-related needs for animals)” (NP41); “Many people encountering this issue do not know where to go for help” (NP19). Finally, other logistical or situational barriers were noted (n = 4): “Logistical” (NP30); “time, effort” (MG4); “those in poverty, homelessness, mental turmoil, fleeing violence or emergency situations” (NP26).
The most commonly noted barrier related to ‘Client-service provider relationship’ was cultural differences and bias (n = 13). Most responses were very general, stating simply “cultural barriers” (NP48), “cultural acceptability of services” (ED4), or “Language/cultural” (NP30). Several focused on dynamics of service providers in particular, for instance: “fear of being judged” (NP1); “[racism] and discriminatory practises in certain clinics” (ED5). Others focused more broadly on historical and systemic issues, specifically in the context of access to care barriers faced by Indigenous communities: “cultural barriers (historic colonialization, racism)” (ED1); “Distrust of non indigenous [sic] peoples with the ability to help these communities. Social and racial and financial barriers” (NP44). One respondent provided a more in depth analysis: “lack of trust with healthcare providers/animal welfare org[anization]s due in some cases to historical trauma and discrimination or due to practitioner judgement when the owner cannot afford care, culture/linguistic/religious barriers” (NP43). Respondents also noted barriers related to trust of service providers and previous negative experiences (n = 7): “distrust of medical profession (seeing animal welfare agencies as punitive and worried they will lose their animal); “trust in veterinary service providers” (ED4); “Past negative experiences in health and veterinary care” (NP7). Finally, participants also noted that service provider knowledge or perspectives can contribute to barriers (n = 4): “Knowledge of spectrum of care opportunities and organizations involved in spectrum of care” (NP7); “lack of practitioner knowledge about shelter medicine” (NP43).
3.3.2 Level of community involvement
Organizations reported varying levels of community partnership when qualitative responses about community involvement in the program were placed on the following spectrum of participation delineated in the ‘Principles of Veterinary Community Engagement’ (66): outreach, consulting, involving, collaborating, and sharing leadership (see Table 4 for Codebook with definitions and frequencies). Aligning with an ‘Outreach’ model, organizations determined community needs on behalf of the communities they work with (n = 1), provided information in a unidirectional manner (n = 3), and/or simply noted that the community uses their services (n = 12): “We observed that they needed help and started the program ourselves” (NP39); “These communities are involved as service recipients” (NP39).
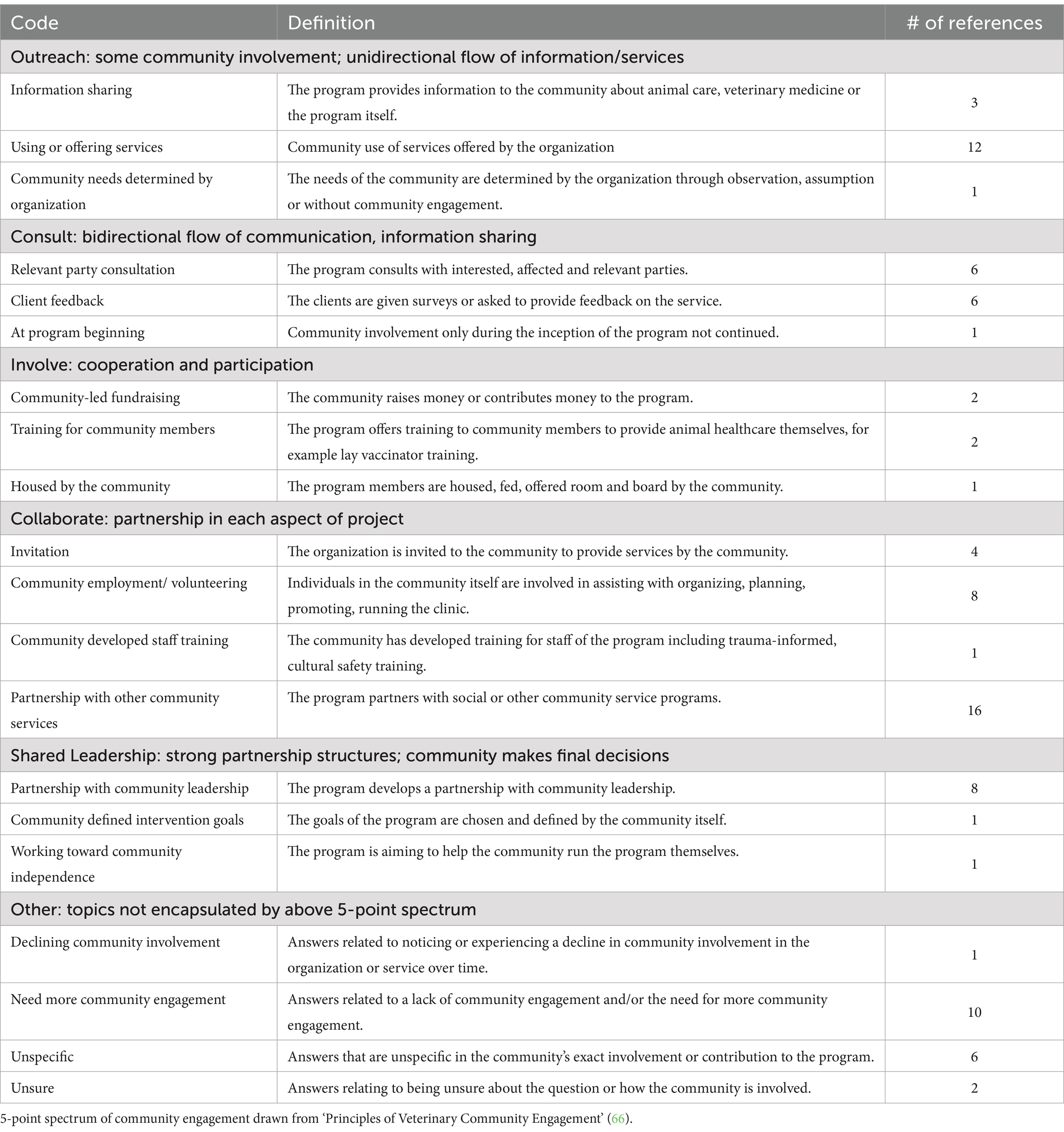
Table 4. Qualitative codebook for level of community involvement in service provision including codes, sub-codes, definitions and frequencies reported in qualitative responses by 97 animal healthcare providing organizations in Canada who completed the organizational survey between December 5, 2023-February 20, 2024.
‘Consultation’ involves a bi-directional flow of information, and some organizations noted that they seek feedback from their clients (n = 6) or the communities they work with (n = 6): “We do seek their input in our strategic planning” (NP40); “Rightsholder engagement” (MG2); “We routinely reach out to our clients for feedback and comments regarding our services, what they need and evaluate how we can improve” (NP26).
Other organizations made statements suggesting that they ‘Involve’ the community, for instance through training for community members (n = 2), community-led fundraising (n = 2), or the community providing room and board during the clinics (n = 1): “Community-led fundraising for our programs that go directly to benefiting their members” (NP11); “We offer training of local vaccinators” (ED3); “We are housed, and fed by the community” (NP17).
‘Collaboration’ involves a partnership throughout service planning and provision, and includes elements like being invited by the community (n = 4), providing employment or volunteer opportunities for community members (n = 8), community-developed training for organization staff (n = 1), and partnership with other community service programs (n = 16): “Provision of all services began at the request of and in collaboration with all of the communities” (ED4); “Our Trauma-Informed & Culturally Safe training program was developed by a group which included Indigenous knowledge, and those currently or previously unhoused” (NP13); “require the communities to be stakeholders - to appoint liaisons who can help with organizing, promoting the clinic and providing some of the needs for the team” (ED1).
Finally, ‘Shared leadership’ was demonstrated through participating organizations’ statements indicating a partnership with community leadership (n = 8), community-defined intervention goals (n = 1), and the goal of working toward community independence (n = 1): “we always partner with local community governments or First Nations governments to bring accessible veterinary care to communities” (MG1); “Our role is to support a community in its journey toward a locally run management plan” (NP4). The type of community involvement tended to vary with the community served. Indigenous Nations and very rural, remote, or geographically isolated communities tended to be more involved in organizational decisions than urban, low-income, unhoused, or precariously housed communities.
3.3.3 Program impact and evaluation
Organizations reported various metrics to assess program impact, including: service availability, organizational input and effort, service utilization, animal health outcomes, and client perceptions of access to care (see Table 5 for Codebook with definitions and frequencies). The most common measure of program impact involved quantitative metrics of the numbers of services provided (n = 25): “We just keep track of how many [animals] we were able to spay/neuter” (NP8); “Just numbers of medical and surgical appointments” (ED2); “Number of animals seen, number of repeat animals seen” (ED5); “how many pets supported in a year, how many guardians supported in a year” (NP13). Another common measure involved client feedback (n = 7): “We have distributed post clinic surveys (exit surveys) in past to gauge whether or not the communities felt our visit was a success” (ED1); “Feedback surveys including how services were accessed (transportation barriers), percentage waived fees, client experience with the service” (NP10).
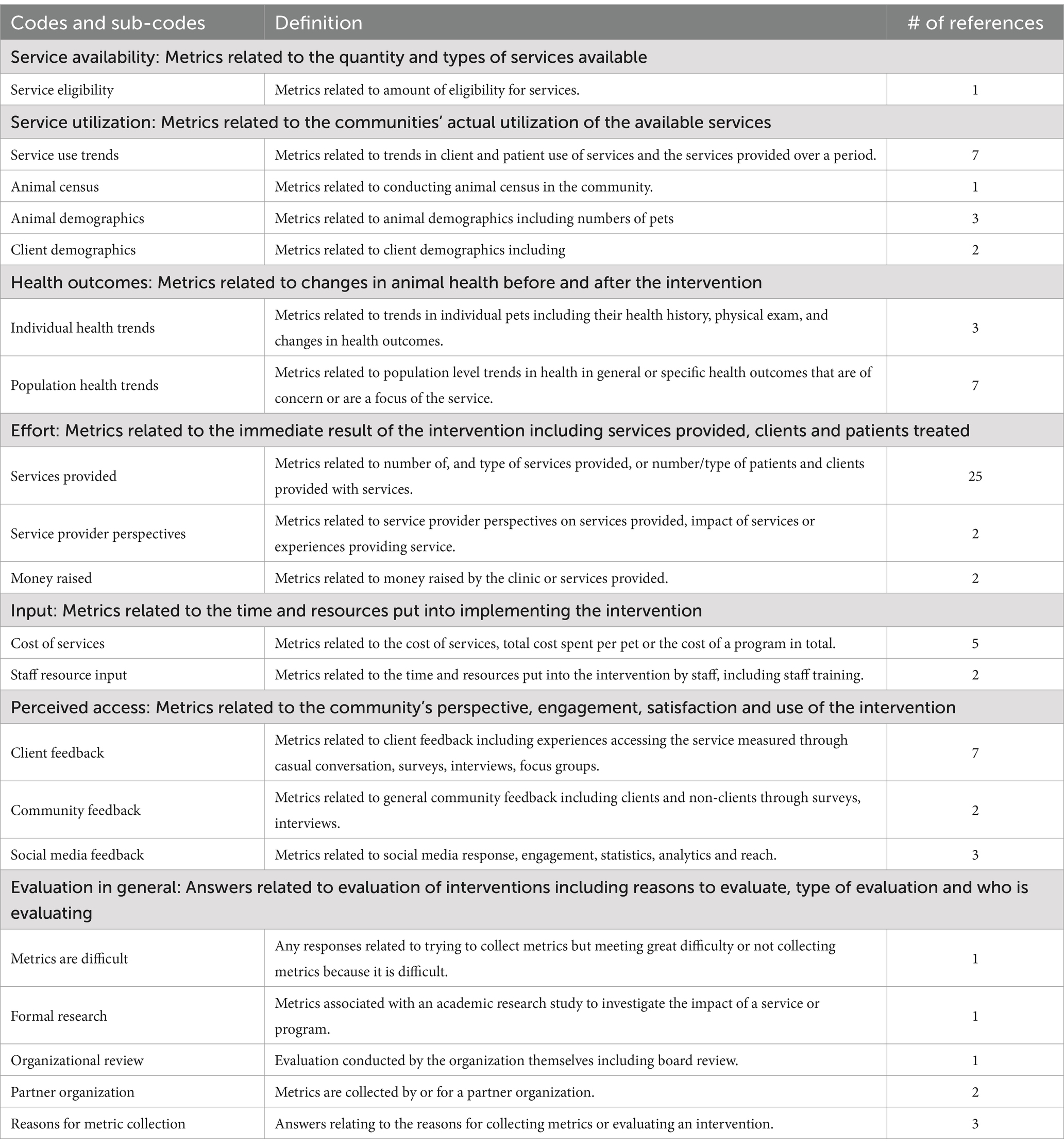
Table 5. Qualitative codebook for metrics used to measure impact of services including codes, sub-codes, definitions and frequencies reported in qualitative responses by 97 animal healthcare providing organizations in Canada who completed the organizational survey between December 5, 2023-February 20, 2024.
Other organizations used social media or website engagements (n = 3): “Although biased, we also have a social media presence and the majority of the response is positive, but perhaps we are not capturing the negative” (ED1); “Facebook statistics and google analytics” (MG3). Organizations also tracked financial measures including the amount of funds raised (n = 2) and the cost of services (n = 5): “average dollar amount spent per pet (which is tied to the complexity of the cases we are taking on)” (NP13); “monthly/quarterly/annual cost” (NP14); “how much funding we raised” (FP10).
Some organizations tracked individual animal health trends (n = 3), while others tracked population health trends (n = 7): “pet history” (NP7); “tracking animals/clients over time to determine numbers of repeat animals and owners” (NP20); “medical records are used for chart reviews to understand change in animal health and welfare metrics over time (including age, BCS [body condition score], breed, sterilization status, vaccination status)” (NP20); “reduction in animal issues, reduction in stray animals” (ED5). Some organizations noted tracking trends for particular health measures, such as tick-borne illnesses and heartworm, and animal (n = 3) as well as client (n = 2) demographics. Service use trends were also tracked (n = 7): “booking capacity rate” (FP14); “Reduction in intake of targeted locations. Reduction in overall intake and owner surrender intake” (NP26); “[number of] new clients per month, [number of] new patients per month” (MG4).
In terms of how gathered data were used, responses indicated that program monitoring or community feedback results were employed for the purposes of organizational review, to ensure objectives are being met, to formally publish or share knowledge, or to share with regulatory bodies as part of licensing requirements. Others noted that metrics were not collected or were challenging to collect: “Not specifically” (NP33); “We work with organizations that collect metrics, but we do not collect metrics ourselves” (NP44); “We try but it is difficult” (NP18).
3.3.4 Other
One additional topic from the open-ended survey responses was a desire from respondents to do more, while acknowledging limitations of time and resources to do so: “We would love to initiate programs to assist our community, however, we have very limited resources” (NP3); “we are very small and wish we were able to do more” (FP9); “I would like our organization to be able to offer more services, but unfortunately we are small” (NP31); “We need collaboration with similar groups and assistance from groups that have large financial means” (NP44).
4 Discussion
A qualitative content analysis of specific barriers mentioned within survey responses strongly reflect barriers identified in other research, indicating that participating organizations seem to understand the main affordability, accessibility, availability, client situation and client-service provider relationship related barriers to care reported generally by clients in the animal healthcare literature (2–4, 7, 8, 10–12, 42–50). For instance, cost of care and appointment availability were key barriers noted by clients in a recent Canadian survey (2) and were also key topics identified by service providers within this study. More information is needed on the prominent barriers present for individuals and/or communities in Canada and whether local organizations are aware of context specific barriers and needs. Similarly, information from service-providers regarding their catchment areas (areas of service provision) reflects results from previous mapping of veterinary care deserts in Canada (39), namely large geographic areas in the Northern provinces and the east coast that seem to be underserved or have less availability to accessible care. Over 90% of organizations participating in this survey offered services in four provinces: Ontario, British Columbia, Alberta, and Quebec. Thus, either our recruitment methodology favored these regions and was not as successful at recruiting participants from eastern Canada, the prairies, and the Territories, or these regions may have fewer organizations providing veterinary care or working to mitigate access to care barriers. A dearth of organizations reporting to offer services in the Territories, with those who do primarily operating pop-up clinics and not year-round brick-and-mortar veterinary clinics, also aligns with existing knowledge of this substantial care desert (5, 6). Future research could target these areas in particular to understand in a more comprehensive fashion the extent of veterinary care deserts and strategies to improve the accessibility of veterinary care.
In terms of how organizations across the country are attempting to address barriers to accessing animal healthcare in underserved communities, over 90% of organizations mobilized tools related to service affordability or geographical access. Cultural and disability-related barriers were each mitigated by less than two-thirds of organizations. Organizations used an average of between 2 and 3 tools to mitigate financial and geographic barriers indicating that one tool is likely insufficient to increase access for diverse clients. The most common tools to mitigate financial barriers were offering free and low-cost services with most organizations working with low-income communities and almost half of organizations working directly with unhoused individuals. Only 15% of organizations surveyed offered payment plans without credit checks, which has been noted as an important tool to increase access by 14.5 times compared with providing full subsidies to fewer clients (67) and reduce the “pain of payment” (68).
Half of the organizations worked with rural communities and a third with northern communities who likely struggle with geographic accessibility. One of the most common tools used to mitigate geographic barriers was pop-up or periodic clinics while only 7% of organizations operate a permanent clinic in a rural, remote, northern community or Indigenous Nation. This indicates that even for those geographically underserved communities who have access to the services provided by organizations in this study, access is likely not regular. Telehealth services were only used by a third of organizations in this study despite gaining popularity during the COVID-19 pandemic with one study reporting a rise from 12 to 38% use by clinics between March–June 2020 (69). Telemedicine has been suggested to reduce cat stress and negative responses (70), increase accessibility of care compared to clinic visits (70–72), and increase clinic efficiency (73). However, some practitioners call into question the safety of telemedicine for new clients or new diagnoses without an in-person establishment of a veterinary-client-patient-relationship raising concerns about a lack of physical exam, missed or wrong diagnoses, technological constraints, and lack of diagnostic tools (71, 74, 75). Open-ended survey responses demonstrated a large range of strategies employed by organizations to target financial and geographic accessibility, showing a diversity of creative approaches and perhaps a need for further research on which tools are most impactful for individual community access.
Tools to mitigate cultural and disability-related barriers were less prevalent, with the average number of tools used by organizations to mitigate these barriers being less than one. Fewer than half of organizations trained staff on cultural safety, and less than 20% of organizations reported having diverse staff reflective of their clientele or offering services in multiple languages. Fewer than half of surveyed organizations had a physically accessible clinic, or trained staff on providing accessible service provision, and only one organization had assistive technology. Increased awareness and use of tools to meet the needs of individuals with disabilities is necessary to increase access to care (46). Given that the most common tool used to address cultural and disability-related barriers is staff training, future research should explore what this training consists of, who is developing the content, and how and by whom it is delivered, as this is likely to influence its effectiveness (76). The limitations of the current Canadian veterinary landscape with regard to cultural and disability related accessibility is an important area of focus to increase access to services, especially given the linkages between factors like health, socio-economic status, ethnicity, and disability (77–79). Relatedly, less than 40% of organizations used at least one tool from each of the four categories of barriers. The intersecting nature of access barriers makes clear the importance of taking a holistic approach that targets multiple axes of inequities (80, 81). Due to limited organizational resources and the availability of wide-ranging tools, future research should investigate the impact of individual tools used to increase access to care and the conditions that facilitate their usefulness in a community and organizational context.
Community involvement in programs ranged from simply accessing the service when it was available (outreach) to giving occasional feedback on their experiences (consulting), being employed or volunteering in program provision (collaborating), and community leadership partnering on initiatives (sharing leadership). Quite a few organizations partnered with other community service programs, demonstrating a One Health model (10), though ‘Promoting One Health’ was ranked as the lowest priority by survey respondents. This could be because some organizations are using partnerships to increase the use of their own program which primarily prioritizes animal welfare, or because they are not familiar with the term ‘One Health’, and a definition was not provided within the survey. These results in the context of the broader literature suggests that communities vary in capacity, interest, and needs regarding community participation or that organizations need resources to deepen their engagement with the diverse communities they serve (66). Future research should investigate community engagement methods in diverse communities to understand the best partnership and capacity-organizing practices.
Program evaluation most often involved organizations collecting quantitative measures of service usage. A smaller number of organizations tracked metrics like population health trends or solicited community feedback through surveys. The collection of only quantitative measures of service use, although useful, will make organizations providing fewer types of services to more clients look more impactful than organizations providing more holistic, long-term support to fewer individuals, which is not necessarily accurate, particularly at the individual level or over longer periods of time. Organizations reported primarily collecting metrics for funders, internal review, or organizational decision-making, all of which could significantly inform the organizational direction and service provision. All of the metrics reported by organizations to assess program impact (service availability, organizational input and effort, service utilization, animal health outcomes, and client perceptions of access) are reflective of barriers faced by clients and therefore each can be useful for understanding program impact to a certain degree, but none tell the complete story (36). There is often a tension in healthcare literature between a desire for a universal, standard, equal service and the development of services based on local needs and priorities (36), and this tension makes it challenging for organizations to know what to prioritize or measure, particularly if funders have impact report requirements. Participant comments that organizations try, or would like to conduct evaluations, but that they are challenging might reflect this very tension. More qualitative data is needed from these organizations with respect to their organizational goals and what access to care means, how and why organizations have developed these programs, what exactly is challenging about evaluation, and what types of support is needed to increase evaluation and community engagement capacity. Additionally, the low prevalence of long-term impact evaluation on health and community voiced needs by programs in Canada might indicate a lack of long-term service provision that is centered on community needs. Alternatively, it could indicate a lack of evaluation capacity in organizations who are providing sustained, relevant community care specifically with regard to community-engaged and continuous program evaluation and adjustment. In reality, these results are likely an indicator of both, and future research should seek to understand qualitatively how program evaluation plays a role in service development, improvement, and impact, what barriers restrict program evaluation, and how service providers would evaluate their program if given the resources and support to do so. These results highlight an area for potential capacity organizing resource sharing and collaboration between researchers, communities, organizations, and funders to make metric collection and program evaluation more accessible. Future research should collaborate with funders, organizations, and community members to create flexible best practices, guiding methodology and resources for program evaluation and impact measurement that is accessible and adds minimal administrative burden to organization staff, meaningful in relation to the needs of the target community, and useful for funders and decision makers to meet their goals (35, 82).
5 Limitations
This study had several limitations that might impact the generalizability or completeness of the data set with respect to Canadian animal healthcare organizations’ perspectives and practices. Selection bias is likely present due to the nature of a cross-sectional survey design and the use of convenience and snowball sampling (83). Participants might be statistically different (e.g., more interested or invested in access to care, have more time to participate in surveys, have more access and/or presence on social media, have more involvement with organizations who distributed our survey) than non-participants which would result in prevalence measurements of service availability, tool use or evaluation, and community involvement that might not be representative of the general population of organizations. If the population of organizations who participated were more likely to be more invested in the topics of the survey, this bias could lead to our prevalence estimates being higher than that of the general population. Additionally, this selection bias will impact the saturation of our qualitative data and therefore our content analysis might be some missing perspectives. In attempt to mitigate this, the survey was distributed as broadly as possible through online data mining, social media, and prominent regulatory bodies and national organizations. Additionally, the findings of the present study are discussed in the context of the population that participated and is intended to contribute to a growing understanding of the landscape of access to care in Canada. Future research could build on our database of organizations by targeting smaller geographic areas one at a time and using more diverse data collection methods including door-to-door survey delivery to attain more accurate prevalence estimates and qualitative perspectives for individual areas.
Recall and social desirability bias might also be present because participants were asked to self-report via online survey (83). Participants have the possibility of being incorrect in their recollection of their organization’s use of tools and metrics and therefore incorrectly answer questions. Participants might not want to answer certain questions truthfully due to fear or judgment or a desire to answer the questions in a way that helps the researchers with the objectives of the study. These biases were minimized by having the survey be anonymous, writing questions in a neutral non-leading way, and not sharing specific objectives of the study with participants. This bias was also addressed by limiting participation to those who felt confident to speak on behalf of their organization which might alternatively have resulted in missing organizational voices who do not have an individual willing or able to speak on their behalf.
Lastly, the options presented in multiple choice questions in the survey were written to include any possible answer that participants had yet these options still might force organizations to answer in ways that do not quite match how they feel. To mitigate this, survey questions were piloted with seven researchers and organizational leaders to ensure options were exhaustive and applicable. Additionally, “other” categories were available for all multiple-choice questions and mixed methods were used to allow participants room to expand in a qualitative manner.
6 Conclusion
This paper sought to use online data mining and a cross-sectional, mixed-methods organizational survey to determine how organizations across Canada are attempting to address barriers to accessing animal healthcare in underserved communities, and how program outcomes are being measured and evaluated. A total of 97 organizations responded to this survey, with a mix of nonprofit groups, for-profit clinics, and education institutions. Responses demonstrate that organizations mitigated access to veterinary care barriers primarily along financial and geographical lines, and to a lesser extent with tools targeting cultural or disability-related barriers. A large diversity of tools is mobilized by organizations, with some (no-cost or low-cost services, pop-up clinics) being more prevalent than others (payment plans, telehealth, services in multiple languages, physically accessible clinic).
Access to care can be hindered by many intersecting and wide-ranging factors, and it only takes one barrier to restrict an individual’s access to animal healthcare. Only 38% of organizations used at least one tool from each of the four categories of barriers, highlighting the importance of building capacity around addressing multiple intersecting barriers. Some organizations reported wishing that they could do more, but resources were limited, and organizations had funding limitations that were a barrier to providing more care. This corroborates the Canadian Veterinary Medical Association’s recent position statement that the need for veterinary care is significantly greater than the care available (84).
This research provides a characterization of the work being done within the private sector and by NGOs to address access to veterinary care barriers within Canada. It provides a necessary understanding of existing organizational efforts, impact evaluation challenges, and diverse perspectives on how communities are being partnered with. This sets the groundwork for evidence-based solutions to addressing animal healthcare service gaps and strategies to mitigate them most effectively through strong community partnership and community-engaged program evaluation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Guelph Research Ethics Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
QR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. MA: Data curation, Investigation, Writing – review & editing. SB: Methodology, Writing – review & editing. ME: Methodology, Writing – review & editing. VF-C: Methodology, Writing – review & editing. CG: Methodology, Writing – review & editing. JS: Data curation, Methodology, Writing – review & editing. MT: Methodology, Writing – review & editing. KW: Methodology, Writing – review & editing. LP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. PetSmart Charities of Canada provided funding for this project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fvets.2025.1581316/full#supplementary-material
References
1. Canadian Animal Health Institute. Biennial pet population survey shines a light on how pet population statistics changed over the course of the COVID-19 pandemic, and pet owner habits. (2022). Available online at: https://cahi-icsa.ca/press-releases/2022-latest-canadian-pet-population-figures-released (Accessed November 28, 2024).
2. Jacobson, LS, Janke, KJ, Probyn-Smith, K, and Stiefelmeyer, K. Barriers and lack of access to veterinary Care in Canada 2022. JSMCAH. (2024) 3:1–12. doi: 10.56771/jsmcah.v3.72
3. Boissonneault, C, and Epp, T. Reflections on the provision of veterinary services to underserved regions: A case example using northern Manitoba, Canada (2018). 59:491–9.
4. Smith, SM, George, Z, Duncan, CG, and Frey, DM. Opportunities for expanding access to veterinary care: lessons from COVID-19. Front Vet Sci. (2022) 9:804794. doi: 10.3389/fvets.2022.804794
5. Baker, T, Rock, M, Brook, R, Van Der Meer, F, and Kutz, S. Indigenous community perspectives on dogs in northern Canada after 10 years of veterinary services indicates improved animal and human welfare. Prev Vet Med. (2020) 181:105061. doi: 10.1016/j.prevetmed.2020.105061
6. GNWT. Government of the Northwest Territories: NWT Bureau of Statistics. (2020). Available online at: https://www.statsnwt.ca/ (Accessed December 07, 2024).
7. Access to Veterinary Care Coalition. Access to Veterinary Care: Barriers, Current Practices, and Public Policy. (2018). Available online at: https://trace.tennessee.edu/utk_smalpubs/17 (Accessed December 11, 2024).
8. Park, RM, Gruen, ME, and Royal, K. Association between dog owner demographics and decision to seek veterinary care. Vet Sci. (2021) 8:7. doi: 10.3390/vetsci8010007
11. Pasteur, K, Diana, A, Yatcilla, JK, Barnard, S, and Croney, CC. Access to veterinary care: evaluating working definitions, barriers, and implications for animal welfare. Front Vet Sci. (2024) 11:1335410. doi: 10.3389/fvets.2024.1335410
12. LaVallee, E, Mueller, MK, and McCobb, E. A systematic review of the literature addressing veterinary care for underserved communities. J Appl Anim Welf Sci. (2017) 20:381–94. doi: 10.1080/10888705.2017.1337515
13. Baker, T, Rock, M, Bondo, K, Van Der Meer, F, and Kutz, S. 11 years of regular access to subsidized veterinary services is associated with improved dog health and welfare in remote northern communities. Prev Vet Med. (2021) 196:105471. doi: 10.1016/j.prevetmed.2021.105471
14. Curran, MM, Feseha, G, and Smith, DG. The impact of access to animal health services on donkey health and livelihoods in Ethiopia. Trop Anim Health Prod. (2005) 37:47–65. doi: 10.1007/s11250-005-9008-z
15. Duamor, CT, Hampson, K, Lankester, F, Sambo, M, Kreppel, K, Wyke, S, et al. Use of lay vaccinators in animal vaccination programmes: a scoping review. PLoS Negl Trop Dis. (2021) 15:e0009691. doi: 10.1371/journal.pntd.0009691
16. Ipara, BO, Otieno, DJ, Nyikal, R, and Makokha, NS. The contribution of extensive chicken production systems and practices to Newcastle disease outbreaks in Kenya. Trop Anim Health Prod. (2021) 53:164. doi: 10.1007/s11250-020-02550-w
17. Ma, GC, Withers, AM, Spencer, J, Norris, JM, and Ward, MP. Evaluation of a dog population management intervention: measuring indicators of impact. Animals. (2020) 10:1061. doi: 10.3390/ani10061061
18. Mtileni, BJ, Muchadeyi, FC, Maiwashe, A, Chimonyo, M, Mapiye, C, and Dzama, K. Influence of socioeconomic factors on production constraints faced by indigenous chicken producers in South Africa. Trop Anim Health Prod. (2012) 45:67–74. doi: 10.1007/s11250-012-0175-4
19. Mueller, MK, Chubb, S, Wolfus, G, and McCobb, E. Assessment of canine health and preventative care outcomes of a community medicine program. Prev Vet Med. (2018) 157:44–9. doi: 10.1016/j.prevetmed.2018.05.016
20. Riley, T, Lovett, R, Thandrayen, J, Cumming, B, and Thurber, KA. Evaluating impacts of a one health approach to companion animal health and Management in a Remote Aboriginal Community in the Northern Territory, Australia. Animals. (2020) 10:1790. doi: 10.3390/ani10101790
21. Schurer, JM, Phipps, K, Okemow, C, Beatch, H, and Jenkins, E. Stabilizing dog populations and improving animal and public health through a participatory approach in indigenous communities. Zoonoses Public Health. (2015) 62:445–55. doi: 10.1111/zph.12173
22. Slayi, M, Zhou, L, Tyasi, TL, and Jaja, I. A community-based intervention approach to control disease outbreaks and climate-related deaths in communally raised goat kids in the eastern Cape Province, South Africa. Trop Anim Health Prod. (2022) 54:140. doi: 10.1007/s11250-022-03143-5
23. Suleiman, A, Jackson, EL, and Rushton, J. Challenges of pastoral cattle production in a sub-humid zone of Nigeria. Trop Anim Health Prod. (2015) 47:1177–85. doi: 10.1007/s11250-015-0845-0
24. Utami, NWA, Agustina, KK, Atema, KN, Bagus, GN, Girardi, J, Harfoot, M, et al. Evaluation of community-based dog welfare and rabies project in Sanur, a sub-district of the Indonesian Island Province of Bali. Front Vet Sci. (2019) 6:193. doi: 10.3389/fvets.2019.00193
25. Kobelt, AJ, Hemsworth, PH, Barnett, JL, and Coleman, GJ. A survey of dog ownership in suburban Australia—conditions and behaviour problems. Appl Anim Behav Sci. (2003) 82:137–48. doi: 10.1016/S0168-1591(03)00062-5
26. Ma, GC, Ford, J, Lucas, L, Norris, JM, Spencer, J, Withers, AM, et al. “They reckon They’re Man’s best friend and I believe that.” understanding relationships with dogs in Australian aboriginal communities to inform effective dog population management. Animals. (2020) 10:810. doi: 10.3390/ani10050810
27. CDC. Social determinants of health. Centers for Disease Control and Prevention. (2022). Available online at: https://www.cdc.gov/about/sdoh/index.html (Accessed December 11, 2024).
28. Fine, A, Mueller, M, Ng, Z, Griffin, T, and Tedeschi, P. Understanding our kinship with animals In: Handbook on animal-assisted therapy. Academic Press, Cambridge, US: Elsevier (2025). 3–15.
29. Jorgenson, J. Therapeutic use of companion animals in health care. Image J Nurs Sch. (1997) 29:249–54.
30. Rodriguez, KE, Herzog, H, and Gee, NR. Variability in human-animal interaction research. Front Vet Sci. (2021) 7:619600. doi: 10.3389/fvets.2020.619600
31. Bir, C, Croney, CC, and Widmar, NJO. US residents’ perceptions of dog welfare needs and canine welfare information sources. J Appl Anim Welf Sci. (2019) 22:42–68. doi: 10.1080/10888705.2018.1476862
32. Kogan, LR, Schoenfeld-Tacher, R, Gould, L, Viera, AR, and Hellyer, PW. Providing an information prescription in veterinary medical clinics: a pilot study. J Med Libr Assoc. (2014) 102:41–6. doi: 10.3163/1536-5050.102.1.008
33. Rioja-Lang, FC, Connor, M, Bacon, HJ, Lawrence, AB, and Dwyer, CM. Prioritization of farm animal welfare issues using expert consensus. Front Vet Sci. (2020) 6:495. doi: 10.3389/fvets.2019.00495
34. Scott, P. The challenges to improve farm animal welfare in the United Kingdom by reducing disease incidence with greater veterinary involvement on farm. Animals. (2013) 3:629–46. doi: 10.3390/ani3030629
35. Baker, T, Kutz, S, Toews, L, Edwards, N, and Rock, M. Are we adequately evaluating subsidized veterinary services? A scoping review. Prev Vet Med. (2018) 157:59–69. doi: 10.1016/j.prevetmed.2018.05.015
36. Gulliford, M, Figueroa-Munoz, J, Morgan, M, Hughes, D, Gibson, B, Beech, R, et al. What does “access to health care” mean? J Health Serv Res Policy. (2002) 7:186–8. doi: 10.1258/135581902760082517
37. Bunke, L, Harrison, S, Angliss, G, and Hanselmann, R. Establishing a working definition for veterinary care desert. javma. (2024) 262:1–8. doi: 10.2460/javma.23.06.0331
38. Roberts, C, Woodsworth, J, Carlson, K, Reeves, T, and Epp, T. Defining the term “underserved:” a scoping review towards a standardized description of inadequate access to veterinary services. Can Vet J. (2023) 64:941–50.
39. Neal, SM, Anderson, M, and Greenberg, M. Mapping veterinary care in Canada: an index of care accessibility. Front. Vet. Sci. (2024) 65:325–33.
40. Neal, SM, and Greenberg, MJ. Putting access to veterinary care on the map: a veterinary care accessibility index. Front Vet Sci. (2022) 9:857644. doi: 10.3389/fvets.2022.857644
41. Reese, L, and Li, X. Animal welfare deserts: human and nonhuman animal inequities. Front Vet Sci. (2023) 10:1189211. doi: 10.3389/fvets.2023.1189211
42. Brown, CR, Garrett, LD, Gilles, WK, Houlihan, KE, McCobb, E, Pailler, S, et al. Spectrum of care: more than treatment options. Javma. (2021) 259:712–7. doi: 10.2460/javma.259.7.712
43. Einav, L, Finkelstein, A, and Gupta, A. Is American pet health care (also) uniquely inefficient? Am Econ Rev. (2017) 107:491–5. doi: 10.1257/aer.p20171087
44. Geller, JM. Street medicine: caring for the pets of the homeless. Javma. (2022) 260:181–5. doi: 10.2460/javma.21.05.0249
46. Hinchcliff, AN, and Harrison, KA. Systematic review of research on barriers to access to veterinary and medical Care for Deaf and Hard of hearing persons. J Vet Med Educ. (2021) 49:151–63. doi: 10.3138/jvme-2020-0116
47. Hohenhaus, AE. Improving access to advanced veterinary care for rescued cats and dogs. J Feline Med Surg. (2023) 25:1–10. doi: 10.1177/1098612X231211755
48. Kent, JL, and Mulley, C. Riding with dogs in cars: what can it teach us about transport practices and policy? Transp Res A Policy Pract. (2017) 106:278–87. doi: 10.1016/j.tra.2017.09.014
49. Morris, A, Wu, H, and Morales, C. Barriers to Care in Veterinary Services: lessons learned from low-income pet guardians’ experiences at private clinics and hospitals during COVID-19. Front Vet Sci. (2021) 8:764753. doi: 10.3389/fvets.2021.764753
50. Winkley, EG, KuKanich, K, Nary, D, and Fakler, J. Accessibility of veterinary hospitals for clients with mobility-related disabilities. javma. (2020) 256:333–9. doi: 10.2460/javma.256.3.333
51. Allen, EM, Call, KT, Beebe, TJ, McAlpine, DD, and Johnson, PJ. Barriers to care and health care utilization among the publicly insured. Med Care. (2017) 55:207–14. doi: 10.1097/MLR.0000000000000644
52. Butterfield, R. The relationship between social determinants of health and healthcare utilization. (2019).
53. Levesque, JF, Harris, MF, and Russell, G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. (2013) 12:18. doi: 10.1186/1475-9276-12-18
54. Ndugga, N, Pillai, D, and Artiga, S. KFF the independent source for health policy research, polling, and news. (2024). Disparities in Health and Health Care: 5 Key Questions and Answers. Available online at: https://www.kff.org/racial-equity-and-health-policy/issue-brief/disparities-in-health-and-health-care-5-key-question-and-answers/ (Accessed November 29, 2024).
55. Scheppers, E. Potential barriers to the use of health services among ethnic minorities: a review. Fam Pract. (2006) 23:325–48. doi: 10.1093/fampra/cmi113
56. Qualtrics. Qualtrics. Provo, Utah, USA: Qualtrics; (2020). Available online at: https://www.qualtrics.com (Accessed November 29, 2024).
57. Atkinson, R, and Flint, J. Accessing hidden and hard-to-reach populations: snowball research strategies (2001). 5 p.
58. Biernacki, P, and Waldorf, D. Snowball sampling: problems and techniques of chain referral sampling. Sociol Methods Res. (1981) 10:141–63.
59. Storozuk, A, Ashley, M, Delage, V, and Maloney, EA. Got bots? Practical recommendations to protect online survey data from bot attacks. TQMP. (2020) 16:472–81. doi: 10.20982/tqmp.16.5.p472
61. Miles, M, Huberman, A, and Saldaña, J. Qualitative data analysis A methods sourcebook. 4th ed. Los Angeles: SAGE (2020). 380 p.
62. Saldaña, J. The coding manual for qualitative researchers. 4th ed. Thousand Oaks, California: SAGE (2021). 414 p.
63. Sandelowski, M. What’s in a name? Qualitative description revisited. Res Nurs Health. (2010) 33:77–84. doi: 10.1002/nur.20362
64. NVivo. Lumivero. (2023). Available online at: www.lumivero.com (Accessed November 28, 2024).
65. MacQueen, KM, McLellan, E, Kay, K, and Milstein, B. Codebook development for team-based qualitative analysis. CAM J. (1998) 10:31–6.
66. Watson, B, Berliner, E, DeTar, L, McCobb, E, Frahm-Gilles, W, Henry, E, et al. Principles of veterinary community engagement. JSMCAH. (2024) 3:S2. doi: 10.56771/VCEprinciples.2024
67. Cammisa, HJ, and Hill, S. Payment options: an analysis of 6 years of payment plan data and potential implications for for-profit clinics, non-profit veterinary providers, and funders to access to care initiatives. Front Vet Sci. (2022) 9:895532. doi: 10.3389/fvets.2022.895532
68. Neill, C, and Zhang, P. Payment plans and veterinary services: Do they reduce the pain of pet owner payment? (2024); Available online at: https://ageconsearch.umn.edu/record/337554 (Accessed November 29, 2024).
69. Dubin, RJ, Angliss, G, Eng, C, Cisneros, T, and Griffon, D. Veterinarians’ perceptions of COVID-19 pandemic–related influences on veterinary telehealth and on pet owners’ attitudes toward cats and dogs. javma. (2021) 259:1140–7. doi: 10.2460/javma.21.04.0203
70. Boone, G, Bain, M, Cutler, J, and Moody, CM. Evaluating video telemedicine for providing virtual health care for cats via mock spay recheck examinations. Appl Anim Behav Sci. (2023) 267:106061. doi: 10.1016/j.applanim.2023.106061
71. Massin Teller, L, and Moberly, HK. Veterinary telemedicine: a literature review. VE. (2020) 5:1–26. doi: 10.18849/ve.v5i4.349
72. Shigekawa, E, Fix, M, Corbett, G, Roby, DH, and Coffman, J. The current state of telehealth evidence: a rapid review. Health Aff. (2018) 37:1975–82. doi: 10.1377/hlthaff.2018.05132
73. Neill, CL, and Morgan, KL. Few differences in rural and urban adoption of veterinary telehealth services. Javma. (2024) 262:1–5. doi: 10.2460/javma.24.01.0070
74. Hassan, M, Abdulkarim, A, and Seida, A. Veterinary telemedicine: a new era for animal welfare. Open Vet J. (2024) 14:952. doi: 10.5455/OVJ.2024.v14.i4.2
75. Watson, K, Wells, J, Sharma, M, Robertson, S, Dascanio, J, Johnson, JW, et al. A survey of knowledge and use of telehealth among veterinarians. BMC Vet Res. (2019) 15:474. doi: 10.1186/s12917-019-2219-8
76. Bezrukova, K, Spell, CS, Perry, JL, and Jehn, KA. A meta-analytical integration of over 40 years of research on diversity training evaluation. Psychol Bull. (2016) 142:1227–74. doi: 10.1037/bul0000067
77. Ly, LH, Gordon, E, and Protopopova, A. Exploring the relationship between human social deprivation and animal surrender to shelters in British Columbia, Canada. Front Vet Sci. (2021) 8:656597. doi: 10.3389/fvets.2021.656597
78. Morris, S. A demographic, employment and income profile of Canadians with disabilities aged 15 years and over, (2017).
79. Kelly, C, Dansereau, L, Sebring, J, Aubrecht, K, FitzGerald, M, Lee, Y, et al. Intersectionality, health equity, and EDI: What’s the difference for health researchers? Int J Equity Health. (2022) 21:182. doi: 10.1186/s12939-022-01795-1
80. Jenkins, JL, and Rudd, ML. Decolonizing animal welfare through a social justice framework. Front Vet Sci. (2022) 8:787555. doi: 10.3389/fvets.2021.787555
81. Blackwell, MJ, and O’Reilly, A. Access to veterinary care–a National Family Crisis and case for one health. Advan Small Animal Care. (2023) 4:145–57. doi: 10.1016/j.yasa.2023.05.003
82. Kelley, JC, Ramirez, V, and Meisner, J. Evaluation of a one health clinic: enhancing access to healthcare and housing for young adults experiencing homelessness with animals. CABI One Health. (2024) 3:1–7. doi: 10.1079/cabionehealth.2024.0004
83. Robert, DI, Martin, SW, and Stryhn, H. Veterinary epidemiologic research. 2nd ed. Charlotte, P.E.I: VER, Inc. (2014). 865 p.
84. Canadian Veterinary Medical Association. Access to veterinary Care in Canada. (2024). Available online at: https://www.canadianveterinarians.net/policy-and-outreach/position-statements/statements/access-to-veterinary-care-in-canada/ (Accessed December 04, 2024).
Keywords: access to care, community and shelter medicine, veterinary desert, underserved community, equity
Citation: Rausch Q, Alhamdan M, Bateman S, Evason M, Fraser-Celin V, Graham C, Saad J, Tuma M, Ward K and Van Patter L (2025) Access to veterinary care in Canada: a cross-sectional survey of animal healthcare organizations and interventions. Front. Vet. Sci. 12:1581316. doi: 10.3389/fvets.2025.1581316
Edited by:
Azalia Boyd, Boyd Veterinary Services and Consulting, LLC., United StatesReviewed by:
Sue Neal, Arkansas State University, United StatesKristin Jankowski, University of California, Davis, United States
Copyright © 2025 Rausch, Alhamdan, Bateman, Evason, Fraser-Celin, Graham, Saad, Tuma, Ward and Van Patter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Quinn Rausch, cXJhdXNjaEB1b2d1ZWxwaC5jYQ==