 Luciana D'Alessio1,2*
Luciana D'Alessio1,2* Guido Pablo Korman3
Guido Pablo Korman3 Mercedes Sarudiansky3
Mercedes Sarudiansky3 Laura Ruth Guelman4
Laura Ruth Guelman4 Laura Scévola2
Laura Scévola2 Alejandra Pastore5
Alejandra Pastore5 Amilcar Obregón5
Amilcar Obregón5 Emilio J. A. Roldán5
Emilio J. A. Roldán5- 1Universidad de Buenos Aires, Facultad de Medicina, IBCN-CONICET, Buenos Aires, Argentina
- 2Universidad de Buenos Aires, Hospital Ramos Mejía, Buenos Aires, Argentina
- 3Universidad de Buenos Aires, Facultad de Psicología, CAEA-CONICET, Buenos Aires, Argentina
- 4Universidad de Buenos Aires, Facultad de Medicina, CEFYBO-CONICET, Buenos Aires, Argentina
- 5Dirección Médica y Científica, Gador SA, Buenos Aires, Argentina
The allostatic load (AL) index constitutes a useful tool to objectively assess the biological aspects of chronic stress in clinical practice. AL index has been positively correlated with cumulative chronic stress (physical and psychosocial stressors) and with a high risk to develop pathological conditions (e.g., metabolic syndrome, cardiovascular pathology, inflammatory disorders) and the so-called stress-related psychiatric disorders, including anxiety and depressive disorders. Chronic stress has negative effects on brain neuroplasticity, especially on hippocampal neurogenesis and these effects may be reversed by antidepressant treatments. Several evidences indicate that non-pharmacological interventions based on physical activity and yoga practice may add synergizing benefits to classical treatments (antidepressant and benzodiazepines) for depression and anxiety, reducing the negative effects of chronic stress. The aim of this review is to provide a general overview of current knowledge on AL and chronic stress in relation to depression and anxiety, physical activity and yoga practice.
Introduction
The concept of allostatic load (AL) index, has been introduced by Bruce McEwen and Stellar in 1993 to objectively assess the biological consequences of chronic stress in the body and the brain (1). Psychosocial factors related to poverty and health risk behaviors across the lifespan have been associated with higher AL index (2, 3). AL index has been positively correlated with cumulative chronic stress (physical and psychosocial stressors) and with a high risk to acquire medical conditions (e.g., metabolic syndrome, cardiovascular pathology, inflammatory disorders) (4–8). Moreover, chronic stress and AL overload may contribute to the expression of the so-called stress-related psychiatric disorders, especially represented by anxiety and depressive disorders (5, 9–12). Furthermore, chronic stress through hypercortisolemia can induce negative effects on brain neuroplasticity, especially on hippocampal neurogenesis (13–16) and these effects may be reversed by antidepressant treatments (17, 18).
Evidences based on experimental data and studies in human patients indicate that physical activity and yoga practice might bring about benefits not only in adult hippocampal neurogenesis and neuroplasticity (19), but also on stress related psychiatric symptoms (anxiety and depression) (20, 21) as well as on AL index (22, 23). Non-pharmacological interventions and classical treatments (psychotherapeutic and pharmacological approaches) may have synergistic effects on brain function and clinical symptoms which helps building the idea of managing depression and anxiety disorders using combined treatments (19, 21). The implementation of these strategies as add-on therapy may optimize the pharmacological treatment reducing the risk of adverse side effects. Therefore, the aims of this review are to provide an overview of the biology aspects of AL and chronic stress in reference to depression and anxiety, and to describe the current knowledge on the non-pharmacological interventions based on physical activity and yoga practice upon AL, depression and anxiety.
The Allostasis Concept and the Allostatic Load Index
The term allostasis refers the ability to achieve stability through changes in response to stress and/or stressful events (4). The most important systems involved in the stress response are the hypothalamic-pituitary-adrenal (HPA) axis, the autonomic nervous system and the inflammatory system, with their respective biochemical mediators, the glucocorticoids, the catecholamines (adrenaline and noradrenaline) and the cytokines. These compounds produce physiologic effects that are adaptive in the short term, however they can be harmful in the long term (chronic stress) (4, 5, 10, 13).
The AL index was proposed with the aim of measuring the cumulative influence of stress on health through a series of clinical and biochemical indicators of the main systems potentially affected (4, 6). Essentially, the AL index constitutes a marker of cumulative biological risk of chronic stress which describes the additive effects of multiple clinical situations that may accelerate the vulnerability to diseases reducing resilience (9, 10, 24–26). The AL index was found to be a good predictor of mortality and physical functioning (27). The clinimetric definition of AL overload, firstly introduced by Feinstein in 1987 to define clinical measurements related to chronic stress, was recently described by Fava and McEwen et al. in 2019 (27). These authors proposed two main criteria: the presence of a current source of distress added to previous symptoms or functioning impairment (27).
AL index includes different biological markers divided in two main groups; 1-Primary mediators: represented by stress hormones (adrenaline, noradrenaline, and cortisol) in combination with inflammatory cytokines (e.g., interleukin-6, tumor necrosis factor), 2- Secondary mediators: represented by biomarkers of metabolic, cardiovascular, and immune systems that compensate primary mediators alterations [e.g., insulin, glucose, total cholesterol, high density lipoprotein cholesterol, triglycerides, visceral fat depositing, systolic and diastolic blood pressure, fibrinogen, c-reactive protein; (2, 8, 28)]. Different authors have applied the AL index in population-based studies and/or in clinical trials and studied the association with depression and anxiety disorders (8, 11, 28–32). Table 1 summarizes the AL index and the cut off points analyzed in a previous study performed by our group, in patients with general anxiety disorder (12, 32).
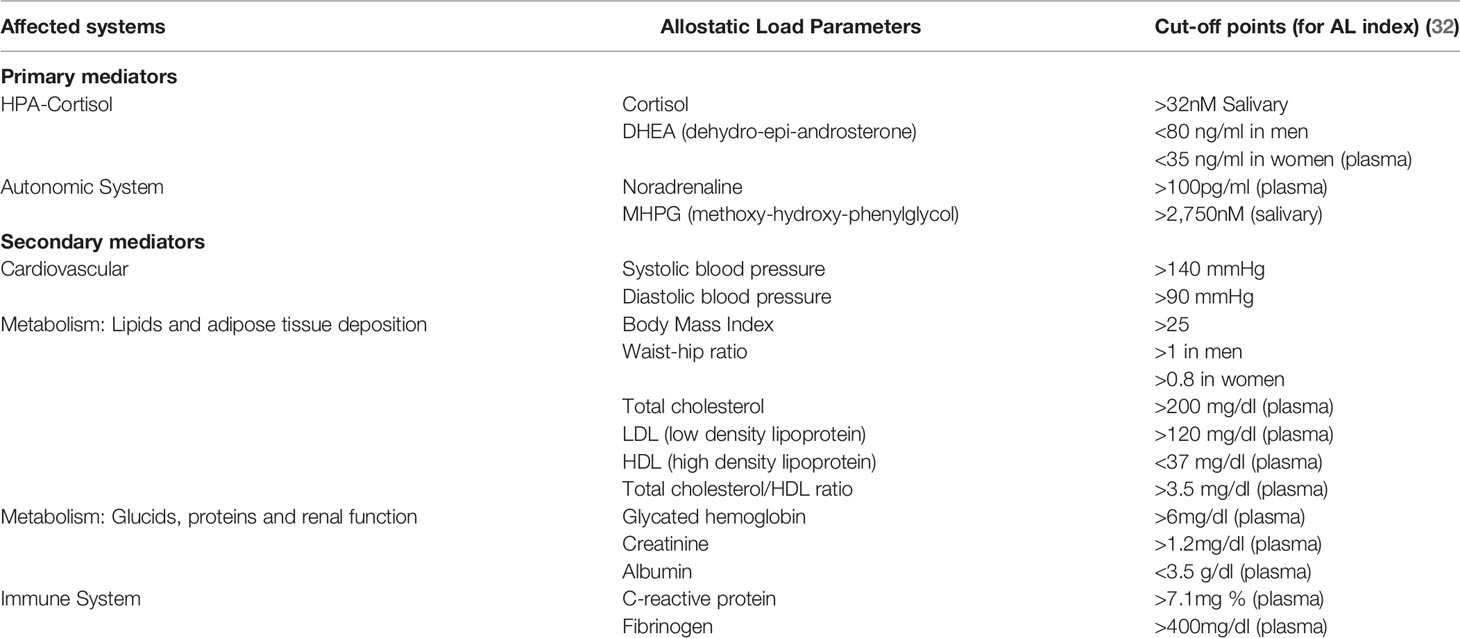
Table 1 Allostatic load parameters and cut-off points.
Depression, Anxiety, and AL
The relationship between chronic stress, depression and anxiety has been extensively described (5, 9, 10, 13). Experimental models showed that stress hormones (glucocorticoids) acting on the brain, may modify emotional arousal, predisposing to depression- and anxiety-like behavior (33). Furthermore, chronic stress models in rodents can cause changes in brain neuroplasticity and changes in behavior consistent with depressive- and anxiety-like symptoms (5, 9, 10, 13, 33–36).
In humans, the administration of exogenous glucocorticoids may produce psychiatric adverse effects, such as steroid psychoses and depression. These symptoms may be blocked by the glucocorticoid antagonist mifepristone (37, 38). In patients with major depressive disorder, cortisol levels are elevated, the diurnal rhythm is distorted and the HPA axis is resistant to suppression by dexamethasone (9, 33, 37, 38). Moreover, higher AL index has been associated with higher levels of depressive symptoms in many studies (8, 11) (28–30, 39). Compared with patients with personality disorders, emergency psychiatric patients primarily diagnosed with bipolar, depressive, or anxiety disorders showed altered AL parameters including cortisol, interleukin-6, systolic blood pressure, and heart rate (11). Also, higher AL index were significantly associated with depressive symptoms (29) showing variations according to sex, gender, race, and sociocultural factors (30, 31).
Cardiovascular parameters of AL index were frequently altered in patients with depression (11, 28, 29). Longitudinal cohort studies showed increase risk of cardiovascular morbidity and mortality among patients with comorbid depression (40). In a recent study, Gillespie et al. analyzed the role of AL and depression in relation to coronary heart disease. Greater depressive symptomatology was associated with higher metabolic, cardiovascular, and immune AL parameters, however coronary heart disease was associated to depression, only in male population (28). Obesity, metabolic abnormalities and higher expression of inflammatory markers were also frequently observed in patients with depression (23, 30, 41). Compared with age- and gender-matched control groups, individuals with major depression had higher metabolic syndrome prevalence, hyperglycaemia, and hypertriglyceridemia (41).
Regarding anxiety, high levels of cortisol and CRH (corticotrophin releasing hormone), have been associated to fear states and anxiety-like behavior in experimental models (13, 33). Disturbances in the HPA with hypercortisolemia were reported among patients with anxiety disorders, in patients with panic disorder (42) and in patients with general anxiety disorder (32, 43). In addition, sympathetic hyperactivity with high levels of methoxyhidroxiphenilglicol (MHPG) (the main metabolite of noradrenaline) was also reported in patients with anxiety disorder (32, 44, 45).
Sex and age related differences in psychiatric symptoms and AL parameters were also described in the literature (28–30, 32, 46). Firstly, a higher prevalence and severity of depression and anxiety disorders has been reported in women compared to men (29, 32, 47). Biological differences have been proposed to explain such differences since experimental studies in rodents suggest sex differences in the neural remodeling pattern after stress (10, 48). However, psychosocial influences cannot be excluded as women are also more exposed to psychosocial stress and trauma (30, 49, 50). Women in fertile age are less prone to cardiovascular disease and mortality than men (28, 31, 51, 52). In a previous study of our group in patients with anxiety disorders, women showed higher anxiety levels than men, with a better profile in many individual AL variables, particularly cardiovascular (systolic blood pressure), obesity (body mass index), and lipids with higher HDL (high density lipoprotein cholesterol) levels (32). On the opposite, AL inflammatory parameters tended to be higher in women (30, 46, 52). Regarding age factors, elderly patients were more vulnerable to stress-related disorders and expressed higher levels of cumulative AL (2, 6, 7, 32).
Chronic Stress and Hippocampal Neuroplasticity: The Role of Antidepressant Treatments
The hippocampus has been in the focus of stress research especially after the finding that glucocorticoids receptors are abundantly expressed in hippocampal cells (53). A large body of evidence in rodents demonstrated that chronic stress, via elevated levels of glucocorticoids, can affect both hippocampal structure and function (16, 33, 54) and can also induce depressive-like behavior (18). Adult hippocampal neurogenesis (the brain capacity to develop new neurons during adult life) (55), decrease with age and is especially affected by chronic stress (15, 56, 57).
Hippocampal structure and function might be altered in patients with depression. Reductions in hippocampal volume based on magnetic resonance imaging studies have been consistently documented in patients with major depression (58, 59). For example, patients suffering from recurrent depressive episodes showed lower hippocampal volume (60, 61). Similarly, in Cushing's disease, the duration of the illness predicts a progressive reduction in the hippocampus volume, which was determined by structural magnetic resonance imaging (62). Besides, the atrophy of the hippocampus has also been reported among patients with anxiety-related disorders and post-traumatic stress disorder (63). Moreover, depression is a common comorbidity in patients with resistant temporal lobe epilepsy and hippocampal sclerosis (14, 64, 65).
In humans, adult hippocampal neurogenesis occurs in the hippocampal dentate gyrus, and newborn neurons can be produced from neural stem cells which can be classified based on their distinctive morphology as radial glia-like (66) and non-radial glial cells (67). Chronic physical stressors, chronic psychosocial stressors, and chronic unpredictable stressors, can inhibit one or more phases of the adult hippocampal neurogenesis process (15). Neurotransmitters systems that regulate adult hippocampal neurogenesis might be affected by chronic stress: The enhance of glutamate release via NMDA (N-methyl-D-aspartate receptor), the reduction of GABA (Gamma aminobutyric acid) levels, the reduction of 5HT (serotonin) levels and the down regulation of 5HT1A (serotonin receptor 1A; stimulation of 5HT1A is pro-neurogenic), and the alterations in noradrenaline, dopamine, and endocannabinoids were described (18, 57, 68). Stress can also reduce the expression of neurotrophic factors involved in adult hippocampal neurogenesis regulation (e.g., brain-derived neurotrophic factor, insulin-like growth factor-1, neuregulin-1; 69, 70). Neurotrophic factors have been shown to increase adult hippocampal neurogenesis and also modulate antidepressant-related effects and behavior in experimental models (18, 71).
Adult hippocampal neurogenesis is involved in mediating the response to antidepressant drugs (18, 72). The suppression of adult hippocampal neurogenesis achieved by chronic stress can be prevented by administering antidepressants (72, 73) which reverse the inhibitory effect of stress after 3–4 weeks of treatment (time course of maturation for newly generated neurons) (17, 72–75). Antidepressants require of adult hippocampal neurogenesis mechanisms to be effective (57, 76) and involve the activation of glucocorticoid receptors in the hippocampus (77). The stimulation of adult hippocampal neurogenesis has been considered a promising property for identifying new antidepressant targets. At the moment almost all antidepressant treatments including pharmacotherapy and behavioral interventions, proved to stimulate adult hippocampal neurogenesis (15, 57, 78).
Chronic Stress and Anxiety: Role of Anxiolytics Treatments
During stress response sympathetic system is simultaneously activated with HPA system, and both noradrenaline and cortisol are released, amplifying the emotional response (4, 5, 10, 13). Anxiety has been proposed as an undifferentiated form of fear or rage, discharged by noradrenaline and cortisol (79). Anxiolytic drugs acting through a positive allosteric modulation of GABA-A receptor (benzodiazepines), reduce the sympathetic discharge leading to lower plasma levels of catecholamines (80–82) and lower salivary levels of MHPG (44, 45, 83, 84). Benzodiazepines, particularly those of high-potency such as alprazolam, have demonstrated anti-hypertensive pleiotropic properties in patients with high blood pressure without affecting the heart rate (81, 85). In our previous work (32), low doses of alprazolam during 12 weeks reduced anxiety levels and the total AL index. We observed a significant reduction on salivary levels of MHPG and on systolic blood pressure (12, 32). As well pharmacotherapy with benzodiazepines in association to psychotherapy demonstrated to be effective in reducing anxiety and AL parameters (86), the risk of inducing pharmacological dependence and/or cognitive adverse events should be considered requiring continuous monitoring (87–89).
Non-Pharmacological Strategies, Physical Activity, and Yoga Practice
Physical Activity
Many studies based on experimental research in rodents demonstrated that physical activity interventions may promote hippocampal neuroplasticity, counteracting the negative effects of chronic stress on the brain (15, 19, 90–95). Models of aerobic exercise potently stimulate adult hippocampal neurogenesis, inducing higher rates of proliferation and/or survival of newborn cells (15, 90). Also, higher synaptic plasticity and higher levels of BDNF (Brain Derived Neurotrophic Factor), were observed in hippocampus, after voluntary and involuntary exercise (91, 92). Additionally, the use of combined treatments (e.g., aerobic exercise and antidepressant treatments), has stronger effect on depressive behavior and on BDNF up-regulating, than antidepressant treatment or aerobic exercise acting individually (93–95).
In humans, neuroimaging studies using MRI (Magnetic Resonance Image) demonstrated that physical activity increased the hippocampal volume and positively correlated with better performances on hippocampus dependent tasks (episodic memory) (96). Physical activity can enhance some indirect signs of neuroplasticity (e.g., increased cerebral blood flow or BDNF plasma concentration) (96). Plasma levels of BDNF have been proposed as a potential biomarker of depression treatment. Serum BDNF is decreased in depressed patients and can be normalized with antidepressant treatment together with moderate to intense physical activity (97, 98).
Physical activity has been considered a non-stigmatizing intervention with few side effects and has been associated with the relief of depression and anxiety symptoms in different studies (20, 21, 99, 100). Different types of physical activity (aerobic, stretching, leisure-physical activities, dance, yoga asanas), have been associated with lower depression and anxiety prevalence in population-based studies (23, 100–102), with a better outcome in patients with depressive disorders (103–106) and with lower scores of self-reported stress, anxiety, and depression scales in healthy subjects (107–109). Physical activity may prevent the development of depression during the follow up according prospective studies (23, 100, 102), can reduce de the risk of anxiety (110) and may enhance the cognitive performance (97) contributing with antidepressant drugs and/or cognitive-behavioral therapy (111). In a meta-analysis of relevant randomized controlled clinical trials, aerobic exercise showed moderate to large effects for patients with major depression and favoured over classical psychological treatments or antidepressants drugs (20). Physical activity may act as an adjunctive treatment to traditional medication and psychotherapy, resulting in a more effective approach toward relief of psychiatric symptoms and AL (19, 20, 99, 105).
Table 2 resumes the main recent studies that have analyzed physiological AL parameters and the effects of physical activity (and/or yoga asanas) on depression and anxiety outcome. All resumed studies, population-based studies and clinical trials, found a positive effect on depression and anxiety symptoms outcome in healthy subjects and in patients with depression. Although the total AL index was not measured, some of these studies analyzed certain AL parameters outcome. Obesity factors were positively associated with depression and negatively with physical activity (23). A lower fitness level in cardiopulmonary exercises was observed in patients with depression (104). Minor resting pulse was associated with physical activity and lower risk to develop depression in healthy subjects (100). Also, lower heart rate and diastolic blood pressure and higher HDL cholesterol, were observed among inpatients with major depressive disorder who underwent to a physical activity-training program (105). Regarding the effects of physical activity on AL parameters sex differences were also reported (106, 112). Women showed higher levels of c-reactive protein, which positively correlated with measures of adiposity and inversely associated with fitness, suggesting that adiposity may play a more substantial role in inflammation in women (106). Although these preliminary findings are promising, larger and adequately powered randomised controlled trials are needed to better evaluate the combined effect of physical activity and classical treatments on allostatic load and on depression and anxiety.
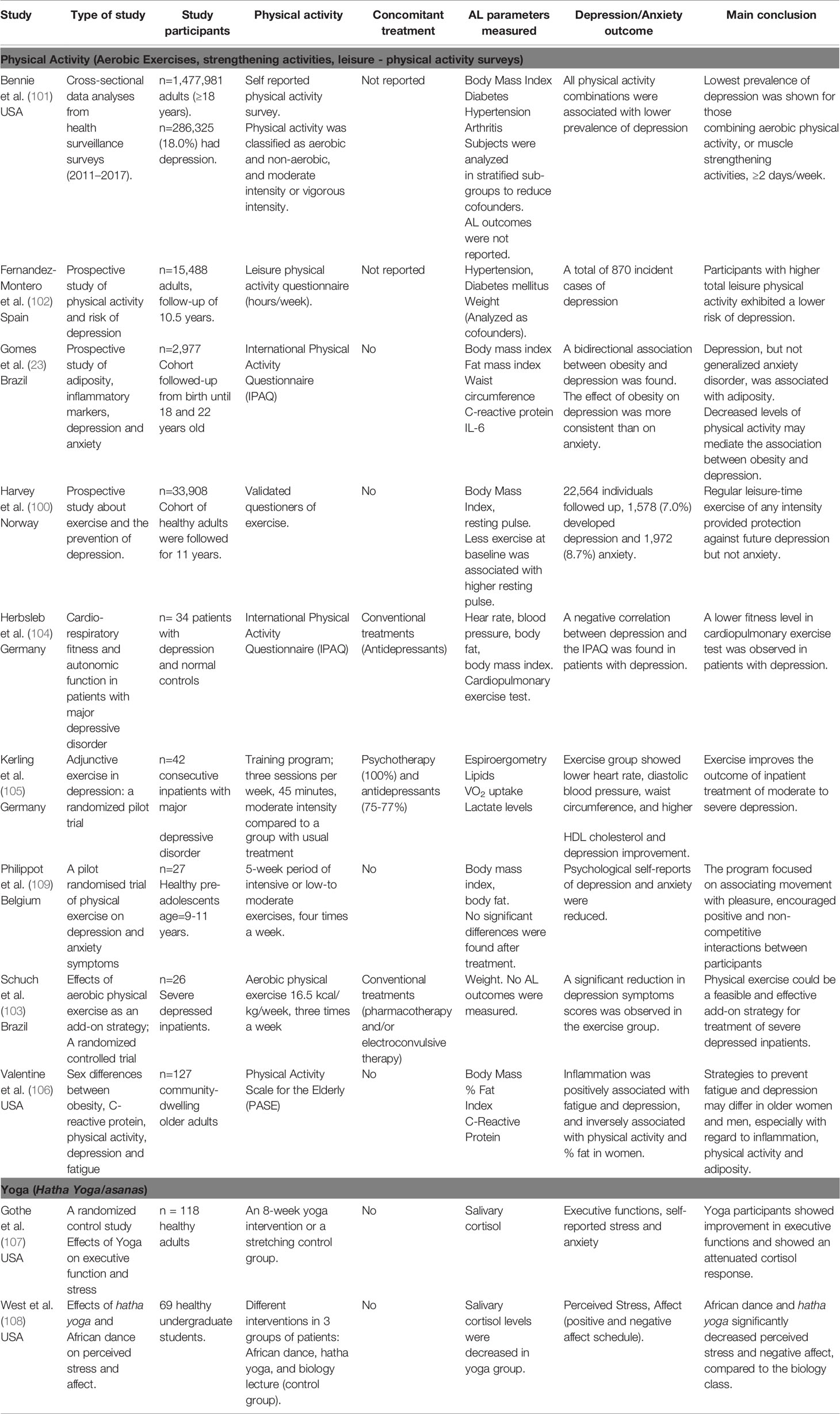
Table 2 Description of the studies that have been analyzed the physiological AL parameters and the effects of physical activity and yoga asanas on anxiety and depression outcome.
Yoga Practice
In the last years, yoga has become popular in western cultures and constitutes an interesting tool for stress management. Although yoga originated in India, different yoga styles are practiced in western societies at present. Most of the different styles contain physical postures (termed asana in Sanskrit), as well as breath control exercises (pranayama) and meditation (dyana) (113). A meta-analysis of randomised controlled trials performed on healthy subjects and on patients with medical conditions (e.g cardiopathy, hypertension, metabolic syndrome, obesity, breast cancer), showed that yoga practice may reduce physiological measures of stress, including cortisol, autonomic measures (systolic blood pressure, heart rate), cytokines, and lipid levels (21). Also, yoga practice showed positive effects on depression and on anxiety symptoms in pregnant women (114), improved the mood states in psychiatric inpatients (115) and had beneficial effects on depression outcome in patients with major depressive disorder (116–118).
Regarding AL parameters, attenuated and decreased levels of salivary cortisol after yoga practice were reported in clinical trials on healthy patients(107, 108). These results correlated with lower perceived stress and negative affect (108) and with better cognitive functions, lower self-reported stress, and minor anxiety levels (107) (Table 2). Clinical evidences showed that yoga asanas can modulate the autonomic nervous system inducing higher parasympathetic activity, lower blood pressure, lower heart rate, higher relaxation and approach behaviors (21, 119). In a recent study using magnetic resonance spectroscopy yoga practice has been associated to higher GABA levels in patients with major depressive disorder (118).
A combination of body awareness-yoga asanas and mindfulness meditation has been developed in a complete program for stress reduction (21) and has been proposed to clinicians as a safe and effective technique to reduce stress and anxiety in diverse patient populations (21, 120, 121) reducing stress, anxiety and depression, increasing the quality of life and well-being (107, 122–124). Yoga practice effectively decreases depressive and anxious symptomatology, although the neurobiological mechanisms involved are not totally elucidated (21). Regarding brain effects, neuroimaging studies demonstrated that hippocampus is activated during yoga practice (113, 125, 126). Moreover, a significantly greater hippocampal volume has been found in experienced yoga practitioners (113, 126, 127) and higher volumetric measures in different brain areas were positively correlated with the years of yoga practice (113).
Conclusions
Non-pharmacological interventions such as physical activity and yoga practice may exert synergizing effects to antidepressant and anxiolytic treatments. The classical treatment of patients with anxiety disorders and depression is psychotherapy, but pharmacotherapy is recommended when psychiatric symptoms are severe enough to induce a significant functional impairment (86). Antidepressants and/or benzodiazepines are indicated (National for Health and Clinical Excellence, UK guidelines) to treat these disorders (86). However, pharmacological treatments may be associated with adverse side effects. Physical activity and yoga practice have been shown to elicit improvements in anxiety and depression symptoms conducting to a better social, physical, and affective well-being optimizing the pharmacological treatment duration and the risk of pharmacological adverse side effects. However, larger and adequately powered randomized controlled trials are needed to evaluate the combined effect of physical activity on allostatic load and on depression and anxiety. Also, is important to emphasize that future studies are needed to reveal the biological mechanisms involved in the therapeutic actions of physical activity and yoga, in particular on depression and anxiety. Furthermore, stratified interventions according to sex and age should be considered in the future to track the therapies toward an individualized schedule in agreement with the current medical practice.
Author Contributions
LD'A, GK, MS, LG, and LS have been involved in drafting and revising the manuscript for intellectual content. AO, AP, and ER have made substantial contributions to the conception and design. LD'A and ER have given the final approval of the version to be published.
Conflict of Interest
LD'A received a grant for participating in this project from Gador SA. AO, AP, and ER are employees of Gador SA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Clara Proverbio for her writing assistance.
References
1. McEwen B, Stellar E. Stress and the individual. Mechanisms leading to disease. Arch Intern Med (1993) 27(153):2093–101. doi: 10.1001/archinte.153.18.2093
2. Seeman T, Epel E, Gruenewald T, Karlamangla A, McEwen BS. Socio-economic differentials in peripheral biology: cumulative allostatic load. Ann N Y. Acad Sci (2010) 1186:223–39. doi: 10.1111/j.1749-6632.2009.05341.x
3. Suvarna B, Suvarna A, Phillips R, Juster RP, McDermott B, Sarnyai Z. Health risk behaviours and allostatic load: A systematic review. Neurosci Biobehav Rev (2020) 108:694–711. doi: 10.1016/j.neubiorev.2019.12.020
4. McEwen BS. Stress, adaptation, and disease. Allostasis and allostatic load. Ann N Y Acad Sci (1998) 1(840):33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
5. McEwen BS. The neurobiology of stress: from serendipity to clinical relevance. Brain Res (2000) 886(1–2):172–89. doi: 10.1016/S0006-8993(00)02950-4
6. Crimmins EM, Johnston M, Hayward M, Seeman T. Age differences in allostatic load: an index of physiological dysregulation. Exp Gerontol (2003) 38:731–4. doi: 10.1016/S0531-5565(03)00099-8
7. Seeman TE, Crimmins E, Huang MH, Singer B, Bucur A, Gruenewald T, et al. Cumulative biological risk and socio-economic differences in mortality: MacArthur Studies of Successful Aging. Soc Sci Med (2004) 58:1985–97. doi: 10.1016/S0277-9536(03)00402-7
8. Juster R, McEwen BS, Lupien SJ. Neuroscience and Biobehavioral Reviews Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev (2010) 35(1):2–16. doi: 10.1016/j.neubiorev.2009.10.002
9. McEwen BS. Mood disorders and allostatic load. Biol Psychiatry (2003) 54(3):200–7. doi: 10.1016/S0006-3223(03)00177-X
10. McEwen BS. Neurobiological and Systemic Effects of Chronic Stress. Chronic Stress (2017) 1:1–17. doi: 10.1177/2470547017692328
11. Juster RP, Sasseville M, Giguère CÉ., Consortium S, Lupien SJ. Elevated allostatic load in individuals presenting at psychiatric emergency services. J Psychosom Res (2018) 115:101–9. doi: 10.1016/j.jpsychores.2018.10.012
12. Soria CA, Remedi C, Núñez D, D'Alessio L, Roldán EJ. Impact of alprazolam in allostatic load and neurocognition of patients with anxiety disorders and chronic stress (GEMA): observational study protocol. BMJ Open (2015) 5:e007231. doi: 10.1136/bmjopen-2014-007231
13. de Kloet ER, Joëls M, Holsboer F. Stress and the brain: from adaptation to disease. Nat Rev Neurosci (2005) 6:463–75. doi: 10.1038/nrn1683
14. Swaab DF, Bao AM, Lucassen PJ. The stress system in the human brain in depression and neurodegeneration. Ageing Res Rev (2005) 4(2):141–94. doi: 10.1016/j.arr.2005.03.003
15. Lucassen P, Meerlo P, Naylor A, Dam AMV, Dayer A, Fuchs E, et al. Regulation of adult neurogenesis by stress, sleep disruption, exercise and inflammation: Implications for depression and antidepressant action. Eur Neuropsychopharmacol (2010) 20(1):1–17. doi: 10.1016/j.euroneuro.2009.08.003
16. McEwen BS, Gianaros PJ. Stress- and allostasis-induced brain plasticity. Annu Rev Med (2011) 62:431–45. doi: 10.1146/annurev-med-052209-100430
17. Santarelli L, Saxe M, Cross C, Surget A, Battaglia F, Dulawa S, et al. Requirement of Hippocampal Neurogenesis for the Behavioral Effects of Antidepressants. Sci (80-. ). (2003) 301:805–9. doi: 10.1126/science.1083328
18. Mahar I, Bambico FR, Mechawar N, Nobrega JN. Stress, serotonin, and hippocampal neurogenesis in relation to depression and antidepressant effects. Neurosci Biobehav Rev (2014) 38:173–92. doi: 10.1016/j.neubiorev.2013.11.009
19. Kandola A, Hendrikse J, Lucassen PJ, Yücel M, Nolan Y. Aerobic Exercise as a Tool to Improve Hippocampal Plasticity and Function in Humans: Practical Implications for Mental Health Treatment. Front Hum Neurosci (2016) 10:1–25. doi: 10.3389/fnhum.2016.00373
20. Morres ID, Hatzigeorgiadis A, Stathi A, Comoutos N, Arpin-Cribbie C, Krommidas C, et al. Aerobic exercise for adult patients with major depressive disorder in mental health services: A systematic review and meta-analysis. Depress Anxiety (2019) 36(1):39–53. doi: 10.1002/da.22842
21. Pascoe MC, Thompson DR, Ski CF. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology (2017) 86:152–68. doi: 10.1016/j.psyneuen.2017.08.008
22. O'Keefe EL, O'Keefe JH, Lavie CJ. Exercise Counteracts the Cardiotoxicity of Psychosocial Stress. Mayo Clin Proc (2019) 94(9):1852–64. doi: 10.1016/j.mayocp.2019.02.022
23. Gomes AP, Soares ALG, Menezes AMB, Assunção MC, Wehrmeister FC, Howe LD, et al. Adiposity, depression and anxiety: interrelationship and possible mediators. Rev Saude Publica (2019) 53:103. doi: 10.11606/S1518-8787.2019053001119
24. McEwen BS. Stressed or stressed out: what is the difference? J Psychiatry Neurosci (2005) 30(5):315–8. doi: 10.1111/j.1365-2702.2008.02347.x
25. Danese A, McEwen BS. Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiol Behav (2012) 106(1):29–39. doi: 10.1016/j.physbeh.2011.08.019
26. Karatsoreos IN, McEwen BS. Resilience and vulnerability: a neurobiological perspective. F1000Prime Rep (2013) 5:13. doi: 10.12703/P5-13
27. Fava GA, McEwen BS, Guidi J, Gostoli S, Offidani E, Sonino N. Clinical characterization of allostatic overload. Psychoneuroendocrinology (2019) 108:94–101. doi: 10.1016/j.psyneuen.2019.05.028
28. Gillespie SL, Anderson CM, Zhao S, Tan Y, Kline D, Brock G, et al. Allostatic Load in the Association of Depressive Symptoms with Incident Coronary Heart Disease: The Jackson Heart Study. Psychoneuroendocrinology (2019) 109:104369. doi: 10.1016/j.psyneuen.2019.06.020
29. Rodriquez EJ, Sabado-Liwag M, Pérez-Stable EJ, Lee A, Haan MN, Gregorich SE, et al. Allostatic Load, Unhealthy Behaviors, and Depressive Symptoms by Birthplace Among Older Adults in the Sacramento Area Latino Study on Aging (SALSA). J Aging Health (2019) 22:1–18. doi: 10.1177/0898264319857995
30. Bey G, Jesdale B, Ulbricht C, Mick E, Person S. Allostatic Load Biomarker Associations with Depressive Symptoms Vary among US Black and White Women and Men. Healthcare (2018) 6(3):105. doi: 10.3390/healthcare6030105
31. Juster RP, Pruessner JC, Desrochers AB, Bourdon O, Durand N, Wan N, et al. Sex and Gender Roles in Relation to Mental Health and Allostatic Load. Psychosom Med (2016) 78(7):788–804. doi: 10.1097/PSY.0000000000000351
32. Soria CA, Remedi C, D'Alessio L, Roldán EJA. Sex and Age-Related Differences in Neuroticism and Allostatic Load Index in Urban Patients with General Anxiety Disorder Treated with Alprazolam. Open J Psychiatry (2018) 8(3):212–32. doi: 10.4236/ojpsych.2018.83019
33. de Kloet ER, Otte C, Kumsta R, Kok L, Hillegers MHJ, Hasselmann H, et al. Stress and Depression: a Crucial Role of the Mineralocorticoid Receptor. J Neuroendocrinol (2016) 28(8):1–12. doi: 10.1111/jne.12379
34. Magariños AM, Verdugo JM, McEwen BS. Chronic stress alters synaptic terminal structure in hippocampus. Proc Natl Acad Sci U S A (1997) 94:14002–8. doi: 10.1073/pnas.94.25.14002
35. Datson NA, Van Den Oever JME, Korobko OB, Magarinos AM, De Kloet ER, McEwen BS. Previous history of chronic stress changes the transcriptional response to glucocorticoid challenge in the dentate gyrus region of the male rat hippocampus. Endocrinology (2013) 154(9):3261–72. doi: 10.1210/en.2012-2233
36. Nasca C, Zelli D, Bigio B, Piccinin S, Scaccianoce S, Nisticò R, et al. Stress dynamically regulates behavior and glutamatergic gene expression in hippocampus by opening a window of epigenetic plasticity. Proc Natl Acad Sci U S A (2015) 112(48):14960–5. doi: 10.1073/pnas.1516016112
37. Belanoff JK, Rothschild AJ, Cassidy F, DeBattista C, Baulieu EE, Schold C, et al. An open label trial of C-1073 (mifepristone) for psychotic major depression. Biol Psychiatry (2002) 52:386–92. doi: 10.1016/S0006-3223(02)01432-4
38. Gallagher P, Young AH. Mifepristone (RU-486) treatment for depression and psychosis: A review of the therapeutic implications. Neuropsychiatr Dis Treat (2006) 2(1):33–42. doi: 10.1111/j.1601-5215.2006.00152.x
39. Juster RP, Marin MF, Sindi S, Nair NPV, Ng YK, Pruessner JC, et al. Allostatic load associations to acute, 3-year and 6-year prospective depressive symptoms in healthy older adults. Physiol Behav (2011) 104(2):360–4. doi: 10.1016/j.physbeh.2011.02.027
40. Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: A meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J (2006) 27(23):2763–74. doi: 10.1093/eurheartj/ehl338
41. Vancampfort D, Correll CU, Wampers M, Sienaert P, Mitchell AJ, De Herdt A, et al. Metabolic syndrome and metabolic abnormalities in patients with major depressive disorder: A meta-analysis of prevalences and moderating variables. Psychol Med (2014) 44(10):2017–28. doi: 10.1017/S0033291713002778
42. Wedekind D RE, Bandelow B, Broocks A, Hajak G. Salivary, total plasma and plasma free cortisol in panic disorder. J Neural Transm (2000) 107(7):831–7. doi: 10.1007/s007020070062
43. Mantella RC, Butters MA, Amico JA, Mazumdar S, Rollman BL, Begley AE, et al. Salivary cortisol is associated with diagnosis and severity of late-life generalized anxiety disorder. Psychoneuroendocrinology (2008) 33(6):773–81. doi: 10.1016/j.psyneuen.2008.03.002
44. Yamada S, Yamauchi K, Yajima J, Hisadomi S, Maeda H, Toyomasu K, et al. Saliva level of free 3-methoxy-4-hydroxyphenylglycol (MHPG) as a biological index of anxiety disorders. Psychiatry Res (2000) 93(3):217–23. doi: 10.1016/S0165-1781(00)00118-9
45. Fries E, Hellhammer DH, Hellhammer J. Attenuation of the hypothalamic-pituitary-adrenal axis responsivity to the Trier Social Stress Test by the benzodiazepine alprazolam. Psychoneuroendocrinology (2006) 31(10):1278–88. doi: 10.1016/j.psyneuen.2006.09.009
46. Yang Y, Kozloski M. Sex Differences in Age Trajectories of Physiological Dysregulation: Inflammation, Metabolic Syndrome, and Allostatic Load. J Gerontol A Biol Sci Med Sci (2011) 5:493–500. doi: 10.1093/gerona/glr003
47. Sramek JJ, Murphy MF, Cutler NR. Sex differences in the psychopharmacological treatment of depression. Dialogues Clin Neurosci (2016) 18(4):447–57.
48. Verma CS, R Balhara YPS, Gupta. Gender differences in stress response: Role of developmental and biological determinants. Ind Psychiatry J (2011) 20(1): 4. doi: 10.4103/0972-6748.98407
49. Scévola L, Teitelbaum J, Oddo S, Centurión E, Loidl CF, Kochen S, et al. Psychiatric disorders in patients with psychogenic nonepileptic seizures and drug-resistant epilepsy: a study of an Argentine population. Epilepsy Behav (2013) 29(1):155–60. doi: 10.1016/j.yebeh.2013.07.012
50. Vinkers CH, Joëls M, Milaneschi Y, Kahn RS, Penninx BWJH, Boks MPM. Stress Exposure Across the Life Span Cumulatively Increases Depression Risk and Is Moderated By Neuroticism. Depress Anxiety (2014) 9 (2013):1–9. doi: 10.1002/da.22262
51. Malik S, Wong ND, Franklin SS, Kamath TV, Italien GJL, Pio JR, et al. Coronary Heart Disease , Cardiovascular Disease , and All Causes in United States Adults. Circulation (2004) 110(10):1245–51. doi: 10.1161/01.CIR.0000140677.20606.0E
52. Ahonen T, Saltevo J, Laakso M, Kautiainen H, Kumpusalo E, Vanhala M. Gender Differences Relating to Metabolic Syndrome and Proinflammation in Finnish Subjects with Elevated Blood Pressure. Mediators Inflamm (2009) 2009(959281):1–6. doi: 10.1155/2009/959281
53. Reul JMHM, de Kloet ER. Two Receptor Systems for Corticosterone in Rat Brain: Microdistribution and Differential Occupation. Endocrinology (1985) 117(6):2505–11. doi: 10.1210/endo-117-6-2505
54. Champagne DL, Bagot RC, van Hasselt F, Ramakers G, Meaney MJ, de Kloet ER, et al. Maternal Care and Hippocampal Plasticity: Evidence for Experience-Dependent Structural Plasticity, Altered Synaptic Functioning, and Differential Responsiveness to Glucocorticoids and Stress. J Neurosci (2008) 28(23):6037–45. doi: 10.1523/JNEUROSCI.0526-08.2008
55. Eriksson PS, Perfilieva E, Björk-Eriksson T, Alborn AM, Nordborg C, Peterson DA, et al. Neurogenesis in the adult human hippocampus. Nat Med (1998) 4(11):1313–7. doi: 10.1038/3305
56. Lucassen PJ, Heine VM, Muller MB, van der Beek EM, Wiegant VM, De Kloet ER, et al. Stress, depression and hippocampal apoptosis. CNS Neurol Disord Drug Targets (2006) 5(5):531–46. doi: 10.2174/187152706778559273
57. Sahay A, Drew MR, Hen R. Dentate gyrus neurogenesis and depression. Prog Brain Res (2007) 163:697–723. doi: 10.1016/S0079-6123(07)63038-6
58. Videbech P, Ravnkilde B. Hippocampal volume and depression: A meta-analysis of MRI studies. Am J Psychiatry (2004) 161(11):1957–66. doi: 10.1176/appi.ajp.161.11.1957
59. Samuels BA, Leonardo ED, Hen R. Hippocampal Subfields and Major Depressive Disorder Benjamin. Biol Psychiatry (2015) 77(3):210–1. doi: 10.1016/j.biopsych.2014.11.007
60. Sheline YI, Sanghavi M, Mintun MA, Gado MH. Depression duration but not age predicts hippocampal volume loss in medically healthy women with recurrent major depression. J Neurosci (1999) 19(12):5034–43. doi: 10.1523/JNEUROSCI.19-12-05034.1999
61. Treadway MT, Waskom ML, Dillon DG, Holmes AJ, Park MTM, Chakravarty MM, et al. Archival Report Illness Progression , Recent Stress , and Morphometry of Hippocampal Sub fi elds and Medial Prefrontal Cortex in Major Depression. Biol Psychiatry (2015) 77(3):285–94. doi: 10.1016/j.biopsych.2014.06.018
62. Starkman MN, Giordani B, Gebarski SS, Berent S, Schork MA, Schteingart DE. Decrease in cortisol reverses human hippocampal atrophy following treatment of Cushing's disease. Biol Psychiatry (1999) 46(12):1595–602. doi: 10.1016/S0006-3223(99)00203-6
63. Yehuda R. Advances in understanding neuroendocrine alterations in PTSD and their therapeutic implications. Ann NY Acad Sci (2006) 1071:137–66. doi: 10.1196/annals.1364.012
64. D'Alessio L, Konopka H, Solís P, Scévola L, Lima MF, Nuñez C, et al. Depression and Temporal Lobe Epilepsy: Expression Pattern of Calbindin Immunoreactivity in Hippocampal Dentate Gyrus of Patients Who Underwent Epilepsy Surgery with and without Comorbid Depression. Behav Neurol (2019) 2019:1–12. doi: 10.1155/2019/7396793
65. D'Alessio L, Konopka H, Escobar E, Acuña A, Oddo S, Solís P, et al. Dentate gyrus expression of nestin-immunoreactivity in patients with drug-resistant temporal lobe epilepsy and hippocampal sclerosis. Seizure (2015) 27:75–9. doi: 10.1016/j.seizure.2015.02.008
66. Bonaguidi MA, Wheeler MA, Shapiro JS, Stadel RP, Sun GJ, Ming GL, et al. In vivo clonal analysis reveals self-renewing and multipotent adult neural stem cell characteristics. Cell (2011) 145(7):1142–55. doi: 10.1016/j.cell.2011.05.024
67. Lugert S, Basak O, Knuckles P, Haussler U, Fabel K, Götz M, et al. Quiescent and active hippocampal neural stem cells with distinct morphologies respond selectively to physiological and pathological stimuli and aging. Cell Stem Cell (2010) 6(5):445–56. doi: 10.1016/j.stem.2010.03.017
68. Anacker C, Hen R. Adult hippocampal neurogenesis and cognitive flexibility-linking memory and mood. Nat Publ Gr (2017) 18:335–46. doi: 10.1038/nrn.2017.45
69. Chen H, Lombès M, Le Menuet D. Glucocorticoid receptor represses brain- derived neurotrophic factor expression in neuron-like cells. Mol Brain (2017) 10(12):1–16. doi: 10.1186/s13041-017-0295-x
70. Taliaz D, Stall N, Dar D, Zangen A. Knockdown of brain-derived neurotrophic factor in specific brain sites precipitates behaviors associated with depression and reduces neurogenesis. Mol Psychiatry (2010) 15(1):80–92. doi: 10.1038/mp.2009.67
71. Lakshminarasimhan H, Chattarji S. Stress leads to contrasting effects on the levels of brain derived neurotrophic factor in the hippocampus and amygdala. PloS One (2012) 7(1):1–6. doi: 10.1371/journal.pone.0030481
72. Malberg JE, Eisch AJ, Nestler EJ, Duman RS. Chronic antidepressant treatment increases neurogenesis in adult rat hippocampus. J Neurosci (2000) 20(24):9104–10. doi: 10.1523/JNEUROSCI.20-24-09104.2000
73. Czéh B, Michaelis T, Watanabe T, Frahm J, de Biurrun G, van Kampen M, et al. Stress-induced changes in cerebral metabolites, hippocampal volume, and cell proliferation are prevented by antidepressant treatment with tianeptine. Proc Natl Acad Sci U S A (2001) 98(22):12796–801. doi: 10.1073/pnas.211427898
74. Lucassen PJ AE, Stumpel MW, Wang Q. Decreased numbers of progenitor cells but no response to antidepressant drugs in the hippocampus of elderly depressed patients. Neuropharmacology (2010) 58:940–9. doi: 10.1016/j.neuropharm.2010.01.012
75. Warner-Schmidt JL, Duman RS. Hippocampal neurogenesis: Opposing effects of stress and antidepressant treatment. Hippocampus (2006) 16(3):239–49. doi: 10.1002/hipo.20156
76. Manji BHK, Duman RS. Impairments of neuroplasticity and cellular resilience in severe mood disorders: Implications for the development of novel therapeutics. Spring (2001) 35(2):5–49.
77. Anacker C, Zunszain PA, Cattaneo A, Carvalho LA, Garabedian MJ, Thuret S, et al. Antidepressants increase human hippocampal neurogenesis by activating the glucocorticoid receptor. Mol Psychiatry (2011) 16:738. doi: 10.1038/mp.2011.26
78. Pollak DD, Monje FJ, Zuckerman L, Denny CA, Drew MR, Kandel ER. An Animal Model of a Behavioral Intervention for Depression. Neuron (2008) 60(1):149–61. doi: 10.1016/j.neuron.2008.07.041
79. Yamamoto KI, Shinba T, Yoshii M. Psychiatric symptoms of noradrenergic dysfunction: A pathophysiological view. Psychiatry Clin Neurosci (2014) 68(1):1–20. doi: 10.1111/pcn.12126
80. Stratton JR, Halter JB. Effect of a benzodiazepine (alprazolam) on plasma epinephrine and norepinephrine levels during exercise stress. Am J Cardiol (1985) 56:136–9. doi: 10.1016/0002-9149(85)90582-X
81. Van Den Berg F, Tulen JHM, Boomsma F, Noten JBGM, Moleman P, Pepplinkhuizen L. Effects of alprazolam and lorazepam on catecholaminergic and cardiovascular activity during supine rest, mental load and orthostatic challenge. Psychopharmacol (Berl) (1996) 128:21–30. doi: 10.1007/s002130050105
82. Tan KR LC, Rudolph U. Hooke don benzodiazepines: GABAA receptor subtypes and addiction. Trends Neurosci (2011) 34:188–97. doi: 10.1016/j.tins.2011.01.004
83. Curtis GC, Abelson JL, Gold PW. Adrenocorticotropic hormone and cortisol responses to corticotropin-releasing hormone: changes in panic disorder and effects of alprazolam treatment. Biol Psychiatry (1997) 41(1):76–85. doi: 10.1016/S0006-3223(95)00578-1
84. Zemishlany Z DM, McQueeney R, Gabriel SM. Neuroendocrine and monoaminergic responses to acute administration of alprazolam in normal subjects. Neuropsychobiology (1990) 23(3):124–8. doi: 10.1159/000119437
85. Yilmaz S, Pekdemir M, Tural U, Uygun M. Comparison of alprazolam versus captopril in high blood pressure: a randomized controlled trial. Blood Press (2011) 20(4):239–43. doi: 10.3109/08037051.2011.553934
86. Hoge EA, Ivkovic A, Fricchione GL. Generalized anxiety disorder: diagnosis and treatment. BMJ (2012) 345:e7500. doi: 10.1136/bmj.e7500
87. Barker MJ, Greenwood KM, Jackson M, Crowe SF. Persistence of cognitive effects after withdrawal from long-term benzodiazepine use: a meta-analysis. Arch Clin Neuropsychol (2004) 19(3):437–54. doi: 10.1016/S0887-6177(03)00096-9
88. Billioti S, Gage D, Bégaud B, Bazin F. Benzodiazepine use and risk of dementia: prospective population based study. BMJ (2012) 345:e6231–e 6231. doi: 10.1136/bmj.e6231
89. Soria CA, Remedi C, D'Alessio L, Roldán EJA. Semantic and Phonemic Verbal Fluency Performance in Patients with General Anxiety Disorders and Allostatic Load under Alprazolam Treatment. Open J Psychiatry (2019) 9(2):138–52. doi: 10.4236/ojpsych.2019.92011
90. Brown J, Cooper-Kuhn CM, Kempermann G, Van Praag H, Winkler J, Gage FH, et al. Enriched environment and physical activity stimulate hippocampal but not olfactory bulb neurogenesis. Eur J Neurosci (2003) 17(10):2042–6. doi: 10.1046/j.1460-9568.2003.02647.x
91. Vaynman S, Ying Z, Gomez-Pinilla F. Hippocampal BDNF mediates the efficacy of exercise on synaptic plasticity and cognition. Eur J Neurosci (2004) 20(10):2580–90. doi: 10.1111/j.1460-9568.2004.03720.x
92. Uysal N, Kiray M, Sisman AR, Camsari UM, Gencoglu C, Baykara B, et al. Effects of voluntary and involuntary exercise on cognitive functions, and VEGF and BDNF levels in adolescent rats. Biotech Histochem (2015) 90(1):55–68. doi: 10.3109/10520295.2014.946968
93. Russo E, Citraro R, Scicchitano F, Urzino A, Marra R, Rispoli V, et al. Vigabatrin has antiepileptogenic and antidepressant effects in an animal model of epilepsy and depression comorbidity. Behav Brain Res (2011) 225, 1:373–6. doi: 10.1016/j.bbr.2011.07.030
94. Baj G, D'Alessandro V, Musazzi L, Mallei A, Sartori CR, Sciancalepore M, et al. Physical exercise and antidepressants enhance BDNF targeting in hippocampal CA3 dendrites: Further evidence of a spatial code for BDNF splice variants. Neuropsychopharmacology (2012) 37(7):1600–11. doi: 10.1038/npp.2012.5
95. Duman RS, Aghajanian GK. Synaptic dysfunction in depression: Potential therapeutic targets. Sci (80-. ). (2012) 338(6103):68–72. doi: 10.1126/science.1222939
96. Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A (2011) 108(7):3017–22. doi: 10.1073/pnas.1015950108
97. Toups MSP, Greer TL, Kurian BT, Grannemann BD, Carmody TJ, Huebinger R, et al. Effects of serum Brain Derived Neurotrophic Factor on exercise augmentation treatment of depression. J Psychiatr Res (2011) 45(10):1301–6. doi: 10.1016/j.jpsychires.2011.05.002
98. de M Coelho FG, Gobbi S, Andreatto CAA, Corazza DI, Pedroso RV, Santos-Galduróz RF. Physical exercise modulates peripheral levels of brain-derived neurotrophic factor (BDNF): A systematic review of experimental studies in the elderly. Arch Gerontol Geriatr (2013) 56(1):10–5. doi: 10.1016/j.archger.2012.06.003
99. Pascoe M, Bailey AP, Craike M, Carter T, Patten R, Stepto N, et al. Physical activity and exercise in youth mental health promotion: A scoping review. BMJ Open Sport Exerc Med (2020) 6(1):1–11. doi: 10.1136/bmjsem-2019-000677
100. Harvey SB, Overland S, Hatch SL, Wessely S, Mykletun A, Hotopf M. Exercise and the prevention of depression: Results of the HUNT cohort study. Am J Psychiatry (2018) 175(1):28–36. doi: 10.1176/appi.ajp.2017.16111223
101. Bennie JA, De Cocker K, Biddle SJH, Teychenne MJ. Joint and dose-dependent associations between aerobic and muscle-strengthening activity with depression: A cross-sectional study of 1.48 million adults between 2011 and 2017. Depress Anxiety (2020) 37(2):166–78. doi: 10.1002/da.22986
102. Fernandez-Montero A, Moreno-Galarraga L, Sánchez-Villegas A, Lahortiga-Ramos F, Ruiz-Canela M, Martínez-González MÁ., et al. Dimensions of leisure-time physical activity and risk of depression in the ‘seguimiento Universidad de Navarra' (SUN) prospective cohort. BMC Psychiatry (2020) 20(1):1–9. doi: 10.1186/s12888-020-02549-5
103. Schuch FB, Vasconcelos-Moreno MP, Borowsky C, Fleck MP. Exercise and severe depression: Preliminary results of an add-on study. J Affect Disord (2011) 133(3):615–8. doi: 10.1016/j.jad.2011.04.030
104. Herbsleb M, Schumann A, Lehmann L, Gabriel HHW, Bär KJ. Cardio-Respiratory Fitness and Autonomic Function in Patients with Major Depressive Disorder. Front Psychiatry (2020) 10:1–10. doi: 10.3389/fpsyt.2019.00980
105. Kerling A, Tegtbur U, Gützlaff E, Kück M, Borchert L, Ates Z, et al. Effects of adjunctive exercise on physiological and psychological parameters in depression: A randomized pilot trial. J Affect Disord (2015) 177:1–6. doi: 10.1016/j.jad.2015.01.006
106. Valentine RJ, McAuley E, Vieira VJ, Baynard T, Hu L, Evans EM, et al. Sex differences in the relationship between obesity, C-reactive protein, physical activity, depression, sleep quality and fatigue in older adults. Brain Behav Immun (2009) 23(5):643–8. doi: 10.1016/j.bbi.2008.12.003
107. Gothe NP, Keswani RK, McAuley E. Yoga practice improves executive function by attenuating stress levels. Biol Psychol (2016) 121:109–16. doi: 10.1016/j.biopsycho.2016.10.010
108. West J, Otte C, Geher K, Johnson J, Mohr DC. Effects of Hatha yoga and African dance on perceived stress, affect, and salivary cortisol. Ann Behav Med (2004) 28(2):114–8. doi: 10.1207/s15324796abm2802_6
109. Philippot A, Meerschaut A, Danneaux L, Smal G, Bleyenheuft Y, De Volder AG. Impact of physical exercise on symptoms of depression and anxiety in pre-adolescents: A pilot randomized trial. Front Psychol (2019) 10:1–11. doi: 10.3389/fpsyg.2019.01820
110. Schuch FB, Stubbs B, Meyer J, Heissel A, Zech P, Vancampfort D, et al. Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depress Anxiety (2019) 36(9):846–58. doi: 10.1002/da.22915
111. Bernard P, Romain AJ, Caudroit J, Chevance G, Carayol M, Gourlan M, et al. Cognitive behavior therapy combined with exercise for adults with chronic diseases: Systematic review and meta-analysis. Heal Psychol (2018) 37(5):433–50. doi: 10.1037/hea0000578
112. Valentine RJ, Vieira VJ, Woods JA, Evans EM. Stronger relationship between central adiposity and C-reactive protein in older women than men. Menopause (2009) 16(1):84–9. doi: 10.1097/gme.0b013e31817fcb8f
113. Villemure C, Čeko M, Cotton VA, Catherine Bushnell M. Neuroprotective effects of yoga practice: Age-, experience-, and frequency-dependent plasticity. Front Hum Neurosci (2015) 9(281):1–12. doi: 10.3389/fnhum.2015.00281
114. Newham JJ, Wittkowski A, Hurley J, Aplin JD, Westwood M. Effects of antenatal yoga on maternal anxiety and depression: A randomized controlled trial. Depress Anxiety (2014) 31(8):631–40. doi: 10.1002/da.22268
115. Lavey R, Sherman T, Mueser KT, Osborne DD, Currier M, Wolfe R. The Effects of Yoga on Mood in Psychiatric Inpatients. Psychiatr Rehabil J (2005) 28(4):399–402. doi: 10.2975/28.2005.399.402
116. Uebelacker LA, Tremont G, Epstein-Lubow G, Gaudiano BA, Gillette T, Kalibatseva Z, et al. Open trial of Vinyasa yoga for persistently depressed individuals: Evidence of feasibility and acceptability. Behav Modif (2010) 34(3):247–64. doi: 10.1177/0145445510368845
117. Cramer H, Anheyer D, Lauche R, Dobos G. A systematic review of yoga for major depressive disorder. J Affect Disord (2017) 213(2016):70–7. doi: 10.1016/j.jad.2017.02.006
118. Streeter CC, Gerbarg PL, Brown RP, Scott TM, Nielsen GH, Owen L, et al. Thalamic Gamma Aminobutyric Acid Level Changes in Major Depressive Disorder After a 12-Week Iyengar Yoga and Coherent Breathing Intervention. J Altern Complement Med (2020) 26(3):190–7. doi: 10.1089/acm.2019.0234
119. Ross A, Thomas S. The health benefits of yoga and exercise: A review of comparison studies. J Altern Complement Med (2010) 16(1):3–12. doi: 10.1089/acm.2009.0044
120. Kuyken W, Warren FC, Taylor RS, Whalley B, Crane C, Bondolfi G, et al. Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse an individual patient data meta-analysis from randomized trials. JAMA Psychiatry (2016) 73(6):565–74. doi: 10.1001/jamapsychiatry.2016.0076
121. Korman GP, Garay CJ. El modelo de Terapia Cognitiva Basada en la Conciencia Plena (mindfulness ). Ecoe (2012) XXI:5–13.
122. Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: A systematic review of the research evidence. Br J Sports Med (2005) 39(12):884–91. doi: 10.1136/bjsm.2005.018069
123. Shapiro SL, Brown KW, Biegel GM. Teaching self-care to caregivers: Effects of mindfulness-based stress reduction on the mental health of therapists in training. Train Educ Prof Psychol (2007) 1(2):105–15. doi: 10.1037/1931-3918.1.2.105
124. Oken BS, Zajdel D, Kishiyama S, Flegal K, Dehen C, Haas M, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: Effects on cognition and quality of life. Altern Ther Health Med (2006) 12(1):40–7.
125. Lazar SW, Bush G, Gollub RL, Fricchione GL, Khalsa G, Benson H. Functional brain mapping of the relaxation response and meditation. Neuroreport (2000) 11(7):1581–5. doi: 10.1097/00001756-200005150-00042
126. Hölzel BK, Lazar SW, Gard T, Schuman-Olivier Z, Vago DR, Ott U. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect Psychol Sci (2011) 6(6):537–59. doi: 10.1177/1745691611419671
Keywords: chronic stress, neuroplasticity, neurogenesis, hippocampus, cortisol, noradrenaline, antidepressants, benzodiazepines
Citation: D'Alessio L, Korman GP, Sarudiansky M, Guelman LR, Scévola L, Pastore A, Obregón A and Roldán EJA (2020) Reducing Allostatic Load in Depression and Anxiety Disorders: Physical Activity and Yoga Practice as Add-On Therapies. Front. Psychiatry 11:501. doi: 10.3389/fpsyt.2020.00501
Received: 18 December 2019; Accepted: 18 May 2020;
Published: 04 June 2020.
Edited by:
Gianluca Serafini, San Martino Hospital (IRCCS), ItalyReviewed by:
Zoltan Sarnyai, James Cook University, AustraliaNuno Dinis Alves, Columbia University, United States
Copyright © 2020 D'Alessio, Korman, Sarudiansky, Guelman, Scévola, Pastore, Obregón and Roldán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luciana D'Alessio, bHVjaWFuYWRAY29uaWNldC5nb3YuYXI=; bHVsYWRhbGVzc2lvQGdtYWlsLmNvbQ==