 Natalia C. Rufino1*
Natalia C. Rufino1* Bojan Mirkovic2
Bojan Mirkovic2 Angèle Consoli3,4Hugues Pellerin3
Angèle Consoli3,4Hugues Pellerin3 Juliana P. M. Santos1
Juliana P. M. Santos1 Thiago M. Fidalgo1
Thiago M. Fidalgo1 Priscille Gerardin2Dartiu X. Silveira1†
Priscille Gerardin2Dartiu X. Silveira1† David Cohen3,4,5†
David Cohen3,4,5†- 1Department of Psychiatry, Universidade Federal de São Paulo, São Paulo, Brazil
- 2Service de Psychiatrie de l’Enfant et de l’Adolescent, CHU Charles Nicolle/CH Le Rouvray, Normandie Université, Rouen, France
- 3Département de Psychiatrie de l’Enfant et de l’Adolescent, AP-HP, Groupe Hospitalier Pitié-Salpêtrière, Paris, France
- 4GRC-15, Approche dimensionnelle des épisodes psychotiques de l’enfant et de l’adolescent, Faculté de Médecine, UPMC, Sorbonne Université, Paris, France
- 5CNRS UMR 7222 “Institut des Systèmes Intelligents et Robotiques”, Sorbonne Université, Paris, France
Background: Suicide is the second most common cause of preventable mortality among Brazilian and French adolescents. The aim of the current study was to compare the main risk and protective factors associated with a suicide attempt (SA) and to highlight differences based on geographical characteristics.
Method: We compared a Brazilian sample (N = 45) of adolescents admitted to the emergency room of a public hospital in São Paulo for SA to a French sample (N = 320) of adolescents hospitalized for SA across 5 paediatric departments. Then, we ran several multivariate models to examine how each selected variable was related to geographic origin and to the other selected variables linked to geographic origin.
Results: The two samples presented no significant differences regarding gender, age or schooling. Both samples had high rates of depressive disorders, anxiety disorders, substance use, disruptive disorders, borderline psychopathology, and lifetime SAs. However, the Brazilian sample presented significantly higher levels of psychopathology and had more insecure attachment relationships (fearful and detached), whereas the French sample had a more secure attachment style. Brazilian adolescents had more recourse to spiritual beliefs and spiritual support, whereas the French adolescents had higher scores on the Reasons for Living Inventory and used more help-seeking strategies from their social network, mainly close friends. Multivariate models showed that two productive coping strategies (seeking spiritual support and social action) and the dependence score were significantly associated with membership in the Brazilian cohort, whereas a secure attachment style and depression severity (evaluated by the Beck Depression Inventory) were significantly associated with membership in the French cohort.
Conclusion: Despite presenting similar psychopathologies, Brazilian adolescents presented a more insecure attachment style and used the religious kind of coping more commonly than their French counterparts. We hypothesize that religion may compensate for the social vulnerabilities present in a middle-income country such as Brazil. More transcultural studies may help to elucidate this phenomenon.
Introduction
Suicide is the second leading cause of death in youth (10 to 24 years) worldwide (1) and a total of 78% of suicides occur in low- and middle-income countries (2). A recent meta-analysis of 686,672 children and adolescents found that the aggregate lifetime and 12-month prevalences of suicide attempts were 6% and 4.5%, respectively (3). The aggregate lifetime and 12-month prevalences of suicidal plans were 9.9% and 7.5%, respectively. The aggregate lifetime and 12-month prevalences of suicidal ideation were 18% and 14.2%, respectively.
In Brazil, suicide is the fourth leading cause of death in young people between the ages of 15 and 29 years old (4). Epidemiological data generated from the Mortality Information System (SIM) of the Brazilian Ministry of Health in 2017 found a suicide rate of 1.1/100.000 among children and adolescents (between the ages of 1 and 19 years old). The prevalence of suicide attempts (SA) in adolescents ranges from 5.9% to 10% (5, 6). Even if Brazil has relatively low suicide rates among young people (ranked 93rd out of 195 countries and territories) (2), there was a 13% increase in the nationwide adolescent (10 to 19 years old) suicide rate from 2006 to 2015 and a 27% increase in the São Paulo metropolitan area (6). In France, suicide is the second leading cause of death among 15- to 24-year-olds. According to the latest national data available, the suicide rate for adolescents aged 15-19 years old is 4.1 per 100,000 inhabitants (7). In 2016, European data reported an average suicide rate of 4.29 per 100,000 inhabitants for subjects aged 15 to 19 years old among the 28 EU countries, with a significantly higher rate among boys than among girls (2.1 vs. 5.9 per 100,000) (8).
Suicidal behavior is considered to result from multiple biopsychosocial interactions (9). On the one hand, an individual’s neurobiological (10), genetic (11), cognitive and emotional (12, 13) characteristics may affect suicidal behavior; on the other hand, an individual’s environment in the broad sense of the term, namely, situations regarding adversity (14), family and social relationships (15, 16) life time trajectory, culture, or spirituality (17), may affect suicidal behavior. In addition to the “opposition” of biological vs. environmental factors, several authors have proposed the modelling suicide behavior risk by the “combination” of time-related risk and protective factors (18). Protective factors are attributes of people, environments, situations and events that appear to moderate psychopathological predictions based on individual risk status (19, 20). Recent studies have highlighted the role of protective factors in the assessment of suicide risk, namely, productive coping skills, reasons for living, social support, or spirituality (18, 21–23). Other protective factors include religion (24, 25) and the resolution of participants (26).
In an integrative model, the evaluation of risk factors remains crucial because a factor is only protective insofar as it moderates the impact of the risk factor(s). For a given individual, protection and risk factors interact in an inversely proportional manner. Thus, when faced with a risk situation, the individual will produce a more positive response if the “protection” pole is dominant and a more negative response if the “vulnerability” pole is dominant (18). In addition, the role of cultural references for interpreting protective factors is matter of debate and has not been studied in detail, as it requires large studies in different cultural settings. To date, only geographical variations have been described at a macro level (e.g., more suicides in rural areas (vs. urban areas) of China (27); a higher proportion of suicides in America and Europe (vs. Asia) meeting criteria for psychiatric disorders (1). Cultural and socioeconomic aspects related to geographical location also play an interchangeable role, as they influence both risk and protective factors. Being part of an ethnic minority is described as a risk factor (28–30), and socioeconomic status could be a protective factor—as it is related to a higher educational level and greater social support (18, 18)—or a risk factor (30, 31) for adolescents who exhibit SB. It is also important to consider that socioeconomic barriers and cultural characteristics could have a considerable impact on adolescents’ treatment, especially those with suicidal risk behavior (32). There are differences in risk factors for suicide between adults and adolescents. Adolescents who attempted suicide have been shown to have comparatively more relationship problems but fewer medical problems than adults (33).
Studies of the prevalence of child and adolescent psychiatric disorders in Brazil have reported similar levels of psychopathology as other international studies but slightly higher levels than findings from developed countries, which corroborates previous epidemiological findings suggesting the universality of psychiatric disorders in children and adolescents across cultures (34, 35). Risk and protective factors associated with SB have been well established in studies from developed countries, but these factors remain underexplored in low- and middle-income countries. Although adolescent suicidal behaviors vary across countries, there is a consistent set of risk factors for suicidal behaviors across all regions and most countries, and little is understood about protective factors and their moderating effects on suicide risk in adolescence (36). In 2002, an intervention study on suicidal behavior—The Suicide Prevention—Multisite Intervention Study on Suicidal Behaviors (SUPRE-MISS)—was initiated by the World Health Organization. The survey was conducted in seven culturally diverse low- and middle-income countries around the world, including one site in Brazil, and provided valuable information regarding socioeconomical and cultural characteristics on SB among adults (37–39), including the role of subjective religiosity (25) and the impact of brief interventions in the emergency department (39) as a protective factor in the Brazilian sample. A process of seeking relief in new religious affiliations that is probably occurring in Brazilian society among subgroups with previous minor psychiatric symptoms has already been described by Dalgalarrondo et al. (40).
There is still much to explore regarding protective factors that are related to cultural and socioeconomic aspects, such as religiosity, coping styles, reasons for living, attachment and stressful life events, especially in the Brazilian adolescent population.
In the current article, we propose a comparison between a Brazilian clinical population of adolescents with suicidal behaviors with a French clinical sample. We aim to identify more well-established associated risk and protective factors by using the same standardized tools to evaluate these samples.
We hypothesized that factors related to the psychopathology of adolescent suicide behaviors (mood disorders, conduct disorders, borderline psychopathology, substance abuse, impulsivity, hopelessness, and lifetime suicide attempt) would be common to both populations, whereas some protective factors (reason for living, spirituality, coping skills or attachment style) would be different based on geographical origin.
Method
Participants
The study was conducted in two countries. The inclusion criteria were similar in both samples and were based on WHO definitions and the most recent classifications of suicidal behaviors. We considered the main inclusion criterion to be showing “a suicide attempt” only if the intent to die was manifested (41). Subjects committing nonsuicidal self-injury without the intent to die were excluded. Other inclusion criteria included being an adolescent aged 12-18 years, being able to understand the purpose of the study, and the absence of prominent mental retardation or organic brain damage. Participants were informed that their answers would remain confidential, and written informed consent for study participation was obtained from participants as well as both parents or guardians.
The French sample included 320 adolescents aged 12 to 18 who were admitted to 1 of 4 paediatric departments following a SA between January 2011 and December 2014 -detailed protocol in previous paper (42). For the purpose of this transcultural study, we recruited a Brazilian sample using identical inclusion and exclusion criteria and a similar assessment protocol. Brazil is a large country that is characterized by high social disparities between regions. São Paulo, the country’s financial centre, is the sixth largest metropolitan area in the world, with a population of over 12 million habitants.
In Brazil, unlike in France, access to mental health care appear to be hampered by multiple socio-cultural and economic factors (43). The Unified Health System (Sistema Único de Saúde), conceived in the late 1980s has enabled substantial progress towards Universal Health Coverage in Brazil. However, structural weakness, economic and political crises and austerity policies have limited its growth and sustainability and outcomes (44).
Therefore, in Brazil, most adolescents are not hospitalized after a SA. Second, few public facilities are associated with a research team. Consequently, for the São Paulo centre, we chose a public centre associated with a research team to avoid socioeconomic biases and to avoid patients who lacked access to free care. From April 2016 to November 2017, 61 adolescents were recruited to participate in this study. Eleven refused to participate, and 4 withdrew their consent during the evaluation process. In total, 45 adolescents aged 11 to 18 were admitted to the emergency department of a university hospital in São Paulo, Brazil, after an SA and were included in the study.
Procedures
For the French sample, assessments were performed during a 1-week inpatient stay. The procedure has been detailed in Mirkovic et al. (42). For the Brazilian sample, access to care is different from that in France, and the inpatient setting for adolescent psychiatric care is more limited. Consequently, Brazilian adolescents could not be assessed in the same way. On admission to the emergency department, participation in the study was systematically proposed to all adolescents who met the inclusion criteria by the psychiatrist in charge. After obtaining the consent of the adolescent and their parents, the research team contacted the patient and his/her family. The evaluation was conducted within 1 month of the visit to the emergency department by psychiatrists trained in conducting the evaluation. To avoid tiring the patients, the evaluation was carried out over multiple interview sessions. The investigators were psychiatrists with more than 3 years of clinical experience. All the evaluation reports were analyzed individually by our study group, and final diagnoses were made after consensus among the group.
Measures
In addition to sociodemographic data, we explored axis I psychiatric disorders using the Scale of Mood Disorders and Schizophrenia for Children and Adolescents of School Age, Current and Past Episodes version (Kiddie-SADS-PL) (45). The interview protocol was translated into French by Mouren-Siméoni et al. (46) and into Portuguese by Brasil HHA et al. (47). The Columbia Suicide Severity Rating Scale (C-SSRS) (41) was used to quantify the severity of suicidal ideation and behavior. This scale allows for the assessment of suicidal behavior and suicidal intentionality. It was completed by the clinician based on the clinical interviews conducted with the adolescents. The Beck Depression Inventory, Second Edition (48) was used to evaluate the severity of depression symptoms. It comprises 21 items rated on a 4-point scale. Scores range from 0 to 63. The Beck Hopelessness Scale (49), a self-report scale designed to measure levels of hopelessness, is composed of 20 true-false items. The Eysenck Questionnaire (50) was used to rate impulsivity. This 24-item self-administered questionnaire was validated for young people aged 8 to 17.
The Ab-Diagnostic Interview for Borderline Patients (Ab-DIB) is a DIB-R–derived self-report to assess impulsiveness among adolescents as well as the effect and cognitive components of the borderline construct (51, 52). Substance use and misuse were assessed with the Dependence Questionnaire for Adolescents (DEP-ADO) (53).
We also explored several variables we hypothesized as potential moderators of suicide risk or relapse (18). 1) We used the Adolescent Coping Scale (ACS), which was designed and validated for adolescents aged 12 to 18. The ACS comprises 77 items grouped into 18 subscales representing 18 specific coping strategies (54). 2) We used the Spirituality Scale, which assessed the broad construct of spirituality and was developed by Delaney et al. (55). This scale goes beyond religious practices and assessed 3 key relational aspects: connection with self (personal), with others (interpersonal), and with the divine (transpersonal) (55). 3) We used the Reasons for Living Inventory for Adolescents (RFL-A), a 32-item self-report inventory (56). 4) We used the Life Events Questionnaire for Adolescents, a 39-item self-questionnaire developed by Newcomb et al. (57). 5) We used the Relationship Scales Questionnaire (RSQ) (58) to assess attachment styles.
All the questionnaires that were not available in Brazilian Portuguese (the Adolescent Coping Scale (ACS), the Spirituality Scale, the Reasons for Living Inventory, the Life Events Questionnaire for Adolescents, the Eysenck Questionnaire, the Ab-DIB, the Relationship Style Questionnaire (RSQ-ADO) and the DEP-ADO Detection of alcohol and drug problems in adolescents) were back translated by two Brazilian psychiatrists who were fluent in both languages and reviewed by a French native speaker who was also fluent in Portuguese.
Ethics
Ethics approval was obtained for this study from CHU Charles Nicolle, France (2010 A00 330—39) and from the Group Ethics and Medical Research Committee of Sao Paulo University, Brazil (706939). Each participant gave their written informed consent prior to participation.
Statistical Analysis
Statistical analyses were performed using R 3.4.0, and p-values less than 0.05 were considered significant. The goal of the analyses was to determine the relationship between geographic origin (Brazilian vs. French) and all sociodemographic and psychopathological variables. We started with univariate analyses to compare the two groups. All quantitative variables were described using the mean and standard deviation or frequencies and percentages. We used Student t-tests or Wilcoxon rank sum tests to compare normally distributed and nonnormally distributed quantitative variables, respectively, and we used Chi-squared or Fisher’s exact tests to compare normally distributed and nonnormally distributed qualitative variables, respectively.
Then, we aimed to compare French and Brazilian samples using multivariate analyses to determine the most robust variables. We selected the variables of interest based on the univariate analyses. We used a rather inclusive threshold (p < 0.2) to allow exploration of subtle effects (see Table 2 below). The 12 variables that were included in the multivariate analyses were secure attachment style total score; Beck depression total score; reasons for living inventory total score; dependence total score; coping-social action; seeking spiritual support; self-discovery; lifetime suicide attempts; life events (autonomy); borderline disorder; anxiety disorders. Multivariate models are usually performed to assess a causal relationship. Here, the predictor variable to be explored was the geographic origin. However, we did not test the hypothesis that living in Brazil (or France) is a causal factor in being severely depressed or having attempted suicide several times, as this is not a plausible hypothesis.
Therefore, we explored each relevant clinical variable using a multivariate model as follows:
By doing so, we were able to calculate the effect of the geographic origin on a given clinical variable while taking into account the effects of other clinical variables. For example, we used the following formula for secure attachment style total score:
The following formula was used for depression:
In total, we ran 12 multivariate models to examine how each selected variable was related to geographic origin and to the other variables linked to geographic origin based on our univariate comparison. We used either linear regression with bootstrap resampling (boot package, R = 10,000) or logistic regression, depending on the nature of the explained variable. Missing values were imputed using a nonparametric random forest method (missForest package). Input variables were model variables, and some auxiliary variables were chosen for their correlation with model variables. In the Results section, we only present the effect of geographic origin on the selected variable (estimate, 95% confidence intervals; standard error, and p) for each model.
Results
The average age among Brazilian adolescents and French adolescents was 14.42 (SD 1.7) years old and 14.73 (SD 1.29) years old, respectively. There were more boys in the Brazilian sample (71.1% girls vs. 28.9% boys), while there were more girls in the French sample (81.1% girls vs. 16.9% boys). Regarding differences in parents’ educational levels between the French and the Brazilians, there was a significant difference, with French parents reporting higher educational levels than Brazilian parents (Table 1).
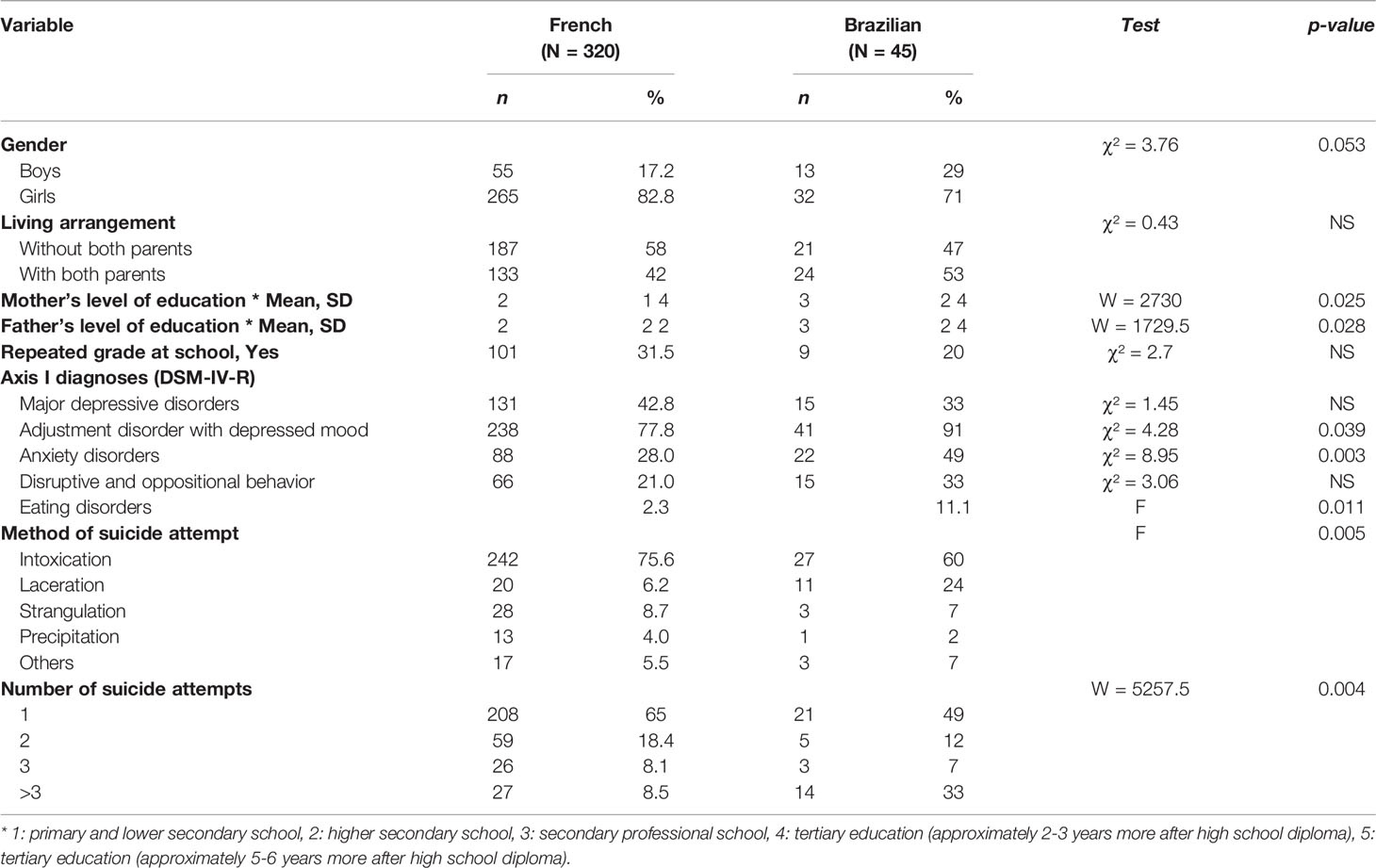
Table 1 Sociodemographic and clinical characteristics.
Univariate Analyses
Brazilian adolescents presented more present adjustment disorders with depressed mood (41% vs. 33%, p=0.039), present anxiety disorders (48.9% vs. 27%; p = 0.003), and present eating disorders (11.1% vs. 2.3%; p = 0.011). No differences were found for present major depressive disorders and present disruptive and oppositional behavior (Table 1). Brazilian adolescents had significantly higher scores of BDI-II depressive symptoms (p < 0.001), BHS hopelessness (p = 0.038), and borderline psychopathology (93.2% vs. 71.6%; p = 0.002) compared to French adolescents (Table 2).
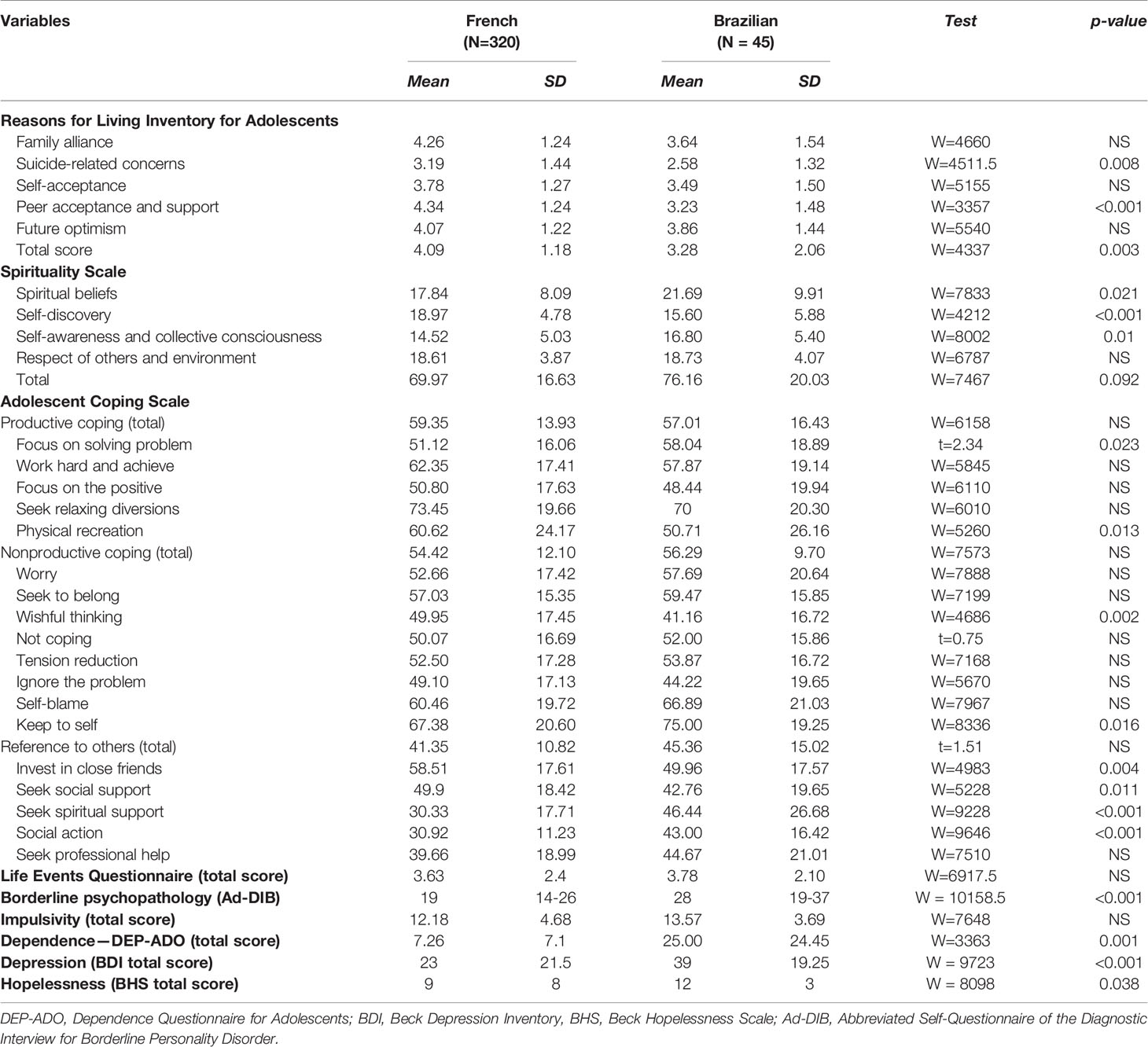
Table 2 Dimensional characteristics.
Regarding suicidal behaviors (C-SSRS), more Brazilian adolescents had a history of SA than their French counterparts [3.07 (SD 2.91) vs. 1.6 (SD 1.12), W = 861, p = 0.001]. Brazilian adolescents also presented more preceding behaviors, such as actively seeking the means to commit suicide or writing a letter to explain their suicide (χ² = 29.68, p < 0.001). The French sample had more definitive intentions than the Brazilian sample (χ² = 7.16, p = 0.007), while the Brazilian adolescents were characterized by more cases of deliberate self-injury (80% vs. 44%, χ² = 20.12, p < 0.001).
Both Brazilian and French adolescents had a detached relationship style (as measured by the RSQ), but Brazilians were significantly more detached (W = 8034.5, p < 0.001), less secure (W = 1899, p < 0.001), and more worried (W = 7762, p = 0.001) than French adolescents.
Regarding drug misuse (as measured by the DEP-ADO), Brazilian adolescents had significantly higher scores for alcohol and cannabis use (W = 3464, p < 0.001), whereas French adolescents scored higher on the use of other drugs (W = 2183.5, p = 0.02). Additionally, Brazilian drug users reported more consequences and overall more punctuation (W = 5423, p = 0.007).
Regarding life events, we assessed several domains: family, illness, sexuality, autonomy, deviance, and relocation. Brazilian adolescents reported significantly more autonomous life events (W = 811, p <0.001). Autonomous experiences, such as gaining a new group of friends or starting to make your own money, are usually perceived as positive and tend to increase with age in adolescence. We found no difference in the total score of life events between the two samples (W = 6917.5, p = 0.348).
Regarding coping skills (as measured by the ACS), Brazilian adolescents made greater use of “focusing on solving problems” (p = 0.023), “social action” (p < 0.001), “keeping to self” (p = 0.016) and “seeking spiritual support” (p < 0.001) strategies, while French adolescents scored significantly higher on “social support” (p = 0.011), “investing in close friends” (p = 0.004), “wishful thinking” (p = 0.002), and “physical recreation” (p = 0.013) items (Table 2).
French adolescents scored higher on the reasons for living inventory. Regarding the subcategories, French adolescents scored higher on the “peer acceptance and support” (p < 0.001), family alliance (p = 0.017), and suicide-related items (p = 0.008). We found no difference between the two groups on the “self-acceptance” and “future optimism” items (Table 2).
Regarding the spirituality scale, French adolescents scored higher on “self-discovery” (p < 0.001), while the Brazilians reported higher scores in “spirituality and beliefs” (p = 0.021) and “respect of others and environment” (p = 0.01). We found no difference between the two groups for “self-awareness and collective consciousness” (Table 2).
Multivariate Models
Based on the results from univariate analyses, we developed 12 multivariate models to examine each selected variable’s relationship to French or Brazilian origin and to the other selected variables linked to geographic origin (see Methods section). The list of the variables and the results of the multivariate models are summarized in Table 3. Four variables were significantly explained by membership in the Brazilian sample, namely, “seeking spiritual support” (ACS) (β = -16.74, [95% CI -28.77 - -5.15], SE = 6.13, p <0.001), “social action” (ACS) (β = -13.98, [95% CI -20.61 - -6.85], SE = 3.47, p <0.001) and “dependence” (DEP-ADO total score) (β = -15.98, [95% CI -22.58 - -11.23], SE = 2.97, p <0.001), and life events (autonomy) (β = -0.27, [95% CI -0.51 - -0.03], SE = 0.12, p 0.032). Two variables were significantly explained by being part of the French sample, namely, “secure attachment style” (RSQ) (β = 12.68, [95% CI 11.37 - 14.33], SE = 0.78, p < 0.001) and a higher score in the Beck Depression Inventory (BDI II) (β = 9.16, [95% CI 3 - 15.46], SE = 3.22, p <0.001) (Table 3).
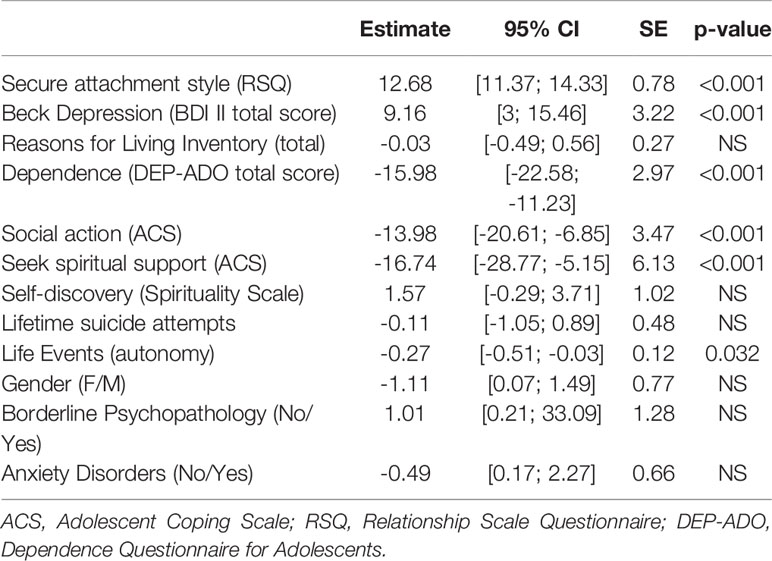
Table 3 Multivariate models to explain each selected variable by the French or Brazilian origin.
Discussion
In this study, we compared two clinical samples of suicidal adolescents to determine the main risk and protective factors associated with SA. To our knowledge, this is the first comparative study on suicidal behavior among adolescents between a European and a Latin American country. We first hypothesized that adolescents in the two groups would not present any difference in the main risk factors associated with suicidal behavior in adolescence. Indeed, the two samples presented very similar characteristics regarding major depressive disorders, disruptive and oppositional disorders, impulsivity, borderline traits, and use of substances, although the Brazilian sample had higher rates of psychopathology in several of these diagnoses (anxiety, borderline traits, use of substances, and suicide behavior). The high rates of psychiatric diagnosis found in the study were consistent with the well-established literature that has shown an association between the occurrence of suicidal behavior in adolescents and psychiatric diagnoses in more than 90% of cases (13). Borderline psychopathology was found in an extremely high percentage of both Brazilian and French adolescents. Studies have demonstrated that this diagnosis is the greatest source of suicidal behaviors in adolescents (59, 60).
The higher psychopathology scores of the Brazilian adolescents in almost all the clinical disorders constituted the major clinical difference between the two samples. A study conducted in Sao Paulo (Megacity Mental Health Survey) revealed that mental disorders are notably prevalent in this city, with an estimated prevalence of 10% of severe cases, which is the largest proportion of severely affected subjects between the countries that also took part in the initiative run by the WHO (61–64). Major depression emerged as one of the most prevalent disorders, with a higher estimated prevalence than has been seen elsewhere in other participating countries (65), which offers evidence on the burden of mental health in a developing country (66). Although the megacity study was conducted only on adults, there are also prevalence studies in children and adolescents, with results showing slightly but significantly higher levels of psychopathology in Brazil than in other countries (34, 35).
Regarding dimensional characteristics, such as attachment relationships, spirituality and coping strategies, we hypothesized that these variables would be influenced by geographical origin. Our second hypothesis was also confirmed. Indeed, there were significant differences in scores for spirituality, reasons for living, life events, attachment style and coping skills. Four protective factors remained significant in the multivariate models: attachment style, spiritual coping, and coping with social action and life events. Having a “secure style of attachment” was a protective factor associated with membership in the French cohort. An increased use of the spiritual type of coping and coping through social action was a protective factor associated with membership in the Brazilian cohort. These results are complex. We believe that per se, the two protective factors have specific effects. The protective effect of secure attachment in adolescent psychopathology in general [e.g., (67)] and regarding suicidality specifically (68) has been shown in several studies. Additionally, it is known from the literature that the relationship between religiosity and suicidal behavior is complex and often protective, although it can vary among different cultures and populations (69). Coping through social action and spiritual coping are both categorized in factor 3 of the ACS, which groups the coping styles characterized by reference to others, whether peers, professionals or deities (54, 70). The “use of others” as a resource that is compatible with a lack of any other resources (social and professional support or recreative activities) and with a more insecure attachment style is found in the Brazilian sample. Although less significant, “autonomous” life events were more common in the Brazilian sample. Some negative life events are related to psychological symptoms; however, personal “autonomous” life events were not associated with dysfunction (57, 71).
It is also important to note that empirical data strongly suggest the association of insecure attachment and substance abuse (72), since secure attachment is a well-described protective factor for drug use (73). These findings are likely related to the differences found in the Brazilian and French samples regarding substance use and attachment. Similarly, there are also some established relationships between religion and style of attachment, in which religiosity serves as a compensatory strategy for insecure attachment (74, 75). In a cross-sectional study using an adolescent sample (76), the results suggested that religiosity played the role of offering emotional support for insecure attachment in childhood. This association was partially supported by a similar study conducted more recently in 2016 (77): the authors found similar results in the cross-sectional arm but found mixed results after the 18-month follow-up period. Interestingly, insecure attachment has also been linked to instability in religiousness, particularly to sudden distress-related religious conversions (78). Brazil has been experiencing profound changes in regards to religiosity in recent decades, with a high number of new conversions to evangelical churches and a decline in absolute numbers of Catholics. The proportion of evangelical individuals in Brazil increased from 10.8% in 1991 to 21% in 2000 and to 34.3% in 2010 (79). The presence of insecure attachment and spiritual coping styles found in the Brazilian sample and confirmed by the multivariate analyses may suggest that religiosity in the Brazilian sample may serve as an emotional compensation strategy. The associations between recent changes in Brazilian society and the occurrence of insecure attachment need to be further investigated. The causes and consequences of these phenomena are complex, but we suggest that they may contribute to our hypotheses of emotional compensation in the Brazilian sample of adolescents with a history of SA.
Limitations
First, the Brazilian sample was much smaller than the French sample. The sample in Brazil came from an emergency department of a public university hospital, which suggests only patients with the most severe cases were included. In addition, only one recruitment site was involved in Brazil, while there were five sites in the French sample. This limits the generalization of the findings to all Brazilian adolescents. Such limitations are related to the difficulties in collecting psychiatric outcome data in a middle-income country (80). However, the Brazilian centre was not chosen randomly (see Method section). Second, modalities to run the interviews were not similar. French adolescents were assessed during an inpatient stay. Brazilian patients were asked to participate when they were in the emergency department and then contacted later by the research team and interviewed within a month.
Third, regarding substance abuse disorders, we only obtained the results from a questionnaire (DEP-ADO). The DEP-ADO is a questionnaire that assesses alcohol and drug use among adolescents and does an initial screening for problematic or at-risk consumption. It can be administered in face-to-face or self-report modes both for screening and for research and epidemiological monitoring purposes. Finally, while all questionnaires used herein have been validated in French, some Brazilian/Portuguese questionnaires were only translated/back translated for the purpose of this study, and the psychometric properties of these translated versions have not been examined.
Conclusions
Although French and Brazilian adolescents present similar rates of disorders, the Brazilian sample presented higher levels of psychopathology (except for depression severity). In addition, Brazilian adolescents had a more insecure pattern of attachment and used religious coping more often than their French counterparts. These differences should be further studied in the future. There are previous studies suggesting that religion may compensate for the social vulnerabilities found in a middle-income country (40). More transcultural studies may help elucidate these findings.
Data Availability Statement
Datasets are available upon request to the corresponding author, BM (Ym9qYW4ubWlya292aWNAY2h1LXJvdWVuLmZy).
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics approval was obtained for this study from CHU Charles Nicolle, France (2010 A00 330 - 39) and from the Group Ethics and Medical Research Committee of Sao Paulo University, Brazil (706939). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
NR and BM were responsible for data collection, preparing the first draft of the manuscript and finishing the final version of it, including the coauthors’ comments and suggestions. JS and AC were involved in the collection and analysis of data. HP was responsible for the data analyses. TF, DS, PG, and DC were responsible for the supervision of data collection and analyses and thoroughly revised all the versions of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was funded by the Universidade Federal de São Paulo (Brazil), the Centre Hospitalier Le Rouvray (France), the Fondation Pfizer, and the Fondation de France.
References
1. World Health Organization. Preventing suicide: a global imperative. Geneva: World Health Organization (2014) p. 88.
2. Asevedo E, Ziebold C, Diniz E, Gadelha A, Mari J. Ten-year evolution of suicide rates and economic indicators in large Brazilian urban centers. Curr Opin Psychiatry (2018) 31:265–71. doi: 10.1097/YCO.0000000000000412
3. Lim KS, Wong CH, McIntyre RS, Wang J, Zhang Z, Tran BX, et al. Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis. Int J Environ Res Public Health (2019) 16(22):4581. doi: 10.3390/ijerph16224581
4. Boletim Epidemiol. https://portalarquivos2.saude.gov.br/images/pdf/2019/julho/17/2019-014-Publicacao-02-07.pdf.
5. Piccin J, Manfro PH, Caldieraro MA, Kieling C. The research output on child and adolescent suicide in Brazil: a systematic review of the literature. Braz J Psychiatry (2019) 42(2). doi: 10.1590/1516-4446-2019-0497
6. Jaen-Varas D, Mari JJ, Asevedo E, Borschmann R, Diniz E, Ziebold C, et al. The association between adolescent suicide rates and socioeconomic indicators in Brazil: a 10-year retrospective ecological study. Braz J Psychiatry (2019) 41:389–95. doi: 10.1590/1516-4446-2018-0223
7. Observatoire National du Suicide. (2016). https://drees.solidarites-sante.gouv.fr/etudes-et-statistiques/la-drees/observatoire-national-du-suicide-ons/article/l-observatoire-national-du-suicide-ons.
8. EUROSTAT. (2016). Suicide death rate by age group. Eurostat. European Comission - Eurostat [5 août 2016]. Disponible sur: http://ec.europa.eu/eurostat/fr/home.
9. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet (2016) 387:1227–39. doi: 10.1016/S0140-6736(15)00234-2
10. Mann JJ. The serotonergic system in mood disorders and suicidal behaviour. Philos Trans R Soc Lond B Biol Sci (2013) 368:20120537. doi: 10.1098/rstb.2012.0537
11. Mirkovic B, Laurent C, Podlipski M-A, Frebourg T, Cohen D, Gerardin P. Genetic Association Studies of Suicidal Behavior: A Review of the Past 10 Years, Progress, Limitations, and Future Directions. Front Psychiatry (2016) 7:158. doi: 10.3389/fpsyt.2016.00158
12. Bridge JA, Goldstein TR, Brent DA. Adolescent suicide and suicidal behavior. J Child Psychol Psychiatry (2006) 47:372–94. doi: 10.1111/j.1469-7610.2006.01615.x
13. Renaud J, Berlim MT, McGirr A, Tousignant M, Turecki G. Current psychiatric morbidity, aggression/impulsivity, and personality dimensions in child and adolescent suicide: a case-control study. J Affect Disord (2008) 105:221–8. doi: 10.1016/j.jad.2007.05.013
14. Turecki G, Ernst C, Jollant F, Labonte B, Mechawar N. The neurodevelopmental origins of suicidal behavior. Trends Neurosci (2012) 35:14–23. doi: 10.1016/j.tins.2011.11.008
15. Brent DA. Risk factors for adolescent suicide and suicidal behavior: mental and substance abuse disorders, family environmental factors, and life stress. Suicide Life Threat Behav (1995) 25 Suppl:52–63. doi: 10.1111/j.1943-278X.1995.tb00490.x
16. Mustanski B, Liu RT. A longitudinal study of predictors of suicide attempts among lesbian, gay, bisexual, and transgender youth. Arch Sex Behav (2013) 42:437–48. doi: 10.1007/s10508-012-0013-9
17. Yonker JE, Schnabelrauch CA, Dehaan LG. The relationship between spirituality and religiosity on psychological outcomes in adolescents and emerging adults: a meta-analytic review. J Adolesc (2012) 35:299–314. doi: 10.1016/j.adolescence.2011.08.010
18. Breton J-J, Labelle R, Berthiaume C, Royer C, St-Georges M, Ricard D, et al. Protective factors against depression and suicidal behaviour in adolescence. Can J Psychiatry (2015) 60:S5–S15. doi: 10.1016/j.neurenf.2012.05.152
19. Richters J, Weintraub S. Beyond diathesis: toward an understanding of high-risk environments. In: Masten AS, Rolf J, Cicchetti D, Nuechterlein R, Weintraub S, editors. Risk and protective factors in the development of psychopathology. New York, NY: Cambridge University Press (1990). p. 67–96.
20. Rutter M. Resilience as a dynamic concept. Dev Psychopathol (2012) 24:335–44. doi: 10.1017/S0954579412000028
21. Consoli A, Cohen D, Bodeau N, Guile J-M, Mirkovic B, Knafo A, et al. Risk and Protective Factors for Suicidality at 6-Month Follow-up in Adolescent Inpatients Who Attempted Suicide: An Exploratory Model. Can J Psychiatry (2015) 60:S27–36.
22. Hollingsworth DW, Slish ML, Wingate LR, Davidson CL, Ramussen KA, O’Keefe VM, et al. The indirect effect of perceived burdensomeness on the relationship between indices of social support and suicide ideation in college students. J Am Coll Health (2018) 66:9–16. doi: 10.1080/07448481.2017.1363764
23. Mirkovic B, Cohen D, Garny de la Riviere S, Pellerin H, Guile J-M, Consoli A, et al. Repeating a suicide attempt during adolescence: risk and protective factors 12 months after hospitalization. Eur Child Adolesc Psychiatry (2020). doi: 10.1007/s00787-020-01491-x
24. Choo CC, Harris KM, Chew PKH, Ho RC. Does ethnicity matter in risk and protective factors for suicide attempts and suicide lethality? PloS One (2017) 12(4):e0175752. doi: 10.1371/journal.pone.0175752
25. Sisask M, Varnik A, Kolves K, Bertolote JM, Bolhari J, Botega NJ, et al. Is religiosity a protective factor against attempted suicide: a cross-cultural case-control study. Arch Suicide Res (2010) 14(1):44–55. doi: 10.1080/13811110903479052
26. Choo CC, Harris KM, Chew PKH, Ho RC. What predicts medical lethality of suicide attempts in Asian youths? Asian J Psychiatr (2017) 29:136–41. doi: 10.1016/j.ajp.2017.05.008
27. Phillips MR, Cheng HG. The changing global face of suicide. Lancet (2012) 379:2318–9. doi: 10.1016/S0140-6736(12)60913-1
28. Kataoka SH, Zhang L, Wells KB. Unmet need for mental health care among U.S. children: variation by ethnicity and insurance status. Am J Psychiatry (2002) 159:1548–55. doi: 10.1176/appi.ajp.159.9.1548
29. Chu J, Chi K, Chen K, Leino A. Ethnic variations in suicidal ideation and behaviors: a prominent subtype marked by nonpsychiatric factors among asian americans. J Clin Psychol (2014) 70:1211–26. doi: 10.1002/jclp.22082
30. Benatov J, Nakash O, Chen-Gal S, Brunstein Klomek A. The Association Between Gender, Ethnicity, and Suicidality Among Vocational Students in Israel. Suicide Life Threat Behav (2017) 47:647–59. doi: 10.1111/sltb.12332
31. Lee M-A. Social relationships, depressive symptoms and suicidality in Korea: Examining mediating and moderating effects in men and women. Int J Soc Psychiatry (2016) 62:67–75. doi: 10.1177/0020764015592434
32. Swanton R, Collin P, Burns J, Sorensen I. Engaging, understanding and including young people in the provision of mental health services. Int J Adolesc Med Health (2007) 19:325–32. doi: 10.1515/ijamh.2007.19.3.325
33. Choo CC, Chew PKH, Ho RC. Suicide Precipitants Differ Across the Lifespan but Are Not Significant in Predicting Medically Severe Attempts. Int J Environ Res Public Health (2018) 15(4):691. doi: 10.3390/ijerph15040691
34. Fleitlich-Bilyk B, Goodman R. Prevalence of child and adolescent psychiatric disorders in southeast Brazil. J Am Acad Child Adolesc Psychiatry (2004) 43:727–34. doi: 10.1097/01.chi.0000120021.14101.ca
35. Anselmi L, Fleitlich-Bilyk B, Menezes AM, Araújo CL, Rohde LA. Prevalence of psychiatric disorders in a Brazilian birth cohort of 11-year-olds. Soc Psychiat Epidemiol (2010) 45:135–42. doi: 10.1007/s00127-009-0052-2
36. McKinnon B, Gariépy G, Sentenac M, Elgar FJ. Adolescent suicidal behaviours in 32 low-and middle-income countries. Bull World Health Organ (2016) 94((5)):340–50. doi: 10.2471/BLT.15.163295
37. Bertolote JM, Fleischmann A, De Leo D, Bolhari J, Botega N, De Silva D, et al. Suicide attempts, plans, and ideation in culturally diverse sites: The WHO SUPRE-MISS community survey. Psychol Med (2005) 35(10):1457–65. doi: 10.1017/S0033291705005404
38. Bertolote JM, Fleischmann A, De Leo D, Phillips MR, Botega NJ, Vijayakumar L, et al. Repetition of suicide attempts: Data from emergency care settings in five culturally different low- and middle-income countries participating in the WHO SUPRE-MISS study. Crisis (2010) 31(4):194–201. doi: 10.1027/0027-5910/a000052
39. Fleischmann A, Bertolote JM, Wasserman D, De Leo D, Bolhari J, Botega NJ, et al. Effectiveness of brief intervention and contact for suicide attempters: A randomized controlled trial in five countries. Bull World Health Organ (2008) 86:703–9. doi: 10.2471/BLT.07.046995
40. Dalgalarrondo P: Religião. Psicopatologia e Saúde Mental [in Portuguese]. Porto Alegre, Brazil: Artmed (2008).
41. Posner K, Oquendo MA, Gould M, Stanley B, Davies M. Columbia Classification Algorithm of Suicide Assessment (C-CASA): classification of suicidal events in the FDA’s pediatric suicidal risk analysis of antidepressants. Am J Psychiatry (2007) 164:1035–43. doi: 10.1176/ajp.2007.164.7.1035
42. Mirkovic B, Labelle R, Guilé JM, Bellonde V, Bodeau N, Knafo A, et al. Coping skills among adolescent suicide attempters: results of a multisite study. Can J Psychiatry (2015) 60(2 Suppl 1):S37–45.
43. BARROS, FPC. A saúde como direito: o difícil caminho de sua apropriação pelos cidadãos. In: Santos R, editor. (Org.). CONASS. Direito à saúde: para entender a gestão do SUS (2015).
44. Massuda A, Hone T, Leles FAG, de Castro MC, Atun R. The Brazilian health system at crossroads: progress, crisis and resilience. BMJ Glob Health (2018) 3(4):e000829. doi: 10.1136/bmjgh-2018-000829
45. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry (1997) 36:980–8. doi: 10.1097/00004583-199707000-00021
46. Mouren-Siméoni MC. Kiddie- SADS-version vie entière (K-SADS-PL). Paris, France: Editions Scientifiques INSERM Edition révisée et modifiée (2002).
47. Brasil HHA. PhD thesis. Universida de Federal de São Paulo, Department of Psychiatry; 2003. Development of the Brazilian version of K-SADS-PL (Schedule for Affective Disorders and Schizophrenia for School Aged Children Present and Lifetime Version) and study of psychometric properties [In Portuguese].
48. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory. San Antonio, TX, USA (1996).
49. Beck AT, Steer RA. Manual for the Beck Hopelessness Scale. San Antonio (TX): Psychol. Corp (1996).
50. Eysenck HJ, Eysenck SBG. Manual of the Eysenck personality questionnaire (junior and adult). London: Hodder and Stoughton (1975).
51. Guile JM, Greenfield B, Berthiaume C, Chapdelaine C, Bergeron L. Reliability and diagnostic efficiency of the abbreviated-diagnostic interview for borderlines in an adolescent clinical population. Eur Child Adolesc Psychiatry (2009) 18:575–81. doi: 10.1007/s00787-009-0015-x
52. Zanarini MC, Gunderson JG, Frankenburg FR, Chauncey DL. The Revised Diagnostic Interview for Borderlines: Discriminating BPD from other Axis II Disorders A. Int J Methods Psychiatr Res (1993) 3(3):167–76. doi: 10.1521/pedi.1989.3.1.10
53. Landry M, Tremblay J, Guyon L, Bergeron J, Brunelle N. La Grille de dépistage de la consommation problématique d’alcool et de drogues chez les adolescents et les adolescentes (DEP-ADO): Développement et qualités psychométriques. Drogues santé société (2004) 3(1):20–37. doi: 10.7202/010517ar
54. Frydenberg E. Adolescent coping styles and strategies: Is there functional and dysfunctional coping? J Psychologists Counsellors Schools (1991) 1:35–42. doi: 10.1017/S1037291100002351
55. Delaney C. The Spirituality Scale: development and psychometric testing of a holistic instrument to assess the human spiritual dimension. J Holist Nurs (2005) 23:145–67; discussion 168-171. doi: 10.1177/0898010105276180
56. Osman A, Downs WR, Kopper BA, Barrios FX, Baker MT, Osman JR, et al. The Reasons for Living Inventory for Adolescents (RFL-A): development and psychometric properties. J Clin Psychol (1998) 54:1063–78. doi: 10.1002/(SICI)1097-4679(199812)54:8<1063::AID-JCLP6>3.0.CO;2-Z
57. Newcomb MD, Huber GJ, Bentler PM. A multidimensional assessement of stressful life events among adolescents. J Health Soc Behav (1981) 22:400–15. doi: 10.2307/2136681
58. Griffin DW, Bartholomew K. Models of the self and other: Fundamental dimensions underlying measures of adult attachment. J Pers Soc Psychol (1994) 67(3):430–45. doi: 10.1037/0022-3514.67.3.430
59. Greenfield B, Henry M, Weiss M, Tse SM, Guile J-M, Dougherty G, et al. Previously suicidal adolescents: predictors of six-month outcome. J Can Acad Child Adolesc Psychiatry (2008) 17:197–201.
60. Guile JM, Boissel L, Alaux-Cantin S, de La Riviere SG. Borderline personality disorder in adolescents: prevalence, diagnosis, and treatment strategies. Adolesc Health Med Ther (2018) 9:199–210. doi: 10.2147/AHMT.S156565
61. Andrade LH, Wang Y-P, Andreoni S, Silveira CM, Alexandrino-Silva C, Siu ER, et al. Mental Disorders in Megacities: Findings from the São Paulo Megacity Mental Health Survey, Brazil. PloS One (2012) 7(2):e31879. doi: 10.1371/journal.pone.0031879
62. Demyttenaere K, Bruffaerts R, Posada-Villa J, Gasquet I, Kovess V, Lepine JP, et al. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys. JAMA (2004) 291:2581–90. doi: 10.1001/jama.291.21.2581
63. Wells JE, Browne MAO, Scott KM, McGee MA, Baxter J, Kokaua J. Prevalence, interference with life and severity of 12 month DSM-IV disorders in Te Rau Hinengaro: the New Zealand Mental Health Survey. Aust N Z J Psychiatry (2006) 40:845–54. doi: 10.1080/j.1440-1614.2006.01903.x
64. Williams DR, Herman A, Stein DJ, Heeringa SG, Jackson PB, Moomal H, et al. Twelve-month mental disorders in South Africa: prevalence, service use and demographic correlates in the population-based South African Stress and Health Study. Psychol Med (2008) 38:211–20. doi: 10.1017/S0033291707001420
65. Kessler RC, Birnbaum HG, Shahly V, Bromet E, Hwang I, McLaughlin KA, et al. Age differences in the prevalence and co-morbidity of DSM-IV major depressive episodes: results from the WHO World Mental Health Survey Initiative. Depress Anxiety (2010) 27:351–64. doi: 10.1002/da.20634
66. UN-HABITAT. The State of Worlds cities 2006/2007: 30 Years of Shaping the Habitat Agenda. United Nations Human Settlements Programme (UNHSP). London, UK: Earthscan (2006).
67. Kobak R, Bosmans G. Attachment and psychopathology: a dynamic model of the insecure cycle. Curr Opin Psychol (2019) 25:76–80. doi: 10.1016/j.copsyc.2018.02.01835
68. Glazebrook K, Townsend E, Sayal K. The Role of Attachment Style in Predicting Repetition of Adolescent Self-Harm: A Longitudinal Study. Suicide Life Threat Behav (2015) 45:664–78. doi: 10.1111/sltb.12159
69. Sun L, Zhang J. Medically Serious Suicide Attempters With or Without Plan in Rural China. J Nerv Ment Dis (2016) 204:851–4. doi: 10.1097/NMD.0000000000000397
70. Frydenberg E. The Adolescent Coping Scale. Melbourne (AU): Australian Council for Educational Research (1993).
71. Compas BE, Slavin LA, Wagner BM, Vannatta K. Relationship of Life Events and Social Support With Psychological Dysfunction Among Adolescents. Youth Adolesc (1986) 15(3):205–21. doi: 10.1007/BF02139123
72. Schindler A, Bröning S. A Review on Attachment and Adolescent Substance Abuse: Empirical Evidence and Implications for Prevention and Treatment. Subst Abuse (2015) 36(3):304–13. doi: 10.1080/08897077.2014.983586)
73. Becoña E, Fernández del Río E, Calafat A, Férnandez-Hermida JR. Attachment and substance use in adolescence: A review of conceptual and methodological aspects. Adicciones (2014) 26(1):77–86. doi: 10.20882/adicciones
74. Granqvist P, Nkara F. Nature meets nurture in religious and spiritual development. Br J Dev Psychol (2017) 35:142–55. doi: 10.1111/bjdp.12170
75. Granqvist P. Attachment, culture, and gene-culture co-evolution: expanding the evolutionary toolbox of attachment theory. Attach Hum Dev (2020) 1–24. doi: 10.1080/14616734.2019.1709086
76. Granqvist P. Attachment and Religiosity in Adolescence: Cross-Sectional and Longitudinal Evaluations. Pers Soc Psychol Bull (2002) 28(2):260–70. doi: 10.1177/0146167202282011
77. Granqvist P, Hesse E, Fransson M, Main M, Hagekull B, Bohlin G. Prior participation in the strange situation and overstress jointly facilitate disorganized behaviours: implications for theory, research and practice. Attach Hum Dev (2016) 18:235–49. doi: 10.1080/14616734.2016.1151061
78. Granqvist P, Mikulincer M, Gewirtz V, Shaver PR. Experimental findings on God as an attachment figure: normative processes and moderating effects of internal working models. J Pers Soc Psychol (2012) 103:804–18. doi: 10.1037/a0029344
79. Alves JE, Cavenaghi S, Barros LF, Carvalho AA. Distribuição espacial da transição religiosa no Brasil. Tempo Soc (2017) 29(2):215–42. doi: 10.11606/0103-2070.ts.2017.112180
Keywords: adolescent, suicide attempt, coping, spirituality, attachment style
Citation: Rufino NC, Mirkovic B, Consoli A, Pellerin H, Santos JPM, Fidalgo TM, Gerardin P, Silveira DX and Cohen D (2020) Suicide Attempts Among French and Brazilian Adolescents Admitted to an Emergency Room. A Comparative Study of Risk and Protective Factors. Front. Psychiatry 11:742. doi: 10.3389/fpsyt.2020.00742
Received: 21 March 2020; Accepted: 15 July 2020;
Published: 06 August 2020.
Edited by:
Sara Calderoni, Fondazione Stella Maris (IRCCS), ItalyReviewed by:
Siddharth Sarkar, All India Institute of Medical Sciences, IndiaRoger C. Ho, National University of Singapore, Singapore
Merike Sisask, Tallinn University, Estonia
Copyright © 2020 Rufino, Mirkovic, Consoli, Pellerin, Santos, Fidalgo, Gerardin, Silveira and Cohen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natalia C. Rufino, bmF0cnVmaW5vQGhvdG1haWwuY29t
†These authors share senior authorship