 Sophie-Kathrin Kirchner1,2*
Sophie-Kathrin Kirchner1,2* Michael Lauseker3
Michael Lauseker3 Kristina Adorjan1,4
Kristina Adorjan1,4 Heike Anderson-Schmidt5
Heike Anderson-Schmidt5 Ion-George Anghelescu6
Ion-George Anghelescu6 Bernhardt T. Baune7,8,9Monika Budde4
Bernhardt T. Baune7,8,9Monika Budde4 Udo Dannlowski7Detlef E. Dietrich10,11,12
Udo Dannlowski7Detlef E. Dietrich10,11,12 Andreas J. Fallgatter13
Andreas J. Fallgatter13 Peter Falkai1
Peter Falkai1 Christian Figge14Katrin Gade5
Christian Figge14Katrin Gade5 Urs Heilbronner4Lena Hiendl15Georg Juckel16Janos L. Kalman1,4,17Farahnaz Klöhn-Saghatolislam4Carsten Konrad18
Urs Heilbronner4Lena Hiendl15Georg Juckel16Janos L. Kalman1,4,17Farahnaz Klöhn-Saghatolislam4Carsten Konrad18 Fabian U. Lang19
Fabian U. Lang19 Mojtaba Oraki Kohshour4,20
Mojtaba Oraki Kohshour4,20 Sergi Papiol1,4Daniela Reich-Erkelenz4
Sergi Papiol1,4Daniela Reich-Erkelenz4 Jens Reimer21,22
Jens Reimer21,22 Eva Z. Reininghaus15Sabrina K. Schaupp4Max Schmauß2
Eva Z. Reininghaus15Sabrina K. Schaupp4Max Schmauß2 Andrea Schmitt1,23
Andrea Schmitt1,23 Eva Christina Schulte1,4Simon Senner24
Eva Christina Schulte1,4Simon Senner24 Carsten Spitzer25Thomas Vogl4Jörg Zimmermann26Alkomiet Hasan1,2
Carsten Spitzer25Thomas Vogl4Jörg Zimmermann26Alkomiet Hasan1,2 Thomas G. Schulze4,27
Thomas G. Schulze4,27 Fanny Senner1,4
Fanny Senner1,4- 1Department of Psychiatry and Psychotherapy, University Hospital, Ludwig-Maximilians-University (LMU) Munich, Munich, Germany
- 2Department of Psychiatry, Psychotherapy and Psychosomatics, Medical Faculty, Bezirkskrankenhaus (BKH) Augsburg, University of Augsburg, Augsburg, Germany
- 3Institute for Medical Information Processing, Biometry, and Epidemiology, Ludwig-Maximilians-University (LMU) Munich, Munich, Germany
- 4Institute of Psychiatric Phenomics and Genomics, University Hospital, Ludwig-Maximilians-University (LMU) Munich, Munich, Germany
- 5Department of Psychiatry and Psychotherapy, University Medical Center Göttingen, Göttingen, Germany
- 6Department of Psychiatry and Psychotherapy, Mental Health Institute Berlin, Berlin, Germany
- 7Department of Psychiatry, University of Münster, Münster, Germany
- 8Department of Psychiatry, Melbourne Medical School, The University of Melbourne, Melbourne, VIC, Australia
- 9The Florey Institute of Neuroscience and Mental Health, The University of Melbourne, Parkville, VIC, Australia
- 10AMEOS Clinical Center Hildesheim, Hildesheim, Germany
- 11Center for Systems Neuroscience (ZSN), Hannover, Germany
- 12Department of Psychiatry, Medical School of Hannover, Hannover, Germany
- 13Department of Psychiatry and Psychotherapy, University Tübingen, Tübingen, Germany
- 14Karl-Jaspers Clinic, European Medical School Oldenburg-Groningen, Oldenburg, Germany
- 15Department of Psychiatry and Psychotherapeutic Medicine, Research Unit for Bipolar Affective Disorder, Medical University of Graz, Graz, Austria
- 16Department of Psychiatry, Ruhr University Bochum, Landschaftsverbund Westfalen-Lippe (LWL) University Hospital, Bochum, Germany
- 17International Max Planck Research School for Translational Psychiatry (IMPRS-TP), Munich, Germany
- 18Department of Psychiatry and Psychotherapy, Agaplesion Diakonieklinikum, Rotenburg, Germany
- 19Department of Psychiatry II, Ulm University, Bezirkskrankenhaus Günzburg, Günzburg, Germany
- 20Department of Immunology, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- 21Department of Psychiatry and Psychotherapy, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 22Department of Psychiatry, Health North Hospital Group, Bremen, Germany
- 23Laboratory of Neuroscience (LIM27), Institute of Psychiatry, University of São Paulo, Butanta, Brazil
- 24Department of Psychiatry and Psychotherapy, Technical University of Munich, School of Medicine, Munich, Germany
- 25Department of Psychosomatic Medicine and Psychotherapy, University Medical Center Rostock, Rostock, Germany
- 26Psychiatrieverbund Oldenburger Land gGmbH, Karl-Jaspers-Klinik, Bad Zwischenahn, Germany
- 27Department of Psychiatry and Behavorial Sciences, SUNY Upstate Medical University, Syracuse, NY, United States
Introduction: According to the World Health Organization, medication adherence is defined as the extent to which a person's behavior corresponds with an agreed recommendation from a healthcare provider. Approximately 50% of patients do not take their medication as prescribed, and non-adherence can contribute to the progress of a disease. For patients suffering from mental diseases non-adherence plays an important role. Various factors have been proposed as contributing to non-adherence, however the literature remains heterogeneous dependent on the analyzed patient subgroups. This study comprehensively evaluates the association of sociodemographic, clinical, personality and quality of life related factors with medication adherence by analyzing data from the PsyCourse study. The PsyCourse study is a large and cross-diagnostic cohort of psychiatric patients from the affective-to-psychotic spectrum.
Methods: The study sample comprised 1,062 patients from the PsyCourse study with various psychiatric diagnoses (mean [SD] age, 42.82 [12.98] years; 47.4% female). Data were analyzed to identify specific factors associated with medication adherence, and adherence was measured by a self-rating questionnaire. Odds ratios (OR) were estimated by a logistic regression for binary outcomes. Missing data were imputed using multiple imputation.
Results: The following factors showed the strongest association with medication adherence: never having used illicit drugs (OR, 0.71), number of prescribed antipsychotics (OR, 1.40), the personality trait conscientiousness (OR, 1.26), and the environmental domain of quality of life (OR, 1.09).
Conclusion: In a large and cross-diagnostic sample, we could show that a higher level of conscientiousness, a higher number of antipsychotic medication, a better quality of life within the environmental domain, and the absence of substance abuse contribute to a better medication adherence independent of the underlying disorder.
Introduction
Psychiatric disorders contribute 7% of the overall global burden of diseases, as measured in disability-adjusted life years, and 19% of all years lived with disability (1). The World Health Organization (WHO) has established a comprehensive mental health action plan to strengthen effective leadership and governance for mental health (2). Strengthening treatment adherence is one of the crucial aspects of the plan to secure sufficient treatment for mental health. Although useful drugs have been discovered for many psychiatric disorders, a substantial amount of patients do not take their medication regularly (3, 4). The consequences of non-adherence for the individual patient include relapses of symptoms, exacerbation of psychopathology, rehospitalization, prolonged disability, poor quality of life or psychosocial outcomes, and increased suicides (4). Additionally, non-adherence leads to increased co-morbid medical conditions and wastage of health care resources (3, 5).
According to a systematic review by Semahegn et al., 56% of patients with schizophrenia, 50% of patients with major depression, and 44% of patients with bipolar disorder are non-adherent (4). The WHO defines medication non-adherence as “a case in which a person's behavior in taking medication does not correspond with agreed recommendations from health personnel” (6). Non-adherence can have various reasons and can be intentional or unintentional. Especially in chronic psychiatric diseases such as bipolar disorder, unipolar depression, schizophrenia, and schizoaffective disorder, stabilization in the long-term often depends on good cooperation between the patient and health care provider and on treatment adherence (7, 8).
Reasons for non-adherence are usually multifactorial. Social support seems to play an important role, as patients from cohesive families and with practical support show higher treatment adherence (9). Disorder-related factors shape adherence behavior: a longer duration of illness favors non-adherence in both psychotic and affective disorders (10–13). Polypharmacy and adverse events were also predictors for lower adherence especially in patients suffering from bipolar and psychotic disorder (14–16). Patients with comorbid substance abuse show in various studies a lower adherence to their somatic and psychiatric medication (17–23). Research findings provide contradicting results on the association of general intelligence and adherence in patients with schizophrenia and bipolar disorder (24–27). Pronounced personality characteristics can complicate patients' interpersonal relationships, and perhaps cooperation in treatment (28). In patients suffering from early psychosis, high agreeableness is associated with poor medication adherence (29). In somatic disorders, studies showed that different personality traits mediate medication adherence, and in particular patients who score higher on conscientiousness are more adherent (30–32). Conscientiousness is defined as the propensity to follow socially prescribed norms for impulse control, to be goal directed, to plan, and to be able to delay gratification (33). In this respect, the question arises as to whether conscientiousness also influences treatment adherence in psychiatric disorders.
As summarized by Semahegn et al. (4), heterogeneous studies suggest that many factors influence treatment adherence in different disorders. By exploratively analyzing data from the PsyCourse study, this study aimed to investigate which sociodemographic, clinical, personality and quality of life-related factors are associated with treatment adherence in a group of 1,062 patients from the affective to psychotic spectrum.
Methods
Participants
Data were used from the longitudinal, multicenter PsyCourse study, which was conducted in Germany and Austria (www.PsyCourse.de) between 2011 and 2019. Diagnoses were assessed with parts of the structured clinical interview for DSM-IV. Participants were phenotyped by a comprehensive battery of tests that collected data on sociodemographics, illness history, treatment setting, psychopathology, cognition, functioning, personality traits, and quality of life. A detailed description of the study concept is available in the publication by Budde et al. (34). In our study, we used data from the first study visit, including all clinical participants with available information on adherence behavior; 161 participants had to be excluded because this information was missing. Healthy controls were not included. The sample comprised 1,062 participants with a DSM-IV diagnosis of schizophrenia, other psychotic disorder, schizoaffective disorder, bipolar disorder, or recurrent unipolar depression. This project analyzed data from the PsyCourse Phenotype Dataset, version 3.1. The study was approved by the local ethics committee and was performed in accordance with the Declaration of Helsinki.
Adherence Instrument
Adherence was measured with a non-standardized self-rating questionnaire that assesses the regularity of medication intake similar to the Brief Adherence Rating Scale (BARS) (35). It asks whether the patient had taken their psychopharmacological medication as prescribed in the past seven days and past 6 months. Reponses for both items ranged from 1 to 6, as follows: 1, “every day, exactly as prescribed;” 2, ”every day, but not always as prescribed;” 3, “regularly, but not every day;” 4, ”sometimes, but not regularly;” 5, “seldom;” and 6, ”not at all.“ In the analyses, we used the responses about the past 6 months and grouped them into two superordinate categories: 1–2, ”daily intake of medication,“ and 3–6, ”irregular intake of medication.“ In the following, for better clarity we refer to patients with daily medication intake as adherent patients and to those with unregular medication intake as non-adherent patients.
Sociodemographic Data
The mean [SD] age of participants was 42.82 [12.98] years; 47.4% of participants were female, and 52.6%, male. We collected information on family and partnerships, living situation, education, and work.
Diagnoses, History of Illness, and Treatment Setting
The distribution of diagnoses was as follows: 39.4% schizophrenia, 8.2% schizoaffective disorder, 1.0% schizophreniform disorder, 0.6% brief psychotic disorder, 34.6% bipolar-I disorder, 9.1% bipolar-II disorder, and 7.3% unipolar depression. For the analyses, we grouped the diagnoses into three categories: psychotic disorder (schizophrenia, schizoaffective disorder, schizophreniform disorder, and brief psychotic disorder), bipolar disorder (bipolar I disorder, bipolar II disorder), and unipolar depression. The PsyCourse dataset also includes information on illness course, including the age of onset and duration; number of hospitalizations; current treatment setting; suicidal ideation and suicide attempts; and comorbidities such as addictive disorders. Functioning and severity of illness were measured with the Clinical Global Impression scale (CGI) (36) and the Global Assessment of Functioning (GAF) (37).
Crystallized Intelligence Score
An approximate measure of general intelligence was obtained from participants in the PsyCourse study in the form of a crystallized intelligence assessed with the multiple-choice vocabulary intelligence test MWT-B (Mehrfachwahl-Wortschatz-Intelligenz Test) (38). In this test, participants are presented with 37 sets of five words each, four of which are “artificial words,” i.e., they do not exist in German. Participants are instructed to mark the real word, and the number of correctly identified real words is summed to give the final score.
Personality Dimensions
To assess personality traits, the PsyCourse study used the Big Five Inventory-10 (BFI-10) questionnaire (39). The inventory is based on the well-known “Big Five” personality model, which comprises the five dimensions extraversion, neuroticism, conscientiousness, agreeableness, and openness. For the analyses, we calculated the sum scores for each personality dimension (40).
Quality of Life
The WHOQOL-BREF was used to assess quality of life in the past 2 weeks (41). This instrument comprises 26 items that measure the following broad domains: physical health, psychological health, social relationships, and environment.
Univariate Analysis
As mentioned above, medication adherence was assessed dichotomously (i.e., as adherent or non-adherent). Numerical and ordinal data were expressed as means [SD], and nominal data, as frequencies. Numerical and ordinal dependent variables were compared by the Mann-Whitney-U test for non-normally distributed measurements, and categorical data, by Chi-squared tests (Phi and Cramer's Test). An alpha value of 0.05 was considered significant. Statistical analyses were performed with IBM SPSS statistics, version 25.0.
Multivariable Analysis
Missing values were multiply imputed using fully conditional specifications (MICE algorithm) (42), resulting in 10 (completed) data sets. Studies have been shown that more imputations do usually not lead to better results (43). The number of missing values is shown in Supplementary Table 1. A logistic regression model was used with the dichotomous outcome medication adherence and 45 variables available from the dataset as independent variables. Variable selection was performed with Akaike's information criterion in each of the completed data sets, resulting in 10 models. Variables were considered for the final model if they were selected in at least 5 of these 10 models. The model was re-run with these 14 variables, and regression coefficients were averaged with Rubin's rules. The analysis was performed with R 4.0.0, in particular the MICE packages (42).
Results
Univariate Analyses
Descriptive data of the study population is displayed in Table 1. One fifth (20.4%) of all patients reported non-adherent behavior within the last six months of treatment. The non-adherent patients were more often male (p = 0.016) and younger (p < 0.001). Descriptive analyses of sociodemographic, and clinical data in the adherent and non-adherent groups are summarized in Table 2.

Table 1. Descriptive data of study population.
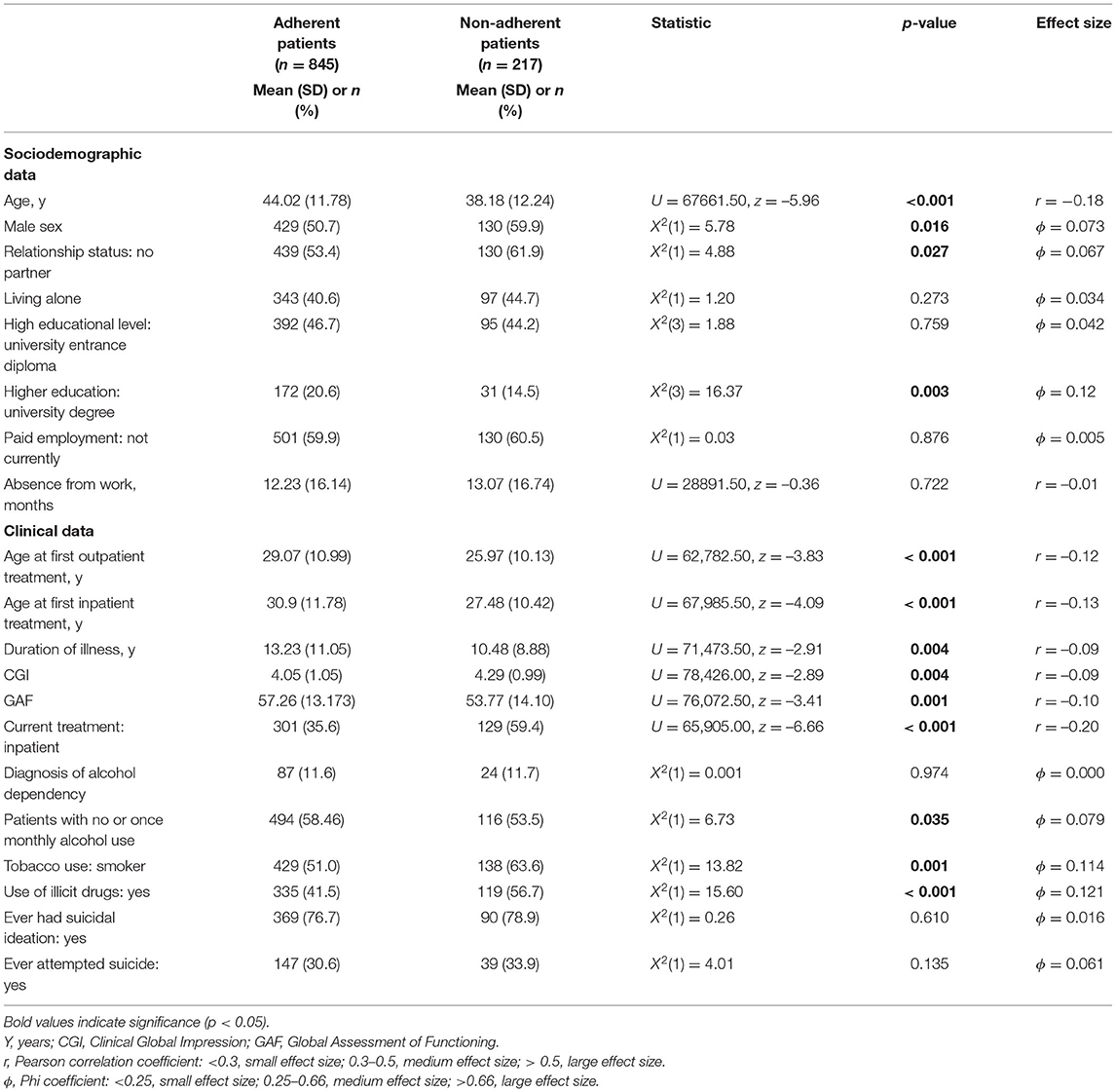
Table 2. Comparison of sociodemographic and clinical variables between the adherent and non-adherent patient groups.
The distribution of the diagnostic groups psychotic disorder and bipolar disorder was significantly different in the adherent and non-adherent groups (X2(1) = 12.67, p = 0.002, Φ = 0.109): Within the adherent group, 46.5% of the patients were diagnosed with a psychotic disorder, 46.3% with bipolar disorder, and 7.2% with unipolar depression. The respective percentages in the non-adherent group were 59.4, 33.2, and 7.4%.
Furthermore, the mean MWT-B score was higher in adherent patients than in non-adherent patients (adherent group, 28.31 [4.89]; non-adherent group, 27.29 [5.12]; U = 55,568.50; z = −2.34; p = 0.02).
The comparison of the number of medications prescribed and adverse events between adherent and non-adherent patient groups is summarized in Table 3.
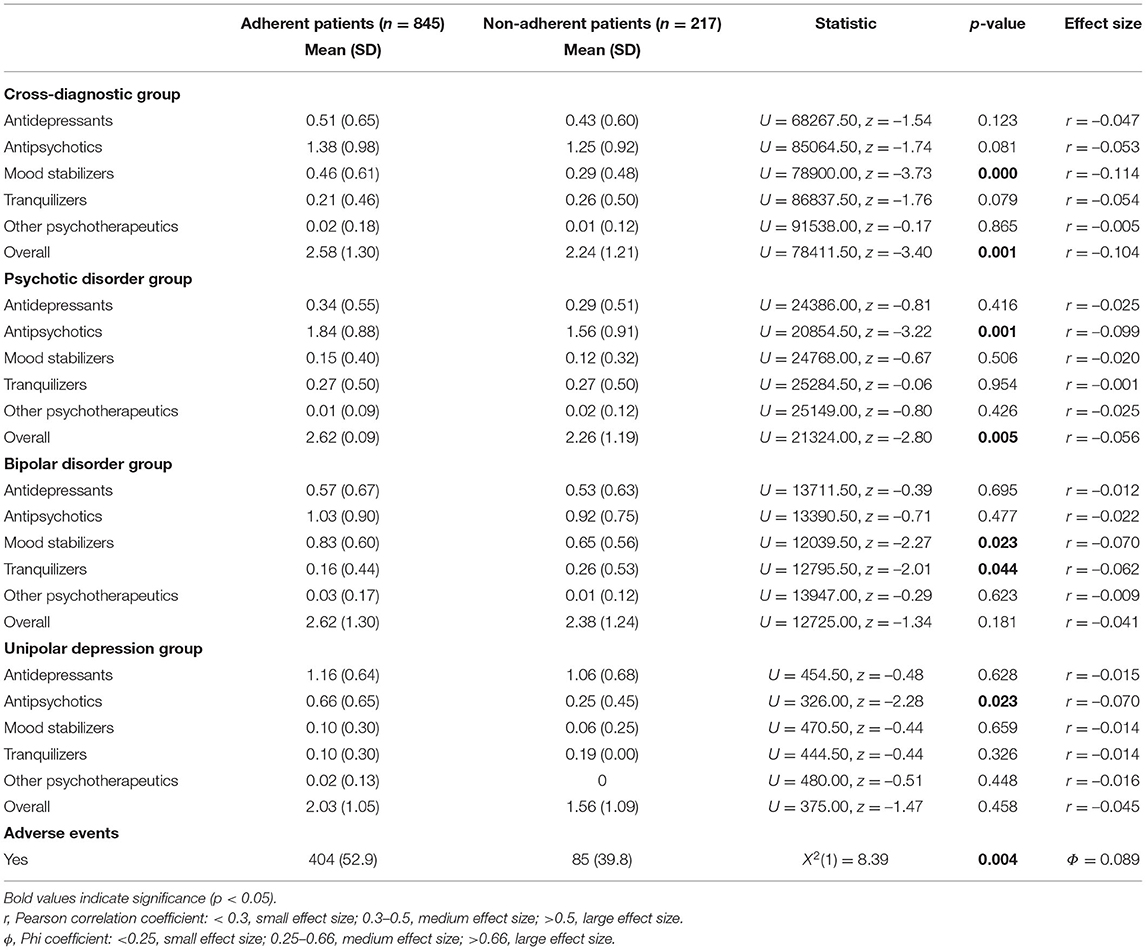
Table 3. Comparison of the number of prescribed medications and adverse events in the adherent and non-adherent patient groups.
The analyses of the association of personality dimensions with adherence behavior were performed both across and within the diagnostic groups. In the cross-diagnostic sample, non-adherent patients scored significantly lower in the domain of conscientiousness (adherent group, 3.63 [0.85]; non-adherent group, 3.43 [0.91]; U = 66051.00; z = −2.74; p = 0.006). The separate analyses within each of the three diagnostic groups found no significant differences.
Adherent and non-adherent patients rated quality of life differently, i.e., non-adherent patients rated quality of life significantly lower in the domains social relationships (adherent group, 13.21 [3.34]; non-adherent group, 12.07 [3.97]; U = 63,397.00; z = –3.58; p < 0.001) and environment (adherent group, 15.05 [2.64]; non-adherent group, 13.97 [2.86]; U = 57,195.00; z = –4.68; p < 0.001). The association between the total quality of life score and medication adherence was marginally significant. Implying that non-adherent patients tended to experience a worse quality of life compared to adherent patients (adherent group, 12.66 [3.75]; non-adherent group, 12.15 [3.67]; U = 70,371.00; z = –1.96; p = 0.051). The quality of life in the domains physical health (adherent group, 13.62 [2.78]; non-adherent group, 13.39 [2.78]; U = 71,173.00; z = –0.83; p = 0.408) and psychological health (adherent group, 12.96 [3.31]; non-adherent group, 12.60 [3.24]; U = 68,890.50; z = –1.47; p = 0.143) was not significantly different between the two groups.
Multivariable Analysis
To find factors potentially associated with medication adherence, we performed a logistic regression analysis. The odds ratios and confidence intervals of the final model are shown in Figure 1.
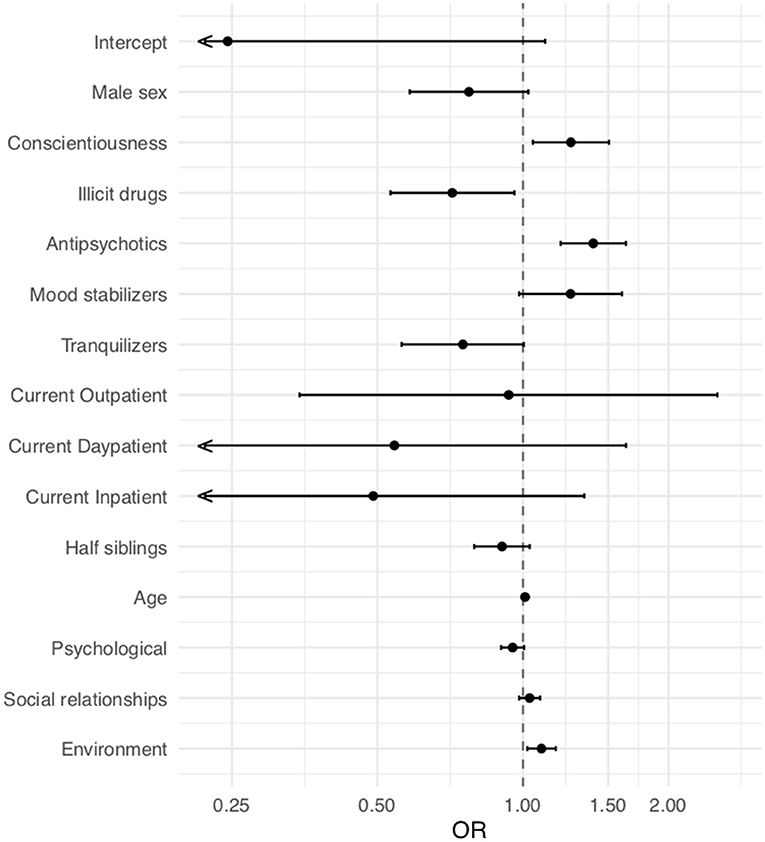
Figure 1. Odds ratios in the final model for adherence (x axis) and 95% CI. Intercept (odds ratio [OR], 0.26; 95% CI, 0.05–1.11; p = 0.069), male sex (OR, 0.77; 95% CI, 0.58–1.02; p = 0.075), conscientiousness (OR, 1.26; 95% CI, 1.05–1.51; p = 0.014), illicit drugs (OR, 0.71; 95% CI,: 0.53–0.96; p = 0.026), antipsychotics (OR, 1.40; 95% CI, 1.20–1.63; p < 0.001), mood stabilizers (OR, 1.25; 95% CI, 0.98–1.60; p = 0.069), tranquilizers (OR, 0.75; 95% CI, 0.56–1.00; p = 0.053), current outpatient status (OR, 0.93; 95% CI, 0.35–2.52; p = 0.893), current day-patient status (OR, 0.54; 95% CI, 0.18–1.63; p = 0.277), current inpatient status (OR, 0.49; 95% CI, 0.18–1.34; p = 0.165), half siblings (OR, 0.91; 95% CI, 0.79–1.03; p = 0.139), age [10 years] (OR, 1.11; 95% CI, 0.99–1.25; p = 0.077), quality of life—psychological (OR, 0.95; 95% CI, 0.90–1.01; p = 0.074), quality of life—social relationships (OR, 1.03; 95% CI, 0.98–1.09; p = 0.216), quality of life—environmental (OR, 1.09; 95% CI, 1.02–1.17; p = 0.011). OR, odds ratio.
Independent of the main disorder, the personality trait conscientiousness (OR, 1.26; 95% CI, 1.05–1.51; p = 0.014) was significantly associated with medication adherence. The use of illicit drugs had a negative effect on medication adherence (OR, 0.71; 95% CI, 0.53–0.96; p = 0.026). The medication regimen seemed to play an important role in our sample, which consisted mainly of patients with psychotic and bipolar disorder. In particular, the number of prescribed antipsychotics was associated with medication adherence (OR, 1.40 per medication; 95% CI, 1.20–1.63; p < 0.001). Moreover, patients with a higher quality of life in the domain environment showed better medication adherence (OR, 1.09; 95% CI, 1.02–1.17; p = 0.011).
Discussion
Medication adherence is a core component of adequate treatment of patients with psychiatric disorders. Previous studies found that medication adherence is affected mainly by demographic characteristics such as age and sex, social support system, comorbidities, substance abuse, and patients' individual attitude toward their medication and insight into their disorder (4). However, evidence investigating the association between personality traits and medication adherence in psychiatric patients remains sparse. In our large-scale, cross-diagnostic sample of chronically ill and well-phenotyped patients, we could identify conscientiousness, the absence of substance abuse and a higher number of antipsychotic medications, and a better quality of life in the domain environment as beneficial for medication adherence. These associations were found in the logistic regression analysis independent of the underlying disorder.
The positive association of conscientiousness and medication adherence is in line with other studies, where patients suffering from chronic somatic disorders or depression and with the prominent trait of conscientiousness were more adherent (44). Conscientious people tend to control impulses, delay gratification, set and reach goals, and plan in advance (45). Therefore, conscientious patients probably find it easier to manage the challenge of treating a chronic psychiatric disorder. Conversely, patients who score low on this personality trait might need more help to adjust to a regular medication regimen. Thus, considering personality traits may help to identify patients who need special support to adhere to their medication.
In line with other studies, we found that patients with a history of substance abuse have a higher risk of discontinuing their treatment regimen (20–23). Personality profiles with low conscientiousness are also associated with addictive disorders (46). Therefore, conscientiousness could be the mediator of this finding.
In our study, the adherent group was treated with a higher number of antipsychotic and mood-stabilizing drugs. This finding contrasts with previous findings that polypharmacy is linked to lower adherence (15, 16). In our study, non-adherent patients with bipolar disorder take more tranquilizers than adherent patients. This finding should make us more vigilant in prescribing tranquilizers, especially to patients who have the risk factors for less adherent behavior. Surprisingly, in our study adverse effects did not seem to have a major impact on medication adherence. In contrast, other studies found an association between adverse effects and non-adherence in patients with schizophrenia, bipolar disorder, and unipolar depression (14, 18, 47–50). Our study mostly comprises patients with chronic disorders and a longer history of medication intake. Adverse effects often occur when new medication is introduced or established medication is altered. This might explain why we could not find an association between adverse effects and non-adherence in our study.
Patients with a higher score for environmental quality of life also adhered better to their medication. This domain includes financial resources; a feeling of freedom; physical safety and security; accessibility and quality of health and social care; home environment; opportunities for acquiring new information and skills; participation in and opportunities for recreation; and physical environment, such as pollution, noise, traffic, climate, and transport (41). In the field of somatic diseases, adherence behavior was shown to increase the quality of life of patients with hypertension (51). Nevertheless, we have to be careful when interpreting findings such as this one because the cause and effect relationship may be unclear.
Additionally to our logistic regression analysis, we observed the following results in our explorative univariate analysis: Patients with male sex and younger age tended to be less adherent. Other studies also found that these characteristics are risk factors for poor adherence to treatment (3, 4, 52). In the univariate analysis, there was an association between higher crystallized intelligence, higher educational level, and adherent behavior. However, we did not investigate the relationship between cognitive deficits and adherence behavior in detail. Many studies point to an association between cognitive deficits and reduced medication adherence, but little is known about the educational level of non-adherent patients (53).
Despite the interesting findings and strengths of our study, some limitations should be discussed. The imputation of missing values might have added a small amount of additional uncertainty, and having a complete data set might also have improved the reliability of the results. No adjustment for multiple testing was implemented, given the exploratory nature of the analysis (54). Therefore, significant results have only exploratory character and a confirmatory validation of these results is necessary in further studies. In contrast to previous research results (4), only one fifth of the patients showed non-adherent behavior in our sample. Our sample consisted mainly of chronically ill patients. Patients with first episodes of a psychiatric disorder were underrepresented. These patients are typically younger and are considered to be less adherent (3, 4, 52). Patients who were asked to be included in the PsyCourse study are originally asked to participate in a longitudinal study. This might lead to a selection bias since the participation in a longitudinal study requires a high level of conscientiousness itself. Another limitation is that we evaluated adherence and the other factors both at the time of study enrolment. Therefore, the variables might have interacted with each other and cannot be interpreted independently. We only investigated medication adherence with a non-standardized, self-report questionnaire that focused on the regularity of medication intake and did not evaluate other important information, such as insight into the illness, attitude toward medication, and the perceived effect of the medication. Psychiatric treatment consists of much more than pure medication intake, for example other treatment forms, such as psycho- and sociotherapy; however, we were unable to investigate this aspect because the respective data were not available. Therefore, prospective studies and randomized controlled trials are needed to investigate the full picture of psychiatric care and treatment and respective patient adherence.
Taking our explorative results into consideration might help to identify those patients who are more adherent and those who require extra care in the form of psychoeducation, shared-decision making, and more frequent psychiatric consultations. Such an approach might help health care providers to determine personalized therapeutic strategies that facilitate adherence in patients at higher risk of discontinuing their medication.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethikkommission bei der Medizinischen Fakultät der LMU München. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
S-KK and FS designed, wrote, and revised the manuscript. ML contributed the statistics (multivariable analysis). ECS, JK, MB, and UH revised the analysis and its interpretation in detail. All authors contributed to the data collection of the PsyCourse study and revised and approved the final version.
Funding
TS was supported by the Deutsche Forschungsgemeinschaft (DFG) within the framework of the projects www.kfo241.de and www.PsyCourse.de (SCHU 1603/4-1, 5-1, 7-1, FA241/16-1) and by the German Federal Ministry of Education and Research (BMBF) through the Integrated Network IntegraMent (Integrated Understanding of Causes and Mechanisms in Mental Disorders), under the auspices of the e:Med Programme (01ZX1614K). TS received additional support from the BMBF within the framework of the BipoLife network (01EE1404H) and the Dr. Lisa Oehler Foundation, Kassel (Germany).
Conflict of Interest
AH has been invited to scientific meetings by Lundbeck, Janssen, and Pfizer, and he received paid speakerships from Janssen, Otsuka, and Lundbeck. He was member of Roche, Otsuka, Lundbeck, and Janssen advisory boards. AS was an honorary speaker for TAD Pharma and Roche and a member of Roche advisory boards. PF has been an honorary speaker for AstraZeneca, Bristol Myers Squibb, Lilly, Essex, GE Healthcare, GlaxoSmithKline, Janssen Cilag, Lundbeck, Otsuka, Pfizer, Servier, and Takeda and has been a member of the advisory boards of Janssen-Cilag, AstraZeneca, Lilly, Lundbeck, Richter, Recordati and Boehringer Ingelheim. CK received fees for an educational program from Aristo Pharma, Janssen-Cilag, Lilly, MagVenture, Servier, and Trommsdorff as well as travel support and speakers honoraria from Aristo Pharma, Janssen-Cilag, Lundbeck, Neuraxpharm and Servier. JZ was employed by Psychiatrieverbund Oldenburger Land gGmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all study participants and colleagues who contributed to the study. We appreciate Ruth E. Eyl for her valuable input.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.713060/full#supplementary-material
References
1. Rehm J, Shield KD. Global burden of disease and the impact of mental and addictive disorders. Curr Psychiatry Rep. (2019) 21:10. doi: 10.1007/s11920-019-0997-0
2. WHO. Adherence to long-term therapies: evidence for action. In: WHO. (2020). Available online at: http://www.who.int/chp/knowledge/publications/adherence_report/en/ (Accessed August 26, 2020)
3. Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. (2002) 63:892–909. doi: 10.4088/JCP.v63n1007
4. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. (2020) 9:17. doi: 10.1186/s13643-020-1274-3
5. Lindström E, Bingefors K. Patient compliance with drug therapy in schizophrenia. Economic and clinical issues. Pharmacoeconomics. (2000) 18:106–24. doi: 10.2165/00019053-200018020-00002
6. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. (2005) 353:487–97. doi: 10.1056/NEJMra050100
7. Beebe LH, Smith K, Phillips C. Descriptions and correlates of medication adherence, attitudes, and self-efficacy in outpatients with Schizophrenia Spectrum Disorders (SSDs). Arch Psychiatr Nurs. (2016) 30:400–5. doi: 10.1016/j.apnu.2016.01.010
8. Chakrabarti S. Treatment-adherence in bipolar disorder: a patient-centred approach. World J Psychiatry. (2016) 6:399–409. doi: 10.5498/wjp.v6.i4.399
9. DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health Psychol. (2004) 23:207–18. doi: 10.1037/0278-6133.23.2.207
10. Alene M, Wiese MD, Angamo MT, Bajorek BV, Yesuf EA, Wabe NT. Adherence to medication for the treatment of psychosis: rates and risk factors in an Ethiopian population. BMC Clin Pharmacol. (2012) 12:10. doi: 10.1186/1472-6904-12-10
11. Hill M, Crumlish N, Whitty P, Clarke M, Browne S, Kamali M, et al. Nonadherence to medication four years after a first episode of psychosis and associated risk factors. PS. (2010) 61:189–92. doi: 10.1176/ps.2010.61.2.189
12. Oller-Canet S, Fernández-San Martín MI, García-Lecina R, Castro Rodríguez JI, Font-Canal T, Lacasta-Tintorer D, et al. Do depressed patients comply with treatments prescribed?: a cross-sectional study of adherence to the antidepressant treatment. Actas Esp Psiquiatr. (2011) 39:288–93.
13. Teferra S, Hanlon C, Beyero T, Jacobsson L, Shibre T. Perspectives on reasons for non-adherence to medication in persons with schizophrenia in Ethiopia: a qualitative study of patients, caregivers and health workers. BMC Psychiatry. (2013) 13:1–9. doi: 10.1186/1471-244X-13-168
14. Baldessarini RJ, Perry R, Pike J. Factors associated with treatment nonadherence among US bipolar disorder patients. Hum Psychopharmacol. (2008) 23:95–105. doi: 10.1002/hup.908
15. Murray MD, Kroenke K. Polypharmacy and Medication Adherence. J Gen Intern Med. (2001) 16:137–9. doi: 10.1007/s11606-001-0033-y
16. Tareke M, Tesfaye S, Amare D, Belete T, Abate A. Antipsychotic medication non-adherence among schizophrenia patients in Central Ethiopia. S Afr J Psychiatr. (2018) 24:1124. doi: 10.4102/sajpsychiatry.v24i0.1124
17. Magura S, Rosenbaum A, Fong X. Factors associated with medication adherence among psychiatric outpatients at substance abuse risk. Open Addiction J. (2011) 4:58–64. doi: 10.2174/1874941001104010058
18. Sajatovic M, Levin J, Fuentes-Casiano E, Cassidy KA, Tatsuoka C, Jenkins JH. Illness experience and reasons for nonadherence among individuals with bipolar disorder who are poorly adherent with medication. Compr Psychiatry. (2011) 52:280–7. doi: 10.1016/j.comppsych.2010.07.002
19. Akerblad A-C, Bengtsson F, Holgersson M, von Knorring L, Ekselius L. Identification of primary care patients at risk of nonadherence to antidepressant treatment. Patient Prefer Adherence. (2008) 2:379–86. doi: 10.2147/PPA.S3511
20. Elbogen EB, Swanson JW, Swartz MS, Van Dorn R. Medication nonadherence and substance abuse in psychotic disorders: impact of depressive symptoms and social stability. J Nerv Ment Dis. (2005) 193:673–9. doi: 10.1097/01.nmd.0000180742.51075.70
21. Novick D, Haro JM, Suarez D, Perez V, Dittmann RW, Haddad PM. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. (2010) 176:109–13. doi: 10.1016/j.psychres.2009.05.004
22. González-Pinto A, Reed C, Novick D, Bertsch J, Haro JM. Assessment of medication adherence in a cohort of patients with bipolar disorder. Pharmacopsychiatry. (2010) 43:263–70. doi: 10.1055/s-0030-1263169
23. Ascher-Svanum H, Zhu B, Faries D, Lacro JP, Dolder CR. A prospective study of risk factors for nonadherence with antipsychotic medication in the treatment of schizophrenia. J Clin Psychiatry. (2006) 67:1114–23. doi: 10.4088/JCP.v67n0715
24. Maeda K, Kasai K, Watanabe A, Henomatsu K, Rogers MA, Kato N. Effect of subjective reasoning and neurocognition on medication adherence for persons with schizophrenia. Psychiatr Serv. (2006) 57:1203–5. doi: 10.1176/ps.2006.57.8.1203
25. Jónsdóttir H, Opjordsmoen S, Birkenaes AB, Simonsen C, Engh JA, Ringen PA, et al. Predictors of medication adherence in patients with schizophrenia and bipolar disorder: Predictors of medication adherence. Acta Psychiatr Scand. (2013) 127:23–33. doi: 10.1111/j.1600-0447.2012.01911.x
26. Lepage M, Bodnar M, Joober R. Malla A. Is there an association between neurocognitive performance and medication adherence in first episode psychosis?: Neurocognition and medication adherence. Early Interv Psychiatry. (2010) 4:189–95. doi: 10.1111/j.1751-7893.2010.00174.x
27. Perkins DO, Gu H, Weiden PJ, McEvoy JP, Hamer RM, Lieberman JA. Predictors of treatment discontinuation and medication nonadherence in patients recovering from a first episode of schizophrenia, schizophreniform disorder, or schizoaffective disorder: a randomized, double-blind, flexible-dose, multicenter study. J Clin Psychiatry. (2008) 69:106–13. doi: 10.4088/JCP.v69n0114
28. Bielańska A, Cechnicki A, Hanuszkiewicz I. The significance of the personality traits of schizophrenic patients and their therapists for the therapeutic relationship. Psychiatr Pol. (2016) 50:771–86. doi: 10.12740/PP/44189
29. Lecomte T, Spidel A, Leclerc C, MacEwan GW, Greaves C, Bentall RP. Predictors and profiles of treatment non-adherence and engagement in services problems in early psychosis. Schizophr Res. (2008) 102:295–302. doi: 10.1016/j.schres.2008.01.024
30. Ko KM, Moon SJ, Koh JH, Pae CU, Min JK. Contribution of personality traits, psychological factors, and health-related quality of life to medication adherence in patients with rheumatoid arthritis. Yonsei Med J. (2020) 61:406–15. doi: 10.3349/ymj.2020.61.5.406
31. Wall CL, McCombie A, Mulder R, Day AS, Gearry RB. Adherence to exclusive enteral nutrition by adults with active Crohn's disease is associated with conscientiousness personality trait: a sub-study. J Hum Nutr Diet. (2020) 33:752–7. doi: 10.1111/jhn.12787
32. Skinner TC, Bruce DG, Davis TME, Davis WA. Personality traits, self-care behaviours and glycaemic control in type 2 diabetes: the Fremantle diabetes study phase II. Diabet Med. (2014) 31:487–92. doi: 10.1111/dme.12339
33. Roberts BW, Jackson JJ, Fayard JV, Edmonds G, Meints J. Conscientiousness. In: Handbook of Individual Differences in Social Behavior. New York, NY, US: The Guilford Press (2009). p. 369–81.
34. Budde M, Anderson-Schmidt H, Gade K, Reich-Erkelenz D, Adorjan K, Kalman JL, et al. A longitudinal approach to biological psychiatric research: The PsyCourse study. Am J Med Genet B Neuropsychiatr Genet. (2019) 180:89–102. doi: 10.1002/ajmg.b.32639
35. Byerly MJ, Nakonezny PA, Rush AJ. The Brief Adherence Rating Scale (BARS) validated against electronic monitoring in assessing the antipsychotic medication adherence of outpatients with schizophrenia and schizoaffective disorder. Schizophr Res. (2008) 100:60–9. doi: 10.1016/j.schres.2007.12.470
37. Aas IM. Guidelines for rating Global Assessment of Functioning (GAF). Ann Gen Psychiatry. (2011) 10:2. doi: 10.1186/1744-859X-10-2
38. Lehrl S. Mehrfachwahl-Wortschatz-Intelligenztest: MWT-B. 5, unveränd Aufl Balingen: Spitta. (2005).
39. Rammstedt B, John OP. Measuring personality in one minute or less: a 10-item short version of the Big Five Inventory in English and German. J Res Pers. (2007) 41:203–12. doi: 10.1016/j.jrp.2006.02.001
40. Rammstedt B, Kemper CJ, Klein MC, Beierlein C, Kovaleva A. Eine kurze Skala zur Messung der fünf Dimensionen der Persönlichkeit. (2012). p. 33.
41. The Whoqol Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. (1998) 28:551–8. doi: 10.1017/S0033291798006667
42. van Buuren S, Groothuis-Oudshoorn K. MICE: Multivariate Imputation by Chained Equations in R. J Stat Softw. (2010) in press:1–68. Available online at: http://localhost/handle/1874/44635 (accessed November 16, 2020).
43. van Buuren S. Flexible Imputation of Missing Data. Second Edition. Boca Raton: CRC Press, Taylor & Francis Group. (2018).
44. Axelsson M, Brink E, Lundgren J, Lötvall J. The influence of personality traits on reported adherence to medication in individuals with chronic disease: an epidemiological study in West Sweden. PLoS ONE. (2011) 6:e18241. doi: 10.1371/journal.pone.0018241
45. Roberts SGB, Wilson R, Fedurek P, Dunbar RIM. Individual differences and personal social network size and structure. Pers Individ Dif. (2008) 44:954–64. doi: 10.1016/j.paid.2007.10.033
46. Dash GF, Slutske WS, Martin NG, Statham DJ, Agrawal A, Lynskey MT. Big Five personality traits and alcohol, nicotine, cannabis, and gambling disorder comorbidity. Psychol Addict Behav. (2019) 33:420–9. doi: 10.1037/adb0000468
48. Rosenheck R, Chang S, Choe Y, Cramer J, Xu W, Thomas J, et al. Medication continuation and compliance: a comparison of patients treated with clozapine and haloperidol. J Clin Psychiatry. (2000) 61:382–6. doi: 10.4088/JCP.v61n0511
49. Hoffman L, Enders J, Luo J, Segal R, Pippins J, Kimberlin C. Impact of an antidepressant management program on medication adherence. Am J Manag Care. (2003) 9:70–80.
50. McCann TV, Boardman G, Clark E, Lu S. Risk profiles for non-adherence to antipsychotic medications. J Psychiatr Ment Health Nurs. (2008) 15:622–9. doi: 10.1111/j.1365-2850.2008.01277.x
51. Fioravanti M, Bianchi V, Cinti ME. Cognitive deficits in schizophrenia: an updated metanalysis of the scientific evidence. BMC Psychiatry. (2012) 12:64. doi: 10.1186/1471-244X-12-64
52. Morken G, Grawe RW Widen JH. Effects of integrated treatment on antipsychotic medication adherence in a randomized trial in recent-onset schizophrenia. J Clin Psychiatry. (2007) 68:566–71. doi: 10.4088/JCP.v68n0409
53. Spiekermann A, Schulz M, Behrens J, Driessen M, Rahn E, Beblo T. Kognitive Leistungen und Adhärenzverhalten bei Patienten mit schizophrenen Psychosen. Fortschr Neurol Psychiatr. (2011) 79:73–82. doi: 10.1055/s-0029-1245622
Keywords: medication adherence, schizophrenia, bipolar disorder, depression, conscientiousness
Citation: Kirchner SK, Lauseker M, Adorjan K, Anderson-Schmidt H, Anghelescu I-G, Baune BT, Budde M, Dannlowski U, Dietrich DE, Fallgatter AJ, Falkai P, Figge C, Gade K, Heilbronner U, Hiendl L, Juckel G, Kalman JL, Klöhn-Saghatolislam F, Konrad C, Lang FU, Oraki Kohshour M, Papiol S, Reich-Erkelenz D, Reimer J, Reininghaus EZ, Schaupp SK, Schmauß M, Schmitt A, Schulte EC, Senner S, Spitzer C, Vogl T, Zimmermann J, Hasan A, Schulze TG and Senner F (2022) Medication Adherence in a Cross-Diagnostic Sample of Patients From the Affective-to-Psychotic Spectrum: Results From the PsyCourse Study. Front. Psychiatry 12:713060. doi: 10.3389/fpsyt.2021.713060
Received: 21 May 2021; Accepted: 07 December 2021;
Published: 20 January 2022.
Edited by:
Peter Uhlhaas, University of Glasgow, United KingdomReviewed by:
Massimo Tusconi, University of Cagliari, ItalyDushad Ram, Shaqra University, Saudi Arabia
David Weiss, Maine Medical Center Research Institute, United States
Copyright © 2022 Kirchner, Lauseker, Adorjan, Anderson-Schmidt, Anghelescu, Baune, Budde, Dannlowski, Dietrich, Fallgatter, Falkai, Figge, Gade, Heilbronner, Hiendl, Juckel, Kalman, Klöhn-Saghatolislam, Konrad, Lang, Oraki Kohshour, Papiol, Reich-Erkelenz, Reimer, Reininghaus, Schaupp, Schmauß, Schmitt, Schulte, Senner, Spitzer, Vogl, Zimmermann, Hasan, Schulze and Senner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sophie-Kathrin Kirchner, c29waGllLWthdGhyaW4ua2lyY2huZXJAYmtoLWF1Z3NidXJnLmRl