Abstract
Background: Safe and effective patient care depends on the teamwork of multidisciplinary healthcare professionals. Unfortunately, the field currently lacks an evidence-based framework for effective teamwork that can be incorporated into medical education and practice across health professions. We introduce a comprehensive framework for team effectiveness. Common challenges to teamwork in healthcare are identified along with evidence-based strategies for overcoming them.
Methods: The framework was developed in four steps: 1) grounding in the existing team science literature, 2) semi-structured interviews (N = 13), 3) thematic analysis and initial framework development, and 4) revision of the framework through input from healthcare professionals representative of different functions across the healthcare system (N = 13). A diagnostic tool consisting of one survey item per team competency was developed to complement the framework. The survey was then administered to healthcare teams across clinical and administrative functions (N = 10 teams, 96 individuals), and results were compiled and then used to conduct debriefs with individual team members and teams. A set of common teamwork challenges were identified using the survey and qualitative data. Qualitative data was analyzed to explore the unique ways these challenges manifest in both clinical and administrative teams.
Results: The five most common challenges that face healthcare teams relate to accountability, conflict management, decision-making, reflecting on progress, and coaching. These challenges were similar across both clinical and administrative team types. Based on the authors' collective experience designing and implementing Team Development Interventions (TDIs), strategies for managing each challenge are provided.
Conclusions: The proposed framework is unique in two ways. First, it's generally applicable across the many types of teams that contribute to the quality and safety of patient care. Second, the levels of the framework build upon each other to contribute to the development of the ideal team states. The framework and accompanying strategies can provide guidance for where and how to target developmental efforts.
Introduction
Multidisciplinary teams have been established as best practice for optimal patient care across many disciplines in healthcare (Haward, 2008; Tripathy, 2003; Merién, et al., 2010). In fact, advancements in medicine and the complex regulatory and economic factors affecting healthcare necessitate the use of multidisciplinary teams across the clinical, research, and administrative sectors of health systems. Although teamwork has been integrated into core competency models of health professional education, there is still an imbalance with a stronger focus on individual skill development, individual contribution, and accountability (Leggat, 2007). Given the decades of evidence that have borne out that teamwork skills contribute to performance (e.g., LePine et al., 2008), this lack of focus on teaming represents an important gap in professional preparation.
While the potential benefits of multidisciplinary teams are clear (e.g., a larger source of knowledge and skill from which the team can draw), working with team members from a wide variety of backgrounds can be challenging (Fleissig, et al., 2006). The practical barriers to these teams reaching their full potential can include differences in training, professional values, approaches to problem solving, and understanding of critical issues (Hall, 2005). Each team member also brings with them their unique personality, values, and communication preferences, which affects how team members interact and ultimately their ability to reach shared goals (Bell et al., 2018). Considering the context in which these teams work, there are a number of challenges inherent to healthcare that can also hinder performance, including psychological barriers (e.g., professional silos, hierarchies, power differentials) and organizational barriers (e.g., distributed teams, hybrid working models; Weller et al., 2014).
It is not surprising then, that teamwork breakdowns continue to be a primary cause of errors and near misses in healthcare, with root cause analysis suggesting lack of effective teamwork (e.g., communication) is involved in 60–70% of serious patient incidents (Rabøl, 2011). In the field, teamwork can affect clinical (e.g., diagnostic accuracy, time to response/treatment), patient (e.g., complications, length of stay; e.g., Schmutz and Manser, 2013), and employee (e.g., well-being and patient satisfaction; Ogbonnaya et al., 2018) outcomes. Fortunately, there is ample evidence to suggest that team interventions in the field can improve teamwork and team performance (Hughes et al., 2016; Weaver, et al., 2014).
For teamwork interventions in healthcare to reach their full potential, we need to first identify what drives or contributes to performance. While we have an understanding of the broad teamwork competencies that contribute to effective performance (e.g., shared mental models, mutual respect and trust, communication; Weller et al., 2014), the healthcare field lacks an evidence-based, comprehensive framework to better understand what facilitates and hinders effective multidisciplinary teamwork. Also lacking is an understanding of the most common teamwork challenges for multidisciplinary teams, how they can manifest in the field, and how they can be addressed.
Purpose
This effort set out to accomplish two primary objectives, both of which hold implications for research and practice: 1) to develop a comprehensive, evidence-based framework for healthcare team effectiveness, and 2) to generate a practical assessment tool that aligns with the framework and use this tool to identify common teamwork challenges. Towards the accomplishment of Objective 1, a framework for team effectiveness, informed by team science and grounded in data from the field, is introduced and critical team competencies defined. At present, the field has yet to establish a robust, evidence-based multidisciplinary framework for effective teamwork that can be integrated into current medical education curriculum. Limited extant team effectiveness research has attempted to generate integrative models that span across multiple healthcare contexts, and incorporate aspects of task design and organizational context (Lemieux-Charles and McGuire, 2006). While we acknowledge these contributions as valuable to the field, existing models fail provide a sufficient, in-depth perspective of teamwork essential to multidisciplinary team effectiveness. In addition, existing frameworks that address teamwork fail to span across multiple health professions (e.g., neonatal resuscitation, Thomas et al., 2004; emergency medicine, Fernandez et al., 2008; and healthcare governance, Brown et al., 2018). Our framework addresses both of these concerns by defining components to team effectiveness that are essential to multidisciplinary teams across healthcare contexts (i.e., clinical, administrative, research).
To achieve our second objective, we created and administered a diagnostic tool aligned with the framework. Follow-up qualitative inquiry was used to provide a case study or enriched interpretation of how teams experience these challenges, potential root causes, and the consequences for team outcomes. Despite the significant progress that has been made in understanding the difficulties healthcare teams face, challenges unique to multidisciplinary teams and how they manifest in the field remain less understood (Hall, 2005). As a result, the increase in multidisciplinary team care in healthcare settings has come with a tradeoff of placing teams in uncharted territory, encountering problems specific to interdependent multidisciplinary work that members are less equipped to navigate effectively. Finally, we complement these two objectives by providing evidence-based strategies or solutions, drawing from both the literature and our collective experience with team development, for addressing these common challenges.
In the sections that follow, we provide a brief discussion of relevant background research and report the development of the unified framework (Objective 1) created through interviews, focus groups, and extant literature. We also outline the development and refinement of a practical tool corresponding to the framework informed by team and healthcare subject matter experts or SMEs (Objective 2). In addition, we discuss deployment of this tool with a diverse sample of healthcare teams spanning multiple contexts within a larger hospital system. Following this, we present teamwork challenges identified through survey data and further explored through follow-up debriefs. We conclude by presenting illustrative case studies exemplifying five of the most common teamwork and evidence-based approaches to address these challenges.
Background
We grounded this effort in the research literature on team effectiveness in healthcare. Below we provide a brief overview of this literature, drawing from three overarching streams of research that informed the present work. Specifically, we introduce the concept of team effectiveness and highlight research supporting three distinct dimensions of team effectiveness: team performance, team functioning, and team viability.
Team Effectiveness
Team effectiveness can remain elusive and ill-defined if not clearly operationalized and consistently measured. Towards this end, team effectiveness is best understood as the combination of 1) team performance (results), 2) team functioning, and 3) team viability (Hackman and Lorsch, 1987). Essentially, effectiveness is a combination of what the team is able to accomplish (results – also referred to as team performance outcomes), how the team functions while working together on a daily basis (team functioning), and whether the team believes they would be able to continue successfully working together in the future (viability; Hackman and Lorsch, 1987). This multidimensional conceptualization is critical as it is not only present-focused, but takes into account future outcomes and members' beliefs about the team.
Team Performance (Results)
Team performance is regarded as a process reflective of individual and team-level teamwork, taskwork, and emergent team-level processes that arise when working towards a shared goal (Kozlowski and Klein, 2000; Salas et al., 2007; Salas et al., 2008). Based on this definition, team performance is often captured through objective production metrics (quotas, rates of production, etc.) in an effort to substantiate assertions of team performance improvement with tangible results (Barrick et al., 1998). Other subjective metrics have also proven useful in capturing team performance, such as peer and supervisor ratings (Barrick et al., 1998). The healthcare industry operates in a high-reliability context, and has a critical need to continually enhance team performance due to the nature and gravity of sub-optimal performance (i.e., patient quality of care and safety). Importantly, patient outcomes are impacted by clinical, administrative, and research teams alike. Thus, understanding factors that underpin team performance across different healthcare functions is essential to promoting team effectiveness in healthcare.
Team Functioning
Team performance results from the combination of two streams of team functioning (i.e., how the team performs on a day-to-day basis): teamwork and taskwork (Salas et al., 2004). Taskwork encompasses actions required for successful task completion contributing towards goal accomplishment (Bowers et al., 1997), and teamwork consists of the interrelated attitudes, behaviors, and cognitions (ABCs) needed to carry out interdependent actions required of the team (Salas et al., 2007). Although taskwork is acknowledged as important, researchers argue the linchpin to team performance is effective teamwork (Weaver et al., 2010). Seminal research on teams in healthcare has established the linkage between teamwork and team performance outcomes. For example, Manser (2009) synthesized multiple streams of research, finding that research on adverse events, healthcare provider perceptions, and clinical performance all supported the positive relationship between teamwork and patient safety. Better teamwork is associated with lower patient morbidity and mortality, as well as other critical outcomes such as reduced nursing turnover and increased patient satisfaction. Taken together, teamwork has proven instrumental to healthcare performance outcomes, meriting efforts to clarify how best to facilitate effective teamwork.
Team Viability
The final component of team effectiveness, team viability, pertains to future predictions of team functioning. A team’s perception of viability is subject to change after each performance episode and can be based on a broad number of factors – team processes, inputs, outcomes, and context – making it a more dynamic feature of effectiveness to capture (Bell, and Marentette, 2011). Despite the higher level of dynamism and fluidity in viability, researchers have asserted it is a critical criterion of effectiveness (Sundstrom et al., 1990), as it can be used to forecast the likelihood of a team operating successfully in the future. As with the preceding criteria, supervisor ratings (Barrick et al., 1998) and self-report measures (e.g., survey items) (Bushe and Coetzer, 2007; Bell and Marentette, 2011) have been used to capture team viability. In sum, many methods have been deployed to assess each facet of team effectiveness; it is with this in mind that we endeavor to provide and pilot test both a framework and a practical diagnostic measure that is carefully aligned with the framework to capture team effectiveness in healthcare.
Method
As previously mentioned, we aimed to achieve two objectives: 1) to develop a comprehensive, evidence-based framework for healthcare team effectiveness, and 2) create a practical assessment tool that aligns with the framework and use this tool to identify common teamwork challenges. Specifically, the framework was informed from multiple sources, including the literature on team science, interviews, and focus groups. Next, a practical tool that aligns with the framework was developed and refined based on input from team and healthcare SMEs. The tool was deployed with a diverse sample of teams across different healthcare functions in a large healthcare system. Finally, teamwork challenges were identified from both quantitative survey data and post-survey follow-up debriefs to add context and rich detail. In the sections that follow, the above process is outlined in more detail, followed by presentation of five of the most common teamwork challenges across the teams, rich illustrative cases studies of each challenge, and evidence-based solutions for addressing these challenges. This study received Institutional Review Board exemption and did not require informed consent (Protocol 2020-0627).
Participants
Objective 1
For development of the Team Effectiveness Framework, participants included 26 (76.9% F, 23.1% M) employees from a large healthcare organization in the Southwest United States. Of all participants, 69.2% were White, 11.5% were Black, and 7.7% were Asian, 3.8% were Hispanic, and 7.7% were other or non-disclosed. These participants included 10 healthcare leaders representing a variety of functional areas (including Nursing Education, Pharmacy, Communications, Interprofessional Education, Performance Improvement, and Leadership Development), three team science SMEs, and 13 frontline healthcare employees.
Objective 2
Survey participants were 96 healthcare professionals (N = 10 teams, 96 individuals; 66.7% F, 32.3% M) from a large healthcare organization in the Southwest United States employed across a variety of clinical and administrative functions. Of all participants, 31.3% were White, 30.2% were Black, and 22.9% were Asian, 12.5% were Hispanic, and 3.1% were other or non-disclosed (note that 13 participants contributed to both Objectives 1 and 2). A subset of 35 participants contributed to further qualitative data collection (20 individual interviews, one 15 person debrief). All participants were involved in an administrative team performance improvement program that was open to all members of the institution across clinical, research, and administrative sectors. The leaders of the teams opted in to the performance improvement program.
Research Design and Procedures
Objective 1
Development of the framework utilized a qualitative research design similar to a grounded theory, which is well-suited to the present effort because it allows for drawing from the vast knowledge on team science (i.e., a deductive approach) as well as for the capture of data unique to multidisciplinary healthcare teams (i.e., an inductive approach). Specifically, the literature on team science was used to create an initial framework based on existing theory. Competencies that have proven critical to teams were drawn from the literature to create an initial list for inclusion in the framework. Team science experts then conducted interviews and focus groups to develop and refine the framework to the unique context. Specifically, input was sought both from individuals who work together in teams in the field and from SMEs who work extensively with a variety of healthcare teams to ensure the framework would be applicable across different aspects of healthcare. The framework was developed through three steps.
Grounding in the Existing Team Science Literature
To identify potential team competencies of interest, we first scanned the literature on teams and team performance models in healthcare. Two team science SMEs reviewed these to establish a preliminary list of critical team competencies.
The two team science SMEs then conducted semi-structured interviews with a group of multidisciplinary healthcare professionals (N = 13). The interview protocol addressed the structure and purpose of teams, individual roles and responsibilities, and factors that facilitate and hinder team performance.
Thematic Analysis and Initial Framework Development
Qualitative interview data were then thematically analyzed. Competencies identified through the interview process were integrated with the preliminary competencies identified from the literature to create an initial framework.
Refinement of the Framework Though Iterative Feedback and Revision
The initial framework was then presented to a working group of key stakeholders representative of the different functions across a healthcare system, including Nursing Education, Pharmacy, Communications, Interprofessional Education, Performance Improvement, and Leadership Development (N = 13). Through a series of focus groups facilitated by two team science SMEs, stakeholders provided feedback that was incorporated into framework revisions. Specifically, stakeholders refined competency terms to aid in understanding and added key components not identified through the literature (e.g., Assume Positive Intent). The final framework contains 27 competencies that are critical to team effectiveness in healthcare (seeFigure 1 for framework and Appendix A for a description of competencies). Teams that exhibit these competencies demonstrate more effective team functioning (e.g., exchanging information effectively) and vitality (e.g., believing they can succeed) and experience conditions that enable team results (e.g., adequately staffed).
FIGURE 1
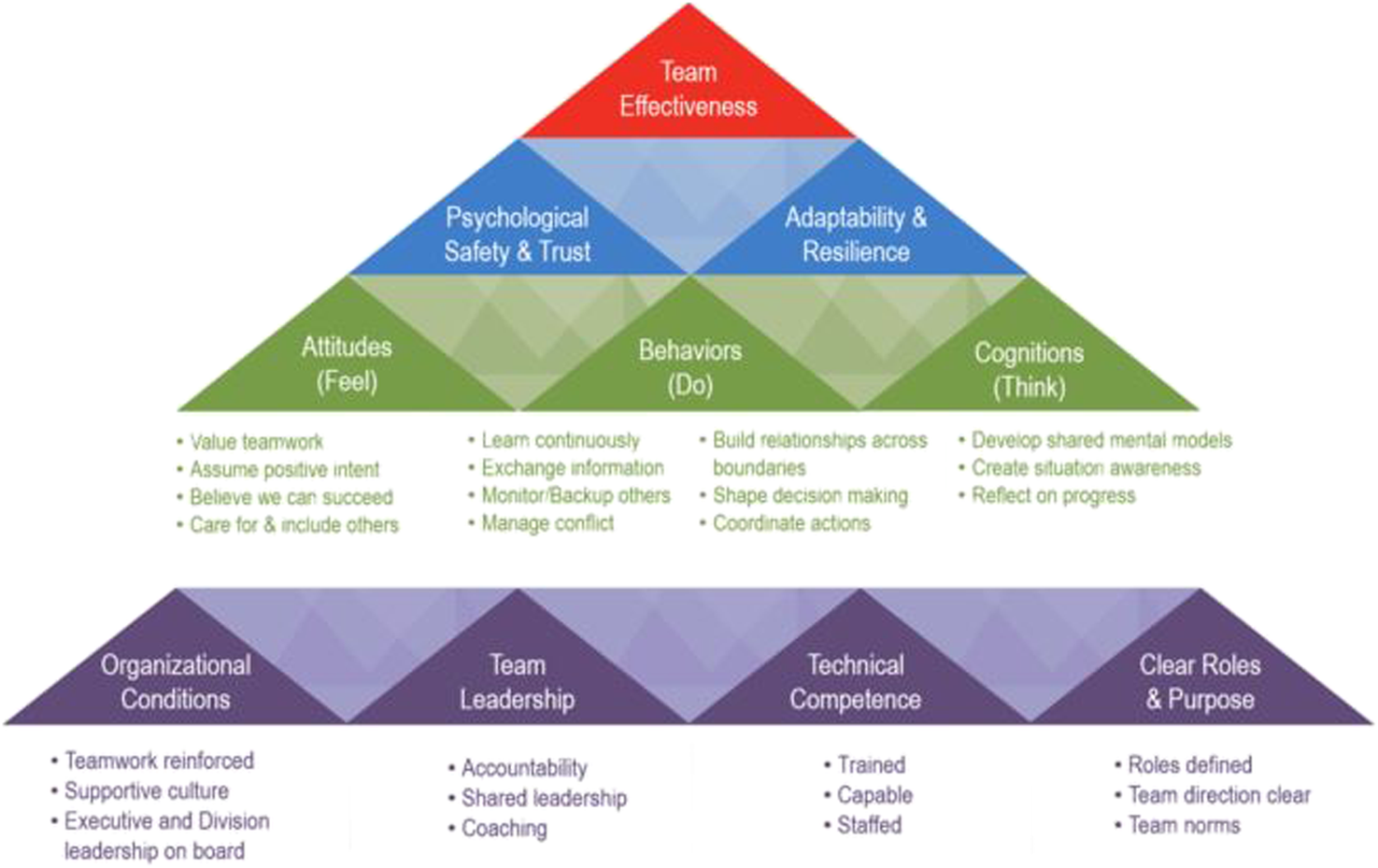
Comprehensive Team Effectiveness Framework.
Objective 2
Team Diagnostic Tool (Objective 2.1)
For Objective 2.1, we first needed to create a practical assessment tool to measure each of the 27 components of the framework (see Appendix A for a description). The Team Diagnostic Tool, designed to capture a snapshot of team effectiveness and reduce the survey fatigue common in healthcare, was developed in three steps:
Initial Item Development
First, one subject matter expert (SME) drafted one survey item per competency in the framework. Survey items were based on the competency definitions available in the literature.
Item Quality Review
Next, each item was independently reviewed by two subject matter experts for clarity and content. Item edits suggested by the SMEs were incorporated into the next iteration of the survey.
Item Comprehension Review
Finally, one expert in the field of employee development, but not in teams and teamwork, reviewed the items to ensure they were easily understandable by healthcare professionals across disciplines (i.e., free from jargon). Final item edits were made after this review, and items were uploaded to Qualtrics survey platform.
The final tool contained a set of 27 items that assess various aspects of team effectiveness. Items were rated on a Likert-type scale with the anchors: 1) Does Not Describe my Team at All to 9) Describes my Team Very Well. Example items include: 1) Both leaders and team members hold individuals accountable for their commitments and for behaving professionally, 2) Roles are defined clearly on this team, including responsibilities, reporting structure, and decision-making authority, and 3) Team members communicate effectively by exchanging information that is clear, accurate, timely, and unique.
Identification of Teamwork Challenges (Objective 2.2)
For Objective 2.2, the identification of common teamwork challenges, we used a mixed method, explanatory design. Quantitative data collection and analysis (i.e., deployment of the Team Diagnostic Tool) was followed up by qualitative data collection (i.e., interviews and focus groups; seeAppendix B for sample items) and analysis to aid in deeper interpretation of the data. Average interview and focus group length was approximately 1 h per interview/focus group.
Diagnosing Team Effectiveness
The Team Diagnostic Tool described above was deployed to each of the teams (N = 10 teams, 96 individuals) that participated in the study. These healthcare teams represented both clinical and administrative functions. The purpose of the tool was to provide a practical and quantitative diagnosis of each team’s competencies as depicted in the framework and assess its strengths and potential challenges to team effectiveness.
Initial Presentation of Results
Once the data from the Team Diagnostic Tool was analyzed (i.e., team averages were calculated for each item), results were presented to the team leader and then team members (de-identified and aggregated to the team level) of each team.
Follow Up Debriefs
Following the presentation of Team Diagnostic Tool data, individual semi-structured interviews (N = 20 individuals) and one focus group (N = 15 individuals) were held. The purpose of the interviews and focus group was to operationalize or provide rich detail around the challenges identified by the initial Team Diagnostic Tool.
In sum, using data aggregated across all teams, teamwork competencies consistently among the lowest rated were identified and represent a set of common challenges to healthcare team performance. Qualitative data from semi-structured interviews and group debriefs were thematically analyzed to explore the unique ways these challenges manifest in both clinical and administrative teams. Below, we introduce the framework, present the common challenges for healthcare teams, and provide evidence-based guidance on how to address the challenges and create high-performing teams.
Results
Framework Introduction
The proposed framework is unique in at least two ways (seeFigure 1; Zajac et al., in press). First, it is broadly applicable across the many types of teams that contribute to the quality and safety of patient care. While the importance of teamwork across all types of healthcare teams (e.g., administrative and research teams; Leggat, 2007) has been recognized, the majority of research is conducted with clinical teams. We aim for the framework to be adopted to create and study team development interventions (TDIs) across all sectors of healthcare, and to be integrated into healthcare professional education. Second, the levels of the framework build upon each other to contribute to the development of the ideal team states. This point is critical when determining where to target limited resources for team development. If gaps exist in lower levels of the framework, efforts may be maximized by focusing there first.
The framework delineates 27 competencies that are essential for high-performing teams functioning in large healthcare systems. Specifically, we present a blueprint for fostering team effectiveness through a hierarchical structure of building blocks organized by overarching themes (i.e., levels). While we acknowledge the importance of individual level traits (e.g., assertiveness, personal cultural traits) on team effectiveness, we did not include them in our framework as we focus specifically on team level variables. The Foundations of team effectiveness can be thought of as laying the groundwork for successful teamwork (e.g., Supportive Culture); if these elements are not in place initially, it can have a negative bottom-up impact on components at higher levels of the framework. Often termed enabling conditions, these critical aspects of teams have been evidenced to account for up to half of the variation in team performance (Hackman, 2012). The attitudes, behaviors, and cognitions, or ABCs of teamwork, refer to how teams think, feel, and act. Some ABCs are team-specific competencies in that they are associated with a specific team and context (e.g., clear roles, shared mental models), while others are generic or transportable and can be trained and brought to any team or situation (e.g., closed-loop communication; Weaver et al., 2010). Finally, the Ideal Team States are emergent properties that arise from individual team member characteristics and the ABCs, or how teams interact over time. According to Kozlowski and Klein (2000), “A phenomenon is emergent when it originates in the cognition, affect, behaviors, or other characteristics of individuals, is amplified by their interactions, and manifests as a higher-level, collective phenomenon’’ (p. 55). Because these ideal team states are emergent and built from the ABCs and foundations, we focus our identification of team challenges at the first two levels of this framework (seeAppendix A for a description of each competency).
Identification of Teamwork Challenges
To identify common challenges, we began by calculating descriptive statistics including the average score of each competency within each team. Further analyses were then conducted to identify the five competencies consistently rated the lowest across all teams (i.e., which competencies were ranked lowest across teams with the highest frequency). The team-level competency ratings were dichotomized such that items rated within the five lowest competencies on the team indicated the presence of a challenge. The dichotomized variables were dummy coded across teams with challenging competencies valued as 1 and not challenging as 0. Frequencies were then generated to identify the five most challenging competencies (i.e., competencies that appeared in the bottom five most frequently). A comparison of clinical and non-clinical teams revealed the top challenges remained largely the same across the different functions.
To build upon these findings, qualitative data was collected in the form of field notes from free response questions embedded in the survey, interviews, and focus groups. This allowed for triangulation of the data and identification of the different ways in which challenges associated with each competency can manifest on teams. Researchers have supported the value of qualitative analyses in healthcare to capture underlying phenomena experienced by healthcare providers and patients (Vaismoradi et al., 2013). The qualitative analyses were carried out by two researchers with expertise in team science. All qualitative data was analyzed by both researchers separately using Atlas.ti (a qualitative data analysis software). Specifically, using the list of team competencies derived from Objective 1 and the Team Effectiveness Framework as a codebook, each coder read through interview or focus group transcripts. Excerpts from the transcripts were coded or labeled with the representative team competency, and extensive notes were captured on how the competency manifested itself. The researchers met to discuss discrepancies at the midpoint and conclusion of the coding process. Taken together, our methodological approach aligns with the literature on teams, by utilizing multiple modalities to capture team-level phenomenon (Salas et al., 2017), providing a quantitative foundation for revealing common challenges, and the qualitative insight to enrich our interpretation and provide examples of how the challenges manifest in the healthcare context. Below, we present five common teamwork challenges along with case studies that were derived from the qualitative data collection effort (i.e., from the interviews and focus groups conducted during the team development activities).
Accountability
Accountability has been regarded as a key feature that enables teams to effectively outperform independent individual efforts (Katzenbach and Smith, 2005). Accountability is often defined in terms of an employee or team accepting responsibility or answering for certain deliverables, for example as, “the means by which individuals and organizations report to a recognized authority (or authorities) and are held responsible for their actions” (Edwards and Hulme, 1996; p. 967). While there is no doubt that following through on commitments is important to performance, accountability can also be defined as something a leader fosters more proactively. Bregman (2016) asserts that getting angry, frustrated, or pleading when goals are not met rarely works as a strategy for holding team members accountable. Instead, the author urges leaders to provide the following to create accountability and set employees up for success: 1) clear expectations around the desired outcome, the desired approach to achieving the outcome, and how success will be measured (2), the skills and resources needed to meet expectations, 3) clear, measurable targets with associated milestones, 4) open and ongoing feedback, and 5) clear consequences for success or failure. The employee or team can help co-create these conditions, but they need to be in place up front.
In the context of healthcare, accountability is of particular importance as the tasks teams engage in ultimately affect patient safety and quality of care. Unfortunately, efforts examining accountability have revealed that many teams face challenges; specifically, Brown et al. (2011) examined conflict in primary healthcare teams (PHCTs), finding that accountability was one of three main sources of conflict. Many of these challenges arise out of incongruences between current approaches to patient care and assignment of accountability (Leggat, 2007; Bell et al., 2011). Put differently, from a multilevel perspective, the accountability structures in many healthcare organizations are seemingly at odds with the team-level care healthcare providers are expected to deliver to patients, and the individual level to which accountability is assigned (Leggat, 2007). This can be problematic as medical errors often occur through multiple breakdowns in teamwork, wherein responsibility falls on several members of the team (Bell et al., 2011).
Below, we examine how accountability challenges manifested on one such team and follow this with recommendations for interventions.
Case Example: Accountability vs. Punishment and Blame
The exemplar team for accountability functioned on the administrative side of processing clinical trials. Because the output of this team directly influenced the research activities and financial outcomes of the institution, expectations for timely and high-quality work were high. To encourage accountability, each member of the team was required to sign an individual accountability contract, holding them to a standard output of quality and quantity. Accountability measures in and of themselves may not be problematic and are commonplace in organizations; they can take the form of formal reporting relationships, individual and team performance evaluations, and group norms (Frink and Klimowksi, 1998). Implemented under the right circumstances, these measures can result in positive outcomes. For example, Thoms et al. (2002) found accountability measures increased employee perception that coworkers and managers were aware of their work, and ultimately improved job satisfaction.While the accountability document was intended to increase motivation and follow-through, it was perceived as a way to place blame and punish those who did not meet goals. Essentially, this effort fell short because it ignored the pre-conditions for success or the proactive establishment of accountability delineated by Bergman (2016). First, clear, challenging (yet achievable) expectations were not established or consistent. Priorities of the team changed rapidly, and changes (although necessary) were implemented without a strong or cohesive message from leadership, leading to the perception by some that change was “optional” or that leadership was enforcing change inconsistently or unfairly. For example, a new policy was implemented and no clear expectations for how it would be enforced were established, leading some team members to wonder if everyone was being held accountable – was everyone actually adhering to the new policy, and moreover was anyone going to check for compliance? Second, not all team members had the capability or skills needed to meet the expectations (i.e., in terms of the Team Effectiveness Framework, they were not trained). Specifically, because the team was in a fast-paced, high-pressure environment, new employees were not receiving the onboarding training they needed to be successful. As is common in many teams, members were required to “figure it out as they go." This resulted in new members working longer hours, missing their performance goals despite these long hours, and making numerous mistakes. In addition to this, qualitative data revealed employees felt they lacked the needed continuing education (e.g., around new processes and procedures) and cross-training to understand how their work affected the group that received it.Ultimately, the end result was a detriment to team morale when members were held accountable for goals they felt they could not achieve. Mistakes led to the threat of additional accountability measures from an institutional body outside of the department, and the formation of an internal accountability team that raised tension and conflict. The department experienced a significant amount of turnover from both managers and frontline staff.
Solutions for Accountability
Accountability is an enormous and sometimes complicated concept; teams presenting with a concern around accountability could be experiencing a number of underlying issues. Often additional information is needed to pinpoint the contributing factors (for example, in the previous case, causes included unclear expectations and lack of training). One such intervention that can provide more insight is the Start, Stop, and Continue (SSC) exercise. The SSC exercise can be thought of as a dedicated time or opportunity for the team to debrief on their collective experience. According to Ciccarelli (2016), the “Start” bucket is the best place to begin—this includes generating new ideas around where the team should invest time, new initiatives, or improved processes that could move the team forward. The “Stop” bucket includes items that get in the team’s way, including activities that cost a great deal of time with little return, distract from the core purpose of the team, or cause undue stress or conflict. Finally, identify the activities that result in positive outcomes, and that the team should “Continue” moving forward.
To create clear expectations and a shared awareness of changes to policy and procedures (and importantly, how changes impact the team’s work) leadership teams should be intentional about creating strategic communication plans. The literature on change management provides a wealth of advice on communicating change. For example, Balogun (2003) examined the complexity of change and how this affects choice of communication media. Routine changes communicated via individual, personal methods (e.g., face-to-face, telephone) may be overly complicated, while complex changes communicated more general (i.e., employee announcements) may lack depth and sensitivity. While a review of the literature around communicating change is beyond the scope of this article, we provide key points that can be used as a checklist when creating a communication strategy (See Table 1).
TABLE 1
| Elements of a strategic communication plan |
|---|
| ❖ What is the purpose of the message (to inform, get input)? |
| ❖ What are the key points of the message to be shared? |
| ❖ What is the connection to/alignment with the organization’s strategy, mission, and values? |
| ❖ What is the “how” and “why” behind the decision? |
| ❖ What process will be used to check for understanding? |
| ❖ How will this impact the employee’s approach to work (structure, processes, priorities)? |
| ❖ How will success be measured? |
| ❖ How (through what media) will the communication take place? |
| ❖ When (or by when) will communication be sent to the team? |
Elements of a strategic communication plan.
Conflict Management
Conflict is inherent to working in diverse teams, and under certain circumstances can be beneficial to team outcomes. Conflict in teams is often broken down into two distinct categories delineated by Jehn (1999), and each has its own unique influence on performance. Relationship Conflict, which arises from interpersonal issues and differences in personality, values, and beliefs, almost universally has a negative influence on team member attitudes and team effectiveness (e.g., motivation, commitment, performance; Chen at al., 2011; Shaw et al., 2011). On the other hand, the association between Task Conflict, defined as disagreements among ideas, opinions, and approaches to the task (Jehn, 1999), and team outcomes is much more complicated. De Dreu (2006) suggests there may be a curvilinear relationship among task conflict and outcomes such as innovation, such that moderate levels of task conflict result in the best outcomes. We argue, whether or not the positive aspects of task conflict are realized may depend largely on how the conflict is managed.
Conflict management has been defined by DeChurch and Marks (2001) as “strategies implemented by group members aimed at reducing or solving conflict” (p. 6). The authors find that task conflict can lead to greater performance and satisfaction; however, this only holds true if managed actively (i.e., open discussion of differences and firm pursuit of one’s ideas) and agreeably (i.e., pleasant, relaxed). The conflict management literature has since steadily grown to include the importance of cooperation and competition styles (Somech et al., 2009). In DeChurch et al. (2013), the authors theoretically separate conflict states (i.e., what teams are disagreeing about) and conflict process (i.e., how teams incorporate disagreements), and find meta-analytic support for this distinction. The authors assert it is the latter, conflict process, which directly influences performance; findings suggest that when conflict states are controlled, processes used to manage conflict predicted more variance in team outcomes than did the states themselves.
Task conflict management strategies are essentially reflective of the way dissent is processed at the team level and have indeed been linked to team outcomes (Behfar et al., 2008). Regardless of what a specific management style is called, taxonomies of conflict style have one underlying theme; effective styles result in sincere consideration and integration of other’s input while ineffective styles lead to dismissal of ideas and lost information (Janssen et al., 1999). Lencioni (2012) describes at one end of extreme teams can experience artificial harmony, where team members don’t engage in open, constructive conflict (e.g., because of low levels of trust, desire to appear agreeable, discomfort with confrontation) and strive to keep a level of peace. On the other end of the conflict continuum, teams can experience abrasive personal attacks during disagreements. To be effective, teams need to find a middle ground characterized by psychological safety, where members can openly disagree, respect each other’s input, and walk away without taking things personally (Edmondson, 1999).
Case Study: Extreme Ends of the Conflict Continuum
At either end of the conflict continuum, artificial harmony or personal attacks, consequences can occur for open exchange of ideas; essentially, under these conditions teams are unable to capitalize on the wider pool of knowledge and experience from diverse members. Healthcare attracts many individuals who are passionate about the purpose and mission of their work. Furthermore, these individuals are well-trained experts in their field, and they are working in an environment where their team’s performance can affect patient care and mistakes hold serious consequences. Because of the combinations of these factors, this exemplar team, a senior leadership team (SLT) involved in clinical care, experienced strong, vocal disagreements between members on one end of the continuum. Each member was enthusiastic and entrenched in their positions, and without the right set of skills to uncover them, mutually satisfying solutions were not sought.
On the opposite end of the continuum, the strong hierarchy inherent in the medical field has been evidenced to present barriers to speaking up, or what Weiss et al. 2017 term voice behavior. The authors note that while research shows employees with lower hierarchical status are often hesitant to speak up because of fear of negative outcomes, the complex, ill-structured nature of problems in healthcare make voicing concerns or opinions even more important. Individual characteristics of employees, including personality (e.g., assertiveness; Weiss et al., 2014) and directness of conflict expression (Weingart et al., 2015) can also create differences in how people speak up, and how comfortable they are doing so. Taken together, these factors can lead to silence being interpreted as agreement when team members are avoidant of conflict. They can also lead to conflict initially focused on the task bleeding over into relationship conflict when conflict styles don’t match (e.g., a direct conflict individual approaches a colleague who prefers indirect expression). In this team, the members varied widely on assertiveness and directness of conflict expression, leaving the less assertive, less direct members to disengage from conflict. Silence from these members was interpreted as agreement.
For this team, experiencing both strong task conflict that turned personal as well as artificial agreement led to a number of different negative team outcomes. First, significant time and energy was lost. Specifically, SLT members not directly involved in the conflict spent time that could have been directed toward the task and accomplishing shared goals instead trying to maintain harmony on the team. Second, the valuable contribution of team members, especially direct frontline staff, was lost. These members were hesitant to speak up with an idea or experiment with the unknown or new and innovative processes. Watching the SLT model behaviors perceived as attacking, or hearing their own leaders express a desire to avoid confrontation, strongly influenced their behavior. Poor conflict management between SLT members also led to each of the units within the department feeling siloed. Areas where collaboration between units may have benefited both parties were evident but not taken advantage of. Overall, otherwise well-intentioned, talented leaders created a culture that was prohibiting the open exchange of team members’ diverse perspectives and getting in the way of this team and their staff achieving their full potential.
Solutions for Conflict Management
To foster constructive task conflict, include courses on negotiation in leadership and team development interventions. According to
Allred et al. (1997), negotiation is the primary process by which conflict can be managed. The authors define effective negotiation as generating mutually satisfying solutions that build or integrate different interests in innovative ways, with the dimensions of claiming value, creating value, and maintaining the ongoing relationship. Solutions that meet the needs of both parties, or create value, include 1) Bridging solutions (i.e., solutions that meet the needs or interest of both people without compromise or tradeoff) and 2) Trade-offs (i.e., strategic trade-offs where one gives up something of lesser importance to obtain something viewed as more important; Rubin et al., 1994). To reach these integrative solutions, team training can include the following behaviors (
Allred et al., 1997):
Free exchange of information between negotiators (being forthcoming about one’s own interests and preferences)
Actively listening and seeking to understand the other side’s perspective
Asking more questions about the other's position and making less statements about one's own position
Considering or negotiating for multiple issues rather than each issue separately
Avoiding fixed-pie bias and assumption of the other party’s key interests and priorities
Use simulation to get team members comfortable with conflict. Simulation is a powerful tool for teaching teamwork or interpersonal skills (e.g., Shapiro et al., 2004), including conflict management. Moreover, as long as psychological fidelity (e.g., the degree to which trainees believe the simulation to be a comparable substitute; Rehmann et al., 1995) is high, simulations need not be costly. The design and development of the simulation, however, plays a large role in the efficacy of this intervention (see Table 2 for best practices).
TABLE 2
| Training design | Example | Citation |
|---|---|---|
| Provide conceptual learning- factual knowledge and content about conflict management. Just like any other skill, team behaviors can be taught. Generalizable team behaviors can be transferred to any team. | Provide content around specific conflict management behaviors (e.g., determining the nature of conflict, looking for conflict patterns, understanding your position, considering emotions, creating a safe environment). | Beaubien and Baker (2004) and Overton and Lowry (2013) |
| Role model positive and negative examples. Model effective behaviors reaching the desired outcomes, and ineffective behaviors reaching undesired outcomes to increase motivation to use or avoid certain behaviors. | Before allowing participants to engage in the situation, have a facilitator and actor demonstrate good and bad behaviors in action. | Taylor et al. (2005) |
| Include deliberate practice. Deliberate practice includes focused, repetitive practice with valid measurements that can be used to provide informative feedback. | Using a realistic conflict scenario for your organization, have participants engage in 5 min difficult conversations to practice skills. Allow peers to observe and provide feedback. | McGaghie et al. (2011) |
Simulation best practices.
Decision Making
Research on individual vs. team decision making bears out that teams can outperform individual decision makers in terms of decision accuracy, and that process gains cannot be explained by the most knowledgeable member or even the average level of knowledge across the team (i.e., there’s a synergistic gain; Michaelsen et al., 1989). Given these benefits, there has been ample research on the factors that contribute to accurate, high-quality team decisions. For example, Hollenbeck et al. (1995) identify three individual characteristics that affect decision accuracy, including how informed each individual member of the decision making team is, the validity of individual member recommendations, and the ability of the team leader to weigh recommendations appropriately. Urban et al. (1996) emphasize the importance of the work environment, including time pressure, resource demand, and workload. In working with teams in the field, however, challenges to decision making most often arise when individual team members must combine their expertise and experience to come to a collective decision.
According to Rogers and Blenko (2006), ambiguity in decision making roles and accountability for decisions are the root causes of decisions stalling inside organizations. The authors present the RAPID model that delineates team decision roles, standing for Recommend, Agree, Perform, Input, and Decide. Those who recommend a course of action are responsible for interpreting relevant data and proposing a course of action. Those who provide input present the facts and the practicality or feasibility of different courses of action. Importantly, both of these can be distinct from those who must agree or sign off on a decision before it can move forward. Finally, the person(s) with the authority to decide makes the final decision, and those who perform carry out the decision.
Equally important is clearly defining what level of agreement those with final decision authority need to achieve. Desired level of agreement depends on a number of factors, including level of risk involved, uncertainty or complexity in the environment, and commitment needed to the implementation. Decision consensus occurs when all members with responsibility for making the final decision agree. Often this level of agreement can be time consuming or difficult to achieve. Further, while this level of consensus may be appropriate in some situations, at the extreme level this can result in loss of individual perspectives and groupthink (Janis, 1982). Majority rule occurs when the decision is put to a vote. In teams where power or influence is distributed unequally, majority rule can have a potential for reducing these inequalities (Falk and Falk, 1981). Majority rule can also be used in situations with time constraints or ambiguous, incomplete information; however, this can leave the dissenting group with less commitment to the outcomes. Finally, leader-made decisions occur when a formal or informal leader is solely responsible for the decision. While Holloman and Hendrick (1972) find decision adequacy increases with the direct participation of more group members, the leader must carefully consider the situation (e.g., sensitivity of the data) and constraints (e.g., time pressure).
Case Example: Unclear Decision Roles
Dyad leadership is defined by Sanford (2015) as two people working together as a team to co-lead a specific department, division, or clinical service line. According to the authors, this model consists of two people with different backgrounds (e.g., professional field, training, education, skill sets) that are paired together with the assumption that they can perform above and beyond what either could individually. Importantly, the dyad members do not report to or work for one another; rather, each has their own responsibilities and accountability for their joint work. Oostra (2016) describes how the dyad leadership structure has evolved from a rigid, largely separate dual reporting system to an interdependent, situationally distributed model with shared roles and responsibilities. For this model to be effective, both leaders must draw from each other’s complementary strengths, be included in decision making, and present as a united front supporting and maintaining any decision made. Saxena et al. (2018) found support for this integrated leadership structure, with the majority of dyad leaders indicating that hybrid leadership, with well-defined responsibilities in both individual and shared domains, is preferred. While the majority of respondents agreed joint-decision making was preferable, nearly all endorsed the importance of presenting a united front to healthcare team members.
In this exemplar of a physician and physician assistant (PA) dyad leadership team, ambiguity in decision roles created a strict division in accountability and confusion that permeated throughout the rest of the team. Instead of clearly defining what fell into shared and individual responsibility (i.e., who held the “Decision” role in the RAPID model), the pair had loosely defined the PA leader as the final decision maker on administrative duties, and the physician leader on clinical duties. This left decision authority on a number of issues that cross those domains (e.g., scheduling for the staff, managing performance issues, resource allocation) unclear and the message to the team divided.
The outcomes the team experienced ranged from uncertainty in how to perform their roles to interpersonal conflict and detriments to team morale. Decisions on how policies and procedures (e.g., billing, covering shifts) should be carried out were often decided by one member of the leadership without involvement from the other dyad leader. Sometimes, each leader made a separate decision on the same issue that did not align, and therefore gave conflicting information to team members. The result left team members unsure of how to carry out key functions or carrying out the same function in different ways. Additionally, as team members became aware that they would receive different answers depending on which leader they approached first, they began to approach the leader who most often provided them with the answer they were seeking. As these consequences unfolded, it created a level of interpersonal conflict that began at the leadership level and had a top-down effect on the team’s morale. Because of this uncertainty at the top level, participative decision making was also low and left members unheard or unappreciated. As the leaders grappled with their own accountability, the team was rarely consulted to provide input or recommendation. Ultimately, this dyad leadership team that had the capability of being a successful partnership instead created what Saxena et al. (2018) warn about as the potential dark side of shared leadership—parallel structures of responsibility characterized by power struggles between leaders.
Solutions for Decision Making
Turpin (2019) shared strategies for building a successful dyadic relationship. The relationship must begin with intentional discussion around how decisions will be made, how to engage in effective communication, and how disagreements will be handled. Corroborating the findings of Saxena and colleagues (2016), the authors also emphasize the importance of 1) clarity around roles and responsibilities that are shared and held individually, and 2) presenting a united front. Presenting a united front includes negotiating and debating before, leaving any lingering disagreements solely between the two leaders, and presenting the same message. Finally, acknowledging that in all situations we are sometimes the mentor and sometimes the learner goes a long way toward the leaders recognizing and appreciating each other’s unique expertise. Although in its nascent stages, there is evidence to suggest that leadership training specifically around improving leadership skills (e.g., coaching) and communication in dyad pairs can positively influence team outcomes (e.g., engagement; James, 2017).
Procedural justice is defined by Cropanzano et al. 2001 as employee perception or judgement regarding the fairness of work-related processes. According to the authors, justice perceptions are not necessarily based on a final outcome, but how the outcome was reached (e.g., whether the process to assign an outcome was fair, if an acceptable justification was given). Applied to decision making, Phillips (2002) asserts that one factor that may influence procedural justice is the perceived decision control, or level of influence the leader gives a team member’s input relative to others. In our collective experience with teams in the field, another factor we suggest may influence justice perceptions (above and beyond the final decision outcome) is the transparency or level of clarity around not only decision roles and level agreement (as discussed above), but also the status of the decision-making process and what is and is not included in the decision.
For example, when team members have a different understanding of the intent of a decision making discussion, it can create problems for the team. As a leader or team member tasked with making a final decision, you can avoid confusion and the potential feeling of lack of voice by being clear with your purpose prior to any team discussion. A simple tool to provide clarity around the status of a decision, or where the decision stands in terms of timeline, is the Update-Input-Decide (UID) Framework. For each agenda item, specify the intent: 1) Update (to simply inform the team about progress of plans), 2) seek Input (to request other’s perspective or feedback), or 3) Decide (to make the decision or determine who will make the decision).
As another example, research on Participation in Decision Making (PDM) suggests that greater inclusion of team members, including those with diverse backgrounds and the dissenting minority, can improve decisions outcomes (e.g., creativity), satisfaction with the process, and organizational commitment (Black and Gregersen, 1997; De Dreu and West, 2001; Elele and Fields, 2010). Scott-Ladd and Chan (2004) echo the importance of PDM, however, they note that not all employees will be able to participate at the same level or time, and there will be times when this participation will not be possible (e.g., critical or urgent decisions). In these circumstances, the authors stress the importance of realistic involvement expectations and clear boundaries of when, what, and how employees will contribute. Toward this end, negotiables (i.e., items the team can weigh in on) and non-negotiables (i.e., items decided at a later point or restricted by external circumstances) can help the team avoid confusion, unmet expectations, and wasted time discussing points that are not within decision limits.
Reflecting on Progress
American philosopher, psychologist, and leader in early educational reform John Dewey underscored that while our experiences are an integral part to learning, we truly learn or learn more deeply from reflecting on that experience (Rodgers, 2002). The education and training field emphasizes learning by doing, whether it be “experiential learning”, “active learning”, or “action learning” (e.g., Kolb, 1984; Bell and Kozlowski, 2008). But an often left out piece is that we also learn by reflecting on what we’ve done—what worked, what didn’t work, and what could be done better next time. In this sense reflection deepens learning, it allows us to develop at a faster pace. This is true in an individual setting, and maybe even more important in a team setting where we’re learning not only how to improve and develop ourselves, but where we’re also learning how to interact effectively with others.
At the team level, team reflexivity is defined as the extent to which team members set aside time to specifically reflect upon the team’s objectives and strategies or processes to meet these objectives, as well as the extent to which teams adapt strategies to current or future situations (West and Beyerlein, 2000). This includes taking time out from performing work to pause, reflect, and plan for future success. Reflexivity has been evidenced to predict team effectiveness, creativity, and innovation (e.g., De Dreu, 2006; Tjosvold et al., 2003; Tjosvold et al., 2004). Schippers et al. (2008) argue team reflexivity may be especially beneficial under high levels of work demands (e.g., high patient-to-clinician ratio, time pressure). The authors tested and found support for their hypothesis with 98 multidisciplinary primary health care teams, including physicians, practice managers, nurses, and administrators. Under high demands, teams who reflect gain a greater awareness of these demands and their consequences and the gap between their current and desired state. This in turn focuses attention and team discussion on ideas for new and innovative ways to work.
Recognizing that medical knowledge and technology in healthcare change rapidly (e.g., Densen, 2011), team reflection plays an essential role in effectively implementing continuous change. In investigating healthcare teams undergoing adoption of new technology, Edmondson et al., 2001 found that teams with successful implementation went through a qualitatively different process for team learning. Specifically, the authors found that organization size, resources, support from senior management, and academic status were not associated with implementation success. Instead, success depended on an implementation process that included reflection. Teams were successful when they took the time to collect and review data, initiate discussions with the whole team, go over what happened immediately after an event, set aside regular time to review activities, review errors, and discuss how to change team process to improve in the future.
Case Example: High Work Demands & Time Pressure
The exemplar team for reflecting on progress was comprised of multi-disciplinary clinical professionals, including physicians and staff members, who were highly interdependent. Specifically, they had a team workflow, meaning there was a simultaneous, multidirectional exchange (Saavedra et al., 1993). In order to manage this interdependency in clinical care, Taplin et al. (2015) point to the importance of workflow reappraisal across the team, fostering situational awareness and flexibility, and awareness of the overall operation. As this team was in the process of hiring physicians to bring them up to a full level of staffing, time to engage in these highly important but non-clinical team duties was limited and was not emphasized as a priority, and the factors below served to compound the issue.
According to Emanuele and Koetter (2007), healthcare organizations are constantly facing the challenge of improving quality of care while reducing overall costs. To address this, many are turning to workflow technology as a way to improve efficiency and quality of care in a cost-effective manner. While the authors highlight the many potential benefits (e.g., automated steps, greater access to information when and where it is needed, decision support, integrated care plan), they also acknowledge potential drawbacks, including issues with communication (i.e., access to the technology, overloading members with messages). What we witnessed in this team is the negative impact this technology can have on the quality of communication if the team does not take the dedicated time to reflect and reappraise. This electronic patient management system made the reactions and stress levels of teammates hard to interpret, and there was less opportunity to get questions answered quickly. Perhaps more importantly, there was little opportunity to discuss cases and reflect as a team to learn collectively, surface concerns, and find ways to communicate more effectively.
Furthermore, this technology reduced the need for the team to experience patient cases together, and therefore understand each other’s roles and responsibilities, how the actions of one group affects the work of the other, and the stressors and pressures each groups faces. In short, there was a lack of a shared mental model or clarity around what each group does and thinks (e.g., how long it takes to do certain tasks, the effect of changes to the patient plan) and awareness of how the situation impacts each group. This not only affects operations, such as how tasks are prioritized and the time allotted for tasks, but is also detrimental to team morale and understanding and empathy between team members.
Solutions for Reflecting on Progress
Team coaching, which focuses on helping the team as a whole, is defined as direct interaction with an intact team to help members coordinate, make use of collective resources, and review and refine strategies (Hackman and Wageman, 2005). According to Clutterbuck et al. (2010), an essential piece of team coaching is assisted reflection and analysis. While research is still in its nascent stages, this type of coaching has been evidenced to improve interpersonal teamwork skills (e.g., communication) and team outcomes including effectiveness and innovation (Peters and Carr, 2013; Rousseau et al., 2013). The coaching process allows teams to engage in the reappraisal of team strategies, building of mental models and situational awareness, and awareness of others roles and responsibilities that Taplin et al. (2015) pointed out as essential to managing interdependencies.
Team coaching is often overlooked or given little attention by team leaders. One reason for the underutilization is that leaders don’t understand the process or know how to engage in coaching effectively (Hackman and Wageman, 2005). Fortunately, Brown and Grant (2010) put forth a practical model for team coaching based on the popular GROW (Goal-Reality-Options-Way Forward) model for individual coaching. The extended framework, called GROUP (Goal-Reality-Options-Understand Others-Perform), includes the importance of shifting both individual and group awareness and treating issues at a systemic and not symptom level (i.e., getting to the root cause of performance issues). The authors include example questions for each phase that can be asked by the team leader or a facilitator in an iterative process (e.g., How have you handled problems in the past? What worked? What didn’t?). Drawing from the literature on a similar group process (i.e., team debriefs), teaming coaching sessions may also be more effective when the development, non-punitive, and non-administrative intent is stressed, when teams reflect on specific events rather than general performance or competencies, and when multiple sources of information are used (e.g., multiple team members, objective data source).
Additionally, individual and team assessments can be useful tools to raise each team member’s level of self-awareness, which at the collective level has been shown to influence team functioning (e.g., coordination, conflict, cohesion, and team performance; Dierdoff et al., 2019). These tools can focus on personality, emotional intelligence, 360 feedback or a number of other critical performance areas. In essence, they help an individual become more aware of their own strengths and how they can be leveraged, as well as areas that represent opportunities for development. These tools can also be used for developmental discussions around how a team member interacts with others on the team. At the team level, these tools can be utilized for coaching sessions around team dynamics (e.g., the roles each members contributes to on the team; Driskell et al., 2017).
Coaching and Development
While team coaching can help teams reflect on and improve team processes, individual coaching is foundational to an employee’s personal development plan. Coaching has received considerable attention from the literature (Smither, 2011; Grant, and Hartley, 2013; Bozer, and Jones, 2018), and has been found to be instrumental to employee learning and development (Ladyshewsky, 2010; Liu and Batt, 2010; Jones et al., 2016). The primary function of workplace coaching is to support the coachee in the achievement of professional outcomes they deem important (Smither, 2011; Jones et al., 2016). This involves one-on-one relationships that are developmental in nature, and characterized as goal-focused, collaborative, and reflective (Smither, 2011; Jones et al., 2016). Dasborough et al. (2009) shed light on how differential attention on behalf of leaders can influence team climate, such that when team members perceive that leaders are treating certain members with favoritism this could act as a contagion to the team invoking negative affective responses. We draw upon this evidence to support our argument as to the influence one-on-one relationships can have on team-level challenges in the context of coaching. Specifically, coaching serves as yet another resource that leaders can provide to the team, and lack of this resource can impede employee development and perceptions of fairness.
In healthcare, coaching is of significant importance (Stapleton et al., 2007; Grant et al., 2017; Wolever et al., 2017). The notion of continual development aligns with the overarching mission of healthcare institutions to strive for continual improvement in quality of care and patient safety, and teams often depend on coaching to provide them with opportunities to grow and improve. Specifically, Chatalalsingh and Reeves (2014) emphasize the importance of coaching to inspire collective learning to enhance task-related knowledge and relational aspects of the team. Coaching responsibilities can often reside with leadership and have been regarded as a critical in directing efforts towards developing others (Calhoun et al., 2008). Challenges with many aforementioned outcomes and processes central to the healthcare context can be addressed through effective coaching strategies (Chatalalsingh and Reeves, 2014; Grant, et al., 2009). Coaching can positively impact goal attainment, resilience, morale, and well-being (Stapleton et al., 2007; Grant et al., 2009). Moreover, leader coaching interventions have been found to be effective at enhancing resilience, self-efficacy, and perspective taking among healthcare providers implementing change (Grant et al., 2017).
However, the healthcare industry has faced challenges with coaching, requiring a cultural shift among healthcare organizations to first recognize the value of providing individuals with opportunities to promote their capacity to attain their own professional goals (Thorn and Raj, 2012). Thorn and Raj (2012) identify four core coaching behaviors: 1) be authentic, 2) ask powerful questions, 3) establish trust, and 4) challenge beliefs. In addition, Thorn and Raj (2012) assert that in valuing professional pursuits a leader can enhance performance in teams. Taken together, healthcare is a domain that strives for continual improvement, and in this context, coaching can serve as a linchpin for improvement on the team and individual level. Thus, this work further supports the importance of coaching in healthcare while noting the challenges many organizations face with facilitating coaching-centered relationships.
Case Example: Lack of Leader Accessibility
Leader accessibility, defined in part by approachability and commitment, has been identified as a top quality of effective leaders (Olanrewaju and Okorie, 2019). This exemplar team, which performed a critical regulatory function within the institution, depicts the consequences of lack of accessibility on employee perception of coaching and development. Importantly, lack of accessibility may have little to do with individual leader characteristics and can be a result of external factors inherent in the field of medicine (e.g., time pressure, heavy workloads) and leadership needs of the institution. However, these factors may not be readily perceptible to the team and can engender perceptions of leader unfairness. If leader accessibility is limited or unequal across members, then the attention leaders devote to certain members of the team could be perceived by other members of the team as being exclusionary, negatively impacting overall team climate (Dasborough et al., 2009).
This exemplar team had experienced frequent changes in leadership over the previous five years. As research bears out, while a change in leadership can enhance team reflection and adaption (Kalmanovich-Cohen et al., 2018), frequent changes in leadership can add to the perception of a lack of coaching and development. In addition, the executive leader of the team had their role expanded to meet the needs of the institution. This left the mid-level manager in charge of implementing new technology that was being integrated into the team’s process as well as the day-to-day functions of the team, requiring they block their schedule to complete a heavy workload—and furthering the perceptions of lack of leader accessibility.
Team members experienced a number of missed opportunities for development. Broadly, these consisted of a general lack of one-on-one meetings with leadership and an absence of feedback on work-related activities and progress. Unfortunately, there were many areas that the team would have benefited from either protected meeting time or feedback. For example, in terms of affect and morale, team members showed considerable concern regarding negative external perceptions of their team; they felt that others in the department did not respect them and voiced their aspiration to change these perceptions. This is a situation where a developmental opportunity allowing them to improve inter-departmental dynamics as well as their collective efficacy was deprived as a result of lack of one-on-one meetings with leadership to address these concerns through coaching. Members also expressed an inclination to improve upon their work and an overall growth mindset; however, this served as another missed opportunity wherein feedback and development was not prioritized and therefore not provided to them.
Solutions for Coaching and Development
To address these challenges, we offer two readily implementable potential solutions: leader–member meetings and creating protected time before meetings to check in with members and build rapport. While we acknowledge that time is a scarce resource in healthcare, oftentimes one-on-one meetings can take place in 15 minutes or less and can be as infrequent as once a month. However, we would encourage leaders to discuss temporal needs amongst their team to ascertain the ideal length and frequency of one-on-one meetings to ensure that the team’s learning and developmental needs are adequately addressed.
Given time constraints, exercises that build familiarity with developmental goals (i.e., “get to know you” exercises) can also take place in shorter durations (e.g., 10 minutes), and could precede regular meetings. The purpose of these exercises would be to give team members an opportunity to share professional goals and aspirations with both the leader and the team. This could later be leveraged by the leader during one-on-one meetings to provide members with learning and developmental opportunities that align with their goals. Finally, researchers have generated evidence-based and theoretically grounded steps to guide coaching efforts: 1) pre-coaching (e.g., identify expectations), 2) self-discovery and awareness (e.g., determine follower motivation(s), needs, and approach to achievement of results), 3) goal setting and accountability (e.g., agree upon goals and objectives), 4) action learning and execution (e.g., provide developmental activities and feedback), and 5) evaluation and revision (e.g., continue to provide feedback and evaluate progress; Harper, 2012).
The effectiveness of these solutions relies heavily on the level of buy-in and commitment from leadership; without this commitment, these efforts could lack follow-through. Hence, prior to the implementation of coaching efforts, it is critical to ascertain this information (i.e., leadership buy-in and commitment). This can be accomplished through a set of structured interview questions prior to the launch of any effort and will help shape expectations and strategies for improvement up front. For example, a leader can be asked if they have the bandwidth to make themselves available to their team and carry out some of these potential solutions. If the leader expresses that they are not available, an important follow-up response to this would be to have the leader identify someone who can champion the implementation of these solutions. Relatedly, it is equally important to present an accurate depiction of what these efforts could entail to the leader to facilitate informed decision making.
Discussion
In this investigation into healthcare team effectiveness, we provided a comprehensive, evidence-based framework that is generalizable across team types. The findings reveal that teams in healthcare face similar challenges, regardless of whether they operate in the clinical, research, or administrative realm. Qualitative inquiry was used to provide rich detail about how each one of these challenges may manifest in the field and the impact of these challenges on team outcomes including performance, functioning, and viability. Finally, we pulled from the literature on team science and our collective experience in the field to provide potential solutions to address these challenges.
Qualitative data analysis made evident the numerous factors, internal and external to the team, that can influence effectiveness, emphasizing that a team of experts does not automatically create an expert team. The healthcare environment itself is characterized by high workloads, time pressure, and continuous change (e.g., new technology, new organizational structures) that can have a top-down effect on how teams perform. At the team level, combining the expertise necessary to tackle the complex and ambiguous problems that healthcare teams often face represents a significant barrier. Finally, characteristics of the team members themselves, including personality and communication or conflict style can create further barriers, even when members are passionate, talented, and working toward the same goal. The solutions presented help teams manage these challenges that manifest across different levels and emphasize the importance of targeting the root cause (and not the symptom) of team issues. They center on being intentional about setting up and carrying through team processes, setting aside dedicated time to develop the team, and practicing team skills just as you would technical skills.
Practical Implications
The Team Effectiveness Framework was designed to inform both research and practice, and as such presents three unique contributions for those that lead and develop teams. First, it is generally applicable across the many types of teams that contribute to the quality and safety of patient care. The development of this framework synthesized literature on teamwork competencies and overall team effectiveness across multiple disciplines within healthcare. This synthesis was bolstered by both quantitative and qualitative analyses of healthcare teams across multiple domains embedded in a larger healthcare organization. The integration of two metrics that capture different aspects of team dynamics, and challenges teams face as a result of breakdowns in teamwork as they occur in different healthcare settings, support the ecological validity of our findings and the applicability of our framework throughout the entire system. Additionally, this supports the practical utility of our framework in that it can be used as a common language or message about team effectiveness across the organization. It can also serve as a solid foundation for any team training program.
Second, the framework is structured to reflect a scaffolded process towards the development of ideal team states, such that each level builds upon the preceding one. The lowest level comprises competencies that provide the foundation and shape emergent attitudes, behaviors, and cognitions. If the team feels, acts, and thinks (i.e., the ABCs of teamwork; Weaver et al., 2010) in accordance with the framework this facilitates the development of ideal team states of psychological safety and trust, and adaptability and resilience. These states are what are ultimately needed in order for the team to successfully perform and accomplish shared goals at present (performance and results) and possess the capacity to continue working together effectively in the future (viability), thereby enabling overall team effectiveness.
Finally, the framework can provide guidance for when and where to target developmental efforts. As discussed, the framework’s hierarchical nature is structured such that each level is dependent on the preceding one, and within each level the competencies are clearly defined. This provides a blueprint leaders and practitioners can use to diagnose challenges and determine where interventions are needed. Specifically, given the scarcity of resources that often faces healthcare teams (e.g., time, financial resources), a team effectiveness measurement tool can guide efforts and maximize effects of any intervention. The potential solutions we generate to address challenges as they arise provide additional insight for leaders and practitioners to tailor their efforts to address the team’s unique needs and determine approaches to improving overall team effectiveness.
The team diagnostic used in this effort, like any cross-sectional measure, is based on a point in time and the framework includes elements that should be monitored on an ongoing basis. Membership changes, or team member fluidity, are quite common in healthcare (e.g., shift changes, membership loss and replacement). As membership changes, it can be helpful to re-assess the team on the framework components. However, in general, teams should be trained on transportable or generalizable teamwork skills (e.g., sharing just enough of the right information, shared leadership) to enable effective adaptation and resiliency throughout membership changes (Bedwell et al., 2012). As specific developmental interventions are conducted overtime, a re-assessment can help clarify if the intended improvements have resulted.
Limitations
The present research effort took place in a larger academic-teaching hospital, thus presenting contextual limitations to the generalizability of our findings and framework. Academic medical institutions are a unique environment in the healthcare domain, and it is the aim of this effort to generalize this framework across institutions. As such, we encourage future research to replicate these findings across different healthcare institutions and care settings. In the same vein, the focal institution was larger in size, warranting needs for replicability across different institution sizes. Size can present an important boundary condition to teams operating as components of a larger system (i.e., teams nested within teams working towards a shared goal). Hence, institutional size could influence the present findings. From a different perspective, our effort does not account for the “nestedness” of teams in larger systems, referred to as multiteam systems (MTSs), which involve collectives of teams working towards a shared goal (Mathieu et al., 2001). It would be both interesting and valuable for future research to expand upon this framework to consider multidisciplinary teams in the context of MTSs.
Future Research
While there have been several reviews of the efficacy of team training or TDIs in healthcare (e.g., Weaver et al., 2014; Hughes et al., 2016), empirical studies have focused largely on clinical teams. While there is no doubt teams with direct patient care responsibilities greatly influence critical outcomes for healthcare organizations (e.g., patient safety, quality of care), research and administrative teams often directly or indirectly influence patient outcomes as well. For example, organizational development teams that train clinical leaders to better manage their teams ultimately impact how these teams care for the patient. Non-clinical teams also play a key role in keeping the organization operating smoothly, including the management of clinical trials, ensuring regulatory guidelines are followed, and caring for the health and well-being of employees. While the competencies that are important for teams across different functions remain the same, how to effectively engage in teamwork (e.g., communication, coordination) may look very different depending on team characteristics like skill differentiation, authority differentiation, and temporal stability (Hollenbeck et al., 2012). For example, effective communication norms of an operating room team, with the surgeon as a clear leader and high skill differentiation between members (e.g., anesthesiologists, nurses, surgical techs), will look very different than that of a more homogenous team managing employee recruitment. Because of this, more research is needed into the efficacy of different training interventions for non-clinical healthcare teams.
Specific developmental interventions have gained more attention in recent years, one of which that stands out is individual leader and team coaching. The benefits of coaching have been touted to be everything from increased goal attainment, professional growth, improved interpersonal relationships, improved productivity, and greater resilience, but strong empirical evidence lags far behind the use of coaching in the field (Jones et al., 2016). This issue is even greater for investigations into team coaching. While there are many practical resources for team coaching best practices (e.g., Thorton, 2010; Hawkins, 2017), more empirical research into overall effectiveness and the specific techniques that work best, the length of engagements, the impact of team types, and specific desired outcomes that are most amenable to coaching is needed.
Finally, as the dyad leadership structure becomes more prevalent in healthcare, leadership training best practices specific to this group are needed. As a starting point, research on the training needs of the dyadic pair and the development of a competency model (essentially, what makes a dyadic pair effective) could help inform leadership development programs. As dyadic pairs can take many forms (e.g., physician and registered nurse, physician and operations manager), uncovering the challenges specific to each of these team types would also move research forward. Finally, the enabling conditions, or what the dyadic pair needs from the organization and environment in which they operate, can add to the overall picture of dyadic leadership team effectiveness.
The very nature of teamwork gives rise to complex, dynamic processes that arise over time from the interactions of team members. While the field of team science has made tremendous progress over the last several decades, researchers note that to move forward we need to “embrace the complexity” of current team-based designs (Mathieu, et al., 2008). Therefore, we encourage future research to look beyond the methodologies traditionally used in teams research and to seek underutilized approaches that may be able to further advance our understanding of multidisciplinary teams in healthcare (e.g., integrated qualitative and quantitative research paradigms, participatory action research (PAR); Baum et al., 2006; Paoletti et al., 2021).
Statements
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by University of Texas MD Anderson IRB Committee. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
SZ, CH, ES, and ST all contributed to the activities related to the development of the framework. SZ and CH developed the diagnostic tool. SZ conducted interviews and debriefs for follow-up to the diagnostic tool. AW contributed substantially to data analysis and manuscript development/writing. All authors contributed to the development, writing, and review of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1
Allred K. G. (1997). “Conflict management.” in What works: training and development practices, Editors BassiL. J.Russ-EftD., (Alexandria, VA: American Society for Training & Development), 27–50.
2
Balogun J. (2003). From blaming the middle to harnessing its potential: Creating change intermediaries. Br. J. Manag.14(1), 69–83. 10.1111/1467-8551.00266
3
Barrick M. R. Stewart G. L. Neubert M. J. Mount M. K. (1998). Relating member ability and personality to work-team processes and team effectiveness. J. Appl. Psychol.83, 377–391. 10.1037/0021-9010.83.3.377
4
Baum F. MacDougall C. Smith D. (2006). Participatory action research. J. Epidemiol. Community Health.60 (10), 854–857. 10.1136/jech.2004.028662
5
Beaubien J. M. Baker D. P. (2004). The use of simulation for training teamwork skills in health care: how low can you go?. BMJ Qual. Saf.13 (suppl 1), i51–i56. 10.4324/9781315243092-22
6
Bedwell W. L. Ramsay P. S. Salas E. (2012). Helping fluid teams work: a research agenda for effective team adaptation in healthcare. Trans. Behav. Med.2 (4), 504–509. 10.1007/s13142-012-0177-9
7
Behfar K. J. Peterson R. S. Mannix E. A. Trochim W. M. (2008). The critical role of conflict resolution in teams: a close look at the links between conflict type, conflict management strategies, and team outcomes. J. Appl. Psychol.93 (1), 170–188. 10.1037/0021-9010.93.1.170
8
Bell S. K. Delbanco T. Anderson-Shaw L. McDonald T. B. Gallagher T. H. (2011). Accountability for medical error: moving beyond blame to advocacy. Chest140 (2), 519–526. 10.1378/chest.10-2533
9
Bell S. Kozlowski S. W. (2008). Active learning: effects of core training design elements on self-regulatory processes, learning, and adaptability. J. Appl. Psychol.93 (2), 296–316. 10.1037/0021-9010.93.2.296
10
Bell S. T. Brown S. G. Colaneri A. Outland N. (2018). Team composition and the ABCs of teamwork. Am. Psychol.73 (4), 349–362. 10.1037/amp0000305
11
Bell S. T. Marentette B. J. (2011). Team viability for long-term and ongoing organizational teams. Organizational Psych. Review1 (4), 275–292. 10.1177/2041386611405876
12
Black J. S. Gregersen H. B. (1997). Participative decision-making: an integration of multiple dimensions. Hum. Relat.50 (7), 859–878. 10.1177/001872679705000705
13
Bowers C. A. Braun C. C. Morgan B. B. Jr. (1997). “Team workload: its meaning and measurement.” in Team performance and measurement: theory, methods, and applications. Editors BrannickM. T.SalasE.PrinceC., (Mahwah, NJ: Lawrence Erlbaum Associates), 85–108.
14
Bozer G. Jones R. J. (2018). Understanding the factors that determine workplace coaching effectiveness: a systematic literature review. Eur. J. Work. Organ. Psychol.27(3), 342–361. 10.1080/1359432X.2018.1446946
15
Bregman P. (2016). The right way to hold people accountable. Harv. Bus. Rev.Available at: https://hbr.org/2016/01/the-right-way-to-hold-people-accountable.
16
Brown A. Dickinson H. Kelaher M. (2018). Governing the quality and safety of healthcare: a conceptual framework. Soc. Sci. Med.202, 99–107. 10.1016/j.socscimed.2018.02.020
17
Brown J. Lewis L. Ellis K. Stewart M. Freeman T. R. Kasperski M. J. (2011). Conflict on interprofessional primary health care teams “can it be resolved?. J. Interprof. Care25 (1), 4–10. 10.3109/13561820.2010.497750
18
Brown S. W. Grant A. M. (2010). From GROW to GROUP: theoretical issues and a practical model for group coaching in organisations. Coaching3 (1), 30–45. 10.1080/17521880903559697
19
Bushe G. R. Coetzer G. H. (2007). Group development and team effectiveness: using cognitive representations to measure group development and predict task performance and group viability. J. Appl. Behav. Sci.43 (2), 184–212. 10.1177/0021886306298892
20
Calhoun J. G. Dollett L. Sinioris M. E. Wainio J. A. Butler P. W. Griffith J. R. et al (2008). Development of an interprofessional competency model for healthcare leadership. J. Healthc. Manag.53 (6), 375–390. 10.1097/00115514-200811000-00006
21
Chatalalsingh C. Reeves S. (2014). Leading team learning: what makes interprofessional teams learn to work well?. J. Interprof. Care28 (6), 513–518. 10.3109/13561820.2014.900001
22
Chen G. Sharma P. N. Edinger S. K. Shapiro D. L. Farh J. L. (2011). Motivating and demotivating forces in teams: cross-level influences of empowering leadership and relationship conflict. J. Appl. Psychol.96 (3), 541–557. 10.1037/a0021886
23
Ciccarelli D. (2016). Start, stop, continue tutorial. New York, NY: Forbes, Available at:https://www.forbes.com/sites/groupthink/2016/02/02/start-stop-continue-tutorial/?sh=5c1752c22798.
24
Clutterbuck D. (2010). “Team coaching.” in The complete handbook of coaching Editors CoxE.BachkirovaT.ClutterbuckD., (London, UK: Sage Publications), 271–283.
25
Cropanzano R. Byrne Z. S. Bobocel D. R. Rupp D. E. (2001). Moral virtues, fairness heuristics, social entities, and other denizens of organizational justice. J. Vocat. Behav.58 (2), 164–209. 10.1006/jvbe.2001.1791
26
Dasborough M. T. Ashkanasy N. M. Tee E. Y. Herman H. M. (2009). What goes around comes around: how meso-level negative emotional contagion can ultimately determine organizational attitudes toward leaders. Leader. Q.20 (4), 571–585. 10.1016/j.leaqua.2009.04.009
27
De Dreu C. K. West M. A. (2001). Minority dissent and team innovation: the importance of participation in decision making. J. Appl. Psychol.86 (6), 1191–1201. 10.1037/0021-9010.86.6.1191
28
De Dreu C. K. (2006). When too little or too much hurts: evidence for a curvilinear relationship between task conflict and innovation in teams. J. Manag.32 (1), 83–107. 10.1177/0149206305277795
29
DeChurch L. A. Marks M. A. (2001). Maximizing the benefits of task conflict: the role of conflict management. Int. J. Conflict Manag.12 (1) 4–22. 10.1108/eb022847
30
DeChurch L. A. Mesmer-Magnus J. R. Doty D. (2013). Moving beyond relationship and task conflict: toward a process-state perspective. J. Appl. Psychol.98 (4), 559–578. 10.1037/a0032896
31
Densen P. (2011). Challenges and opportunities facing medical education. Trans. Am. Clin. Climatol. Assoc.122, 48–58.
32
Dierdorff E. C. Fisher D. M. Rubin R. S. (2019). The power of percipience: consequences of self-awareness in teams on team-level functioning and performance. J. Manag.45 (7), 2891–2919. 10.1177/0149206318774622
33
Driskell T. Driskell J. E. Burke C. S. Salas E. (2017). Team roles: a review and integration. Small Group Res.48 (4), 482–511. 10.1177/1046496417711529
34
Edmondson A. C. Bohmer R. M. Pisano G. P. (2001). Disrupted routines: team learning and new technology implementation in hospitals. Adm. Sci. Q.46 (4), 685–716. 10.2307/3094828
35
Edmondson A. (1999). Psychological safety and learning behavior in work teams. Adm. Sci. Q.44 (2), 350–383. 10.2307/2666999
36
Edwards M. Hulme D. (1996). Too close for comfort? The impact of official aid on nongovernmental organizations. World Dev.24 (6), 961–973. 10.1016/0305-750X(96)00019-8
37
Elele J. Fields D. (2010). Participative decision making and organizational commitment. Cross Cult. Manag.: Int. J.17 (4), 368–392. 10.1108/13527601011086586
38
Emanuele J. Koetter L. (2007). Workflow opportunities and challenges in healthcare. BPM & Workflow Handbook1, 157–166.
39
Falk G. Falk S. (1981). The impact of decision rules on the distribution of power in problem-solving teams with unequal power. Group Organ. Stud.6 (2), 211–223. 10.1177/105960118100600207
40
Fernandez R. Kozlowski S. W. Shapiro M. J. Salas E. (2008). Toward a definition of teamwork in emergency medicine. Acad. Emerg. Med.15 (11), 1104–1112. 10.1111/j.1553-2712.2008.00250.x
41
Fleissig A. Jenkins V. Catt S. Fallowfield L. (2006). Multidisciplinary teams in cancer care: are they effective in the UK?. Lancet Oncol.7 (11), 935–943. 10.1016/S1470-2045(06)70940-8
42
Frink D. D. Klimoski R. J. (1998). Toward a theory of accountability in organizations and human resource management. Res. Person. Hum. Resour. Manag.17, 1–51.
43
Grant A. M. Curtayne L. Burton G. (2009). Executive coaching enhances goal attainment, resilience and workplace well-being: a randomised controlled study. J. Posit. Psychol.4 (5), 396–407. 10.1080/17439760902992456
44
Grant A. M. Hartley M. (2013). Developing the leader as coach: insights, strategies and tips for embedding coaching skills in the workplace. Coaching6 (2), 102–115. 10.1080/17521882.2013.824015
45
Grant A. M. Studholme I. Verma R. Kirkwood L. Paton B. O’Connor S. (2017). The impact of leadership coaching in an Australian healthcare setting. J. Health Organ. Manag.31 (2) 237–252. 10.1108/JHOM-09-2016-0187
46
Hackman J. R. (2012). From causes to conditions in group research. J. Organ. Behav.33 (3), 428–444. 10.1002/job.1774
47
Hackman J. R. Wageman R. (2005). A theory of team coaching. Acad. Manag. Rev.30 (2), 269–287. 10.5465/amr.2005.16387885
48
Hackman J. R. (1987). “The design of work teams.” in Handbook of organizational behavior. Editor LorschW., (Upper Saddle River, NJ: Prentice Hall), 315–342.
49
Hall P. (2005). Interprofessional teamwork: professional cultures as barriers. J. Interprof. Care19 (Suppl. 1), 188–196. 10.1080/13561820500081745
50
Harper S. (2012). The leader coach: a model of multi-style leadership. J. Pract. Consult.4 (1), 22–31.
51
Haward R. (2008). “Organizing a comprehensive framework for cancer control.” in Responding to the challenge of cancer in Europe Editors AlexeM.AlbrehtT.McKeeM.ColemanM. P. (Ljubljana, Slovenia: Institute of Public Health of the Republic of Slovenia and European Observatory on Health Systems and Policies (EOHSP)), 113–134.
52
Hawkins P. (2017). Leadership team coaching: Developing collective transformational leadership. London, UK: Kogan Page Publishers.
53
Hollenbeck J. R. Beersma B. Schouten M. E. (2012). Beyond team types and taxonomies: a dimensional scaling conceptualization for team description. Acad. Manag. Rev.37 (1), 82–106. 10.5465/amr.2010.0181
54
Hollenbeck J. R. Ilgen D. R. Sego D. J. Hedlund J. Major D. A. Phillips J. (1995). Multilevel theory of team decision making: decision performance in teams incorporating distributed expertise. J. Appl. Psychol.80 (2), 292–316. 10.1037/0021-9010.80.2.292
55
Holloman C. R. Hendrick H. W. (1972). Adequacy of group decisions as a function of the decision-making process. Acad. Manag. J.15 (2), 175–184. 10.5465/254909
56
Hughes A. M. Gregory M. E. Joseph D. L. Sonesh S. C. Marlow S. L. Lacerenza C. N. et al (2016). Saving lives: a meta-analysis of team training in healthcare. J. Appl. Psychol.101 (9), 1266–1304. 10.1037/apl0000120
57
James L. (2017). Improving leadership communication in nurse-physician dyad teams. [Doctoral dissertation], Columbia, SC: University of South Carolina. Available at:https://scholarcommons.sc.edu/etd/4460
58
Janis I. L. (1982). Groupthink (2nd ed.). Boston, MA: Houghton-Mifflin.
59
Janssen O. Van de Vliert E. Veenstra C. (1999). How task and person conflict shape the role of positive interdependence in management teams. J. Manag.25 (2), 117–141. 10.1016/S0149-2063(99)80006-3
60
Jehn K. A. (1999). Diversity, conflict, and team performances summary of program of research. Perform. Improv. Q.12 (1), 6–19. 10.1111/j.1937-8327.1999.tb00112.x
61
Jones R. J. Woods S. A. Guillaume Y. R. (2016). The effectiveness of workplace coaching: a meta analysis of learning and performance outcomes from coaching. J. Occup. Organ. Psychol.89 (2), 249–277. 10.1111/joop.12119
62
Kalmanovich-Cohen H. Pearsall M. J. Christian J. S. (2018). The effects of leadership change on team escalation of commitment. Leader. Q.29 (5), 597–608. 10.1016/j.leaqua.2018.03.004
63
Katzenbach J. R. Smith D. K. (2005). The discipline of teams. Harv. Bus. Rev.83 (7), 11–120.
64
Kolb D. A. (1984). Experiential learning. Englewood Cliffs, NJ: Prentice-Hall.
65
Kozlowski S. W. J. Klein K. J. (2000). “A multilevel approach to theory and research in organizations: contextual, temporal, and emergent processes.” in Multilevel theory, research and methods in organizations: foundations, extensions, and new directions. Editors KleinK. J.KozlowskiS. W. J., (San Francisco, CA: Jossey-Bass). 3–90.
66
Ladyshewsky R. K. (2010). Building competency in the novice allied health professional through peer coaching. J. Allied Health39 (2), 77E–82E.
67
Leggat S. G. (2007). Effective healthcare teams require effective team members: defining teamwork competencies. BMC Health Serv. Res.7 (1), 17. 10.1186/1472-6963-7-17
68
Lemieux-Charles L. McGuire W. L. (2006). What do we know about health care team effectiveness? A review of the literature. Med. Care Res. Rev.63 (3), 263–300. 10.1177/1077558706287003
69
Lencioni P. M. (2012). The five dysfunctions of a team: team assessment. Hoboken, NJ: John Wiley & Sons. 10.1108/k.2011.06740aae.002
70
LePine J. A. Piccolo R. F. Jackson C. L. Mathieu J. E. Saul J. R. (2008). A meta analysis of teamwork processes: tests of a multidimensional model and relationships with team effectiveness criteria. Person. Psychol.61 (2), 273–307. 10.1111/j.1744-6570.2008.00114.x
71
Liu X. Batt R. (2010). How supervisors influence performance: a multilevel study of coaching and group management in technology mediated services. Person. Psychol.63 (2), 265–298. 10.1111/j.1744-6570.2010.01170.x
72
Manser T. (2009). Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol. Scand.53 (2), 143–151. 10.1111/j.1399-6576.2008.01717.x
73
Mathieu J. E. Marks M. A. Zaccaro S. J. (2001). “Multi-team systems.” in Handbook of industrial, work and organizational psychology Editors AndersonN.OnesD. S.SinangilH. K.ViswesvaranC., (London, UK: Sage), Vol. 2, 289–313.
74
Mathieu J. Maynard M. T. Rapp T. Gilson L. (2008). Team effectiveness 1997-2007: A review of recent advancements and a glimpse into the future. J. Manag.34 (3), 410–476. 10.1177/0149206308316061
75
McGaghie W. C. Issenberg S. B. Cohen M. E. R. Barsuk J. H. Wayne D. B. (2011). Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad. Med.86 (6), 706–711. 10.1097/ACM.0b013e318217e119
76
Merién A. E. R. Van de Ven J. Mol B. W. Houterman S. Oei S. G. (2010). Multidisciplinary team training in a simulation setting for acute obstetric emergencies: a systematic review. Obstet. Gynecol.115 (5), 1021–1031. 10.1097/AOG.0b013e3181d9f4cd
77
Michaelsen L. K. Watson W. E. Black R. H. (1989). A realistic test of individual versus group consensus decision making. J. Appl. Psychol.74 (5), 834–839. 10.1037/0021-9010.74.5.834
78
Ogbonnaya C. Tillman C. J. Gonzalez K. (2018). Perceived organizational support in health care: the importance of teamwork and training for employee well-being and patient satisfaction. Group Organ. Manag.43 (3), 475–503. 10.1177/1059601118767244
79
Olanrewaju O. I. Okorie V. N. (2019). Exploring the qualities of a good leader using principal component analysis. J. Eng. Proj. Prod. Manag.9 (2), 142–150. 10.2478/jeppm-2019-0016
80
Oostra R. D. (2016). Physician leadership: a central strategy to transforming healthcare. Front. Health Serv. Manag.32 (3), 15–26. 10.1097/01974520-201601000-00003
81
Overton A. R. Lowry A. C. (2013). Conflict management: difficult conversations with difficult people. Clin. Colon Rectal Surg.26 (4), 259–264. 10.1055/s-0033-1356728
82
Paoletti J. Bisbey B. Zajac S. Waller M. J. Salas E. (2021). Looking to the middle of the qualitative-quantitative spectrum for integrated mixed methods. Small Group Research, 1–35. 10.1177/1046496421992433
83
Peters J. Carr C. (2013). Team effectiveness and team coaching literature review. Coaching6 (2), 116–136. 10.1080/17521882.2013.798669
84
Phillips J. M. (2002). Antecedents and consequences of procedural justice perceptions in hierarchical decision-making teams. Small Group Res.33 (1), 32–64. 10.1177/104649640203300102
85
Rabøl L. I. Andersen M. L. Østergaard D. Bjørn B. Lilja B. Mogensen T. (2011). Descriptions of verbal communication errors between staff. An analysis of 84 root cause analysis-reports from Danish hospitals. BMJ Qual. Saf.20 (3), 268–274. 10.1136/bmjqs.2010.040238
86
Rehmann A. J. Mitman R. D. Reynolds M. C. (1995). A handbook of flight simulation fidelity requirements for human factors research. AFB, OH: Crew System Ergonomics Information Analysis Center Wright-Patterson.
87
Rodgers C. (2002). Defining reflection: another look at John Dewey and reflective thinking. Teach. Coll. Rec.104 (4), 842–866. 10.1111/1467-9620.00181
88
Rogers P. Blenko M. (2006). Who has the d?. Harv. Bus. Rev.84 (1), 52–61.
89
Rousseau V. Aubé C. Tremblay S. (2013). Team coaching and innovation in work teams. Leader. Organ. Dev. J.34 (4), 344–364. 10.1108/LODJ-08-2011-0073
90
Rubin J. Z. (1994). Models of conflict management.J. Soc.50 (1), 33–45.
91
Saavedra R. Earley P. C. Van Dyne L. (1993). Complex interdependence in task- performing groups. J. Appl. Psychol.78(1), 61–72. 10.1037/0021-9010.78.1.61
92
Salas E. DiazGranados D. Klein C. Burke C. S. Stagl K. C. Goodwin G. F. et al (2008). Does team training improve team performance? A meta-analysis. Hum. Factors50 (6), 903–933. 10.1518/001872008X375009
93
Salas E. Kosarzycki M. P. Tannenbaum S. I. Carnegie D. (2004). “Principles and advice for understanding and promoting effective teamwork in organizations.” in, Leading in turbulent times: managing in the new world of work. Editors BurkeR.CooperC.Malden, MA: Blackwell). 95–120.
94
Salas E. Priest H. A. Stagl K. C. Sims D. E. Burke C. S. (2007). “Work teams in organizations: a historical reflection and lessons learned.” in Historical perspectives in industrial and organizational psychology. Editor KoppesL. L., (Mahwah, NJ: Lawrence Erlbaum Associates Publishers), 407–438.
95
Salas E. Reyes D. L. Woods A. L. (2017). “The assessment of team performance: observations and needs.” in Innovative assessment of collaboration. Editors von DavierA.ZhuM.KyllonenP. (Cham., Switzerland: Springer), 21–36. 10.1007/978-3-31933261-1_2
96
Sanford K. (2015). Dyad leadership in healthcare: when one plus one is greater than two. Philadelphia, PA: Lippincott Williams & Wilkins.
97
Saxena A. Davies M. Philippon D. (2018). Structure of health-care dyad leadership: an organization’s experience. Leader. Health Serv.31 (2), 238–253. 10.1108/LHS-12-2017-0076
98
Schippers M. C. Den Hartog D. N. Koopman P. L. Van Knippenberg D. (2008). The role of transformational leadership in enhancing team reflexivity. Hum. Relat.61 (11), 1593–1616. 10.1177/0018726708096639
99
Schmutz J. Manser T. (2013). Do team processes really have an effect on clinical performance? A systematic literature review. Br. J. Anaesth.110 (4), 529–544. 10.1093/bja/aes513
100
Scott Ladd B. Chan C. C. (2004). Emotional intelligence and participation in decision making: strategies for promoting organizational learning and change. Strat. Change13 (2), 95–105. 10.1002/jsc.668
101
Shapiro M. J. Morey J. C. Small S. D. Langford V. Kaylor C. J. Jagminas L. et al (2004). Simulation based teamwork training for emergency department staff: does it improve clinical team performance when added to an existing didactic teamwork curriculum?. BMJ Qual. Saf.13 (6), 417–421. 10.1136/qshc.2003.005447
102
Shaw J. D. Zhu J. Duffy M. K. Scott K. L. Shih H. A. Susanto E. (2011). A contingency model of conflict and team effectiveness. J. Appl. Psychol.96 (2), 391–400. 10.1037/a0021340
103
Smither J. W. (2011). Can psychotherapy research serve as a guide for research about executive coaching? An agenda for the next decade. J. Bus. Psychol.26 (2), 135–145. 10.1007/s10869-011-9216-7
104
Somech A. Desivilya H. S. Lidogoster H. (2009). Team conflict management and team effectiveness: the effects of task interdependence and team identification. J. Organ. Behav.30 (3), 359–378. 10.1002/job.537
105
Stapleton P. Henderson A. Creedy D. K. Cooke M. Patterson E. Alexander H. et al (2007). Boosting morale and improving performance in the nursing setting. J. Nurs. Manag.15 (8), 811–816. 10.1111/j.13652934.2007.00745.x
106
Sundstrom E. De Meuse K. P. Futrell D. (1990). Work teams: applications and effectiveness. Am. Psychol.45 (2), 120–133. 10.1037/0003-066X.45.2.120
107
Taplin S. H. Weaver S. Chollette V. Marks L. B. Jacobs A. Schiff G. et al (2015). Teams and teamwork during a cancer diagnosis: interdependency within and between teams. J. Oncol. Pract.11 (3), 231–238. 10.1200/JOP.2014.003376
108
Taplin S. H. Weaver S. Salas E. Chollette V. Edwards H. M. Bruinooge S. S. et al (2015). Reviewing cancer care team effectiveness. J. Oncol. Pract.11 (3), 239–246. 10.1200/JOP.2014.003350
109
Taylor P. J. Russ-Eft D. F. Chan D. W. (2005). A meta-analytic review of behavior modeling training. J. Appl. Psychol.90 (4), 692–709. 10.1037/0021-9010.90.4.692
110
Thomas E. J. Sexton J. B. Helmreich R. L. (2004). Translating teamwork behaviours from aviation to healthcare: development of behavioural markers for neonatal resuscitation. BMJ Qual. Saf.13 (Suppl. 1), i57–i64. 10.1136/qshc.2004.009811
111
Thoms P. Dose J. J. Scott K. S. (2002). Relationships between accountability, job satisfaction, and trust. Hum. Resour. Dev. Q.13 (3), 307–323. 10.1002/hrdq.1033
112
Thorn P. M. Raj J. M. (2012). A culture of coaching: achieving peak performance of individuals and teams in academic health centers. Acad. Med.87 (11), 1482–1483. 10.1097/ACM.0b013e31826ce3bc
113
Thornton C. (2010). Group and team coaching: the essential guide. Abingdon, UK: Routledge.
114
Tjosvold D. Hui C. Yu Z. (2003). Conflict management and task reflexivity for team in-role and extra-role performance in China. Int. J. Conflict Manag.14 (2), 141–163. 10.1108/eb022895
115
Tjosvold D. Tang M. M. L. West M. A. (2004). Reflexivity for team innovation in China: the contribution of goal interdependence. Group & Organizational Management29 (5), 540–559. 10.1177/1059601103254911
116
Tripathy D. (2003). Multidisciplinary care for breast cancer: barriers and solutions. Breast J.9 (1), 60–63. 10.1046/j.1524-4741.2003.09118.x
117
Turpin C. (2019). The dyad leadership model: defining a new physician/nurse relationship (Publication no. 22617608). [Doctoral dissertation]. Victoria, Canada: Royal Roads University.
118
Urban J. M. Weaver J. L. Bowers C. A. Rhodenizer L. (1996). Effects of workload and structure on team processes and performance: implications for complex team decision making. Hum. Factors38 (2), 300–310. 10.1177/001872089606380210
119
Vaismoradi M. Turunen H. Bondas T. (2013). Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs. Health Sci.15 (3), 398–405. 10.1111/nhs.12048
120
Weaver S. J. Dy S. M. Rosen M. A. (2014). Team-training in healthcare: a narrative synthesis of the literature. BMJ Qual. Saf.23 (5), 359–372. 10.1136/bmjqs-2013-001848
121
Weaver S. J. Lyons R. DiazGranados D. Rosen M. A. Salas E. Oglesby J. et al (2010). The anatomy of health care team training and the state of practice: a critical review. Acad. Med.85 (11), 1746–1760. 10.1097/ACM.0b013e3181f2e907
122
Weingart L. R. Behfar K. J. Bendersky C. Todorova G. Jehn K. A. (2015). The directness and oppositional intensity of conflict expression. Acad. Manag. Rev.40 (2), 235–262. 10.5465/amr.2013.0124
123
Weiss M. Kolbe M. Grote G. Dambach M. Marty A. Spahn D. R. et al (2014). Agency and communion predict speaking up in acute care teams. Small Group Res.45 (3), 290–313. 10.1177/1046496414531495
124
Weiss M. Kolbe M. Grote G. Spahn D. R. Grande B. (2017). Why didn’t you say something? Effects of after-event reviews on voice behaviour and hierarchy beliefs in multi-professional action teams. Eur. J. Work. Organ. Psychol.26 (1), 66–80. 10.1080/1359432X.2016.1208652
125
Weller J. Boyd M. Cumin D. (2014). Teams, tribes and patient safety: overcoming barriers to effective teamwork in healthcare. Postgrad. Med.90 (1061), 149–154. 10.1136/postgradmedj-2012-131168
126
West M. A. (2000). “Reflexivity, revolution and innovation in work teams.” in Product development teams: advances in interdisciplinary studies of work teams. Editor BeyerleinM., (California: JAI Press), 1–30.
127
Wolever R. Moore M. Jordan M. (2017). “Coaching in healthcare.” in The sage handbook of coaching Editors BachkirovaT.SpenceG.DrakeD., (London, UK: Sage), 521–543.
128
Zajac S. Holladay C. Tannenbaum S. Salas E. (Forthcoming In Press). Building effective healthcare team development interventions in uncertain times: tips for success. Organ. Dynam.
129
Zitzman E. Berkley H. Jindal R. M. (2018). Accountability in global surgery missions. BMJ Global Health3, e001025. 10.1136/bmjgh-2018-001025
Appendix A
Table A1
| Organizational Conditions | Descriptions |
|---|---|
| Teamwork reinforced | Policies, practices, rewards send the message that teamwork is valued. |
| Supportive culture | Organizational norms support teamwork, learning, and safety. |
| Executive and division leadership on board | Members of leadership set the example by behaving, working together, and communicating in ways that demonstrate they value teamwork. |
| Team Leadership | |
| Accountability | Team members hold everyone accountable to commitments/behaviors. |
| Shared Leadership | Team members “step up” and perform leader functions when needed. |
| Coaching | Team members provide coaching and development advice to each other. |
| Clear Roles and Purpose | |
| Roles defined | Responsibilities, reporting structure, and decision authority are clear. |
| Team direction clear | The team’s purpose is clear with objectives, goals, and priorities. |
| Team Norms | The team follows standards or informal rules to regulate behavior. |
| Technical Competence | |
| Trained | Team members receive the training to be competent in their roles. |
| Capable | Team members possess needed knowledge, skills, and competencies. |
| Staffed | The team has the right number of people to accomplish its objectives. |
| Attitudes | |
| Value teamwork | Team members think “team first” with a shared commitment. |
| Assume positive intent | Team members believe that other members want to do the right thing. |
| Believe Can Succeed | The team collectively believes they can accomplish their mission. |
| Care for / Include Others | Team members feel empathy towards and care about their teammates. |
| Behaviors | |
| Learn continuously | The team takes actions to continuously learn and improve. |
| Exchange information | The team communicates accurate, timely information to one another. |
| Monitor/Backup others | The team monitors progress toward goals and provides backup. |
| Manage conflict | The team manages disagreements and conflicts constructively. |
| Establish relationships across boundaries | The team does an effective job of managing relationships with people and groups outside the team. |
| Shape decision making | The team knows the process to make decisions and who to involve. |
| Coordinate actions | Team members integrate their actions effectively to reach shared goals. |
| Cognitions | |
| Develop shared mental models | Team members possess a common understanding about key factors such as priorities, norms, responsibilities, and expertise areas. |
| Create situation awareness | Team members have a clear understanding of what is going on within the team and happening “to” the team. |
| Reflect on progress | The team collectively reflects upon goals and outcomes for debriefs. |
| Emergent States | |
| Psychological Safety and Trust | Team members trust one another and feel they can speak up and be honest with one another. |
| Adaptability and Resilience | The team has the capacity to adjust as needed, and to withstand and bounce back from challenges. |
Framework Competency Descriptions
Appendix B
Sample in-field interview items
- 1
What is your role on the team?
- 2
How effectively do team members work together?
- a
What is helping your team? What are your team’s strengths?
- b
What do you think may be hindering your team’s effectiveness? What are your team’s weaknesses?
- 3
If you could change on thing on this team, what would it be?
- 4
What do you need to able to succeed as a member of this team?
Summary
Keywords
teams and groups, leadership, communication, decision making, coaching, reflection, conflict management, accountability
Citation
Zajac S, Woods A, Tannenbaum S, Salas E and Holladay CL (2021) Overcoming Challenges to Teamwork in Healthcare: A Team Effectiveness Framework and Evidence-Based Guidance. Front. Commun. 6:606445. doi: 10.3389/fcomm.2021.606445
Received
15 September 2020
Accepted
06 January 2021
Published
17 March 2021
Volume
6 - 2021
Edited by
Leah M. Omilion-Hodges, Western Michigan University, United States
Reviewed by
Rafael Obregon, UNICEF United Nations International Children's Emergency Fund, United States
Bryan Abendschein, Western Michigan University, United States
Updates
Copyright
© 2021 Zajac, Woods, Tannenbaum, Salas and Holladay.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stephanie Zajac sazajac@mdanderson.org
This article was submitted to Health Communication, a section of the journal Frontiers in Communication
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.