 Devalina Mookerjee1*
Devalina Mookerjee1* Shubhabrata Roy2
Shubhabrata Roy2- 1Jadavpur University Press, Kolkata, India
- 2Behavioural Insights, Architecture and Strategy, New Delhi, India
When urban workplaces shut down for the COVID-19 pandemic lockdown in India, a very large number of migrant workers were forced to reverse-migrate to their largely rural points of origin. This article looks at the mental health implications of the period migrants spent without work, back at the low-resource places from which they had out-migrated, in hopes of a better life. Based on qualitative interviews conducted with reverse migrants during the COVID-19 pandemic lockdown, this article has a two-fold aim. The first aim is to reach the experiences and voiced concerns of precarious and vulnerable migrants to those who may be in a position to ameliorate their distress. Since policy-makers tend to lack time, findings from the qualitative data have been summarized in the form of a multi-dimensional typology, open to expansion by further research. The typology sees themes in money, health, information, and isolation. Second, the article follows the issues in the typology to suggest that acknowledgment of the significant role of migrant workers in India's economy, via sensitive enumeration, would be a first, and essential step to address the multiple concerns raised by migrant workers themselves. This baseline information could then be used to build subsequent dependent steps addressing the myriad causes of mental health distress among migrant workers in India.
1. Introduction
When the lockdown was declared in March 2020, institutions and organizations in urban centers downed shutters until further notice. This meant that at least 60–80 million work-related interstate migrants in India (Thakur, 2020), found themselves abruptly stranded without work and income. They had to find their way back to their resource-poor homes in the small towns and villages of India to stay until further notice–a situation in which that notice depended on the unpredictability of the pandemic. It was a fearful, anxious time for marginalized migrant workers in India, a large number of whom were already coping with the stressful consequences of work in the informal sector of cities, and earnings in low wages, under adverse conditions of living and employment (Mukherjee et al., 2013). Mental health experts have pointed out that the psychological impacts of the reverse migration and lockdown point to the high possibility of a public mental health crisis among Indian migrant workers in the near future (Chaudhari, 2020; Singh, 2021).
Reverse migration is defined as “the process of internal and international migrants returning to their place of origin from destination state/countries” (Khan and Arokkiaraj, 2021, p. 4). Here, our focus is on the internal reverse migration engendered by the COVID-19 lockdown in India, so points of destination and origin are both within the country. Although migration within the country usually entails less travel and paperwork than international migration, the precarity patterns of internal migrants in India seem to echo the patterns of international migrants across South Asia. As Silvey and Parreñas (2020) point out, international patterns include (1) the precarity of migration, which is a factor at the point of origin determining the reasons for, and shape of the migration. For internal migrants in India, this would largely be livelihood precarity at origin homes (Berchoux et al., 2019; Dandekar and Ghai, 2020); (2) the precarity of labor defines conditions at the destination points of work. These are difficult, across conditions of living and work for migrants in the cities of India (Babu et al., 2017); (3) the precarity of the future points to cycles of continuing labor across sites. In India, this takes the form of chains of circular migration (Jesline et al., 2021), which is an effort to earn enough to support the family at points of origin, pay any debts, and support migrant labor at destinations. In this regard, it is clear that migrant labor is subject to an entire working life's worth of stress. This constant stress may be heightened at crisis points like the pandemic lockdown but is rarely relieved.
Mental health is a serious concern (WHO, 2022), and an underserved problem in India. Anxiety and depression are particularly widespread and rarely addressed, with the National Mental Health Survey 2015–2016 seeing that about 80% of people suffering from mental health distress had not received any treatment in the last 12 months due to reasons including lack of knowledge, and high cost of care (Gururaj et al., 2016). Mental health distress is also subject to deep-rooted socio-cultural stigma (Chauhan and Chauhan, 2022). As with access to other systems in a country as economically lopsided as India, marginal people like migrant workers suffer this lack of understanding and infrastructure the most (Yadav and Shekhar, 2014).
Public policy decision-making in India is largely top-down, with the voices of those most affected by decision-making rarely part of the process (Basu, 2019). The implications of such communicative inequity are serious in the Global South, with long-term, wide-ranging implications. Dutta and Pal (2020) point out that in these spaces, “erasures from the spaces of decision-making are the bases for policies and programs,” “resulting in extractive practices that expel subaltern communities from their livelihoods” (p. 355). In this article, empirical evidence from reverse migrant workers in India during the COVID-19 lockdown provides a difficult illustration of what happens on the ground in the Global South when the voices of the working poor are not included in the policy that impacts them.
This article aims to address the lack of inclusion of the voices of the poor in conditions of precarity, in the area of mental health, at a time of possible coming crisis. It does this by first, creating a multidimensional typology of the causes of anxiety and fear experienced, and voiced, by reverse migrants, during the COVID-19 lockdown. As far as we are aware, this is the first time that typology has been used as a tool to categorize and classify sources of distress with reverse migrant workers in India. Second, this article uses the typology as a springboard to lay out policy recommendations in the areas connected with the mental health of migrants. The purpose of this two-fold exercise is to point to the shape of a policy that addresses the challenges of mental health for migrant workers, by directly taking into account the perspectives and concerns of the marginalized people such policy is meant to address. Following these aims, the research questions are:
RQ1: What experiences did migrant workers go through, that they are aware contribute to the feelings of fear and anxiety they suffered through the lockdown?
RQ2: What shape would policy interventions around mental health take, if they were designed to address the burdens of the marginalized, as the marginalized experience and voice them?
The authors have built a typology for the qualitative findings in the first stage, in an effort to build a communicative bridge from research to policy in this area in India, since typology has a history of association with policy-making based on evidence in other parts of the world (DeMarchi et al., 2016; Bond, 2018).
2. Materials and methods
2.1. Mental health, migrants, and COVID-19 in India
The Global Burden of Disease Study 1990–2017 (Sagar et al., 2020) found 197.3 million people with mental disorders in India, which was 14.3% of the population. In terms of contribution to Disability Adjusted Life Years (DALY), the study saw high rates of depressive disorders (33.8%) and anxiety disorders (18%). Mental health stigma is widespread in India, where socio-cultural factors inhibit treatment-seeking and care (Gaiha et al., 2014). This leads to delays in seeking help for mental illness, delayed diagnosis and treatment, discontinued treatment, and lower possibilities that individuals are able to overcome the condition and participate in a full life (Shrivastava et al., 2012). The National Mental Health Survey 2015–2016 found a truly alarming treatment gap between 70 and 92%, with common mental disorders including depression and anxiety showing a treatment gap of 85%, and severe mental disorders showing a 73.6% of treatment gap (Gururaj et al., 2016).
In terms of policy that governs mental health in India, the Mental Health Act of 1987 was in effect until it was overturned by the Mental Healthcare Act of 2017, the latter focused on the rights of those suffering from mental illness. Unfortunately, law and policy experts say that the new act comes with little obligation to action on the part of either government or health systems (Karia and Deshmukh, 2020). The National Mental Health Programme, which has existed since 1982, was given a new form in 1996. However, as Murthy et al. (2016) point out the reports from the National Human Rights Commission have demonstrated “gross deficiencies” in the institutional care of the mentally distressed, as well as pointing to inadequate human resources, and the use of “poor psychosocial interventions” (p. 7). While there are small-scale mental health interventions reaching select low-income populations in various parts of the country, it is clear that reaching mental health to general populations is a challenge for India.
Dutta and Jamil (2013) argue that “communicative marginalizations work hand-in-hand with structural deprivations, suggesting that the communities that exist at the margins of healthcare are also marginalized through their absence from policy platforms, and platforms of decision-making about their health outcomes” (p. 171). This idea is directly applicable to the area of mental health in India, and migrant mental health in particular, where the people who suffer are rendered doubly invisible—as migrants, and as those who suffer the health consequences of being migrants. In their study with Filipino and Indonesian migrant domestic workers in the United Arab Emirates, Parreñas et al. (2019) found patterns of serial migration that echo the patterns of migration for work within India. In their analysis of “the precarity and itinerancy that follows low-wage migrant workers across various stages of the migration cycle” (p. 1231), they point to the financial insecurity that causes workers to move away from home or points of origin in the first place, the discomfort of being migrant in spaces which are exclusionary toward them, and the continuing financial insecurity that implies that these workers will almost never be able to retire peacefully with savings enough to last the rest of their lives. This “serial labor migration,” which Silvey and Parreñas (2020) call precarity chains, is similar to the experience of internal migrants within India. They leave resource-poor homes to migrate to the cities for work, return home to the point of origin between jobs, or after a project is complete, and then back again to work in the city, in a pattern of circular migration. Similar to their female counterparts moving between South Asia and the UAE, migrant workers in India do find themselves working under difficult conditions at their destination in the city, and struggling to support their families at home while hoping that this cycle of repeatedly leaving home will eventually be worth the effort and isolation of being away from loved ones (Datta, 2020). To people living out such precarity chains, the pandemic and forced reverse migration became an enormous and immediate source of distress.
Migrant workers in India suffered multiple stressful marginalization experiences, even before COVID-19. In the cities and larger towns in which they live and work, mostly as informal labor in the manufacturing, construction, and service sectors of the Indian economy, they are exploited by both employers and middlemen, and often denied adequate wages, food, housing, sanitation, and healthcare (Chatterjee, 2006). Kusuma and Babu (2018) found that migrant workers suffer widely from diabetes, hypertension, and bouts of malaria. Access to healthcare or other forms of benefit is often a problem for migrant workers since development and planning in the urban centers of India very rarely recognize that migrant workers need benefits at their urban points of destination (Bhagat et al., 2020).
The national lockdown at the beginning of March 2020 made an already bad situation even worse for migrant workers. With income stopped due to loss of work, and no prospect of future income, they had to return by whatever means possible to their resource-poor homes and wait until earning became possible in the cities again. Chaudhari (2020) pointed out that the traumatic experiences of these migrant workers made them uniquely vulnerable to mental health distress on several dimensions, including (1) susceptibility to new infections, since many of the workers already suffer from respiratory and other conditions related to living and working conditions; (2) mental disorders, due to a pre-existing susceptibility to stress, as compared to non-migrants; (3) resource and space limitations, which hinder the successful following of safety norms; (4) social exclusion, loss of social status, and discrimination; (5) peri-traumatic psychological distress during the pandemic, particularly anxiety, depression, and mental stress; (6) barriers to access to mental health consultation and care; and (7) the absence of effective laws to protect workers in the unorganized sectors of India.
A study involving migrant workers during the lockdown in the district of Varanasi by Srivastava et al. (2021) found that major stressors included financial crisis; lack of social support; psychological stressors from uncertainties related to information and the future, and fear of infection. Drawing on their work as volunteers with the Stranded Workers Action Network (SWAN) during the pandemic, Adhikari et al. (2020) saw migrant workers having problems with access to food and cash during the lockdown, with the regulatory frameworks of banks being unsympathetic to those who could not maintain a minimum balance. They also suffered from low access to medical assistance. Since the attention of the vastly overstretched medical system had turned entirely to COVID-19, those with diabetes, heart conditions, tuberculosis, and wounds or injuries, who would normally access the lower-fee public healthcare system, were forced to either find the money for more expensive private healthcare or if unable to find funds, remain untreated.
Using the Interstate Migrant Policy Index (IMPEX) score, Rao et al. (2020) found that Kerala, despite its low in-migration, provided rations and other benefits to migrant workers, whereas Uttar Pradesh and Gujarat provided no support to migrant workers. Instead, the government of Uttar Pradesh passed the Uttar Pradesh Temporary Exemption from Certain Labor Laws Ordinance, valid for 3 years, that exempts organizations from having to implement all but three state labor acts (Nanda, 2020). A four-center study involving reverse migrant workers from Northern India found that migrants feel low, gloomy, restless, and uncertain, worried about money to survive, having family at home in their native towns and villages, and fearful of getting infected with COVID-19 (Chavan et al., 2021). In a review of the literature on psychosocial and mental health issues of Indian migrant workers during the pandemic, Singh (2021) found themes in living conditions, basic needs, housing, transport, concerns about family, infection, poverty, unemployment, and future insecurity.
The current literature on reverse migrants and mental health during the COVID-19 lockdown in India appears to have two gaps. One is that much of the primary research that feeds the literature was conducted with migrants who were still in urban centers during the lockdown, in transit back home, or had just arrived back at their homes in villages and small towns and were still in, or just out of the mandatory 14-day quarantine. This means they had not yet spent some time at home, with family, and without income. Since the lockdown lasted close to a year in India, there is a chronologically significant period for mental health that finds a low focus in the literature. Second, while there is important and necessary research in this growing area, it is fragmented and scattered, and takes time and energy to collate. This makes it difficult to access for people like policymakers, who are always working on time-deficit.
The next part of this article tries to address both these gaps by creating a multidimensional typology with the primary qualitative data of interviews with reverse migrants, who had already been home for 3–4 months. We hope that this typology will be extended over time, with more information coming into the necessary area of research in migrant mental health. Since our aim is to focus directly on the voices and concerns voiced by the workers themselves, we build this typology from the qualitative interview data of a research project that mapped the challenges of being a resource-poor reverse migrant during the COVID-19 lockdown.
2.2. Method
The source of primary data for the typology is 54 semi-structured, in-depth interviews with COVID-19 reverse migrants in India. They were conducted during the first lockdown, which, barring short phases of re-opening, continued for almost a year.
2.2.1. Inclusion criteria
The criteria for inclusion were: (1) return to point of origin during the mass reverse migration over late March and early April 2020; (2) been back home with family for 3–4 months; (3) religion; (4) education; and (5) latest period as an outmigrant.
Religion was included because the marginalization of about 15% Muslim minority is on the rise in India (Subramanian, 2020). With little available data on internal migrants, the sample had 36 Hindus and 18 Muslims, roughly reflecting this difference in population. Education was included because it is related to access to work across urban and rural India. Although education does not guarantee income, lower education means that opportunities are restricted to the informal sector (Kumar and Sahu, 2013). This was included because we wanted to see if differences in education, implying differences in access to work, could show differences in lockdown experiences. Period as outmigrant was used to accommodate a variety of patterns of migration. The range of work migration in India runs the range from relatively stable contracts, to seasonal agriculture daily wage labor (Srivastava, 2012). We followed The National Sample Survey, which uses more or <6 months to differentiate between circular patterns of work and home.
2.2.2. Recruitment and sampling
Recruitment was conducted by local recruiters who were known to the second author through previous projects he had worked on, based in rural and semi-rural Uttar Pradesh, Bihar, and West Bengal. The research protocol received approval from the Monk Prayogshala IRB, which is compliant with the US Department of Health and Human Services and specializes in ethical review for social science studies in India. Informed consent as outlined in the APA guidelines was sought from all participants.
The reverse migrants in this study were located in the Indian states of Bihar, Uttar Pradesh, and West Bengal. These three states are significant points of origin for internal migrants in India (Bhagat et al., 2020). Participants had returned to their homes with the wave of reverse migration that swept across India by the end of March and April 2020. They had completed quarantine and been back with the family for 3–4 months. The sample included 36 Hindus and 18 Muslims (Table 1).
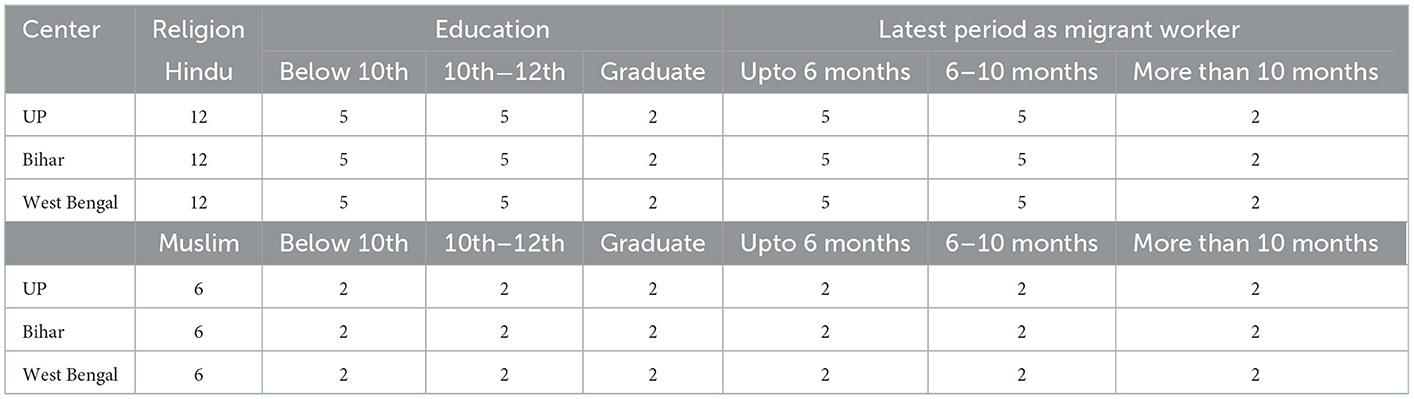
Table 1. Sample for the study on which the typology is based.
2.2.3. Interview guide and data gathering
The semi structured guide asked participants about the impacts of the pandemic lockdown on their lives. Drawing on Chaudhari's (2020) list of migrant vulnerabilities included open-ended questions in the following areas (Table 2).

Table 2. Areas in which open-ended questions were asked, with some of the questions.
Interviews were conducted in Hindi or Bengali, according to the preference of the participant. Since travel was impossible during the national lockdown, they were conducted over the phone, by researchers based in Delhi. The first author and a team of three researchers conducted interviews at varying times of the day and evening, depending on when participants were available and free to talk. Interviews lasted between 30 and 40 min since participants were not able to give longer periods to interviews at that difficult time. The two limitations of this study are, first, that the data includes no visual dimension because interviews were conducted on the phone. Second, the data includes no women, as local recruiters were unable to locate any women willing to give time to talk to researchers on the phone.
The voluntary nature of participation was emphasized at the beginning of interviews, with the researcher starting the interaction by reminding the participant that he could refuse to answer any question, and was free to exit the interview anytime he liked. The interviews were recorded on in-phone apps, translated, and transcribed by the researchers conducting the interviews. Researchers' understandings and observations of the interviews were included in the data and used as a reference in the process of strengthening the categories. Identity information was securely stored, with access granted only to the researchers in the study.
2.2.4. Data analysis
The first author started open coding as interviews started to come in. Regular code-checks were conducted between the first and second authors as further interviews came in, and coding proceeded. This part of the analysis used the process of constant comparison to evolve categories and codes (Glaser and Strauss, 1967). A total of 62 categories were evolved through the process of open coding. Lack of earnings, mounting debt, unsafeness of city life, the feeling of home, and worries about infection were among the strong codes. During this first coding exercise, we saw feelings of depression, fear, anxiety, and uncertainty voiced constantly through the interviews, thus, we coded for as many experiences related to these feelings as possible. The 62 open codes yielded 19 focused codes, including making a living; coronavirus fears; home; the city as a migrant; safety in the pandemic, coping understandings, and coping behaviors. Further reduction saw the core categories from the grounded theory analysis, which included home, city, money, and infection, as they have been reported in an earlier piece based on this study (Mookerjee et al., 2021).
The typology of sources of precarity was co-created by the two authors. We went back to the open codes that had been evolved by the process of constant comparison, while simultaneously consulting the data that fed those codes. Using feelings of distress as a lens, we started reducing the categories, through a process of back-and-forth, until an agreement between coders was established in each category. The term “feelings of distress” was used as a label to denote affective states that included feelings of insecurity, helplessness, fear, anxiety, perceptions of at-riskness, confusion, and loneliness. This cluster of terms (translated from the original languages) was drawn from the interview data, as we wanted the voices of participants to frame the typology.
Rounds of the back-and-forth process between the authors gradually tightened and polished concept areas, while trying to ensure that each emerging dimension had the properties of both internal homogeneity on the level of the type, and external heterogeneity on the level of the typology, or Bailey (1994) says, were “both exhaustive and mutually exclusive” (p. 3). To evolve the typology, we followed these four steps for empirically grounded type construction: (1) development of analyzing dimensions; (2) grouping cases, and analysis to identify empirical regularities (attribute space); (3) figuring out meaningful relationships and type construction; and (4) characterizing the types (Kluge, 2000).
3. Results
The typology below is multidimensional and exploratory. It is necessarily the latter since a search of the literature shows that sources of mental health stress among reverse migrant workers in India have not yet been a topic of typology.
3.1. A typology of sources of mental health distress among reverse migrants
The participants were all men and mostly heads of households. They were supporting households of 2–5 people, at home (point of origin). Each was in a cycle of migration, either returning to the same place for work, or cycling between destinations, depending on where kin was already located in the city, or middlemen said work was available. As already mentioned, they were Hindu and Muslim, with differential education and periods of migration, and had been back home and with family, and without income, for 3–4 months at the time of the interviews.
Age was not included in the criteria, but we ended up with a range of 22–48, which straddles the “young adult” (15–34) and “old adult” (35–59) categories in internal migration (Khan et al., 2016). All but a few with 12th-grade or above degrees worked in the informal sector. These urban working migrants were located in the construction (manual labor, lower on-site management), service (lower grade staff in call centers, offices, eateries, hospitals), and manufacturing (factory work with fabric, appliance parts, etc.), industries.
In this section, we show how the typology evolved. Step 1 shows how the categories evolved, with the superordinate categories labeled: money, health, information, and isolation (Table 3).
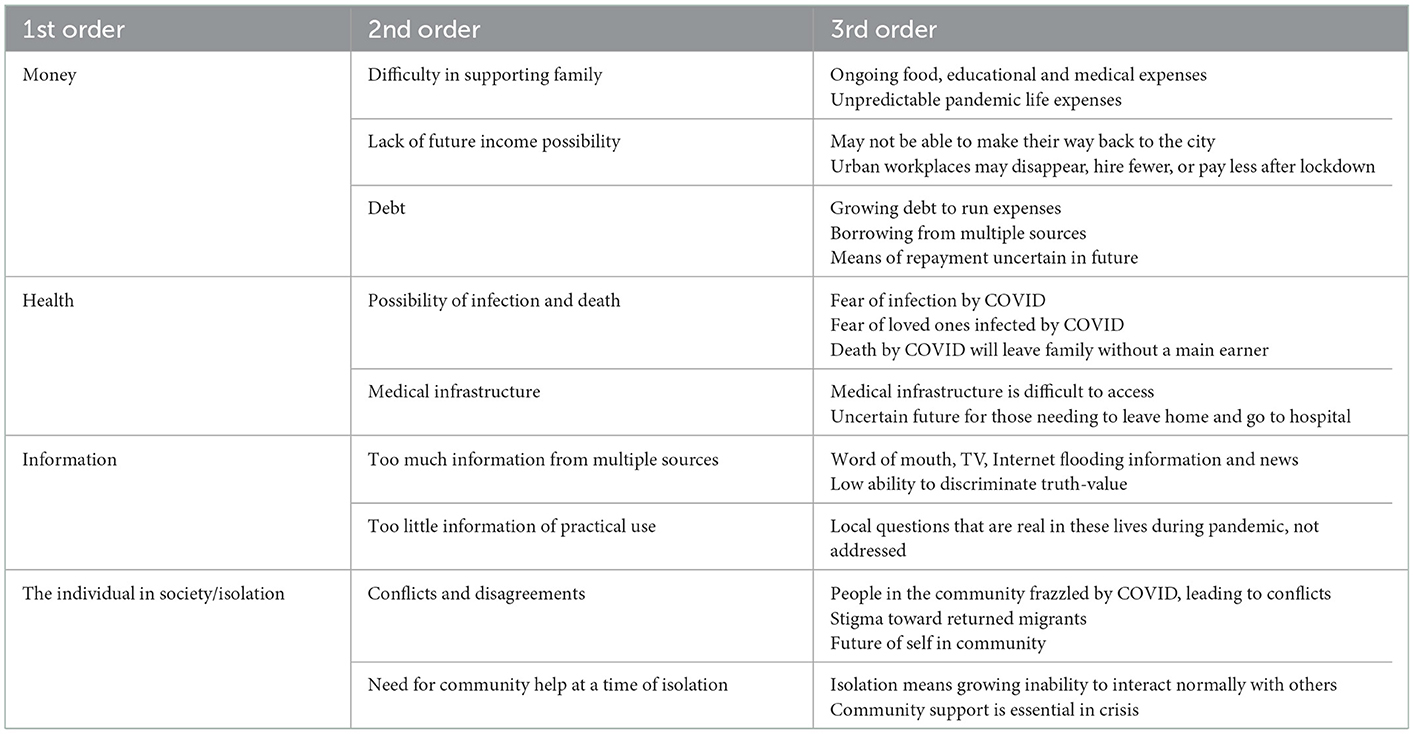
Table 3. Evolution of typology, step 1.
In the next part of the process, we map the relationships of each source-of-distress dimension (above) with the core investigative area of precarity. Since “feelings of distress” may be considered manifestations or expressions of living in precarity, precarity was (as mentioned in “methods”), defined by the voices of participants expressing feelings of insecurity, helplessness, confusion, fear, anxiety, perceptions of at-riskness, and loneliness.
Analysis showed that the feelings of precarity participants associated with money are primarily insecurity and helplessness; those associated with health are primarily anxiety, fear, and (feelings of being at) risk; those associated with information are primarily confusion and helplessness; those associated with isolation are primarily loneliness and anxiety (Tables 4–7).
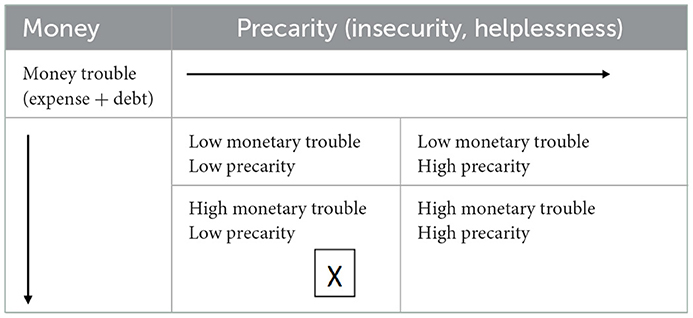
Table 4. Evolution of typology, step 2a–Money.
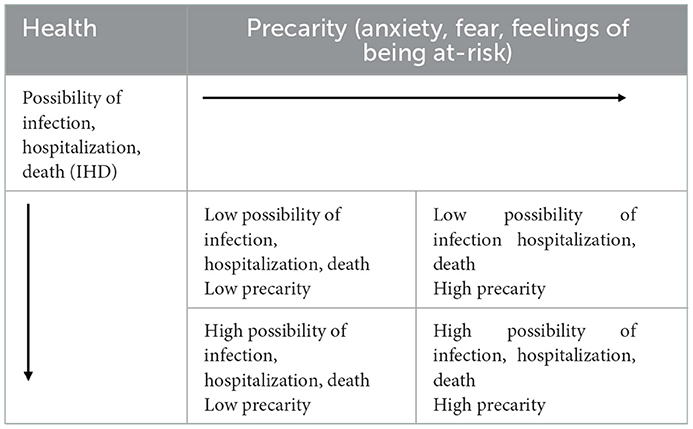
Table 5. Evolution of typology, step 2b–Health and precarity.
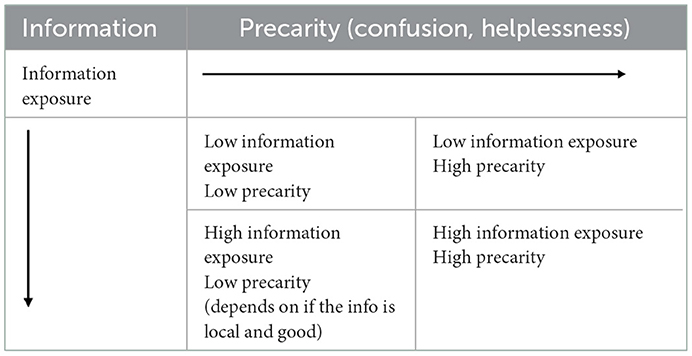
Table 6. Evolution of typology, step 2c–Information and precarity.
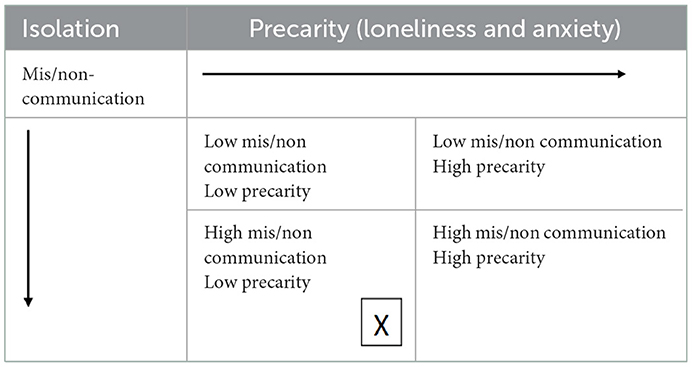
Table 7. Evolution of typology, step 2d–Isolation and precarity.
In the final step of the typology, we superimposed the four dimension tables on each other. This gave us a horizontal axis that mapped feelings of precarity (FP) and a vertical axis that mapped sources of distress (SD), as below (Table 8).
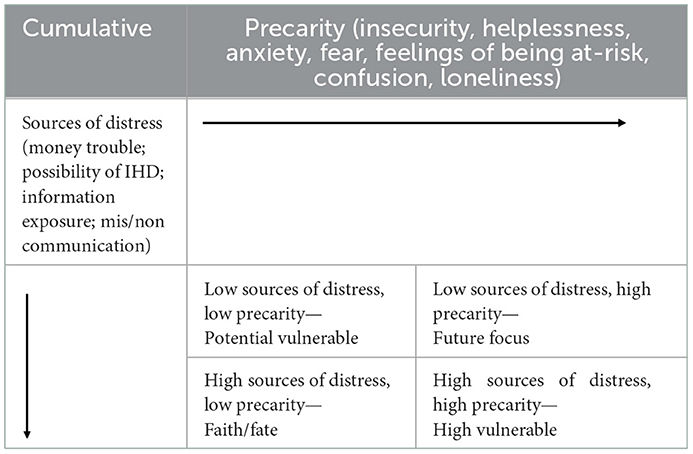
Table 8. Final typology, with sources of distress mapped against precarity.
3.1.1. Characterization of typology
Please note that, (1) although we characterize all four quartiles, we will focus on the bottom right quartile, which is High Vulnerable. This is because the characteristics of High Vulnerability appeared in every interview conducted for this study, on one or more dimensions. (2) Although COVID-19 has been eponymously referred to everywhere else in this article, the quotes have been translated faithfully, using the terms migrant workers used in the interviews–“covid,” or “corona.” (3) Names have been changed to protect the anonymity of migrant workers participating in the study.
3.1.1.1. Low sources of distress, low precarity: Potential vulnerable
The label “Potential Vulnerable” defines a situation of low reported sources of distress (SD), accompanied by low feelings of precarity (FP). In terms of financial stress, low SD, accompanied by low FP serves as a marker of pre-COVID-19 times, when migrant workers were free to leave points of origin and travel to better-paying jobs in the city. Even though those jobs and the life of being a low-resource work migrant are not easy, it still allowed these men, who are usually the primary earners in the family, to support loved ones back home.
“I am a father, in my family, I earn, and that's how everyone eats, that's how it is.” (Anil, 24, UP)
In terms of health, the Possibility of Infection, Hospitalization, and Death (IHD) were seen by participants to be related to their physical distance from active cases, and places where COVID-19-infected people congregate, like hospitals. Thus, being placed in a village that had no cases, and was distant from the nearest active cases, was usually enough for participants to feel less anxiety and fear about being at risk. Another factor that made for low precarity in health was the presence of open space and nature.
“Here, we are safe, no corona. There are fields all around–everyone here works in agriculture. Every evening it is cool and breezy (…) No cases in any of the villages around.” (Tajibur, 27, WB)
In terms of Information, the combination of low information exposure, combined with low precarity was relatively uncommon, since many participants, and, reportedly, their families, were constantly watching the sensationalistic national 24/7 news as COVID-19 unfolded across the country. In this context, low exposure is voluntary. Keeping away from exposure to information in the media is largely an individual decision, that individuals implement themselves, for their own peace of mind. Those who preferred to avoid this barrage of information were still receiving information from friends and relatives.
“The TV news is on all the time at home, I don't like that (…) it's stressful. So I go out for a walk.” (Ranjan, 38, UP)
In terms of isolation, reports of healthy ongoing social and personal relationships were associated with low feelings of loneliness, depression, and anxiety. Those who had a local friendship cohort went out of the home and met up, this in particular kept men from loneliness and feelings of depression. Male participants reported that the women in their lives seemed to be coping better than them in this regard because even before the pandemic, mobility-restricted women were conducting many of their social relationships on the phone.
“I don't know what I would do if I could not meet them (his friends). This is only possible because they have come back too (pandemic reverse migrants). We meet in the evening, talk, drink tea (…) I think I would go mad (if that was not possible).” (Om Prakash, 25, UP)
However, given the situation of the overall cohort of this study, the state of low SD and low FP cannot be considered an absolute or static state. Marginal lives are always vulnerable to change in financial and health terms, leaving safety nets behind. That is why this quartile has been labeled Potential Vulnerable.
“A few more months will be fine. But if someone falls ill (in his family) everything changes at once. I have seen that happen to others.” (Bijoy, 45, WB)
3.1.1.2. Low sources of distress, high precarity: Future focus
The label “Future focus” has been used to show situations in which low sources of distress are paired with high feelings of precarity. This is called future focus because this combination tends to gloss over current solvency, and a current/now of relative stability, to a future that may never entirely recover from the multi-aspect breakdown of the pandemic lockdown.
The focus here is on the notion of a future world that never becomes post-COVID-19. Migrants never get to go back to work, and they are stuck in their resource-poor points of origin, with little hope of a future. In terms of money, this projected future looks disastrous, with no earnings, and growing expenses.
“Sometimes I think, this will never end (..) there will be no money left, all run out (…) no food. There will be no job (…). The city will never open. I have nightmares about this, wake up sweating with my heart racing.” (Pradip, 31, Bihar)
In terms of health, this combination of low possibility of Infection, Hospitalization, and Death (IHD), and high precarity marked the mindspace in which there was quite a low perceived hazard to health at the time of the study, but COVID-19 was described as a deeply unpredictable phenomenon, which could at any time move with incredible speed in ways no one could map or predict, and strike at will. This caused feelings of precarity, even though the immediate hazard to themselves and loved ones was perceived, and admitted, to be low.
“This covid, one day it's in the city, next day there's a case in the close-by town, then three days later it's here. It is a terrible thing, like a demon (…) no one knows anything about it” (rakshas, in the sense of an unpredictable demonic being, powered by magic). (Sajid, 24, UP)
In terms of information, Low information exposure, combined with high precarity marked an area where those who thought they had lower access to information than others, whether voluntary or involuntary (e.g., no-internet phone) felt that they were missing out on vital nuggets in the stream of information. It was felt that such misses could have an unpredictable effect on the future. This was reported to be a stressful and confusing situation, even among those who were voluntarily limiting their information exposure.
“It's a worry in the back of my mind, always there, what if they say something important on the news and I don't hear it because I wasn't listening? (…) When should I be listening?” (Karna, WB, 30)
In the field of isolation, even self-regulated exposure to media does not keep migrants safe from the word-of-mouth information and rumors circulating in their community. These rumors pertained to COVID-19, cases of infection, and the non/availability of resources, and caused spikes of deep feelings of precarity and confusion. Word of mouth sometimes turned out to be untrue, causing even greater confusion.
“Everyone was saying she (a woman in a nearby village) had corona, that they came in the white van and took her away (…) but actually she had TB, it was bad, poor thing (…) So much fear for days. (…) Who do I believe?” (Kapil, 43, UP)
Migrants were anxious about the confusion they were experiencing with regard to the information and anticipated that as more information came in via various channels, the more their confusion would grow.
“News says this, TV says that, my friend looks his phone and says something, it will only get worse as this (lockdown) goes on.” (Rafi, 27, WB)
3.1.1.3. High sources of distress, low precarity: Faith/fate
This dimension is labeled “Faith/fate” in an attempt to encapsulate the idea that letting go in the face of a larger design made for feelings of lower precarity, even in situations of relative distress. Faith in a higher power is common in India, and leaving it up to faith and/or fate was a mechanism that helped migrants deal with pervasive stress in the context of the pandemic. Another dimension of faith here is faith in the self, which showed up in the dimension of information.
The first null cell (one of two) in this multidimensional typology is that of high monetary trouble, combined with low precarity. Running out of financial resources was a constant, top-of-mind distress that no faith or belief in fate could alleviate.
“Who will feed my children? I believe in god, but no one will do that!” (Sajjad, 34, Bihar)
In health, the perpetual anxiety of possible infection was somewhat offset by the idea that nothing one could do to protect oneself could make a difference, because, ultimately, what was going to happen, was going to happen. If someone was destined to be ill, they would be ill. If someone else was destined not to get it, no matter what they did, this would not happen.
“It is already written, on our forehead–what is going to happen. Everyone running around, being scared, that will not change anything (…) just follow the rules they're saying, the rest is up to god.” (Rajnish, 46, Bihar)
High information exposure was combined with low precarity when the information itself was felt to be trustworthy. Trusted friends and neighbors with known exposure to the wider world beyond the locality who had records of reporting correct information, or sources of information that were thought to be credible on the mass media, featured in this dimension. Listening to a source they perceived as credible, and ignoring others, was a choice made by some migrant workers. What characterized this behavior was faith in their own ability to discriminate between information and know which is correct.
“I am not stupid. I know that many of the things I hear are wrong, some are not even possible (…) Just one or two people I trust (…) always been right before.” (Neeraj, 26, UP)
The second null cell in this multidimensional typology says that there were no combinations of high mis/non communication and low feelings of precarity. As the fourth cell in “Isolation” shows, high mis/non communication–conflict, misunderstandings, moving away from others in the community, and not staying in touch with people, was invariably accompanied by a heightened sense of precarity.
“I can't go out, so I talk to no one but my family, just 2 people (…) In the beginning, it felt good to be back (…). Now, I don't feel like talking to anyone at all, just sleeping so I don't have to think.” (Ranjan, 41, Bihar)
3.1.1.4. High sources of distress, high precarity: High vulnerable
The quadrant labeled High Vulnerable is the unfortunate combination of high sources of distress and high feelings of precarity. Every migrant worker participating in this study fell into this quadrant in one or more dimensions, thus, it requires particular focus.
Please note that the definition of hyperlocal here follows the Oxford Languages dictionary, “relating to, or focused on a very small geographical community.” In the case of this study, the hyperlocal is bordered by village boundaries or the boundaries of individual localities in towns. Any part of this area can be reached by walking or non-motorized transport such as bicycles and pedal-operated rickshaws. Local is here defined as the geographical area just beyond the hyperlocal, including a cluster of villages, or a small town. While it is possible to use non-motorized transport to travel within the local, motorized rickshaws or motorcycles/scooters are more often used in India. Beyond the local area is often the highway and fully motorized transport that travels long distances.
3.1.1.4.1. Money
The High Vulnerable experienced feelings of anxiety, insecurity, and helplessness as money ran rapidly out, with no income. These migrant workers support their families at home. Food is an ongoing necessity. Older parents need medical assistance, and children need education (school fees had to be paid through the lockdown), which are all ongoing expenses. Participants said they felt afraid of not being able to discharge the basic responsibilities they have as householders. This led to reported feelings of extreme stress, sleeplessness, and occasional periods of not being able to do anything at all.
“Some days I wake up and think about how fast my little savings are running out (…) have to feed family (…) and then I can't get up, or move, or even do the daily things (…) I want to do them, I just can't.” (Dhruv, 29, UP)
Financially high vulnerable participants reported that even while they had no income, household expenses for daily needs seemed to have gone up, largely due to the national lockdown. With nearby shops shut, many had to take transport to get to the nearest open market. Sourcing became a problem at this time, so the prices of commonly available items sometimes rose without notice. Milk and other items needed for children became harder to procure and more expensive. Regular medical bills also rose in local areas. The fact that money was flowing out in unpredictable ways at a time of no income was very stressful.
“We had shops in the village where everyday shopping could be done, but they open only twice a week now. I have to take a bus to the market that is open, and there are so few buses now (…) you need government permission to run a bus now. So now it even costs more (…) every day money runs out and no money coming in.” (Bilal, 33, UP)
“Every time I come back from the market, I have no money left in my wallet. I don't know what will happen if this goes on (…) where will the money come from?” (Amit, 23, WB)
The lack of earning possibilities in the future is like a sword of Damocles hanging over the heads of the highly vulnerable. Since there are far fewer earning possibilities in hometowns and villages than in urban centers, participants were acutely aware that returning to the city was not a choice, but a necessity. The research saw this as an area of deep anxiety since participants are well aware of the unpredictability of the informal sector in which they work. They reported having heard that their workplace at the city had closed permanently, or that the middleman who is their source of city work had told them that places of employment would have less need for workmen once they could re-open. Some local middlemen, who take groups of migrant workers to urban centers for work, seemed to have disappeared, with repeated attempts to call or find the person having met with no results. Reported insecurity and stress were very high around the area of future earnings.
“If I could think—it is bad now, but soon I will be able to take a (long-distance) bus back to my work, that would make me feel better (…) don't know if there will remain a workplace.” (Deepak, 37, Bihar)
“He (the middleman) told all of us (group of workers wanting to know when they could return to work) that he doesn't know what's going on in the city. In any case, they will not want all of us back (…) Things are closed down even there, and if the business does not bring in money, how will they hire?” (Pramod, 25, UP)
Debt is a source of deep and continuous anxiety. Participants reported being wary of being in debt even before the time of COVID-19. However, many were already in debt before the lockdown, and working at urban centers to work off that debt. The end of debt was a prospect respondents said they looked forward to with feelings of self-efficacy and satisfaction. Thus, the fact that they are having to defer paying off that debt, and most are also needing to borrow further to sustain a living through the pandemic lockdown, is a source of very deep anxiety, because these debts will have to be paid off at some point.
A parallel source of helplessness that participants talked about is that bank loans need too much paperwork and minimum balance, thus, migrants borrow from local moneylenders. Moneylenders are known to draw the poor into debt traps with high rates of interest, which endure over cycles of repeated borrowing (Karlan et al., 2019). In this context, debt traps are also cycles of precarity, as described by Silvey and Parreñas (2020). Being in financial debt, in such a context, is deeply stressful. While participants in this study talked freely about the troubles they were experiencing during the lockdown, not one migrant disclosed the rate of interest at which they were borrowing money. They did, however, express a great deal of anxiety about the constant growth in the size of the debt.
“Sometimes I wake up in the middle of the night, and my heart is beating so fast I think I'll have a heart attack (…) I had a big loan from before, it was almost paid back. I was working in the city, it would take just a few more months. Then I had to come away, everything shut down (…) another loan, just last month, my daughter fell ill and I had no money to take her to a doctor, medicines. Now there's another loan” (Baleswar, 31, WB)
3.1.1.4.2. Health
Fear of infection by COVID-19 was prevalent among participants. They had come away from the city with the fear of infection, in a reverse migration unprecedented in their lifetime. In the small towns and villages from which participants talked to us, rumors were rife about COVID-19, how easy it was to get it (someone just had to breathe on you), and how difficult it was to recover once you had it—because even if you were cured once, it could always come back. For these migrant laborers, even greater anxiety lay in the possibility that a loved one would get infected, and they would be helpless to get the ill person the needed assistance, either because they did not have the resources, or because medical assistance would not be available.
They worried about having to leave the house for chores or shopping, because they could be the medium of bringing the virus back with them, to infect children or older people in the household. An additional source of anxiety for these workers was that if they became too ill or disabled to work, their household would be left without a principal earner. Given that these households were already resource-poor, their heads of household were very fearful that if they got infected, and became unable to work or died, they would leave their loved ones destitute.
“What will happen to my family if I get it? Who will take care of them, feed them, buy medicines for my old mother, and send my child to school? It will all be over (…) not just for me, but for them too (…) they will be on the street. So I must not catch it, must not fall ill.” (Rajnish, 46, Bihar)
“I don't go out every day, but I have to go out to do household shopping, pay bills. Then I am very scared. This covid it is everywhere, it is in the air. I keep thinking that if I am not very careful, I will take it home with me to my children, my wife, my younger sister also lives with us (…) They don't go anywhere, only I go out.” (Om, 38, UP)
Participants were aware of the overstretched state of medical infrastructure all over the country because this information was coming to them constantly through 24/7 national news. In India, this runs through the day and most of the night and is available through TV and the internet. Local word of mouth news, which is very important in the hyperlocal contexts in which participants live, also confirmed that local health facilities were swamped with patients. An image that recurred in the interviews as triggering fear was the white van with the medical personnel in white safety-suits who would show up at the doors to take away those infected, to hospitals. Knowing about the acutely overstressed and under-equipped state of medical infrastructure in the non-urban areas in which they lived, participants felt that if anyone was taken away in that manner, they were unlikely to return.
Those who had tried accessing local public healthcare with injuries, heart problems, or any chronic non-COVID-19 health issues had been turned away. In rural and semi-rural India, local quacks, or “Bengali doctors” as they are called in North India, are to members of communities an indispensable part of the health system. Rarely formally trained in any way, Banerjee (2021) estimates that about 80% of first health-related visits in rural India are to these doctors. They practice Allopathy, Ayurveda, Unani, Homeopathy, home remedies, and/or other therapies. However, even trusted local quacks seemed inadequate in the context of the newness, speed, and viciousness of COVID-19.
“Everyone is saying here that if they take you away in the white van, you will die in the hospital (…) your family will never see you again, you will never come back.” (Rakesh, 35, UP)
“Here our local (quack) doctor is very good, he has helped many people. Anyone falls sick, we go straight to him, he gives the correct medicine (…) but now, things are different. No one has ever heard of this corona before, how can he have medicine for it. So he does not have the medicine. If someone falls sick, there is only the hospital in the next town (…) we don't like to go to the hospital, this is a real problem.” (Deb, 28, WB)
3.1.1.4.3. Information
As the pandemic assumed larger and more uncertain proportions through the summer of 2020, reverse migrants at home were following the news. They were hoping that the 24/7 news made in urban centers like the national capital, Delhi, and Mumbai, would be able to allay their fears. Younger migrants, with access to smartphones, were actively looking up news from various sources, and watching views and commentary about India's COVID-19 situation on YouTube, and news websites on the internet. People pooled information over the phone, via text or forwards on WhatsApp, or on the occasions they met, updating each other, passing on what they may have heard from other sources and local word of mouth. The highly vulnerable reported that this situation was very confusing, with different news sources and talk shows reporting different scenarios, making it impossible for them to distinguish between what was true and may impact their lives, and what was not. Whatever they heard and saw on the news channels and the internet created more confusion and anxiety, with little to no information they received, allaying their fears about survival.
“I thought it was because I didn't know enough, I can't read properly, so maybe I am not getting the correct news. But they (his family) are watching the news on TV at home all the time since this began, and I started watching with them (…) all they do on TV is shout at each other (…) they say so many things, everything can't be right, even I can see that (…) nephew tells me news from the internet. The more I hear, the more my head spins.” (Tapan, 46, WB)
On the one hand, there was a surfeit of information leading to an inability to distinguish truth-value, and on the other, there was almost no news about the things that impacted these people directly in terms of the needs of their daily lives, and prospects of surviving the pandemic lockdown. There was no news of food rations that pertained to their areas, information about possible paying work, news about government schemes, school reopening, or any upgrades in medical support. Important local news like which market was likely to be open on which day was only passed around by word of mouth, and sometimes found to not be reliable, causing further distress and expense.
“When will the ration come? Why is the factory (he works at, in the city) not opening, even for a few people to work? If someone at home falls sick at night, what will I do? All day they give the news, but nobody gives me the news I need.” (Rajaul, 35, UP)
3.1.1.4.4. Isolation
Participants reported sudden outbreaks of anger and acrimony in their local communities, even among people who had, before the pandemic, had relationships of amity. Neighbors were building brick and mortar walls between properties where there had formerly been paths through. Conservative members of local communities were vocal in their apprehension that workers returning from cities would return with COVID-19, and infect the less-exposed people in relatively safe small town and village communities. The families of migrants, and the returning migrants themselves, who used to be valuable members of the local community, were both fearful and angry about being at the receiving end of this stigma, even in their village communities, where they had looked forward to safety and comfort, a place to rest. There were also regular conflicts about resources such as medicines at the shops, and milk for children, since a lack of supply during the national lockdown meant that anything not entirely supplied hyper locally had suddenly become a rare commodity.
“Our whole village has always been friendly. We go to each other's homes, drink tea. (…) but since this (COVID-19) happened, it has all changed. Now if I walk in front of some people's houses, on the road, they get angry (…) tell others that I am bad luck from the city, I will infect people in their house.” (Manoj, Bihar, 23)
The small towns and villages of India are largely resource-poor and survive on community support. High vulnerable migrants across centers voiced the fear that the isolation imposed by COVID-19 was making them isolated and withdrawn, and unable to communicate normally with people outside their bubble. Even apart from the individual mental distress caused by these feelings, there was a practical edge to the inability to interact normally with other people. Since doing almost anything in these contexts needs community approval and support, a lack of communication with others also means a lack of the ability to access this kind of support. Knowing this, and being unable to do anything about it, added a dimension of deep helplessness to the anxieties and fears already experienced by these reverse migrants.
“Ever since the time I left (to be a migrant worker), I felt that I was alone in the city, but here, at home, there are so many people who will help if anything happens. I thought that here, we are one. (…) I would say that to others in the city, too (…) that everything is always fine once I get home, where there are so many people I know. But now I can't meet people, can't talk properly, I feel like I can't talk to people anymore. Even on the phone, I don't feel like talking to anyone. Then sometimes my wife tells me if there is a problem (emergency), who will you call? (…) no, she is right. I am very afraid of that.” (Kapil, 43, UP)
3.1.1.4.5. The future
An additional dimension that did not map onto the typology, but needs particular mention in the context of High Vulnerable, is the notion of the future. This notion of the future differs from the notion of the future in the “Future focus” (low sources of distress, high feelings of precarity) quadrant, because High Vulnerability holds a much closer possibility of resources running out, and families being left destitute.
Unable to catch any glimpse of what the future would hold, this made those in highly vulnerable situations anxious, depressed, and angry. Some felt that giving in to fate was the only recourse, others were depressed and angry about the fact that they had tried their best to support their families, and done everything right, but there they were, back in the homes they had migrated out of, struggling to make ends meet. A future in which everything returns to normal was the dearest hope of these migrants, this includes work, school, mobility, and the relatively easy availability of food and medicine.
“I can't see anything ahead. When will this (the lockdown) end, when will I return to the city, will there be work or not (…) what do I do if there is no work? I can't come back here (to the village home). There is no work here.” (Dinesh, 34, UP)
“When I have bad headaches, I know that I am scared of the future, what will happen now, in the next few months (…) until covid ends, that feels like a headache. Sometimes I think about that so much that my head feels it is going to explode.” (Robi, 41, WB)
In the absence of working welfare systems, children are the social security for parents in India. Education is an investment in their own futures, as well as the future of their children. Online school was difficult for children of all ages, with issues with internet access and no upgraded textbooks. But the impacts of no school were the most profound on younger children, those whose ability in reading and writing develops from day to day. Parents felt that the lack of school was setting children back quite badly, and they doubted that this gap in the critical learning years would be made up in the future.
Another dimension of worry with regard to children was that they were not being socialized in the company of their peers, because of the lockdown. This socialization is perceived as essential, because in the local communities in which these participants live, getting along with others and having access to community resources is an important way to get through both ordinary and difficult times.
“When she (his young daughter) was going to school, every time I would come back (from the city), she would say, look I learned this! I learned this too! Then she would say, I know more than you! I loved seeing that, hearing that (…) Now she is just at home, no lessons, it's been so long (…) don't know if she will ever go back to being that way.” (Latif, UP, 32)
“My wife cannot read and write, I read a little. There is no one at home to help him. They would help him in school, but who knows when school will open again. Do you think he will be able to catch up?” (Kumar, Bihar, 31)
4. Discussion
Jhadav et al. (2015) propose “ecologies of suffering” as a term necessary to understand the issues of mental health in India. In this conception, “suffering is profoundly affected by ecological relations that are contingent on local particularities (…) Asymmetric interactions between people, the environment, and institutions governing both, generate socially toxic landscapes that are actively counter-therapeutic (…) Within the context of India's new development agenda, such local ecologies are continually emerging across the country (…).” (p. 12–13). The mental health ecologies that participants described in this study fall under the ambit of these “ecologies of suffering,” and any humanistic forward movement in this area must seek to alleviate this suffering. Moreover, in order not to fall into top-down policy making, it would approach this through the possible intervention points that precarious migrant workers themselves voice as important in their lives (Dutta and Kaur-Gill, 2018).
In his work with migrant construction workers in Singapore, Dutta (2017) theorizes that simply training for behavior change (on the part of migrant workers) may be less effective than a more inclusive approach that compliments such training with policies that create structural change relevant in the lives of migrants, and ensuring “a broader culture of respect for migrant construction workers” (p. 10).
Keeping this idea of respect front and center while looking into the “ecologies of suffering” in this study, we initially sought to move from the voiced distress of migrants to possible individual policy and program solutions that would address this suffering. However, as we thought through the issues in the typology, it was clear that this may not be an appropriate moment to suggest fine-grained solutions that address individual points and offer specific interventions. The reason for this is that specific solutions address specific issues, whereas, in the area of mental health and India, we are dealing with a much broader systemic disrespect of the constantly difficult lives and labor of migrants and their enormous and ongoing contribution to the building of contemporary India. Therefore, in our suggestions of actions that aim to ameliorate the mental distress of migrants, especially migrants during the crisis, we start at the beginning.
It is difficult to reach support to marginal people when there exist no concrete and updated figures about the number of people a policy or program is meant to address. There exist no contemporary, updated figures for the number of migrants in India. This lack of concrete enumeration and acknowledgment implies that in experience the positions of migrants are extremely fluid, with not even theoretical categories holding them in place in the economic structure—they are truly invisible, always precarious, and constantly at risk of falling into greater vulnerability.
4.1. An accurate count
In the first step of acknowledgment, it is both urgent and essential to do an actual count of the number of migrant workers in India, at both aggregated, and disaggregated levels. Furthermore, it is important that this count is updated regularly, like the Census. This would be the first step in being able to reach vulnerable migrants, in order to deliver any benefits that they need. The further research questions that need to be asked here are in the domain of demography and beyond the scope of this paper.
4.2. Cycles of mobility
In the second step of acknowledgment, systems and structures will need to acknowledge that migrants live across points of origin and destination–and that the points of destination change over cycles of migrancy. Here, acknowledgment follows the Oxford Languages Dictionary definition of “the recognition of the existence or truth of something.” Apart from the clear need for policy to recognize the mobility of migrant's lives, the larger truth being recognized here is that migrant workers are essential to contemporary India and deserve resources and benefits channeled toward their wellbeing, no matter where they may be located.
4.3. A portable ID
In the third step of acknowledgment, migrants would ideally be issued a portable ID. This would be the equivalent of a US social security number, portable across states of India, and linking the national, state, and district levels for migrant origin and destination–so any benefits can move as migrants do. Banks and other institutions would accept this card as a valid ID.
Participants pointed out that they did not have access to healthcare, rations, or any other benefits such as a school for their children when they were migrants in the city. These benefits were tied to their points of origin, where, as migrant workers, they spent relatively little time, before the pandemic. Since their benefits at points of origin were not regularly used, it was difficult to start accessing them when they returned, particularly at the short, or no notice that the pandemic reversed migration engendered. An ID that moves with workers may help alleviate this problem, and allow workers to access resources wherever they go for work. It would also allow single-destination longer-term migrants to take families with them. There are at least two questions for further research arising from the idea of a portable ID. The first is the manner and robustness of the counts that feed the ID, and the second is the shape of the ID itself.
4.4. Response from financial institutions
Banks are key to a safety-net for migrants because they (1) hold personal savings that can be accessed at times of distress like the pandemic lockdown, (2) may be available for loans, to build local capacity for income generation at ordinary times (i.e., loans to start small businesses such as shops, or buy rickshaws), and (3) serve as a buffer for survival (i.e., loans to buy food and medicine, and start up small businesses as above) at times of crisis like the lockdown. Participants across centers reported that such small loans would ease their stress considerably, and some said that if such modes of starting up income at their points of origin were open to them, they would probably choose not to migrate.
Those who had a bank account reported the difficulties they experienced when they opened it, because of the kinds of paperwork required to open a savings bank account. As discussed in the previous section, identification documentation is a problem for migrants. Even though the government eased the bank account documentation rules for migrants in late 2019 (Press Trust of India, 2019), participants said that the process is still complex enough to be intimidating.
While paperwork rules may have been relaxed for migrants to open bank accounts, highly vulnerable participants reported that paperwork and minimum balance rules for loans remain difficult for migrants to navigate. Those with financially High Vulnerable characteristics are hesitant to apply for loans and are frequently refused when they apply. The lack of local loans, except with high-interest moneylenders, implies that migrants will have to leave points of origin, again and again, never being able to set up a viable source of income at home. This echoes the kind of cyclical migration situation that Silvey and Parreñas (2020) describe as precarity chains–“the transfer of insecure jobs and financial insecurity (low wages, indebtedness) across places and people” (p. 3461), within India.
It is clear from the interviews and analysis that the financial burden is extremely stressful for migrant workers. Further research by specialists in this area is required, in order to map how the processes that currently restrict migrant access to financial support can be eased to make them workable for the marginalized.
4.5. Response from health institutions
The field of health has two components: (1) health care relating to the pandemic and other physical ailments and (2) mental health care helps migrants deal with the stress of their experiences.
Going by the many anxieties participants reported about the healthcare system, it is essential that health systems be updated to provide better healthcare to people in rural and semi-rural areas. At times of crisis such as the pandemic, healthcare systems need to take into account wider events in the public space, such as reverse migration. Such a movement of people across spaces is bound to challenge local health capacities at points of origin, so it would make sense for program plans to already be in place at such points. In situations of lockdown, when mobility is difficult and transport expensive, it is necessary to provide outreach health services to reach vulnerable populations.
An additional factor related to health that requires an institutional response is the availability and prices of medicines. Participants reported that medicines were difficult to source during the pandemic lockdown, and the prices of medicines were subject to fluctuation. The stabilization of the prices and distribution of medicine is important at all times but assumes particular urgency in the context of the pandemic.
In terms of mental health, experts seem to agree that the current capacity for marginal people is lacking in both quality and quantity (Singh, 2018; Harihara et al., 2021). Addressing this gap is a matter of urgency, since the multiple stresses of the pandemic lockdown, added to the already marginalized conditions of migrant life, make for a potent mixture of sources of distress–as is clear in this study. Since resources are of prime importance to the implementation of policy, it must be noted here that India's 2022 mental health budget is <0.7% of the budget for health and family welfare (India Mental Health Observatory, 2022).
Pathare (2022) comments that the financial allocation in mental health for each district remains unaltered from several years before the pandemic. This leaves little space for resources to train mental health personnel, or provide outreach services, both of which are essential to address the difficult situation in mental health at the current time, snowballing into the near future. It is essential that budgetary resources be increased to build appropriate and affordable infrastructure to shore against that time. It is also important that the facilities so created be approachable, affordable, and portable, for migrant workers experiencing chains of precarity.
4.6. The correct information
A way needs to be found to address the widespread anxiety that participants reported with regard to information. The overwhelming amount of information coming in from multiple mass media and interpersonal sources was identified by them as causing a lot of stress. This stress was heightened when parts of the information were found to be exaggerated or untrue. As participants pointed out, discovering that information they believed was true, was actually untrue, made them doubt the validity of other information they heard. This, in turn, led to more uncertainty and confusion.
It is difficult to prevent rumors and half-truths from circulating among people, particularly in contexts of high anxiety like a pandemic. In India, this is as true of the sensationalistic TV mass media, as it is of localized rumors that fire fear and panic through hyperlocal and local contexts. This is an area that needs detailed mapping, as relatively short-lived rumors and hearsay (cases of infection, availability of essential medication) were reported to create spikes of severe distress in migrants.
From a communication point of view, it may be useful to create tools that are easy to understand and implement, that help low-literacy individuals distinguish between degrees of truth-value in information. Also from a communication point of view, that sounds like an immensely complex and challenging task, and further research is needed to define even the most useful shape of the framing question.
What holds true, however, is that ways need to be found to collate reliable local information that is relevant to the everyday needs of marginal people, and reach the people who are most affected by the lack of such information. Going by the voices of participants in this study, these areas would be access to food/ration, loans, medicine, and healthcare facilities, but this is only the beginning of such a list. The mapping needed in this area will need to center around two basic questions: (1) what kinds of local information do marginal people require during times of crisis? and (2) how best to reach them?
4.7. Community and mental health care
In the context of migrant mental health, movement makes for precarity. Their movements between a point of origin and multiple destination points create chains of precarity, keeping them from settling in one place, and creating durable relationships that sustain over time. The findings from this study on the dimension of isolation show how important community and social support are to these migrants, and how distressed they feel when it draws away or becomes unavailable for any other reason.
The informal community support that migrants depend on is still available to some. However, the affection of friends and relatives may not be enough, to deal with the mental health issues that seem inevitably consequent to the experiences of these migrants. It is, therefore, imperative to build sustainable infrastructure and other capacities in mental health, to help migrants cope, with experiences like the pandemic lockdown and its consequences. The results of this study say that at least part of such an initiative would need to create ways for people to interact regularly with each other, so that, social relationships do not slide as badly as participants reported they did.
Dutta (2015) discusses how neoliberal ideologies make it necessary for the poor of the Global South to move between sites of precarity. This maps a movement, including a starting point, a process of shift, and a destination, all three of which are spaces in which the unique vulnerabilities of migrants are intensified. The movement itself also creates precarity, making it difficult for migrants to move toward either financial or relational stability within communities, over the longer term. This article focuses on an in-between point during crisis—home, which during the reverse migration was all three—an origin point, a destination, and an in-between point, since the migrants would eventually return to urban and semi-urban sites of work.
The intention of this typology is to provide an organized window into the large range of voiced experiences, and codified understandings, from the rich description provided by migrants of their own lives. By doing this, it hopes to help inform the development of both further research, and policy in this area. The COVID-19 crisis may arguably be passing, but the possibility of a public crisis related to climate change or further disease remains real in India.
The multidimensional typology in this article is also intended to be a starting point, and we very much hope that it is added to, and grows through future research at the intersection of migrants and mental health. While money, health, information, the individual in society/ Isolation, and the future—the major themes here, are consistent with the literature in this area, more fine-grained issues, both vertical and horizontal, need to be explored in detail by intersectional experts in this area and connected fields. As the research grows, we hope that policy-makers will move toward including the voiced concerns of marginalized migrants in their consideration-set when setting the agenda for mental health in India.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by IRB, Monk Prayogshala, Mumbai, India. The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Acknowledgments
Thanks to Varun Arora and Subhashish Sarkar for their help with this difficult project.
Conflict of interest
SR was employed by Behavioural Insights, Architecture and Strategy.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adhikari, A., Goregaonkar, N., Narayanan, R., Panicker, N., and Ramamoorthy, N. (2020). Manufactured maladies: lives and livelihoods of migrant workers during covid19 lockdown in India. Indian J. Labour Econ. 63, 969–997. doi: 10.1007/s41027-020-00282-x
Babu, V. B., Kusuma, Y. S., Sivakamy, M., Lal, D. K., Marimuthu, P., Geddam, J. B., et al. (2017). Living conditions of internal labour migrants: a nationwide study in 13 Indian cities. Int. J. Migr. Border Stud. 3, 328–351. doi: 10.1504/IJMBS.2017.086963
Bailey, K. D. (1994). Typologies and Taxonomies: An Introduction to Classification Techniques. Thousand Oaks, CA: Sage. doi: 10.4135/9781412986397
Banerjee, A. (2021). 80% first visits in rural India are to unqualified doctors. NDTV Oct 4. Available online at: https://www.youtube.com/watch?v=r0L3fc5kmYk (accessed July 1, 2022).
Basu, R. (2019). Public policy in India: transformatory shifts or incremental changes? Indian J. Public Adm. 65, 225–228. doi: 10.1177/0019556118822030
Berchoux, T., Watmough, G. R., Hutton, C. W., and Atkinson, P. M. (2019). Agricultural shocks and drivers of livelihood precariousness across Indian rural communities. Landsc. Urban Plan. 189, 307–319. doi: 10.1016/j.landurbplan.2019.04.014
Bhagat, R. B., Reshmi, R. S., Sahoo, H., Roy, A. K., and Govil, D. (2020). COVID19, Migration and Livelihood in India: A Background Paper for Policymakers. Mumbai: Indian Institute for Population Sciences. Available online at: https://iipsindia.ac.in/sites/default/files/iips_covid19_mlli.pdf (accessed January 11, 2022).
Bond, G. R. (2018). Evidence-based policy strategies: a typology. Clin. Psychol. Sci. Pract. 25, e12267. doi: 10.1111/cpsp.12267
Chatterjee, C. B. (2006). Identities in Motion: Migration and Health in India. Mumbai: Centre for Enquiry into Health and Allied Themes (CEHAT). Available online at: http://www.cehat.org/go/uploads/Hhr/migrants.pdf (accessed January 13, 2022).
Chaudhari, R. (2020). COVID19 pandemic: mental health challenges of internal migrant workers of India. Asian J. Psychiatr. 54, 102254. doi: 10.1016/j.ajp.2020.102254
Chauhan, V. S., and Chauhan, S. (2022). Mental health in India: a perspective. Indian Express: Health Feb 11, 10.50. am. Available online at: https://indianexpress.com/article/lifestyle/health/mental-health-in-india-a-perspective-anxiety-depression-stress-7764309/ (accessed 8 May 2022).
Chavan, B. S., Sidhana, A., Arun, P., Rohilla, R., Singh, G. P., et al. (2021). Factors leading to reverse migration among migrant workers during the COVID19 pandemic: a multicenter study from North India. Prim. Care Companion CNS Disord. 23, 20m02810. doi: 10.4088/PCC.20m02810
Dandekar, A., and Ghai, R. (2020). Migration and reverse migration in the age of COVID19. Econ. Polit. Wkly. 55, 28–31.
Datta, A. (2020). Circular migration and precarity: perspectives from rural Bihar. Indian J. Labour Econ. 63, 1143–1163. doi: 10.1007/s41027-020-00290-x
DeMarchi, G., Lucertini, G., and Tsoukiàs, A. (2016). (2016). From evidence-based policy making to policy analytics. Ann. Oper. Res. 236, 15–38. doi: 10.1007/s10479-014-1578-6
Dutta, M. J. (2015). Neoliberal Health Organizing: Communication, Meaning, and Politics. Walnut Creek, CA: West Coast Press. doi: 10.4324/9781315423531
Dutta, M. J. (2017). Migration and health in the construction industry: culturally centering voices of Bangladeshi workers in Singapore. Int. J. Environ. Res. Public Health 14, 132. doi: 10.3390/ijerph14020132
Dutta, M. J., and Jamil, R. (2013). Health at the margins of migration: culture-centered co-constructions among Bangladeshi migrants. Health Commun. 28, 170–182. doi: 10.1080/10410236.2012.666956
Dutta, M. J., and Kaur-Gill, S. (2018). Precarities of migrant work in Singapore: migration, (Im)mobility, and neoliberal Governmentality. Int. J. Commun. 12, 4066–4084. doi: 10.1177/09732586211002927
Dutta, M. J., and Pal, M. (2020). Theorizing from the Global South: dismantling, resisting, and transforming communication theory. Commun. Theory 30, 349–369. doi: 10.1093/ct/qtaa010
Gaiha, S. M., Sunil, G. A., Kumar, R., and Menon, S. (2014). Enhancing mental health literacy in India to reduce stigma: the fountainhead to improve help-seeking behaviour. J. Public Ment. Health 13, 146–158. doi: 10.1108/JPMH-06-2013-0043
Glaser, B., and Strauss, A. (1967). The Discovery of Grounded Theory: Strategies for Qualitative Research. Mill Valley, CA: Sociology Press. doi: 10.1097/00006199-196807000-00014
Gururaj, G., Varghese, M., Benegal, V., Rao, G. N., Pathak, K., Singh, L. K., et al. (2016). National Mental Health Survey 2015-16, Summary. Bengaluru: National Institute of Mental Health and Neuro Sciences (NIMHANS). NIMHANS publication no. 128.
Harihara, S., Damodaran, D., Malathesh, B. C., Nirisha, L. P., Narayana, M., et al. (2021). Telepsychiatry during the COVID19 pandemic: reflection from India. Telemed. Health Today 6. doi: 10.30953/tmt.v6.263
India Mental Health Observatory (2022). Budget for Mental Health: Analysis of Union Budget 2022-2023. The Centre for Mental Health, Policy and Law. Available online at: https://cmhlp.org/wp-content/uploads/2022/02/IMHO-Union-Budget-for-Mental-Health-2022-23.pdf (accessed March 02, 2022).
Jesline, J., Romeate, J., Rajkumar, E., and George, A. J. (2021). The plight of migrants during COVID-19 and the impact of circular migration in India: a systematic review. Humanit. Soc. Sci. Commun. 8, 1–12. doi: 10.1057/s41599-021-00915-6
Jhadav, S., Jain, S., Kannuri, N., Bayetti, C., and Barua, M. (2015). Ecologies of suffering: mental health in India. Econ. Polit. Wkly. 50, 12–15.
Karia, M. T., and Deshmukh, K. (2020). Urgent need for reforms in law and policy for mental health in India. Bar and Bench, 13 December, 11.04. am. Available online at: https://www.barandbench.com/columns/urgent-need-for-reforms-in-law-and-policy-for-mental-health-in-india (accessed 5 May 2022).
Karlan, D., Mullainathan, S., and Roth, B. N. (2019). Debt traps: market vendors and moneylender debt in India and the Philippines. Am. Econ. Rev. Insights 1, 27–42. doi: 10.1257/aeri.20180030
Khan, A., and Arokkiaraj, H. (2021). Challenges of reverse migration in India: a comparative study of Indian and International comparative migrants in the post-COVID economy. Comp. Migr. Stud. 9, 49. doi: 10.1186/s40878-021-00260-2
Khan, J. H., and Shazia, and Shamshad (2016). Age-sex wise reasons for internal migration in Uttar Pradesh, India. Glob. J. Multidiscip. Stud. 5, 113–132.
Kluge, S. (2000). Empirically grounded construction of types and typologies in qualitative social research. Forum Qual. Sozialforschung 1, 14. doi: 10.17169/fqs-1.1.1124
Kumar, S. M., and Sahu, P. P. (2013). Employment growth, education and skills in India: Emerging perspectives. Indian J. Labour Econ. 56, 95–122. Available online at: https://www.researchgate.net/publication/256848415_Employment_Growth_Education_and_Skills_in_India_Emerging_Perspectives
Kusuma, Y. S., and Babu, B. V. (2018). Migration and health: a systematic review on health and health care of internal migrants in India. Int. J. Health Plann. Manag. 33, 775–793. doi: 10.1002/hpm.2570
Mookerjee, D., Chakravarty, S., Roy, S., Tagat, A., and Mukherjee, S. (2021). A culture-centered approach to experiences of the Coronavirus pandemic among internal migrants in India. Am. Behav. Sci. 65, 1426–1444. doi: 10.1177/00027642211000392
Mukherjee, P., Paul, G. D., Bino Paul, G. D., and Pathan, J. I. (2013). “Migrant workers in the informal sector: a probe into working conditions,” in ATLMRI Discussion Paper Series no. 9. Available online at: https://www.shram.org/researchpapers/papers/20130305105845 (accessed February 24, 2022).
Murthy, P., Malathesh, B. C., Kumar, C. N., and Bara Math, S. (2016). Mental health and the law: an overview and need to develop and strengthen the discipline of forensic psychiatry in India. Indian J. Psychiatry 58 (Suppl. 2), 181–186. doi: 10.4103/0019-5545.196828
Nanda, P. K. (2020). (2020) Uttar Pradesh invokes ordinance to exempt businesses from all key labour laws. Mint, 8 May 2020, 12.05 a.m. IST. Available online at: https://www.livemint.com/news/india/uttar-pradesh-invokes-ordinance-to-exempt-businesses-from-all-key-labour-laws-11588876096259.html (accessed January 17, 2022).
Parreñas, R., Silvey, R., Hwang, M. C., and Choi, C. A. (2019). Serial labor migration: precarity and Itineracy among Filipino and Indonesian domestic workers. Int. Migr. Rev. 53, 1230–1258. doi: 10.1177/0197918318804769
Pathare, S. (2022). India's COVID-hit mental health sector deserves more than 1% of health budget. The Quint 8 Feb, 1:07 IST. Available online at: https://www.thequint.com/voices/opinion/indias-covid-hit-mental-health-crisis-deserves-more-than-1-of-health-budget#read-more (accessed February 09, 2022).
Press Trust of India (2019). Govt eases norms for opening account for migrants using Aadhar KYC. Business Standard, November 14, 2019. Available online at: https://www.business-standard.com/article/pti-stories/govt-eases-norms-for-opening-bank-account-for-migrants-with-aadhaar-kyc-119111401822_1.html (accessed January 25, 2022).
Rao, N., Narain, N., Chakraborty, S., Bhanjdeo, A., and Pattnayak, A. (2020). Destinations matter: social policy and migrant workers in the times of covid. Eur. J. Dev. Res. 32, 1639–1661. doi: 10.1057/s41287-020-00326-4
Sagar, R., Dandona, R., Gopalkrishna, G., Dhaliwal, R. S., Singh, A., et al. (2020). (2020). The burden of mental disorders across the states of India: the Global Burden of Disease Study 1990-2017. Lancet Psychiatry 7, 148–61. doi: 10.1016/S2215-0366(19)30475-4
Shrivastava, A., Johnston, M., and Bureau, Y. (2012). Stigma of mental illness 1: clinical reflections. Mens Sana Monogr. 10, 70–84. doi: 10.4103/0973-1229.90181
Silvey, R., and Parreñas, R. (2020). Precarity chains: cycles of domestic worker migration from Southeast Asia to the Middle East. J. Ethn. Migr. Stud. 46, 3457–3471. doi: 10.1080/1369183X.2019.1592398
Singh, G. P. (2021). Psychosocial and mental health issues of migrants amidst COVID-19 pandemic in India: a narrative review. Indian J. Psychol. Med. 43, 473–478. doi: 10.1177/02537176211044802
Singh, O. P. (2018). District Mental Health Programme: need to look into strategies in the era of Mental Healthcare Act, 2017 and moving beyond Bellary model. Indian J. Psychiatry 60, 163–164. doi: 10.4103/psychiatry.IndianJPsychiatry_304_18
Srivastava, A., Arya, Y. K., Joshi, S., Singh, T., Kaur, H., Chauhan, H., et al. (2021). Major stressors and coping strategies of internal migrant workers during the COVID-19 pandemic: a qualitative exploration. Front. Psychol. 12, 648334. doi: 10.3389/fpsyg.2021.648334
Srivastava, R. (2012). “Internal migration in India: an overview of its features, trends, and policy challenges,” in Workshop Compendium (Vol. 2: Workshop Papers) of the National Workshop on Internal Migration and Human Development in India, 6–7 December. Varanasi: UNESCO, UNICEF, and ICSSR.
Subramanian, S. (2020). How Hindu supremacists are tearing India apart. The Guardian. Available online at: https://www.theguardian.com/world/2020/feb/20/hindu-supremacists-nationalism-tearing-india-apart-modi-bjp-rss-jnu-attacks (accessed March 03, 2022).
Thakur, A. N. (2020). Economic implications of reverse migration in India. J. Migr. Affairs III, 16–31. doi: 10.36931/jma.2020.3.1.16-31
WHO (2022). Health Topics: Mental Health in India. Available online at: https://www.who.int/india/health-topics/mental-health#:$\sim$:text=WHO%20estimates%20that%20the%20burden,estimated%20at%20USD%201,03.%20trillion (accessed 5 May 2022).
Keywords: migrants, COVID-19, mental health, precarity, India, voices, typology, policy
Citation: Mookerjee D and Roy S (2023) A typology of the sources of mental health precarity among migrant workers in India during the COVID-19 lockdown. Front. Commun. 7:969879. doi: 10.3389/fcomm.2022.969879
Received: 15 June 2022; Accepted: 12 December 2022;
Published: 20 February 2023.
Edited by:
Naomi Tan, University of Texas MD Anderson Cancer Center, United StatesReviewed by:
Raihan Jamil, University of Liberal Arts Bangladesh, BangladeshSmrithi Vijayakumar, National University of Singapore, Singapore
Copyright © 2023 Mookerjee and Roy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Devalina Mookerjee,  ZGV2YWxpbmFtQGdtYWlsLmNvbQ==
ZGV2YWxpbmFtQGdtYWlsLmNvbQ==