Abstract
Context: Dementia is one of the top five chronic diseases, which has an overwhelming impact on patients' life quality, family, and caregivers. Currently, research relating to people with dementia (PwD) focuses on the deterioration of cognitive abilities. A more innovative approach, and the one taken by this paper, is focusing on methods to maintain and improve functionality, communication and quality of life of PwD by building on remaining capacities in the yet unexplored domain of emotional and social intelligence (ESI). The use of serious games for PwD (SG4D) aimed at building social and emotional capacity is a budding field of research.
Objectives: Proof of concept that the, low cost, easy to deploy SG4D, called “My Brain Works” (MBW), co-designed with PwD, enhances ESI, based on the Bar-On ESI model.
Methods: 27 PwD, clients at MELABEV dementia day center, participated in a mixed methods 12 weeks pilot, proof of concept study using a tablet SG4D co-designed with PwD. Quantitative performance data was collected automatically by the tablet during game sessions. In this paper we focus on the analysis of the qualitative and quantitative data related to ESI, observed by 10 different researchers, during each game session.
Results: Quantitative data revealed: both the PwD with high and low MoCA scores had similar average ESI scores. Qualitative analysis revealed that the PwD demonstrated 9 sub-components of the Bar-On ESI Model.
Conclusion: While there is no drug to stop cognitive decline associated with dementia, interventions related to ESI, on the other hand, may improve functioning and quality of life. Despite declines in cognitive abilities, our study shows that a tablet based SG4D can stimulate their ESI and evoke responses in self-awareness, empathy, social and communication capacities. Using SG4D to exercise and maintain social skills is an area that may be promising in the future and may help counter the negative effects of social isolation and loneliness. Such games, while not focusing on cognitive improvement, may also impact on cognitive functioning and help bridge the gap between caregiver and PwD. More research is needed with larger sample sizes.
Introduction
Dementia is a neurodegenerative illness, which has an overwhelming impact on the patient, family and caregivers (World Health Organization, 2019). Most research relating to people with dementia (PwD) focuses on the deterioration of cognitive abilities. Rarely does it take note of the remaining capacities of emotional and social intelligence (ESI), though many researchers suggest that these intelligences are much more accurate determinants of successful communication and relationships than mental intelligence (Goleman, 2006). This is true especially in dementia, leading the current study to focus on emotional and social intelligence and dementia. Specifically, we aimed to show a proof of concept for a novel serious game for dementia SG4D, entitled “My Brain Works” (MBW) (Tziraki et al., 2017). We focused on whether PwD, even with severe dementia, can engage with a computerized game, enjoy the game and socially interact with it in a meaningful way.
Cognitive functioning in several domains may change in healthy aging (e.g., executive functions, see Hasher and Zacks, 1988), while functioning in others are retained (e.g., speech processing in ideal listening conditions, see Ben-David et al., 2011) or even increase (e.g., vocabulary, see Ben-David et al., 2015). Compared to cognitive performance, emotional processing is taken to be relatively reserved in healthy aging (even if changed; Ben-David et al., 2019) and in unhealthy aging. This leads the current literature to recommend that care of people with dementia should be focused on the stimulation of emotional function (e.g., sympathy and empathy), rather than relying solely on the stimulation of cognitive function (Hirazakura et al., 2008; Fujii et al., 2014a).
Not all emotional processes are preserved in dementia. PwD may have emotion processing deficits in several domains, along with their cognitive deficits, for example reduced perception of emotional facial expressions (Hoffmann et al., 2010; Klein-Koerkamp et al., 2012a,b; Kumfor et al., 2014). This ability plays a significant role in communication and is one of the most important aspects of social cognition (León et al., 2011; Torres et al., 2015; Torres Mendonça De Melo Fádel et al., 2018). Social cognition allows individuals to partake in social situations, enabling them to perceive and recognize the thoughts, emotions, and behaviors of others (Shany-Ur and Rankin, 2011). An intact association between implicit and explicit cognitive functions are required in order to successfully decipher and interact with the social environment around us. As PwD show changes in social cognition (Snowden et al., 2003; Poveda et al., 2017) it can further impair their quality of life. Indeed, PwD may display difficulties in understanding social cues or recognizing emotions (Phillips et al., 2010). For instance, some PwD have trouble adapting to change, are unconcerned with others' feelings and are unable to control emotions. These social cognition deficits are independent of cognitive dysfunction and may increase over time (Cosentino et al., 2014). Impairment in emotion recognition by PwD has a large effect on the caregiver. These impairments can cause failures to modify behavior that is offensive to others (Blair, 2003).
The psychological and behavioral symptoms of dementia are reported to occur in ~90% of people with dementia. These symptoms can include such things as: anxiety, apathy, emotional lability, aggressiveness, disinhibition, and irritability. This can lead to breakdowns in communication and increased conflict in relationships, and has implications for caregiver burden and depression (Martinez et al., 2018). Apathy and withdrawal in PwD can be as distressing to caregivers as agitation and aggression (Burns and Iliffe, 2009). Taken together, these factors play an important role in caregivers' decisions to institutionalize the PwD and are detrimental to their quality of life (McLellan et al., 2008).
Empathy is essential for social interaction as well, and a crucial trait to understand the intentions and behaviors of others and to react accordingly. Empathy results from the interaction of four components: shared neural representation, self-awareness, mental flexibility, and emotion regulation. All these capacities can also be affected in dementia (Bartochowski et al., 2018; Fischer et al., 2019). This may relate to a deficit in perception of positive emotions. Perceiving positive emotions in others helps people feel connected to one another. Failure to recognize and respond to positive emotions can make people with dementia seem cold and distant, making it harder for others to connect to them.
On top of all the other difficulties, PwD tend to be socially isolated and therefore lack opportunities to exercise various aspects of their remaining emotional and social intelligence (ESI). They are unable to express themselves clearly, so they spend most of their time alone, doing little and not being engaged in meaningful activity. The health and well-being consequences of social isolation and loneliness are increasingly recognized (Cacioppo and Hawkley, 2009; Cacioppo and Cacioppo, 2014; Cole et al., 2015). Engaging a PwD in meaningful activity is therefore important and is a priority when providing care for this population in order to improve well-being through an increase in positive emotions (Jones et al., 2015).
Unfortunately, most efforts related to PwD focus on cognitive changes from dementia while ignoring the fact that there is remaining emotional intelligence. That while there is a growing call in the recent literature to focus on the remaining capacities of emotional intelligence (Hirazakura et al., 2008; Fujii et al., 2014a). Indeed, the most common, and recognized, cognitive evaluations used with PwD are the Montreal Cognitive Assessment Scale (MoCA) (Wallace et al., 2019), and the Mini-Mental State Examination (MMSE) (Creavin et al., 2016); while there is very little evaluation of emotional and social abilities related to PwD. However recently, researchers in Japan (Fujii et al., 2014b) have developed and tested a Mini-Emotional State Examination (MESE) for the examination of emotional functions in people with dementia, to accompany the MMSE. They found that the difference in distribution of MMSE and MESE scores show that cognitive and emotional functions are independently affected in dementia, and therefore assessment of both these functions should be taken into consideration in the care and management of PwD. In fact, they encourage working with the remaining emotional intelligence of PwD (Hirazakura et al., 2008; Fujii et al., 2014a). Following this, the goal of the current study is to test whether PwD can engage with our novel serious game, “MBW,” in a meaningful way (social and emotional) accompanied by positive emotions.
The Current Study: Can PwD Engage Emotionally and Socially With MBW SG4D?
There are currently three major conceptual models relating to emotional and social intelligence: (a) the Mayer-Salovey-model (Mayer and Salovey, 1997) which defines this construct as the ability to perceive, understand, manage and use emotions to facilitate thinking, measured by an ability-based measure (Mayer et al., 2002); (b) the Goleman model (1998) which views this construct as a wide array of competencies and skills, measured by multi-rater assessment (Goleman, 2006); and (c) the Bar-On (2000) model which describes a cross-section of interrelated emotional and social competencies, skills and facilitators that impact intelligent behavior, measured by self-report (Bar-On, 1997, 2004) or multi-rater assessment (Bar On and Handley, 2003). The latter model was chosen as the theoretical basis for this study, as it was considered to be the most suited for observational analyses and training of the PwD population.
Table 1 presents three of the core elements in the Bar-On model of Emotional-social intelligence (ESI), (Bar-On, 2006) that were the focus of the current study. ESI, as conceptualized by the Bar-On model, is a multi-factorial array of interrelated emotional and social competencies, skills and facilitators that influence one's ability to understand and express themselves, understand others and interact with them, as well as cope with daily demands and challenges and pressures (Cherniss, 2004; Bar-On, 2006). It contains five main components (divided into 15 sub-components): intrapersonal, interpersonal, adaptability, stress management, and general mood. These core elements are at the basis for effective social interactions. Indeed, to accurately perceive, understand and express our feelings, and control our emotions (so they work for us and not against us) are essential qualities for effective communication, social adeptness, adaptability, self-actualization and happiness (Bar-On and Parker, 2000). Emotionally and socially intelligent behavior can be enhanced in school, the workplace and in the clinical setting in order to improve performance, self-actualization and subjective well-being (Bar-On, 2006). Much more research is needed in this area (Birks and Watt, 2007). As well, little has been done in the area of exercising and enhancing the emotional intelligence capabilities in those with dementia (McLellan et al., 2008). While there is decline in emotional social intelligence capacities associated with dementia, there are still many ESI abilities remaining that might not be apparent to the caregivers and could be enhanced (Fujii et al., 2014a).
Table 1
| Components | Sub-components | |
|---|---|---|
| Intrapersonal | Self-awareness and self-expression: | |
| Self-regard | To accurately perceive, understand and accept oneself. | |
| Emotional self- awareness | To be aware of and understand one's emotions. | |
| Assertiveness | To effectively and constructively express one's emotions and oneself. | |
| Independence | To be self-reliant and free of emotional dependency on others. | |
| Self-actualization | To strive to achieve personal goals and actualize one's potential. | |
| Interpersonal | Social awareness and interpersonal relationship: | |
| Empathy | To be aware of and understand how others feel. | |
| Social responsibility | To identify with one's social group and cooperate with others. | |
| Interpersonal relationship | To establish mutually satisfying relationships and relate well with others. | |
| Adaptability | Change management: | |
| Reality testing | To objectively validate one's feelings and thinking with external reality. | |
| Flexibility | To adapt and adjust one's feelings and thinking to new situations. | |
| Problem solving | To effectively solve problems of a personal and interpersonal nature. |
Three components of Bar-On's model of emotional social intelligence.
Serious games, developed especially for PwD (SG4D), in order to engage them through ESI, may help to exercise these remaining abilities, which may even also have some positive effects on cognitive functioning. Serious games may offer the promise of low cost easy to deploy interventions in the care of PwD (Astell, 2010; Robert et al., 2014). In addition, they require minimal professional supervision (i.e., by an occupational therapist) and can be played with the assistance of formal or informal caregivers.
Our novel SG4D, “My Brain Works” (MBW) was designed to answer these specific needs. In our original study, we presented MBW, a low cost, easy to deploy serious game, co-designed with and developed especially for PwD. Our major goal was to bridge the transfer gap between “game designers” practice and knowledge and neuro-psychosocial scientific knowledge of aging and dementia (Tziraki et al., 2017). The overall aim of our gaming approach was to facilitate people with moderate and advanced dementia to arrive at an increased sense of self efficacy, which, according to recent research in neuropsychology, directly contributes to psychological, cognitive, and physical health, and thus serves as a key enabler in augmenting and prolonging functionality (Choi and Twamley, 2013). The target was to train a set of functional simple daily tasks, essential and culturally relevant to daily life. For example, choosing current utensils for dinner (see Figure 1). Each task was then divided into subtasks, utilizing an occupational therapy methodology, primarily adapted from neuro-rehabilitation. The game screens were designed in a visually engaging way, considering several design issues related to sensory degradation (Ben-David and Schneider, 2009, 2010), topic (Ben-David and Icht, 2017, 2018) and goal changes (for discussion, see Ben-David et al., 2018). Users are asked to sort, find, drag, and move items on a tablet, using the simple and easy to use qualities of a touch screen. The original study (Tziraki et al., 2017) was designed to answer the following questions: (1) Are serious computer games acceptable, accessible and engaging for people with moderate and advanced dementia? (2) Are people with moderate and advanced dementia able to use a tablet? and (3) Can PwD improve the speed of performing a task with practice, indicating their ability to learn? That study demonstrated that “MBW” is (1) accessible, acceptable, and enjoyable for the target population; (2) PwD were able to use the tablet, enjoyed the game; and (3) were able to improve their speed of performance in “MBW.”
Figure 1
As a follow-up for the original findings, the current study aimed to investigate whether use of an improved version of the novel game can engage PwD, stimulate and exercise their remaining emotional and social capacities? To meet these objectives, 10 researchers were asked to observe PwD playing several sessions on the “MBW” SG4D to collect data on interactions, engagement both emotional and social. We present qualitative and quantitative analyses of their observations. The data was collected using a novel tool designed specifically for this study, the “MBW Emotional and Social Intelligence Evaluation Form” (see Appendix A). This observation form is an adaptation of the ACIS, occupational therapy assessment (Forsyth et al., 1999), to explore the emotive and social capacities of PwD's interactions with the MBW SG4D. This assessment tool includes the key domains of the Bar-On Model of Emotional and Social Intelligence.
The current study had several hypotheses tested in qualitative and quantitative analysis of observations. (1) PwD will interact with the SG4D; (2) PwD will be able to operate the game; (3) PwD will enjoy using the SG4D and will not be frustrated; and most importantly, (4) the use of a serious game may be able to act as an augmentative alternative communication for PwD and their caregivers, allowing the caregiver to enter the world of the PwD and learn about their hidden capacities, especially their emotional and social abilities (Berenbaum et al., 2011). This was tested by interactions with the tablet and by gauging effective communication with the care giver present during the game play.
Methods
Design of the New SG4D “MBW”
Goals and General Design
For the current proof of concept pilot study, we improved the English version of the SG4D “MBW” and built a user management and data collection system around it. We used the development process theory described at length previously (Tziraki et al., 2017), aiming to create a theory-based SG4D, with input from a multi-disciplinary team familiar with aging, dementia, user experience design, gaming theory, and technology, as well as direct input from end users (using the iterative process, see Valdez et al., 2015) and data collected automatically by the system.
In the second stage of development of “MBW” we focus further on user interface and design, aiming to increase social and emotional engagement—the act of being occupied or involved with external stimuli. It is not always clear how to effectively engage PwD in activities and derive the desired benefits, as well as how to measure engagement, especially since there has been a dearth of research examining engagement in PwD (Trahan et al., 2014; Perugia et al., 2018). There is evidence though, to suggest that interventions that support the sense of self, by using tasks or objects with specific meaning to the person, are more likely to engage PwD (Cohen-Mansfield et al., 2009; Zimmerman et al., 2011). Thus, explicit models of emotional identity offer an attractive mechanism for developing more appropriate and effective technologies. This is of specific importance, as PwD are much more focused on emotional and social issues than on abstract problems (Carstensen and Mikels, 2005; Mikels et al., 2005; Blanchard-Fields, 2007). But how exactly does one turn a flat screened tablet into a serious game that can evoke emotions and social interaction in PwD? This is truly challenging.
The methodology that we followed began with the choice of a multidisciplinary team familiar with aging, dementia, user experience design, gaming theory, and technology. Multidisciplinary collaboration is often encouraged in user centered design (UCD) including partnerships between designers and clinicians (Robert et al., 2014; Cornet et al., 2020). The synergies of the team helped to translate appropriate game ideas that came from the aging and dementia experts into emotionally and socially stimulating experiences designed with input of the user experience (UX), gaming and technology experts. We gave special consideration to design aspects that would trigger the PwD emotionally and socially, keeping in mind the importance of emotional alignment (Ienca et al., 2017; Robillard et al., 2018). We used the inclusive participatory design method which ensures benefits to end-users, promotes engagement and ensures usability (Robillard et al., 2018). We also considered more personalized aspects of the game screens (i.e., culturally appropriate, clear, welcoming pictures and design choices to enhance PwDs engagement with the SG4D).
Great care was devoted to the choice of each picture used, in order to increase emotional and social interaction with the SG4D. First, we chose to use real life photos as opposed to animations to make them more realistic and understandable. We chose pictures that would be familiar to a broad range of cultures, not childish, but that includes pictures of children, and all the generations. These intergenerational and family images with clear unambiguous emotional expressions were chosen to make it easier for PwD to recognize the emotions of the characters and empathize, sympathize and interact with them (McAllister et al., 2020), and give a feeling of warmth and belonging (see Figure 2). Nature scenes were included as well, to elicit emotions of calmness and enjoyment (Gamble et al., 2014; Thake et al., 2017).
Figure 2
The interdisciplinary team worked together to ensure instructions are clear, friendly and inviting for a person with dementia (Di Rosa et al., 2014; Mondini et al., 2014; Lam et al., 2015). Another aspect included throughout was appropriate and respectful humor (Berenbaum, 2003). Being able to understand humor is one of the capacities remaining for many in the middle stages of dementia. Since most people are not able to laugh spontaneously, the SG4D acts as a stimulus to trigger laughter. Indeed, laughing has positive psychological, physical and social benefits. It releases tensions, dilutes stress, and induces relaxation (Eng, 2000). Throughout, game tasks were designed to match the abilities of PwD in order to increase self-efficacy (Tziraki et al., 2017).
Each game screen was person-centered (Kitwood, 1997), and culturally appropriate to engage them in an interactive way. Figure 1 is a depiction of a sample game screen where the PwD was instructed to follow written and oral instructions to sort, find, drag, and move items on the tablet touch screen. Game screens targeted the following skills: eye hand coordination, language skills (reading, comprehension), understanding and following instructions, praxis, memory, sustained attention, and object recognition. They also targeted other physical, cognitive and emotional social skills such as gnosis, association, mental rigidity, recognition, abstraction, association, inhibition, basic math skills, logic, language and communication responses. All tasks included in game screens were in order to maintain appropriate challenges and spark interest throughout gameplay.
The system was designed in a modular way so that the game screens sequence can be interchanged, and various timings in the game are configurable. This allows for testing a variety of game experience scenarios.
The game's length, interaction timers and difficulty levels are all configurable in the system and may entail further experimentation. Indeed, the design, playfulness, feel, and looks of the system and game, were all inspired by the field of dementia care, as well as input of the MELABEV staff. We had a co-design approach to the game development based on the clients' feedback in terms of usability, and clarity for each screen of the game. We also included a training session for the PwD, before commencing the pilot, so they could learn how to use the technology. At the end of the iterative development stage, we had a prototype of a tablet-based game for PwD with 23 game screens including 15 “physical interaction screens” —where the PwD must sort, find, drag, and move items on the tablet touch screen, and eight “sensory interaction screens” —not requiring physical interaction with the tablet but where the PwD looks at pictures on the screen and interacts sensorially, emotionally and socially. This prototype was used for the pilot proof of concept study described here.
Technology Readiness Levels (TRL) Scale
The design of the novel “MBW” SG4D can be examined using an adaptation of NASA's Technology readiness levels (TRL) scale, similar to the EU's adaptation of the scale methodology (Earto, 2014). We also look at the methodology described by a publication by the LEITAT organization (Jamier et al., 2018). MBW's readiness level can be described by the matrix (see Table 2) using a similar adaptation to the TRL scale, as described by the LEITAT organization. We denote five components of the system, aiming to ultimately provide a competitive marketable solution, which encompasses the many aspects of therapy and user interaction described by this article, is robust and scalable, and is also coupled by credible research data and analysis.
Table 2
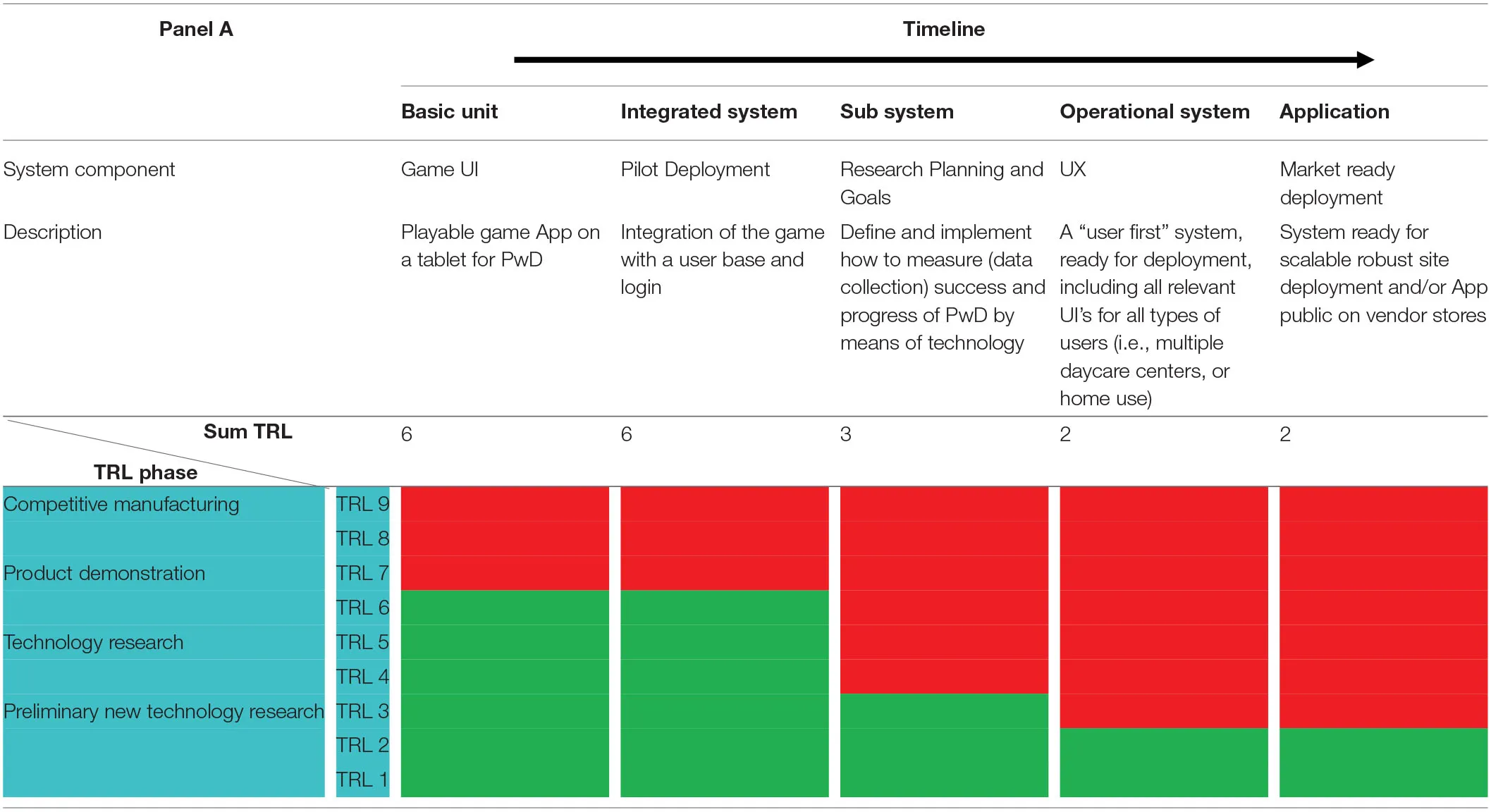 |
“MBW” technology readiness matrix.
Conceptually, we split development to specific research and development components, ranging from abstract ideas, to operational physical systems, and place them on a timeline, from left to right. The components and timeline are described by the columns of the Matrix. The various TRL's, according to the chosen scale, are placed on the Matrix's row. A table cell then links any component with any TRL. In the Matrix a green/red cell describes a completed/ uncompleted TRL, for the corresponding system component. The TRL phase is highlighted in blue.
Our (1) basic unit is the game itself, an App which can run on a tablet and shows the various game screens in succession. Next, we denote the (2) Integrated System, coupling the game App with a user login base and a server back-end to collect data. All development and coding having to do with the accompanying research are denoted (3) Sub System. Lastly, the penultimate and ultimate components are the (4) Operational System, a market deployment ready prototype, and (5) Application, the final software deployment solution, a robust and scalable technology product, encompassing all stages of physical site deployment.
The different components of the system are at various readiness levels ranging from “technology concept formulated” (TRL 2) to “technology demonstrated in a relevant environment” (TRL6; i.e., an active dementia day care center) as seen in Table 2. The basic unit and integrated system of “MBW” (column 1, 2 of Table 2) have been demonstrated to be at TRL level 6. We have successfully completed an initial system pilot, testing the various aspects of the system in one of MELABEV's 4 day-care centers, which can be regarded as a relevant environment for this game.
Proof of Concept Pilot Study
Setting
The present proof of concept pilot study took place at MELABEV, an English speaking, dementia day center, Jerusalem, Israel (Berenbaum, 2010). MELABEV has 4 day-care centers attended by ~500 PwDs, ranging from people with moderate cognitive impairment (MCI) to advanced dementia. While the literature reports on it being difficult to engage PwD in activities, the activity staff at MELABEV do their utmost to find the appropriate activities for each client (Berenbaum et al., 2017a,b). MELABEV's professional staff routinely uses computer games on a one-to-one basis for cognitive stimulation gaming (Berenbaum et al., 2011), as well as reminiscence therapy at the computer (Douglas et al., 2004). Primary family caregivers who enroll the PwD in the day care program consent to the participation of their family member with these kinds of technology, as well as all other activities in the day care center.
Meaningful informed consent for people with dementia is challenging. Thus, for our pilot study, we utilized the participatory consent process (Dewing, 2007, 2008). Before each gaming session, the research assistant asked the PwD if he/she agreed to participate in the gaming session. Upon agreement, the PwD voluntarily got up and was guided by the research assistant to a designated space (one of four quiet rooms) to play the SG4D. If the PwD did not agree to participate, or if he/she said or acted as if he/she didn't want to continue, the game session was promptly terminated, and the PwD was led to the regular activity room at the center, with no consequences whatsoever to the services they received in the center.
Participants
Twenty-seven PwD, clients at the MELABEV dementia day center, were recruited to the proof of concept study. During recruitment, we excluded clients with aggression, delusional behavior, a history of alcohol or substance abuse, depression, severe auditory, and/or visual or motor deficits, as assessed by the professional staff at MELABEV. From the 27 who started the pilot, eight were removed from analysis for the following reasons: (a) reached ceiling in performance (the task was apparently not challenging as evident in their higher scores on cognitive assessment, N = 2); (b) did not complete more than one session (N = 4); (c) extremely low affect (N = 2). Performance of nine-teen participants was analyzed (14 women and five men, ages ranging from 65 to 97 years; M age = 87 years, SD = 8 years). Fifty-six percent were from the US, 26% from Eastern European countries, 9% from South Africa, and 9% from England. The participants had worked in various professions in the past including: programing, beautician, architecture, accounting, social work, teaching, and business.
The 19 participants included in the analysis came from two different groups at the Melabev center: Higher Functioning (13 participants) and Lower Functioning (six participants). PwD are placed in these groups based on various criteria set by the Melabev staff, which include group dynamics as well as cognitive abilities. To assess participants' preserved cognitive abilities, Melabev center uses the Montreal Cognitive Assessment Scale (MoCA; Wallace et al., 2019). Participants in the Higher Functioning group scored between nine and 28 on the MoCA scale, and participants in the Lower Functioning groups scored below six.
Gaming Sessions
Ten researchers (all graduate or undergraduate interns from the fields of psychology, nursing, social work, pharmacology, pre-med, and speech therapy), who were not involved in the development process of the game, participated in the proof of concept study. They accompanied the PwD during game play. Their main task was to observe the sessions and document the PwDs engagement with the game, focusing on emotional, and social abilities. During each 20–30 min gaming session, the research assistant, working one-on-one with each client, filled in two different assessment forms (as described in the Tools section). Researchers were also instructed to help with any technological issues that might arise during game play (i.e., no internet connection; Manera et al., 2017).
Tablet Setup
Attention was paid to tablet set up before each session. The sound level was set to the client's most comfortable level, noting the impact of auditory sensory degradation in aging (for example, see Ben-David et al., 2016). Before starting, each PwD was reminded by the researchers to use only one hand on the tablet and to keep the other on the table or on their lap. Research assistants were encouraged to let the client interact with the game independently and not complete the tasks for them.
Training. Before commencing with the pilot, each PwD was presented with a tutorial on how to use the tablet properly (Cunnah et al., 2019). The research assistant informed the PwD:
“In case you have never used a tablet before—we will now do something to learn how to use this one, since each tablet is a bit different. You will use your finger to select items by tapping them with a finger and dragging them (left or right or up or down) on the screen. We will learn how hard or soft to touch the screen, and how to drag things from place to place on the screen.”
Gaming Sessions
Following instructions, participants commenced with the game session. In each gaming session, the PwD could play with all 23 game screens. After the completion of each game session, the PwD was asked for their feedback which they gave both verbally to the researchers and by entering it into the tablet. When mistakes (or inactivity) were recorded by the system, it provided cues/prompts to guide the participants toward expected activity (usually, by repeating the instructions). After two cues, participants were shown the correct answer, and the game advanced to the next game screen. The duration of each game session was between 20 and 30 min. All sessions took place at approximately the same time of day in a quiet room. In every game session, each PwD had the opportunity to play the complete game of 23 game screens.
Data Collection and Tools
This was a mixed methods study with both quantitative and qualitative data collected (Creswell and Creswell, 2017).
MBW Emotional and Social Intelligence (ESI) Evaluation Form
All researchers described their observations, during the game play, on an ESI evaluation form, designed especially for this study. This ESI form, presented in Appendix A, was modified from the ACIS (Assessment of Communication and Interaction Skills, used by occupational therapists) (Forsyth et al., 1999; D'Amico, 2017) by a multidisciplinary team (gerontologist, MD, OT, speech therapist, psychologist). The ACIS is a structured observation tool with 20 discrete skills concerning physicality, information exchange and relations. The ESI tool is designed to capture, in detail, a person's social interactional ability while he or she is participating in a meaningful social context. It identifies strengths as well as problem areas. We included social interactional abilities from the ACIS that were feasible for the research assistants to observe during game play and that corresponded to three components of the Bar-On emotional social intelligence model: interpersonal, intrapersonal, and adaptability (Birks and Watt, 2007).
The “MBW ESI Evaluation Form” includes 11 parameters related to communication and interpersonal social skills rated on a 5-point Likert scale. If the research assistants witnessed any of the following 11 capacities in the reactions of the PwD to the tablet during any of the game screens they would rate it from 1 to 5 (one being the lowest frequency, five being the highest). The form also included one other parameter. This was filled in if at any time during the gaming session, the PwD initiated communication with the research assistant who sat next to them throughout the gaming session. This was rated on a 5-point Likert scale. This form was filled out by the researchers as the PwD was using the game. A total ESI score was derived, in order to assess reliability of the ESI Form, we conducted a Cronbach's Alpha test which indicated that the evaluation has an acceptable reliability (α = 0.92).
Subjective Observations
In addition to the ESI form, the “MBW Game Screen Subjective Evaluation Form” (see Appendix B) was used which prompted researchers to report on their subjective feelings related to the PwDs' performance on each of the 23 game screens during each game play session. The form included both close and open-ended questions, such as: (1) “Did the client enjoy the game?” (2) “Document specific quotes that the PwD shared during the game session”, respectively. The open-ended part of the form had no specific guiding questions.
Correct Engagement Score
A login-based system was used to monitor game plays by the PwD and saved on a centralized anonymized database for analyses. The analysis in the current study focused on “physical interaction screens.” These are 15 of the MBW game screens, where the PwD was asked to actively engage with the game—e.g., choose a specific object on the screen and drag it to a designated place on the screen.
Accuracy of performance was found to be very low in the first three sessions, as expected. Likewise, the time users spent with each game screen varied significantly between participants, which can be explained by the inability of the PwD to focus on a specific task. As a result, an aggregate “correct engagement” score was calculated. Specifically, in each game screen, choosing and/or dragging the correct object was considered correct engagement with the tablet, irrespective of success in the game screen. The maximum score for each session was 15 (as 15 physical interaction screens were analyzed) and minimal score was 0.
Qualitative Data Analysis
Subjective observations and quotation data from MBW game screen subjective evaluation form, was collected on an Excel document and analyzed using grounded theory (Chun-Tie et al., 2019). Five different researchers analyzed the data for themes, three are co-authors on this paper, and the other two had not been involved in the game development or pilot study. The group spanned different fields of expertise (medicine, occupational therapy, gerontology, social work, and neurobiology) and levels of expertise (from interns to emerita). Each researcher read the Excel data a number of times on their own searching for themes. Then they discussed all the themes found by all the researchers with about 92% of original agreement between them and came to a consensus on the themes. Then two of the researchers returned to the data to collect the quotes they felt best portrayed the themes that had been chosen that related to emotional and social intelligence. They came up with a long list of quotes which together they narrowed down to about 20 quotes for each sub-category of the Bar-On Model of Emotional Social Intelligence (total of 180 quotes). This list of quotes was given to four different professionals (three social workers and a speech-language therapist) who were asked to, each on their own, choose the three most representative quotes from the list of 20 demonstrating each sub-category of the Bar-On ESI. The quotes that best represent the different themes are presented in Table 3.
Table 3
| Components | Quotes of PwD while using MBW |
|---|---|
| Sub-components | |
| Intrapersonal | |
| Self-regard | “This is too easy for me.” “I know what to do but can't get it to move.” “I should be wearing my glasses” “I really wanted to put the fork here but knew it wouldn't go” “I'm a slow poke”, “I've had enough”, she took a break and then continued till the end. |
| Emotional self- awareness | “I'd really enjoy that I'm sure” “this is not my cup of tea I must tell you” nodding, “I'd be happy here” “I'd like to have some too” |
| Assertiveness | “This picture is disgusting” “The flowers are pretty, not the lady” “I think I'm getting a little fed up with this you know.” |
| Self-actualization | After realizing that she didn't get the answer correctly “wait, can we start over?” “something more?” wanting to know what else she could do |
| Interpersonal | |
| Empathy | “they're enjoying themselves” “she's having a good time” “She looks a bit worried” “Let's leave her alone” “Now you feel better” |
| Social responsibility | “Thank you” Wishes the characters “Bon appetite” “Good morning how are you today?” “When should we come again?” While raising cup towards research assistants says “Cheers!” “Congratulations” “he finished his soup give him something else” |
| Interpersonal Relationship | “Hello” “Oh, my, what family is this?” “A lovely family” “Beautiful” “You're so sweet and beautiful” started laughing “you can eat the soup because I love you.” |
| Adaptability | |
| Reality testing | “I've seen this before” “This is funny, those are the same faces from yesterday.” “This must be you and your Dad?” “Where is that?” — nature screen “Where is she talking from?” |
| Problem solving | Asks clarifying questions “is this what we are supposed to do?” Reread instructions “Who goes first?” -trying to clarify instructions “I can't see it”, “this goes here I guess” |
Quotes demonstrating selected sub-components of Bar-On's model of emotional social intelligence.
Results
Quantitative Data
In the following analyses, we tested for significant differences between the two subgroups of PwD participants, higher functioning (n = 13) and lower functioning (n = 6).
As expected, the average number of “correct engagements” was significantly higher for the higher functioning group compared to the lower functioning group, t(17) = 3.5, p = 0.003 (see Figure 3A; M = 9.7/15, SE = 2.3, and M = 5.4/15, SE = 2.5; for the higher and lower functioning subgroups, respectively). However, no significant difference was found between the two subgroups on the ESI scores, t(17) = 1.6, p = 0.131, (see Figure 3B; M = 3.7/5, SE = 0.9, and M = 2.9/5, SE = 0.8; for the higher and lower functioning subgroups, respectively).
Figure 3
In the next step, we tested the link between correct engagement performance and ESI scores. The analysis, conducted across both PwD groups, suggested that engagement performance was significantly correlated with ESI, F(1, 17) = 5.1, p = 0.038, with performance in the SG4D explaining 23% of the ESI variance, r2 = 0.23 (See Figure 4). When correlation analysis was conducted separately for each of the PwD subgroups, the link was found to be significant only for the higher functioning subgroup, F(1, 11) = 5.1, p = 0.046, r2 = 0.31, but not for the lower functioning subgroup, F(1, 4) = 0.47, p = 0.53. This could hint on the higher relation between performance and ESI in higher functioning group, or simply be an artifact of the smaller number of participants in the lower functioning group (and hence, smaller variance in performance).
Figure 4
In sum, higher functioning PwD participants (as assessed by the MoCA) performed better on the game (as assessed by correct engagement) than their lower-functioning peers. However, both groups were not differently assessed on ESI. Thus, PwD's cognitive functioning was predictive of performance on the game, but not of ESI. Interestingly, ESI and performance on the game were significantly correlated for the higher functioning PwD group, suggesting that with residual cognitive capacity, ESI could be possibly used to improve performance on the game.
Qualitative Data
Three general overarching themes emerged from the grounded theory analysis: (1) Manifestations: manifestations of aging and dementia symptoms, and the types of associated mistakes; (2) Learning: learning techniques and signs of learning; and (3) Emotional Social Intelligence. These three themes are interweaved with three categories of interactions: interactions with the technology, interactions with the research assistants, and interactions with the objects on the screen.
Aging and Dementia Symptoms and Types of Mistakes
Symptoms of dementia appear to cause difficulties for the PwD when playing the SG4D. Some issues that arose were related to disorientation, distractions in their surroundings, stress, and slow speed of processing related to figuring out answers and implementing them by dragging on the screen. Motor impairments, such as physical rigidity, poor fine motor skills and sleepiness, were also mentioned as a factor. The types of mistakes mentioned by research assistants were related to mental rigidity (i.e., mentally stuck on the previous screen), apraxia (inability to initiate drag movement), poor spatial orientation (i.e., dragging in wrong direction), disinhibition (i.e., circling aimlessly on the screen), and impaired abstraction (i.e., understanding instructions literally).
Learning Techniques and Signs of Learning
The research assistants were also clear in their reports on demonstrated learning by PwD. They also reported that in 89% of the game plays participants appeared to enjoy playing the game. Some were even able to anticipate the instructions to the game, after practice. Observations indicated the use of various learning techniques in order to complete the game. Some of the PwD used the trial and error method. It was sometimes evident that they used a self-correcting mechanism when they felt that their first attempt was incorrect. Others asked the research assistants for help with specific tasks, or with their general confusion. Some reread the instructions out loud or to themselves and consciously contemplated the instructions. For example, sometimes they counted out loud to keep track of what they were doing.
Emotional and Social Intelligence
In our grounded theory analysis of the research assistants' written observations of the PwD playing the SG4D, and their quotes, we found the following 9 sub-components of the Bar-On Model of ESI, as divided to three categories: (1) Intrapersonal: self-regard, emotional self-awareness, assertiveness, self-actualization; (2) Interpersonal: Empathy, social responsibility, interpersonal relationship; and (3) Adaptability: Reality testing, Problem solving. Table 3 shows selected quotes as examples demonstrating each sub-component: (words in italics are to explain the context to the reader).
In sum, the qualitative analysis suggests that PwD encountered difficulties related to dementia in playing the game. However, they demonstrated the ability to overcome these difficulties, to learn new techniques and to interact in a meaningful emotional and social way with the research assistants.
Discussion
The world of people with dementia (PwD), as well as their family and caregivers, is filled with isolation. This is due both to the neurodegenerative aspects of the disease, as well as the challenges caregivers face on how best to communicate with a PwD. The disease makes it hard for the PwD to interact with their surroundings and social settings. Social exchange and communication become difficult. This, in turn, creates a social barrier and a social distance between those around the PwD and the PwD. Technological tools such as serious games could facilitate elimination of barriers, allowing the PwD and their caregiver to communicate in a more meaningful and positive way. Technologies for evaluating and exercising emotional and social capacities are not well-studied in the dementia population (Goodkind et al., 2015; Dourado et al., 2019; Nazareth, 2019).
The current proof of concept pilot study suggests that PwD with moderate to severe dementia can engage with our novel tablet-based SG4D “MBW” and found it accessible and acceptable. This was demonstrated by the observed enthusiasm and participation of PwD with the game system, and by specific data collected by the researchers and tablet that document Bar-On's markers of emotional and social intelligence (Bar-On and Parker, 2000).
Data collected in our pilot study hints that PwD may be able to recognize emotions in the characters on the screens of the SG4D, and react and express their own emotions. They even expressed empathy toward characters in the game. They were able to respond appropriately to social interactions and initiate interactions with both the objects on the screen and the research assistants. These are emotive and social capacities that have not been studied in PwD, especially with moderate and advanced dementia (MoCA scores as low as 4). In fact, there is still a paucity of research on emotional and social intelligence in PwD, and how it can be used to improve interactions with caregivers (Calabria et al., 2009). The current study suggests that the use of a serious game designed with the unique needs of a PwD in mind can facilitate expression of emotions and thus open doors for communication for PwD and their caregivers.
Our preliminary findings also suggest that emotional and cognitive abilities may not be similarly affected by dementia. Cognitive abilities, as assessed by the (routinely used) MoCA test were not found to have an effect on PwD's emotional and social intelligence assessments by research assistants, even though cognitive scores significantly affected accuracy of performance in the game. These results relate to Fujii et al.' (2014a) assertion that cognitive and emotional functions are independently affected in dementia. Our results further highlight their suggestion that assessment of both cognitive and ESI should be taken into consideration when testing PwD. Taken together, findings indicate that remaining ESI skills in dementia may be used as scaffoldings to improve functioning. Technology may play a role in improving these remaining capacities.
Finally, it seems that the use of a touch-screen, tablet-mediated, serious game can exercise ESI capacities that may be relatively preserved but typically remain hidden in dementia. As well, such a SG4D, may be used as a more accurate tool to assess reserved cognitive functioning since it is done when the PwD is relaxed, playful and even laughing, rather than stressed and threatened by a formal cognitive battery. As Plato said “You can discover more about a person in an hour of play than in a year of observation.”
More research should be done to better understand how to maintain, exercise and utilize remaining ESI capacities in dementia and to explore further technologies in various settings. We hope to be able to do this in the process of moving to TRL6-7 (prototype demonstration) and indeed in turn eight and nine (operational system) which will define in detail our planned public use cases. Our aim is to expand the use to all of MELABEV's daycare centers, other daycare centers in Israel and other countries, as well as home use for the client with his/her personal aid. Use cases of the system can vary greatly between daycare center and home use deployment. While deploying the system in a daycare center aids the accompanying research, we believe that many other aspects of use and user interaction with the game system can be contrived and observed from analysis of home use, see suggestions for adaptation of paradigms to remote acess, given COVID-19 social restrictions, in Ben-David et al. (2020). Our aim is to further investigate use cases in the future, using even more advanced analytics. Indeed, a publicly available App will serve a greater therapeutic purpose for a larger population, than focusing on daycare center deployment.
We believe that remaining ESI capacities might even be used to improve, or at least slow the deterioration of, cognitive abilities, functionality and communication between the PwD and their caregivers and families. Further research in this area may impact on the quality of life of PwD and their caregivers.
Limitations
While this study has benefits due to it being a mixed methods study, including rich qualitative data, as well as many research assistants involved in doing the testing, it has limitations as well. As in many studies related to care of PwD, the sample size is small, yet no different than common in published research in the field (see Appendix C). Another limitation is the fact that the study was carried out in a dementia day care center with a full schedule, which at times interested the people with dementia more than being involved in the pilot study. We hope in future studies to test the effect of playing “MBW” in a home setting as well.
Conclusion
An earlier research from our team (Tziraki et al., 2017) documented that the use of a serious game, designed with the input from unique needs of a PwD in mind, is acceptable accessible and engaging for people with moderate and advanced dementia. We also found the serious game may be helpful in improving cognitive function, such as speed of processing. The current study focused on assessing how and if PwD can interact in a meaningful emotional and social manner with a technology-based serious game, and whether playing the game will be accompanied by meaningful interactions with caregivers present. Our preliminary results suggest that the use of a serious game can facilitate the expression of ESI capacities that typically remain hidden in dementia. We further suggest that the serious game developed for this specific aim, SG4D “MBW,” may be able to facilitate the stimulation of these capacities in ways that caregivers can also recognize and thus contribute to improved social connectivity.
There is yet no drug to stop the cognitive decline associated with dementia, thus we suggest that interventions related to PwD and ESI may improve functioning and quality of life. Despite declines in cognitive abilities, our two studies may indicate that PwD can interact with a tablet SG4D using social and communication capacities. Using SG4D with PwD in order to help them exercise and maintain social skills is an area that may be promising in the future and may help counter the negative effects of social isolation and loneliness. Such games may also have an impact on cognitive functioning and even on improving the quality of life for both PwD and their caregivers by facilitating communication. Further research should explore whether SG4D may be used as evaluation for reserved cognitive, and ESI abilities on one hand, and as a gauge for functional capacities that could possibly be improved with training, on the other. More research is needed in this area with larger sample sizes.
Statements
Data availability statement
The datasets generated for this study are available on request to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. All identifiable images used in this manuscript have been obtained from a stock image repository.
Author contributions
RBe and CT planned the research, including the pilot, the qualitative analysis, and its interpretation. RBa and BB-D conducted the quantitative analysis and its interpretation. TR participated in the qualitative analysis. JA helped plan the pilot and gave input to writing the paper. DN and AR wrote the section on design and technology considerations. The manuscript was written in collaboration of BB-D, RBe, CT, and RBa. All authors contributed to the article and approved the submitted version.
Funding
Yad Hanadiv and Arison foundations partially funded this research and development. The corresponding author was partially supported by a grant from the Israeli Science Foundation (ISF grant number 861/18).
Acknowledgments
We would like to thank MELABEV Talpiot staff, for making it possible for the study to take place in their center (Dvora Marcus, Nancy Brown, Noach Cohen, Jackie Diamond, Frayda Vizental-Shomron, Tamar Berger, and Sharon Finkel). As well as J-interns, Skilled volunteers for Israel for sending us interns to participate in this research. Dvora Katsev, speech therapist, for helping with ACIS adaptation and research assistants Rachel Feldstein, Skylar Dixon, Raquel Deviance, Esther Chaya, Daniella Yarrow, Naomi Ehrenkranz, Riva Kent, Daniella Spero, and Tova Leon for helping with the pilot. We wish to thank Maya Mentzel, CANlab manager for all of her help.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomp.2020.536880/full#supplementary-material
References
1
AstellA. (2010). Developing computer games for people with dementia. Gerontechnology9:189. 10.4017/gt.2010.09.02.289.00
2
Bar OnR.HandleyR. (2003). The Bar On EQ-360. Toronto: Multi-Health Systems.
3
Bar-OnR. (1997). The Emotional Quotient Inventory (EQ-i): A Test of Emotional Intelligence. Toronto: Multi-Health Systems.
4
Bar-OnR. (2000). “Emotional and social intelligence: insights from the Emotional Quotient Inventory (EQ-i),” In Handbook of emotional intelligence. San Francisco: Jossey-Bass.
5
Bar-OnR. (2004). “The bar-on emotional quotient inventory (EQ-i): rationale, description and summary of psychometric properties,” in Measuring Emotional Intelligence: Common Ground and Controversy, Hauppauge, NY: Nova Science Publishers. 115–145.
6
Bar-OnR. (2006). The Bar-On model of emotional-social intelligence (ESI). Psicothema18, 13–25.
7
Bar-OnR.ParkerJ. D. A. (2000). The Handbook of Emotional Intelligence: Theory, Development, Assessment, and Application at Home, School and in the Workplace. SanDiego, CA: Jossey-Bass.
8
BartochowskiZ.GatlaS.KhouryR.Al-DahhakR.GrossbergG. T. (2018). Empathy changes in neurocognitive disorders: a review. Ann. Clin. Psychiatry30, 220–232.
9
Ben-DavidB. M.Avivi-ReichM.SchneiderB. A. (2016). Does the degree of linguistic experience (native versus nonnative) modulate the degree to which listeners can benefit from a delay between the onset of the maskers and the onset of the target speech?Hear. Res.341, 9–18. 10.1016/j.heares.2016.07.016
10
Ben-DavidB. M.ChambersC. G.DanemanM.Pichora-FullerM. K.ReingoldE. M.SchneiderB. A. (2011). Effects of aging and noise on real-time spoken word recognition: Evidence from eye movements. J. Speech Lang. Hear. Res.? 54, 243–262. 10.1044/1092-4388(2010/09-0233)
11
Ben-DavidB. M.ErelH.GoyH.SchneiderB. A. (2015). “Older is always better”: age-related differences in vocabulary scores across 16 years. Psychol. Aging30, 856–862. 10.1037/pag0000051
12
Ben-DavidB. M.Gal-RosenblumS.van LieshoutP. H.ShakufV. (2019). Age-related differences in the perception of emotion in spoken language: The relative roles of prosody and semantics. J. Speech Lang. Hear. Res.62, 1188–1202. 10.1044/2018_JSLHR-H-ASCC7-18-0166
13
Ben-DavidB. M.IchtM. (2017). Oral-diadochokinetic rates for Hebrew-speaking healthy ageing population: non-word versus real-word repetition. Int. J. Lang. Commun. Disord.52, 301–310. 10.1111/1460-6984.12272
14
Ben-DavidB. M.IchtM. (2018). The effect of practice and visual feedback on oral-diadochokinetic rates for younger and older adults. Lang. Speech61, 113–134. 10.1177/0023830917708808
15
Ben-DavidB. M.MalkinG.ErelH. (2018). “Ageism and neuropsychological tests,”in Contemporary Perspectives on Ageism, (Cham: Springer). 277–297. 10.1007/978-3-319-73820-8_17
16
Ben-DavidB. M.MentzelM.IchtM.GiladM.DorY. I.Ben-DavidS.et al. (2020). Challenges and opportunities for telehealth assessment during COVID-19: iT-RES, adapting a remote version of the test for rating emotions in speech. Int. J. Audiol.10.1080/14992027.2020.1833255. [Epub ahead of print].
17
Ben-DavidB. M.SchneiderB. A. (2009). A sensory origin for color-word stroop effects in aging: a meta-analysis. Aging Neuropsychol. Cogn.16, 505–534. 10.1080/13825580902855862
18
Ben-DavidB. M.SchneiderB. A. (2010). A sensory origin for color-word Stroop effects in aging: simulating age-related changes in color-vision mimics age-related changes in Stroop. Aging Neuropsychol. Cogn.17, 730–746. 10.1080/13825585.2010.510553
19
BerenbaumR. (2003). The humorous side of dementia. J Dement. Care. 11:12. Available online at: https://careinfo.org/jdc-archive/the-humorous-side-of-dementia/
20
BerenbaumR. (ed.). (2010). Alzheimer's and Other Dementias. Treating and Coping with Mentally Frail in the Community. Jerusalem: Melabev and Eshel.
21
BerenbaumR.LangeY.AbramowitzL. (2011). “Augmentative alternative communication for Alzheimer's patients' families using SAVION,” in Proceedings of the 4th International Conference on PErvasive Technologies Related to Assistive Environments, (Crete). 10.1145/2141622.2141677
22
BerenbaumR.TzirakiC.Cohen-MansfieldJ. (2017b). The right to mourn in dementia: to tell or not to tell when someone dies in dementia day care. Death Stud. 353–359. 10.1080/07481187.2017.1284953
23
BerenbaumR.TzirakiC.MazuzK. (2017a). The enduring self: personhood, autonomy and compassion in the context of community-based dementia daycare centers. J. Compassion. Health Care, 4:8. 10.1186/s40639-017-0037-z
24
BirksY.WattI. (2007). Emotional intelligence and patient-centred care. J. R. Soc. Med100, 368–374. 10.1258/jrsm.100.8.368
25
BlairR. (2003). Facial expressions, their communicatory functions and neuro–cognitive substrates. Philos. Trans. Roy. Soc. London Series B Biol Sci.358, 561–572. 10.1098/rstb.2002.1220
26
Blanchard-FieldsF. (2007). Everyday problem solving and emotion: an adult developmental perspective. Curr. Direct. Psychol. Sci.16, 26–31. 10.1111/j.1467-8721.2007.00469.x
27
BurnsA.IliffeS. (2009). Clinical review: dementia. Br. Med. J.338:b75. 10.1136/bmj.b75
28
CacioppoJ.CacioppoS. (2014). Older adults reporting social isolation or loneliness show poorer cognitive function 4 years later. Evid. Based Nursing17, 59–60. 10.1136/eb-2013-101379
29
CacioppoJ.HawkleyL. (2009). Perceived social isolation and cognition. Trends Cogn. Sci.13, 447–454. 10.1016/j.tics.2009.06.005
30
CalabriaM.CotelliM.AdenzatoM.ZanettiO.MiniussiC. (2009). Empathy and emotion recognition in semantic dementia: a case report. Brain Cogn.70, 247–252. 10.1016/j.bandc.2009.02.009
31
CarstensenL. L.MikelsJ. A. (2005). At the intersection of emotion and cognition. Aging and the positivity effect. Curr. Direc. Psychol. Sci.14, 117–121. 10.1111/j.0963-7214.2005.00348.x
32
ChernissC. (2004). “Emotional intelligence,” in Encyclopedia of Applied Psychology, Vol. 2, ed C. Spielberger (Oxford: Elsevier). 315–321. 10.1016/B0-12-657410-3/00565-1
33
ChoiJ.TwamleyE. W. (2013). Cognitive rehabilitation therapies for Alzheimer's disease: a review of methods to improve treatment engagement and self-efficacy. Neuropsychol. Rev.23, 48–62. 10.1007/s11065-013-9227-4
34
Chun-TieY.BirksM.FrancisK. (2019). Grounded theory research: a design framework for novice researchers. Sage Open Med.7:2050312118822927. 10.1177/2050312118822927
35
Cohen-MansfieldJ.Dakheel-AliM.MarxM. (2009). Engagement in persons with dementia: the concept and its measurement. Am. J. Geriatr. Psychiatry17, 299–307. 10.1097/JGP.0b013e31818f3a52
36
ColeS.CapitanioJ.ChunK.ArevaloJ.MaJ.CacioppoJ. (2015). Myeloid differentiation architecture of leukocyte transcriptome dynamics in perceived social isolation. Proc. Natl. Acad. Sci. U.S.A. 112, 15142–15147. 10.1073/pnas.1514249112
37
CornetV. P.ToscosT.BolchiniD.Rohani GhahariR.AhmedR.DaleyC.et al. (2020). Untold stories in user-centered design of mobile health: practical challenges and strategies learned from the design and evaluation of an app for older adults with heart failure. JMIR Mhealth Uhealth8:asssese17703. 10.2196/17703
38
CosentinoS.ZahodneL.BrandtJ.BlackerD.AlbertM.DuboisB.et al. (2014). Social cognition in Alzheimer's disease: a separate construct contributing to dependence. Alzheimers Dement.10, 818–826. 10.1016/j.jalz.2013.12.021
39
CreavinS.WisniewskiS.Noel-StorrA.TrevelyanC.HamptonT.RaymentD.et al. (2016). Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 13:CD011145. 10.1002/14651858.CD011145.pub2
40
CreswellJ. W.CreswellJ. D. (2017). Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Sage publications.
41
CunnahK.HoweD.ThorpeJ.DunnR.PlattR.WhiteC.et al. (2019). Training people with dementia/cognitive impairment and their carers in the use of web-based supportive technologies (Innovative practice). Dementia. 10.1177/1471301219887592
42
D'AmicoM. (2017). A review of occupation and impairment based assessments used in occupational therapy. OCCUPATION: A Medium of Inquiry for Students, Faculty and Other Practitioners Advocating for Health through Occupational Studies2:4. Available online at: https://nsuworks.nova.edu/occupation/vol2/iss1/4
43
DewingJ. (2007). Participatory research: a method for process consent with persons who have dementia. Dementia6, 11–25. 10.1177/1471301207075625
44
DewingJ. (2008). Process consent and research with older persons living with dementia. Res. Ethics4, 59–64. 10.1177/174701610800400205
45
Di RosaE.HanniganC.BrennanS.ReillyR.RapčanV.RobertsonI. (2014). Reliability and validity of the Automatic Cognitive Assessment Delivery (ACAD). Front. Aging Neurosci.6:34. 10.3389/fnagi.2014.00034
46
DouglasS.JamesI.BallardC. (2004). Non-pharmacological interventions in dementia. Adv. Psychiatr. Treat.10, 171–177. 10.1192/apt.10.3.171
47
DouradoM.Torres Mendonça de Melo FádelB.Simões NetoJ.AlvesG.AlvesC. (2019). Facial expression recognition patterns in mild and moderate alzheimer's disease. J. Alzheimers Dis.69, 539–549. 10.3233/JAD-181101
48
Earto (2014) The TRL Scale as a Research and Innovation Policy Tool EARTO Recommendations. Available online at: https://www.earto.eu/wp-content/uploads/The_TRL_Scale_as_a_R_I_Policy_Tool_-_EARTO_Recommendations_-_Final.pdf (accessed October, 2020).
49
EngM. (2000). The appropriate useof humour in Alzheimer's care. Alzheimer's Care Guide, 8, 1–2.
50
FischerA.Landeira-FernandezJ.Sollero de CamposF.MograbiD. (2019). Empathy in Alzheimer's Disease: Review of Findings and Proposed Model. J. Alzheimers Dis.69, 921–933. 10.3233/JAD-180730
51
ForsythK.LaiJ.KielhofnerG. (1999). The Assessment of Communication and Interaction Skills (ACIS): measurement properties. Br. J. Occup. Ther.62, 69–74. 10.1177/030802269906200208
52
FujiiM.ButlerJ.HirazakuraA.SasakiH. (2014b). Mini-emotional state examination for dementia patients. Geriatr. Gerontol. Int.14, 508–513. 10.1111/ggi.12127
53
FujiiM.ButlerJ.SasakiH. (2014a). Emotional function in dementia patients. Psychogeriatrics14, 202–209. 10.1111/psyg.12059
54
GambleK.HowardJ.HowardD. (2014). Not just scenery: viewing nature pictures improves executive attention in older adults. Exp. Aging Res.40, 513–530. 10.1080/0361073X.2014.956618
55
GolemanD. (2006). Emotional Intelligence. New York, NY: Random House.
56
GoodkindM.SturmV.AscherE.ShdoS.MillerB.RankinK.et al. (2015). Emotion recognition in frontotemporal dementia and Alzheimer's disease: a new film-based assessment. Emotion15, 416–427. 10.1037/a0039261
57
HasherL.ZacksR. T. (1988). Working memory, comprehension, and aging: a review and a new view. Psychol. Learn Motivation22, 193–225. 10.1016/S0079-7421(08)60041-9
58
HirazakuraA.HatakeyamaR.FukuokaY.SatohA.KobayashiK.FujiiM.et al. (2008). Emotional therapy for patients with dementia. Geriatr. Gerontol. Int.8, 303–306. 10.1111/j.1447-0594.2008.00486.x
59
HoffmannM.CasesL.HoffmannB.ChenR. (2010). The impact of stroke on emotional intelligence. BMC Neurol.10:103. 10.1186/1471-2377-10-103
60
IencaM.FabriceJ.ElgerB.CaonM.Scoccia PappagalloA.KressigR.et al. (2017). Intelligent assistive technology for Alzheimer's disease and other dementias: a systematic review. J. Alzheimers Dis.56, 1301–1340. 10.3233/JAD-161037
61
JamierV.IrvineB.AucherC. (2018). Demystifying TRLs for Complex Technologies. LEiTaT Project Blogs. Available online at: https://projects.leitat.org/demystifying-trls-for-complex-technologies/ (accessed October 20, 2019).
62
JonesC.SungB.MoyleW. (2015). Assessing engagement in people with dementia: a new approach to assessment using video analysis. Arch. Psychiatr. Nursing29, 377–382. 10.1016/j.apnu.2015.06.019
63
KitwoodT. M. (1997). Dementia Reconsidered: The Person Comes First. London: Open University Press.
64
Klein-KoerkampY.BaciuM.HotP. (2012b). Preserved and impaired emotional memory in alzheimer's disease. Front. Psychol.3:331. 10.3389/fpsyg.2012.00331
65
Klein-KoerkampY.BeaudoinM.BaciuM.HotP. (2012a). Emotional decoding abilities in alzheimer's disease: a meta-analysis. J. Alzheimers Dis.32, 109–125. 10.3233/JAD-2012-120553
66
KumforF.Sapey-TriompheL.LeytonC.BurrellJ.HodgesJ.PiguetO. (2014). Degradation of emotion processing ability in corticobasal syndrome and Alzheimer's disease. Brain137, 3061–3072. 10.1093/brain/awu246
67
LamK. J.DijkstraT.RueschemeyerS. A. (2015). Feature activation during word recognition: action, visual, and associative-semantic priming effects. Front. Psychol.6:659. 10.3389/fpsyg.2015.00659
68
LeónF. G.HernándezL. M.MartínezJ. M. A.MeilánJ. J. G. (2011). Emotional processing of facial expressions in normal and pathological Aging48, 33–38. 10.5538/1137-1242.2011.48.33
69
ManeraV.Ben-SadounG.AalbersT.AgopyanH.AskenazyF.BenoitM.et al. (2017). Recommendations for the use of serious games in neurodegenerative disorders: 2016 Delphi Panel. Front. Psychol.8:1243. 10.3389/fpsyg.2017.01243
70
MartinezM.MultaniN.AnorC.MisquittaK.Tang-WaiD.KerenR.et al. (2018). Emotion detection deficits and decreased empathy in patients with alzheimer's disease and parkinson's disease affect caregiver mood and burden. Front. Aging Neurosci.10:120. 10.3389/fnagi.2018.00120
71
MayerJ. D.SaloveyP. (1997). What is Emotional Intelligence. Emotional Development and Emotional Intelligence: Educational Implications. New York, NY: Harper Collins, 3–34.
72
MayerJ. D.SaloveyP.CarusoD. R. (2002). Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT).Toronto: Multi-Health Systems, Inc.
73
McAllisterM.DaytonJ.OprescuF. I.KatsikitisM.JonesC. M. (2020). Memory keeper: a prototype digital application to improve engagement with people with dementia in long-term care (innovative Practice). Dementia19, 1287–1298.
74
McLellanT.JohnstonL.Dalrymple-AlfordJ.PorterR. (2008). The recognition of facial expressions of emotion in Alzheimer's disease: a review of findings. Acta Neuropsychiatr.20, 236–250. 10.1111/j.1601-5215.2008.00315.x
75
MikelsJ.LarkinG.Reuter-LorenzP.CarstensenL. (2005). Divergent trajectories in the aging mind: changes in working memory for affective versus visual information with age. Psychol. Aging20, 542–553. 10.1037/0882-7974.20.4.542
76
MondiniS.ArcaraG.JaremaG. (2014). Semantic and syntactic processing of mass and count nouns: data from dementia. J. Clin. Exp. Neuropsychol.36, 967–980. 10.1080/13803395.2014.958437
77
NazarethD. S. (2019). “Emotion recognition in dementia: advancing technology for multimodal analysis of emotion expression in everyday life,” Presented at the 2019 8th International Conference on Affective Computing and Intelligent Interaction Workshops and Demos (ACIIW).
78
PerugiaG.Van BerkelR.Díaz-BoladerasM.Català-MallofréA.RauterbergM.BarakovaE. (2018). Understanding engagement in dementia through behavior. the ethographic and laban-inspired coding system of engagement (ELICSE) and the evidence-based model of engagement-related behavior (EMODEB). Front. Psychol. 9:690. 10.3389/fpsyg.2018.00690
79
PhillipsL.ScottC.HenryJ.MowatD.BellJ. (2010). Emotion perception in Alzheimer's disease and mood disorder in old age. Psychol. Aging25, 38–47. 10.1037/a0017369
80
PovedaB.Osborne-CrowleyK.LaidlawK.MacleodF.PowerK. (2017). Social cognition, behaviour and relationship continuity in dementia of the alzheimer type. Brain Impair.18, 175–187. 10.1017/BrImp.2016.35
81
RobertP.KönigA.AmievaH.AndrieuS.BremondF.BullockR.et al. (2014). Recommendations for the use of serious games in people with alzheimer's disease, related disorders and frailty. Front. Aging Neurosci.6:54. 10.3389/fnagi.2014.00054
82
RobillardJ.ClelandI.HoeyJ.NugentC. (2018). Ethical adoption: a new imperative in the development of technology for dementia. Alzheimers Dement.14, 1104–1113. 10.1016/j.jalz.2018.04.012
83
Shany-UrT.RankinK. (2011). Personality and social cognition in neurodegenerative disease. Curr. Opin. Neurol.24, 550–555. 10.1097/WCO.0b013e32834cd42a
84
SnowdenJ.GibbonsZ.BlackshawA.DoubledayE.ThompsonJ.CraufurdD.et al. (2003). Social cognition in frontotemporal dementia and Huntington's disease. Neuropsychologia41, 688–701. 10.1016/S0028-3932(02)00221-X
85
ThakeC.BamblingM.EdirippuligeS.MarxE. (2017). A psychoevolutionary approach to identifying preferred nature scenes with potential to provide restoration from stress. HERD: Health Environ. Res. Design J.10, 111–124. 10.1177/1937586717705085
86
Torres Mendonça De Melo FádelB.Santos De CarvalhoR.Belfort Almeida Dos SantosT.DouradoM. (2018). Facial expression recognition in Alzheimer's disease: a systematic review. J. Clin. Exp. Neuropsychol.41, 192–203. 10.1080/13803395.2018.1501001
87
TorresB.SantosR.SousaM.Simões NetoJ.NogueiraM.BelfortT.et al. (2015). Facial expression recognition in Alzheimer's disease: a longitudinal study. Arquivos de Neuro-Psiquiatria73, 383–389. 10.1590/0004-282X20150009
88
TrahanM.KuoJ.CarlsonM.GitlinL. (2014). A systematic review of strategies to foster activity engagement in persons with dementia. Health Educ. Behav.41, 70S–83S. 10.1177/1090198114531782
89
TzirakiC.BerenbaumR.GrossD.AbikhzerJ.Ben-DavidB. (2017). Designing serious computer games for people with moderate and advanced dementia: interdisciplinary theory-driven pilot study. JMIR Serious Games5:e16. 10.2196/games.6514
90
ValdezR.HoldenR.NovakL.VeinotT. (2015). Transforming consumer health informatics through a patient work framework: connecting patients to context. J. Am. Med. Inform. Assoc.22, 2–10. 10.1136/amiajnl-2014-002826
91
WallaceS.Donoso BrownE.SimpsonR.D'AcuntoK.KranjecA.RodgersM.et al. (2019). A comparison of electronic and paper versions of the montreal cognitive assessment. Alzheimer Dis. Assoc. Disord.33, 272–278. 10.1097/WAD.0000000000000333
92
World Health Organization (2019). Dementia. Available online at: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed October 15, 2019).
93
ZimmermanS.HasherL.GoldsteinD. (2011). “Cognitive ageing: a positive perspective,” in Paradoxical Brain, ed N. Kapur (Cambridge: Cambridge University Press), 130–150. 10.1017/CBO9780511978098.009
Summary
Keywords
serious games for dementia (SG4D), emotional intelligence, social intelligence, caregiving, communication, quality of life, human computer interaction, human human interaction
Citation
Berenbaum R, Tziraki C, Baum R, Rosen A, Reback T, Abikhzer J, Naparstek D and Ben-David BM (2020) Focusing on Emotional and Social Intelligence Stimulation of People With Dementia by Playing a Serious Game—Proof of Concept Study. Front. Comput. Sci. 2:536880. doi: 10.3389/fcomp.2020.536880
Received
21 February 2020
Accepted
16 November 2020
Published
23 December 2020
Volume
2 - 2020
Edited by
Carlos Vaz De Carvalho, Polytechnic Institute of Porto, Portugal
Reviewed by
Alejandro Catala, University of Santiago de Compostela, Spain; Maria Chiara Pino, University of L'Aquila, Italy
Updates
Copyright
© 2020 Berenbaum, Tziraki, Baum, Rosen, Reback, Abikhzer, Naparstek and Ben-David.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rakel Berenbaum melabev1@gmail.comBoaz M. Ben-David boaz.ben.david@idc.ac.il
This article was submitted to Human-Media Interaction, a section of the journal Frontiers in Computer Science
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.