 Maria Kamusheva1*
Maria Kamusheva1* Konstantin Tachkov1
Konstantin Tachkov1 Maria Dimitrova1
Maria Dimitrova1 Zornitsa Mitkova1
Zornitsa Mitkova1 Gema García-Sáez2,3
Gema García-Sáez2,3 M. Elena Hernando2,3
M. Elena Hernando2,3 Wim Goettsch4,5
Wim Goettsch4,5 Guenka Petrova1
Guenka Petrova1- 1Faculty of Pharmacy, Medical University of Sofia, Sofia, Bulgaria
- 2Bioengineering and Telemedicine Group, Centro de Tecnología Biomédica, Escuela Técnica Superior de Ingenieros de Telecomunicación, Universidad Politécnica de Madrid, Madrid, Spain
- 3CIBER-BBN: Networking Research Centre for Bioengineering, Biomaterials and Nanomedicine, Madrid, Spain
- 4Utrecht Centre for Pharmaceutical Policy, Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences (UIPS), Utrecht University, Utrecht, Netherlands
- 5National Health Care Institute (ZIN), Diemen, Netherlands
Introduction: Diabetes monitoring systems (DMS) are a possible approach for regular control of glucose levels in patients with Type 1 or 2 diabetes in order to improve therapeutic outcomes or to identify and modify inappropriate patient behaviors in a timely manner. Despite the significant number of studies observing the DMS, no collective evidence is available about the effect of all devices.
Goal: To review and consolidate evidences from multiple systematic reviews on the diabetes monitoring systems and the outcomes achieved.
Materials and methods: Internet-based search in PubMed, EMBASE, and Cochrane was performed to identify all studies relevant to the research question. The data regarding type of intervention, type of diabetes mellitus, type of study, change in clinical parameter(s), or another relevant outcome were extracted and summarized.
Results: Thirty-three out of 1,495 initially identified studies, involving more than 44,100 patients with Type 1, Type 2, or gestational diabetes for real-time or retrospective Continuous Glucose Monitoring (CGMS), Sensor Augmented Pump Therapy (SAPT), Self-monitoring Blood Glucose (SMBG), Continuous subcutaneous insulin infusion (CSII), Flash Glucose Monitoring (FGM), Closed-loop systems and telemonitoring, were included. Most of the studies observed small nominal effectiveness of DMS. In total 11 systematic reviews and 15 meta-analyses, with most focusing on patients with Type 1 diabetes (10 and 6, respectively), reported a reduction in glycated hemoglobin (HbA1c) levels from 0.17 to 0.70% after use of DMS.
Conclusion: Current systematic review of already published systematic reviews and meta-analyses suggests that no statistically significant difference exists between the values of HbA1c as a result of application of any type of DMS. The changes in HbA1c values, number and frequency of hypoglycemic episodes, and time in glucose range are the most valuable for assessing the appropriateness and effectiveness of DMS. Future more comprehensive studies assessing the effectiveness, cost-effectiveness, and comparative effectiveness of DMS are needed to stratify them for the most suitable diabetes patients’ subgroups.
Introduction
Diabetes mellitus is a lifelong, chronic metabolic disease leading to various complications. It affects significant number of people worldwide as the newly diagnosed cases are increasing rapidly. That makes diabetes a global epidemic and a major cause of morbidity and mortality (1, 2). Being difficult to treat and expensive to manage, diabetes could be defined as a demanding and fast-growing problem for healthcare systems (3).
Several challenges exist for ensuring a better control of patients with diabetes mellitus. First of all, the most appropriate pharmacological treatment for every patient should be ensured based on patient’s personal characteristics and needs. A high level of adherence to therapy should be provided and periodically reassessed in order to achieve the treatment goals: adequate glycemic control with low risk of complications. Therefore, continuous and strict monitoring of patients’ condition, focusing on regular assessment of glycemic control, as HbA1c levels and blood glucose levels, should be performed and the most appropriate personalized, cost-effective method for continuous monitoring should be selected. As a result, an adequate and optimal resources allocation could be provided for every health care system.
Consistent engagement of patients within the process of effective management and control of glucose levels correlates with optimal health outcomes. Healthy eating, physical activity programs, adherence, and close monitoring are some of the most important self-management actions for the purpose of successful treatment (4). Glucose monitoring systems (GMS) are devices which provide information about glucose values ensuring an efficient and safe glucose control by detecting fluctuations in glucose levels and giving a precise picture of what a patient’s condition is (5, 6). These devices are crucial especially for patients with high risk of hypo- or hyperglycemia. Diabetes Monitoring Systems (DMS) are systems which integrate one or more GMS devices to support diabetes management. On the basis of the literature, currently available different types of DMS could be classified in several groups: conventional (glucose meters), continuous glucose monitoring systems (CGMS) being a variety of devices (professional, personal, retrospective, real-time, flash, etc.), non-invasive, closed-loop systems, Sensor Augmented Pump Therapy (SAPT), and telemedicine/mobile technologies which integrate glucose monitoring systems or telemonitoring (Figure 1). The conventional ones are commonly used by patients but the small number of measurements per day causes the unawareness of fluctuations in glucose levels and asymptomatic hypoglycemia. Continuous glucose monitoring systems measure glucose levels continuously throughout the day and provide information on the glucose values fluctuations (7, 8). The main advantage of closed-loop systems (so-called artificial pancreas systems) and sensor augmented pump therapy is the option to allow precise adjustment of patient’s insulin injections due to transmission of glucose readings between CGMS and insulin pump. These combined devices lead to increased life expectancy, delayed onset and prоgression of microvascular complications as they are an effective method for improvement of metabolic control (9–11). Further development of more sophisticated glucose-monitoring devices and techniques could help to overcome many challenges such as reduction of pain due to frequent pricking of skin for the purposes of glucose levels testing (1). Telemedicine systems or mobile applications which integrate glucose monitoring systems have shown an increasing adoption to improve adherence to treatment and contribute to improve diabetes management.
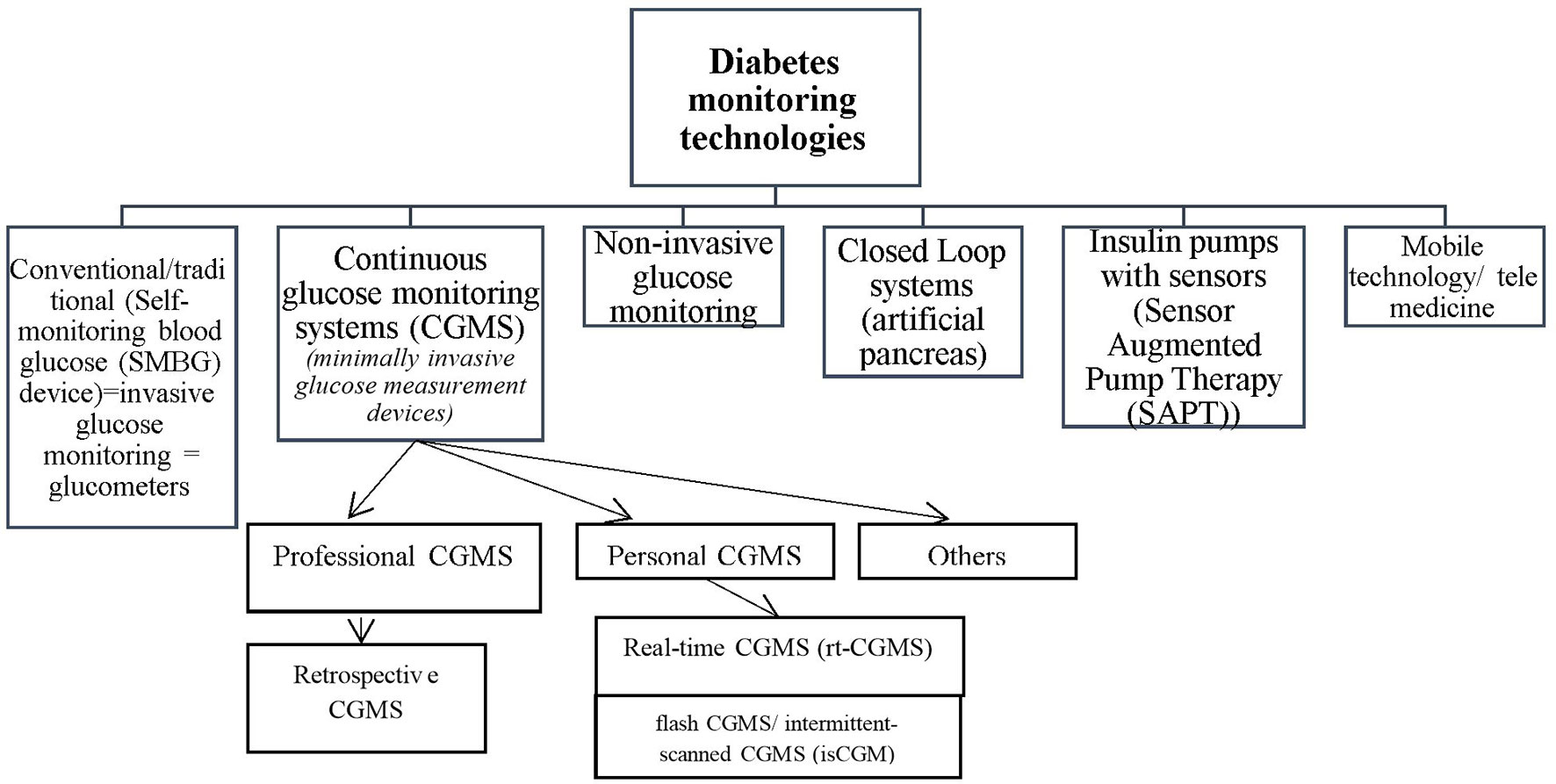
Figure 1 Classification of diabetes monitoring technologies.
Many systematic and literature reviews focusing on effectiveness of glucose monitoring devices are published in the literature. They differ in terms of the type of analyzed glucose monitoring device, type of diabetes, type of study—systematic review or systematic review and meta-analysis. No studies gather and systematize the available evidences for all diabetes patient subgroups on use of all types of DMS, their application, effectiveness, and cost-effectiveness. Due to expanding knowledge and inconsistent results between published studies we attempted to perform a systematic review of already published systematic reviews and systematic reviews + meta-analysis. Moreover, the future in diabetic patients’ medical care is in finding the most suitable individualized approach for treatment, diagnosis, or monitoring condition for the purposes of achieving the desired outcomes. Therefore, a comprehensive patient-oriented analysis of the available diabetes monitoring systems is required which could be used as a basis for defining the effective and cost-effective approaches for regular monitoring and control of diabetes patients. Furthermore, as an ever-growing body of evidence emerges, new ways of agglomerating all available data will be needed, in order to consolidate all relevant information to help decision makers paint a clearer picture. Our attempt in this paper to use existing methods in a different way could provide a steppingstone upon which to build more reliable assessments in diabetes. This work is part of the H2020 HTx project, whose goal is to provide a new generation of health technology assessments (https://www.htx-h2020.eu/). For this purpose, the project proposes to apply technological improvements to data curation, combining evidence extracted from real-world data sources in addition to evidence obtained reviewing existing methods.
The primary goal of the study is to review and consolidate evidences from multiple systematic reviews on the diabetes monitoring systems and the outcomes achieved. In addition, we wanted to systematize the approaches used for personalized treatment and monitoring of diabetes patients via new technologies. Moreover, this paper’s results and conclusions will be used as a basis for development of future technological improvements in the HTx project.
Materials and Methods
Study Design
A comprehensive systematic review of published systematic reviews investigating the effect of diabetes monitoring systems was performed. It was based on the following approach: (1) identification of a research question; (2) identification of inclusion and exclusion criteria; (3) data extraction; (4) reporting results; (5) assessment of risk of bias; (6) discussion and interpretation of the results. The research questions formulated during the study were focused on the available new technologies for diabetes monitoring; available systematic reviews and meta-analyses reporting the treatment outcomes; types of therapeutic outcomes reported and their variability.
The type of treatment outcomes that were observed were changes in the clinical parameters (HbA1c, glucose level, etc.); changes in the quality of life (QoL); number and frequency of hypo- and hyperglycemia episodes; change in the risk for complications; level of satisfaction from the intervention.For the identification of the studies, we performed an internet search of electronic databases PubMed, Cochrane library, Embase and proposed by them related articles. The key words for the search were “diabetes” AND “systematic review,” AND “CGMS” OR “SAPT” OR “CSII” OR “FGM” OR “Closed loop systems” OR “telemedicine.” For the presentation of the search results was used the principles of the PRISMA checklist with its four steps the search approach, as follows: identification, screening, eligibility, and inclusion. The search encompasses the period since the first systematic review identified till the end of 2019.
Inclusion and Exclusion Criteria
Specific inclusion and exclusion criteria were formulated. The criteria for inclusion were to be a systematic review of interventional or non-interventional (observational) studies about diabetes monitoring systems, to present clinical and/or economic effect of new technologies on diabetes patients, English language. The criteria for exclusion were lifestyle maintaining technologies, medicines, diet,exercise, algorithms’ decision supporting systems, mobile apps (especially those that relate to the lifestyle maintaining), alarms, and m-health. Our focus on excluding some studies was more on removing ones that rely solely on telemonitoring by physicians. If more than two studies were found from the same authors, the latest published article was taken into account.
Selection of Studies
Five authors (MK, MD, ZM, KT, GP) reviewed selected articles for duplication, relevance to the inclusion and exclusion criteria, and consolidate the evidences by systematizing them according to the technology described, type of the diabetes for which the technology is recommended, sources of information, clinical and/or economic results reported, recommendations for future application or improvement. Each author independently reviewed the articles for eligibility. Discrepancies between the authors were overcome through discussion, until reaching consensus. The main focus was on technologies aiming to improve diabetes control via improvement in glycated hemoglobin (HbA1c), hypo- or hyperglycemic episodes, or glucose secretion monitoring and not on improving the lifestyle habits and compliance.
Data Extraction and Summarization
The data extracted were summarized in tables including the following relevant information:
1. Supplementary Table 1—excluded full-text articles with reasons, publication year, name of the first author, type of technology observed, type of diabetes, type of review (systematic review or systematic review and meta-analysis), search strategy (database searched), number of relevant studies, and total number of participants;
2. Table 1, Table 2, and Table 3—included studies, reasons for inclusion, publication year, name of the first author, type of technology observed, type of diabetes, type of review (systematic review or systematic review and meta-analysis), search strategy (database searched), number of relevant studies, and total number of participants; intervention observed, comparator(s), change in clinical parameters, change in quality of life; comments and strength of evidence.
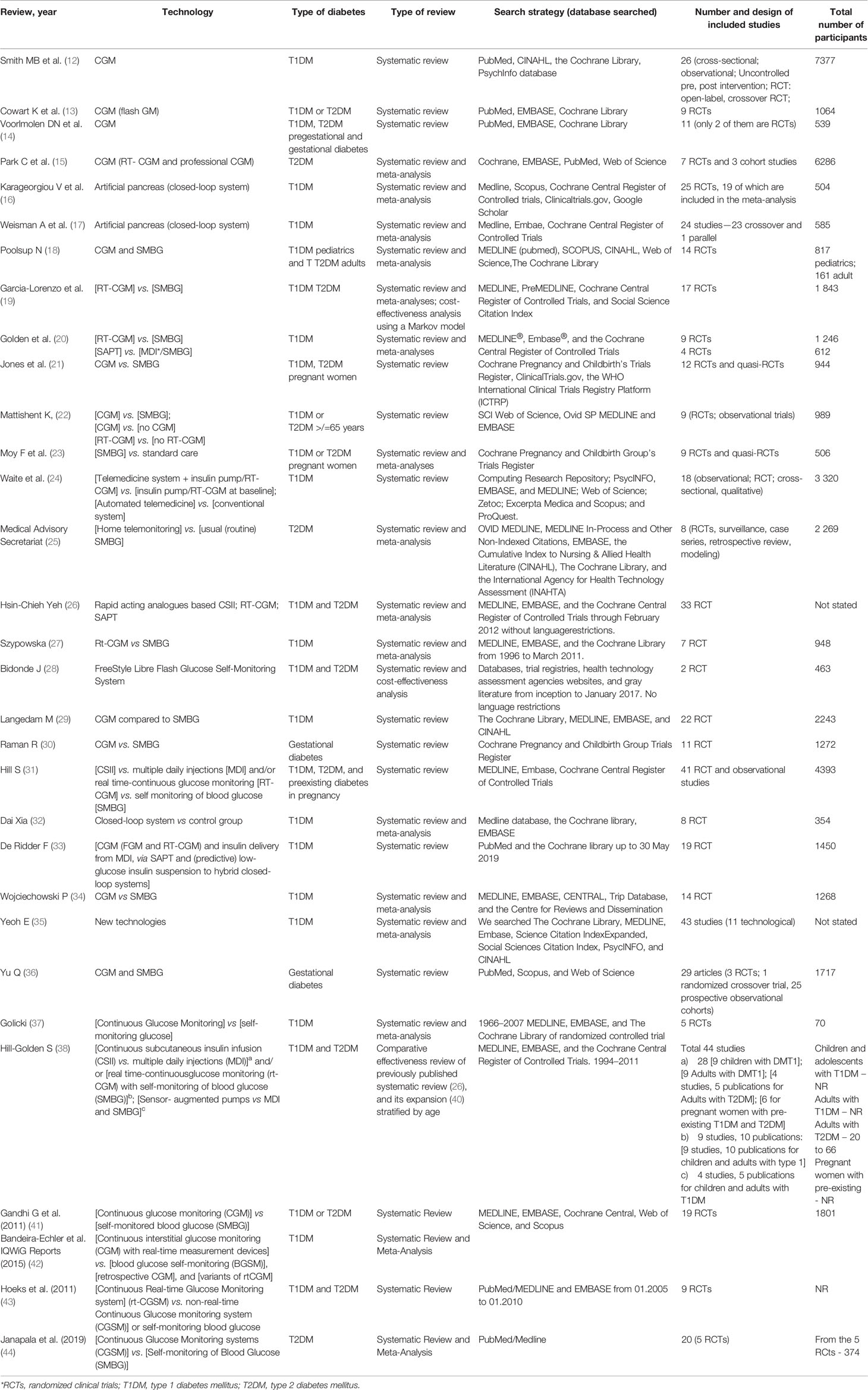
Table 1 Characteristics of the included systematic reviews and meta-analyses.
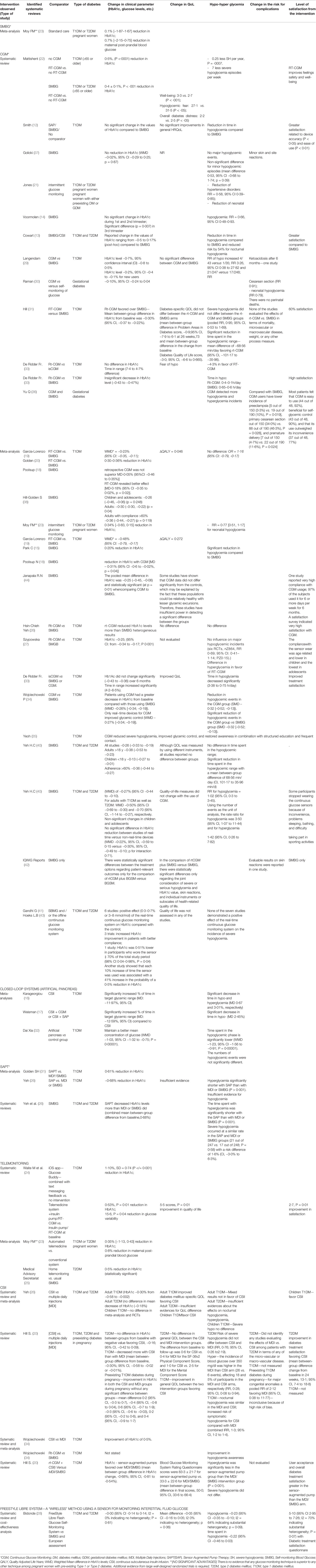
Table 2 Key findings of the included systematic reviews and meta-analyses by type of intervention.
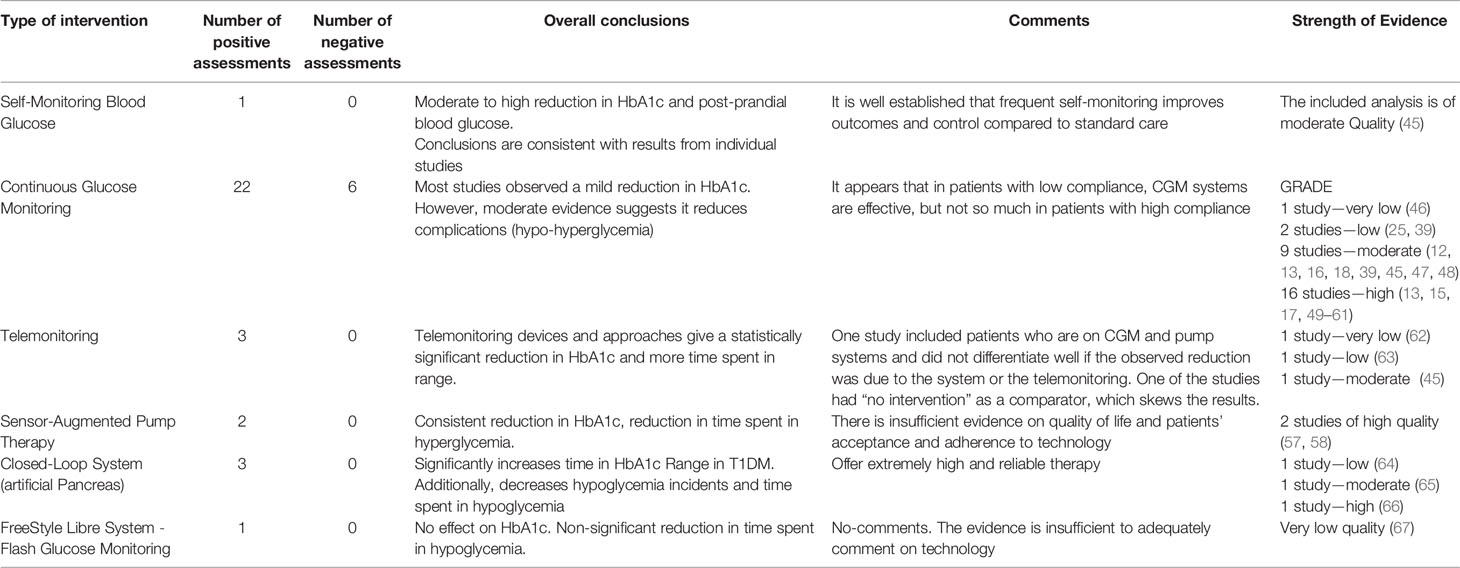
Table 3 Summary of the main results and conclusions.
Data Analysis
The upper and lower changes in clinical parameters were summarized by intervention, type of diabetes, and type of review [systematic review (SR) or systematic review and meta-analysis (SR/MA)]. The results were presented in tables and figures. We have not included detailed information about the sample size of primary studies and location of the study because we have focused mainly on the clinical outcomes described in the published systematic reviews and/or meta-analyses.
Assessment of the Risk of Bias in the Included Systematic Reviews
The methodology quality of systematic reviews and meta-analysis included in the current systematic review was assessed using the GRADE system (Table 3). GRADE has four levels of evidence—also known as certainty in evidence or quality of evidence: very low, low, moderate, and high. All included SRs and MAs were evaluated in five domains—Risk of Bias, Imprecision, Inconsistency, Indirectness, and Publication Bias. Publication bias in this context refers to the stated values of HbA1c in the reviewed papers and the conclusions drawn from the results, since unpublished and unreferenced studies are not available. All study conclusions were carefully reviewed along with the Supplemented Data. To minimize the risk of including predominantly “positive” analyses, we aimed to include also government-sanctioned assessments, which were available online, such as IQWiG reports, and reports by the US AHRQ (Agency for Health Research and Quality).
Results
Search Results
After the search in PubMed, and EMBASE with key words diabetes and new technologies 1,495 studies were screened based on abstracts. Then we performed the second search in PubMed and Cochrane library with the terms diabetes, systematic review, and new technologies and we identified 300 studies. We excluded 195 due to duplication and 1,216 due to non-correspondence with the inclusion criteria, and 84 studies were reviewed manually. After adding the term meta-analysis, we expand the list to 138 studies. Out of them 56 candidate full texts were reviewed a third time by an independent reviewer, and a further 24 were excluded. There are multiple reasons for excluding studies, which are all summarized in Supplementary Table 1, some of the reasons are systematic review of the application of the technologies, not purely on effectiveness, systematic reviews commissioned by regulatory bodies, which did not provide all evidence, but just a full working summary and others. Finally, we included 32 full systematic reviews and/or meta-analyses for which the research quеstion was clearly defined (12–38, 40–44). The included studies were of high quality, predominantly focusing on randomized controlled trials. Seven of the included systematic reviews included also observational studies assessing the effect of DMS in everyday clinical practice.
They are summarized in Table 1. A narrative synthesis is presented. Figure 2 presents the search process flow chart.
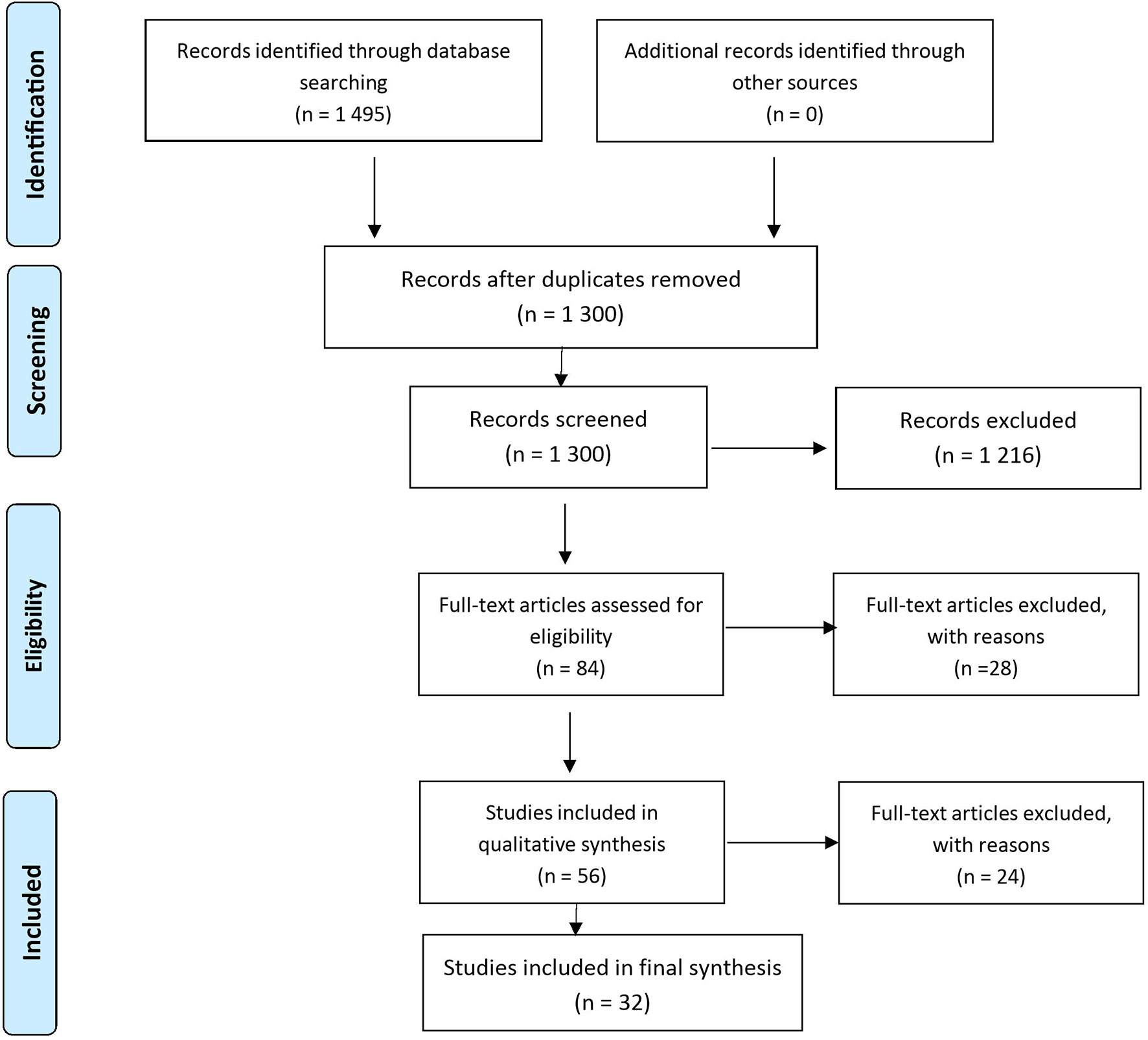
Figure 2 PRISMA 2009 Flow Diagram.
Characteristics of the Studies and Patient Populations
The details of the included SRs (n = 16) and SRs plus MAs (n = 16) are presented in Table 2. They were published in the period 2008–2019 and the number of analyzed studies (randomized clinical trials, cohort, crossover or parallel or prospective observational studies, etc.) in each separate SR or MA varied between 2 and 44. Diabetes monitoring systems observed were: Continuous Glucose Monitoring (CGMS), Sensor Augmented Pump Therapy (SAPT), Self-monitoring Blood Glucose (SMBG), Continuous subcutaneous insulin infusion (CSII), Flash Glucose Monitoring (FGM) or Intermittent-scanned continuous glucose monitoring (isCGM), Closed-loop systems, and telemedicine. All studies analyzed and reported the changes in glycated hemoglobin (HbA1c) levels as a primary clinical outcome. Some of them reported results about well-being, hypoglycemic fear and episodes, hyperglycemia incidents, overall diabetes distress, quality of life, patients’ satisfaction. Standard care (for example a weekly venipuncture protocol), conventional treatment (non-meter through urine tests and blood-glucose levels measured at the fortnightly clinic visits), or no comparator was used mainly as comparators for all CGMS. CGMSs were also compared with SMBG with or without CSII.
The technologies, that were assessed in the analyzed systematic reviews and meta-analyses, and the relevant number of studies identified are presented on Figures 3 and 4. The most reviewed technologies were the continuous glucose monitoring systems with 11 systematic reviews and 15 meta-analyses. One analysis focused on self-monitoring approaches. It should be noted that CGMS studies also evaluated continuous subcutaneous injections as a method of insulin delivery and had many analyzed subsections. Most analyses focused on Type 1 diabetes (26) with only a small amount analyzing separately intensive insulin control in Type 2 patients, or in a mixed sample of Type 1 and Type 2 diabetes patients. The number of studies investigating gestational diabetes patients are limited (6) as they mostly compare SMBG vs. CGM and SMBG vs. standard care.
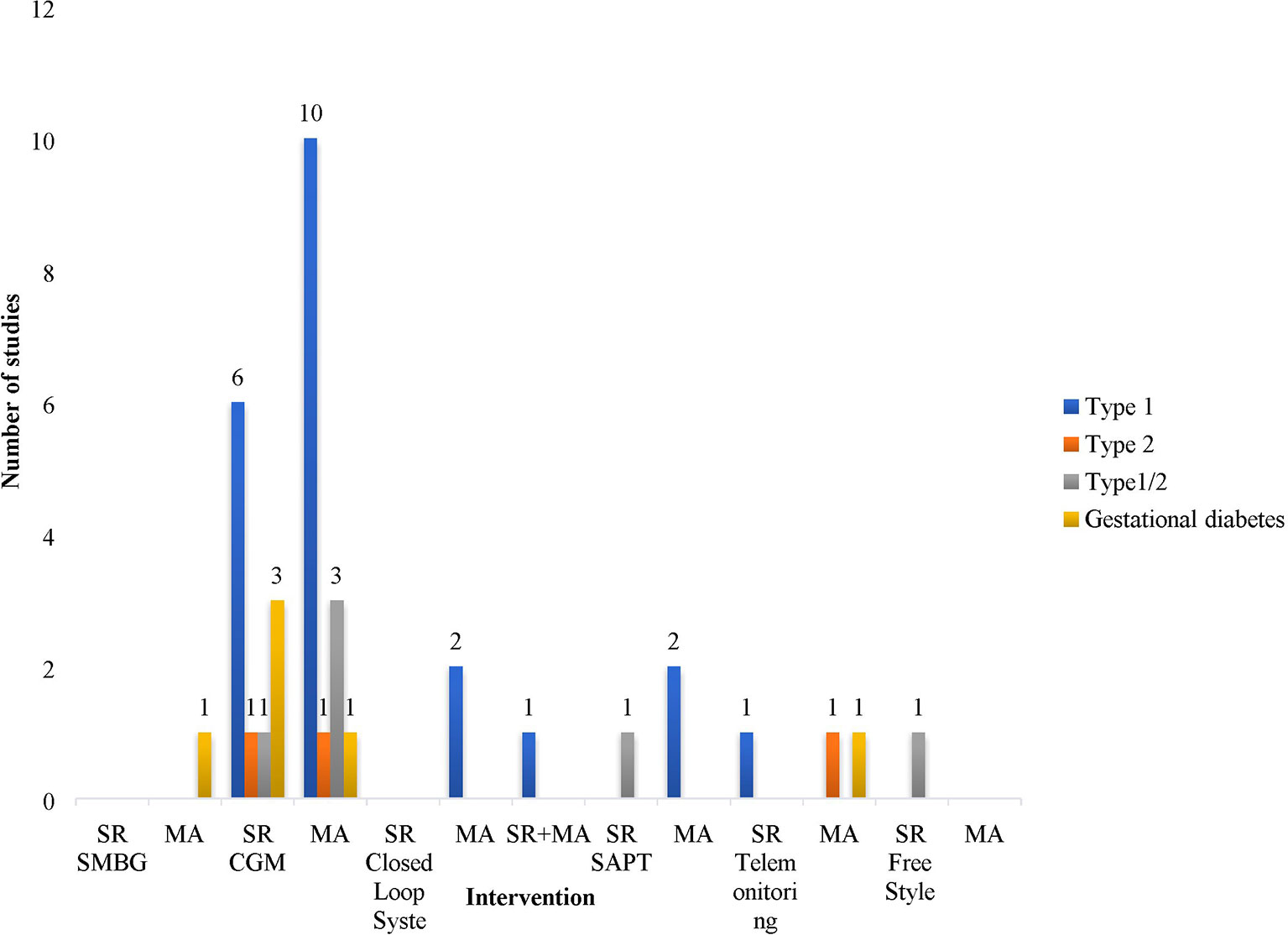
Figure 3 Number of studies presented by type of intervention and type of diabetes.
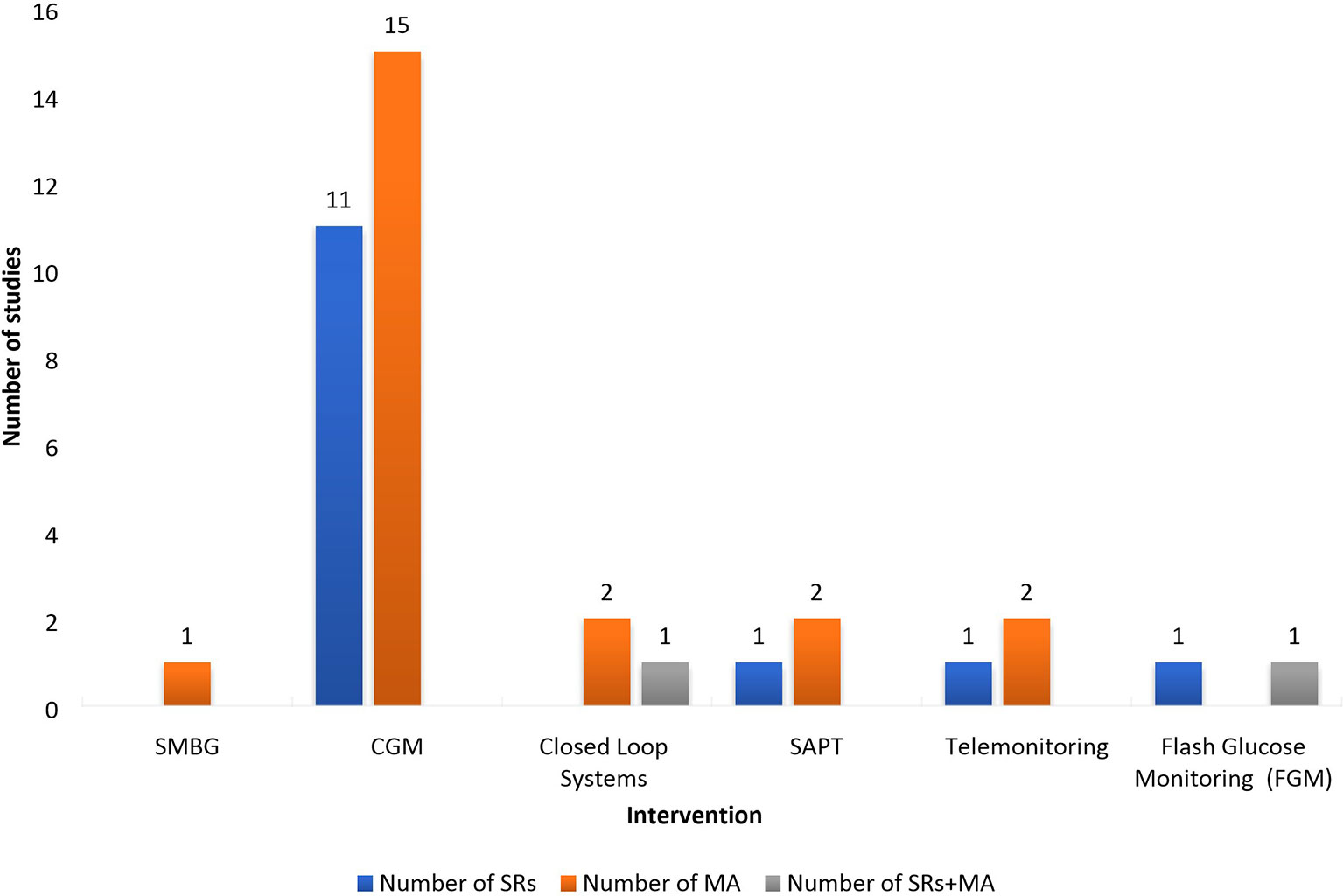
Figure 4 Number of studies presented by type of intervention and type of studies. SMBG, Self-monitoring Blood Glucose; CGM, Continuous Glucose Monitoring; MA, Meta-Analysis; SAPT, Sensor Augmented Pump Therapy; SR, Sytematic review.
Clinical Outcomes
Blood glucose levels are an important clinical measure for estimating effectiveness, and overall analysis of all included studies showed that there is a reduction in HbA1c levels. These can be seen in both Type 1 and Type 2 diabetes, for all interventions.The reductions are indeed almost negligble. Since the aim of control, even self-control of diabetes mellitus (DM), is to reduce HbA1c levels, the purpose of the new diabetes technologies, apart from blood glucose control is to reduce glycemic excursions, hypo- or hyperglycemia episodes, increase time spent within desired ranges, and improve compliance, especially in children. The reduction in glycated hemoglobin (HbA1c) levels varies from 0·17 to 0·70% during use of CGM. It is most significant for CGM identified in meta-analysis—from 0·23 to 0·37% for patients with Type 1 diabetes and from 0·20 to 0·48% for Type 2 diabetes. In systematic reviews a wider range and greater reduction of HbA1c were observed: from 0·20 to 0·70% in Type 1 and from 0·17 to 0·50% in Type 2. Telemonitoring would support the reduction of the HbA1c-levels in patients with Type 1 diabetes from 0·53 to 1·10%. Data for gestational diabetes was identified only for CGM where the reduction is 0·26–0·34% (23). Change in QALY (ΔQALY) was observed only in one study (19) and it is higher in Type 2 diabetes (0·272) than in Type 1 diabetes (0·046) when comparing real-time CGM vs. SMBG.
When using CGM the time spent in hypoglycemia is expected to be lower vs. SMBG—0·4–0·1 h/day vs. 0·65–0·6 h/day (31). Hill et al. (20), reported significant reduction in time spent in hyperglycemia—the mean difference was −68.56 min/day favoring RT-CGM (95% CI, −101·17 to −35·96) vs. SMBG. CGM ensured the rate for hypoglycemia of 3·50 (95% CI, 1·07 to 11·44) and for hyperglycemia 1·42 (95% CI, 0·26 to 7·82) when comparing SMBG and CGM. Significant decrease in time in hypo- and hyperglycemia for closed-loop systems in comparison with CSII was observed—mean difference of 0·67 and 3·01%, respectively (16).
Discussion
Summary of Results
We took a much broader approach of including systematic reviews of randomized clinical trials (RCTs) and observational studies because regulatory authorities prefer to have a real-world evidence for the decision making when they decide to reimburse a particular device. The most notable conclusions, with the level of evidence used are summarized in Table 2. Since we predominantly focused on SRs and MAs of randomized trials, the strength of evidence for most studies is high, such as in DMS, where 16 of the 26 studies were of high quality and 9 of moderate. We used the GRADE system to assess study quality, and it should be noted, that GRADE includes some subjectivity, since it is implemented manually and not mechanically. Although the GRADE system is transparent, the decision ultimately falls on the reviewer whether to downgrade a randomized trial based on the GRADE system’s “factors which may influence the quality level of a body of evidence.” The closed-loop systems significantly reduce complications such as hypo- or hyperglycemia, as well as the CGMs, which although moderately effective, increased the time spent in range regardless if the monitoring system was with self-injection or continuous injection delivery methods. Patients with high-compliance benefit less than patients with low compliance. Based on the collected evidence the current systematic review could highlight that the CGM is an effective and suitable method for monitoring of blood glucose levels. It could ensure reductions in HbA1c as they vary in a wide range—between 0.20–0.70% in Type 1 and between 0.17 and 0.50% in Type 2 diabetes patients. The accuracy and benefits of CGM utilization are deeply examined and confirmed. The evidences reveal that real-time CGM in Type 1 diabetes improves clinical parameters, whereas a smaller number of studies consider the results of patients with Type 2 diabetes. The recommendations mainly concern improvement of unforeseen hypoglycemia risk and glucose variability in Type 2 diabetes patients (49, 51). In our study we also found that larger number of analysis are focused on Type 1 diabetes, while those analyzing the results in Type 2 or combined studies are a smaller number.
The latest years precision of CGM systems has improved and their accuracy within glucose levels >80–200 mg/dl is similar (46). CGM could be used for self-adjustment of dosage, interpretation of hypoglycemia results, and measurement of response to therapy as it covers a wide range of glucose values. Its accuracy depends also on glucose levels variability (39). CGM is likely to improve treatment results, improve glycemic control and quality of life, as well as lower micro- and macro-vascular outcomes despite the existing barriers and educational needs for physicians and patients (55, 65, 66). The utilization of CGM with remote monitoring in children with Type 1 diabetes leads to better quality of life, parental sleep, and decreases family stress (56), while utilization in youth with Type 1 diabetes resulted in improved adherence, glycemic control, as well as a low psychosocial distress (57). Moreover, CGM is able to pick up asymptomatic hypoglycemic episodes in older patients with diabetes Type 1 or 2 and to ensure a reduction in severe hypoglycemic episodes (47). Argento et al. reported that the severe hypoglycemic episodes dropped from 52 (5 years before CGM initiation) to 12 after starting CGM (50). The proportion of patients with Type 1 diabetes with any severe hypoglycemia felt from 79 to 31% after initiation of CGM. However, Lagarde et al. concluded that no difference exists between the number of minor hypoglycemic episodes between the CGMS and the control group of children with Type 1 diabetes (mean difference 0·53, 95% CI, −0·68 to 1·74; p = 0·39) (47). Similar results are presented by Langendam et al. —no significant difference is revealed in risk of severe hypoglycemia or ketoacidosis between CGM and SMBG adults with Type 1 diabetes (29). However, due to the small number of participants and limitations, findings should be interpreted with significant caution. Hill et al. did not find any significant difference in severe hypoglycemia events between the rt-CGM and SMBG groups, but found a significant reduction in time spent in the hyperglycemic range (31). Decreased time in hypoglycemia (13 out of 15 studies) in Type 1 diabetes as well as increased time in range (TIR) as a result of CGM usage were also observed in a systematic review by De Ridder et al. (33). Other study reported that adult patients with Type 1 diabetes who use CGM perceive improvements in their quality of life, especially related to hypoglycemia fear (22). Only a few studies have found positive outcomes regarding hypoglycemia when using CGM (reduction in nocturnal hypoglycemia episodes by 54% with is CGM vs. SMBG (−0·29 ± 0·08 h per 7 h; P = 0·0001) (45, 63) but no decrease in time spent in hypoglycemia was observed. The other important outcome, Time in Glycemic Range (70–180 mg/dl), is reported to increase with isCGM (intermittently scanned) among well-controlled patients with Type 1 diabetes (33). Whereas, the results are controversial among adult patients with uncontrolled T2DM using insulin (62).
Jones et al., reported that CGM is able to reduce neonatal hypoglycemia (RR 0·66, 95% CI 0·48 to 0·93; 3 studies, 428 infants) (21). Latest updated evidence from 2019 by Yu et al. suggests that CGM is superior to SMBG among pregnant women with gestational diabetes mellitus as it is able to detect hypoglycemic and hyperglycemic episodes (36). Therefore, regular monitoring of glucose levels in pregnant women with diabetes through specific glucose monitoring devices could ensure limitation of hypoglycemic episodes and then influence the outcomes for both mother and child. No significant improvement in the frequency of neonatal hypoglycemia or any other primary outcomes were detected among pregnant women with pre-existing diabetes when using glucose monitoring technique.
Our study reveals a small number of MAs and SRs exploring results in CGM utilization in children. The findings show that CSII was associated with improved quality of life compared with MDI and similar results on HbA1c levels and severe hypoglycemia. Regarding closed-loop systems, meta-analyses by Karageorgiou et al., and by Weisman et al., showed that these systems lead to significantly higher percentage of time spent in the target glycemic range and to lower percentages of time in hyperglycemia and hypoglycemia for non-adult Type 1 diabetes patients (16, 17). Free Style Libre Flash Glucose Self-Monitoring System also showed promising results for reduction in time and number of events with glucose levels <3·9 in 24 h in comparison with SMBG. Evidence regarding isCGM (Intermittent-scanned continuous glucose monitoring) impact on improving time in glycemic range, glycemic variability, and hypoglycemia are variable and further clinical trials should investigate these devices (12).
Because of the variability and lack of enough strong evidence, no general conclusion or recommendation about the patients target groups who might be most suitable for particular DMS could be highlighted. Basing on the available evidence, it could be mentioned that patients’ satisfaction, preferences, lifestyle habits, age, therapy applied, and severity of the condition (type of diabetes, duration, concomitant diseases, etc.) are some of the main criteria for choosing a method for monitoring and control.
Limitations and Strengths
The current systematic review has significant strengths as it gathers evidence for the effectiveness of a variety of diabetes monitoring devices both from controlled interventional studies and observational studies from the everyday clinical practices thus providing the opportunity to assess the effects of DMS from the perspective of different study desings. Moreover, a wide range of diabetes patients were included in the analysis—diagnosed with Type 1, Type 2, or gestational diabetes. Multiple databases were searched to identify relevant studies which answer to the research question. This systematic review of reviews provides evidence to inform both clinical practice and future research.
The main limitation is that the number of evidences for some diabetes monitoring systems such as telemonitoring, closed-loop systems, and SAPT, is too narrow, not sufficiently enough, and lack of statistical significance to make general conclusions. Moreover, different outcomes are measured and compared in the different studies which is a strong complication for a more comprehensive synthesis and analysis. Because of the limited data for assessing the effectiveness of monitoring technologies only the reduction in HbA1c levels for some DMS was analyzed. There are other criteria for assessing the quality of glycemic control such as number, duration of hypo- and hyperglycemic episodes, and time in glycemic range. Due to insufficient and controversial evidence for all valuable parameters, we assessed and presented only the variability in HbA1c for different patients’ groups and by type of study analysed (SR or SR+MA). Moreover, due to the heterogeneity of the methodologies, patient populations, and gathered data, we were not able to perform formal meta-analysis. So, a narrative synthesis is presented which could also be highlighted as a strong limitation of the study. Some DMS are innovative and not commonly applied so there is not enough relevant evidence. No studies comparing FGM and rt-CGM were included and analyzed in the current review which could be highlighted as another limitation of the review.
We made a distinction between the studies only on the criteria of whether they are only systematic reviews or include and meta-analysis of the analysed studies. No other selection criteria were applied for the primary studies included in each one of the observed reviews. We recognize that it might be a limitation of our analysis but trusted the authors performing the systematic reviews in their proper selection of the comparable RCTs or observational studies.
Comparison With Other Studies
Very few studies performing a systematic review of already published SR and SR+MA of continuous glucose monitoring systems were identified. Published studies focus mainly on specific group of patients with Type 1 or Type 2 diabetes and on specific intervention (58).
However, a similar approach of systematizing published MA assessing supported self-management for people with Type 2 diabetes was identified. The authors focus on the role of self-management mechanism as one of main factors affecting the treatment outcomes and quality of life of patients. Some of the studies in the systematic review of meta-analysis show that self-monitoring systems and tele-health may provide some advantages in the process of self-management. Authors’ conclusions focus mainly on informative type of these findings which could be in favor to policy makers and health care professionals (59).
Other systematic review of reviews evaluates technology-enabled diabetes self-management. The study shows that mobile technologies for self-management of diabetes improve patient-generated health data and communication between patients and health care professionals. The results show that technology-enabled diabetes self-management solutions significantly improve HbA1c (67).
Similar to our results, a conducted narrative review showed that use of CGM in Type 2 diabetes patients leads to greater reductions in HbA1c in comparison with traditional self-monitoring as higher compliance to CGM was also reported. Logically, addition of other methods to CGM such as lifestyle counseling could lead to further improvements (52).
Evidences of key publications associating CGMS reported improvement in clinical outcomes, reducing of hypoglycemia and impact on physical, emotional, and relational aspects of everyday life (48). The positive effects of CGMS utilization are discussed from American Association of Clinical Endocrinologists and the American College of Endocrinology. The conclusion they reach is that increasing utilization of CGMS will probably improve the health outcomes, decrease health care resource costs for acute and chronic complications (53).
A review on studies observing glucose management reported that according to current literature evidence utilization of CGMS is mainly recommended in T1DM patients with a poor control of HbA1c levels after SMBG and risk of hypoglycemia, which confirms our findings. Utilization of CGMS is favored for patients with Type 2 diabetes who reported severe hypoglycemia or suspected hypoglycemia, particularly nocturnal (64).
We found very few studies reporting the M-value (durable nyctohemeral measurement of glycemic behavior) (16, 17) and SD of 24-h glucose (24, 32, 33) and did not find a study reporting the Mean amplitude of glycemic excursion (MAGE). We recognize that those measures of continuous diabetes control are currently introduced and might be more informative for the endocrinologist. Further studies need to be done to explore the previous research/systematic reviews investigating the effect of DMS on indices of glycemic variability such as MAGE, M-value, and SD of average 24-h glucose concentrations in patients with diabetes.
Only a few studies, however, assess the role of meta-analyses and systematic reviews on diabetes monitoring systems and their efficacy in terms of the HTA perspective. Insufficient cost-effectiveness studies and randomized clinical trials in specific patient populations used in HTA resulted in different criteria and rate of reimbursement among countries (54). In 2018 EUnetHTA published an HTA core model for rapid relative effectiveness assessment of continuous glucose monitoring (CGM real time, rtCGM) and flash glucose monitoring (FGM) as personal, standalone system in patients with diabetes mellitus treated with insulin (60). This report shows that in the light of the increasing number of different systems for rtCGM available on the market, systematic reviews and meta-analyses assessing their relative clinical effectiveness could be of a great importance in the assessment of their cost-effectiveness in terms of decision making. These studies could provide a summary of the best scientific available evidence which could facilitate the appraisal process and decision making and could favor the national/regional/local HTA. Health Technology Wales evidence appraisal report also included systematic review on the clinical and cost-effectiveness when providing decision for FreeStyle Libre flash glucose monitoring for the management of Type 1 or Type 2 diabetes (61).
Future Studies
Future studies should be performed to evaluate each technology for all subgroups of patients, since preliminary results showed also that effectiveness is better in adults than in children. In children, however, the habituation with the devices is better which determines better compliance. These findings could also facilitate not only the process of patient-centered care but also could provide methodologies for personalized information on the effectiveness and cost-effectiveness of such health technologies thus improving the decision making process in terms of reimbursement.
Conclusions
Current systematic review of already published systematic reviews and meta-analyses suggests that no statistically significant difference exists between the values of HbA1c as a result of application of any type of DMS. The most notable are the changes in HbA1c for patients with Type 1 diabetes using CGM devices. The number of hypo- and hyperglycemic episodes and Time in Glycemic Range are some of the most valuable outcomes that should be considered when choosing the most appropriate diabetes monitoring system for each patient. Undoubtedly, as the American Diabetes Association currently recommends, CGM are most suitable for diabetes patients with insufficient and unsatisfied disease control and high risk of hypoglycemia. However, due to the diversity of the results about the real effectiveness of DMS, future more comprehensive studies assessing the effectiveness, cost-effectiveness, and comparative effectiveness of DMS, stratifying the patients in different subgroup, are needed.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
All the authors have provided valuable contributions to the manuscript. Conceptualization: GP, WG, GG-S. Formal analysis: MK, KT, MD, ZM, GP. Methodology: GP, MD, ZM. Project administration: GP, WG. Writing: MK, KT, MD, ZM, GP. Writing—review and editing: WG, GG-S, KT, MH. Validation: WG, GG-S, MH, MK. All authors contributed to the article and approved the submitted version.
Funding
The investigation has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 825162: “HTx: Next Generation Health Technology Assessment to support patient-centered, societally oriented, real-time decision-making on access and reimbursement for health technologies throughout Europe” (H2020-825162, 2019-2023).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2021.636959/full#supplementary-material
References
1. Vashist SK. Non-invasive glucose monitoring technology in diabetes management: a review. Anal Chim Acta (2012) 750:16–27. doi: 10.1016/j.aca.2012.03.043
2. Olokoba AB, Obateru OA, Olokoba LB. Type 2 diabetes mellitus: a review of current trends. Oman Med J (2012) 27(4):269–73. doi: 10.5001/omj.2012.68
3. Asif M. The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. J Educ Health Promot (2014) 3:1. doi: 10.4103/2277-9531.127541
4. Adu MD, Malabu UH, Malau-Aduli AEO, Malau-Aduli BS. Enablers and barriers to effective diabetes self-management: A multi-national investigation. PloS One (2019) 14(6):e0217771. doi: 10.1371/journal.pone.0217771
5. van Steen SC, Rijkenberg S, Limpens J, van der Voort PH, Hermanides J, DeVries JH. The Clinical Benefits and Accuracy of Continuous Glucose Monitoring Systems in Critically Ill Patients-A Systematic Scoping Review. Sensors (Basel) (2017) 17(1):146. doi: 10.3390/s17010146
6. Aberer F, Hajnsek M, Rumpler M, Zenz S, Baumann P, Elsayed H, et al. Evaluation of subcutaneous glucose monitoring systems under routine environmental conditions in patients with type 1 diabetes. Diabetes Obes Metab (2017) 19(7):1051–5. doi: 10.1111/dom.12907
8. Health Quality Ontario. Continuous Monitoring of Glucose for Type 1 Diabetes: A Health Technology Assessment. Ont Health Technol Assess Ser (2018) 18(2):1–160.
9. Gómez AM, Henao D, Imitola A, Muñoz OM, Sepúlveda MA, Kattah L, et al. Efficacy and safety of sensor-augmented pump therapy (SAPT) with predictive low-glucose management in patients diagnosed with type 1 diabetes mellitus previously treated with SAPT and low glucose suspend. Endocrinol Diabetes y Nutrición (2018) 65(8):451–7. doi: 10.1016/j.endien.2018.03.015
10. Gómez AM, Henao Carrillo DC, Muñoz Velandia OM. Devices for continuous monitoring of glucose: update in technology. Med Devices (Auckl) (2017) 12; 10:215–24. doi: 10.2147/MDER.S110121
11. Steineck I, Ranjan A, Nørgaard K, Schmidt S. Sensor-Augmented Insulin Pumps and Hypoglycemia Prevention in Type 1 Diabetes. J Diabetes Sci Technol (2017) 11(1):50–8. doi: 10.1177/1932296816672689
12. Smith MB, Albanese-O'Neill A, Macieira TGR, Yao Y, Abbatematteo JM, Lyon D, et al. Human Factors Associated with Continuous Glucose Monitor Use in Patients with Diabetes: A Systematic Review. Diabetes Technol Ther (2019) 21(10):589–601. doi: 10.1089/dia.2019.0136
13. Cowart K, Updike W, Bullers K. Systematic review of randomized controlled trials evaluatingglycemic efficacy and patient satisfaction of intermittent-scanned continuous glucose monitoring inpatients with diabetes. Diabetes Technol Ther (2019) 22(5):337–45. doi: 10.1089/dia.2019.0345
14. Voormolen DN, DeVries HJ, Evers IM, Mol BWJ, Franx A. The efficacy and effectiveness of continuous glucose monitoring during pregnancy: a systematic review. Obstetrical Gynaecol Survey (2013) 68(11):753–63. doi: 10.1097/OGX.0000000000000002
15. Park C, Le QA. The Effectiveness of Continuous Glucose Monitoring in Patients with Type 2 Diabetes: A Systematic Review of Literature and Meta-analysis. Diabetes Technol Ther (2018) 20(9):613–21. doi: 10.1089/dia.2018.0177
16. Karageorgiou V, Papaioannou TG, Bellos I, Alexandraki K, Tentolouris N, Stefanadis C, et al. Effectiveness of artificial pancreas in the non-adult population: A systematic review and network meta-analysis. Metabolism (2019) 90:20–30. doi: 10.1016/j.metabol.2018.10.002
17. Weisman A, Bai JW, Cardinez M, Kramer CK, Perkins BA. Effect of artificial pancreas systems on glycaemic control in patients with type 1 diabetes: a systematic review and meta-analysis of outpatient randomised controlled trials. Lancet Diabetes Endocrinol (2017) 5(7):501–12. doi: 10.1016/S2213-8587(17)30167-5
18. Poolsup N, Suksomboon N, Kyaw AM. Systematic review and meta-analysis of the effectiveness of continuous glucose monitoring (CGM) on glucose control in diabetes. Diabetol Metab Syndr (2013) 235:39. doi: 10.1186/1758-5996-5-39
19. García-Lorenzo B, Rivero-Santana A, Vallejo-Torres L, Castilla-Rodríguez I, García-Pérez S, García-Pérez L, et al. Cost-effectiveness analysis of real-time continuous monitoring glucose compared to self-monitoring of blood glucose for diabetes mellitus in Spain. J Eval Clin Pract (2018) 24(4):772–81. doi: 10.1111/jep.12987
20. Golden SH, Brown T, Yeh HC, Maruthur N, Ranasinghe P, Berger Z, et al. Methods for Insulin Delivery and Glucose Monitoring: Comparative Effectiveness. Rockville (MD): Agency for Healthcare Research and Quality (US) (2012).
21. Jones LV, Ray A, Moy FM, Buckley BS. Techniques of monitoring blood glucose during pregnancy for womenwith pre-existing diabetes. Cochrane Database Syst Rev (2019) 5(5):CD009613. doi: 10.1002/14651858.CD009613.pub4
22. Mattishent K, Loke YK. Detection of asymptomatic drug-induced hypoglycemia using continuous glucose monitoring in older people - Systematic review. J Diabetes Complications (2018) 32(8):805–12. doi: 10.1016/j.jdiacomp.2018.05.005
23. Moy FM, Ray A, Buckley BS. Techniques of monitoring blood glucose during pregnancy for women with pre-existing diabetes. Cochrane Database Syst Rev (2014) 4):CD009613. doi: 10.1002/14651858.CD009613.pub2
24. Waite M, Martin C, Franklin R, Duce D, Harrison R. Human Factors and Data Logging Processes With the Use of Advanced Technology for Adults With Type 1 Diabetes: Systematic Integrative Review. JMIR Hum Factors (2018) 5(1):e11. doi: 10.2196/humanfactors.9049
25. Medical Advisory Secretariat. Home telemonitoring for type 2 diabetes: an evidence-based analysis. Ont Health Technol Assess Ser (2009) 9(24):1–38.
26. Yeh H, Brown TT, Maruthur N, Ranasinghe P, Berger Z, Suh YD, et al. Comparative Effectiveness and Safety of Methods of Insulin Delivery and Glucose Monitoring for Diabetes Mellitus: A Systematic Review and Meta-analysis. Ann Intern Med (2012) 157:336–47. doi: 10.7326/0003-4819-157-5-201209040-00508
27. Szypowska A, Ramotowska A, Dzygalo K, Golicki D. Beneficial effect of real-time continuous glucose monitoring system on glycemic control in type 1 diabetic patients: systematic review and meta-analysis of randomized trials. Eur J Endocrinol (2012) 166(4):567–74. doi: 10.1530/EJE-11-0642
28. Bidonde J, Fagerlund BC, Frønsdal KB, Ulrikke H, Robberstad B. (2017). Single-technology assessment: FreeStyle Libre Flash Glucose Self-Monitoring System. Norwegian Institute of Public Health (NIPH), Oslo. Available at: https://www.fhi.no/globalassets/dokumenterfiler/rapporter/2017/freestyle-libre-flash-glucose-self-monitoring-system-a-single-technology-assessment-rapport-2017-v3.pdf.
29. Langendam M, Luijf YM, Hooft L, Devries JH, Mudde AH, Scholten RJ. Continuous glucose monitoring systems for type 1 diabetes mellitus. Cochrane Database Syst Rev (2012) 1(1):CD008101. doi: 10.1002/14651858.CD008101.pub2
30. Raman P, Shepherd E, Dowswell T, Middleton P, Crowther CA. Different methods and settings for glucose monitoring for gestational diabetes during pregnancy. Cochrane Database Syst Rev (2017) 10(10):CD011069. doi: 10.1002/14651858.CD011069.pub2
31. Golden SH, Brown T, Yeh HC, Maruthur N, Ranasinghe P, Berger Z, et al. Comparative Effectiveness Review No. 57. Rockville MD: Agency forHealthcare Research and Quality; Jul, 2012. Methods for Insulin Delivery and Glucose Monitoring: Comparative Effectiveness. Prepared by Johns Hopkins University Evidence-based Practice Center under Contract No. 290-2007-10061-I. Rockville (MD): Agency for Healthcare Research and Quality (US) (2012).
32. Xia D, Luo Z-c, Zhai LU, Zhao W-p, Huang F. Artificial Pancreas as an Effective and Safe Alternative in Patients with Type 1 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Ther (2018) 9:1269–77. doi: 10.1007/s13300-018-0436-y
33. De Ridder F, den Brinker M, De Block C. The road from intermittently scanned continuous glucose monitoringto hybrid closed-loop systems. Part B: results from randomized controlled trials. Ther Adv Endocrinol Metab (2019)10:1–17. doi: 10.1177/2042018819871903
34. Wojciechowski P, Ryś P, Lipowska A, Gawęska M, Małecki MT. Efficacy and safety comparison of continuous glucose monitoring and self-monitoring of blood glucose in type 1 diabetes: systematic review and meta-analysis. Pol Arch Med Wewn (2011) 121(10):333–43. doi: 10.20452/pamw.1087
35. Yeoh E, Choudhary P, Nwokolo M, Ayis S, Amiel SA. Interventions That Restore Awareness of Hypoglycemia in Adults With Type 1 Diabetes: A Systematic Review and Meta-analysis. Diabetes Care (2015) 38(8):1592–609. doi: 10.2337/dc15-0102
36. Yu Q, Aris IM, Tan KH, Li L-J. Application and Utility of Continuous Glucose Monitoring in Pregnancy: A Systematic Review. Front Endocrinol (2019) 10:697. doi: 10.3389/fendo.2019.00697
37. Golicki DT, Golicka D, Groele L, Pankowska E. Continuous Glucose Monitoring System in children with type 1 diabetes mellitus: a systematic review and meta-analysis. Diabetologia (2008) 51:233–40. doi: 10.1007/s00125-007-0884-9
38. Golden SH, Sapir T. Methods for insulin delivery and glucose monitoring in diabetes: summary of a comparative effectiveness review. J Manag Care Pharm (2012) 18(6 Suppl):S1–S17. doi: 10.18553/jmcp.2012.18.s6-a.1
39. Rodbard D. Characterizing accuracy and precision of glucose sensors and meters. J Diabetes Sci Technol (2014) 8(5):980–5. doi: 10.1177/1932296814541810
40. Yeh HC, Lau BD, Golden SH, Donner T, Brown TT, Bass EB. Insulin Delivery and Glucose Monitoring Methods: Future Research Needs: Identification of Future Research Needs From Comparative Effectiveness Review No. 57. Rockville (MD): Agency for Healthcare Research and Quality (US) (2013).
41. Gandhi G, Kovalaske M, Kudva Y, Walsh K, Elamin M, Beers M. Efficacy of Continuous Glucose Monitoring in Improving Glycemic Control and Reducing Hypoglycemia: A Systematic Review and Meta-Analysis of Randomized Trials. J Diabetes Sci Tech (2011) 5(4):952–64.
42. IQWiG Reports. (2015). Executive summary of final report D12-01. Continuous interstitial glucose monitoring (CGM) with real-time measurement devices in insulin-dependent diabetes mellitus. Cologne. available from: D12-01_Executive-Summary_Continuous-glucose-monitoring-CGM-with-real-time-measurement-devices.pdf
43. Hoeks LB, Greven WL, de Valk HW. Real-time continuous glucose monitoring system for treatment of diabetes: a systematic review. Diabetes Med (2011) 28(4):386–94. doi: 10.1111/j.1464-5491.2010.03177.x
44. Janapala RN, Jayaraj JS, Fathima N, Kashif T, Usman N, Dasari A, et al. Continuous Glucose Monitoring Versus Self-monitoring of Blood Glucose in Type 2 Diabetes Mellitus: A Systematic Review with Meta-analysis. Cureus (2019) 11(9):e5634.
45. Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline JP, Rayman G. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther (2017) 8(1):55–73.
46. Fokkert MJ, van Dijk PR, Edens MA, Abbes S, de Jong D, Slingerland RJ, et al. Performance of the FreeStyle Libre Flash glucose monitoring system in patients with type 1 and 2 diabetes mellitus. BMJ Open Diabetes Res Care (2017) 5:e000320. doi: 10.1136/bmjdrc-2016-000320
47. Lagarde WH, Barrows FP, Davenport ML, Kang M, Guess HA, Calikoglu AS. Continuous subcutaneous glucose monitoring in children with type 1 diabetes mellitus: a single-blind, randomized, controlled trial. Pediatr Diabetes (2006) 7:159–64. doi: 10.1111/j.1399-543X.2006.00162.x
48. Bode BW, Battelino T. Continuous Glucose Monitoring in 2018. Diabetes Technol Ther (2019) 21(S1):S13–31. doi: 10.1089/dia.2019.2502
49. Carlson AL, Mullen DM, Bergenstal RM. Clinical Use of Continuous Glucose Monitoring in Adults with Type 2 Diabetes. Diabetes Technol Ther (2017) 19(S2):S4–S11. doi: 10.1089/dia.2017.0024
50. Argento NB, Nakamura K. Personal real-time continuous glucose monitoring in patients 65 years and older. Endocr Pract (2014) 20:1297–302. doi: 10.4158/EP14017.OR
51. Wood A, O'Neal D, Furler J, Ekinci EI. Continuous glucose monitoring: a review of the evidence, opportunities for future use and ongoing challenges. Intern Med J (2018) 48(5):499–508. doi: 10.1111/imj.13770
52. Taylor PJ, Thompson CH, Brinkworth GD. Effectiveness and acceptability of continuous glucose monitoring for type 2 diabetes management: A narrative review. J Diabetes Investig (2018) 9(4):713–25. doi: 10.1111/jdi.12807
53. Fonseca V, Grunberger G, Anhalt H, Bailey T, Blevins T, Garg S, et al. Continuous glucose monitoring: a consensus conference of the American association of clinical endocrinologists and American college of endocrinology. Endocr Pract (2016) 22(8):1008–21. doi: 10.4158/EP161392.CS
54. Graham C. Continuous Glucose Monitoring and Global Reimbursement: An Update. Diabetes Technol Ther (2017) 19(S3):S60–6. doi: 10.1089/dia.2017.0096
55. Vigersky RA. Going beyond HbA1c to understand the benefits of advanced diabetes therapies. J Diabetes (2019) 11(1):23–31. doi: 10.1111/1753-0407.12846
56. Burckhardt MA, Roberts A, Smith GJ, Abraham MB, Davis EA, Jones TW. The Use of Continuous Glucose Monitoring With Remote Monitoring Improves Psychosocial Measures in Parents of Children With Type 1 Diabetes: A Randomized Crossover Trial. Diabetes Care (2018) 41(12):2641–3. doi: 10.2337/dc18-0938
57. Giani E, Snelgrove R, Volkening LK, Laffel LM. Continuous Glucose Monitoring (CGM) Adherence in Youth With Type 1 Diabetes: Associations With Biomedical and Psychosocial Variables. J Diabetes Sci Technol (2017) 11(3):476–83. doi: 10.1177/1932296816676280
58. Magwood GS, Zapka J, Jenkins C. A review of systematic reviews evaluating diabetes interventions. Diabetes Educ (2008) 34(2):242–65. doi: 10.1177/0145721708316551
59. Captieux M, Pearce G, Parke HL, Epiphaniou E, Wild S, Taylor SJC, et al. Supported self-management for people with type 2 diabetes: ameta-review of quantitative systematic reviews. Diabetes Endocrinol(2018) 8(12):1–11. doi: 10.1136/bmjopen-2018-024262
60. EUnetHTA Joint Action 3 WP4. (2018). Rapid assessment of other technologies using the HTA Core Model® for Rapid Relative Effectiveness Assessment. Continuous glucose monitoring (CGM real-time) and flash glucose monitoring (FGM) as personal, standalone systems in patients with diabetes mellitus treated with insulin. Project ID: OTJA08. Version 1.4, 27 July. Available at: https://eunethta.eu/wp-content/uploads/2018/07/OTJA08_CGM-real-time-and-FGM-aspersonal2c-standalone-systems-in-patients-with-diabetes-mellitus-treatedwith-insulin.pdf
61. Evidence Appraisal Report. (2018). Clinical and cost effectiveness of FreeStyle Libre flash glucose monitoring for the management of type 1 or type 2 diabetes. Available at: https://www.healthtechnology.wales/wp-content/uploads/2018/11/EAR004-FreeStyle-libre.pdf.
62. Ajjan RA, Jackson N, Thomson SA. Reduction in HbA1c using professional flash glucose monitoring in insulin-treated type 2 diabetes patients managed in primary and secondary care settings: A pilot, multicentre, randomised controlled trial. Diabetes Vasc Dis Res (2019) 16(4):385–95. doi: 10.1177/1479164119827456
63. Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kroger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. Lancet (London England) (2016) 388(10057):2254–63. doi: 10.1016/S0140-6736(16)31535-5
64. Ajjan RA. How can we realize the clinical benefits of continuous glucose monitoring? Diabetes Technol Ther (2017) 19(S2):S27–36. doi: 10.1089/dia.2017.0021
65. Rodbard D. Continuous Glucose Monitoring: A Review of Successes, Challenges, and Opportunities. Diabetes Technol Ther (2016) Suppl 2:S3–S13. doi: 10.1089/dia.2015.0417
66. Beck RW, Riddlesworth T, Ruedy K, Ahmann A, Bergenstal R, Haller S, et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Adults With Type 1 Diabetes Using Insulin Injections: The DIAMOND Randomized Clinical Trial. JAMA (2017) 317(4):371–8. doi: 10.1001/jama.2016.19975
Keywords: diabetes monitoring systems, diabetes, glucose control, systematic review, personalized approach
Citation: Kamusheva M, Tachkov K, Dimitrova M, Mitkova Z, García-Sáez G, Hernando ME, Goettsch W and Petrova G (2021) A Systematic Review of Collective Evidences Investigating the Effect of Diabetes Monitoring Systems and Their Application in Health Care. Front. Endocrinol. 12:636959. doi: 10.3389/fendo.2021.636959
Received: 02 December 2020; Accepted: 11 February 2021;
Published: 16 March 2021.
Edited by:
Charumathi Sabanayagam, Singapore Eye Research Institute (SERI), SingaporeCopyright © 2021 Kamusheva, Tachkov, Dimitrova, Mitkova, García-Sáez, Hernando, Goettsch and Petrova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Kamusheva, bWthbXVzaGV2YUBwaGFybWZhYy5tdS1zb2ZpYS5iZw==