 Théo Charnay1,2
Théo Charnay1,2 Gregory Mougel1,2
Gregory Mougel1,2 Cyril Amouroux3Iva Gueorguieva4
Cyril Amouroux3Iva Gueorguieva4 Florence Joubert5Morgane Pertuit2Rachel Reynaud1,6
Florence Joubert5Morgane Pertuit2Rachel Reynaud1,6 Anne Barlier1,2Thierry Brue1,7
Anne Barlier1,2Thierry Brue1,7 Alexandru Saveanu1,2*
Alexandru Saveanu1,2*- 1Institut National de la Santé et de la Recherche Médicale (INSERM) U1251, Marseille Medical Genetics (MMG), Institut Marseille Maladies Rares (MarMaRa), Aix-Marseille Université, Marseille, France
- 2Laboratory of Molecular Biology, Centre Hospitalier Universitaire Conception, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 3Paediatric Department, Endocrinology Unit, Arnaud de Villeneuve Hospital, Montpellier University Hospital, Montpellier, France
- 4Paediatric Department, Endocrinology Unit, Children’s Center, Jeanne-de-Flandre Hospital, Lille University Hospital, Lille, France
- 5Department of Pediatrics, Centre Hospitalier d’Avignon, Avignon, France
- 6Department of Multidisciplinary Peadiatrics, Centre de Référence des Maladies Rares d’origine hypophysaire HYPO, Hôpital Timone-Enfants, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
- 7Department of Endocrinology, Centre de Référence des Maladies Rares de l’hypophyse HYPO, Hôpital de la Conception, Assistance Publique-Hôpitaux de Marseille (AP-HM), Marseille, France
Isolated ACTH deficiency (IAD) is a life-threatening condition, particularly in the neonatal period, while a main consequence of undiagnosed isolated ACTH deficiency in survivors is cognitive impairment. TBX19 is involved in the differentiation and proliferation of corticotropic cells and TBX19 mutations are responsible for more than 60% of neonatal cases of IAD. We describe a new variant of the main TBX19 transcript (NM 005149.3, c.840del (p.(Glu280Asp fs*27)), classified as pathogenic, whose pathogenicity is assumed to be due to nonsense mediated decay leading to non-expression of T-box transcription factor TBX19. Moreover we summarize the TBX19 mutations published as individual cases since our last large cohort. Interestingly, this pathogenic variant was identified in four patients from three apparently unrelated families. Two of these families were consanguineous, and after investigations all of three were discovered to have roots in the same mountainous region of northern Morocco, suggesting a founder effect. Early diagnosis, timely treatment (hydrocortisone therapy) and preventive education allowed normal development, growth and quality of life in all patients.
1 Introduction
Isolated ACTH deficiency (IAD) is a rare cause of adrenocortical insufficiency, characterized by low ACTH and cortisol levels, which causes early and severe secondary adrenal insufficiency without other pituitary defects. Low cortisol manifests in the neonatal period as hypoglycemia, prolonged cholestatic jaundice, and seizures (1, 2), and families frequently have a history of neonatal death. Only a few cases of delayed diagnosis at up to 1 year of age have been reported. TBX19 mutations have been implicated in more than 60 percent of cases of neonatal IAD. As in other autosomal recessive diseases, incidence is much higher in consanguineous families. Since adrenal insufficiency is a life threatening condition, early detection of TBX19 mutations is crucial to ensure rapid management at birth and avoid neonatal mortality.
The TBX19 gene (formerly known as TPIT) codes for a T-box transcription factor found in proopiomelanocortin (POMC)-expressing pituitary cells (3). TBX19 is required for the terminal differentiation of these cells and the expression of the POMC gene. TBX19 is located on chromosome 1q24.2 and its main transcript is composed of 8 exons (NM 005149.3) (4).
Since the description in 2012 of a series of 91 IAD patients with 21 pathogenic variants (1), 13 other mutations have been described in patients with IAD, mostly as individual cases, and six further mutations have been reported in public databases (ClinVar, LOVD, HGMD) (5–16). TBX19 mutations are distributed across all exons other than exon 8 and all types of pathogenic variants have been described, including missense and truncating mutations (nonsense or indel frameshifts, larger deletions of one or several exons, or intronic mutations affecting splicing), in homozygous or compound heterozygous state.
We report four cases of IAD in three different families, all due to a new homozygous TBX19 mutation, c.840del (p.(Glu280Asp fs*27)). In two of the families, the patient’s parents were consanguineous. All parents were carriers of the c.840del mutation in heterozygous state, and despite living in different regions of France, they all came from the same small area in northern Morocco.
2 Subjects and methods
2.1 Subjects
Patients with isolated ACTH deficiency (IAD) were screened for TBX19 variants (RefSeq: NM 005149.3; OMIM 604614) in the context of GENHYPOPIT, a clinical research network created to investigate the genetic basis of congenital hypopituitarism (17, 18). Patients with a known postnatal cause of acquired IAD were excluded. Hormonal studies and intracranial imaging were performed in all patients in the respective hospitals. Pituitary and cerebral malformations were sought on MRI and recorded. Blood samples were collected from patients and, if possible, from first-degree relatives. Written informed consent was obtained from parents, caretakers, or guardians on behalf of children enrolled in the study. The study was approved by the ethics committee of the French Ministry of Health (Cellule de Bioéthique, Direction générale de la Recherche et de l’Innovation, approval n° DC 2019-3568) and by the French data protection authority (Commission Nationale Informatique et Libertés, CNIL 16 September 2016, N° 1991429 v 0).
2.2 Next-generation sequencing
Genomic DNA was extracted from blood lymphocytes (standard EDTA samples) using QiaSymphony DS DNA Midi kits (Qiagen, France). The 8 exons and 20 bp flanking introns of TBX19 were amplified using QIAseq Targeted DNA Custom Panels (Qiagen, France). Other genes involved either in ACTH deficiency associated with common immune variable deficit (David syndrome - NFKB2) or associated to other pituitary deficits in non-syndromic combined pituitary deficiency (17) provided the necessary diversity for the interpretation of SNV (single nucleotide variant) and CNV (copy number variants) data. The library was prepared according to manufacturer instructions. All samples were then sequenced using a MiseqDX device (Miseq V2 Reagent Kit, 300 cycles; Illumina®, San Diego, CA, USA). Sequencing data were exported and further analyzed (base calling, read filtering, alignment to the human genome (GRCH37/hg19) and annotated using CLC Genomic Workbench v6 (Qiagen, France). Variant calling analysis was verified using VariantStudio v3.0 (Illumina®, San Diego, CA, USA). Sequence coverage was deeper than 30× across all targeted regions. All variants of interest were visually inspected in the Integrative Genomics Viewer (“https://www.broadinstitute.org/igv”) to evaluate mapping and variant calling quality. Candidate variants were classified as pathogenic, likely pathogenic, variants of uncertain significance (VUS), likely benign, or benign according to ACMG (American College of Medical Genetics and Genomics) guidelines (19). Variants classified as pathogenic, likely pathogenic, or VUS were confirmed by Sanger sequencing using specific primers for each exon (4). Sequencing was performed on an ABI 3500xl DxGenetic Analyzer (Thermo Fisher Scientific).
3 Clinical presentation
3.1 Family 1
The index case was a boy born at term with neonatal hypoglycemia and axial hypotonia, both of which resolved spontaneously. The patient had no other severe clinical symptoms until 5 months of age, when he developed hypoglycemia associated with prolonged cholestatic jaundice. Endocrine investigations revealed cortisol and ACTH levels below laboratory detection thresholds (<27 nmol/and <1.1 pmol/L, respectively). The patient recovered rapidly after hydrocortisone treatment was started (2.5 mg, three times daily). Other pituitary hormone levels were normal for age, with the exception of TSH, which was initially above the normal range (16.79 mUI/L versus 0.73–8.35 mUI/L) but rapidly normalized. The anterior and posterior pituitary and the pituitary stalk were normal on MRI. Replacement therapy was continued with no severe infectious or episodes of acute adrenal insufficiency and normal growth (99th percentile) as of last follow-up, at 3 years of age.
Targeted NGS sequencing revealed a homozygous c.840del mutation in TBX19. The patient’s parents, who live in southeastern France but were born in Morocco, are first cousins. Both are heterozygous carriers of the mutation and have no signs of ACTH deficiency. They have two other healthy children (not investigated) and the mother reported two miscarriages in the first trimester of pregnancy.
3.2 Family 2
The index case was a boy who presented respiratory distress with pulmonary arterial hypertension within minutes of birth, requiring intubation for 3 days and then noninvasive ventilation for 11 days. The patient also had hemodynamic instability (treated by intravenous fluids and noradrenaline), severe hypoglycemia, prolonged cholestatic jaundice, and axial hypotonia. Brain MRI and EEG findings were normal.
The patient was admitted to the emergency department two months later for weakness and loss of appetite in the context of severe bronchiolitis. Laboratory tests showed severe hypoglycemia (0.2 g/L), hyponatremia and hyperkalemia. Hormone testing revealed cortisol and ACTH levels below laboratory detection thresholds (<3 nmol/L and <0.6 pmol/L, respectively) leading to a diagnosis of ACTH deficiency. Aldosterone and renin levels were within normal ranges. All investigated pituitary axes and free thyroid hormones were in the normal range. Hydrocortisone replacement therapy was initiated (15 mg/m2/day) and the patient’s clinical condition improved rapidly. Subsequent pituitary MRI showed a moderately hypoplastic anterior pituitary. Clinical examination and echocardiography revealed a bicuspid aortic valve. Hydrocortisone therapy was continued at 15 mg/m2/day (increased as appropriate in stress situations). As of last follow-up, at 5 years of age, the patient was in good health, with no other severe infections or episodes of adrenal insufficiency. The episodes of severe hypoglycemia and hyponatremia in infancy seem not to have affected psychomotor development.
Targeted NGS sequencing revealed a homozygous c.840del mutation in TBX19. The patient’s parents, who live in the south of France but were born in Morocco, are first cousins. Both are asymptomatic heterozygous carriers of the TBX19 mutation. No miscarriages were reported. They subsequently had a second child, who was also found to be a heterozygous carrier of the TBX19 variant, and is also asymptomatic.
3.3 Family 3
The index case was a full-term girl who had repeated episodes of hypoglycemia (0.10 g/L) after 8 h of life, associated with low plasma cortisol and ACTH levels (below laboratory detection thresholds; <27 nmol/L and <1.1 pmol/L, respectively). Daily oral hydrocortisone replacement therapy was initiated at 6 days of life. Other pituitary axes were found to be normal, apart from transiently low FT4 (13.7 pmol/L) at the lower end of the normal range for age (11 to 32 pmol/L), with normal TSH levels. Persistent ACTH deficiency was subsequently confirmed under normoglycemic conditions. Pituitary MRI at 18 days of life showed normal anterior and posterior lobes and a normal pituitary stalk. Higher quality MR images were obtained 6 years later, with the same findings. As of last follow-up, at 7 years of age, the patient had had three episodes of adrenal insufficiency with hypoglycemia and seizures in the context of infectious diseases.
Six years after the index case, a younger brother was born post-term with forceps delivery, an APGAR score of 2, neonatal hypotonia, feeding difficulties, and hyponatremia (130 mmol/L). He partially recovered for a few days in the intensive care unit but then developed a fever due to orchitis, treated surgically. Hormone tests at 10 days or age revealed cortisol and ACTH levels below laboratory detection thresholds (respectively <3 nmol/L and <1.7 pmol/L), while other pituitary hormone levels were normal, leading to a diagnosis of IAD. Hydrocortisone treatment was started (15 mg/m2/day) and the patient rapidly improved. Clinical examination revealed grade II mitral insufficiency and scaphocephaly. Hydrocortisone treatment was continued, and as of last follow-up one year later, the patient was in good health, with no complications.
Targeted NGS sequencing revealed a homozygous c.840del TBX19 mutation in both children. Their parents, who live in northern France, are apparently not consanguineous but both their families come from the same region in northern Morocco. As expected, both were found to be asymptomatic heterozygous carriers of the c.840del mutation. They have one other child (asymptomatic, not studied) and reported one miscarriage due to ectopic pregnancy.
4 Genomic data on the TBX19 mutation
The same molecular defect, a homozygous c.840del mutation, was identified by NGS in all four children with IAD, and all parents were heterozygous carriers (Figure 1). All the NGS results were confirmed by Sanger sequencing (heterozygous and homozygous example in Figure 2). The variant, which is not found in the general population gnomAD database (v2.1.1), is situated in exon 6 of the TBX19 gene, in the 3’ region. Only 3 of the 39 previously described pathogenic variants of the gene are situated in this region (Figure 3).
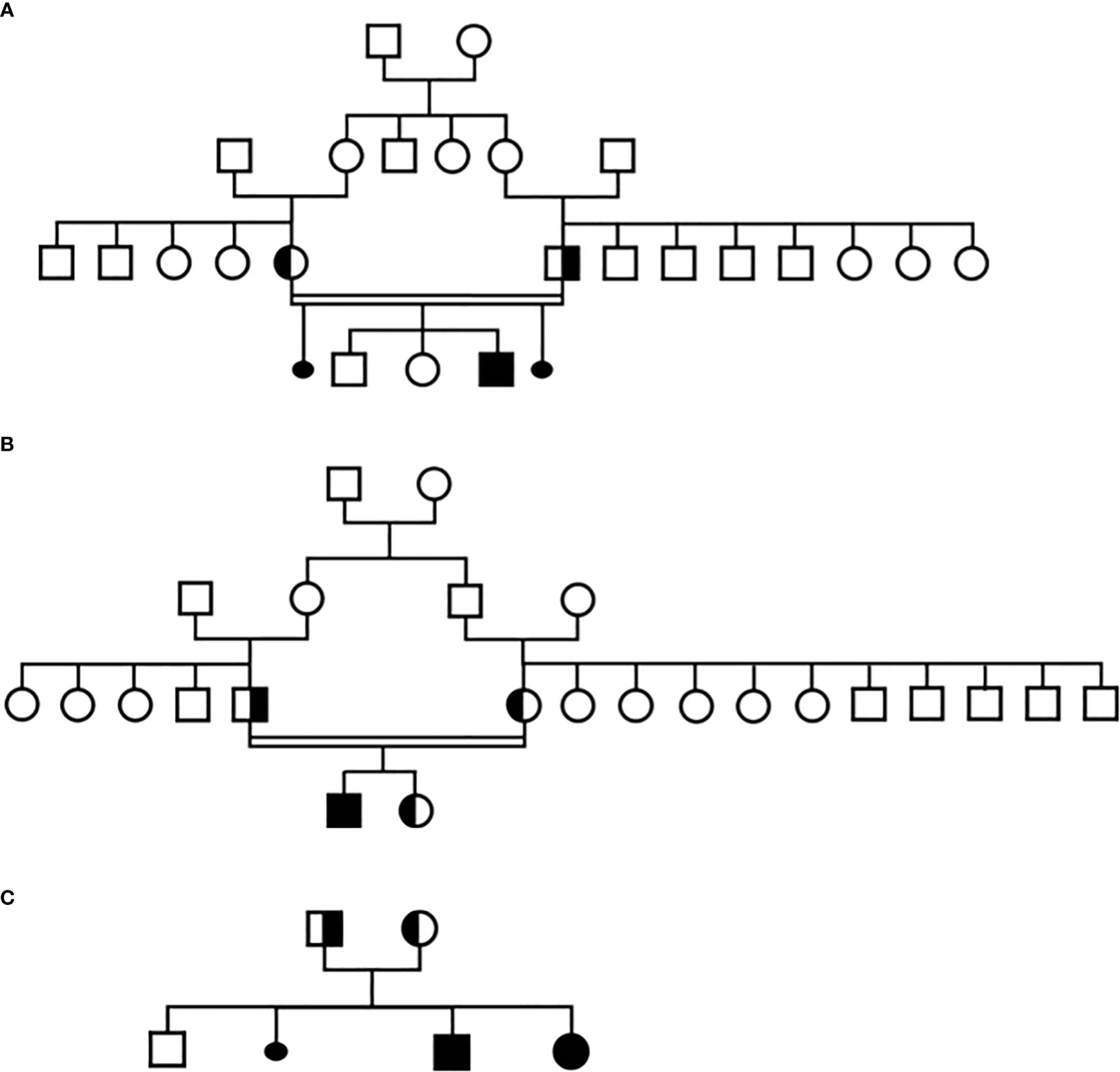
Figure 1 Pedigree of the three families in this study, (A) Family 1, (B) Family 2, (C) Family 3.
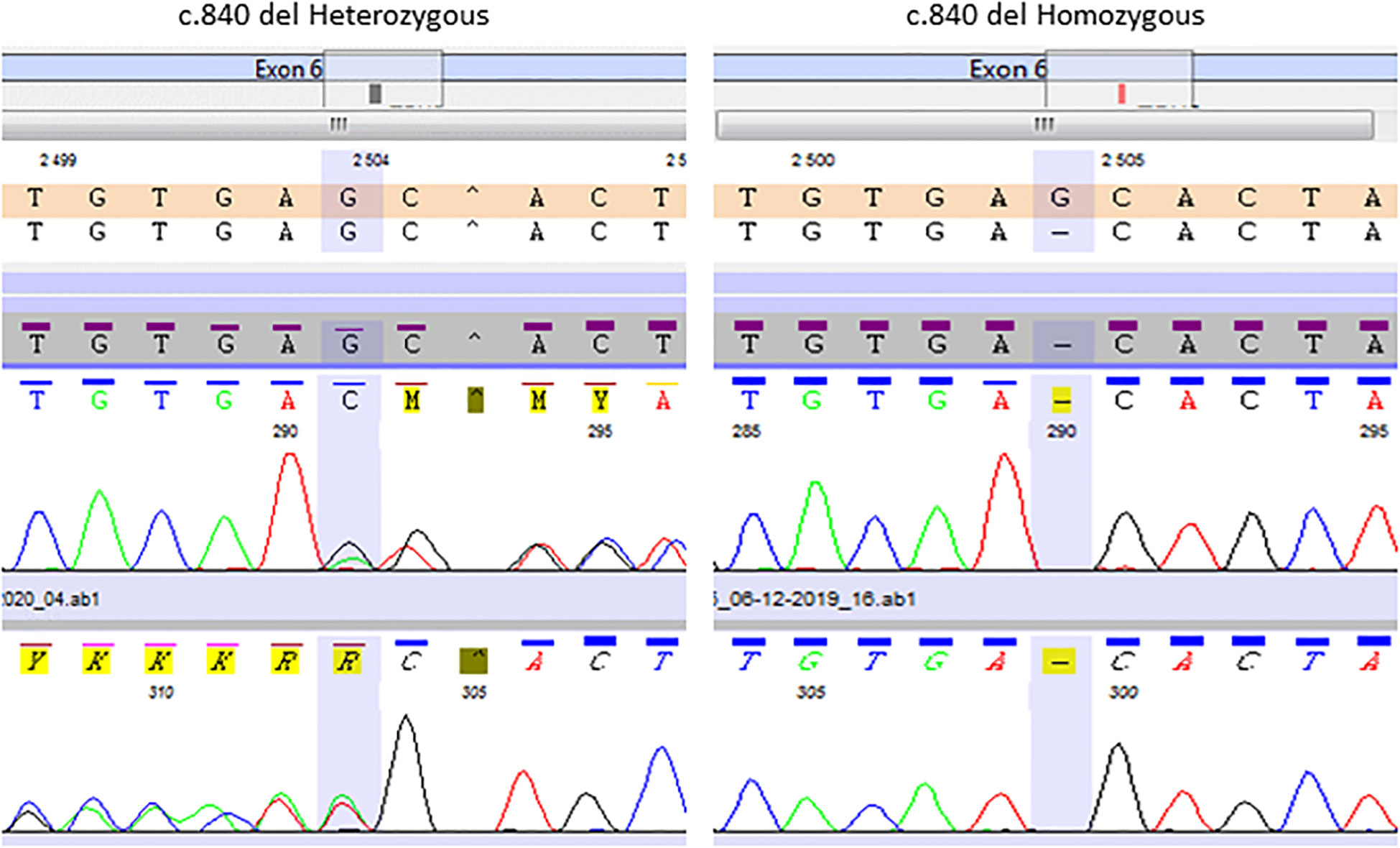
Figure 2 Representative Sanger chromatogram of the TBX19 c.840del homozygous patients and heterozygous relatives.
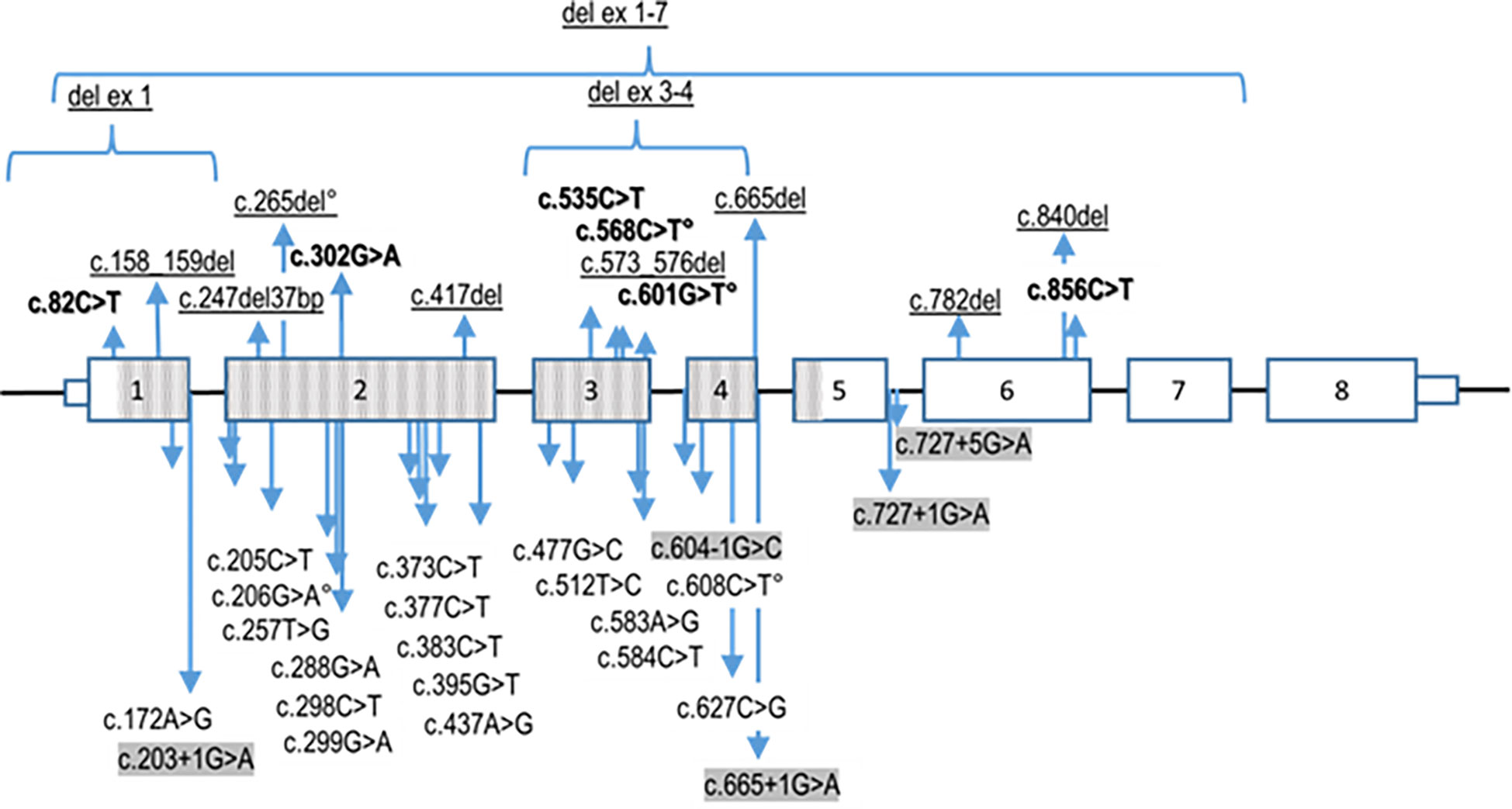
Figure 3 Summary of reported pathogenic TBX19 variants. The nonsense variants (in bold), deletions of exons and indels (frameshift) variants (underligned) are listed above the TBX19 gene schematic representation, whereas the missense and splice site (highlighted in grey) variants are presented underneath. Transcribed sequences are boxed. Small boxes indicate 5’- and 3’- untranslated regions. The bigger boxes represent the translated exons, while the hatched gray boxes indicates the region translated into the T-box protein domain. ° signals the variants reported on Clinvar without linked publication. Variants nomenclature is based on NM 005149.3 (MANE select) transcript.
The single-base deletion induces a frameshift with a premature nonsense codon, leading either to the synthesis of a truncated (so presumably nonfunctional) protein of 307 amino acids instead of 448 (p.(Glu280Asp fs*27)), or more probably, since the mutation is situated in exon 6 (out of 8), to nonsense- mediated decay and the complete absence of protein synthesis.
In terms of ACMG criteria, these observations—PVS1 (null variant in a gene where LOF is a known mechanism of IAD) plus PM2 (absent from controls in gnomAD V2.1.1 and dbSNP) plus PP4 (patient’s phenotype or family history is highly specific for a disease with a single genetic etiology, here, IAD) and/or PP1 (disease cosegregated with genotype)—classify the TBX19 variant as pathogenic.
5 Discussion
This article describes four cases of IAD (from three families) due to the same previously undescribed pathogenic variant of TBX19. Our investigation of these cases was initiated following the discovery within 2 years of the same TBX19 mutation associated with IAD in three different families with different names, from different regions of France. The link between these three families appeared after subsequent investigations. Suggestions of a common geographical origin from name research on genealogy websites were confirmed by patients when genetic testing results were delivered. All three families come from the same mountainous region of northern Morocco (Rif), strongly suggesting these cases are due to a founder effect.
Isolated adrenal deficiency was diagnosed in the neonatal period in two of the four children with this pathogenic TBX19 variant, and in the two others at 2 and 5 months of life. Early onset IAD, diagnosed before 1 year of life is a typical feature of TBX19 mutations (1). This point is noteworthy because four recently reported cases were diagnosed in older children, up to 5 years of age. However, the medical history of these patients (repeated hospitalizations and hydrocortisone treatment) suggests that IAD symptoms were already present before 1 year of age (5–7, 10).
Our patients’ phenotypes were very similar to those described for other TBX19 mutations (1). Three patients had hypoglycemia, and this was only avoided in the fourth by the timely initiation of parenteral nutrition in the intensive care unit before IAD was diagnosed. Two patients also had hyponatremia, prolonged cholestatic jaundice, and or hypotonia, and one patient had seizures. Symptoms improved rapidly in all patients after hydrocortisone treatment was started, and with close monitoring and appropriate treatment adjustments, each of these children has shown normal growth, apparently good quality of life, and no signs of psychomotor retardation, over follow-up periods ranging from 7 months to 6 years. One patient nevertheless had three episodes of acute adrenal insufficiency during infections, probably because of a lack of timely dose adjustment. Avoiding decompensation and repeated severe hypoglycemic or hyponatremic episodes is essential for the outcomes of these children, especially in the first years of life. Indeed, one of the main consequences of undiagnosed adrenal crises and inadequately adjusted hydrocortisone treatment in IAD due to TBX19 mutations is cognitive impairment (2, 4, 5, 20). Early diagnosis, close clinical monitoring in specialized centers and multiple therapeutic education sessions for parents are critical to avoid brain damage. The importance of parental education was highlighted in family 3, where better management of the second child led to clearly improved outcomes with fewer episodes of adrenal insufficiency.
No third trimester miscarriages or neonatal deaths were reported by these families, in contrast with previous studies in which they were reported in up to 25 percent of cases (1). However, two families reported first trimester miscarriages, including one due to ectopic pregnancy.
Since TBX19 is only expressed in the pituitary gland, TBX19 mutations are unlikely to lead to extrapituitary malformations. However, since autosomal recessive diseases are typically associated with consanguinity, other genetic defects cannot be excluded. Extrapituitary malformations, including a Chiari I malformation (1, 5) and microcephaly (5), have been reported in other cases of TBX19 mutation. One of our patients had scaphocephaly (1/4) and two had cardiac valve defects (a bicuspid aortic valve, mitral regurgitation). These malformations are relatively frequent [1–2% for bicuspid aortic valve for instance (21)], and are therefore unlikely to be directly linked to the TBX19 defect.
Our patients’ ACTH and cortisol levels were below laboratory thresholds in all cases, suggesting complete ACTH deficiency, as observed in the majority of previously described cases (1). The pituitary gland was considered normal on MRI in two of three patients and mildly hypoplastic in the third, in keeping with the results of a previous study in which all 11 investigated patients had normal pituitary MRI findings (1). Indeed, since TBX19 is only required for the differentiation and proliferation of corticotropic cells, which represent roughly 15% of all pituitary cells (22), pituitary volume should only be marginally affected in TBX19-deficient patients.
All four patients had the same homozygous c.840del truncating mutation in TBX19. Most (22/39) of the TBX19 gene variations described to date are truncating mutations, through various mechanisms (nonsense, frameshift, splice variants). It is noteworthy however, as shown in Figure 2, that almost all the described mutations (33/39) and all the missense mutations are located in the T box that encodes the DNA binding domain (1). The pathogenic variant reported here is only the sixth to have been found outside the T box domain, all of which are truncating mutations. The most frequently reported mutation (c.856C>T p.(Arg286*) (3, 7, 23), in line with our own experience (17), is located relatively close to the new c.840del mutation (p.Glu280Asp fs*27). Both mutations probably lead to an absence of protein expression through nonsense mediated decay (1, 4, 24).
The identification of a TBX19 mutation in several members of a relatively small ethnic group, with strong arguments in favor of a founder effect, is unique. The only other TBX19 mutation associated with a possible founder effect is the c.82C>T p.(Gln28Ter) mutation found almost exclusively in the Finnish population (43/45 of identified heterozygous individuals in gnomAD). Consanguinity increases the risk of autosomal recessive diseases and two of the three families in this study were consanguineous, in keeping with previous reports (5, 6, 20). Further studies are required to confirm the presence of a founder effect for the c.840del mutation and estimate the incidence of the variant in heterozygous state in the corresponding population.
For this purely autosomal recessive disease, the risk for heterozygous parents having a child with IAD is 25%. While measurement of estriol levels in pregnant women has been suggested as a means of diagnosing IAD before birth (22), prenatal diagnosis is not commonly used and access to a pediatric intensive care unit at birth is crucial in families with a history of IAD, to ensure optimal neonatal management.
6 Conclusion
In conclusion, we describe a new TBX19 truncating mutation, identified in four children from three seemingly unrelated families and causing early onset IAD, a life-threatening neonatal condition. Our results highlight the importance of early diagnosis and treatment based on the observation of characteristic clinical signs, hypoglycemia and prolonged jaundice, sometimes appearing a few hours after birth and associated with complete IAD and normal pituitary MRI findings. Early diagnosis, timely treatment and preventive education allowed normal development, growth and quality of life in all four patients.
Data availability statement
The data presented in the study are deposited in the ENA repository, accession number PRJEB59437.
Ethics statement
The studies involving human participants were reviewed and approved by French Ministry of Health (Cellule de Bioe´thique, Direction generale de la Recherche et de l’Innovation, approval n° DC 2019-3568) and by the French data protection authority(Commission Nationale Informatique et Liberte´s, CNIL 16 September 2016, N° 1991429 v 0). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributions
TC and AS analyzed the data, identified the pathogenic variant, and wrote the paper. AS and TB led the project and reviewed the manuscript. GM designed the primers and reviewed the manuscript. MP performed the technical NGS work. AB supervised NGS sequencing. RR, AC, IG, and FJ were the patients’ attending physicians, recorded their symptoms, medical history, and origin, and performed follow-up.
Funding
This work was supported by the “Association pour le développement des recherches biologiques et médicales” (ADEREM).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Couture C, Saveanu A, Barlier A, Carel JC, Fassnacht M, Flu¨ck CE, et al. Phenotypic homogeneity and genotypic variability in a large series of congenital isolated ACTH-deficiency patients with TPIT gene mutations. J Clin Endocrinol Metab (2012) 97:E486–495. doi: 10.1210/jc.2011-1659
2. Vallette-Kasic S, Brue T, Pulichino A-M, Gueydan M, Barlier A, David M, et al. Congenital isolated adrenocorticotropin deficiency: an underestimated cause of neonatal death, explained by TPIT gene mutations. J Clin Endocrinol Metab (2005) 90:1323–31. doi: 10.1210/jc.2004-1300
3. Lamolet B, Pulichino AM, Lamonerie T, Gauthier Y, Brue T, Enjalbert A, et al. A pituitary cell-restricted T box factor, tpit, activates POMC transcription in cooperation with pitx homeoproteins. Cell (2001) 104:849–59. doi: 10.1016/s0092-8674(01)00282-3
4. Pulichino A-M, Vallette-Kasic S, Couture C, Gauthier Y, Brue T, David M, et al. Human and mouse TPIT gene mutations cause early onset pituitary ACTHdeficiency. Genes Dev (2003) 17:711–6. doi: 10.1101/gad.1065603
5. Kardelen Al AD, Poyrazog˘lu S¸, Aslanger A, Yes¸il G, Ceylaner S, Bas¸ F, et al. A rare cause of adrenal insufficiency – isolated ACTH deficiency due to TBX19 mutation: Long-term follow-up of two cases and review of the literature. Horm Res Paediatr (2019) 92:395–403. doi: 10.1159/000506740
6. Abali ZY, Yesil G, Kirkgoz T, Kaygusuz SB, Eltan M, Turan S, et al. Evaluation of growth and puberty in a child with a novel TBX19 gene mutation and review of the literature. Hormones (Athens) (2019) 18:229–36. doi: 10.1007/s42000-019-00096-7
7. Akcan N, Serakıncı N, Turkgenc B, Bundak R, Bahceciler N, Temel SG. A novel TBX19 gene mutation in a case of congenital isolated adrenocorticotropic hormone deficiency presenting with recurrent respiratory tract infections. Front Endocrinol (Lausanne) (2017) 8:64. doi: 10.3389/fendo.2017.00064
8. Metherell LA, Savage MO, Dattani M, Walker J, Clayton PE, Farooqi IS, et al. TPIT mutations are associated with early-onset, but not late-onset isolated ACTH deficiency. Eur J Endocrinol (2004) 151:463–5. doi: 10.1530/eje.0.1510463
9. Alsaleem M, Saadeh L, Misra A, Madani S. Neonatal isolated ACTH deficiency (IAD): a potentially life-threatening but treatable cause of neonatal cholestasis. BMJ Case Rep (2016) 2016:bcr2016215032. doi: 10.1136/bcr-2016-215032
10. Weijing K, Liping Z, Tiantian Z, Pei Z, Yan M. A case of congenital isolated adrenocorticotropic hormone deficiency caused by two novel mutations in the TBX19 gene. Front Endocrinol (Lausanne) (2019) 10:251. doi: 10.3389/fendo.2019.00251
11. Peng C, Sun G, Tang Z, Hou X. Congenital isolated ACTH deficiency caused by TBX19 gene mutation: A family report. Front Pediatr (2019) 7:546. doi: 10.3389/fped.2019.00546
12. Al-Shamsi A, Hertecant JL, Souid A-K, Al-Jasmi FA. Whole exome sequencing diagnosis of inborn errors of metabolism and other disorders in united Arab Emirates. Orphanet J Rare Dis (2016) 11:94. doi: 10.1186/s13023-016-0474-3
13. Mueller OT, Coovadia A. Gene symbol: TBX19. disease: ACTH deficiency, isolated? Hum Genet (2008) 123:538.
14. Yang Y, Muzny DM, Xia F, Niu Z, Person R, Ding Y, et al. Molecular findings among patients referred for clinical whole-exome sequencing. JAMA (2014) 312:1870–9. doi: 10.1001/jama.2014.14601
15. Maudhoo A, Maharaj A, Buonocore F, Martos-Moreno GA, Argente J, Achermann JC, et al. Missplicing due to a synonymous, T96= exonic substitution in the T-box transcription factor TBX19 resulting in isolated ACTH deficiency. Endocrinol Diabetes Metab Case Rep (2021) 2021:EDM21–0128. doi: 10.1530/EDM-21-0128
16. Wu S, Chen Q, Shen L, Wei H, Chen Y. [Analysis of TBX19 gene variant in a child with congenital isolated adrenocorticotropic hormone deficiency]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi (2021) 38:59–62. doi: 10.3760/cma.j.cn511374-20191107-00563
17. Jullien N, Saveanu A, Vergier J, Marquant E, Quentien MH, Castinetti F, et al. Clinical lessons learned in constitutional hypopituitarism from two decades of experience in a large international cohort. Clin Endocrinol (Oxf) (2021) 94:277–89. doi: 10.1111/cen.14355
18. Reynaud R, Gueydan M, Saveanu A, Vallette-Kasic S, Enjalbert A, Brue T, et al. Genetic screening of combined pituitary hormone deficiency: experience in 195 patients. J Clin Endocrinol Metab (2006) 91:3329–36. doi: 10.1210/jc.2005-2173
19. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American college of medical genetics and genomics and the association for molecular pathology. Genet Med (2015) 17:405–24. doi: 10.1038/gim.2015.30
20. Unal E, Yıldırım R, Tas¸ FF, Tekin S, Sen A, Haspolat YK. A rare cause of neonatal hypoglycemia in two siblings: TBX19 gene mutation. Hormones (Athens) (2018) 17:269–73. doi: 10.1007/s42000-018-0028-2
21. Cripe L, Andelfinger G, Martin LJ, Shooner K, Benson DW. Bicuspid aortic valve is heritable. J Am 294 Coll Cardiol (2004) 44:138–43. doi: 10.1016/j.jacc.2004.03.050
22. Weintrob N, Drouin J, Vallette-Kasic S, Taub E, Marom D, Lebenthal Y, et al. Low estriol levels in the maternal triple-marker screen as a predictor of isolated adrenocorticotropic hormone deficiency caused by a new mutation in the TPIT gene. Pediatrics (2006) 117:e322–327. doi: 10.1542/peds.2005-1973
23. Xiong HY, Alipanahi B, Lee LJ, Bretschneider H, Merico D, Yuen RKC, et al. RNA Splicing. the human splicing code reveals new insights into the genetic determinants of disease. Science (2015) 347:1254806. doi: 10.1126/science.1254806
Keywords: isolated ACTH deficiency, low ACTH and cortisol, adrenal insufficiency, TBX19, TPIT, recessive disorder, founder effect
Citation: Charnay T, Mougel G, Amouroux C, Gueorguieva I, Joubert F, Pertuit M, Reynaud R, Barlier A, Brue T and Saveanu A (2023) A novel TBX19 gene mutation in patients with isolated ACTH deficiency from distinct families with a common geographical origin. Front. Endocrinol. 13:1080649. doi: 10.3389/fendo.2022.1080649
Received: 26 October 2022; Accepted: 28 December 2022;
Published: 15 February 2023.
Edited by:
Rosario Pivonello, University of Naples Federico II, ItalyReviewed by:
Sumita Danda, Christian Medical College and Hospital, IndiaLeonard Cheung, University of Michigan, United States
Copyright © 2023 Charnay, Mougel, Amouroux, Gueorguieva, Joubert, Pertuit, Reynaud, Barlier, Brue and Saveanu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandru Saveanu, QWxleGFuZHJ1LnNhdmVhbnVAYXAtaG0uZnI=