 Giulia Sapuppo1*†‡
Giulia Sapuppo1*†‡ Maria Ausilia Giusti1†Demetrio Aricò2Romilda Masucci3
Maria Ausilia Giusti1†Demetrio Aricò2Romilda Masucci3 Martina Tavarelli1
Martina Tavarelli1 Marco Russo1
Marco Russo1 Gabriella Pellegriti1,4
Gabriella Pellegriti1,4- 1Department of Clinical and Experimental Medicine, University of Catania, Garibaldi-Nesima Medical Center, Catania, Italy
- 2Department of Nuclear Medicine, Humanitas Oncological Centre of Catania, Catania, Italy
- 3Clinical and Diagnostic Center, Giovan Battista (G.B.) Morgagni, Catania, Italy
- 4Department of Clinical and Experimental Medicine, University of Catania, Catania, Italy
Introduction: Parathyromatosis is a rare cause of primitive hyperparathyroidism characterized by the presence of numerous parathyroid tissue foci in the neck/mediastinum, due to hyperplasia of parathyroid embryologic residues (primary-form) or to local parathyroid tissue implantation (secondary-form). 63 cases have been described in the literature. In our patient parathyromatosis was due to a combination of two mutations.
Case report: A 36-years-old woman was diagnosed with osteoporosis secondary to primary hyperparathyroidism. Subsequent right parathyroidectomy showed a parathyroid adenoma. The follow-up was negative but after 10 years she had a relapse. The genetic screening showed a rare intronic mutation of the MEN1 gene and a heterozygous mutation never described in exon 8 of the CASR gene, coding for the calcium receptor. Calcemia and PTH increased over the years with the onset of nephrocalcinosis and the worsening of osteoporosis despite the therapy with Cinacalcet, bisphosphonates and Vitamin D. She had therefore two additional surgical procedures (parathyroid tissue without malignancy). At follow-up she showed elevated levels of PTH (>1000 pg/ml) and calcium (11.2 mg/dl) and CT scans multiple subcentimetric nodules in the neck/upper mediastinum. Since the 68Ga-DOTATATE showed an increased uptake in the neck/mediastinum, lanreotide was added. After two months there was a significant biochemical response but, unfortunately, after six months, the patient showed a new worsening.
Conclusions: a rare case of parathyromatosis due to a combination of two genetic alterations never described. The main issues concern the diagnosis and the radical treatment. Somatostatin analogues may have a useful role in both diagnosis and therapy.
Introduction
Hyperparathyroidism (HPT) is a rare condition characterized by excessive secretion of PTH. It may be the result of: 1) autonomous secretion of PTH by parathyroid glands (primary hyperparathyroidism, PHPT); 2) excessive secretion of hormone as a consequence of chronic hypocalcemia in patients with chronic renal failure (secondary hyperparathyroidism, SHPT); 3) functional autonomy of parathyroid glands occurs during a long-lasting secondary hyperparathyroidism (tertiary hyperparathyroidism, THPT) (1, 2). PHPT is currently the most common cause of hypercalcemia. PHPT is more frequent in in the postmenopausal years with women/men ratio of 4:1. In Europe, the prevalence is 1.07% (1, 3).
About 90% of all cases are sporadic and 10% are part of a hereditary syndrome, mainly multiple endocrine neoplasia syndromes (MEN-1, MEN-2,MEN-4),hyperparathyroidism-jaw tumor syndrome (HPT-JT), familial hypocalciuric hypercalcemia (FHH-1, FHH-2, FHH-3), familial hypercalciuric hypercalcemia and isolated familial HPT. Hereditary syndromes are characterized by a multiglandular disorder which are asynchronous; the diagnosis is usually defined at early age, generally at the age of 50 years old (1, 4). Almost all patients with PHPT have benign tumors, typical or atypical adenomas (85% of cases) or hyperplasia or multiple abnormal parathyroid glands (15% of cases)). In only 4% of patients are identified Less common causes double adenomas; a very rare cause (<1%) is a parathyroid carcinoma. the only curative treatment for PHPT is the complete surgical resection of abnormal “hyperfunctioning” tissue. The dosage of PTH intraoperatively is of fundamental relevance confirming the completeness in the removal hyperfunctioning tissue. In only 5% of patients a second surgery is needed. It’s necessary to distinguish: persistent hyperparathyroidism (development of high calcium and PTH values within 6 months of parathyroidectomy for incomplete resection) and recurrent hyperparathyroidism (development of high calcium and PTH values after 6 months of eucalcemia). The most frequent causes of recurrent hyperparathyroidism are: parathyroid adenoma (typical/atypical, single/double), parathyroid carcinoma and a very rare condition known as parathyromatosis, due to benign hyperfunctioning parathyroid tissue scattered in the neck and/or superior mediastinum. Two forms can be distinguished: 1)from hyperplasia of parathyroid during embryologic development (primary form, without previous surgery); 2) from tissue spillage during parathyroidectomy and implantation (secondary form) Primary parathyromatosis may occur in patients with multiple endocrine neoplasia (usually MEN-1), due to parathyroid hyperplasia of embryological residues. The development of scattered rests of benign parathyroid cells can be favored by genetic mutations. The secondary form is more frequent in patients with chronic renal and in patient with hereditary syndromes. To date only 63 cases have been described in literature. In our patient parathyromatosis was due to a combination of genetic alterations (MEN1 gene and CASR gene) never described in the literature. Being a rare syndrome the challenges concern not only the management but also the diagnosis. The main differential diagnosis is parathyroid carcinoma. The intraoperative findings and the histopathologic features are important for making the appropriate diagnosis. Parathyromatosis has high failure rates both with medical and surgical management. Bisphosphonates and cinacalcet therapies are of little benefit and patients often remain symptomatic (5–7). In literature there are some case reports where the addition of denosumab, a humanized monoclonal antibody which inhibits receptor activator of nuclear factor κ-B ligand, can be effective in the treatment of refractory hypercalcemia in parathyroid cancer and in the setting of benign hyperparathyroid-related hypercalcemia such as parathyromatosis (8–10). In patients with MEN1 syndrome, parathyroid tumors (hyperplasia or single or multiple adenomas of the parathyroid glands) express somatostatin receptors (SST) on their cell surface, which can be targeted by somatostatin analogs for tumor localization (68Ga-DOTATATE positrion-emission tomography/computed tomography) and therapy. Somatostatin analogues (SSA) control hormone excess and block tumor growth in several type of neuroendocrine tumors (NET). In MEN1 patients SSA are for duodeno-pancreatic NET and pituitary adenomas. Data on the effects of SSA in PHPT are discordant (11, 12).
Case report
A 52-years-old woman, who had at 36 years old a diagnosis of osteoporosis secondary to primary hyperparathyroidism, underwent surgery with the removal of inferior right parathyroid gland. On histology it was a parathyroid adenoma. She had a family history of osteoporosis and renal stones (mother). After this, she has been followed by an endocrine specialist with referred normal PTH and calcium value. After 10 years she had a recurrence of hyperparathyroidism with PTH 504 pg/ml (12-65), calcium 11,9 mg/dl (8,8–10,6) and phosphorus 1,1 mg/dl (2,5–4,5). The Tc99MIBI scan revealed two foci of increased uptake in the lower pole of the right thyroid lobe and paratracheal left region. Therefore she was referred to our hospital, where she was screened for MEN1, MEN2A and familial benign hypocalciuric hypercalcemia (FHH) because of the youth at diagnosis of osteoporosis. She was on bisphosphonates and vitamin D supplements. Urinary calcium/24h was 148 (50-400), phosphaturia/24h 448 (330-1200), chromogranin A 8 (2-18); negative urinary catecholamine; gastrin 30 (28-185), calcitonin 2 (<11.5), prolactin 7.9 (1.9-25). Genetic screening was done for: FHH heterozygous in exon 8 of the CASR gene of the sequence variant c.2549C>G p.Ala850Gly; MEN1: no evidence of known pathogenetic variants and no genomic rearrangements, in intron 4 variant c.655-6C>A in heterozygosis. HPT-JT: in the CDC73 gene no recognized variants were highlighted as pathogenic (see Table 1). Serum calcium and PTH increased in the following years (Ca 10,8 –11,8 and 12 mg/dl and PTH 732–1413 and 1753 pg/ml), with the onset of nephrocalcinosis. Cinacalcet 30 mg was prescribed and, after Tc99MIBI scan and ultrasound, she underwent again surgery with evidence of two adenoma of left and right parathyroid gland. During the operation PTH was monitored with a reduction > 50% after 15-20 minutes from the removal of abnormal tissue but after a month PTH value was 647 pg/ml, serum calcium dropped to 9,3 mg/dl and phosphorus 1,1 md/dl. After three months an ultrasound showed a nodule behind the right thyroid lobe and a PTH-wash was done (> 3278 pg/ml). There was a worsening in the bone mineral density (L1-L4 spine T-score of -3) and hydronephrosis of the right kidney. Serum calcium was 12,8 mg/dl, phosphorus 1,3 mg/dl and PTH 1121 pg/ml, Vitamin D 11,7 ng/ml. She was in therapy with cinacalcet 60 mg/die and vitamin D supplements. On the CT scan, multiple subcentimetric hypervascularized lesions were noted behind the right thyroid lobe and scattered throughout the superior mediastinum, ascribed to parathyroid glands.
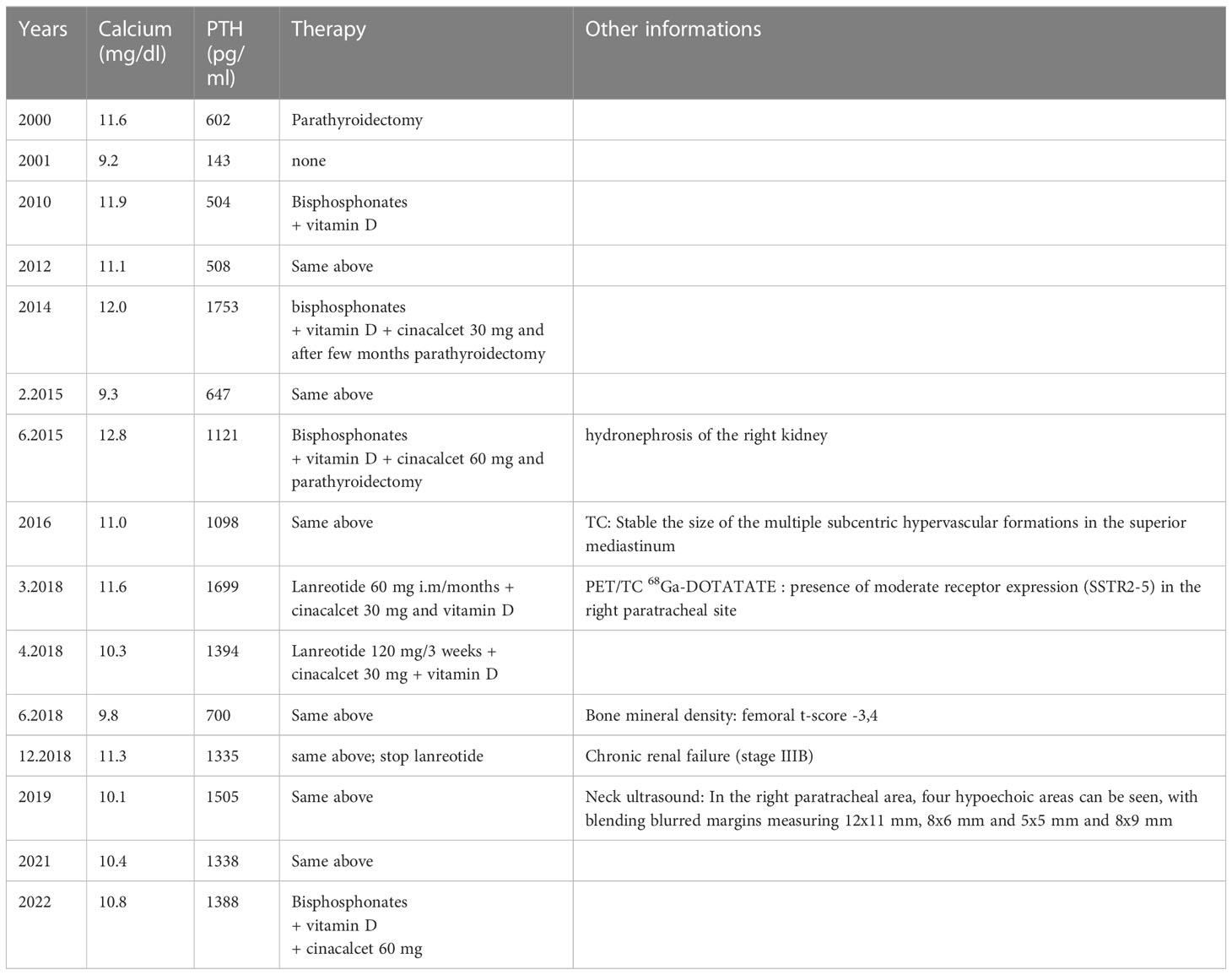
Table 1 Calcium and PTH values, therapy and other informations throughout the years.
She underwent further surgery with thyroidectomy, on histology were multiple iperplastic parathyroid tissue between the muscle (see Figure 1). After a month, PTH was 1251 pg/ml with low levels of vitamin D (3 ng/ml). On the Tc99MIBI scan, there was a recurrence of parathyroid tissue on para-jugular right side. At subsequent follow-up visit PTH was 1098 pg/ml, Vitamin D 15 ng/ml, calcium 11 mg/dl, phosphorus 1.1 mg/dl; albumin 4.5 g/dl, calcitonin 0.5 pg/ml, creatinine 1.2 mg/dl on treatment with Cinacelcet 30 mg twice daily and Vitamin D3 25000 every 15 days. For hydronephrosis an ureteral stent was implanted and to date it is still in follow-up for the deterioration of the right kidney function. The 68Ga-DOTATATE PET/CT scan showed an increased uptake in the neck and in the upper mediastinum (Figure 1). Lanreotide therapy was given at a dose of 60 mg i.m./4 weeks in addition to cinacalcet 30 mg and vitamin D 25000 UI every 15 days. After two months PTH was 700 pg/ml, calcium 9.8 mg/dl and phosphorus 3 mg/dl.
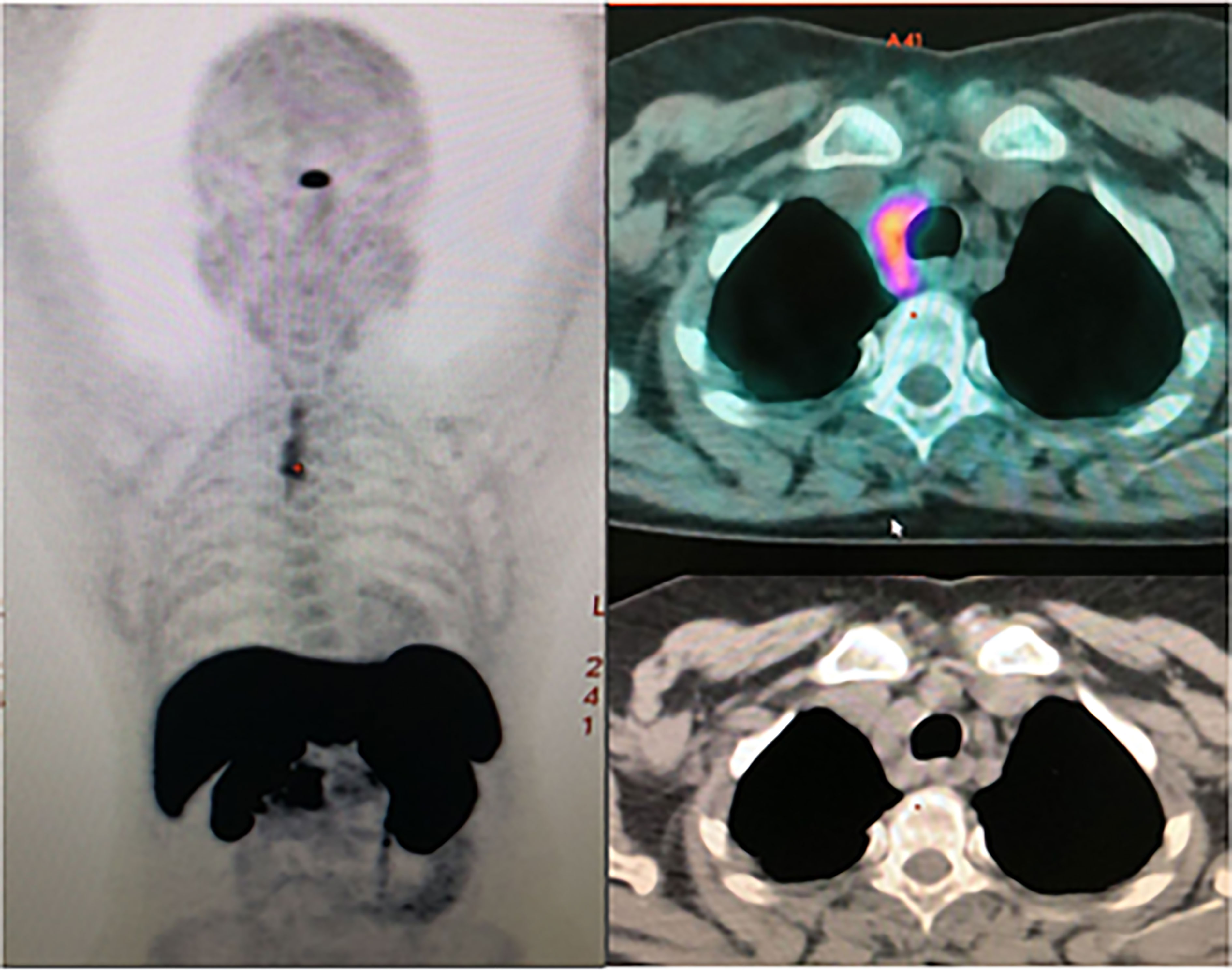
Figure 1 68Ga-DOTATATE PET/CT scan: evidence of extended uptake in the neck in then upper mediastinum.
Unfortunately, after about 6 months, the patient showed a new worsening of the clinical and biochemical parameters.
In Figure 2 the trend of calcium and PTH values and their respective therapies are shown. Furthermore a table shows Calcium and PTH values, therapy and other information throughout the years.
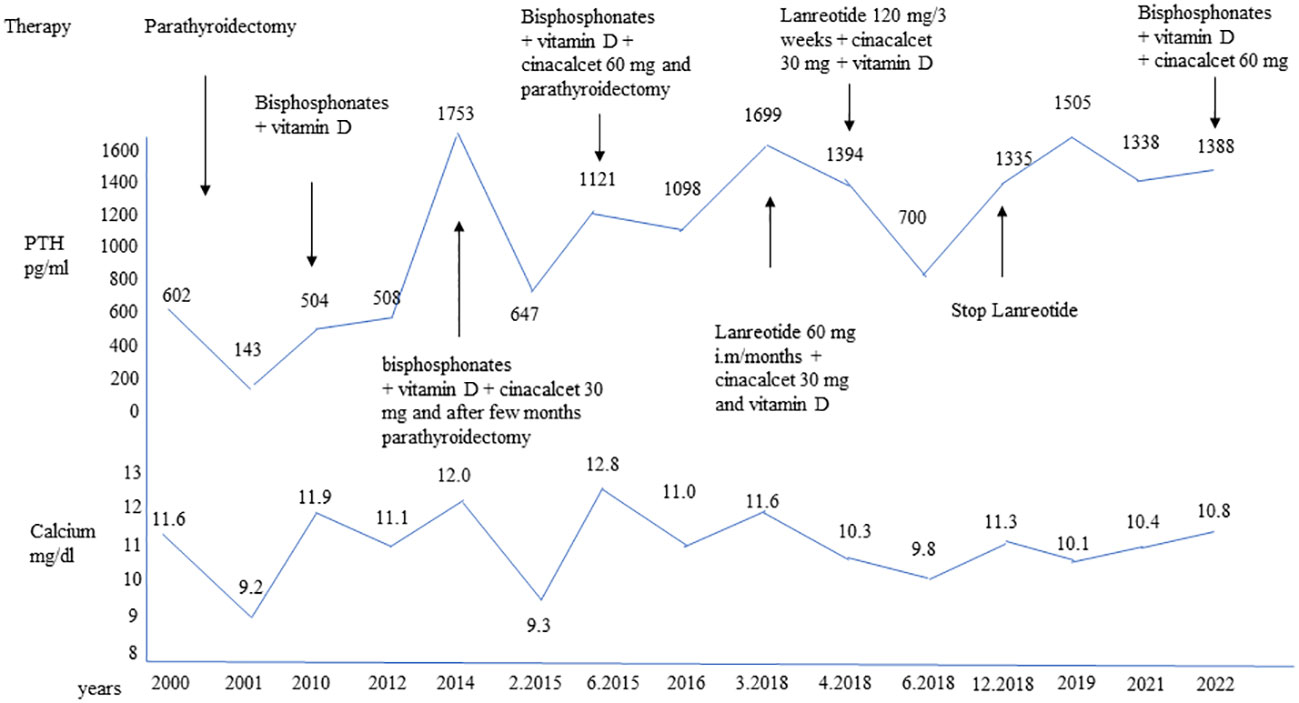
Figure 2 Trend of calcium and PHT values and their respective therapies.
Discussion
Parathyromatosis is defined as multiple nodules of benign hyperfunctioning parathyroid tissue scattered in the neck and superior mediastinum, resulting in recurrent or persistent hyperparathyroidism (5, 7). The first case of parathyromatosis was described by Palmer et al. parathyromatosis in 1975 in a series of 250 patients with recurrence after parathyroidectomies (13). After 2 years, Reddick classified parathyromatosis as a disease entity (14). Sporadic case reports and small series were described in the literature (overall 63 cases). The most common form of parathyromatosis is the second one in patient with previous neck surgery. The spilling of parathyroid tissue in the neck and/or mediastinum during surgery for adenoma or hyperplastic tissue can lead to a hyperplasia of these tissue implants (mainly due tohypocalcemia, hypophosphatemia and hypovitaminosis D for chronic renal failure). The primary form due to embryonic parathyroid residues is less common. Patients with multiple endocrine neoplasia (usually MEN-1) can develop the primary form of parathyromatosis. Genetic mutations could favor the development of scattered rests of benign parathyroid cells. The secondary form is more frequent in patients with chronic renal and in patient with hereditary syndromes (15). Symptoms include fatigue, weakness, polydipsia and polyuria, bone and back pain, constipation, mood disorders, loss of appetite with weight loss and bone fracture. Clinically, moderate hypercalcemia(usually less than 14 mg/dl) is present. Serum PTH levels decrease after surgery and then increase again. Hypophosphatemia and high alkaline phophatase value may be present. The diagnosis should be suspected if previous parathyroid surgeries and/or recurrent/persistent high PTH levels (5).Hage et al. (16) showed how the initial diagnosis of benign parathyroid lesion leads to repeat surgeries for hyperplasia, adenoma or ectopic parathyroid tissue. Multiple local recurrences after parathyroidectomy could lead to suspect the diagnosis of parathyroid carcinoma, so pathological distinction is crucial for treatment. During surgery, in parathyromatosis multiple small grey nodules are typical, instead in the parathyroid carcinoma as a solitary large hard white nodule with infiltrative borders is more frequent. In both cases adherent fibrous tissue is present. Histological features associated with malignancy are: capsular and/or vascular invasion, 5/10 HPF mitoses, tumor necrosis, cellular atypia, trabecular growth pattern andintratumoral fibrosis. However, these histological features don’t absolutely distinguish the two conditions. Use of some immunohistochemical markers (the overexpression of galectin-3 and the loss of parafibromin and Rb), could be used for distinction of benignant of malignant form. Instead the difference between parathyromatosis and parathyroid adenoma is the lack of the classical features and the encapsulation (5, 6). Parathyromatosis’s management remains challenging. The aim of surgery is the removal of all the disseminated nodules but unfortunately it is in almost all of cases unsuccessful so medical management is crucial. Vitamin D therapy leads to PTH level and bone turnover reduction. Cinacalcet, an oral calciomimetic that decrease PTH secretion binding calcium sensing receptor, has been used with success mainly in chronic renal failure patients. Another group of drug with contrastant and often inconsistent results in primary hyperparathyroidism are the bisphosphonates (17). Since our patient had a gene mutation associated with MEN 1, we performed a 68Ga-DOTATATE PET/CT scan to see if parathyroid cells express somatostatin receptors (11). Having obtained a good response to 68Ga-DOTATATE positron-emission tomography/computed tomography, we started the somatostatin analogue therapy (SSA) (Lanreotide 120 mg, i.m. every 4 weeks). After two months of therapy, PTH and calcium levels decreased but did not normalize. Several studies in literature reported the use of somatostatin analogs in the treatment of primitive hyperparapathyroidism in patients with MEN 1 with conflicting results. SSA are used in gastroentero- pancreatic neuroendocrine tumors and/or pituitary adenomas, because they express SST receptors. Also parathyroid adenomas are included in the NET; in fact in patients with MEN1, they showed a common pathogenic origin with gastro-entero-pancreatic NET and pituitary adenomas. A study by Faggiano et al. showed the potential utility of long-acting somatostatin analogues in hyperparathyroidism in patients with MEN-1 (12). In fact, during a 6 month therapy with depot somatostatin analogue, serum PTH, calcium and phosphorus values, urine calcium excretion and phosphorus renal reabsorption resulted stably improved Octreotide could lead to an improvement of calcium and phosphorus values through direct effects on PTH hypersecretion, due to SST expression on parathyroid cells.
Review of literature
To our knowledge 63 cases of parathyromatosis have previously been described (Table 2).
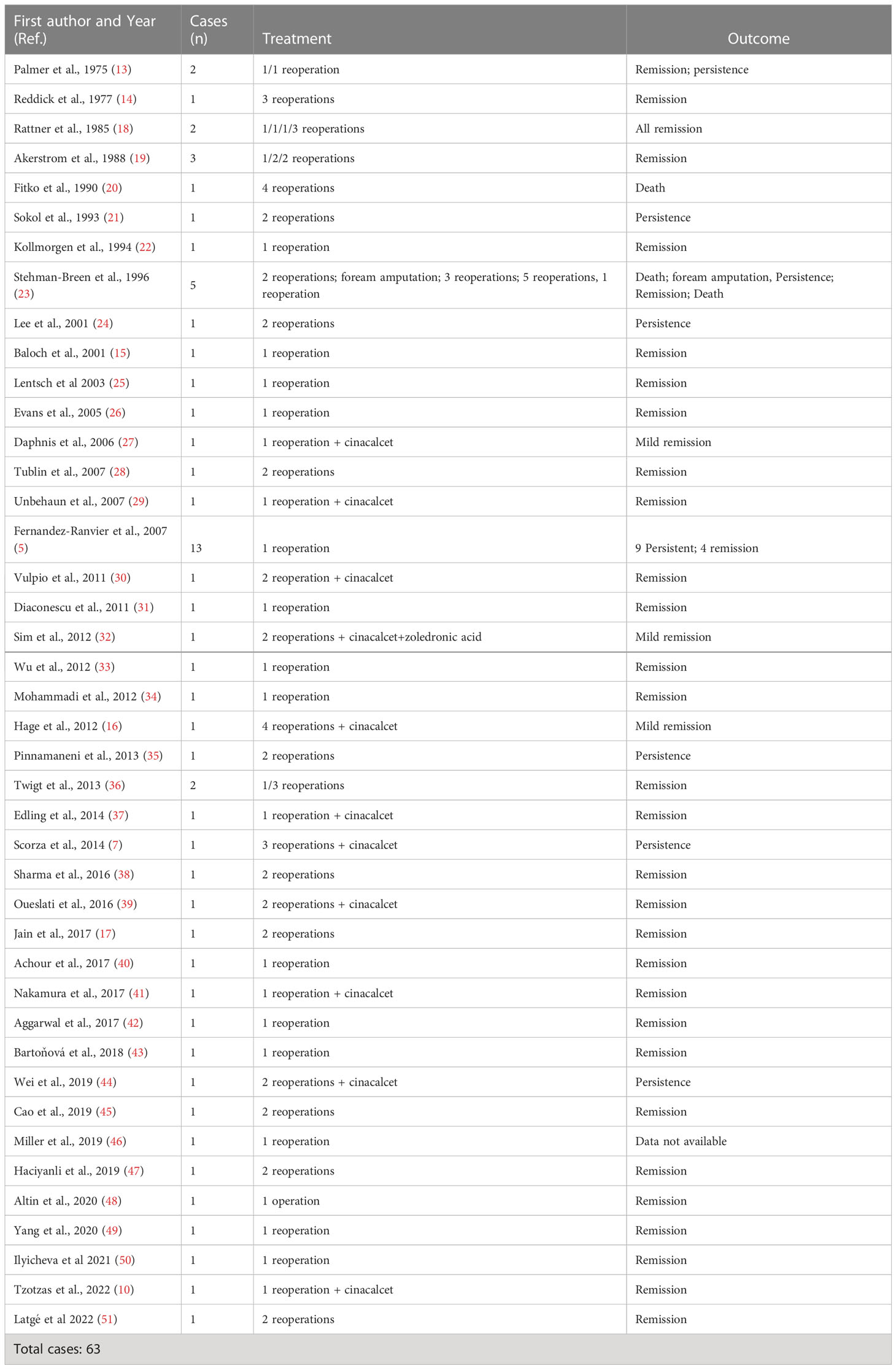
Table 2 Parathyromatosis: review of literature.
In most cases in the literature (42 cases) the disease went into remission. In 16 cases, however, parathyromatosis remained persistent and in 3 cases it led to death from complications related to hyperparathyroidism.
In 9 cases, cinacalcet was used in addition to surgical treatment. In 2 of these cases the disease remained in the persistent form.
Conclusion
Parathyromatosis is a rare cause of recurrent or persistent hyperparathyroidism characterized by the presence of multiple parathyroid tissue foci in the neck and mediastinum. It usually occurs in patients after parathyroidectomy for adenoma or hyperplastic disease (secondary form), but may occur “de novo” (primary form). Only about 60 cases have been described to date in the literature, in patients with familial forms of primary hyperparathyroidism (MEN1, FIHPT) or with chronic kidney disease. The main differential diagnosis is with parathyroid carcinoma. It is a difficult condition to diagnose and to treat radically. In patients with MEN1 syndrome, parathyroid tumors express somatostatin receptors on their cell surface, which can be targeted by somatostatin analogues for both tumor localization (68Ga-DOTATATE PET/CT) and treatment.
We report a rare case of parathyromatosis due to a combination of genetic alterations (MEN1 gene and CASR gene) never described in the literature. The lack of complete removal of parathyroid tissue foci, despite repeated surgery and medical treatment caused metabolic consequences of chronic hypercalcemia. Lanreotide treatment was beneficial in our patient, but due to the rarity of this condition, his potential aggressiveness of and the lack of clinical evidence in large series medical treatment need to be personalized.
An important challenge includes the functional relevance of rare genetic variants and/or the i of mutations in non-coding regions, the possible influence of epigenetic mechanisms in this rare condition which can help to identify potential new therapies.
Author contributions
Conception and design, GS, MG, and GP. Provision of study materials or patients, GS, MG, and GP. Collection and assembly of data, GS, MG, DA, RM, MT, MR, and GP. Data analysis and interpretation, GS, MG, and GP. Manuscript writing, GS, MG, and GP. Revision and final approval of manuscript, all authors. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Silva BC, Cusano NE, Bilezikian JP. Primary hyperparathyroidism. Best Pract Res Clin Endocrinol Metab (2018) 32(5):593–607. doi: 10.1016/j.beem.2018.09.004
2. Messa P, Alfieri CM. Secondary and tertiary hyperparathyroidism. Front hormone Res (2019) 51:91–108. doi: 10.1159/000491041
3. Khan AA, Hanley DA, Rizzoli R, Bollerslev J, Young JE, Rejnmark L, et al. Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. a Canadian and international consensus. Osteoporosis Int (2017) 28(1):1–19. doi: 10.1007/s00198-016-3716-2
4. Kamilaris CDC, Stratakis CA. Multiple endocrine neoplasia type 1 (MEN1): An update and the significance of early genetic and clinical diagnosis. Front endocrinology (2019) 10:339. doi: 10.3389/fendo.2019.00339
5. Fernandez-Ranvier GG, Khanafshar E, Jensen K, Zarnegar R, Lee J, Kebebew E, et al. Parathyroid carcinoma, atypical parathyroid adenoma, or parathyromatosis? Cancer (2007) 110(2):255–64. doi: 10.1002/cncr.22790
6. Fernandez-Ranvier GG, Khanafshar E, Tacha D, Wong M, Kebebew E, Duh QY, et al. Defining a molecular phenotype for benign and malignant parathyroid tumors. Cancer. (2009) 115(2):334–44. doi: 10.1002/cncr.24037
7. Scorza AB, Moore AG, Terry M, Bricker LA. Secondary parathyromatosis in a patient with normal kidney function: review of diagnostic modalities and approaches to management. Endocrine Pract (2014) 20(1):e4–7. doi: 10.4158/EP13053.CR
8. Nadarasa K, Theodoraki A, Kurzawinski TR, Carpenter R, Bull J, Chung TT, et al. Denosumab for management of refractory hypercalcaemia in recurrent parathyroid carcinoma. Eur J Endocrinol (2014) 171(3):L7–8. doi: 10.1530/EJE-14-0482
9. Vellanki P, Lange K, Elaraj D, Kopp PA, El Muayed M. Denosumab for management of parathyroid carcinoma-mediated hypercalcemia. J Clin Endocrinol Metab (2014) 99(2):387–90. doi: 10.1210/jc.2013-3031
10. Tzotzas T, Goropoulos A, Karras S, Terzaki A, Siolos A, Doumas A, et al. Effective long-term management of parathyromatosis-related refractory hypercalcemia with a combination of denosumab and cinacalcet treatment. Hormones. (2022) 21(1):171–6. doi: 10.1007/s42000-021-00343-w
11. Lastoria S, Marciello F, Faggiano A, Aloj L, Caraco C, Aurilio M, et al. Role of (68)Ga-DOTATATE PET/CT in patients with multiple endocrine neoplasia type 1 (MEN1). Endocrine. (2016) 52(3):488–94. doi: 10.1007/s12020-015-0702-y
12. Faggiano A, Tavares LB, Tauchmanova L, Milone F, Mansueto G, Ramundo V, et al. Effect of treatment with depot somatostatin analogue octreotide on primary hyperparathyroidism (PHP) in multiple endocrine neoplasia type 1 (MEN1) patients. Clin endocrinology (2008) 69(5):756–62. doi: 10.1111/j.1365-2265.2008.03301.x
13. Palmer JA, Brown WA, Kerr WH, Rosen IB, Watters NA. The surgical aspects of hyperparathyroidism. Arch surgery (1975) 110(8):1004–7. doi: 10.1001/archsurg.1975.01360140148028
14. Reddick RL, Costa JC, Marx SJ. Parathyroid hyperplasia and parathyromatosis. Lancet (1977) 1(8010):549. doi: 10.1016/S0140-6736(77)91414-3
15. Baloch ZW, Fraker D, LiVolsi VA. Parathyromatosis as cause of recurrent secondary hyperparathyroidism: a cytologic diagnosis. Diagn cytopathology (2001) 25(6):403–5. doi: 10.1002/dc.10004
16. Hage MP, Salti I, El-Hajj Fuleihan G. Parathyromatosis: a rare yet problematic etiology of recurrent and persistent hyperparathyroidism. Metabolism: Clin experimental (2012) 61(6):762–75. doi: 10.1016/j.metabol.2011.11.001
17. Jain M, Krasne DL, Singer FR, Giuliano AE. Recurrent primary hyperparathyroidism due to type 1 parathyromatosis. Endocrine. (2017) 55(2):643–50. doi: 10.1007/s12020-016-1139-7
18. Rattner DW, Marrone GC, Kasdon E, Silen W. Recurrent hyperparathyroidism due to implantation of parathyroid tissue. Am J surgery (1985) 149(6):745–8. doi: 10.1016/S0002-9610(85)80178-1
19. Akerstrom G, Rudberg C, Grimelius L, Rastad J. Recurrent hyperparathyroidism due to peroperative seeding of neoplastic or hyperplastic parathyroid tissue. case report. Acta chirurgica Scandinavica (1988) 154(9):549–52.
20. Fitko R, Roth SI, Hines JR, Roxe DM, Cahill E. Parathyromatosis in hyperparathyroidism. Hum pathology (1990) 21(2):234–7. doi: 10.1016/0046-8177(90)90136-S
21. Sokol MS, Kavolius J, Schaaf M, D'Avis J. Recurrent hyperparathyroidism from benign neoplastic seeding: a review with recommendations for management. Surgery. (1993) 113(4):456–61.
22. Kollmorgen CF, Aust MR, Ferreiro JA, McCarthy JT, van Heerden JA. Parathyromatosis: a rare yet important cause of persistent or recurrent hyperparathyroidism. Surgery. (1994) 116(1):111–5.
23. Stehman-Breen C, Muirhead N, Thorning D, Sherrard D. Secondary hyperparathyroidism complicated by parathyromatosis. Am J Kidney Dis (1996) 28(4):502–7. doi: 10.1016/S0272-6386(96)90459-X
24. Lee PC, Mateo RB, Clarke MR, Brown ML, Carty SE. Parathyromatosis: a cause for recurrent hyperparathyroidism. Endocrine Pract (2001) 7(3):189–92. doi: 10.4158/EP.7.3.189
25. Lentsch EJ, Withrow KP, Ackermann D, Bumpous JM. Parathyromatosis and recurrent hyperparathyroidism. Arch otolaryngology–head Neck surgery (2003) 129(8):894–6. doi: 10.1001/archotol.129.8.894
26. Evans CF, Mansfield L, Sharma AK. Recurrent hyperparathyroidism caused by parathyromatosis. Hosp Med (2005) 66(7):424–5. doi: 10.12968/hmed.2005.66.7.18390
27. Daphnis E, Stylianou K, Katsipi I, Stratigis S, Karamitopoulou E, Karkavitsas N, et al. Parathyromatosis and the challenge of treatment. Am J Kidney Dis (2006) 48(3):502–5. doi: 10.1053/j.ajkd.2006.05.010
28. Tublin ME, Yim JH, Carty SE. Recurrent hyperparathyroidism secondary to parathyromatosis: clinical and imaging findings. J ultrasound Med (2007) 26(6):847–51. doi: 10.7863/jum.2007.26.6.847
29. Unbehaun R, Lauerwald W. Successful use of cinacalcet HCl in a patient with end-stage renal failure and refractory secondary hyperparathyroidism due to parathyromatosis. Clin nephrology (2007) 67(3):188–92. doi: 10.5414/CNP67188
30. Vulpio C, D'Errico G, Mattoli MV, Bossola M, Lodoli C, Fadda G, et al. Recurrent renal hyperparathyroidism due to parathyromatosis. NDT plus (2011) 4(5):318–20. doi: 10.1093/ndtplus/sfr075
31. Diaconescu MR, Glod M, Grigorovici M, Diaconescu S. Parathyromatosis coexisting with papillary thyroid microcarcinoma. Chirurgia. (2011) 106(5):669–72.
32. Sim IW, Farrell S, Grodski S, Jung C, Ng KW. Parathyromatosis following spontaneous rupture of a parathyroid adenoma: natural history and the challenge of management. Internal Med J (2013) 43(7):819–22. doi: 10.1111/imj.12185
33. Wu TJ, Wang YT, Chang H, Lin SH. Parathyromatosis. Kidney Int (2012) 82(10):1140. doi: 10.1038/ki.2012.257
34. Mohammadi A, Ghasemi-Rad M. Parathyromatosis or recurrent multiple parathyroid adenomas? a case report. Maedica. (2012) 7(1):66–9.
35. Pinnamaneni N, Shankar PR, Muthukrishnan A. (99m)Tc MIBI SPECT findings in parathyromatosis–a rare entity causing recurrent hyperparathyroidism. Clin Nucl Med (2013) 38(11):e443–5. doi: 10.1097/RLU.0b013e318279bc2c
36. Twigt BA, van Dalen T, Vroonhoven TJ, Consten EC. Recurrent hyperparathyroidism caused by benign neoplastic seeding: two cases of parathyromatosis and a review of the literature. Acta chirurgica Belgica (2013) 113(3):228–32. doi: 10.1080/00015458.2013.11680918
37. Edling KL, Korenman SG, Janzen C, Sohsman MY, Apple SK, Bhuta S, et al. A pregnant dilemma: primary hyperparathyroidism due to parathyromatosis in pregnancy. Endocrine Pract (2014) 20(2):e14–7. doi: 10.4158/EP13105.CR
38. Sharma S, Dey P, Gude G, Saikia UN. Parathyromatosis-a rare occurrence along the endoscopic tract detected on fine needle aspiration cytology. Diagn cytopathology (2016) 44(12):1125–7. doi: 10.1002/dc.23571
39. Oueslati I, Khiari K, Khessairi N, McHirgui N, Ben Abdallah N. Parathyromatosis: a rare cause of persistent primary hyperparathyroidism. La Tunisie medicale (2016) 94(8-9):633–4.
40. Achour I, Charfi S, Chaabouni MA, Chakroun A, Guermazi F, Hammami B, et al. [Parathyromatosis: An uncommon cause of recurrent hyperparathyroidism]. La Rev medecine interne (2017) 38(1):61–4. doi: 10.1016/j.revmed.2016.03.005
41. Nakamura M, Tanaka K, Fujii T. Hyperparathyroidism caused by distant pulmonary lesions and parathyromatosis after ethanol injection/parathyroidectomy for secondary hyperparathyroidism. Hemodialysis Int Int Symposium Home Hemodialysis (2017) 21(3):E45–E9. doi: 10.1111/hdi.12525
42. Aggarwal A, Wadhwa R, Aggarwal V. Parathyromatosis following endoscopic parathyroid surgery: A rare occurrence. Indian J Endocrinol Metab (2017) 21(4):641–2. doi: 10.4103/ijem.IJEM_61_17
43. Bartonova L, Campr V, Chmelova R, Taudy M, Kodet R. Nonfunctioning parathyroid carcinoma associated with parathyromatosis. a case report. Ceskoslovenska patologie (2018) 54(1):37–42.
44. Wei AE, Garrett MR, Gupta A. Parathyromatosis: A rare case of recurrent hyperparathyroidism localized by four-dimensional computed tomography. AACE Clin Case Rep (2019) 5(6):e384–e7. doi: 10.4158/ACCR-2019-0225
45. Cao H, Zeng M, Fang H, Tang L, Liu W. Parathyromatosis type 2 detected by (99m)Tc-MIBI SPECT/CT. Gland surgery (2019) 8(6):806–9. doi: 10.21037/gs.2019.11.13
46. Miller MJ, Agrawal N, Katz G, Ogilvie J, Melamed J. Parathyromatosis with a papillary architecture. Histopathology. (2019) 75(4):598–602. doi: 10.1111/his.13928
47. Haciyanli M, Karaisli S, Gucek Haciyanli S, Atasever A, Arikan Etit D, Gur EO, et al. Parathyromatosis: a very rare cause of recurrent primary hyperparathyroidism - case report and review of the literature. Ann R Coll Surgeons England (2019) 101(8):e178–e83. doi: 10.1308/rcsann.2019.0105
48. Altin O, Sari R. Pericardial type 1 parathyromatosis: A very rare cause of primary hyperparathyroidism. Acta Endocrinol (Buchar) (2020) 16(4):505–7. doi: 10.4183/aeb.2020.505
49. Yang J, Zhang J, Liu NH, Liu H, Dong MJ. Persistent secondary hyperparathyroidism caused by parathyromatosis and supernumerary parathyroid glands in a patient on haemodialysis. BMC nephrology (2020) 21(1):257. doi: 10.1186/s12882-020-01917-3
50. Ilyicheva EA, Bersenev GA. Parathyromatosis as a cause of recurrence primary hyperparathyroidism: A case report. Int J Surg Case Rep (2021) 80:105689. doi: 10.1016/j.ijscr.2021.105689
Keywords: case report, MEN 1 syndrome, parathyromatosis, CASR alterations, somatostatin analogues (SSAs)
Citation: Sapuppo G, Giusti MA, Aricò D, Masucci R, Tavarelli M, Russo M and Pellegriti G (2023) Recurrent parathyromatosis in a patient with concomitant MEN1 and CASR gene alterations: Clinical management of a case report and literature review. Front. Endocrinol. 14:1108278. doi: 10.3389/fendo.2023.1108278
Received: 25 November 2022; Accepted: 02 March 2023;
Published: 14 March 2023.
Edited by:
Arif Ansori, Airlangga University, IndonesiaReviewed by:
Khashayar Sakhaee, University of Texas Southwestern Medical Center, United StatesArli Aditya Parikesit, Indonesia International Institute for Life-Sciences (i3L), Indonesia
Copyright © 2023 Sapuppo, Giusti, Aricò, Masucci, Tavarelli, Russo and Pellegriti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giulia Sapuppo, Z2l1bGlhc2FwdXBwb0Bob3RtYWlsLml0
†These authors have contributed equally to this work
‡ORCID: Giulia Sapuppo, orcid.org/0000-0002-8471-7310