 Lucilla Crudele1†
Lucilla Crudele1† Oihane Garcia-Irigoyen1,2†
Oihane Garcia-Irigoyen1,2† Marica Cariello1
Marica Cariello1 Marilidia Piglionica1Natasha Scialpi1Marilina Florio1Giuseppina Piazzolla1
Marilidia Piglionica1Natasha Scialpi1Marilina Florio1Giuseppina Piazzolla1 Patrizia Suppressa1
Patrizia Suppressa1 Carlo Sabbà1
Carlo Sabbà1 Raffaella Maria Gadaleta1*‡
Raffaella Maria Gadaleta1*‡ Antonio Moschetta1,3*‡
Antonio Moschetta1,3*‡- 1Department of Interdisciplinary Medicine, University of Bari “Aldo Moro”, Bari, Italy
- 2Department of Biosciences and Nutrition, Karolinska Institutet, Huddinge, Sweden
- 3National Institute for Biostructures and Biosystems (INBB), Rome, Italy
Objective: Increased Fibroblast Growth Factor-21 (FGF-21) circulating levels have been described in obesity. In this observational study, we analysed a group of subjects with metabolic disorders to unravel the putative link between visceral adiposity and FGF-21 serum levels.
Methods: Total and intact serum FGF-21 concentration was measured with an ELISA assay respectively in 51 and 46 subjects, comparing FGF-21 levels in dysmetabolic conditions. We also tested Spearman’s correlations between FGF-21 serum levels and biochemical and clinical metabolic parameters.
Results: FGF-21 was not significantly increased in high-risk conditions such as visceral obesity, Metabolic Syndrome, diabetes, smoking, and atherosclerosis. Waist Circumference (WC), but not BMI, positively correlated with total FGF-21 levels (r=0.31, p <0.05), while HDL-cholesterol (r=-0.29, p <0.05) and 25-OH Vitamin D (r=-0.32, p <0.05) showed a significant negative correlation with total FGF-21. ROC analysis of FGF-21 in prediction of increased WC, showed that patients with total FGF-21 level over cut-off value of 161.47 pg/mL presented with impaired FPG. Conversely, serum levels of the intact form of FGF-21 did not correlate with WC and other metabolic biomarkers.
Conclusion: Our newly calculated cut-off for total FGF-21 according to visceral adiposity identified subjects with fasting hyperglycemia. However, waist circumference correlates with total FGF-21 serum levels but does not correlate with intact FGF-21, suggesting that functional FGF-21 does not necessarily relate with obesity and metabolic features.
1 Introduction
The Fibroblast Growth Factor-21 (FGF-21) is an atypical member of the Fibroblast Growth Factors (FGFs) family. FGF-21 lacks the conventional FGF heparin-binding domain (1, 2), therefore can diffuse away from its tissues of origin and functions as an endocrine hormone. In humans, FGF-21 production mainly occurs in the liver under the control of Peroxisome Proliferator-activated Receptor-alpha (PPAR-α), responsible for the downregulation of energy expenditure as a metabolic adaptation in response to prolonged starvation, high sugar intake, and dietary protein restriction (3). FGF-21 is a small protein comprising 181 amino acids that binds a receptor complex consisting of a classical FGF Receptor 1c (FGFR1c) and the co-receptor β-klotho (KLB), which is selectively expressed in metabolic tissues, such as white and brown adipose tissue (WAT and BAT), pancreas, muscle, heart, thymus where FGF-21 exploits several functions aimed to counteract metabolic derangement, metaflammation and stress damage (4). Fibroblast activation protein (FAP), a member of dipeptidyl peptidase-IV (DPP-IV) family, has been identified as the protease responsible for the proteolytic inactivation of human FGF-21 in blood, and cleavage of 10 amino acid residues at the C-terminus of the intact FGF-21 form, essential for its receptor binding and signaling activity (5). Indeed, Dunshee et al. showed that inhibiting FAP results in increased intact FGF-21 levels in cynomolgus monkeys (6). However, the exact mechanisms whereby FGF-21 mediates its pleiotropic actions have not been fully elucidated and information on FGF-21 gene expression in human tissues is limited since several discrepancies between animals and humans have been detected (7). A role for FGF-21 as a regulator of food intake and preferences in the central nervous system has been hypothesized (8); nevertheless, a wide interindividual variation of its serum level in the fasting state has been established (9). Physical exercise and lifestyle (9, 10), as well as drugs and dietary regimens (11), also influence FGF-21 levels as well as circadian variations have been detected with lower levels in the afternoon, likely due to increased free fatty acids (FFAs) plasma levels inducing the PPAR-α expression. Moreover, although direct correlations between FGF-21 levels and triglycerides (TG), glycemia, lipids, and insulin levels have been shown (12), the role of FGF-21 in obesity, diabetes, non-alcoholic fatty liver disease (NAFLD), Metabolic Syndrome (MetS), and coronary artery disease (CAD) is still debated (13–15). In fed state, FGF-21 cooperates with glucagon in promoting glucose synthesis, and stimulating glucose uptake in an insulin-independent manner (16). Paradoxically, it has been previously shown that circulating FGF-21 levels are already increased in these pathological conditions and several hypotheses have been formulated to explain this incongruity. It could either acting as a protecting factor against a metabolic overload or as a response to metabolic stress (7); for instance, a recent study found that FGF-21 increases in response to hypoxia and related oxidative stress in patients with obstructive sleep apnea, generally considered a component of MetS (17). Moreover, an FGF-21 resistance mechanism, similar to the insulin-resistance seen in diabetes, has been proposed (18).
From a clinical standpoint, assessing FGF-21 levels and understanding its function could make it a diagnostic and/or prognostic biomarker (19), as well as help discriminate patients responder vs non-responder to therapies, since Dutchark et al. showed that FGF-21 mediates thiazolidinediones antidiabetic actions (20). Furthermore, the pharmacological use of FGF-21 analogues has been proposed in the treatment of dyslipidemia, obesity, type 2 diabetes, and NASH (21–23).
In this study, we assessed intact and total FGF-21 levels in two cohorts of subjects with putative risk for MetS and obesity-related diseases with the goal of identifying the relationships between FGF-21 serum level and visceral obesity and its related complications.
2 Methods
2.1 Study population
Patients’ enrollment and clinical, biochemical, and instrumental evaluation were carried out at the Outpatient Clinic of Metabolic Disease of the Internal Medicine Division at Department of Interdisciplinary Medicine – “Aldo Moro” University of Bari (Italy). Patients with acute cardiovascular, renal, and hepatic failure, Inflammatory Bowel Disease and neoplastic diseases diagnosed less than 10 years before enrollment were excluded. The study was approved by the Ethics Committee of the Azienda Ospedaliero-Universitaria Policlinico di Bari (Bari, Italy) in accordance with the principles of the Declaration of Helsinki and all patients provided written informed consent prior to enrollment. In accordance with the approved Ethics Committee, only 18 years old or older patients were included in the study.
2.2 Clinical assessment
All participants underwent a detailed anamnesis and physical examination. Anthropometric assessment was performed using standardized procedures. The diagnosis of MetS was assessed in accordance to the National Cholesterol Education Program - Adult Treatment Panel III (NCEP-ATPIII) (24). Accordingly, visceral adiposity is defined as Waist Circumference (WC) > 102 cm for males and >88 cm for females. WC was measured at the midpoint between the inferior part of the 12th rib and the anterior-superior iliac crest. Body Mass Index (BMI) was computed as weight (Kg) divided by the height squared (sqm) and BMI values (Kg/sqm) between 25 and 29.9 and over 30 were classified as overweight and obesity, respectively. The population included patients affected by chronic high blood pressure (HBP) together with a chronic condition of hypertensive cardiopathy, diabetes, chronic renal failure, and chronic gastrointestinal diseases (gastroesophageal reflux, chronic gastritis, irritable bowel syndrome). Diabetes was defined according to HbA1c (percentage of glycosylated hemoglobin) ≥ 6.5%, fasting plasma glucose (FPG) ≥ 126 mg/dL (25) and/or treatment for diabetes (24). Hypertension was defined as systolic arterial blood pressure ≥ 130 mmHg, diastolic arterial blood pressure ≥ 85 mmHg and/or treatment with antihypertensive agents. B-mode ultrasonography with a 4- to 7-MHz linear array transducer was performed to detect carotid plaques in evaluation of atherosclerosis. Color and power Doppler were used to further delineate the plaque border (26).
2.3 Biochemical measurements
Morning blood samples were obtained after 12 hours of fasting from the antecubital veins. After blood clotting and centrifugation, serum was processed for analysis of biochemical markers of glucose and lipid metabolism. Liver, renal, thyroid, and inflammatory markers were also measured following standardized biochemical procedures. All biochemical measurements were performed in the ISO 9001 certified laboratories of the University Hospital of Bari.
Serum concentrations of total and intact forms of FGF-21 were assesed with ELISA assays and all measurements were carried out according to the manufacturers’ protocols. The Standard Curve was generated by plotting the absorbance versus human FGF-21 concentration for each standard provided by the supplier. Concentrations of unknown samples were determined by interpolation using this standard curve. Results are reported as concentration of FGF-21 (pg/mL) in the analysed samples. Total FGF-21 serum levels were measured with the RD191108200R Human FGF-21 ELISA (BioVendor Laboratory Medicine, Inc., Modrice, Czech Republic). Kit sensitivity was 7 pg/mL and upper limit of detection was 1920 pg/mL.
Intact FGF-21 was measured with the EDI Human Intact FGF-21 ELISA Kit (Epitope Diagnostics, Inc., San Diego, USA). The assay utilizes two selective antibodies that specifically bind to both the N- and C- terminus of human FGF-21. Kit sensitivity was 1.7 pg/mL and its upper limit of detection was 20000 pg/mL. All samples with values under or above the detectability limits were not considered for the analyses and those samples were excluded from both population studies.
2.4 Statistical analysis
All results are expressed as means ± standard error of the mean (SEM), in counts and percentages for categorical data. FGF-21 significant differences between two groups were determined by Mann-Whitney U test. The correlation between continuous variables was analysed using Spearman Correlation (r). All reported p-values were based on two-sided tests and compared to a significance level of 5%.
Cut-off point analysis was used to determine the optimal value of FGF-21 that differentiates patients who had increased WC. In particular, the crucial point was defined by the largest distance from the diagonal line of the receiver operating characteristic curve (ROC) (sensitivity x {1-specificity}). Empirical ROC curves were plotted along with calculation of the Area under the Curve (AUC) with 95% confidence intervals and one-sided upper p-values for null hypothesis AUC=0.5. Youden’s Index, or equivalently, the highest Sensitivity + Specificity, was used to determine the optimal cut-off. P-values of less than 0.05 were considered significant.
All analyses were performed using the NCSS 12 Statistical Software, version 12.0.2018 (NCSS, LLC Company, Kaysville, UT, USA) and GraphPad Prism, version 9.1.0 (GraphPad Software; San Diego, CA, USA).
3 Results
3.1 Clinical characterization of the study population
Fifty-one patients at their first assessment (24 males and 27 females), were recruited for evaluation of total FGF-21 serum levels from May 2015 to May 2016. Mean age of subjects was 61 ± 2 years. 30 patients (59%) were diagnosed with MetS, while 25 (49%) were diagnosed with Type 2 Diabetes. HBP was diagnosed in 36 patients (71%) and a carotid atherosclerotic plaque was detected in 14 subjects (27%). Total (cleaved and intact forms) FGF-21 mean serum level was 189.9 ± 38.1 pg/mL. Clinical characteristics of enrolled patients are shown in Supplementary Table 1.
No significant difference was found between males (242.9 ± 73.6 pg/mL) and females (142.6 ± 28.9 pg/mL). Data in Table 1 display an increasing trend of FGF-21 levels (although not significant) when comparing patients with increased WC vs normal WC (NCEP-ATPIII criterion cut-off for WC), those affected by MetS vs patients without MetS, diabetic vs non diabetic, and patients with atherosclerosis vs patients without it.
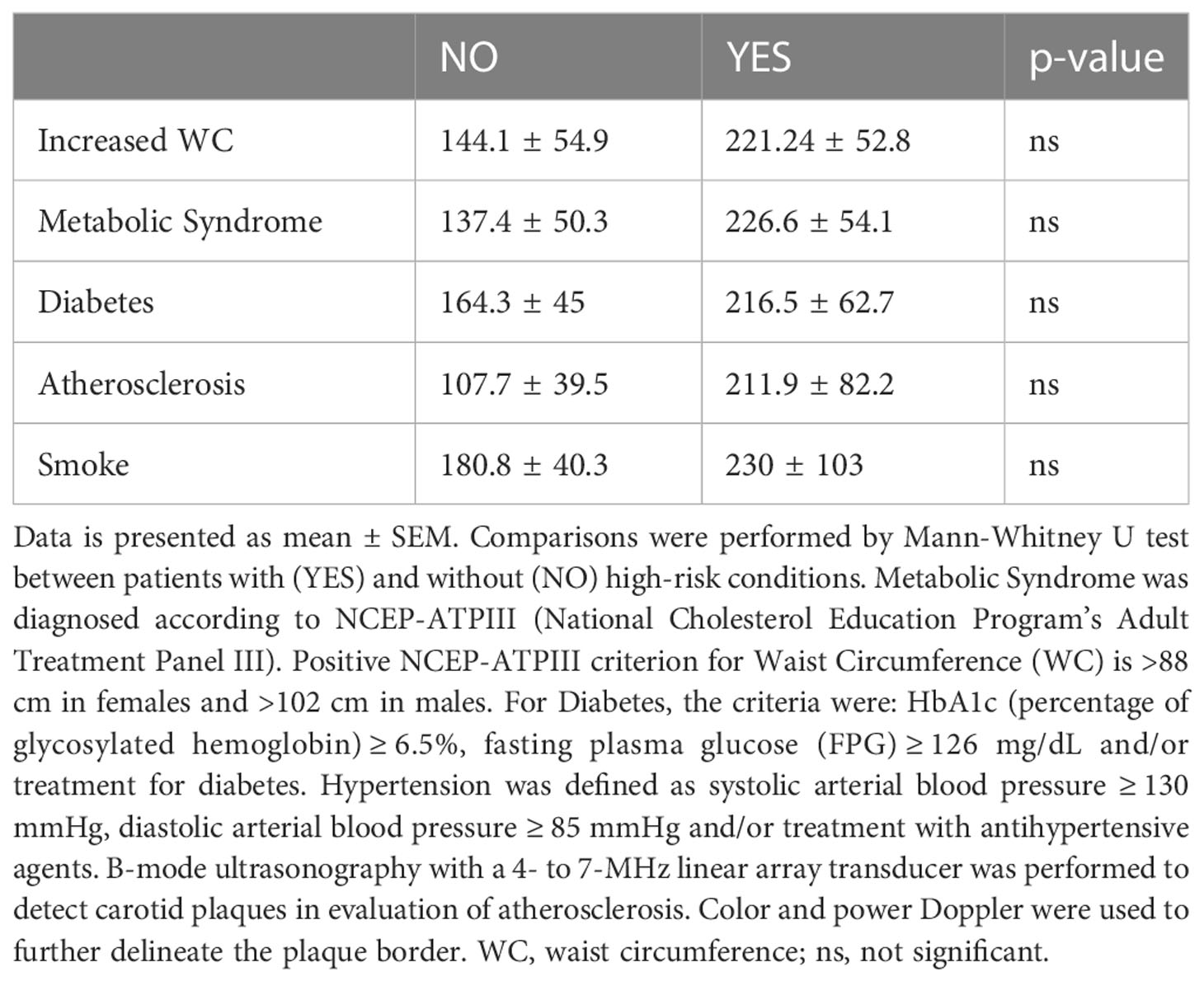
Table 1 FGF-21 total serum level comparisons in individuals with and without high-risk conditions.
3.2 Total FGF-21 serum level and visceral adiposity in high-risk conditions
Given the role of visceral obesity in determining dysmetabolism and the strong interplay among several biochemical variables and patients’ metabolic status, the relationships between WC and glucose and lipid metabolism biomarkers were assessed (Figure 1). Statistical analyses showed that there was a strong positive correlation between WC and FPG (r=0.34, p<0.05) and TG (r=0.53; p<0.001) levels. While total cholesterol did not correlate with WC, a remarkable inverse correlation between HDL cholesterol and WC was observed (r=-0,4, p<0.01). Since HDL-cholesterol levels reflect patients’ metabolic disorders and significantly correlates with obesity, correlation analyses between HDL and BMI, WC, and Vitamin D were also performed. HDL-cholesterol levels showed a negative significant correlation with both BMI and WC. Intriguingly, a positive significant correlation was found between HDL-cholesterol and 25-OH Vitamin D (r=0.48, p<0.01).
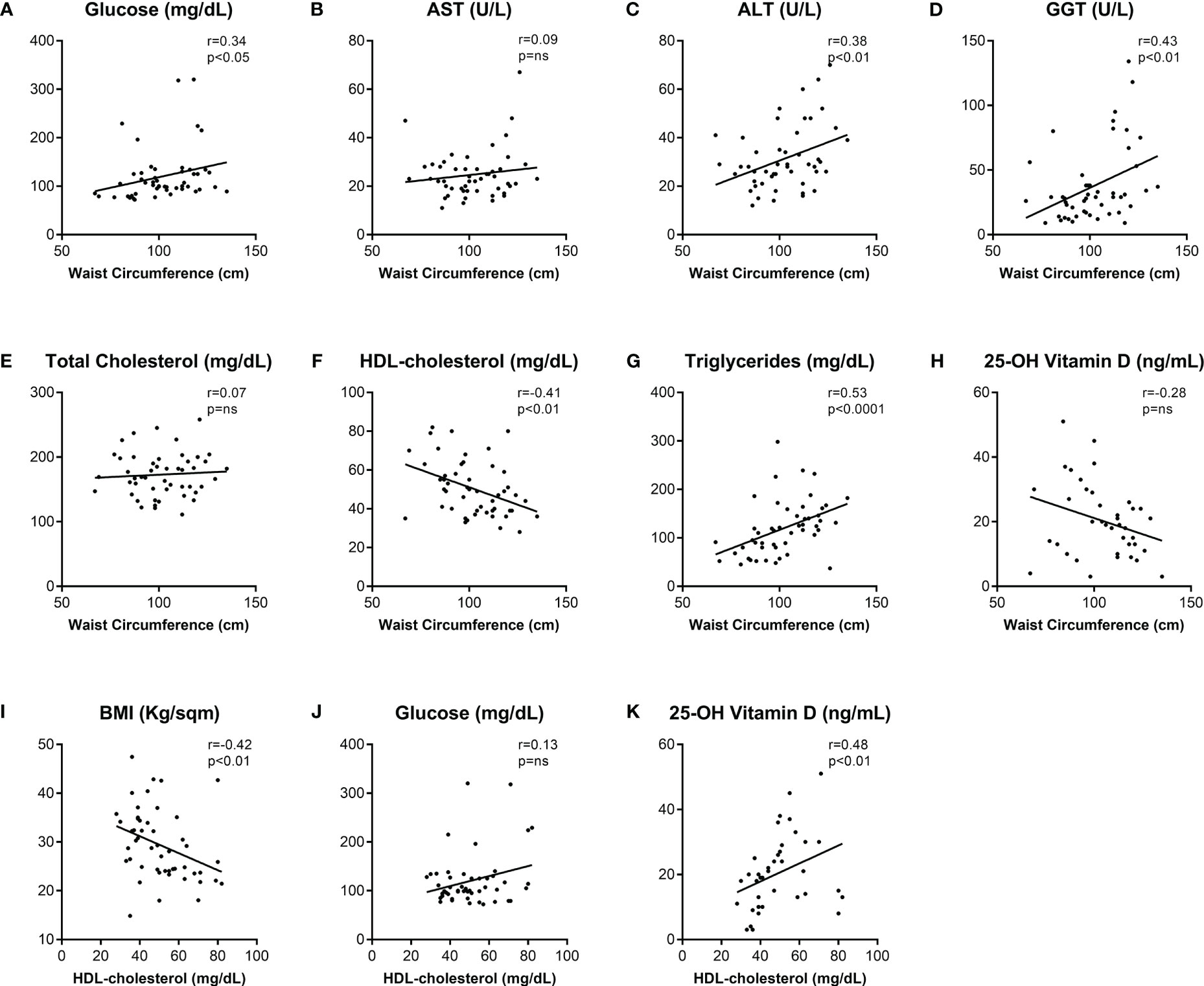
Figure 1 Correlations among clinical and biochemical metabolic biomarkers in the population study.Spearman’s correlations (r) of Waist Circumference (A–H) and HDL-cholesterol (I–K) with biochemical metabolic variables. p-values <0.05 were considered significant. Abbreviations: AST, aspartate transaminase; ALT, alanine transaminase; GGT, gamma-glutamyl transpeptidase; HDL, high-density lipoprotein; BMI, body mass index; ns, not significant.
In order to study the relation between patients dysmetabolism and FGF21 levels, serum total FGF-21 levels were correlated with other clinical and biochemical serum biomarkers. Age was not associated to total FGF-21 levels in the studied cohort (Figure 2A). Strikingly, while BMI did not correlate with total FGF-21 (Figure 2B), increase of WC directly reflected total FGF-21 levels (Figure 2C; r=0.31, p<0.05). Glucose, total cholesterol, and TG levels did not correlate with serum total FGF-21 (Figures 2D–F). Finally, an inverse relation between FGF-21 and both HDL-cholesterol (r=-0.29, p<0.05) and 25-OH Vitamin D (r=-0.32, p<0.05) were uncovered (Figures 2G, H).
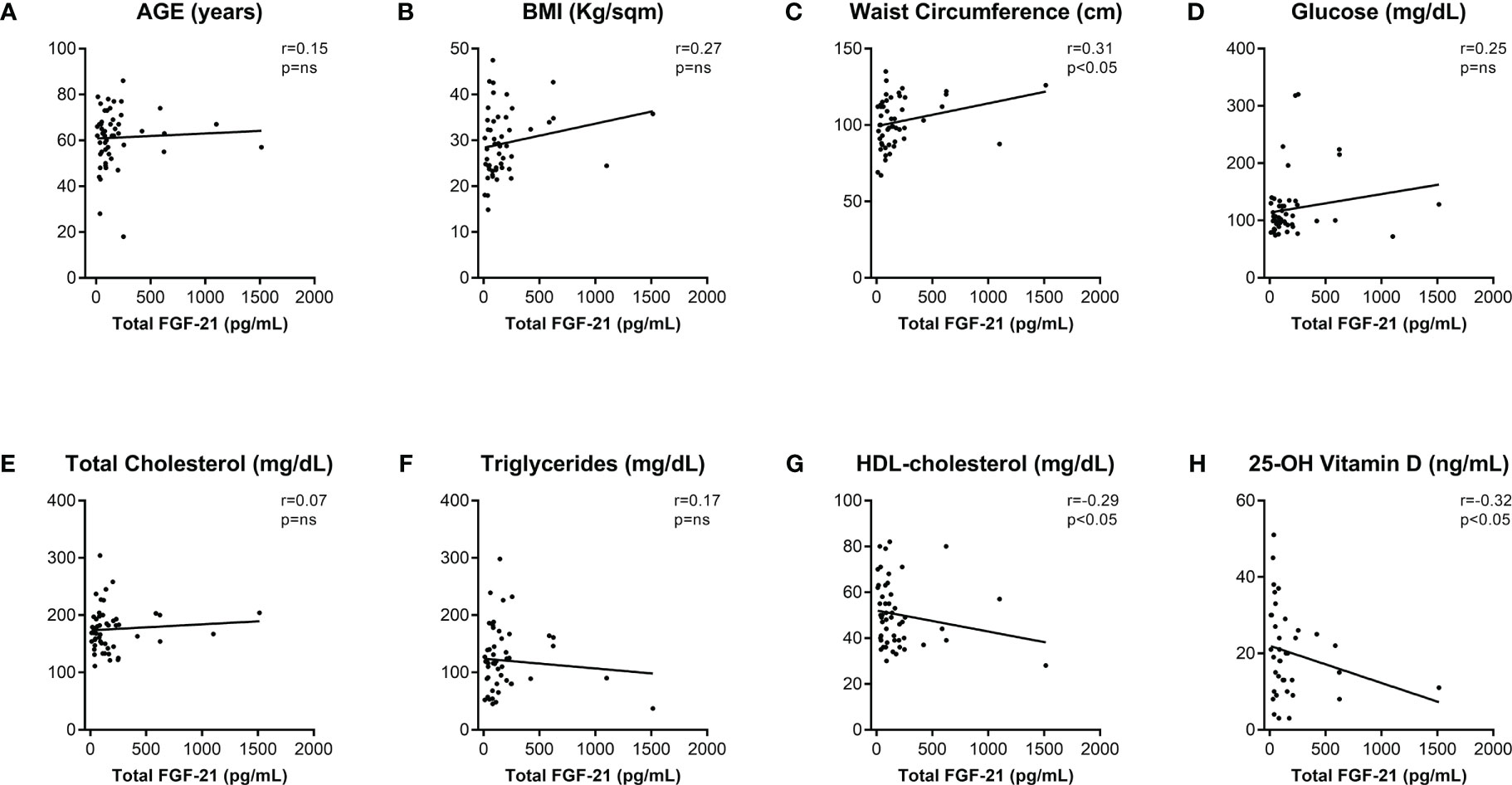
Figure 2 Correlations of total FGF-21 serum level with clinical and biochemical metabolic biomarkers. Total FGF-21 Spearman’s correlations (r) with clinical (A–C) and biochemical (D–H) metabolic variables metabolic variables. p-values <0.05 were considered significant. BMI, body mass index; HDL, high-density lipoprotein; ns, not significant.
3.3 Detection of FGF-21 cut-off value for prediction of visceral obesity
Given the direct relationship between FGF-21 and WC, we performed a cut-off point analysis (AUC=0.63, p-value <0.05) to determine the serum total FGF-21 value able to discriminate patients who had visceral obesity according to NCEP-ATPIII WC criterion (Figure 3A). A cut-off value of 161.47 pg/mL was found, with a sensitivity of 45% and a specificity of 84%. Then, we categorized patients in two subgroups according to total FGF-21 serum level under (n=34) or above (n=17) the newly found cut-off value and a comparison of several biochemical parameters was performed. We found that FPG was significantly increased in those with increased FGF-21 levels (Figure 3B), discriminating people with fasting hyperglycemia (105.82 mg/dL vs 148.65 mg/dL). Also, there was an increase, although not significant, of GGT and TG levels (Figures 3C, D) in patients with total serum FGF-21 levels above the cut-off. Vitamin D and HDL were unchanged in the two groups (Figures 3E, F).
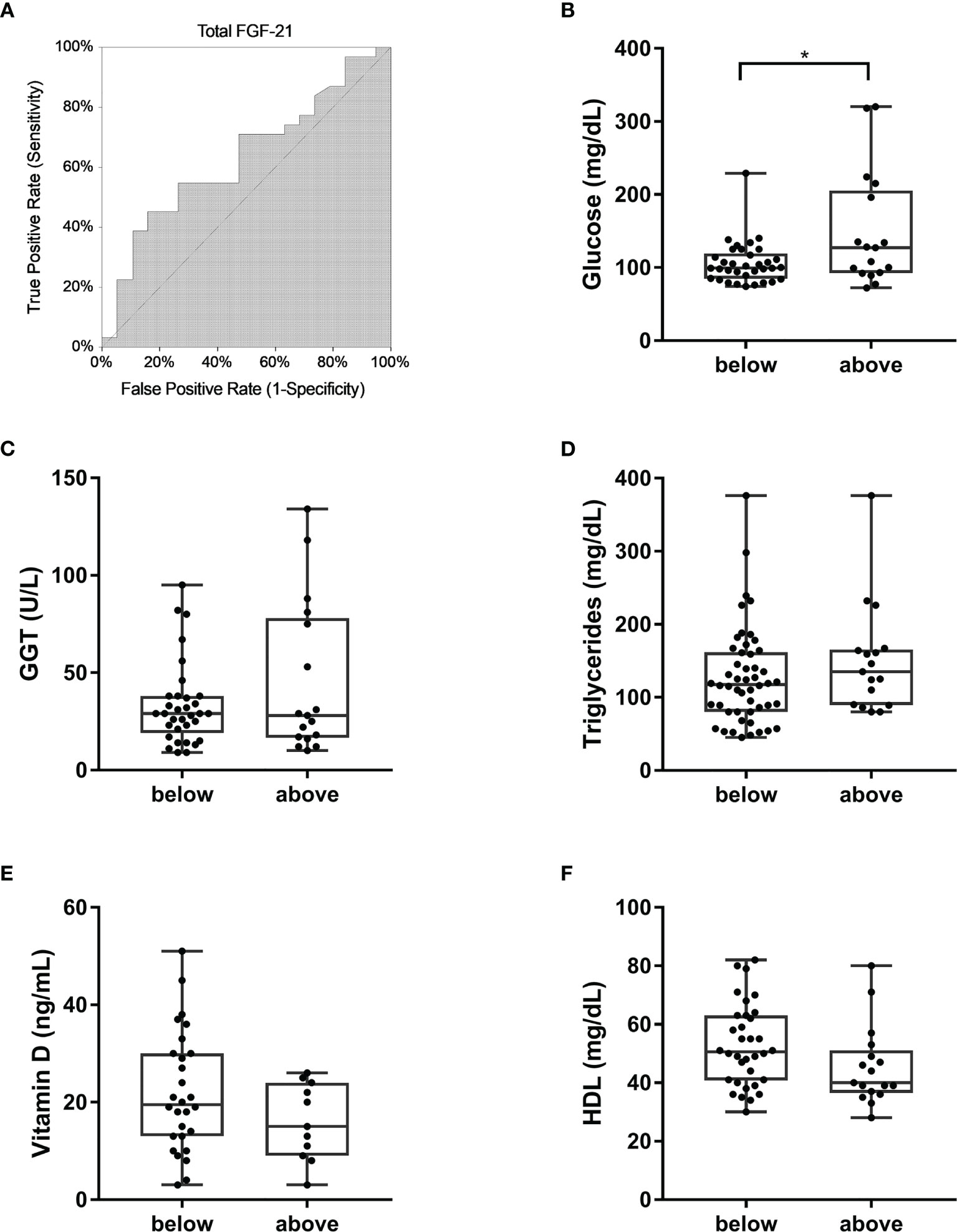
Figure 3 Total FGF-21 in prediction of visceral obesity and diabetes. (A) ROC curve of total FGF-21 for diagnosis of increased WC according to NCEP-ATPIII criterion. AUC=0.63, Z-value to test AUC>0.5=1.65, upper 1-sided p-value <0.05. Cut-off value=161.47 pg/mL. Comparisons of glucose (B), GGT (C), triglycerides (D), Vitamin D (E), and HDL-cholesterol (F) levels in patients with serum total FGF-21 level below and above the calculated cut-off value. *p-value <0.001. GGT, gamma-glutamyl transpeptidase; HDL, high-density lipoprotein.
3.4 Intact FGF-21 serum level and visceral adiposity in high-risk conditions
Since only intact FGF-21 is able to cross-bind the co-receptor FGFR1c-KLB thus initiating the FGF-21 signaling cascade, and an assay determining total FGF-21 (both cleaved and intact forms) levels could overestimate the biological activity of this hormone (27), we measured intact FGF-21 levels in the serum of an additional population of forty-six patients at their first assessment (18 males, 28 females; mean age 54 ± 3 years) recruited from January to May 2023. Clinical characterization of these patients is included in Supplementary Table 2. The mean value of intact FGF-21 levels was 147.4 ± 42.2 (179.7 ± 99.8 in males, 126.7 ± 28.5 in females, p-value=not significant). Similar to the measurements of total serum FGF-21 levels, no significant differences in the FGF-21 intact form serum level were found in patients with high-risk conditions (Table 2). Moreover, also correlations between WC and glucose and lipid metabolism biomarkers (Figures 4A–H), as well as those between HDL and BMI, glucose, and Vitamin D were confirmed (Figures 4I–K) in this additional population. Similarly, age (Figure 5A), BMI (Figure 5B), glucose (Figure 5D), total cholesterol (Figure 5E) and triglycerides (Figure 5F) did not show any significant association with serum intact FGF-21 levels. Conversely, serum intact FGF-21 levels did not correlate any longer with WC (Figure 5C), HDL-c (Figure 5G) and Vitamin D (Figure 5H) levels. We also performed a ROC analysis for prediction of visceral adiposity by intact FGF-21 serum level finding a not-significant (p-value=0.18) AUC of 0.58.
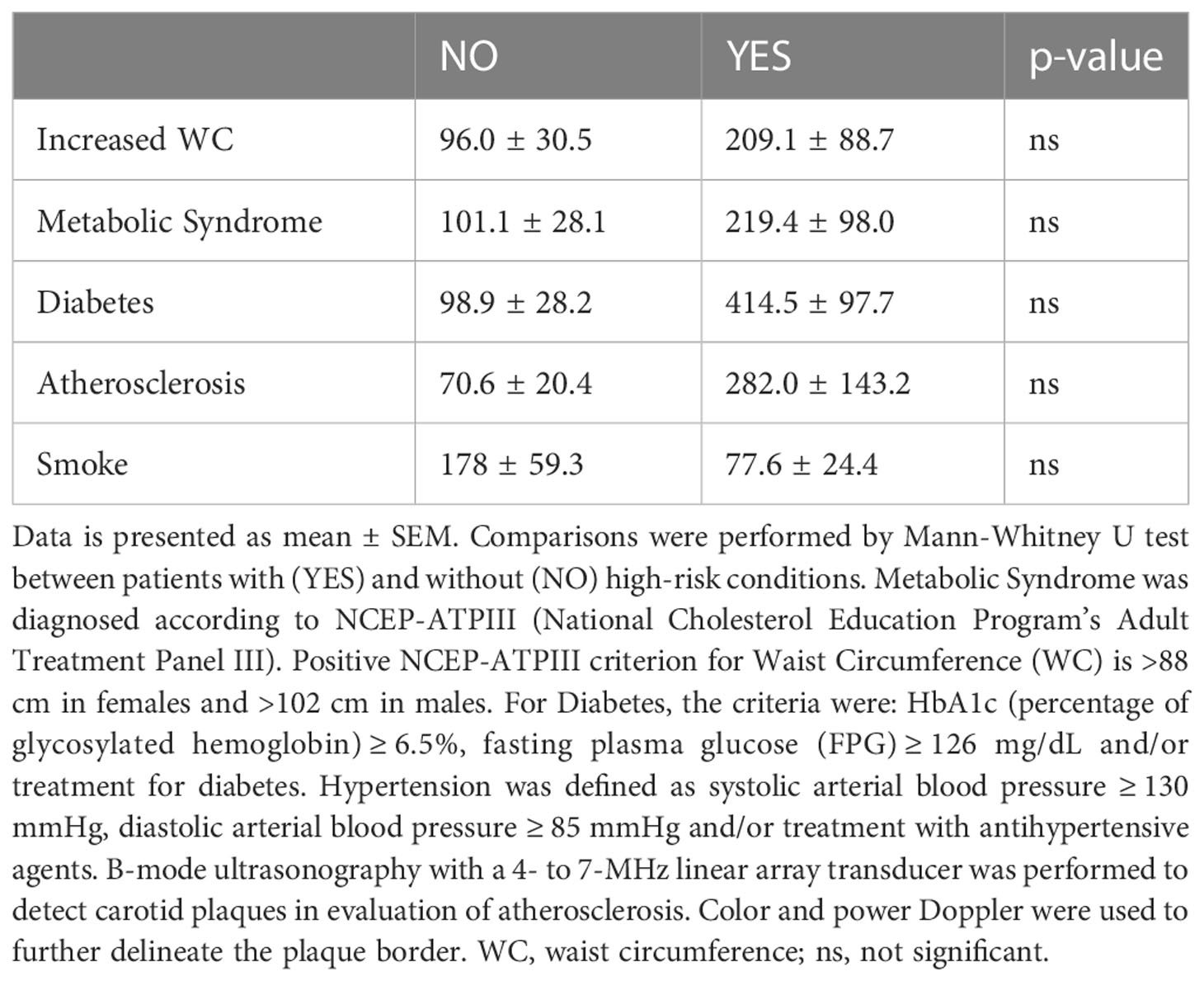
Table 2 FGF-21 intact serum level comparisons in individuals with and without high-risk conditions.
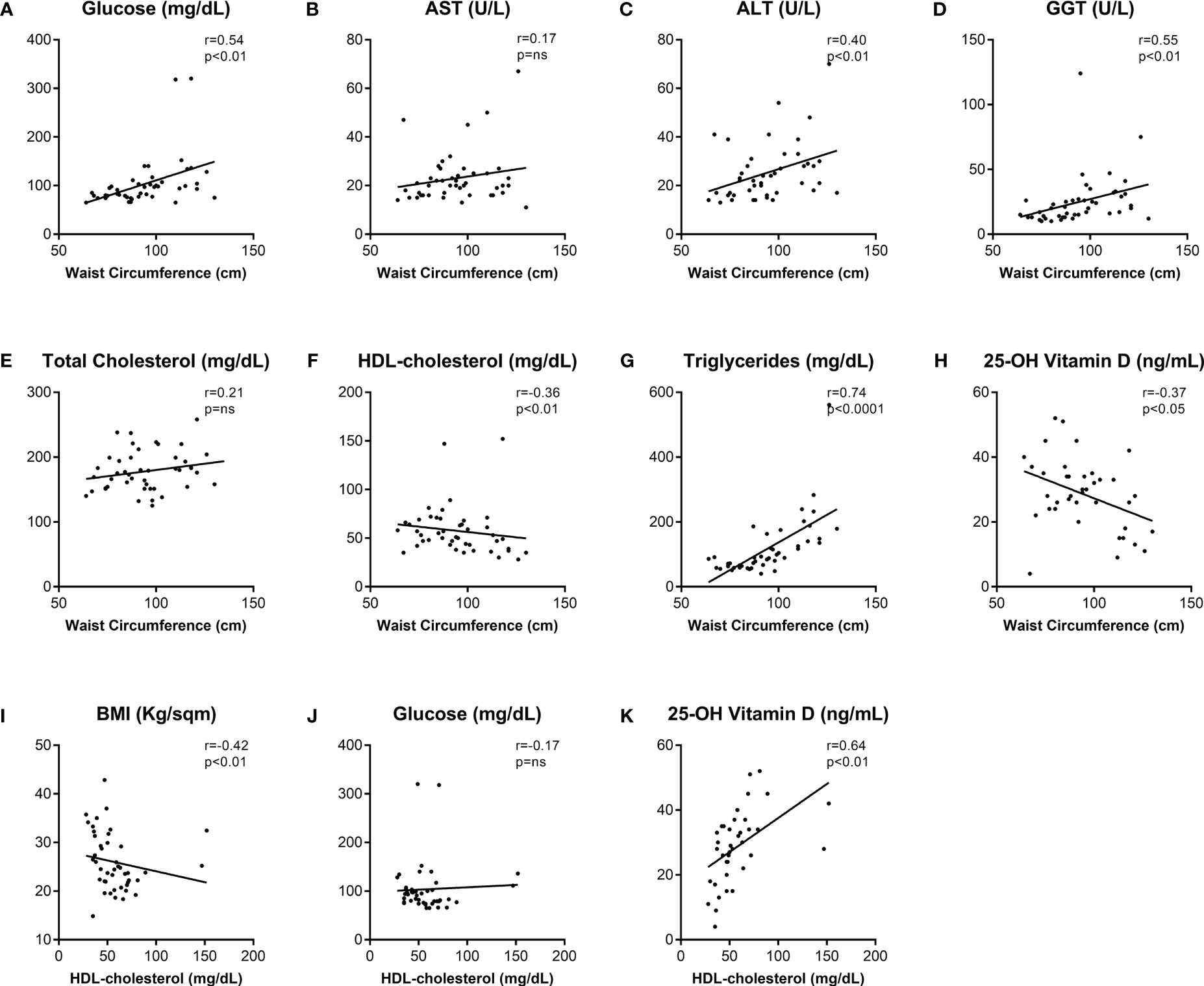
Figure 4 Correlations among clinical and biochemical metabolic biomarkers in another cohort of subjects. Spearman’s correlations (r) of Waist Circumference (A–H) and HDL-cholesterol (I–K) with biochemical metabolic variables. p-values <0.05 were considered significant. Abbreviations: AST, aspartate transaminase; ALT, alanine transaminase; GGT, gamma-glutamyl transpeptidase; HDL, high-density lipoprotein; BMI, body mass index; ns, not significant.
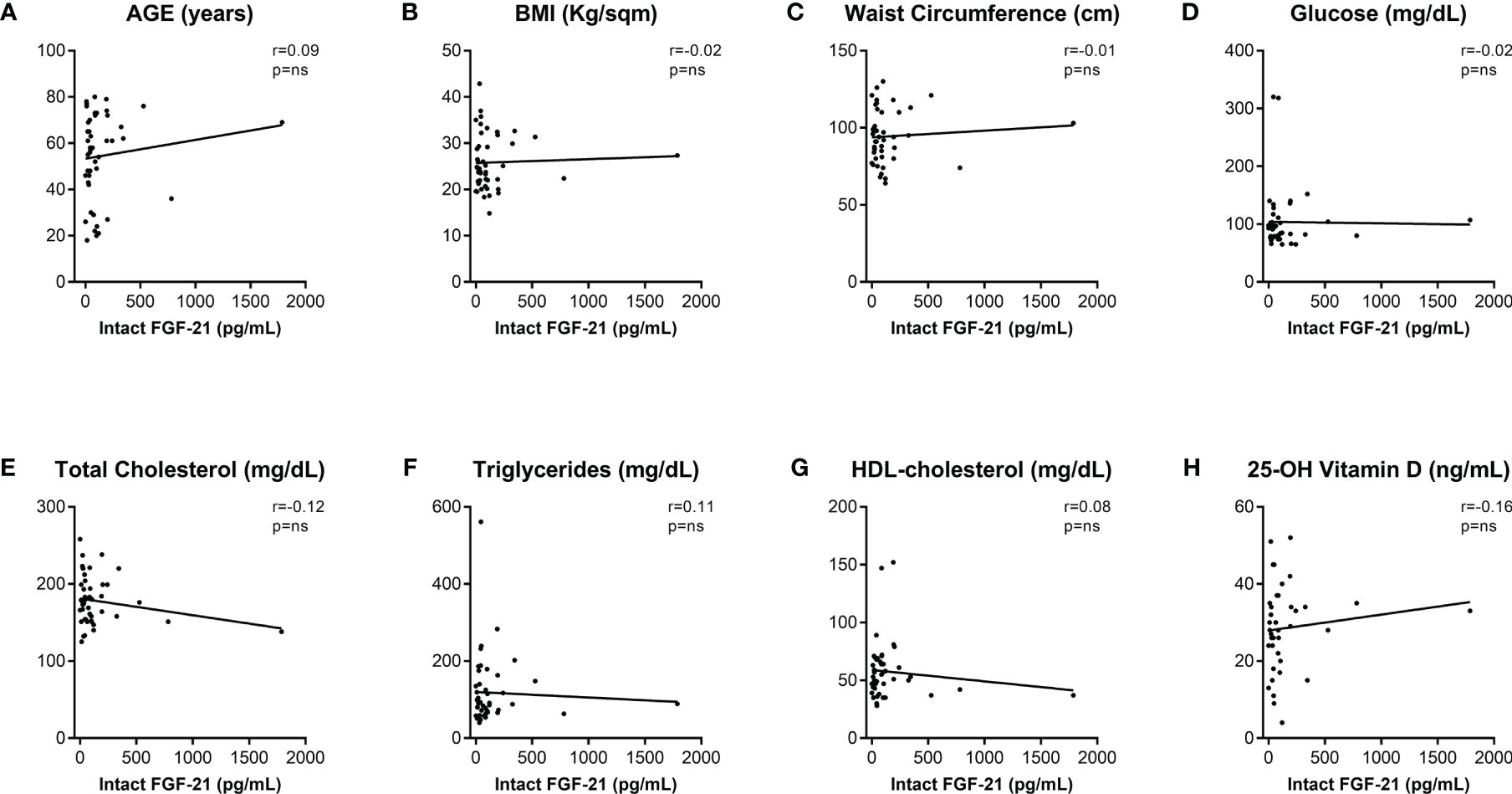
Figure 5 Correlations of intact FGF-21 serum level with clinical and biochemical metabolic biomarkers. Intact FGF-21 Spearman’s correlations (r) with clinical (A–C) and biochemical (D–H) metabolic variables. p-values <0.05 were considered significant. BMI, body mass index; HDL, high-density lipoprotein; ns, not significant.
4 Discussion
FGF-21 is a peculiar stress-induced hormone-like molecule with pleiotropic functions regulating body energy homeostasis and lipid and glucose metabolism. In the last years, FGF-21 has drawn attention for its putative beneficial role in obesity-associated metabolic complications (28). Nevertheless, its complex mechanism of action is yet to be resolved, especially considering its tissue specificity and the current fragmentary translation of its physiological and pharmacological actions from rodents to humans. In this study, FGF-21 levels were analyzed in a cohort of patients with risk for dysmetabolic disorders.
Firstly, the hypothesis that FGF-21 serum level may predict or reflect a specific condition was tested. In line with previously published data, showing extremely variable FGF-21 levels, up to 250-fold variation even in healthy individuals (12, 29–31), our analysed cohort showed a heterogeneous amount of this hormone, regardless of sex and dysmetabolic conditions.
Interestingly, the level of total FGF-21 in our patients with diabetes and MetS were lower than the one previously shown in literature. While threshold values of 260 pg/mL and 270 pg/mL were proposed in differentiating patients with Insulin Resistance and MetS, respectively (32), in our sample mean values of circulating FGF-21 in diabetics and metabolic patients were lower and in line to another study that found median FGF-21 concentration of 239.9 pg/mL in diabetics subjects (33).
In the current study, an intriguingly significant correlation between circulating FGF-21 levels and WC, but not BMI and body weight, was established. This is in agreement with the concept that WC, rather than BMI, is a stronger indicator of Visceral Adipose Tissue (VAT) deposition and a stronger risk factor for the development of dysmetabolism-associated diseases. Here, with a ROC analysis we found that FGF-21 circulating level of 161.47 pg/mL serve as a discriminant value to identify people with visceral obesity. Moreover, individuals with FGF-21 level above this cut-off also presented with fasting hyperglycemia. Conversely, in a previous study by Mashili et al. (34) all measures of adiposity (BMI, waist circumference, and body fat percentage) were highly correlated with circulating total FGF-21 in patients with and without diabetes.
Intriguingly, FGF-21 mRNA expression in humans is almost exclusively limited to liver and its expression in adipose tissue (AT) is still debated (11, 35). Hepatic FGF-21 transcription is regulated by PPAR-α, PPAR-γ coactivator-1α (PGC-1α), retinoid acid receptor-related orphan receptor alpha (ROR-α), and high-carbohydrate diets, whereas in WAT its regulation depends on PPAR-γ, sirtuin 1 (SIRT1), and fast/refeeding regimens (16). Intriguingly, a difference in mRNA expression level between patients with and without obesity was found in VAT, but not in Subcutaneous AT (SAT) (11). Consequently, only VAT seems to be implied in FGF-21-regulated pathways in obesity. In this study, the direct correlations between WC and FPG, ALT, GGT, and TG, suggest that the VAT-derived adipokines and signaling factors could indeed drive diabetes onset and development and NAFLD pathogenesis, as previously reported (36, 37). In the analysed samples the inverse correlation between GGT and WC becomes stronger when FGF-21 levels increased, suggesting that FGF-21 is higher in patients with a more severe condition of fatty liver and impaired metabolism.
The inverse correlations between HDL-c levels and either WC or BMI confirmed what we have previously shown in a cohort of metabolic patients (38). HDL particles are implied in reverse cholesterol transport (RCT), conveying cholesterol from peripheral tissues to the liver, a crucial process to prevent atherosclerosis (39). In the current study, there was no significant increase in circulating FGF-21 level in patients with atheromatous plaque however FGF-21 inversely correlated with HDL. In line with previously reported data (12, 40, 41), this study shows not only an inverse relationship between FGF-21 and HDL-c but also a direct correlation between HDL-c and Vitamin D levels, as we previously reported (42), thus supporting the hypothesis that FGF-21-driven putative protective role against diabetes and obesity may depend on normal Vitamin D and HDL-cholesterol levels. For these reasons, for the first time, we went further and evaluated the relation between FGF-21 and 25-OH Vitamin D. In the analysed cohort, 25-OH Vitamin D showed a significant inverse correlation with FGF-21 levels. Vitamin D is mainly stored in AT, slowly released in the systemic circulation during fasting periods and regulates adipogenesis (43). Furthermore, this hormone is implicated in the modulation of genes involved in cholesterol homeostasis via the activation of Vitamin D Receptor (VDR) and its serum levels are negatively associated to higher WC and inflammation (44). A recent systematic review and meta-analysis has shown that Vitamin D may be considered an adiponectin secretagogue in patients with diabetes (45). Serum adiponectin levels are positively associated with 25-OH Vitamin D levels and HDL, and negatively correlates with inflammatory markers, FPG, TG, LDL (46). Vitamin D supplementation increased adiponectin serum levels in diabetic patients ameliorating HbA1c and BMI (47). Adiponectin is critical for FGF-21 glycemic and insulin sensitizing effects. Indeed, FGF-21 stimulates adiponectin secretion in rodents while adiponectin-knockout mice are refractory to changes in energy expenditure evoked by FGF-21 administration (48, 49). Significant inverse correlations between FGF-21 concentrations and adiponectin and HDL cholesterol were already observed (33) but if Vitamin D may explain, mediate or being a consequence of this relationship has never been explored. Vitamin D involvement in FGF-21 pathway should not be unexpected considering that 1,25-OH Vitamin D activates nuclear receptor VDR and increases FGF-23 production in bones (21). FGF-23 belongs to the same family of FGF-21 and acts as an endocrine nexus between hormones and mineral ions with the result of preventing hyperphosphatemia and hyper-vitaminosis. Consequently, pinpointing FGF-21 interaction with other hormones, such as adiponectin, may help our understanding about its involvement in metabolic pathways.
The FGF21 paradox lays its foundation on the finding that although counteracting metabolic derangement, high levels of this hormone are observed in obese and dysmetabolic subjects. It has been speculated that FGF-21 production could represent a response of the organism to cope with dysmetabolism caused by obesity and MetS (50). Consequently, the higher, although not significantly, total serum FGF-21 concentration in diabetics could potentially be the result of a compensatory mechanism to metabolic disturbances or tissue resistance to FGF-21 activity. In fact, previous findings about increased total serum FGF21 levels could putatively be ascribed to a coping mechanism trying to overcome its impaired biological function in obese patients according to two possible mechanisms: FGF21 receptors dysfunctional activation (51) and/or increased FAP enzymatic cleavage activity. Our results showing that intact FGF-21 levels are not correlated with waist circumference, Vitamin D and HDL-c, differently from total serum FGF-21 levels, suggests the fact that functional FGF-21 does not necessarily relate with obesity and metabolic features. This is in line with hypothesis that those subjects might have increased total FGF-21 but not functional FGF-21 that therefore does not predict the dysmetabolic conditions. Overall, from a clinical point of view, measurement of intact functional serum form of FGF-21 will help clinicians to identify those patients who could eventually benefit from therapies aiming to increase the hormone level in serum as well as treatments increasing endogenous functional level of FGF-2, using DPP-IV or FAP inhibitors. For instance, the association of fibrate and a FAP inhibitor may offer an oral therapy to augment endogenous FGF-21 actions (52) as well as sitagliptin, a DPP-IV inhibitor, has been found to inhibit FAP-activity and increase intact FGF-21 (53). Moreover, despite enduring controversy, lifestyle and pharmacological anamnesis should potentially be considered when characterizing patients since physical exercise and drugs have been suggested to affect FGF-21 levels.
In conclusions, our newly calculated cut-off of total FGF-21 according to visceral adiposity identified subjects with fasting hyperglycemia, and visceral adiposity appears to be responsible for increased levels of total FGF-21, although this does not necessarily translate into an increased hormonal biological activity, since levels of intact functional FGF-21 hormone are not related to abdominal obesity.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Azienda Ospedaliero-Universitaria Policlinico di Bari (Bari, Italy). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization, AM; methodology-visualization, LC; software-formal analysis, LC; lab methodology, OG-I, MP, NS, MF, RG; investigation, LC, MF, GP, PS; resources, LC, RG, MF, AM; data curation, LC; writing—original draft preparation, LC, RG, MC; writing—review and editing, AM; supervision, AM; project administration, AM; funding acquisition, AM. All authors contributed to the article and approved the submitted version.
Funding
AM is funded by EU-JPI HDL-INTIMIC –MIUR FATMAL; MIUR-PON “R&I” 2014–2020 “BIOMIS” cod.ARS01_01220; POR Puglia FESR—FSE 2014– 2020, “INNOMA” cod. 4TCJLV4; National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3 - Call for tender No. 341 of 15 March 2022 of Italian Ministry of University and Research funded by the European Union – NextGenerationEU; Award Number: Project code PE00000003, Concession Decree No. 1550 of 11 October 2022 adopted by the Italian Ministry of University and Research, CUP D93C22000890001, Project title “ON Foods - Research and innovation network on food and nutrition Sustainability, Safety and Security – Working ON Foods”.
Acknowledgments
We thank the physicians and nurses of the Unità Operativa Complessa Universitaria di Medicina Interna “Cesare Frugoni” of the Azienda Ospedaliero—Universitaria Policlinico di Bari for their help and support during the study. A special thanks to Roberta Le Donne for her support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1159127/full#supplementary-material
References
1. Itoh N, Ornitz DM. Functional evolutionary history of the mouse fgf gene family. Dev Dyn (2008) 237:18–27. doi: 10.1002/dvdy.21388
2. Goetz R, Beenken A, Ibrahimi OA, Kalinina J, Olsen SK, Eliseenkova AV, et al. Molecular insights into the klotho-dependent, endocrine mode of action of fibroblast growth factor 19 subfamily members. Mol Cell Biol (2007) 27:3417–28. doi: 10.1128/MCB.02249-06
3. Flippo KH, Potthoff MJ. Metabolic messengers: FGF21. Nat Metab (2021) 3:309–17. doi: 10.1038/s42255-021-00354-2
5. Zhen EY, Jin Z, Ackermann BL, Thomas MK, Gutierrez JA. Circulating FGF21 proteolytic processing mediated by fibroblast activation protein. Biochem J (2016) 473:605–14. doi: 10.1042/BJ20151085
6. Dunshee DR, Bainbridge TW, Kljavin NM, Zavala-Solorio J, Schroeder AC, Chan R, et al. Fibroblast activation protein cleaves and inactivates fibroblast growth factor 21. J Biol Chem (2016) 291:5986–96. doi: 10.1074/jbc.M115.710582
7. Angelin B, Larsson TE, Rudling M. Circulating fibroblast growth factors as metabolic regulators–a critical appraisal. Cell Metab (2012) 16:693–705. doi: 10.1016/j.cmet.2012.11.001
8. Hsuchou H, Pan W, Kastin AJ. The fasting polypeptide FGF21 can enter brain from blood. Peptides (2007) 28:2382–6. doi: 10.1016/j.peptides.2007.10.007
9. Porflitt-Rodríguez M, Guzmán-Arriagada V, Sandoval-Valderrama R, Tam CS, Pavicic F, Ehrenfeld P, et al. Effects of aerobic exercise on fibroblast growth factor 21 in overweight and obesity. A systematic review. Metab (2022) 129:155137. doi: 10.1016/j.metabol.2022.155137
10. Qian Z, Zhang Y, Yang N, Nie H, Yang Z, Luo P, et al. Close association between lifestyle and circulating FGF21 levels: a systematic review and meta-analysis. Front Endocrinol (2022) 13:984828. doi: 10.3389/fendo.2022.984828
11. Mraz M, Bartlova M, Lacinova Z, Michalsky D, Kasalicky M, Haluzikova D, et al. Serum concentrations and tissue expression of a novel endocrine regulator fibroblast growth factor-21 in patients with type 2 diabetes and obesity. Clin Endocrinol (Oxf) (2009) 71:369–75. doi: 10.1111/j.1365-2265.2008.03502.x
12. Lee Y, Lim S, Hong E-S, Kim JH, Moon MK, Chun EJ, et al. Serum FGF21 concentration is associated with hypertriglyceridaemia, hyperinsulinaemia and pericardial fat accumulation, independently of obesity, but not with current coronary artery status. Clin Endocrinol (2014) 80:57–64. doi: 10.1111/cen.12134
13. Wang Y-S, Ye J, Cao Y-H, Zhang R, Liu Y, Zhang S-W, et al. Increased serum/plasma fibroblast growth factor 21 in type 2 diabetes mellitus: a systematic review and meta-analysis. Postgrad Med J (2019) 95:134–9. doi: 10.1136/postgradmedj-2018-136002
14. Solomon TPJ, Carter S, Haus JM, Karstoft K, von Holstein-Rathlou S, Nielsen MS, et al. Plasma FGF21 concentrations are regulated by glucose independently of insulin and GLP-1 in lean, healthy humans. PeerJ (2022) 10:e12755. doi: 10.7717/peerj.12755
15. Lakhani I, Gong M, Wong WT, Bazoukis G, Lampropoulos K, Wong SH, et al. Fibroblast growth factor 21 in cardio-metabolic disorders: a systematic review and meta-analysis. Metabolism (2018) 83:11–7. doi: 10.1016/j.metabol.2018.01.017
16. Cicione C, Degirolamo C, Moschetta A. Emerging role of fibroblast growth factors 15/19 and 21 as metabolic integrators in the liver. Hepatology (2012) 56:2404–11. doi: 10.1002/hep.25929
17. Huang W, Zhang J, Zou J, Wang X, Xu H, Guan J, et al. Fibroblast growth factor 21 is an independent predictor of prevalent and incident obstructive sleep apnea. iScience (2023) 26:105985. doi: 10.1016/j.isci.2023.105985
18. Kliewer SA, Mangelsdorf DJ. Fibroblast growth factor 21: from pharmacology to physiology. Am J Clin Nutr (2010) 91:254S–7S. doi: 10.3945/ajcn.2009.28449B
19. Lenart-Lipińska M, Matyjaszek-Matuszek B, Gernand W, Nowakowski A, Solski J. Serum fibroblast growth factor 21 is predictive of combined cardiovascular morbidity and mortality in patients with type 2 diabetes at a relatively short-term follow-up. Diabetes Res Clin Pract (2013) 101:194–200. doi: 10.1016/j.diabres.2013.04.010
20. Dutchak PA, Katafuchi T, Bookout AL, Choi JH, Yu RT, Mangelsdorf DJ, et al. Fibroblast growth factor-21 regulates PPARγ activity and the antidiabetic actions of thiazolidinediones. Cell (2012) 148:556–67. doi: 10.1016/j.cell.2011.11.062
21. Degirolamo C, Sabbà C, Moschetta A. Therapeutic potential of the endocrine fibroblast growth factors FGF19, FGF21 and FGF23. Nat Rev Drug Discov (2016) 15:51–69. doi: 10.1038/nrd.2015.9
22. Harrison SA, Ruane PJ, Freilich B, Neff G, Patil R, Behling C, et al. A randomized, double-blind, placebo-controlled phase IIa trial of efruxifermin for patients with compensated NASH cirrhosis. JHEP Rep (2023) 5:100563. doi: 10.1016/j.jhepr.2022.100563
23. Gaich G, Chien JY, Fu H, Glass LC, Deeg MA, Holland WL, et al. The effects of LY2405319, an FGF21 analog, in obese human subjects with type 2 diabetes. Cell Metab (2013) 18:333–40. doi: 10.1016/j.cmet.2013.08.005
24. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult treatment panel III). JAMA (2001) 285:2486–97. doi: 10.1001/jama.285.19.2486
25. American Diabetes Association. 2. classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care (2021) 44:S15–33. doi: 10.2337/dc21-S002
26. Qureshi AI, Alexandrov AV, Tegeler CH, Hobson RW, Dennis Baker J, Hopkins LN, et al. Guidelines for screening of extracranial carotid artery disease: a statement for healthcare professionals from the multidisciplinary practice guidelines committee of the American society of neuroimaging; cosponsored by the society of vascular and interventional neurology. J Neuroimaging (2007) 17:19–47. doi: 10.1111/j.1552-6569.2006.00085.x
27. Umberger TS, Sloan JH, Chen J, Cheng C, Siegel RW, Qian Y, et al. Novel sandwich immunoassays for the measurement of total and active FGF21. Bioanalysis (2014) 6:3283–93. doi: 10.4155/bio.14.241
28. Lewis JE, Ebling FJP, Samms RJ, Tsintzas K. Going back to the biology of FGF21: new insights. Trends Endocrinol Metab (2019) 30:491–504. doi: 10.1016/j.tem.2019.05.007
29. Gälman C, Lundåsen T, Kharitonenkov A, Bina HA, Eriksson M, Hafström I, et al. The circulating metabolic regulator FGF21 is induced by prolonged fasting and PPARα activation in man. Cell Metab (2008) 8:169–74. doi: 10.1016/j.cmet.2008.06.014
30. Ren F, Huang J, Dai T, Gan F. Retrospective analysis of factors associated with serum levels of fibroblast growth factor-21 in patients with diabetes. Ann Palliat Med (2021) 10:3258–66. doi: 10.21037/apm-21-525
31. Akduman F, Şıklar Z, Özsu E, Doğan Ö, Kır MK, Berberoğlu M. Fibroblast growth factor 21 levels and bone mineral density in metabolically healthy and metabolically unhealthy obese children. J Clin Res Pediatr Endocrinol (2022) 14:433–43. doi: 10.4274/jcrpe.galenos.2022.2022-1-15
32. Karamfilova V, Assyov Y, Nedeva I, Gateva A, Ivanova I, Cherkezov I, et al. Fibroblast growth factor 21 as a marker of prediabetes in patients with non-alcoholic fatty liver disease. Turk J Gastroenterol (2022) 33:233–9. doi: 10.5152/tjg.2021.201165
33. Matuszek B, Lenart-Lipińska M, Duma D, Solski J, Nowakowski A. Evaluation of concentrations of FGF-21 - a new adipocytokine in type 2 diabetes. Endokrynol Pol (2010) 61:50–4.
34. Mashili FL, Ramaiya K, Lutale J, Njelekela M, Francis F, Zierath J, et al. Adiposity is a key correlate of circulating fibroblast growth factor-21 levels in African males with or without type 2 diabetes mellitus. J Obes (2018) 2018:1–8. doi: 10.1155/2018/7461903
35. Dushay J, Chui PC, Gopalakrishnan GS, Varela-Rey M, Crawley M, Fisher FM, et al. Increased fibroblast growth factor 21 in obesity and nonalcoholic fatty liver disease. Gastroenterology (2010) 139:456–63. doi: 10.1053/j.gastro.2010.04.054
36. Liu C, Feng X, Li Q, Wang Y, Li Q, Hua M. Adiponectin, TNF-α and inflammatory cytokines and risk of type 2 diabetes: a systematic review and meta-analysis. Cytokine (2016) 86:100–9. doi: 10.1016/j.cyto.2016.06.028
37. Polyzos SA, Aronis KN, Kountouras J, Raptis DD, Vasiloglou MF, Mantzoros CS. Circulating leptin in non-alcoholic fatty liver disease: a systematic review and meta-analysis. Diabetologia (2016) 59:30–43. doi: 10.1007/s00125-015-3769-3
38. Crudele L, De Matteis C, Piccinin E, Gadaleta RM, Cariello M, Di Buduo E, et al. Low HDL-cholesterol levels predict hepatocellular carcinoma development in individuals with liver fibrosis. JHEP Rep (2023) 5:100627. doi: 10.1016/j.jhepr.2022.100627
39. Härdfeldt J, Cariello M, Simonelli S, Ossoli A, Scialpi N, Piglionica M, et al. Abdominal obesity negatively influences key metrics of reverse cholesterol transport. Biochim Biophys Acta Mol Cell Biol Lipids (2022) 1867:159087. doi: 10.1016/j.bbalip.2021.159087
40. Nar G, Cetin S, Nar R, Kilic O, Furkan O, Gunver G, et al. Is serum fibroblast growth factor 21 associated with the severity or presence of coronary artery disease? J Med Biochem (2022) 41:162–7. doi: 10.5937/jomb0-30191
41. Wang Y, Si S, Liu J, Wang Z, Jia H, Feng K, et al. The associations of serum lipids with vitamin d status. PloS One (2016) 11:e0165157. doi: 10.1371/journal.pone.0165157
42. De Matteis C, Crudele L, Cariello M, Battaglia S, Piazzolla G, Suppressa P, et al. Monocyte-to-HDL ratio (MHR) predicts vitamin d deficiency in healthy and metabolic women: a cross-sectional study in 1048 subjects. Nutrients (2022) 14:347. doi: 10.3390/nu14020347
43. Narvaez CJ, Simmons KM, Brunton J, Salinero A, Chittur SV, Welsh JE. Induction of STEAP4 correlates with 1,25-dihydroxyvitamin d 3 stimulation of adipogenesis in mesenchymal progenitor cells derived from human adipose tissue: VITAMIN d, STEAP4 AND ADIPOGENESIS. J Cell Physiol (2013) 228:2024–36. doi: 10.1002/jcp.24371
44. Abbas MA. Physiological functions of vitamin d in adipose tissue. J Steroid Biochem Mol Biol (2017) 165:369–81. doi: 10.1016/j.jsbmb.2016.08.004
45. Nikooyeh B, Neyestani TR. Can vitamin d be considered an adiponectin secretagogue? a systematic review and meta-analysis. J Steroid Biochem Mol Biol (2021) 212:105925. doi: 10.1016/j.jsbmb.2021.105925
46. Udomsinprasert W, Manoy P, Yuktanandana P, Tanavalee A, Anomasiri W, Honsawek S. Decreased serum adiponectin reflects low vitamin d, high interleukin 6, and poor physical performance in knee osteoarthritis. Arch Immunol Ther Exp (2020) 68:16. doi: 10.1007/s00005-020-00580-8
47. Nikooyeh B, Hollis BW, Neyestani TR. The effect of daily intake of vitamin d-fortified yogurt drink, with and without added calcium, on serum adiponectin and sirtuins 1 and 6 in adult subjects with type 2 diabetes. Nutr Diabetes (2021) 11:26. doi: 10.1038/s41387-021-00168-x
48. Holland WL, Adams AC, Brozinick JT, Bui HH, Miyauchi Y, Kusminski CM, et al. An FGF21-adiponectin-ceramide axis controls energy expenditure and insulin action in mice. Cell Metab (2013) 17:790–7. doi: 10.1016/j.cmet.2013.03.019
49. Lin Z, Tian H, Lam KSL, Lin S, Hoo RCL, Konishi M, et al. Adiponectin mediates the metabolic effects of FGF21 on glucose homeostasis and insulin sensitivity in mice. Cell Metab (2013) 17:779–89. doi: 10.1016/j.cmet.2013.04.005
50. Cariello M, Moschetta A. Fibroblast growth factor 21: a new liver safeguard: cariello and moschetta. Hepatology (2014) 60:792–4. doi: 10.1002/hep.27147
51. Hong ES, Lim C, Choi HY, Lee YK, Ku EJ, Moon JH, et al. Plasma fibroblast growth factor 21 levels increase with ectopic fat accumulation and its receptor levels are decreased in the visceral fat of patients with type 2 diabetes. BMJ Open Diabetes Res Care (2019) 7:e000776. doi: 10.1136/bmjdrc-2019-000776
52. Sonoda J, Chen MZ, Baruch A. FGF21-receptor agonists: an emerging therapeutic class for obesity-related diseases. Horm Mol Biol Clin Investig (2017) 30(2):20170002. doi: 10.1515/hmbci-2017-0002
Keywords: visceral obesity, HDL cholesterol, intact FGF21, waist circumference, vitamin D
Citation: Crudele L, Garcia-Irigoyen O, Cariello M, Piglionica M, Scialpi N, Florio M, Piazzolla G, Suppressa P, Sabbà C, Gadaleta RM and Moschetta A (2023) Total serum FGF-21 levels positively relate to visceral adiposity differently from its functional intact form. Front. Endocrinol. 14:1159127. doi: 10.3389/fendo.2023.1159127
Received: 06 February 2023; Accepted: 29 May 2023;
Published: 20 June 2023.
Edited by:
Ana Luísa De Sousa-Coelho, Algarve Biomedical Center Research Institute (ABC-RI), PortugalReviewed by:
Thomas Bobbert, Charité University Medicine Berlin, GermanyMette Bjerre, Aarhus University, Denmark
Copyright © 2023 Crudele, Garcia-Irigoyen, Cariello, Piglionica, Scialpi, Florio, Piazzolla, Suppressa, Sabbà, Gadaleta and Moschetta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raffaella Maria Gadaleta, cmFmZmFlbGxhLmdhZGFsZXRhQHVuaWJhLml0; Antonio Moschetta, YW50b25pby5tb3NjaGV0dGFAdW5pYmEuaXQ=
†These authors share first authorship
‡These authors have contributed equally to this work and share senior authorship