 Denise H. van Abswoude1,2,3,4
Denise H. van Abswoude1,2,3,4 Karlijn Pellikaan1,2,3,4
Karlijn Pellikaan1,2,3,4 Naomi Nguyen1
Naomi Nguyen1 Anna G. W. Rosenberg1,2,3,4Kirsten Davidse1,2,3,4Franciska M. E. Hoekstra1,5
Anna G. W. Rosenberg1,2,3,4Kirsten Davidse1,2,3,4Franciska M. E. Hoekstra1,5 Ilse M. Rood6Christine Poitou7,8,9
Ilse M. Rood6Christine Poitou7,8,9 Graziano Grugni8,9,10
Graziano Grugni8,9,10 Charlotte Høybye8,9,11,12
Charlotte Høybye8,9,11,12 Tania P. Markovic8,13,14
Tania P. Markovic8,13,14 Assumpta Caixàs8,15,16Antonino Crinò8,17,18
Assumpta Caixàs8,15,16Antonino Crinò8,17,18 Sjoerd A. A. van den Berg1,19
Sjoerd A. A. van den Berg1,19 Aart J. van der Lely1,2,4Laura C. G. de Graaff1,2,3,4,9*
Aart J. van der Lely1,2,4Laura C. G. de Graaff1,2,3,4,9*- 1Department of Internal Medicine, Division of Endocrinology, Erasmus Medical Center, University Medical Center Rotterdam, Rotterdam, Netherlands
- 2Center for Adults with Rare Genetic Syndromes, Department of Internal Medicine, Division of Endocrinology, Erasmus Medical Center, University Medical Center Rotterdam, Rotterdam, Netherlands
- 3Dutch Center of Reference for Prader–Willi Syndrome, Rotterdam, Netherlands
- 4Academic Center for Growth Disorders, Erasmus Medical Center, University Medical Center Rotterdam, Rotterdam, Netherlands
- 5Internal Medicine, Division of Nephrology, Reinier de Graaf Gasthuis, Delft, Netherlands
- 6Department of Nephrology, Radboud University Medical Center, Radboud Institute for Health Sciences, Nijmegen, Netherlands
- 7Assistance Publique-Hôpitaux de Paris, Rare Diseases Center of Reference ‘Prader-Willi Syndrome and Obesity with Eating Disorders’ (PRADORT), Nutrition Department, Institute of Cardiometabolism and Nutrition (ICAN), Pitié-Salpêtrière Hospital, Sorbonne Université, National Institute of Health and Medical Research (INSERM), Nutriomics, Paris, France
- 8International Network for Research, Management & Education on adults with Prader-Willi Syndrome (INfoRMEd-PWS)
- 9European Reference Network on Rare Endocrine Conditions (ENDO-ERN)
- 10Division of Auxology, Istituto Auxologico Italiano, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Piancavallo, Italy
- 11Department of Molecular Medicine and Surgery, Karolinska Institute and Karolinska University Hospital, Stockholm, Sweden
- 12Department of Endocrinology, Karolinska Institute and Karolinska University Hospital, Stockholm, Sweden
- 13Metabolism & Obesity Service, Royal Prince Alfred Hospital, Camperdown, NSW, Australia
- 14Charles Perkins Center and Sydney Medical School, University of Sydney, Sydney, NSW, Australia
- 15Department of Endocrinology and Nutrition, Parc Tauli Hospital Universitari, Institut d’Investigació i Innovació Parc Taulí (I3PT) Instituto de Salud Carlos III (CERCA-ISCIII), Sabadell, Spain
- 16Department of Medicine, Universitat Autònoma de Barcelona, Sabadell, Spain
- 17Reference Center for Prader-Willi syndrome, Bambino Gesù Hospital, Research Institute, Palidoro, Italy
- 18Center for Rare Diseases and Congenital Defects, Fondazione Policlinico Universitario A. Gemelli, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy
- 19Department of Clinical Chemistry, Erasmus Medical Center (MC), University Medical Center Rotterdam, Rotterdam, Netherlands
Background: Prader-Willi syndrome (PWS) is a rare, complex, genetic disorder characterized by hyperphagia, hypotonia, delayed psychomotor development, low muscle mass and hypothalamic dysfunction. Adults with PWS often have obesity, hypertension and type 2 diabetes mellitus (DM2), known risk factors for cardiovascular disease (CVD) and chronic kidney disease (CKD). Early symptoms of CVD and CKD may be masked by intellectual disability and inability to express physical complaints. Furthermore, kidney diseases are often asymptomatic. Therefore, renal and cardiovascular disease might be missed in patients with PWS. Microalbuminuria is an early sign of microvascular damage in the kidneys and other vascular beds. Therefore, we screened our adult PWS cohort for the presence of elevated urinary albumin and (micro)albuminuria.
Methods: We retrospectively collected anthropometric measurements, blood pressure, medical history, medication use, urine dipstick and biochemical measurements form electronic patient files. In addition, we performed a systematic literature review on kidney disease in PWS.
Results: We included 162 adults with genetically confirmed PWS (56% male, median age 28 years), of whom 44 (27%) had DM2. None had known CVD. All subjects had normal estimated glomerular filtration rate (eGFR) according to non-PWS reference intervals. Elevated urinary albumin or (micro)albuminuria was present in 28 (18%); 19 out of 75 (25%) had an increased urinary albumin-to-creatinine ratio (UACR) and 10 out of 57 (18%) had an increased urinary protein-to-creatinine ratio. Elevated urinary albumin was present at a young age (median age 26 (IQR 24-32) years) and was associated with an significantly higher BMI and LDL-cholesterol levels and higher prevalence of DM2, hypertension and dyslipidemia than those with normal UACR (p=0.027, p=0.019, p<0.001, p<0.001, p=0.011 and respectively).
Conclusion: Upon screening, one in every five adults with PWS had increased urinary albumin or (micro)albuminuria, early signs of microvascular disease. All had normal eGFR, according to non-PWS reference intervals, and none had a formal diagnosis of CVD. As muscle mass is low in PWS, creatinine levels and eGFR may be spuriously normal. Urinalysis in this patient group can be used as a screening tool for microvascular (kidney) disease. We propose an algorithm for the detection and management of microvascular disease in adults with PWS.
Introduction
Prader-Willi syndrome (PWS) is a complex, genetic, neurodevelopmental disorder caused by loss of expression of a cluster of paternally expressed genes on chromosome 15q11-13 (1). In most cases, this syndrome is caused by a paternal deletion (60-70%) or a maternal uniparental disomy (mUPD, 25-35%). Less common genetic findings include imprinting center defects (ICD, 1-3%), balanced translocations (0.1%) and gene mutations (<0.1%) (1, 2).
During early infancy, PWS is characterized by hypotonia and failure to thrive due to a poor sucking reflex and lethargy (1, 3, 4). In childhood, motor development is delayed and adults often show muscle weakness and decreased muscle mass (5–7).In both children and adults, hypothalamic dysfunction often results in pituitary hormone deficiencies, such as hypogonadism (estimated in 98% in males and 94% in females), growth hormone deficiency and hypothyroidism (estimated prevalence of 14-17%) (1, 8–14). Especially in patients without growth hormone treatment (GHt) (1, 15–19), basal metabolic rate (BMR) is low due to low lean body mass and reduced physical activity. The combination of low BMR and hyperphagia leads to an increased risk of obesity (42% of adults with PWS) (20). This high prevalence of obesity, in turn, leads to an increase in the prevalence of DM2 (17%), hypertension (18%) and hypercholesterolemia (19%) (20). These are known risk factors for cardiovascular disease (CVD) (20) and chronic kidney disease (CKD) (21–23).
With improved healthcare for patients with PWS, life expectancy has increased. As patients with PWS become older, age-related diseases like CVD and CKD become increasingly relevant. Early detection and treatment are crucial to prevent complications, loss of quality of life and early mortality (24, 25).
As symptoms are often atypical, non-specific or even absent (26–29), the detection of CKD can be challenging. In patients with PWS, the detection of CVD and CKD might be even more complicated due to the presence of intellectual disability (mild in the majority of patients) and reduced ability to express physical complaints (30, 31). Furthermore, patients with PWS have a high pain threshold that might mask the sudden thoracic pain or headache that may indicate cardiac or cerebrovascular events. The lack of fever and pain in people with PWS can also mask other risk factors for CKD, including chronic urinary tract infections (UTIs) (1, 8, 32, 33) that may further increase the risk of CKD (34). Although never investigated, CKD and CVD might be more difficult to detect due to the combination of physical, behavioral, and neurocognitive potentially increasing morbidity and mortality in adults with PWS.
CKD can be diagnosed based on a decreased (estimated) glomerular filtration rate (eGFR) and the presence of (micro)albuminuria (35). (Micro)albuminuria can be defined as an increased urinary albumin-to-creatinine ratio (UACR) or urinary protein-to-creatinine ratio (UPCR) and is associated with an increased mortality independent of the eGFR (36, 37). Preferably, the UACR should be assessed in first morning urine samples as it corresponds more closely with a 24-hour urine collection, which is the golden standard (35, 38, 39). Microalbuminuria can indicate microvascular injury and is therefore a risk factor for CKD and CVD (40–42). In patients with diabetes mellitus, microalbuminuria is predictive of early mortality (43). Besides (micro)albuminuria, an increase in the exertion of low molecular weight (LMW) proteins such as cystatine-C, ubiquitin, retinol binding protein or alpha1-microglobulin, might also indicate kidney disease (44–46).
Little is known about CKD and CVD in the general population of adults with PWS, as these co-morbidities have only been studied in specific ‘subtypes’ of patients with PWS. In hospitalized patients with PWS, the prevalence of CKD was estimated to be 6.5% (47). In PWS patients with DM, microalbuminuria was found in 6.9-55.6% and proteinuria in 3.4-11.1% of (48–50), which is similar to the prevalence in the general population with DM (51). Apart from these studies in PWS ‘subpopulations’ of hospitalized and/or diabetic PWS patients, microalbuminuria and proteinuria have not been systematically assessed in the broader adult PWS population. This lack of information is relevant, as both microalbuminuria and proteinuria are associated with an increased risk of CKD and cardiovascular morbidity and mortality (40–42, 52–56). Also, to our knowledge, systematic screening for kidney disease (by both urine and serum analysis) has never been performed in adults with PWS. As a result, there are no guidelines for screening and treatment of CKD in adults with PWS.
To fill this knowledge gap, we have systematically screened urine and serum samples for signs of CKD in a cohort of adults with PWS. We also assessed risk factor for CKD and performed a systematic literature review on kidney and urinary tract disease in PWS. Based on our cohort study and systematic review, we provide practical recommendations for the screening and treatment of (micro)albuminuria and CKD in patients with PWS.
Method
This international cross-sectional study was performed at the Center for Adults with Complex Rare Genetic Syndromes (CRGS) at the Erasmus University Medical Center, Rotterdam, the Netherlands, the Rare Disease Center of reference ‘Prader-Willi Syndrome and obesity with eating disorders’, in Paris, France and the Division of Auxology in Piancavallo, Italy. Only adults with genetically confirmed PWS who visited the outpatient clinic of one of these reference center between January 2020 and December 2022 were included. Urinalysis was part of a routine systematic health screening in all included PWS patients. Ethical approval and/or individual informed consent was obtained by the Medical Ethics Committee of participating centers according to local rules and regulations.
As previously described (20), the systematic screening generally consists of a structured interview, an extensive physical examination, a medical questionnaire (depending on local guidelines), a review of medical records and biochemical measurements. The systematic screening took place during the first or follow-up visit to the outpatient clinic. If measurements could not be done during the first visit (due to behavioral or logistic issues), the next available measurement was used for the statistical analysis, provided that the time interval between first and follow up visit was less than 12 months.
Height and weight measurements were collected from medical records. When multiple measurements were available, we included the measurement the was closest (in time) to the biochemical and urinalysis. A Body Mass Index (BMI, in kg/m2) between 18.5 and 24.9 kg/m2 was considered lean, between 25.0 and 29.9 kg/m2 overweight, 30.0 or more kg/m2 obese and a BMI of 40.0 or more grade III obesity according to the World Health Organization Criteria (57).
Resting blood pressure was measured in all patients during their routine visit to the outpatient clinic. In the Dutch cohort, blood pressure was measured using a Mindray sphygmomanometer with trueBP™ technology. If the blood pressure was above 140/90 mmHg (58), the measurement was repeated. If the blood pressure was still elevated, a 30-minute automated blood pressure measurement was carried out. The most recent blood pressure was included in the analysis. As patients with PWS in the Dutch reference center were not evaluated yearly for substance abuse (smoking, alcohol), most recent data were included. However, in some cases, this was more than twelve months prior to blood and urine sample collection.
Biochemical analysis
Blood and midstream urine samples were collected for general medical screening. As the outpatient clinic was often in the afternoon and fasting can be problematic in PWS due to hyperphagia, non-fasting blood samples were used. We evaluated kidney function (urea, creatinine, eGFR using Chronic Kidney Disease Epidemiology Collaboration (CKD-epi) calculation) and lipid profiles ((non-fasting) low density lipoprotein (LDL)-cholesterol, high density (HDL)-cholesterol, triglycerides, total cholesterol), glucose metabolism (fasting or random glucose, hemoglobin A1c (HbA1c)) in blood. In random spot urine samples, we measured microalbumin, urinary albumin-to-creatinine ratio (UACR), total protein and/or urinary protein-to-creatinine ratio (UPCR). As the outpatient clinic was in the afternoon in some centers, first morning urine samples were not available. If microalbuminuria was found, the patients were referred to the general practitioner to confirm microalbuminuria in a second urine sample. Second samples were not available for this study. A urine dipstick was used to evaluate the presence of glucose, protein, leukocytes, and nitrite. If urine and blood samples could not be collected on the same day, the blood samples with the shortest time to urinalysis were used. If urine and blood samples were collected more than 12 months apart, the blood sample was excluded from analysis.
Cut-off levels
DM2 was defined as a fasting glucose of 7.0 mmol/L or higher (if available) or a repeated non-fasting glucose above 11.1 mmol/L. As fasting glucose were only available in a few patients, non-fasting glucoses were used in further analysis. Impaired glucose tolerance was tested using an oral glucose tolerance test and diagnosed if measured serum glucoses was between 7.8 to 11.1 mmol/L after two hours according to the American Diabetes Association classification (59). HbA1c was not used as a diagnostic criterium for DM2, but was used to monitor glycemic control. Furthermore, patients with a previous diagnosis of DM2 were considered as having DM2. Hypercholesterolemia was defined as a non-fasting LDL-cholesterol above 4.1 mmol/L and dyslipidemia was defined as a non-fasting LDL-cholesterol above 4.1 mmol/L or a (non-fasting or fasting) triglyceride above 2.0 mmol/L (60). The CKD-epi formula was used to calculate the estimated glomerular filtration rate (eGFR) values (61). An eGFR >90 mL/min was defined as normal kidney function. Microalbumin was considered elevated when >0.02 g/L (measured in one random spot urine sample). Microalbuminuria was defined as an UACR between 3 and 30 mg/mmol creatinine and proteinuria as an UACR >30 mg/mmol creatinine according to the Kidney Disease: Improving Global Outcomes (KDIGO) guideline (35). Proteinuria was defined as an UPCR of >20 mg/mmol creatinine (0.2 mg/mg) and nephrotic proteinuria as an UPCR of >300 mg/mmol creatinine (3.0 mg/mg) (62). Urinary total protein levels >0.15 g/L in a24 hour urine collection were considered elevated. An albumin excretion rate of 30-300mg/24 hours was considered increased and >300 mg/24 hours was considered severely increased or nephrotic proteinuria (35). When leukocytes and/or nitrite was positive in urine dipstick analysis, patients were referred to their general practitioner for urine culture and, if positive, (antibiotic) treatment.
Systematic literature review
We performed a literature search in June 2020 (updated in March 2022) using Embase, Medline, the Web of Science Core Collection, Cochrane Central Register of Controlled Trials and Google Scholar (Table S1). Studies were assessed for eligibility using the PRISMA 2020 (63) guideline and were included if they reported on both 1) (the prevalence of) kidney disease, urological abnormalities, treatment for kidney disease or markers for kidney function and 2) PWS, Prader-Willi-like syndrome (PWLS) with an abnormality in 15q11.2-13 or one of the genes on the PWS critical region. We also scanned the references of included articles. Studies reporting on cases of kidney or urological cancer, combinations of PWS with other genetic syndromes, PWLS with a deletion extending beyond the PWS critical region and articles only describing the expression of a gene in the kidney were excluded. Meeting reports, workshop summaries, reviews, conference abstracts, guidelines, articles without full-text availability and articles that were not available in English were also excluded.
Screening based on title and abstract was performed independently by three reviewers (either NN and KP or DA and KP). Full-text screening was performed independently by DA and KP. Disagreements were resolved in a meeting with a third reviewer (LG). Data was extracted by DA and NN.
Data analysis
Data was analyzed using IBM SPSS version 28.0. Continuous variables are presented as median [interquartile range (IQR)], dichotomous variables as number and percentage of patients n (%). To investigate the association between microalbuminuria, macroalbuminuria and the presence of risk factors (e.g. smoking, alcohol usage, DM2, blood pressure/hypertension and hypercholesterolemia), a Chi-squared test was used for dichotomous variables and a Mann-Whitney U test for continuous variables. A p-value of <0.05 was considered statistically significant. To adjust for BMI as possible confounder, a logistic regression analysis was performed.
Results
We included 162 adults with PWS. Baseline characteristics are displayed in Table 1. Median age at urinalysis was 28 [IQR 22-38] years. Ninety out of 162 patients were male (56%). Most patients had a deletion as the underlying genotype (n=102 (63%)), followed by mUPD (n=52 (32%)) and ICD in 1%. In six patients, PWS was genetically confirmed, but the genotype was unknown or unspecified. Sixty-seven percent of patients had received GHt, 65% received GHt during childhood and 56% were currently using GHt. The median BMI was 33.0 [IQR 26.8-41.0] kg/m2 and 60% of subjects had obesity. Grade III obesity was present in 47 of 97 (48.5%) of patients with obesity. Forty-four (27%) patients were diagnosed with DM2 and 17out of 162 (11%) had IGT. Hypertension and hypercholesterolemia were present in 29 (18%) and 23 patients (14%) respectively. In the French cohort, dyslipidemia was present in 37%. None of the patients were diagnosed with cardiovascular events (myocardial infarction or CVA).
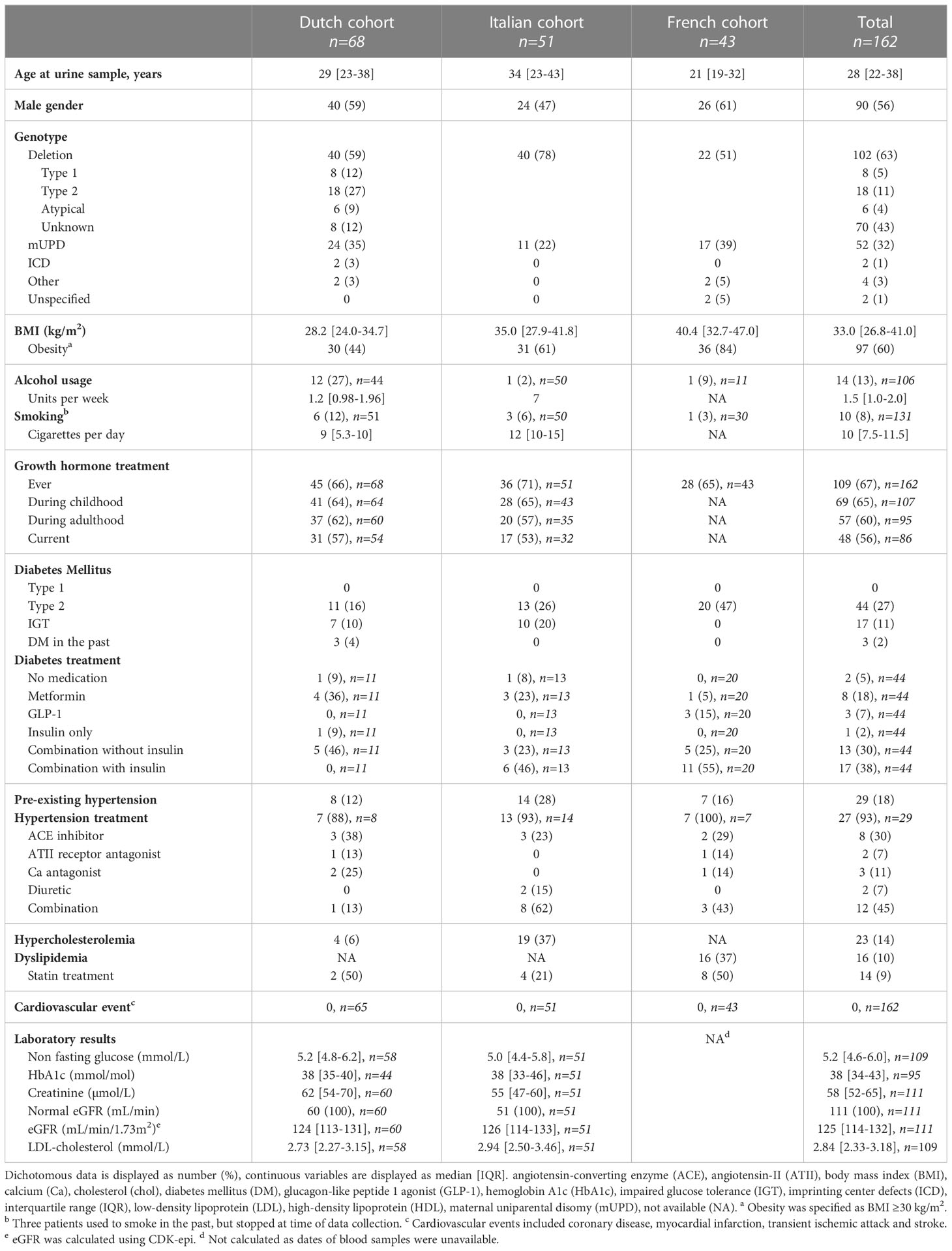
Table 1 Baseline characteristics of included adults with PWS.
In eight Dutch and all French patients, urine samples were present without recent blood samples (i.e. <12 months between urine and blood sample collection). Of the patients with available recent blood samples, all had normal eGFR (CKD-EPI eGFR >90 mL/min/1.73m2). Median eGFR (CDK-epi) was 125 [IQR 114-132] mL/min/1.73m2. In males, median creatinine was 61 [IQR 54-69] µmol/L (reference value 65-115 µmol/L) and eGFR was 127 [IQR 118-135] mL/min/1.73m2. In females, median creatinine levels were 55 [IQR 47-61] µmol/L (reference value 55-90 µmol/L) and eGFR was 120 [IQR 111-128] mL/min/1.73m2. All patients were classified as CKD stage G1 (35). When applying previously suggested alternative reference values for eGFR for adults with PWS (>98 ml/min/1.73m2 in males and >93 ml/min/1.73m2 in females) (20) renal function of only two males and two females were below the reference value (94 and 98 ml/min/1.73m2 in males and 90 and 92 ml/min/1.73m2 in females respectively).
Urinalysis
Microalbuminuria and proteinuria
Twenty-eight out of 160 patients (18%) had elevated urine albumin, microalbuminuria or proteinuria (Table 2). Two patients were excluded from this analysis as data on (micro)albuminuria, proteinuria, UACR and UPCR were missing. Of the two males and two females with impaired renal function according to alternative reference values for eGFR for adults with PWS, only one female had microalbuminuria (Case 8, Table 3) (20).
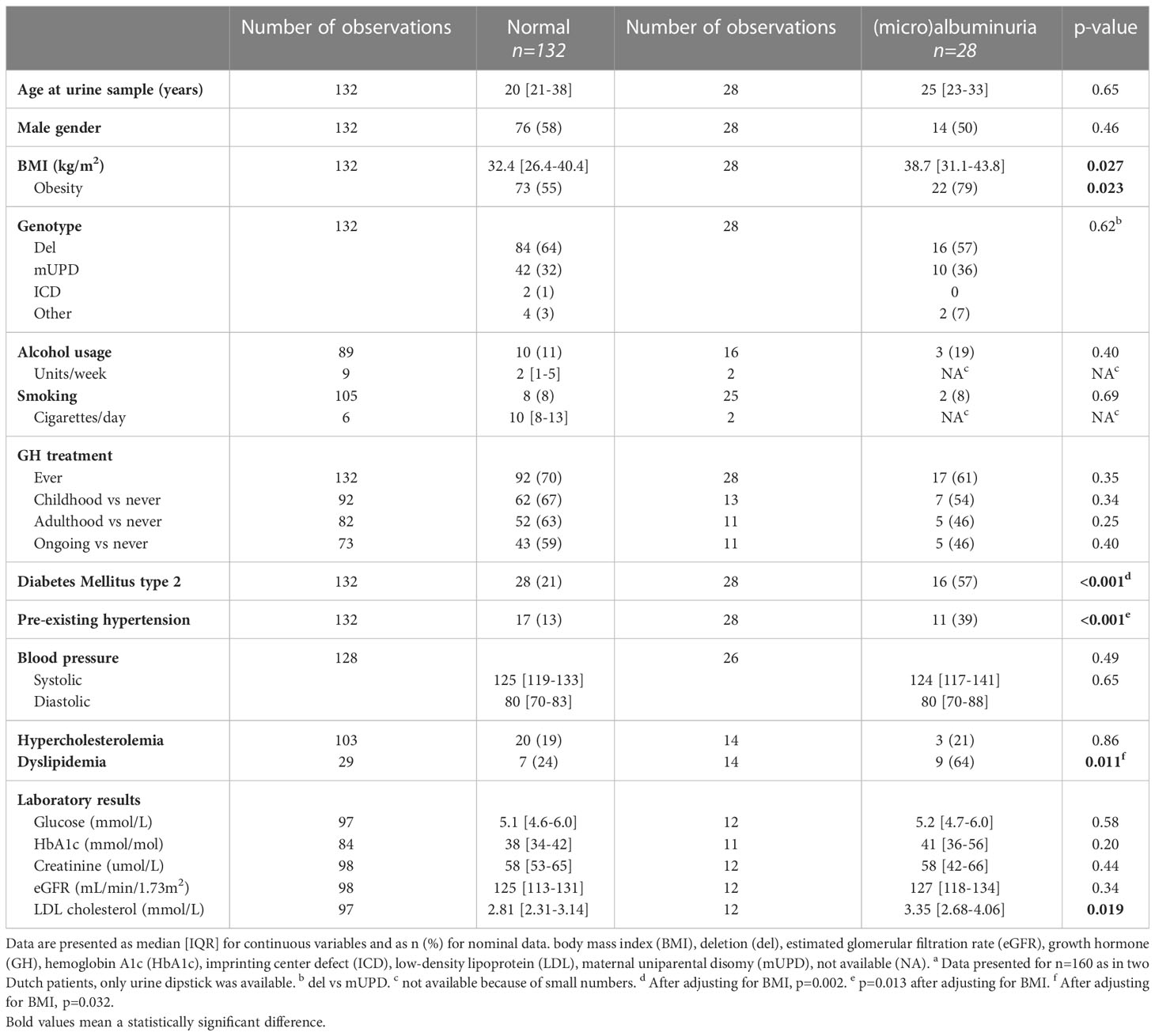
Table 2 Comparison of adults with PWS and normal versus (micro)albuminuriaa.
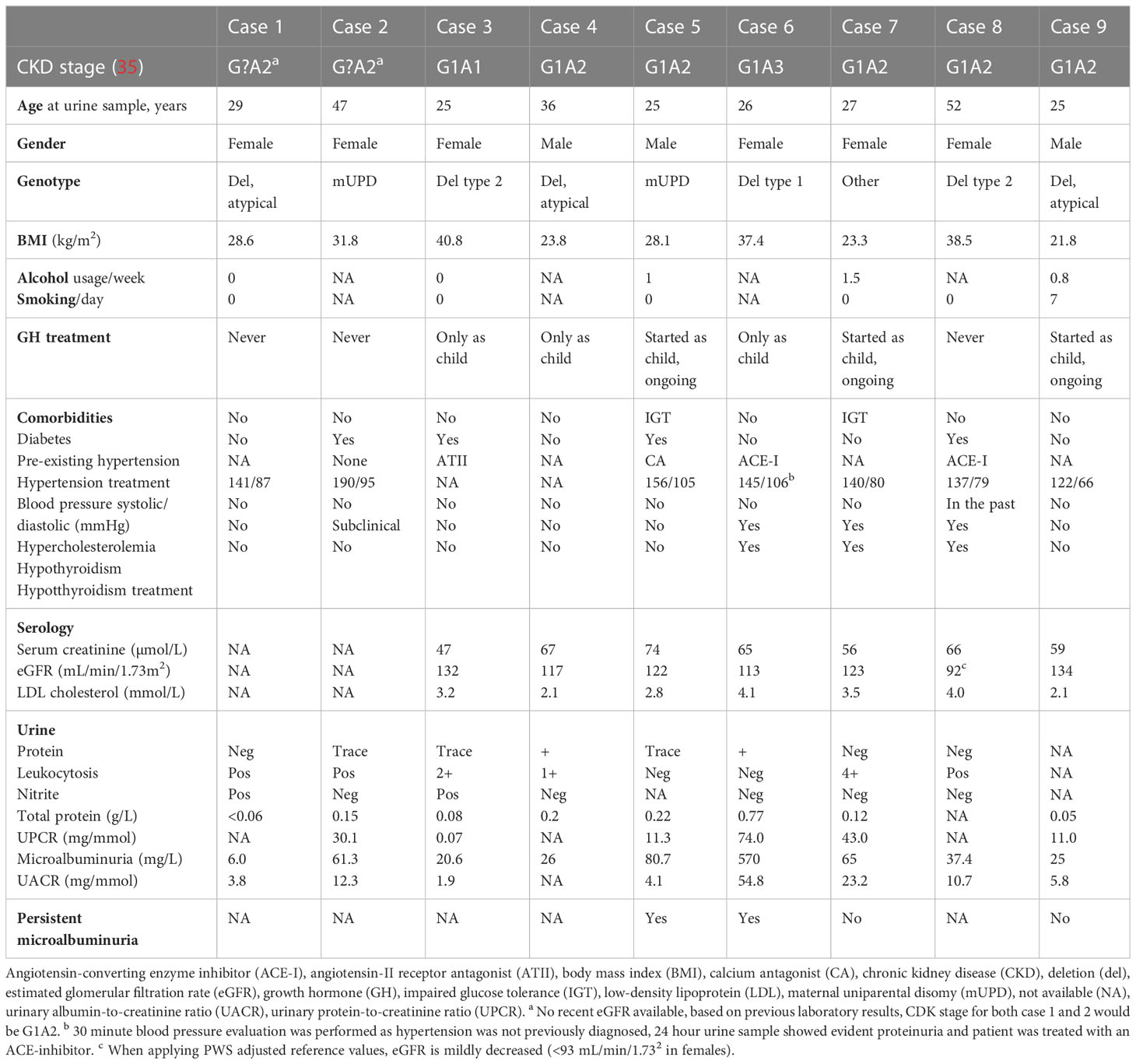
Table 3 Clinical characteristics and laboratory results of nine Dutch adults with PWS and microalbuminuria or elevated UACR.
Urine albumin was elevated in 24 of 157 subjects (15%). The UACR was calculated in 75 patients, as urine creatinine was not systematically assessed in all patients, and was abnormal in 19 of 75 patients (25%), of whom 15 had microalbuminuria and four had macroalbuminuria. UPCR was available for 57 patients, of whom ten (18%) had proteinuria and one nephrotic proteinuria (i.e. 460 mg/mmol).
We did not find any association between elevated urine microalbumin or (micro)albuminuria and age, gender, genotype, GH treatment, alcohol consumption or smoking (Table 2). Three of 28 patients with normal BMI, three of 37 who were overweight and 22 of 95 with obesity had elevated urine microalbumin or (micro)albuminuria. Patients with elevated urine microalbumin or (micro)albuminuria had significantly higher BMI (38.7 vs 32.4 kg/m2, p=0.027) and obesity was more prevalent (22 out of 28 (79%) vs 73 of 132 (55%), p=0.023). DM2 and hypertension were more prevalent in those with elevated urine microalbumin or (micro)albuminuria than without (57% vs 21%, p<0.001 and 39% vs 13%, p<0.001 respectively). After adjusting for BMI as possible confounder, these variables remained significantly associated with elevated urine microalbumin or (micro)albuminuria (p=0.02 and p=0.013 respectively). Laboratory results on glucose, HbA1c, creatinine, eGFR did not differ significantly between the patients with and without elevated urine microalbumin or (micro)albuminuria. However, LDL cholesterol was significantly higher in those with elevated urine microalbumin or (micro)albuminuria than those without (3.35 [2.68-4.06] vs 2.81 [2.31-3.14], p=0.019).
Characteristics, comorbidities, and laboratory results of the Dutch patients with elevated urine microalbumin or UACR are shown in Table 3. In the Dutch cohort, six out of nine (67%) patients with elevated UACR or UPCR also had leukocyturia and in two subjects, nitrite was also positive. Patients with both leukocyturia and nitrite in the urine sample were advised to have their urine checked for urinary tract infection at the general practitioner. Two patients had transient microalbuminuria or proteinuria (Table 3), one of them had leukocytosis at dipstick analysis. Neither had hypertension. Two other Dutch patients had microalbuminuria/proteinuria that persisted after repeating the urine sample. In one case (case 6) a 24-hour urine sample was collected that showed an elevated total protein of 0.56g/24h). A 30-minute blood pressure measurement at home was carried out, which showed systolic and diastolic hypertension. During analysis of hypertension, psychosocial stress turned out to be a strong contributing factor. This patient was referred to our neuropsychologist for psychosocial support and stress management. In addition, an angiotensin-converting enzyme (ACE) inhibitor was prescribed.
Leukocyturia in the Dutch cohort
Urine dipstick in the Dutch cohort was positive for leukocytes in 18 of 55 (33%) patients and nitrite in two of 54 (4%). In males, leukocyturia was seen in four of 33 patients (12%, and there was 1+ protein in two, 2+ protein in one and amount unknown in one patient). In females, 14 out of 22 (64%) had leukocyturia with 1+ protein in two, 2+ protein in four, 3+ protein in one, 4+ protein in two and amount unknown in five patients. As in the non-PWS population, leukocyturia was more prevalent in females than in males (p<0.001).
Glucosuria in the Dutch cohort
Urinary glucose was present in three out of 51 (6%) patients, all of whom had DM2 and were already on a treatment regime. Non-fasting (random) blood glucose levels of these patients ranged from 11.9 to 17.4 mmol/L and HbA1c from 62 to 70 mmol/mol, indicating suboptimal glucose management. None of them had proteinuria.
Systematic literature review
Forty-nine publications were included in the literature search (Figure 1). Multiple case reports have been published on patients with PWS and kidney disease. We found eight case reports describing proteinuria (64–71). There were three case reports in which albuminuria was reported in patients with PWS and DM2 (72–74). One article described a patient with stage 3 CKD (75). Five cases were found describing acute kidney injury (76–80) due to several different causes: pneumoperitoneum with abdominal compartment syndrome (76), secondary rhabdomyolysis caused by hyperpyrexia (77), nephrotoxic medication (78), hyperosmolar hyperglycemic state (79) and respiratory failure due to obesity hypoventilation syndrome (80). We found two case reports describing adults with PWS who needed hemodialysis due to end stage kidney disease, one patient from intrinsic nephrotic disease, the other case from uncontrolled diabetes mellitus (81, 82). Congenital renal or urological abnormalities, such as a horseshoe kidney, bilateral non-communicating paraurethral meatus, and absence of one kidney were also reported (83–85). Multiple UTI were reported in one case report (86) and a congenital disorder (megacystic-microcolon-intestinal hypoperistalsis syndrome) in another (87). Two articles reported on potential underlying genetic components: i) the NDN gene which is on the PWS region and ii) NIPA2, a gene not imprinted in patients with PWS that influences magnesium transportation, and that possibly reflects an association between kidney homeostasis or disease and PWS (88, 89). Three studies reported on the use of specific medications, such as ACE-inhibitors and (loop)diuretics, that could influence kidney function (90–92). One article mentioned the use of these drugs, without reporting on kidney function (90). In two other articles about these drugs, kidney function was normal (91, 92).
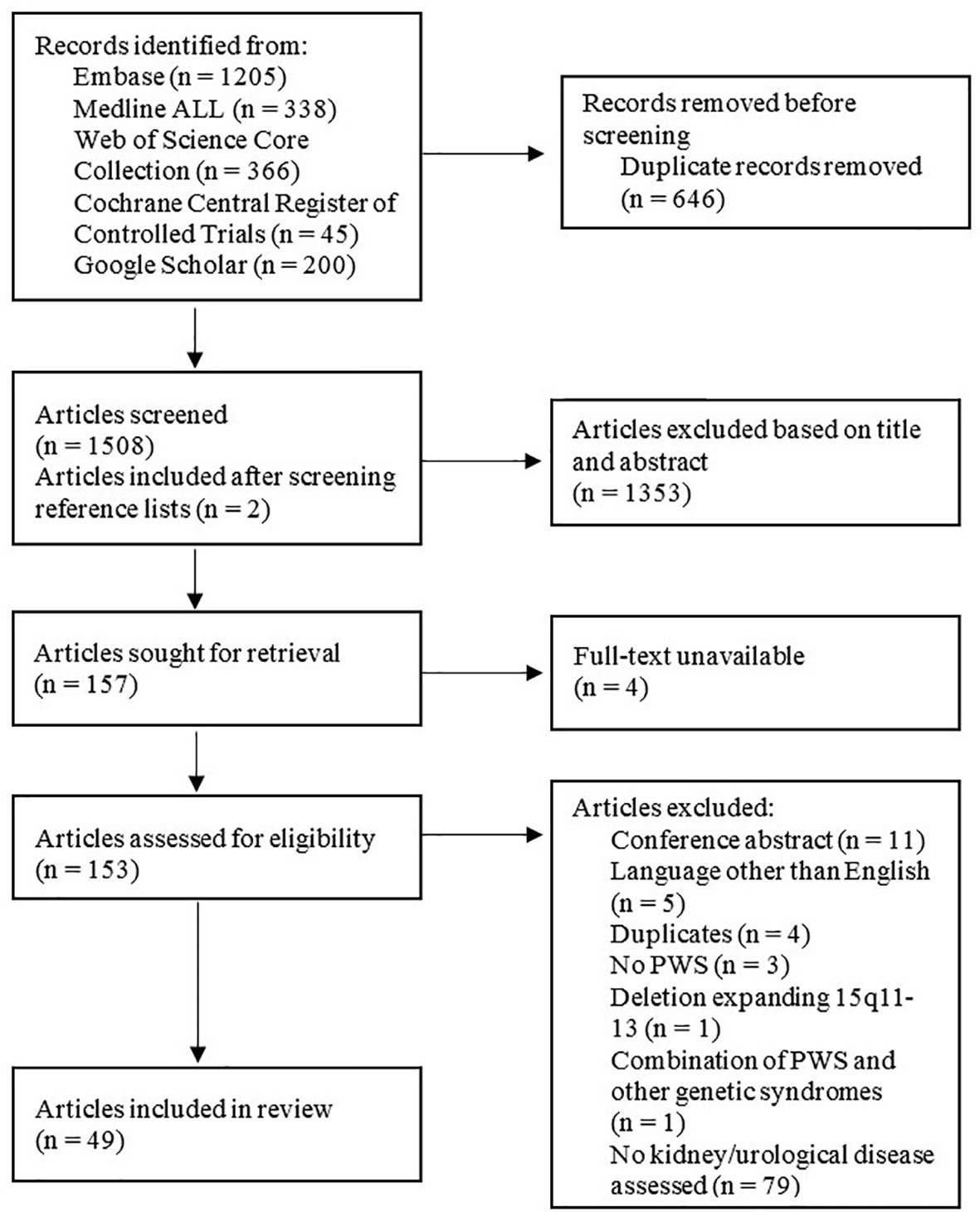
Figure 1 Systematic literature review (63).
Kidney disease
We found 16 studies reporting on kidney disease in patients with PWS (Table 4). Sinnema et al. (17) reported a prevalence of urinary tract problems or kidney disorders in 6% (six of 102 adults) with a confirmed diagnosis of PWS. In these patients, blood and urine analysis were performed based on a clinical suspicion of urine tract or kidney problems. Systematic screening of urine or blood samples was not performed in these patients.
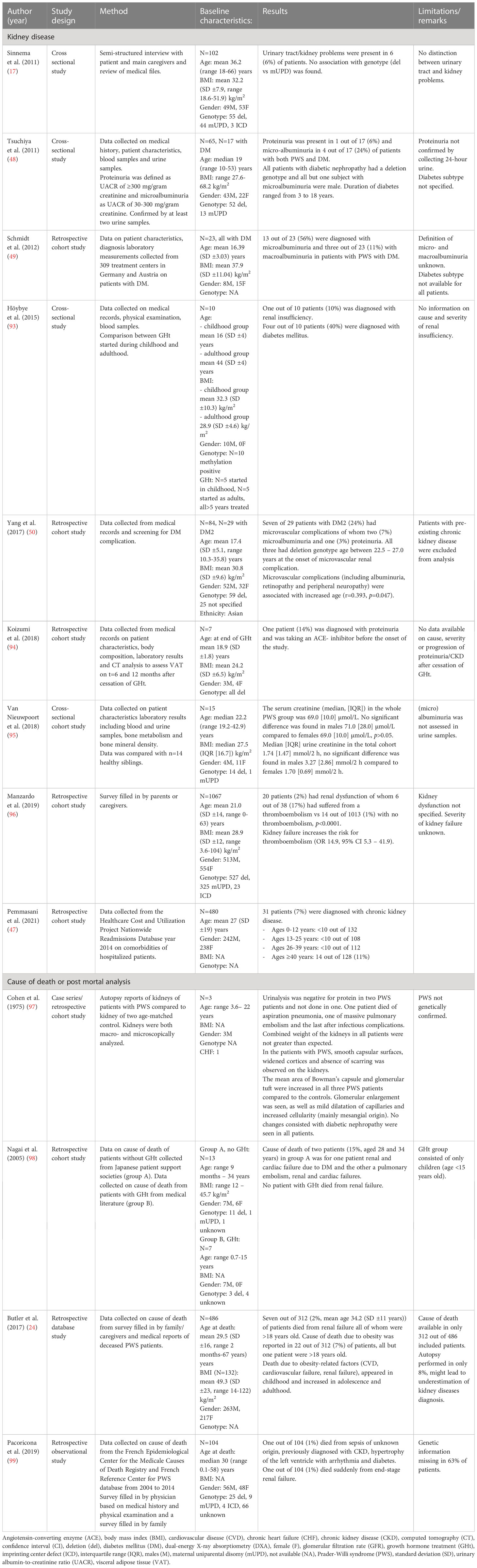
Table 4 Results of studies reporting on PWS and kidney diseases with more than one patients.
In patients with PWS and diabetes, three studies reported microalbuminuria (7-56%) or proteinuria (3-11%) (48–50). In 480 patients with PWS, Pemmasani et al. (47) reported a prevalence of CKD of 6.5% (31 patients), that increased with age. Renal insufficiency was reported by Höybye et al. (93) in one out of ten patients with PWS who were treated with GHt. Koizumi et al. studied body composition in seven patients with PWS, one of whom was diagnosed with proteinuria and was taking an ACE-inhibitor (94). Van Nieuwpoort et al. reported a median [IQR] serum creatinine in 15 patients of 69.0 [10.0] µmol/L with no significant difference between men and women. According to Manzardo et al. (96) renal dysfunction was more prevalent in patients with PWS who had been diagnosed with thromboembolism than those without (6 out of 34 (17%) vs 14 out of 1013 (1.4%), p<0.001).
Multiple studies have investigated causes of death in PWS. Cohen et al. (97) described autopsy results in three children with PWS in whom urinalysis was negative for proteinuria. The kidneys had normal weight but showed glomerular enlargement and dilatation of capillaries as well as increased cellularity compared to controls, suggesting hyperfiltration. Nagai et al. (98) compared 20 patients with PWS with (age range 0.7 to 15 years) and without (never received, age range 9 months to 34 years) GHt. In the group that did not receive GHt, two patients died from renal and cardiac failure, versus none in the GHt group. Two other studies investigating causes of death in PWS both found that 2% died with or because of CKD (24, 99).
Urological disorders, diseases and congenital anomalies of kidney and urinary tract
Results of studies reporting urological disorders in PWS are shown in Table 5. Torrado et al. (104) reported that five out of 180 (3%) patients with PWS had Congenital Anomalies of Kidney and Urinary Tract (CAKUT), which was significantly higher than in the general population (0.1-0.5%) (p<0.05). Malformations found included renal hypoplasia, ureteral duplication, bifid renal pelvis, vesicoureteral reflux, pelvicalyceal dilatation and ureteral valves (104). No association between genotype and reno-ureteral malformations was found (p=1.00). Sinnema et al. (101) found CAKUT (bilateral duplication of kidney and ureter system) in one of 12 patients and Pacilli et al. (105) found a horseshoe kidney in one of 33 patients.
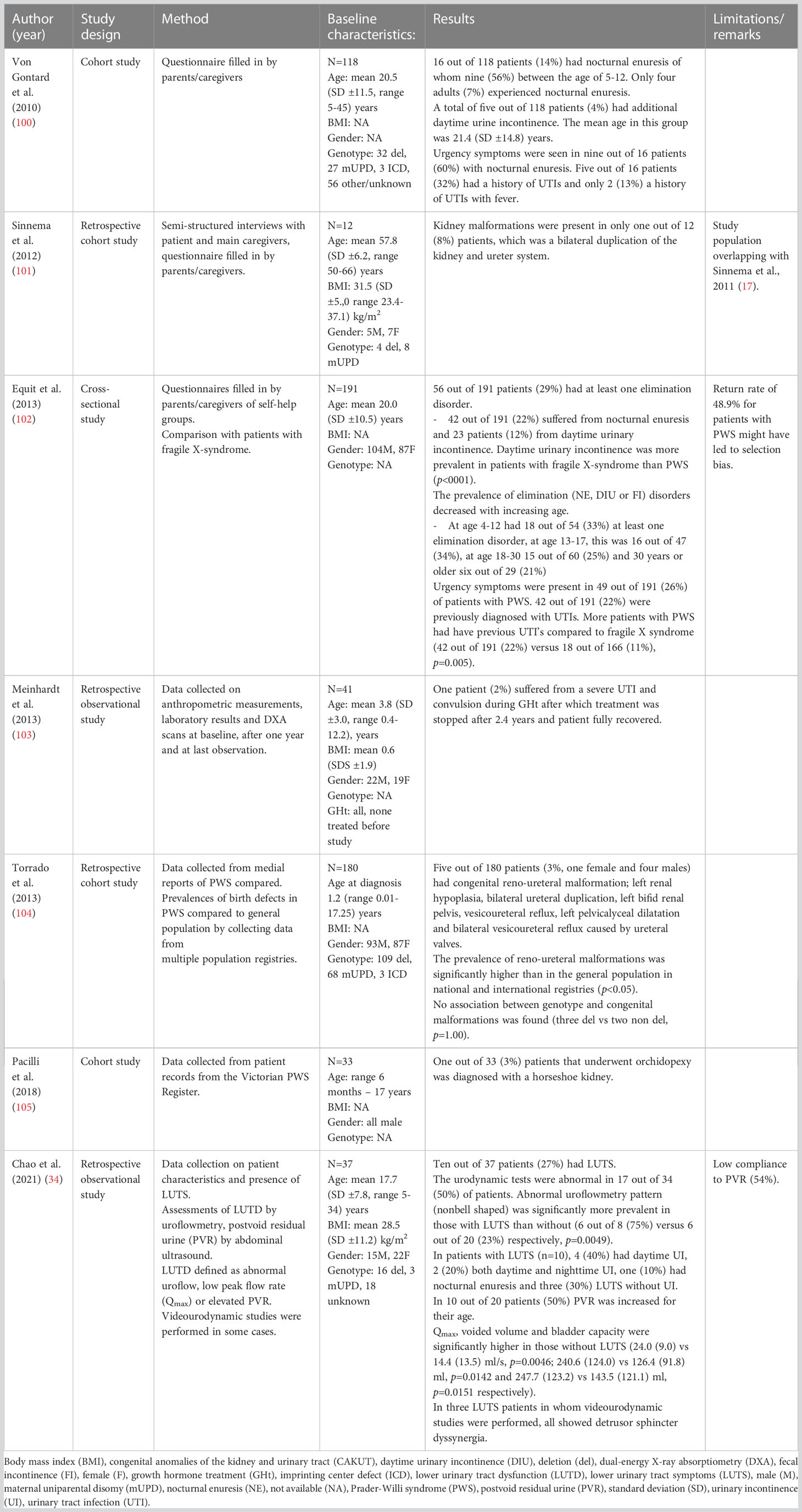
Table 5 Results of studies reporting on PWS and urological diseases, symptoms or congenital anomalies with more than one patients.
Nocturnal enuresis was described in 14-22% (100, 102). Two studies found a decrease in nocturnal enuresis with increasing age (100, 102). Daytime urinary incontinence was present in 3-12% (100, 102). Urgency symptoms, possibly related to overactive bladder, were reported in 26-60% of whom 22-32% had a history of UTI’s (100, 102).
Chao et al. (34) reported that urodynamic tests were abnormal in 17 out of 34 patients with PWS, with abnormal flowmetry in 12 out of 34 and elevated residual bladder volume in 10 out of 20. In patients with lower urinary tract symptoms (LUTS), peak flow rate, voided volume, and bladder capacity were significantly decreased compared to patients without LUTS.
Discussion
Our study in 162 adults with PWS showed that one in every five (young) adults had early signs of microvascular disease, measured by elevated urine microalbumin or (micro)albuminuria, while eGFR was normal. However, as muscle mass is low in PWS (6), creatinine levels and eGFR may be falsely ‘normal’. Our findings suggest that pre-symptomatic kidney injury may be missed when only blood measurements are performed. Therefore, in this patient group, urinalysis is essential for timely screening of microvascular (kidney) disease. We propose an algorithm for the detection and management of microvascular disease in adults with PWS.
Twenty-eight out of 160 (18%) patients had elevated urine albumin, (micro) albuminuria or proteinuria; eleven of whom were diagnosed with hypertension and sixteen with DM2. No age difference was found between patients with normal and elevated UACR.
In our literature review, we found an overall prevalence of microalbuminuria of 7-56% and macroalbuminuria of 3-11% in patients with PWS and diabetes (48–50). We did not find any studies on microalbuminuria or proteinuria in patients with PWS without DM2. Our study is the first to analyze the presence of (micro)albuminuria in patients with PWS with and without DM2. In the general population, around 25% of patients with longstanding (>10 years) DM2 have microalbuminuria and 5-20% proteinuria (51). Before antihypertensive treatment, patients with essential hypertension (in the general population) developed proteinuria in 35-65% and renal insufficiency in 33%, depending on severity of hypertension, DM2, medication, and age (106). In our cohort, 16 of 44 (36%) of patients with DM2 had (micro)albuminuria. Notably, the prevalence of albuminuria in our PWS patients without DM2 was similar to that in non-PWS patients with long-term DM2. The albuminuria in our PWS patients suggests microvascular damage is already present at a young age (23-33 years).
In this study, as in the normal population, albuminuria was associated with hypertension, DM2 and obesity. Obesity is associated with chronic kidney disease and glomerulosclerosis. A possible mechanism is hyperfiltration, which leads to albuminuria, regardless of the presence or absence of diabetes (107–110). Furthermore, obesity has been associated with increased progression of CKD (111).
In the general population, microalbuminuria is an indicator for microvascular injury, and a risk factor for both CKD and CVD (40–42, 53, 54). Although none of our patients was formally diagnosed with CVD, the presence of microalbuminuria might indicate latent CVD. Young adults with PWS often have cardiovascular risk factors including obesity (60%), DM2 (27%), hypertension (18%), smoking (8%) and hypercholesterolemia (14%) or dyslipidemia (10%). Timely and adequate follow-up of microalbuminuria and treatment of these risk factors might decrease cardiovascular and renal comorbidities and complications.
Clinical recommendations
Initial visit
During the initial visit, the physician should ask about previous UTIs and use of cigarettes and/or alcohol. In case of multiple UTIs, one should consider a kidney ultrasound to detect malformations, assess the post-void residual urine volume and referral to a urologist. In case of substance use, we advise to encourage cessation of smoking or alcohol usage. Furthermore, weight and blood pressure should be measured yearly. In case of hypertension, one should consider analysis to secondary causes such as stress, left ventricle hypertrophy or renal causes and manage both obesity and hypertension according to general guidelines.
Monitoring of eGFR
In our study, we showed that median creatinine levels were at the lower limit of the reference interval of the general (non-PWS) population in both male and female adults with PWS. This finding could be related to low muscle mass, which is decreased by 25 to 37% in patients with PWS (6), resulting in an overestimation of kidney function when measured by eGFR. The eGFR (calculated using the CKD-EPI) might therefore not be the optimal test to estimate kidney function in adults with PWS. We previously proposed alternative reference values of eGFR for adults with PWS (>98 ml/min/1.73m2 in males and >93 ml/min/1.73m2 in females) (20) to avoid underdiagnosis of CKD. Another method of assessing kidney injury is by measuring the excretion of LMW proteins, such as cystatine-C, retinol binding protein and alpha1-microglobulin. LMW proteins are filtered and reabsorbed by the kidneys. In kidney injury and (diabetic) proteinuria, an increased excretion of these proteins might be found in urine samples (44–46). Therefore, a more accurate methods of assessing kidney function in patients with PWS might include cystatin-C clearance adjusted for BMI (112, 113) or 24-hour urine creatinine measurement. However, multiple factors such as thyroid dysfunction and corticosteroid use might influence cystatin-C levels (114, 115). We therefore recommend yearly evaluation of creatinine and eGFR according to PWS-specific cut-off values and yearly urinalysis in all adults with PWS (see Figure 2) (20).
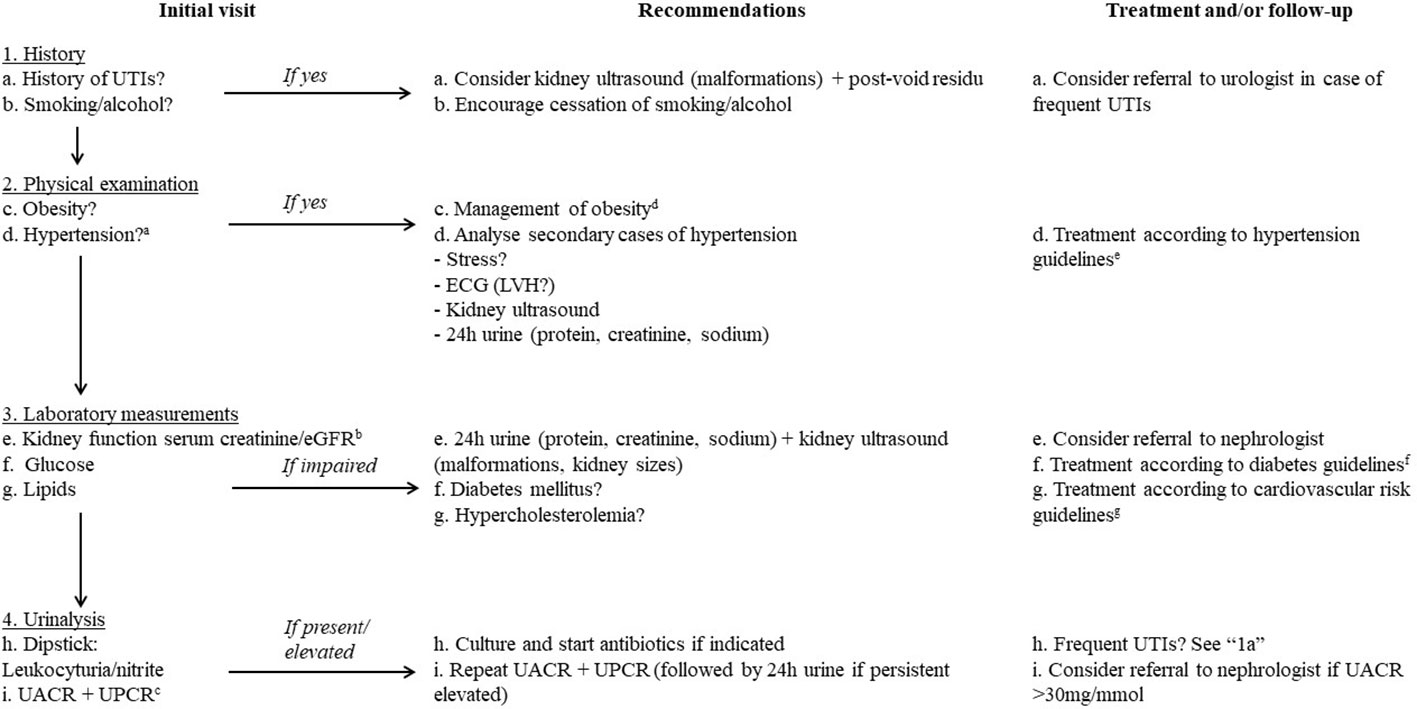
Figure 2 Recommendations for screening and the management for (micro)albuminuria and its risk factors in adults with PWS. angiotensin-converting enzyme inhibitor (ACE-I), angiotensin-II receptor antagonist (ATII) electrocardiogram (ECG), estimated glomerular filtration rate (eGFR), Left ventricular hypertrophy (LVH), minutes (min), urinary tract infection (UTI), urinary albumin-to-creatinine ratio (UACR), urinary protein-to-creatinine ratio (UPCR). a. Diagnosed by repeated measurements or 30-minute measurement. b. preferably in a first morning urine sample. c. Consider using adjusted reference values for adults with PWS (e.g. >98 ml/min/1.73m2 in males and >93 ml/min/1.73m2 in females) (20). d. Obesity in adults with PWS should be aggressively management with for example a hypocaloric diet, structured regular exercise and restriction of access to food. e. For example the 2018 ESC/ESH guidelines for the management of arterial hypertension (116). f. For example the 2019 ESC guidelines on diabetes (117). g. For example the ESC 2021 guideline (118) on cardiovascular disease prevention.
Laboratory measurements
We advise yearly evaluation of kidney function, glucose levels and lipids. If an impaired renal function is detected, additional investigation using a 24-hour urine and kidney ultrasound should be performed to identify the cause. In addition, a nephrologist could be consulted. A new diagnosis of diabetes or hypercholesterolemia should be managed according to non-PWS guidelines.
Detection of UTIs
Urgency symptoms (sudden need to pass urine with or without urine incontinence) and UTIs are common in adults with PWS, according to our literature review and previous study in our cohort (26-60% and 22-32%, respectively) (100, 102, 119). UTIs might be prevalent in adults with PWS related to obesity (120). Health care providers should be aware of the increased pain threshold and inability to mount a fever (due to disturbed temperature regulation) in patients with PWS (8, 32). This combination of features might lead to an atypical presentation of UTI (e.g. only changes in behavior), causing underdiagnosis of UTIs in this vulnerable patient population. If leukocytes and/or nitrite are positive, a urine culture should be performed and the patient should be treated with antibiotics if indicated.
Urinalysis for the detection of micro- or macroalbuminuria
We recommend performing urinalysis (midstream urinalysis using urine dipstick and measurement of UACR and UPCR) yearly in all adults with PWS. First morning urine samples are preferred over random urine samples to decrease the influence of orthostatic proteinuria (35). In those diagnosed with hypertension and DM2, we advise stringent control of blood pressure and glucose levels. In addition, we recommend performing urinalysis yearly, as per guidelines for DM2 and hypertension in the general population (116, 117).
In case of abnormalities, a second sample urinalysis should be performed. When microalbuminuria or proteinuria persists, 24-hour urine should be collected to calculate the 24 hour creatinine- and protein excretion. However, in people with of intellectual disability, collecting 24 hour urine might be challenging. In those with normal eGFR but elevated UACR or UPCR without a UTI, an renal ultrasound should be performed.
When proteinuria is confirmed, patients should be screened for underlying diseases and any risk factors should be treated. Cardiovascular status should be optimized and cardiovascular risk should be assessed. Referral to (or consultation with) a nephrologist should be considered. Those with progressive proteinuria should be referred to a nephrologist. In adults with PWS with albuminuria and hypertension, an ACE inhibitor or angiotensin-II receptor antagonist should be the first line of treatment due to their renoprotective effects (121). If obesity is present, a weight reducing regime should be started.
Strengths and limitations
As all studies, our study has strengths and limitations. This study is, to our knowledge, the first cohort study to systematically assess kidney function and urinalysis in adults with PWS. However, there are several limitations. Blood and urine samples were not always collected on the same day as the blood samples [and in eight Dutch and all French patients, blood results were not included in the statistical analysis due to the prolonged time interval between blood and urine samples (>12 months)]. As random spot urine samples were collected instead of first morning urine samples, the high prevalence of (micro)albuminuria might partly be caused by sample contamination, orthostatic proteinuria or physical exertion. Furthermore, microalbuminuria was not confirmed in a second sample as repeated samples were only available in four patients. In addition, as muscle mass might be low in patients with PWS, leading to a low serum creatinine, defining microalbuminuria by the UACR or UPCR might have led to an overestimation (6). Smoking and alcohol usage were not assessed yearly in some patients, and data could therefore have been out of date. Patients with leukocyturia or nitrites were first referred to their general practitioner for urine culture and UTI treatment if positive for infection, after which urinalysis was repeated. Therefore, the results of urine cultures were not available at our center. Urinalysis was not available in the entire cohort, which might have led to selection bias and a 24-hour urinalysis was only available in one patient. Additionally, patients were not routinely screened for CVD (e.g. by an ECG or cardiac ultrasound). Furthermore, this cohort consists of relatively young adults without cardiovascular events, though risk factors for CVD are present, which justifies urinalysis even in young patients with PWS. Prospective studies in a larger cohort are needed to overcome these limitations.
Conclusion
Upon screening, one in every five adults with PWS had elevated urine albumin or (micro)albuminuria which was already present at young age. All had normal eGFR according to non-PWS reference intervals. However, as muscle mass is low in PWS, normal creatinine levels and eGFR may overestimate kidney function in people with this syndrome. As kidney function may be overestimated when only measured by serum creatinine, renal problems may be missed when urinalysis is omitted. Routine screening for microalbuminuria may allow early intervention to avoid CVD and CKD. Health care providers should be aware of the increased risk for CKD and CVD in adults with PWS and should optimize treatment to reduce these risk factors. To prevent long-term complications and impaired quality of life, we provide an algorithm for the screening and management of micro-albuminuria and proteinuria in adults with PWS (Figure 2).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors on request, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Medical Ethics Commission of the Erasmus Medical Center, Rotterdam, the Netherlands. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
Conceptualization, KP, FH and LG. Methodology, KP and LG. Formal analysis, DA. Investigation, DA, NN. Resources, LG. Data curation, DA, NN, GG, CP. Writing—original draft preparation, DA. Writing—review and editing, all authors. Visualization: DA. Supervision, KP, LG and AL. Project administration, DA, KP and LG. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to thank Sabrina Meertens-Cunput from the Erasmus Medical University Library for developing and updating the search strategy for the literature review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1168648/full#supplementary-material
References
1. Cassidy SB, Schwartz S, Miller JL, Driscoll DJ. Prader-willi syndrome. Genet Med (2012) 14(1):10–26. doi: 10.1038/gim.0b013e31822bead0
2. Butler MG, Hartin SN, Hossain WA, Manzardo AM, Kimonis V, Dykens E, et al. Molecular genetic classification in prader-willi syndrome: a multisite cohort study. J Med Genet (2019) 56(3):149–53. doi: 10.1136/jmedgenet-2018-105301
3. Holm VA, Cassidy SB, Butler MG, Hanchett JM, Greenswag LR, Whitman BY, et al. Prader-willi syndrome: consensus diagnostic criteria. Pediatrics (1993) 91(2):398–402. doi: 10.1542/peds.91.2.398
4. Whittington J, Holland A, Webb T, Butler J, Clarke D, Boer H. Relationship between clinical and genetic diagnosis of prader-willi syndrome. J Med Genet (2002) 39(12):926–32. doi: 10.1136/jmg.39.12.926
5. Cassidy SB. Prader-willi syndrome. Curr Probl Pediatr (1984) 14(1):1–55. doi: 10.1016/0045-9380(84)90043-4
6. Reus L, Zwarts M, van Vlimmeren LA, Willemsen MA, Otten BJ, Nijhuis-van der Sanden MWG. Motor problems in prader–willi syndrome: a systematic review on body composition and neuromuscular functioning. Neurosci Biobehav Rev (2011) 35(3):956–69. doi: 10.1016/j.neubiorev.2010.10.015
7. Festen DAM, Wevers M, Lindgren AC, Böhm B, Otten BJ, Wit JM, et al. Mental and motor development before and during growth hormone treatment in infants and toddlers with prader–willi syndrome. Clin Endocrinol (2008) 68(6):919–25. doi: 10.1111/j.1365-2265.2007.03126.x
8. Angulo MA, Butler MG, Cataletto ME. Prader-willi syndrome: a review of clinical, genetic, and endocrine findings. J Endocrinol Invest (2015) 38(12):1249–63. doi: 10.1007/s40618-015-0312-9
9. Swaab DF. Prader-willi syndrome and the hypothalamus. Acta Paediatr Suppl (1997) 423:50–4. doi: 10.1111/j.1651-2227.1997.tb18369.x
10. Höybye C, Tauber M. Approach to the patient with prader-willi syndrome. J Clin Endocrinol Metab (2022) 107(6):1698–705. doi: 10.1210/clinem/dgac082
11. Pellikaan K, Ben Brahim Y, Rosenberg AGW, Davidse K, Poitou C, Coupaye M, et al. Hypogonadism in adult males with prader-willi syndrome-clinical recommendations based on a Dutch cohort study, review of the literature and an international expert panel discussion. J Clin Med (2021) 10(19):4361. doi: 10.3390/jcm10194361
12. Pellikaan K, Ben Brahim Y, Rosenberg AGW, Davidse K, Poitou C, Coupaye M, et al. Hypogonadism in women with prader-willi syndrome-clinical recommendations based on a Dutch cohort study, review of the literature and an international expert panel discussion. J Clin Med (2021) 10(24):5781. doi: 10.3390/jcm10194361
13. Pellikaan K, Snijders F, Rosenberg AGW, Davidse K, van den Berg SAA, Visser WE, et al. Thyroid function in adults with prader-willi syndrome; a cohort study and literature review. J Clin Med (2021) 10(17):3804. doi: 10.3390/jcm10173804
14. Iughetti L, Vivi G, Balsamo A, Corrias A, Crinò A, Delvecchio M, et al. Thyroid function in patients with prader-willi syndrome: an Italian multicenter study of 339 patients. J Pediatr Endocrinol Metab (2019) 32(2):159–65. doi: 10.1515/jpem-2018-0388
15. Diene G, Mimoun E, Feigerlova E, Caula S, Molinas C, Grandjean H, et al. Endocrine disorders in children with prader-willi syndrome–data from 142 children of the French database. Horm Res Paediatr (2010) 74(2):121–8. doi: 10.1159/000313377
16. Grugni G, Crino A, Bosio L, Corrias A, Cuttini M, De Toni T, et al. The Italian national survey for prader-willi syndrome: an epidemiologic study. Am J Med Genet A (2008) 146A(7):861–72. doi: 10.1002/ajmg.a.32133
17. Sinnema M, Maaskant MA, van Schrojenstein Lantman-de Valk HM, Caroline van Nieuwpoort I, Drent ML, Curfs LM, et al. Physical health problems in adults with prader-willi syndrome. Am J Med Genet Part A (2011) 155(9):2112–24. doi: 10.1002/ajmg.a.34171
18. Schoeller DA, Levitsky LL, Bandini LG, Dietz WW, Walczak A. Energy expenditure and body composition in prader-willi syndrome. Metabolism (1988) 37(2):115–20. doi: 10.1016/S0026-0495(98)90003-8
19. Butler MG, Theodoro MF, Bittel DC, Donnelly JE. Energy expenditure and physical activity in prader-willi syndrome: comparison with obese subjects. Am J Med Genet A (2007) 143A(5):449–59. doi: 10.1002/ajmg.a.31507
20. Pellikaan K, Rosenberg AGW, Kattentidt-Mouravieva AA, Kersseboom R, Bos-Roubos AG, Veen-Roelofs JMC, et al. Missed diagnoses and health problems in adults with prader-willi syndrome: recommendations for screening and treatment. J Clin Endocrinol Metab (2020) 105(12):e4671–87. doi: 10.1210/clinem/dgaa621
21. Whelton PK, Klag MJ. Hypertension as a risk factor for renal disease. review of clinical and epidemiological evidence. Hypertension (1989) 13(5 Suppl):I19–27. doi: 10.1161/01.hyp.13.5_suppl.i19
22. Trevisan R, Dodesini AR, Lepore G. Lipids and renal disease. J Am Soc Nephrol (2006) 17(4 Suppl 2):S145–7. doi: 10.1681/ASN.2005121320
23. Kovesdy CP, Furth SL, Zoccali C, World Kidney Day Steering C. Obesity and kidney disease: hidden consequences of the epidemic. Can J Kidney Health Dis (2017) 4:2054358117698669. doi: 10.1177/2054358117698669
24. Butler MG, Manzardo AM, Heinemann J, Loker C, Loker J. Causes of death in prader-willi syndrome: prader-willi syndrome association (USA) 40-year mortality survey. Gen Med (2017) 19(6):635–42. doi: 10.1038/gim.2016.178
25. Manzardo AM, Loker J, Heinemann J, Loker C, Butler MG. Survival trends from the prader-willi syndrome association (USA) 40-year mortality survey. Genet Med (2018) 20(1):24–30. doi: 10.1038/gim.2017.92
26. Dhondup T, Qian Q. Electrolyte and acid-base disorders in chronic kidney disease and end-stage kidney failure. Blood Purif (2017) 43(1-3):179–88. doi: 10.1159/000452725
27. Lehnhardt A, Kemper MJ. Pathogenesis, diagnosis and management of hyperkalemia. Pediatr Nephrol (2011) 26(3):377–84. doi: 10.1007/s00467-010-1699-3
28. Levy AR, Xing S, Brunelli SM, Cooper K, Finkelstein FO, Germain MJ, et al. Symptoms of secondary hyperparathyroidism in patients receiving maintenance hemodialysis: a prospective cohort study. Am J Kidney Dis (2020) 75(3):373–83. doi: 10.1053/j.ajkd.2019.07.013
29. Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet (2017) 389(10075):1238–52. doi: 10.1016/S0140-6736(16)32064-5
30. Roof E, Stone W, MacLean W, Feurer ID, Thompson T, Butler MG. Intellectual characteristics of prader–willi syndrome: comparison of genetic subtypes. J Intellectual Disability Res (2000) 44(1):25–30. doi: 10.1046/j.1365-2788.2000.00250.x
31. Yang L, Zhan GD, Ding JJ, Wang HJ, Ma D, Huang GY, et al. Psychiatric illness and intellectual disability in the prader-willi syndrome with different molecular defects–a meta analysis. PloS One (2013) 8(8):e72640. doi: 10.1371/journal.pone.0072640
32. Williams MS, Rooney BL, Williams J, Josephson K, Pauli R. Investigation of thermoregulatory characteristics in patients with prader-willi syndrome. Am J Med Genet (1994) 49(3):302–7. doi: 10.1002/ajmg.1320490312
33. Chu CM, Lowder JL. Diagnosis and treatment of urinary tract infections across age groups. Am J Obstet Gynecol (2018) 219(1):40–51. doi: 10.1016/j.ajog.2017.12.231
34. Chao T-C, Yang SSD, Chang S-J, Tsai L-P. High prevalence of lower urinary tract dysfunction in patients with prader–willi syndrome. Neurourol Urodyn (2021) 40(4):1063–8. doi: 10.1002/nau.24669
35. Stevens PE, Levin A, Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group M. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med (2013) 158(11):825–30. doi: 10.7326/0003-4819-158-11-201306040-00007
36. O'Hare AM, Hailpern SM, Pavkov ME, Rios-Burrows N, Gupta I, Maynard C, et al. Prognostic implications of the urinary albumin to creatinine ratio in veterans of different ages with diabetes. Arch Intern Med (2010) 170(11):930–6. doi: 10.1001/archinternmed.2010.129
37. Chang DR, Yeh HC, Ting IW, Lin CY, Huang HC, Chiang HY, et al. The ratio and difference of urine protein-to-creatinine ratio and albumin-to-creatinine ratio facilitate risk prediction of all-cause mortality. Sci Rep (2021) 11(1):7851. doi: 10.1038/s41598-021-86541-3
38. Saydah SH, Pavkov ME, Zhang C, Lacher DA, Eberhardt MS, Burrows NR, et al. Albuminuria prevalence in first morning void compared with previous random urine from adults in the national health and nutrition examination survey, 2009-2010. Clin Chem (2013) 59(4):675–83. doi: 10.1373/clinchem.2012.195644
39. Witte EC, Lambers Heerspink HJ, de Zeeuw D, Bakker SJ, de Jong PE, Gansevoort R. First morning voids are more reliable than spot urine samples to assess microalbuminuria. J Am Soc Nephrol (2009) 20(2):436–43. doi: 10.1681/ASN.2008030292
40. Sarafidis PA, Bakris GL. Microalbuminuria and chronic kidney disease as risk factors for cardiovascular disease. Nephrol Dial Transplant (2006) 21(9):2366–74. doi: 10.1093/ndt/gfl309
41. Xia F, Liu G, Shi Y, Zhang Y. Impact of microalbuminuria on incident coronary heart disease, cardiovascular and all-cause mortality: a meta-analysis of prospective studies. Int J Clin Exp Med (2015) 8(1):1–9.
42. Sheer R, Nair R, Pasquale MK, Evers T, Cockrell M, Gay A, et al. Predictive risk models to identify patients at high-risk for severe clinical outcomes with chronic kidney disease and type 2 diabetes. J Prim Care Community Health (2022) 13:21501319211063726. doi: 10.1177/21501319211063726
43. Mogensen CE. Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetes. N Engl J Med (1984) 310(6):356–60. doi: 10.1056/NEJM198402093100605
44. Waldmann TA, Strober W, Mogielnicki RP. The renal handling of low molecular weight proteins. II. disorders of serum protein catabolism in patients with tubular proteinuria, the nephrotic syndrome, or uremia. J Clin Invest (1972) 51(8):2162–74. doi: 10.1172/JCI107023
45. Tomlinson PA. Low molecular weight proteins in children with renal disease. Pediatr Nephrol (1992) 6(6):565–71. doi: 10.1007/BF00866510
46. Patel DN, Kalia K. Characterization of low molecular weight urinary proteins at varying time intervals in type 2 diabetes mellitus and diabetic nephropathy patients. Diabetol Metab Syndr (2019) 11:39. doi: 10.1186/s13098-019-0430-1
47. Pemmasani G, Yandrapalli S. Age-stratified prevalence of relevant comorbidities and etiologies for hospitalizations in prader-willi syndrome patients. Am J Med Genet A (2021) 185(2):600–1. doi: 10.1002/ajmg.a.61968
48. Tsuchiya T, Oto Y, Ayabe T, Obata K, Murakami N, Nagai T. Characterization of diabetes mellitus in Japanese prader-willi syndrome. Clin Pediatr Endocrinol (2011) 20(2):33–8. doi: 10.1297/cpe.20.33
49. Schmidt F, Kapellen TM, Wiegand S, Herbst A, Wolf J, Fröhlich-Reiterer EE, et al. Diabetes mellitus in children and adolescents with genetic syndromes. Exp Clin Endocrinol Diabetes (2012) 120(10):579–85. doi: 10.1055/s-0032-1306330
50. Yang A, Kim J, Cho SY, Jin DK. Prevalence and risk factors for type 2 diabetes mellitus with prader-willi syndrome: a single center experience. Orphanet J Rare Dis (2017) 12(1):146. doi: 10.1186/s13023-017-0702-5
51. Gross JL, de Azevedo MJ, Silveiro SP, Canani LH, Caramori ML, Zelmanovitz T. Diabetic nephropathy: diagnosis, prevention, and treatment. Diabetes Care (2005) 28(1):164–76. doi: 10.2337/diacare.28.1.164
52. Lorenzo V, Saracho R, Zamora J, Rufino M, Torres A. Similar renal decline in diabetic and non-diabetic patients with comparable levels of albuminuria. Nephrol Dial Transplant (2010) 25(3):835–41. doi: 10.1093/ndt/gfp475
53. Valmadrid CT, Klein R, Moss SE, Klein BE. The risk of cardiovascular disease mortality associated with microalbuminuria and gross proteinuria in persons with older-onset diabetes mellitus. Arch Intern Med (2000) 160(8):1093–100. doi: 10.1001/archinte.160.8.1093
54. Toto RD. Microalbuminuria: definition, detection, and clinical significance. J Clin Hypertens (Greenwich) (2004) 6(11 Suppl 3):2–7. doi: 10.1111/j.1524-6175.2004.4064.x
55. de Zeeuw D, Parving HH, Henning RH. Microalbuminuria as an early marker for cardiovascular disease. J Am Soc Nephrol (2006) 17(8):2100–5. doi: 10.1681/ASN.2006050517
56. Mulè G, Castiglia A, Cusumano C, Scaduto E, Geraci G, Altieri D, et al. Subclinical kidney damage in hypertensive patients: a renal window opened on the cardiovascular system. focus on microalbuminuria. Adv Exp Med Biol (2017) 956:279–306. doi: 10.1007/5584_2016_85
57. Obesity WHOCo, World Health Organization, Division of Noncommunicable D, World Health Organization. Programme of nutrition f, reproductive h. obesity : preventing and managing the global epidemic : report of a WHO consultation on obesity, Geneva, 3-5 June 1997. Geneva: World Health Organization (1998).
58. Giles TD, Berk BC, Black HR, Cohn JN, Kostis JB, Izzo JL Jr., et al. Expanding the definition and classification of hypertension. J Clin Hypertens (Greenwich) (2005) 7(9):505–12. doi: 10.1111/j.1524-6175.2005.04769.x
59. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care (1997) 20(7):1183–97. doi: 10.2337/diacare.20.7.1183
60. Scott MG, Neil JS, Alison LB, Craig B, Kim KB, Roger SB, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American college of Cardiology/American heart association task force on clinical practice guidelines. Circulation (2019) 139(25):e1082–e143. doi: 10.1161/CIR.0000000000000625
61. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med (2009) 150(9):604–12. doi: 10.7326/0003-4819-150-9-200905050-00006
62. Kamińska J, Dymicka-Piekarska V, Tomaszewska J, Matowicka-Karna J, Koper-Lenkiewicz OM. Diagnostic utility of protein to creatinine ratio (P/C ratio) in spot urine sample within routine clinical practice. Crit Rev Clin Lab Sci (2020) 57(5):345–64. doi: 10.1080/10408363.2020.1723487
63. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev (2021) 10(1):89. doi: 10.1136/bmj.n71
64. Bassali R, Hoffman WH, Chen H, Tuck-Muller CM. Hyperlipidemia, insulin-dependent diabetes mellitus, and rapidly progressive diabetic retinopathy and nephropathy in prader-willi syndrome with del(15) (q11.2q13). Am J Med Genet (1997) 71(3):267–70. doi: 10.1002/(SICI)1096-8628(19970822)71:3<267::AID-AJMG3>3.0.CO;2-R
65. Chee C, Olczak SA. A prader-willi tricky situation: no. 69 in aregular educational series of brief illustrated descriptions of interesting or unusual diabetes-related cases and conditions. Pract Diabetes Int (2008) 25(5):192. doi: 10.1002/pdi.1247
66. Ito T, Ishikawa E, Fujimoto M, Murata T, Yamada N, Ito M. Severe intimal thickening of interlobular arteries revealed by a renal biopsy in an adult with prader-willi syndrome complicated by IgA nephropathy. Intern Med (2016) 55(2):161–4. doi: 10.2169/internalmedicine.55.4863
67. Nyumura I, Miura J, Shimura K, Oya J, Hanai K, Babazono T, et al. A case of diabetes mellitus associated with severe sleep apnea and prader-willi syndrome. Diabetol Int (2014) 5(1):69–73. doi: 10.1007/s13340-013-0134-y
68. Printza N, Bersos E, Zafeiriou D, Leontsini M, Stamou M, Papachristou F. Mesangioproliferative glomerulonephritis in an infant with prader-willi syndrome. Hippokratia (2009) 13(2):125–6.
69. Robson WLM, Leung AKC. Membranoproliferative glomerulonephritis in a child with prader-willi syndrome. Am J Med Genet (1992) 43(5):858–9. doi: 10.1002/ajmg.1320430521
70. Kuramochi Y, Kato T, Sudou M, Sugano H, Takagi H, Morita T. Cardiac tamponade due to systemic lupus erythematosus in patient with prader-willi syndrome after growth hormone therapy. Lupus (2007) 16(6):447–9. doi: 10.1177/0961203307077995
71. Landau D, Hirsch HJ, Gross-Tsur V. Case report: severe asymptomatic hyponatremia in prader-willi syndrome. BMC Pediatr (2016) 16(1):28. doi: 10.1186/s12887-016-0563-4
72. Horikawa Y, Enya M, Komagata M, Hashimoto KI, Kagami M, Fukami M, et al. Effectiveness of sodium-glucose cotransporter-2 inhibitor as an add-on drug to GLP-1 receptor agonists for glycemic control of a patient with prader–willi syndrome: a case report. Diabetes Ther (2018) 9(1):421–6. doi: 10.1007/s13300-018-0369-5
73. Paisey RB, Bower L, Rosindale S, Lawrence C. Successful treatment of obesity and diabetes with incretin analogue over four years in an adult with prader-willi syndrome. Pract Diabetes (2011) 28(7):306–7. doi: 10.1002/pdi.1621
74. Tomoda Y, Okauchi Y, Deguchi A, Takenoshita Y, Iwahashi H, Mineo I. Prader-willi syndrome with slowly progressive insulin-dependent diabetes mellitus. Intern Med (2021) 60(9):1423–6. doi: 10.2169/internalmedicine.5267-20
75. Jabbar A, Khan JN, Singh A, McCann GP. 'A one-sided affair': unilateral pulmonary oedema and the role of cardiac MRI in diagnosing premature coronary artery disease in a patient with prader-willi syndrome. BMJ Case Rep (2013) 2013:bcr2013008692. doi: 10.1136/bcr-2013-008692
76. Kniese CM, Jan MY, Diab K. Pneumomediastinum and pneumoperitoneum caused by tracheostomy displacement. BMJ Case Rep (2015) 2015:bcr2015211238. doi: 10.1136/bcr-2015-211238
77. McVea S, Thompson AJ, Abid N, Richardson J. Thermal dysregulation in prader-willi syndrome: a potentially fatal complication in adolescence, not just in infancy. BMJ Case Rep (2016) 2016:bcr2016215344. doi: 10.1136/bcr-2016-215344
78. Raj R, Owen D, Kannan L, Syeda U. Polypharmacy in a patient with intellectual and developmental disabilities. Cureus (2022) 14(2):e22019. doi: 10.7759/cureus.22019
79. Wordsworth G, Robinson A, Ward A, Atkin M. HHS - full or prophylactic anticoagulation? Br J Diabetes Vasc Dis (2014) 14(2):64–6. doi: 10.15277/bjdvd.2014.011
80. Santos VM, Paula FHD, Osterne EMC, Nery NS, Turra TZ. Morbid obesity in an adolescent with prader-willi syndrome. Rev Med Chile (2009) 137(2):264–8. doi: 10.4067/S0034-98872009000200012
81. Anno E, Hori K, Hoshimoto A, Harano M, Hagiwara S, Oishi K, et al. Successful peritoneal dialysis for the end-stage kidney disease associated with prader–willi syndrome: a case report. CEN Case Rep (2019) 8(3):216–20. doi: 10.1007/s13730-019-00395-3
82. Choi JW, Kim EJ, Min BW, Ban JS, Lee SG, Lee JH. Experience of severe desaturation during anesthetic induction period in an obese adult patient with prader-willi syndrome -a case report. Korean J Anesth (2012) 62(2):179–83. doi: 10.4097/kjae.2012.62.2.179
83. Liu APY, Tang WF, Lau ET, Chan KYK, Kan ASY, Wong KY, et al. Expanded prader-willi syndrome due to chromosome 15q11.2-14 deletion: report and a review of literature. Am J Med Genet Part A (2013) 161(6):1309–18. doi: 10.1002/ajmg.a.35909
84. Cento RM, Alberti A, Brancati G, Ragusa L, Pettinato R, Rossodivita A, et al. Bilateral non-communicating paraurethral meatus in prader-willi syndrome. GYNECOL Endocrinol (1997) 11(2):135–7. doi: 10.3109/09513599709152524
85. Fraga B, Gomes C, Gouveia R, Oliveira G. Herlyn-Werner-Wunderlich and prader-willi syndromes: more than a coincidence? BMJ Case Rep (2015) 2015:bcr2015212597. doi: 10.1136/bcr-2015-212597
86. Stevenson DA, Anaya TM. Unexpected death and critical illness in prader–willi syndrome: report of ten individuals. Am J Med Genet (2004) 124A(2):158–64. doi: 10.1002/ajmg.a.20370
87. Szigeti R, Chumpitazi BP, Finegold MJ, Ranganathan S, Craigen WJ, Carter BA, et al. Absent smooth muscle actin immunoreactivity of the small bowel muscularis propria circular layer in association with chromosome 15q11 deletion in megacystis-microcolon-intestinal hypoperistalsis syndrome. Pediatr Dev Pathol (2010) 13(4):322–5. doi: 10.2350/09-07-0678-CR.1
88. Goytain A, Hines RM, Quamme GA. Functional characterization of NIPA2, a selective Mg2+ transporter. Am J Physiol Cell Physiol (2008) 295(4):C944–C53. doi: 10.1152/ajpcell.00091.2008
89. Wu M, Yang C, Tao B, Bu S, Guay-Woodford LM. The ciliary protein cystin forms a regulatory complex with necdin to modulate myc expression. PloS One (2013) 8(12):e83062. doi: 10.1371/journal.pone.0083062
90. Höybye C, Hilding A, Jacobsson H, Thorén M. Metabolic profile and body composition in adults with prader-willi syndrome and severe obesity. J Clin Endocrinol Metab (2002) 87(8):3590–7. doi: 10.1210/jcem.87.8.8735
91. Marzullo P, Marcassa C, Campini R, Eleuteri E, Minocci A, Priano L, et al. The impact of growth hormone/insulin-like growth factor-I axis and nocturnal breathing disorders on cardiovascular features of adult patients with prader-willi syndrome. J Clin Endocrinol Metab (2005) 90(10):5639–46. doi: 10.1210/jc.2005-0829
92. Kobayashi S, Murakami N, Oto Y, Toide H, Kimura N, Hayashi A, et al. Subtle cardiovascular abnormalities in prader-willi syndrome might begin in young adulthood. Intern Med (2021) 60(21):3377–84. doi: 10.2169/internalmedicine.7073-21
93. Höybye C. Growth hormone treatment of prader-willi syndrome has long-term, positive effects on body composition. Acta Paediatr Int J Paediatr (2015) 104(4):422–7. doi: 10.1111/apa.12898
94. Koizumi M, Ida S, Shoji Y, Nishimoto Y, Etani Y, Kawai M. Visceral adipose tissue increases shortly after the cessation of gh therapy in adults with prader-willi syndrome. Endocr J (2018) 65(11):1127–37. doi: 10.1507/endocrj.EJ18-0107
95. van Nieuwpoort IC, Twisk JWR, Curfs LMG, Lips P, Drent ML. Body composition, adipokines, bone mineral density and bone remodeling markers in relation to IGF-1 levels in adults with prader-willi syndrome. Int J Pediatr Endocrinol (2018) 2018(1). doi: 10.1186/s13633-018-0055-4
96. Manzardo AM, Heinemann J, McManus B, Loker C, Loker J, Butler MG. Venous thromboembolism in prader–willi syndrome: a questionnaire survey. Genes (2019) 10(7):550. doi: 10.3390/genes10070550
97. Cohen AH. Massive obesity and the kidney. a morphologic and statistical study. Am J Pathol (1975) 81(1):117–30.
98. Nagai T, Obata K, Tonoki H, Temma S, Murakami N, Katada Y, et al. Cause of sudden, unexpected death of prader-willi syndrome patients with or without growth hormone treatment. Am J Med Genet A (2005) 136(1):45–8. doi: 10.1002/ajmg.a.30777
99. Pacoricona Alfaro DL, Lemoine P, Ehlinger V, Molinas C, Diene G, Valette M, et al. Causes of death in prader-willi syndrome: lessons from 11 years' experience of a national reference center. Orphanet J Rare Dis (2019) 14(1):238. doi: 10.1186/s13023-019-1214-2
100. Von Gontard A, Didden R, Sinnema M, Curfs L. Urinary incontinence in persons with prader-willi syndrome. BJU Int (2010) 106(11):1758–62. doi: 10.1111/j.1464-410X.2010.09457.x
101. Sinnema M, Schrander-Stumpel CT, Maaskant MA, Boer H, Curfs LM. Aging in prader-willi syndrome: twelve persons over the age of 50 years. Am J Med Genet A (2012) 158A(6):1326–36. doi: 10.1002/ajmg.a.35333
102. Equit M, Piro-Hussong A, Niemczyk J. Elimination disorders in persons with prader–willi and fragile-X syndromes. Neurourol Urodyn (2013) 32(7):986–92. doi: 10.1002/nau.22352
103. Meinhardt U, Christiansen JS, Farholt S, Lämmer C, Ostergaard JR, Schmidt F, et al. The efficacy and safety of long-term norditropin® treatment in children with prader-willi syndrome. Horm Metab Res (2013) 45(7):532–6. doi: 10.1055/s-0033-1343449
104. Torrado M, Foncuberta ME, De Castro Perez MF, Gravina LP, Araoz HV, Baialardo E, et al. Change in prevalence of congenital defects in children with prader-willi syndrome. Pediatrics (2013) 131(2):e544–e9. doi: 10.1542/peds.2012-1103
105. Pacilli M, Heloury Y, O'Brien M, Lionti T, Rowell M, Hutson J. Orchidopexy in children with prader–willi syndrome: results of a long-term follow-up study. J Pediatr Urol (2018) 14(1):63.e1–.e6. doi: 10.1016/j.jpurol.2017.10.003
106. Johnson RJ, Segal MS, Srinivas T, Ejaz A, Mu W, Roncal C, et al. Essential hypertension, progressive renal disease, and uric acid: a pathogenetic link? J Am Soc Nephrol (2005) 16(7):1909. doi: 10.1681/ASN.2005010063
107. Rea DJ, Heimbach JK, Grande JP, Textor SC, Taler SJ, Prieto M, et al. Glomerular volume and renal histology in obese and non-obese living kidney donors. Kidney Int (2006) 70(9):1636–41. doi: 10.1038/sj.ki.5001799
108. Valensi P, Assayag M, Busby M, Pariès J, Lormeau B, Attali JR. Microalbuminuria in obese patients with or without hypertension. Int J Obes Relat Metab Disord (1996) 20(6):574–9.
109. Savage S, Nagel NJ, Estacio RO, Lukken N, Schrier RW. Clinical factors associated with urinary albumin excretion in type II diabetes. Am J Kidney Dis (1995) 25(6):836–44. doi: 10.1016/0272-6386(95)90565-0
110. Ribstein J, du Cailar G, Mimran A. Combined renal effects of overweight and hypertension. Hypertension (1995) 26(4):610–5. doi: 10.1161/01.HYP.26.4.610
111. Othman M, Kawar B, El Nahas AM. Influence of obesity on progression of non-diabetic chronic kidney disease: a retrospective cohort study. Nephron Clin Pract (2009) 113(1):c16–23. doi: 10.1159/000228071
112. Muntner P, Winston J, Uribarri J, Mann D, Fox CS. Overweight, obesity, and elevated serum cystatin c levels in adults in the united states. Am J Med (2008) 121(4):341–8. doi: 10.1016/j.amjmed.2008.01.003
113. Naour N, Fellahi S, Renucci JF, Poitou C, Rouault C, Basdevant A, et al. Potential contribution of adipose tissue to elevated serum cystatin c in human obesity. Obes (Silver Spring) (2009) 17(12):2121–6. doi: 10.1038/oby.2009.96
114. Fricker M, Wiesli P, Brändle M, Schwegler B, Schmid C. Impact of thyroid dysfunction on serum cystatin c. Kidney Int (2003) 63(5):1944–7. doi: 10.1046/j.1523-1755.2003.00925.x
115. Bökenkamp A, van Wijk JAE, Lentze MJ, Stoffel-Wagner B. Effect of corticosteroid therapy on serum cystatin c and β2-microglobulin concentrations. Clin Chem (2002) 48(7):1123–6. doi: 10.1093/clinchem/48.7.1123
116. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of cardiology (ESC) and the European society of hypertension (ESH). Eur Heart J (2018) 39(33):3021–104. doi: 10.1093/eurheartj/ehy339
117. Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J (2020) 41(2):255–323. doi: 10.1093/eurheartj/ehz486
118. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J (2021) 42(34):3227–337. doi: 10.1093/eurheartj/ehab484
119. Rosenberg AGW, Pater MRA, Pellikaan K, Davidse K, Kattentidt-Mouravieva AA, Kersseboom R, et al. What every internist-endocrinologist should know about rare genetic syndromes in order to prevent needless diagnostics, missed diagnoses and medical complications: five years of 'Internal medicine for rare genetic syndromes'. J Clin Med (2021) 10(22):5457. doi: 10.3390/jcm10225457
120. Semins MJ, Shore AD, Makary MA, Weiner J, Matlaga BR. The impact of obesity on urinary tract infection risk. Urology (2012) 79(2):266–9. doi: 10.1016/j.urology.2011.09.040
Keywords: Prader-Willi Syndrome, kidney function tests, proteinuria, urine tract infections, cardiovascular disease, kidney disease
Citation: van Abswoude DH, Pellikaan K, Nguyen N, Rosenberg AGW, Davidse K, Hoekstra FME, Rood IM, Poitou C, Grugni G, Høybye C, Markovic TP, Caixàs A, Crinò A, van den Berg SAA, van der Lely AJ and de Graaff LCG (2023) Kidney disease in adults with Prader-Willi syndrome: international cohort study and systematic literature review. Front. Endocrinol. 14:1168648. doi: 10.3389/fendo.2023.1168648
Received: 17 February 2023; Accepted: 03 July 2023;
Published: 21 July 2023.
Edited by:
Katja Dumic Kubat, University of Zagreb, CroatiaReviewed by:
Lovro Lamot, University of Zagreb, CroatiaOlga Gimenez Palop, Corporació Sanitària Parc Taulí, Spain
Copyright © 2023 van Abswoude, Pellikaan, Nguyen, Rosenberg, Davidse, Hoekstra, Rood, Poitou, Grugni, Høybye, Markovic, Caixàs, Crinò, van den Berg, van der Lely and de Graaff. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura C. G. de Graaff, bC5kZWdyYWFmZkBlcmFzbXVzbWMubmw=