 Márton Eördögh1*
Márton Eördögh1* László Bárány2Christian Rosenstengel1Victoria Bogaczyk1Jörg Baldauf1Silke Vogelgesang3Andreas Stahl4Michael Kirsch5Werner Hosemann6Antje Steveling7
László Bárány2Christian Rosenstengel1Victoria Bogaczyk1Jörg Baldauf1Silke Vogelgesang3Andreas Stahl4Michael Kirsch5Werner Hosemann6Antje Steveling7 Ahmed Al Menabbawy1Henry W. S. Schroeder1
Ahmed Al Menabbawy1Henry W. S. Schroeder1- 1Department of Neurosurgery, University Medicine Greifswald, Greifswald, Germany
- 2Department of Neurosurgery, University Hospital Erlangen, Friedrich-Alexander-University, Erlangen, Germany
- 3Institute of Pathology, University Medicine Greifswald, Greifswald, Germany
- 4Department of Ophthalmology, University Medicine Greifswald, Greifswald, Germany
- 5Institute of Diagnostic Radiology and Neuroradiology, University Medicine Greifswald, Greifswald, Germany
- 6Department of Ear, Nose and Throat Diseases, Head and Neck Surgery, University Medicine Greifswald, Greifswald, Germany
- 7Department of Internal Medicine “A”, University Medicine Greifswald, Greifswald, Germany
Objective: The value of endoscopic versus microsurgical approach has not yet been defined in transsphenoidal pituitary adenoma surgery. In this study, we compare both methods and analyze the long-term surgical, radiological, endocrinological, ophthalmological, and rhinological results as well as the patients’ quality of life.
Methods: A total of 33 individuals with elective transsphenoidal pituitary adenoma surgery were randomized (pure endoscopic approach or endoscope-assisted microscopic approach) and prospectively underwent investigations with a focus on patient-related subjective outcome measurements.
Results: The mean follow-up period was 6.3 years. In the microsurgical group, endoscopic inspection revealed residual tumor in seven of 15 patients (46.7%) not seen by the microscope. Endoscopic resection provided long-term tumor-free state in all of them. Compared to pure microsurgical treatment, endoscopy was associated with a lower probability of tumor recurrence (OR = 0.24) and appeared advantageous in the long-term achievement of any surgical goal (OR = 3.80) as well as in anterior pituitary lobe function improvement (OR = 1.60). Where gross total tumor resection was the stated preoperative goal, there was no long-term tumor recurrence in 81.8% (endoscopy group) and 83.3% (endoscope-assisted microsurgical group). Most aspects showed no significant difference between the techniques, such as length of hospital stay, complication rate (endoscopy: 16.7%, endoscope-assisted microsurgery: 20.0%), long-term maintenance of any preoperatively stated extent of resection, pituitary and olfactory function, rates of DI and SIADH, ophthalmological improvement, and SNOT scores.
Conclusions: Both techniques provide good long-term surgical, radiological, endocrinological, rhinological, and ophthalmological results. Endoscopy clearly improved the rate of long-term achievement of the initial surgical goal and the anterior pituitary lobe function.
Introduction
Decades after Schloffer’s (1) and Hirsch’s (2) first attempts to remove a pituitary tumor, transnasal neurosurgery became inseparable from the microscope (3–5). Nowadays, panoramic endoscopic visualization—introduced by Jankowski et al.—with angled optics excels the microscopic image which is further narrowed by retractors (5–10). Endoscopy seems advantageous concerning not only the extent of tumor resection (8, 11–15) or rhinological outcome (11, 12) but also the length of hospital stay (6, 12, 16). However, the value of endoscopic transsphenoidal pituitary surgery compared to microscopic techniques remains a subject of debate, as the evidence is mostly based on retrospective studies, and prospective, randomized analyses on this topic are rare (8, 17–21). There is also a need for investigations where patients’ subjective measurements (PROM) are confronted with the objective clinical data. To address this, we present our monocentric long-term prospective study of 33 consecutive randomized individuals who underwent endoscopic (E) or endoscope-assisted microscopic (M) transsphenoidal pituitary tumor resection.
Materials and methods
Patient population
This study involves patients who underwent elective transnasal pituitary adenoma surgery in our department between 2010 and 2011. A total of 40 adults were assigned to the E or M group by simple randomization. Rathke cleft cysts, active malignancies, emergency or revision surgeries, and extended endonasal approaches were excluded. Within the study period, both techniques were regularly performed by the surgeon (HWSS) in our department. Table 1 gives a detailed description of the investigated aspects of the follow-up examinations.
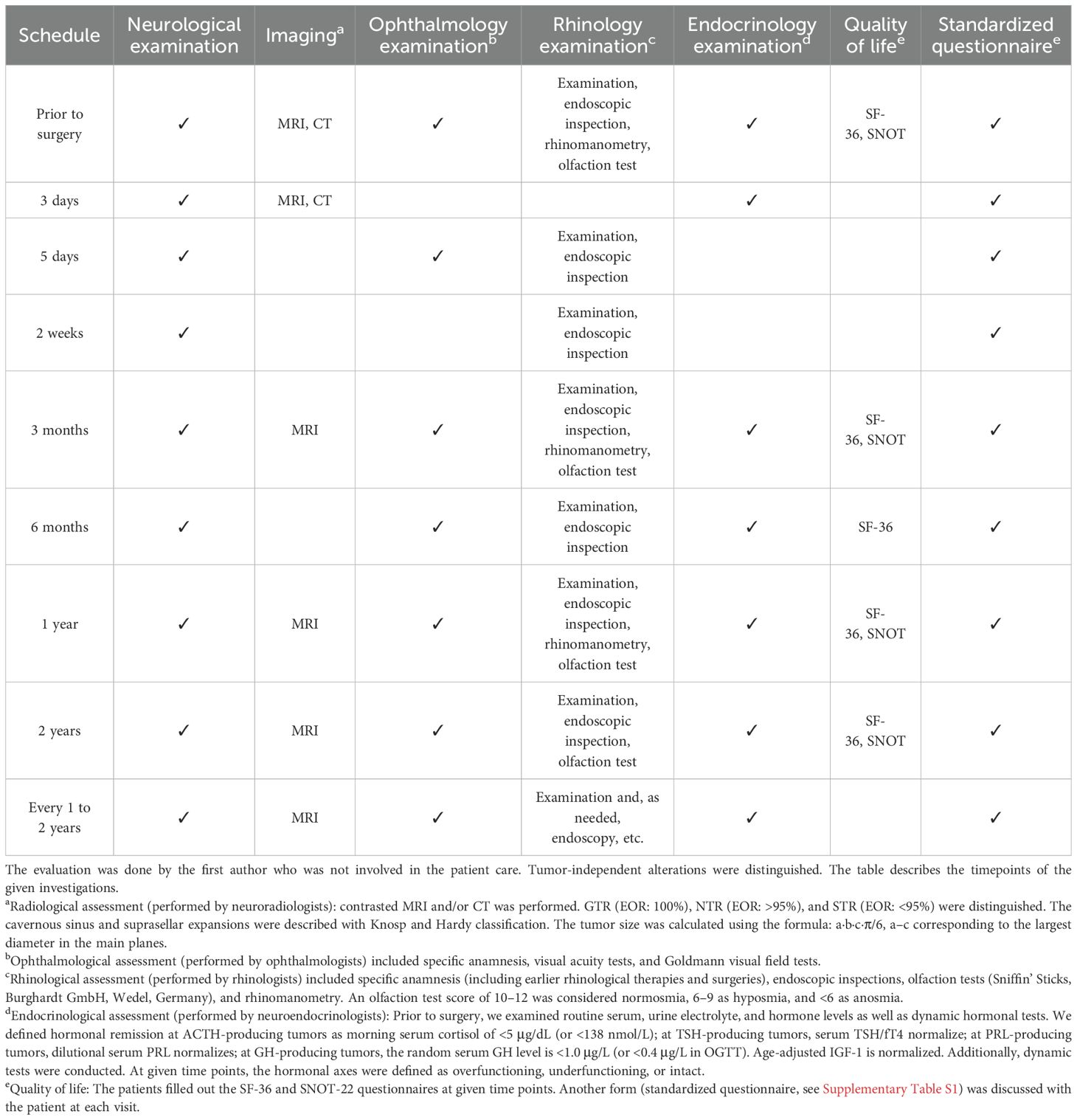
Table 1. Study agenda.
Ethics and human rights
All procedures were in accordance with the Helsinki declaration and its amendments. A local ethic committee approval was obtained (BB-38/09). The patients enrolled in this study gave informed consent for study participation.
Endoscopic binostril transnasal paraseptal transsphenoidal approach
After putting the patient in a supine position, adrenaline-impregnated pledgets were inserted toward the sphenoethmoidal recesses. The 0°-endoscope was introduced. The turbinates were lateralized. The posterior nasal septum was incised, then detached from the sphenoid rostrum, and displaced with the contralateral mucoperiosteum. The dorsal 1 cm of the bony nasal septum and the rostrum were resected. A wide bilateral sphenoidotomy was completed and the sphenoid septa removed. Only the sellar floor’s mucosa and bony floor were removed. The dura was incised and the tumor exposed. Then, 30° and 45° endoscopes helped to complete the tumor resection.
Endoscope-assisted microscopic mononostril transnasal paraseptal transsphenoidal approach
A speculum was inserted through one nostril. The turbinates were lateralized. The nasal septum was displaced to the contralateral side. The rostrum was drilled. The other steps were identical to E. Finally, angled endoscopes were introduced to find tumor remnants.
Statistical analysis
The statistical analysis was performed with the R-programming language (version 4.0.3) (22). Fisher exact tests and chi-square tests were used for categorical data; the continuous variables were compared using t-tests and Wilcoxon tests. Shapiro–Wilk test was used to control the normal distribution of the continuous variables. The significance level was p <0.05.
Results
Patient-specific and surgical parameters
A total of 18 (E) and 15 (M) patients with a histopathological diagnosis of pituitary adenoma were eligible—four patients had a Rathke cleft cyst and were excluded, and three further cases were also ruled out from the analysis (due to wish or independent death). Table 2 shows a comparison of the relevant patient-specific and surgical data of both groups. The M-surgeries’ duration was significantly shorter; further parameters were similar between the groups.
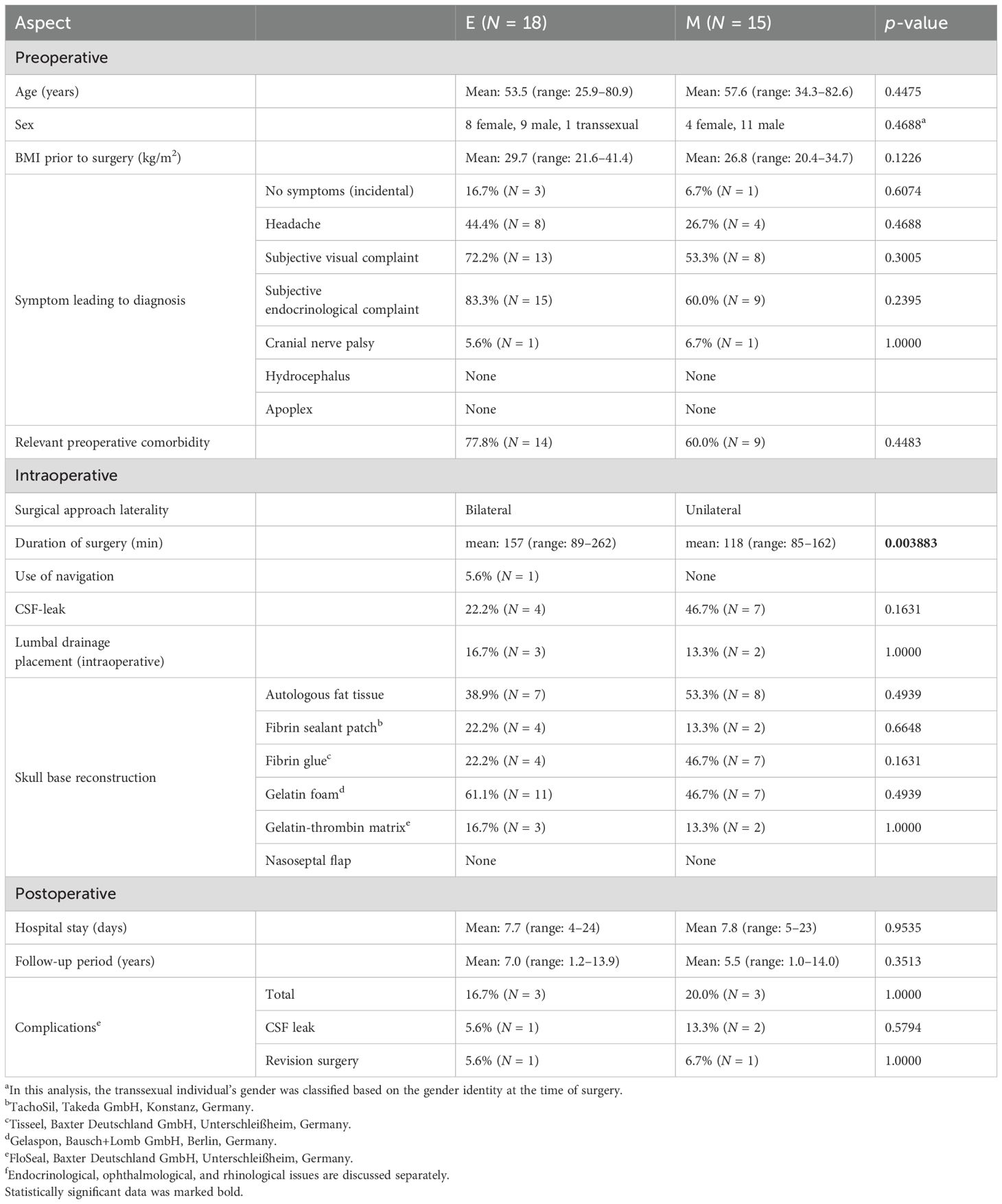
Table 2. Patient-specific and surgical data.
Histology and morphology
The histological features were comparable (Table 3). The lesions’ presurgical volume was similar. After dichotomization into infiltrating versus non-infiltrating tumors, there were no significant differences.
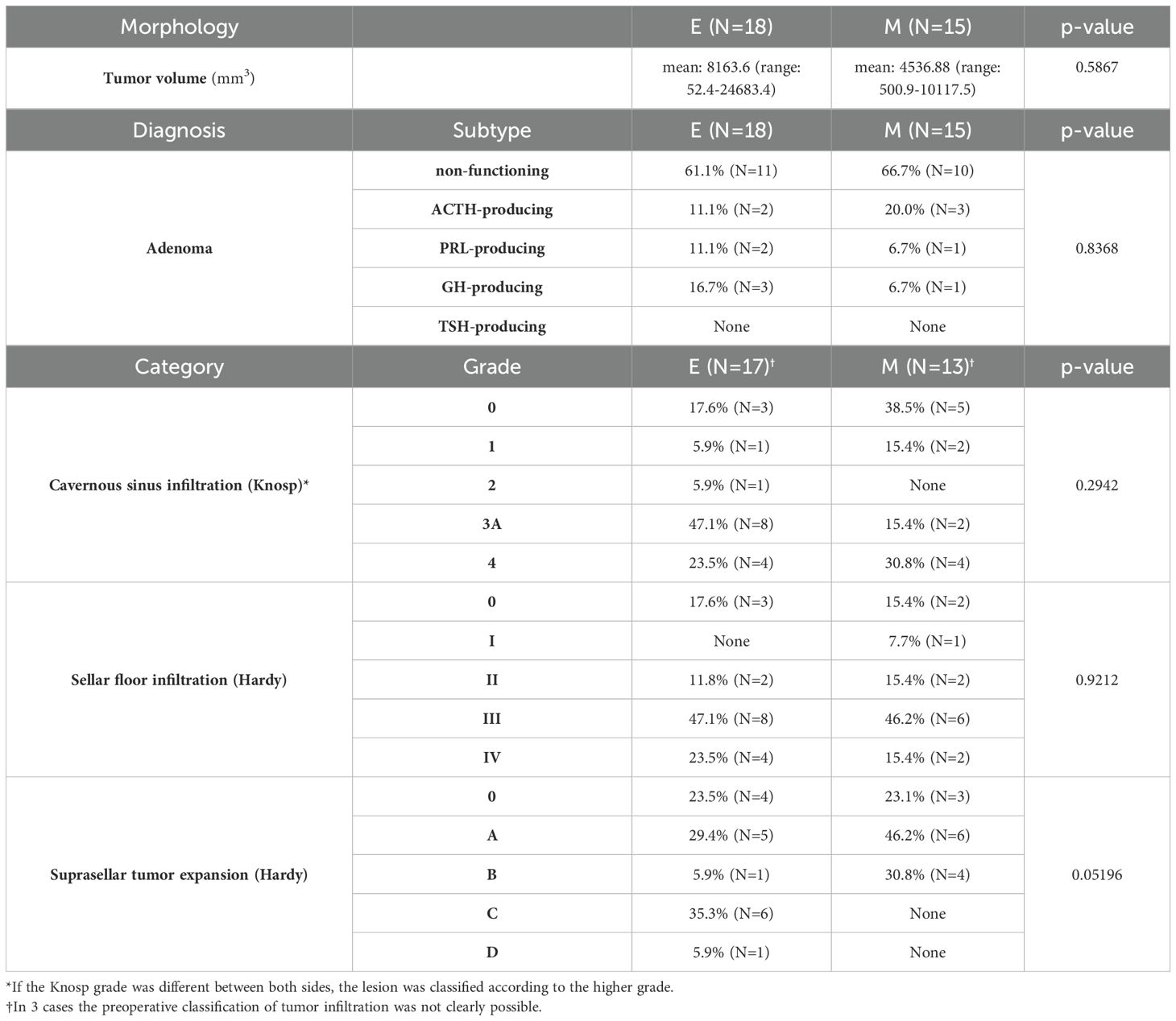
Table 3. Parameters of lesions.
Complications
Complications occurred in three E and three M patients (total: 18.2%, intercohort rate: p = 1.0000, OR = 0.80). The rhinological/endocrinological aspects are discussed separately. Postoperative CSF leak emerged in 9.1% (N = 3). The morbidities had no long-term medical consequences. There was no related mortality.
A total of 15 individuals (83.3%) of E were without complications: one patient underwent surgical revision due to CSF leak (5.6%), and another’s epistaxis was treated conservatively (5.6%). Another patient needed prolonged intensive care due to Addisonian crisis and pneumothorax (5.6%).
A total of 12 patients (80.0%) of M were without complications. A postoperative CSF leak (6.7%) was treated with lumbal drainage. Another patient underwent early revision surgery (6.7%) due to residual tumor and later again due to paraumbilical hemorrhage (6.7%) and CSF leak. One individual complained of nostril skin tear (6.7%).
Extent of resection
Angled optics revealed tumor in 63.6% (E; N = 7 from 11) and 58.3% (M; N = 7 from 12) where GTR was set as a goal of the surgery. The endoscopic or microsurgical technique carried no significant long-term recurrence rate difference in these subgroups (p = 1.0000, OR = 1.20). Independently from any goal, pure surgical long-term tumor-free state was achieved in E in 61.1% (N = 11), stable residuum in 16.7% (N = 3), and recurrence in 22.2% (N = 4, here adjuvant therapy was started). In M, pure surgical long-term tumor-free state was described in 86.7% (N = 13), stable residuum in 6.7% (N = 1), and recurrence in 6.7% (N = 1, here revision surgery was later performed). All patients underwent solo surgery with one M exception. The main results are detailed in Table 4.
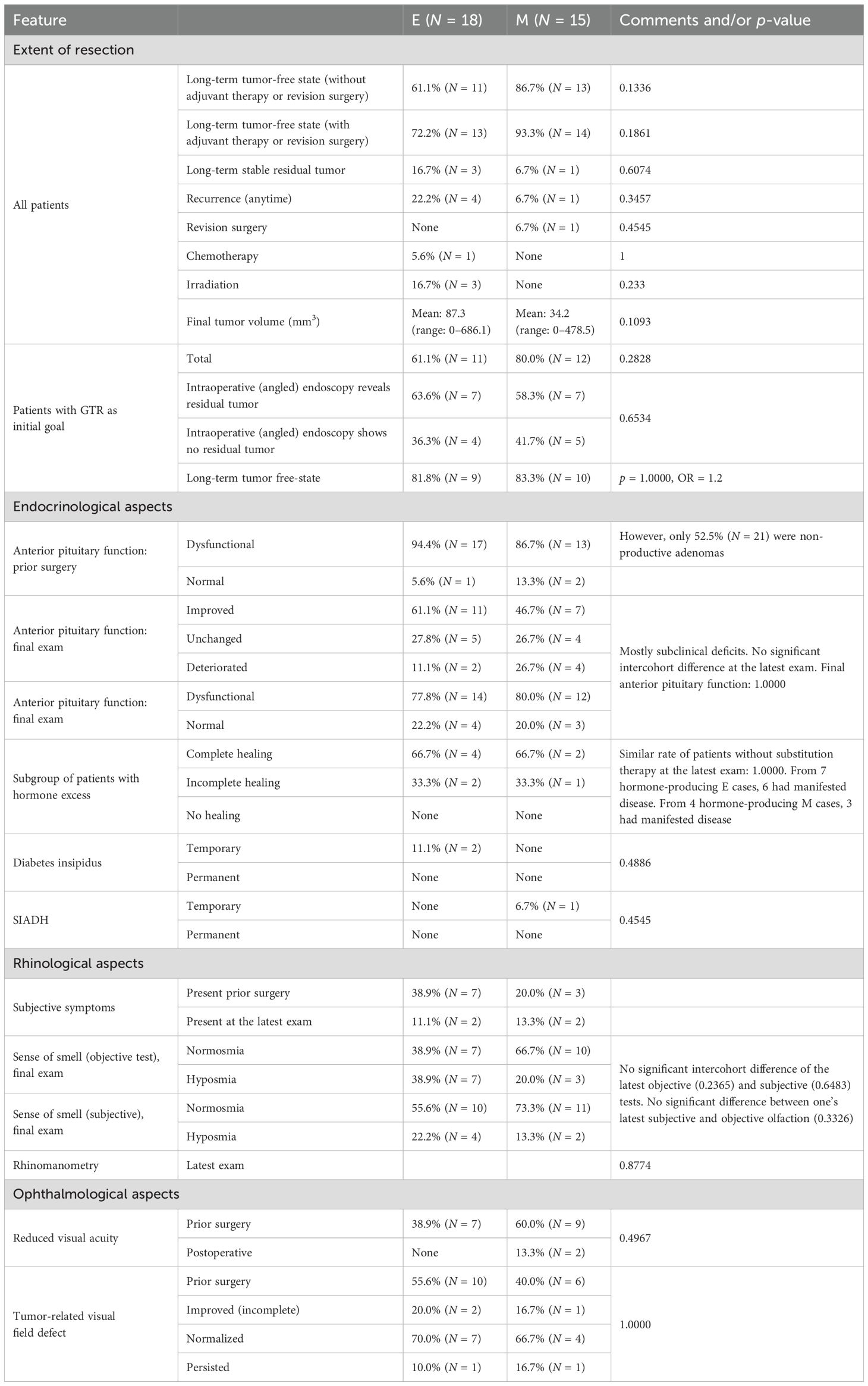
Table 4. Outcome data.
Endocrinological outcome
There were 94.4% (E; N = 17) and 86.7% (M; N = 13) patients who had preoperative anterior pituitary dysfunction (Table 4). However, 63.6% (N = 21) were non-functioning adenomas. Finally, four (E; 22.2%) and three (M; 20.0%) patients had normal anterior pituitary function. The deteriorations were mostly subclinical without hormonal substitution.
Table 5 demonstrates anterior lobe function dynamics. Furthermore, 83.3% (N = 5 from 6) with deterioration already presurgically presented multiaxial deficiency. Endoscopic technique was related to a higher probability of anterior pituitary lobe function improvement (OR = 1.60). Figure 1 demonstrates the pituitary function over time. There was neither a significant intercohort difference at the latest follow-up (p = 0.3166) nor in the overall trends (p = 0.2583).
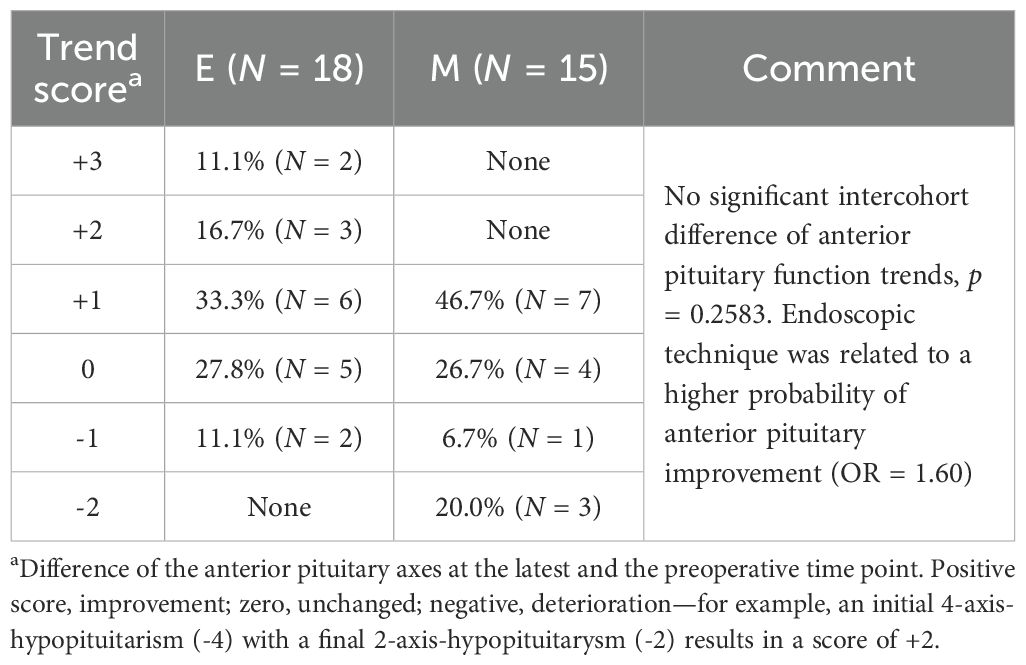
Table 5. Anterior pituitary lobe function.
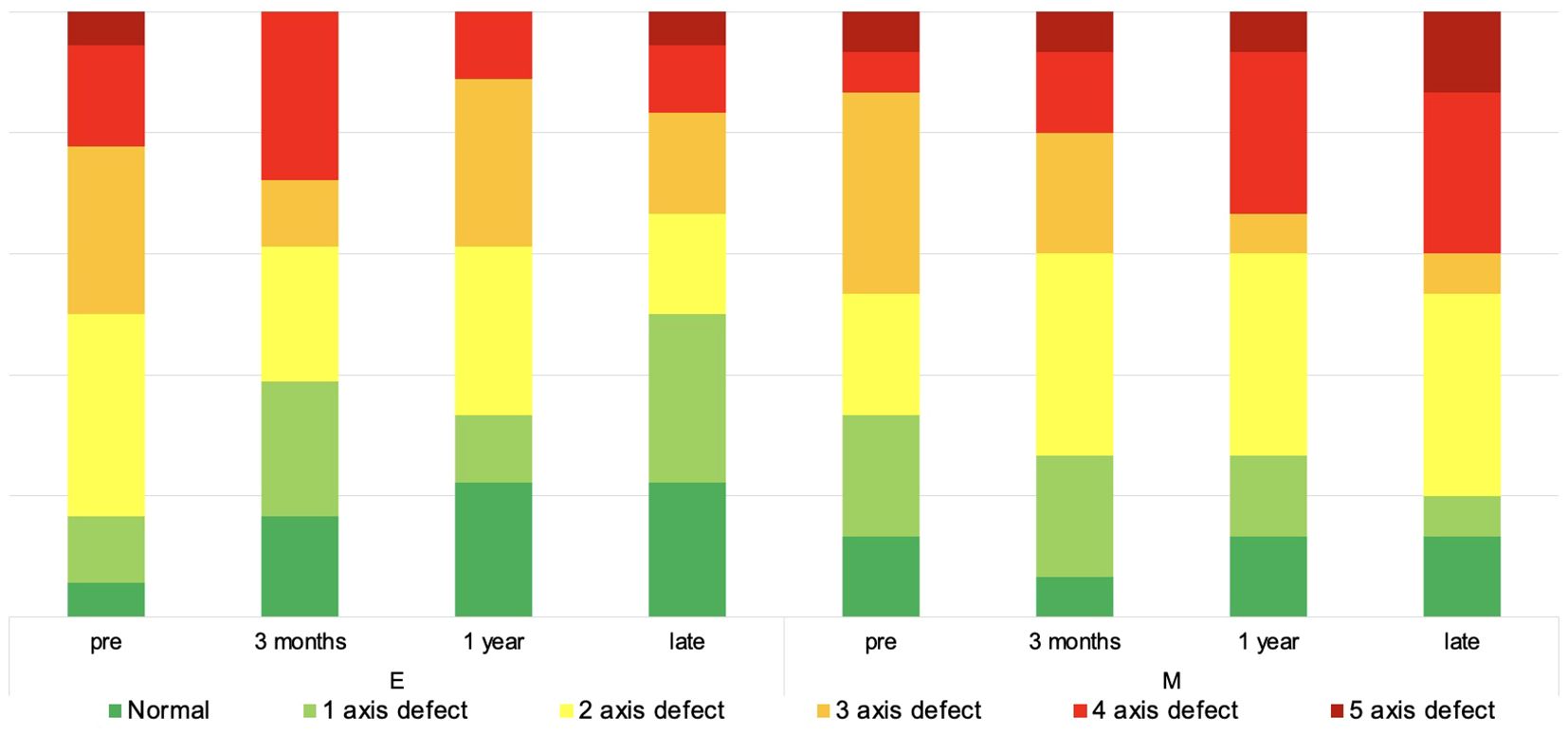
Figure 1. Anterior pituitary lobe function over time. The diagram depicts the non-continuous development of anterior pituitary lobe function over time.
Rhinological outcome
We recognized no significant intercohort differences of rhinological aspects. There were no relevant postsurgical pathologies (Table 4).
Ophthalmological outcome
The improvement of the visual acuity and visual field, respectively, were similar in both groups (Table 4). There was no deterioration of any visual function.
Quality of life
All patients had presurgical complaints (Supplementary Table S1). Finally, 94.4% (E; N = 17) and 86.7% (M; N = 13) achieved subjective well-being (Figure 2). Contrary to the early rhinological reconvalescence (Figure 3), the general recovery showed unspecific distribution. The working status data was comparable in both groups.
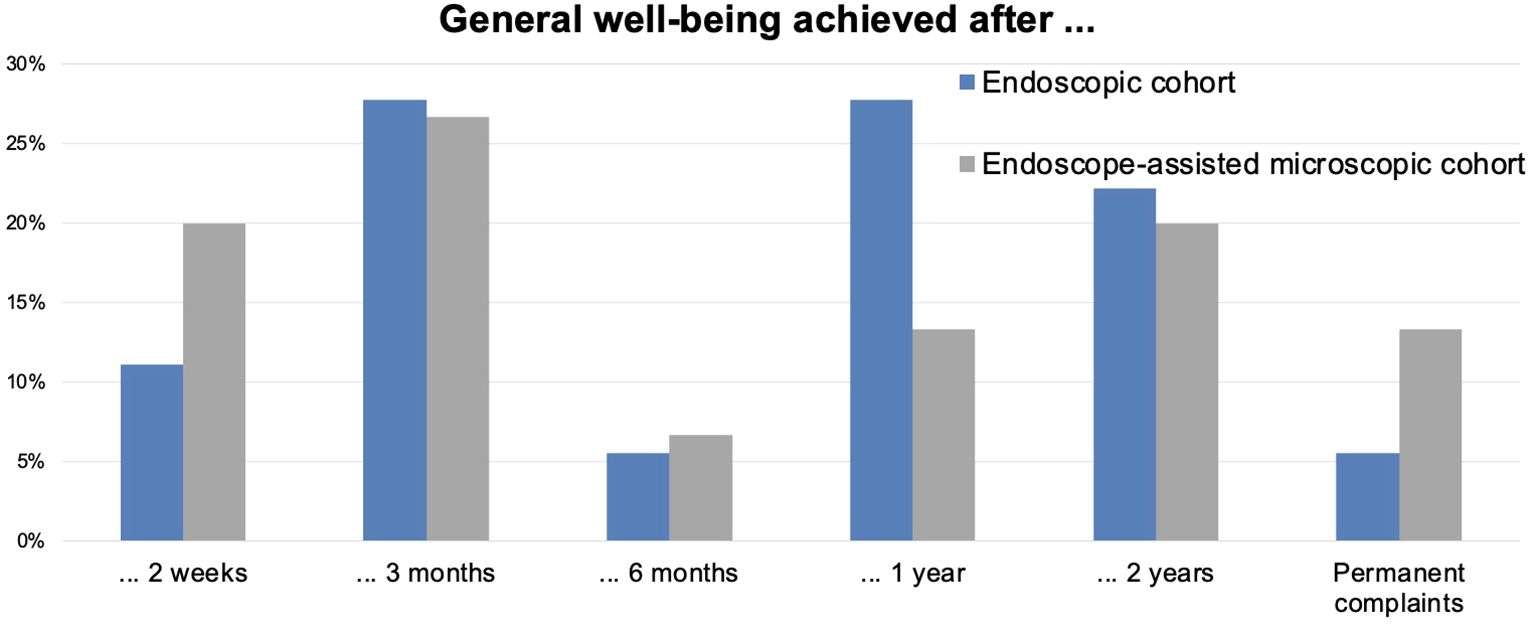
Figure 2. Achievement of overall well-being over time. The diagram depicts the non-continuous time point when symptom-free well-being was achieved. The values are in %.
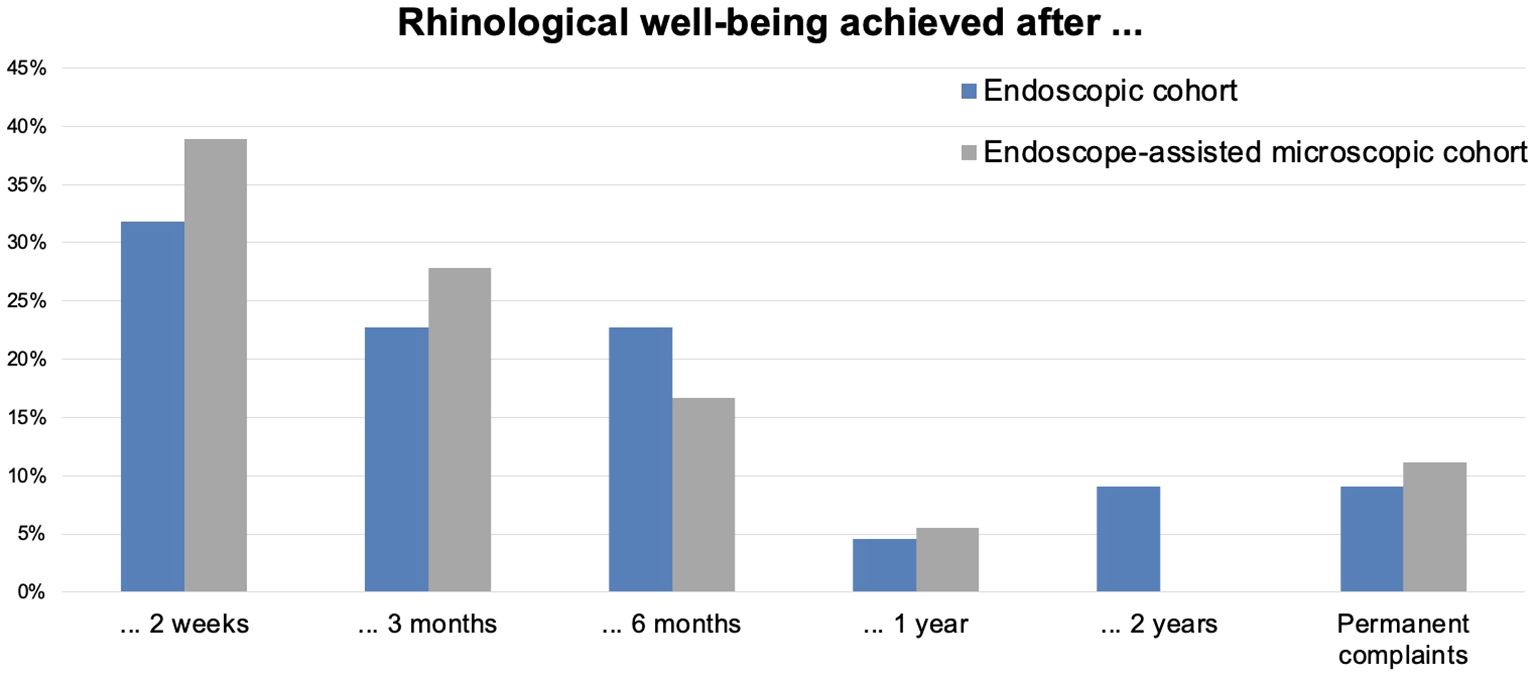
Figure 3. Achievement of rhinological well-being over time. The diagram depicts the non-continuous time point when symptom-free well-being was achieved. The values are in %.
The data of SF-36 was available in 15 E and 13 M cases. The SF-36 summarizes eight domains in the physical (PCS) and mental (MCS) score. The MCS showed no relevant changes across time between the groups and compared to the normal value (Figure 4). The PCS was significantly worse than the normal value but without difference between the groups across time.
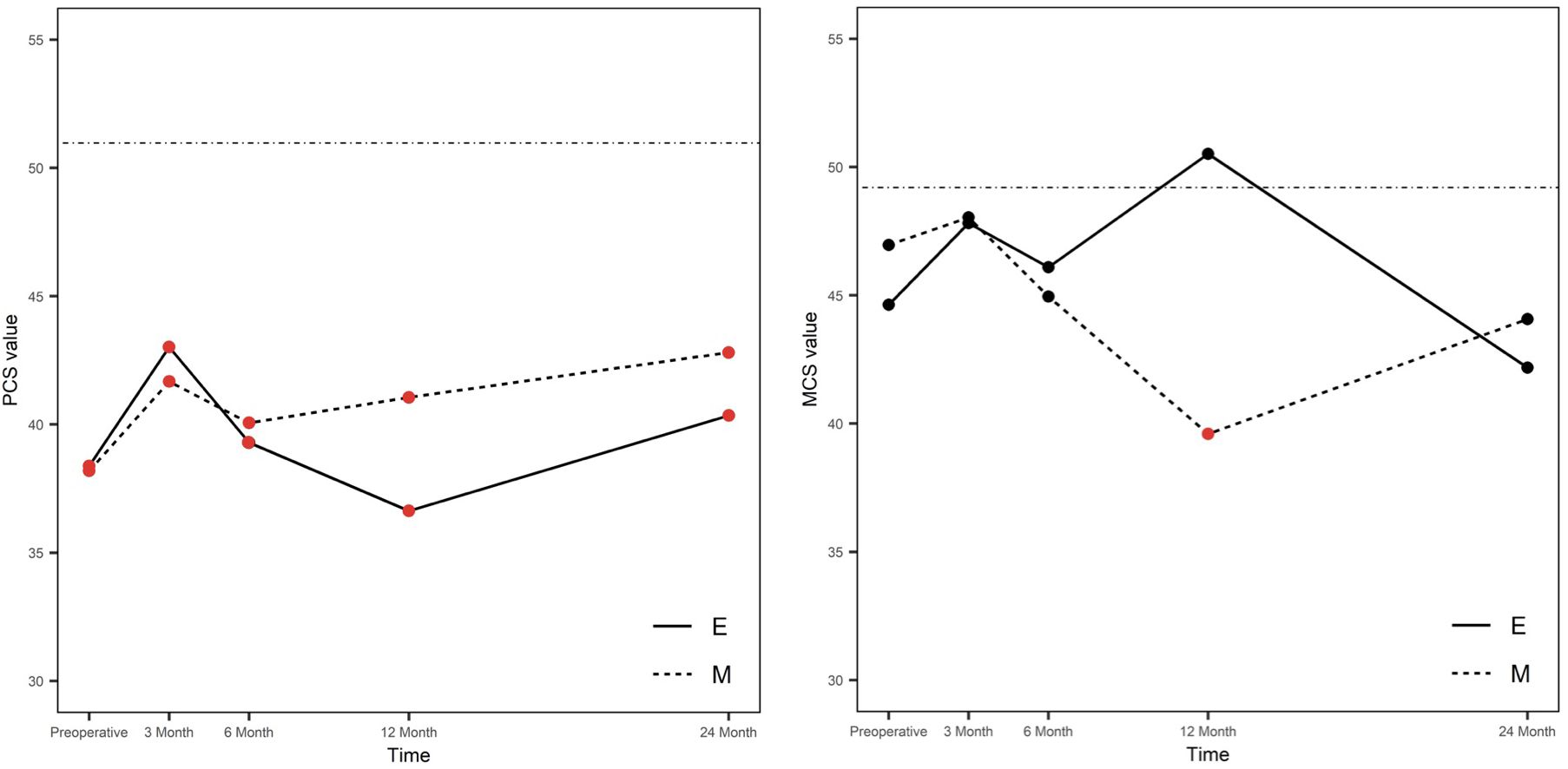
Figure 4. Mental and physical scores of SF-36 over time. E, endoscopic group; M, microsurgical group; MCS, mental component summary score; PCS, physical component summary score; continuous line, normal value of German population. Higher scores indicate a higher quality of life. Significant (red dots) and non-significant (black dots) results compared to the normal value are distinguished. We compared our data to the healthy German population (46) (straight line).
SNOT-22 results were available in seven E and eight M cases. The average trend of the preoperative and final scores was similar, p = 0.5474. Moreover, 14 E and 11 M patients filled the questionnaire 1 year after surgery; there was no relevant difference (p = 0.8588).
The value of microsurgical pituitary surgery
Endoscopy revealed residual tumor in 46.7% of cases (M group; N = 7) that had not been detected using the microscope alone. These remnants were subsequently removed with the endoscope, and follow-up MRI confirmed no recurrence in these patients.
We hypothesized that endoscopy was not added in M. Tumor-free state without adjuvant therapy would be then long-term maintained in favor of the endoscopic group (N = 11; 61.1%) compared to the pure microscopic cohort (N = 6, 40.0%; p = 0.4939, OR = 1.76). As a comparison, the factual OR in this aspect was 0.19 between the endoscopic and endoscope-assisted microsurgical groups. Endoscopy seemed also advantageous concerning the achievement of the initial surgical goal (p = 0.08272, OR = 3.80) and the recurrence rate without (p = 0.08272, OR = 0.26) as well as with adjuvant therapy (p = 0.1264, OR = 0.24). Consequently, added endoscopy relevantly improved the surgical outcome.
In eight M cases (53.3%), endoscopy revealed no residual tumor. Here a pure microsurgical manner would have been sufficient. We compared this subgroup (M*) to the E cohort: there was no significant difference of the trends in the anterior pituitary lobe function (p = 0.2810), the trends of the objective (p = 0.2433), and subjective olfaction (p = 0.5132) or the ophthalmologic outcome (p = 0.6655). At 24 months after surgery, the PCS and MCS of SF-36 did not differ significantly between the E and M* groups (p = 0.4561 and 0.4598, respectively). Table 6 presents a summary of our most relevant findings along with their statistical power.
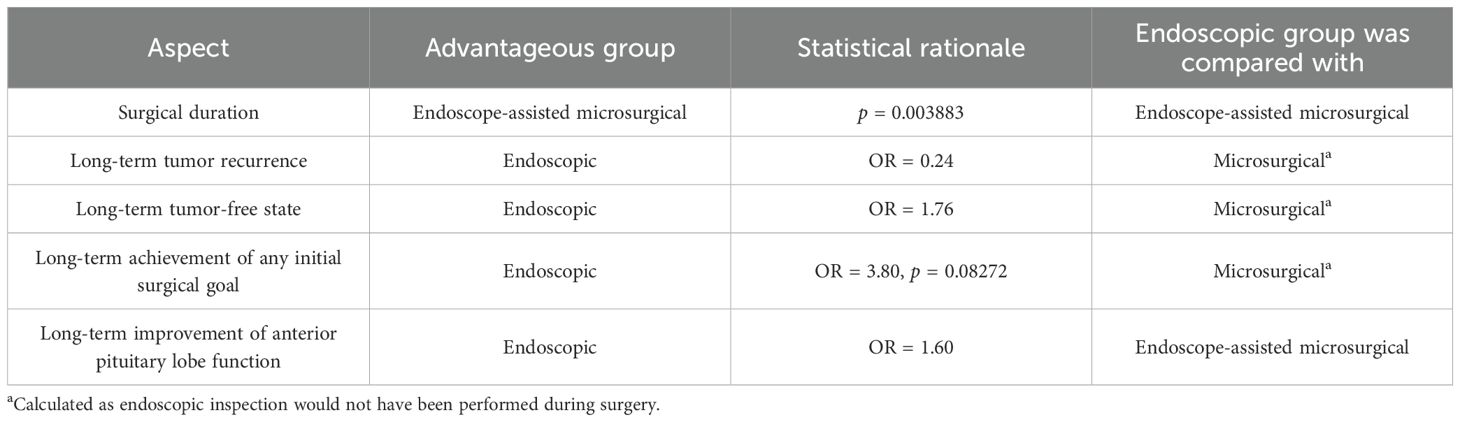
Table 6. Key observations.
Discussion
The superiority of endoscopy over microsurgery is a recurring statement (9, 10, 12, 20, 23, 24). This conclusion is primarily drawn from retrospective case series and meta-analyses that lack randomization and offer less control of confounding variables. Consequently, controversies regarding surgical outcomes persist, underscoring the need for randomized studies (21, 25).
There are only a few prospective (26–29) or randomized (27, 30) comparative studies. We believe that our study design offers valuable contributions by minimizing potential biases and presenting long-term data that complement the existing evidence. Additionally, the brief patient enrollment period reduces the influence of external factors such as changes in technology and medical care over the course of our series. Our review underlined the need for prospective (to reduce observer bias), randomized (no surgeon’s influence on division), and long-term (late morbidity/recurrence recognition) comparative studies which implement subjective PROMs.
Surgical parameters and complications
Razak et al. (31) reported increased endoscopic surgical duration, contrary to others (16, 27, 30). Due to the time-consuming nasal endoscopic phase, our M procedures were significantly shorter. At the time of our study, surgery starting point was defined by the beginning of anesthesia. This explains the relatively long durations. Contrary to us, others found shorter hospital stay in E cases (11, 12, 16, 30, 32).
We observed few complications without intercohort difference. The complication rates are around 20% (17, 32). Li et al. (33) showed comparable results of epistaxis, CSF leak, and meningitis. Castanão-Leon et al. (12) explain the lower endoscopic incidence of CSF-leak due to better visualization; however, others described higher rates (8, 34). Major complications are rare (6, 14, 15, 35).
Extent of resection
Endoscopy is believed to reduce recurrence (8, 11, 12, 36, 37). This advantage was significant in the study of Castanão-Leon et al. (12) (63.9% versus 42.2%). Recent metaanalyses found similar GTR rates of both techniques (21, 25). Our final rate of tumor-free state was 72.2% (endoscopy), 93.3% (endoscope-assisted microscopy), and 40.0% (hypothetical pure microscopic group). Recurrence usually appeared late, often after many years.
Endocrinological outcome
Anterior pituitary dysfunction occurs in 3%–6% (microsurgery) and 1%–3% (endoscopy) (16, 38, 39). Eseonu et al. (16) found comparable risks of hypopituitarism. According to Asemota et al. (35), the endoscopic rates of DI and SIADH were significantly higher. D’Haens et al. (34) described similar hypersecretion remission rates of 50% (microscopy) and 63% (endoscopy).
Due to the superior magnification with the endoscope, the normal pituitary can be protected, making hypopituitarism less likely (28, 30). We observed anterior lobe deterioration in 11.1% (E) and 26.7% (M). All of these patients already showed preoperative multiaxial deficiency. What could explain the differences? Firstly, our testing often revealed subclinical presurgical hormonal deficits which are not commonly registered. Secondly, the remission of pituitary function can be delayed.
In our series, the intercohort trends of anterior pituitary function were comparable. Contrarily, Castanão-Leon et al. (12) described better endoscopic remission rates (except Cushing’s disease). ACTH-producing microadenomas reportedly have outstanding microsurgical results; however, Bora et al. (40) found better endoscopic remission rates. Razak et al. (31) reported higher remission rates of functional adenomas after endoscopic surgery (94% vs. 57%). Phan et al. (41) described similar rates of endocrine remission in acromegaly patients.
Visual outcome
Endoscopy is thought to be advantageous in this field (12). In accordance with others (14, 25, 30), we found no significant differences. Asemota et al. (35) described visual field defects (4.7%), paralytic strabismus (2.2%), and diplopia (1.6%) without significant intercohort difference. Another study (11) postulates that endoscopy may provide better visual outcomes with an improvement rate of 71% vs. 56%. Bryl et al. (42) described a benefit for the endoscopic approach concerning visual QOL.
Rhinological outcome
Four of our patients (12.1%) had late rhinological complaints; three of them would otherwise qualify as “surgical success” without tumor recurrence. PROMs should be implemented in the daily routine as they revealed preoperative sinonasal complaints in a quarter of our patients.
Endoscopy is considered to be less traumatic to the olfactory function as no retractor is used (26, 43). Nevertheless, Bryl et al. (42) found similar rhinological QOL data. Osborne et al. (44) found comparable long-term outcomes.
Quality of life
Kuan et al. (45) found no significant endoscopic surgery-related changes of SF-36 scores. Pledger et al. (15) identified no relevant differences of SF-36 scores between endoscopic and microscopic cohorts. SF-36 is a useful but general tool which should be complemented by specific pituitary-relevant aspects. We believe that our results are not specific as MCS and PCS relevantly differ. Another questionnaire (Supplementary Table S1) revealed long-term patients’ satisfaction in 86.7% M and 94.4% E.
Statistical power and limitations
The higher number of male subjects in the M group is a possible limitation; however, the gender distribution differences were not statistically significant. Similarly, the differences of the Knosp and Hardy grades were statistically not significant, but they may have had a subtle influence on the results.
The main limitation of this single-center, single-surgeon analysis is the low case number. However, we believe that our study design complements the existing literature and adds value by applying PROMs, minimizing biases and contributing long-term data (up to 14 years). We included consecutive cases without patient selection bias. The outcome assessment was blinded; the patients were not aware of their group allocation. Most prospective trials report of shorter follow-up periods (e.g., 6 months) (25). We recognized delayed surgical consequences emphasizing the necessity of long-term observations. A larger sample size would allow more profound conclusions. Meta-analyses provide data of high numbers of patients; however, different study methods and interpretations reduce their feasibility. Therefore, future large-scale, randomized analyses are necessary to confirm our results.
Conclusions
Both endoscopic and endoscope-assisted microsurgical techniques provide good long-term endocrinological, rhinological, and ophthalmological results. Endoscopy improved the rate of long-term achievement of the initial surgical goal, the tumor-free state, and the anterior pituitary lobe function.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Klinisches Ethikkomitee, Walther-Rathenau-Str. 49, 17475 Greifswald. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ME: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. LB: Data curation, Formal analysis, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. CR: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. VB: Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. JB: Formal analysis, Supervision, Writing – original draft, Writing – review & editing. SV: Data curation, Methodology, Writing – original draft, Writing – review & editing. AndS: Data curation, Supervision, Writing – original draft, Writing – review & editing. MK: Data curation, Visualization, Writing – original draft, Writing – review & editing. WH: Data curation, Methodology, Supervision, Writing – original draft, Writing – review & editing. AntS: Data curation, Methodology, Writing – original draft, Writing – review & editing. AM: Data curation, Project administration, Writing – original draft, Writing – review & editing. HS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to thank Mrs. Kornelia Hagemeister (Department of Neurosurgery, University Medicine Greifswald) for contacting the patients and coordinating their examinations. We also appreciate the efforts of all participating nurses who conducted the examinations.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. For minor language editing, ChatGPT was used.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1552526/full#supplementary-material
Abbreviations
E, endoscopic cohort of the present study; M, endoscope-assisted microscopic cohort of the present study; M*, pure microscopic cohort of the present study (hypothetical); ACTH, adrenocorticotropic hormone; BMI, body mass index; CSF, cerebrospinal fluid; CT, computed tomography; DI, diabetes insipidus; EOR, extent of tumor resection; fT4, free thyroxine hormone ; GH, growth hormone; GTR, gross total resection rate; IGF-1, insulin-like growth factor-1; MCS, mental component summary score of SF-36; MRI, magnetic resonance imaging; N, number of patients; NTR, nearly total resection rate; OGTT, oral glucose tolerance test; OR, odds-ratio; PCS , physical component summary score of SF-36; PRL, prolactin; PROM, patient-related outcome measurement; QOL, quality of life; SF-36, Short Form (36) Health Survey; SIADH, syndrome of inappropriate antidiuretic hormone secretion; SNOT, Sino-Nasal Outcome Test 20; STR, subtotal resection rate; TSH, thyroid-stimulating hormone.
References
1. Schloffer H. Zur Frage der Operation eines Hypophysentumors auf nasalem Wege. Beitr Klin Chir. (1906) 50:767–817.
2. Hirsch O. Eine neue Methode der endonasalen Operation von Hypophysentumoren. Wien Med Wochenschr. (1909) 59:636–8.
3. Hardy J. The transsphenoidal surgical approach to the pituitary. Hosp Pract. (1979) 14:81–9. doi: 10.1080/21548331.1979.11707562
4. Hardy J. Transsphenoidal hypophysectomy. J Neurosurg. (1971) 34:582–94. doi: 10.3171/jns.1971.34.4.0582
5. Griffith HB and Veerapen R. A direct transnasal approach to the sphenoid sinus. J Neurosurg. (1987) 66:140–2. doi: 10.3171/jns.1987.66.1.0140
6. Goshtasbi K, Lehrich BM, Abouzari M, Abiri A, Birkenbeuel J, Lan M-Y, et al. Endoscopic versus nonendoscopic surgery for resection of pituitary adenomas: a national database study. J Neurosurg. (2021) 134:816–24. doi: 10.3171/2020.1.JNS193062
7. Jankowski R, Auque J, Simon C, Marchal JC, Hepner H, and Wayoff M. Endoscopic pituitary tumor surgery. Laryngoscope. (1992) 102:198–202. doi: 10.1288/00005537-199202000-00016
8. Khalafallah AM, Liang AL, Jimenez AE, Rowan NR, Oyesiku NM, Mamelak AN, et al. Trends in endoscopic and microscopic transsphenoidal surgery: a survey of the international society of pituitary surgeons between 2010 and 2020. Pituitary. (2020) 23:526–33. doi: 10.1007/s11102-020-01054-y
9. Linsler S, Szameitat N, Senger S, and Oertel J. Visualization and identification of the pituitary gland tissue in endonasal pituitary surgery: is there a difference between high-definition endoscopy and microscopy? World Neurosurg. (2018) 116:e921–8. doi: 10.1016/j.wneu.2018.05.129
10. Little AS, Kelly DF, White WL, Gardner PA, Fernandez-Miranda JC, Chicoine MR, et al. Results of a prospective multicenter controlled study comparing surgical outcomes of microscopic versus fully endoscopic transsphenoidal surgery for nonfunctioning pituitary adenomas: the Transsphenoidal Extent of Resection (TRANSSPHER) Study. J Neurosurg. (2019) 132:1043–53. doi: 10.3171/2018.11.JNS181238
11. DeKlotz TR, Chia SH, Lu W, Makambi KH, Aulisi E, and Deeb Z. Meta-analysis of endoscopic versus sublabial pituitary surgery. Laryngoscope. (2012) 122:511–8. doi: 10.1002/lary.v122.3
12. Castaño-Leon AM, Paredes I, Munarriz PM, Jiménez-Roldán L, Hilario A, Calatayud M, et al. Endoscopic transnasal trans-sphenoidal approach for pituitary adenomas: A comparison to the microscopic approach cohort by propensity score analysis. Neurosurgery. (2020) 86:348–56. doi: 10.1093/neuros/nyz201
13. Guo-Dong H, Tao J, Ji-Hu Y, Wen-Jian Z, Xie-Jun Z, Jian G, et al. Endoscopic versus microscopic transsphenoidal surgery for pituitary tumors. J craniofacial Surg. (2016) 27:e648–55. doi: 10.1097/SCS.0000000000003000
14. Messerer M, battista JCD, Raverot G, Kassis S, Dubourg J, Lapras V, et al. Evidence of improved surgical outcome following endoscopy for nonfunctioning pituitary adenoma removal: Personal experience and review of the literature. Neurosurg Focus. (2011) 30:E11. doi: 10.3171/2011.1.FOCUS10308
15. Pledger CL, Elzoghby MA, Oldfield EH, Payne SC, and Jane JJA. Prospective comparison of sinonasal outcomes after microscopic sublabial or endoscopic endonasal transsphenoidal surgery for nonfunctioning pituitary adenomas. J Neurosurg. (2016) 125:323–33. doi: 10.3171/2015.6.JNS142695
16. Eseonu CI, ReFaey K, Rincon-Torroella J, Garcia O, Wand GS, Salvatori R, et al. Endoscopic versus microscopic transsphenoidal approach for pituitary adenomas: comparison of outcomes during the transition of methods of a single surgeon. World Neurosurg. (2017) 97:317–25. doi: 10.1016/j.wneu.2016.09.120
17. Chen X, Huang W, Li H, Huan Y, Mai G, Chen L, et al. Comparison of outcomes between endoscopic and microscopic transsphenoidal surgery for the treatment of pituitary adenoma: a meta-analysis. Gland Surg. (2020) 9:2162–74. doi: 10.21037/gs-20-851
18. Dallapiazza R, Bond AE, Grober Y, Louis RG, Payne SC, Oldfield EH, et al. Retrospective analysis of a concurrent series of microscopic versus endoscopic transsphenoidal surgeries for Knosp Grades 0–2 nonfunctioning pituitary macroadenomas at a single institution: Clinical article. J Neurosurg. (2014) 121:511–7. doi: 10.3171/2014.6.JNS131321
19. Hong SD, Nam D-H, Seol HJ, Choi NY, Kim HY, Chung S-K, et al. Endoscopic binostril versus transnasal transseptal microscopic pituitary surgery: sinonasal quality of life and olfactory function. Am J Rhinol Allergy. (2015) 29:221–5. doi: 10.2500/ajra.2015.29.4165
20. Mortini P. Cons: endoscopic endonasal transsphenoidal pituitary surgery is not superior to microscopic transsphenoidal surgery for pituitary adenomas. Endocrine. (2014) 47:415–20. doi: 10.1007/s12020-014-0365-0
21. Chen J, Liu H, Man S, Liu G, Li Q, Zuo Q, et al. Endoscopic vs. Microscopic transsphenoidal surgery for the treatment of pituitary adenoma: A meta-analysis. Front Surg. (2022) 8:806855. doi: 10.3389/fsurg.2021.806855
22. Team R Core. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2017).
23. Guo S, Wang Z, Kang X, Xin W, and Li X. A meta-analysis of endoscopic vs. Microscopic transsphenoidal surgery for non-functioning and functioning pituitary adenomas: comparisons of efficacy and safety. Front Neurol. (2021) 12:614382. doi: 10.3389/fneur.2021.614382
24. Strychowsky J, Nayan S, Reddy K, Farrokhyar F, and Sommer D. Purely endoscopic transsphenoidal surgery versus traditional microsurgery for resection of pituitary adenomas: systematic review. J Otolaryngol - Head Neck Surg Le J d’oto-rhino-Laryngol Chir cervico-faciale. (2011) 40:175–85.
25. Al-dardery NM, Khaity A, Soliman Y, Ali MOM, Zedan EM, Muyasarah K, et al. Safety and efficacy of endoscopic vs. microscopic approaches in pituitary adenoma surgery: A systematic review and meta-analysis. Neurosurg Rev. (2025) 48:471. doi: 10.1007/s10143-025-03600-3
26. Kahilogullari G, Beton S, Al-Beyati ESM, Kantarcioglu O, Bozkurt M, Kantarcioglu E, et al. Olfactory functions after transsphenoidal pituitary surgery: endoscopic versus microscopic approach. Laryngoscope. (2013) 123:2112–9. doi: 10.1002/lary.v123.9
27. Jain AK, Gupta AK, Pathak A, Bhansali A, and Bapuraj JR. Excision of pituitary adenomas: randomized comparison of surgical modalities. Br J Neurosurg. (2007) 21:328–31. doi: 10.1080/02688690701395447
28. Little AS, Kelly DF, Milligan J, Griffiths C, Prevedello DM, Carrau RL, et al. Comparison of sinonasal quality of life and health status in patients undergoing microscopic and endoscopic transsphenoidal surgery for pituitary lesions: a prospective cohort study. J Neurosurg. (2015) 123:799–807. doi: 10.3171/2014.10.JNS14921
29. Enseñat J, Quesada JL, Aparicio J, Pàmies C, Barber X, Topczewski T, et al. Prospective comparative study on 50 patients between microsurgical sublabial transsphenoidal approach and endoscopic endonasal transsphenoidal approach. Neurocirugia (Asturias Spain). (2009) 20:335–44-discussion 344-5.
30. Cho D-Y and Liau W-R. Comparison of endonasal endoscopic surgery and sublabial microsurgery for prolactinomas. Surg Neurol. (2002) 58:371–5-discussion 375-6. doi: 10.1016/S0090-3019(02)00892-3
31. Razak AA, Horridge M, Connolly DJ, Warren DJ, Mirza S, Muraleedharan V, et al. Comparison of endoscopic and microscopic trans-sphenoidal pituitary surgery: early results in a single centre. Br J Neurosurg. (2013) 27:40–3. doi: 10.3109/02688697.2012.703353
32. Li K, Zhang J, Wang X-S, Ye X, and Zhao Y-L. A systematic review of effects and complications after transsphenoidal pituitary surgery: endoscopic versus microscopic approach. Minimally invasive Ther Allied technologies: MITAT: Off J Soc Minimally Invasive Ther. (2020) 29:317–25. doi: 10.1080/13645706.2019.1660369
33. Li J, Ding W, Huang Z, Xie B, and Li Z-Y. Comparison of short-term outcomes between endoscopic and microscopic trans-sphenoidal surgery for the treatment of pituitary adenoma. J craniofacial Surg. (2019) 30:2421–4. doi: 10.1097/SCS.0000000000005676
34. D’Haens J, Rompaey KV, Stadnik T, Haentjens P, Poppe K, and Velkeniers B. Fully endoscopic transsphenoidal surgery for functioning pituitary adenomas: a retrospective comparison with traditional transsphenoidal microsurgery in the same institution. Surg Neurol. (2009) 72:336–40. doi: 10.1016/j.surneu.2009.04.012
35. Asemota AO, Ishii M, Brem H, and Gallia GL. Comparison of complications, trends, and costs in endoscopic vs microscopic pituitary surgery: analysis from a US health claims database. Neurosurgery. (2017) 81:458–72. doi: 10.1093/neuros/nyx350
36. Karppinen A, Kivipelto L, Vehkavaara S, Ritvonen E, Tikkanen E, Kivisaari R, et al. Transition from microscopic to endoscopic transsphenoidal surgery for nonfunctional pituitary adenomas. World Neurosurg. (2015) 84:48–57. doi: 10.1016/j.wneu.2015.02.024
37. Gompel JJV, Atkinson JLD, Choby G, Kasperbauer JL, Stokken JK, Janus JR, et al. Pituitary tumor surgery: comparison of endoscopic and microscopic techniques at a single center. Mayo Clin Proc. (2021) 96:2043–57. doi: 10.1016/j.mayocp.2021.03.028
38. Singh H, Essayed WI, Cohen-Gadol A, Zada G, and Schwartz TH. Resection of pituitary tumors: endoscopic versus microscopic. J neuro-oncology. (2016) 130:309–17. doi: 10.1007/s11060-016-2124-y
39. Wang F, Zhou T, Wei S, Meng X, Zhang J, Hou Y, et al. Endoscopic endonasal transsphenoidal surgery of 1,166 pituitary adenomas. Surg endoscopy. (2015) 29:1270–80. doi: 10.1007/s00464-014-3815-0
40. Bora SK, Suri A, Khadgawat R, Tandon N, Suri V, Sharma MC, et al. Management of cushing’s disease: changing trend from microscopic to endoscopic surgery. World Neurosurg. (2020) 134:e46–54. doi: 10.1016/j.wneu.2019.08.165
41. Phan K, Xu J, Reddy R, Kalakoti P, Nanda A, and Fairhall J. Endoscopic endonasal versus microsurgical transsphenoidal approach for growth hormone-secreting pituitary adenomas-systematic review and meta-analysis. World Neurosurg. (2017) 97:398–406. doi: 10.1016/j.wneu.2016.10.029
42. Bryl M, Woźniak J, Dudek K, Czapiga B, and Tabakow P. The quality of life after transnasal microsurgical and endoscopic resection of nonfunctioning pituitary adenoma. Adv Clin Exp Med. (2020) 29:921–8. doi: 10.17219/acem/123351
43. Baudracco I, Ekanayake J, Warner E, Grieve JP, and Dorward NL. Olfactory outcomes after transsphenoidal endonasal surgery. Br J Neurosurg. (2020) 34:35–9. doi: 10.1080/02688697.2019.1680798
44. Osborne C, Lewis D, Dixon B, Caputo C, Magee A, Gnanalingham K, et al. Equivalent outcomes in nasal symptoms following microscopic or endoscopic transsphenoidal surgery: results from multi-centre, prospective study. Acta Neurochir. (2022) 164:1589–97. doi: 10.1007/s00701-022-05138-5
45. Kuan EC, Yoo F, Chyu J, Oh A, Bergsneider M, and Wang MB. Quality of Life before and after Endoscopic Pituitary Surgery as Measured by the Short-Form-36. J neurological surgery Part B Skull base. (2018) 79:314–8. doi: 10.1055/s-0037-1608648
Keywords: endonasal, pituitary, pituitary adenoma, transsphenoidal surgery, endoscopic transnasal approach
Citation: Eördögh M, Bárány L, Rosenstengel C, Bogaczyk V, Baldauf J, Vogelgesang S, Stahl A, Kirsch M, Hosemann W, Steveling A, Al Menabbawy A and Schroeder HWS (2025) Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study. Front. Endocrinol. 16:1552526. doi: 10.3389/fendo.2025.1552526
Received: 28 January 2025; Accepted: 23 June 2025;
Published: 22 July 2025.
Edited by:
Rosario Pivonello, University of Naples Federico II, ItalyReviewed by:
Dario Fontanelli, Federico II University Hospital, ItalyLuca Bruno, University of Naples Federico II, Italy
Copyright © 2025 Eördögh, Bárány, Rosenstengel, Bogaczyk, Baldauf, Vogelgesang, Stahl, Kirsch, Hosemann, Steveling, Al Menabbawy and Schroeder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Márton Eördögh, bS5lb3Jkb2doLm1kQGdtYWlsLmNvbQ==