 Gergő A. Molnár
Gergő A. Molnár Zoltán Kiss
Zoltán Kiss István Wittmann
István Wittmann- 2nd Department of Medicine and Nephrology-Diabetes Centre, University of Pécs Medical School, Pécs, Hungary
The absolute number of complications of type 2 diabetes mellitus increases with age. Recent data indicated that young individuals with type 2 diabetes are at a high risk compared to their non-diabetic counterparts, yet most data arose from high-income countries. Data in the literature indicates that young individuals indeed have a higher relative risk in terms of mortality as well as cardiovascular or renal events and cancer. We also present data on a set of nationwide analyses from Hungary, a middle-high-income country, a representative of the East-Central European Region, showing that the excess risk—when compared to non-diabetic individuals—is highest in the youngest age groups in terms of risk of mortality, myocardial infarction, stroke, dialysis, and also risk of cancer. We would like to raise the attention of caregivers to young individuals with type 2 diabetes who might be at a high risk as well.
Introduction
Type 2 diabetes mellitus (T2DM) is a high-frequency disease in the general population with an increase in prevalence (1, 2). It leads to several chronic complications, including cardiovascular, cerebrovascular, lower extremity arterial disease, microvascular complications such as diabetic kidney disease (DKD), retinopathy or neuropathy, and also non-vascular diseases such as an increased risk of cancer or infections (3). Cardiovascular events tend to develop earlier in cases with T2DM as compared to individuals without T2DM (4). The absolute number of such events generally increases with age and is highest in individuals with T2DM and advanced age (5).
In a recent publication of Emerging Risk Factors Collaboration (ERFC) Study group, the life expectancies in young patients with type 2 diabetes mellitus (T2DM) were proven to be less favorable than in older patients (6). On the other hand, they stated that “The generalizability of the findings was enhanced by inclusion of data from 97 prospective studies from 19 high-income countries…” The Emerging Risk Factors Collaboration Study included data from the USA, the UK, Australia, Austria, Canada, Caribbean countries, China, Denmark, Finland, France, Germany, Iceland, Ireland, Israel, Italy, Japan, Netherlands, New Zealand, Norway, Scotland, Spain, Sweden, Turkey, and Venezuela; however, over 98% of individual data arose from high-income countries. The related editorial (7) also called for attention related to young individuals with T2DM but asked if the findings of the original study were similar in middle- or high-income countries. Moreover, there is only sparse data regarding this perspective of lower-income countries in general in the literature.
The aim of our review was to summarize the data of countries with higher sociodemographic index and also to provide data on Hungary as a country with high-middle sociodemographic index for comparison as a bit of answer to the question raised by the abovementioned editorial (7). Furthermore, we aimed to provide data not only on overall survival but also on most important components of mortality and morbidity, as they also severely impact the life of the individuals living with T2DM. In the present paper, we would like to draw attention to young individuals with T2DM and propose that these individuals are also at a marked risk and prove that they could have a higher relative risk compared to the non-diabetic population than the older patients with T2DM.
Methods
Search strategy and selection criteria
For the purpose of the narrative review, several PubMed searches have been run on articles published in English in the period 2000–2024 using combinations of the terms “diabetes mellitus” or “type 2 diabetes mellitus” or “diabetes mellitus (type 2)” and “risk” or “relative risk” or “hazard ratio” or “odds ratio” and “complications” and “cardiovascular” or “renal” or “kidney” or “nephropathy” or “AMI” or “stroke” or “cancer” and “age at diagnosis” or “young age” or “early-onset” or “young-onset”.
Methods related to the studies from Hungary
The inclusion and exclusion criteria of the studies from Hungary as well as the detailed methods are provided in the original papers (8–13). Briefly, the data sources were the National Health Insurance Fund (NHIF) database and the Central Statistical Office (CSO) databases. The NHIF database covers mainly data related to diseases, medical diagnoses, interventions (such as coronary angiography, CT scans), and exact prescriptions of medications. The state insurance has nearly 100% coverage of the adult Hungarian population; thus, the NIF database enables a nationwide analysis. Therefore, data of all cases with T2DM and the entire population without DM can be compared. Furthermore, it also enables the use of matched control groups. Codes of the International Classification of Diseases (ICD) and data related to prescriptions of antidiabetic agents were used to set the diagnosis of T2DM as detailed in our original papers. Briefly, from the total population with diabetes, cases with gestational diabetes and polycystic ovary syndrome as well as cases with type 1 diabetes mellitus were excluded (12, 14–20). In our analysis of the period 2010–2013, data of more than 150,000 cases and more than 300,000 age-, gender-, and zip-code-matched controls could be compared in a 1:2 ratio manner (8, 9). The risks of mortality, acute myocardial infarction (AMI), stroke, and dialysis were analyzed, respectively. Because of the high costs, each individual dialysis case and event is captured by the NHIF database. Hemodialysis and peritoneal dialyses events were likewise taken into consideration. Event-free survival was tested in Cox regression models. As for the risk of cancer, in the studies, a population with incident T2DM of approximately 50,000 cases and a population with prevalent T2DM of approximately 600,000 cases could be compared to a non-diabetic adult population of approximately 7,000,000 cases (10, 11). In the studies on cancer, data were analyzed in the years 2015–2018 time frame, while we excluded cases diagnose with cancer in the preceding 5 years (i.e., 2009–2014) in order to try to exclude the recidivism of a previous cancer. Also here, a logistic regression was run for the analysis (10, 11).
Results
Epidemiological data related to age distribution of T2DM
Based on data of the IDF Atlas (2021 Edition), the worldwide number of cases with diabetes in the 20-24-year-old group is approx. 10 million, that of the 25-29-year-old-group is approx. 17 million, that of the 30-35-year-old group is approx. 25 million, that of the 35-39-year-old group is approx. 35 million. Summing up, the <40-year-old group could account for over 80 million cases worldwide. The 40-49-year-old age group could account for further 100 million cases worldwide (1). In the UK, the incidence of T2DM diagnosed at the age < 40 years, rose from 239 to 1541/100,000 individuals (21). The 2019 Global Burden of Disease (GBD) Study found that the incidence of individuals with T2DM in the 15–39 years age-range increased from 117.22 (95% CI: 117.07-117.36)/100,000 population in 1990 to 183.36 (95% CI: 183.21-183.51)/100,000 population in 2019 (2). Other data also indicate a rise in incidence of youth-onset T2DM that also accounts for an increasing burden for the society (22).
We have to mention, that the definition on young-onset T2DM or youth-onset T2DM or early-onset T2DM is quite heterogenous. Most studies refer to a <40-year-old adult population (6, 23–29), others use other cut-offs, some also include adolescent populations, as well (2, 30). Also, some papers compare <40 vs. >40-year-old groups (25), others a <40 vs. >60-year-old group, some show more detailed data in groups of decades of age (6, 8–11), thus the literature is quite heterogenous in that regard, as well. In the present review, we tried to capture data on young adults with T2DM, in the age of 18 to 39 years.
The role of long duration and young age at diagnosis of diabetes as a risk factor of developing complications
When talking about the development of complications in young individuals with T2DM, it is hard to disclose the effect of diabetes duration on the risk of complications. With a long observation period, the younger the patient developed T2DM, the longer the duration will be by the end of the observational period. Unfortunately, in the literature, terms of young individuals and young-onset individuals are frequently used interchangeably, here, lower age at observation shall in fact be accompanied by a lower diabetes duration. Actually, the use of terms is more problematic in case of the older individuals with T2DM, as here, older individuals have frequently also a longer duration of diabetes, but since T2DM frequently develops also in more advanced age, some older individuals may have a short duration of diabetes. Diabetes duration is a known risk factor of developing complications (5), thus, in the present review we intended to find data related to age itself.
Data related to risk factors (including hypertension and dyslipidemia) and age
In a study from Hong-Kong, patients with younger age at diagnosis had higher HbA1c slope, faster deterioration of glycemic control and reacted less to metformin-based glucose-lowering treatment (31). A UK primary-care database-derived dataset found that individuals diagnosed with T2DM at an age of 18–39 years had higher HbA1c, higher LDL-cholesterol and more frequent obesity and lower use of antihypertensives or statins (26). In a cross-sectional study, the percentage of patients with CV disease and hypertension without receiving an antihypertensive agent was significantly higher in <40 years-age at diagnosis vs. >40 years-age at diagnosis (26.3 vs. 16.8) (25).
Another UK-based analysis also found that younger (< 40 years) age at diagnosis of T2DM is associated with higher HbA1c, LDL-cholesterol, triglycerides and obesity as compared to individuals with higher age at diagnosis of T2DM (28). A US-based analysis found a decrease in global longitudinal strain in young individuals with T2DM or with obesity as compared to controls, and this showed an association with age. The authors proposed that young-onset T2DM or obesity could predispose to the development of heart failure (32). According to a review, in general, a change in beta cell mass and obesity may contribute to early onset of T2DM (21). Besides, in a meta-analysis age-stratified analysis showed slightly higher adherence to oral antidiabetic drugs in older T2DM patients, with rates ranging from 49% in the youngest group to 58% in the oldest, although this trend was not statistically significant (p = 0.14) (33). In one of our earlier papers (14), we also found age-related differences in statin medication adherence in Hungary, where the younger cohort presented significantly lower, 7.9%-11.8% adherence during 12 months, while rates of adherence were 15.9% to 23.5% in older cohorts. Overall, age seemed to influence adherence more than gender, though the results did not reach significance, consequently, worse adherence to OADs may also play a relevant role in higher risk of diabetes complications.
Data related to risk of mortality and age
The earlier mentioned study analyzing data of the Emerging Risk Factors Collaboration project found a higher hazard ratio (HR) values of mortality in patients diagnosed with T2DM at young age [30–39 years, 2.69 (95% CI 2.43–2.97)], while it decreased with age 40–49 years, 2.26 (2.08–2.45); 50–59 years, 1.84 (1.72–1.97); 60–69 years, 1.57 (1.47–1.67) and 70+ years, 1.39 (1.29–1.51) (6). The majority of cases of death were non-cardiovascular and were not related cancer, either (7). Despite worse status of cardiovascular risk factors in the young, the UK primary care-based analysis found similar mortality in different age groups (26).
Data related to risk of macrovascular complications, cardiovascular disease, and age
In a study from China, the OR of developing CVD was 1.72 (1.36-2.17) in patients diagnosed with T2DM at the age of <40 as compared to those diagnosed with >60 years of age. The earlier T2DM was diagnosed, the higher was the odds of developing CVD (14% OR increase for every 5 years decrease in age) (27).
Worse glycemic control was associated with micro- and macrovascular complications [HR, 1.389 (1.163-1.658) and 1.252 (1.110-1.413), respectively] in individuals with young-onset diabetes, but not in middle-age-onset diabetes or late-onset-diabetes in a study from Korea (29). One study found a higher CVD risk in younger-onset T2DM vs. older-onset T2DM [hazard ratio: 1.48 (1.17-1.88)] (34). Research data from Singapore suggest that early-onset (<40 years) T2DM is associated with an 1.91 (1.19-2.40) hazard ratio of incident heart failure as compared to usual-onset T2DM. Adjustment for traditional risk factors had only a mild impact on the association, while adjustment for renal parameters abolished the association (35).
One study investigated data from Australia related to overall and cardiovascular mortality at different age at diagnosis of T2DM and found that there is an excess risk of CV mortality associated with earlier age at diagnosis, but this was mainly the effect of diabetes duration (36).
Data related to risk of diabetic neuropathy and age
Another study, using propensity score matching, has found higher odds ratio in early-onset vs. in late-onset T2DM (<40 years vs. > 40 years) diabetic polyneuropathy (OR: 1.672), however, the risk disappeared when correcting for duration of diabetes (34). In the study, duration of T2DM especially that of >20 years had a marked effect, but in a logistic regression, also age of T2DM onset was associated with CV complications, the risk of neuropathy was only associated with age in the <40 year-old at diagnosis group, not the >40 year-old group (25). In a follow-up study of patients with a long duration (11.6+/-9.6 years for young-onset T2DM and 7.2+/-6.8 years for later-onset T2DM) form Korea, the risk of neuropathy was higher in the younger age group [OR: 3.05 (2.57-3.61)], and this has remained significant, even after correcting for duration of diabetes [OR: 1.39 (1.13-1.71)] (37).
Data related to risk of diabetic retinopathy and age
Young-onset T2DM (<40 years) is associated with a high risk of diabetic retinopathy, especially in association with diabetic kidney disease, even with a duration of diabetes of only 3.7 ± 4.3 years (38). Another study also found a higher risk of retinopathy (2.906) in younger cases with T2DM (39). In the already mentioned study from Korea of patients with a longer duration (overall 8.0 ± 7.5 years) of diabetes, the risk of retinopathy was higher in the younger cohort [OR: 2.68 (2.14–3.35)], but this was mainly the consequence of a longer duration of DM, as after statistical correction for the duration the excess risk disappeared [OR: 0.98 (0.75–1.30)] (37).
Data related to risk of diabetic kidney disease and age
Addressing kidney disease in epidemiological studies may be a hard issue, as various definitions and various endpoints could be used. Diabetic nephropathy is nowadays rather regarded as a histopathological diagnosis, and especially in individuals with T2DM, diabetic kidney disease (DKD) or chronic kidney disease (CKD) in DM could be appropriate endpoints. However, the definition of CKD or DKD would rely on abnormal albuminuria/proteinuria and/or decreased GFR in larger-scale studies, which may be affected by substantial bias in testing and may not be available in nationwide analyses. Moreover, CKD may be severely underreported when relying on ICD codes (40). In some analyses, hard endpoints such as initiation of dialysis and/or renal-related mortality are rather investigated.
A study with a median follow-up of 7.1 years found that young-onset (<40 years) T2DM was associated with a 35% higher hazard of CKD when compared to late-onset T2DM, but—just like in the case of CVD risk—this has vanished after controlling for diabetes duration (34). In the Korean study, young-onset T2DM was associated with higher odds of CKD [OR: 2.98 (2.27–3.90)] as compared to late-onset T2DM even in a multivariate analysis. However, when further correcting for T2DM duration, the excess risk disappeared [OR: 1.30 (0.93–1.80)]. Using cluster analysis, the same study found a higher percentage of severe insulin-deficient diabetes (46.4% vs. 22.7%) and less mild age-related (27.5% vs. 44.0%) and mild obesity-related (18.5% vs. 27.9%) diabetes within the persons with T2DM in the early-onset vs. the late-onset group (37).
A propensity-score-matched study found a higher risk of chronic kidney disease (CKD) (1.967) in younger-onset vs. older-onset T2DM (39). With regard to CKD, another study from Korea found that young-onset T2DM was associated with 1.70 (1.15–2.51) times higher odd as compared to late-onset T2DM. Within the young-onset group, hypertension, dyslipidemia, and sulphonylurea use determined the development of CKD (41). Data from Australia have shown that when investigating a combined endpoint of renal replacement therapy or renal-related death, young-onset T2DM was associated with a 2.0 (1.4–2.9) hazard ratio, even after adjustment for the duration of diabetes and other parameters. Adjustment for BMI weakened the association significantly (42).
Data related to cancer
Since the prevention and treatment of acute complications and chronic, vascular complications have improved, we are faced with an increase of lifespan in our patients with T2DM. Thus, new long-term complications such as cancer or dementia are on the rise (3). Furthermore, data from the US suggest a rise in incidence of cancer in young individuals in general (these data are not related to T2DM specifically) between 2010 and 2019 [annual percent change, APC,+0.28% (+0.09–+0.47%)] (43).
A further paper presents data on newly diagnosed cases with T2DM with regards of cancer risk and age and found that the relative risk, expressed as standardized incidence ratio was highest [1.48 (1.41-1.54)] in the 20-54-year-old subgroup, decreased with the increase of age and turned even lower than 1.0 in the 76+ age group [0.86 (0.84-0.89)]. In that paper, data related site-specific cancer occurrence was also analyzed and similar result were found for individual cancer types (44).
Data from Australia show that cancer mortality (not incidence) rate ratio comparing young-onset vs. late-onset T2DM increased with increasing actual age; however, diabetes duration had a main influence on the data (36).
Data arising for Hungary, a middle-high income country, related to the risk of mortality, cardiovascular and renal complications, and cancer in young individuals with T2DM
Hungary is found in the $50,000–100,000 income category along with, e.g., Poland, the Czech Republic, Slovakia, Croatia, and Romania (i.e., East-Central Europe) according to an analysis of Credit Suisse from 2021. For comparison, most countries participating in the ERFC Study are either in the $150,000–250,000 income category (such as Italy of Spain) or in the 250,000–350,000$ group (such as Austria, Canada, France, Germany, Iceland, Japan, New Zealand, the UK, Sweden, or Norway), in the $350,000–500,000 category (such as Australia, Belgium, Denmark, and Netherlands), or in the >$500,000 income category (such as the USA) (45, 46).
In addition, Hungary has ranked #52 in the list of countries according to wealth as opposed to the countries participating in the EFRC Study, where most countries rank higher than #25 (47). Thus, our data represents a country with a substantially lower income and wealth than that of the ERFC Study Group. Moreover, the GBD Study methodology also creates six so-called super-regions: the high-income super-region includes the US, Canada, Greenland, Australia, New Zealand, Brunei, Japan, Korea, Singapore, Argentina, Chile, Uruguay, and all countries from Western Europe. On the contrary, another super-region category was created to include Central Europe, Eastern Europe, and Central Asia, and this region includes Hungary (48). Thus, data related to Hungary may rather represent this super-region than that of high-income countries.
Between 2016 and 2024, our workgroup has published numerous analyses related to the field of epidemiology of diabetes mellitus in a program supported by the Hungarian Diabetes Association and based on data of the National Health Insurance Fund in Hungary (8–11, 13, 20, 49, 50). In general, the studies are based on data of NHIF and the CSO of Hungary.
According to our studies, upon the age pyramid of the populations, the relative frequency of the 18- to 39-year-old age group was 4.49% among patients with incident T2DM and 1.47% among patients with prevalent T2DM, while the frequency of the 40- to 49-year-old age group was 12.80% among patients with incident T2DM and 6.59% among patients with prevalent T2DM in Hungary (10, 11).
Our workgroup has investigated mortality and cardiovascular risk in T2DM in a nationwide analysis in different age groups as compared to individuals without diabetes from the same age group. We found that the hazard of all-cause mortality was highest in the 31–40 group [HR, 1.98 (1.34–2.92)], and similar data were found for myocardial infarction [3.50 (1.70–7.23)] and stroke [4.64 (2.55–8.45)]. The hazards for all three outcomes decreased steeply with increasing age but remained significant even in the 70+ age group (Figure 1). Individuals with an age between 19 and 30 years had a low event rate. Thus, the HR values were too broad to achieve statistical significance (8).
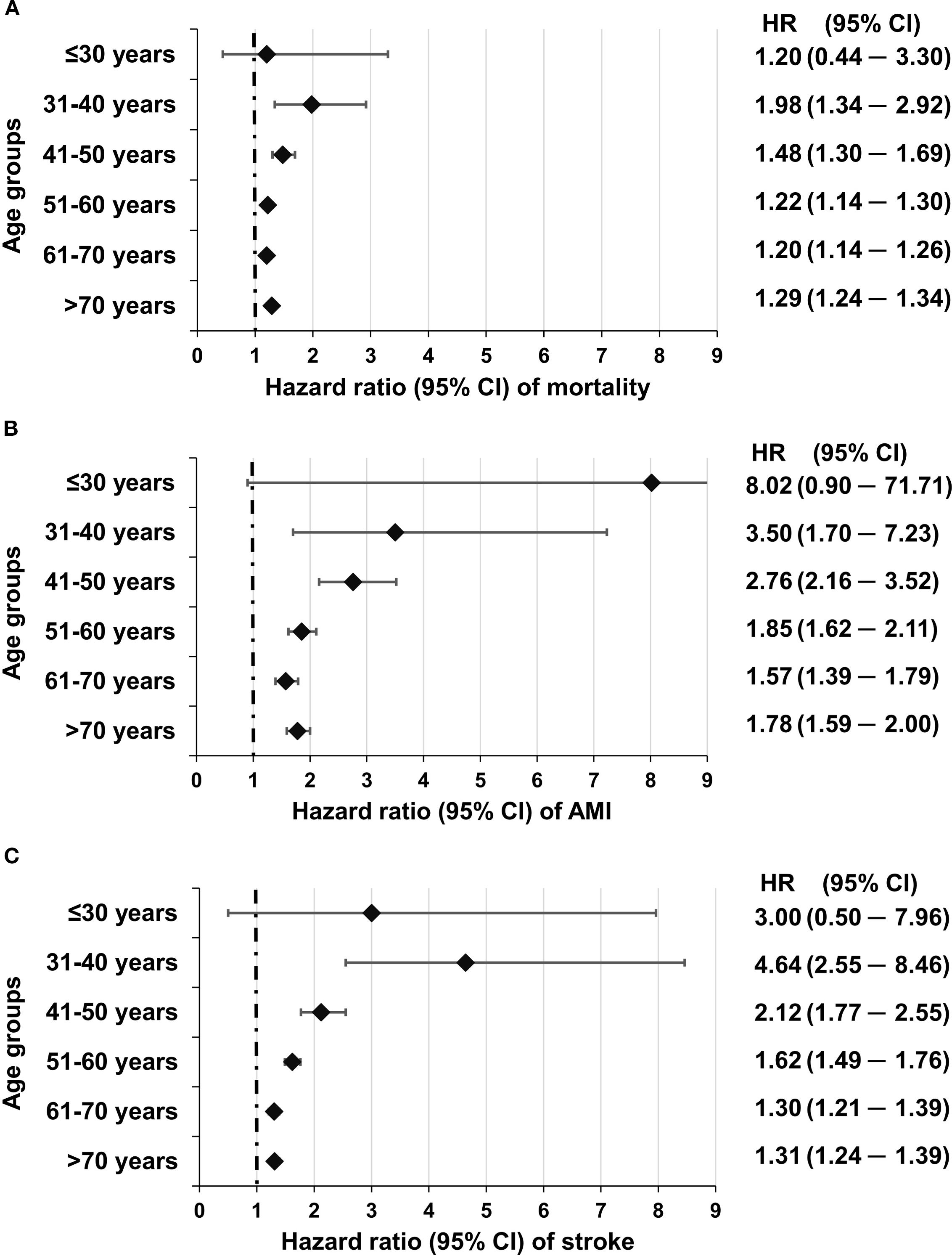
Figure 1. Risk of mortality (A) myocardial infarction (B) and stroke (C) in different age groups in individuals with T2DM as compared to individuals without diabetes from the same age group. Reproduced with permission from (8), under a Creative Commons 4.0 license.
As for the risk of dialysis, the data of our workgroup have shown that there is also a significant (p<0.05) interaction between the hazard of dialysis and the age of the patients. Moreover, for this endpoint, the highest hazard ratio was found in the ≤40-year-old group [HR (95% CI), 2.80 (1.55–5.05)], which gradually decreased with increasing age [41–50 years, 2.38 (1.74–3.27); 51–60 years, 2.28 (1.90–2.74); 61–70 years, 1.79 (1.54–2.07)], and it was lowest yet still significant in patients >70 years of age [1.71 (1.49–1.97)] (9) (Figure 2). Furthermore, here we must acknowledge that the confidence interval of HR was widest in the youngest age group, yet the data of more than 11,000 patients were compared to the data of more than 23,000 subjects (T2DM vs. controls).
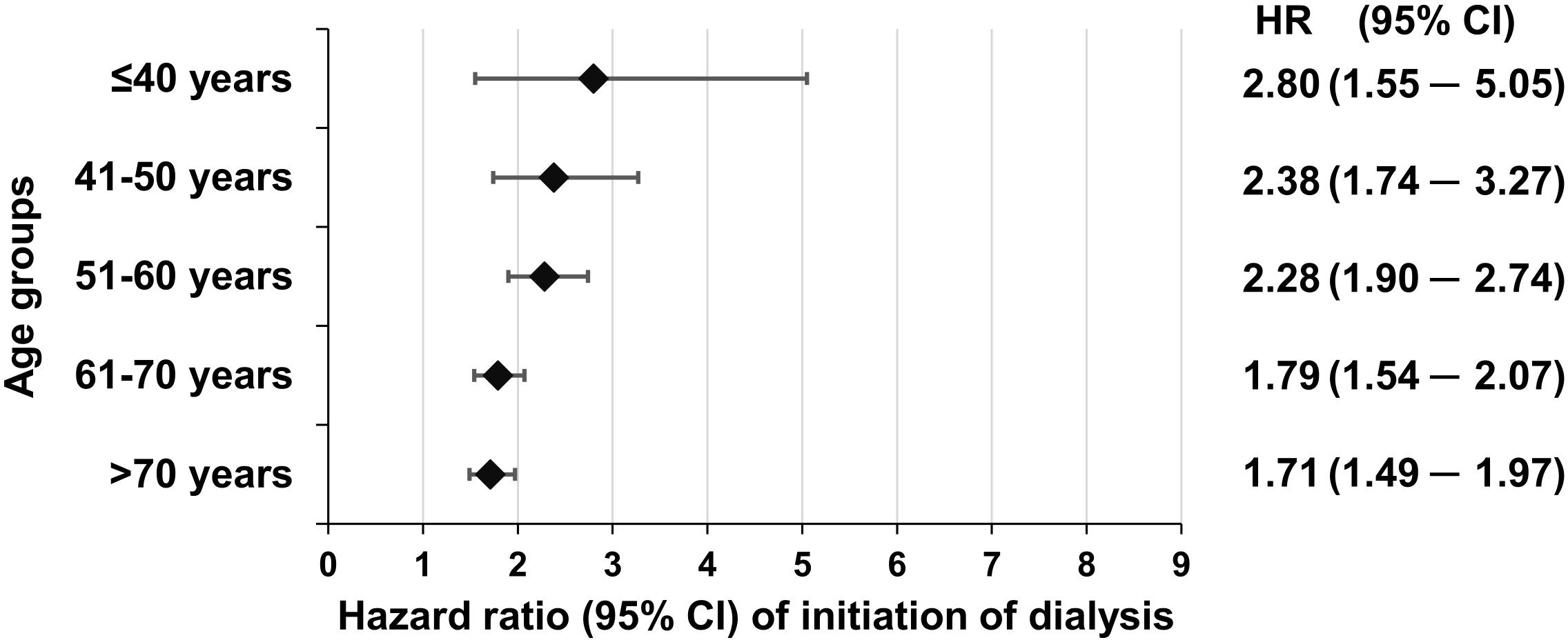
Figure 2. Adjusted hazard ratios related to the initiation of dialysis in individuals with T2DM in different age groups as compared to non-diabetic individuals. Reproduced from (9) with the permission of the publisher.
As for the risk of cancer, our workgroup found in a further nationwide study that in patients with incident T2DM (which is independent from duration of diabetes), when compared to more than 7,000,000 non-diabetic individuals, the risk of developing cancer was highest [OR, 4.22 (2.45–7.92)] in the 18–39 years old age group, and it was higher than in the 60–69, in the 70–79, or the 80+ age groups (Figure 3) (10).
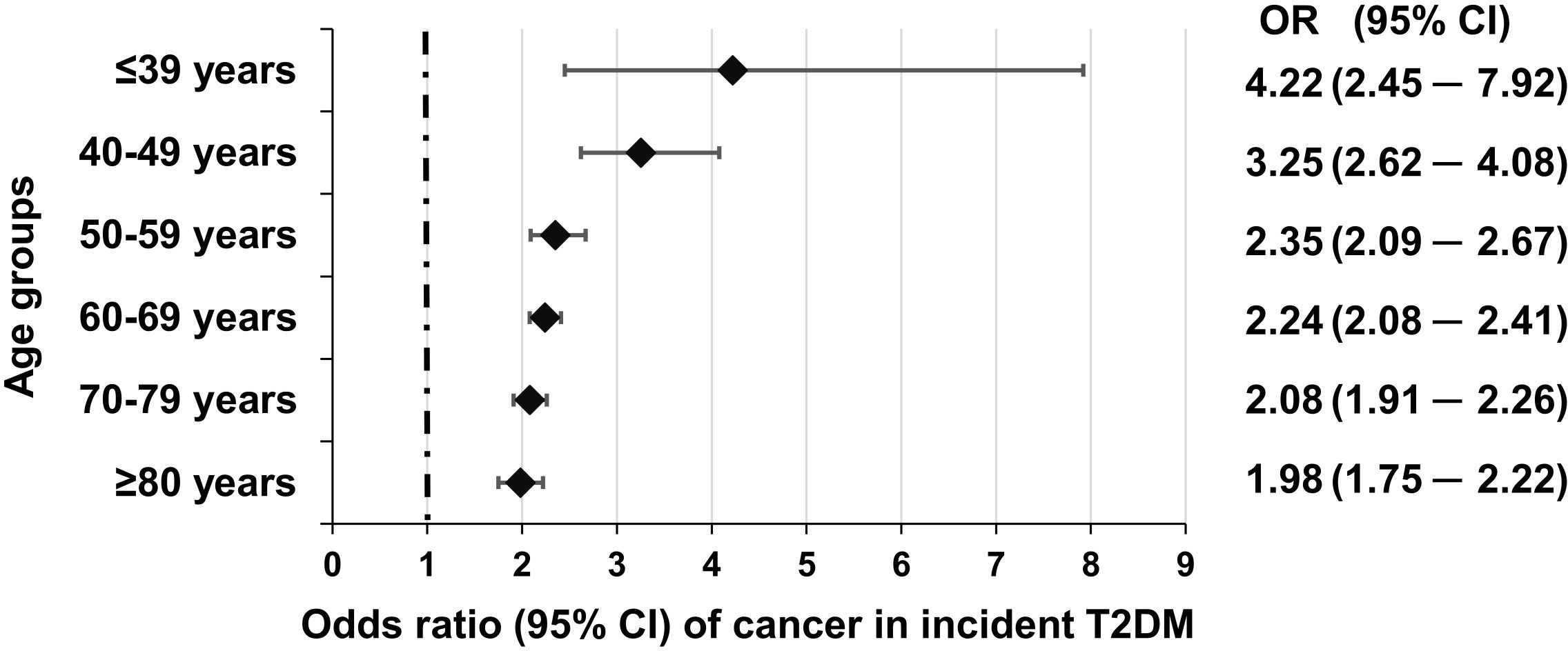
Figure 3. Odds of incident cancer in individual age groups in incident T2DM as compared to non-diabetic individuals. Reproduced from (10) under a Creative Commons license.
In another paper, we analyzed the prevalent cases of T2DM derived from the nationwide dataset, and also here we found a similar pattern than in the case of incident diabetes, the odds of developing cancer was highest in the 18–39 age group [2.23 (1.58–3.25)], and the odds ratio decreased with increasing age (11) (Figure 4).
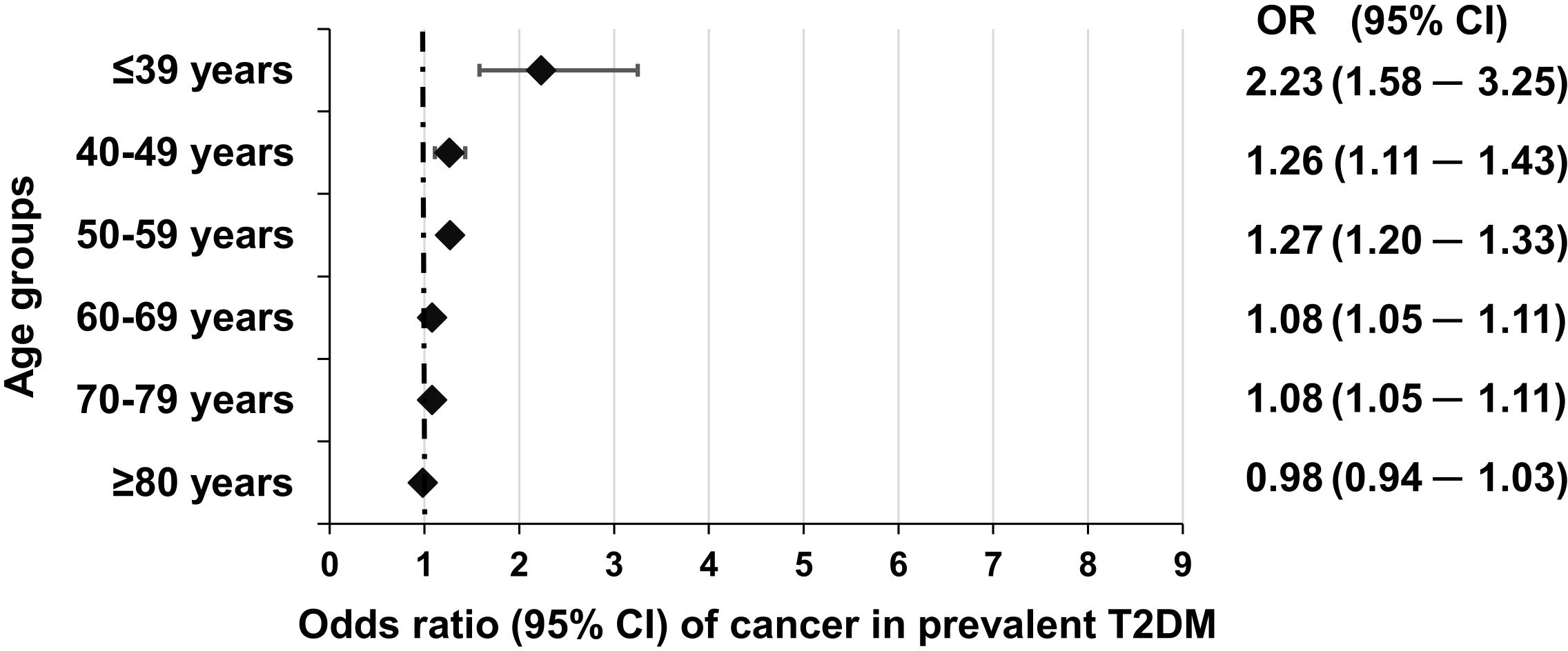
Figure 4. Odds of incident cancer in individual age groups in prevalent T2DM as compared to non-diabetic individuals. Reproduced from (11) under a Creative Commons license.
Pathogenesis of early T2DM
The pathogenesis of classical T2DM developing in middle-aged to elderly patients is well established; that of young-onset T2DM shares some characteristics but has also distinct features. The risk factors may include female gender, positive family history, obesity, gestational diabetes, maternal diabetes with in utero exposure, hypertension, dyslipidemia (51–55), and certain ethnic groups (such as Native people, Latino, Pacific Islander in the US (56) or Asian and Black people in England and Wales (57)). Obesity and prolonged insulin resistance may even be a stronger determinant of the development of early-onset T2DM than in the case of late-onset T2DM (22, 58–60). Puberty and related hormonal changes may affect the development of prediabetes in young adolescents and hence contribute to the development of early-onset T2DM (61, 62).
Data in the literature suggests that the fate of beta cells is different in early-onset vs. late-onset T2DM. Cases with early-onset T2DM may have a faster progression of deterioration of beta cell function (51, 52, 61); some data imply that the marked insulin resistance in these individuals further increases the loss of beta cell function (61).
In addition to genetic and metabolic factors, emerging evidence points to the role of psychosocial stress, adverse childhood experiences (63), sleep deprivation (64), and environmental endocrine-disrupting chemicals (65) in the early development of insulin resistance and T2DM in young people. These influences may contribute to unhealthy coping mechanisms (e.g., emotional eating), central adiposity, and chronic inflammation.
Prevention of early-onset type 2 diabetes mellitus
The real primary prevention would be related to preventing the development of a manifest T2DM in high-risk young adults or even adolescents. A secondary prevention strategy could be used to reverse the development of T2DM and lead to remission in a patient who has already developed T2DM. A tertiary prevention aim could be the prevention of the development of complications of DM.
Non-pharmacological approaches may include patient education, diet (with omission of ultra-processed foods, high-carbohydrate-content meal, and soft-drinks), and exercise (62, 66). Of the pharmacological treatment possibilities, data related to metformin is rather controversial. Metformin has a label indication of use in case of prediabetes in adults, but not children or adolescents, and it is also indicated in polycystic ovary syndrome, another risk factor of the development of T2DM (62). However, the failure rate with metformin may be substantial (62, 67). Of the classical antidiabetic agents, a meta-analysis showed that pooled data of sodium-glucose transporter-2 (SGLT2) inhibitors empagliflozin and dapagliflozin indicate a protective effect against new-onset T2DM (62). In patients with prediabetes and obesity, GLP-1+/- GIP receptor agonists may be beneficial (68) also in young individuals (69), and recent data indicate that large doses of semaglutide led to a higher chance of normoglycemia (70), while large doses of tirzepatide led to a lower risk of new-onset T2DM as compared to placebo (62). Data also suggest that inhibitors of the renin–angiotensin–aldosterone system as well as supplementation with vitamin D might have a positive impact on the development of T2DM (68).
Beyond western medicine, traditional Chinese medicine (TCM) may also be an alternative way of preventing T2DM or its complications when used by a skilled person. Moreover, in TCM, non-pharmacological approaches such as specific types of exercise, emotional therapy, acupuncture, and nutritional approaches exist to try to prevent the development of T2DM (71). Furthermore, TCM gained attention in relation to specific medicines that could be used for delaying the progression by acting on glucose control, on inflammation, the microbiome, the glucagon-like-peptide-1 system, the glycogen metabolism, and the function of the beta cells. These medications may include Jinlida granule, Tianqi capsule, Tang-Min-Ling-Wan, Xiaoke Pill, or Jinqi Jiangtang. For a more profound overview, we suggest the review by Ni et al. (72) and Chen et al. (73), respectively. A meta-analysis suggests that Tianqi capsules may be effective in the prevention of T2DM (74).
Young-onset T2DM and associated risk in male vs. female subjects
A detailed discussion of this topic is beyond the scope of the review, but we must admit that data is controversial. Some data suggest that young-onset T2DM is more frequent in women than in men and relate this fact to the effect of puberty and/or polycystic ovarian syndrome (21, 61, 75, 76). However, data from the US suggest that during adolescence, men may be more frequently affected by T2DM than women (22). The prevalence increases in both men and women worldwide, with a numerically higher increase in men, and in 2021, the number of cases was slightly higher in men than in women according to the Global Burden of Disease (GBD) Study (77). Furthermore, the age-standardized incidence was approximately 30% higher in the GBD study (2).
As to the complications, according to our studies, the hazard ratio related to the mortality of women with T2DM [1.37 (1.31–1.42)] was higher than that of men with T2DM [1.17 (1.12–1.21), p<0.001] when compared to women and men without T2DM. The HR of AMI was not different for women vs. men with T2DM [1.77 (1.59–1.98) vs. 1.83 (1.68–2.00), p=0.64), but the risk of stroke was again higher in women than in men with T2DM [HR: 1.14 (1.40–1.55) vs. 1.33 (1.26–1.41), p=0.01] (8). Concerning the risk of dialysis, the HR was higher in men than in women [2.21 (1.94–2.52) vs. 1.91 (1.68–2.17), p=0.031] (9). In cases with incident T2DM, the risk of cancer was similar in women and men with a tendency of favoring men (10). As for prevalent T2DM cases and cancer, the risk was significantly higher in men than in women [OR: 2.76 (2.76–2.82) vs. 2.27 (2.22–2.33), p<0.05] (11).
It is important to note that women generally have a lower baseline cardiovascular and mortality risk in the general population compared to men (78). Therefore, since the absolute risks of complications or death are similar or even moderately elevated in women with T2DM, the relative risks (e.g., hazard ratios vs. non-diabetic controls) may appear higher than in men. We could say that T2DM annihilates the relative protection seen in healthy women. This well-known epidemiological phenomenon may partly explain the seemingly higher excess risk observed in female patients with T2DM, especially in outcomes like all-cause mortality and stroke (8).
Young-onset T2DM worldwide
The regional distribution of cases with young-onset T2DM is heterogenous. According to the Global Burden of Disease 2019 study, while the incidence of young-onset T2DM was highest in countries with low-middle to middle incomes, the related mortality of young-onset T2DM was highest in low-income countries. This may be related also to a high variance in the geographical distribution of risk factors such as the high consumption of processed or red meat, low consumption of fruits and whole grains, and differences in smoking habits (2). According to data from the IDF, the prevalence of young-onset (<40 years) T2DM was highest in the Western Pacific region, followed by Southeast Asia, the Middle East and North Africa region, and Africa, and it was substantially lower in Europe, North America and the Caribbean region, and South and Central America region (21). Moreover, the increase in prevalence was most notable in the Western Pacific Region, followed by Southeast Asia and the Middle East and North Africa region. There was a much lower rate of increase in North and South-Central America, while the prevalence was more or less stagnant in Europe (21).
Conclusions
As for the general population, data indicate that while trends related to cardiovascular risk in elderly or middle-aged individuals are beneficial, on the contrary, young individuals have constant or even slightly increasing trends in the rate of events (79). A narrative review summarized evidence related to age and risk factors in the general population and strengthens the previous observation (80).
The data summarized in the present review indicates that young individuals do have a high risk of developing complications. In epidemiological studies, it is hard to distinguish the role of age, age at diagnosis, or diabetes duration as risk factors. The longer the follow-up, the more the results may be influenced by diabetes duration. Therefore, studying cases with incident T2DM is of excess value.
We have to emphasize that the absolute risk and the number of cases with complications is increasing as the age increases, but the relative risks or hazards may be highest in individuals with lower ages, as the number of events is relatively high in individuals with T2DM in these age groups. At the same the time, the number of events is low in the background population in the same age groups.
We presented a complex dataset from a middle-high income country supporting the excess risk of young individuals with T2DM in terms of overall mortality, the risk of myocardial infarction, the risk of stroke, the risk of dialysis and, as a novelty, also the risk of cancer. Our observations provide unique data for an East-Central European country.
Summing up, we believe that we should broaden our perspective related to T2DM and focus on young individuals as well. We should try to implement strategies not only to prevent the development of T2DM in young individuals but also to screen for complications in young cases with T2DM.
Limitations
The present study was aimed at describing the risks associated with young-onset T2DM. It is not a systematic review, and no formal meta-analysis was carried out. Related to the data from Hungary, a clear limitation is that data of only one country were analyzed. However, we do not have access to data from any of the neighboring countries. We are not aware of another set of epidemiological studies from other countries in Central Europe as the set of more than 20 papers from the analyses of Hungarian data introduced above. The studies have been published between 2018 and 2024, cover the time frame 2009–2020, and represent not only one study but a set of studies arising from the same database system, on different time periods, with different populations, and of different methodologies.
A further limitation is that the NIF database does not cover any anthropometric parameters, laboratory data, nor data related to smoking, a clear risk factor in terms of cardiovascular, renal, or malignant diseases. Thus, comparisons could not be corrected to these factors.
In addition, the effect of the duration of diabetes cannot be ruled out in the case of studies on cases with prevalent T2DM. However, the analysis on cancer risk in individuals with incident T2DM rules out the contribution of longer duration to the excess risk in younger patients with T2DM.
Author contributions
GM: Writing – review & editing, Writing – original draft. ZK: Writing – original draft, Writing – review & editing. IW: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
The authors are grateful to Professor Dr. József Andor for the linguistic revision.
Conflict of interest
GM received honoraria for lectures from Astra Zeneca, Boehringer Ingelheim, Eli Lilly, Krka, Merck, NovoNordisk, Novartis, Sanofi, Swixx, was supported for attending meetings by AstraZeneca, Boehringer Ingelheim, Medtronic, Eli Lilly, NovoNordisk, Sanofi, and was an advisory board member for Eli Lilly and NovoNordisk. ZK is a post-doc research fellow at the University of Pécs Medical School, 2nd Department of Medicine and Nephrology-Diabetes Centre, Pécs, Hungary, however he is at the same time also an employee of MSD Pharma Hungary Ltd, that provides no relevant conflict of interest with the present study. IW received honoraria for lectures from Astra Zeneca, Boehringer Ingelheim, Eli Lilly, Krka, Merck, NovoNordisk, Novartis, Sanofi, was supported for attending meetings by AstraZeneca, Boehringer Ingelheim, Medtronic, Eli Lilly, NovoNordisk, Sanofi, and was an advisory board member for AstraZeneca, Boehringer Ingelheim, Eli Lilly, NovoNordisk and Sanofi.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1638565/full#supplementary-material
References
1. International Diabetes Federation. IDF Diabetes Atlas. 10th edition. Brussels, Belgium: International Diabetes Federation (2021). Available online at: www.diabetesatlas.org (Accessed August 10, 2025).
2. Xie J, Wang M, Long Z, Ning H, Li J, Cao Y, et al. Global burden of type 2 diabetes in adolescents and young adults, 1990-2019: systematic analysis of the Global Burden of Disease Study 2019. BMJ. (2022) 379:e072385. doi: 10.1136/BMJ-2022-072385
3. Harding JL, Pavkov ME, Magliano DJ, Shaw JE, and Gregg EW. Global trends in diabetes complications: a review of current evidence. Diabetologia. (2019) 62:3–16. doi: 10.1007/s00125-018-4711-2
4. Booth GL, Kapral MK, Fung K, and Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet. (2006) 368:29–36. doi: 10.1016/S0140-6736(06)68967-8
5. Huang ES, Laiteerapong N, Liu JY, John PM, Moffet HH, and Karter AJ. Rates of complications and mortality in older patients with diabetes mellitus the diabetes and aging study. JAMA Intern Med. (2014) 174:(2):251–8. doi: 10.1001/jamainternmed.2013.12956
6. Kaptoge S, Seshasai SRK, Sun L, Walker M, Bolton T, Spackman S, et al. Life expectancy associated with different ages at diagnosis of type 2 diabetes in high-income countries: 23 million person-years of observation. Lancet Diabetes Endocrinol. (2023) 11:731–42. doi: 10.1016/S2213-8587(23)00223-1
7. Duncan BB and Schmidt MI. Many years of life lost to young-onset type 2 diabetes. Lancet Diabetes Endocrinol. (2023) 11:709–10. doi: 10.1016/S2213-8587(23)00255-3
8. Kiss Z, Rokszin G, Abonyi-Tóth Z, Jermendy G, Kempler P, Aradi D, et al. Dissimilar impact of type 2 diabetes on cardiovascular outcomes according to age categories: A nationwide population study from Hungary. Cardiovasc Diabetol. (2018) 17:1–8. doi: 10.1186/s12933-018-0751-7
9. Rokszin G, Kiss Z, Abonyi-Tóth Z, Jermendy G, Kempler P, Wittmann I, et al. Dialízis T2DM-ben szenvedő betegekben – a hazai adatbázis elemzésének eredményei. Diabetol Hungarica. (2023) 31:7–15. doi: 10.24121/dh.2023.1
10. Abonyi-Tóth Z, Rokszin G, Fábián I, Kiss Z, Jermendy G, Kempler P, et al. Incident cancer risk in patients with incident type 2 diabetes mellitus in Hungary (Part 1). Cancers (Basel). (2024) 16:1745. doi: 10.3390/cancers16091745
11. Abonyi-Tóth Z, Rokszin G, Sütő G, Fábián I, Kiss Z, Jermendy G, et al. Incident cancer risk of patients with prevalent type 2 diabetes part 2). Cancers (Basel). (2024) 16:2414. doi: 10.3390/cancers16132414
12. Jermendy G, Kempler P, Abonyi-Tóth Z, Rokszin G, and Wittmann I. Changes in features of diabetes care in Hungary in the period of years 2001–2014. Aims and methods of the database analysis of the National Health Insurance Fund - in Hungarian. Orv Hetil. (2016) 157:1259–65. doi: 10.1556/650.2016.30519
13. Jermendy G, Kiss Z, Rokszin G, Fábián I, Wittmann I, and Kempler P. Changes in mortality rates and ratios in people with pharmacologically treated type 2 diabetes mellitus between 2001 and 2016 in Hungary. Diabetes Res Clin Pract. (2020) 163:108134. doi: 10.1016/J.DIABRES.2020.108134
14. Kiss Z, Nagy L, Reiber I, Paragh G, Molnar MP, Rokszin G, Abonyi-Toth Z, Mark L, et al. Persistence with statin therapy in Hungary. Arch Med Sci. (2013) 9:409. doi: 10.5114/AOMS.2013.35327
15. Jermendy G, Kiss Z, Rokszin G, Abonyi-Tóth Z, Wittmann I, and Kempler P. Decreasing incidence of pharmacologically treated Type 2 diabetes in Hungary from 2001 to 2016: A nationwide cohort study. Diabetes Res Clin Pract. (2019) 155:107788. doi: 10.1016/j.diabres.2019.107788
16. Sütő G, Molnár GA, Rokszin G, Fábián I, Kiss Z, Szekanecz Z, et al. Risk of morbidity and mortality in patients with type 2 diabetes treated with sodium-glucose cotransporter-2 inhibitor and/or dipeptidyl peptidase-4 inhibitor: a nationwide study. BMJ Open Diabetes Res Care. (2021) 9(1):e001765. doi: 10.1136/bmjdrc-2020-001765
17. Rokszin G, Kiss Z, Sütő G, Kempler P, Jermendy G, Fábián I, et al. Sodium-glucose co-transporter 2 inhibitors may change the development of urinary tract and hematological malignancies as compared with dipeptidyl peptidase-4 inhibitors: Data of the post-hoc analysis of a nationwide study. Study. Front Oncol. (2021) 11:725465. doi: 10.3389/fonc.2021.725465
18. Jermendy G, Kiss Z, Rokszin G, Abonyi-Tóth Z, Lengyel C, Kempler P, et al. Changing patterns of antihyperglycaemic treatment among patients with type 2 diabetes in hungary between 2015 and 2020-nationwide data from a register-based analysis. Medicina (Kaunas). (2022) 58(10):1382. doi: 10.3390/medicina58101382
19. Jermendy G, Kiss Z, Rokszin G, Abonyi-Tóth Z, Wittmann I, and Kempler P. Decreasing incidence of pharmacologically treated Type 2 diabetes in Hungary from 2001 to 2016: A nationwide cohort study. Diabetes Res Clin Pract. (2019) 155:107788. doi: 10.1016/j.diabres.2019.107788
20. Jermendy G, Kiss Z, Rokszin G, Abonyi-Tóth Z, Wittmann I, and Kempler P. Persistence to treatment with novel antidiabetic drugs (Dipeptidyl peptidase-4 inhibitors, sodium-glucose co-transporter-2 inhibitors, and glucagon-like peptide-1 receptor agonists) in people with type 2 diabetes: A nationwide cohort study. Diabetes Ther. (2018) 9:2133–41. doi: 10.1007/s13300-018-0483-4
21. Lascar N, Brown J, Pattison H, Barnett AH, Bailey CJ, and Bellary S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. (2018) 6:69–80. doi: 10.1016/S2213-8587(17)30186-9
22. Rodriquez IM and O’Sullivan KL. Youth-onset type 2 diabetes: burden of complications and socioeconomic cost. Curr Diabetes Rep. (2023) 23:59–67. doi: 10.1007/s11892-023-01501-7
23. Song SH. Young-onset type 2 diabetes: No room for complacency. Lancet Glob Heal. (2014) 2:924–5. doi: 10.1016/S2213-8587(14)70147-0
24. Song SH. Young-onset type 2 diabetes and retinopathy: evidence of an adverse phenotype. BMJ Open Diabetes Res Care. (2024) 12:2023–4. doi: 10.1136/bmjdrc-2023-003899
25. Song SH and Hardisty CA. Early onset type 2 diabetes mellitus: a harbinger for complications in later years—clinical observation from a secondary care cohort. QJM Int J Med. (2009) 102:799–806. doi: 10.1093/QJMED/HCP121
26. Koye DN, Ling J, Dibato J, Khunti K, Montvida O, and Paul SK. Temporal trend in young-onset type 2 diabetes-macrovascular and mortality risk: Study of U.K. primary care electronic medical records. Diabetes Care. (2020) 43:2208–16. doi: 10.2337/dc20-0417
27. Hu C, Lin L, Zhu Y, Zhang Y, Wang S, Zhang J, et al. Association between age at diagnosis of type 2 diabetes and cardiovascular diseases: A nationwide, population-based, cohort study. Front Endocrinol (Lausanne). (2021) 12:717069. doi: 10.3389/fendo.2021.717069
28. Barker MM, Zaccardi F, Brady EM, Gulsin GS, Hall AP, Henson J, et al. Age at diagnosis of type 2 diabetes and cardiovascular risk factor profile: A pooled analysis. World J Diabetes. (2022) 13:260–71. doi: 10.4239/wjd.v13.i3.260
29. Baek HS, Park JY, Yu J, Lee J, Yang Y, Ha J, et al. Characteristics of glycemic control and long-term complications in patients with young-onset type 2 diabetes. Endocrinol Metab. (2022) 37:641–51. doi: 10.3803/ENM.2022.602
30. Constantino MI, Molyneaux L, Limacher-Gisler F, Al-Saeed A, Luo C, Wu T, et al. Long-term complications and mortality in young-onset diabetes: Type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care. (2013) 36:3863–9. doi: 10.2337/dc12-2455
31. Ke C, Stukel TA, Shah BR, Lau E, Ma RC, So WY, et al. Age at diagnosis, glycemic trajectories, and responses to oral glucose-lowering drugs in type 2 diabetes in Hong Kong: A population-based observational study. PLoS Med. (2020) 17:1–16. doi: 10.1371/journal.pmed.1003316
32. Haley JE, Zhiqian G, Philip KR, Nicolas ML, Thomas KR, Lawrence DM, et al. Reduction in myocardial strain is evident in adolescents and young adults with obesity and type 2 diabetes. Pediatr Diabetes. (2020) 21:243–50. doi: 10.1111/pedi.12961
33. Piragine E, Petri D, Martelli A, Calderone V, and Lucenteforte E. Adherence to oral antidiabetic drugs in patients with type 2 diabetes: systematic review and meta-analysis. J Clin Med. (2023) 12:1981. doi: 10.3390/JCM12051981/S1
34. Chan JCN, Lau ESH, Luk AOY, Cheung KKT, Kong APS, Yu LWL, et al. Premature mortality and comorbidities in young-onset diabetes: A 7-year prospective analysis. Am J Med. (2014) 127:616–24. doi: 10.1016/j.amjmed.2014.03.018
35. Liu JJ, Liu S, Wang J, Lee J, Tang JIS, Gurung RL, et al. Risk of incident heart failure in individuals with early-onset type 2 diabetes. J Clin Endocrinol Metab. (2022) 107:E178–87. doi: 10.1210/clinem/dgab620
36. Huo L, Magliano DJ, Rancière F, Harding JL, Nanayakkara N, Shaw JE, et al. Impact of age at diagnosis and duration of type 2 diabetes on mortality in Australia 1997-2011. Diabetologia. (2018) 61:1055–63. doi: 10.1007/s00125-018-4544-z
37. Cho Y, Park HS, Huh BW, Seo SH, Seo DH, Ahn SH, et al. Prevalence and risk of diabetic complications in young-onset versus late-onset type 2 diabetes mellitus. Diabetes Metab. (2022) 48:101389. doi: 10.1016/j.diabet.2022.101389
38. Au A, Bajar BT, Wong BM, Daskivich LP, Hosseini H, and Prasad PS. Systemic and ocular outcomes in patients with young-onset type 2 diabetes. J Diabetes Complications. (2024) 38:108670. doi: 10.1016/j.jdiacomp.2023.108670
39. Huang L, Wu P, Zhang Y, Lin Y, Shen X, Zhao F, et al. Relationship between onset age of type 2 diabetes mellitus and vascular complications based on propensity score matching analysis. J Diabetes Investig. (2022) 13:1062–72. doi: 10.1111/jdi.13763
40. Zemplényi A, Sághy E, Kónyi A, Szabó L, Wittmann I, and Laczy B. Prevalence, cardiometabolic comorbidities and reporting of chronic kidney disease; A hungarian cohort analysis. Int J Public Health. (2023) 68:1605635. doi: 10.3389/ijph.2023.1605635
41. Lee J, Lee SH, Yoon KH, Cho JH, Han K, and Yang Y. Risk of developing chronic kidney disease in young-onset Type 2 diabetes in Korea. Sci Rep. (2023) 13:1–10. doi: 10.1038/s41598-023-36711-2
42. Middleton TL, Chadban S, Molyneaux L, D’Souza M, Constantino MI, Yue DK, et al. Young adult onset type 2 diabetes versus type 1 diabetes: Progression to and survival on renal replacement therapy. J Diabetes Complications. (2021) 35:108023. doi: 10.1016/j.jdiacomp.2021.108023
43. Koh B, Tan DJH, Ng CH, Fu CE, Lim WH, Zeng RW, et al. Patterns in cancer incidence among people younger than 50 years in the US, 2010 to 2019. JAMA Netw Open. (2023) 6:E2328171. doi: 10.1001/jamanetworkopen.2023.28171
44. Li Y, Tian J, Hou T, Gu K, Yan Q, Sun S, et al. Association between age at diabetes diagnosis and subsequent incidence of cancer: A longitudinal population-based cohort. Diabetes Care. (2024) 47:353–61. doi: 10.2337/dc23-0386
45. Credit Suisse Global Wealth Databook. Credit suisse(2022). Available online at: https://www.credit-suisse.com/media/assets/corporate/docs/about-us/research/publications/global-wealth-databook-2022.pdf (Accessed August 25, 2024).
46. UBS Global Wealth Databook. UBS(2023). Available online at: https://www.ubs.com/global/en/family-office-uhnw/reports/global-wealth-report-2023/_jcr_content/mainpar/toplevelgrid_5684475/col2/linklistnewlook/link_copy.0357374027.file/PS9jb250ZW50L2RhbS9hc3NldHMvd20vZ2xvYmFsL2ltZy9nbG9iYWwtZmFtaWx5LW9mZmljZS9kb2NzL2RhdGFib29rLWdsb2JhbC13ZWFsdGgtcmVwb3J0LTIwMjMtZW4ucGRm/databook-global-wealth-report-2023-en.pdf (Accessed August 25, 2024).
47. List of countries by wealth per adult - Wikipedia. Available online at: https://en.wikipedia.org/wiki/List_of_countries_by_wealth_per_adult (Accessed August 25, 2024).
48. Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease 2021: Findings from the GBD 2021 Study. Seattle, Washington: Institute for Health Metrics and Evaluation (IHME). (2024). Available online at: www.healthdata.org/sites/default/files/2024-05/GBD_2021_Booklet_FINAL_2024.05.16.pdf.
49. Kiss Z, Rokszin G, Abonyi-Tóth Z, Jermendy G, Kempler P, and Wittmann I. Different changes of risks for stroke and myocardial infarction in patients with type 2 diabetes in Hungary between the two periods of 2001–2004 and 2010-2013. Front Endocrinol (Lausanne). (2019) 10:170. doi: 10.3389/fendo.2019.00170
50. Barkai L, Kiss Z, Rokszin G, Abonyi-Tóth Z, Jermendy G, Wittmann I, et al. Changes in the incidence and prevalence of type 1 and type 2 diabetes among 2 million children and adolescents in Hungary between 2001 and 2016 - A nationwide population-based study. Arch Med Sci. (2020) 16:34–41. doi: 10.5114/aoms.2019.88406
51. Sadat A. Alarming surge in early-onset type 2 diabetes: A global catastrophe on the horizon. touchREVIEWS Endocrinol. (2023) 19:7–8. doi: 10.17925/EE.2023.19.2.5
52. Strati M, Moustaki M, Psaltopoulou T, Vryonidou A, and Paschou SA. Early onset type 2 diabetes mellitus: an update. Endocrine. (2024) 85:965–78. doi: 10.1007/s12020-024-03772-w
53. Xu L, Ran J, Shao H, Chen M, Tang H, Li Y, et al. Incidence and risk factors of diagnosed young-adult-onset type 2 diabetes in the U.S.: the national health interview survey 2016–2022. Diabetes Care. (2025) 48:371–80. doi: 10.2337/dc24-1699
54. Enesco A. Youth-onset type 2 diabetes: an awakening epidemic. EMJ Diabetes. (2023) 46(3):490–499. doi: 10.2337/dci22-0046
55. Murtaza G, Riaz S, Zafar M, Ahsan Raza M, Kaleem I, Imran H, et al. Examining the growing challenge: Prevalence of diabetes in young adults (Review). Med Int. (2024) 5:1–8. doi: 10.3892/mi.2024.201
56. CDC.gov. Diabetes in young patients is on the rise(2025). Available online at: https://www.cdc.gov/diabetes/data-research/research/young-people-diabetes-on-rise.html (Accessed August 10, 2025).
57. The Lancet Diabetes & Endocrinology. Alarming rise in young-onset type 2 diabetes. Lancet Diabetes Endocrinol. (2024) 12:433. doi: 10.1016/S2213-8587(24)00161-X
58. Nadeau KJ, Mayer-Davis EJ, Gubitosi-Klug R, Zeitler PS, Kahn SE, and Dabelea D. Youth-Onset Type 2 Diabetes: What We’ve Learned From Key Youth-Onset Type 2 Diabetes Studies, What We Still Don’t Know, and Why It Is Important. Diabetes Care. (2025) 48:1136–49. doi: 10.2337/dc25-0001
59. Kim JY, Lee J, Moon JH, Park SE, Ko SH, Choi SH, et al. Prevalence, Incidence, and Metabolic Characteristics of Young Adults with Type 2 Diabetes Mellitus in South Korea (2010–2020). Diabetes Metab J. (2025) 49:172–82. doi: 10.4093/dmj.2024.0826
60. Nagaratnam S, Rajoo S, Long Bidin MB, Che Rahim NS, Tharmathurai S, Arip M, et al. A Cross-sectional Study to Assess Beta-Cell Function in Individuals with Recently Diagnosed Young-Onset Type 2 Diabetes Mellitus and Its’ Complications. J ASEAN Fed Endocr Soc. (2023) 38:20–27. doi: 10.15605/JAFES.038.02.13
61. Titmuss A, Korula S, Wicklow B, and Nadeau KJ. Youth-onset type 2 diabetes: an overview of pathophysiology, prognosis, prevention and management. Curr Diabetes Rep. (2024) 24:183–95. doi: 10.1007/s11892-024-01546-2
62. Niechciał E, Wais P, Bajtek J, and Kędzia A. Current perspectives for treating adolescents with obesity and type 2 diabetes: A review. Nutr. (2024) 16:4084. doi: 10.3390/nu16234084
63. Huang H, Yan P, Shan Z, Chen S, Li M, Luo C, et al. Adverse childhood experiences and risk of type 2 diabetes: A systematic review and meta-analysis. Metabolism. (2015) 64:1408–18. doi: 10.1016/j.metabol.2015.08.019
64. Shan Z, Ma H, Xie M, Yan P, Guo Y, Bao W, et al. Sleep duration and risk of type 2 diabetes: A meta-analysis of prospective studies. Diabetes Care. (2015) 38:529–37. doi: 10.2337/dc14-2073
65. Song Y, Chou EL, Baecker A, You NCY, Song Y, Sun Q, et al. Endocrine-disrupting chemicals, risk of type 2 diabetes, and diabetes-related metabolic traits: A systematic review and meta-analysis. J Diabetes. (2016) 8:516–32. doi: 10.1111/1753-0407.12325
66. Sandforth L, Kullmann S, Sandforth A, Fritsche A, Jumpertz-von Schwartzenberg R, Stefan N, et al. Prediabetes remission to reduce the global burden of type 2 diabetes. Trends Endocrinol Metab. (2025) xx:1–18. doi: 10.1016/j.tem.2025.01.004
67. TODAY Study Group, Bjornstad P, Drews KL, Caprio S, Gubitosi-Klug R, Nathan DM, et al. Long-term complications in youth-onset type 2 diabetes. N Engl J Med. (2021) 385:416–26. doi: 10.1056/nejmoa2100165
68. Majety P, Lozada Orquera FA, Edem D, and Hamdy O. Pharmacological approaches to the prevention of type 2 diabetes mellitus. Front Endocrinol (Lausanne). (2023) 14:1118848. doi: 10.3389/fendo.2023.1118848
69. Berman C, Vidmar A, and Chao L. Glucagon-like peptide-1 receptor agonists for the treatment of type 2 diabetes in youth. touchREVIEWS Endocrinol. (2023) 19:38–45. doi: 10.2337/dc11-s215
70. McGowan BM, Bruun JM, Capehorn M, Pedersen SD, Pietiläinen KH, Muniraju HAK, et al. Efficacy and safety of once-weekly semaglutide 2·4 mg versus placebo in people with obesity and prediabetes (STEP 10): a randomised, double-blind, placebo-controlled, multicentre phase 3 trial. Lancet Diabetes Endocrinol. (2024) 12:631–42. doi: 10.1016/S2213-8587(24)00182-7
71. Liu J, Yao C, Wang Y, Zhao J, and Luo H. Non-drug interventions of traditional Chinese medicine in preventing type 2 diabetes: a review. Chin Med (United Kingdom). (2023) 18:1–15. doi: 10.1186/s13020-023-00854-1
72. Ni Y, Wu X, Yao W, Zhang Y, Chen J, and Ding X. Evidence of traditional Chinese medicine for treating type 2 diabetes mellitus: from molecular mechanisms to clinical efficacy. Pharm Biol. (2024) 62:592–606. doi: 10.1080/13880209.2024.2374794
73. Chen C, Gao H, Wei Y, and Wang Y. Traditional Chinese medicine in the prevention of diabetes mellitus and cardiovascular complications: mechanisms and therapeutic approaches. Front Pharmacol. (2025) 16:1511701. doi: 10.3389/fphar.2025.1511701
74. Pang B, Zhang Y, Liu J, He Ls, Zheng Yj, Lian Fm, et al. Prevention of type 2 diabetes with the Chinese herbal medicine Tianqi capsule: A systematic review and meta-analysis. Diabetes Ther. (2017) 8:1227–42. doi: 10.1007/s13300-017-0316-x
75. Perng W, Conway R, Mayer-Davis E, and Dabelea D. Youth-onset type 2 diabetes: the epidemiology of an awakening epidemic. Diabetes Care. (2023) 46:490–9. doi: 10.2337/dci22-0046
76. Buttermore E, Campanella V, and Priefer R. The increasing trend of Type 2 diabetes in youth: An overview. Diabetes Metab Syndr Clin Res Rev. (2021) 15:102253. doi: 10.1016/j.dsx.2021.102253
77. Xu S, Sun M, and Xiang Y. Global, regional, and national trends in type 2 diabetes mellitus burden among adolescents and young adults aged 10–24 years from 1990 to 2021: a trend analysis from the Global Burden of Disease Study 2021. World J Pediatr. (2025) 21:73–89. doi: 10.1007/s12519-024-00861-8
78. Lv Y, Cao X, Yu K, Pu J, Tang Z, Wei N, et al. Gender differences in all-cause and cardiovascular mortality among US adults: from NHANES 2005–2018. Front Cardiovasc Med. (2024) 11:1283132. doi: 10.3389/fcvm.2024.1283132
79. Andersson C and Vasan RS. Epidemiology of cardiovascular disease in young individuals. Nat Rev Cardiol. (2018) 15:230–40. doi: 10.1038/nrcardio.2017.154
Keywords: young people with type 2 diabetes mellitus, cardiovascular risk, myocardial infarction, stroke, mortality, renal risk, cancer risk
Citation: Molnár GA, Kiss Z and Wittmann I (2025) Young patients with type 2 diabetes have high relative risks for complications in a country with middle-high sociodemographic index, similarly to those countries with high index. Front. Endocrinol. 16:1638565. doi: 10.3389/fendo.2025.1638565
Received: 30 May 2025; Accepted: 22 September 2025;
Published: 15 October 2025.
Edited by:
Åke Sjöholm, Gävle Hospital, SwedenReviewed by:
Zengzheng Li, The First People’s Hospital of Yunnan Province, ChinaShimaa Hussein Kotb, Sphinx University, Egypt
Muhammad Abul Hasanat, Bangabandhu Sheikh Mujib Medical University (BSMMU), Bangladesh
Serap Tuna, Muğla Sıtkı Koçman University, Türkiye
Copyright © 2025 Molnár, Kiss and Wittmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: István Wittmann, d2l0dG1hbm4uaXN0dmFuQHB0ZS5odQ==