 Julia K. Gundersen
Julia K. Gundersen Anne Katrin Torsheim Holmøy2
Anne Katrin Torsheim Holmøy2 Per Kristian Eide
Per Kristian Eide- 1Department of Physiology, Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway
- 2Department of Neurology, Akershus University Hospital, Lørenskog, Norway
- 3Department of Neurosurgery, Oslo University Hospital - Rikshospitalet, Oslo, Norway
- 4Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
- 5KG Jebsen Centre for Brain Fluid Research, University of Oslo, Oslo, Norway
- 6Department of Endocrinology, Akershus University Hospital, Lørenskog, Norway
Introduction: Plasma osmolality is maintained within a narrow range by secretion of arginine vasopressin (AVP). AVP deficiency (formerly known as central diabetes insipidus) is a rare complication of surgery in the hypothalamic and pituitary region.
Case description: A 50-year-old male patient developed postoperative dehydration, polyuria and cognitive impairment following surgical clip ligation of an unruptured anterior communicating artery (ACOM) aneurysm. Endocrine tests revealed moderate hypernatremia, plasma hyperosmolality and urine hypoosmolality. Magnetic resonance imaging of the brain uncovered delayed cerebral infarctions in genu rostrum of corpus callosum and bilateral oedema of fornix anterior columns. All clinical findings supported the diagnosis of central AVP deficiency, likely involving the anterior hypothalamic nuclei. Follow-up 2 months postoperatively confirmed persisting AVP deficiency and cognitive impairment.
Conclusion: AVP deficiency without associated haemorrhage is exceedingly rare, with only seven cases identified in our literature review. This case highlights that postoperative AVP deficiency may present with mild or unspecific symptoms. Importantly, concurrent cognitive impairment may occur, further complicating compliance to treatment. Therefore, close postoperative monitoring is crucial for correct diagnosis and bed-side management.
1 Introduction
Sodium is a major determinant of osmotic pressure; hypernatremia is therefore a common cause of hyperosmolality. Clinically, subacute plasma hyperosmolality may manifest as confusion, dysphoria, drowsiness, convulsions or coma (1). In acute cases, it may cause substantial brain volume loss (2), increasing the risk of haemorrhage and irreversible brain injury (1). The body is able to maintain plasma osmolality within a narrow physiological range via the hormone arginine vasopressin (AVP) (3). AVP is released in response to extracellular hyperosmolality and maintains homeostasis by regulating renal water reabsorption. AVP is synthetised within the supraoptic nuclei (SON) and the paraventricular nuclei (PVN) of the anterior hypothalamus, transported along the neuronal axons and released from the neurohypophysis (4). AVP-release is triggered by specialised osmoreceptors, such as the delta-n transient receptor potential vannilloid (TRPV1) channel, located in the subfornical organ (SFO), organum vasculosum of the lamina terminalis (OVLT) and median preoptic nucleus (MnPO). These neurons also coordinate drinking behaviour (5). TRPV1-activation is primarily driven by changes in cell volume, indicating that osmoreceptors function essentially as mechanical stretch receptors (6). Interestingly, TRPV1 is also involved in sensation of body temperature (6).
AVP deficiency is characterised by polyuria, leading to dehydration and hyperosmolality. Hyperosmolality typically triggers a pronounced thirst response, but damage to the osmoreceptors or the neural circuitry mediating thirst perception can lead to simultaneous adipsia. The most common causes of central AVP deficiency are cerebral pathology or surgical intervention affecting the hypothalamus or pituitary gland. AVP deficiency has been reported in association with intracranial aneurysms, in particular those affecting the anterior communicating artery (ACOM), although involvement of anterior cerebral artery and middle cerebral artery aneurysms has also been documented (7). In the majority of these cases, AVP deficiency occurs following rupture of an ACOM aneurysm and subsequent subarachnoid haemorrhage (SAH) (Table 1). However, in very rare instances, a patient may develop AVP deficiency following surgical ligation of an unruptured ACOM aneurysm. Here, we report such a rare clinical case, which presented with non-specific symptoms that can be challenging to recognise and treat in the clinical setting.
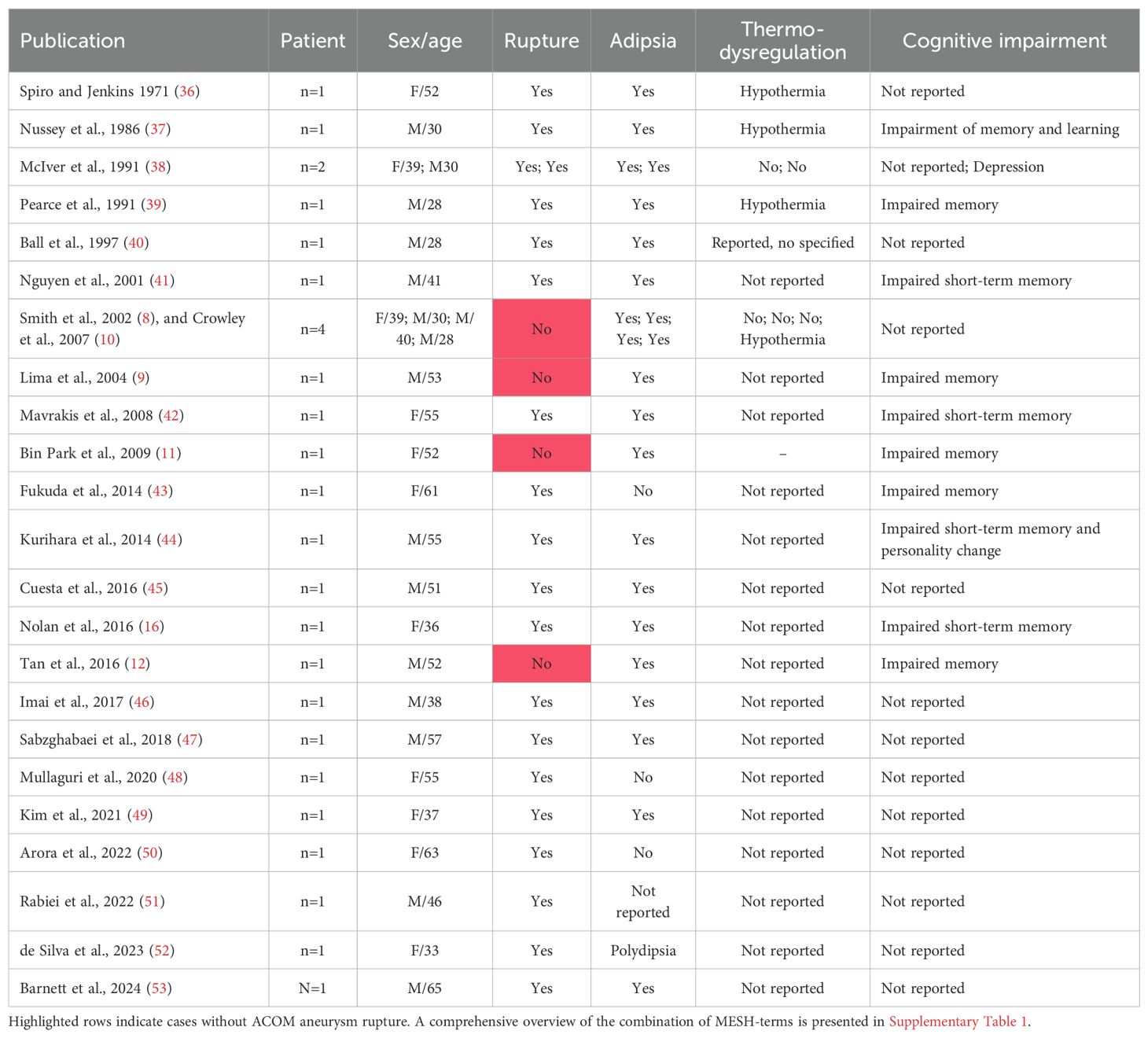
Table 1. A systematic literature review of AVP deficiency and ACOM aneurysm surgery was performed in PubMed, MEDLINE and Embase.
To evaluate the rarity of this condition, we also performed a systematic literature review of AVP deficiency following ACOM aneurysm surgery. A comprehensive search using PubMed, Ovid MEDLINE and Embase of papers published between 1st of January 1946 and 29th of May 2025 was performed using the MESH-terms presented in Supplementary Table 1. Publications describing cases of AVP deficiency following ruptured or unruptured ACOM aneurysms after surgical ligation were included (Table 1). To date, only seven cases of AVP deficiency following unruptured ACOM aneurysm surgery have been reported worldwide (8–12) (Table 1), in addition to the present case.
2 Case description
2.1 Clinical presentation
A 50-year-old man was diagnosed with an unruptured ACOM aneurysm measuring 8 mm in diameter, with no prior history of cerebral bleeding. Significant medical history included granulomatosis with polyangiitis (GPA, formerly known as Wegener’s granulomatosis) with renal involvement, treated with daily prednisolone (5 mg) and annual rituximab infusions, the last of which was administered 6 months prior to surgery.
Given the aneurysmal size of 8 mm, surgical repair was indicated and consensus on repair modality was reached in a multidisciplinary team of interventional radiologists and neurosurgeons. Initially, a stent procedure was favoured due to the wide aneurysmal neck, however, clip ligation was ultimately recommended because of a right hypoplastic A1. The procedure was performed through a right pterional craniotomy under general anaesthesia. The aneurysm was exposed via the Sylvian and interhemispheric fissures without tissue resection. Due to several perforators at the base of the ACOM aneurysm providing collateral perfusion, clipping was done under temporary occlusion of the left A1 and A2 arteries. Micro-Doppler was used to verify open vessels after clipping, particularly the open perforators from the ACOM. Topical papaverine was applied to prevent vasospasms. Postoperatively, no immediate neurological deficits were encountered, but disorientation was noted. Cerebral computed tomography (CT) and angiography (CTA) on the first postoperative day revealed a closed aneurysm with no evidence of vessel occlusions.
Two days postoperatively, the patient was transferred to the department of neurology for postoperative care. Upon admission, he had a Glasgow Coma Scale (GCS) score of 14 due to disorientation, but no other clinical neurological deficits. On the following day he exhibited signs of delirium and somnolence with a GCS score of 13. Over the subsequent days, delirium persisted and was accompanied by increasing restlessness, for which haloperidol was prescribed in addition to standard clinical care. During the first week of admission, ongoing delirium and cognitive impairment prompted a formal cognitive assessment by an occupational therapist. The patient scored 18/30 on the Mini Mental State Examination (MMSE), which is markedly abnormal for his age and substantially deviating from his reported preoperative cognitive status.
The patient’s vital signs were within normal physiological ranges, exception for a low-grade fever during the first few days. Biochemically, he exhibited elevated C-reactive protein (CRP) of 56 mg/L, creatinine of 129 μmol/L, an estimated glomerular filtration rate (eGFR) of 54 mL/min/1.73 m² and marked hypernatremia of 153 mmol/L. The hypernatremia was initially attributed to reduced perioperative water intake and managed with intravenous 5% glucose infusions. While CRP levels normalised over a few days, sodium and creatinine levels remained elevated despite daily administration of 2–4 L of 5% glucose solution (Figure 1). He began to exhibit clinical signs of dehydration, such as reduced skin turgor and dry oral mucous membranes, and reported excessive urination. The persistent hypernatremia prompted further evaluation by an endocrinologist. A comprehensive panel of blood and urine tests (Table 2) revealed high plasma osmolality (305 mOsm/kg) and hypernatremia (148 mmol/L), combined with low urine osmolality (205 mOsm/kg). These results indicated impaired ability to concentrate urine and conserve water.
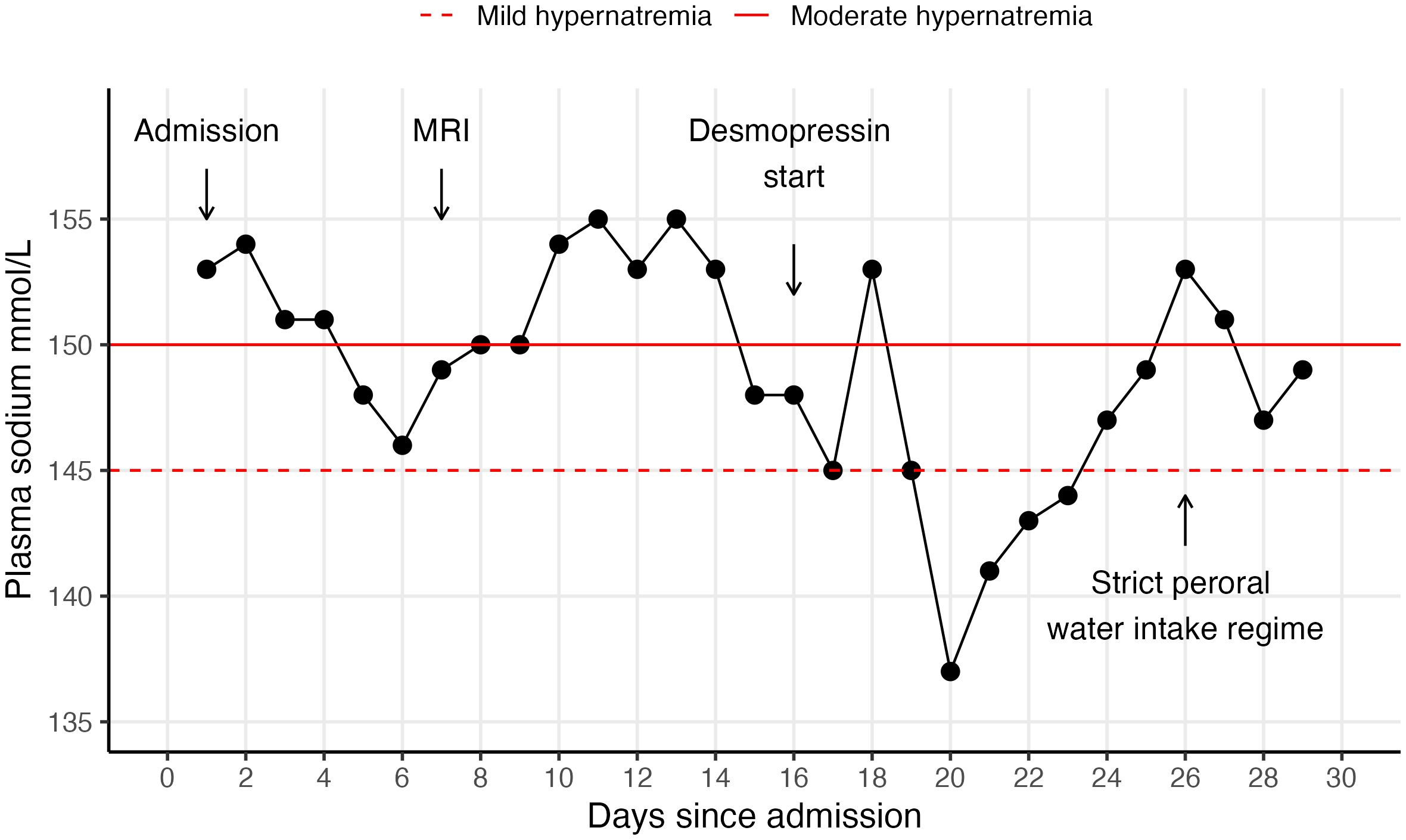
Figure 1. Timeline of daily monitoring of serum sodium levels. The patient was administered desmopressin treatment from day 16 of admission. Daily IV glucose 5% IV infusions were stopped on day 20, after which the plasma sodium concentration gradually increased despite optimal desmopressin dosage due to adipsia. Strict peroral water intake of 2-2.5 L was recommended on day 26, after which the plasma sodium concentration gradually increased due to adipsia despite optimal desmopressin dosage.
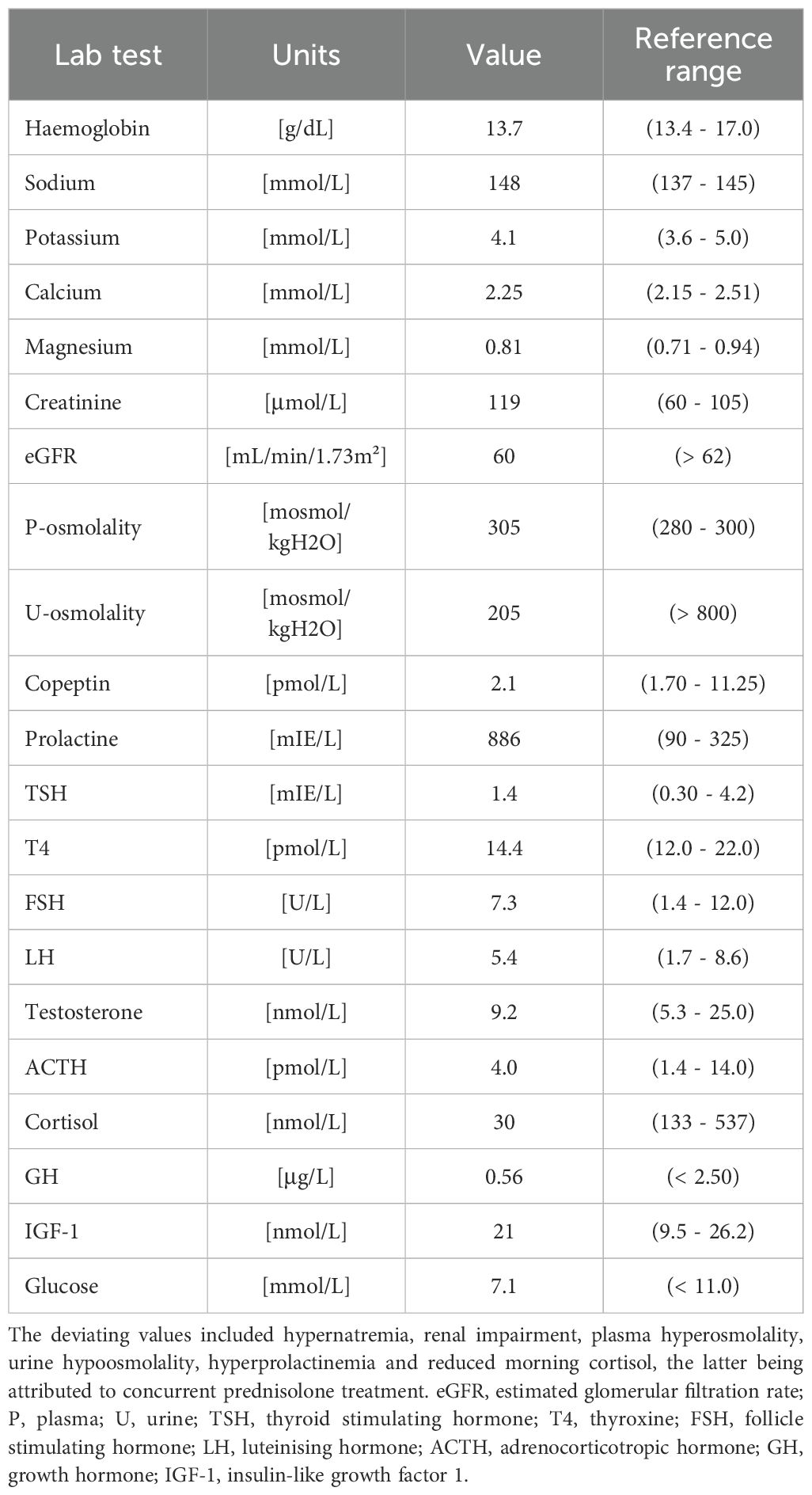
Table 2. A comprehensive panel of endocrine tests was obtained on day 16 of admission.
2.2 Diagnostic assessment and therapeutic intervention
An impaired ability to concentrate urine in the setting of elevated plasma osmolality after brain surgery suggested the diagnosis of AVP deficiency, although the typical thirst sensation was absent. A low plasma concentration of copeptin (2.1 pmol/L), the C-terminal segment of the AVP peptide precursor co-secreted in equimolar amounts (13, 14), provided further support for the diagnosis. Finally, administration of desmopressin (a synthetic AVP analogue) resulted in a marked improvement in renal concentration ability, with urine osmolality ultimately reaching 950 mOsm/kg, thereby confirming the diagnosis of AVP deficiency.
Due to these unexpected findings, a magnetic resonance image (MRI) scan of the brain was performed on the 7th postoperative day (Figure 2). The MRI revealed infarction in the genu rostrum of corpus callosum and bilateral oedema of the fornix anterior columns and the hypothalamus, in addition to ischemic changes nearby the surgical route (the anterior temporal and the basal frontal pole). No changes were observed in the hippocampus or the mamillary bodies. A follow-up MRI confirmed the infarctions. An MRI of the pituitary gland was also obtained, which showed no pathology in the pituitary gland.
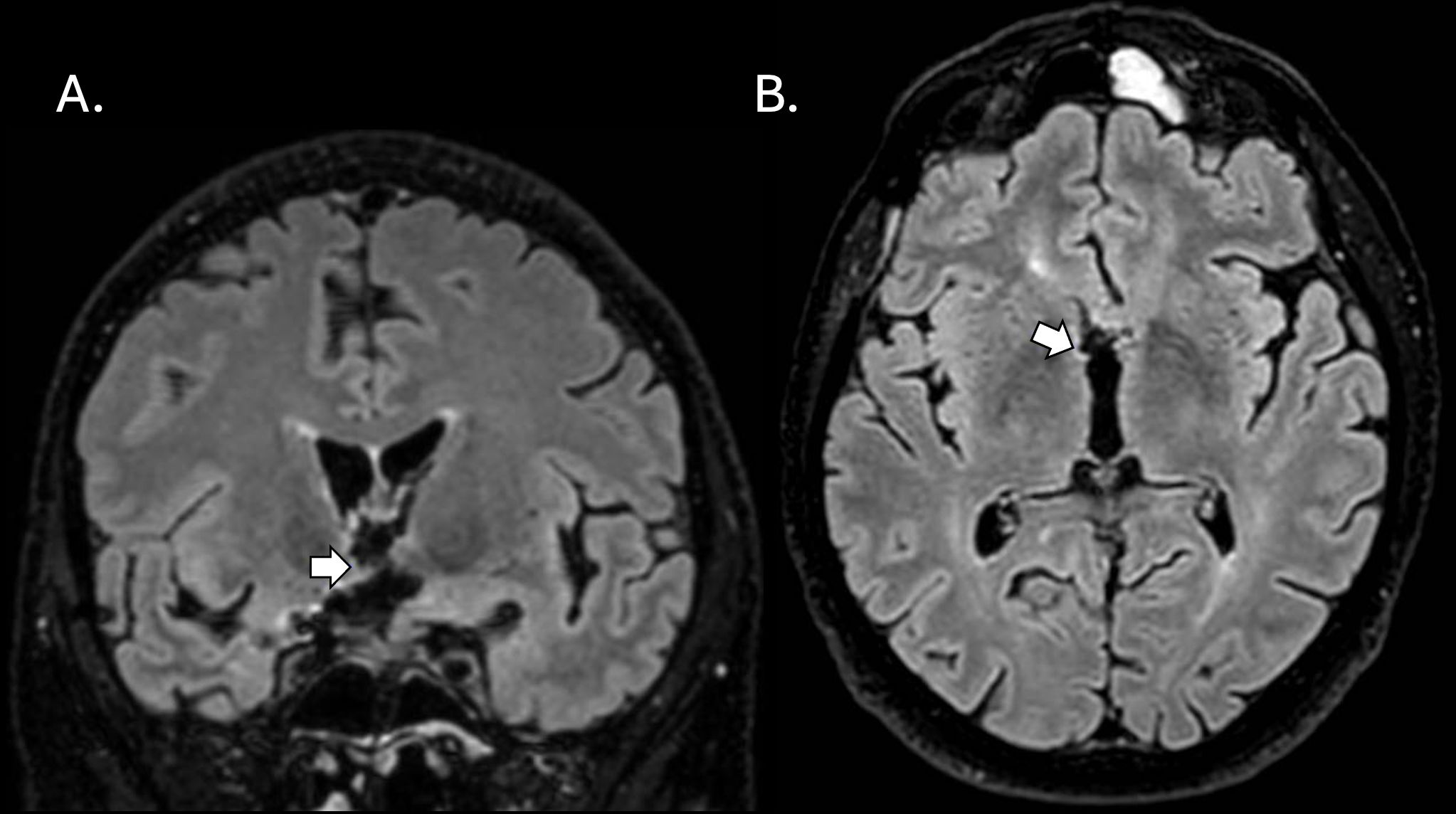
Figure 2. Magnetic resonance imaging (MRI) FLAIR SPIR 1.2mm scans of the brain obtained at follow-up 1 month after the surgical clip ligation. White arrows in coronal (A) and axial (B) planes point to subacute infarction in the right hypothalamus. MRI scans were assessed by a specialist neuroradiologist (J.O.).
Despite reaching adequate urine osmolality on desmopressin treatment, maintaining normal plasma sodium levels proved difficult without water supplementation in the form of glucose 5% infusions. The patient did not experience thirst despite dehydration and elevated plasma osmolality, a state that under normal conditions would elicit a strong thirst response. This necessitated a strict fluid regimen to ensure sufficient oral fluid intake before stable water homeostasis could be achieved. He was advice to maintain a daily water intake of 2-2.5 L.
2.3 Follow-up and outcome
The patient was scheduled for follow-up assessment with both a specialist neurologist and specialist endocrinologist within 1 month of discharge (approximately 2 months postoperatively). At follow-up, he appeared in good general condition, well-hydrated and did not report fluctuations in weight. His blood analysis showed normal levels of osmolality and sodium concentration. However, the patient still reported difficulty with maintaining an adequate water intake, which he attributed to a lack of thirst and forgetfulness regarding drinking water. Interestingly, he also described a persistent sensation of feeling cold, despite his skin being normothermic to the touch and other household members perceiving the ambient temperature as warm.
Repeated assessment of his cognitive function revealed a decline in selective attention, learning and memory recall. In contrast, executive function, processing speed, and working memory remained within the normal limits. These findings indicate persistent cognitive impairment with amnesia, identifying him as a candidate for further cognitive rehabilitation, which he was scheduled for in the near future.
2.4 Patient perspective
The patient and his family were informed of the diagnosis and the likelihood that it represented a postoperative complication. He reported significant impact on his quality of life since discharge, providing the example that he was unable to resume work as usual due to the difficulties posed by his impaired memory. He also emphasised the importance of clinician awareness of this condition in order to reduce the risk of and improve the diagnosis of postoperative AVP deficiency. At the time of his statement, the patient was still undergoing cognitive rehabilitation.
3 Discussion
We present a rare case of hypothalamic dysfunction – manifesting as AVP deficiency, adipsia cognitive impairment, and thermodysregulation – following surgical clip ligation of an unruptured ACOM aneurysm. Th clinical picture is consistent with partial hypothalamic syndrome (15) likely secondary to delayed ischemia of the anterior hypothalamus, including the nuclei responsible for osmoregulation. This case highlights the anatomical relationship between the anterior hypothalamus and the ACOM. AVP-producing neurons in the SON and PVN receive blood supply from the perforating branches of the ACOM (16, 17), which may be compromised by vasospasms of the perforators. Similarly, the osmosensitive neurons in the SFO, OVLT and MnPO are supplied by perforators of the anterior cerebral artery and anterior choroid artery (17, 18). Interestingly, excessive AVP secretion is a known complication of subarachnoid haemorrhage, leading to hyponatremia in the syndrome of inappropriate antidiuretic hormone secretion (SIADH) (19–21), for which the ACOM is the most commonly affected site (22).
Delayed cerebral ischemia is commonly associated with ruptured cerebral aneurysms; however it is increasingly recognised as a complication to surgical clip ligation of unruptured cerebral aneurysms as well (23, 24). Prophylactic treatment of vasospasms with calcium-channel blocker nimodipine may be considered, although its efficacy remains to be validated. Ischaemic complications have also been reported following endovascular repair of unruptured cerebral aneurysms (25).
The patient developed persistent cognitive impairment postoperatively, most likely related to ischaemia of the anterior fornix. No visible ischemic lesions in the hippocampus or mammillary bodies were detected. Notably, AVP deficiency has been linked to cognitive impairment in several other case reports (Table 1). Experimental evidence indicates that AVP may play a direct role in formation of new memories in the hippocampus (26). Importantly, cognitive impairment may critically impede compliance to desmopressin and appropriate water intake, especially when combined with adipsia. This was the case with our patient. Despite administering high doses of desmopressin, his plasma sodium levels surged when IV fluid infusions were stopped (Figure 1), representing inadequate water intake. Also, reliable urine volumes were difficult to obtain due to reduced compliance. It is important for clinicians to recognise that adequate water consumption is just as crucial as desmopressin therapy in the management of patients with AVP deficiency and adipsia.
The patient also exhibited signs of thermodysregulation, manifesting as a persistent sensation of feeling cold. Thermodysregulation, along with endocrine dysfunction and cognitive impairment are recognised features of hypothalamic dysfunction. Increased appetite and sleep disorders are also commonly reported in this context (27), however, our patient did not experience such symptoms. Speculatively, the altered thermoregulation reported by our patient may also be related to dysfunction TRPV1 expressing neurons in the hypothalamus, even in the absence of visible lesions on the MRI. TRPV1 channels are known to play a role in thermoregulation, and experimental studies have shown that TRPV1 agonists (e.g. capsaicin) induce hypothermia that is not reversed by hot ambient temperature (28).
Several factors complicated the interpretation of this case. First, hypernatremia is a common postoperative comorbidity in neurological patients. Given the absence of other neurological symptoms, the patient’s cognitive impairment and/or lethargy could have been explained by transient postoperative hypernatremia. Unfortunately, a reliable assessment of fluid balance, which is a key to diagnosing AVP deficiency, was difficult to obtain due the patient’s persistent cognitive impairment. A second complicating factor was the patient’s co-morbidity with GPA. Autoimmune multisystem diseases, such as GPA may be accompanied with cerebral vasculitis (29), which has been reported to cause subarachnoid (30, 31) and intracerebral (32) haemorrhages, as well as brain infarction (33). GPA thus represents a risk factor for the postoperative complications. In rare cases, GPA may also involve the pituitary gland, causing hypophysitis and dysfunction with AVP deficiency being the most prevalent manifestation (34, 35). However, in this case, the absence of pituitary abnormalities on MRI, along with no visual disturbances, no evidence of other pituitary axes dysfunction, and no multisystem organ involvement (e.g. respiratory system) ultimately weakened the clinical suspicion of autoimmune hypophysitis.
4 Conclusion
AVP deficiency without associated SAH is a rare complication to repair of an unruptured ACOM aneurysm. Because patients may exhibit only mild neurological and/or cognitive symptoms, close postoperative monitoring is crucial for timely diagnosis and effective bedside management. Prophylactic treatment with nimodipine may be considered to reduce the risk of vasospasms and delayed cerebral ischemia. Importantly, adipsia in conjuncture with cognitive impairment may significantly reduce adherence to desmopressin therapy and adequate water intake, increasing the risk of developing outpatient hypernatremia. To mitigate this, clear patient education and structured follow-ups are critical to support compliance and prevent complications.
Data availability statement
The datasets presented in this article are not readily available because Clinical blood samples are available in Table 2. Any other data or clinical information is considered identifiable, and therefore not available. Requests to access the datasets should be directed to anVsaWFrZ3VuZGVyc2VuQGhvdG1haWwuY29t.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
JG: Formal analysis, Visualization, Writing – original draft, Writing – review & editing, Data curation. AH: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. PE: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. JW: Formal analysis, Investigation, Writing – original draft, Writing – review & editing, Supervision. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
We extend our gratitude to our colleagues in the neurology, endocrinology and radiology department for their valuable assistance in the diagnosis and treatment of the patient.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Generative AI was used to improve grammar and syntax for parts of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1662205/full#supplementary-material
Supplementary Table 1 | The systematic literature review collected publications, which were then manually screened based on title, abstract and full text by one investigator (JKG). Duplicate cases reported in multiple papers were excluded, with only the original paper included. Only cases reporting on ACOM pathology or surgery where included. The search was assisted by staff at the medical library at Akershus University Hospital.
Abbreviations
SON, Supraoptic Nuclei; PVN, Paraventricular Nuclei; TRPV1, Transient Receptor Potential Vanilloid; SFO, Subfornical Organ; OVLT, Organum Vasculosum of the Lamina Terminalis; MnPO, Median Preoptic Nucleus; ACOM, Anterior Communicating Artery; SAH, Subarachnoid Haemorrhage; GPA, Granulomatosis with Polyangiitis; CT, Computed Tomography; CTA, Computed Tomography Angiography; GCS, Glasgow Coma Scale; CRP, C-Reactive Protein; eGFR, Estimated Glomerular Filtration Rate; MMSE, Mini Mental State Examination; MRI, Magnetic Resonance Imaging.
References
1. Sterns RH. Disorders of plasma sodium — Causes, consequences, and correction. New Engl J Med. (2015) 372:55–65. doi: 10.1056/NEJMra1404489
2. Morland C, Pettersen MN, and Hassel B. Hyperosmolar sodium chloride is toxic to cultured neurons and causes reduction of glucose metabolism and ATP levels, an increase in glutamate uptake, and a reduction in cytosolic calcium. NeuroToxicology. (2016) 54:34–43. doi: 10.1016/j.neuro.2016.03.005
3. Onwuka OM. Physiological basis of arginine vasopressin deficiency (AVP-D, formerly central diabetes insipidus) and AVP-resistance (AVP-R, formerly nephrogenic diabetes insipidus). Explor Med. (2025) 6:1001289. doi: 10.37349/emed.2025.1001289
4. Bichet DG. Vasopressin at central levels and consequences of dehydration. Ann Nutr Metab. (2016) 68:19–23. doi: 10.1159/000446200
5. Augustine V, Gokce SK, Lee S, Wang B, Davidson TJ, Reimann F, et al. Hierarchical neural architecture underlying thirst regulation. Nature. (2018) 555:204–9. doi: 10.1038/nature25488
6. Bourque CW. Central mechanisms of osmosensation and systemic osmoregulation. Nat Rev Neurosci. (2008) 9:519–31. doi: 10.1038/nrn2400
7. Dalan R, Chin H, Hoe J, Chen A, Tan H, Boehm BO, et al. Adipsic diabetes insipidus-the challenging combination of polyuria and adipsia: A case report and review of literature. Front Endocrinol. (2019) 10:630. doi: 10.3389/fendo.2019.00630
8. Smith D, McKenna K, Moore K, Tormey W, Finucane J, Phillips J, et al. Baroregulation of vasopressin release in adipsic diabetes insipidus. J Clin Endocrinol Metab. (2002) 87:4564–8. doi: 10.1210/jc.2002-020090
9. Lima EQ, Aguiar FC, Barbosa DM, and Burdmann EA. Severe hypernatraemia (221 mEq/l), rhabdomyolysis and acute renal failure after cerebral aneurysm surgery. Nephrol Dial Transplant. (2004) 19:2126–9. doi: 10.1093/ndt/gfh324
10. Crowley RK, Sherlock M, Agha A, Smith D, and Thompson CJ. Clinical insights into adipsic diabetes insipidus: a large case series. Clin Endocrinol. (2007) 66:475–82. doi: 10.1111/j.1365-2265.2007.02754.x
11. Park JB, Jin AR, Yu TY, Noh HJ, Lee MY, Park BH, et al. A case of adipsic hypothalamic diabetes insipidus after clipping of an anterior communicating artery aneurysm. Korean J Med. (2009) 77:1217–21. Available online at: https://www.ekjm.org/journal/view.php?number=20874 (Accessed December 10, 2023).
12. Tan J, Ndoro S, Okafo U, Garrahy A, Agha A, and Rawluk D. Delayed recovery of adipsic diabetes insipidus (ADI) caused by elective clipping of anterior communicating artery and left middle cerebral artery aneurysms. N Z Med J. (2016) 129:86–90. Available online at: https://www.ekjm.org/journal/view.php?number=20874 (Accessed December 10, 2023).
13. Hui C, Khan M, Khan Suheb MZ, and Radbel JM. Diabetes insipidus. In: StatPearls. StatPearls Publishing, Treasure Island (FL (2023). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK470458/ (Accessed November 17, 2023).
14. Tomkins M, Lawless S, Martin-Grace J, Sherlock M, and Thompson CJ. Diagnosis and management of central diabetes insipidus in adults. J Clin Endocrinol Metab. (2022) 107:2701–15. doi: 10.1210/clinem/dgac381
15. Müller HL, Tauber M, Lawson EA, Özyurt J, Bison B, Martinez-Barbera J-P, et al. Hypothalamic syndrome. Nat Rev Dis Primers. (2022) 8:1–22. doi: 10.1038/s41572-022-00351-z
16. Nolan B and Inder WJ. Managing adipsic diabetes insipidus following anterior communicating artery aneurysm in a subtropical climate. Clin Case Rep. (2016) 4:664–7. doi: 10.1002/ccr3.590
17. Daniel PM. The blood supply of the hypothalamus and pituitary gland. Br Med Bull. (1966) 22:202–8. doi: 10.1093/oxfordjournals.bmb.a070474
18. Polzović A, Cvejin B, and Budimlija Z. Vascular characteristics of the human subfornical organ. Med Pregl. (1994) 47:307–9. Available online at: https://www.ekjm.org/journal/view.php?number=20874 (Accessed March 09, 2024).
19. Dai K, Ji C, Wang W, and Xia P. Risk factors and treatment strategies for hyponatremia following aneurysm clipping in patients with aneurysmal subarachnoid haemorrhage: A Single Centre experience. Interdiscip Neurosurg. (2025) 40:102032. doi: 10.1016/j.inat.2025.102032
20. Cardoso APD, Dragosavac D, Araujo S, Falcao ALE, Terzi RGG, de Castro M, et al. Syndromes related to sodium and arginine vasopressin alterations in post-operative neurosurgery. Arq Neuropsiquiatr. (2007) 65:745–51. doi: 10.1590/S0004-282X2007000500003
21. Ridwan S, Zur B, Kurscheid J, Esche J, Kristof R, Klingmuller D, et al. Hyponatremia after spontaneous aneurysmal subarachnoid haemorrhage-A prospective observational study. World Neurosurg. (2019) 129:e538–44. doi: 10.1016/j.wneu.2019.05.210
22. Hoffman H, Ziechmann R, Gould G, and Chin LS. The impact of aneurysm location on incidence and aetiology of hyponatremia following subarachnoid haemorrhage. World Neurosurg. (2018) 110:e621–6. doi: 10.1016/j.wneu.2017.11.058
23. Campe C, Neumann J, Sandalcioglu IE, Rashidi A, and Luchtmann M. Vasospasm and delayed cerebral ischemia after uneventful clipping of an unruptured intracranial aneurysm – a case report. BMC Neurol. (2019) 19:226. doi: 10.1186/s12883-019-1458-4
24. Peterson CM, Podila SS, and Girotra T. Unruptured aneurysmal clipping complicated by delayed and refractory vasospasm: case report. BMC Neurol. (2020) 20:344. doi: 10.1186/s12883-020-01925-8
25. Park JC, Lee DH, Kim JK, Ahn JS, Kwun BD, Kim DY, et al. Microembolism after endovascular coiling of unruptured cerebral aneurysms: incidence and risk factors. J. Neurosurg. (2016) 124(3):777–783. doi: 10.3171/2015.3.JNS142835
26. Abramova O, Zorkina Y, Ushakova V, Zubkov E, Morozova A, and Chekhonin V. The role of oxytocin and vasopressin dysfunction in cognitive impairment and mental disorders. Neuropeptides. (2020) 83:102079. doi: 10.1016/j.npep.2020.102079
27. Sanchez Jimenez JG and De Jesus O. Hypothalamic dysfunction. In: StatPearls. StatPearls Publishing, Treasure Island (FL (2025). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK560743/.
28. Gavva NR. Body-temperature maintenance as the predominant function of the vanilloid receptor TRPV1. Trends Pharmacol Sci. (2008) 29:550–7. doi: 10.1016/j.tips.2008.08.003
29. Guzman-Soto MI, Kimura Y, Romero-Sanchez G, Cienfuegos-Alvear JA, Candanedo-Gonzalez F, Kimura-Sandoval Y, et al. From head to toe: granulomatosis with polyangiitis. Radiographics. (2021) 41:1973–91. doi: 10.1148/rg.2021210132
30. Baran O, Ozdogan S, Demirel N, Evran S, Duzkalir HG, and Kocak A. Extremely rare complication of granulomatosis with polyangiitis: Aneurysmal subarachnoid haemorrhage. Romanian Neurosurg. (2019) 2019):438–42. doi: 10.33962/roneuro-2019-069
31. Kimura H, Akutsu N, Shiomi R, and Kohmura E. Subarachnoid haemorrhage caused by ruptured intracranial fusiform aneurysm associated with microscopic polyangiitis. Neurol Med Chir (Tokyo). (2012) 52:495–8. doi: 10.2176/nmc.52.495
32. Ceri M, Ortabozkoyun L, Unverdi S, Kirac M, and Duranay M. Massive intracerebral haemorrhage associated with Wegener granulomatosis. Rheumatol Int. (2012) 32:1813–4. doi: 10.1007/s00296-011-1954-3
33. Satoh J, Miyasaka N, Yamada T, Nishido T, Okuda M, Kuroiwa T, et al. Extensive cerebral infarction due to involvement of both anterior cerebral arteries by Wegener’s granulomatosis. Ann Rheum Dis. (1988) 47:606–11. doi: 10.1136/ard.47.7.606
34. Ramakrishna MP, Arun CS, Pavithran PV, Bhagavaldas MC, and Kumar H. Hypophysitis in granulomatosis with polyangiitis: rare presentation of a multisystem disease. J R Coll Physicians Edinb. (2020) 50:287–90. doi: 10.4997/JRCPE.2020.315
35. Vega-Beyhart A, Medina-Rangel IR, Hinojosa-Azaola A, Fernández-Barrio M, Vargas-Castro AS, García-Inciarte L, et al. Pituitary dysfunction in granulomatosis with polyangiitis. Clin Rheumatol. (2020) 39:595–606. doi: 10.1007/s10067-019-04735-7
36. Spiro SG and Jenkins JS. Adipsia and hypothermia after subarachnoid haemorrhage. Br Med J. (1971) 3:411–2. doi: 10.1136/bmj.3.5771.411
37. Nussey SS, Ang VT, and Jenkins JS. Chronic hypernatraemia and hypothermia following subarachnoid haemorrhage. Postgrad Med J. (1986) 62:467–71. doi: 10.1136/pgmj.62.728.467
38. McIver B, Connacher A, Whittle I, Baylis P, and Thompson C. Adipsic hypothalamic diabetes insipidus after clipping of anterior communicating artery aneurysm. BMJ. (1991) 303:1465–7. doi: 10.1136/bmj.303.6815.1465
39. Pearce SH, Argent NB, and Baylis PH. Chronic hypernatremia due to impaired osmoregulated thirst and vasopressin secretion. Acta Endocrinol (Copenh). (1991) 125:234–9. doi: 10.1530/acta.0.1250234
40. Ball SG, Vaidja B, and Baylis PH. Hypothalamic adipsic syndrome: diagnosis and management. Clin Endocrinol. (1997) 47:405–9. doi: 10.1046/j.1365-2265.1997.2591079.x
41. Nguyen BN, Yablon SA, and Chen CY. Hypodipsic hypernatremia and diabetes insipidus following anterior communicating artery aneurysm clipping: diagnostic and therapeutic challenges in the amnestic rehabilitation patient. Brain Inj. (2001) 15:975–80. doi: 10.1080/02699050110063459
42. Mavrakis AN and Tritos NA. Diabetes insipidus with deficient thirst: report of a patient and review of the literature. Am J Kidney Dis. (2008) 51:851–9. doi: 10.1053/j.ajkd.2007.11.028
43. Fukuda H, Iwasaki K, Murao K, Yamagata S, Lo BWY, and Macdonald RL. Risk factors and consequences of unexpected trapping for ruptured anterior communicating artery aneurysms. Surg Neurol Intl. (2014) 5:136701. doi: 10.4103/2152-7806.136701
44. Kurihara I, Miyashita K, Kobayashi S, Yokota K, Murai-Takeda A, Mitsuishi Y, et al. A case of adipsic diabetes incipidus with impaired response to desmopressin treatment. Endocr Rev. (2014) 35. doi: 10.1210/endo-meetings.2014.NP.18.MON-0693
45. Cuesta M, Gupta S, Salehmohamed R, Dineen R, Hannon MJ, Tormey W, et al. Heterogenous patterns of recovery of thirst in adult patients with adipsic diabetes insipidus. QJM. (2016) 109:303–8. doi: 10.1093/qjmed/hcv175
46. Imai E, Kaneko S, and Tsukamoto Y. Renal compensatory adaptation for water handling in a patient with adipsic diabetes insipidus after clipping of a ruptured aneurysm of the anterior communicating artery. Clin Nephrol. (2017) 88:112–6. doi: 10.5414/CN108963
47. Sabzghabaei F, Akhtar M, Hashemi SMR, and Mollahoseini R. Adipsic diabetes insipidus: A single-centre case series. Nephro-Urol Mon. (2018) 10:e14264. doi: 10.5812/numonthly.14264
48. Mullaguri N, Omer T, George P, and Newey CR. Refractory polyuria secondary to cerebral salt wasting successfully treated with DDAVP and hypertonic saline. Interdiscip Neurosurg Adv Tech Case Manage. (2020) 22:100814. doi: 10.1016/j.inat.2020.100814
49. Kim WK, Lee T, Kim AJ, Ro H, Chang JH, Lee HH, et al. Adipsic hypernatremia after clipping of a ruptured aneurysm in the anterior communicating artery: A case report. Electrolyte Blood Press. (2021) 19:56–60. doi: 10.5049/EBP.2021.19.2.56
50. Arora I, Lechan R, Kung J, and McCallum W. Subarachnoid haemorrhage complicated by nephrogenic and central diabetes insipidus. J Endocr Soc. (2022) 6:A584. doi: 10.1210/jendso/bvac150.1210
51. Rabiei S, Jaffa M, and Kantorovich V. Supraphysiologic vasopressin-induced receptor desensitization: A case report. J Endocr Soc. (2022) 6:A564. doi: 10.1210/jendso/bvac150.1171
52. de Silva NL, Gunathilaka H, Wadanamby S, Sumanatilleke M, and Somasundaram N. Rathke’s cleft cyst discovered with ruptured anterior communicating artery aneurysm: a case report. J Med Case Rep. (2023) 17:388. doi: 10.1186/s13256-023-04115-5
Keywords: vasopressin, insipidus, sodium, osmolality, aneurysm, ACOM, hypothalamus, MRI
Citation: Gundersen JK, Holmøy AKT, Eide PK and Winther JA (2025) Arginine vasopressin deficiency after surgical ligation of an unruptured anterior communicating artery aneurysm – a case report and literature review. Front. Endocrinol. 16:1662205. doi: 10.3389/fendo.2025.1662205
Received: 08 July 2025; Accepted: 27 October 2025;
Published: 18 November 2025.
Edited by:
Hubert Vaudry, Université de Rouen, FranceReviewed by:
Osah Martins Onwuka, Gregory University, NigeriaMaxim Barnett, Albert Einstein Medical Centre, United States
Copyright © 2025 Gundersen, Holmøy, Eide and Winther. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia K. Gundersen, anVsaWFrZ3VuZGVyc2VuQGhvdG1haWwuY29t